Friends of MSF UK & Ireland 2011 AGM Report
27
…………………………………………………………………………………………………………………………………………………………… Friends of Médecins Sans Frontières UK & Ireland …………………………………………………………………………………………………………………………………………………………… AGM Report …………………………………………………………………………………………………………………………………………………………… 2011
-
Upload
friends-of-medecins-sans-frontieres-uk-and-ireland -
Category
Documents
-
view
223 -
download
1
description
London School of Hygiene and Tropical Medicine, June 18th, 2011
Transcript of Friends of MSF UK & Ireland 2011 AGM Report

AGM Report 2011
1
……………………………………………………………………………………………………………………………………………………………
Friends of Médecins Sans Frontières UK & Ireland ……………………………………………………………………………………………………………………………………………………………
AGM Report
……………………………………………………………………………………………………………………………………………………………
2011

AGM Report 2011
2
……………………………………………………………………………………………………………………………………………………………
Contents
1. Introduction - p3
2. Agenda - p4
3. Elected NC 2011-12 Profiles - p5 4. NC 2011-12 Position Descriptions - p8 5. Key Notes Speech – Katy Athersuch - p9
6. Key Notes Speech – Sid Wong - p10 7. Workshops
Jeroen Jansen - Sudan - Beyond Everyday News p11 Sid Wong - Refugee Health: Case studies from Uganda and Chad p12 Joel Cunningham and Pete Scolding - What is Humanitarianism Anyway? p15
8. An MSF Career – Plenary Q&A Session - p16
9. FoMSF Group Contact details - p20 10. Feedback - p22 Photos by Lucinda Wahlers

AGM Report 2011
3
……………………………………………………………………………………………………………………………………………………………
Introduction Dear all Welcome to the report on the Friends of MSF UK & Ireland 2011 Annual General Meeting (AGM). This year was the 5th such meeting since the original meeting held at King’s College London in 2007. The AGM was held at the London School of Hygiene and Tropical Medicine on June 18th, following the trend of previous years to hold the event in London. The London School of Hygiene and Tropical Medicine is a world leader in the postgraduate teaching and promotion of public and global health. The association with this institution reflects developments within Friends of MSF itself; with the growth of Friends of MSF International and the MSF-Hospital Links Initiative. This year differed from previous years with the AGM being held during the summer break, with more than 45 in attendance. The feedback during and following the event strongly indicated that the event was a resounding success On the day Like previous years, the morning session focused on Friends of MSF activity, national and international news and the election of the new National Committee. The afternoon session focused on MSF itself; with Sid Wong’s keynote speech 'The Challenges of 2010: Medecins Sans Frontieres in the UK' and workshops dealing with issues such as refugee health and MSF’s work in Sudan. The event was capped off with a panel discussion which had every member of the audience enthralled Thanks Thanks to everyone who helped with the running of the day from registration, note taking to cleanup. The National Committee offers a special thanks to Peter Siordet Scolding who acted as AGM coordinator. His tremendous efforts are an example to us all. Thanks to the MSF staff who volunteered their time and efforts. We thank you all who attended and helped to make the event success it was and we look forward to hearing from you over the coming year Alan Quinn President, Friends of MSF National Committee, 2011- Friends of MSF National Committee, 2010-2011

AGM Report 2011
4
……………………………………………………………………………………………………………………………………………………………
Agenda AM 10:00 – 10:05 – Welcome 10:05 – 10:55 – Key Notes Speech: ‘Campaigning for Access’ - Katy Athersuch, Medical Innovation & Access Policy Adviser, MSF's Campaign for Access to Essential Medicines 11:25 – 11:35 – National Committee (NC) 2010-11 Updates and National News 11:55 – 12:10 – NC 2011-12 Candidate presentations PM 13:15 – 13:20 – Election Results 13:20 – 14:10 – 'The Challenges of 2010: Medecins Sans Frontieres in the UK' - Key Notes Speech - Sid Wong, Public Health Advisor, Global Health team at the Department of Health; Chair of the Board of Directors, MSF-UK 14:20 – 15:40 – Workshops 1) ‘Sudan - Beyond Everyday News’ - Jeroen Jensen, Head of the Programmes Unit, MSF-UK 2) ‘Refugee Health: Case Studies from Uganda and Chad’ - Sid Wong, Public Health Advisor,
Global Health team, Department of Health; Chair of the Board of Directors, MSF-UK 3) ‘What is Humanitarianism Anyway?’ - Joel Cunningham and Peter Siordet Scolding,
Former Presidents of University College London FoMSF and the FoMSF National Committee 16:00 – 16:45 – Careers Panel and Q&A – Chaired by Polly Markandya, Head of Communications, MSF-UK, featuring Jeroen Jensen and Sid Wong. 16:45 – Closing Thoughts 17:00 – Late – Social

AGM Report 2011
5
……………………………………………………………………………………………………………………………………………………………
National Committee 2011-12 – Elected Candidates
The position of: President Name: Alan Quinn Subject: Medicine Year of Study: 3. Entering iBSc year University: University College Cork (UCC), Ireland Please tell us why you feel you should be elected to this position: I’ve been very actively involved with Friends of MSF for the past 3 years. I initially became involved in 1st year by becoming a year rep in Cork, which was the only active FoMSF group in Ireland at that time. I went on to become the President of the Cork group the following year. During my time as President I helped to transform the group from a group on the verge of collapse to a very active established group with a strong support base. Also during this time I supported Trinity College Dublin with the early phases of their establishment. I was co-opted onto the National Committee after the 2010 to focus on the continued development of FoMSF in Ireland. Successes over the past year include supporting the establishment of FoMSF groups in University College Dublin and the Royal College of Surgeons, Ireland. My time on the National Committee has given me great opportunities to become involved in FoMSF initiatives such as Starved for Attention and help with the organisation of the National AGM. I’m also very excited about the development of FoMSF International and Post-FoMSF groups. Over the next year I want to build on the successes of the previous National Committees. I would like to see more co-ordinated national events such those already seen for World AIDS Day and the “Hands Off” campaign. In addition to the establishment of more FoMSF groups, I would encourage FoMSF to reach out to new groups of people that aren’t involved with FoMSF with particular attention on non-medical students from Nursing to Humanities to more accurately reflect life within MSF. With regard to fundraising I would love to see the amount raised by the movement to exceed £100,000. As a movement, I believe Friends of MSF has enormous potential and I would be honoured and humbled if I received your vote Other experience: Peer Support Leader; uLink Peer Support Programme (UCC), 2009-2010 Member of the uLink Peer Support Programme Steering Committee, 2009-2010 Favourite quote: “To the brave and the faithful, nothing is impossible” – Munster Rugby ……………………………………………………………………………………………………………………………………………………………. The position of: Advocacy Liaison
Name: Alisha Allana Subject: Medicine Year of Study: 3rd year University: University College London Please tell us why you feel you should be elected to this position: I have been a committee member of UCL Friends of MSF for three years: Events Co-ordinator in my first year and Secretary the following year, ultimately becoming President during 2010-11. I have

AGM Report 2011
6
thoroughly enjoyed being involved in FoMSF; my experiences with the society have been very rewarding, motivating me to apply for the position of Advocacy Liaison. This year, I have been able to understand the importance not only of raising money for MSF, but perhaps more significantly, raising awareness about certain issues faced by nations around the world. This was the case with the ‘Starved for Attention’ campaign, which we promoted at UCL: the campaign was launched through a film screening and discussion, allowing our members to appreciate the consequences of malnutrition and lack of vital nutrients. This event proved to be a huge success, generating a good discussion, and it was followed by a photo competition on the theme of ‘Starved for Attention’. As Advocacy Liaison, I would be keen to work with MSF-UK and the university FoMSF societies to organise campaigns at their universities, thinking of new ideas and ways to increase awareness of issues, particularly those that are not given much attention. Nevertheless, I would also be looking to promote the HIV/AIDS campaigns, whose importance struck me two years ago whilst volunteering in a school in Zanzibar. In their textbooks, it stated: “if you have AIDS, you will die” as part of a grammar exercise. Although this is not the reality given the remarkable development of treatment over the past few decades, this is sadly the belief of numerous individuals all over the world. My realisation of the importance of education has further stimulated me to become more involved with the MSF campaigns and I am keen to help individual groups to organise speaker events, symposia and film screenings to promote these issues, and also to organise such events on a wider scale, enabling networking and interaction between members. I am a reliable and dedicated individual, and I believe that I have demonstrated my good organisation and time management skills through my role as Event Co-ordinator of the National FoMSF Fun Run this year, which was a brilliant experience. I look forward to the challenges of being part of the National Committee, and I am excited by the prospect of becoming more involved with an organisation that has truly inspired me during the past three years. ……………………………………………………………………………………………………………………………………………………………. The position of: Events Liaison Name: Tamsin Smith Subject: MEng (Hons) Environmental Engineering Year of Study: 1st year of MEng conversion University: Open University Please tell us why you feel you should be elected to this position: I am currently studying with the Open University in the hope to become a chartered water and sanitation engineer and I am a volunteer lifeboat crew for the RNLI where I respond to emergencies on the river Thames. I love travelling where I can actively engage with local populations and experience different lifestyles and I am also a keen runner. Experience co-ordinating events: For the last year I have been the FoMSF representative for Oxford Global Health Group where I played an instrumental role in the organisation of the 2011 Oxford Global Careers Fair. I co-ordinated the management of over 30 stall holders and assisted to ensure the efficient running of the event. I published a short leaflet introducing the stalls and speakers and a more detailed document describing the work of the organisations represented at the fair. My personal reasons for running for FoMSF Events Co-ordinator: 1) Enjoyment of event organisation I would love to work with FoMSF groups in order to improve events, enhance the awareness of MSF and increase fund raising potential. Above all I think that events should be fun for everyone involved so I am a real believer in the volunteer ethos! My role as a volunteer at Chiswick lifeboat station

AGM Report 2011
7
requires a large amount of commitment and has allowed me to really appreciate the sacrifices made by both MSF and FoMSF volunteers. I am particularly excited about the opportunity to organise the fun run and the article competition. I am currently training to run the Great North Run for charity and I have a real passion for public communication of science and medicine, being a founding member of the Henry’s Club (part of the Wellcome Museum). 2) Engagement with MSF I would hope that this role would allow me to build up my personal network within MSF in order to enhance my own career aspirations. My long term goal is to work as a Water and Sanitation Engineer for MSF and over the next few years I will complete the graduate programme at Thames Water whilst attaining my MEng and taking evening French classes in order to enhance my application. My enthusiasm for the work of MSF is enormous and I am really passionate about the opportunity to have an input into FoMSF events to raise awareness and funds for MSF. ……………………………………………………………………………………………………………………………………………………………. The position of: Groups Liaison
Name: Germaine Liu Subject: Medicine Year of Study: 2nd, going on 3rd University: Cambridge University Please tell us why you feel you should be elected to this position: I have been involved with the FoMSF committee at my university since my first year and have learnt a lot from being secretary and now treasurer of the committee. As part of the team, I helped to organise the various events and campaigns that we held for the university, and also gained a deeper insight into the workings and opportunities for a group like FoMSF. One thing that I feel could strengthen individual FoMSF groups is a great cooperation between the various FoMSF groups around different universities. The FoMSF run in London in March was one of 2 times that I had the opportunity to speak with members of other groups to learn about what they were doing in their groups, which helped a lot in getting new ideas. As such, my motivation in applying for this position is to play a role in strengthening these links, which I personally have found to be very useful. The other opportunity I had to discuss with students from other FoMSF groups was at the Cambridge Medsin Global Health Conference 2011. This was a conference that I helped to organise as the Delegates Officer. My role was a mixture of logistics and public relations, and involved ensuring that over 300 delegates from around the country got as much out of the conference as they could. It gave me the experience of liaising with students from other universities who had an interest in Global Health, something that would be useful for the role of Groups Officer. Apart from that, I have been involved in various events and initiatives around College and in my High School. In addition, this summer, I will be leading a group of 8 fellow students from various universities around the UK to the Philippines for a medical service project.

AGM Report 2011
8
……………………………………………………………………………………………………………………………………………………………
NC Position Descriptions
President Role: To co-ordinate the National Committee and oversee the progress of FoMSF groups nationally Responsibilities: Co-ordinating and supporting the National Committee Supporting FoMSF groups with advice and guidance Lead responsibility for co-ordinating the National AGM 2012 Co-ordinate 2-3 FoMSF newsletters / year Represent FoMSF at MSF events and inter-group events Maintain online facilities – i.e. website and Facebook group Events Liaison Role: To support local groups with planning and running events to raise funds and awareness for the work of MSF Responsibilities: Work with groups to generate and develop ideas for events Encourage groups to create Events Templates of successful events Work with MSF and other NC members on new or national events Co-ordinate the FoMSF Article Competition Helping to organise the National AGM Recruit FoMSF support for MSF events Support the co-ordination of the FoMSF Fun Run 2011/12 Advocacy Liaison Role: Liaison for all advocacy-related activity – both with FoMSF groups and MSF-UK supporting or developing campaigns for the coming year. Responsibilities: Develop and support FoMSF Advocacy initiatives involving FoMSF groups nationally Working with MSF and with the FoMSF NC to extend and adapt MSF’s advocacy work for
students Working to co-ordinate advocacy events for World AIDS Day Helping to organise the National AGM Groups Liaison Role: To work closely with groups and maintain consistent support Responsibilities: Maintain a close relationship with all groups Support new groups or new committees in their development Aid groups with their annual handover process Take advantage of opportunities to expand the FoMSF movement within the UK Helping to organise the National AGM Compiling Group Updates for FoMSF Newsletter and 2012 AGM

AGM Report 2011
9
……………………………………………………………………………………………………………………………………………………………
Key Notes Speeches Campaigning for Access - Katy Athersuch Medical Innovation & Access Policy Adviser, MSF's Campaign for Access to Essential Medicines Katy Athersuch Katy has been working as the innovation and access policy adviser with the Access Campaign in Geneva since November 2009. During this time the campaign has run the 'Make It Happen' Campaign to get pharmaceutical companies to license their HIV medicines patents to the Patent Pool, and the 'EU Hands Off Our Medicines' Campaign to challenge the actions of the European Commission in undermining access to affordable medicines. Before joining MSF, Katy was the coordinator of the UK Consortium on AIDS and International Development's Stop AIDS Campaign, and before that coordinated the student arm of the Stop AIDS Campaign as the Campaigns and Advocacy coordinator at Restless Development. Katy studied International Relations and Development Studies at the University of Sussex. Report – by Irene Ruberto Katy Athersuch talked about MSF campaign for Access to Essential Medicines. The campaign started in 1999 from the frustration of MSF doctors and nurses being unable to treat patients due to either lack of drug supply, high prices of treatment, or unsuitability of the formulations. The main focus of the campaign has been particularly access to HIV treatment, as 6 million people are still dying of the disease, despite the presence of safe anti-retrovirals. Availability- Several tropical diseases are still treated with highly toxic and old drugs because pharmaceutical companies have no commercial interest in developing cures, which have no market. Indeed only 1 % of the drugs in the last 30 years were developed for malaria, tuberculosis or other neglected tropical diseases. MSF has spoken up to stimulate the development of new drugs, vaccines and diagnostic tools for tropical diseases. Affordability- The price of treatment is one of the main factors affecting access to medicines. MSF campaign has been particularly successful in negotiating the prices of antiretroviral drug for the treatment of HIV infection, which went from $12,000 to $80 per treatment. In addition MSF has recently launched two new campaigns: the first one targeting the EU-India trade agreement, which would stop the production of generic drugs; the second one focused on patent pool, as a new way of making HIV drugs more affordable. For this aim MSF managed to persuade some pharmaceutical companies to license their patents for antiretroviral drugs, but much work remains to be done. Quality- since 2001 MSF has been lobbying the WHO to set up a quality assurance department to increase the availability of quality-controlled medicines, which now amount to as many as 240 drugs. Suitability- MSF has been also speaking up about the lack of drug suitable to developing countries’ conditions. For example the need of more children-friendly formulations or heat stable vaccines and diagnostics.

AGM Report 2011
10
The Challenges of 2010: Medecins Sans Frontieres in the UK - Sid Wong Sid Wong Sid is a medical doctor specializing in Public Health. He has worked in the field for MSF in West Africa and Northern Uganda as well as undertaking consultancy work for local NGOs in South East Asia. In 2007 he completed a Masters in epidemiology and public health at Cambridge University and currently works as a public health advisor in the Global Health team, Department of Health. He was elected to the MSF UK Board of Directors in 2009 and is currently the Chair of the Board. Report – by Dele Sasegbon 2010
Haiti: Dealing with the aftermath of the earthquake. 120,000 treated
Floods in Pakistan: Heavy monsoon rains flooded the Indus river basin submerging a fifth of the country. Millions of people were affected.
Nutrition crisis in Chad: Drought induced famine affected the Sahel region of Africa, putting millions of people at immediate risk of starvation.
Lead poisoning in northern Nigeria: Local metal panning contaminated the food and drinking water of several villages in Zamfara State northern Nigeria. MSF treated 400 children for lead poisoning.
HIV: MSF treats 120,000 HIV sufferers with ARV therapy 5 challenges over the next 10 years Climate change: This would lead to:
Natural disasters Population migration Food and water insecurity
Population growth: Leading to: Mega-slums Rapid urbanisation (changing way aid organisations like MSF work)
Epidemiology transitions Leading to changing disease burden i.e more chronic diseases
Politicisation of humanitarianism Shifting role of state: No longer have weak governments allowing NGOs like MSF total autonomy within their borders.

AGM Report 2011
11
…………………………………………………………………………………………………………………………………………………………….
Workshops
Workshop 1: ‘Sudan - Beyond Everyday News’ – Jeroen Jansen Head of the Programmes Unit, Médecins Sans Frontières-UK Jeroen Jansen Jeroen Jansen started with MSF-OCA in 2002 as a logistician in Herat, Afghanistan (1 year mission). After Afghanistan he went to Liberia for 1 year; 6 months as a logistician and the last 6 months as Project Coordinator. He then worked as project coordinator with MSF-OCA until 2006 in Nigeria and Darfur. In 2006 Jeroen started as Deputy Head of Mission in Khartoum for 1 year and supported the operations in Darfur by starting Seleah project (South Darfur) and acting as interim project coordinator for Muhajariya (South Darfur). In 2008 he went to Juba, South Sudan, as Head of Mission for MSF-OCBA. Cumulatively Jeroen worked more than 2 years in Sudan Starting in 2008, Jeroen studied for 2 years at the American University in Cairo, receiving a Masters in International Human Rights Law and Graduate Diploma in Migration and Refugee Studies. He started in the UK office in October 2010, responsible as part of his current function for Sudan humanitarian affairs for MSF-OCA. Report - by Alan Quinn Recent referendum voted in favour of the creation of a separate South Sudan, governed by Juba, increased tensions and conflicts with independence approaching (9th July). Constantly changing political positions; particularly with President al Bashir. Border conflicts – no defined borders in several areas: Darfur, North vs South (conflict hotspots such as Abyei), East (4-5 militia groups currently operational), North East (conflict with Egypt), South East (dispute with Ethiopia/Kenya/Uganda) Several belligerent groups: SPLA (association with SPLM), LRA Several MSF sections operational: MSF Holland is the biggest section – South: Swiss and French operational, Darfur: Belgian and Spanish operational Internal displaced people (IDP): Total in Sudan: 4.5-5.5 million – largest in the world (2.6 million in Darfur). In addition, refugees are now moving into Sudan from Ethiopia, Eritrea and Libya. Operational differences between IDP camps and constantly moving refugees – use of mobile clinics Maternal health is the worst in the world, even in Khartoum where services are much more developed than the rest of the country. The rate is double that of South Africa Neglected diseases: Sleeping sickness particularly affecting the South. Others include Kala Azar and Meningitis. Repatriation in preparation for South Sudanese independence will result in the worst Kala Azar rate in 10 years (which moves in 10 year cycles) Hunger gap – natural disasters such as droughts and floods affect the country every year NGOs are currently propping up the health system. Conflict is driving away development NGOs. Politicisation of aid is a major issue Khartoum currently controlling wealth/resources such as oil – issues with oil sharing, pipeline routes and ownership – border conflict with Kenya

AGM Report 2011
12
Water – Sudan controls the source of the Nile – currently plans to build several dams which will kill supply to Egypt Political issues: What defines citizenship? South Sudan is a member of the International Criminal Court, the North opposes this membership. Comprehensive peace agreement has expired UN Mission in Sudan (UNMIS) – positioning: The North doesn’t want the UN on the ground while the South does. What will happen after independence? Who will pay off the $40 billion foreign debt after independence? Further issues: Changing temoignage – are our principles changing? Fortress Europe – responsibility to protect IDP? Who should the responsibility to build peace lie with? Discussion: Maintaining principles and keeping them independent Making sure money/mission mandate isn’t wasted – What are the achievements? Cost benefit analysis. Keep transparency …………………………………………………………………………………………………………………………………………………………….
Workshop 2: ‘Refugee Health: Case studies from Uganda and Chad’ – Sid Wong (see biography above) Public Health Advisor, Global Health team, Department of Health; Chair of the Board of Directors of MSF-UK Report - by Alisha Allana Sid began the workshop with a slide of a number of different images representing global health/MSF related individuals, logos and places, such as:
- Margaret Chan, director general of the WHO, who recently pledged £1.2m for the GAVI (Global Alliance for Vaccines and Immunisations) fund
- UN building in Geneva: the chair symbolises people who have lost limbs as a result of landmines Refugees and IDPs (internally displaced persons)
Refugees: individuals displaced from their home countries owing to war, politics, famine and disease, scared and fleeing for their lives
The UNHCR (UN High Commissioner for Refugees) is responsible for both the care and health of refugees; when it was first developed (~1950), there was no differentiation for IDPs (refugees displaced within their own countries), but these individuals are now under the care of the UNHCR and are treated by MSF, so there is now no distinction
Indicators of death are a good measure of the health of a population e.g. the crude death rate: the health of refugees is very different to normal individuals; they are more vulnerable and have numerous health needs so require rapid aid e.g. from MSF. Eastern Chad had a huge influx of Sudanese refugees (Darfurian refugees AND internal conflict): a refugee camp was formed with over 15,000 individuals. The UNHCR worked in the camp, as did a number of other NGOs. The camp was half a mile away from a town called Ade.

AGM Report 2011
13
We are the first MSF team in the situation, and need to rapidly assess what has been going on. What are the objectives of carrying out an assessment? What are the key areas or headliners to assess?
Key areas/headliners Basic needs: food, water, shelter, hygiene and health issues Transport/logistics Numbers/demographics; population breakdown (numbers, ages) Location/environment Supplies; on ground resources already available Systems already in place – NGOs, refugees, governments (local and international) Triage requirements Long term ideas/skills of refugees living in camp Interaction of camp with Ade (local town) Causation: why did the refugees have to flee? Political climate Safety and access Objectives What is going on – what exactly is the situation? What are our assets – people/supplies What do we need to do? How will we deliver it? - Identify demands - Assess urgency and safety - Consider political and cultural aspects Working in groups, we considered the questions posed by Sid and came up with the ideas listed above. This already showed qualities such as teamwork, facing time challenges and taking into account structure, which are all necessary when working with MSF in the field. However, the objectives can be firmly divided into the following aspects: 1. Do we need to intervene or not? – Is it required/feasible/urgent? 2. Define the priorities of intervention (adapt) 3. Plan implementation of priorities (strategies, time frame, resources e.g. if there has been a
measles outbreak, need vaccinations) 4. Advocacy: pass on information to the international community/donors – observations of refugee
living conditions; human rights ~ Medicine is protocol based: we need to think about WHY we are doing anything, and this dictates HOW we carry out tasks We then re-classified the key areas under eight different headings and considered not only the information that we needed to collect, but also HOW to collect it. 1) GEO-POLITICAL CONTEXT Perception – how MSF are viewed (we are well recognised as impartial and neutral so are more
likely to be well received) Why are there refugees here? – Talk to the locals, refugees, local media hub, local government,
local police etc to get different opinions Camps often have hierarchical communities – talk to the leaders

AGM Report 2011
14
Read government/UNHCR documents Ministry of Health
Need interpreters to overcome language barriers Background research in the UK – some historical knowledge How the host country feels about the camp – talk to people from Ade; what is the relationship
between the refugees and the townspeople? How old is camp: short/long term; may be old, continuous refugee movement FCO (foreign commonwealth office) produces stats about risk ratings – check before arrival in the
country Which areas does the government control? – Barrier crossing points 2) DEMOGRAPHY Where they are from, age, sex, religion, health; cultural norms, status of individuals in the group Conform to their values and religious beliefs; gain their trust and respect Community structures/how they interact – work with them not over them Use tent number to sample population – designated areas, rough estimate of number OR may
already have camp register Satellite imaging to count structures Want to know about vulnerable groups (under 5s, older people) Extrapolate from set figures; NGOs may already have vaccination registers Number of live births/birth and death rates – registration of birth is a human right; proof of
existence but no legal requirement of this in Africa Sample survey – what did everyone bring with them? 3) ENVIRONMENT MAP of water supplies, access; full survey of ground Climate, potential for monsoons? Flood plains, potential for natural disasters Meningitis belt Weather: will it be possible to store medication? Roads – quality; transport routes (air, water, road) – teams and supplies Local resources, food availability – go to local town and assess whether markets have enough food Location of causal factor (fighting, disease) Burial sites Environmentally spread disease e.g. TB Need for non-medical items – blankets, cooking utensils 4) MORBIDITY Pre-existing conditions – chronic conditions e.g. HIV, measles, malnutrition, malaria, tuberculosis,
diarrhoeal diseases/cholera Information from NGOs and local organisations, records from hospitals Vaccinate against measles (infection spreads fast in closed camps); psychological diseases
(violence/trauma), stab and gunshot wounds, rape 5) MORTALITY Crude death rate: standardised measurements for emergency are >1 death per day per 10,000
people, and >2 deaths per 10,000 people per day for under 5s Community health worker surveillance; pay refugees to ask each house how many people have
died in a certain time period Causes of mortality; maternal health/births; where and how people die

AGM Report 2011
15
Death rates fluctuate and are very sensitive Body disposal/burial sites – cultural aspects 6) CO-ORDINATION Contact with base – communications offices (supplies) Other NGOs, local town, local government, secondary care Education, teach basic skills: hygiene (leaders of communities) WITHIN base – meetings with doctors, engineers, logisticians etc Military presence Resource allocation (must prioritise), between refugees Keep MoH and other NGOs involved Ask WHY – what is the added benefit of MSF – distasteful impulse to want to be at every
emergency, not necessary 7) SURVEILLANCE Needed in the beginning, especially for death indicators, to see how well the population is doing Photos; administrator can set up internet, work with HR 8) HR-RESOURCES Funding Access to camp Use local refugees; exit strategies Longevity of resources Energy supplies – renewable Communication with central MSF Security If the situation is urgent then assessment and treatment can be done in parallel. This is a real life situation; it is going well when crude death rates decrease. ……………………………………………………………………………………………………………………………………………………………. Workshop 3: ‘What is Humanitarianism Anyway?’ - Joel Cunningham and Pete Scolding Joel Cunningham is currently a fourth year medical student at University College London and been involved with Friends of MSF for the past 4 years. He was President of the UCL branch for 09/10. Pete Scolding is currently studying the International Studies and Diplomacy MA at the School of Oriental and African Studies, London. He will return to UCL Medical School in 2011. He has also been involved with FoMSF for the past 4 years, serving as President of UCL FoMSF 2008-09, Speaker Liaison on the National Committee 2008-09, President 2009-10 and Co-Opted Advisor 2010-11. ‘What is Humanitarianism Anyway?’ is a workshop designed to be run by students, without it being necessary to have a great deal of background knowledge. The master copy and handouts are available online at http://issuu.com/fomsf/docs/humanitarianism_discussionset_mastercopy http://issuu.com/fomsf/docs/humanitarianism_discussionset_handout

AGM Report 2011
16
…………………………………………………………………………………………………………………………………………………………….
An MSF Career – Plenary Q&A Session CHAIR: Polly Markandya - Head of Communications, MSF-UK PANEL: Sid Wong - Public Health Advisor, Global Health Team at the Department of Health; Chair of the Board of Directors, MSF-UK Jeroen Jensen - Head of the Programmes Unit, MSF UK Report - by Laura Gill
How did you first get involved in MSF Sid? Having completed medical school and started his training in general medicine Sid was able to take some time out before taking up a trainee registrar post and used this opportunity to go on his first mission with MSF. Whilst he planned to spend a year ‘out of the system’ and then return to complete his training, by day 5 of his first mission he had realised that he wanted to spend more than a year working with MSF! With that realisation he began his career in public health.
What was your first mission like? Unlike many other organisations, MSF do take first-timers on missions. When you start as an FY1 doctor your realise that medical school does not prepare you for everything and every day is a question of survival – remembering enough to get you by and learning as you go along. In some respects, your first mission with MSF is very similar to this. You’re absolutely thrown in at the deep end. However, it is not just a question of learning how to work in a new environment; one of the biggest hurdles to overcome is leaving your family and other familiar faces behind and being surrounded by new people 24/7. You are pushed to work outside your initial limits.
How do you get a job with MSF? Competition to work with MSF is now greater than ever. However, the panel highlighted several key attributes which would help make your CV stand out:
LANGUAGES Languages are a key discriminator in MSF recruitment so even if you studied a language to
GCSE or took basic classes several years ago it is absolutely worth working up to A Level standard or beyond. Languages are not necessarily a limiting factor but can certainly open doors for you.
There are many languages which come in handy but French is particularly useful as it is spoken in several of the countries where MSF works and by many MSF staff.
Other useful languages include Arabic and Spanish. In addition to communication with local communities, international teams on the ground
tend to speak the majority language so languages can be a key way to get to know colleagues and make a mission that much smoother.
PERSONAL EXPERIENCE OF LIVING AND WORKING IN A SMALL TEAM AND COPING WITH STRESS This can be the hardest aspect of the job – the intensity of relationships, barriers to making
friends outside colleagues and being together 24 hours a day, 7 days a week makes for testing social environment.
Relevant experience to prepare you for this can be anything from time spent working on a boat to being an overland driver in West Africa.

AGM Report 2011
17
Travelling as much as possible also helps you to become a more rounded person and teaches you skills which will prepare you for working in new environments with an international team.
COMMITMENT TO THE MSF MISSION Those recruiting for MSF are looking to see that you’ve made a well-informed, conscious
choice that this is exactly what you want to do. JJ didn’t get in first time but gave it another go and he’s here now so determination is really
important. He said you should absolutely take the time to think it over – it’s tough and despite being surrounded by romance the realities of working with MSF are nothing like Angelina Jolie’s glamorous portrayal of humanitarian work in her movie, Beyond Borders!
The panel also had some top tips, aimed particularly at medics considering a career with MSF:
Make the most of opportunities such as the iBSc and internships while you have the chance – they are difficult to do once you are qualified.
Use your elective as an opportunity to test yourself in a developing country.
What specialties would be worth considering for a medic wanting to work with MSF? This varies depending on whether you’re planning on going on a single mission with MSF or want to make it your career. For those looking for a short-term role, what you choose to specialise in has less impact on the opportunities available. Below are a few examples of useful areas to consider:
General Practice - there are almost always jobs available for GPs, especially short term Infectious Disease - specialists in this area are also sought after, however it’s worth
remembering that by no means do you have to go down this route to work for MSF Surgery - to work for MSF a surgeon must be independent operating, i.e. a year 4 or year 5
registrar Obstetrics and Gynaecology - this is always a useful specialty for MSF as in any new project
an O&G case will often be the first through the door
So you complete a 9 month mission…then what happens? People often want to get straight back into the field as soon as possible after completing a mission. However, it is generally recommended that you take some time out to recharge. After months away on a mission it is easy to lose your roots and become nomadic, without a sense of belonging anywhere so it is healthier to take some time to reconnect at home and seriously consider exactly what it is you want to do next. In terms of being taken on again by MSF, if you’ve had a good experience and good evaluation there is a high chance of you being re-hired.
Is burn out a big problem? Probably less than half of those who work for MSF go out on a second mission. It is difficult
to tell how someone will cope on a mission, whatever precautions you take. The MSF film Living in Emergency gives the viewer a feel for this, showing a whole range of personal experiences working in the field.
In terms of avoiding burn out, it’s important to be realistic about what you can manage. It’s all too easy to go mission to mission but it’s absolutely worth listening to advice, looking after yourself and taking a bit of time out in between.

AGM Report 2011
18
The MSF support system is good and it’s there if you need. For example, after his first mission in Afghanistan, JJ spent 2 months receiving psychosocial support to help him come to terms with his experiences but within 4 months he was ready to head out on his next mission.
The most important thing is to realise that there will be ups and downs and not to feel like a failure if you realise that working for MSF isn’t the career for you.
Also, there are many different organisations with which you can work within the humanitarian and development sectors. MSF may not offer exactly what you’re looking for but that doesn’t mean you should give up on your career plans, you may just need to look beyond MSF.
Is it really ‘pocket money’ you get paid for a mission with MSF? MSF staff on a mission get paid around £500 per month as a per diem to cover their overheads while they are away from home. In your first year, you earn the very lowest wage but this does go up slightly over repeated missions. The idea is that it should cover your home bills/debts so you don’t come back in the red and the cost of living while you are actually on the ground is very low so most people come back a few hundred pounds in credit. In fact, Sid managed to save more on one mission with MSF than in 5 years living in London. However, whilst it is enough to live on, what you earn with MSF will never equal that for working in the UK, for the UN or for other NGOs.
What opportunities might MSF offer a pharmacy student? Pharmacists are needed in the field. Specific details of positions are available on the MSF website. As for any MSF staff, the personal attributes described above would also be important for pharmacists.
Can a clinician progress within MSF? There is no opportunity for you to progress parallel to the UK as the two working systems do
not directly integrate. This means that stepping out of the system lower down the career path i.e. before becoming a registrar would mean the need to step back in at the same level in order to work in the UK later. However, some UK training programmes do now offer opportunities to spend time working abroad, e.g. a paediatric registrar may be able to incorporate some time with VSO into their training.
For someone looking at a long-term career with MSF this would start with roles as a practising field doctor. Within this role you could then move on to supervising others, but the main route for progression would be to become medical coordinator for a programme. Beyond this, there are opportunities for research in public health through the Manson Unit or an operational centre but this often means a return from the field.
MSF want to keep good medical people and draw them into management, with more medics as heads of mission. Having more ‘medical leadership’ is useful as it helps to develop good relationships with Health Ministries in countries with MSF projects. However, a lot of great doctors want to stay in more hands on roles, working directly with patients so don’t take up this opportunity for progression.

AGM Report 2011
19
A possible initiative for MSF is development of private MSF hospitals around the world where there would be more training opportunities, however this idea is very much in the development stage.
Could you give us your best and worst memories of working with MSF? POLLY
Over her 15 years in MSF the office Polly has visited lots of projects and these trips have given her both her best and worst moments. The best is the intense pride in seeing an MSF project and the effect it’s having, such as an MSF clinic in the middle of nowhere with a huge queue offering medical care that no one else will provide. Her worst experiences have been the very, very sad moments, like seeing a child dying, when it’s difficult to keep professional distance. The experience of visiting a project can be very emotional, especially seeing or hearing things about people hurting others for pleasure. You see the light and dark in human nature played out right in front of you.
JJ JJ’s worst memories are the loss of colleagues – both national and international staff. His best have all involved childbirth! Despite being a logistician and not a medic he was once asked to scrub in and assist in a C-section. He also helped with a delivery in the back of a land cruiser when the realisation that they had just helped save both mother and child was fantastic.
SID Sid was inspired by Jim Orbinski’s 1999 Nobel Peace Prize acceptance speech on behalf of MSF. It highlighted the inequalities in the world and it is Sid’s belief that these are wrong and unacceptable. His work with MSF is a symbol that he doesn’t support them. He knows that what he does won’t save the world but if just one person is kept alive for another day, week or year then he’s doing his little bit. Hopefully that will give others the opportunity to change systems for the better. This belief in MSF and its work is his best experience but the worst part of humanitarian work is that MSF and aid work/humanitarianism in general are not perfect and so you do always ask yourself ‘Why am I doing this?’. Ultimately though, he loves MSF so will keep doing what he’s doing.
What opportunities are there for operational research? The initial question is posed by the Public Health Department/Manson Unit then it’s a joint effort to find the answers so often people on missions are directly involved in research. The Programmes Unit also carries out research, e.g. in social sciences.
Is it true that UK medical training is not that relevant for development work? Whilst UK training isn’t specifically aimed at development work, training to be a medical doctor
and junior training both help to develop good generic skills. Often MSF work involves carrying out generic primary care, similar to that in the UK, but in a very isolated environment. The ability to cope and think on your feet is the key skill. You won’t have an answer to everything but books and the internet mean a lot of resources are available to you.
However, if you have the opportunity, doing a diploma in tropical medicine then spending 6 months in a country where the training is more applicable to development work, e.g. South Africa would undoubtedly be very useful.

AGM Report 2011
20
FoMSF Group Contact Address
Aberdeen [email protected]
St Andrews [email protected]
Bart's and the London [email protected]
Birmingham [email protected]
Brighton & Sussex [email protected]
Bristol [email protected]
Cambridge University [email protected]
Cardiff [email protected]
Cork [email protected]
Dundee [email protected]
Durham [email protected]
Edinburgh [email protected]
Glasgow [email protected]
Hull and York Medical School [email protected]
Imperial [email protected]
Keele [email protected]
Kingston University and St George's University London (KU & SGUL) [email protected]

AGM Report 2011
21
Leeds [email protected]
Leicester [email protected]
Liverpool [email protected]
London School Hygiene & Tropical Medicine [email protected]
Manchester [email protected]
Newcastle [email protected] [email protected]
Nottingham [email protected]
Oxford [email protected]
Royal College of Surgeons, Ireland [email protected]
Sheffield [email protected]
Southampton [email protected]
Swansea [email protected]
Trinity, Dublin [email protected]
University College Dublin [email protected]
University of East Anglia (UEA) [email protected]
Warwick [email protected]

AGM Report 2011
22
…………………………………………………………………………………………………………………………………………………………….
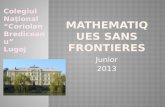
Feedback (25 respondents) Overall how satisfied were you with the AGM?
72%
28%
5 out of 54 out of 5
Were you happy to see the event take place in London?
68%
28%
4%
YesDon't mindNo
How likely are you to attend a future event?
54%38%
8%
5 out of 54 out of 53 out of 5

AGM Report 2011
23
Why did you get involved with FoMSF? General interest in global health issues/ humanitarian work To help fundraise and raise awareness about MSF. To help get my foot in door for MSF itself. I wanted to raise awareness of this organisation among not only medical students but whole university. I would like to work with MSF in the future. To help, to learn and to spread the word. Raise money and awareness for an organisation that I feel is very worthwhile. To develop my knowledge of the charity to work with them in the future. Humanitarianism Career option one day? Aspire to join MSF as a pharmacist Great respect for MSF. Also member of Oxford Global Health Group Interest in global & public health modules in Medical School (that I subsequently withdrew from). Wanted to learn more about MSF; interested in humanitarian work in the future. Agree with the basic principles of MSF and there was good publciity at the uni freshers fair. They were the only group in college dealing with such issues of humanitarianism that I'm interested. I wanted to know more about MSF itself and be actively involved in a humanitarian organisation I believed in and could work with at some. The more I learn about MSF the more I stand behind their actions and goals. I've always been interested in a career in the humanitarian sector and MSF is an organisation that I feel manages to remain neutral and effective in their work, while still providing healthcare in the most difficult of settings. Interest in MSF as a possible career choice/year out. Interest in working with them later. Humanitarian aid work Because I'm interested in becoming part of MSF when I graduate and I think its a worthwhile cause. Knew of them before medicine (military background). Event was held and committee formed in 2009 (Dec) The opportunity arose at BSMS and I just happend to be right place right time. Loved it since. To help support something which I believe in. Find out more about MSF/ Careers + also thought good for CV. The work and principles of the organisation inspire me.

AGM Report 2011
24
What were the highlight(s) of the day for you?
Workshops - nice chance to work with other participants Talk from Katie on pharmaceutical HIV/AIDS etc Finishing panel discussion answered a lot of my questions. The workshop "what is humanitarianism anyway". Workshops and speaker on AIDS were really interesting and informative Enjoyed Sid's talk The panel question and answer session at the end. The open half-hour Chance to ask questions at the end. JJ's session. Panel session Panel Q & A session - great to get a good insight. All the keynote speeches and workshops + learning about all the different groups. Workshop/ panel discussion - reality of working with MSF. The workshop The workshop was really interesting and interactive. All the speakers were excellent. Two key note speakers were very informative, as was the question answer session Speaker from Sid Wong and Q&A at end of AGM. Workshop Question session Sid Wong's lecture and workshop. The Q&A panel Scenarios and workshops! Excellent key note speakers Q&A Session at end very very useful! Workshops great. Key Notes speech really good (Katy). Career session at the end was brilliant and inspiring. Sudan workshop. Sid Wong's info. Question time Sid Wong's speech. JJ's workshop

AGM Report 2011
25
Additional comments, ideas or suggestions: Tea would be amazing!!! It was good. AGM was useful to share experiences of our own societies, compare raising awareness and fundraising events. Well done. Not over 2 days! I really enjoyed the idea of interacting with local schools to each university. Think it’s important and wouldn't be too difficult to implement (?). Really good, enjoyed the day. Possibly more ideas and support on fundraising events. A screening of "Living in Emergency". Co-ordinating between groups Possibly an extra talk in the morning, with photos of an example mission? Fantastic AGM! Thank you This was a great time to recharge and get enthused again, through the keynote speeches and learning from other groups. The voting for committee was a bit futile I thought. The person who spoke last in group seemed to get elected. Focus on more integration. More non-medical group involvement.

AGM Report 2011
26

AGM Report 2011
27