From Data to Practice Change: Bringing Youth ADHD Evidence ......# of GA children (2-18 years)...
67
WORKSHOP LINDA MCCALL, L.C.S.W. DEPARTMENT OF COMMUNITY HEALTH ANGELA SNYDER, PH.D. GEORGIA STATE UNIVERSITY CENTER OF EXCELLENCE FOR CHILDREN’S BEHAVIORAL HEALTH WENDY WHITE TIEGREEN, M.S.W. DEPARTMENT OF BEHAVIORAL HEALTH & DEVELOPMENTAL DISABILITIES OCTOBER 2016 From Data to Practice Change: Bringing Youth ADHD Evidence-Based Practice to Scale
Transcript of From Data to Practice Change: Bringing Youth ADHD Evidence ......# of GA children (2-18 years)...
W O R K S H O P
L I N D A M C C A L L , L . C . S . W .D E P A R T M E N T O F C O M M U N I T Y H E A L T H
A N G E L A S N Y D E R , P H . D .G E O R G I A S T A T E U N I V E R S I T Y
C E N T E R O F E X C E L L E N C E F O R C H I L D R E N ’ S B E H A V I O R A L H E A L T H
W E N D Y W H I T E T I E G R E E N , M . S . W .D E P A R T M E N T O F B E H A V I O R A L H E A L T H & D E V E L O P M E N T A L D I S A B I L I T I E S
O C T O B E R 2 0 1 6
From Data to Practice Change: Bringing Youth ADHD Evidence-Based
Practice to Scale
2Georgia Department of Behavioral Health and Developmental Disabilities
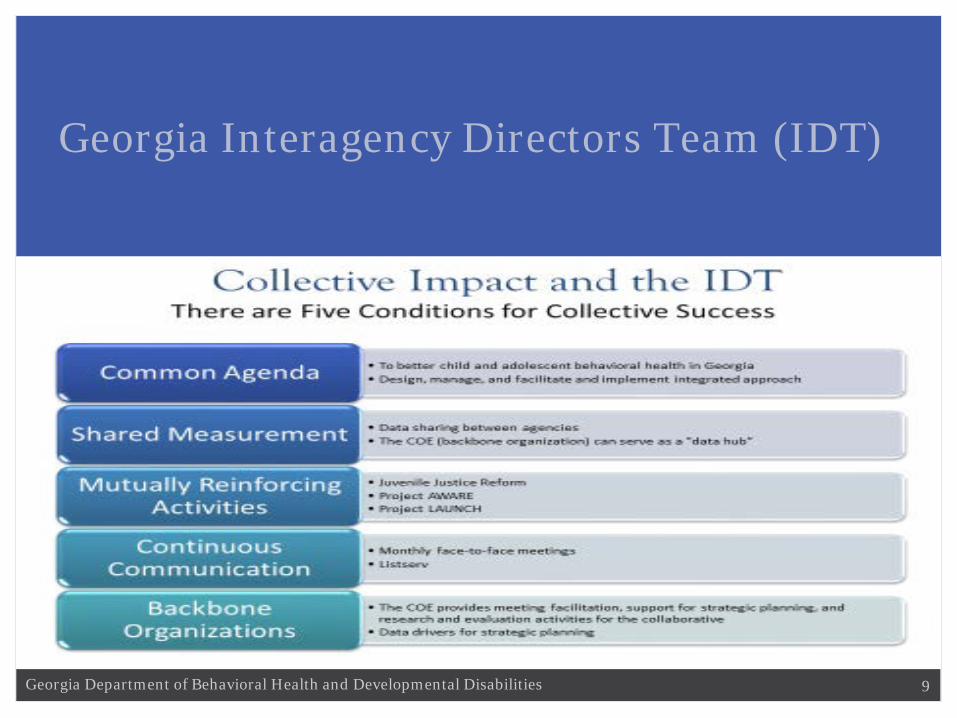
Georgia Interagency Directors Team (IDT)
3Georgia Department of Behavioral Health and Developmental Disabilities
Georgia Interagency Directors Team (IDT)
4Georgia Department of Behavioral Health and Developmental Disabilities
Georgia Interagency Directors Team (IDT)
5Georgia Department of Behavioral Health and Developmental Disabilities
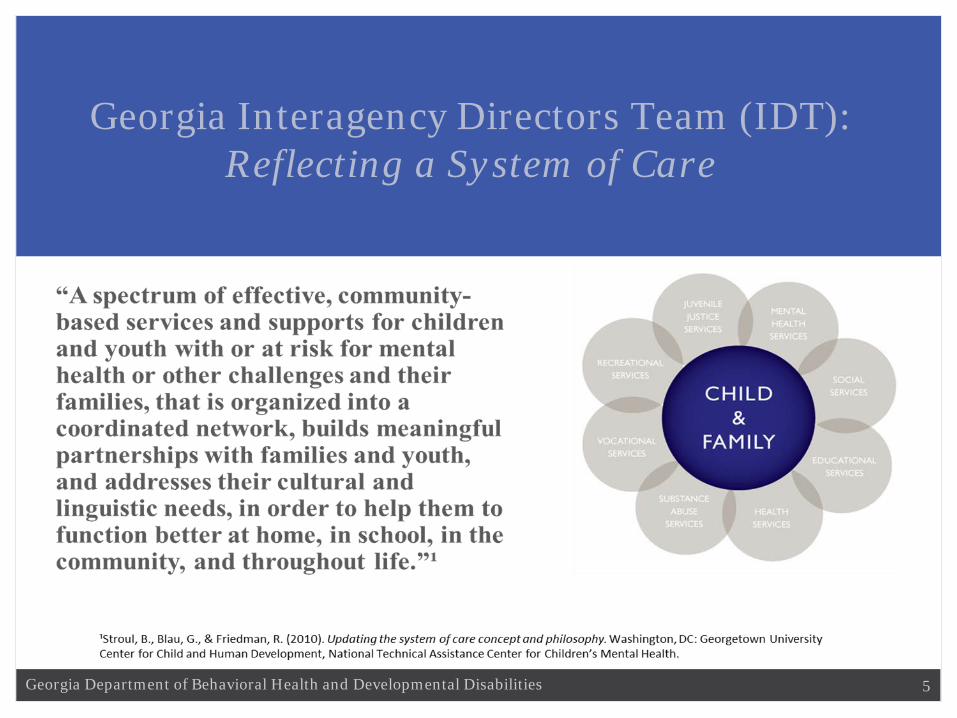
Georgia Interagency Directors Team (IDT):Reflecting a System of Care
6Georgia Department of Behavioral Health and Developmental Disabilities
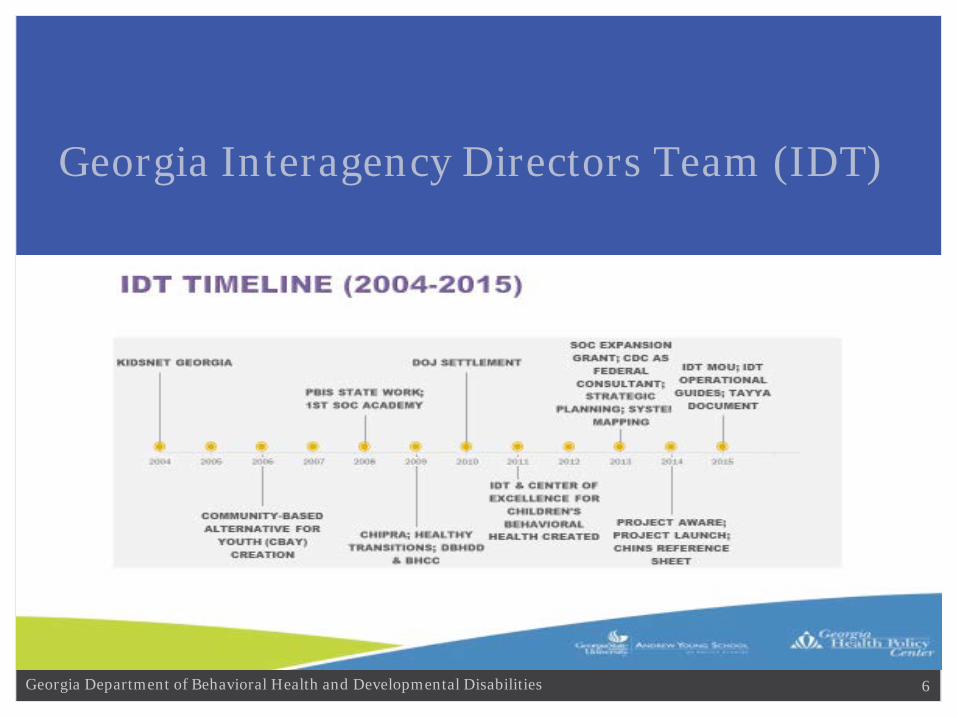
Georgia Interagency Directors Team (IDT)

7Georgia Department of Behavioral Health and Developmental Disabilities
Georgia Interagency Directors Team (IDT)

8Georgia Department of Behavioral Health and Developmental Disabilities
Georgia Interagency Directors Team (IDT)
9Georgia Department of Behavioral Health and Developmental Disabilities
Georgia Interagency Directors Team (IDT)

10Georgia Department of Behavioral Health and Developmental Disabilities
Prevalence of ADHD among School-Aged Youth
National Population Estimates 6.4 million youth 4-17 years diagnosed as of 2011-20122 million more than in 2003
5.1 million with a current ADHD diagnosis
National Prevalence Rate (%) 11% of youth 4-17 years of age ever diagnosedUp from 7.8% in 2003-2004; a 42% increase
8.8% with a current diagosis
Visser, S. N., Danielson, M. L., Bitsko, R. H., Holbrook, J. R., Kogan, M. D., Ghandour, R. M., . . . Blumberg, S. J. (2014).Trends in the Parent-Report of Health Care Provider-Diagnosed and Medicated Attention-Deficit/Hyperactivity Disorder: United States, 2003–2011. Journal of the American Academy of Child and Adolescent Psychiatry, 53(1), 34-46.e32.

11Georgia Department of Behavioral Health and Developmental Disabilities
0
2
4
6
8
10
12
1998 2000 2002 2004 2006 2008 2010 2012 2014
Pre
vale
nce
est
imat
e (%
)
Year
Diagnosed ADHD Prevalence Estimates: National Survey Data
National Survey of Children's Health
National HealthInterview Survey

0% 5% 10% 15% 20% 25%
4567891011121314151617
Girls
Current ADHDdiagnosis andtaking medication
Current ADHDdiagnosis but nottaking medication
Ever had ADHDdiagnosis but notcurrent ADHD
0%5%10%15%20%25%
Boys
2011-2012
Age in years
Weighted Prevalence Estimates (%) of Attention-Deficit/Hyperactivity Disorder (ADHD) Diagnosis by a Health Care Provider among U.S. Children, by Age and Medication Status
Parent-Reported Data from the National Survey of Children’s Health
Visser, S. N., Danielson, M. L., Bitsko, R. H., Holbrook, J. R., Kogan, M. D., Ghandour, R. M., . . . Blumberg, S. J. (2014). Trends in the Parent-Report of Health Care Provider-Diagnosed and Medicated Attention-Deficit/Hyperactivity Disorder: United States, 2003–2011. Journal of the American Academy of Child and Adolescent Psychiatry, 53(1), 34-46.e32.

13Georgia Department of Behavioral Health and Developmental Disabilities
WHAT DO WE KNOW ABOUT ADHD
DIAGNOSIS AND TREATMENT IN
GEORGIA?

14Georgia Department of Behavioral Health and Developmental Disabilities
Current ADHD Diagnosis: United States, 2011-12
National Average: 8.8%
9.3%
15Georgia Department of Behavioral Health and Developmental Disabilities
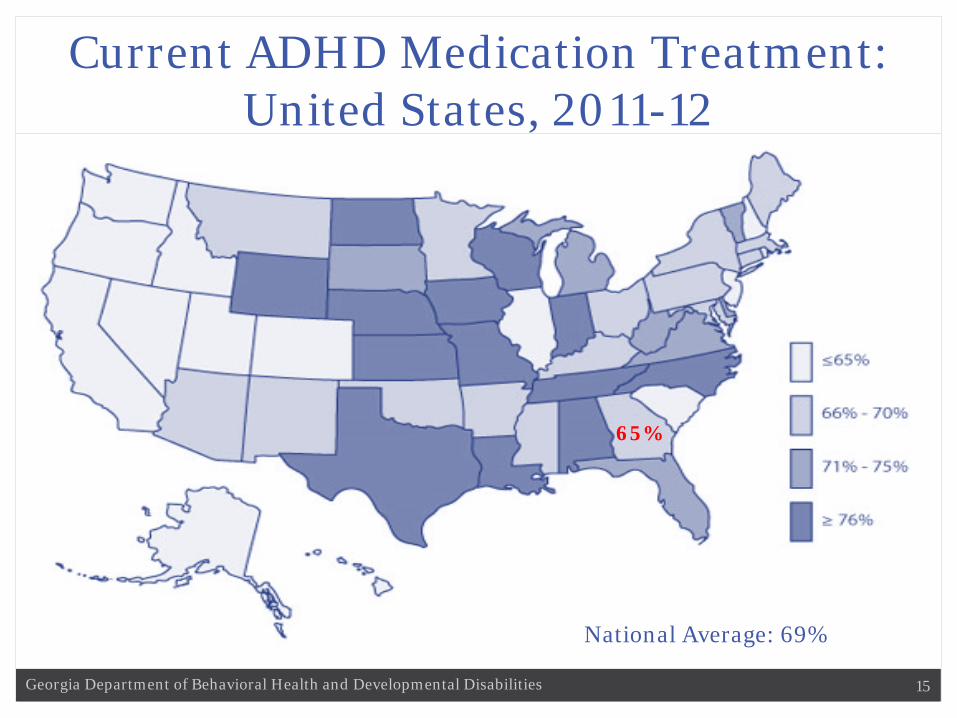
Current ADHD Medication Treatment: United States, 2011-12
National Average: 69%
65%

Diagnosed and Medicated ADHD in GA
7.8%
9.5%
11.0%9.4%
9.2%
12.1%
0%2%4%6%8%
10%12%14%16%18%20%
2003 2007 2011
% R
epor
ting
ADH
D
Ever Diagnosed: GA
US Georgia
In 2011, 8.8% of US children and 9.3% of children in GA had current ADHD, by parent report.
9.3%
Among all US states, GA ranked 25th highest.
In 2011, 6.1% of US children and 6.1% of children in GA were taking medication for ADHD.
6.1%
Among all US states, GA ranked 30th highest.

17Georgia Department of Behavioral Health and Developmental Disabilities
IDT COLLABORATION
GA MEDICAID DATA ANALYSES

18Georgia Department of Behavioral Health and Developmental Disabilities
Medicaid Claims Data System
Medically managed ADHD (2012-2014) # of GA children (2-18 years) enrolled in
Medicaid with >= 1 ADHD Dx codes by year % of children in Medicaid who had medically managed ADHD by year
Medicated ADHD (2012-2014) # of GA children (2-18 years) enrolled in Medicaid with >= 1 ADHD Dx code
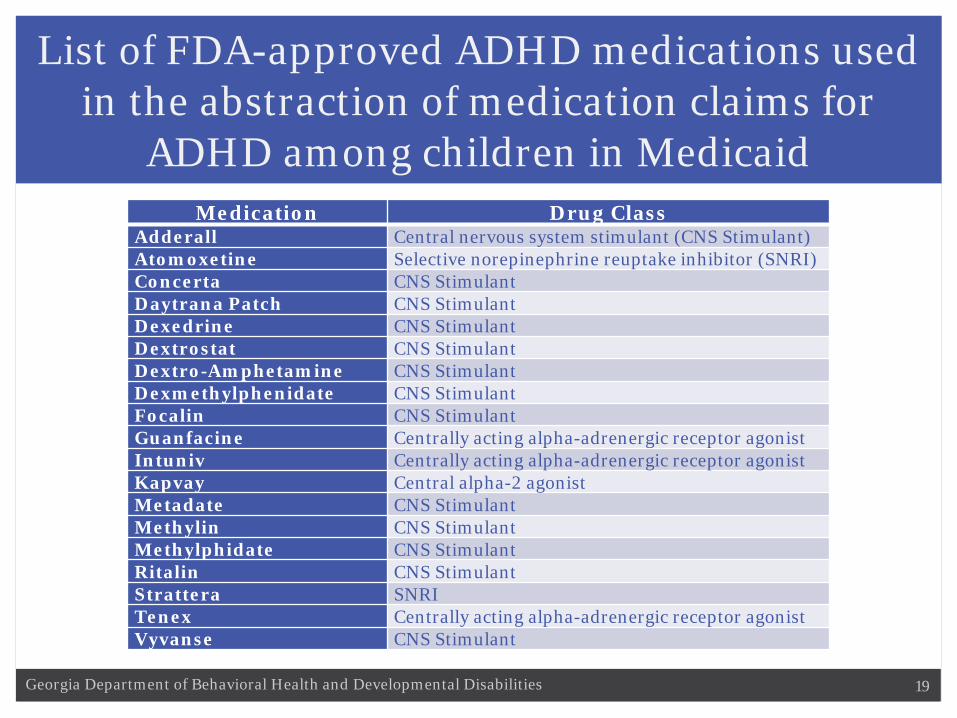
and >= 1 ADHD medication claim, using National Drug Codes for medications FDA-approved for pediatric ADHD treatment*
% of children in Medicaid with ADHD who received medication by year
Behavioral Treatment (2012-2014) # of GA children (2-18 years) enrolled in Medicaid who have received
behavioral treatment or psychological services by year % of children in Medicaid with ADHD receiving behavioral therapy by year
* AAP Subcommittee on Attention-Deficit/Hyperactivity Disorder Steering Committee on Quality Improvement and Management, Wolraich M, Brown L, et al. ADHD: Clinical Practice Guideline for the Diagnosis, Evaluation, and Treatment of Attention-Deficit/Hyperactivity Disorder in Children and Adolescents. Pediatrics. 2011; 128(5):1007-1022.
19Georgia Department of Behavioral Health and Developmental Disabilities
List of FDA-approved ADHD medications used in the abstraction of medication claims for
ADHD among children in MedicaidMedication Drug Class
Adderall Central nervous system stimulant (CNS Stimulant)Atomoxetine Selective norepinephrine reuptake inhibitor (SNRI)Concerta CNS StimulantDaytrana Patch CNS StimulantDexedrine CNS StimulantDextrostat CNS StimulantDextro-Amphetamine CNS StimulantDexmethylphenidate CNS StimulantFocalin CNS StimulantGuanfacine Centrally acting alpha-adrenergic receptor agonistIntuniv Centrally acting alpha-adrenergic receptor agonistKapvay Central alpha-2 agonistMetadate CNS StimulantMethylin CNS StimulantMethylphidate CNS StimulantRitalin CNS StimulantStrattera SNRITenex Centrally acting alpha-adrenergic receptor agonistVyvanse CNS Stimulant
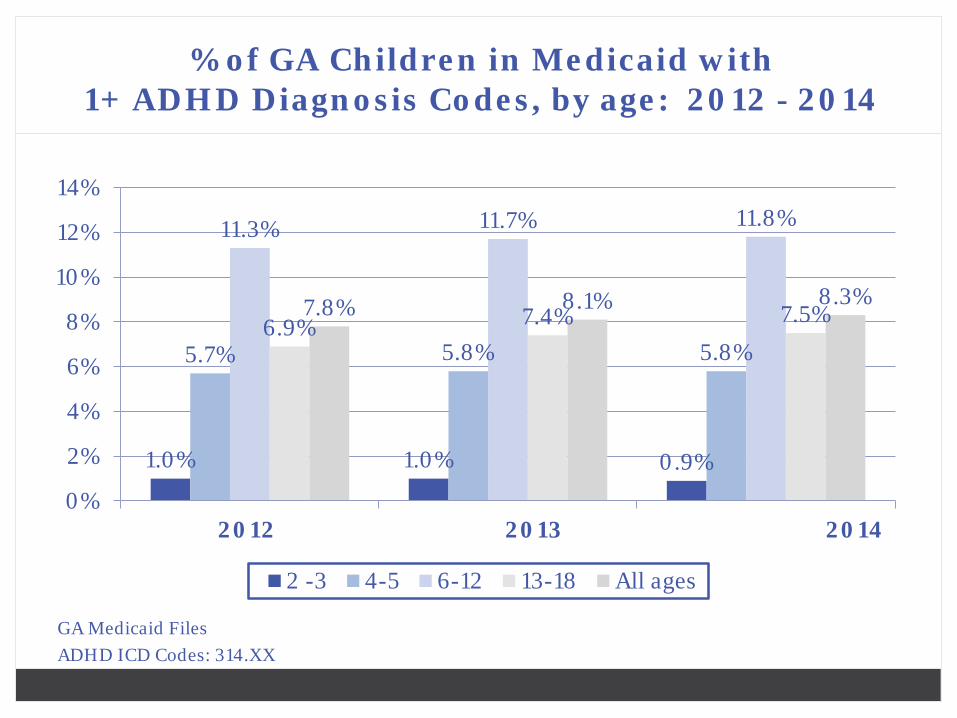
% of GA Children in Medicaid with 1+ ADHD Diagnosis Codes, by age: 2012 - 2014
GA Medicaid FilesADHD ICD Codes: 314.XX
1.0% 1.0% 0.9%
5.7% 5.8% 5.8%
11.3% 11.7% 11.8%
6.9% 7.4% 7.5%7.8% 8.1% 8.3%
0%
2%
4%
6%
8%
10%
12%
14%
2012 2013 2014
2 -3 4-5 6-12 13-18 All ages
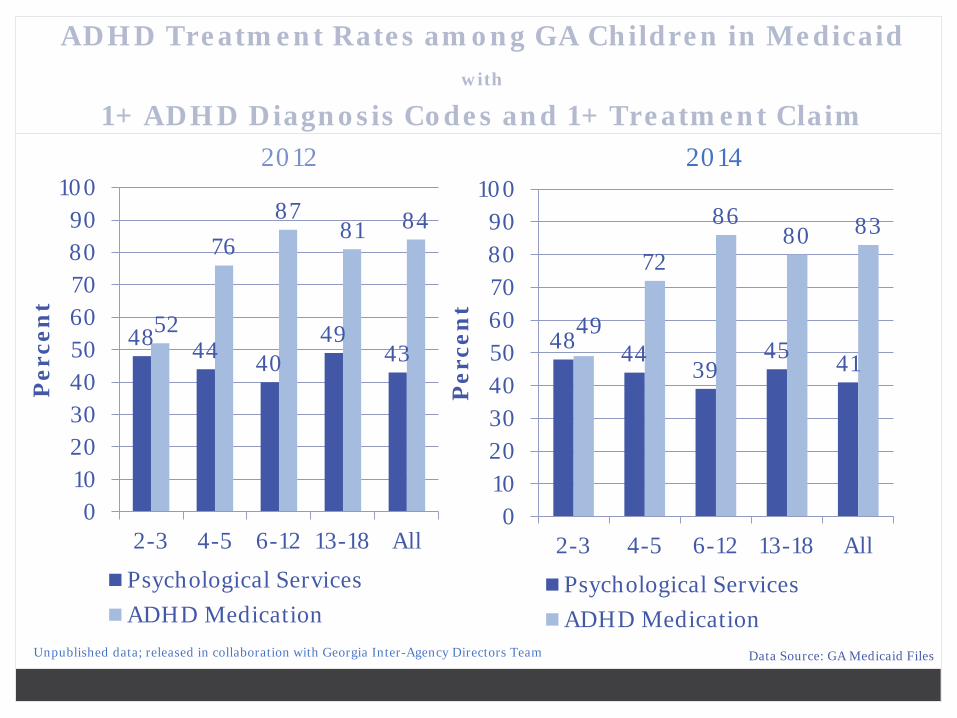
ADHD Treatment Rates among GA Children in Medicaid with
1+ ADHD Diagnosis Codes and 1+ Treatment Claim
48 44 4049
4352
7687
81 84
0102030405060708090
100
2-3 4-5 6-12 13-18 All
Per
cen
t
Psychological ServicesADHD Medication
48 4439
45 41
49
72
8680 83
0102030405060708090
100
2-3 4-5 6-12 13-18 All
Per
cen
t
Psychological ServicesADHD Medication
Unpublished data; released in collaboration with Georgia Inter-Agency Directors Team
2012 2014
Data Source: GA Medicaid Files

22Georgia Department of Behavioral Health and Developmental Disabilities
ADHD Treatment among GA Toddlers
T H E R E A R E N O C U R R E N T G U I D E L I N E S T H A T G U I D E T H E D I A G N O S I S A N D T R E A T M E N T O F A D H D A M O N G C H I L D R E N U N D E R 4 Y E A R S O F A G E
• In GA, about 1% of 2-3 year olds in Medicaid had an ADHD diagnosis code
• 48% had a behavioral therapy claim, while 52% had a medication claim in 2012
• Only amphetamine and d-amphetamine is FDA-approved for ADHD treatment for children as young as 3 years of age
• Valid diagnosis of ADHD in a toddler is not supported by evidence.T H E S E M E D I C A T I O N T R E A T M E N T P A T T E R N S A R E N O T U N I Q U E T O G E O R G I A

23Georgia Department of Behavioral Health and Developmental Disabilities
National MarketScan Database: PathwaysUS: ADHD Diagnosis and Medication Treatment
among 2-3 Year Olds (Private Claims)
* Among a MarketScan sample of 10,000,000 individuals
38.8%34.4% 37.9%
31.2%37.7%
0.29%0.25%
0.27% 0.27%0.24%
0.00%
0.10%
0.20%
0.30%
0.40%
0.50%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2008 2009 2010 2011 2012
Per
cen
t of
2-3
Yea
r O
lds
wit
h A
DH
D
Dx
Per
cen
tage
of
AD
HD
Med
icat
ed
ADHD Meds among Dx (%) ADHD Dx (%)
Implications
In 2012, approximately 1,660 toddlers in GA were being medically managed for ADHD in GA and about 760 of these had a claim for ADHD medication (class II controlled substances)
Only about 43% of all children 2-18 with an ADHD Dx code had a behavioral therapy/psych claim in 2012
Data suggest areas for quality improvement in GA and beyond, particularly among toddlers and preschoolers
Additional research and investigation is needed Education about AAP best practices Investigation of coding practices Investigation of the infrastructure for the provision of behavioral
therapy

25Georgia Department of Behavioral Health and Developmental Disabilities
M U C H L I K E T H E I D T C O N S I D E R E D …
Participant Interaction 1
…seeing this data, what are challenges?
26Georgia Department of Behavioral Health and Developmental Disabilities
SHARE
Participant Interaction 1

27Georgia Department of Behavioral Health and Developmental Disabilities
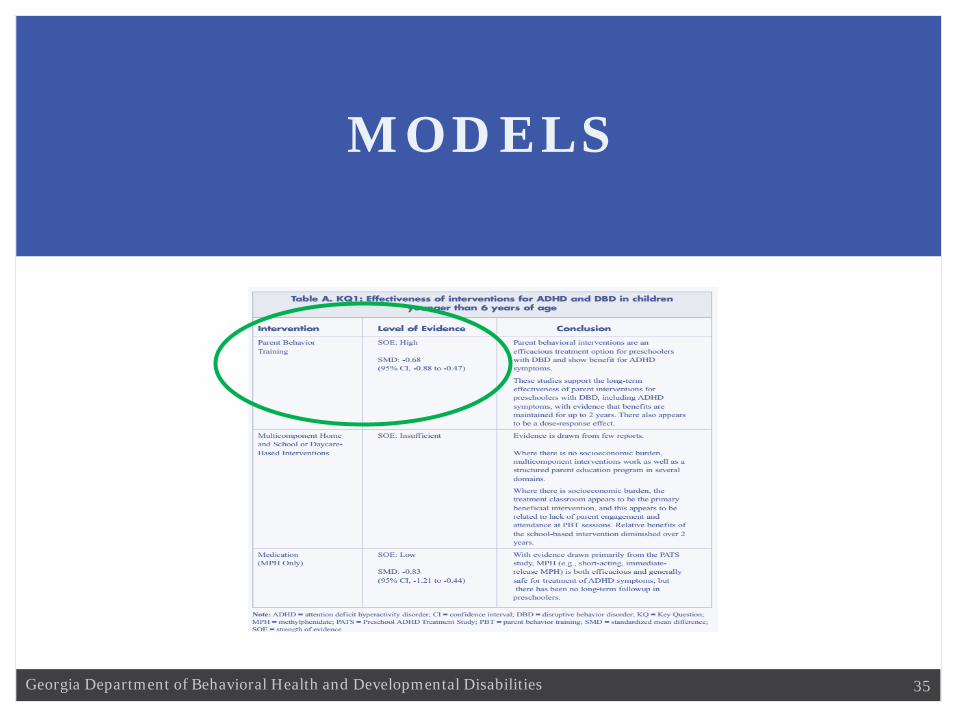
28Georgia Department of Behavioral Health and Developmental DisabilitiesAHRQ, 2011

29Georgia Department of Behavioral Health and Developmental Disabilities
Refer parents of young children with ADHD for training in behavior therapy
before prescribing medicine (CDC-Vital Signs and AAP)
Steps for healthcare providers
1. Assess a young child with ADHD symptoms using clinical practice guidelines (CDC) Evaluate anyone with academic or behavioral problems and symptoms
of inattention, hyperactivity, or impulsivity [AAP] Determine whether DSM criteria have been met (Ruling out other
causes, based on reports from parents and other supportive sources, etc.) [AAP]
Assess comorbidities [AAP] Recognize ADHD as a chronic condition [AAP]
30Georgia Department of Behavioral Health and Developmental Disabilities
Refer parents of young children with ADHD for training in behavior therapy
before prescribing medicine (CDC, Vital Signs)
Steps for healthcare providers
2. Talk with parents about ADHD treatment and explain the benefits of behavior therapy as the first line of treatment [CDC, AAP]
a. Improved behavior, self-control, and self-esteem for children. b. Better relationships and reduced stress for families.c. Benefits are lifelong for children and families.

31Georgia Department of Behavioral Health and Developmental Disabilities
CDC

32Georgia Department of Behavioral Health and Developmental Disabilities

33Georgia Department of Behavioral Health and Developmental Disabilities
Refer parents of young children with ADHD for training in behavior therapy
before prescribing medicine (CDC, Vital Signs)
Steps for healthcare providers
3. Refer parents to a therapist before prescribing medicine. Find a therapist who:
a. Teaches parents to better manage their child’s behavior and strengthen parent-child relationship.
b. Encourages parents to practice between sessions, regularly monitors progress, and adjusts strategies as needed.
34Georgia Department of Behavioral Health and Developmental Disabilities
Refer parents of young children with ADHD for training in behavior therapy
before prescribing medicine (CDC, Vital Signs)
Steps for healthcare providers
4. Follow up with the family during and after treatment to confirm progress.
35Georgia Department of Behavioral Health and Developmental Disabilities
MODELS
36Georgia Department of Behavioral Health and Developmental Disabilities
MODELS
Incredible Years Parenting Program
Parent Child Interaction
TherapyNew Forest Parenting
Programme
Triple P: Positive
Parenting Program

37Georgia Department of Behavioral Health and Developmental Disabilities
• T r a i n s p a r e n t s v a r i o u s s t r a t e g i e s t o h e l p c h i l d r e n r e g u l a t e t h e i r e m o t i o n s , i m p r o v e t h e i r s o c i a l s k i l l s , a n d d o b e t t e r a c a d e m i c a l l y .
• P a r e n t s a r e g i v e n o p p o r t u n i t i e s t o c o l l e c t i v e l y a n d i n d i v i d u a l l y d e v e l o p n e w s t r a t e g i e s f o r m a n a g i n g t h e i r c h i l d r e n a n d w o r k i n g t o g e t h e r i n c o l l a b o r a t i v e p a r t n e r s h i p s .
• C h i l d r e n r e c e i v e t r a i n i n g i n h o w t o f o l l o w r u l e s a n d c o o p e r a t e , e x p r e s s e m o t i o n s , p r o b l e m - s o l v e , m a n a g e a n g e r , a n d m a k e g o o d f r i e n d s .
• G r o u p a n d I n d i v i d u a l m o d e s o f d e l i v e r y
Incredible Years Parenting Program

38Georgia Department of Behavioral Health and Developmental Disabilities
E m p h a s i z e s p a r e n t i n g s k i l l s k n o w n t o p r o m o t e c h i l d r e n ' s s o c i a l c o m p e t e n c e a n d r e d u c e b e h a v i o r p r o b l e m s s u c h a s :
• how to play with children, • social, emotional , academic and persistence skills coaching, • effective praise and use of incentives, • establishing predictable routines and rules and promoting responsibility, • effective limit-setting, • strategies to manage behavior,• teaching children to problem solve. • effective communication skills, • anger and depression management, • problem-solving between adults, • ways to give and get support • approaches designed to promote children’s academic skills.
Incredible Years Parenting Program

39Georgia Department of Behavioral Health and Developmental Disabilities
Incredible Years Parenting Program

40Georgia Department of Behavioral Health and Developmental Disabilities
Parent
Child
Family

41Georgia Department of Behavioral Health and Developmental Disabilities
Incredible Years Parenting Program
COMMUNITY SUPPORTS: Skills Development; Skills Acquisition for Managing Behavior; Skills/Strategies for personal development, school performance, work performance, and functioning; Enhancing social and coping skills; etc.
FAMILY TRAINING: development of methods of intervention, interaction and mutual support the family can use to assist their family member; symptom management; behavioral management; Adaptive behaviors and skills; Interpersonal skills, etc.
GROUP TRAINING: development of methods of intervention, interaction and mutual support the family can use to assist their family member; symptom management; behavioral management; Adaptive skills; Interpersonal skills, etc.

42Georgia Department of Behavioral Health and Developmental Disabilities
• An evidence-based treatment for young chi ldren with emotional and behavioral disorders
• Places emphasis on improving the qual i ty of the parent-chi ld relat ionship and changing parent-chi ld interact ion patterns.
Parent Child Interaction Therapy

43Georgia Department of Behavioral Health and Developmental Disabilities
A P P R O A C H :
• C h i l d r e n a n d t h e i r c a r e g i v e r s a r e s e e n t o g e t h e r i n P C I T . • M o s t o f t h e s e s s i o n t i m e i s s p e n t c o a c h i n g c a r e g i v e r s i n
t h e a p p l i c a t i o n o f s p e c i f i c t h e r a p e u t i c s k i l l s . • T h e r a p i s t s t y p i c a l l y c o a c h f r o m a n o b s e r v a t i o n r o o m w i t h
a o n e - w a y m i r r o r i n t o t h e p l a y r o o m , u s i n g a “ b u g - i n - t h e -e a r ” s y s t e m f o r c o m m u n i c a t i n g t o t h e p a r e n t s a s t h e y p l a y w i t h t h e i r c h i l d .
• C o n c l u d i n g e a c h s e s s i o n , t h e r a p i s t a n d c a r e g i v e r t o g e t h e r d e c i d e w h i c h s k i l l t o f o c u s o n m o s t d u r i n g d a i l y 5 - m i n u t e h o m e p r a c t i c e s e s s i o n s t h e f o l l o w i n g w e e k .
Parent Child Interaction Therapy

44Georgia Department of Behavioral Health and Developmental Disabilities
Parent Child Interaction Therapy
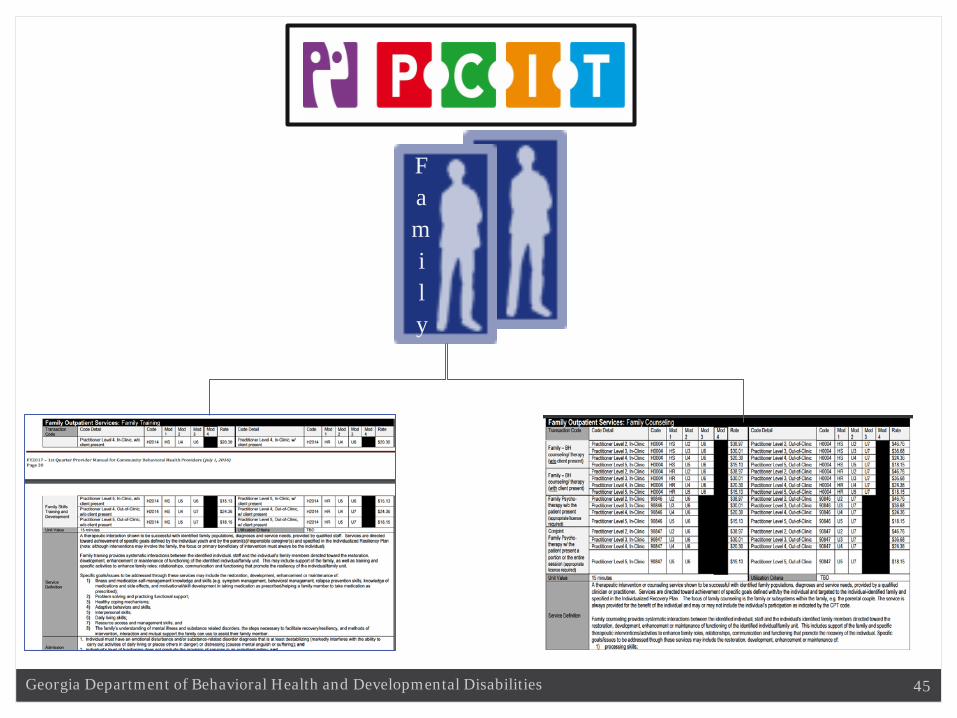
45Georgia Department of Behavioral Health and Developmental Disabilities
Family
46Georgia Department of Behavioral Health and Developmental Disabilities
Incredible Years Parenting Program
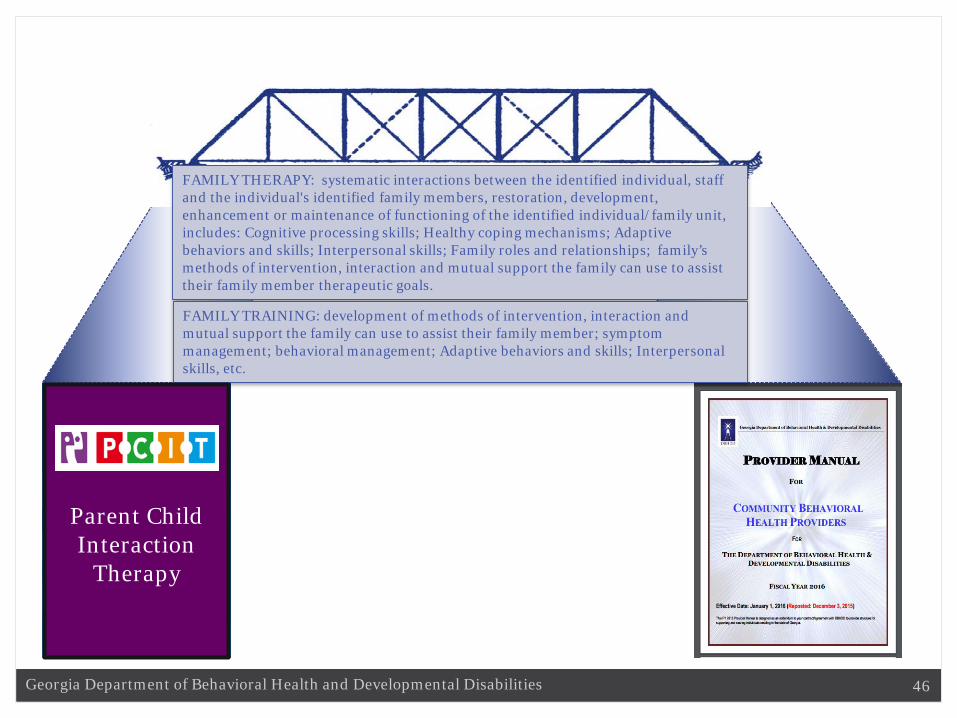
FAMILY THERAPY: systematic interactions between the identified individual, staff and the individual's identified family members, restoration, development, enhancement or maintenance of functioning of the identified individual/family unit, includes: Cognitive processing skills; Healthy coping mechanisms; Adaptive behaviors and skills; Interpersonal skills; Family roles and relationships; family’s methods of intervention, interaction and mutual support the family can use to assist their family member therapeutic goals.
FAMILY TRAINING: development of methods of intervention, interaction and mutual support the family can use to assist their family member; symptom management; behavioral management; Adaptive behaviors and skills; Interpersonal skills, etc.
Parent Child Interaction
Therapy
47Georgia Department of Behavioral Health and Developmental Disabilities
• T a r g e t s y o u t h a g e s 3 - 1 1 w i t h m o d e r a t e t o s e v e r e s y m p t o m s o f A D H D
• T a k e s p l a c e i n t h e f a m i l y ’ s h o m e t h r o u g h e i g h t w e e k l y v i s i t s .
• Each session lasts two hours and is either for the parent only (four sessions) or the parent and child together.
• Single Practitioner Intervention• During these visits, parents learn strategies for managing their
children’s behavior and difficulties with attention.
New Forest Parenting Programme (NFPP)
48Georgia Department of Behavioral Health and Developmental Disabilities
W H A T H A P P E N S D U R I N G T H E I N T E R V E N T I O N ?
• P a r e n t s l e a r n a b o u t t h e n a t u r e o f A D H D a n d h o w t o m a n a g e t h e i r c h i l d ’ s b e h a v i o r t h r o u g h g a m e s t h a t e n g a g e c h i l d r e n ’ s a t t e n t i o n , e n c o u r a g e t h e i r p a t i e n c e a n d i n c r e a s e t h e i r c o n c e n t r a t i o n .
• T h e p r a c t i t i o n e r o b s e r v e s t h e p a r e n t a n d c h i l d p l a y i n g t h e g a m e t o g e t h e r a n d p r o v i d e s f e e d b a c k o n t h e q u a l i t y o f t h e i r i n t e r a c t i o n .
New Forest Parenting Programme (NFPP)

49Georgia Department of Behavioral Health and Developmental Disabilities
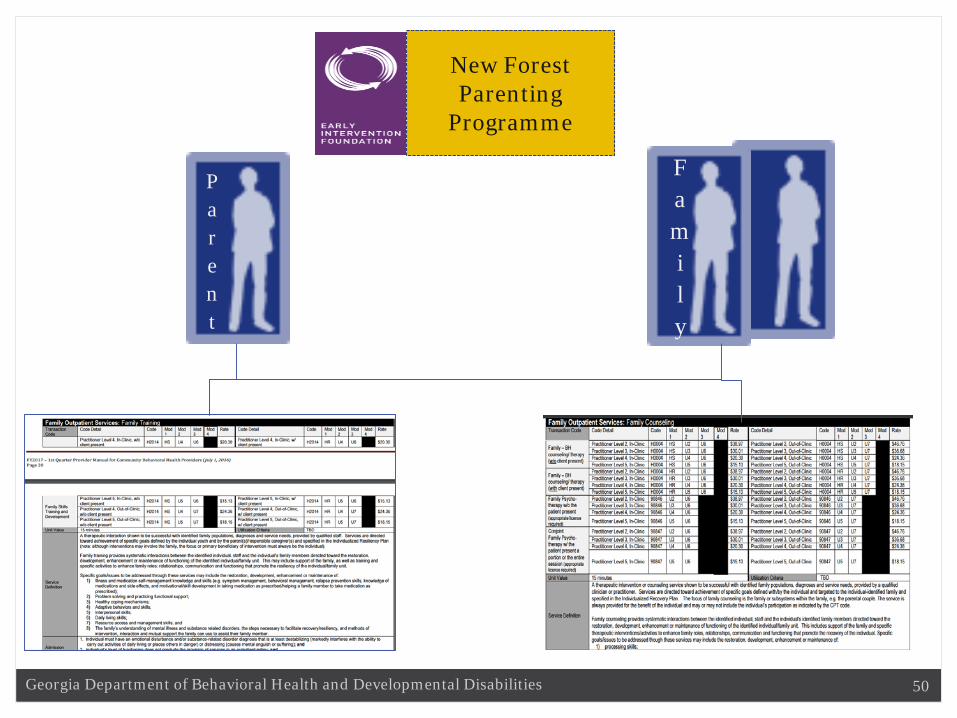
New Forest Parenting
Programme
50Georgia Department of Behavioral Health and Developmental Disabilities
Parent
Family
New Forest Parenting
Programme

51Georgia Department of Behavioral Health and Developmental Disabilities
Incredible Years Parenting Program
FAMILY THERAPY: systematic interactions between the identified individual, staff and the individual's identified family members, restoration, development, enhancement or maintenance of functioning of the identified individual/family unit, includes: Cognitive processing skills; Healthy coping mechanisms; Adaptive behaviors and skills; Interpersonal skills; Family roles and relationships; family’s methods of intervention, interaction and mutual support the family can use to assist their family member therapeutic goals.
FAMILY TRAINING: development of methods of intervention, interaction and mutual support the family can use to assist their family member; symptom management; behavioral management; Adaptive behaviors and skills; Interpersonal skills, etc.
New Forest Parenting
Programme

52Georgia Department of Behavioral Health and Developmental Disabilities
Triple P: Positive Parenting Program
Levels Modality1 Public Health Approach2 Direct Family Intervention3 Direct Family Intervention4 Direct Family Intervention5 Direct Family Intervention

53Georgia Department of Behavioral Health and Developmental Disabilities
Triple P: Positive Parenting Program
Levels Modality
1 Public Health Approach
2 Direct Family Intervention
3 Direct Family Intervention
4 Direct Family Intervention
5 Direct Family Intervention
“Stay Positive”

54Georgia Department of Behavioral Health and Developmental Disabilities
Triple P: Positive Parenting Program
Levels Modality
1 Public Health Approach
2 Direct Family Intervention
3 Direct Family Intervention
4 Direct Family Intervention
5 Direct Family Intervention
• "light touch" intervention• provides one-time assistance to parents who are
generally coping well but have 1-2 concerns with their child's behavior or development
• Seminar or brief consultation

55Georgia Department of Behavioral Health and Developmental Disabilities
Triple P: Positive Parenting ProgramLevels Modality
1 Public Health Approach
2 Direct Family Intervention
3 Direct Family Intervention
4 Direct Family Intervention
5 Direct Family Intervention
• Targeted counseling for parents of a child with mild to moderate behavioral difficulties
• Deal with a specific problem behavior or issue• One-on-One Modality: Brief face-to-face or telephone
intervention • Group Modality: Two-hour small group sessions, targeting a
specific problem behavior or issue.

56Georgia Department of Behavioral Health and Developmental Disabilities
Triple P: Positive Parenting ProgramLevels Modality
1 Public Health Approach
2 Direct Family Intervention
3 Direct Family Intervention
4 Direct Family Intervention
5 Direct Family Intervention
• Promotes core positive parenting skills that can be adapted to a wide range of parenting situations.
• Variety of service delivery modalities:• Group– Groups of no more than 12 parents attend five sessions and supported
with three phone counseling/catch-up sessions at home. • Individual counseling- Delivered over ten (1 hour) sessions. • Online – Eight-session web-based program that guides parents through Triple
P's 17 core parenting skills• Self-directed– A ten week workbook self-help program, Parents who need
additional support can receive weekly 15–30 minute telephone consultations.
• For parents of children with more behavioral difficulties
57Georgia Department of Behavioral Health and Developmental Disabilities
Triple P: Positive Parenting ProgramLevels Modality
1 Public Health Approach
2 Direct Family Intervention
3 Direct Family Intervention
4 Direct Family Intervention
5 Direct Family Intervention
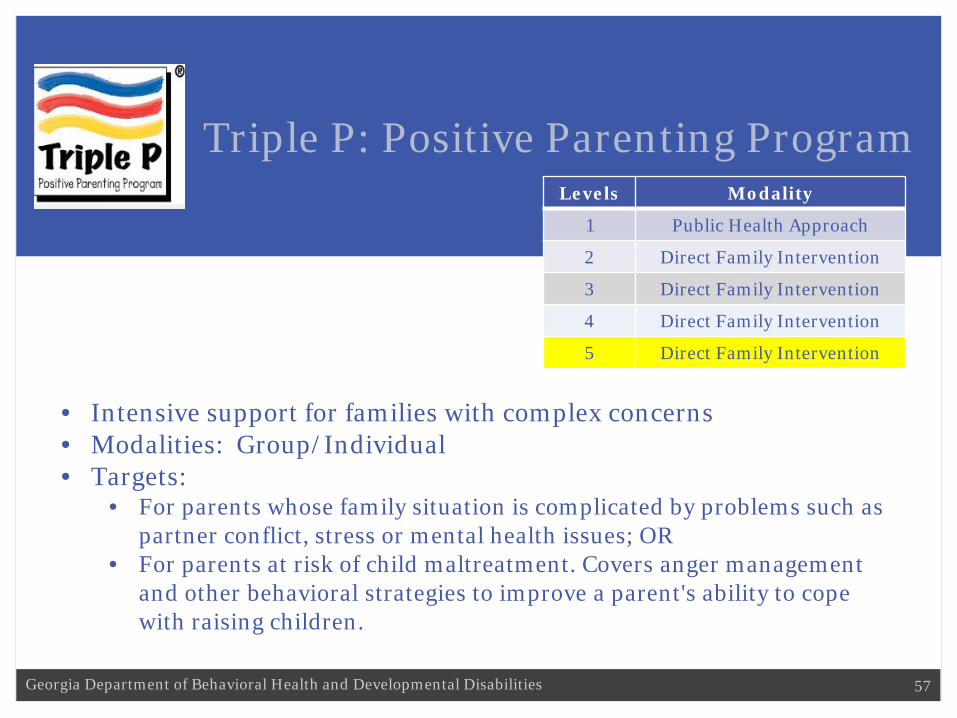
• Intensive support for families with complex concerns• Modalities: Group/Individual• Targets:
• For parents whose family situation is complicated by problems such as partner conflict, stress or mental health issues; OR
• For parents at risk of child maltreatment. Covers anger management and other behavioral strategies to improve a parent's ability to cope with raising children.
58Georgia Department of Behavioral Health and Developmental Disabilities
Triple P: Positive Parenting Program
59Georgia Department of Behavioral Health and Developmental Disabilities
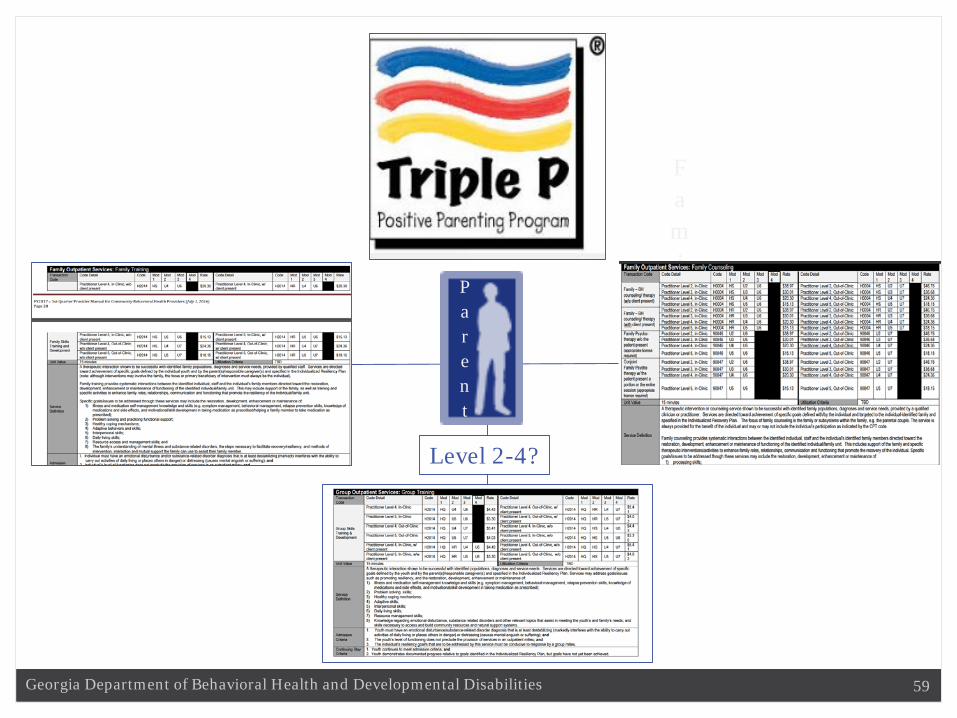
Parent
Family
Level 2-4?
60Georgia Department of Behavioral Health and Developmental Disabilities
COMMON ELEMENTS?
Trends

61Georgia Department of Behavioral Health and Developmental Disabilities
Participant Interaction 2
BASED ON THIS INFORMATION, WHAT ARE 3
CHANGES THAT YOU PROPOSE TO MAKE IN YOUR
UNIQUE SETTING?
62Georgia Department of Behavioral Health and Developmental Disabilities
SHARE
Participant Interaction 2

63Georgia Department of Behavioral Health and Developmental Disabilities
Participant Interaction 3
WHAT ARE TWO WAYS TO GET BUY-IN FROM YOUR
AGENCY LEADERSHIP ON ACCOMPLISHING YOUR
NAMED GOALS?
64Georgia Department of Behavioral Health and Developmental Disabilities
SHARE
Participant Interaction 3
65Georgia Department of Behavioral Health and Developmental Disabilities
Next Steps
• Consideration Of Alternative ADHD Strategies (UR Analysis, PBM Controls, Etc.)
• Statewide Practitioner Survey• CEU Webinars• Provider/Practitioner Registry

66Georgia Department of Behavioral Health and Developmental Disabilities
Resources and References
ADHD in Young Children, http://www.cdc.gov/vitalsigns/pdf/2016-05-vitalsigns.pdf, Publication date: 05/03/2016, accessed August 30, 2016.
American Academy of Pediatrics' Subcommittee on Attention-Deficit/Hyperactivity Disorder Steering Committee on Quality Improvement and Management, Wolraich M, Brown L, et al. ADHD: Clinical Practice Guideline for the Diagnosis, Evaluation, and Treatment of Attention-Deficit/Hyperactivity Disorder in Children and Adolescents. Pediatrics. November 1, 2011 2011;128(5):1007-1022.
Attention-Deficit/Hyperactivity Disorder (ADHD): Behavior therapy for young children with ADHD, Centers for Disease Control and Prevention, http://www.cdc.gov/ncbddd/adhd/behavior-therapy.html, accessed June 20, 2016.
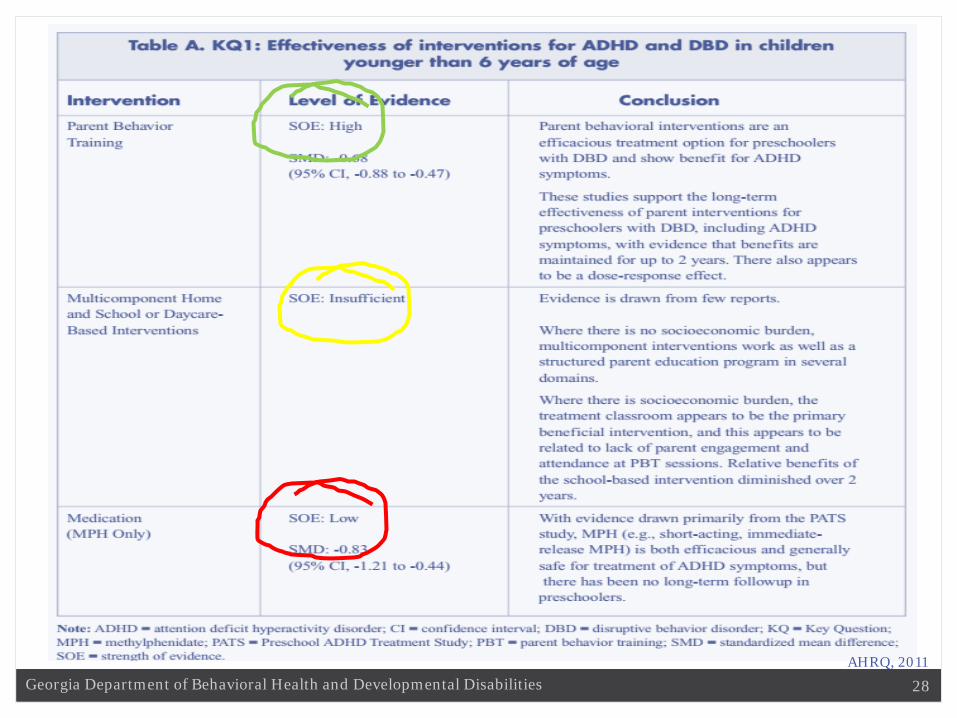
Attention Deficit Hyperactivity Disorder: Effectiveness of Treatment in At-Risk Preschoolers; Long-Term Effectiveness in All Ages; and Variability in Prevalence, Diagnosis, and Treatment, Agency for Healthcare Research and Quality, Comparative Effectiveness Review Number 44, Pun No. 12-EHC003-1, October 2011.
Georgia State University, Center of Excellence in Child & Adolescent Behavioral Health, Interagency Directors’ Team, http://gacoeonline.gsu.edu/idt/, Accessed September 19, 2016.
The Incredible Years, http://incredibleyears.com/, Accessed August 30, 2016.

67Georgia Department of Behavioral Health and Developmental Disabilities
Resources and References Visser, et.al. The State of ADHD Care in Georgia: From Data to Action, Georgia Mental
Health Forum, The Carter Center, May 16, 2014 Visser, et.al. Attention-Deficit/Hyperactivity Disorder among Preschoolers and Toddlers,
http://gacoeonline.gsu.edu/files/2014/05/SOC-Presentation_06-25-14_final2.pdf, June 2014.
Visser, S. N., Danielson, M. L., Bitsko, R. H., Holbrook, J. R., Kogan, M. D., Ghandour, et.al. (2014). Trends in the Parent-Report of Health Care Provider-Diagnosed and Medicated Attention-Deficit/Hyperactivity Disorder: United States, 2003–2011. Journal of the American Academy of Child and Adolescent Psychiatry, 53(1), 34-46.e32.
Parent-Child Interaction Therapy (PCIT), International, http://www.pcit.org/, Accessed September 30, 2016.
Stroul, B. A., Blau, G., & Friedman, R. (2010). Updating the System of Care concept and philosophy. Washington, D.C., Georgetown University Center for Child and Human Development National Technical Assistance Center for Children’s Mental Health.
The New Forest Parenting Programme, http://guidebook.eif.org.uk/programmes-library/new-forest-parenting-programme-nfpp, Accessed September 21, 2016.
Triple P, http://www.triplep-parenting.com/us-en/triple-p/, Accessed September 30, 2016.