
Fracture Strength of Implant-Supported Full … · Fracture strength of implant supported...
64
Fracture Strength of Implant-Supported Full-Contoured Titanium and Zirconia Single Crowns Connected to Titanium Cores By Hooman Mohandesan A thesis submitted in conformity with the requirements for the degree of Masters of Science in Prosthodontics School of Graduate Studies and Discipline of Prosthodontics Faculty of Dentistry University of Toronto © Copyright by Hooman Mohandesan (2016)
Transcript of Fracture Strength of Implant-Supported Full … · Fracture strength of implant supported...

Fracture Strength of Implant-Supported Full-Contoured Titanium and Zirconia Single Crowns Connected to
Titanium Cores
By
Hooman Mohandesan
A thesis submitted in conformity with the requirements for the degree of Masters of Science in Prosthodontics
School of Graduate Studies and Discipline of Prosthodontics Faculty of Dentistry
University of Toronto
© Copyright by Hooman Mohandesan (2016)

ii
Fracture strength of implant supported full-contoured titanium and zirconia single crowns connected to titanium cores
Hooman Mohandesan, DMD
Masters of Science in Prosthodontics
School of Graduate Studies and Discipline of Prosthodontics
Faculty of Dentistry
University of Toronto
2016
Abstract
Objectives: To investigate the fracture strength and failure mode of implant-supported
screw-retained customized 2-piece zirconia and 1-piece titanium restorations, and to
evaluate the effect of aging on the mechanical performance of zirconia restorations.
Materials and Methods: Thirty identical specimens simulating maxillary first premolar
replacements were divided in 3 groups. Groups ZrA and ZrNA consisted of zirconia and
Group Ti consisted of titanium restorations, anchored to implants embedded in PMMA.
Specimens in Group ZrA underwent chewing simulation. Static load was applied until
failure.
Results: Group Ti showed the highest fracture strength. The difference was significant
between Groups ZrA and Ti. Failures included partial or complete fracture of titanium
insert or deformation of restoration with screw fracture.
Conclusion: Evidence was inadequate to reject similarity in fracture strength between
non-aged zirconia and titanium restorations, or between zirconia restorations with
different aging conditions. Aging affected the failure mode of zirconia restorations.
iii
Acknowledgements
I would like to sincerely thank Dr. Grace De Souza for kindly accepting to be my
Supervisor on the research topic of my interest and for all her patience,
constructive guidance and practical assistance throughout the course of the
research project.
I would also like to express my gratitude to Dr. Laura Tam (Co-supervisor and
Committee Member) and Dr. Babak Shokati (Committee Member) for their kind
contribution and support. Their knowledge and expertise was instrumental in the
fulfillment of this project.
I would like to acknowledge the generous provision of the implant fixtures and
prosthetic components by Straumann North America, with special thanks to Ms.
Jade Lee Choon, Mr. Matthew Reynolds and Mr. Dino Vlahavas (Straumann
Canada) for their endless efforts in this regard.
I would further like to thank LHM Dental Studios, Toronto, especially Mr. Slawek
Bilko (President), Mr. Jim Agoritsas (Manager), Mr. Evan Katz and Ms. Sarah
Leandro for letting me use their facility and for their kind assistance in designing
and preparing the specimens.
Lastly, I want to thank my life-long mentor, my devoted mother, Shirin
Bozorgmehr, whose wisdom, unconditional support and life-long guidance have
played an important role in the achievements through my life journey and also
my responsible and caring father, Mehrdad Mohandesan, for his endless support
that has made my educational goals come true.

iv
Table of Contents Abstract ii Acknowledgements ii List of Tables v List of Figures vi Chapter 1. Introduction 1 Chapter 2. Literature Review 2
Type of fixation of restoration to the implant 2 Abutment material 4 Types of commercially available zirconia restorations 7 Configuration of implant-abutment connection 8 One-piece zirconia restorations 9 Two-piece zirconia restorations with intermediary titanium insert 11
Chapter 3. Rationale and Objectives 16 Rationale 16 Objectives 17 Hypotheses 17
Chapter 4. Materials and Methods 18 Materials 18 Experimental groups 18 Fabrication of the CAD/CAM restorations 22 Preparation of the restorations and attachment to fixtures 22 Artificial aging 24 Fracture strength test 25 Visual evaluation of the specimens 26 Scanning Electron Microscopy assessment 26 Statistical analysis 26
Chapter 5. Results 27 Outcome of chewing simulation 27 Fracture strength 27 Mode of failure 28
Chapter 6. Discussion 32 Chapter 7. Conclusions and Clinical Significance 43
Conclusion 43 Clinical Significance 43
Chapter 8. Future Research Directions 44 References 45 Appendices 54
Appendix A: Fracture strength values and failure mode of the specimens 54 Appendix B: Representative stress-strain curves for each test group 57
v
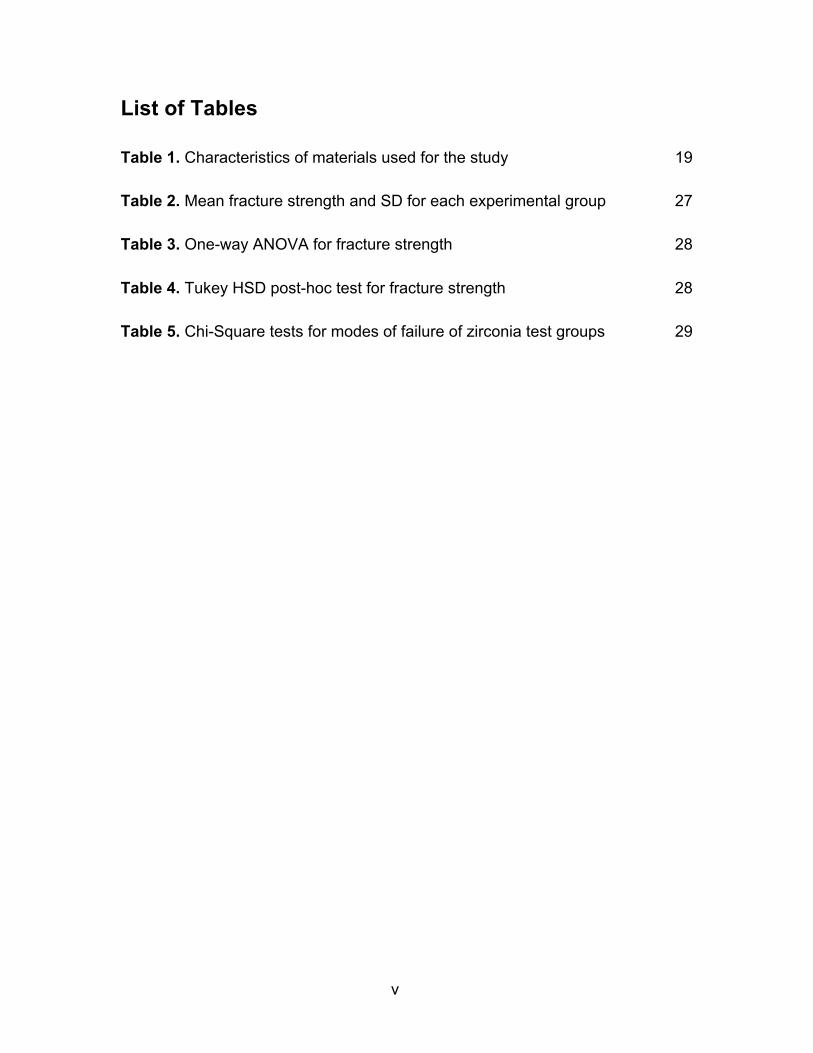
List of Tables
Table 1. Characteristics of materials used for the study 19
Table 2. Mean fracture strength and SD for each experimental group 27
Table 3. One-way ANOVA for fracture strength 28
Table 4. Tukey HSD post-hoc test for fracture strength 28
Table 5. Chi-Square tests for modes of failure of zirconia test groups 29
vi
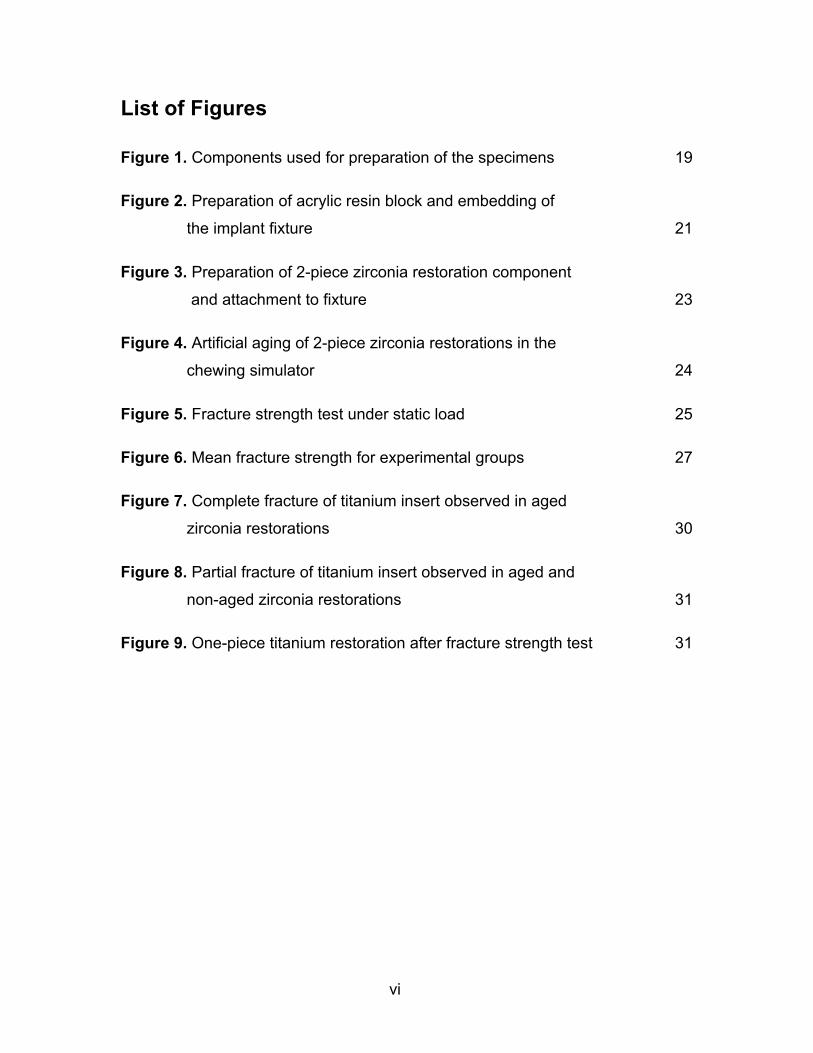
List of Figures
Figure 1. Components used for preparation of the specimens 19
Figure 2. Preparation of acrylic resin block and embedding of
the implant fixture 21
Figure 3. Preparation of 2-piece zirconia restoration component
and attachment to fixture 23
Figure 4. Artificial aging of 2-piece zirconia restorations in the
chewing simulator 24
Figure 5. Fracture strength test under static load 25
Figure 6. Mean fracture strength for experimental groups 27
Figure 7. Complete fracture of titanium insert observed in aged
zirconia restorations 30
Figure 8. Partial fracture of titanium insert observed in aged and
non-aged zirconia restorations 31
Figure 9. One-piece titanium restoration after fracture strength test 31

1
Chapter 1. Introduction
Use of implants for single tooth restorations was first reported by Jemt in 1986
and has currently become a standard treatment modality with high survival rates
and predictability (Jung et al. 2008, 2012; Pjetursson et al. 2004, 2007, 2012).
Besides various biological and health outcomes such as patient comfort,
enhanced masticatory function, stable physiologic occlusion, sustained osseo-
integration, level of alveolar bone support and health of peri-implant soft tissues,
the success of implant-based treatments also depends on surrogate clinical
outcomes such as mechanical stability of the prosthetic components, rate of
technical complications and satisfactory esthetics (Bidra and Rungruanganunt
2013).
The association of mechanical stability and satisfactory esthetics is particularly
important for reconstructions in the areas of the mouth where esthetics becomes
a critical factor in overall success of the treatment and patient satisfaction.
Selection of the implant-supported restoration in the esthetic zone depends on
various factors such as patient’s expectations, position of the smile line, gingival
biotype, position and angulation of the fixture, available restorative space,
preferred type of retention of the restoration to the fixture and treatment
expenses (Bidra and Rungruanganunt 2013). The selection of the most suitable
implant-based replacement for a single missing tooth that can be satisfactory for
the esthetically demanding patient along with long-term mechanical resistance to
heavy occlusal forces is a controversial issue in the dental literature and among
the restorative dentists.
The aim of the present in vitro study is to evaluate and compare the mechanical
performance of 2 types of implant-supported screw-retained customized full-
contoured restorations, and to evaluate the effect of simulated oral conditions on
full-contoured 2-piece zirconia restorations.
2
Chapter 2. Literature Review
Different types of implant-supported restorations for replacement of a single
missing tooth have been described in the literature. These restorations can be
categorized based on type of fixation to the supporting fixture, material, method
of fabrication and the configuration of the connection with the restorative platform
of the implant.
Type of fixation of restoration to the implant For implant-supported single crowns, the connection of the final restoration to the
implant can be cement-retained or screw-retained (Hebel and Gajjar 1997). In
cement-retained prostheses, the abutment (mesostructure) is fabricated
separately and the restoration is cemented to the abutment (two-piece). This
technique resembles the clinical and laboratory procedures for tooth-supported
restorations. Multiple factors affect the strength of cement retention between the
abutment and the super-structure, including the abutment degree of taper,
surface area and roughness and type of cement (Hebel and Gajjar 1997).
With screw-retained prostheses, the restoration might be separate from the
abutment (two-piece) or combined as part of the fabrication procedure and
directly screwed to the implant (one-piece). An important stabilizing factor for
screw-retained systems is the “preload” or the tensile force developed on the
connecting screw thread by the tightening torque, which creates compressive
forces at the interface of the restoration and the implant and helps hold the
components together (Dittmer et al. 2012). Screw joint stability is maintained by
adequate preloading of the screw, precise fit between the implant platform and
the restoration, effective anti-rotational interface and adequate friction between
the screw threads and the implant (Dhingra et al. 2013).
Both retention methods are associated with a number of advantages and
limitations (Wittneben et al. 2014). The main advantage of screw-retained
implant reconstructions is predictable retrievability, which facilitates the removal
of the restoration with lower risk of damage to the restoration or the fixture.
3
Removal of the supra structures is sometimes necessary for periodontal
maintenance, for management of mechanical complications such as tightening of
loosened screws, repair or modification of the prosthesis and replacement of
prosthetic components or when surgical interventions are required for
management of biologic complications (Michalakis et al. 2003). Other important
advantages of screw-retention include applicability in areas with limited inter-arch
space and elimination of the cement from the restoration assembly (Sailer et al.
2012). However, screw-retained reconstructions require precise placement of the
fixture, due to the position of the screw access channel. Compromised structural
durability and difficulty in achieving proper occlusion are other concerns related
to screw-retained restorations. Screw channel access might occupy 50% - 75%
of the occlusal surface of the premolar and molar teeth, compromising the
integrity of the framework and the veneering layers, as well as interfering with
centric and excursive occlusal contacts (Hebel and Gajjar 1997; Wittneben et al.
2014). The conventional manufacturing process of screw-retained restorations is
more technique-sensitive than cemented reconstructions (Michalakis et al.
2003).
The advantages of cement-retained restorations are the possibility of
compensation for discrepancies in implant position and angulation, passivity of
fit, easier seating and chair-side adjustments, higher esthetics, and easier control
of occlusion (Hebel and Gajjar 1997; Michalakis et al. 2003). Major
disadvantages of cement-retained prostheses are difficulty in retrieving the
restoration, need for more inter-arch space and limitations in proper removal of
excess cement (Linkevicius et al. 2013). A prospective clinical study on the
relationship between remaining cement and peri-implant disease reported that
excessive dental cement was associated with the development of peri-implant
soft and hard tissue diseases and bone loss in 81% of the cases (Wilson 2009).
A recent comprehensive systematic review of 73 studies with 5858 different fixed
implant reconstructions including single crowns (1720), partial prostheses (979),
full arch prostheses (928) and cantilever partial prostheses (61), different
retention systems including one-piece screw-retained (59%) and cement-
4
retained (41%), and different materials, with follow-up of at least 3 years reported
estimations of 5- and 10-year survival rates as 95.5% and 91.3% for screw-
retained and 96.0% and 92.2% for cement-retained restorations respectively.
None of the reconstruction groups showed statistically significant differences in
the estimated survival rates, based on the type of retention. The review reported
a significantly higher total event rate of biological and technical complications
associated to cement-retained implant-based fixed restorations. Due to easier
retrievability for management of technical and biologic complications, screw-
retained restorations were recommended (Wittneben et al. 2014).
Abutment material Commercially pure titanium has been traditionally used as the material of choice
for fabrication of the implant abutment or the restoration framework for
replacement of the single tooth, because of its well-proven biocompatibility (Adell
et al. 1981; Buser et al. 1997; Lindhe and Berglundh 1998; Linkevicius et al.
2010) and mechanical properties (Pjetursson et al. 2007). Historically, the
prosthetic components for single implant restorations were derived from the
previous designs for rehabilitation of completely edentulous patients. These
restorations were initially made of machined titanium components veneered with
acrylic resin (Jemt 1986). This design then evolved to a restoration consisting of
a prefabricated titanium abutment supporting a cemented metal-ceramic crown
(Bidra and Rungruanganunt 2013). This was followed by the introduction of
UCLA abutments, in which for the first time a customized cast metal restoration
could be directly screwed to the dental implant (Lewis et al. 1988). UCLA
abutments are still used for screw- and cement-retained implant-supported
prostheses.
A systematic review reported a few complications associated with metal
abutments supporting fixed implant-based prostheses; with the most frequently
occurring problem being the loosened abutment screw (Pjetursson et al. 2007).
A major complication of titanium-based restorations is the unnatural blue or gray
discoloration at the peri-implant soft tissues (Tan and Dunne 2004). This
5
phenomenon might compromise the clinical outcome of the implant-borne
reconstruction in the esthetic zone, particularly in patients with high smile line,
thin (less than 2mm) gingival biotype, when the fixture is placed in close
proximity to the labial cortical plate or superficially in the residual alveolar bone
and also following peri-implant bone loss and soft tissue recession (Sailer et al.
2007a, Sailer et al. 2007b; Jung et al. 2008; van Brakel et al. 2011).
Numerous strategies have been developed in order to overcome the esthetic
complications related to the dark-hued titanium supra-structures, including the
use of cast gold alloys and gold-colored titanium nitride-coated abutments (Sailer
et al. 2009b). These materials might improve the gingival discoloration to some
extent, but the overall translucency of the restoration may remain unsatisfactory
due to the opaque nature of the metal (Bressan et al. 2011).
In order to achieve optimal esthetics in the anterior and premolar regions, all-
ceramic abutments made of alumina or zirconia were introduced. The use of
alumina implant abutments was first reported by Prestipino and Ingber in 1993.
These abutments, made of densely sintered highly purified 99.5% aluminum-
oxide ceramic cores, provided improved esthetics but showed relatively low
fracture resistance of about 241N (Att et al. 2006). Fracture of alumina
abutments was also reported in a number of clinical studies (Andersson et al.
2003; Henriksson and Jemt 2003). The weaknesses of the alumina restorations
prompted the development of zirconia implant abutments.
Pure zirconia is a polymorphic crystal that can be found in 3 different phases:
monoclinic (room temperature – 1170°C), tetragonal (1170° – 2370°C) and cubic
(2370° – melting point) (Piconi and Maccauro 1999). “Stabilizers” such as yttrium
are added to the composition of zirconia to minimize the phase transformation
and to retain the crystals in the more stable tetragonal phase with enhanced
physical and mechanical properties, at room temperature (Zembic et al. 2013).
Wohlwend et al. introduced the first 3-yttria-stabilized tetragonal zirconia
polycrystalline (Y-TZP) as an all-zirconia abutment in 1997. Glauser et al. first
6
described the densely sintered (Y-TZP) as an implant abutment, in 2004.
Zirconia is a biocompatible material with high mucosal attachment
(Abrahamsson et al. 1998) and lower rates of bacterial adhesion, compared to
titanium (Scarano et al. 2004). This material has shown high flexure strength of
900 to 1200 MPa, high fracture toughness (resistance to crack propagation or
the tensile stress that must be achieved in a crack tip before fracture is initiated)
of 9 to 10 MPa/m2 (although lower than 45 MPa/m2 reported for pure titanium),
low thermal conductivity and low corrosion potential (Kim et al. 1997, Andersson
et al. 2001, Yildirim et al. 2003, Adatia et al. 2009; Zembic et al. 2013, Delben et
al. 2014). Zirconia is also radiopaque and presents superior optical properties
over titanium (Brodbeck 2003; Tan and Dunne 2004). Depending on its
thickness, zirconia exhibits different degrees of translucency and therefore
enables the fabrication of an esthetic restoration. A systematic review of clinical
studies showed that based on spectrophotometric analyses, peri-implant
mucosal discoloration is significantly lower for zirconia abutments compared to
titanium or cast metal abutments (Bidra and Rungruanganunt 2013).
Several weaknesses have been mentioned for zirconia-based restorations. In
contrast to ductile metals with enhanced tolerance to both compressive and
tensile forces, zirconia is brittle and vulnerable to bending and subcritical crack
growth (Guazzato et al. 2004), especially when prepared in thin sections (less
than 0.5 mm) or with sharp edges (Aboushelib and Salameh 2009). The
configuration of the implant-restoration connection, abutment thickness at the
implant interface, and angulation of the loading forces might also have a
substantial influence on the durability and stability of the all-zirconia abutments
(Albosefi et al. 2014). Another shortcoming of zirconia is its inherent accelerated
aging (Zembic et al. 2013), in which a spontaneous slow transformation of the
tetragonal to the monoclinic phase occurs in the moist oral environment with
changing temperatures and constant load that may lead to decreased strength of
the material and increased risk of catastrophic failures over time (Kim et al.
2010). Aggressive adjustments or improper laboratory and clinical handling might

7
exacerbate this aging process (Luthardt et al. 2004).
Types of commercially available zirconia restorations Zirconia abutments are currently available as standard prefabricated or
individually customized components, using computer-aided design/computer
aided manufacturing (CAD/CAM) technology (Conrad et al. 2007). The
standardized shape and diameter of prefabricated abutments may be a limiting
factor in proper positioning of the future crown margin and also in establishing an
appropriate emergence profile. The need for substantial modifications of these
abutments prior to insertion might increase the risk of micro crack formation,
accelerated phase transformation and possible catastrophic mechanical failures
(Canullo et al. 2013). The CAD/CAM systems enable the fabrication of an
individualized component with the desired diameter, contour, emergence profile
and relationship with the adjacent soft and hard tissues that mimic the properties
of the lost natural dentition (Abbo et al. 2008). Customized zirconia restoration is
initially milled in its soft (green) state to the final shape and then sintered with
minimal need for further adjustments. The custom-made abutment can also be
colored before stabilization for enhanced esthetic results (Conrad et al. 2007).
Several clinical studies have demonstrated the longevity of zirconia abutments in
implant-supported single restorations for anterior and premolar regions. One of
these was a combined prospective and retrospective study investigating the
clinical outcomes for 185 implant-supported custom-made single-tooth zirconia
abutments for up to 5 years. Various biological, mechanical and esthetic
parameters as well as subjective patient factors were considered. The results of
this study demonstrated satisfactory performance of zirconia abutments over the
follow-up period with relatively low biological and technical complications and
high patient satisfaction rates. Biological complications were reported for 36% of
the implants. Regarding the mechanical complications, only 2 abutments (1%)
fractured and were replaced, 3 crowns exhibited non-significant chipping of the
veneering porcelain and 1 abutment experienced screw loosening. The authors
concluded that zirconia abutments for single implant crowns demonstrate good
8
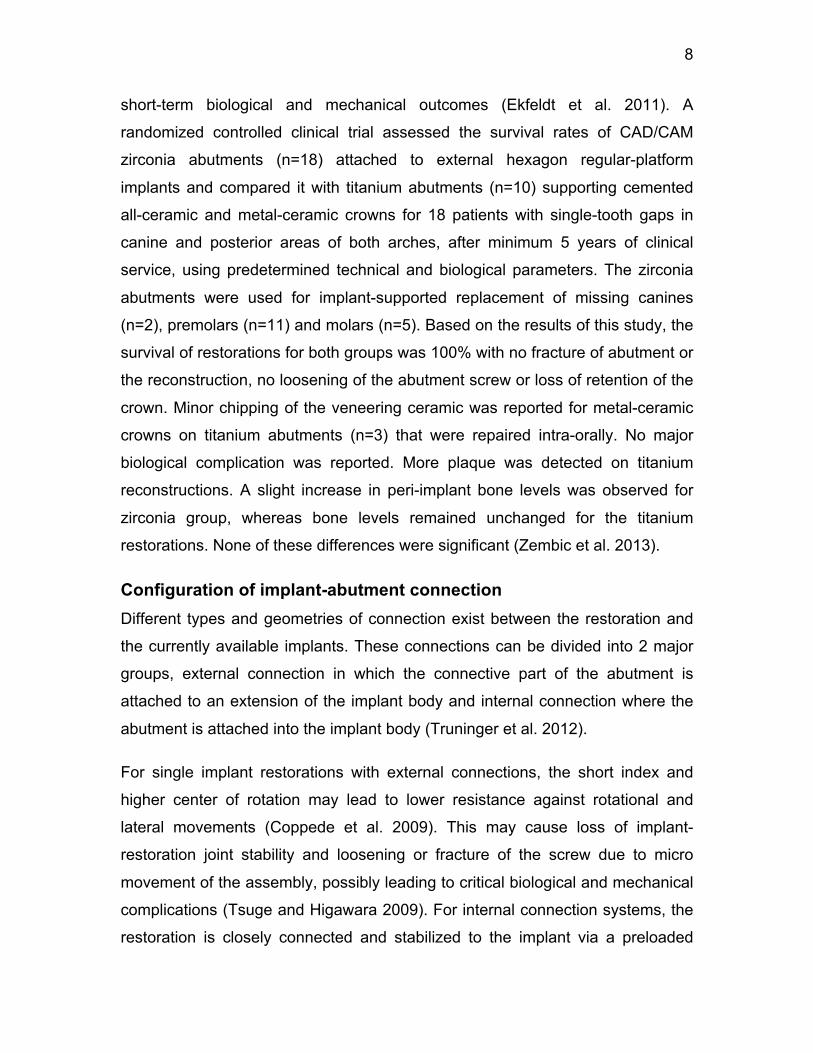
short-term biological and mechanical outcomes (Ekfeldt et al. 2011). A
randomized controlled clinical trial assessed the survival rates of CAD/CAM
zirconia abutments (n=18) attached to external hexagon regular-platform
implants and compared it with titanium abutments (n=10) supporting cemented
all-ceramic and metal-ceramic crowns for 18 patients with single-tooth gaps in
canine and posterior areas of both arches, after minimum 5 years of clinical
service, using predetermined technical and biological parameters. The zirconia
abutments were used for implant-supported replacement of missing canines
(n=2), premolars (n=11) and molars (n=5). Based on the results of this study, the
survival of restorations for both groups was 100% with no fracture of abutment or
the reconstruction, no loosening of the abutment screw or loss of retention of the
crown. Minor chipping of the veneering ceramic was reported for metal-ceramic
crowns on titanium abutments (n=3) that were repaired intra-orally. No major
biological complication was reported. More plaque was detected on titanium
reconstructions. A slight increase in peri-implant bone levels was observed for
zirconia group, whereas bone levels remained unchanged for the titanium
restorations. None of these differences were significant (Zembic et al. 2013).
Configuration of implant-abutment connection Different types and geometries of connection exist between the restoration and
the currently available implants. These connections can be divided into 2 major
groups, external connection in which the connective part of the abutment is
attached to an extension of the implant body and internal connection where the
abutment is attached into the implant body (Truninger et al. 2012).
For single implant restorations with external connections, the short index and
higher center of rotation may lead to lower resistance against rotational and
lateral movements (Coppede et al. 2009). This may cause loss of implant-
restoration joint stability and loosening or fracture of the screw due to micro
movement of the assembly, possibly leading to critical biological and mechanical
complications (Tsuge and Higawara 2009). For internal connection systems, the
restoration is closely connected and stabilized to the implant via a preloaded

9
screw and the friction locking effect at the longer junction of the abutment and
the restorative platform of the implant (Chun et al. 2015). In order to investigate
the effect of connection on mechanical performance of the implant-restoration
assembly an in vitro study evaluated the resistance to bending forces of metal
abutments attached to 7 implant systems (n=10) with various connections and
joint depths (0.6 – 6.0 mm), under static load at 90° angle. Systems with external
connection and shallow joints showed significantly less resistance compared to
internally connected systems with deep joining walls (Mollersten et al. 1997).
Internal connections provide better biological sealing, joint stability, stress
distribution and resistance to bending forces, because of deeper joining walls,
increased surface contact area, more intimate contact with the implant platform
and overall enhanced anti-rotational effect (Delben 2014).
Zirconia restorations are compatible with both external and internal connections.
Internal connection of zirconia abutments can be established by the uniform
zirconia component (one-piece system) or by a secondary element made of
titanium alloy that engages with the restorative platform of the implant on one
side and with the zirconia abutment/restoration on the other side (two-piece
system) (Sailer et al. 2007a).
One-piece zirconia restorations There are certain weaknesses associated with the 1-piece zirconia abutments.
Firstly, these abutments cannot be machined to the same degree of precision as
metal abutments and therefore their fit with the restorative platform of the implant
would be less intimate (Ebert et al. 2007). This matter was tested by an in vitro
study that measured the rotational misfit between the abutment and implant at
their junction for 5 abutment systems (2 zirconia, 2 alumina, 1 titanium, n=10)
connected to 2 different implant systems (Branemark Nobel Biocare and Biomet
3i), using scanning electron microscopy and a precision optical encoder. 1-piece
all-zirconia abutments showed significantly higher values of abutment-implant
linear gap and rotational misfit compared to 2-piece systems. The titanium
10
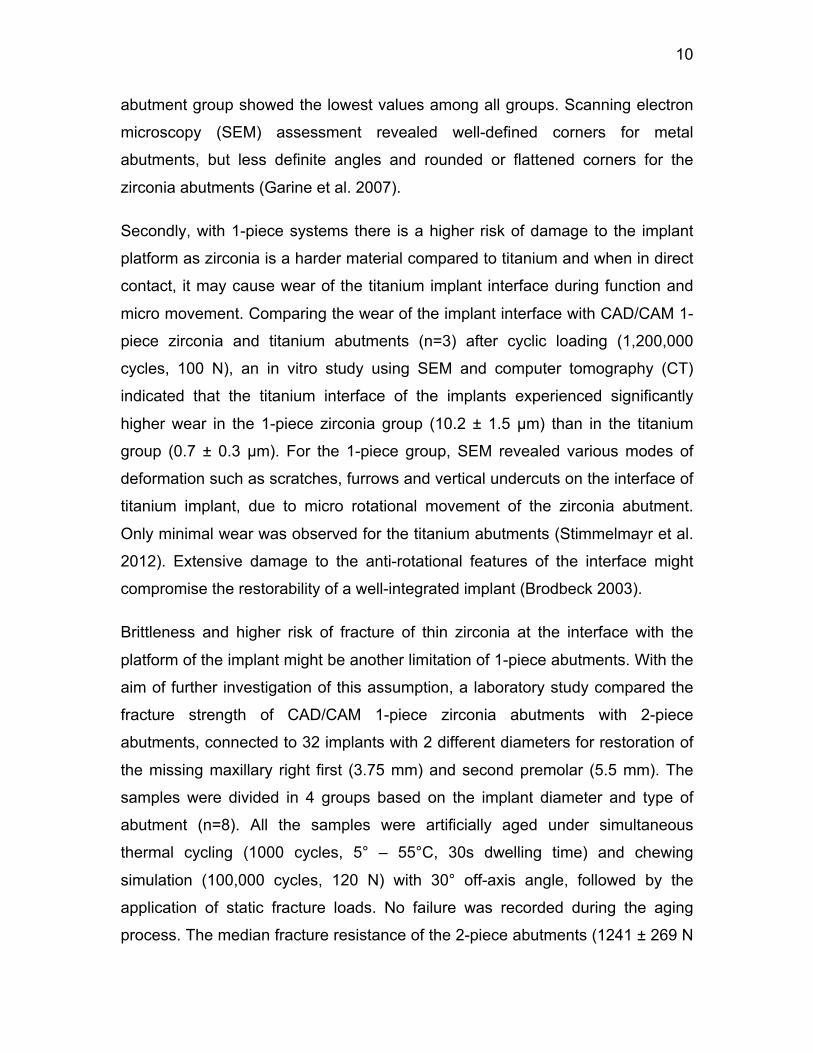
abutment group showed the lowest values among all groups. Scanning electron
microscopy (SEM) assessment revealed well-defined corners for metal
abutments, but less definite angles and rounded or flattened corners for the
zirconia abutments (Garine et al. 2007).
Secondly, with 1-piece systems there is a higher risk of damage to the implant
platform as zirconia is a harder material compared to titanium and when in direct
contact, it may cause wear of the titanium implant interface during function and
micro movement. Comparing the wear of the implant interface with CAD/CAM 1-
piece zirconia and titanium abutments (n=3) after cyclic loading (1,200,000
cycles, 100 N), an in vitro study using SEM and computer tomography (CT)
indicated that the titanium interface of the implants experienced significantly
higher wear in the 1-piece zirconia group (10.2 ± 1.5 µm) than in the titanium
group (0.7 ± 0.3 µm). For the 1-piece group, SEM revealed various modes of
deformation such as scratches, furrows and vertical undercuts on the interface of
titanium implant, due to micro rotational movement of the zirconia abutment.
Only minimal wear was observed for the titanium abutments (Stimmelmayr et al.
2012). Extensive damage to the anti-rotational features of the interface might
compromise the restorability of a well-integrated implant (Brodbeck 2003).
Brittleness and higher risk of fracture of thin zirconia at the interface with the
platform of the implant might be another limitation of 1-piece abutments. With the
aim of further investigation of this assumption, a laboratory study compared the
fracture strength of CAD/CAM 1-piece zirconia abutments with 2-piece
abutments, connected to 32 implants with 2 different diameters for restoration of
the missing maxillary right first (3.75 mm) and second premolar (5.5 mm). The
samples were divided in 4 groups based on the implant diameter and type of
abutment (n=8). All the samples were artificially aged under simultaneous
thermal cycling (1000 cycles, 5° – 55°C, 30s dwelling time) and chewing
simulation (100,000 cycles, 120 N) with 30° off-axis angle, followed by the
application of static fracture loads. No failure was recorded during the aging
process. The median fracture resistance of the 2-piece abutments (1241 ± 269 N
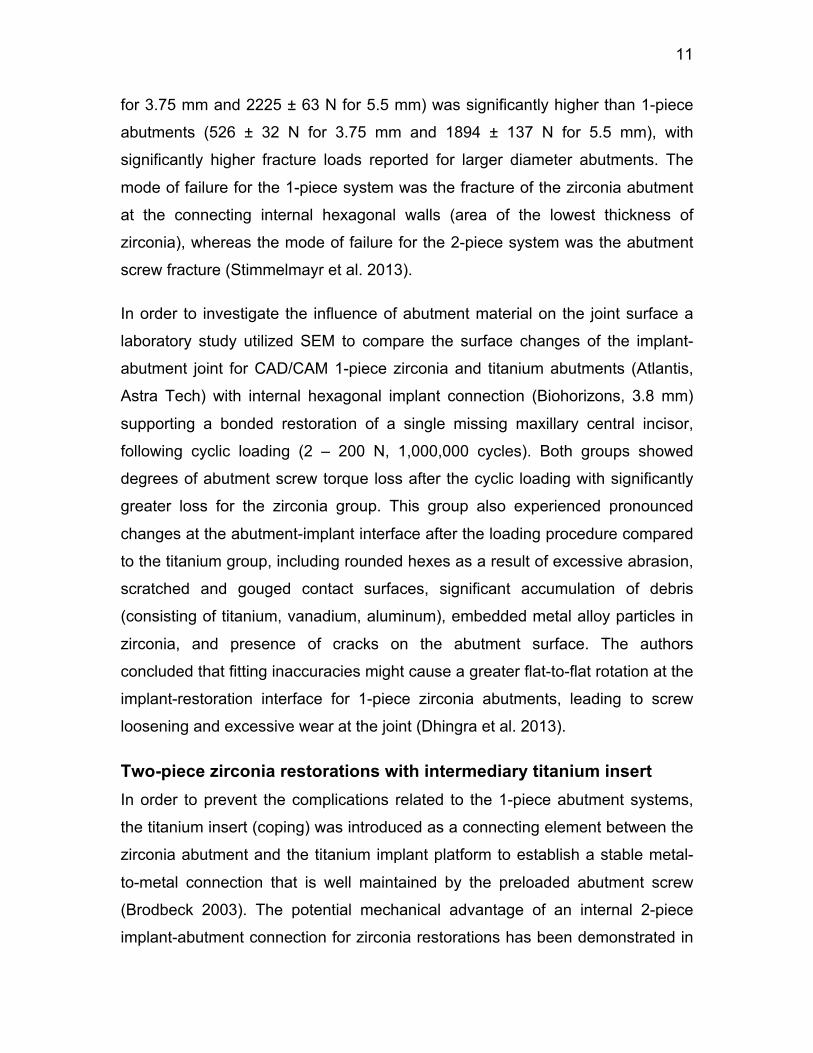
11
for 3.75 mm and 2225 ± 63 N for 5.5 mm) was significantly higher than 1-piece
abutments (526 ± 32 N for 3.75 mm and 1894 ± 137 N for 5.5 mm), with
significantly higher fracture loads reported for larger diameter abutments. The
mode of failure for the 1-piece system was the fracture of the zirconia abutment
at the connecting internal hexagonal walls (area of the lowest thickness of
zirconia), whereas the mode of failure for the 2-piece system was the abutment
screw fracture (Stimmelmayr et al. 2013).
In order to investigate the influence of abutment material on the joint surface a
laboratory study utilized SEM to compare the surface changes of the implant-
abutment joint for CAD/CAM 1-piece zirconia and titanium abutments (Atlantis,
Astra Tech) with internal hexagonal implant connection (Biohorizons, 3.8 mm)
supporting a bonded restoration of a single missing maxillary central incisor,
following cyclic loading (2 – 200 N, 1,000,000 cycles). Both groups showed
degrees of abutment screw torque loss after the cyclic loading with significantly
greater loss for the zirconia group. This group also experienced pronounced
changes at the abutment-implant interface after the loading procedure compared
to the titanium group, including rounded hexes as a result of excessive abrasion,
scratched and gouged contact surfaces, significant accumulation of debris
(consisting of titanium, vanadium, aluminum), embedded metal alloy particles in
zirconia, and presence of cracks on the abutment surface. The authors
concluded that fitting inaccuracies might cause a greater flat-to-flat rotation at the
implant-restoration interface for 1-piece zirconia abutments, leading to screw
loosening and excessive wear at the joint (Dhingra et al. 2013).
Two-piece zirconia restorations with intermediary titanium insert In order to prevent the complications related to the 1-piece abutment systems,
the titanium insert (coping) was introduced as a connecting element between the
zirconia abutment and the titanium implant platform to establish a stable metal-
to-metal connection that is well maintained by the preloaded abutment screw
(Brodbeck 2003). The potential mechanical advantage of an internal 2-piece
implant-abutment connection for zirconia restorations has been demonstrated in
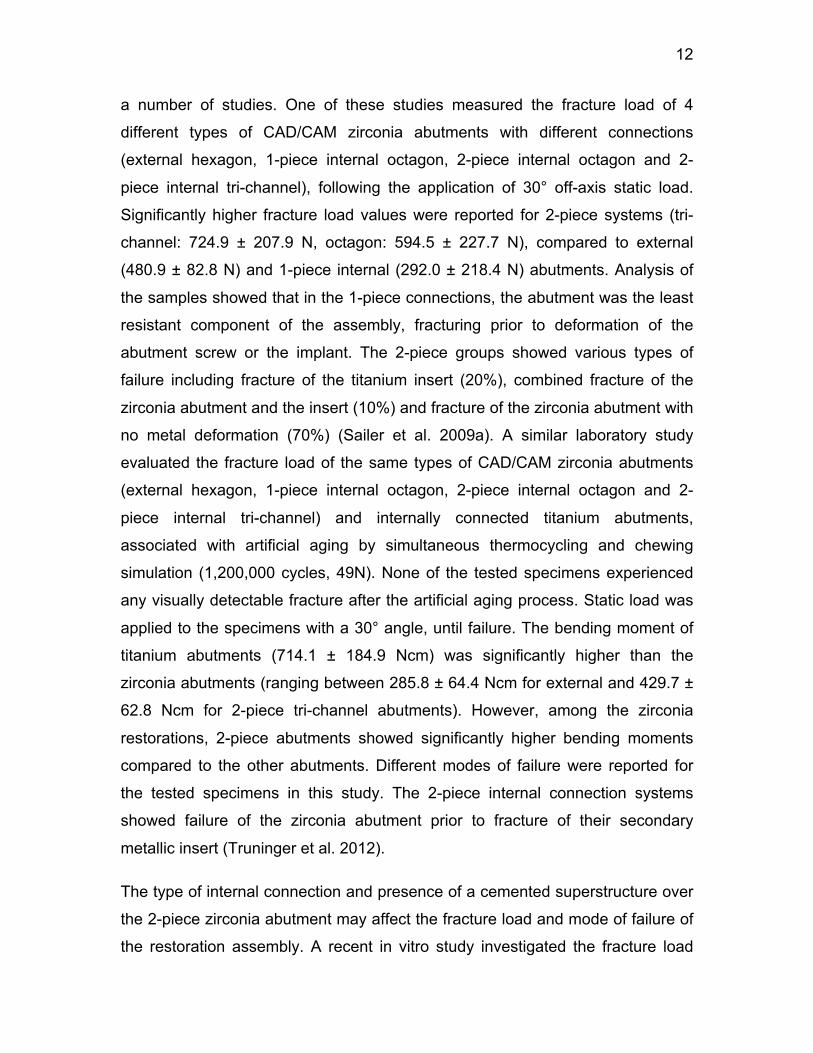
12
a number of studies. One of these studies measured the fracture load of 4
different types of CAD/CAM zirconia abutments with different connections
(external hexagon, 1-piece internal octagon, 2-piece internal octagon and 2-
piece internal tri-channel), following the application of 30° off-axis static load.
Significantly higher fracture load values were reported for 2-piece systems (tri-
channel: 724.9 ± 207.9 N, octagon: 594.5 ± 227.7 N), compared to external
(480.9 ± 82.8 N) and 1-piece internal (292.0 ± 218.4 N) abutments. Analysis of
the samples showed that in the 1-piece connections, the abutment was the least
resistant component of the assembly, fracturing prior to deformation of the
abutment screw or the implant. The 2-piece groups showed various types of
failure including fracture of the titanium insert (20%), combined fracture of the
zirconia abutment and the insert (10%) and fracture of the zirconia abutment with
no metal deformation (70%) (Sailer et al. 2009a). A similar laboratory study
evaluated the fracture load of the same types of CAD/CAM zirconia abutments
(external hexagon, 1-piece internal octagon, 2-piece internal octagon and 2-
piece internal tri-channel) and internally connected titanium abutments,
associated with artificial aging by simultaneous thermocycling and chewing
simulation (1,200,000 cycles, 49N). None of the tested specimens experienced
any visually detectable fracture after the artificial aging process. Static load was
applied to the specimens with a 30° angle, until failure. The bending moment of
titanium abutments (714.1 ± 184.9 Ncm) was significantly higher than the
zirconia abutments (ranging between 285.8 ± 64.4 Ncm for external and 429.7 ±
62.8 Ncm for 2-piece tri-channel abutments). However, among the zirconia
restorations, 2-piece abutments showed significantly higher bending moments
compared to the other abutments. Different modes of failure were reported for
the tested specimens in this study. The 2-piece internal connection systems
showed failure of the zirconia abutment prior to fracture of their secondary
metallic insert (Truninger et al. 2012).
The type of internal connection and presence of a cemented superstructure over
the 2-piece zirconia abutment may affect the fracture load and mode of failure of
the restoration assembly. A recent in vitro study investigated the fracture load
13
and modes of failure of CAD/CAM zirconia abutments with 5 different implant
connections (external hexagon, 1-piece octagon, 1-piece long conical, 2-piece
tri-channel and 2-piece octagon) supporting an all-ceramic crown for
replacement of a missing maxillary central incisor, and compared it with the
performance of titanium abutments (1-piece octagon). All the specimens were
exposed to thermocycling and chewing simulation (1,200,000 cycles, 49 N),
followed by application of static load at 30° angle from the implant axis. The
titanium abutments demonstrated the highest bending moment (1042.0 ± 86.8
Ncm), followed by 2-piece octagon (605.4 ± 54.7 Ncm), 2-piece tri-channel
(581.8 ±172.8 Ncm), external (556.7 ± 128.4 Ncm), 1-piece octagon (464.9 ±
106.6 Ncm) and 1- piece long conical (216.4 ± 90.0 Ncm) abutment systems.
The differences were found to be significant for the titanium (highest) and 1-
piece long conical abutments (lowest). All the abutments survived the artificial
aging. However, after the fracture strength test, fracture of 1-piece abutments
was observed on the internal part of the cone at the thinnest portion of the
zirconia and for the 2-piece octagon group, at the apical part of the junction
between the zirconia abutment and the titanium insert. The authors concluded
that 2-piece connections demonstrated a more favorable mechanical
performance compared to the 1-piece systems and also the type of 2-piece
internal connection had a minor effect on the performance of zirconia abutments
(Muhlemann et al. 2014).
The attachment of zirconia restoration to the titanium insert in 2-piece internal
connection systems could be achieved mainly through friction fit or bonding by
resin cement. In bonded assemblies, the adhesion of components is optimized
under proper laboratory conditions to enhance the long-term stability of the
bonding and health of the peri-implant soft tissues (Rosentritt et al. 2015). In
order to assess the effect of implant-abutment interface and also method of
attachment of zirconia to titanium insert on fracture resistance of the assembly, a
laboratory study compared the maximum static load capacity and mode of failure
for 3 different types of CAD/CAM zirconia abutments (1-piece, 2-piece with
friction-fitted titanium insert and 2-piece with resin bonded titanium insert),
14
attached to regular platform implants through a tri-channel internal connection
(Nobel Replace Tapered Groovy RP), for replacement of a single missing
maxillary central incisor. All samples were exposed to artificial aging by means of
thermocycling (20000 cycles, 5° – 55°C, 20s dwelling time). The result of this
study showed significantly higher fracture loads for the 2-piece abutment with
bonded titanium insert (729.2 ± 35.9 N) compared to 2-piece with friction-fitted
titanium insert (484.6 ± 56.6 N) and 1-piece system (503.09 ± 46.3 N).
Furthermore, different modes of failure were detected among the samples: 1-
piece samples fractured at the thinnest segment of zirconia, located between the
walls of the tri-channel connection. 2-piece friction-fitted system showed fracture
of zirconia at the internal aspect of the contact area with the titanium insert,
whereas 2-piece bonded systems showed separation between the zirconia
abutment and titanium insert and fracture of the titanium insert (Kim et al. 2013).
Two-piece zirconia abutment systems are advocated for minimizing the
shortcomings of 1-piece abutments by eliminating the direct contact of the thin
and weak point of zirconia abutment with the implant surface, and therefore
maintaining the biological and biomechanical advantages of the internal
connection along with the esthetic properties of zirconia (Brodbeck 2003). To
clinically test this hypothesis, a prospective clinical study investigated the
survival rate of 30 single implant-supported 2-piece CAD/CAM customized
zirconia abutments bonded to titanium inserts, supporting all-ceramic crowns for
replacement of maxillary and mandibular incisors (n=6), canines (n=2),
premolars (n=8 and 2) and molars (n=2) for 25 patients. The survival rate of the
restorations was 100% over a period of 36 to 44 months with no biologic or
technical complication during the follow-up period. Favorable soft tissue reaction
to the abutment assembly was reported (Canullo 2007). Additionally, an in vitro
study evaluated the effect of the titanium insert on the fracture strength of the
zirconia abutments by comparing 3 different abutments (titanium, 1-piece and 2-
piece zirconia; n=5) with a specific internal hexagonal implant connection, for
replacement of a missing maxillary single anterior tooth. This study showed that
under 30° off-axis compressive loading, titanium abutments had the highest
15
fracture load (1404.7 ± 19.5 N), followed by 2-piece (1216.8 ± 41.2 N) and 1-
piece (1119.5 ± 4.8 N) zirconia abutments, with statistically significant
differences among groups. The failure mode for titanium abutments was found to
be deformation while the failure mode for both zirconia groups was fracture of
zirconia with or without screw fracture. In titanium and 1-piece zirconia abutment
groups, the failure occurred at the implant-abutment junction, while in the 2-piece
group, it occurred at the junction of zirconia and the titanium insert, above the
level of the implant platform. This failure mode might be more desirable in a
clinical situation due to higher retrievability of the components without further
damage to the implant (Chun et al. 2015).
Aging of the zirconia has been considered to influence the mechanical
performance of 2-piece zirconia restoration assemblies. To test this matter, a
recent in vitro study compared the fracture load of 36 CAD/CAM 2-piece
customized zirconia abutments with different marginal preparation depths on the
abutments (0.5 mm, 0.7 mm and 0.9 mm) supporting a cemented all-ceramic
crown for replacement of a missing maxillary right central incisor. Half of the
samples (n=18) were exposed to 5-year artificial aging under chewing simulation
(1,200,000 cycles, 49N, 45° angle) and thermocycling (5° - 55°), prior to fracture
test under static load. Preparation depth and artificial aging significantly affected
the fracture load. Marginal preparation depth of 0.5 mm had a significantly higher
fracture load than the other groups for both aged and non-aged samples.
Artificially aged samples experienced significant decrease in fracture load for all
groups of different preparation depths. However, the effect of preparation depth
on the fracture load of 2-piece zirconia abutments found to be more critical than
the artificial aging. For all groups, the mode of failure was fracture of the titanium
insert at the internal connection with the implant (Joo et al. 2015).
16
Chapter 3. Rationale and Objectives
Rationale As previously reported, several in vitro studies have investigated the load
capacity of 1- and 2-piece zirconia abutments attached to different implant
systems, with or without the overlying full-coverage restoration. Limited
information is available on the fracture strength of implant-supported full-
contoured 2-piece zirconia restorations as well as the effect of artificial aging on
the fracture load and mode of failure of these restorations. Furthermore, the
majority of the existing in vitro investigations have evaluated the fracture strength
of implant-supported replacements for single missing anterior maxillary teeth.
There is not a significant amount of data available regarding the performance of
posterior restorations. When compared with the incisors, occlusal forces are
significantly higher in the premolar regions. This matter becomes more critical in
patients with strong musculature or when lateral parafunctional forces are
applied to the restorations (Ferrario et al. 2004, de Zee et al. 2007).
For implant-supported replacement of a single missing maxillary first premolar
tooth, metal restorations with veneering porcelain have been traditionally used
with relatively high biological and mechanical predictability. However, there is a
growing demand among patients for esthetic replacements for the missing
posterior teeth. To address this demand and with the recent advancements in
materials and manufacturing technologies, highly esthetic high precision
customized milled 2-piece zirconia restorations with a prefabricated titanium
insert have been introduced by the manufacturers at a relatively low cost. It is
claimed that these restorations associate the mechanical resistance and esthetic
properties of zirconia, and they also assert increased stability of the connection
between the titanium insert and the restorative platform of the implant. It is
critical to verify these claims by well-designed in vitro and in vivo studies prior to
recommending these relatively recent restorations to the patients. Although in
vitro studies have inevitable integral limitations, they can provide valuable
information regarding the mechanical performance of these restorations by
17
measuring the fracture strength and defining the mode of failure under simulated
extreme conditions using precise and sophisticated methodologies.
Objectives The aims of the present in vitro study are:
- To investigate the fracture strength of implant-supported screw-retained
CAD/CAM customized full-contoured 2-piece zirconia and 1-piece titanium
single restorations with internal octagon connection;
- To evaluate the effect of artificial aging on the fracture strength of the
implant-supported full-contoured 2-piece zirconia restorations;
- To evaluate the mode of failure for the tested implant-restoration
assemblies.
Hypotheses The null hypotheses are:
- There is no difference between the fracture strength of implant-supported
screw-retained CAD/CAM full-contoured 2-piece zirconia and 1-piece
titanium restorations for replacement of single missing maxillary first
premolars;
- Artificial aging has no effect on fracture strength of 2-piece zirconia single
restorations.

18
Chapter 4. Materials and Methods
Materials Identical titanium endosseous dental implants with internal conical octagon
connection configuration (Bone Level, diameter: 4.1mm, length: 10 mm, Regular
Cross fit, SLActive, Straumann, Basel, Switzerland) were used for this in vitro
study to support the restorations. The tested restorations were 2-piece zirconia
restoration consisting of a customized high translucency zirconia component
(CARES, X-Stream, Zerion HT, Straumann, Basel, Switzerland) bonded to a
prefabricated titanium insert (CARES RC Variobase TAN abutment, Diameter:
4.5mm, Height: 3.5mm, Straumann, Basel, Switzerland) with resin cement
(Panavia 21, Kuraray Dental, Tokyo, Japan), and 1-piece customized titanium
restoration (CARES RC abutment Ti/TAN, Straumann, Basel, Switzerland). All
the restorations were anchored to their supporting dental implants with identical
titanium screws (RC Basal Screw TAN, Straumann). The dimensions and
characteristics of the components used in the present study are described in
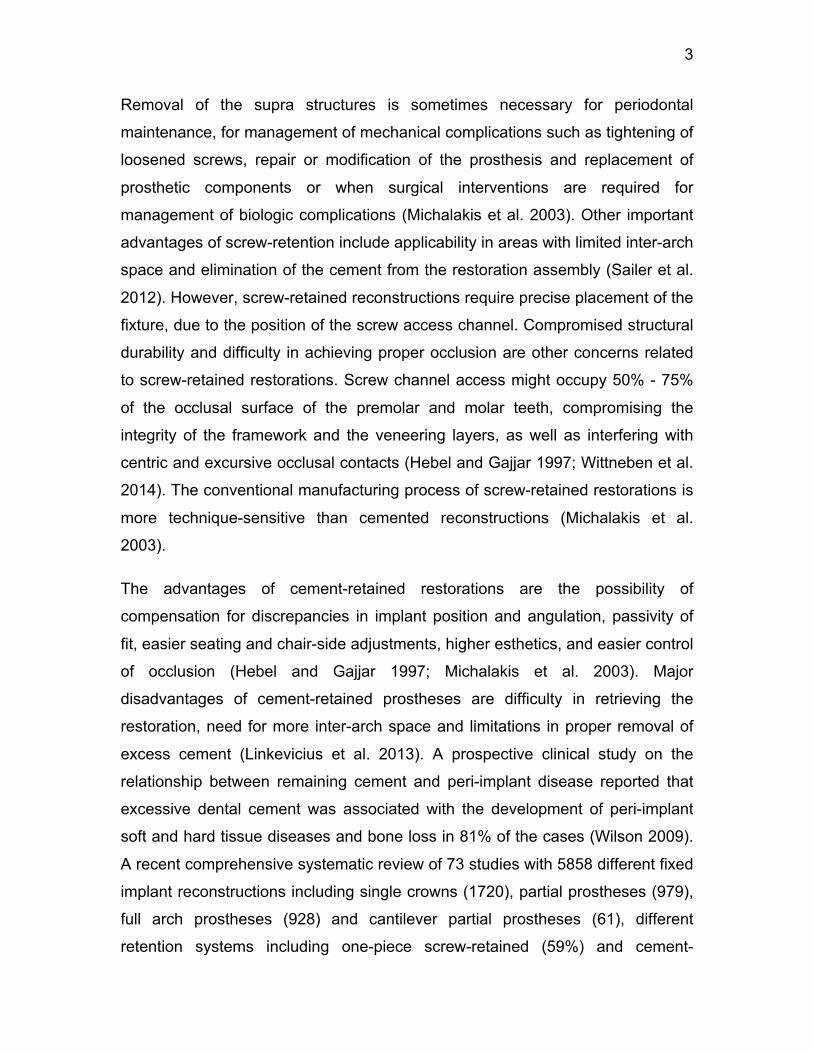
Table 1 and presented in Figure 1.
Experimental groups Thirty specimens were prepared for three experimental groups (n=10). The
sample size was determined based on sample size calculations using data from
previously performed similar studies (Sailer et al. 2009a, Apicella et al. 2011,
Canullo et al. 2013, Dhingra et al. 2013, Albosefi et al. 2014). Groups “Aged
Zirconia” (ZrA) and “Non-Aged Zirconia” (ZrNA) consisted of implant-supported
screw-retained CAD/CAM customized full-contoured high translucency 2-piece
zirconia restorations. Group “Titanium” (Ti) included implant-supported screw-
retained CAD/CAM customized full-contoured 1-piece titanium restorations.
Zirconia restorations in Group ZrA were exposed to artificial aging under chewing
simulation. The tested samples represented implant-supported replacements for
a single missing left maxillary first premolar tooth 24 and were identical in shape
and diameter.

19
A
B
C
D
Figure 1. Components used for preparation of the specimens. A) Implant fixture (BL, RC,
SLActive, Straumann) attached to the transfer piece. B) Titanium insert (Variobase, RC,
Straumann). C) Screw-retained customized CAD/CAM full-contoured high translucency
zirconia component (CARES, Zerion HT, Straumann). D) Screw-retained full-contoured milled
titanium restoration (CARES, RC, TAN, Straumann).
Table 1. Characteristics of materials used for the present study
Preparation of the implant fixtures Each implant fixture was embedded in auto-polymerizing polymethyl
methacrylate resin (Shade Clear, Jet Tooth Shade Powder and Jet Liquid, Lang
Dental Manufacturing Co, Inc, Wheeling, IL.) inside a hard plastic container with
Components Characteristics Composition N
Implant Fixture Straumann® Bone Level, Ø4.1mm X 10mm, Regular CrossFit®, SLActive® Titanium 30
Restorations 30 Full-contoured customized titanium Straumann® CARES RC abutment Ti/TAN. Titanium-aluminum-niobium 10
Full-contoured customized zirconia CARES® X-Stream™ Zerion® HT crown High translucency
zirconium-dioxide ceramic 20
Titanium insert Straumann® CARES® RC Variobase™ TAN abutment, Diameter: 4.5mm, Height: 3.5mm Titanium-aluminum-niobium 20
20
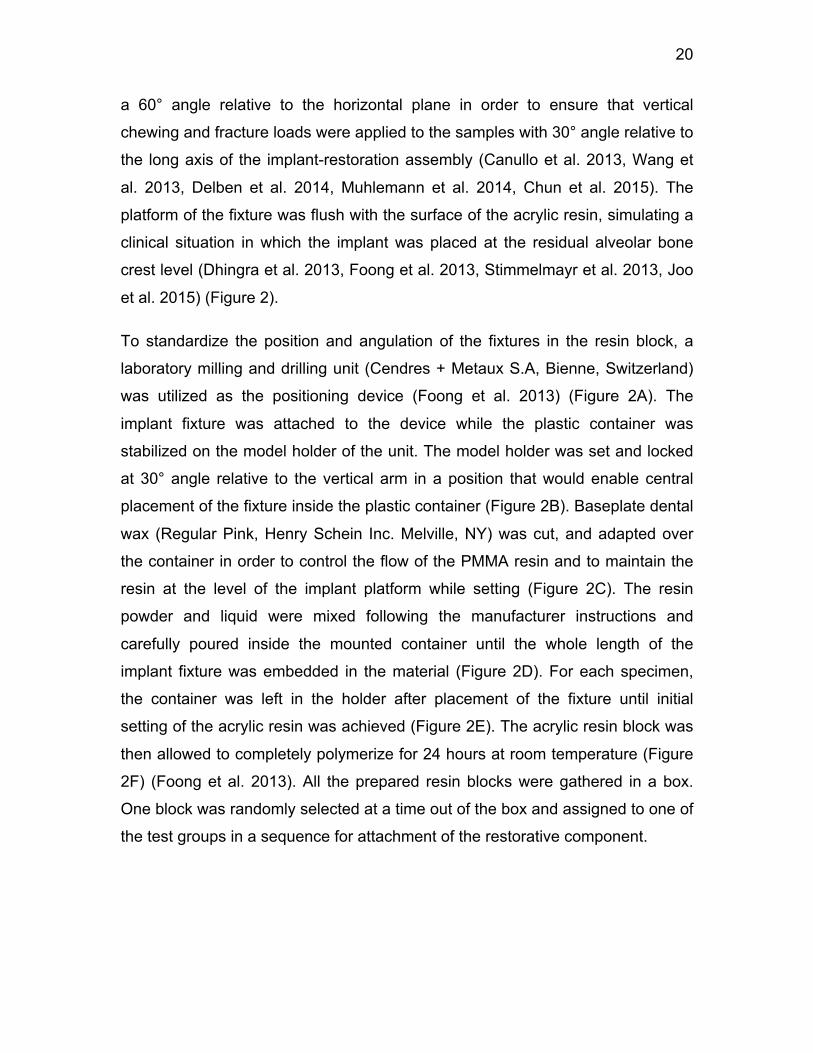
a 60° angle relative to the horizontal plane in order to ensure that vertical
chewing and fracture loads were applied to the samples with 30° angle relative to
the long axis of the implant-restoration assembly (Canullo et al. 2013, Wang et
al. 2013, Delben et al. 2014, Muhlemann et al. 2014, Chun et al. 2015). The
platform of the fixture was flush with the surface of the acrylic resin, simulating a
clinical situation in which the implant was placed at the residual alveolar bone
crest level (Dhingra et al. 2013, Foong et al. 2013, Stimmelmayr et al. 2013, Joo
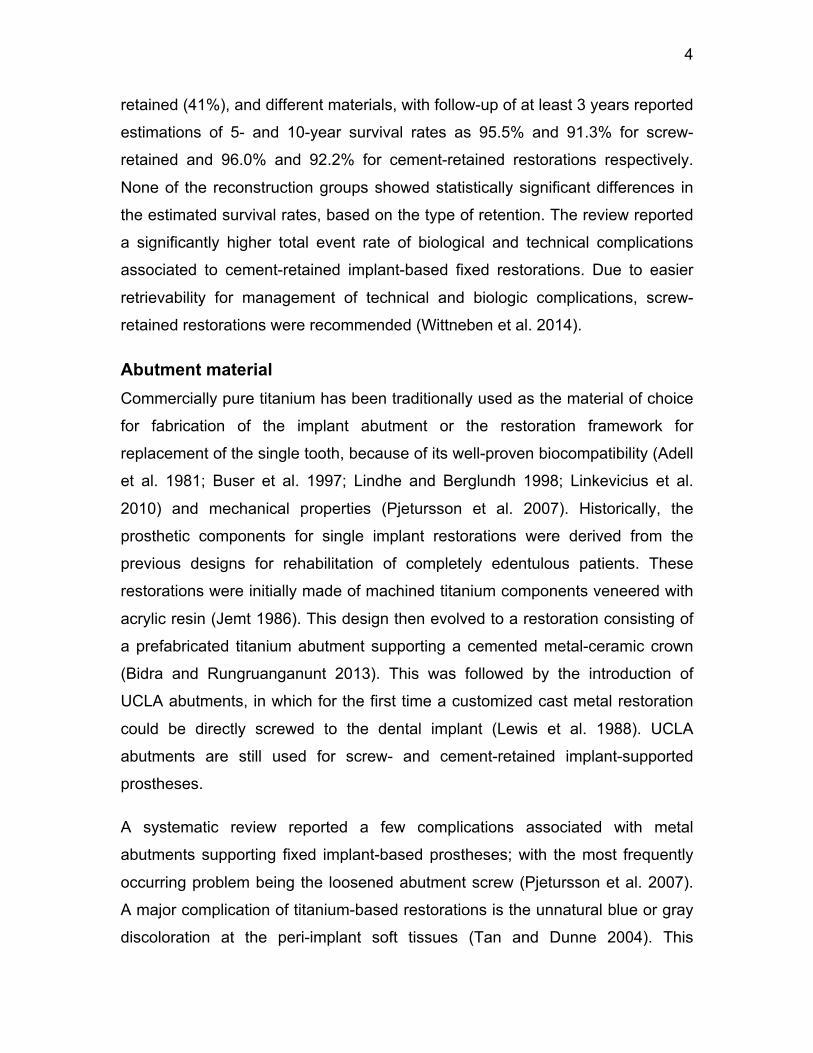
et al. 2015) (Figure 2).
To standardize the position and angulation of the fixtures in the resin block, a
laboratory milling and drilling unit (Cendres + Metaux S.A, Bienne, Switzerland)
was utilized as the positioning device (Foong et al. 2013) (Figure 2A). The
implant fixture was attached to the device while the plastic container was
stabilized on the model holder of the unit. The model holder was set and locked
at 30° angle relative to the vertical arm in a position that would enable central
placement of the fixture inside the plastic container (Figure 2B). Baseplate dental
wax (Regular Pink, Henry Schein Inc. Melville, NY) was cut, and adapted over
the container in order to control the flow of the PMMA resin and to maintain the
resin at the level of the implant platform while setting (Figure 2C). The resin
powder and liquid were mixed following the manufacturer instructions and
carefully poured inside the mounted container until the whole length of the
implant fixture was embedded in the material (Figure 2D). For each specimen,
the container was left in the holder after placement of the fixture until initial
setting of the acrylic resin was achieved (Figure 2E). The acrylic resin block was
then allowed to completely polymerize for 24 hours at room temperature (Figure
2F) (Foong et al. 2013). All the prepared resin blocks were gathered in a box.
One block was randomly selected at a time out of the box and assigned to one of
the test groups in a sequence for attachment of the restorative component.
21
A
B
C
D
E
F
Figure 2. Preparation of acrylic resin block and embedding of the implant fixture. A) Positioning
device and mounted container on the model holder. B) Attachment of the implant fixture to the
device, model holder is set and locked at 30° angle relative to the long axis of the implant. C) Implant fixture centrally positioned inside the container with the adapted base plate wax for
controlling the flow of the acrylic resin. D) Acrylic resin powder and liquid mixed and poured in the
container. E) Container left on the model holder till initial setting of the acrylic resin achieved. F) Acrylic resin block with the embedded implant 24 hours after initial setting.
22
Fabrication of the CAD/CAM restorations A customized implant-supported full-contoured screw-retained single restoration
for a missing maxillary left first premolar tooth 24 was virtually designed using
the manufacturer’s specific computer software (Straumann CARES Visual CAD).
The digital file was then electronically submitted to the manufacturer’s milling
centre (Straumann, Arlington, TX) for fabrication of computer-aided
design/computer-aided manufacture (CAD/CAM) restorations with identical
shapes and dimensions, using high precision, high-speed cutting (HSC) milling
technology. To ensure proper and standardized engagement of the indenters of
chewing simulation and load devices with the specimens, all the restorations had
a mild depression (3 mm diameter) on the occlusal table (lingual incline of the
buccal cusp), 2 mm away from the buccal cusp tip, as part of the original design.
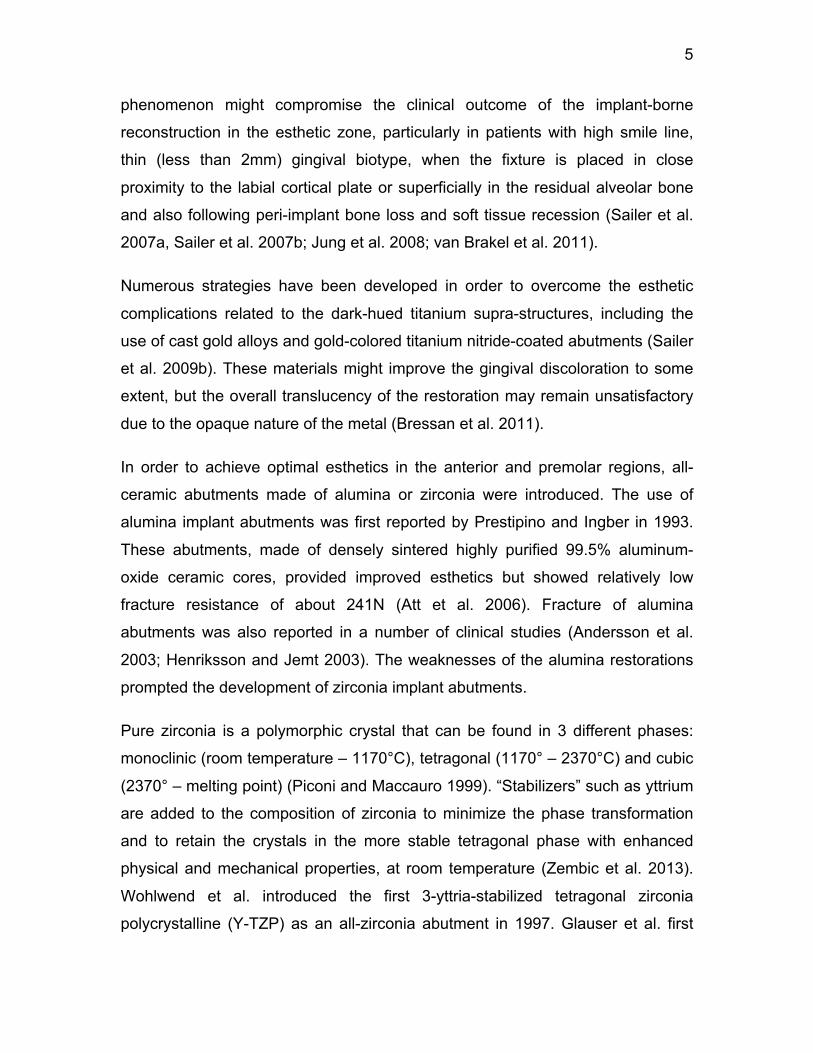
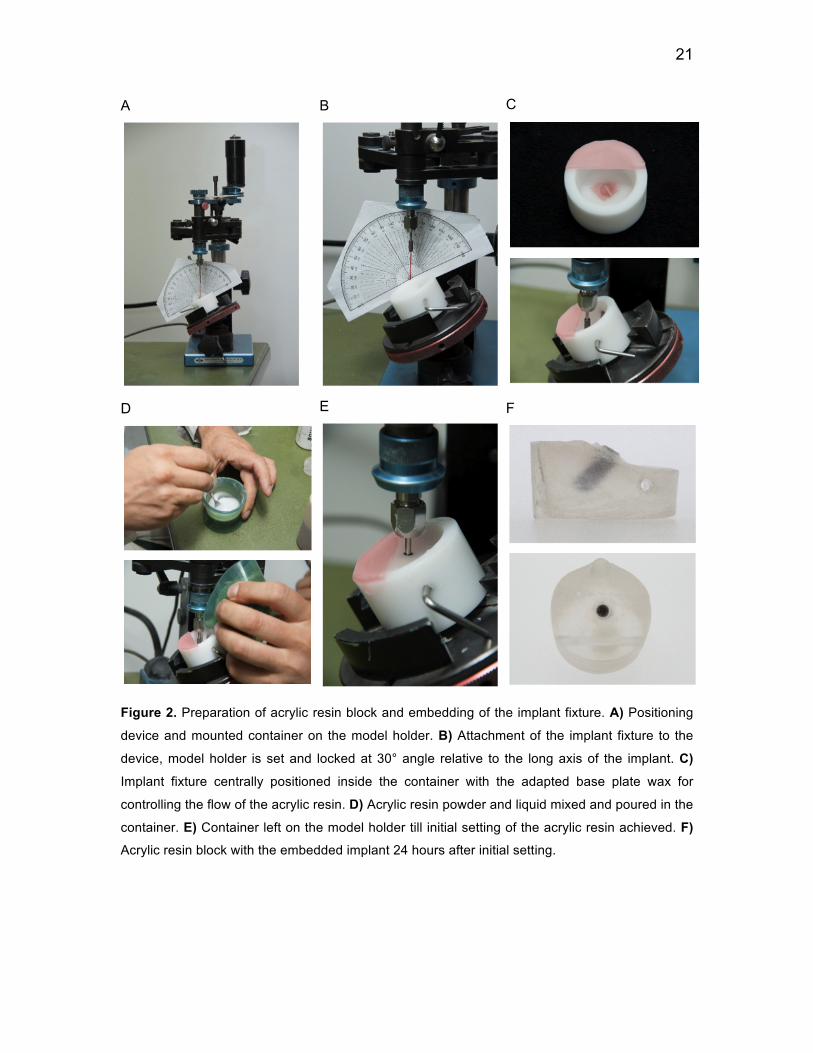
Preparation of the restorations and attachment to fixtures For each of the 2-piece zirconia specimens, the zirconia component was bonded
to the titanium insert, according to the manufacturer’s recommendations. Each
component was first cleaned with pressurized steam and alcohol (Figure 3B).
The titanium insert was then fixed to the implant with a laboratory screw (Figure
3C). Polytetrafluoroethylene (Teflon) tape was placed over the screw to block the
screw channel from penetration of the adhesive cement. After the application of
a thin layer of the mixed anaerobic-curing adhesive resin cement (Panavia 21,
Kuraray Dental, Tokyo, Japan) to the internal surface of the zirconia component
(Figures 3D and 3E), it was seated on the titanium insert and stabilized with
finger pressure for 2 minutes as per the manufacturer instructions (Figure 3F).
Oxygen barrier agent (Oxyguard II) was applied for 5 minutes to ensure
complete setting of the cement (Figure 3G). The restoration was then detached
from the implant and excess cement was gently removed with a periodontal
scaler under x10 magnification. Complete setting of the cement was allowed for
24 hours at room temperature. The assembly was then anchored to the implant
in the resin block with the definitive titanium screw (Figure 3I), tightened with a
calibrated torque control device (Straumann®) to 35 N/cm, according to the

23
manufacturer’s recommendation. The preload was checked and the screw
retightened if required, after 5 minutes (Delben et al. 2014).
For the 1-piece titanium specimens, each restoration was cleaned with
pressurized steam and alcohol and attached to the corresponding implant with a
similar abutment screw and preload force of 35 N/cm. All the specimens were
stored in room temperature prior to artificial aging process.
A
B
C
D
E
F
G
H
I
Figure 3. Preparation of 2-piece zirconia restoration and attachment to fixture. A) Components of
Straumann screw-retained restoration assembly (Variobase insert, full-contoured high
translucency Zerion crown and the RC Basal screw). B) Cleaning of the insert with pressurized
steam. C) Stabilization of the insert to the implant with a laboratory screw. D, E) Mixing of the
adhesive cement (Panavia) and application to the internal surface of the zirconia component. F) Seating and stabilization of the zirconia component on the insert. G) Application of the oxygen
barrier agent for initiation of setting. H) 2-piece zirconia restoration assembly after complete
setting of the adhesive cement. I) Attachment of the restoration to the implant fixture with the
definitive screw (RC, Basal)
24
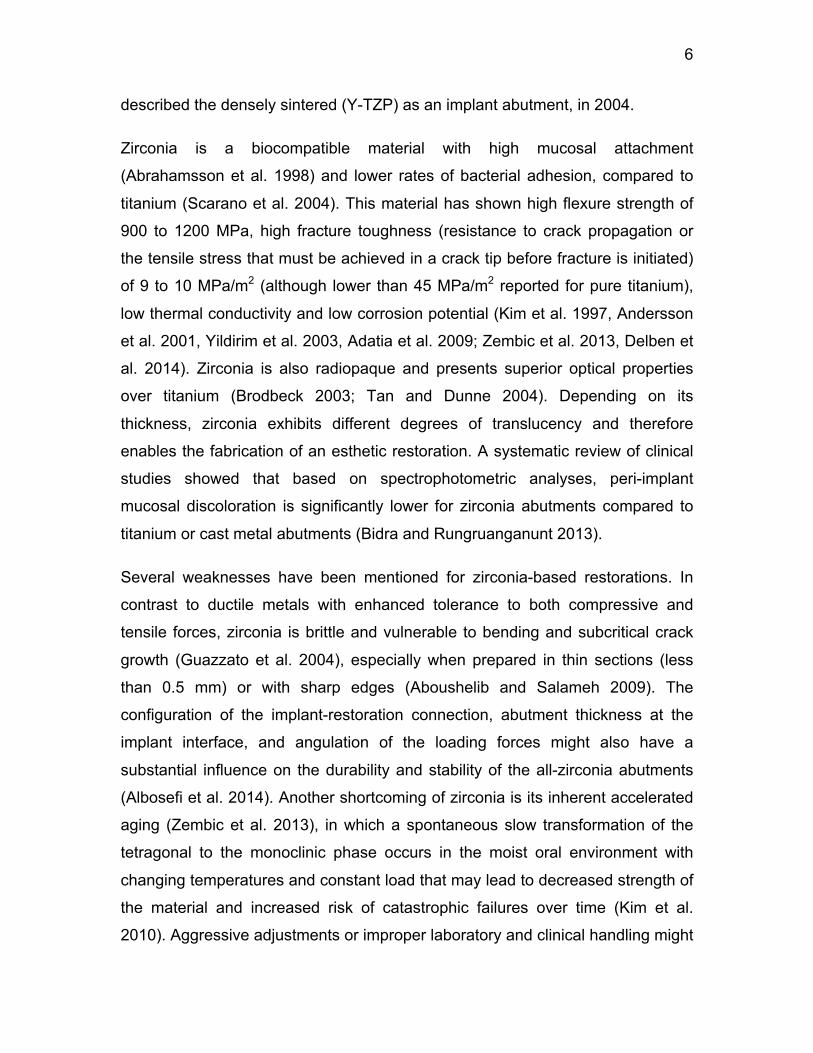
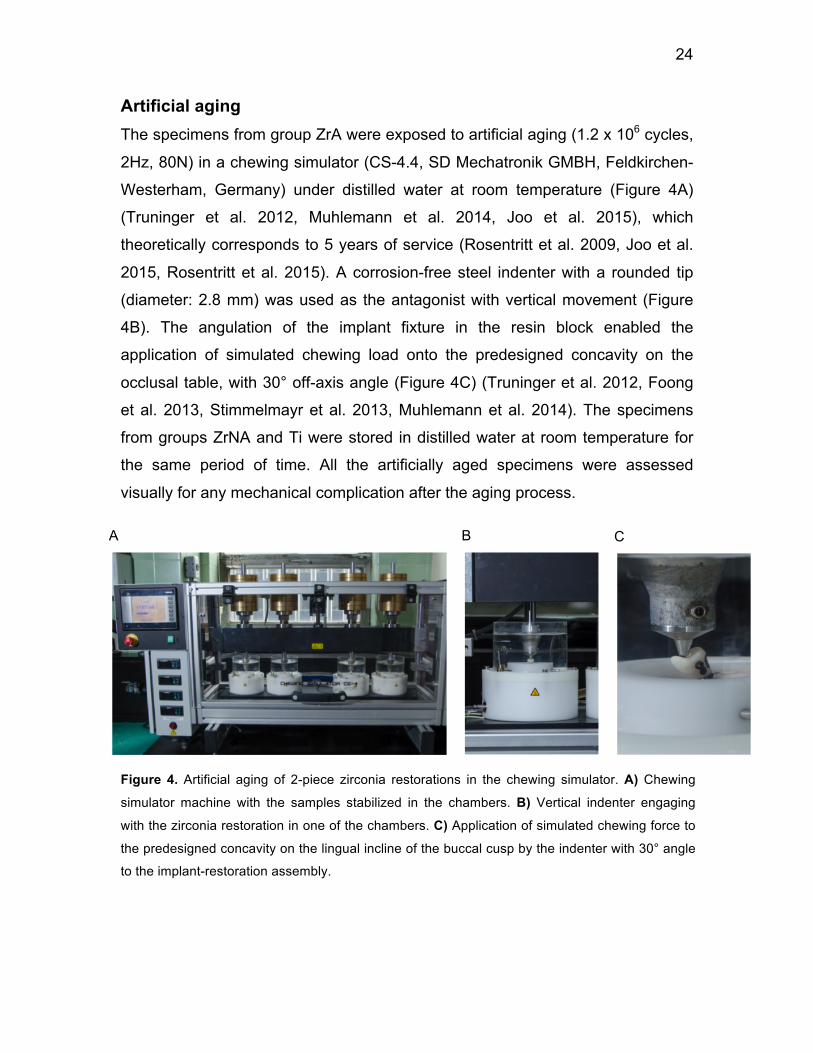
Artificial aging The specimens from group ZrA were exposed to artificial aging (1.2 x 106 cycles,
2Hz, 80N) in a chewing simulator (CS-4.4, SD Mechatronik GMBH, Feldkirchen-
Westerham, Germany) under distilled water at room temperature (Figure 4A)
(Truninger et al. 2012, Muhlemann et al. 2014, Joo et al. 2015), which
theoretically corresponds to 5 years of service (Rosentritt et al. 2009, Joo et al.
2015, Rosentritt et al. 2015). A corrosion-free steel indenter with a rounded tip
(diameter: 2.8 mm) was used as the antagonist with vertical movement (Figure
4B). The angulation of the implant fixture in the resin block enabled the
application of simulated chewing load onto the predesigned concavity on the
occlusal table, with 30° off-axis angle (Figure 4C) (Truninger et al. 2012, Foong
et al. 2013, Stimmelmayr et al. 2013, Muhlemann et al. 2014). The specimens
from groups ZrNA and Ti were stored in distilled water at room temperature for
the same period of time. All the artificially aged specimens were assessed
visually for any mechanical complication after the aging process.
A
B
C
Figure 4. Artificial aging of 2-piece zirconia restorations in the chewing simulator. A) Chewing
simulator machine with the samples stabilized in the chambers. B) Vertical indenter engaging
with the zirconia restoration in one of the chambers. C) Application of simulated chewing force to
the predesigned concavity on the lingual incline of the buccal cusp by the indenter with 30° angle
to the implant-restoration assembly.
25
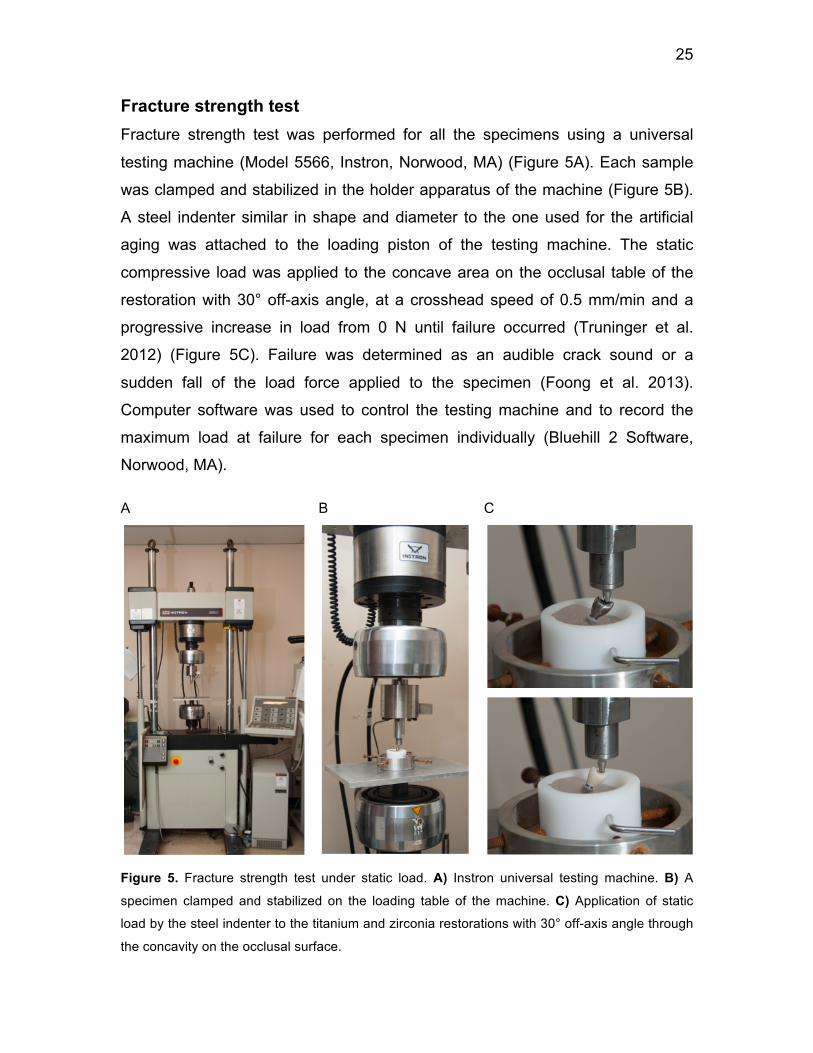
Fracture strength test Fracture strength test was performed for all the specimens using a universal
testing machine (Model 5566, Instron, Norwood, MA) (Figure 5A). Each sample
was clamped and stabilized in the holder apparatus of the machine (Figure 5B).
A steel indenter similar in shape and diameter to the one used for the artificial
aging was attached to the loading piston of the testing machine. The static
compressive load was applied to the concave area on the occlusal table of the
restoration with 30° off-axis angle, at a crosshead speed of 0.5 mm/min and a
progressive increase in load from 0 N until failure occurred (Truninger et al.
2012) (Figure 5C). Failure was determined as an audible crack sound or a
sudden fall of the load force applied to the specimen (Foong et al. 2013).
Computer software was used to control the testing machine and to record the
maximum load at failure for each specimen individually (Bluehill 2 Software,
Norwood, MA).
A
B
C
Figure 5. Fracture strength test under static load. A) Instron universal testing machine. B) A
specimen clamped and stabilized on the loading table of the machine. C) Application of static
load by the steel indenter to the titanium and zirconia restorations with 30° off-axis angle through
the concavity on the occlusal surface.
26
Visual evaluation of the specimens After aging and fracture load testing, all of the specimens were checked for
presence of mobility and visually analyzed to determine the mode of failure.
Failed specimens were examined under light microscope with 20x magnification.
Digital images of the fractured surfaces were recorded.
Scanning Electron Microscopy assessment One sample was randomly selected from each zirconia restoration test group
(groups ZrA and ZrNA), and then observed with Scanning Electron Microscopy
(SEM) for closer evaluation of the fractured surface and characteristics of the
failure mode (Foong et al. 2013, Kim et al. 2013, Muhlemann et al. 2014).
Representative specimens were cleaned with acetone in ultrasonic device for 15
minutes and then mounted on aluminum blocks with double sided carbon tape
and sputtered with gold in an argon gas environment (Polaran Range Sputter
Coater SC7620; Quorum Technologies Ltd, East Sussex, England) prior to
examination with SEM (JEOL JSM-6610LV, JEOL Ltd, Tokyo, Japan) with
secondary electron imaging. Digital images of these specimens were obtained at
various magnifications.
Statistical analysis Statistical Software (SPSS Version 21.0, SPSS Inc. Chicago, IL) was used for
statistical assessment. Descriptive statistics including means, standard
deviations, minimum and maximum values with 95% confidence interval were
reported for each group. The homogeneity of variance among groups was
checked by Levene’s test. The statistical significance of differences between
fracture load of artificially aged and non-aged 2-piece zirconia groups was
verified by independent-samples t-test. Under the equal variance assumption,
one-way analysis of variance (ANOVA) and Tukey HSD post-hoc tests were
performed to analyze the differences of fracture loads among all the test groups.
The significance of differences in the modes of failure between the aged and
non-aged zirconia restorations (groups ZrA and ZrNA) was assessed by Chi-
Square test. The level of statistical significance (P) was set at 5%.
27
Chapter 5. Results
Outcome of chewing simulation None of the tested specimens exhibited any visible morphological change or
mechanical complication after the 1,200,000 artificial chewing cycles with 80 N
force in the chewing simulator. All the restorations were found to be intact and
stable to their supporting fixtures in the acrylic resin block.
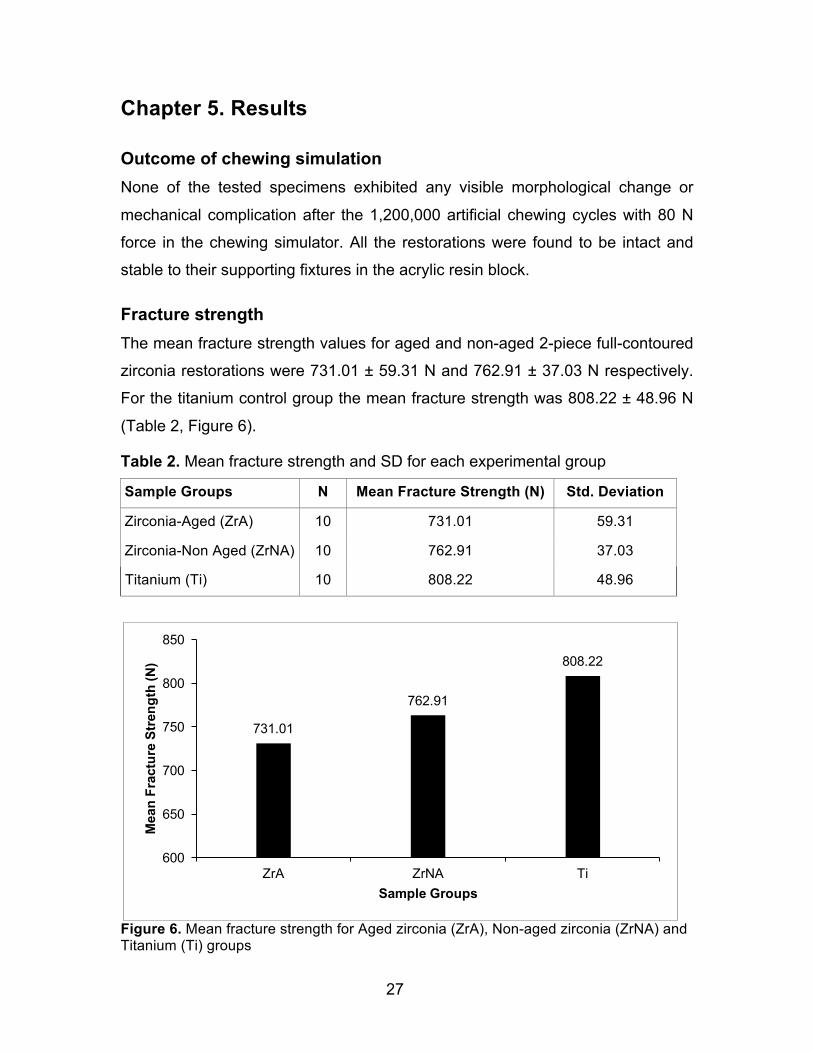
Fracture strength The mean fracture strength values for aged and non-aged 2-piece full-contoured
zirconia restorations were 731.01 ± 59.31 N and 762.91 ± 37.03 N respectively.
For the titanium control group the mean fracture strength was 808.22 ± 48.96 N
(Table 2, Figure 6).
Table 2. Mean fracture strength and SD for each experimental group
Sample Groups N Mean Fracture Strength (N) Std. Deviation
Zirconia-Aged (ZrA) 10 731.01 59.31
Zirconia-Non Aged (ZrNA) 10 762.91 37.03
Titanium (Ti) 10 808.22 48.96
Figure 6. Mean fracture strength for Aged zirconia (ZrA), Non-aged zirconia (ZrNA) and Titanium (Ti) groups
731.01
762.91
808.22
600
650
700
750
800
850
ZrA ZrNA Ti
Mea
n Fr
actu
re S
treng
th (N
)
Sample Groups
28
Independent-samples t-test did not identify any significant effect of artificial aging
on fracture strength of 2-piece zirconia restorations at a significance level of 5%.
Under the assumption of equal variance among groups, confirmed by Levene’s
test, one-way analysis of variance (ANOVA) detected significant differences in
fracture strength among the test groups (p=0.006) (Table 3). Tukey HSD post
hoc test indicated that the fracture strength values only differed significantly
between 1-piece titanium restorations and aged 2-piece zirconia restorations
(p=0.04) (Table 4). This test also confirmed the earlier observation that the
difference in fracture strength between aged and non-aged zirconia groups was
not statistically significant.
Table 3. One-way ANOVA exhibiting significant differences in fracture strength among test groups Sum of Squares df Mean Square F Sig. Between Groups 30108.91 2 15054.45 6.20 .006 Within Groups 65573.23 27 2428.64
Total 95682.13 29
Table 4. Tukey HSD post-hoc test. Mean values for groups in homogenous subsets are displayed
Sample Groups N Subset for alpha = 0.05 1 2
Zirconia-Aged (ZrA) 10 731.01
Zirconia-Non Aged (ZrNA) 10 762.91 762.91 Titanium 10 808.22 Sig. .332 .118
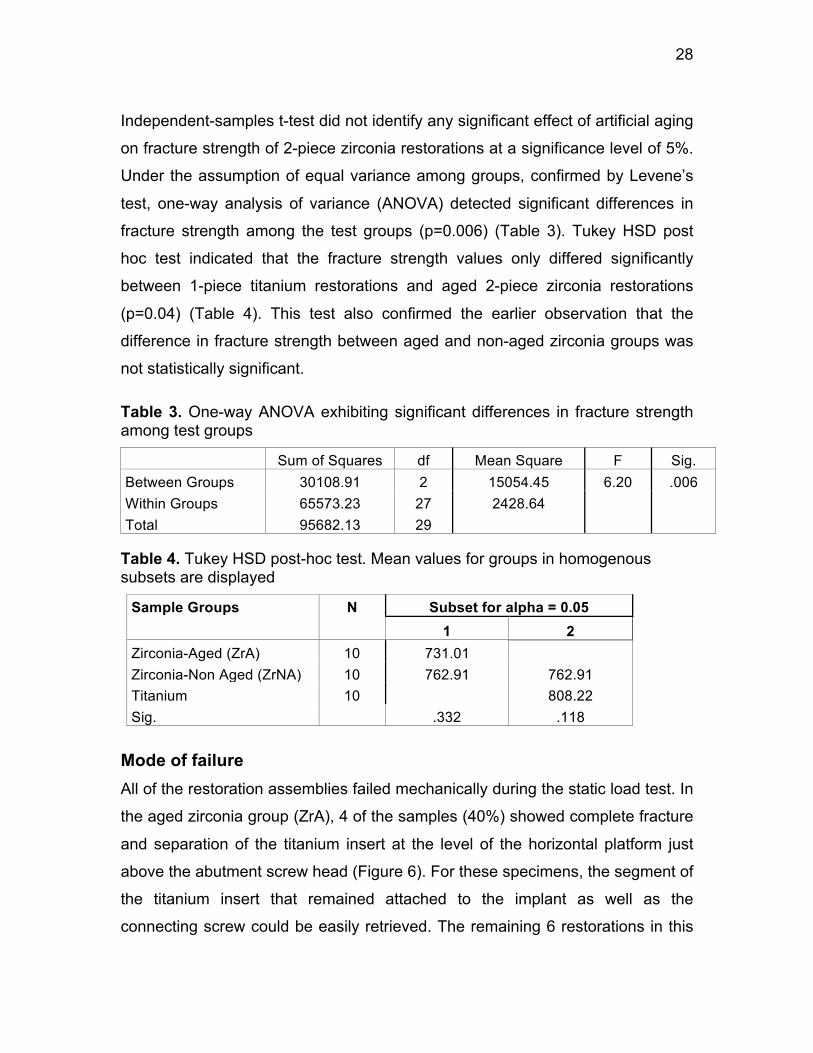
Mode of failure All of the restoration assemblies failed mechanically during the static load test. In
the aged zirconia group (ZrA), 4 of the samples (40%) showed complete fracture
and separation of the titanium insert at the level of the horizontal platform just
above the abutment screw head (Figure 6). For these specimens, the segment of
the titanium insert that remained attached to the implant as well as the
connecting screw could be easily retrieved. The remaining 6 restorations in this
29
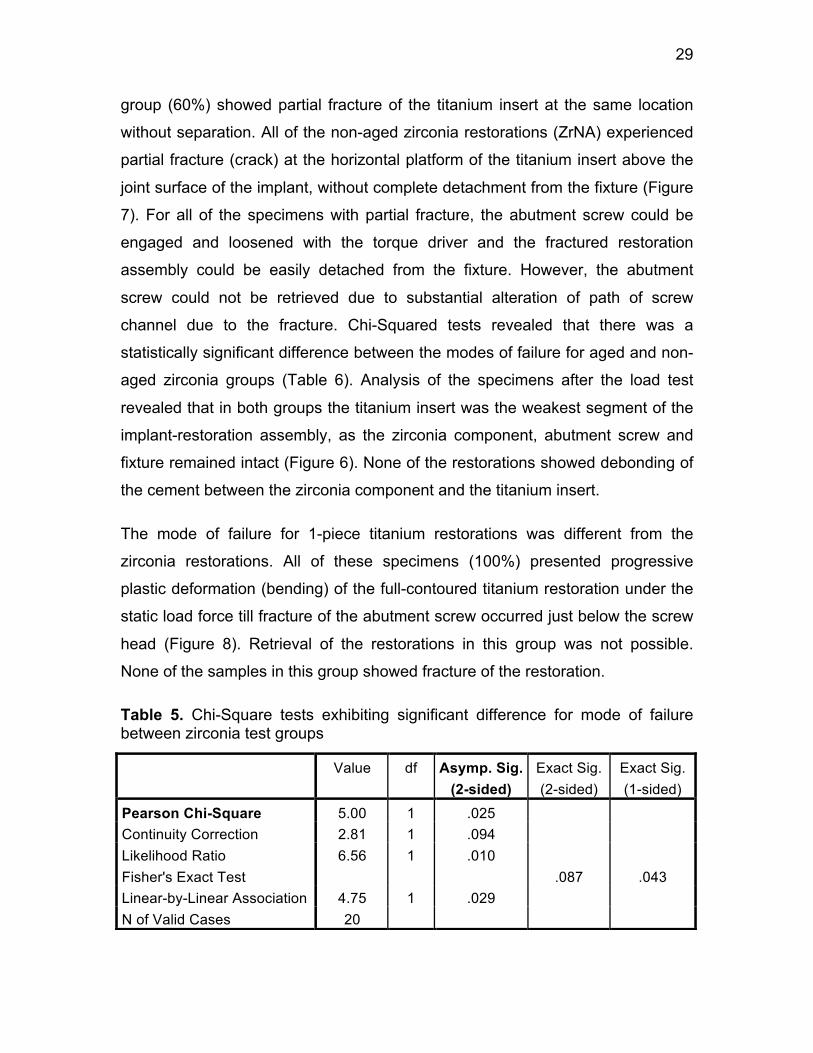
group (60%) showed partial fracture of the titanium insert at the same location
without separation. All of the non-aged zirconia restorations (ZrNA) experienced
partial fracture (crack) at the horizontal platform of the titanium insert above the
joint surface of the implant, without complete detachment from the fixture (Figure
7). For all of the specimens with partial fracture, the abutment screw could be
engaged and loosened with the torque driver and the fractured restoration
assembly could be easily detached from the fixture. However, the abutment
screw could not be retrieved due to substantial alteration of path of screw
channel due to the fracture. Chi-Squared tests revealed that there was a
statistically significant difference between the modes of failure for aged and non-
aged zirconia groups (Table 6). Analysis of the specimens after the load test
revealed that in both groups the titanium insert was the weakest segment of the
implant-restoration assembly, as the zirconia component, abutment screw and
fixture remained intact (Figure 6). None of the restorations showed debonding of
the cement between the zirconia component and the titanium insert.
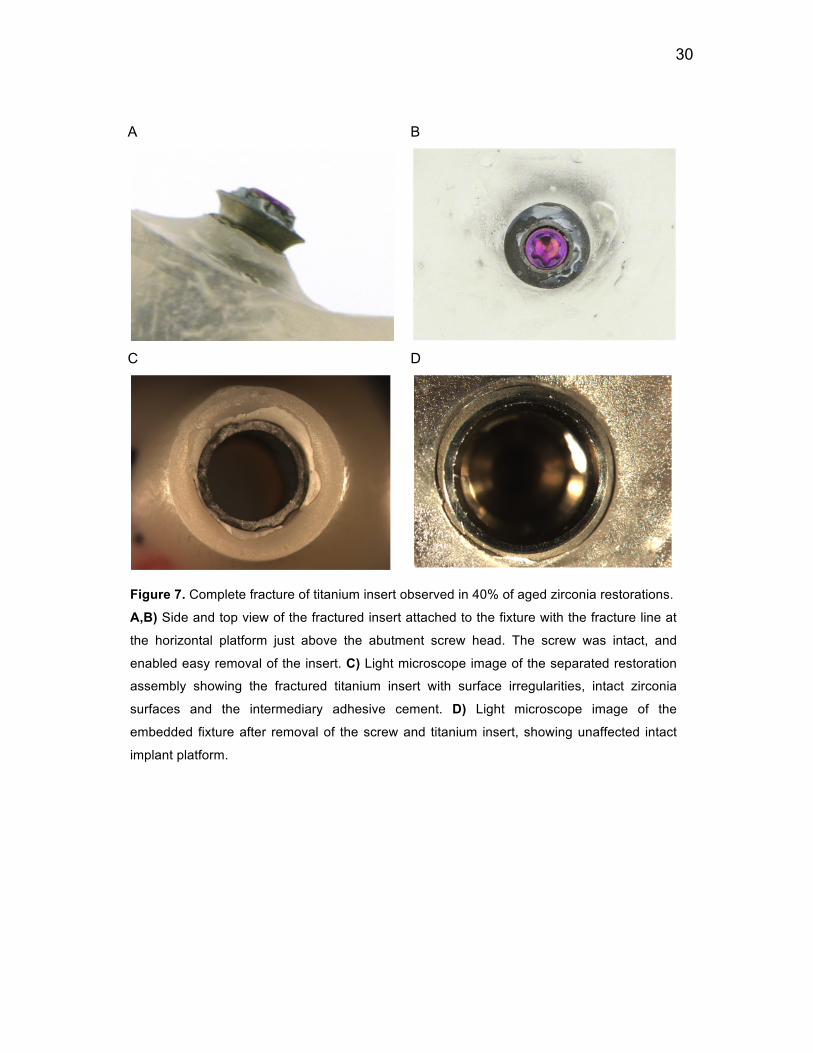
The mode of failure for 1-piece titanium restorations was different from the
zirconia restorations. All of these specimens (100%) presented progressive
plastic deformation (bending) of the full-contoured titanium restoration under the
static load force till fracture of the abutment screw occurred just below the screw
head (Figure 8). Retrieval of the restorations in this group was not possible.
None of the samples in this group showed fracture of the restoration.
Table 5. Chi-Square tests exhibiting significant difference for mode of failure between zirconia test groups
Value df Asymp. Sig. (2-sided)
Exact Sig. (2-sided)
Exact Sig. (1-sided)
Pearson Chi-Square 5.00 1 .025
Continuity Correction 2.81 1 .094
Likelihood Ratio 6.56 1 .010
Fisher's Exact Test .087 .043 Linear-by-Linear Association 4.75 1 .029
N of Valid Cases 20
30
A
B
C
D
Figure 7. Complete fracture of titanium insert observed in 40% of aged zirconia restorations.
A,B) Side and top view of the fractured insert attached to the fixture with the fracture line at
the horizontal platform just above the abutment screw head. The screw was intact, and
enabled easy removal of the insert. C) Light microscope image of the separated restoration
assembly showing the fractured titanium insert with surface irregularities, intact zirconia
surfaces and the intermediary adhesive cement. D) Light microscope image of the
embedded fixture after removal of the screw and titanium insert, showing unaffected intact
implant platform.
31
A
B
Figure 8. Partial fracture of titanium insert in 60% of aged and 100% of the non-aged zirconia
restorations. A) Partial fracture of the insert. The restoration still attached to the implant with
significant change in orientation. The restoration assembly could be completely disconnected
from the implant by loosening of the abutment screw. B) Same restoration assembly viewed by
Scanning Electron Microscopy shows the fractured secondary insert with intact zirconia
component.
A
B
Figure 9. One-piece titanium restoration after fracture strength test. A) Side view showing plastic
deformation of the restoration. B) Top view showing the fractured abutment screw head
32
Chapter 6. Discussion
In the present in vitro study, the fracture strength of implant-supported screw-
retained CAD/CAM customized full-contoured 2-piece zirconia and 1-piece
titanium restorations for replacement of a single missing maxillary first premolar
tooth was investigated. The effect of artificial aging by means of chewing
simulation on fracture strength of zirconia restorations was also assessed.
Previous in vitro studies generally focused on the performance of implant
abutments with or without cemented restorations for simulated missing maxillary
incisor teeth. There is no research in the literature investigating the performance
of full-contoured restorations for premolar teeth. Only one study simulated a
mandibular premolar replacement to evaluate the fracture strength of 1-piece
zirconia and titanium abutments but not full-contoured restorations (Apicella et al.
2011). The maxillary first premolar was selected for the experiments of the
present study, as there is a growing demand for esthetic implant restorations in
posterior regions, where high functional occlusal forces would require
restorations with reliable mechanical performance.
Materials and testing conditions in the present study were chosen in a manner to
simulate clinical conditions as best as possible. This applies to implant selection,
embedding of fixture in the holding material, design and fabrication of the
prostheses and also the artificial aging protocol. Bone-level implants with internal
conical octagon connection were utilized to support the restorations. This type of
implant is regularly placed in esthetically critical areas of the mouth, enabling
proper control of the dimensions, contour and emergence profile of the
corresponding restoration. The diameter of the selected implant (RC, 4.1mm)
was also in accordance with the surgical and prosthodontic treatment protocols
for replacement of a missing premolar under normal clinical conditions, based on
the dimensions of the tooth and local anatomical considerations. Some studies
tested the abutments that were supported by implant analogs (Aramouni et al.
2008, Adatia et al. 2009, Kim et al. 2013, Albosefi et al. 2014). Most analogs are
33
made of stainless steel and are used solely to replicate the dimensions and
configurations of the restorative platform of the corresponding endosseous
titanium implant inside the master cast without having the same mechanical
performance (Foong et al. 2013). Therefore, use of implant replicas instead of
titanium fixtures may affect the behavior of the implant restoration assembly
during the mechanical tests and fail to relate the laboratory tests to clinical
conditions.
The selected implant fixtures for the current investigation were embedded in
chemically cured PMMA resin. According to the manufacturer claim and previous
studies, the resin has a modulus of elasticity of approximately 12 GPa, which is
relatively close to that of human cancellous bone (Att et al. 2006, Delben et al.
2014). The acrylic resin holder was at the level of the implant shoulder, in
accordance with previous studies (Yildirim et al. 2003, Apicella et al. 2011,
Foong et al. 2013, Joo et al. 2015, Rosentritt et al. 2015), imitating absence of
clinical peri-implant horizontal bone loss. The angle of the fixture in the acrylic
resin enabled vertical chewing and fracture loads to be applied with 30° angle
relative to the long axis of the implant-restoration assembly, simulating a clinical
situation where the implant is angulated relative to the restoration axis or an
exaggerated scenario of parafunctional lateral movements, in accordance with
several previous studies (Truninger et al. 2012, Dittmer et al. 2012, Foong et al.
2013, Albosefi et al. 2014, Delben et al. 2014, Chun et al. 2015).
Full-contoured zirconia restorations without veneering porcelain layer were
tested in the present study. Developments in materials and manufacturing
technologies have lead to fabrication of strong monolithic zirconia restorations
with significantly improved esthetic properties for application in less esthetically
critical areas of the mouth. In conjunction with the CAD/CAM process, staining is
performed to achieve the desired shade of the milled zirconia restoration in its
green or soft state, prior to the sintering stage. Elimination of the veneering
porcelain layer can prevent a number of mechanical complications related to
these restorations such as cohesive failure within the veneering porcelain and
34
adhesive failure at abutment-veneer interface (Ekfeldt et al. 2011), which are
mostly related to the restoration geometry, mechanical limitations of the layering
porcelain and weak bonds between the veneering layer and underlying zirconia
structure (Delben et al. 2014). Moreover, in the absence of this layer a thicker
and mechanically stronger monolithic restoration can be fabricated in areas
where limited amount of restorative space is available.
The titanium specimens were also designed and fabricated as full-contoured with
no veneering porcelain. Although this type of restoration is rarely applied in a
clinical setting, it was decided to utilize it in the present study in order to maintain
homogeneity with the machined zirconia samples with regards to dimension and
contour, area of loading force application and length of the lever arm and to
eliminate the human factor related to the sintering process. Another reason was
to exclude any possible effect of the layering porcelain on the performance of the
titanium restoration under loading force.
All the components used in the present study were machine made using highly
advanced designing and milling technologies, and fabricated by the same
manufacturer in an effort to control the possible undesirable deficiencies caused
by human error and misfit of components from different manufacturing sources.
The present study showed that under the same non-aged conditions, implant-
supported screw-retained CAD/CAM customized full-contoured 2-piece zirconia
and 1-piece titanium restorations did not present a significant difference in
fracture strength; therefore there is not enough evidence available to reject the
first null hypothesis. However, the fracture strength of the artificially aged 2-piece
zirconia replacements was significantly lower than that of the 1-piece titanium
restorations.
Several methods have been introduced for assessing the resistance of implant-
restoration assemblies to fracture among which, fatigue testing is considered as
the most reliable method (Canullo et al. 2013). Although the fracture strength test
under compressive static load performed in the present investigation may not be
35
the best simulation of in vivo conditions, it offers the possibility to evaluate and
compare the mechanical performance of the restorations, as well as identifying
the modes of failure and weaker segments of the assembly (Dittmer et al. 2012).
This test may also model situations where an individual occludes into a hard
object or receives trauma (Kim et al. 2013). Several other studies have followed
a similar loading protocol (Sailer et al. 2009a, Dittmer et al. 2011, Dittmer et al.
2012, Kim et al. 2013, Stimmelmayr et al. 2013, Albosefi et al. 2014) but
relatively few have compared the fracture strength of titanium and 2-piece
zirconia abutments. Among these, an in vitro study exhibited significantly higher
fracture strength for titanium abutments compared to 1- and 2-piece zirconia
abutments under no artificial aging (Chun et al. 2015), while others observed the
same difference between titanium and various types of zirconia abutments
following artificial aging by thermocycling and chewing simulation (Truninger et
al. 2012, Muhlemann et al. 2014).
The mean fracture load for the sample groups in the present study ranged
between 731 N and 808 N. The physiologic occlusal forces at maximum
intercuspation range between 31 N and 145 N in the first premolar region,
depending on the length of the dental arch and the occlusal scheme (Hattori et
al. 2003). Higher occlusal forces are expected in individuals with parafunctional
habits such as clenching and bruxism. Clinical studies have recorded load peaks
of up to 255 N for first premolar teeth during maximal clenching (Ferrario et al.
2004) and 440 N during unilateral parafunctional movements (de Zee et al. 2007)
in healthy male young adults. Fracture load values for all groups in the present
study exceeded the normal occlusal forces. Moreover, the application of forces
to the specimens with 30° off-axis angle represents exaggerated lateral forces
that might be observed during parafunctional movements. Based on our findings,
it may be speculated that the implant-restoration assemblies evaluated in this
study would have a satisfactory performance under physiologic chewing forces in
a clinical scenario. However, due to the inevitable limitations of in vitro studies,
any clinical interpretation should be expressed with caution.
36
Identifying the failure mode is important for predictability of the treatment
outcome and retrievability of the components in case a mechanical failure
occurs. In the present investigation, the type of failure for full-contoured aged
zirconia restorations was complete fracture with separation of the titanium insert
(40%) or partial fracture without separation (60%), whereas 100% of the non-
aged zirconia restorations experienced partial fracture of the insert, with the
fracture line located on the axial wall just above the titanium screw head for all
the specimens. In both groups, the zirconia component, the implant platform and
the clamping screw remained intact. For specimens with complete fracture, it
was possible to detach the titanium insert from the implant and retrieve the
screw. The partially fractured assemblies could be disengaged from their
corresponding implants but recovery of the screw was not possible due to
substantial change in the path of the screw access. Some of the previous
investigations have reported similar failure modes (Sailer et al. 2009a,
Muhlemann et al. 2014), while other modes of failure for internally connected 2-
piece zirconia abutments with or without the overlying cemented restoration have
been observed in different studies. These failures include fracture of the titanium
insert at the implant-abutment joint (Joo et al. 2015), fracture of the screw
(Stimmelmayr et al. 2013, Rosentritt et al. 2015), separation of the zirconia
component from the titanium insert (Kim et al. 2013, Rosentritt et al. 2015),
fracture of zirconia component and adhesive failure between zirconia and
titanium insert by itself (Att et al. 2006, Sailer et al. 2009a, Truninger et al. 2012,
Canullo et al. 2013, Kim et al. 2013, Delben et al. 2014) or in conjunction with
screw fracture (Chun et al. 2015, Rosentritt et al. 2015) or plastic deformation of
the metallic components of the assembly (insert, screw and implant) (Sailer et al.
2009a, Truninger et al. 2012, Kim et al. 2013, Muhlemann et al. 2014).
Partial or complete fracture of the titanium insert under load without damage to
the fixture, the zirconia component and the screw might be due to the long and
thin wall of the insert in the tested implant-restoration system and the relatively
long lever arm. The stress that is generated from the compressive load reaches
the fracture strength of the titanium insert before affecting the implant-insert
37
interface or the zirconia component. Increasing the thickness of the walls of the
titanium insert may increase the resistance against fracturing loads. However,
thickening of the insert wall may result in thinness of the zirconia component due
to the limited available space between the implant platform and the surrounding
soft tissues and the subsequent possible risk of fracture of this component.
Moreover, the cross sectional square shape of the abutment screw head and the
intimate contact between the head of the preloaded screw and the wall of the
titanium insert may create areas of high stress concentration at the interface with
the insert, causing fracture right above the head, as observed in the present
study. Beveling of the angles of the screw head in order to relieve the areas of
stress concentration may increase the resistance of the assembly to the
unfavorable fracture loads.
An interesting finding of the present study was the preserved integrity of the
zirconia component after the mechanical failure of the assembly, which was
observed visually and confirmed by Scanning Electron Microscopy (SEM). This
phenomenon may be due to the enhanced mechanical properties of the tested
yttrium-stabilized polycrystalline zirconia component, including flexure strength
and fracture toughness (Vagkopoulou et al. 2009), exceeding the ones for the
titanium insert, under static fracture load conditions in the present study. These
properties may also be crucial for the satisfactory performance and survival of
these components under chewing simulation conditions.
Clinically, the mode of failure for the 2-piece zirconia restorations in the present
study may act as a protective mechanism for the implant fixture and the
anchoring screw, since the fracture of the insert will occur first, away from the
implant-restoration joint and above the screw head. Moreover, with this type of
failure all the components can be easily detached from the implant fixture. The
zirconia component can be separated from the titanium insert following the
disintegration of the adhesive resin cement by application of heat in a dental
porcelain furnace at temperatures ranging between 306° and 363°C, based on
the type of cement (Linkevicius et al. 2012) for approximately 5 minutes
38
(Saponaro et al. 2015). The temperature and duration of heat application
required for debonding of the cement is below the values critical for structural
stability and mechanical properties of zirconia (Swab 1991). Following the
retrieval process, the failed restoration can be easily replaced by bonding the
retrieved zirconia component to a new prefabricated titanium insert, anchored to
the fixture with a new abutment screw. Therefore the entire process of retrieval
and replacement of the failed restorations can be completed in a relatively short
period of time and at a low cost.
In the present study the failure mode for full-contoured 1-piece titanium
restorations was progressive deformation of the restoration and fracture of the
screw at the head as well as deformation of the implant platform. This finding
was in accordance with other investigations that evaluated titanium abutments
supported by the same (Dittmer et al. 2011, Truninger et al. 2012, Muhlemann et
al. 2014) or other implant systems (Apicella et al. 2011, Foong et al. 2013, Chun
et al. 2015). The screw is generally regarded as the most vulnerable component
in the implant-restoration assembly due to its structural and dimensional
limitations as well as high stress concentration at the head (Sailer et al. 2009b).
It may be hard to manage a mechanical failure of a titanium restoration similar to
the one observed in the present study in a clinical setting, as the retrieval of the
restoration and fractured screw would be very complicated. Furthermore,
deformation of the implant platform may result in non-restorability and the
inevitable need for removal of the osseointegrated fixture. According to the
findings of the present study it may be claimed that from a clinical standpoint the
mode of failure of implant-supported single 2-piece zirconia restorations is more
favorable than single 1-piece titanium restorations based on ease of retrievability
of the failed restoration, the time and the cost involved in replacement and also
preservation of the endosseous implant. However, plastic deformation of metal
components to the extreme level observed for the titanium restorations in the
present investigation may be a very rare clinical incidence. Even slight degrees
of deformation would affect the occlusal and proximal relationship of the
39
restoration with the neighboring teeth, resulting in altered patient perception and
the need to seek prosthodontic care. Moreover, higher fracture strength recorded
for titanium restorations may result in a lower rate of this type of failures that
would require removal or replacement of the restorations.
This study showed that artificial aging by means of chewing simulation
(1,200,000 cycles, 80 N) had no significant effect on fracture strength of implant-
supported customized full-contoured 2-piece zirconia restorations. Thus, not
enough evidence was available to reject the second null hypothesis. However,
this aging process significantly influenced the mode of failure of zirconia
restorations under static compressive fracturing loads.
Artificial aging of the specimens with a predetermined number of cycles and
force value is performed in laboratory studies to assess 2 major effects; one is
the direct effect of simulated chewing function on the mechanical performance
and stability of different components in the implant-restoration assembly and also
the adhesive bond between zirconia component and titanium insert; the other
one is the indirect effect caused by degradation and phase transformation of the
zirconia component in an aqueous environment under constant masticatory
loads. Several factors may influence the mechanical performance of the
restoration assembly after aging by chewing simulation such as the number of
chewing cycles and the frequency, amount and angulation of the force, the
features of the aging environment as well as the characteristics of zirconia
including the forming constituents and their percentage, and manufacturer
specific processing technique. The number of chewing cycles for this study was
determined based on previous investigations (Truninger et al. 2012, Muhlemann
et al. 2014, Joo et al. 2015), which is theoretically claimed to be equal to 5 years
of clinical service (Rosentritt et al. 2009, Joo et al. 2015, Rosentritt et al. 2015).
The chewing load force of 80 N was set, based on the average physiologic
forces recorded for the first premolars during physiologic masticatory functions
(Hattori et al. 2003). Several investigations have tested the fracture load of
different types of implant-supported restorations after exposing all of the test

40
samples to various aging protocols (Truninger et al. 2012, Kim et al. 2013,
Stimmelmayr et al. 2013, Muhlemann et al. 2014, Rosentritt et al. 2015).
Conversely, very few studies have been designed to examine the effect of aging
on the fracture strength of the 2-piece zirconia restorations. An in vitro study
claimed that the fracture load of 2-piece zirconia abutments was reduced after
1,200,000 chewing cycles combined with thermocycling (temperature 5° - 55°C,
dwelling time 120S) (Joo et al. 2015). For the specific implant-restoration
assembly tested in the present investigation, the aged zirconia restorations had
slightly lower, although not significant, fracture strength than the non-aged group
and also a significantly different mode of failure (complete fracture) was
observed for the specimens in this group. Meanwhile, Scanning Electron
Microscopy (SEM) analysis of the completely fractured components from the
aged restorations did not indicate any structural phase transformation of zirconia
at the fracture margin. Thus, the slight difference in fracture strength between the
aged and non-aged zirconia groups may be attributed to the mechanical effect of
the simulated off-axis chewing forces on the preload of the abutment screw and
its clamping action rather than phase transformation in the polycrystalline
structure of the zirconia component. Preload is the tensile force that is generated
in the screw threads by torque forces applied during screw tightening, which
firmly connects and retains the restoration assembly to the fixture by friction
resistance between the screw threads and implant platform (Hebel and Gajjar
1997). Lateral forces have shown the capacity for detrimental effects on the
preload of the abutment screw, leading to its loosening, stretching or fracture
over time (Hebel and Gajjar 1997). Chewing simulation in the present study may
have had a similar effect on the clamping action of the screw, compromising the
stability of the implant-restoration joint and proper distribution of occlusal forces
through the restoration into the implant body. This process may have ultimately
resulted in the lower fracture strength as well as the more catastrophic mode of
failure, observed among the aged specimens.
Based on the results of the present in vitro study, it is possible to estimate that
the application of a more aggressive chewing simulation with higher number of
41
cycles and/or load value under fluctuating temperatures and also use of an aging
medium with more similarity to the human saliva might have a more prominent
effect on fracture strength of full-contoured zirconia restorations and therefore
result in significant differences. Moreover, including the titanium restorations in
the process of artificial aging would be helpful for evaluation of the effect of
simulated chewing function on the stability of the components and the
performance of the assembly under fracturing loads and to compare these
findings with the ones for the zirconia restorations. Therefore, the findings of the
present study indicate the importance of replicating clinical conditions for a more
meaningful estimation of the performance of different restoration assemblies.
Clear comparison of the observations of the present study with those of previous
investigations seems complicated, due to the differences in design and sample
size of in vitro studies, characteristics of the selected implant system, and
implant-restoration connection configurations as well as variations in design,
dimensions, material compositions and methods of fabrication of restorations.
Furthermore, diversities in the angulation and position of the fixture platform
relative to the resin holder may impact the results. In some investigations a
vertical distance between the implant shoulder and the holding resin has been
left exposed in an attempt to mimic different degrees of horizontal peri-implant
bone loss (Sailer et al. 2009a, Dittmer et al. 2012, Albosefi et al. 2014, Joo et al.
2015), which may affect the location of the fulcrum and stress concentration
areas, the length of the lever arm, amount of stress as well as the pattern of
force distribution through the restoration assembly and implant body. Efforts
should be made to conduct standardized in vitro studies to allow better
comparison of the findings.
The performance of 2-piece zirconia restorations that were designed for a
specific implant system and diameter for replacement of simulated single missing
maxillary first premolars was tested in the present study, therefore the findings
might not be applicable to other implant systems. Additional studies are
necessary to achieve more comprehensive results and to provide guidelines for

42
fabrication and use of full-contoured 2-piece zirconia restorations supported by
other implant systems for replacement of different teeth in the dentition.
43
Chapter 7. Conclusions and Clinical Significance
Conclusion Implant-supported screw-retained CAD/CAM customized full-contoured 2-piece
zirconia and 1-piece titanium single restorations did not present a significant
difference in fracture strength, under the same non-aging conditions.
Two-piece zirconia assemblies that were exposed to artificial aging showed
lower fracture strength than 1-piece non-aged titanium restorations.
Evidence was inadequate to reject the assumption that artificial aging has no
effect on the fracture strength of full-contoured 2-piece zirconia restorations.
Artificial aging impacted the mode of failure of full-contoured 2-piece zirconia
restorations.
Clinical Significance The specific implant-supported screw-retained CAD/CAM customized 2-piece
zirconia restorations tested in the present investigation demonstrated high
reliability during artificial aging and withstood loads that were higher than the
average functional load forces reported for the premolar region. In addition, they
showed a relatively favorable mode of failure with regards to retrievability and
replacement of the mechanically failed restoration and preservation of the
structural integrity of the supporting implant. Therefore, these restorations may
be considered as mechanically and esthetically suitable options for implant-
based replacement of single missing maxillary first premolar teeth in patients
with high esthetic demands. However, the effect of long-term exposure to the
potentially detrimental intra oral conditions such as persistent functional loads,
fluctuating temperatures and the aqueous environment in presence of saliva on
the mechanical performance of these restorations is still unclear.
44
Chapter 8. Future Research Directions
Further in vitro studies are recommended on the following subjects:
- To evaluate the effect of artificial aging on the mechanical performance of
implant-supported single titanium restorations in comparison with zirconia
restorations.
- To investigate the effect of more aggressive artificial aging protocols on
the structural stability and mechanical performance of implant-supported
2-piece full-contoured zirconia restorations.
- To assess the fracture strength and mode of failure of full-contoured 2-
piece zirconia restorations with various heights and thicknesses of the
secondary titanium insert.
- To examine the effect of various screw head designs and dimensions on
the technical performance of the 2-piece zirconia restoration assembly.
- To compare the mechanical performance of various commercially
available 2-piece zirconia restorations for the simulated replacement of a
similar tooth under standard artificial aging and loading protocols.
Due to the various limitations of laboratory studies, high quality clinical trials with
large sample sizes and long follow-up periods are necessary to support the
laboratory findings and to help the patients make informed clinical decisions
based on valid and reliable scientific evidence.
45
References
Abbo B, Razzoog ME, Vivas J, Sierraalta M. Resistance to dislodgement of
zirconia copings cemented onto titanium abutments of different heights. J
Prosthet Dent. 2008;99:25-29.
Aboushelib MN, Salameh Z. Zirconia implant abutment fracture: clinical case
reports and precautions for use. Int J Prosthodont. 2009;22:616-619.
Abrahamsson I, Berglundh T, Glantz PO, Lindhe J. The mucosal attachment at
different abutments. An experimental study in dogs. J Clin Periodontol.
1998;25:721-727.
Adatia ND, Bayne SC, Cooper LF, Thompson JY. Fracture resistance of yttria-
stabilized zirconia dental implant abutments. J Prosthodont. 2009;18:17-22.
Adell R, Lekholm U, Rockler B, Brånemark PI. A 15-year study of
osseointegrated implants in the treatment of the edentulous jaw. Int J Oral Surg.
1981;10:387-416.
Albosefi A, Finkelman M, Zandparsa R. An in vitro comparison of fracture load of
zirconia custom abutments with internal connection and different angulations and
thickness: part 1. J prosthodont. 2014;23:296-301.
Andersson B, Taylor A, Lang BR, Scheller H, Scharer P, Sorensen JA, Tarnow
D. Alumina ceramic implant abutments used for single-tooth replacement: a
prospective 1- to 3-year multicenter study. Int J Prosthodont. 2001;14: 432-438.
Andersson B, Glauser R, Maglione M, Taylor A. Ceramic implant abutments for
short-span FPDs: A prospective 5-year multicenter study. Int J Prosthodont.
2003;16:640-646.
Apicella D, Veltri M, Balleri P, Apicella A, Ferrari M. Influence of the abutment
46
material on fracture strength and failure modes of abutment-fixture assemblies
when loaded in a bio-faithful simulation. Clin Oral Implant Res. 2011;22:182-188.
Aramouni P, Zebouni E, Tashkandi E, Dib S, Salameh Z, Almas K. Fracture
resistance and failure location of zirconium and metallic implant abutments. J
Contemp Dent Pract. 2008;9:41-8.
Att W, Kurun S, Gerds T, Strub JR. Fracture resistance of single-tooth implant-
supported all-ceramic restorations after exposure to the artificial mouth: An in
vitro study. J Oral Rehabil. 2006;33:380-386.
Bidra AS, Rungruanganunt P. Clinical outcomes of implant abutments in the
anterior region: a systematic review. J Esthet Restor Dent. 2013;25:159-176.
van Brakel R, Noordmans HJ, Frenken J, de Roode R, de Wit GC, Cune MS.
The effect of zirconia and titanium implant abutments on light reflection of the
supporting soft tissues. Clin oral Implants Res. 2011;22:1172-1178.
Bressan E, Paniz G, Lops D, Corazza B, Romeo E, Favero G. Influence of
abutment material on the gingival color of implant supported all-ceramic
restorations: a prospective multicenter study. Clin Oral Implants Res.
2011;22:631-637.
Brodbeck U. Zi-Real Post: a new ceramic implant abutment. J Esthet Dent.
2003;15:10-24.
Buser D, Mericske-Stern R, Bernard JP, Behneke A, Behneke N, Hirt HP, et al.
Long-term evaluation of non-submerged ITI implants. Part 1: 8-year life table
analysis of a prospective multi-center study with 2359 implants. Clin Oral
Implants Res. 1997;8:161-172.
Canullo L. Clinical outcome study of customized zirconia abutments for single-
implant restorations. Int J Prosthodont. 2007;20:489-493.
Canullo L, Coelho PG, Bonifante EA. Mechanical testing of thin-walled zirconia
47
abutments. J Appl Oral Sci. 2013;21:20-24.
Chun HJ, Yeo IS, Lee JH, Kim SK, Heo SJ, Koak JY, Han JS, Lee SJ. Fracture
strength study of internally connected zirconia abutments reinforced with titanium
inserts. Int J Oral Maxillofac Implants. 2015;30:346-350.
Conrad HJ, Seong W-J, Pesun IJ. Current ceramic materials and systems with
clinical recommendations: a systematic review.J Prosthet Dent.2007;98:389-404.
Coppede AR, Bersani E, de Mattos Mda G, Rodrigues RC, Sartori IA, Ribeiro
RF. Fracture resistance of the implant-abutment connection in implants with
internal hex and internal conical connections under oblique compressive loading:
an in vitro study. Int J Prosthodont. 2009; 22: 283-286.
Delben JA, Barao VA, Ferreira MB, da Silva NR, Thompson VP, Assuncao WG.
Influence of abutment-to-fixture design on reliability and failure mode of all-
ceramic crown systems. Dent Mater. 2014;30: 408-416.
Dhingra A, Weiner S, Luke AC, Ricci JL. Analysis of dimensional changes in the
screw and surface topography at the interface of a titanium screw and a zirconia
abutment under cyclic loading: an in vitro study. Int J Oral Maxillofac Implants.
2013; 28:661-669.
Dittmer S, Dittmer MP, Kohorst P, Jendras M, Borchers L, Stiesch M. Effect of
implant-abutment connection design on load bearing capacity and failure mode
of implants. J Prosthodont. 2011;20:510-516.
Dittmer MP, Dittmer S, Borchers L, Kohorst P, Stiesch M. Influence of the
interface design on the yield force of the implant-abutment complex before and
after cyclic mechanical loading. J Prosthodont Res. 2012; 56:19-24.
Ebert A, Hedderich J. Kern M. Retention of zirconia ceramic copings bonded to
titanium abutments. Int J Oral Maxillofac Implants. 2007;22:921-927.
Ekfeldt A, Furst B, Carlsson GE. Zirconia abutments for single-tooth implant
48
restorations: a retrospective and clinical follow-up study. Clin Oral Implants Res.
2011;22:1308-1314.
Ferrario VF, Sforza C, Serrao G, Dellavia C, Tartaglia GM. Single tooth bite
forces in healthy young adults. J Oral Rehabil. 2004;31:18-22.
Foong JKW, Judge RB, Palamara JE, Swain MV. Fracture resistance of titanium
and zirconia abutments: an in vitro study. J Prosthet Dent. 2013;109:304-312.
Garine WN, Funkenbusch PD, Ercoli C, Wodenscheck J, Murphy WC.
Measurement of the rotational misfit and implant-abutment gap of all-ceramic
abutments. Int J Oral Maxillofac Implants. 2007;22:928-938.
Glauser R, Sailer I, Wohlwend A, et al. Experimental zirconia abutments for
implant-supported single-tooth restorations in esthetically demanding regions: 4-
year results of a prospective clinical study. Int J Prosthodont. 2004;17:285-90.
Guazzato M, Albakry M, Ringer SP, Swain MV. Strength, fracture toughness and
microstructure of all-ceramic materials. Part II. Zirconia-based dental ceramics.
Dent Mater. 2004;20:449-456.
Hattori Y, Satoh C, Seki S, Watanbe Y, Ogino Y, Watanabe M. Occlusal and
TMJ loads in subjects with experimentally shortened dental arches. J Dent Res.
2003;82:532-536.
Hebel KS, Gajjar RC. Cement-retained versus screw-retained implant
restorations: achieving optimal occlusion and esthetics in implant dentistry. J
Prosthet Dent. 1997;77:28-35.
Henriksson K, Jemt T. Evaluation of custom-made procera ceramic abutments
for single-implant tooth replacement: a prospective 1-year follow-up study. Int J
Prosthodont. 2003;16:626-630.
Jemt T. Modified single and short span restorations supported by
osseointegrated fixtures in the partially edentulous jaw. J Prosthet Dent.
49
1986;55:243-246.
Joo HS, Yang HS, Park SW, Kim HS, Yun KD, Ji MK, Lim HP. Influence of
preparation depths on the fracture load of customized zirconia abutments with
titanium insert. J Adv Prosthodont. 2015;7:183-190.
Jung RE, Holderegger C, Sailer I, Khraisat A, Suter A, Hammerle CH. The effect
of all-ceramic and porcelain-fused-to-metal restorations on marginal peri-implant
soft tissue color: a randomized controlled clinical trial. Int J Periodontics
Restorative Dent. 2008;28: 357-365.
Jung RE, Zembic A, Pjetursson BE, Zwahlen M, Thomas DS. Systematic review
of the survival rate and incidence of biological, technical, and aesthetic
complications of single crowns on implants reported in longitudinal studies with a
mean follow-up of 5 years. Clin Oral Implants Res. 2012; 23(Suppl.6):2-21.
Kim KH, Choi MY, Kishi T. Fracture analysis of cast pure Ti and Ti-6Al-4V alloy
for dental use. Biomed mater Eng. 1997;7:271-6
Kim JW, Covel NS, Guess PC, Rekow ED, Zhang Y. Concerns of hydrothermal
degradation in CAD/CAM zirconia. J Dent Res. 2010;89:91-95.
Kim JS, Raigrodski AJ, Flinn BD, Rubenstein JE, Chung KH, Mancl LA. In vitro
assessment of three types of zirconia implant abutments under static load. J
Prosthet Dent. 2013;109:255-263.
Lewis S, Beumer J 3rd, Hornburg W, Moy P. The “UCLA” abutment. Int J Oral
Maxillofac Implants. 1988;3:183-189.
Lindhe J, Berglundh T. The interface between the mucosa and the implant.
Periodontol 2000. 1998;17:47-54.
Linkevicius T, Apse P, Grybauskas S, Puisys A. Influence of thin mucosal tissues
on crestal bone stability around implants with platform switching: a 1-year pilot
study. J Oral Maxillofac Surg. 2010;68:2272-2277.
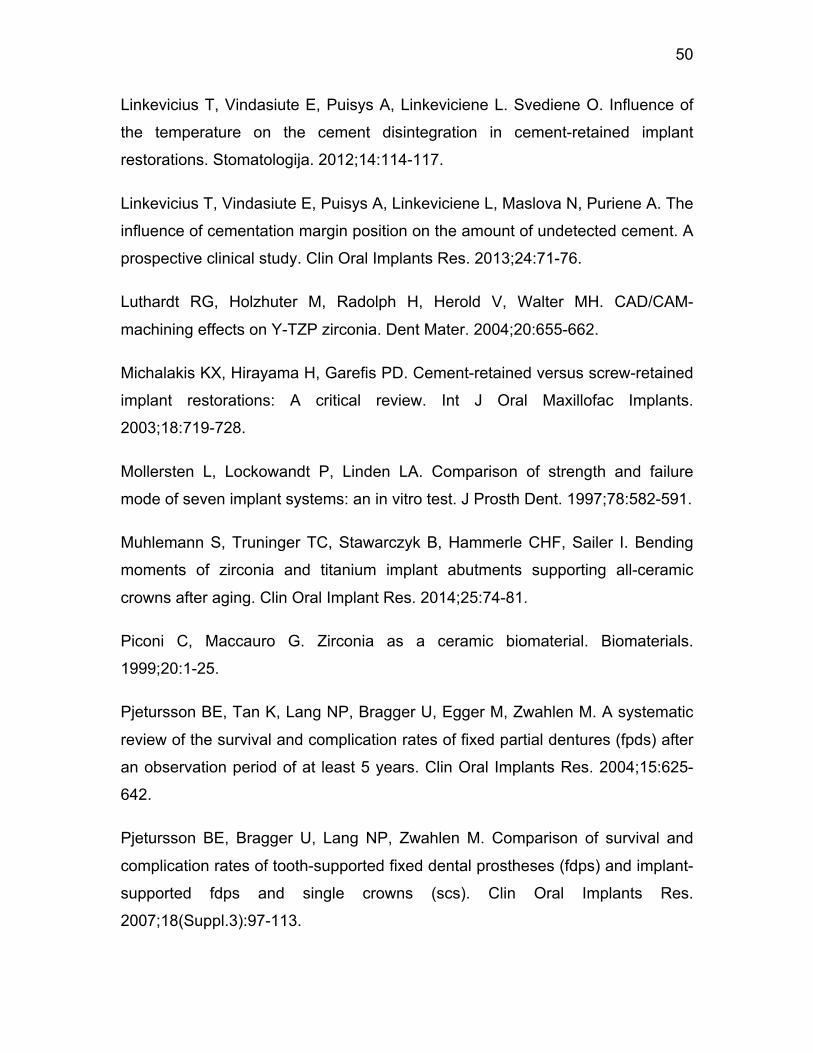
50
Linkevicius T, Vindasiute E, Puisys A, Linkeviciene L. Svediene O. Influence of
the temperature on the cement disintegration in cement-retained implant
restorations. Stomatologija. 2012;14:114-117.
Linkevicius T, Vindasiute E, Puisys A, Linkeviciene L, Maslova N, Puriene A. The
influence of cementation margin position on the amount of undetected cement. A
prospective clinical study. Clin Oral Implants Res. 2013;24:71-76.
Luthardt RG, Holzhuter M, Radolph H, Herold V, Walter MH. CAD/CAM-
machining effects on Y-TZP zirconia. Dent Mater. 2004;20:655-662.
Michalakis KX, Hirayama H, Garefis PD. Cement-retained versus screw-retained
implant restorations: A critical review. Int J Oral Maxillofac Implants.
2003;18:719-728.
Mollersten L, Lockowandt P, Linden LA. Comparison of strength and failure
mode of seven implant systems: an in vitro test. J Prosth Dent. 1997;78:582-591.
Muhlemann S, Truninger TC, Stawarczyk B, Hammerle CHF, Sailer I. Bending
moments of zirconia and titanium implant abutments supporting all-ceramic
crowns after aging. Clin Oral Implant Res. 2014;25:74-81.
Piconi C, Maccauro G. Zirconia as a ceramic biomaterial. Biomaterials.
1999;20:1-25.
Pjetursson BE, Tan K, Lang NP, Bragger U, Egger M, Zwahlen M. A systematic
review of the survival and complication rates of fixed partial dentures (fpds) after
an observation period of at least 5 years. Clin Oral Implants Res. 2004;15:625-
642.
Pjetursson BE, Bragger U, Lang NP, Zwahlen M. Comparison of survival and
complication rates of tooth-supported fixed dental prostheses (fdps) and implant-
supported fdps and single crowns (scs). Clin Oral Implants Res.
2007;18(Suppl.3):97-113.

51
Pjetursson BE, Zwahlen M, Lang NP. Quality of clinical studies to assess and
compare performance of implant supported restorations. J Clin Periodontol.
2012;39(Suppl.12):139-159.
Prestipino V, Ingber A. Esthetic high strength implant abutments. Part I. J Esthet
Dent. 1993;5:29-36.
Rosentritt M, Behr M, Van der Zel JM, Feilzer AJ. Approach for valuating the
influence of laboratory simulation. Dent Mater. 2009;20:4-31.
Rosentritt M, Rembs A, Behr M, Hahnel S, Preis V. In vitro performance of
implant-supported monolithic zirconia crowns: Influence of patient-specific tooth-
coloured abutments with titanium adhesive bases. J Dent. 2015;43:839-845.
Sailer I, Pjetursson BE, Zwahlen M, Hammerle CH. A systematic review of the
survival and complication rates of all-ceramic and metal ceramic reconstructions
after an observation period of at least 3 years. Part II: fixed dental prostheses.
Clin Oral Implants Res. 2007a;18 (Suppl.3):86-96.
Sailer I, Zembic A, Jung RE, Hammerle CH, Mattiola A. Single-tooth implant
reconstructions: esthetic factors influencing the decision between titanium and
zirconia abutments in anterior regions. Eur J Esthet Dent. 2007b;2:296-310.
Sailer I, Sailer T, Stawarczyk B, Jung RE, Hammerle CHF. In vitro study of
influence of the type of connection on the fracture load of zirconia abutments
with internal and external implant-abutment connections. Int J Oral Maxillofac
Implants. 2009a;24:850-858.
Sailer I, Philipp A, Zembic A, Pjetursson BE, Hammerle CH, Zwahlen M. A
systematic review of the performance of ceramic and metal implant abutments
supporting fixed implant reconstructions. Clin Oral Implants Res.
2009b;20(Suppl. 4):4-31.
Sailer I, Muhlemann S, Zwahlen M, Hammerle CH, Schneider D. Cemented and
screw-retained implant reconstructions: A systematic review of the survival and

52
complication rates. Clin Oral Implants Res. 2012;23(Suppl. 6):163-201.
Saponaro PC, Heshmati RH, Lee DJ. Using a porcelain furnace to debond
cement-retained implant crown from the abutment after screw fracture: a clinical
report. J Prosthodont. 2015;24:239-242.
Scarano A, Piattelli M, Caputi S, Favero GA, Piattelli A. Bacterial adhesion on
commercially pure titanium and zirconium oxide disks: An in vivo human study. J
Periodont. 2004;75:292-296.
Stimmelmayr M, Edelhoff D, Guth JF. Wear at the titanium-titanium and the
titanium-zirconia implant-abutment interface: a comparative in vitro study. Dent
Mater. 2012;28:1215-1220.
Stimmelmayr M, Sagerer S, Erdelt K, Beuer F. In vitro fatigue and fracture
strength testing of one-piece zirconia implant abutments and zirconia implant
abutments connected to titanium cores. Int J Oral Maxillofac Implants.
2013;28:488-493.
Swab JJ. Low temperature degradation of Y-TZP materials. J Mater Sci.
1991;26:6706-6714.
Tan PL, Dunne JT. An esthetic comparison of a metal ceramic crown and cast
metal abutment with an all-ceramic crown and zirconia abutment: a clinical
report. J Prosthet Dent. 2004;91:215-217.
Truninger TC, Stawarczyk B, Leutert CR, Sailer TR, Hammerle CH, Sailer I.
Bending moments of zirconia and titanium abutments with internal and external
implant-abutment connections after aging and chewing simulation. Clin Oral
Implants Res. 2012;23:12-18.
Tsuge T, Higawara W. Influence of lateral oblique cyclic loading on abutment
screw loosening of internal and external hexagon implants. Dent Mater.
2009;28:373-381.
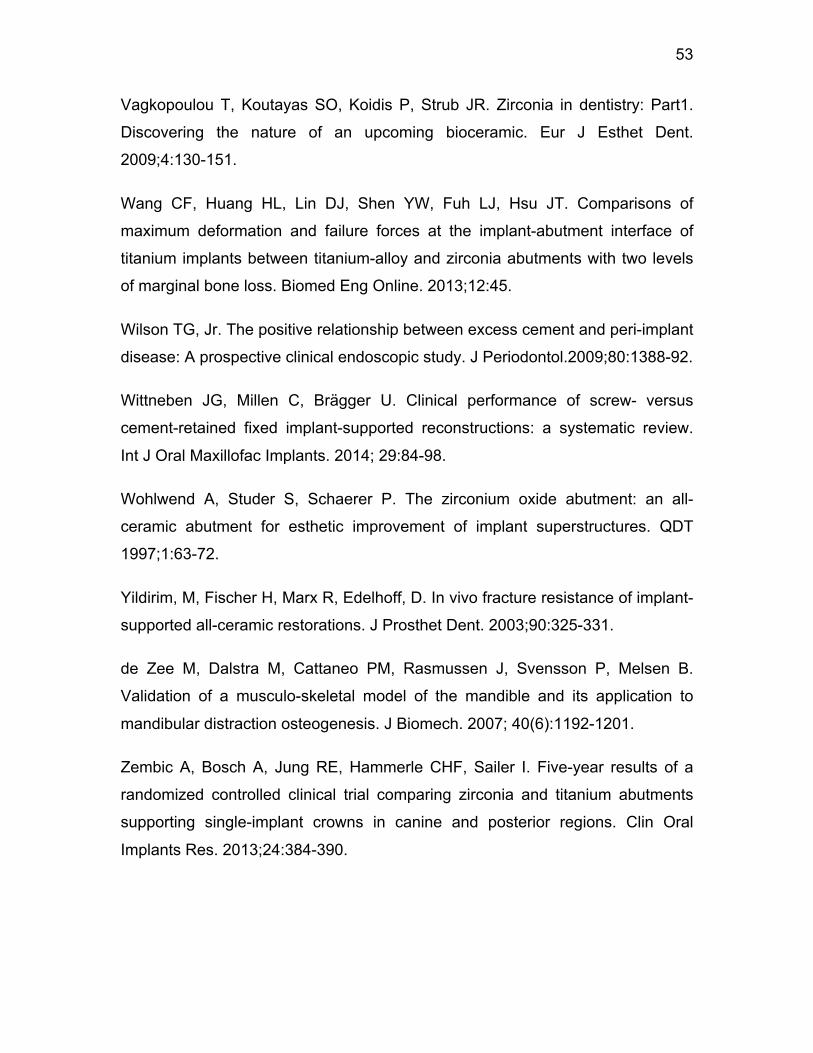
53
Vagkopoulou T, Koutayas SO, Koidis P, Strub JR. Zirconia in dentistry: Part1.
Discovering the nature of an upcoming bioceramic. Eur J Esthet Dent.
2009;4:130-151.
Wang CF, Huang HL, Lin DJ, Shen YW, Fuh LJ, Hsu JT. Comparisons of
maximum deformation and failure forces at the implant-abutment interface of
titanium implants between titanium-alloy and zirconia abutments with two levels
of marginal bone loss. Biomed Eng Online. 2013;12:45.
Wilson TG, Jr. The positive relationship between excess cement and peri-implant
disease: A prospective clinical endoscopic study. J Periodontol.2009;80:1388-92.
Wittneben JG, Millen C, Brägger U. Clinical performance of screw- versus
cement-retained fixed implant-supported reconstructions: a systematic review.
Int J Oral Maxillofac Implants. 2014; 29:84-98.
Wohlwend A, Studer S, Schaerer P. The zirconium oxide abutment: an all-
ceramic abutment for esthetic improvement of implant superstructures. QDT
1997;1:63-72.
Yildirim, M, Fischer H, Marx R, Edelhoff, D. In vivo fracture resistance of implant-
supported all-ceramic restorations. J Prosthet Dent. 2003;90:325-331.
de Zee M, Dalstra M, Cattaneo PM, Rasmussen J, Svensson P, Melsen B.
Validation of a musculo-skeletal model of the mandible and its application to
mandibular distraction osteogenesis. J Biomech. 2007; 40(6):1192-1201.
Zembic A, Bosch A, Jung RE, Hammerle CHF, Sailer I. Five-year results of a
randomized controlled clinical trial comparing zirconia and titanium abutments
supporting single-implant crowns in canine and posterior regions. Clin Oral
Implants Res. 2013;24:384-390.
54
Appendices
Appendix A: Fracture strength values and failure mode of the specimens
Group ZrA. Implant-supported customized 2-piece aged zirconia restorations
Aged Zirconia Sample #
Fracture Force (N) Mode of Failure
Zr-A-1 658.53 Partial fracture of insert above the screw head
Zr-A-2 732.7 Complete fracture of insert above screw head
Zr-A-3 788.67 Partial fracture of insert above the screw head
Zr-A-4 725.18 Complete fracture of insert above the screw head
Zr-A-5 745.68 Complete fracture of insert above the screw head
Zr-A-6 757.73 Partial Fracture of insert above the screw head
Zr-A-7 599.77 Complete fracture of insert above the screw head
Zr-A-8 772.71 Partial fracture of insert above the screw head
Zr-A-9 785.74 Partial fracture of insert above the screw head
Zr-A-10 743.4 Partial fracture of insert above the screw head

55
Group ZrNA. Implant-supported customized 2-piece non-aged zirconia restorations
Non-Aged Zirconia Sample #
Fracture Force (N) Mode of failure
Zr-NA-1 799.09 Partial fracture of insert above the screw head
Zr-NA-2 804.71 Partial fracture of insert above the screw head
Zr-NA-3 698.86 Partial fracture of insert above the screw head
Zr-NA-4 736.31 Partial fracture of insert above the screw head
Zr-NA-5 735.99 Partial fracture of insert above the screw head
Zr-NA-6 761.07 Partial fracture of insert above the screw head
Zr-NA-7 765.62 Partial fracture of insert above the screw head
Zr-NA-8 822.29 Partial fracture of insert above the screw head
Zr-NA-9 752.27 Partial fracture of insert above the screw head
Zr-NA-10 752.92 Partial fracture of insert above the screw head
56
Group Ti. Implant-supported customized 1-piece titanium restorations
Titanium Sample # Fracture Force (N) Mode of Failure
Ti-1 768.3 Plastic deformation of restoration, Fracture of the screw head, Deformation of implant
Ti-2 829.75 Plastic deformation of restoration, Fracture of the screw head, Deformation of implant
Ti-3 780.91 Plastic deformation of restoration, Fracture of the screw head, Deformation of implant
Ti-4 807.93 Plastic deformation of restoration, Fracture of the screw head, Deformation of implant
Ti-5 768.52 Plastic deformation of restoration, Fracture of the screw head, Deformation of implant
Ti-6 825.19 Plastic deformation of restoration, Fracture of the screw head, Deformation of implant
Ti-7 740.51 Plastic deformation of restoration, Fracture of the screw head, Deformation of implant
Ti-8 790.34 Plastic deformation of restoration, Fracture of the screw head, Deformation of implant
Ti-9 892.23 Plastic deformation of restoration, Fracture of the screw head, Deformation of implant
Ti-10 878.56 Plastic deformation of restoration, Fracture of the screw head, Deformation of implant
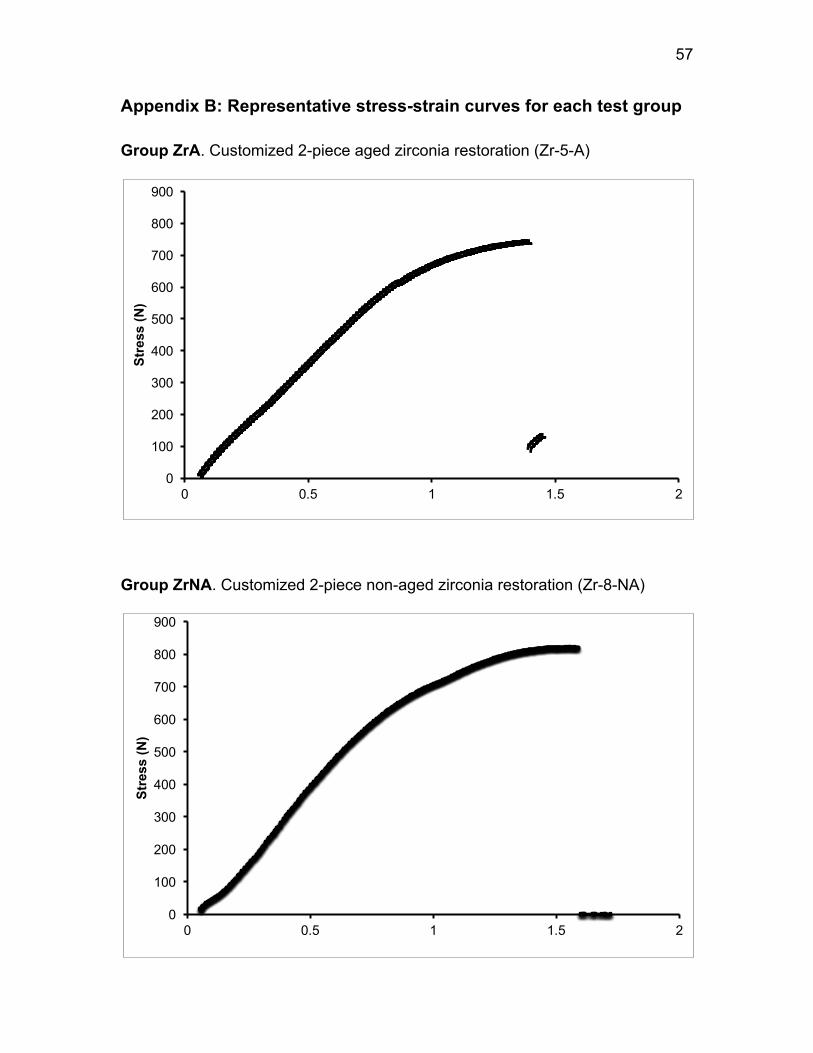
57
Appendix B: Representative stress-strain curves for each test group
Group ZrA. Customized 2-piece aged zirconia restoration (Zr-5-A)
Group ZrNA. Customized 2-piece non-aged zirconia restoration (Zr-8-NA)
0
100
200
300
400
500
600
700
800
900
0 0.5 1 1.5 2
Stre
ss (N
)
0
100
200
300
400
500
600
700
800
900
0 0.5 1 1.5 2
Stre
ss (N
)
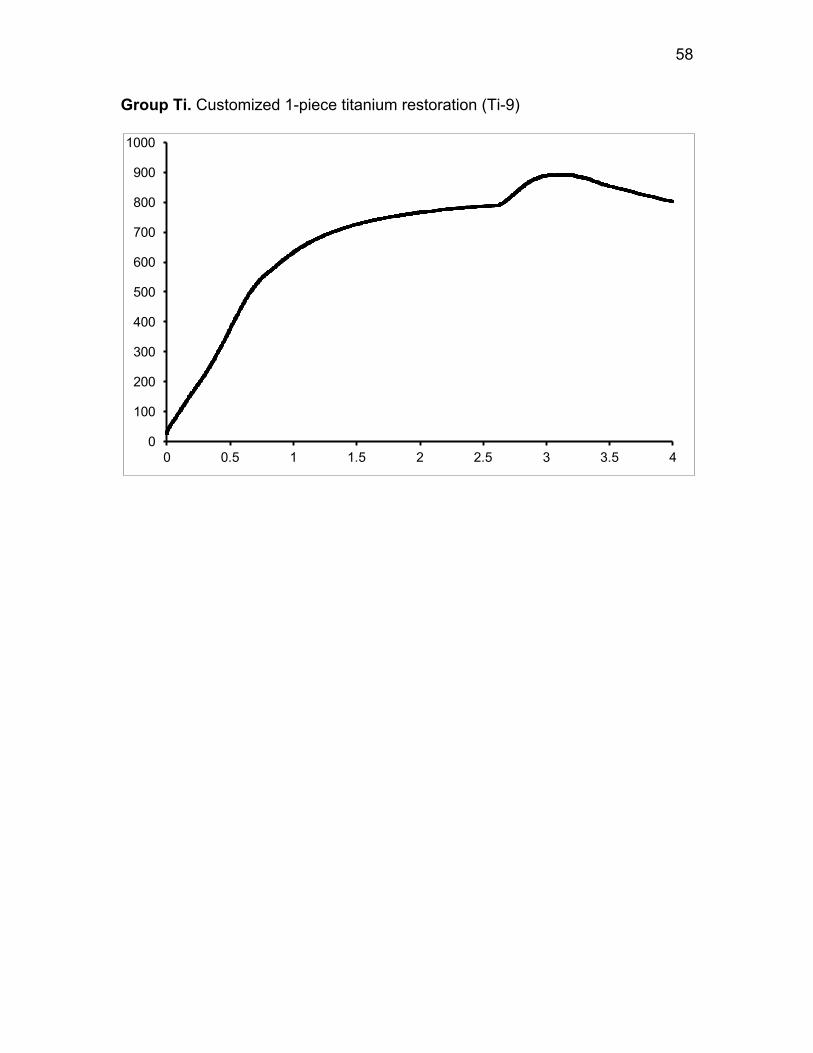
58
Group Ti. Customized 1-piece titanium restoration (Ti-9)
0
100
200
300
400
500
600
700
800
900
1000
0 0.5 1 1.5 2 2.5 3 3.5 4





![New Titanium Dioxide Nanotube Arrays for Biomedical Implant … · 2018. 6. 19. · interface) and further delamination (or fracture) between bone and implant material [ 26 , 27 ].](https://static.fdocuments.us/doc/165x107/606879eee0592a35547aa506/new-titanium-dioxide-nanotube-arrays-for-biomedical-implant-2018-6-19-interface.jpg)












