FRACTURES OF THE DISTAL RADIUS & ULNA IN CHILDREN · 2 FRACTURES OF THE DISTAL RADIUS & ULNA IN...
14
1 FRACTURES OF THE DISTAL RADIUS & ULNA IN CHILDREN Kaye E. Wilkins, M.D. Clinical Professor Orthopaedics & Pediatrics The University of Texas Health Science Center at San Antonio San Antonio, Texas
Transcript of FRACTURES OF THE DISTAL RADIUS & ULNA IN CHILDREN · 2 FRACTURES OF THE DISTAL RADIUS & ULNA IN...

1
FRACTURES OF THE
DISTAL RADIUS & ULNA
IN CHILDREN
Kaye E. Wilkins, M.D.
Clinical Professor Orthopaedics & Pediatrics
The University of Texas Health Science Center at San Antonio San Antonio, Texas
2
FRACTURES OF THE DISTAL RADIUS & ULNA IN CHILDREN
I. GENERAL CONSIDERATIONS
A. Introduction: A Benign Injury? 1.Usually good results
a. In a series of 1,767 fractures, only 2.5% showed significant angulation (1). b. A more recent series of 1,346 fractures reported a 7% remanipulation rate (2).
2.Analysis of factors leading to poor results may facilitate avoiding the pitfalls that
can occur. B. Incidence of All Forearm Fractures
1.Various series (3, 4) have all confirmed that with age, the geographic location of fractures of the radius migrates distally due to the increased discrepancy between wider weaker distal metaphysis and the more proximal and stronger diaphysis. 2.Regional Distribution (1, 4, 5, 6, 7, 8)
Shaft: 20% Distal Metaphysis: 66% Distal Physis : 14% Proximal 1/3 fractures: 1-2%.
C. Mechanism of Injury 1.Most common mechanism is a fall on the outstretched arm. 2.Modern children are exposed to even newer mechanisms.
a.Acute: small wheels mobility devices such as roller skates, in-line skates, skate boards and small wheel scooters all increase the forward kinetic energy of the child increasing the likelihood of a fracture. b. Chronic: Gymnastics, (9,10) breakdancing, (11) and bicycle "Wheelies" (12) all put
chronic compressive forces across the distal radial physis specifically increasing the incidence of chronic stress fractures.
II. PHYSEAL FRACTURES OF THE DISTAL RADIUS
A. Incidence 1. 2% of all children's fractures 2. 39% of all physeal injuries 3. Peak ages:
a. Males 13 - 14 years b. Females 9 - 10 years
4. Male: Female ratio 77:33 5. Incidence of growth arrest 4% 6. 75% S-H II patterns (13) 7. Rarely an isolated injury, usually associated with:
a. Distal ulnar metaphysis b. Avulsion ulnar styloid c. Distal ulnar physeal injury (extremely rare) d. Common ipsilateral injuries include: scaphoid, supracondylar humerus.
B. Mechanisms 1. Acute
a. Dorsiflexion injuries with wrist dorsiflexed 95% b. Palmar flexion injuries with wrist acutely palmar flexed 5%
2. Chronic a. Chronic weight bearing in hyperextension most commonly associated with gymnastics (14,15) b. Produces ulnar variance with chronic wrist pain
C. Diagnosis 1. Displaced fractures usually obvious 2. Peterson I Fracture Patterns
a. Fracture pattern involves comminution of the adjacent metaphysis of the distal radius. b. The fracture lines extend up to, but not across the physis (Fig. 1).

3
. b. While benign appearing, a significant number of these develop a silent arrest
3. Pronator Sign: Swelling or displacement of the fat pad anterior to pronator quadratus indicates bleeding into this muscle from an undisplaced fracture of the distal radial physis(Fig.
2)
D. Classification (two basis)
1. Direction of Displacement ( Fig.3) a. Type A - Distal Fragment Dorsal (95%) b. Type B - Distal Fragment Volar (5%)
2. Type of physeal fracture pattern, i.e., Salter-Harris or Peterson E. Treatment
1. Non-Operative a. Closed Reduction: the main stay of treatment.
Type A Type B
Figure 1 Peterson Type I The metaphysel fracture lines
extend up to the physis (arrows).
Pitfall
Figure 2. Pronator farpad sign Subperiotseal hemmorrage from the
occult fracture of the distal radial physis causes anterior displacement of the fat pad overlying the pronator quadratus
(arrows)
Figure 3 Displacement patterns Type A Dorsal, Type B Volar

4
1)Traction - Distraction method:
a) Using finger trap traction (Fig. 4) b)Theoretically decreases the shear forces across the physis
FIGURE 4. Author's method of closed reduction of
distal physeal fractures of the radius. (A) Position of the fracture fragments as finger-trap traction with traction is applied (arrows). (B) Often with traction alone the
fracture will reduce without external pressure (arrows). (C ) If the reduction is incomplete, simplying direct pressure over the fracture site in a distal volar direction with the thumb often completes the reduction while maintaining traction. This technique theoretically decreases the shear forces across the physis during the reduction process.
2) Immobilization:
a) Good three-point molding more important than wrist flexion. b) Four weeks usually adequate. c) Don't remanipulate if late displacement occurs. d) Don't manipulate primarily if fracture more than 3 days old
unless severly displaced. e) Aitken has shown remarkable remodeling capacity (16,17)
2. Operative Indications a. Percutaneous Pin Fixation
1) Most common indication is with ipsilateral fractures 2) Obese patients or severe swelling 3) Single pin is placed obliquely dorsally avoiding physis to serve as a dorsal buttress preventing dorsal displacement ( Fig. 5 )
b. Failure to achieve adequate reduction due to interposed structures, i.e., and or tendons.
c. Open fractures. d. Comminuted intra-epiphyseal and intra-articular fractures. e. Carpal tunnel or compartment syndromes.
Pitfall
A B C
Figure 5 Percutaneous pin The pin is placed obliquely dorsally to avoid physis but still serves as a buttress to prevent dorsal displacement.
5
3. Beware the Type B Fractures. They are unstable!
a. A reverse 3-point molding of the cast at the fracture site is required if the fracture is stable with closed reduction alone. b. Almost all should undergo pin fixation because of the high incidence of late
displacement and unacceptable cosmetic appearance when they displace. Ill. FRACTURES OF THE DISTAL ULNAR PHYSIS.
A. Incidence. 1.Thirty percent of distal radial fractures (physeal and metaphyseal fractures) have an associated fracture of the ulnar styloid. 2.Trans physeal fractures through the distal ulna constitute only 5% of all children's physeal fractures. B. Grow th Arrest. 1. While incidence of ulnar physeal fractures are rare, the incidence of growth arrest is very high, i.e., 60%. (18)
2. Thus don't ignore the trans physeal fractures of the ulna. They can arrest (Fig. 6)
C. Treatment.
1.Styloid fractures usually can be ignored even if nonunion. It is extremely rare that operative management is indicated. 2.Transphyseal fractures:
a .Usually respond to closed reductions. b. If associated with an unstable distal radius (Galeazzi equivalent) pin fixation of the distal ulna may be required to maintain radial length. (19) c. Occasionally there are interposed structures (tendons, uInar nerve) which need to be extracted surgically.
IV. FRACTURES OF THE DISTAL RADIAL METAPHYSIS. A. Anatomical Factors.
1. The metaphysis is an area of remodeling, thus the cortex is thin predisposing it to incomplete failure patterns such as torus compression and greenstick tension fractures. 2.Extensive remodeling due to adjacent physis. 3.Bulk of soft tissues volar which help hide apex-volar deformities. However, dorsal-apex deformities are more prominent clinically ( Fig.7 ).
a. Thus one needs to be more aggressive in reducing apex dorsally angulated fractures.
Pitfall
Pitfall
Pitfall
Pitfall
Pitfal l
Figure 6. Distal ulnar
physeal arrest An 8 y.o. developed complete growth arrest of the distal ulnar physis three years after a Type I S-H Fracture..

6
B. Incidence. 1. Peak incidence related to growth velocity, i.e., females 10 - 12 years, males 13 - 14 years. 2. 57% Non-dominant extremity. 3. 70% Males. 4. Ipsilateral.
a. Five percent have ipsilateral humeral supracondylar fractures. b. The incidence of associated scaphoid fractures is high enough so that with all distal radial metaphyseal fractures, the navicular and its fat stripe should always be evaluated.
C. Classification - important because it dictates the treatment. 1. Directional displacement (distal fragment).
a. Dorsal 98 - 99%. b. Volar.
2. Fracture combinations. a. Isolated distal radius. b. Distal radius with distal ulna.
1) Ulnar styloid. 2) Ulnar physis. 3) Ulnar metaphysis incomplete. 4) Ulnar metaphysis complete.
3. Biomechanical patterns. a. Torus. b. Greenstick.
1) One cortex. a) Usually termed Compression Greenstick b) Usually stable ie: rarely angulate late.
2) Both cortices a) If volar cortex disrupted termed Tension Greenstick b) Beware!!! These fracture patterns tend to angulate late
(Fig.8). c. Complete.
1) Length maintained. 2) Bayonet apposition
Pitfall
Pitfall
Figure 7. Dorsal angulation This 7 y.o. developed 20
0
which was more apparent clinically because there is only minimal soft tissue to cover the angulation on the dorsum of the distal forearm.
7
Fig. 8A. Fig. 8B
D. Pathology.
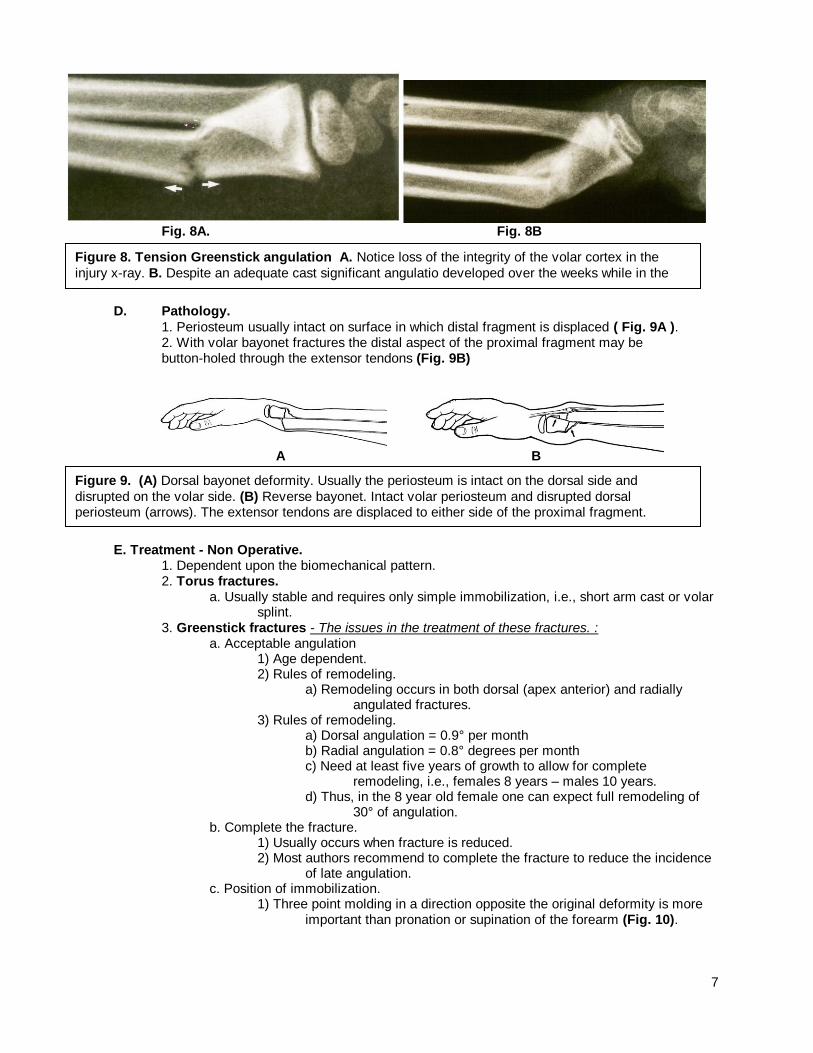
1. Periosteum usually intact on surface in which distal fragment is displaced ( Fig. 9A ). 2. With volar bayonet fractures the distal aspect of the proximal fragment may be button-holed through the extensor tendons (Fig. 9B)
E. Treatment - Non Operative. 1. Dependent upon the biomechanical pattern. 2. Torus fractures.
a. Usually stable and requires only simple immobilization, i.e., short arm cast or volar splint.
3. Greenstick fractures - The issues in the treatment of these fractures. : a. Acceptable angulation
1) Age dependent. 2) Rules of remodeling.
a) Remodeling occurs in both dorsal (apex anterior) and radially angulated fractures.
3) Rules of remodeling. a) Dorsal angulation = 0.9° per month b) Radial angulation = 0.8° degrees per month c) Need at least five years of growth to allow for complete
remodeling, i.e., females 8 years – males 10 years. d) Thus, in the 8 year old female one can expect full remodeling of
30° of angulation. b. Complete the fracture.
1) Usually occurs when fracture is reduced. 2) Most authors recommend to complete the fracture to reduce the incidence
of late angulation. c. Position of immobilization.
1) Three point molding in a direction opposite the original deformity is more important than pronation or supination of the forearm (Fig. 10).
A B
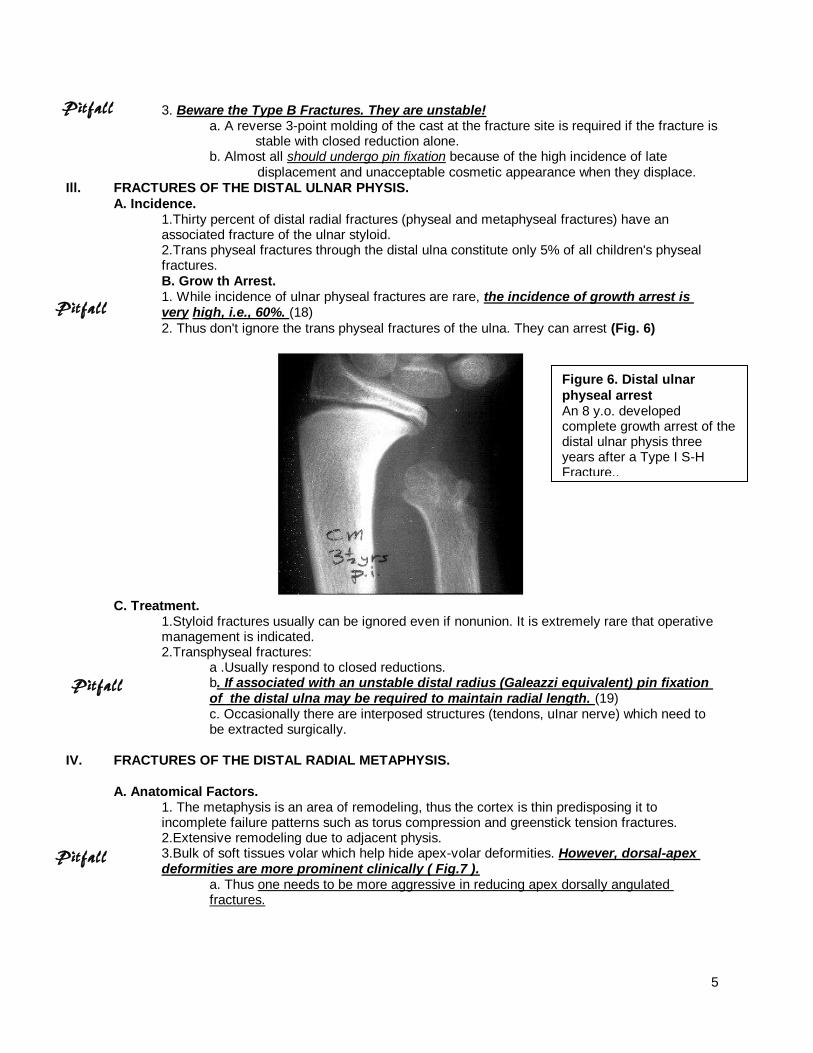
Figure 8. Tension Greenstick angulation A. Notice loss of the integrity of the volar cortex in the
injury x-ray. B. Despite an adequate cast significant angulatio developed over the weeks while in the cast.
Figure 9. (A) Dorsal bayonet deformity. Usually the periosteum is intact on the dorsal side and
disrupted on the volar side. (B) Reverse bayonet. Intact volar periosteum and disrupted dorsal periosteum (arrows). The extensor tendons are displaced to either side of the proximal fragment. .

8
Figure 10. Three Point Molding
Once the cast is applied a three point mold is applied with proximal and distal (down arrows ) dorsal pressure points and a middle volar (up arrow) pressure point.
3. Complete fracture a. Length maintained - simply correct the angulation.
b. Bayonet apposition (dorsal). 1) Obtain reduction in two steps:
a) Regain length and then reduce by hyperextending the distal fragment (Fig. 11)
Figure 11. Use of the thumb to push the distal fragment hyperdorsiflexed 90° (solid arrow) until length is reestablished. Countertraction is applied in the opposite direction.
b) Once length regained
replace fragment by volar flexion (Fig. 12).
Figure 12. Once length has been reestablished, the distal fragment is flexed into the correct position. Alignment is checked by determining the position of the fragments with the thumb and forefingers of each hand.
2) Immobilization a) Short arm cast is adequate but it must be oval with cast index of 0.7 or less (Fig. 13).

9
Figure 13. The cast index is obtained by dividing the sagittal diameter (A) by its coronal diameter (B) at the fracture site. To be adequate, the ratio or index should be 0.7 or less.
b) Apply the cast with patient in finger traps traction (negates need for an assistant). (Fig. 14) Include thumb in cast to eliminate thenar
eminence pressure on edge of cast. (Fig. 15)
c) Apply a very tight cast then split
the cast along the ulnar border and spread to allow
for delayed swelling. (Fig. 16)
Figure 14. Suspended in finger-traps, a very snug cast is applied incorpo-rating the thumb
Figure 15. Thumb incorporated in cast.
Figure 16. While still suspended and before release of the tourniquet for the Bier block, the cast is split and spread in its distal three fourths. The separation should include the padding down to the skin.

10
3) Postoperative care. a) See in one week. Check position with x-rays b) close cast and cut-out around the thumb .c) Six weeks adequate for cast immobilization c) Use volar splint for light protection during activity hours another
7-10 days until strength and mobility regained. c. Volar (Reverse) Bayonet (Fig. 17)
1) Beware!! 2) Less stable. 3) Reduction and immobilization techniques are reversed from dorsal
bayonet. 4) Proximal fragment may be button-holed through the extensor tendons (See
Fig. 8B). F. Treatment Operative Indications.
1. Percutaneous pin fixation - same as for distal physeal injuries. 2.Open fractures. 3. Primary open reductions. 4. Remember dorsal bayonet apposition will remodel up to 12.5 years of age.
G. Complications. 1. Loss of position. a. Voto's series reported up to 7% required remanipulation. (2)
b. Loosening of the cast after swelling subsides appears to be the greatest cause for loss of reduction.
c. In those fractures which are massively swollen due to the primary injury or frequent remanipulation, redisplacement may be prevented by securing the reduction with a simple cross pin.
d. The decision to remanipulate depends upon the amount of remodeling expected. e. If fracture remanipulated, often pin fixation may be needed to prevent recurrence
of the deformity. 2. Neurological dysfunction.
a. As with distal radial physeal injuries, the nerve dysfunction which resolves with reduction.
b. Rare cases have been reported in which there has been incorporation of the median and uInar nerves in the fracture site. (20,21).
Pitfall
Figure 17. Volar
Bayonet. The distal fragment lies volar to the proximal fragment.
11
3. Compartment syndrome (22,23 ). a. The recent literature reports that compartment syndrome can occur more
commonly than originally suspected after the fractures of the distal radius. b. The classic findings of marked swelling, pain out of proportion to the injury, and
pain on passive extension of the fingers are all usually present. c. However, these findings are inherent with the fracture itself. d. Compartment pressure measurements may be the only accurate method of
determining the presence of a compartment syndrome. e. In some cases, i.e. difficult reductions with massive injury post reduction
compartment measurements have been recommended. (15) f. Before releasing compartment surgically one needs to be sure the entire
compartment has an elevated pressure. Don’t measure only at the fracture site. Measure proximally as well.
4. Cross union - extremely rare. 5. Refracture.
a. Occurs within six months and through the old fracture site. b. Prevented by protecting the forearm with a splint during rehabilitation phase.
V. GALEAZZI FRACTURES - DISRUPTION OF THE DISTAL RADIOULNAR JOINT A. Incidence. (24)
1. Occurs in 3% of distal radial injuries. 2. But initiallly recognized in only 40% of the cases. 3. Of all age groups of Galeazzi Fractures only 11.2% involve children. (25,26,27)
B. Mechanism. 1. Probably axial loading plus rotation.
C. Classification (Walsh). (24)
1. Two major types (Figs. 18,19).
a. Dorsal – distal fragment supinated. b. Volar - distal fragment pronated.
A B
A B
12
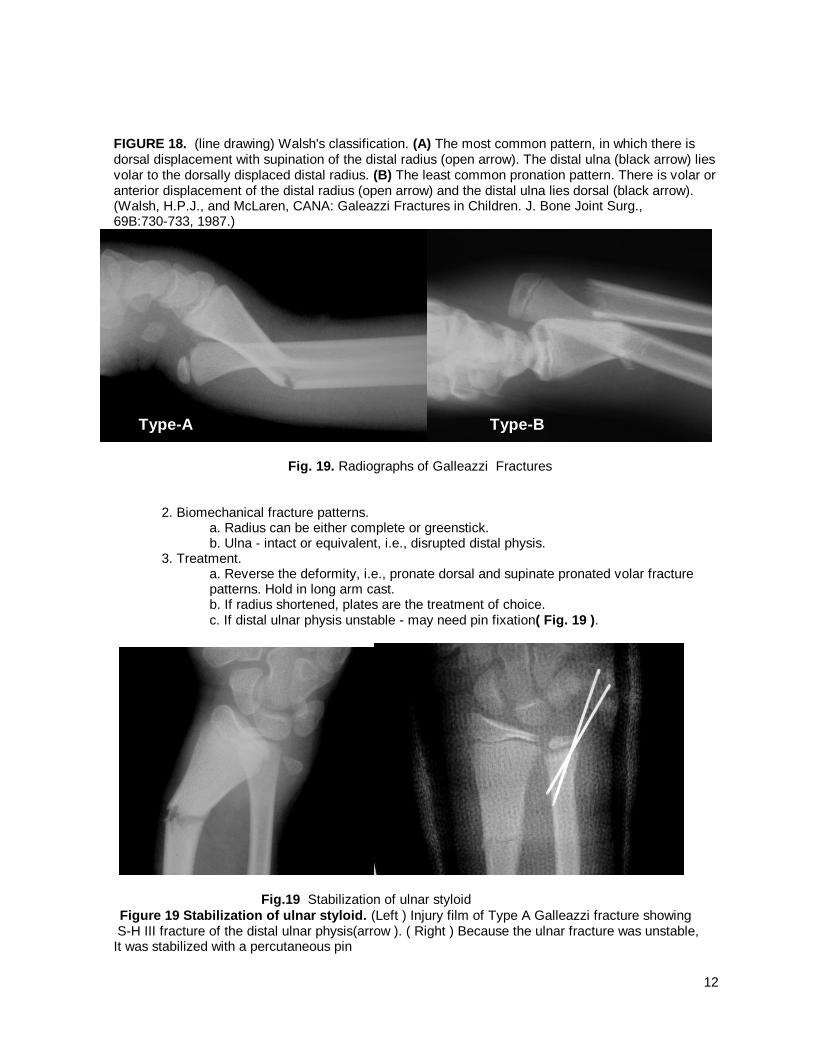
FIGURE 18. (line drawing) Walsh's classification. (A) The most common pattern, in which there is dorsal displacement with supination of the distal radius (open arrow). The distal ulna (black arrow) lies volar to the dorsally displaced distal radius. (B) The least common pronation pattern. There is volar or anterior displacement of the distal radius (open arrow) and the distal ulna lies dorsal (black arrow). (Walsh, H.P.J., and McLaren, CANA: Galeazzi Fractures in Children. J. Bone Joint Surg., 69B:730-733, 1987.)
Fig. 19. Radiographs of Galleazzi Fractures
2. Biomechanical fracture patterns.
a. Radius can be either complete or greenstick. b. Ulna - intact or equivalent, i.e., disrupted distal physis.
3. Treatment. a. Reverse the deformity, i.e., pronate dorsal and supinate pronated volar fracture patterns. Hold in long arm cast. b. If radius shortened, plates are the treatment of choice. c. If distal ulnar physis unstable - may need pin fixation( Fig. 19 ).
Fig.19 Stabilization of ulnar styloid
Figure 19 Stabilization of ulnar styloid. (Left ) Injury film of Type A Galleazzi fracture showing S-H III fracture of the distal ulnar physis(arrow ). ( Right ) Because the ulnar fracture was unstable, It was stabilized with a percutaneous pin
Type-A Type-B

13
.
REFERENCES 1. Ghandi, R.K.; Wilson, P.; Brown, J.J.M.; and Macleod, W.: Spontaneous Correction of Deformity
Following Fractures of the Forearm in Children. Br. J. Surg., 50:5-10, 1962. 2. Voto, S.J.; Weiner, D.S. and Leighley (need initials): Redisplacement After Closed Reduction of
Forearm. J. Pediatra. Orthop., 10:79-84, 1990. 3. Bailey, D.A.; Wedge, J.H.; McCulloch, R.G.; Martin, A.D.; and Bernhardson, S.C.: Epidemiology of
Fractures of the Distal End of the Radius in Children Associated With Growth. J. Bone Joint Surg., 71A:1225-1231, 1989.
4. Thomas, E.M.; Tuson, K.W.R., and Browne, P.S.H.: Fractures of the Radius and Ulna in Children.
Injury, 7:120-124,1975. 5. Davis, D.R. and Green, D.P.: Forearm Fractures in Children. Pitfalls and Complications. Clin. Orthop,
120:172-184, 1976. 6. lqbal, Q.M.: Long. Bone Fractures Among Children in Malaysia. Int. Surg., 59:410, 1975. 7. Mitzuta, T.; Benson, W.M.; Foster, M.B.; Paterson, D.C. arid Morris, L.L.: Statistical Analysis of the
Incidence of Physeal Injuries. J. Pediatr. Orthop., 7:518-523,1987. 8. Onne, L. and Sandblom, P.H.: Late Results in Fractures of the Forearm in Children. Acta Chir.
Scand., 98:549-567,1949. 9. Albanese, S.A.; Palmer, A.K.; Kerr, D.R.; Carpenter, C.W. Lisi, D. and Levinsohn, E.M.: Wrist Pain
and Distal Growth Plate Closure of the Radius in Gymnasts. J Pediatr. Orthop., 9:23-28,1987. 10. Caine, D.; Roy, S.; Singer, K.M. and Broekhoff, J.: Stress Changes of the Distal Radial Growth Plate.
A Radiographic Survey and Review of the Literature. Am. J. Sports Med., 20:290-298,1992. 11. Gerber, S.D.; Griffing, P.P., and Simmons, B.P.: Breakdancer's Wrist. J. Pediatr. Orthop.,
6:98-99,1986. 12. Eisenberg, D.; Kirschner, S.G. and Green, N.E.: Stress Fracture of the Distal Radius Caused by
"Wheelies." South Med. J., 79:918-919, 1986. 13. Lee, B.S.; Esterhai, J.I., Jr., and Das, M.: Fracture of the Distal Radial Epiphysis. Characteristics and
Surgical Treatment of Premature, Post-Traumatic Epiphyseal Closure. Clin. Orthop., 185:90-96,1983. 14. Altram, L.J. and Thompson, G.H.: Deformity after Premature Closure of the Distal Radial Physis
Following a Torus Fracture with a Physeal Compression Injury. J. Bone Joint Surg., 69A:1450-1453,1987.
15. Royle, S.G.: Compartment Syndrome Following Forearm Fracture in Children. Injury, 21:73-76, 1990. 16. Aitken, A.P.: The End Results of Fractured Distal Radial Epiphysis. J. Bone Joint Surg.,
27:302-308,1935. 17. Aitken, A.P.: Further Observations on the Fractured Distal Radial Epiphysis. J. Bone Joint Surg.,
27:922- 927,1935. 18. Nelson, O.A.; Buchanon, J.R. and Harrison, C.S.: Distal UInar Growth Arrest. J. Hand Surg.,
9:164-170, 1984.

14
19. Landfried, M.J.; Stenclik, M., and Susi, J.G.: Variant of Galeazzi Fracture-Dislocation in Children. J.
Pediatr. Orthop., 11:332-335, 1991. 20. Prosser, A.J. and Hooper, G.: Entrapment of the Ulnar Nerve in a Greenstick Fracture of the Ulna. J.
Hand Surg., I 113:211-212, 1986. 21. Wolfe, J.S. and Eyring, E.J.: Median Nerve Entrapment within a Greenstick Fracture. J. Bone Joint
Surg., 56A: 270-1272, 1974. 22. Matsen, 111, F.A. and Veith, R.G.: Compartmental Syndromes in Children, J. Pediatr. Orthop.,
1:33-41,1981. 23. Stockley, I.; Harvey, I.A. and Getty, C.J.C.: Acute Volar Compartment Syndrome of the Forearm
Secondary to Fractures of the Distal Radius. Injury, 19:101-104, 1988. 24. Walsh, H.P.J.; McLaren, C.A.N. and Owen, R.:: Galeazzi Fractures in Children. J. Bone Joint Surg.,
69B:730-733,1987. 25. Reckling, F.W.: Unstable Fracture-Dislocations of the Forearm (Monteggia and Galeazzi Lesions). J.
Bone Joint Surg., 64A:857-863,1982. 26. Macule Beneyto, F.; Arandes Renu, J.M.; Freres Claramunt, A. and Ramon Soler, R.: Treatment of
Galeazzi Fracture-Dislocations. J. Trauma, 36:352-355, 1994. 27. Mikic,A.: Galeazzi Fracture-Dislocations. J. Bone Joint Surg., 57A:a 071-1080, 1975.