Frailty in liver transplantation: An expert opinion ......11Division of Gastroenterology & Liver...
12
Transcript of Frailty in liver transplantation: An expert opinion ......11Division of Gastroenterology & Liver...

Am J Transplant. 2019;00:1–11. amjtransplant.com | 1© 2019 The American Society of Transplantation and the American Society of Transplant Surgeons
Received:2February2019 | Revised:18March2019 | Accepted:28March2019DOI: 10.1111/ajt.15392
M E E T I N G R E P O R T
Frailty in liver transplantation: An expert opinion statement from the American Society of Transplantation Liver and Intestinal Community of Practice
Jennifer C. Lai1 | Christopher J. Sonnenday2 | Elliot B. Tapper3 | Andres Duarte‐Rojo4 | Michael A. Dunn5 | William Bernal6 | Elizabeth J. Carey7 | Srinivasan Dasarathy8 | Binita M. Kamath9 | Matthew R. Kappus10 | Aldo J. Montano‐Loza11 | Shunji Nagai12 | Puneeta Tandon13
1Division of Gastroenterology and Hepatology, University of California‐San Francisco, San Francisco, California2SectionofTransplantation,UniversityofMichigan,AnnArbor,Michigan3DivisionofGastroenterology,UniversityofMichigan,AnnArbor,Michigan4DivisionofGastroenterology&Hepatology,UniversityofArkansasforMedicalSciences,LittleRock,Arkansas5CenterforLiverDiseases,ThomasE.StarzlTransplantationInstitute,andPittsburghLiverResearchCenter,UniversityofPittsburgh,Pittsburgh,Pennsylvania6InstituteofLiverStudies,KingsCollegeHospital,London,UK7DivisionofGastroenterologyandHepatology,MayoClinic,Scottsdale,Arizona8DivisionofGastroenterologyandHepatology,ClevelandClinic,Cleveland,Ohio9Division of Gastroenterology, Hepatology, and Nutrition, University of Toronto, Toronto, Canada10DivisionofGastroenterology,DukeUniversitySchoolofMedicine,Durham,NorthCarolina11DivisionofGastroenterology&LiverUnit,UniversityofAlberta,Edmonton,Alberta,Canada12DivisionofTransplantSurgery,HenryFordHospital,Detroit,Michigan13CirrhosisCareClinic,DivisionofGastroenterology,UniversityofAlberta,Edmonton,Alberta,Canada
Abbreviation:ADLs,activitiesofdailyliving.
CorrespondenceJenniferC.LaiEmail:[email protected]
Funding informationMikatiFoundationGrant;NationalInstituteofGeneralMedicalSciences,Grant/AwardNumber:R01GM119174;NationalInstitute of Diabetes and Digestive and KidneyDiseases,Grant/AwardNumber:R01DK113196andU01DK061732;OfficeofAIDSResearch,Grant/AwardNumber:R21AR071046;NationalInstituteonAging,Grant/AwardNumber:K23AG048337andR01AG059183;NationalInstituteonAlcoholAbuseandAlcoholism,Grant/AwardNumber:P50AA024333andU01AA0026976
Frailty has emerged as a powerful predictor of outcomes in patientswith cirrho‐sis and has inevitablymade itsway into decisionmakingwithin liver transplanta‐tion.Inanefforttoharmonizeintegrationoftheconceptoffrailtyamongtransplantcenters,theASTandASTSsupportedtheeffortsofourworkinggrouptodevelopthisstatementfromexpertsinthefield.Frailtyisamultidimensionalconstructthatrepresentstheend‐manifestationofderangementsofmultiplephysiologicsystemsleadingtodecreasedphysiologicreserveandincreasedvulnerabilitytohealthstress‐ors.Inhepatology/livertransplantation,investigationoffrailtyhaslargelyfocusedonphysicalfrailty,whichsubsumestheconceptsoffunctionalperformance,functionalcapacity,anddisability.Therewasconsensus thatevery liver transplantcandidateshouldbeassessedatbaselineand longitudinallyusingastandardized frailty tool,whichshouldguidetheintensityandtypeofnutritionalandphysicaltherapyinindi‐viduallivertransplantcandidates.Theworkinggroupagreedthatfrailtyshouldnotbeusedasthesolecriterionfordelistingapatientforlivertransplantation,butrather

2 | LAI et AL.
1 | INTRODUC TION
Frailtyhasemergedasafundamentalforceshapingthefieldoflivertransplantation.Liverdiseaseseverityattransplantationisworsen‐ing,theproportionofolderadults(≥65years)awaitingtransplanta‐tion is rising,andtheprevalenceofobesity‐related liverdisease israpidlyescalating—allofwhicharecontributingtoacohortoflivertransplant patients who are sicker, more medically complex, andincreasingly being described as “frail.” Clinicians caring for thesepatientshavelongintuitedtheimportanceoffrailtyonhealthout‐comes before and after liver transplantation, even removing patients fromthewaitlistforbeing“toofrailfortransplant.”Yetdespitethefactthattheconceptoffrailtyhasinevitablymadeitswayintotrans‐plantdecision‐making,itsintegrationintoclinicaltransplantpracticethus far has been haphazard, hindered by a lack of consensus onits definition, tools for assessment, and implications for transplant decision‐making.1
To overcome these barriers, the American Society ofTransplantationsupportedtheeffortsofourworkinggroupofex‐pertsinthefieldtodevelopthisstatementonfrailtyinlivertrans‐plantation.Ourspecificgoalswereto:(a)definefrailty,(b)appraisetoolsforfrailtymeasurement,and(c)developanalgorithmforprac‐tical incorporation of frailty into clinical practice.While much ofthisdocumentappliestopatientswithcirrhosis,regardlessoftheirtransplanteligibility, thisstatementwasprimarily intendedfor thetransplantsetting;wehavehighlightedspecificareas inwhichourrecommendationsmaydifferwhetherornotthepatientislistedforliver transplantation.
Onewordofcautionwhenimplementingourrecommendations:wedonotsupporttheuseofaone‐timeassessmentoffrailtyasthesole criterion for declining a patient for liver transplantation. Our goalwiththisdocumentistofacilitatethesystematicincorporationofastandardizedfrailtyassessmentforevery patient at evaluation andlongitudinallywhileawaitinglivertransplantationinordertoac‐curatelycaptureprogressionoffrailtyonthewaitlistaswellasserveasthefoundationforfrailtyintervention.
1.1 | Defining “frailty” in the setting of liver transplantation
Theconceptoffrailty ismostcommonlydefinedasadistinctbio‐logicsyndromeofdecreasedphysiologicreserveandincreasedvul‐nerabilitytohealthstressorsthatpredisposesonetoadversehealth
outcomes.2 Frailty is a multidimensional construct, and represents theend‐manifestationofderangementsofmultiplephysiologicsys‐temsincludingallindividualsolidorgansystems(eg,theliver,kidney,heart),inflammatory,endocrine,cognitive,andmusculoskeletalsys‐tems,aswellaspsychosocialfactors.
While frailty has generally been conceptualized in the geriatricsarenaasdistinctfromfunctionalstatus,inthefieldsofhepatology/livertransplantation,theterm“frailty”haslargelyfocusedonphysical frailty (theaspectoffrailtyrelatedtofunctionalimpairment)duetoconsider‐ationsofmeasurementinthehepatologyandtransplantsettings.Tobeclear, functional status refers to one's ability to perform daily activities, fulfill social roles, andmaintain health/well‐being3and subsumes theconcepts of functional performance, functional capacity, and disability. Inthecontextoflivertransplantation,thefocusonthephysicalfunc‐tionalaspectsoffrailtyhastheadvantageoverabroaderconceptual‐izationoffrailty(thatincludescognitive,social,andemotionalaspects)given the need for objectivity of measurement. Although cognitivefrailtyispredictiveofoutcomeincirrhosis,4,5thelackofstandardizedtoolsfortheassessmentofcognitivedysfunctionincirrhosisandtheoverlapwithhepaticencephalopathymakes itdifficult toobjectivelyevaluate this more encompassing definition of frailty at this time.Importantly,“physicalfrailty,”asinvestigatedinpatientswithcirrhosis,isacriticaldeterminantofadversehealthoutcomesinthispopulation,includingwaitlistmortality,6‐11mortalityafterhospitalizationandafterliver transplantation,12‐15needforhospitalization,lengthofstay,14,16‐18 anddischargelocation(ie,rehabilitationfacility)13,14(Table1).
Major components of frailty in all patients include skeletalmuscle mass depletion (sarcopenia), progressive immobility, de‐creased energy expenditure, andmalnutrition.2 In patientswithcirrhosis, there aremultiple liver‐specific factors that exacerbateandacceleratethiscycleoffrailty(Figure1).Chronicinflammationfromtheunderlyingliverdiseaseisoftentheinitialinsult.Hepaticsyntheticdysfunctionresultsintheimpairmentofmuscleproteinsynthetic response that can rapidly lead to progressive musclebreakdown. Anorexia associated with malaise (from chronic in‐flammation)andearlysatiety(fromascites)leadstomalnutrition,furtheracceleratingmusclewasting.Hepaticencephalopathyandcognitivedeclinemagnifytheexpressionoffrailtythroughmulti‐ple pathways, including altered taste perception, fatigue, immo‐bility,anddecreasedenergyexpenditure.Theobligatoryshiftofammoniafromlivertomuscleforexportasglutamine—divertingglutamateneededformuscleproteinsynthesis—isalsorecognizedtobeapivotaldriverofmusclewasting.Ammoniaitselfpromotes
shouldbeconsideredoneofmanycriteriawhenevaluatingtransplantcandidacyandsuitability.Aroadmaptoadvancefrailtyintheclinicalandresearchsettingsoflivertransplantationispresentedhere.
K E Y W O R D S
clinicalresearch/practice,guidelines,livertransplantation/hepatology,nutrition,recipientselection

| 3LAI et AL.
TAB
LE 1
Metricsofphysicalfrailty,fitness,ordisabilitystudiedinpatientswithcirrhosis(wherethestudyincludedanadjustmentforliverdiseaseseverity)
Tool
Stud
yD
etai
lsN
Scor
eA
ssoc
iatio
n w
ith o
utco
mes
(ove
rall
mor
talit
y
unle
ss o
ther
wis
e sp
ecifi
ed)
ADL
Lai20146
Out
patie
nt29
4≥1disability(24%)
HR:1.2395%CI(0.91‐1.66)
Sam
oylo
va 2
01728
Out
patie
nt458
≥1disability(49%)
sHR:1.895%CI(1.4‐2.4)
Tapp
er 2
01514
Inpa
tient
73
4ADL<12:9.2%withoutHEand24%
withHE**
ADL<12:HR1.895%CI(1.1‐3.2)
CFS
Ran
ge 1
‐9Ta
ndon
201
616O
utpa
tient
300
CFS>4:18%
CFS>3:51%
OR(per1unit):1.9(1.4‐2.6)
Ney20184
Out
patie
nt35
5MoCA‐CFSscore(cognitive+physical
frailty)
ORofanHE‐relatedhospitalization:
01
13.3(1.5‐7.7)
25.7(1.9‐17.3)
KarnofskyPerformanceScale
(rangeA‐Cor0‐100)
Malinis201429
Tran
spla
nt re
gist
ry
35686
KPS(BorC):63.4%
5‐yrmortality:sHR1.30(1.23‐1.37)
Orm
an 2
01611
Tran
spla
nt re
gist
ry70
092
KPS(BorC):56%
1‐yearmortalitybyKPS:A(11.4%),B(15.5%),C
(27.4%)KPSB:HR1.0895%CI(1.04‐1.111)KPS
C:HR1.2695%CI(1.20‐1.33)
Tand
on 2
01715
Hospitalized
DecompensatedCirrhosis
954
KPS(BorC):68%
3‐monthpostdischargemortality:ByKPS:A(5%),
B(11%),C(23%)KPS(per1‐unit):OR0.9795%CI
(0.96‐0.98)
BradenScaleRange6‐23
Tapp
er 2
01514
Hospitalized
DecompensatedCirrhosis
734
Moderate‐tohigh‐riskBradenScale:
≤18(28.1%HE,13.7%withoutHE)
90‐d
ay m
orta
lity
Score16‐18:2.7195%CI(1.88‐3.90)
Score<16:1.8595%CI(0.83‐4.12)
Sund
aram
201
713O
utpa
tient
Alltransplantlisted
341
Moderate‐tohigh‐riskBradenScale:
16‐18:(17%),≤16(20%)
Posttransplantmortality:insufficientoutcomes
FFPRange0‐5
Lai20146
OutpatientAlltransplantlisted
294
FFP≥3:17%
Perpoint:1.4595%CI(1.04‐2.02)
Tand
on 2
01616
Out
patie
nt
Cirrhosis
300
FFP≥3:35%
OR
4.0
Sinc
lair
201718
Out
patie
nt
Alltransplantlisted
587
FFP≥3:32%
Hospitalizationdaysper12months
IRR:1.295%CI(1.02‐1.44)
Tapper20185
Out
patie
nt
Alltransplantevaluated
685
FFP≥3:41%
Tran
spla
nt‐f
ree
surv
ival
H
R pe
r FFI
poi
nt:
WithoutHE:1.37(1.20‐1.58)
WithHE:1.14(0.98‐1.33)
(Continued)

4 | LAI et AL.
Tool
Stud
yD
etai
lsN
Scor
eA
ssoc
iatio
n w
ith o
utco
mes
(ove
rall
mor
talit
y
unle
ss o
ther
wis
e sp
ecifi
ed)
6MWDMeterswalked
Car
ey 2
0109
Out
patie
nt
Alltransplantlisted
121
Mean6MWD
6
9 ±
122
mPer100m:0.5895%CI(0.37‐0.93)
Yadav2015
30O
utpa
tient
Alltransplantlisted
213
Mean6MWD
37
1 ±
121
m
12%≤250m
250mcutoff:HR2.195%CI(0.9‐4.7)
FaustiniPereira
2016
12O
utpa
tient
86Mean6MWD
410±27.8m
<410mwalked(unadjusted):RR4.2195%CI
(1.25‐6.41)
Gaitspeed(meters/second)
Dun
n17O
utpa
tient
373
Meangaitspeed
0.95
± 0
.25
m/s
Hos
pita
l bed
‐day
s Per0.1m/s:RR0.85(0.74‐0.98)
SPPBRange0‐12
Lai20146
Out
patie
nt
Alltransplantlisted
294
SPPB<9:31%
Perpoint:1.1995%CI(1.07‐1.32)
Tand
on 2
01616
Out
patie
nt
Cirrhosis
300
SPPB<10:38%
OR
2.5
LiverFrailtyIndexperpoint
Lai20177
Out
patie
nt
Alltransplantlisted
529
MedianLFI:3.8(3.4‐4.3)
Wai
tlist
mor
talit
y Perpoint:HR2.295%CI(1.7‐2.9)
CardiopulmonaryExercise
TestingmL/kg/min
Ney
201
610Systematicreviewof:Outpatient
Alltransplantlisted
1107
Ventilatoryanaerobicthreshold(AT)
Peakexerciseoxygenuptake(peak
VO2)
Posttransplantmortality(meandifferencebe‐
tweensurvivorandnonsurvivors)
AT:2.095%CI(0.42‐3.59)
PeakVO2:0.7795%CI(−1.36‐2.90)
Abbreviations:6MWT,6‐minutewalktest;6MWD,6‐minutewalktestdistance;ADL,ActivitiesofDailyLiving;AT,anaerobicthreshold;CFS,ClinicalFrailtyScale;CPET,cardiopulmonaryexercisetest
‐ing;FFP,FriedFrailtyPhenotype;HE,hepaticencephalopathy;HR,hazardratio;KPS,KarnofskyPerformanceStatus;IADL,InstrumentalActivitiesofDailyLiving;IRR,incidencerateratio;LFI,Liver
FrailtyIndex;MoCA,MontrealCognitiveAssessment;OR,oddsratio;SPPB,ShortPhysicalPerformanceBattery.
TAB
LE 1
(Continued)

| 5LAI et AL.
muscleautophagy,directlyimpairscontractility,andtriggerssyn‐thesis and release ofmyotoxins contributing to sarcopenia.19 In additiontotheseliver‐relatedfactors,patientswithcirrhosisalsoexperiencenon–liver‐relatedfactors includingchronologicaging,non‐hepatic comorbidities (eg, coronary artery disease, diabeticperipheralneuropathy),andage‐relatedmusclewasting.Thecon‐tributions of these non–liver‐related factors are particularly im‐portantfortransplantdecision‐making,astheyarenotmodifiableandwillnotimproveaftertransplantation.20
Whilesarcopeniaisacentralanddominantcomponentoffrailtyinpatientswithcirrhosis,theconceptoffrailtyismoremultifacetedthansarcopeniaalone.Theinclusionoffunctionalmeasures(eg,chairstands,gaitspeed)invalidatedfrailtymetricssuggeststhattheinfluenceofsar‐copenia may be modified by factors related to muscle function ratherthanpurelymusclemass.Furthermore,theinfluenceofpatient‐reportedoutcomes (eg,exhaustion,sedentary time) implies thatan individual'sexperienceoftheirfrailtystatemayalsoinfluencehealthoutcomes.Thisconsensusstatementonlyaddressessarcopeniaasitrelatestotheover‐allconstructoffrailty;aseparateworkinggrouphasbeenassembledtomore specifically address sarcopenia as a single entity.
Key points
• Frailty is amultidimensional construct that represents theend‐manifestation of derangements ofmultiple physiologic systemsthatleadstodecreasedphysiologicreserveandincreasedvulner‐abilitytohealthstressors.
• Inhepatology/livertransplantation,theinvestigationoffrailtyhaslargely focused on physicalfrailtywhichsubsumestheconceptsoffunctional performance, functional capacity, and disability.
• Whilesarcopeniaisaprimarydriveroffrailtyinpatientswithcir‐rhosis,frailtyismoremultifacetedthansarcopeniaalone,offeringacomprehensiveassessmentofmusclefunctionandtheindividualpatient'sexperienceoftheirfrailtystatein addition to muscle mass.
1.2 | Measuring frailty in adult liver transplant patients
Table2 liststhetoolstocapturetheconstructoffrailtythathavebeen studied in patients with cirrhosis, including those awaiting
liver transplantation.We,again,emphasize that thestudies in thispatientpopulationhavelargelyfocusedonthephysicalcontributorsto frailty, including functional performance, functional capacity, and disability.
Intheresearcharena,frailtyindicesthatbestcapturethemulti‐dimensionalityoffrailtysuchastheFriedFrailtyPhenotype2ortheFrailty Index (“deficitmodel”21)may be necessary to demonstrateconstructvalidityofnewtoolsinpatientswithcirrhosis.However,these“traditional”modelsoffrailtyhavelimitedapplicabilitytotheclinicalpracticeoflivertransplantationinthattheyarenotcontin‐uously scored, display strong ceiling and/or floor effects, or are too complextouseinabusyclinicalpractice.1
With respect to the application of frailty tools in the clinicalarena,werecommendthateverytransplantcentershouldincorpo‐ratea standardized tool tomeasure frailty in their liver transplantpatientsbothatinitialevaluationandlongitudinallyonthewaitlist.This recommendation was based on evidence that standardizedfrailtymetrics can improve the accuracy of the “eyeball test” andtraditionalliverdiseasemetricstopredictmortalityinpatientswithcirrhosis.5,7‐14,21
Giventhatthereisnosinglefrailtytoolthathasemergedintheliteratureassuitable forevaluationofpatientswithcirrhosis inallclinicalscenarios (outpatientvs. inpatient; transplantvs.nontrans‐plant),werecommendafrailtytool kittoprovidearangeoftoolsthatcanbeuseddependingupontheclinicalsetting,availableresources,andintendedclinicaldecisionsthatwillbemadebasedonthetestresult. Here, we offer several points for each center to considerwhendecidingonwhichstandardized frailty tool(s) to incorporateinto clinical practice:
1. Frailty tools have been best studied in the outpatient setting.Measuressuch as the Fried Frailty Phenotype2 or Liver Frailty Index7 have, to date, only been studied in the outpatient hepatology/liver transplant settings where patients are in their “steadystate.” Hospitalized patients often have transient perturbationsin physical and cognitive function, which limit the ability ofthese performance‐based frailty assessments to represent trueunderlyingphysiologicreserve.However,whileperformance‐based tests may have limited use in the inpatient setting, provider‐and patient‐assessed tools such as the Karnofsky PerformanceStatus (KPS)andActivitiesofDailyLiving (ADL)scalehavebeenevaluated in the inpatient settings and demonstrated to predict
F I G U R E 1 Liver‐relatedandnon–liver‐relatedfactorsthatcontributetothedevelopmentofphysicalfrailtyinpatientswithcirrhosis

6 | LAI et AL.
TAB
LE 2
Propertiesofthetoolsevaluating“frailty”thathavebeenevaluatedinpatientswithcirrhosisa
Subj
ectiv
e ←
——
——
——
——
——
——
——
——
——
——
→
O
bjec
tive
CFS
KPS
AD
L/IA
DL
Brad
en s
cale
FFP
SPPB
LFI
Grip
str
engt
hG
ait s
peed
6MW
TCP
ET
Subj
ectiv
ityRe
quire
s cl
inic
ian
judg
men
t✔
✔✗
✔✗
✗✗
✗✗
✗✗
Can
be
bias
ed b
y pa
tient
repo
rtin
g ✔
✔✔
✔✔
✗✗
✗✗
✗✗
Predictivevalidity
For p
retr
ansp
lant
ou
tcom
es✔
✔✔
✔✔
✔✔
✔✔
✔✔
For p
ostt
rans
plan
t ou
tcom
es−
✔−
−−
−−
−−
−✔
Testcharacteristics
Reliability(internal
cons
iste
ncy
and
repeatability)
✔−
−−
−−
−✔
✔−
−
Resp
onsi
vene
ss to
changeovertime
✗✗
✗✗
✗✔
✔✔
✔−
−
Clin
ical
feas
ibili
tyEstimatedtimetaken
(minutes)
<1<1
<2<5
<10
<5<5
<1<2
<10
<60
Needforspecialized
equi
pmen
t✗
✗✗
✗✗
✗✔
✔✗
✗✔✔
Needforhighly
trai
ned
pers
onne
l ✗
✗✗
✗✗
✗✗
✗✗
✗✔✔
Abbreviations:6MWT,6‐minutewalktest;ADL,ActivitiesofDailyLiving;CFS,ClinicalFrailtyScale;CPET,cardiopulmonaryexercisetesting;IADL,InstrumentalActivitiesofDailyLiving;FFP,Fried
FrailtyPhenotype;KPS,KarnofskyPerformanceStatus;LFI,LiverFrailtyIndex;SPPB,ShortPhysicalPerformanceBattery.
Note:Doublecheckmarkindicatesthatthesetestsreallyneedspecializedtechniciansandequipmentmoresothantheotherteststhathaveonlyonecheckmark.
a No
data
ava
ilabl
e; ✔
yes
; ✗ n
o.

| 7LAI et AL.
nontransplant mortality,11,14,15 re‐admissions,14,16 and mortality after liver transplantation.11
2. Subjective tools for “screening” versus more objective frailty as‐sessment. Becauseof thepotential implications of frailty in thedecision to proceed with transplant, there was a consensusthatwaitlisted patients require assessmentwith objective, per‐ formance‐based frailty tools (eg, Liver Frailty Index, 6‐minutewalktest).Provider‐orpatient‐assessedmetricsoffrailty(eg,KPS,ADLs,ClinicalFrailtyScale),whilesimpleandfeasibletoadminister systematically in a busy clinical setting, may be insensitive to sub‐tle,butprognostic,gradientsofthefrailtyspectrum.Thatbeingsaid,inthelargerpopulationofpatientsinthenontransplantset‐ting, a stepwise approachwherepatients are screenedwith an“easy‐to‐perform” test, followedby amore comprehensive testtoeitherconfirmordefinitivelyruleoutfrailtymaybethemostpractical.
3. Measurement of longitudinal changes in frailty is clinically relevant in the transplant setting and requires frailty tools that are sensitive to change.Longitudinalchanges in frailtyarepredictiveofwait‐list mortality above and beyond a single assessment alone.22 MetricssuchasthecompositeLiverFrailtyIndex,whichiscon‐tinuous,lacksafloor/ceilingandhasbeenshowntobereliable/repro ducible,23areparticularlywell‐suitedforlongitudinalmeas‐urement, although additional research is needed to validatethe prognostic value of “Δfrailty” using the Liver Frailty Index.Identificationof frailty tools thataresensitivetochange ispar‐ticularlyrelevantasanendpointforclinicaltrialsaimingtoslowtheprogressionof—orevenreverse—frailty.
Basedonthesethreecriteria,weofferaparsimonioustoolkitcon‐sistingoftheKPSscale,ADL/IADLs,LiverFrailtyIndex,andthe6‐min‐utewalktestfortransplantclinicians (Table3).Whilenosingletool isperfectforeveryclinicalscenario,weselectedthesefourtoolsspecifi‐callytobalancetheneedsforspeed,low‐cost,patient‐centeredness,andobjectivity.
1.3 | Measuring frailty in pediatric liver transplantation
Arecent17‐centerstudydemonstratedthatfrailtyassessmentwiththeFriedFrailtyPhenotype is feasible in school‐agedchildrenwithchronicliverdisease;nearlyhalfofchildrenwithend‐stageliverdis‐ease met criteria for being frail.24 It isnotyetknowntheextent towhich frailty measures impact mortality. Metrics that incorporateperformance‐basedtestshavelimitedapplicationininfantsandtod‐dlerswhomaynotbeabletofullycooperatewithtestinginstructions(eg,gripstrength,chairstands).Frailtyassessment inpediatric livertransplantpatients<5yearsofagewilllikelyrequireacombinationofquantitativemusclemassmeasurement,laboratoryand/oranthropo‐metricnutritionalbiomarkers,andobservedassessmentsofactivity.
Key points
• Everypatientwithcirrhosisawaiting liver transplantation shouldbeassessedatbaselineandlongitudinallyusingastandardizedfrailtytool.
• Frailtymeasurementwithobjectiveperformance‐basedmeasures(eg,LiverFrailty Index) isbest studied in theoutpatient settingwhenpatientsareintheir“steadystate.”However,provider‐andpatient‐assessed instruments (eg, KPS, ADLs) have prognosticvalueamonghospitalizedpatients.
• Todate,theLiverFrailtyIndexhasthebroadestapplicabilityamongallthefrailtyinstrumentsforpracticalfrailtyassessmentinthelivertransplantsettingandhastheadvantagesofbeingobjective,per‐formance‐based, and suitable for longitudinal measurement.
1.4 | Incorporating frailty into clinical decision‐making
Webelieve that a single assessmentof frailty shouldnotbeusedasthesolecriterionforremovingapatientfromthelivertransplant
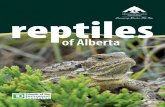
F I G U R E 2 Aconceptualmodelofsomeofthepatientcomponentsthatcliniciansincorporateintotheirglobalassessment of a patient's transplant candidacyandthetoolsthattheyusetoinformthisholisticassessment.Anobjectivefrailtytoolkitshouldbeusedtoinform clinicians’ assessments of muscle wasting,under‐nutrition,andphysicalinactivity—which,together,formthemajorcomponentsofphysicalfrailty—toimproveobjectivityandaccuracyoftheclinician's global assessment of transplant candidacyforthepurposesoftransplantdecision‐making(adaptedfromLaiJC,AJG2017)8
GlobalAssessment ofTransplantCandidacy
Patient Components
MELDNaChild Pugh Score
Vital signsEchocardiogram
CreatinineUrinalysis
Spirometry,Hemoglobin A1c,
Colonoscopy
Synthetic dysfunctionPortal hypertension
Measurement Tools
Cardiac function
Renal function
Other co-morbidities
Muscle wastingUnder-nutritionPhysical inactivity Objective Frailty Tool Kit
Eyeball test

8 | LAI et AL.
waitlist, as there are no data to support a single frailty cutoff atwhich a patient should not undergo liver transplantation. Instead,weadvocatethatastandardizedtoolforfrailtybeconsideredasone of manyobjectivecomponentsthatareroutinelyincorporatedintoaclinician'sassessmentofapatient'sglobalhealthstatusthatulti‐matelydetermineshisorhertransplantcandidacy(Figure2).8
Incorporating frailty into transplant decision‐making can offerthe liver transplant communitymore than simply prognostication.Whatmakes frailty suchaunique risk factor forpatientswithcir‐rhosis is that,unlikemore“traditional” transplantriskfactorssuchasage,sex,orModelforEnd‐StageLiverDiseasescore, individualcomponents of frailty (eg, physical function, sarcopenia, andmal‐nutrition) are potentially modifiable with exercise and nutritionalinterventions.25,26
Recently, the concept of “prehabilitation” has gained signifi‐cant momentum in transplant and nontransplant surgical fields.27 Prehabilitation refers to multidisciplinary “training” to enhancephysicalstrengthandnutritionalstatus—withthetheoreticalbenefitofimprovingphysiologicreservepriortosurgery.Althoughdataontheimpactofprehabilitationinlivertransplantationarelimitedtoasmallcohortatasinglecenter,27thereisemergingevidenceinstud‐iesofpatientsundergoingmajorabdominalsurgeriesthatprehabil‐itationprogramsimproveoutcomesandreducecosts.Examplesofspecific interventionshaveincludedcomprehensivephysicalactiv‐ity programs, supervised and home‐based exercises, educational/behavioralmodification,and/ornutritioncounseling.
Basedonthesedata,wehavedevelopedasimplealgorithmthatleveragesthepotential“modifiability”offrailtythroughprehabilita‐tion(Figure3).Specifically,thisalgorithmusesastandardizedfrailtymetrictoguiderecommendationsregardingtheintensityofpreha‐bilitation for liver transplant candidates.Whileourworkinggroupagreedthatalllivertransplantcandidatesshouldbeprovidedexer‐ciseandnutritionalrecommendations,inlightoflimitedavailability
ofoutpatientphysicaltherapyanddieticianresources—nottomen‐tionlimitedreimbursement—ouralgorithmallowsforintensificationof resources in those patientswho aremost vulnerable (ie, frail).Thespecificgoalsofthisalgorithmwereto:(a)increasephysiologicreservepretransplantsothatpatientsmaybetterwithstandacutedecompensating events, (b) improve clinical outcomes after livertransplantation, and (c) more efficiently and effectively allocatehealthcareresourcesinlivertransplantation.
Ouralgorithminvolvesthefollowingsteps:
• Step 1: Stratify risk by frailty status. All liver transplant candidatesshould undergo risk stratification using a standardized frailty as‐sessment tool. Our proposed frailty stratification system, based on expertopinion,foraselectnumberoftools,ispresentedinTable4.
• Step 2: Recommend a prehabilitation program based on risk stra‐tum.Theintensityoffrailtyinterventionshouldbetailoredtothedegree of frailty. Patientswith severe frailtymay benefit fromintensiveprehabilitation,withconsiderationofreferraltoan in‐patient rehabilitationcenter.We recommend thatpatientswitha moderate degree of frailty engage in a home‐based exerciseprogramdevelopedbyacertifiedexerciseprofessionalthattar‐getsthepatient'sgreatestfunctional impairment(s) (eg,balance,chairstands)butalsoincorporatesaerobictrainingandsimulatesADLs(toimprovequalityoflife).Patientswithmildornofrailtyshouldfollowrecommendationsdevelopedforthegeneralpop‐ulation(iemoderate‐intensityexercise≥150minutesperweek),withgradualbuildupphysicalenduranceandstrength.Physicalactivitytrackers(eg,accelerometers)maybeconsideredtoassessadherence.
• Step 3: Reassess and re‐stratify. Reversal of frailty among liver transplant candidates is feasible but has not been systemat‐ically studied. Lack of progression, however, is a clinically rele‐vant achievement that should incentivize liver transplantation,
F I G U R E 3 Algorithmtotailorprehabilitationrecommendationsbasedon frailty assessment

| 9LAI et AL.
particularlyifearlyposttransplantrehabilitationwillbeprovided.Werecommendclosemonitoringofpatientsonthewaitlist,withreassessmentintervalsbasedonthepatient'sseverityoffrailtyatthelastavailableexamination(Figure3).
Key points
• Standardizedassessmentsoffrailtymaybeusedtotailorthein‐tensity and type of nutritional and physical therapy in patientsawaitingandundergoinglivertransplantation.
• Frailtyshouldnotbeusedasthesolecriterionfordelistingapa‐tient for liver transplantation, but rather should be consideredoneofmany criteriawhen evaluating transplant candidacy andsuitability(Figure2).
2 | A ROADMAP TO ADVANCE FR AILT Y IN THE CLINIC AL AND RESE ARCH SET TINGS OF LIVER TR ANSPL ANTATION
Frailtyisnowwell‐recognizedinthescientificliteratureasastrongpredictor of outcomes in patients with cirrhosis, including in theliver transplant setting.While the frailty literature in hepatology/livertransplantationiscurrentlyrichwithhighqualitystudies,manyquestions remain: (a) the impact of frailty onmortality after liver transplantation, (b)the impactof longitudinalchanges infrailtyonoutcomes,and(c)therelationshipbetweenliverdiseaseprogressionandfrailty.Perhaps,themostexcitingtargetforfutureinvestigationisthenotionthatfrailtyisactionable,andthatitscomponentscanbearrestedorevenreversed.Hereweproposeapathforwardtoadvanceourunderstandingof frailty and improve the careof ourpatients:
ToolRationale for inclusion in the frailty tool kit
Estimated time to assess
Populations studied
Karnofskyperfor‐mance status
Intuitive and instant <10s Inpatient and outpatientNo cost
Lowflooreffects
Canbeassessedbythepatientortheprovider
Activitiesofdailyliving/instrumental activities of daily living
No cost 2‐4 min Inpatient and outpatientPatientreported
Well‐accepted patient‐oriented outcome
Liverfrailtyindex Objective, performance‐based 1‐3 min Outpatient
Continuousscalewithoutceilingorfloor effects
Quicklyadministered
Can be repeatedly performed in theoutpatientsetting
6‐minutewalktest Objective, performance‐based 6 min Outpatient
Continuousscalewithoutceilingorfloor effects
Noneedforspecializedequipment
TA B L E 3 Suggestedfrailtytoolkit
Stages of frailty
Severe Moderate Mild/Absent
ADL14,31 Difficultywith≥2ADLs Difficultywith1ADL
No difficulty withADLs
Clinical Frailty Scale16 ≥7 6 1‐5
FriedFrailtyPhenotype6 ≥3 1‐2 0
KarnofskyPerformanceStatus Scale11,15
0‐40 50‐70 ≥80
LiverFrailtyIndex7 ≥4.5 3.2‐4.4 <3.2
6‐minutewalktest9 <250m <350‐250m >350 m
Abbreviation:ADL,activitiesofdailyliving.
TA B L E 4 Recommended criteria to stage frailty in liver transplant candidates

10 | LAI et AL.
1. Obtain funding for multicenter consortia for prospective studies on frailty in liver transplantation. Now is an opportune timefor formal financial sponsorship of multicenter consortia toaccelerate progress. Engagement with other teams studyingfrailty in other chronic diseases, geriatrics/gerontology, andother solid organ transplant disciplines may have a highvalue.
2. Implement evidence‐based, objective frailty measurement as part of standard‐of‐care.Givenitsstrongassociationswithhealth‐relatedoutcomes,frailtyshouldbeconsideredavitalsignandmeasuredsystematically and routinely during clinic visits.
3. Develop interventions targeting modifiable aspects of physical frailty through rigorous multicenter randomized clinical trials. Specific modi‐fiable targets include muscle mass, muscle function, activity level, and nutrition. Interventions can focus on a single aspect or offer a more comprehensive approach (eg, prehabilitation program).Randomizationshouldofferclinicalequipoise:becausewebelievethatallpatientswithcirrhosiswouldbenefitfromsomeformofactivity andnutritional counseling, trials should explore varyingintensities(eg,twotimesperweekvs.daily)ortypesofinterven‐tion (eg, home‐ vs. center‐based; telephone calls vs. text mes‐sages)ratherthanrandomizingpatientstoa“nointervention”arm.
4. Investigate nonphysical aspects of frailty.These includecognitive,emotional, social, and environmental aspects that expand theconceptoffrailtybeyondphysicalfrailtyalone.
5. Integrate the concept of frailty into training curricula for hepa‐tology/surgery trainees and into national society guidelines for management of patients with cirrhosis. Educational modulesshould be developed to assess transplant trainees’ ability toobjectively assess, document, and incorporate frailty into clini‐caldecision‐making.Assessmentof frailtyshouldbe formallyincorporated into national guidelines for evaluation of liver transplant candidates.
6. Include objective measurement of frailty into research studies and national registries. Frailty can be treated as a predictor, a con‐founder,orevenanoutcomeinresearchstudies.Inclusionofob‐jectivemeasurementoffrailtyintonationalregistrydatawouldaccelerateresearchinthisfieldandenableadjustmentforfrailtyinanystudyevaluatingpre‐andposttransplantmortality.Basedontheevidencetodateandtheneedforuniformityofobjective frailtymeasurement in this setting,we recommend use of theLiverFrailtyIndexforthispurpose.
ACKNOWLEDG MENTS
This manuscript is a work product of the American Society ofTransplantation's Liver and Intestine Community of Practice andhas been endorsed by the American Society of Transplantationand theAmericanSocietyofTransplantSurgeons.This studywasfundedbyNIHK23AG048337(Lai),NIHR01AG059183(Lai),NIHRO1GM119174 (Dasarathy); P50 AA024333 (Dasarathy); R21AR71046 (Dasarathy); UO1 AA0026976 (Dasarathy); UO1DK061732(Dasarathy); RO1DK113196 (Dasarathy); Mikati Foundation Grant
(Dasarathy).Thesefundingagenciesplayednoroleintheanalysisofthedataorthepreparationofthismanuscript.
DISCLOSURE
Theauthorsof thismanuscripthavenoconflictof interest todis‐closeasdescribedbytheAmerican Journal of Transplantation.
DATA AVAIL ABILIT Y S TATEMENT
Datasharingnotapplicabletothisarticleasnodatasetsweregener‐atedoranalyzedduringthecurrentstudy.
ORCID
Shunji Nagai https://orcid.org/0000‐0003‐2612‐8427
R E FE R E N C E S
1. Lai JC. Advancing adoption of frailty to improve the care of pa‐tientswithcirrhosis:timeforaconsensusonafrailtyindex.Am J Gastroenterol.2016;111(12):1776‐1777.
2. FriedLP,TangenCM,WalstonJ,etal.Frailtyinolderadults:evidenceforaphenotype.J Gerontol A Biol Sci Med Sci.2001;56(3):146‐156.
3. American Thoracic Society: Quality Life Resource. FunctionalStatus. Available at: http://qol.thoracic.org/sections/key‐concepts/functional‐status.html.AccessedFebruary23,2018.
4. NeyM,TangriN,DobbsB,etal.Predictinghepaticencephalopa‐thy‐relatedhospitalizationsusingacompositeassessmentofcog‐nitive impairment and frailty in 355 patientswith cirrhosis.Am J Gastroenterol.2018;113(10):1‐10.
5. Tapper EB, KonermanM,Murphy S, Sonnenday CJ. Hepatic en‐cephalopathy impacts the predictive value of the Fried FrailtyIndex.Am J Transplant.2018;18(10):2566‐2570.
6. Lai JC, Feng S, Terrault NA, Lizaola B, Hayssen H, Covinsky K.Frailtypredictswaitlistmortalityinlivertransplantcandidates.Am J Transplant.2014;14(8):1870‐1879.
7. LaiJC,CovinskyKE,DodgeJL,etal.Developmentofanovelfrailtyindextopredictmortalityinpatientswithend‐stageliverdisease.Hepatology.2017;66(2):564‐574.
8. LaiJC,CovinskyKE,McCullochCE,FengS.Theliverfrailtyindeximproves mortality prediction of the subjective clinician assess‐mentinpatientswithcirrhosis.Am J Gastroenterol.2017;10:1‐8.
9. Carey EJ, Steidley DE, Aqel BA, et al. Six‐minute walk distancepredicts mortality in liver transplant candidates. Liver Transpl. 2010;16(12):1373‐1378.
10. NeyM,HaykowskyMJ,VandermeerB,ShahA,OwM,TandonP.Systematic review: pre‐ and post‐operative prognostic value ofcardiopulmonary exercise testing in liver transplant candidates.Aliment Pharmacol Ther.2016;44(8):796‐806.
11. Orman ES, Ghabril M, Chalasani N. Poor performance status isassociatedwithincreasedmortalityinpatientswithcirrhosis.Clin Gastroenterol Hepatol.2016;14(8):1189‐1195.e1.
12. Faustini Pereira JXL,Galant LH,RossiD, et al. Functional capac‐ity, respiratorymusclestrength,andoxygenconsumptionpredictmortality in patients with cirrhosis. Can J Gastroenterol Hepatol. 2016;2016(1):1‐6.
13. SundaramV,LimJ,TholeyDM,etal.TheBradenScale,astandardtoolforassessingpressureulcerrisk,predictsearlyoutcomesafterliver transplantation. Liver Transpl.2017;23(9):1153‐1160.

| 11LAI et AL.
14. Tapper EB, Finkelstein D, Mittleman MA, Piatkowski G, LaiM. Standard assessments of frailty are validated predictors ofmortality in hospitalized patients with cirrhosis. Hepatology. 2015;62(2):584‐590.
15. TandonP,ReddyKR,O'LearyJG,etal.AKarnofskyperformancestatus‐based score predicts death after hospital discharge in pa‐tientswithcirrhosis.Hepatology.2017;65(1):217‐224.
16. TandonP,TangriN,ThomasL,etal.Arapidbedsidescreentopre‐dict unplanned hospitalization and death in outpatientswith cir‐rhosis: a prospective evaluation of the clinical frailty scale.Am J Gastroenterol.2016;111(12):1759‐1767.
17. DunnMA,JosbenoDA,TevarAD,etal.Frailtyastestedbygaitspeedisanindependentriskfactorforcirrhosiscomplicationsthatrequirehospitalization.Am J Gastroenterol.2016;111(12):1768‐1775.
18. SinclairM,PoltavskiyE,DodgeJL,LaiJC.Frailtyisindependentlyassociatedwith increased hospitalisation days in patients on thelivertransplantwaitlist.World J Gastroenterol.2017;23(5):899.
19. DasarathyS,MerliM.Sarcopeniafrommechanismtodiagnosisandtreatment in liver disease. J Hepatol.2016;65(6):1232‐1244.
20. LaiJC.Aframeworktodeterminewhenlivertransplantationisfu‐tile. Clin Liver Dis.2016;8(6):137‐139.
21. RockwoodK,MitnitskiA.Frailtyinrelationtotheaccumulationofdeficits. J Gerontol A Biol Sci Med Sci.2007;62(7):722‐727.
22. LaiJC,DodgeJL,SenS,CovinskyK,FengS.Functionaldeclineinpatientswithcirrhosisawaiting liver transplantation: results fromtheFunctionalAssessmentinLiverTransplantation(FrAILT)study.Hepatology.2016;63:574‐580.
23. WangCW,LebsackA,ChauS,LaiJC.Therangeandreproducibilityof the Liver Frailty Index (publishedonline aheadof printMarch2019).Liver Transpl.https://doi.org/10.1002/lt.25449..
24. LurzE,QuammieC,EnglesbeM,etal.Frailtyinchildrenwithliverdis‐ease: a prospective multicenter study. J Pediatr.2018;194:109‐115.
25. Duarte‐Rojo A, Ruiz‐Margáin A, Montano‐Loza AJ, Macías‐RodríguezRU,FerrandoA,KimWR.Exerciseandphysicalactivityforpatientswithend‐stageliverdisease:improvingfunctionalsta‐tusandsarcopeniawhileonthetransplantwaitinglist.Liver Transpl. 2017;24(1):122‐139.
26. TandonP,IsmondKP,RiessK,etal.Exerciseincirrhosis:translatingevidenceandexperiencetopractice.J Hepatol.2018;69:1164‐1177.
27. VolkML,SonnendayC.Patient‐centeredlivertransplantation.Clin Liver Dis.2016;8(1):24‐27.
28. SamoylovaML,CovinskyKE,HaftekM,KuoS,RobertsJP,LaiJC.Disabilityinpatientswithend‐stageliverdisease:resultsfromthefunctional assessment in liver transplantation study. Liver Transpl. 2017;23(3):292‐298.
29. MalinisMF,ChenS,AlloreHG,QuagliarelloVJ.Outcomesamongolderadultlivertransplantationrecipientsinthemodelofendstageliverdisease(MELD)era.Ann Transplant.2014;19:478‐487.
30. YadavA,ChangY‐H,CarpenterS,etal.Relationshipbetweensar‐copenia,six‐minutewalkdistanceandhealth‐relatedqualityoflifein liver transplant candidates. Clin Transpl.2015;29(2):134‐141.
31. RakoskiMO,McCammonRJ,Piette JD,etal.BurdenofcirrhosisonolderAmericans and their families: analysis of thehealth andretirement study. Hepatology.2012;55(1):184‐191.
How to cite this article:LaiJC,SonnendayCJ,TapperEB,etal.Frailtyinlivertransplantation:AnexpertopinionstatementfromtheAmericanSocietyofTransplantationLiverandIntestinalCommunityofPractice.Am J Transplant. 2019;00:1‐11. https://doi.org/10.1111/ajt.15392