Friday 16 February 2018 - RCP London
31
West Midlands Physician Associates Conference Friday 16 February 2018
Transcript of Friday 16 February 2018 - RCP London
West Midlands
Physician Associates Conference
Friday 16 February 2018

Developing a role for the Physician Associate in
Rheumatology Dr Andrew Whallett
Consultant Rheumatologist
Dudley Group NHS Foundation Trust
Deputy Postgraduate Dean, HEE West Midlands

An approach to Musculoskeletal Medicine

Musculoskeletal pain

Common
20 – 25% GP consultations
30% of all disability due to musculoskeletal disorders

Who’s who?
ORTHOPAEDICS Trauma
Mechanical
Developmental
RHEUMATOLOGY
Severe
(often systemic)
joint disorders
GENERAL PRACTICE
Minor traumatic and ‘arthritic’
conditions
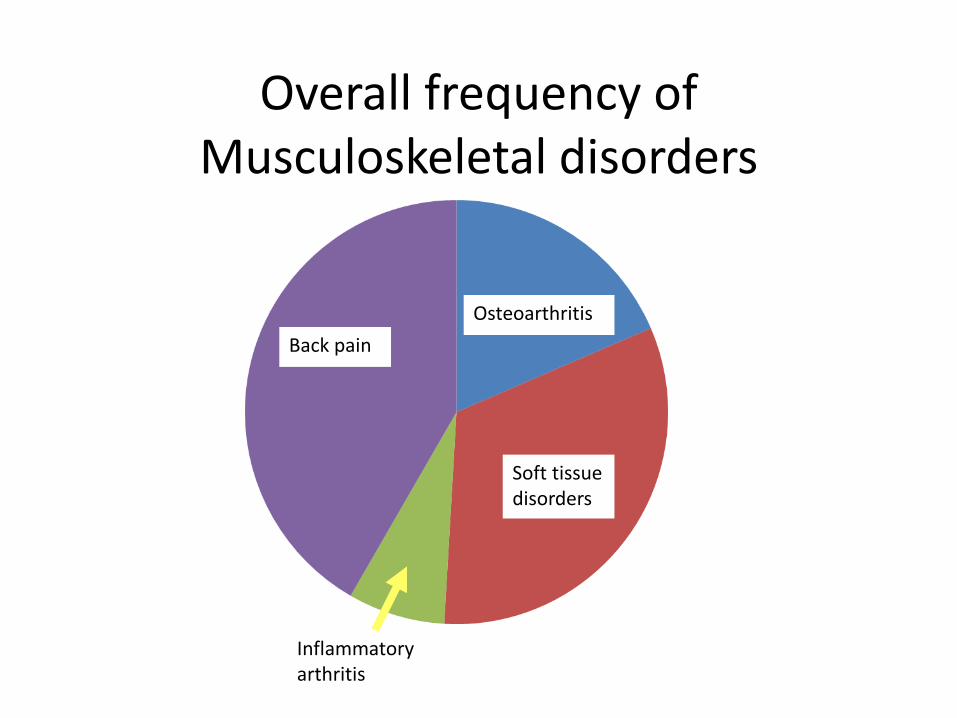
Overall frequency of Musculoskeletal disorders
Back pain
Osteoarthritis
Soft tissue disorders
Inflammatory arthritis
Presentation of musculoskeletal disorders in New Patient Clinics

PATTERNS OF MUSCULOSKELETAL DISEASE
• Monoarthritis vs. polyarthritis
• Inflammatory vs. non-inflammatory (i.e. mechanical/structural) arthritis

Inflammatory/Mechanical
• Inflammatory – pressure and stretching of synovium and peri-articular structures
• Inflammation(red, warm, swollen)
• Systemic upset.
• Mechanical – prevents normal smooth movement
• Pain localized and reproduced by certain movements
• Crepitus/clicking/locking

Extra-articular manifestations
Multi-system Involvement
Disease
Therapy

Diagnosis and Assessment
of rheumatic disease

Diagnosis and Assessment
HISTORY EXAMINATION
INVESTIGATION
Screening (minimum) musculoskeletal examination
• Minimum examination standing (spine, neck, upper limb)
• Minimum examination lying down (lower limb)

Investigation
• Bloods
• Radiology
• Synovial fluid


Managing ongoing inflammatory conditions in Rheumatology

Activity or damage?

Activity x Time = Damage
SZP MTX Rx
Humira


Connective tissue
diseases

Then and now….

The Biologics Revolution

The changing settings in which patients are cared for
• Inpatient
• Outpatient
• Day Case
• Community

Blurring of ‘Professional boundaries’
• Focus on what patients need, rather than on who or where care is provided
• Multi-disciplinary team
• Patients

What can a Physician Associate do in Rheumatology?

What can a Physician Associate do in Rheumatology?
What can’t a Physician Associate do in Rheumatology?

Joint Injections Already performed by many members
of the team

Clinical Rheumatology ‘tasks’
• History, Examination, Diagnosis
• Diagnosis
• Treatment and Management Plans
• Joint and soft tissue injections
• Disease Monitoring

Beyond Clinical Rheumatology ‘tasks’
• Data gathering and recording
• Quality Improvement
• Research
• Education
• ‘Management’

Conclusion
• Visit your local Rheumatology Department
• Raise the profile of PAs
• Recognise that there are exciting prospects of career development for PAs in Rheumatology – there is something for everyone