Frequency of reported European ancestry among multiple sclerosis patients from four cities in the...
5
Clinical Neurology and Neurosurgery 115 (2013) 1642–1646 Contents lists available at ScienceDirect Clinical Neurology and Neurosurgery j o ur nal hom epage: www.elsevier.com/locate/clineuro Frequency of reported European ancestry among multiple sclerosis patients from four cities in the southern and southeastern regions of Brazil Elizabeth Regina Comini-Frota a,∗ , Doralina Guimarães Brum b,e , Damacio Ramon Kaimen-Maciel c , Yara Dadalti Fragoso d , Amilton Antunes Barreira b , Eduardo Antonio Donadi b a General Hospital, Federal University of Minas Gerais, Belo Horizonte, MG, Avenida Alfredo Balena 110, CEP 30130-100, Belo Horizonte, MG, Brazil b Faculdade de Medicina de Ribeirão Preto, Universidade de São Paulo, Universidade do Estado de São Paulo (USP), SP, Ribeirão Preto, São Paulo, Brazil c Health Sciences Center, Londrina State University, Londrina, PR, Brazil d Metropolitan University of Santos, MS Reference Center DRS-IV, Santos, SP, Brazil e Faculdade de Medicina de Botucatu, Universidade Estadual Paulista, Botucatu, SP, Brazil a r t i c l e i n f o Article history: Received 15 August 2011 Received in revised form 31 December 2012 Accepted 16 February 2013 Available online 25 March 2013 Keywords: Multiple sclerosis Brazilian patients Epidemiology Immigration Prevalence a b s t r a c t Recent reports on the prevalence of multiple sclerosis (MS) have described discrepancies between the rates in cities in the northeastern and southeastern regions of Brazil, representing a north–south gradi- ent. European immigrants settled in southeastern and southern Brazil at the beginning of the twentieth century. In this study, we report the frequency of European ancestors among Brazilian MS patients in four cities in the southern and southeastern regions of Brazil. Methods: A total of 652 consecutive patients with confirmed MS diagnoses seen at four centers in Belo Horizonte, Ribeirão Preto, Londrina and Santos were asked about the origin of their ancestors, going back three generations. Results: 287 (44%) reported Italian ancestry, 211 (32%) reported that all ancestors were born in Brazil, 49 (7.5%) had Portuguese ancestry and 70 (10%) had Spanish ancestry. The patients in Belo Horizonte and Londrina reported higher proportions of Italian ancestry than the proportions estimated for the populations of their respective States. Conclusion: Brazil has a north–south gradient of 0.91/100,000 per degree of latitude, which is higher than the gradient for Latin America. Since the largest immigrant group that settled in southern and southeastern Brazil was from Italy, it is possible that Italian immigration was one of the factors that have contributed toward increasing the prevalence of MS in these regions. © 2013 Elsevier B.V. All rights reserved. 1. Introduction Brazil is a country of continental dimensions located between the latitudes 5 ◦ north and 33 ◦ south. There are many differences between the northern, northeastern, southern and southeast- ern regions of Brazil. The populations in these regions represent five centuries of inter-ethnic miscegenation between Europeans, Africans and native Americans, although the contribution from each ethnic group differs between the different geographic regions [1]. In northern Brazil, the admixture with native Americans was more significant, while in northeastern Brazil there was a greater contribution by Africans and in the southern and southeastern ∗ Corresponding author at: Department of Neurology, Federal University of Minas Gerais. E-mail address: [email protected] (E.R. Comini-Frota). regions the biggest contribution was from diverse Europeans [2]. The climate varies from equatorial in the north to temperate in the south, along with variations in the amount of sunlight, the fauna and flora and human culture. According to previous reports, the prevalence of multiple scle- rosis (MS) varies depending on different genetic and environmental factors, including the geographical region and ethnic composition of the population [3,4]. Since this disease is more prevalent among Caucasians, with a gradient of increasing distribution from low to high latitudes worldwide, higher prevalence of MS would be expected in southern and southeastern Brazil than in northern and northeastern Brazil, because of differences in genetic background and climate [5]. A recent study covering much of Latin America has demonstrated that there is a north–south gradient in MS prevalence rates [6]. The survey went from Panama (northern hemi- sphere) to Argentina (southern hemisphere), and found that the prevalence increases from 0.75/100,000 in Ecuador (on the equator) 0303-8467/$ – see front matter © 2013 Elsevier B.V. All rights reserved. http://dx.doi.org/10.1016/j.clineuro.2013.02.024
-
Upload
eduardo-antonio -
Category
Documents
-
view
213 -
download
1
Transcript of Frequency of reported European ancestry among multiple sclerosis patients from four cities in the...

FpB
EDAa
b
c
d
e
a
ARR3AA
KMBEIP
1
tbefiAe[mc
G
0h
Clinical Neurology and Neurosurgery 115 (2013) 1642– 1646
Contents lists available at ScienceDirect
Clinical Neurology and Neurosurgery
j o ur nal hom epage: www.elsev ier .com/ locate /c l ineuro
requency of reported European ancestry among multiple sclerosisatients from four cities in the southern and southeastern regions ofrazil
lizabeth Regina Comini-Frotaa,∗, Doralina Guimarães Brumb,e,amacio Ramon Kaimen-Maciel c, Yara Dadalti Fragosod,milton Antunes Barreirab, Eduardo Antonio Donadib
General Hospital, Federal University of Minas Gerais, Belo Horizonte, MG, Avenida Alfredo Balena 110, CEP 30130-100, Belo Horizonte, MG, BrazilFaculdade de Medicina de Ribeirão Preto, Universidade de São Paulo, Universidade do Estado de São Paulo (USP), SP, Ribeirão Preto, São Paulo, BrazilHealth Sciences Center, Londrina State University, Londrina, PR, BrazilMetropolitan University of Santos, MS Reference Center DRS-IV, Santos, SP, BrazilFaculdade de Medicina de Botucatu, Universidade Estadual Paulista, Botucatu, SP, Brazil
r t i c l e i n f o
rticle history:eceived 15 August 2011eceived in revised form1 December 2012ccepted 16 February 2013vailable online 25 March 2013
eywords:ultiple sclerosis
razilian patientspidemiology
a b s t r a c t
Recent reports on the prevalence of multiple sclerosis (MS) have described discrepancies between therates in cities in the northeastern and southeastern regions of Brazil, representing a north–south gradi-ent. European immigrants settled in southeastern and southern Brazil at the beginning of the twentiethcentury. In this study, we report the frequency of European ancestors among Brazilian MS patients infour cities in the southern and southeastern regions of Brazil.Methods: A total of 652 consecutive patients with confirmed MS diagnoses seen at four centers in BeloHorizonte, Ribeirão Preto, Londrina and Santos were asked about the origin of their ancestors, going backthree generations.Results: 287 (44%) reported Italian ancestry, 211 (32%) reported that all ancestors were born in Brazil,49 (7.5%) had Portuguese ancestry and 70 (10%) had Spanish ancestry. The patients in Belo Horizonte
mmigrationrevalence
and Londrina reported higher proportions of Italian ancestry than the proportions estimated for thepopulations of their respective States.Conclusion: Brazil has a north–south gradient of 0.91/100,000 per degree of latitude, which is higherthan the gradient for Latin America. Since the largest immigrant group that settled in southern andsoutheastern Brazil was from Italy, it is possible that Italian immigration was one of the factors that have
asing
contributed toward incre. Introduction
Brazil is a country of continental dimensions located betweenhe latitudes 5◦ north and 33◦ south. There are many differencesetween the northern, northeastern, southern and southeast-rn regions of Brazil. The populations in these regions representve centuries of inter-ethnic miscegenation between Europeans,fricans and native Americans, although the contribution fromach ethnic group differs between the different geographic regions
1]. In northern Brazil, the admixture with native Americans wasore significant, while in northeastern Brazil there was a greaterontribution by Africans and in the southern and southeastern
∗ Corresponding author at: Department of Neurology, Federal University of Minaserais.
E-mail address: [email protected] (E.R. Comini-Frota).
303-8467/$ – see front matter © 2013 Elsevier B.V. All rights reserved.ttp://dx.doi.org/10.1016/j.clineuro.2013.02.024
the prevalence of MS in these regions.© 2013 Elsevier B.V. All rights reserved.
regions the biggest contribution was from diverse Europeans [2].The climate varies from equatorial in the north to temperate in thesouth, along with variations in the amount of sunlight, the faunaand flora and human culture.
According to previous reports, the prevalence of multiple scle-rosis (MS) varies depending on different genetic and environmentalfactors, including the geographical region and ethnic compositionof the population [3,4]. Since this disease is more prevalent amongCaucasians, with a gradient of increasing distribution from lowto high latitudes worldwide, higher prevalence of MS would beexpected in southern and southeastern Brazil than in northern andnortheastern Brazil, because of differences in genetic backgroundand climate [5]. A recent study covering much of Latin America has
demonstrated that there is a north–south gradient in MS prevalencerates [6]. The survey went from Panama (northern hemi-sphere) to Argentina (southern hemisphere), and found that theprevalence increases from 0.75/100,000 in Ecuador (on the equator)
E.R. Comini-Frota et al. / Clinical Neurology an
FSS
to
lli1cwSHttF
idaTaaadlw
irtTtbtfl
ec
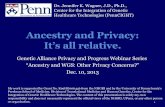
ig. 1. Brazil, showing the locations of the cities of Belo Horizonte, Ribeirão Preto,ão Paulo, Santos, Londrina and Recife, in their respective states of Minas Gerais,ão Paulo, Paraná and Pernambuco.
o 21.5/100,000 in Argentina, thus showing an increasing gradientf 0.33/100,000 inhabitants per degree of latitude [6].
Recent studies conducted in Brazil have also reported preva-ence rates for MS. In the northeastern city of Recife, situated atatitude 8◦ S, the prevalence was found to be 1.3 patients/100,000nhabitants [7]. In the southeastern city of Santos, it was5.5/100,000 [8], and São Paulo, 15/100,000 [9], which are bothities in the State of São Paulo. In the southern city of Londrina,hich situated at the same latitude as Santos and São Paulo, at 23◦
, the prevalence was found to be 13.8/100,000 [10], while in Beloorizonte, situated at latitude 19◦ S, it was 18/100,000 [11]. Even
hough these data are limited to a few cities, they point towardhe existence of a north–south gradient of MS prevalence in Brazil.ig. 1 presents a map illustrating the locations of the cited cities.
Four studies on the genetics of MS patients in Brazil, conductedn Ribeirão Preto [12,13], Londrina [14] and Rio de Janeiro [15],emonstrated that there was a strong association between HLA 15*nd susceptibility to MS among Brazilian patients in those cities.he HLA-DRB1*1501 allele was over represented in white Braziliannd Afro-Brazilian MS patients [12,13], and the HLA-DRB1*1503llele in Afro-Brazilians [14,15]. Mulatto was used in those papersnd here to describe individuals of mixed European and Africanescent. Those studies showed that MS cases in Brazil have simi-
arities regarding genetic background with MS in other countriesith European populations.
Between 1890 and 1930, large numbers of European and Asianmmigrants arrived and settled in the southeastern and southernegions of Brazil, thereby influencing the ethnic composition, cul-ure and patterns of life of the populations in these regions [1,2].hese immigrants and their descendants lived under environmen-al conditions that differed in many aspects from what they hadeen accustomed to in Europe or Asia, for example in relation tohe amount of exposure to sunlight, hygiene facilities, fauna and
ora.We hypothesized that the patterns of immigration from West-rn Europe in the nineteenth and twentieth centuries may haveontributed toward the differences in the prevalence of MS
d Neurosurgery 115 (2013) 1642– 1646 1643
between different regions of Brazil; and in particular, that these pat-terns were one of the factors contributing toward higher prevalencein the southern and southeastern regions than in the northeasternregion. To test this hypothesis, we started asking our patients fromour four cities about their ancestry. Here, we describe the ances-try reported by MS patients from four Brazilian cities: three in thesoutheastern region (Ribeirão Preto, Santos and Belo Horizonte)and one in the southern region (Londrina).
2. Subjects and methods
2.1. Characteristics of the four cities studied
Belo Horizonte is the capital of the State of Minas Gerais, locatedat a latitude of 19◦ south. Its urban area has 2,412,937 inhabitants[2]. The city is located 400 km inland, at an altitude of 900 m, with atropical highland climate (Köppen-Geiger classification). The ultra-violet index (UVI) variation is from above 10 (extreme) (WHO 2002)between October and April to 7 (high) between May and September[16]. The city’s human development index (HDI) in 2011 was 0.85while it was 0.71 for the whole of Brazil [17].
Ribeirão Preto is a city in the State of São Paulo, located at alatitude of 21◦ south. Its urban area has 504,923 inhabitants [2].The city is located 400 km inland, at an altitude of 558 m, with atropical highland climate. The UVI ranges from 6 to 8 between Mayand September and is greater than 10 between October and April[18]. The city’s HDI in 2011 was 0.85.
Santos is a city in the State of São Paulo, located at a latitudeof 23◦ south. Its urban area has 417,098 inhabitants [2]. The city islocated on the coast, with a subtropical climate. The UVI range isfrom 5 between May and September and above 10 between Octoberand April [19]. The city’s HDI in 2011 was 0.87.
Londrina is a city in the State of Paraná, in the southern region,located at a latitude of 23◦ south. Its urban area has 505,184 inhabi-tants [2]. The city is located 300 km inland, at an altitude of 610 m,with a subtropical climate. The UVI range is from 6 to 9 betweenMay and September to above 10 from October to May [19]. Thecity’s HDI in 2011 was 0.82.
2.2. Patients
The patients were seen consecutively in MS centers where theauthors worked, between January 1, 2002, and December 31, 2009.All the patients, without any exception, originate from those fourcities and from nearby, when they were visiting the centers forthe first time, in between questions about their disease, they wereasked about their ancestry. The answers from the patients withMS diagnoses confirmed using the McDonald criteria of 2001 [20]were included. The first four authors of the present paper per-sonally interviewed the patients in each city at the time of theirroutine visits. The patients were asked about their ancestry, goingback three generations. If unable to answer the questions, thepatients were requested to ask their parents and relatives, or evento find documents regarding their ancestry. The patients wouldthen provide the required information at a subsequent visit. Theancestry was considered according to the origin of the patient’s par-ents, grandparents or great-grandparents. Patients who reportedhaving two or more ancestors of origins other than Brazilian wereregistered according to their maternal ancestry, as had previouslybeen decided.
The patients voluntarily consented to give their informa-tion for this study. The whole dataset forms part of thepatients’ medical files. The ethics committees of the MedicalSchool of Ribeirão Preto (USP), Londrina State University and

1644 E.R. Comini-Frota et al. / Clinical Neurology and Neurosurgery 115 (2013) 1642– 1646
Table 1Epidemiological and clinical profile of 652 MS patients from four cities in Brazil.
Ribeirão Preto Belo Horizonte Londrina Santos
Patients (n) 273 184 150 45Gender
Female(%) 186 (68) 139 (75) 103 (68) 39 (86)Ethnicity
Whites (%) 145 (53) 142 (77) 135 (90) 35 (78)Afro-Brasilians 123 51 10 8Blacks 5 2 3 2Orientals 0 0 2 0
Age at last visit * (y)Median (range/IQR) 43 (10–82/23–37) 40 (17–62/23–38) 43 (18–69/26–43) 42 (12–65/27–43)
Disease duration (y)Median (range/IQR) 10 (1–48/6–15) 8 (0.5–42/3–13) 7 (0.5–40/3–11) 5 (0.5–22/4–15)
EDSS at last visitMedian (range/IQR) 3.0 (0–9.5/2.0–6.5) 3.0 (0–9.5/1.5–5.0) 2.0 (0–8.0/1.0–3.5) 1.0 (0–6.5/2.5–4.5)
Table 2Reported ancestries of 652 MS patients from four cities in Brazil.
Ancestries n (%) Ribeirão Preto Belo Horizonte Londrina Santos Total
Brazilian 94 (34.4) 101 (54.8) 5 (3.3) 11 (24.4) 211 (32.3)Italian 103 (37.7) 63 (34.2) 105 (70.0) 16 (35.5) 287 (44)Spanish 29 (10.6) 3 (1.6) 12 (8.0) 5 (11.1) 49 (7.5)
Ma
swtoP
2
(cwteiDsS
3
crtwiSwler
rlo
(64%) came as complete families from northern Italy, primarilyfrom the Veneto, Piedmont and Lombardy regions [23]. The currentprevalence of MS in northern Italy is high, ranging from 69/100,000in Ferrara [24] to 82.5/100.000 in Padua [25] and 94/100,000
Table 3Reported maternal ancestries of 379 MS patients of Belo Horizonte, Londrina andSantos n (%).
Belo Horizonte Londrina Santos Total
Italians 36(58) 38 (36) 9(56) 83(45)
Portuguese 41 (15.0) 8 (4.3)Others 6 (2.1) 9 (4.8)
Total 273 184
etropolitan University of Santos (i.e. the authors’ institutions)pproved the study.
The records relating to the MS patients in the four cities wereubsequently reviewed to verify whether their European ancestryas maternal or paternal. This information was ascertained in rela-
ion to the patients in Belo Horizonte, Londrina and Santos (a totalf 379 patients). However, the records from the patients in Ribeirãoreto did not contain information in this regard.
.3. Statistical analyses
The statistical analyses used the GraphPad Prism Software 5.02Prism Inc, San Diego, USA, 2007). The Fisher test was used toompare the proportion of European ancestry of the MS patientsith the proportion of European ancestry of each state’s popula-
ion. Two-way ANOVA and the Mann–Whitney test were used tovaluate parental ancestry relating to each city and each geograph-cal origin of ancestries. The significance level was set at P < 0.05.ata on immigration from Western Europe and population cen-
uses were obtained from the Brazilian Institute for Geography andtatistics (IBGE) website, www.ibge.org.br [2].
. Results
From January 1, 2002, to December 31, 2009, 652 patients withonfirmed diagnoses of MS visited our centers and their answerselating to ancestry were included in this study. Table 1 summarizeshe clinical and epidemiological data from these patients. Out of thehole group of 652 patients interviewed, 287 (44%) reported Ital-
an ancestry, 70 (10.5%) had Portuguese ancestry and 49 (7.5%) hadpanish ancestry, while 211 (32%) reported that all their ancestorsere born in Brazil. The other 35 (5.5%) reported other ancestries
ike Lebanese, English, German or Polish, with only a few patientsach. Table 2 summarizes the most prevalent ancestral groupseported by the patients in each city.
On the basis of the numbers of Italian immigrants that wereegistered and settled in each State, the proportions of the popu-ation with Italian ancestry was calculated to be 39% in the Statef Paraná, 30% in the State of São Paulo and 8% in the State of
14 (9.3) 7 (15.5) 70 (10.7)14 (9.3) 6 (13.3) 35 (5.3)
150 45 652
Minas Gerais [2]. There were no estimates relating to Portugueseor Spanish ancestry in these States. The MS patients interviewed inBelo Horizonte and Londrina reported higher proportions of Italianancestors than in the whole populations of the respective States(Fisher test, P < 0.0001). The patients in Ribeirão Preto and Santos,both in the State of São Paulo, also reported larger numbers of Ital-ian ancestors than in the whole population of the State, but thesenumbers did not reach statistical significance. The characteristicsrelating to the disease (age of onset, EDSS [21] and disease dura-tion) did not differ for groups of patients with different ancestry(P > 0.05 for all comparisons, data not shown).
Parental ancestry was not a significant factor (P > 0.05) differen-tiating MS patients who reported a European ancestor, regardlessof the city (Belo Horizonte or Londrina or Santos) or geographicalorigin of ancestor (Italian, Spanish, Portuguese or others) (Table 3).
4. Discussion
This is the first report on ancestry among Brazilian MS patients.Unexpectedly, most of our patients with a European ancestor wereof Italian origin. In fact, 42% of the 3,078,937 immigrants who cameto Brazil between 1890 and 1930 were from Italy, 31% were Por-tuguese and 15% were Spanish. Other immigrants were German,Polish or from other origins like Syrian, Lebanese, Japanese andother Europeans [2,22]. Most Italians who immigrated to Brazil
Spanish 3(100) 5(41) 5(100) 13(65)Portuguese 3(37.5) 8(57) 4(58) 15(51)Others 5(55) 3(21) 5(83) 13(44)Total 47(56) 54(37) 23(67) 124(47)

gy an
igHedSw
dedTfc6iaoc
wtrwddmwaEwoBUUgtewgB
fEtHiwhileoi
ttPdmnwsaet
E.R. Comini-Frota et al. / Clinical Neurolo
n Genoa [26]. Italian immigrants came preferentially to coffee-rowing areas and to flourishing cities, which Ribeirão Preto, Beloorizonte and Londrina all were at the time of immigration. Theystablished their families in these areas and participated in theevelopment of these cities. Around 30% of the Italians settled in thetate of São Paulo, close to areas where Portuguese communitiesere also established [23].
The Portuguese workers (mostly men) who immigrated to Braziluring the first half of the twentieth century came from north-rn Portugal and settled in commercial areas of big cities like Rioe Janeiro and São Paulo, and in the port city of Santos [2,22].he prevalence of MS in Portugal was studied recently and wasound to be 46.5/100,000 inhabitants in the central region of theountry [27]. In Spain, MS prevalence ranges from 40.1/100,000 to8.6/100,000 in different regions [28,29]. The majority of Spanish
mmigration consisted of workers without families, from Galiciand Andalucía. Seventy-eight percent of them settled in the Statef São Paulo, mostly in port cities like Santos, and others went to bigities in the States of Rio de Janeiro, Minas Gerais and Bahia [22].
At the time of the mass immigration, these Brazilian citiesere underdeveloped with regard to hygienic sanitation, educa-
ion or public healthcare facilities. On the other hand, the Europeansegions from where the majority of the immigrants came were notell developed, either. However, differences in climate gave rise toifferences in the infesting microorganisms and parasites. Tropicaliseases like cestodes, helminths, neurocysticercosis, schistoso-iasis and American trypanosomiasis (Chagas disease) infestationsere the most important public health problems in southeastern
nd southern Brazil in the first half of the twentieth century. Inurope, there were no reports of these infestations and Influenzaas the most important public health problem [30]. Otherwise,
ne of the most important environmental differences between therazilian cities studied here and those European countries was theVI. The majority of the immigrants moved from countries withVI ranging from 1 to 5 (very low to low), to cities with UVI ran-ing from 7 to 11 (high to extreme). The body of evidence pointsoward these two environmental factors, infections and sunlightxposure, as important influences on MS prevalence around theorld [3,4,31,32]. Hence, these factors could have influenced the
enetic background of Europeans and their descendants living inrazil.
The frequency of Italian ancestry among the MS patients in theour cities was significantly higher than the frequency of any otheruropean ancestry, or even the frequency of solely Brazilian ances-ry in three of the cities. These results especially stood out in Beloorizonte and Londrina. We observed that the majority of the Ital-
an immigrants came with their whole families, which did not occurith Spanish and Portuguese immigrants. This characteristic mayave led to a longer time without admixture in Brazil for the Ital-
ans and earlier admixture of the Spanish and Portuguese with theocal populations at that time. We could not find any equivalentstimates of Portuguese and Spanish ancestry for the populationsf the cities and States studied, with regard to the most recentmmigration.
The city of Ribeirão Preto did not differ in Italian ancestry fromhe State of São Paulo. In explaining this, it should firstly be notedhat the majority of the Italian immigrants settled in the State of Sãoaulo, and therefore the whole State has large numbers of descen-ants from immigrants. On the other hand, Ribeirão Preto is theost important industrial, university and medical center of the
orthern region of the State and the native population is mixedith many other migrants from other regions of Brazil. It is pos-
ible that these two situations together have created differencesmong patients in Ribeirão Preto with regard to ancestry. In Santosither had any difference, as a harbor city, the immigration settledhere was a small sample of all immigrants who came to Brazil.
d Neurosurgery 115 (2013) 1642– 1646 1645
From the five published studies on prevalence rates in Brazil-ian cities, we calculated the gradient from Recife to São Paulo andfound that there was an increase in prevalence of 0.91/100,000inhabitants per degree of latitude. This rate is three times greaterthan the gradient determined for Latin America [6], although it islower than the mean for the regions with European populations(3.57/100,000). On the other hand, it is higher than in the regionswith non-European populations (0.07/100,000) [5]. The gradientfrom Recife to Belo Horizonte was found to be an increase of1.5/100,000 per degree of latitude. Belo Horizonte seemed to standout from the overall gradient.
According to this scenario, Italian immigration in particular, outof all the European immigration, was possibly one of the factorscontributing toward the MS prevalence rates in two out of the fourcities studied. As a corollary, admixtures with other ethnic groups,including Africans and Native Americans, and associations withenvironmental factors, especially infections and sunlight exposure,may have been factors that contributed toward lower MS frequencyin the southern and southeastern regions of Brazil, in compari-son with the levels observed recently in Europe, especially in Italy,Spain and Portugal.
Our study has many limitations. The most important of thesewere that this was a descriptive study on reported ancestry, andin Ribeirão Preto we were unable to analyze which generation orwhich parent had immigrant origins. The reason for this is thatwhen we started this study, there was no reference to the origin ofparents in the way that is now available [33,34]. However, amongthe 379 patients for whom analysis on maternal or paternal Euro-pean ancestry was possible, no significant differences were seenwith regard to parental origins, or the cities or geographical ori-gins of ancestors. It is likely that the study design, with informationgathered on three generations of ancestry, may have diluted suchinfluence. The patients studied were attended at regional referencecenters and therefore came not only from these cities, but also fromcommunities in the surrounding municipalities. Nonetheless, theywere a reasonably large sample representing the respective Statepopulations, which was why we compared them with the propor-tions of descendants in the States. We did not find any data on theSpanish and Portuguese proportions in the State populations, andso we were unable to compare the proportions of these two ances-tries among our MS patients. Other important limitation was thedesign of study itself because reported ancestry is not a guaranteeof genetic background. However, it should be noted that the HLAalleles of some of our patients in Ribeirão Preto and Londrina weredetermined [12–14] and the same linkage disequilibrium towardHLA DRB*1501 that has been found in patients in other parts of theworld, especially in Italy, Spain and Portugal.
Other studies trying to understand the genetic diversity andbackground of Brazilian patients have been conducted [35–37].Because this population is so highly admixed, with such great dif-ferences between the country’s regions, many more studies areneeded in order to confirm or complete our data.
5. Conclusion
Despite the few data on MS prevalence rates in Brazil, thereseems to be a latitude-dependent north–south gradient of preva-lence in this country. The gradient is greater than what has beenfound overall for Latin America. Cities in the southern and south-eastern regions of Brazil had higher prevalence than northeastern,thereby increasing the north–south gradient. According to our data,
the massive European immigration, especially from Italy, that ledto settlement in south and southeastern regions at the beginningof the twentieth century, was one of the factors that contributedtoward these findings.
1 ogy an
F
aB
C
i
R
[
[
[
[
[
[
[
[[
[[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
646 E.R. Comini-Frota et al. / Clinical Neurol
unding
This work was partially funded by FAEPA (Fundacão de Amparoo Ensino e Pesquisa) of Medical School of Ribeirão Preto (USP),razil.
onflict of interest
The authors declare that no conflicts of interest were involvedn this work.
eferences
[1] Ferreira LB, Mendes-Junior CT, Wiezel CE, Luizon MR, Simoes AL. Genomicancestry of a sample population from the state of Sao Paulo, Brazil. AmericanJournal of Human Biology 2006;18:702–5.
[2] Brazilian Statistics and Geography Institute website www.ibge.org.br (IBGE).[3] Ascherio A, Munger K. Epidemiology of multiple sclerosis: from risk factors to
prevention. Seminars in Neurology 2008;28:17–28.[4] Wingerchuk DM, Weinshenker BG. Multiple sclerosis: epidemiology, genetics,
classification, natural history, and clinical outcome measures. NeuroimagingClinics of North America 2000;10:611–24, vii.
[5] (a) Kurtzke JF. Geography in multiple sclerosis. Journal of Neurology1977;215(1):1–26;(b) Simpson Jr S, Blizzard L, Otahal P, Van der Mei I, Taylor B. Latitude is signif-icantly associated with the prevalence of multiple sclerosis: a meta-analysis.Journal of Neurology, Neurosurgery and Psychiatry 2011;82:1132–41.
[6] Risco J, Maldonado H, Luna L, Osada J, Ruiz P, Juarez A, et al. Latitudinalprevalence gradient of multiple sclerosis in Latin America. Multiple Sclerosis2011;17:1055–9.
[7] Ferreira ML, Machado MI, Vilela ML, Guedes MJ, Ataide Jr L, Santos S, et al.Epidemiology of 118 cases of multiple sclerosis after 15 years of follow-up onthe reference center of Hospital da Restauracao, Recife, Pernambuco, Brazil.Arquivos de Neuro-Psiquiatria 2004;62:1027–32.
[8] Fragoso YD, Peres M. Prevalence of multiple sclerosis in the city of Santos SP.Revista Brasileira de Epidemiologia 2007;4:479–82.
[9] Callegaro D, Goldbaum M, Morais L, Tilbery CP, Moreira MA, Gabbai AA, et al.The prevalence of multiple sclerosis in the city of Sao Paulo, Brazil, 1997. ActaNeurologica Scandinavica 2001;104:208–13.
10] Kaimen-Maciel DR, Medeiros M, Pistori R, Biaggio C, Rocha F, Lopes LHG. Theprevalence of multiple sclerosis in two cities in the north of Parana State, Brazil.ECTRIMS Multiple Sclerosis 2004;10:S158.
11] Lana-Peixoto MA, Frota ERC, Campos GB, Monteiro LP. The prevalence ofmultiple sclerosis in Belo Horizonte Brazil. Arquivos de Neuro-Psiquiatria2012;70(2):102–7.
12] Brum DG, Barreira AA, Louzada-Junior P, Mendes-Junior CT, Donadi EA. Asso-ciation of the HLA-DRB1*15 allele group and the DRB1*1501 and DRB1*1503alleles with multiple sclerosis in White and Mulatto samples from Brazil. Jour-nal of Neuroimmunology 2007;189(September (1/2)):118–24.
13] Brum DG, Barreira AA, dos Santos AC, Kaimen-Maciel DR, Matiello M, CostaRM, et al. HLA-DRB association in neuromyelitis optica is different fromthat observed in multiple sclerosis. Multiple Sclerosis 2010;16(January (1)):
21–9.14] Kaimen-Maciel DR, Reiche EM, Borelli SD, Morimoto HK, Melo FC, LopesJ, et al. HLA-DRB1* allele-associated genetic susceptibility and protectionagainst multiple sclerosis in Brazilian patients. Molecular Medicine Reports2009;2(November–December (6)):993–8.
[
d Neurosurgery 115 (2013) 1642– 1646
15] Alves-Leon SV, Papais-Alvarenga R, Magalhães M, Alvarenga M, Thuler LC,Fernández, et al. Ethnicity-dependent association of HLA DRB1-DQA1-DQB1alleles in Brazilian multiple sclerosis patients. Acta Neurologica Scandinavica2007;115(May (5)):306–11.
16] Silva A. UV radiation measures and public health in Belo Horizonte. RevistaBrasileira de Geofísica 2008;26(October–December (4)).
17] United Nations Development Programme http://www.undp.org18] Kirschoff VWJH, Echer E, Leme NP, Silva AA. The seasonal variation of biologi-
cally active UV-B. Brazilian Journal of Geophysics 2000;18(1).19] National Institute of Spacial Reaserch, Brazil http://satelite.cptec.inpe.br/uv20] McDonald WI, Compston A, dan G, Goodkin D, Hartung HP, Lublin FD, et al.
Recommended diagnostic criteria for multiple sclerosis: guidelines from theInternational Panel on the diagnosis of multiple sclerosis. Annals of Neurology2001;50:121–7.
21] Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expandeddisability status scale (EDSS). Neurology 1983;33:1444–52.
22] Cenni F. Italianos no Brasil, vol. 186. Sã̃o Paulo: Editora da Universidade de SãoPaulo; 2003.
23] Hakkert R. Republic of Italy (country profile). International demographics1986;5:1–9.
24] Granieri E, Malagu S, Casetta I, Tola MR, Govoni V, Paolino E, et al. Multiplesclerosis in Italy. A reappraisal of incidence and prevalence in Ferrara. Archivesof Neurology 2001;53:793–8.
25] Ranzato F, Perini P, Tzintzeva E, Tiberio M, Calabrese M, Ermani M, et al. Increas-ing frequency of multiple sclerosis in Padova, Italy: a 30 year epidemiologicalsurvey. Multiple Sclerosis 2006;9:387–92.
26] Solaro C, Allemani C, Messmer Uccelli M, Canevari E, Dagnino N, et al. Theprevalence of multiple sclerosis in the north-west Italian province of Genoa.Journal of Neurology 2005;252:436–40.
27] De Sa J, Paulos A, Mendes H, Becho J, Marques J, Roxo J. The prevalence ofmultiple sclerosis in the District of Santarem, Portugal. Journal of Neurology2006;253:914–8.
28] Garcia-Gallego A, Morera-Guitart J. Prevalence and characteristics of multi-ple sclerosis in the health district of the Marina Alta. Revista de Neurologia2002;34:732–7.
29] Casquero P, Villoslada P, Montalban X, Torrent M. Frequency of multiple sclero-sis in Menorca, Balearic islands, Spain. Neuroepidemiology 2001;20: 129–33.
30] Scotto G. Infections in the history of medicine: globalization and infections inmedicine, the past and the future. Le Infezioni in Medicina 2011;1:56–61.
31] Disanto G, Morahan JM, Ramagopalan SV. Multiple sclerosis: risk factorsand their interactions. CNS and Neurological Disorders – Drug Targets2012;11(August (5)):545–55.
32] Ramagopalan SV, Sadovnick AD. Epidemiology of multiple sclerosis. NeurologicClinics 2011;29(May (2)):207–17.
33] Ramagopalan SV, Yee IM, Dyment DA, Orton SM, Marrie RA, Sadovnick AD,et al. Parent-of-origin effect in multiple sclerosis: observations from interracialmatings. Neurology 2009;73(8):602–5.
34] Ebers GC, Sadovnick AD, Dyment DA, Yee IM, Willer CJ, Risch N. Parent-of-origin effect in multiple sclerosis: observations in half-siblings. Lancet2004;363(9423):1773–4.
35] Brum DG, Barreira AA, Donadi EA, Santos A, Costa R, Kaimen Maciel DR,et al. Genetic and geographic descriptors of ancestry in Brazilian multiplesclerosis and neuromyelitis optica patients. ECTRIMS 2009. Multiple Sclerosis2009;15:S-182.
36] Vasconcelos CC, Fernández O, Leyva L, Thuler LC, Alvarenga RM. Does theDRB1*1501 allele confer more severe and faster progression in primary pro-
gressive multiple sclerosis patients? HLA in primary progressive multiplesclerosis. Journal of Neuroimmunology 2009;214(September (1/2)): 101–3.37] Ferreira Vasconcelos CC, Cruz Dos Santos GA, Thuler LC, Camargo SM, PapaisAlvarenga RM. African ancestry is a predictor factor to secondary progressionin clinical course of multiple sclerosis. ISRN Neurology 2012;2012:410629.