
([FOXVLYH GLVFRXQW RQ DFXSXQFWXUH QHHGOHV …
112
Acupuncture in Physiotherapy TM Journal of the Acupuncture Association of Chartered Physiotherapists Spring 2016 Volume 28, Number 1 ISSN 2058-3281 Acupuncture in Physiotherapy Volume 28, Number 1, Spring 2016
Transcript of ([FOXVLYH GLVFRXQW RQ DFXSXQFWXUH QHHGOHV …

Acupuncture in PhysiotherapyTM
Journal of the Acupuncture Associationof Chartered Physiotherapists
Spring 2016 Volume 28, Number 1
ISSN 2058-3281
Acupuncture in Physiotherapy
TMVolum
e 28, Num
ber 1, Spring 2016

© 2016 Acupuncture Association of Chartered Physiotherapists 1
Acupuncture in Physiotherapy
www.aacp.org.ukAcupuncture in Physiotherapy is printed twice a year for the membership of AACP. It aims to provide information for members that is correct at the time of going to press. Articles for inclusion should be submitted to the clinical editor at the address below or by e-mail. All articles are reviewed by the clinical editor, and while every effort is made to ensure validity, views given by contributors are not necessarily those of the Association, which thus accepts no responsibility.
Editorial addressDr Val Hopwood18 Woodlands CloseDibden PurlieuSouthampton SO45 4JGUK
E-mail: [email protected]
The AssociationThe British association for the practice of Western research-based acupuncture in physiotherapy, AACP is a professional network affiliated with the Chartered Society of Physiotherapy. It is a member-led organization, and with around 6500 subscribers, the largest professional body for acupuncture in the UK. We represent our members with lawmakers, the public, the National Health Service and private health insurers. The organization facilitates and evaluates postgraduate education. The development of professional awareness and clinical skills in acupuncture are founded on research-based evidence and the audit of clinical outcomes.
AACP LtdSefton House, Adam Court, Newark Road, Peterborough PE1 5PP, UK
Tel: 01733 390007
Printed in the UK by Henry Ling Ltd at the Dorset Press, Dorchester DT1 1HD
ContentsSpring 2016
Editorial ........................................................................3Chairman’s report .......................................................5Chief Executive Officer’s report .............................7Conference Coordinator’s report ............................9
Meta- analysisAcupuncture and other physical treatments for the relief of pain due to osteoarthritis of the knee: network meta- analysis by M. S. Corbett, S. J. C. Rice, V. Madurasinghe, R. Slack, D. A. Fayter, M. Harden, A. J. Sutton, H. MacPherson & N. F. Woollacott ....11
Clinical papersAn auricular acupuncture protocol for the attenuation of pain and anxiety in humanitarian aid environments: a consensus study to determine a theoretically safe and effective beta protocol by K. Charlesworth .......................................................25Does superficial dry needling improve hamstring muscle flexibility in normal subjects? by W. Fish ...................................................................33
Meridian masterclassesThe Heart meridian: the hand Shao Yin channel by J. Wood ....................................................................41The Bladder meridian: the foot Tai Yang channel by R. Kyte ....................................................................49
Case reportsAcupuncture for De Quervain’s disorder/tenosynovitis by N. Thompson ..................................57Acupuncture for plantar fasciitis by K. Fishlock & G. Aldridge ..................................................................67A biopsychosocial approach to chronic mid- portion Achilles tendinopathy by A. M. Davidson .....................................................77Acupuncture for pain management of osteoarthritis in the glenohumeral joint by E. L. Hellard .........................................................85Acupuncture for cancer- related hot flashes and night sweating in a 44- year- old woman with breast cancer by V. Ramasamy ............................................93
ReviewsBook reviews ........................................................... 99
News, views and interviews ................................ 103
Guidelines for authors ......................................... 105


© 2016 Acupuncture Association of Chartered Physiotherapists 3
Acupuncture in Physiotherapy
www.aacp.org.uk
Journal Committee
Clinical EditorDr Val Hopwood FCSP
Corporate EditorAndrew J. Wilson(e-mail: [email protected])
Book Review EditorWendy Rarity(e-mail: [email protected])
News EditorRosemary Lillie(e-mail: [email protected])
Marketing ManagerLisa Stephenson(e-mail: [email protected])
AACP Ltd Board Members
Chairman: Jon HobbsLesley PattendenPaul BattersbyDiana LacraruGeorge ChiaChristopher HallWendy RarityCaspar van Dongen Chief Executive Officer: Caspar van DongenAuditor: Rawlinsons, PeterboroughCompany Secretary: Michael Tolond
Editorial
Welcome to the Spring 2016 edition of Acupuncture in Physiotherapy. A few problems have delayed this issue, but I’m pleased to announce that these have all been resolved! I hope you enjoy this issue.
We are pleased to be able to reprint “Acupuncture and other physical treatments for the relief of pain due to osteoarthritis of the knee: network meta- analysis” by M. S. Corbett et al. (2013) from Osteoarthritis and Cartilage (see pp. 11–24). One of the authors of this important paper was Hugh MacPherson, and since he spoke of this work during his presen-tations at last year’s AACP Annual Conference (MacPherson 2015; Wilson 2015), we felt that this research deserved to be read in full. Please note that the continuing professional develop-ment (CPD) questions on this edition will be based on this paper. Taking an hour to answer these online is an easy and interesting way to swell your CPD portfolio!
We were also fortunate to persuade Karen Charlesworth to restructure her excellent poster, “An auricular acupuncture protocol for the attenuation of pain and anxiety in humanitar-ian aid environments: a consensus study to determine a theoretically safe and effective beta protocol”, which was first seen at the 2015 Acupuncture Research Resource Centre conference (pp. 25–32). With the increase in the number of health professionals volunteering to work in dangerous places world- wide, it is good to note that interest is being taken in ways to lighten their emotional load.
Wayne Fish has allowed us to publish his MSc research work, “Does superficial dry needling improve hamstring muscle flexibility in normal subjects?”, on the possible use of trigger points to influence muscle stretching (pp. 33–39).
Following in the excellent tradition set up by my predecessor, Helen Oakes, I have com-missioned more meridian masterclasses. We have two valuable and contrasting examples in this issue that illustrate different approaches to meridian theory. John Wood has included some of the fascinating ideas and theories held by

Editorial
© 2016 Acupuncture Association of Chartered Physiotherapists4
the Chinese to support his work on the Heart meridian (pp. 41–48). Rachel Kyte has taken a different approach to the Bladder meridian, but nonetheless, she has included a wealth of information (pp. 49–56).
As always, AACP members have provided a number of clear and helpful case studies, and this issue, these mostly deal with musculo-skeletal issues. Nora Thompson will inter-est you in “Acupuncture for De Quervain’s disorder/tenosynovitis” (pp. 57–66), and Kathryn Fishlock & Garry Aldridge stay on the extremities, describing “Acupuncture for plantar fasciitis” (pp. 67–75). Andrew Davidson offers “A biopsychosocial approach to chronic mid- portion Achilles tendinopathy” (pp. 77–84). Ellen Louise Hellard writes about “Acupuncture for pain management of osteo arthritis in the glenohumeral joint” (pp. 85–91). Finally, Visweswaran N. Ramaswamy suggests a way to use “Acupuncture for cancer- related hot flashes and night sweating in a 44- year- old woman with breast cancer” (pp. 93–98).
In addition, this edition also includes the usual reports from our officers and staff (pp. 5–9), some book reviews (pp. 99–102), and some ideas on publishing your work (pp. 103–104). However, there are no news items in this issue. If you know of any controversies or problems that would interest your colleagues, please let us know so that we can investigate.
Val HopwoodClinical Editor
ReferencesCorbett M. S., Rice S. J. C., Madurasinghe V., et al.
(2013) Acupuncture and other physical treatments for the relief of pain due to osteoarthritis of the knee: network meta- analysis. Osteoarthritis and Cartilage 21 (9), 1290–1298.
MacPherson H. (2015) Acupuncture compared to other physical therapies for osteoarthritis of the knee. [Abstract.] Acupuncture in Physiotherapy 27 (2), 107.
Wilson A. J. (2015) Acupuncture compared to other physical therapies for osteoarthritis of the knee. [Report.] Acupuncture in Physiotherapy 27 (2), 107.

© 2016 Acupuncture Association of Chartered Physiotherapists 5
Acupuncture in Physiotherapy, Volume 28, Number 1, Spring 2016, 5
Chairman’s report
The past 6 months have been another busy period for AACP, and a number of key develop-ments have taken place. One major advance has been the creation of the new full- time public relations and marketing officer role, which has been filled by Jennifer Hodges. Some of you may have met her at the Scottish Conference, where she acted as the master of ceremonies for the whole day and an acupuncture model during the practical demonstrations. Jennifer’s role is crucial to the development of AACP and the promotion of acupuncture within physiother-apy across the UK. To this end, she has taken considerable steps to promote the practice of acupuncture within physiotherapy to the wider audience of the general public. Another aspect of Jennifer’s role is to inform the public and commissioners of the key message of AACP, i.e. the integration of evidence- based acupunc-ture into physiotherapy for the benefit of the patient, which she is doing across a number of media platforms. She is also responsible for the new format of monthly e- newsletter, which will highlight media activity, training courses, inno-vations, upcoming events and member benefits as we progress through 2016.
As ever there is much to look forward to this year, including the Annual Conference on Friday 13 and Saturday 14 May 2016 in Coventry (see p. 9), and the third Scottish Conference on 1 October 2016, which, because of its success, has been expanded into a Scotland/Ireland event.
The 2016 Annual Conference boasts a truly outstanding line- up of international speakers, including Jim Chalmers and Andrew Hutton, who will be delivering workshop sessions cov-ering auricular acupuncture and acupuncture for sports injuries, respectively. Dr Jay Shah will discuss his latest work on the underlying physiological mechanisms of pain. Dr Giovanna Franconi will talk about male fertility. Also in attendance will be Team GB physiotherapist Raphael Rinaldi, who will present his work on performance enhancement through auricular acupuncture. Other notable speakers will
include: consultant in pain management Dr Jacqueline Filshie, who will discuss acupunc-ture for symptom control in cancer pain; Dr Fokke Jonkman, who will talk about the use of acupuncture in cardiovascular disease; and the always- enlightening Peter Deadman. The even-ing’s entertainment will also include an after- dinner speaker: broadcaster, naturalist, former Royal Marine, marine biologist, travel writer and leadership specialist Monty Halls, who is known internationally for his BBC Great Escape series and Great Barrier Reef, and the Discovery Channel’s Lost Worlds.
Other notable developments for 2016 will include advanced modules in a variety of acupuncture- related areas, which will cover both traditional Chinese medicine and Western medical acupuncture. These will be available in blended learning formats, allowing both practi-cal and online learning.
As AACP moves forward, it continues to build commercial relationships with a view to offering members more and more offers that represent a real- world saving for clinicians across the UK. Watch out for these in our monthly e- newsletters, and also look out for the upcoming AACP online store, which will stock key items for members at exclusive reduced prices. These savings are yet another good reason to be an AACP member.
On a personal note, I see my role as AACP chairman evolving as the year progresses, and our organization works to support chartered physiotherapists across the UK. As always, our aim is to ensure that we continue to integrate evidence- based acupuncture into physiotherapy for the benefit of the patient.
As ever, please feel free to get in touch with the AACP Office or me directly (e- mail: [email protected]), and let us know what our organi-zation can do to support its members. It just remains for me to wish you all the best with your clinical practice. I look forward to meeting up with you at Conference.
Jonathan HobbsChairman

© 2016 Acupuncture Association of Chartered Physiotherapists 7
Acupuncture in Physiotherapy, Volume 28, Number 1, Spring 2016, 7–8
Chief Executive Officer’s report
Perception and realityWith around 6500 physiotherapists in its mem-bership, AACP is shaping the future perception of acupuncture treatment in the UK.
Many misunderstandings arise because of a confusion between facts and perception in all kinds of areas and many subjects, including acupuncture. Logically, if people differentiate between facts and perception, and then align perception with the facts, they will be able to avoid or overcome such problems and mis-understandings, benefitting all involved.
What is even more important is that percep-tion is often more influential than reality in shaping opinion.
Acupuncture in the UKTake acupuncture in the UK, for example. The perception of acupuncture, both by the public and others, is still often one of an alternative way of treating patients that is far removed from conventional protocols. It is seen as a form of treatment that only works when the patient really believes in it, and one that doesn’t really have any measurable effect.
Worse, some would tell you that it’s a kind of wizardry. Such an opinion is often fuelled by the practices of acupuncturists with no other medi-cal background, who claim to be able to cure all kinds of ailments on the basis of ancient Oriental theories and beliefs.
The fact is that there is a whole host of current research and case studies, all based on Western medical principles, showing that acu-puncture is a very effective treatment for a wide range of issues. In its Evidence and Commissioning Resource (Dascanio et al. 2015), which was sent to all of its members last year, AACP lists 160 systematic reviews and other pieces of evidence from this century alone that support the use of Western medical acupuncture, as practised by the physiotherapists who are members of the organization.
Acupuncture as a part of physiotherapy is also very cost- effective. This is because, follow-ing training, little, if any, additional therapeutic time is needed during treatment, meaning that there are minimal or no additional costs involved in achieving a better outcome.
The Acupuncture Association of Chartered PhysiotherapistsTake AACP, for example. It is the oldest and largest organization representing acupuncture in the UK. Nevertheless, when members of the public, journalists or other professionals look for information on acupuncture, it is often the traditional Chinese acupuncture information that they obtain. This is because it is what they know and are familiar with, and it is based on the incorrect perception of acupuncture described above.
The fact is that, on the basis of 3 years of undergraduate physiotherapy education and more than 300 h of acupuncture training, every AACP member is ideally suited and best qualified to deliver acupuncture; their broad knowledge of physiology forms a sound basis for their acupuncture treatments. Therefore, AACP should be the first port of call not only for acupuncture treatment, but also for any acupuncture information, all of which will be based on clear, evidence- based Western medical data.
Changing perceptionThis year saw the beginning of some thorough work by AACP to create better awareness of acupuncture in physiotherapy among both the public, and health journalists and editors. In doing so, we aim to identify and promote the special and professional position that acupunc-ture physiotherapists have in the UK.
We encourage media professionals to contact AACP for further information when writing their articles, and members of the public to

Chief Executive Officer’s report
© 2016 Acupuncture Association of Chartered Physiotherapists8
look for their nearest acupuncture physio-therapist via the online search function on the AACP website.
It is time to make sure that the reality of an organization with approximately 6500 physio-therapists as members is shaping future opinions on acupuncture treatment in the UK.
If you’re looking for support in your drive for more awareness, or have suggestions about how to do this best, please don’t hesitate to
contact me directly at the AACP Office (e- mail: [email protected]).
Caspar van DongenChief Executive Officer
ReferenceDascanio V., van Dongen C., Ireland C. M. & Wilson
A. J. (2015) The Evidence and Commissioning Resource. Acupuncture Association of Chartered Physiotherapists, Peterborough.

© 2016 Acupuncture Association of Chartered Physiotherapists 9
Acupuncture in Physiotherapy, Volume 28, Number 1, Spring 2016, 9
Conference Coordinator’s report
We are pleased to announce that our 2016 Annual Conference will be held at the Hilton Hotel in Coventry (Fig. 1) on Friday 13 and Saturday 14 May 2016. The venue has ample space for car parking, as well as an on- site spa for you to use, if time allows.
Enjoy 2 days of lectures, discussions and demonstrations, with distinguished lecturers on research, developments and techniques in medical acupuncture. This year, there will be an impressive line- up of renowned speakers with an international flavour covering a number of topics.
Speakers include:• Dr Jay P. Shah;
• Dr Fokke Jonkman;
• Dr Jacqueline Filshie
• Andrew Hutton;
• Peter Deadman;
• Jim Chalmers; and
• Dr Giovanna Franconi.
The evening gala dinner on Friday 13 May 2016 will offer an opportunity to talk to speakers and delegates, as well as enjoying an inspirational speech from adventurer Monty Halls!
To book your place online, please visit the AACP website (www.aacp.org.uk). We hope to welcome you at Conference in May.
Lisa StephensonOffice Manager
Figure 1. The Hilton Coventry Hotel.


© 2013 Osteoarthritis Research Society International 11
Acupuncture in Physiotherapy, Volume 28, Number 1, Spring 2016, 11–24
META- ANALYSIS
Acupuncture and other physical treatments for the relief of pain due to osteoarthritis of the knee: network meta- analysis
M. S. Corbett University of York, York, UK
S. J. C. Rice, V. Madurasinghe,* R. Slack, D. A. Fayter & M. Harden University of York, York, UK
A. J. Sutton University of Leicester, Leicester, UK
H. MacPherson & N. F. Woollacott University of York, York, UK
AbstractObjective: To compare the effectiveness of acupuncture with other relevant physical treat-ments for alleviating pain due to knee osteoarthritis.Design: Systematic review with network meta- analysis, to allow comparison of treatments within a coherent framework. Comprehensive searches were undertaken up to January 2013 to identify randomized controlled trials in patients with osteoarthritis of the knee, which reported pain.Results: Of 156 eligible studies, 114 trials (covering 22 treatments and 9709 patients) pro-vided data suitable for analysis. Most trials studied short- term effects and many were classed as being of poor quality with high risk of bias, commonly associated with lack of blinding (which was sometimes impossible to achieve). End- of- treatment results showed that eight interventions: interferential therapy, acupuncture, transcutaneous electrical nerve stimulation, pulsed electrical stimulation, balneotherapy, aerobic exercise, sham acupuncture, and muscle- strengthening exercise produced a statistically significant reduction in pain when compared with standard care. In a sensitivity analysis of satisfactory and good- quality studies, most studies were of acupuncture (11 trials) or muscle- strengthening exercise (nine trials); both interventions were statistically significantly better than standard care, with acupuncture being statistically significantly better than muscle- strengthening exercise (standardized mean difference = 0.49; 95% credible interval = 0.00–0.98).Conclusions: As a summary of the current available research, the network meta- analysis results indicate that acupuncture can be considered as one of the more effective physical treatments for alleviating osteoarthritis knee pain in the short- term. However, much of the evidence in this area of research is of poor quality, meaning there is uncertainty about the efficacy of many physical treatments.
Keywords: knee, network meta- analysis, osteoarthritis, pain, physical treatments.
*Now at: Perinatal Institute, Birmingham, UK.

Relief of pain due to osteoarthritis of the knee
© 2013 Osteoarthritis Research Society International12
IntroductionThe objective of treating osteoarthritis of the knee is usually the alleviation of pain and improving quality of life. Failure to control pain may result in reduced mobility and reduced participation in daily activities, which may further exacerbate symptoms. The regular use of pharmacological agents for pain may be associated with significant side effects (such as gastro intestinal bleeding) (Tramèr et al. 2000), and many patients want non- pharmacological treatments for pain relief (Arthritis Care 2004; Pound et al. 2005). Effective alternatives to phar-macological pain relief are therefore desirable.
Five guidelines [American College of Rheumatology (ACR; Hochberg et al. 2012), American Academy of Orthopaedic Surgeons (AAOS 2008), Osteoarthritis Research Society International (OARSI; Zhang et al. 2008), European League Against Rheumatism (EULAR; Jordan et al. 2003), and the National Institute for Health and Clinical Excellence (NICE, now the National Institute for Health and Care Excellence; NCCCC 2008)] have evaluated treatment effects on key outcomes of knee osteoarthritis (including pain, func-tion and disability). All recommend treatment with muscle- strengthening and aerobic exercise, education, weight loss (if required), and where necessary, paracetamol and/or topical non- steroidal anti- inflammatory drugs (NSAIDs); when these are ineffective, a choice of one or more options from a range of pharmacological and non- pharmacological treatments is some-times recommended, including transcutaneous electrical nerve stimulation (TENS), thermal (heat/cooling) treatments, insoles and braces. The OARSI guideline recommended using acupuncture, AAOS found the acupuncture evidence to be inconclusive, and the ACR conditionally recommended acupuncture only for patients with moderate- to- severe pain who are unable or unwilling to undergo total knee arthroplasty. EULAR and NICE did not recom-mend use of acupuncture; one of the reasons
for the commissioning of this review – as part of a programme of projects on acupuncture and chronic pain, funded by the National Institute for Health Research (NIHR) under its Programme Grant for Applied Research Programme – was the uncertainty within the NICE decision- making process with regard to the level of evidence on acupuncture for osteo-arthritis relative to other physical treatments. The rationale for this systematic review was to compare acupuncture with available alternative physical treatments that might be prescribed by a general practitioner, or used by a physiother-apist, since uncertainty exists regarding which treatments are best.
Although numerous reviews have evaluated individual types of physical treatment, few randomized trials have directly compared these treatments. One way to overcome this limitation is to use network meta- analysis, which allows assessment of relative efficacy when direct treatment comparisons are insufficient or un available. In the context of the present review, it should enable all relevant physical treatments to be compared with each other. The purpose of this systematic review, therefore, was to con-duct a comprehensive synthesis using network meta- analysis methods in order to compare the effectiveness of acupuncture with other relevant physical treatments for alleviating pain due to osteoarthritis of the knee.
MethodsA systematic review was conducted following the general principles outlined in the Centre for Reviews and Dissemination (CRD) Guidance (CRD 2009) and the PRISMA Statement (Moher et al. 2009). This paper reports an update of a systematic review and network meta- analysis conducted in 2011, which is available on the CRD website (Corbett et al. 2012).
Literature searchA range of resources was searched for pub-lished and unpublished studies, grey literature, and ongoing research [see “eMethods 1”: http://www.oarsijournal.com/article/S1063- 4584(13)00800- 5/addons]. We searched 17
Correspondence: M. S. Corbett, Centre for Reviews and Dissemination, University of York, Heslington, York YO10 5DD, UK (e- mail: [email protected]).

M. S. Corbett et al.
© 2013 Osteoarthritis Research Society International 13
electronic databases from inception to January 2013, without language restrictions. A combina-tion of relevant free- text terms, synonyms and subject headings relating to osteoarthritis of the knee and named physical treatments were included in the strategy. Bibliographies of rel-evant reviews and guidelines were also checked, and Internet searches were made of websites relating to osteoarthritis.
Study selection and intervention definitionsTwo reviewers independently screened all abstracts and full papers, with disagreements resolved by discussion, or a third reviewer. We included randomized controlled trials (RCTs) assessing pain (as a primary or secondary out-come) in adults with knee osteoarthritis (with a population mean age of ≥ 55 years). Eligible treatments were any of the following: acupunc-ture, balneotherapy, braces, aerobic exercise, muscle- strengthening exercise, heat treatment, ice/cooling treatment, insoles, interferential therapy, laser/light therapy, manual therapy, neuromuscular electrical stimulation (NMES), pulsed electrical stimulation (PES), pulsed electromagnetic fields (PEMFs), static magnets, Tai Chi, TENS and weight loss. The following were excluded: predominantly home- based and unsupervised exercise interventions, surgical interventions, pharmaceutical interventions, interventions which combined two or more physical treatments, and studies comparing only different regimens/durations/modalities of the same intervention. Populations with varus/val-gus malalignment were excluded, as were studies which did not report data in a format suitable for network meta- analysis (see the “Outcomes and data transformations” section below).
We classified adjunctive components of the experimental interventions into five categories, based on what was reported in the trials: “treat-ment as usual”, “treatment as usual” plus speci-fied home exercise or education, “treatment as usual” plus specified (trial- specific) analgesics, no medication, and no medication plus specified home exercise or education. Eligible compara-tors included any form of standard/usual care or waiting list control (which could incorporate
analgesics, education and exercise advice), all of which we called “standard care”. Placebo interventions, no intervention and sham acu-puncture were also eligible. Sham acupuncture was treated as a separate comparator because of evidence suggesting it is more active than an inert “placebo” (Lund et al. 2009; Linde et al. 2010). All pain scales were eligible.
Assessment of trial quality and data extractionTrial quality was assessed using an adaptation of a checklist (14 questions) from a previous review by CRD (Rodgers et al. 2008). Using an algorithm, studies were then graded as excel-lent, good, satisfactory or poor, and also given an assessment based on the Cochrane risk of bias tool (Higgins et al. 2011) [see eTables 1a and 1b: http://www.oarsijournal.com/article/S1063- 4584(13)00800- 5/addons]. Data extrac-tion and quality assessments were performed by one reviewer and independently checked by a second. Disagreements were resolved by discus-sion or a third reviewer.
Outcomes and data transformationsThe Western Ontario and McMaster Universities Arthritis Index (WOMAC) [using a visual ana-logue (VAS) or Likert scale] was the preferred pain measure. When studies did not measure WOMAC pain, another pain scale was included in the analysis with prioritization of scales made on a clinical, or prevalence, basis (further details in the 2011 report) (Corbett et al. 2012). Hedges’ g standardized mean differences (SMDs) were calculated for the meta- analyses (studies report-ing medians could not be analysed). Results for different doses/regimens of the same type of treatment within a study were pooled. In an initial analysis, only final values were used. However, we included more studies by calcu-lating final values for trials reporting change from baseline data, provided trial baseline data together with variance estimates (e.g. standard deviations) were also reported. In order to present more clinically meaningful results, we present both SMDs, and SMDs converted to the WOMAC pain VAS 0–100 scale.

Relief of pain due to osteoarthritis of the knee
© 2013 Osteoarthritis Research Society International14
SynthesisA network meta- analysis draws on both direct evidence (treatments compared in the same trial) and indirect evidence (different treatments studied in separate trials, but compared when they use a common comparator), with the ben-efit of randomization in each study retained. For indirect and direct evidence to be consist-ent, population and intervention characteristics must be similar across comparisons (Lu & Ades 2004; Caldwell et al. 2005; Salanti et al. 2008; Cooper et al. 2009; Welton et al. 2009; Dias et al. 2010). Inconsistency between direct and indirect evidence was assessed using the node- splitting method (Caldwell et al. 2005; Lu & Ades 2006; Salanti et al. 2008; Cooper et al. 2009; Welton et al. 2009; Dias et al. 2010). The SMD was assumed to be normally distributed and a random effects network meta- analysis model was selected since clinical and methodological heterogeneity within treatments appeared likely (Ades et al. 2007). Analyses were conducted using WinBUGS software (Version 1.4, MRC Biostatistics Unit, Cambridge Institute of Public Health, Cambridge, UK). Further method detail can be found in “eMethods 2” [http://www.oar-sijournal.com/article/S1063- 4584(13)00800- 5/addons].
We conducted analyses with interventions categorized both with, and without, any adjunct treatments. Furthermore, in order to attempt to assess both the immediacy and durability of effects, we planned analyses for three time points: end of treatment (our primary time point), as defined in the studies; 3 months from the start of treatment (the time point closest to 3 months from the start of treatment, excluding outcomes recorded at less than 4 weeks from the start of treatment); and 3 months after the end of treatment (the time point closest to 3 months, but between 8 and 16 weeks, from end of treatment). However, due to a lack of medium- and long- term data, we report here results for the end- of- treatment time point only.
To evaluate the impact of study quality on the results, two sets of analyses were per-formed: one including all studies regardless of quality (“any quality”), and a primary sensitivity analysis including studies of satisfactory, or
better, quality (“better quality”). Studies with atypical populations, interventions or results were excluded in a second sensitivity analysis. When possible, examination of funnel plots was used to assess for publication bias.
ResultsOne hundred and fifty- six original trials (of 22 distinct interventions and comparators) met the inclusion criteria. Four of 10 foreign language papers which appeared eligible based on their English abstracts could not be translated, so had to be excluded from our analyses (Jezek et al. 1990; Jensen et al. 1997; Durmus et al. 2005; Salli et al. 2006). One retracted study was removed from all analyses (Ni et al. 2010; Schumacher 2010). Twenty- two new studies were identified from the 2013 update searches. A study selection flow diagram is presented in eFig. 1 [http://www.oarsijournal.com/article/S1063- 4584(13)00800- 5/addons].
Study characteristicsAn overview of all eligible studies – regard-less of whether they reported data suitable for network meta- analysis – is presented in Table 1. The range of mean treatment durations (and timing of end- of- treatment assessment) varied widely from just a single session (TENS) to 69.3 weeks (weight loss interventions), although a majority of interventions were administered over a 2–6- week period. Most studies were classified as having recruited a general knee osteoarthritis population, although weight loss trials (as expected) recruited only overweight or obese participants. The mean body mass indices (BMIs) of some studies recruiting a general population fell into the overweight or obese classification, although most studies did not report BMI.
Around three- quarters of the studies were classed as being of poor quality (110 of 152). The remainder were “satisfactory” (33 studies) or “good” (nine studies), together classed as “better quality”. In the network meta- analyses, only 12 trials were considered to be at low risk of bias. Most trials were hampered by a lack of adequate blinding, and small sample sizes

M. S. Corbett et al.
© 2013 Osteoarthritis Research Society International 15
Tab
le 1
. Su
mm
ary
char
acte
ristic
s of
tria
ls i
nclu
ded
in t
he s
yste
mat
ic r
evie
w:
(TE
NS)
tra
nscu
tane
ous
elec
tric
al n
erve
stim
ulat
ion;
(PE
S) p
ulse
d el
ectr
ical
stim
ulat
ion;
(N
ME
S) n
euro
mus
cula
r el
ectr
ical
stim
ulat
ion;
and
(PE
MFs
) pu
lsed
ele
ctro
mag
netic
fiel
ds
Inte
rven
tion
Num
ber
of t
rials
elig
ible
fo
r th
e re
view
(nu
mbe
r
of p
atie
nts*
)
Type
of
popu
latio
n re
crui
ted
(num
ber
of s
tudi
es)
Ran
ge o
f m
ean
ages
(ye
ars)
Ran
ge o
f pe
r ce
nt f
emal
e
Com
para
tors
(nu
mbe
r of
tre
atm
ent
arm
s†)
Acu
punc
ture
25 (
2794
)G
ener
al (
23),
both
kne
es
affe
cted
(1)
, aw
aitin
g su
rger
y (1
)58
–85
50–9
6Sh
am a
cupu
nctu
re (
15),
stan
dard
car
e (1
3), T
EN
S (3
), m
uscl
e-
stre
ngth
enin
g ex
erci
se (
1), i
ce/c
oolin
g (1
)B
alne
othe
rapy
14 (
1008
)G
ener
al (
12),
both
kne
es
affe
cted
(2)
54–7
0‡47
–100
Plac
ebo
(8),
stan
dard
car
e (6
), he
at t
reat
men
t (1
)
Bra
ces
1 (
24)
Gen
eral
(1)
59.5
63In
sole
s (1
)A
erob
ic e
x erc
ise
13 (
1136
)G
ener
al (
9), b
oth
knee
s
affe
cted
(2)
, ove
rwei
ght
or
obes
e (2
)
54–7
5‡50
–100
Stan
dard
car
e (1
3), m
uscl
e- st
reng
then
ing
exer
cise
(2)
, wei
ght
loss
(1)
Mus
cle-
stre
ngth
enin
g ex
erci
se34
(30
13)
Gen
eral
(26
), bo
th k
nees
af
fect
ed (
5), a
wai
ting
surg
ery
(2)
53–7
7‡31
–100
Stan
dard
car
e (2
2), p
lace
bo (
4), n
o tr
eatm
ent
(2),
aero
bic
exer
cise
(2
), he
at t
reat
men
t (1
), T
EN
S (1
), ac
upun
ctur
e (1
), PE
S (1
), m
anua
l th
erap
y (1
), N
ME
S (2
)
Hea
t tr
eatm
ent
7 (
412)
Gen
eral
(7)
61–7
463
–100
Plac
ebo
(4),
stan
dard
car
e (1
), T
EN
S (1
), m
uscl
e- st
reng
then
ing
exer
cise
(1)
, bal
neot
hera
py (
1), i
ce/c
oolin
g (1
)
Ice/
cool
ing
trea
tmen
t 4
(21
1)G
ener
al (
4)56
–61
48–9
1T
EN
S (2
), ac
upun
ctur
e (1
), st
anda
rd c
are
(1),
heat
tre
atm
ent
(1),
plac
ebo
(1),
no t
reat
men
t (1
)
Inso
les
6 (
893)
Gen
eral
(6)
58–6
854
–100
Plac
ebo
(5),
brac
es (
1)In
terf
eren
tial t
hera
py 5
(24
0)G
ener
al (
5)59
–67
67–8
0Pl
aceb
o (3
), T
EN
S (1
), no
tre
atm
ent
(1)
Las
er/l
ight
the
rapy
9 (
379)
Gen
eral
(6)
, bot
h kn
ees
af
fect
ed (
3)58
–74
68–9
0Pl
aceb
o (8
), st
anda
rd c
are
(1)
Man
ual t
hera
py 6
(48
6)G
ener
al (
6)56
–68
63–7
8St
anda
rd c
are
(4),
plac
ebo
(2),
mus
cle-
stre
ngth
enin
g ex
erci
se (
1)N
ME
S 3
(78
)G
ener
al (
3)60
–71
42–7
9St
anda
rd c
are
(2),
mus
cle-
stre
ngth
enin
g ex
erci
se (
2)PE
S 8
(39
2)G
ener
al (
8)55
–70
46–1
00Pl
aceb
o (7
), st
anda
rd c
are
(1),
mus
cle-
stre
ngth
enin
g ex
erci
se (
1), n
o tr
eatm
ent
(1)
PEM
Fs 6
(52
1)G
ener
al (
6)60
–69
28–8
0Pl
aceb
o (6
)St
atic
mag
nets
3 (
131)
Gen
eral
(3)
63–6
560
–79
Plac
ebo
(3)
Tai
Chi
4 (
307)
Gen
eral
(4)
65–7
075
–93
Stan
dard
car
e (4
)T
EN
S18
(80
5)G
ener
al (
17),
awai
ting
su
rger
y (1
)56
–85
48–9
7Pl
aceb
o (1
2), s
tand
ard
care
(3)
, acu
punc
ture
(3)
, ice
/coo
ling
(2),
heat
tr
eatm
ent
(1),
inte
rfer
entia
l (1)
, no
trea
tmen
t, m
uscl
e st
reng
then
ing
exer
cise
(1)
Wei
ght
loss
(di
etin
g) 5
(87
0)O
verw
eigh
t or
obe
se (
5)61
–70
26–8
9St
anda
rd c
are
(5),
aero
bic
exer
cise
(1)
*Num
ber
of p
atie
nts
anal
ysed
by
the
prim
ary
stud
ies
for
end-
of- t
reat
men
t pa
in –
thi
s w
as n
ot a
lway
s cl
early
sta
ted.
†Diff
eren
t do
ses
of t
he s
ame
trea
tmen
t in
a t
rial w
ere
pool
ed, c
ount
ing
as o
ne a
rm.
‡Tria
l re
port
ed m
ean
age
by t
reat
men
t gr
oup,
and
con
tain
ed a
gro
up w
ith a
mea
n ag
e of
≥ 5
5. S
ome
stud
ies
com
pare
d tw
o or
mor
e di
ffer
ent
inte
rven
tions
. “G
ener
al”
is u
sed
as a
bro
ad t
erm
for
stu
dies
whi
ch d
id
not
recr
uit
very
spe
cific
pop
ulat
ion
type
s.

Relief of pain due to osteoarthritis of the knee
© 2013 Osteoarthritis Research Society International16
(which limited the effectiveness of randomiza-tion, resulting in baseline imbalances). Full study quality assessment results are presented in eTables 1a and 1b [http://www.oarsijournal.com/article/S1063- 4584(13)00800- 5/addons]. Study quality did vary by intervention, making the evidence base more robust in some areas than in others (see Table 2a). No evidence was found for publication bias (only assessable for muscle- strengthening exercise). Individual study characteristics and a reference list of all studies included in the systematic review can be found in eTable 2 [http://www.oarsijournal.com/article/S1063- 4584(13)00800- 5/addons].
Network meta- analysisOverall, 114 trials (9709 patients) reported data suitable for the end- of- treatment analyses. In addition to the 22 new studies identified from the update searches, nine studies – excluded from the original review analyses – were included in this updated analysis by calculating
final values using change from baseline data. Our original analyses (based on searches up to 2010) provided no indication of a treatment effect difference related to the majority of adjunctive components of the experimental interventions [see eFig. 2: http://www.oarsijournal.com/article/S1063- 4584(13)00800- 5/addons]. The exception was that standard care incorporat-ing active analgesia was more effective than standard care with “treatment as usual” (with or without home exercise/education). However, analgesic adjuncts were used in only eight trials. Furthermore, most studies were classified as using the “treatment as usual” adjunct, where little adjunct detail was defined. We therefore focussed on comparing the interventions cat-egorized without adjuncts.
Tables 2a and 2b, and Fig. 1a and 1b (cat-erpillar plots) present the primary results, with interventions ordered by treatment effect. The network is illustrated in eFig. 3 [http://www. oarsijournal.com/article/S1063- 4584(13)00800-5/
Table 2a. Results of network meta- analyses for comparisons with standard care: trials of any quality: (WOMAC) Western Ontario and McMaster Universities Arthritis Index; and (VAS) visual analogue scale*
Intervention (abbreviations in brackets relate to Fig. 1a–d)
Number of trials (number of patients)
Standardized mean difference (95% credible interval)
Difference expressed on a WOMAC VAS 0–100 pain scale (95% credible interval)†
Standard care (comparator) – –Interferential therapy (INT) 3 (98) –1.63 (–2.39 to –0.87) –26.90 (–39.39 to –14.40)Acupuncture (ACU) 24 (1219) –0.89 (–1.18 to –0.59) –14.69 (–19.52 to –9.80)Transcutaneous electrical nerve stimulation (TENS)
12 (285) –0.65 (–1.06 to –0.25) –10.77 (–17.50 to –4.05)
Pulsed electrical stimulation (PES) 6 (180) –0.65 (–1.19 to –0.10) –10.65 (–19.59 to –1.66)Balneotherapy (BAL) 9 (275) –0.60 (–1.04 to –0.15) –9.87 (–17.15 to –2.48)Aerobic exercise (AE EX) 11 (428) –0.55 (–0.89 to –0.21) –9.02 (–14.68 to –3.51)Tai Chi (TAI) 4 (159) –0.51 (–1.03 to 0.01) –8.39 (–16.98 to 0.13)Static magnets (MAG) 2 (41) –0.50 (–1.34 to 0.33) –8.27 (–22.08 to 5.43)Sham acupuncture (SH ACU) 14 (892) –0.47 (–0.84 to –0.09) –7.76 (–13.89 to –1.52)Manual therapy (MAN) 4 (166) –0.44 (–0.96 to 0.09) –7.21 (–15.90 to 1.49)Muscle- strengthening exercise (MU EX) 28 (1254) –0.40 (–0.61 to –0.19) –6.54 (–9.99 to –3.11)Ice/cooling treatment (ICE) 3 (51) –0.35 (–1.03 to 0.33) –5.81 (–16.94 to 5.44)Heat treatment (HEA) 5 (123) –0.31 (–0.86 to 0.24) –5.14 (–14.20 to 3.98)Laser therapy (LAS) 5 (155) –0.27 (–0.86 to 0.32) –4.53 (–14.19 to 5.20)Weight loss (WEI) 5 (436) –0.26 (–0.67 to 0.15) –4.25 (–10.97 to 2.43)Pulsed electromagnetic fields (PEMFs) 5 (238) –0.15 (–0.71 to 0.42) –2.43 (–11.76 to 6.90)Placebo (PLA) 42 (1077) –0.07 (–0.42 to 0.29) –1.15 (–6.98 to 4.70)Braces (BRA) 1 (12) 0.00 (–1.39 to 1.39) 0.07 (–22.84 to 22.94)Insoles (INS) 3 (197) 0.10 (–0.65 to 0.85) 1.64 (–10.71 to 13.97)Neuromuscular electrical stimulation (NMES)
2 (28) 0.22 (–0.62 to 1.05) 3.58 (–10.26 to 17.33)
No intervention (NO INT) 5 (87) 0.44 (–0.15 to 1.04) 7.25 (–2.51 to 17.12)
*Data points: 131; residual deviance: 152; between- study standard deviation: 0.45 (95% credible interval: 0.36–0.55).†See Table 2d footnote.

M. S. Corbett et al.
© 2013 Osteoarthritis Research Society International 17
addons]. When compared with standard care, eight physical treatments had a mean effect sug-gesting benefit, namely: interferential therapy, acupuncture, TENS, PES, balneotherapy, aerobic exercise, sham acupuncture and muscle- strengthening exercise (Fig. 1a and Table 2a). When acupuncture (rather than standard care) was the comparator, acupuncture was sig-nificantly better at reducing pain than sham acu-puncture, muscle- strengthening exercise, weight loss, PEMFs, placebo, insoles, NMES and no intervention (Fig. 1b and Table 2b). Across all comparisons, inconsistency at a P- value less than 0.05 was only identified for the two com-parisons involving PES.
The primary sensitivity analysis of only better- quality studies involved 35 trials, nine types of intervention and 3499 patients. A small study of muscle- strengthening exercise versus PES was excluded as it was identified as causing inconsistency in the main analysis. The network is illustrated in Fig. 2. The reduction in the num-ber of studies per comparison, as well as loops
in the network, increased uncertainty around the true between- study variance. Some interven-tions were represented by few studies, although there were 11 acupuncture studies and nine muscle- strengthening exercise studies. There was a statistically significant reduction in pain compared with standard care for acupuncture, balneotherapy, sham acupuncture and muscle- strengthening exercise (Fig. 1c and Table 2c). Acupuncture was statistically significantly better at a 95% level of credibility than sham acupunc-ture, muscle- strengthening exercise, weight loss, aerobic exercise and no intervention when the analysis of better- quality studies was presented as a comparison with acupuncture (Fig. 1d and Table 2d). We found that acupuncture and balneotherapy were the two interventions with the highest rank, a probability statistic calculated from the treatment effect distributions (Table 3), although there is uncertainty around these rankings, as reflected in the overlapping cred-ible intervals with sham acupuncture, muscle- strengthening exercise and Tai Chi.
Table 2b. Results of network meta- analyses for comparisons with acupuncture: trials of any quality: (WOMAC) Western Ontario and McMaster Universities Arthritis Index; and (VAS) visual analogue scale*
Intervention (abbreviations in brackets relate to Fig. 1a–d)
Number of trials (number of patients)
Standardized mean difference (95% credible interval)
Difference expressed on a WOMAC VAS 0–100 pain scale (95% credible interval)†
Acupuncture (comparator) – –Interferential therapy (INT) 3 (98) –0.74 (–1.54 to 0.05) –12.21 (–25.33 to 0.84)TENS (TENS) 12 (285) 0.24 (–0.22 to 0.70) 3.92 (–3.70 to 11.50)PES (PES) 6 (180) 0.25 (–0.35 to 0.84) 4.04 (–5.78 to 13.87)Balneotherapy (BAL) 9 (275) 0.29 (–0.22 to 0.81) 4.82 (–3.60 to 13.28)Aerobic exercise (AE EX) 11 (428) 0.34 (–0.11 to 0.79) 5.67 (–1.84 to 13.00)Tai Chi (TAI) 4 (159) 0.38 (–0.22 to 0.98) 6.30 (–3.58 to 16.12)Static magnets (MAG) 2 (41) 0.39 (–0.48 to 1.25) 6.41 (–7.86 to 20.61)Sham acupuncture (SH ACU) 14 (892) 0.42 (0.15 to 0.70) 6.93 (2.50 to 11.46)Manual therapy (MAN) 4 (166) 0.45 (–0.14 to 1.05) 7.47 (–2.30 to 17.23)Muscle- strengthening exercise (MU EX) 28 (1254) 0.49 (0.15 to 0.84) 8.14 (2.41 to –13.83)Ice/cooling treatment (ICE) 3 (51) 0.54 (–0.16 to 1.25) 8.88 (–2.70 to 20.61)Heat treatment (HEA) 5 (123) 0.58 (–0.02 to 1.18) 9.55 (–0.30 to 19.44)Laser therapy (LAS) 5 (155) 0.62 (–0.02 to 1.25) 10.16 (–0.28 to 20.61)Weight loss (WEI) 5 (436) 0.63 (0.13 to 1.14) 10.44 (2.13 to 18.72)Pulsed electromagnetic fields (PEMFs) 5 (238) 0.74 (0.13 to 1.36) 12.26 (2.22 to 22.36)Placebo (PLA) 42 (1077) 0.82 (0.40 to 1.25) 13.53 (6.58 to 20.53)Standard care (SC) 53 (2308) 0.89 (0.59 to 1.18) 14.69 (9.80 to 19.52)Braces (BRA) 1 (12) 0.89 (–0.51 to 2.31) 14.76 (–8.49 to 38.01)Insoles (INS) 3 (197) 0.99 (0.21 to 1.78) 16.33 (3.41 to 29.30)Neuromuscular electrical stimulation (NMES)
2 (28) 1.11 (0.22 to 1.98) 18.27 (3.57 to 32.72)
No intervention (NO INT) 5 (87) 1.33 (0.69 to 1.97) 21.95 (11.30 to 32.52)
*Data points: 131; residual deviance: 152; between- study standard deviation: 0.45 (95% credible interval: 0.36–0.55).†See Table 2d footnote.

Relief of pain due to osteoarthritis of the knee
© 2013 Osteoarthritis Research Society International18
Several trials were excluded in a second-ary sensitivity analysis based on population or intervention differences, or on extreme data: the results were not sensitive to these changes, although the model fit improved [see eResults 1: http://www.oarsijournal.com/article/S1063- 4584(13)00800- 5/addons].
For the analysis of better- quality studies, no network link could be made with the placebo- controlled studies. We therefore conducted a separate network meta- analysis for these
studies. The results, and network, are presented in eResults 1 [http://www.oarsijournal.com/article/ S1063- 4584(13)00800- 5/addons]. Both inter- ferential therapy and heat treatment were statisti-cally significantly more effective than placebo, but laser therapy, PES and insoles were not.
DiscussionThe comprehensive network meta- analysis reported here, in which physical treatments for osteoarthritis of the knee were compared with
Figure 1. (a) Standardized mean differences (SMDs) of each treatment compared to standard care for the analysis including studies of any quality. (b) Standardized mean differences of each treatment compared to acupuncture for the analysis including studies of any quality. (c) Standardized mean differences of each treatment compared to standard care for the analysis including better- quality studies. (d) Standardized mean differences of each treatment compared to acupuncture for the analysis including better- quality studies. (For an explanation of the abbreviations, see Table 2a.)

M. S. Corbett et al.
© 2013 Osteoarthritis Research Society International 19
each other within a coherent framework, pro-vides the first estimate of the relative effect of these treatments, which is essential for decision- makers. A network meta- analysis provides a basis of synthesizing all the available evidence in a consistent framework, obviating the need to make decisions by subjective inferences from disparate data. Numerous systematic reviews, some summarized in a review of reviews (Jamtvedt et al. 2008), have evaluated the inter-ventions (or classes of interventions) included in this review. However, our analysis represents the use of the most practical methods currently
available to compare a large number of different types of treatment, i.e. enabling us to compare the physical treatments (including acupuncture) with each other.
Of the 22 interventions evaluated, eight – interferential therapy, acupuncture, TENS, PES, balneotherapy, aerobic exercise, sham acu-puncture and muscle- strengthening exercise – produced a statistically significant reduction in pain, compared with standard care. Of these, only acupuncture and muscle- strengthening exercise were represented by more than three trials in the sensitivity analysis of better- quality studies, with acupuncture (11 trials) being statistically significantly better than muscle- strengthening exercise (nine trials). Acupuncture and balneotherapy (one trial) were the interven-tions with the highest rank, although there is some uncertainty around these. For the better- quality placebo- controlled studies, interferential therapy (one trial) showed a strong effect when compared to placebo.
Like a standard meta- analysis, a network meta- analysis requires an assumption of exchange-ability between the trials. We sought to minimize concerns which might arise from within- or between- intervention heterogeneity by using an age restriction as part of our inclusion criteria, and by excluding interventions consisting of more than one physical treatment. The patient characteristics appeared broadly comparable across interventions. Some clinical heterogene-ity is inevitable in a wide- ranging study such as this, but baseline pain did not appear to vary
Figure 2. Network diagram for the end- of- treatment analysis of better- quality trials. The number of trials and patients included in the analysis are stated in Tables 2c and 2d. Each solid arrow indicates that there is a data point for that comparison entered into the analysis. The thickness reflects the number of trials. The dotted line reflects an extra comparison in a multi- arm trial. The numbers are a measure of inconsistency: 0 is no inconsistency; 1 is complete inconsistency.
Table 2c. Results of network meta- analyses for comparisons with standard care: trials of better- quality: (WOMAC) Western Ontario and McMaster Universities Arthritis Index; and (VAS) visual analogue scale*
Intervention (abbreviations in brackets relate to Fig. 1a–d)
Number of trials (number of patients)
Standardized mean difference (95% credible interval)
Difference expressed on a WOMAC VAS 0–100 pain scale (95% credible interval)†
Standard care (comparator) – –Acupuncture (ACU) 11 (878) –1.01 (–1.43 to –0.61) –16.70 (–23.61 to –10.07)Balneotherapy (BAL) 1 (40) –1.01 (–1.92 to –0.11) –16.65 (–31.73 to –1.74)Sham acupuncture (SH ACU) 8 (685) –0.68 (–1.17 to –0.19) –11.14 (–19.29 to –3.16)Muscle- strengthening exercise (MU EX) 9 (450) –0.52 (–0.84 to –0.22) –8.62 (–13.92 to –3.58)Tai Chi (TAI) 2 (51) –0.26 (–0.96 to 0.44) –4.29 (–15.87 to 7.23)Weight loss (WEI) 3 (357) –0.08 (–0.55 to 0.39) –1.34 (–9.10 to 6.41)Aerobic exercise (AE EX) 1 (80) 0.07 (–0.69 to 0.84) 1.23 (–11.30 to 13.78)No intervention (NO INT) 1 (30) 0.19 (–0.77 to 1.14) 3.11 (–12.72 to 18.77)
*Data points: 31; residual deviance: 31.4; between- study standard deviation: 0.39 (95% credible interval: 0.24–0.58).†See Table 2d footnote.

Relief of pain due to osteoarthritis of the knee
© 2013 Osteoarthritis Research Society International20
systematically between interventions, as far as it was possible to tell – given the wide varia-tion of scales used. We conducted sensitivity analyses excluding trials causing heterogeneity. Our analyses used a random effects model to incorporate heterogeneity, and we undertook an evaluation of levels of inconsistency and model fit. Despite this, it is possible there are unknown confounding factors affecting the results of indirect comparisons, although in our results heterogeneity is accounted for in the credible intervals. The majority of trials which used placebo interventions studied electrical or electromagnetic interventions; it is not unrea-sonable to assume the placebo effects were similar (since the interventions were similar). A further strength of our review is that trials
covering a diverse range of interventions were all assessed using the same quality- assessment tools; this enabled fair comparisons to be made by evaluating the reliability of the evidence base for each intervention.
However, although we conducted a sensitiv-ity analysis of the better- quality studies, this resulted in fewer trials per comparison, and fewer network loops, meaning there is greater uncertainty about the true heterogeneity and about the differences between the direct and indirect evidence. Fewer loops in relation to the size of the network means there is less data to quantify inconsistency, and so it is possible that uncertainty associated with inconsistency is not captured in the results. Further limitations are that we could not include all studies in our analyses due to the variable reporting of pain results, and the end- of- treatment data available was mostly short- term: of the trials which did investigate medium- or long- term effectiveness, only a few could provide the data required by our analyses. However, given that the treatments under consideration are not intended as being cures, and that any treatment effect is expected to attenuate over time, a comparison of their maximum effect is not without merit.
It is important that our results are evaluated in context. Methodological limitations exist which are often inherent and unavoidable in clinical trials of physical treatments. Additionally, we
Table 2d. Results of network meta- analyses for comparisons with acupuncture: trials of better- quality: (WOMAC) Western Ontario and McMaster Universities Arthritis Index; and (VAS) visual analogue scale*
Intervention (abbreviations in brackets relate to Fig. 1a–d)
Number of trials (number of patients)
Standardized mean difference (95% credible interval)
Difference expressed on a WOMAC VAS 0–100 pain scale (95% credible interval)†
Acupuncture (comparator) – –Balneotherapy (BAL) 1 (40) 0.00 (–0.99 to 1.01) 0.05 (–16.36 to 16.62)Sham acupuncture (SH ACU) 8 (685) 0.34 (0.03 to 0.66) 5.57 (0.42 to 10.86)Muscle- strengthening exercise (MU EX) 9 (450) 0.49 (0.00 to 0.98) 8.08 (0.02 to 16.21)Tai Chi (TAI) 2 (51) 0.75 (–0.05 to 1.57) 12.42 (–0.81 to 25.84)Weight loss (WEI) 3 (357) 0.93 (0.31 to 1.57) 15.36 (5.18 to 25.81)Standard care (ST CARE) 17 (928) 1.01 (0.61 to 1.43) 16.70 (10.07 to 23.61)Aerobic exercise (AE EX) 1 (80) 1.09 (0.23 to 1.96) 17.94 (3.82 to 32.27)No intervention (NO INT) 1 (30) 1.20 (0.18 to 2.23) 19.80 (2.94 to 36.81)
*Data points: 31; residual deviance: 31.4; between- study standard deviation: 0.39 (95% credible interval: 0.24–0.58).†To help evaluate these conversions, studies have reported the “minimal clinically important change” as –15 mm (on a VAS 0–100 scale, and derived from a prior Delphi exercise; Bellamy et al. 1992), and the “minimal perceptible clinical improvement” (the smallest change detectable by the patient) as –9.7 mm (on a WOMAC VAS 0–100 scale; Ehrich et al. 2000). Another study estimated the “minimal clinically important improvement” (MCII), although only for pain on movement, as being –19.9 mm on a VAS 0–100 scale; this figure varied by baseline pain score, with patients with less pain having a smaller MCII (10.8 mm) and patients with severe pain having a larger MCII (36.6 mm) (Tubach et al. 2005).
Table 3. Ranking of interventions (using only better- quality studies)
InterventionNumber of trials
Median rank
Ninety- five per cent credible interval
Acupuncture 11 2 1–3Balneotherapy 1 2 1–6Sham acupuncture 8 3 2–6Muscle- strengthening exercise
9 4 2–6
Tai Chi 2 5 2–9Weight loss 3 6 4–9Standard care 17 7 6–9Aerobic exercise 1 8 3–9No intervention 1 8 3–9

M. S. Corbett et al.
© 2013 Osteoarthritis Research Society International 21
found flaws which trialists could have avoided by using better methodology and reporting practices. Most of the studies in our review were rated as being of poor quality, and even many of the better- quality studies were prag-matic trials, where blinding of patients was not possible, i.e. most studies are likely to have been subject to some form of bias. For the trials where patients were not blinded, and treatments were compared with standard care, the overall treatment effect is likely to incorporate non- specific (placebo) effects. We assumed that such non- specific effects were similar across all inter-ventions, but variation may in fact be present.
In light of our results, consideration of what might be the true (or specific) effect of acupuncture is warranted. A Cochrane Review reported a statistically significant, clinically rel-evant, short- term improvement in pain, similar to our findings [acupuncture versus waiting list control: SMD = –0.96; 95% confidence interval (CI) = –1.19 to –0.72] (Manheimer et al. 2010). The comparison of acupuncture with sham acupuncture also showed a similar effect to ours, and was described as being clinically irrel-evant (SMD = –0.35; 95% CI = –0.55 to –0.15). However, the largest study in this Cochrane analysis, indicating no significant difference, had, for many participants, the primary pain assess-ment 7 weeks after the end of treatment, and was one of two trials which used an intensive sham needling technique, which may have had physiological effects. Also, our analysis included a recent large trial (discussed below) which used what appeared to be a very active sham. It is therefore possible that the pooled results from both reviews underestimate the short- term effect of acupuncture. It is also worth noting that the effect size of acupuncture versus sham is of the same order as that seen for NSAIDs versus pla-cebo (SMD = 0.32; 95% CI = 0.24–0.39), which has also been described as being too small to be clinically significant (Bjordal et al. 2004). An analysis of individual patient data on patients with knee osteoarthritis was recently reported for acupuncture studies (in which the allocation concealment methods had to be unambiguously adequate) (Vickers et al. 2012). These results also indicated acupuncture to be more effective than
sham acupuncture, and also found a smaller effect size than when acupuncture was com-pared with no acupuncture (usual care) controls. Non- specific effects therefore seem to play an important role in the pain- alleviating effects of acupuncture. However, for our comparisons, the lack of blinding in trials of the other interven-tions (where blinding was not possible) in our network of better- quality studies would also be likely to result in non- specific effects contribut-ing to results; it is reasonable to assume that fair comparisons between treatments have therefore been made.
Studies have presented evidence suggesting that sham acupuncture is associated with larger treatment effects than pharmacological and other physical placebos (Lund et al. 2009; Linde et al. 2010). However, one of two opposing fac-tors – inadequacy of patient blinding by using unsuitable shams, or the use of physiologically active shams – may impact on the effect of sham acupuncture in a given trial; the former may result in an overestimation of the true effect of acupuncture, while the latter may result in an underestimation. In our review, important details about sham acupuncture (e.g. depth of insertion) were sometimes poorly reported, or were not reported, so the possibility of further clinical heterogeneity remains. One study in particular had a very active sham: the depth of needle insertion was similar to depths used for (active) acupuncture in some of the other trials; different needle placement formed a large component of the sham. This large study, which found no difference in pain between acu-puncture and sham, partly explains the relatively large effect estimate seen for sham acupuncture in our analyses (when compared with standard care) (Suarez- Almazor et al. 2010).
Several quantifications of the clinical rele-vance of improvements in knee pain scores exist (see the footnote to Table 2d). In this context, our results (derived from the better- quality trials) indicate that acupuncture produces both a mini-mal perceptible clinical improvement (MPCI; Ehrich et al. 2000) and quite possibly a minimal clinically important change (Bellamy et al. 1992; Ehrich et al. 2000), but may only yield a minimal clinically important improvement (Tubach et al.

Relief of pain due to osteoarthritis of the knee
© 2013 Osteoarthritis Research Society International22
2005) for patients with low levels of pain. For muscle- strengthening exercise (with evidence from nine trials) an MPCI remains a possibility. Overall, our results suggest that few physical treatments are likely to have a clinically relevant pain- relieving effect. Other factors to consider when interpreting effectiveness results are safety, the rapidity of onset – and durability – of treatment benefit, and the convenience, cost and likelihood of patient adherence to treatment (Dworkin et al. 2009); these factors would clearly differ across the diverse range of interventions we studied, or when comparing them with phar-macological treatments.
Our analyses of the better- quality studies suggest that acupuncture should be consid-ered as one of the physical treatment options for relieving pain due to osteoarthritis of the knee in the short term. They indicate that balneotherapy, interferential therapy and heat treatment may also be effective, but the results for all three interventions were informed by single small studies, so a cautious interpretation is warranted. It is worth noting that some of our results on effectiveness do not concur with existing guidance on physical treatments, spe-cifically: EULAR (for insoles, braces and weight loss); NICE (for TENS, insoles, braces, weight loss, manual therapy, and heat or cooling treat-ment); ACR (for weight loss, insoles, thermal agents and Tai Chi); AAOS (for weight loss); and OARSI (for insoles, braces, heat or cooling treatment, TENS, and weight loss). Our analyses found little evidence (of significant differences from standard care, let alone clinically relevant differences) to support such guidance with respect to treating pain, other than for TENS, where the evidence was of poor quality and likely to be unreliable. It should be remembered though that our review was focused on pain outcomes, rather than on function, disability or cost- effectiveness.
Larger RCTs, with risk of bias reduced to a minimum and with longer treatment periods, which also examine the effectiveness of re- treatment following treatment cessation (to evaluate durability and attenuation effects) are needed in order to comprehensively assess the value of many of these interventions. The
optimum timing and parameters of treatment for both acupuncture and muscle- strengthening exercise also need to be more clearly defined by future studies.
The evidence available for our network meta- analyses, in which physical interventions for osteoarthritis of the knee were compared with each other within a coherent framework, suggests that overall effectiveness is limited, but that acupuncture can be considered as one of the more effective physical treatments for alle-viating pain in the short term. However, despite the large evidence base found, the methodologi-cal limitations associated with many of the trials indicate that high- quality trials of many of the physical treatments are still required.
ContributorsH.M. and N.W. conceived the study along with Lesley Stewart and Mark Sculpher. N.W., M.C., V.M., A.S. and H.M. developed the protocol. M.H. performed the searches. S.R. performed the analyses in collaboration with V.M. and A.S. M.C. wrote the first draft of the manuscript. M.C., N.W., V.M. and R.S. were responsible for the acquisition of data. All authors critically revised the manuscript for important intellectual content and approved the final version of the manuscript. H.M. obtained public funding. N.W. is guarantor.
Conflicts of interestThe authors declare that they have no compet-ing interests.
FundingThis article presents independent research funded by the NIHR under its Programme Grants for Applied Research Programme (Grant Reference Number RP- PG- 0707- 10186) titled, “Acupuncture for chronic pain and depression in primary care”. The views expressed are those of the author(s) and not necessarily those of the National Health Service, the NIHR or the Department of Health. The funders had no role in study design, data collection, data synthesis, data interpretation or writing the report.
M. S. Corbett et al.
© 2013 Osteoarthritis Research Society International 23
AcknowledgmentsThanks to Philip Conaghan, Mark Roman, Peter Hall, Mark Sculpher, Lesley Stewart, Andrea Manca, Cynthia Iglesias, Tony Danso- Appiah and Ann Hopton for their help at various stages of the review, particularly during protocol development.
ReferencesAdes A. E., Welton N. & Lu G. (2007) Introduction to
Mixed Treatment Comparisons. [WWW document.] URL http://www.bristol.ac.uk/social- community- medicine/media/mpes/intro- to- mtc.pdf
American Academy of Orthopaedic Surgeons (AAOS) (2008) Treatment of Osteoarthritis of the Knee (Non- arthroplasty). [WWW document.] URL http://www.revivestudio.com.au/media/content_posts/35/Treatment- of- Osteoarthritis- of- the- Knee- (Guideline).pdf
Arthritis Care (2004) Osteoarthritis Nation: The Most Comprehensive UK Report of People with Osteoarthritis. Arthritis Care, London.
Bellamy N., Carette S., Ford P. M., et al. (1992) Osteoarthritis antirheumatic drug trials. III. Setting the delta for clinical trials – results of a consensus devel-opment (Delphi) exercise. The Journal of Rheumatology 19 (3), 451–457.
Bjordal J. M., Ljunggren A. E., Klovning A. & Slørdal L. (2004) Non- steroidal anti- inflammatory drugs, includ-ing cyclo- oxygenase- 2 inhibitors, in osteoarthritic knee pain: meta- analysis of randomised placebo controlled trials. BMJ 329 (7478), 1317.
Caldwell D. M., Ades A. E. & Higgins J. P. T. (2005) Simultaneous comparison of multiple treatments: com-bining direct and indirect evidence. BMJ 331 (7521), 897–900.
Centre for Reviews and Dissemination (CRD) (2009) Systematic Reviews: CRD’s Guidance for Undertaking Reviews in Health Care. [WWW document.] URL https://www.york.ac.uk/media/crd/Systematic_Reviews.pdf
Cooper N. J., Sutton A. J., Morris D., Ades A. E. & Welton N. J. (2009) Addressing between- study heterogeneity and inconsistency in mixed treatment comparisons: application to stroke prevention treatments in indi-viduals with non- rheumatic atrial fibrillation. Statistics in Medicine 28 (14), 1861–1881.
Corbett M., Rice S., Slack R., et al. (2012) Acupuncture and Other Physical Treatments for the Relief of Chronic Pain Due to Osteoarthritis of the Knee: A Systematic Review and Network Meta- analysis. [WWW document.] URL http://www.york.ac.uk/media/crd/crdreport40.pdf
Dias S., Welton N. J., Caldwell D. M. & Ades A. E. (2010) Checking consistency in mixed treatment comparison meta- analysis. Statistics in Medicine 29 (7–8), 932–944.
Durmus D., Alayli G. & Cantürk F. (2005) Diz osteoar-tritli hastalarda biofeedback yardımlı izometrik egzersiz ve elektrik stimülasyon programının agrı, anksiyete ve depresyon üzerine etkisi. [Effects of biofeedback assisted isometric exercise and electrical stimulation on pain, anxiety and depression scores in knee osteoarthri-tis.] Türkiye Fiziksel Tıp ve Rehabilitasyon Dergisi 51 (4), 142–145. [In Turkish.]
Dworkin R. H., Turk D. C., McDermott M. P., et al. (2009) Interpreting the clinical importance of group differences in chronic pain clinical trials: IMMPACT recommendations. Pain 146 (3), 238–244.
Ehrich E. W., Davies G. M., Watson D. J., et al. (2000) Minimal perceptible clinical improvement with the Western Ontario and McMaster Universities osteo-arthritis index questionnaire and global assessments in patients with osteoarthritis. The Journal of Rheumatology 27 (11), 2635–2641.
Higgins J. P. T., Altman D. G., Gøtzsche P. C., et al. (2011) The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 343: d5928. DOI: 10.1136/bmj.d5928.
Hochberg M. C., Altman R. D., April K. T., et al. (2012) American College of Rheumatology 2012 recommen-dations for the use of nonpharmacologic and pharma-cologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care and Research 64 (4), 465–474.
Jamtvedt G., Dahm K. T., Christie A., et al. (2008) Physical therapy interventions for patients with osteoarthritis of the knee: an overview of systematic reviews. Physical Therapy 88 (1), 123–136.
Jensen H., Harreby M. & Kjer J. (1987) Infrarod laser – effekt ved smertende knaeartose? [Infrared laser – effect in painful arthrosis of the knee?] Ugeskrift for Laeger 149 (46), 3104–3106. [In Danish.]
Jezek J., Laznicky J. & Kyjovsky A. (1990) [Pulsatile magnetic field within the framework of comprehen-sive spa treatment in patients with clinically manifest gonarthritis.] Fysiatrický a revmatologický véstník 68 (4), 203–208. [In Czech.]
Jordan K. M., Arden N. K., Doherty M., et al. (2003) EULAR Recommendations 2003: an evidence based approach to the management of knee osteoarthritis: Report of a Task Force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Annals of the Rheumatic Diseases 62 (12), 1145–1155.
Linde K., Niemann K. & Meissner K. (2010) Are sham acupuncture interventions more effective than (other) placebos? A re- analysis of data from the Cochrane review on placebo effects. Forschende Komplementärmedizin 17 (5), 259–264.
Lu G. & Ades A. E. (2004) Combination of direct and indirect evidence in mixed treatment compari-sons. Statistics in Medicine 23 (20), 3105–3124.
Lu G. & Ades A. E. (2006) Assessing evidence incon-sistency in mixed treatment comparisons. Journal of the American Statistical Association 101 (474), 447–459.
Relief of pain due to osteoarthritis of the knee
© 2013 Osteoarthritis Research Society International24
Lund I., Näslund J. & Lundeberg T. (2009) Minimal acupuncture is not a valid placebo control in randomised controlled trials of acupuncture: a physiologist’s perspective. Chinese Medicine 4: 1. DOI: 10.1186/1749- 8546- 4- 1.
Manheimer E., Cheng K., Linde K., et al. (2010) Acupuncture for peripheral joint osteoarthritis. Cochrane Database of Systematic Reviews, Issue 1. Art. No.: CD001977. DOI: 10.1002/14651858.CD 001977.pub2.
Moher D., Liberati A., Tetzlaff J. & Altman D. G. for the PRISMA Group (2009) Preferred reporting items for systematic reviews and meta- analyses: the PRISMA statement. BMJ 339: b2535. DOI: http://dx.doi.org/10.1136/bmj.b2535.
National Collaborating Centre for Chronic Conditions (NCCCC) (2008) Osteoarthritis: National Clinical Guideline for Care and Management in Adults. Royal College of Physicians, London.
Ni G.- X., Song L., Yu B., Huang C.- H. & Lin J.- H. (2010) Tai chi improves physical function in older Chinese women with knee osteoarthritis. Journal of Clinical Rheumatology 16 (2), 64–67.
Pound P., Britten N., Morgan M., et al. (2005) Resisting medicines: a synthesis of qualitative studies of medi-cine taking. Social Science and Medicine 61 (1), 133–155.
Rodgers M., McKenna C., Palmer S., et al. (2008) Curative catheter ablation in atrial fibrillation and typical atrial flutter: systematic review and economic evalua-tion. Health Technology Assessment 12 (34), iii–iv, xi–xiii, 1–198.
Salanti G., Higgins J. P. T., Ades A. E. & Ioannidis J. P. A. (2008) Evaluation of networks of randomized trials.Statistical Methods in Medical Research 17 (3), 279–301.
Salli A., Ugurlu H. & Emlik D. (2006) Diz osteoartritinde konsantrik, kombine konsantrik- eksantrik ve izometrik egzersizlerin semptomlar ve fonksiyonel kapasite üzerine etkinliginin karsılastırılması. [Comparison of the effectiveness of concentric, combined concentric- eccentric and isometric exercises on symptoms and functional capacity in patients with knee osteoarthritis.] Türkiye Fiziksel Tıp ve Rehabilitasyon Dergisi 52 (2), 61–67. [In Turkish.]
Schumacher H. R. (2010) Tai Chi improves physical function in older Chinese women with knee osteo-arthritis: retraction. Journal of Clinical Rheumatology 16 (7), 357.
Suarez- Almazor M. E., Looney C., Liu Y., et al. (2010) A randomized controlled trial of acupuncture for osteoarthritis of the knee: effects of patient- provider communication. Arthritis Care and Research 62 (9), 1229–1236.
Tramèr M. R., Moore A. R., Reynolds J. M. D. & McQuay H. J. (2000) Quantitative estimation of rare adverse events which follow a biological progression: a new model applied to chronic NSAID use. Pain 85 (1–2), 169–182.
Tubach F., Ravaud P., Baron G., et al. (2005) Evaluation of clinically relevant changes in patient reported out-comes in knee and hip osteoarthritis: the minimal clini-cally important improvement. Annals of the Rheumatic Diseases 64 (1), 29–33.
Vickers A. J., Cronin A. M., Maschino A. C., et al. (2012) Acupuncture for chronic pain: individual patient data meta- analysis. Archives of Internal Medicine 172 (19), 1444–1453.
Welton N. J., Caldwell D. M., Adamopoulos E. & Vedhara K. (2009) Mixed treatment comparison meta- analysis of complex interventions: psychological interven-tions in coronary heart disease. American Journal of Epidemiology 169 (9), 1158–1165.
Zhang W., Moskowitz R. W., Nuki G., et al. (2008) OARSI recommendations for the management of hip and knee osteoarthritis, part II: OARSI evidence- based, expert consensus guidelines. Osteoarthritis and Cartilage 16 (2), 137–162.
This is an open- access article distributed under the terms of the Creative Commons Attribution- NonCommercial- ShareAlike Licence, which permits non- commercial use, distribution and reproduction in any medium, provided the original author and source are credited.
This article is reprinted from Osteoarthritis and Cartilage. Original publication: Osteoarthritis and Cartilage, Vol. 21, No. 9, pp. 1290–1298 (September 2013).
Appendix 1Supplementary data related to this article can be found online (http://dx.doi.org/10.1016/ j.joca.2013.05.007).

© 2016 Acupuncture Association of Chartered Physiotherapists 25
Correspondence: Karen Charlesworth, Northern College of Acupuncture, 61 Micklegate, York YO1 6LJ, UK (e- mail: karen@appa- acupuncture.org).
Acupuncture in Physiotherapy, Volume 28, Number 1, Spring 2016, 25–32
CLINICAL PAPER
An auricular acupuncture protocol for the attenuation of pain and anxiety in humanitarian aid environments: a consensus study to determine a theoretically safe and effective beta protocol
K. CharlesworthNorthern College of Acupuncture, York, UK
AbstractOn the basis of current research, it was hypothesized that a standardized auricular acu-puncture protocol might be a suitable treatment to attenuate pain and anxiety in humanitar-ian aid environments (HAEs). The aim of this study was to construct, by consensus, a theoretically safe and effective standardized auricular acupuncture protocol that would be suitable for use in HAEs. The Internet- based iterative sequential (mixed methods) model was used to combine quantitative and qualitative data. Data from each round were analysed in order to determine the components with the greatest level of support to progress to suc-cessive rounds. A repeated- measures analysis of variance was used as a surrogate measure of consensus. Consensus was achieved on a suitable protocol for use in HAEs that the participants rated theoretically as highly effective in the attenuation of pain and anxiety. The Auricular Protocol for Pain and Anxiety (APPA) is comprised of five auricular points and 13 administration procedures covering effectiveness and safety. The study made a range of secondary findings, including a level of “component instability” and a level of bias that may have affected the quality of the beta protocol. The study concludes that it is possible to use a consensus process to construct a standardized auricular acupuncture protocol that is theoretically safe and effective in the attenuation of pain and anxiety, and suitable for use in HAEs. However, it should be noted that the consensus was gained on theoretical safety and effectiveness. It is recommended that a further research programme that takes into account the primary and secondary findings of this study is structured to determine the actual effectiveness and safety of APPA.
Keywords: anxiety, auricular acupuncture, ear, humanitarian aid environments, pain, standard-ized protocol.
Introduction
Humanitarian aid environmentsThe twenty- first century has seen an increase in armed conflict, and both natural and man- made disasters, and there has been an associated rise
in the number of global citizens living in condi-tions of extreme deprivation (Metz 2000; Green 2009, 2012; USEPA 2016).
While each humanitarian aid environment (HAE) differs in its characteristics, and there-fore, in its impact on the health of the local population, research has shown that the general healthcare conditions most prevalent in HAEs are related to:

Auricular Protocol for Pain and Anxiety
© 2016 Acupuncture Association of Chartered Physiotherapists26
• mental health, including generalized anxiety and fear, sleep disturbance, and components of the post- traumatic stress spectrum includ-ing depression (Ronquillo 1999; Naku 2010; Chan & Koo 2011; Nakagawa et al. 2013; Silove et al. 2014); and
• pain, including neuropathic pain – typically located in areas including the lower back, knees, neck and/or shoulders, and abdomen (Mateen 2010; Angeletti et al. 2012, 2014; Lippert et al. 2013; Wen et al. 2013).
Multiple investigations over the past 40 years have demonstrated the effectiveness of auricu-lar acupuncture (AA) as a treatment for pain and anxiety (Alimi et al. 2000; Ahadian 2002; Berman et al. 2004; Pilkington et al. 2007; Chang et al. 2010; Niemtzow 2007, 2010; Holzer, et al. 2011; Bergdahl et al. 2014; Chang & Sommers 2014; Marignan 2014; Romoli et al. 2014).
In an HAE, AA offers several positive attrib-utes that render it suitable as either a sole or an adjunctive therapy: it requires no special-ist storage; the equipment is neither bulky nor heavy in comparison to pharmaco-logical equivalents (Knowlton et al. 2011); needles have shelf lives of between 3 and 5 years; and a delivery programme is faster and easier to establish than mental health services. When delivered in a standardized form, AA requires relatively little training, little or no verbal communication, and no diagnostic skills to administer safely, effectively and swiftly. This helps to enable wide- scale treatment programmes by local practitioners, increasing local resilience in vulnerable populations, and decreasing reliance on outside agencies at a time of acute humanitarian crisis (Arnold 2002).
The aim of the present study was to deter-mine whether it is possible, by consensus, to construct a standardized AA protocol that is: theoretically safe; effective in attenuating pain and anxiety; quick to administer; cost- effective; and capable of delivery to the greatest number of patients possible by (local) volunteers with-out extensive training or any diagnostic skills, and using little or no verbal communication,
in the challenging treatment conditions that are typical of HAEs.
Auricular acupunctureAuricular acupuncture is a relatively modern phenomenon, and its mechanisms of action remain the subject of some debate between its various schools.
In the early twentieth century, French physi-cian Paul Nogier hypothesized that: a represen-tation of an inverted foetus (a “homunculus”) could be imagined as superimposed on the auricle; pathology in the body was indicated by detection of painful points corresponding to the foetus on the auricle; and this pathology could be influenced by stimulating the auricular points (Oleson 2013). In the 1950s, the Nanjing Army Ear Acupuncture Research Team in China con-ducted trials that claimed to validate the clini-cal effectiveness of this model. More recently, research published in the past 4 years proposes a rationale for AA action specifically focused on the mechanism of the auricular branch of the vagus nerve, influencing functions such as gastrointestinal motility and sweating, and indi-rectly, blood pressure and heart rate (White & Ernst 1999; Nedeljkovic 2011; Gao et al. 2011, 2012; He et al. 2012; Napadow et al. 2012; Arai et al. 2013; Li & Wang 2013; da Silva & Dorsher 2014).
The late 1970s saw the emergence of the world’s first standardized AA “protocol”, a set prescription of points that was administered to all patients with little or no variation. The National Acupuncture Detoxification Association (NADA) five- point protocol was developed by the Lincoln Hospital in New York, NY, USA, as an aid for recovering substance abusers (Kolenda 2000; Bemis 2013a). Since that time, the NADA model has been employed in several HAEs, including: the 9/11 and Hurricane Katrina inci-dents in North America; ongoing community health programmes in deprived areas in India; refugee camps in Thailand and East Africa; and UK prisons (Deadman et al. 2005; Smith 2009; Bemis 2013b). This five- point protocol has also been used in UK National Health Service stud-ies (de Valois et al. 2012). Robust critical evalua-tion of NADA’s effectiveness in HAEs remains
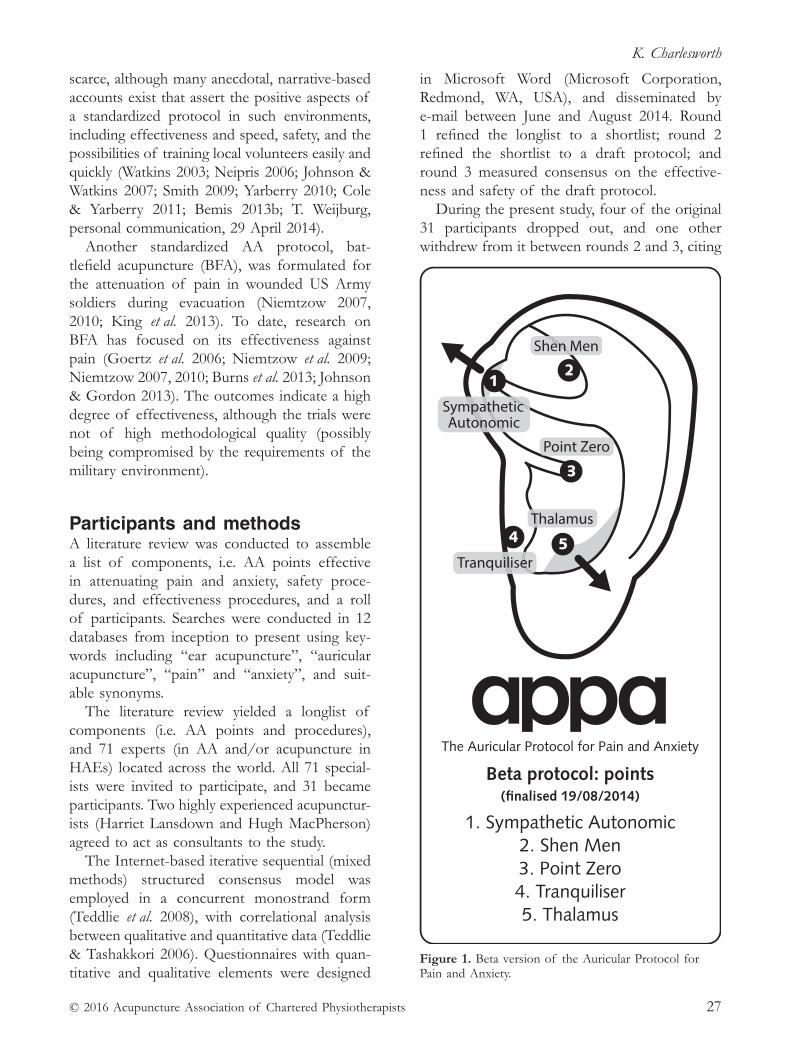
K. Charlesworth
© 2016 Acupuncture Association of Chartered Physiotherapists 27
scarce, although many anecdotal, narrative- based accounts exist that assert the positive aspects of a standardized protocol in such environments, including effectiveness and speed, safety, and the possibilities of training local volunteers easily and quickly (Watkins 2003; Neipris 2006; Johnson & Watkins 2007; Smith 2009; Yarberry 2010; Cole & Yarberry 2011; Bemis 2013b; T. Weijburg, personal communication, 29 April 2014).
Another standardized AA protocol, bat-tlefield acupuncture (BFA), was formulated for the attenuation of pain in wounded US Army soldiers during evacuation (Niemtzow 2007, 2010; King et al. 2013). To date, research on BFA has focused on its effectiveness against pain (Goertz et al. 2006; Niemtzow et al. 2009; Niemtzow 2007, 2010; Burns et al. 2013; Johnson & Gordon 2013). The outcomes indicate a high degree of effectiveness, although the trials were not of high methodological quality (possibly being compromised by the requirements of the military environment).
Participants and methodsA literature review was conducted to assemble a list of components, i.e. AA points effective in attenuating pain and anxiety, safety proce-dures, and effectiveness procedures, and a roll of participants. Searches were conducted in 12 databases from inception to present using key-words including “ear acupuncture”, “auricular acupuncture”, “pain” and “anxiety”, and suit-able synonyms.
The literature review yielded a longlist of components (i.e. AA points and procedures), and 71 experts (in AA and/or acupuncture in HAEs) located across the world. All 71 special-ists were invited to participate, and 31 became participants. Two highly experienced acupunctur-ists (Harriet Lansdown and Hugh MacPherson) agreed to act as consultants to the study.
The Internet- based iterative sequential (mixed methods) structured consensus model was employed in a concurrent monostrand form (Teddlie et al. 2008), with correlational analysis between qualitative and quantitative data (Teddlie & Tashakkori 2006). Questionnaires with quan-titative and qualitative elements were designed
in Microsoft Word (Microsoft Corporation, Redmond, WA, USA), and disseminated by e- mail between June and August 2014. Round 1 refined the longlist to a shortlist; round 2 refined the shortlist to a draft protocol; and round 3 measured consensus on the effective-ness and safety of the draft protocol.
During the present study, four of the original 31 participants dropped out, and one other withdrew from it between rounds 2 and 3, citing
21
3
54
Figure 1. Beta version of the Auricular Protocol for Pain and Anxiety.

Auricular Protocol for Pain and Anxiety
© 2016 Acupuncture Association of Chartered Physiotherapists28
concerns regarding the safety of a standardized protocol (see “Discussion” below).
ResultsThe final draft of the Auricular Protocol for Pain and Anxiety (APPA) is comprised of five AA points delivered bilaterally: Shen Men, Sympathetic Autonomic, Point Zero, Thalamus and Tranquilizer (Fig. 1). The points are sup-ported by seven “effectiveness” procedures, which cover issues such as dosage levels and retention time, and six “safety” procedures,
including practitioner hand hygiene, patient ear cleansing and disposal of waste.
A quantitative assessment of the draft pro-tocol’s theoretical effectiveness in attenuating pain and anxiety was provided via three overall rating questions in the round 3 questionnaire. First, the participants were asked to rate the theoretical effectiveness of the draft protocol’s points as a whole (Table 1). Secondly, the participants were asked to rate the theoretical effectiveness of the effectiveness procedures as a whole (Table 2). Thirdly, the participants were asked to rate the theoretical safety of the safety procedures as a whole (Table 3). These ratings were supported by qualitative data, with 25.81% of participants commenting positively on the theoretical effectiveness of the points to attenuate pain and anxiety.
A one- way within- subjects (or repeated meas-ures) analysis of variance (ANOVA) was con-ducted on quantitative data in order to analyse levels of agreement on the 16 components that were subjected to consultation across all three rounds of consensus. The ANOVA showed a significant effect of “time and the administra-tion of questionnaires” (see “Discussion” below): Wilks’ Lambda = 0.24, F(2, 14) = 21.9, P = 0 (Table 4). This strongly suggests that time and the administration of questionnaires affected consensus levels, and specifically, that the participants’ levels of agreement increased over the three rounds of consultation.
Discussion
Component instabilityThree main areas of component instability emerged between participants during the pre-sent study. These were: confusion over point
Table 3. Theoretical safety of the draft protocol safety proce-dures (rating scale: 1–9)
Analysis of central tendency Result
Mean 8.4 (93.3% theoretical safety)Median 8.5 (94.4% theoretical safety)Mean absolute deviation 0.6Respondents rating ≥ 8/9 (%) 84.6 (n = 22 of 26)
Table 4. Results of a one- way analysis of variance comparing the participants’ levels of agreement across three rounds of consultation for 16 components (design: intercept)
Degrees of freedom
Effect Value F- test Hypothesis Error P- value
Time and questionnaires: Pillai’s Trace 0.758 21.907* 2.000 14.000 0.000 Wilks’ Lambda 0.242 21.907* 2.000 14.000 0.000 Hotelling’s Trace 3.130 21.907* 2.000 14.000 0.000 Roy’s Largest Root 3.130 21.907* 2.000 14.000 0.000
*Exact statistic.
Table 1. Theoretical effectiveness of draft protocol points (rat-ing scale: 1–9)
Analysis of central tendency Result
Mean 7.3 (81.1% effectiveness of points)
Median 7.8 (86.6% effectiveness of points)
Mean absolute deviation 1.0Respondents rating ≥ 8/9 (%) 46.2 (n = 12 of 26)
Table 2. Theoretical effectiveness of the draft protocol effec-tiveness procedures (rating scale: 1–9)
Analysis of central tendency Result
Mean 7.9 (87.7% effectiveness of effectiveness procedures)
Median 8.0 (88.8% effectiveness of effectiveness procedures)
Mean absolute deviation 0.6Respondents rating ≥ 8/9 (%) 69.2 (n = 18 of 26)

K. Charlesworth
© 2016 Acupuncture Association of Chartered Physiotherapists 29
locations versus names between the different AA schools; confusion over point locations within the European/Nogier school; and confu-sion over point names within all schools.
Practically speaking, to allow the consensus process to achieve a level of robust agree-ment, consensus should ideally be sought on items that are, in themselves, stable. In other words, these should be more or less uniformly recognized and understood conceptually and in their effects. To attempt consensus on un stable components – which become a matter of debate as a result of the consensus process – is to court divergence rather than convergence. In the case of the present study, although the consensus process yielded a high level of agree-ment, the level at which its constituent elements were “understood” by all the participants – and by extrapolation, the quality of the protocol itself – must remain open to question.
The standardized protocol: can one size fit all?There may be safety implications for standard-ized protocols: some of the functions claimed by AA’s most respected sources (Chen & Cui 1991; Oleson 2013; Chalmers 2014) for the points in APPA (in common with other stand-ardized AA protocols) may not be appropriate for all patients. For example, the Shen Men point, which is included in the BFA and NADA protocols, as well as the beta version of APPA, is believed to lower blood pressure (Oleson 2013), and on that basis, would be contraindi-cated for a patient with hypotension. The study populations of numerous protocol- based trials in the past decade have presumably included a proportion of hypotensive patients, but few (if any) adverse reactions related to this effect have been reported. It remains unclear why this apparent contraindication is not borne out by studies. There are other points within the APPA, BFA and NADA protocols that raise similar questions.
The effect of missing data on consensus levelsAlthough the decision to analyse and report rating questions to participants by a percentage
measure of those involved rating a given component at the highest level was justified on grounds of its clarity and meaningfulness for them, it should be noted that correction for attrition magnified the reported levels of consensus in each successive questionnaire, and this may have influenced some participants’ suc-cessive responses.
For instance, the Shen Men AA point, which attracted 22 participants’ highest rating in round 1, was reported to those involved as 71% of them (total n = 31). In round 2, 23 participants gave the highest rating to this point, which emerged as a percentage total of 82.6% of those involved (total n = 28 for round 2, three partici-pants having withdrawn). In the round 3 ques-tionnaire, both rounds’ ratings were shown; it is hypothesized that the apparently sizeable jump in consensus levels between rounds 1 and 2 may have influenced some participants’ responses. The effect of this influence was not measurable, and therefore, must remain unknown.
Since it is hypothesized that the measure-ment instrument itself may have influenced the outcomes by reporting (apparently sizeable) consensus levels, ANOVA data analysis modi-fied the value of the independent variable from simply “time” (as is more usual in a longitudinal repeated- measures study) to “time and the administration of questionnaires”.
BiasSeveral types of bias may have affected the study outcomes. At the outset, it was hypoth-esized that systematic bias could arise as a result of recruiting a proportionately high number of individuals who were adherents of one or more existing standardized protocols. The participants were asked to submit personal data in round 1, and an exploratory weighting exercise was carried out to detect such bias. This exercise revealed that participant profile was not a pre-dictor of such bias.
Given the nature of the APPA project, the participants may also have been inclined to positive affective component of attitude bias stemming from an emotional attachment to the study’s success. The effect of this bias is potentially exacerbated by the possibility that

Auricular Protocol for Pain and Anxiety
© 2016 Acupuncture Association of Chartered Physiotherapists30
a lack of attachment to the APPA outcomes may have contributed to the withdrawal of five participants by round 3, and therefore, left a higher concentration of participants with such a bias. Since its existence is not measurable, the only reliable conclusion that can be drawn regarding affective component of attitude bias is that this may have affected individual compo-nent responses, and the overall section ratings in round 3.
Finally, the requirement for “active manage-ment” in this study can be seen to reinforce internal validity by promoting its aims, but it can also be seen to pose a danger to internal valid-ity. Where researcher judgement has a “casting vote”, there is a clear possibility of internal bias affecting outcomes. In mixed- methods studies, creative mitigation of the effects of personal bias might begin with biographical self- disclosure, as required by the consoli-dated criteria for reporting qualitative research (COREQ) (Tong et al. 2007), but should con-tinue forwards, acknowledging the reflexive possibilities of the researcher’s personal and cultural context, and embedding the awareness of biography’s possible effect on every aspect of study design, implementation, analysis and reporting. The present study has attempted to take account of personal bias at every juncture, particularly with regard to “active management” processes, by various means including cross- referencing decisions with the two consultant acupuncturists. However, it would be useful to explore the dimensions in which personal bias becomes active during mixed- methods studies. A secondary recommendation of this study is the development of personal bias indicators throughout the qualitative research process, as a supplementary extension of COREQ and/or other qualitative reporting models.
ConclusionsThe present study met its aims of formulating a beta AA protocol that was agreed by experts to be theoretically safe and effective in HAEs. However, this result was not achieved by the consensus process alone since it required some “active management” by the researcher and
consultant acupuncturists. Some methodological limitations may also have affected the quality of the outcome.
It is recommended that the beta version of APPA should progress to a series of rigorous controlled trials, which should be designed to take account of the limitations encountered in the present study, to ascertain whether theoreti-cal safety and effectiveness translate into actual safety and effectiveness.
A full outline of the theoretically effective version of APPA is available on request from the present author.
AcknowledgementsThe author wishes to thank the consensus participants who contributed their expertise and time to formulating the theoretically effective APPA protocol. Those who agreed to be named were: Young- Chang P. Arai; Dr Gary Asher; Dr Lena Bergdahl; Dr Kenneth O. Carter; Carla Cassler; Dr Francesco Ceccherelli; Dr Bryan L. Frank; Greg Golden; Dr Luigi Gori; Dr Matthias Karst; Leonice Fumiko Sato Kurebayashi; Kajsa Landgren; Pamela Olton; Juliana Miyuki do Prado; Dr Marco Romoli; Professor Dr Fernando Mendes Sant’Anna; Professor Sabine Sator- Katzenschlager; Di Shimell; Dr Nader Soliman; Dr Elizabeth Sommers; Dr Elizabeth Stuyt; Dr Beverley de Valois; and Dr Elizabeth Wilmot.
ReferencesAhadian F. M. (2002) Acupuncture in pain medicine: an
integrated approach to the management of refractory pain. Current Pain and Headache Reports 6 (6), 444–451.
Alimi D., Rubino C., Pichard- Léandri E. & Fermand- Brulé S. (2000) Analgesic effects of auricular acupuncture for cancer pain. [Letter.] Journal of Pain and Symptom Management 19 (2), 81–82.
Angeletti C., Guetti C., Papola R., et al. (2012) Pain after earthquake. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 20: 43. DOI: 10.1186/1757- 7241- 20- 43.
Angeletti C., Guetti C., Ursini M. L., et al. (2014) Low back pain in a natural disaster. Pain Practice 14 (2), E8–E16.
Arai Y.- C. P., Sakakima Y., Kawanishi J., et al. (2013) Auricular acupuncture at the “Shenmen” and “Point Zero” points induced parasympathetic activation. Evidence- Based Complementary and Alternative Medicine 2013: 4. DOI: 10.1155/2013/945063.
K. Charlesworth
© 2016 Acupuncture Association of Chartered Physiotherapists 31
Arnold J. L. (2002) Disaster medicine in the 21st century: future hazards, vulnerabilities, and risk. Prehospital and Disaster Medicine 17 (1), 3–11.
Bemis R. (2013a) Evidence for the NADA Ear Acupuncture Protocol Summary of Research: A Review of Literature. [WWW document.] URL http://acudetox.com/phoca-download/Research_Summary_2013%20(2).pdf
Bemis R. (2013b) Ear Acupuncture and Humanitarian Aid: History, Application, and Improvement of the NADA model. [WWW document.] URL http://acudetox.com/phoca-download/Research_Summary_2013%20(2).pdf
Bergdahl L., Berman A. H. & Haglund K. (2014) Patients’ experience of auricular acupuncture during protracted withdrawal. Journal of Psychiatric and Mental Health Nursing 21 (2), 163–169.
Berman A. H., Lundberg U., Krook A. L. & Gyllenhammar C. (2004) Treating drug using prison inmates with auricular acupuncture: a randomized controlled trial. Journal of Substance Abuse Treatment 26 (2), 95–102.
Burns S., York A., Niemtzow R. C., et al. (2013) Moving acupuncture to the frontline of military medical care: a feasibility study. Medical Acupuncture 25 (1), 48–54.
Chalmers J. (2014) Auriculotherapy Ear Acupuncture: The Practitioner’s Guide. Chalatalrick Publishers, Castle Douglas.
Chan E. Y. Y. & Koo S. D. (2011) Systematic literature review on pediatric sleep disturbance management post- disaster: implications of post- disaster pediatric clinical management in developing countries. [Abstract.] Prehospital and Disaster Medicine 26 (Suppl. 1), S38.
Chang B.- H., Sommers E. & Herz L. (2010) Acupuncture and relaxation response for substance use disorder recovery. Journal of Substance Use 15 (6), 390–401.
Chang B.- H. & Sommers E. (2014) Acupuncture and relaxation response for craving and anxiety reduction among military veterans in recovery from substance use disorder. The American Journal on Addictions 23 (2), 129–136.
Chen K. & Cui Y. (1991) Handbook to Chinese Auricular Therapy. Foreign Languages Press, Beijing.
Cole B. & Yarberry M. (2011) NADA training provides PTSD relief in Haiti. Deutsche Zeitschrift für Akupunktur 54 (1), 21–24.
Da Silva M. A. H. & Dorsher P. T. (2014) Neuroanatomic and clinical correspondences: acupuncture and vagus nerve stimulation. The Journal of Alternative and Complementary Medicine 20 (4), 233–240.
Deadman P., Cox S. & Wagner K. (2005) SMART UK: The Substance Misuse Acupuncture Register and Training. The Journal of Chinese Medicine 78 (June), 52–54.
De Valois B., Young T. E., Robinson N., McCourt C. & Maher E. J. (2012) NADA ear acupuncture for breast cancer treatment- related hot flashes and night sweats: an observational study. Medical Acupuncture 24 (4), 256–268.
Gao X.- Y., Li Y.- H., Liu K., et al. (2011) Acupuncture- like stimulation at auricular point Heart evokes
cardiovascular inhibition via activating the cardiac- related neurons in the nucleus tractus solitarius. Brain Research 1397, 19–27.
Gao X.- Y., Wang L., Gaischek I., et al. (2012) Brain- modulated effects of auricular acupressure on the regulation of autonomic function in healthy volunteers. Evidence- Based Complementary and Alternative Medicine 2012: 8. DOI: 10.1155/2012/714391.
Goertz C. M., Niemtzow R., Burns S. M., et al. (2006) Auricular acupuncture in the treatment of acute pain syndromes: a pilot study. Military Medicine 171 (10), 1010–1014.
Green D. (2009) Natural Disasters Will Hurt 50% More People by 2015. Why? Climate Change + Inequality. [WWW document.] URL http://oxfamblogs.org/fp2p/natural- disasters- will- hurt- 50- more- people- by- 2015- why- climate- change- inequality/
Green D. (2012) From Poverty to Power: How Active Citizens and Effective States Can Change the World, 2nd edn. Practical Action Publishing, Rugby, and Oxfam International, Oxford.
He W., Wang X., Shi H., et al. (2012) Auricular acupuncture and vagal regulation. Evidence- Based Complementary and Alternative Medicine 2012: 6. DOI: 10.1155/2012/786839.
Holzer A., Leitgeb U., Spacek A., et al. (2011) Auricular acupuncture for postoperative pain after gynaeco-logical surgery: a randomized controlled trial. Minerva Anestesiologica 77 (3), 298–304.
Johnson G. & Watkins S. (2007) Needles for Ethiopia. Acupuncture in Medicine 25 (1–2), 50–52.
Johnson T. & Gordon J. (2013) Retrospective review of efficacy and safety of acupuncture for treatment of active duty service members with headaches after non- penetrating blast exposure. [Abstract.] Cephalalgia 33 (8, Suppl.), 246–247.
King H. C., Hickey A. H. & Connelly C. (2013) Auricular acupuncture: a brief introduction for military provid-ers. Military Medicine 178 (8), 867–874.
Knowlton L. M., Gosney J. E., Jr, Chackungal S., et al. (2011) Consensus statements regarding the multidis-ciplinary care of limb amputation patients in disasters or humanitarian emergencies: report of the 2011 Humanitarian Action Summit Surgical Working Group on Amputations Following Disasters or Conflict. Prehospital and Disaster Medicine 26 (6), 438–448.
Kolenda J. (2000) A Brief History of Acupuncture for Detoxification in the United States. [WWW document.] URL http://www.acupuncturetoday.com/mpacms/at/article.php?id=27686
Li H. & Wang Y.- P. (2013) Effect of auricular acupunc-ture on gastrointestinal motility and its relationship with vagal activity. Acupuncture in Medicine 31 (1), 57–64.
Lippert S. C., Nagdev A., Stone M. B., Herring A. & Norris R. (2013) Pain control in disaster settings: a role for ultrasound- guided nerve blocks. Annals of Emergency Medicine 61 (6), 690–696.

Auricular Protocol for Pain and Anxiety
© 2016 Acupuncture Association of Chartered Physiotherapists32
Marignan M. (2014) Auriculotherapy treatment pro-tocol for low- back pain: a randomized trial. Medical Acupuncture 26 (3), 154–160.
Mateen F. J. (2010) Neurological disorders in complex humanitarian emergencies and natural disasters. Annals of Neurology 68 (3), 282–294.
Metz S. (2000) Armed Conflict in the 21st Century: The Information Revolution and Post- Modern Warfare. [WWW document.] URL http://www.au.af.mil/au/awc/ awcgate/ssi/metz_info_rev.pdf
Nakagawa S., Sugiura M., Sekiguchi A., et al. (2014) Fatigue and relating to others 3 months after the 2011 Great East Japan Earthquake. Psychiatry Research 218 (3), 324–328.
Naku C. (2010) Trauma Relief and School Support for Kenyan Refugees in Uganda. [WWW document.] URL http://www.realmedicinefoundation.org/our- work/countries/uganda/initiatives/kiryandongo- refugee- settlement- project/reports/2010/trauma- relief- and- school- support- for- kenyan- refugees- in- uganda/
Napadow V., Edwards R. R., Cahalan C. M., et al. (2012) Evoked pain analgesia in chronic pelvic pain patients using respiratory- gated auricular vagal afferent nerve stimulation. Pain Medicine 13 (6), 777–789.
Nedeljkovic M. (2011) Ohrakupunktur und der Einfluss auf die Herztätigkeit – Möglichkeiten und Grenzen wissenschaftlicher Vorgehensweisen. [Ear- acupuncture and its influence on the heart activity – possibilities and limits of scientific procedures.] Schmerz und Akupunktur 37 (1), 16–19. [In German.]
Neipris C. (2006) Acupuncture hurricane relief. Oriental Medicine 2006 (Winter), 20–22.
Niemtzow R. C. (2007) Battlefield acupuncture. Medical Acupuncture 19 (4), 225–228.
Niemtzow R. C. (2010) Battlefield acupuncture. Journal of the Acupuncture Association of Chartered Physiotherapists 2010 (Autumn), 55–59.
Niemtzow R. C., Litscher G., Burns S. M. & Helms J. M. (2009) Battlefield acupuncture: update. Medical Acupuncture 21 (1), 43–46.
Oleson T. (2013) Auriculotherapy Manual: Chinese and Western Systems of Ear Acupuncture, 4th edn. Churchill Livingstone, Edinburgh.
Pilkington K., Kirkwood G., Rampes H., Cummings M. & Richardson J. (2007) Acupuncture for anxiety and anxiety disorders – a systematic literature review. Acupuncture in Medicine 25 (1–2), 1–10.
Romoli M., Avgerinos C., Baratto L. & Giommi A. (2014) Auriculotherapy for persisting postoperative pain caused by total knee replacement. Medical Acupuncture 26 (2), 97–102.
Ronquillo E. L. (1999) Mental health in disaster: the Philippine experience. [Abstract.] Prehospital and Disaster Medicine 14 (Suppl. 1), S46–S47.
Silove D., Liddell B., Rees S., et al. (2014) Effects of recurrent violence on post- traumatic stress disorder and severe distress in conflict- affected Timor- Leste: a 6- year longitudinal study. The Lancet Global Health 2 (5), e293–e300.
Smith M. O. (2009) Ear acupuncture protocol meets global needs. Medical Acupuncture 21 (2), 75.
Teddlie C., Tashakkori A. & Johnson B. (2008) Emergent techniques in the gathering and analysis of mixed methods data. In: Handbook of Emergent Methods (eds S. N. Hesse- Biber & P. Leavy), pp. 389–413. The Guilford Press, London.
Teddlie C. & Tashakkori A. (2006) A general typology of research designs featuring mixed methods. Research in the Schools 13 (1), 12–28.
Tong A., Sainsbury P. & Craig J. (2007) Consolidated criteria for reporting qualitative research (COREQ): a 32- item checklist for interviews and focus groups. International Journal for Quality in Health Care 19 (6), 349–357.
United States Environmental Protection Agency (USEPA) (2016) Future Climate Change. [WWW document.] URL https://www3.epa.gov/climatechange/science/future.html
Watkins S. (2003) Practising acupuncture in the develop-ing world. Acupuncture in Medicine 21 (1–2), 47–51.
Wen H., Reinhardt J. D., Gosney J. E., et al. (2013) Spinal cord injury- related chronic pain in victims of the 2008 Sichuan earthquake: a prospective cohort study. Spinal Cord 51 (11), 857–862.
White A. & Ernst E. (1999) The effect of auricular acu-puncture on the pulse rate: an exploratory randomised controlled trial. Acupuncture in Medicine 17 (2), 86–88.
Yarberry M. (2010) The use of the NADA protocol for PTSD in Kenya. Deutsche Zeitschrift für Akupunktur 53 (4), 6–11.
Before becoming a traditional Chinese acupuncturist, Karen Charlesworth worked as a senior consultant editor for Health Building Notes, the Department of Health’s series of consensus- based guidelines on best practice in healthcare building. She received an MSc in Acupuncture (Distinction) in 2013. Karen is currently designing a small- scale randomized controlled trial to indicate the clinical effectiveness of APPA, and she expects to have results by the end of 2017.
© 2016 Acupuncture Association of Chartered Physiotherapists 33
Correspondence: Wayne Fish, Orthopaedic Tier 2 Clinic, Longsight Health Centre, Longsight, Manchester M13 0RR UK (e- mail: [email protected]).
Acupuncture in Physiotherapy, Volume 28, Number 1, Spring 2016, 33–39
CLINICAL PAPER
Does superficial dry needling improve hamstring muscle flexibility in normal subjects?
W. FishOrthopaedic Tier 2 Clinic, Longsight Health Centre, Central Manchester University Hospitals NHS Foundation Trust, Manchester, and Private Practice, Wilmslow, Cheshire, UK
AbstractHamstring muscle flexibility is important because it optimizes musculoskeletal function and may prevent injury to the muscle. The most common way of improving muscle flexibility is through stretching, which has been shown to bring about viscoelastic and neurophysiological changes in the muscle. In the clinical setting, acupuncture is routinely used to treat myo-fascial trigger points, which are commonly found in tight muscles. The aim of this study was to investigate whether the acupuncture technique referred to as superficial dry needling could improve hamstring muscle flexibility. Twenty healthy male volunteers with tight ham-strings participated in this trial. The study used a same- subject experimental design. Knee extension angle was used to measure hamstring muscle flexibility before and after treatment with superficial dry needling at the Bladder (BL) 37 acupuncture point. There was a highly significant difference in the scores for hamstring muscle flexibility before [mean ± standard deviation (SD) = 35.10 ± 13.21] and after (mean ± SD = 28 ± 13.86) treatment with superficial dry needling (t = 5.87; P < 0.001). These results suggest that there is a highly significant change in hamstring muscle flexibility immediately after being treated with superficial dry needling at BL37.
Keywords: acupuncture, dry needling, hamstring muscle, muscle flexibility.
IntroductionThe literature reports that the hamstring is the most commonly injured muscle during sporting activity (O’Hora et al. 2011). Hamstring muscle flexibility is considered to be important in pre-ventative and clinical rehabilitation programmes (Schuback et al. 2004; O’Hora et al. 2011). Stretching exercises are recommended on the basis that they may prevent injuries (Schuback et al. 2004; O’Hora et al. 2011), improve athletic performance (Thacker et al. 2004), and improve muscle and joint flexibility (Thacker et al. 2004). Flexibility varies between individuals, and it has
been suggested that muscles spanning more than one joint are more at risk of injury (Davis et al. 2008). Musculoskeletal flexibility is defined as the absolute range of movement in a joint or series of joints, and the length of muscles cross-ing the joints (McHugh et al. 1998). Stretching has been advocated as a way of improving the flexibility of the hamstring muscle (O’Hora et al. 2011).
Stretching brings about a change in flexibility through its viscoelastic and neurophysiological effects (Kabrak et al. 2001). Static stretching has a viscoelastic effect on the muscle (McHugh et al. 1998; Ryan et al. 2010). This suggests that a stretch on a muscle is time- and history- dependent (Taylor et al. 1997). Proprioceptive neuromuscular facilitation (PNF) stretching

Superficial dry needling and hamstring flexibility
© 2016 Acupuncture Association of Chartered Physiotherapists34
has a neurophysiological effect (Schuback et al. 2004). A PNF stretch involves the contrac-tion of the agonist or the antagonist muscle in order to improve flexibility. The proposed mechanisms underlying PNF stretching include reciprocal inhibition and autogenic inhibition (Schuback et al. 2004; O’Hora et al. 2011). Static and PNF stretching are performed actively, and involve a direct stretch of the muscle.
Treatment techniques that improve muscle length without stretching may provide evidence that further supports the neurophysiological mechanisms affecting muscle flexibility. These may also provide a more effective way of improving muscle flexibility. A common treat-ment technique used in the management of myofascial pain is acupuncture. Although evi-dence exists to support the use of acupuncture for managing pain (Edwards & Knowles 2003; Stux et al. 2003; Bradnam- Roberts 2007), there seems to be no recent data that support the use of acupuncture for changing muscle flexibility (Alvarez & Rockwell 2002; Huguenin 2004; Kalichman & Vulfsons 2010).
The acupuncture technique known as dry needling is commonly used to treat myofas-cial pain and dysfunction (Baldry 2002a, b; Huguenin 2004). It is known as “dry” needling because no substance is injected (Baldry 2002a). Two types of dry needling are discussed in the literature: deep and superficial dry needling. The advantages of using superficial dry nee-dling are that it is a painless procedure, there is minimal risk of damage to nerves, blood vessels and other structures, and there is a low incidence of post- treatment soreness (Baldry 2002b).
In the clinical setting, superficial dry needling is commonly used to deactivate myofascial trigger points (MTPs) (Macdonald et al. 1983; Edwards & Knowles 2003; Fu et al. 2007). There is evidence to support the use of superfi-cial dry needling to deactivate MTPs both when the technique is used in isolation and when it is combined with stretching (Macdonald et al. 1983; Edwards & Knowles 2003; Fu et al. 2007). However, no studies to date have investigated the effect of superficial dry needling on muscle flexibility.
The aim of the present study was to deter-mine the effect of superficial dry needling on hamstring muscle flexibility in normal subjects with tight hamstrings.
Participants and methods
Study designA quantitative research approach using a same- subject experimental design was employed (Hicks 2009). The independent variable (IV) was superficial dry needling, and the depend-ent variable (DV) was hamstring muscle length. The present research was carried out as a pilot study. Each participant acted as his own control.
ParticipantsTwenty normal male participants with tight hamstrings were chosen from a convenience sample. Their ages ranged from 24 to 65 years (mean = 41 years). The participants were volunteers from the present author’s place of work (Central Manchester University Hospitals NHS Foundation Trust, Manchester, UK). Hamstring muscle tightness is defined as a knee extension angle (KEA) of greater than 20° (Davis et al. 2008). The KEA is the degree of knee flexion from terminal knee extension, as measured with a goniometer (Davis et al. 2008).
All participants completed consent forms confirming that they had agreed to take part in the study and undergo acupuncture. They were given an information leaflet 24 h before the study began. Ethical approval was granted by the ethics committee of Coventry University, Coventry, UK.
The exclusion criteria included individuals who had experienced low back pain, pelvic pain, hip pain, knee pain or sciatica in the past 2 years. Anyone who had had any surgical procedures, pain, numbness, weakness, or pins and needles affecting their legs were also excluded. Potential participants who had suffered a knee or ham-string injury in the past 2 years were excluded, as were those who had any contraindications to undergoing acupuncture.

W. Fish
© 2016 Acupuncture Association of Chartered Physiotherapists 35
ProcedureTwo physiotherapists were involved in the procedure. All participants were required to wear shorts so that their lumbar spine and legs were exposed. The research was carried out on the participant’s dominant leg. The KEA was used to measure hamstring muscle flex-ibility. The position for measuring the KEA is illustrated in Figure 1. The measurement was performed before and after acupuncture treatment, and the position was held only long enough to measure the KEA with the goniometer.
Therapist 1 was responsible for stabilizing the non- dominant lower limb with a seat belt. Following this, therapist 1 passively placed the hip into 90° flexion, as measured with the goni-ometer. Therapist 2 then passively extended the knee until the participant reported a strong and tolerable stretch, and no further knee extension was possible because of tissue extensibility. The goniometer reading of the KEA was taken immediately, and the leg was then returned to the anatomical position. The initial KEA measurement was taken by therapist 1. Once the superficial dry needling technique was com-pleted, the KEA was immediately remeasured using the same procedure.
A goniometer was used to measure hip flexion and the KEA. This is the preferred instrument for measuring range of movement (Gajdosik & Bohannon, 1987), and it has been shown to be valid and reliable when measuring knee flexion
and extension (Gogia et al. 1987; Rheault et al. 1988; Brosseau et al. 2001).
Acupuncture point selectionBladder (BL) 37 (Fig. 2) was selected as the acupuncture point employed in the present study. In traditional Chinese medicine, the indications for using BL37 are sciatica, low back pain, occipital headaches, and paralysis and numbness of the lower extremities (Ding 1991). Bladder 37 was chosen because of its location over the hamstring muscle, and also because it shows some correlation with the common MTPs of the hamstrings described by Travell & Simons (1992). Since the participants had no active pathology, BL37 was used because it was reproducible.
Acupuncture techniqueThe acupuncture technique known as superfi-cial dry needling was used. Classic Plus (HMD Europe Ltd, Chipping Norton, Oxfordshire,
Figure 1. Position for measuring knee extension angle.
Figure 2. Location of Bladder (BL) 37 on the posterior aspect of the thigh, 6 cun below BL36, on the line connecting BL36 and BL40 (Ding 1991) (illustration reproduced with the kind permission of Jon Hobbs).
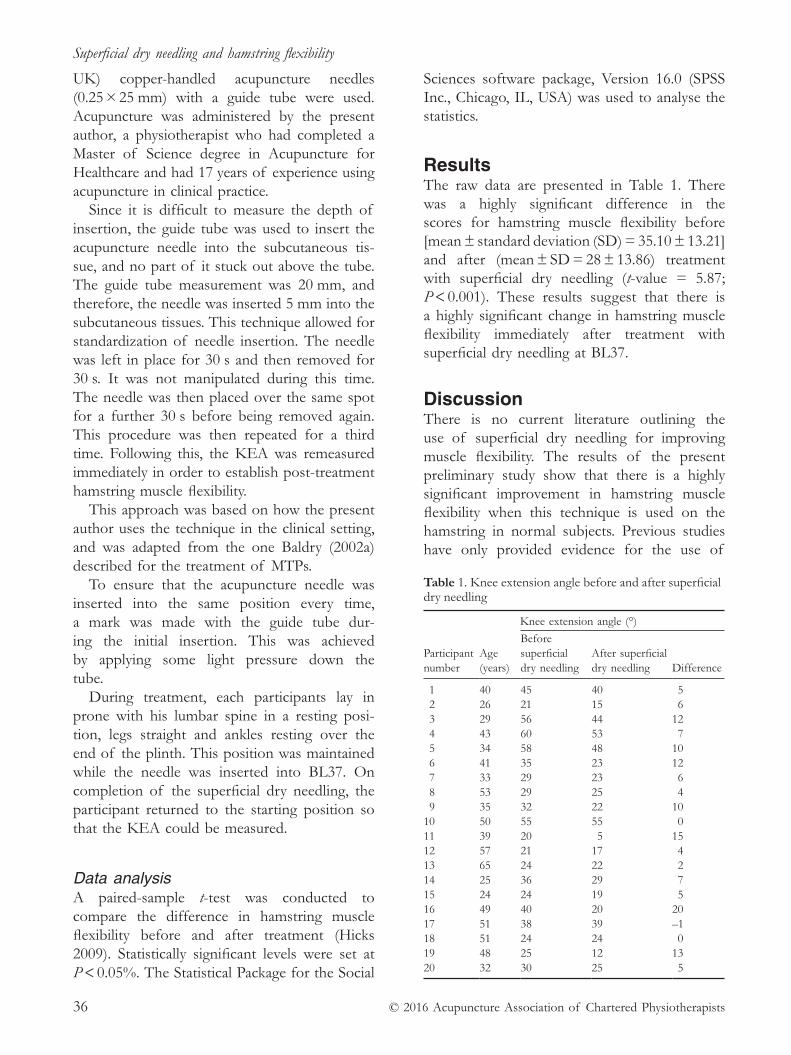
Superficial dry needling and hamstring flexibility
© 2016 Acupuncture Association of Chartered Physiotherapists36
UK) copper- handled acupuncture needles (0.25 × 25 mm) with a guide tube were used. Acupuncture was administered by the present author, a physiotherapist who had completed a Master of Science degree in Acupuncture for Healthcare and had 17 years of experience using acupuncture in clinical practice.
Since it is difficult to measure the depth of insertion, the guide tube was used to insert the acupuncture needle into the subcutaneous tis-sue, and no part of it stuck out above the tube. The guide tube measurement was 20 mm, and therefore, the needle was inserted 5 mm into the subcutaneous tissues. This technique allowed for standardization of needle insertion. The needle was left in place for 30 s and then removed for 30 s. It was not manipulated during this time. The needle was then placed over the same spot for a further 30 s before being removed again. This procedure was then repeated for a third time. Following this, the KEA was remeasured immediately in order to establish post- treatment hamstring muscle flexibility.
This approach was based on how the present author uses the technique in the clinical setting, and was adapted from the one Baldry (2002a) described for the treatment of MTPs.
To ensure that the acupuncture needle was inserted into the same position every time, a mark was made with the guide tube dur-ing the initial insertion. This was achieved by applying some light pressure down the tube.
During treatment, each participants lay in prone with his lumbar spine in a resting posi-tion, legs straight and ankles resting over the end of the plinth. This position was maintained while the needle was inserted into BL37. On completion of the superficial dry needling, the participant returned to the starting position so that the KEA could be measured.
Data analysisA paired- sample t- test was conducted to compare the difference in hamstring muscle flexibility before and after treatment (Hicks 2009). Statistically significant levels were set at P < 0.05%. The Statistical Package for the Social
Sciences software package, Version 16.0 (SPSS Inc., Chicago, IL, USA) was used to analyse the statistics.
ResultsThe raw data are presented in Table 1. There was a highly significant difference in the scores for hamstring muscle flexibility before [mean ± standard deviation (SD) = 35.10 ± 13.21] and after (mean ± SD = 28 ± 13.86) treatment with superficial dry needling (t- value = 5.87; P < 0.001). These results suggest that there is a highly significant change in hamstring muscle flexibility immediately after treatment with superficial dry needling at BL37.
DiscussionThere is no current literature outlining the use of superficial dry needling for improving muscle flexibility. The results of the present preliminary study show that there is a highly significant improvement in hamstring muscle flexibility when this technique is used on the hamstring in normal subjects. Previous studies have only provided evidence for the use of
Table 1. Knee extension angle before and after superficial dry needling
Knee extension angle (°)
Participant number
Age (years)
Before superficial dry needling
After superficial dry needling Difference
1 40 45 40 5 2 26 21 15 6 3 29 56 44 12 4 43 60 53 7 5 34 58 48 10 6 41 35 23 12 7 33 29 23 6 8 53 29 25 4 9 35 32 22 1010 50 55 55 011 39 20 5 1512 57 21 17 413 65 24 22 214 25 36 29 715 24 24 19 516 49 40 20 2017 51 38 39 –118 51 24 24 019 48 25 12 1320 32 30 25 5

W. Fish
© 2016 Acupuncture Association of Chartered Physiotherapists 37
superficial dry needling in reducing pain caused by active MTPs (Macdonald et al. 1983; Edwards & Knowles 2003; Fu et al. 2007).
Neurophysiological versus viscoelastic effectsThere has been a lot of research into the viscoelastic and neurophysiological effects of stretching (Taylor et al. 1997; McNair et al. 2000; Kabrak et al. 2001; Schuback et al. 2004). Viscoelastic effects are believed to occur when a muscle is held in a position over an extended time period, or when it is subjected to repeated movements (McNair et al. 2001). The results of the present study appear to provide more evidence to support the neurophysiological effect of superficial dry needling, as opposed to a viscoelastic one, when improving muscle flexibility. The evidence for a neurophysiological effect is supported by the stretch in this study occurring over a very short duration, and the limb not undergoing repeated movements.
Kabrak et al. (2001) suggested that there might be viscoelastic and a neurophysiological components to muscle flexibility, which could be influenced by both these mechanisms. Those participants in the present study who had tight hamstrings and responded to acupuncture might have had more of a neurophysiological compo-nent limiting their hamstring muscle flexibility than those who did not respond. This finding may have some implications for the manage-ment of patients whose muscle flexibility is not changing. Being able to identify the different mechanisms involved might help individuals for whom a stretching programme does not bring about the required changes in muscle flexibility. Kabrak et al. (2001) hypothesized that the neural system may play a greater role in regulating the intrinsic viscoelastic properties, and that there is likely to be interdependence between the neural and muscular influences.
One participant in the present study (number 17) experienced a negative change in hamstring muscle flexibility following acupuncture (Table 1). This may have occurred as a result of a measurement error during the use of the goni-ometer. Goniometer measurement error has
been found to be as much as 3.76°, even when carried out by an experienced physiotherapist (Unver et al. 2009). It has also been suggested that the long levers of the knees may cause occasional errors in reliability when a universal goniometer is used (Brosseau et al. 2001).
Possible mechanisms for the improvement of muscle flexibilityThe results of the present study suggest that the most likely mechanism is a local neurophysio-logical change in the muscle or a central one within the spinal cord. When acupuncture is used to treat pain and MTPs, there can be local, segmental and supraspinal effects (Baldry 2002a; Bradnam- Roberts 2007). The mechanism by which acupuncture is hypothesized to improve pain may explain the changes seen in hamstring muscle flexibility in this study.
Baldry (2002a) described the mechanism of how superficial dry needling works in the treatment of MTPs. Stimulation of Αδ nerve fibres triggers the release of opioid peptides from enkephalinergic inhibitory interneurons in the dorsal horn. These peptides then inhibit the intradorsal horn transmission of nociceptive information conveyed to the cord via group IV sensory afferents from the MTPs. The Αδ fibres are small- diameter fibres that respond to high- intensity mechanical stimulus. Baldry (2002b) also suggested that there is an indirect supraspinal link to the enkephalinergic inhibi-tory interneurons via the neospinothalamic pathway, which has connections to the sero-tonergic descending inhibitory systems. These also project to the enkephalinergic inhibitory interneurons. This indirect link requires more- intense and longer stimulation to activate the supraspinal mechanisms (Bradnam- Roberts 2007). In the present study, the stimulation was brief and not intense, and therefore, it is not likely that the supraspinal mechanisms were responsible for changes in flexibility.
This mechanism describes changes in the dorsal horn. It primarily refers to pain reduc-tion, which may have had some influence over the end- of- range flexibility of the hamstring. However, given the present results, it is possible

Superficial dry needling and hamstring flexibility
© 2016 Acupuncture Association of Chartered Physiotherapists38
that the same mechanism responsible for a reduction in pain may also affect the excitability of the neurogenic system, and ultimately, the flexibility of the muscle.
Limitations and future researchThe present research has some limitations. First, it was conducted as a pilot and the sample size was small, which reduces the power of the study, and caution should be taken when considering the statistical significance of the intervention. Secondly, the light pressure down through the guide tube to mark the acupuncture point was not standardized in the procedure. It is possible that this might have had some influence over the present results: Huguenin (2004) suggested that muscle penetration with superficial dry needling is not always necessary to produce an analgesic effect. Thirdly, the present research was conducted on the hamstring muscles of normal adult male participants, and therefore, any conclusions can only be made for this population. The results of this study cannot be generalized to different muscle groups or other populations presenting with hamstring pathol-ogy. Fourthly, there might have been some bias since therapist 1, who measured the KEA, was not blinded to the study. Finally, this research also only investigated the initial changes in ham-string muscle flexibility, and therefore, conclu-sions cannot be made regarding any long- term changes that might occur.
Further research is required into the effects of superficial dry needling on muscle flex-ibility. This should initially include studies with larger sample sizes and trials to investigate the effects of the technique over a prolonged time period. If this provides further evidence to support an improvement in muscle flexibility, then a comparison of the changes in flex-ibility between common stretching techniques and superficial dry needling would need to be investigated.
ConclusionsThe aim of the present study was to determine whether superficial dry needling would change
hamstring muscle flexibility. The results of this research provide statistically significant evidence to support the use of this technique to improve hamstring muscle flexibility without stretching.
Clinically, this is an important finding since there is no current evidence to support the use of superficial dry needling to improve muscle flexibility. If further research demonstrates the effectiveness of superficial dry needling on muscle flexibility, it might become a technique that is routinely included in future preventative and rehabilitation programmes.
ReferencesAlvarez D. J. & Rockwell P. G. (2002) Trigger points:
diagnosis and management. American Family Physician 65 (4), 653–660.
Baldry P. (2002a) Management of myofascial trigger point pain. Acupuncture in Medicine 20 (1), 2–10.
Baldry P. (2002b) Superficial versus deep dry needling. Acupuncture in Medicine 20 (2–3), 78–81.
Birch S. (2003) Trigger point–acupuncture point cor-relations revisited. The Journal of Alternative and Complementary Medicine 9 (1), 91–103.
Bradnam- Roberts L. (2007) A physiological underpin-ning or treatment progression of Western acupunc-ture. Journal of the Acupuncture Association of Chartered Physiotherapists 2007 (Autumn), 25–33.
Brosseau L., Balmer S., Tousignant M., et al. (2001) Intra- and intertester reliability and criterion validity of the parallelogram and universal goniometers for measuring maximum active knee flexion and extension of patients with knee restrictions. Archives of Physical Medicine and Rehabilitation 82 (3), 396–402.
Davis D. S., Quinn R. O., Whiteman C. T., Williams J. D. & Young C. R. (2008) Concurrent validity of four clinical tests used to measure hamstring flexibility. The Journal of Strength and Conditioning Research 22 (2), 583–588.
Ding L. (1991) Acupuncture, Meridian Theory and Acupuncture Points. Foreign Languages Press, Beijing.
Edwards J. & Knowles N. (2003) Superficial dry needling and active stretching in the treatment of myofascial pain – a randomised control trial. Acupuncture in Medicine 21 (3), 80–86.
Fu Z.- H., Wang J.- H., Sun J.- H., Chen X.- Y. & Xu J.- G. (2007) Fu’s Subcutaneous Needling: possible evidence of the subcutaneous connective tissue in acupuncture. The Journal of Alternative and Complementary Medicine 13 (1), 47–51.
Gajdosik R. L. & Bohannon R. W. (1987) Clinical meas-urement of range of movement: review of goniometry
W. Fish
© 2016 Acupuncture Association of Chartered Physiotherapists 39
emphasizing reliability and validity. Physical Therapy 67 (12), 1867–1872.
Gogia P. P., Braatz J. H., Rose S. J. & Norton B. J. (1987) Reliability and validity of goniometric measurements at the knee. Physical Therapy 67 (2), 192–195.
Hicks C. M. (2009) Research Methods for Clinical Therapists: Applied Project Design and Analysis, 5th edn. Churchill Livingstone, Edinburgh.
Huguenin L. K. (2004) Myofascial trigger points: the cur-rent evidence. Physical Therapy in Sport 5 (1), 2–12.
Kabrak B. J., Laskowsi E. R., Smith J., Stuart M. J. & Wong G. Y. (2001) Neurophysiologic influences on hamstring flexibility. Clinical Journal of Sport Medicine 11 (4), 241–246.
Kalichman L. & Vulfsons S. (2010) Dry needling in the management of musculoskeletal pain. Journal of the American Board of Family Medicine 23 (5), 640–646.
Macdonald A. J., Macrae K. D., Master B. R. & Rubin A. P. (1983) Superficial acupuncture in the relief of chronic low back pain. Annals of the Royal College of Surgeons of England 65 (1), 44–46.
McHugh M. P., Kremenic I. J., Fox M. B. & Gleim G. W. (1998) The role of mechanical and neural restraints to joint range of motion during passive stretch. Medicine and Science in Sports and Exercise 30 (6), 928–932.
McNair P. J., Dombroski E. W., Hewson D. J. & Stanley S. N. (2001) Stretching at the ankle joint: viscoelastic responses to holds and continuous passive motion. Medicine and Science in Sports and Exercise 33 (3), 354–358.
O’Hora J., Cartwright A., Wade C. D., Hough A. D. & Shum G. L. K. (2011) Efficacy of static stretching and proprioceptive neuromuscular facilitation stretch on hamstrings length after a single session. The Journal of Strength and Conditioning Research 25 (6), 1586–1591.
Rheault W., Miller M., Nothnagel P., Straessle J. & Urban D. (1988) Intertester reliability and concurrent validity of fluid- based and universal goniometers for active knee flexion. Physical Therapy 68 (11), 1676–1678.
Ryan E. D., Herda T. J., Costa P. B., et al. (2010) Viscoelastic creep in the human skeletal muscle–tendon unit. European Journal of Applied Physiology 108 (1), 207–211.
Schuback B., Hooper J. & Salisbury L. (2004) A com-parison of a self- stretch incorporating proprioceptive neuromuscular facilitation components of a therapist- applied PNF- technique on hamstring flexibility. Physiotherapy 90 (3), 151–157.
Stux G., Berman B. & Pomeranz B. (2003) Basics of Acupuncture, 5th edn. Springer- Verlag, Berlin
Taylor D. C., Brooks D. E. & Ryan J. B. (1997) Viscoelastic characteristics of muscle: passive stretching versus muscular contractions. Medicine and Science in Sports and Exercise 29 (12) 1619–1624.
Thacker S. B., Gilchrist J., Stroup D. F. & Kimsey C. D., Jr (2004) The impact of stretching on sports injury risk: a systematic review of the literature. Medicine and Science in Sports and Exercise 36 (3), 371–378.
Travell J. G. & Simons D. G. (1992) Myofascial Pain and Dysfunction: The Trigger Point Manual, Vol. 2 – The Lower Extremities. Williams & Wilkins, Baltimore, MD.
Unver B., Karatosun V. & Bakirhan S. (2009) Reliability of goniometric measurements of flexion in total knee arthroplasty patients: with special reference to the body position. Journal of Physical Therapy Science 21 (3), 257–262.
Wayne Fish graduated from Auckland University of Technology, Auckland, New Zealand, with a BHSc in Physiotherapy in 1997. He has extensive experi-ence in musculoskeletal physiotherapy and regularly uses acupuncture as part of his clinical practice. Wayne has developed a special interest in the effect of acupuncture on the musculoskeletal system, and specifically, how it may improve muscle flexibility. He has extensive postgraduate qualifications and completed an MSc in Manipulative Physiotherapy in 2003 and an MSc in Acupuncture in Healthcare in 2013.


© 2016 Acupuncture Association of Chartered Physiotherapists 41
Acupuncture in Physiotherapy, Volume 28, Number 1, Spring 2016, 41–48
MERIDIAN MASTERCLASS
The Heart meridian: the hand Shao Yin channel
J. WoodPrivate Practice, Sheffield, UK
AbstractThe Heart meridian consists of nine points on the arm, and it can influence both physical and mental aspects of health. In traditional Chinese medicine (TCM), the Heart is con-sidered to control the blood vessels, and therefore, the energy levels of the former are reflected by the state of the latter. Moreover, the inner links of the Heart are as important as its superficial course. The “emotional mind” (which is called the limbic system in Western medicine) is intimately linked with the Heart, both as an organ and a meridian. The ability to positively influence the mental/emotional aspect of a patient’s condition can add a valu-able additional level to overall therapeutic input. Therefore, an enhanced understanding of the Heart meridian is clearly of benefit to the physiotherapist.
Keywords: acupuncture, hand Shao Yin channel, Heart meridian, traditional Chinese medicine.
IntroductionThe Heart meridian is a yin channel that is paired with the yang Small Intestine meridian. In traditional Chinese medicine (TCM), the Heart is considered to control the blood vessels, and therefore, the energy levels of the former are reflected by the state of the latter. Moreover, the inner links of the Heart are as important as its superficial course.
When Heart energy, or Heart- Qi (in Western medical terms, Qi effectively means “energy” or “metabolism”), is strong, the Blood will also be in good condition. This will be reflected by a full and regular pulse. However, if the Heart- Qi is weak, the pulse will be feeble and irregular. Therefore, the Heart is believed to dominate the blood vessels, and furthermore, those vessels are
said to house the Mind. According to Maciocia (1997, p. 72): “The Heart’s function of housing the Mind depends on an adequate nourish-ment from the Blood and, conversely, the Heart’s job of governing Blood depends on the Mind.”
Therefore, the “emotional mind” (which is called the limbic system in Western medicine) is intimately linked with the Heart, both as an organ and a meridian (Damasio 2000). The effect of the emotions on the body via the functions of the Heart is nicely illustrated in the “Simple Questions” section of the Huangdi Neijing. This ancient Chinese textbook, which is often referred to as The Yellow Emperor’s Classic of Medicine, describes how sadness affects the lungs via the Heart: “Sadness makes the Heart cramped and agitated; this pushes towards the lungs’ lobes, the Upper Burner becomes obstructed, Nutritive and Defensive Qi cannot circulate freely [. . .]” (quoted by Maciocia 2007, pp. 214–215).
Correspondence: John Wood, Clinical Director/Specialist Physiotherapist, Sheffield Physiotherapy, 476 Ecclesall Road, Sheffield S11 8PX, UK (e- mail: [email protected])
The Heart meridian
© 2016 Acupuncture Association of Chartered Physiotherapists42
Functions of the HeartIn TCM, the Heart is considered to be the most important of all the internal organs. According to Maciocia (1997, p. 71, author’s emphasis), again quoting the “Simple Questions” section of the Huangdi Neijing: “The ‘Spiritual Axis’ in chapter 71 says: ‘The Heart is the Monarch of the 5 Yin organs and the 6 Yang organs and it is the residence of the mind (Shen).’”
The functions of the Heart are to:
• govern the Blood;
• control the blood vessels;
• manifest in the complexion;
• house the mind;
• open into the tongue; and
• control sweat.
Governing the Blood and blood vessels, and manifesting in the complexionThe Heart and blood vessels, and the blood circulating within these, are clearly intercon-nected. Since there are many blood vessels on the face, the strength of the Heart- Qi and the amount of Blood circulating will be indicated by changes in both the pulse and the com-plexion. According to the “Simple Questions” section of the Huangdi Neijing: “The glory of the Heart is manifested on the face, since the Blood fills up the Vessels” (Cheng 1999, p. 27). Therefore, vigorous Heart- Qi and ample blood result in a strong and regular pulse, and a rosy complexion. Conversely, if the Heart- Qi (i.e. energy or metabolism) and Blood are deficient, then the pulse will be weak and thready, and the complexion pale.
Housing the Mind/SpiritTraditional Chinese medicine holds that the Mind/Spirit (thinking) is related to the five yin organs, and principally, to the physiological functions of the Heart. However, Shen, the Chinese word for Spirit, has yet another con-notation, a subtle and hard- to- define quality of “life”, “flourishing” or “glitter” that can be observed in health (Maciocia 2007). Therefore, “to have the spirit is the splendor of life, to lose the spirit is annihilation” (Hicks et al. 2010, p. 288).
Thus, if the Heart is strong and the mind healthy, then thinking, memory, and the state of a person’s consciousness and insight will be good. He or she will also sleep soundly, and his or her intelligence and wisdom will be optimal. However, if the Heart becomes affected and the mind weak, a person will not think clearly, his or her memory and insight will be poor, and sleep will be restless. The individual’s intel-ligence will dwindle, and he or she will act in a muddled and unwise fashion.
When someone suffers emotional stress, the first effect on their body is that the proper cir-culation and direction of Qi is impaired. Each emotion is thought to be unique in its effect on the circulation of Qi.
Again according to the “Simple Questions” section of the Huangdi Neijing: “Anger makes Qi rise, joy slows down Qi, sadness dissolves Qi, fear makes Qi descend . . . shock scatters Qi . . . pensiveness knots Qi” (Maciocia 2007, p. 211).
From personal experience, we know that our thoughts are intimately connected to our feel-ings. We also know that we can have a feeling without consciously being aware of the thought with which it is associated. In Western medi-cine, we call this process of feeling sensations in the body associated with emotions the “vis-ceralization of cognition”, and it is thought to be related to the activity of the insular cortex in the brain, an area that is considered to be part of the limbic system or “emotional mind” (Gu et al. 2013).
From a Western perspective, we also under-stand that stressful situations activate the sym-pathetic nervous system (triggering the fight- or- flight response), and this stimulation will reduce blood flow to the viscera. Ongoing stress can result in adrenal fatigue, and may also chronically affect blood flow through the organs, impair-ing their function. In TCM terms, this would amount to a reduction in Essence. The “Simple Questions” section of the Huangdi Neijing states that: “When the Stomach and Intestines are coordinated the 5 Yin organs are peaceful, Blood is harmonized and mental activity is stable. The mind derives from the refined Essence of water and food” (Maciocia 2007, p. 198).

J. Wood
© 2016 Acupuncture Association of Chartered Physiotherapists 43
Emotional stress will affect Qi first, which is what we feel as the emotion to some extent, and then weaken Essence. The state of the Qi and the Blood of each organ can influence the Mind or Spirit, and conversely, alterations of Mind or Spirit can influence the smooth flow of Qi and Blood. This means that the Mind/Spirit lies at the deepest level of an organ’s Qi (energy/metabolism). Therefore, there is a recognition of the interconnectedness between the mind and the body in TCM. When we use acupuncture, it is believed that the acupuncture points are places of entry or portals for Qi, and therefore, Spirit.
Recognizing problems at the Mind/Spirit levelWe can recognize problems at the Mind/Spirit level by observing:
• the body (posture, gestures and vitality);
• the Mind (beliefs, values, language, thinking, flexibility and capabilities); and
• the Spirit (identity, sense of purpose, comfort with self, internal stillness and equanimity) (Hicks 2015).
Another kind of painThroughout the ages, poets and songwriters have pontificated voluminously on the sorrow of a broken heart, but they have remained largely silent on the agony of a stubbed toe.
Patients frequently find that emotional pain is more troubling than physical pain. Emotions such as depression, sadness and anxiety are common sequelae to the pain of a physical injury, particularly in chronic conditions. Patients may often feel that there are “things they can’t talk about”. These strong emotions cause Qi to stagnate, and in time, the Blood also stagnates. Talking can help to alleviate this, as can acu-puncture to Spleen 10, Liver 3, Bladder 17 and Pericardium (PC) 4.
Therefore, it is said in the Huangdi Neijing that: “The Heart is in control of the blood ves-sels and the spirit resides in the blood vessels. A hollowness of the energy in the Heart will cause the emotion of sadness [. . .]” (Lu 1972, quoted in Hicks et al. 2010, p. 82).
Emotions become causes of disease only when these are excessive or prolonged, or both. In TCM, emotions are mental stimuli that disturb the Mind/Spirit, which alters the Qi and Blood, and through these, the harmony of the internal organs. Conversely, and this is an important feature of TCM, the condition of the organs affects our emotional state. The Huangdi Neijing illustrates such a reciprocal relationship: “The Heart’s fear, anxiety and pensiveness injure the mind . . . the Spleen’s worry injures the intellect . . .” (Maciocia 2007, p. 209, author’s emphasis). Conversely, it later says: “If Liver- Blood is deficient there is fear, if it is in excess there is anger . . . if Heart- Qi is deficient there is sadness, if it is in excess there is manic behavior . . .” (Maciocia 2007, p. 210, author’s emphasis).
The Huangdi Neijing describes five emotions and the specific yin organs that these affect (Maciocia 2007):• anger and the Liver;
• joy and the Heart;
• pensiveness and the Spleen;
• worry and the Lungs; and
• fear and the Kidney.
In summary, it is worth considering that Huangdi Neijing states that: “When one discusses medical treatment one must keep in mind first of all the patient’s Spirit. [. . .] In order to make acupunc-ture thorough and effective one must first treat the Spirit” (Lu 1972, quoted in Hicks et al. 2010, p. 15).
Opening into the tongueIn TCM, the tongue is considered to be the “offshoot” of the Heart, and via this connec-tion, it dominates the sense of smell and speech. When the Heart functions normally, the tongue will be rosy, moist and lustrous, the sense of taste will be normal, and the tongue will move freely. Conversely, disorders of the Heart will be reflected in the condition of the tongue, and stagnation of Heart- Blood may give it a dark, purplish colour (Cheng 1999).
Controlling sweatThe Heart is related to sweat since the former governs Blood, and this has a relationship of

The Heart meridian
© 2016 Acupuncture Association of Chartered Physiotherapists44
mutual interchange with other bodily fluids, including sweat.
The course of the Heart meridianThe Heart meridian originates in the organ itself and emerges through the “heart system”, i.e. the tissues connecting the heart with other internal organs (Fig. 1). It then travels down-wards, passing through the diaphragm to con-nect with the small intestine. One branch of the “heart system” ascends to the throat and eye, and another enters the lung and emerges at the axilla. From the axilla, it follows the brachial artery to the elbow, and then continues down the inner aspect of the arm next to the ulnar artery before finishing at the little finger. Daniel Keown (2014, p. 138) made an interesting observation regarding the connection between the Heart meridian and the eye:
“Like a snail’s eye emerging unblinking from its shell, the brain actually grows into the eye to form the retina. As a result the back of your eye (retina) is actually brain [. . .]
“This mingling between Heart and brain is why the eyes tell so much about a person, for when you look into their eyes you really are peering into their soul: that twinkle in their eye is the nourishment of their mind by their Heart.”
Clinical application of the meridian and acupuncture pointsFor the purposes of the present paper, infor-mation pertaining to both TCM and Western medical acupuncture (WMA) will be discussed.
Heart 3: Shao Hai, “Lesser Sea”Heart (HT) 3 is the He- Sea point of the Heart meridian, which indicates that it is where the Qi of this channel collects before going deeper into the body. It is found at the midpoint of the line connecting the medial end of the transverse cubital crease and the medial epicondyle of the humerus when the elbow is flexed. According to TCM, HT3 “[c]alms the Shen, activates the merid-ian, transforms Phlegm, clears Heat, benefits the arm, [and] alleviates pain” (ACATCM 2015a).
Physiotherapists most commonly use this point in the treatment of medial epicondylitis (golfer’s elbow). From a TCM perspective, this condition is normally considered to be the result of painful obstruction (Bi) syndrome. In such cases, excessive exposure to Wind, Cold or Dampness results in obstruction of the circula-tion of Qi, and possibly Blood, in the Heart meridian.
The ancient Chinese believed that the muscles were arranged in channels in a manner similar to a string of sausages (Cheng 1999; Langevin & Yandow 2002). These “muscle channels” are similar to the Anatomy Trains described by Tom Myers (2013), broadly following the course of the main meridians, and contribut-ing to the general circulation of Qi and Blood. The obstruction created by a pathogenic factor only affects the channels, and does not enter into the internal organs. The stagnation of Qi in a “muscle channel” will lead to muscle ache and distension, while Blood Stasis will cause pain.
The aim of the treatment with HT3 is sim-ply to expel the pathogenic factors that have invaded the main Heart meridian and the Heart “muscle channel”, and eliminate the resulting local stagnation of Qi and Blood (Maciocia 2006).
Heart 5: Tong Li, “Connecting Interior”Located on the palmar aspect of the forearm, this point is found on the radial side of the tendon of the flexor carpi ulnaris muscle, 1.0 cun above the transverse crease of the wrist. Heart 5 is the Luo- Connecting point of the Heart meridian, and its function is to calm the Shen, benefit the tongue and regulate heartbeat (ACATCM 2015b).
Luo- Connecting points are where a separate channel splits off from the main flow and con-nects with a yin or yang paired meridian. In the case of HT5, this is the Small Intestine merid-ian, and as discussed above, the Connecting Channel links the Heart meridian with the eye and the tongue. It is through the Connecting Channels that nutritive and defensive Qi, and Blood are spread in all directions, permeating and irrigating the internal organs. Most of the

J. Wood
© 2016 Acupuncture Association of Chartered Physiotherapists 45
Figure 1. The course of the Heart meridian, the hand Shao Yin channel (illustration reproduced with the kind permission of Jon Hobbs).

The Heart meridian
© 2016 Acupuncture Association of Chartered Physiotherapists46
stagnation in the body actually occurs in the Connecting Channels because these act like a net or web that easily “catches” pathogenic factors, or in which Qi and/or Blood become stagnant (Maciocia 2006). From a WMA perspective, we might interpret this as describing the fascial web of loose connective tissues enveloping every-thing under the skin.
Ye Tian Shi stated that: “In the beginning of a disease the pathogenic factor is at the Qi level in the main channel, in the late stages it enters the Blood level in the Connecting Channels” (Maciocia 2006, p. 253). From a WMA perspec-tive, the Connecting Channels where Blood can become stagnant probably describe the connec-tive tissue planes that run through a muscle. Disharmonized and stagnant Qi results in pain, and severe chronic pain (e.g. that seen in condi-tions such as complex regional pain syndrome) is often associated with Blood Stasis within the Connecting Channels.
When a Main Channel is diseased, we can puncture the Yuan Point of the affected merid-ian; for example, Small Intestine 4 and the Luo- Connecting point of its yin/yang paired meridian, i.e. HT5. As physiotherapists, we see a lot of patients suffering from pain affecting the Small Intestine meridian, so this can be a useful combination. The Connecting Channels occupy the bodily cavities in a net- like way and are also found on the surface of the body. For this rea-son, pathogenic factors on one side can move and cause symptoms on the other in a manner that is not normally possible with the Main Channels. In fact, the Luo- Connecting points are often needled on the opposite side to the symptoms; this facilitates equalization between the right and the left sides, and therefore, helps to reduce pain further (Maciocia 2006).
Heart 6: Yin Xi, “Yin Cleft”Also located on the palmar aspect of the fore-arm and on the radial side of the tendon of the flexor carpi ulnaris muscle, this point is found 0.5 cun above the transverse crease of the wrist. The Xi- Cleft point of the Heart meridian, HT6 “[c]alms the Shen, clears deficiency Heat, nourishes Heart Yin [and] stops night sweating” (ACATCM 2015c).
The word “Xi” means a small gap or hole. From the TCM perspective, as energy moves up the Heart meridian, it goes deeper into the body at this point, resembling a mountain stream that disappears underground for a while. If there is some blockage further along the channel, this is the point at which you might find energy “backing up” because it cannot drain effectively (Clogstoun- Willmott 2015a). For this reason, HT6 and the Xi- Cleft points on other meridians are very effective for acute painful conditions since these can be used to restore the flow of Qi and Blood.
Heart 6 can also be a useful point for acute emotional traumas, such as severe shock. Shock will tend to freeze Qi and the Spirit/Mind, stop-ping the natural movement of Qi and causing stagnation. The sudden depletion of Heart- Qi makes the heart smaller, and may lead to palpi-tations, breathlessness and insomnia (Lau 2010). It is as if the shock has scattered the Qi, and using HT6 will help it to accumulate again. Clinically, we may find that, although patients who have suffered from a significant trauma have recovered physically, they can remain in a state of mild shock. Heart 6 may be of benefit in such cases. Hollifield (2011) conducted a review of the literature related to the use of acupuncture for post- traumatic stress disorder (PTSD). He stated that: “Conceptual, clinical, and biological data support the potential efficacy of acupuncture for PTSD” (Hollifield 2011, p. 769). However, this review documented some equivocal outcomes within the literature, which demonstrates that there is a need for further research in this area (Hollifield 2011).
Heart 7: Shen Men, “Spirit Gate”Located at the ulnar end of the transverse crease of the wrists, in the depression on the on the radial side of the tendon of the flexor carpi ulnaris muscle, HT7 is the Yuan- Source and Shu- Stream point of the Heart meridian. It pacifies the Heart, calms the Mind/Spirit, and tonifies and regulates the Blood and Qi of the Heart (ACATCM 2015d).
It is probably the most popular, and there-fore, most frequently used point on the Heart meridian. As its Chinese name suggests, this is

J. Wood
© 2016 Acupuncture Association of Chartered Physiotherapists 47
the point that has the most influence upon the Spirit or Mind from a Western perspective. The word “Men” means “gate”, and needling HT7 is said to help open the “Spirit Gate” so that someone is more open to outside influences and can let out the negative emotions. It can be used in combination with PC6, which is another point that is said to help people to open them-selves up (Clogstoun- Willmott 2015b). When individuals have Qi stagnation that is affecting them emotionally, HT7 can help to calm and steady them so that they can take a more meas-ured approach to life.
From a TCM perspective, puncturing the Yuan- Source points stimulates the vital energy of the meridian, and regulates the functional activities of the internal organs. This is a way to treat the root causes of diseases, which is particularly important in the case of the Heart meridian since this organ plays such an important role in the function of all the oth-ers. In a way, HT7 might be considered to be the axis of the Mind/Body connection since its role in harmonizing these two aspect is so pivotal. Research into HT7 has shown that it has a sedative effect on the sympathetic nerv-ous system, as measured by heart rate variability (HRV), and that this translates into a beneficial effect on sleep by ameliorating insomnia (Chen et al. 2010). A recent study into the effects of electrical stimulation of HT7 during a surgical procedure to reduce paediatric “emergence agi-tation” following surgery demonstrated that this was significantly lower (31.7 vs 56.7, P = 0.010) when a patient who underwent the treatment was compared with a control subject who received no stimulation (Hijikata 2015).
ConclusionsAs both an organ and a meridian, the Heart is one of the most interesting and intriguing parts of TCM theory. At its core is the concept that, for any organ or part of the body to function optimally, and resist degenerative and disease processes, then it must receive a generous flow of well- oxygenated blood; any less than this and trouble will ensue at some point. In this regard, the close link that TCM makes between the
Heart and the Mind seems less alien because, in an emergency, the brain thirstily receives blood at the expense of virtually all other areas of the body.
The literature on the effects of needling points on the Heart meridian lends support to the notion that this is a clinically effective way of treating emotional issues. With advances in science, our ability to measure the effects of acupuncture on cerebral blood flow and HRV using functional magnetic resonance imaging has given research into this area a fresh impetus and greatly improved its validity (Napadow et al. 2005).
For physiotherapists, the ability to positively influence the mental/emotional aspect of a patient’s condition can add a valuable addi-tional level to their overall therapeutic input. Therefore, an enhanced understanding of the Heart meridian is clearly of benefit to the thera-pist, and the aim of the present article has been to help practitioners to achieve this outcome.
ReferencesAlberta College of Acupuncture and Traditional Chinese
Medicine (ACATCM) (2015a) HT- 3 (Shao Hai). [WWW document.] URL http://www.acatcm.com/heart- meridian- hand- shao- yin- points/343- ht- 3- shao- hai
Alberta College of Acupuncture and Traditional Chinese Medicine (ACATCM) (2015b) HT- 5 (Tong Li). [WWW document.] URL http://www.acatcm.com/heart- meridian- hand- shao- yin- points/341- ht- 5- tong- li
Alberta College of Acupuncture and Traditional Chinese Medicine (ACATCM) (2015c) HT- 6 (Yin Xi). [WWW document.] URL http://www.acatcm.com/heart- meridian- hand- shao- yin- points/340- ht- 6- yin- xi
Alberta College of Acupuncture and Traditional Chinese Medicine (ACATCM) (2015d) HT- 7 (Shen Men). [WWW document.] URL http://www.acatcm.com/heart- meridian- hand- shao- yin- points/339- ht- 7- shen- men
Chen J.- Q., Wu J.- X., Li T., et al. (2010) Study on the effect of needling Shenmen (HT7) on heart rate variability time domain indices. Lishizhen Medicine and Materia Medica Research 2010 (8), 139.
Cheng X. (1999) Chinese Acupuncture and Moxibustion. Foreign Languages Press, Beijing.
Clogstoun- Willmott J. (2015a) Xi- Cleft Points. [WWW document.] URL http://www.acupuncture- points.org/xi- cleft.html
Clogstoun- Willmott J. (2015b) Heart 7. Shen Men: Spirit Gate. [WWW document.] URL http://www.acupuncture- points.org/heart- 7.html

The Heart meridian
© 2016 Acupuncture Association of Chartered Physiotherapists48
Damasio A. (2000) The Feeling of What Happens: Body, Emotion and the Making of Consciousness. Vintage Books, London.
Gu X., Hof P. R., Friston K. J. & Fan J. (2013) Anterior insular cortex and emotional awareness. Journal of Comparative Neurology 521 (15), 3371–3388.
Hicks A. (2015) Top 10 Tips for Treating the Spirit: Why Your Treatment on the Shen May Not Be Working and How to Sort It Out. [WWW video.] URL: http://acupunctureprofessional.com
Hicks A., Hicks J. & Mole P. (2010) Five Element Constitutional Acupuncture, 2nd edn, Churchill Livingstone, Edinburgh.
Hijikata T., Mihara T., Nakamura N., et al. (2015) Electrical stimulation of the heart 7 acupuncture site for pre-venting emergence agitation in children: a randomised controlled trial. European Journal of Anaesthesiology 33: 1–8. DOI: 10.1097/EJA.0000000000000379.
Hollifield M. (2011) Acupuncture for posttraumatic stress disorder: conceptual, clinical, and biological data sup-port further research. CNS Neuroscience and Therapeutics 17 (6), 769–779.
Keown D. (2014) The Spark in the Machine: How the Science of Acupuncture Explains the Mysteries of Western Medicine. Singing Dragon, London.
Langevin H. M. & Yandow J. A. (2002) Relationship of acupuncture points and meridians to connective tissue planes. The Anatomical Record 269 (6), 257–265.
Lau S. (2010) Qi Stagnation. [WWW document.] URL http://www.simonlaucentre.co.uk/blog/2010/07/27/qi- stagnation/
Lu H. (1972) A Complete Translation of the Yellow Emperor’s Classic of Internal Medicine (Nei Jing and Nan Jing). Academy of Oriental Heritage, Vancouver.
Maciocia G. (1997) The Foundations of Chinese Medicine: A Comprehensive Text for Acupuncturists and Herbalists. Churchill Livingstone, Edinburgh.
Maciocia G. (2006) The Channels of Acupuncture: Clinical Use of the Secondary Channels and Eight Extraordinary Vessels. Churchill Livingstone, Edinburgh.
Maciocia G. (2007) The Practice of Chinese Medicine: The Treatment of Diseases with Acupuncture and Chinese Herbs, 2nd edn. Churchill Livingstone, Edinburgh.
Myers T. W. (2013) Anatomy Trains: Myofascial Meridians for Manual and Movement Therapists, 3rd edn. Churchill Livingstone, Edinburgh.
Napadow V., Dhond R. P., Purdon P., et al. (2005) Correlating acupuncture FMRI in the human brainstem with heart rate variability. In: 27th Annual International Conference of the Engineering in Medicine and Biology Society, 2005 (ed. IEEE- EMBS), pp. 4496–4499. IEEE, New York, NY.
John Wood qualified as a physiotherapist in 1988, and completed a 2- year part- time diploma in acupuncture in 1998. He has been involved in training physiotherapists in how to use acupuncture as part of their practice since 1999, and teaches both foundation and continuing professional development courses. John is an advanced member of AACP and an accredited tutor, as well as being the regional representative for the North East and serving on the Education, Training and Research Committee. He is currently the clinical director and lead therapist of a private clinic in Sheffield. John is passionate about helping physiotherapists to integrate acupuncture into their clinical practice effectively, so that it enhances both the clinical outcomes that they achieve and the patient’s therapeutic experience.

© 2016 Acupuncture Association of Chartered Physiotherapists 49
Correspondence: Rachel Kyte MSc PGCertHE MCSP FHEA, Senior Lecturer, Institute of Health and Society, University of Worcester, Henwick Grove, Worcester WR2 6AJ, UK (e- mail: [email protected])
Acupuncture in Physiotherapy, Volume 28, Number 1, Spring 2016, 49–56
MERIDIAN MASTERCLASS
The Bladder meridian: the foot Tai Yang channel
R. KyteInstitute of Health and Society, University of Worcester, Worcester, UK
AbstractThis article describes the path and anatomy of the Bladder meridian. It explores the acu-puncture points that are commonly used by physiotherapists, and explains both the Western medical and traditional Chinese medicine (TCM) rationales behind the indications for these points. The concept of Back- Shu points is analysed, and key safety considerations are highlighted. This masterclass draws on current research to highlight parallels between the Western medical and TCM philosophical perspectives.
Keywords: acupuncture, Back- Shu points, Bladder meridian, foot Tai Yang channel, traditional Chinese medicine.
IntroductionWith a total of 67 points, the Bladder merid-ian is the longest in the body. It begins at the inner canthus of the eye, then travels up and over the top of the head before descending via the dorsal surface of the trunk and lower limbs, and terminating on the outer border of the little toe (Fig. 1). The Bladder meridian is frequently used by physiotherapists in the treat-ment of headaches, spinal pain and lower limb disorders because this channel goes though the paraspinal and posterior lower limb muscula-ture. However, points on the channel are not only useful from a musculoskeletal perspective, but can also be used for a range of treatments, including those for eye disorders and turn-ing breach babies (Deadman et al. 2007). The present paper provides an overview of the Bladder meridian and its key points from both
the Western medical and traditional Chinese medicine (TCM) perspectives, drawing on cur-rent literature to explore the links between these two philosophies.
From a Western perspective, the bladder is simply a reservoir for storing and excreting urine. However, in TCM, the Bladder is not only responsible for collecting and excreting urine, but also for its production (Kaptchuk 2000). The Bladder is said to receive fluids from the Small Intestine and transform these into urine using yang Qi from the Kidney (Maciocia 2005). In TCM, the function of each yang organ is inextri-cably linked to those of its yin partner, which, in this instance, is the Kidney. The Kidney is com-monly regarded as the most important organ in the body, governing birth, growth, reproduction and ageing. It is responsible for storing our Jing or “essence”, which is the driving force behind the function of all other organs and essential for life itself (Maciocia 2005).
An understanding of the TCM perspective on the relationships between the organs and merid-ians can help to explain some point indications

The Bladder meridian
© 2016 Acupuncture Association of Chartered Physiotherapists50
that can initially appear obscure. In TCM, each of the 12 main meridians are arranged in paired layers, which are collectively known as the Six Chaos. These layers vary in depth, and can be
thought of as the body’s protective mechanism (Hopwood 2004). The Bladder and Small Intestine meridians comprise the layer nearest the surface, which is known as the Tai Yang.
Figure 1. The course of the Bladder meridian, the foot Tai Yang channel (illustration reproduced with the kind permission of Jon Hobbs).
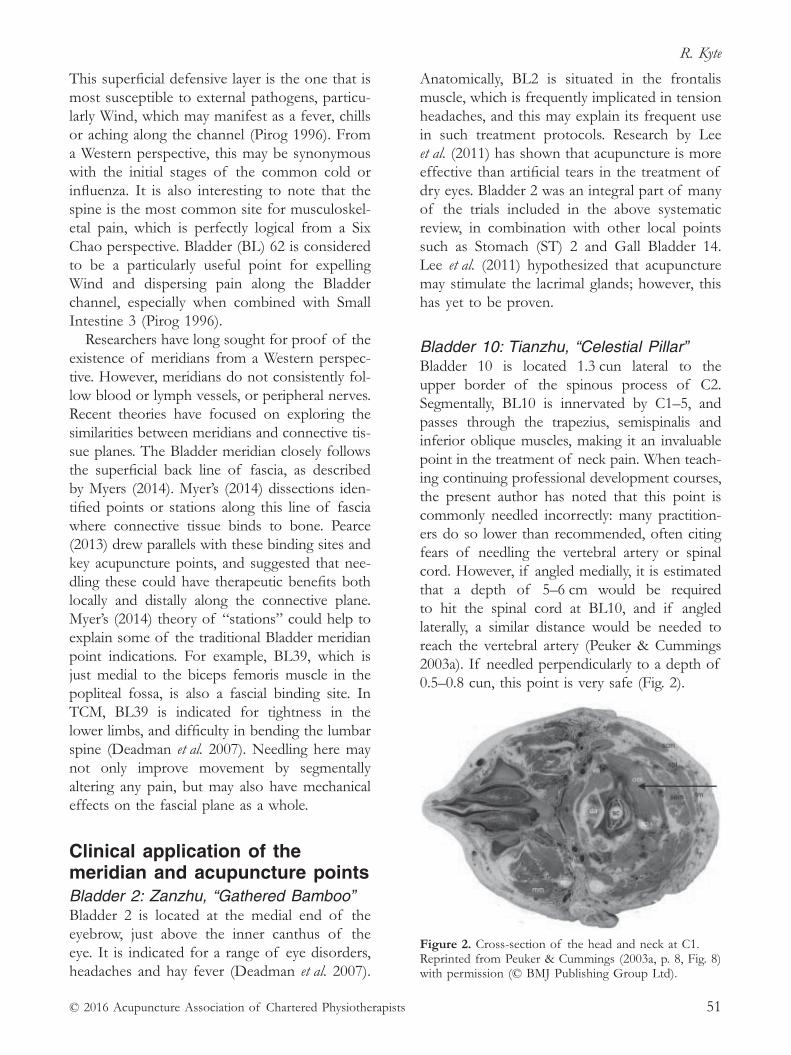
R. Kyte
© 2016 Acupuncture Association of Chartered Physiotherapists 51
This superficial defensive layer is the one that is most susceptible to external pathogens, particu-larly Wind, which may manifest as a fever, chills or aching along the channel (Pirog 1996). From a Western perspective, this may be synonymous with the initial stages of the common cold or influenza. It is also interesting to note that the spine is the most common site for musculoskel-etal pain, which is perfectly logical from a Six Chao perspective. Bladder (BL) 62 is considered to be a particularly useful point for expelling Wind and dispersing pain along the Bladder channel, especially when combined with Small Intestine 3 (Pirog 1996).
Researchers have long sought for proof of the existence of meridians from a Western perspec-tive. However, meridians do not consistently fol-low blood or lymph vessels, or peripheral nerves. Recent theories have focused on exploring the similarities between meridians and connective tis-sue planes. The Bladder meridian closely follows the superficial back line of fascia, as described by Myers (2014). Myer’s (2014) dissections iden-tified points or stations along this line of fascia where connective tissue binds to bone. Pearce (2013) drew parallels with these binding sites and key acupuncture points, and suggested that nee-dling these could have therapeutic benefits both locally and distally along the connective plane. Myer’s (2014) theory of “stations” could help to explain some of the traditional Bladder meridian point indications. For example, BL39, which is just medial to the biceps femoris muscle in the popliteal fossa, is also a fascial binding site. In TCM, BL39 is indicated for tightness in the lower limbs, and difficulty in bending the lumbar spine (Deadman et al. 2007). Needling here may not only improve movement by segmentally altering any pain, but may also have mechanical effects on the fascial plane as a whole.
Clinical application of the meridian and acupuncture pointsBladder 2: Zanzhu, “Gathered Bamboo”Bladder 2 is located at the medial end of the eyebrow, just above the inner canthus of the eye. It is indicated for a range of eye disorders, headaches and hay fever (Deadman et al. 2007).
Anatomically, BL2 is situated in the frontalis muscle, which is frequently implicated in tension headaches, and this may explain its frequent use in such treatment protocols. Research by Lee et al. (2011) has shown that acupuncture is more effective than artificial tears in the treatment of dry eyes. Bladder 2 was an integral part of many of the trials included in the above systematic review, in combination with other local points such as Stomach (ST) 2 and Gall Bladder 14. Lee et al. (2011) hypothesized that acupuncture may stimulate the lacrimal glands; however, this has yet to be proven.
Bladder 10: Tianzhu, “Celestial Pillar”Bladder 10 is located 1.3 cun lateral to the upper border of the spinous process of C2. Segmentally, BL10 is innervated by C1–5, and passes through the trapezius, semispinalis and inferior oblique muscles, making it an invaluable point in the treatment of neck pain. When teach-ing continuing professional development courses, the present author has noted that this point is commonly needled incorrectly: many practition-ers do so lower than recommended, often citing fears of needling the vertebral artery or spinal cord. However, if angled medially, it is estimated that a depth of 5–6 cm would be required to hit the spinal cord at BL10, and if angled laterally, a similar distance would be needed to reach the vertebral artery (Peuker & Cummings 2003a). If needled perpendicularly to a depth of 0.5–0.8 cun, this point is very safe (Fig. 2).
Figure 2. Cross- section of the head and neck at C1. Reprinted from Peuker & Cummings (2003a, p. 8, Fig. 8) with permission (© BMJ Publishing Group Ltd).

The Bladder meridian
© 2016 Acupuncture Association of Chartered Physiotherapists52
Bladder 11: Dazhu, “Great Shuttle”Situated 1.5 cun lateral to the base of the spinous process of T1, BL11 is an influential point for bone, and as such, is indicated in the treatment of any bony pathology, particularly painful bony obstruction, which is synonymous in Western medicine with arthritic disorders. There is a lack of empirical evidence specifically concerned with the effects of this point on bony pain or the mechanisms behind this, although it is included in some osteoarthritis study proto-cols (Hinman et al. 2012). From an anatomical perspective, several important muscles attach locally, including the trapezius, splenius capitis and cervicis. There are also sympathetic links to the head and neck, and connections to the trigeminocervical nucleus, an area that is often sensitized in migraine (Goadsby 2005), making this a useful point in the treatment of headaches and neck pain.
Bladder 12: Fengmen, “Wind Gate”Located 1.5 cun lateral to the base of the spinous process of T2, Fengmen is a key point for expelling pathogens, especially Wind, to which this channel is particularly susceptible. From a Western perspective, “Wind” in the Bladder meridian may be interpreted as a virus such as the common cold, and the aching in the head or neck that can accompany this. Bladder 12 is often combined with BL13, the Back- Shu point for the lung, in the treatment of such ailments. Research into patients with allergic asthma has shown that acupuncture at BL12, BL13 and Governor Vessel 14 may actually have immune- boosting effects, and is associated with increased levels of T- lymphocytes (Yang et al. 2013).
Back- Shu pointsAccording to TCM theory, each organ has a corresponding Back- Shu point. These lie along the inner bladder line 1.5 cun from the base of the corresponding spinous processes (Table 1). “Shu” translates as “to transport”, and implies that the Qi of a particular organ can be moved between the organ itself and the correspond-ing Back- Shu point (Deadman et al. 2007). For
example, BL13, the Back- Shu point for the lung, may be used to treat asthma or chest infections. Some practitioners also use Back- Shu for diagnostic purposes, carefully observ-ing and palpating the points in order to look for changes, which may imply signs of organ dysfunction. This is not dissimilar to the way in which Western practitioners employ visceral referred pain to aid diagnosis; for example, low back pain (LBP) may be indicative of a kidney infection, and acute right- sided mid- thoracic pain may suggest cholecystitis.
Is there any evidence that Back- Shu points can influence organ function? Hsu et al. (2006) found that 10 min of low- frequency electro-acupuncture (EA) at BL15 (the Back- Shu point for the Heart) produced significant reductions in heart rate in healthy subjects. Animal studies have also shown that EA at BL21 (the Back- Shu point for the Stomach) can produce sig-nificant increases in gastric motility (Wang et al. 2013).
From a Western perspective, the action of the Back- Shu points may partly be explained by the sympathetic innervation of the organs. For example, sympathetic nerves originating from T2–5 control bronchodilation. Gentle needling has been shown to decrease sympathetic tone in the corresponding spinal segment (Haker et al. 2000), and therefore, could explain how BL13 (the Back- Shu point for the Lung, level with T2) may be useful in the treatment of asthma.
Unfortunately, not all of the Back- Shu points correspond neatly with Western sympathetic
Table 1. Organs and corresponding Back- Shu points according to traditional Chinese medicine: (BL) Bladder; and (N/A) not applicable
Organ
Back- Shu point
Spinal level
Sympathetic innervation
Lung BL13 T3 T2–5Pericardium BL14 T4 T1–5Heart BL15 T5 T1–5Liver BL18 T9 T7–9Gall Bladder BL19 T10 T7–9Spleen BL20 T11 N/AStomach BL21 T12 T6–10San Jiao BL22 L1 N/AKidney BL23 L2 T5–9Large Intestine BL25 L4 T11–L2Small Intestine BL27 S1 T9–10Bladder BL28 S2 T11–L2

R. Kyte
© 2016 Acupuncture Association of Chartered Physiotherapists 53
innervations (see Table 1). Clinicians who want to influence sympathetic tone may wish to use a more Western clinical reasoning model for point selection, choosing points on the Bladder meridian that correspond to the known sym-pathetic innervation rather than the traditional Back- Shu locations.
The neurophysiological mechanism for changes in visceral activity following acupunc-ture is probably more complex than simple segmental modulation of autonomic nerves. Research has suggested that these changes may also involve autonomic regulatory systems in the brainstem and hypothalamus (Li et al. 2013). Keown (2014) has also theorized that the con-nections between organs and corresponding Back- Shu points may partly be explained by shared embryological origins.
Safety is a critical consideration when nee-dling the thoracic Back- Shu points. Although the lungs, pleura and spinal cord could all potentially be pierced from this location, ensur-ing that points are needled medially towards the spine to a maximum depth of 0.5–1 cun (depending on the build of the patient) should guarantee that needles remain in the paraspinal musculature. It is estimated that the spinal cord lies between 2.5 and 4.5 cm from the surface of the skin along the inner bladder line (Peuker & Cummings 2003b). Greater care is required when needling points along the outer bladder line, where the parietal pleura may be as super-ficial as 1.5 cm (Peuker & Cummings 2003b). These points should be needled transversely and medially to a depth of 0.3–0.5 cun (Fig. 3). It can be tempting to needle laterally in the mid- thoracic region when trying to reach trigger points in the rhomboid muscles; however, this carries a substantial risk of pneumothorax and should be avoided (Karavis et al. 2015).
Bladder 23: Shenshu, “Kidney Shu”Bladder 23, located on the inner bladder line, level with the base of L2, is one of the most commonly used points for the treatment of LBP. From a TCM perspective, LBP is com-monly caused by deficient Kidney Qi, and as the Back- Shu point of the Kidney, BL23 is a
key point in treating this disorder. The Bladder relies on Kidney Qi to function, and if this is deficient, normal urinary function can be affected. Therefore, BL23 can be used for a range of urinary problems, the effects of which may be partially explained by modulation of the sympathetic nerve supply to the bladder, which originates from T11–L2. A recent systematic review of acupuncture for incontinence failed to demonstrate any significant difference between verum and sham needling, but the poor meth-odological quality of the trials prevented firm conclusions from being drawn (Paik et al. 2013). However, one study found that acupuncture for overactive bladder was as effective as medica-tion, and had significantly less side effects. This trial combined BL23 with sacral points, and ST36 and Spleen (SP) 6, which are thought to boost Kidney Qi according to TCM (Kelleher et al. 1994).
Bladder 35: Huiyang, “Meeting of Yang”Located 0.5 cun lateral to the tip of the coc-cyx, the present author has found BL35 to be invaluable in the treatment of coccydynia when combined with BL33 and BL34. However, there is an absence of clinical research in this area. Classically, these points are also indicated in
Figure 3. Cross- sectional anatomy at T5. Image reprinted from Karavis et al. (2015, p. 240, Fig. 2B) in accordance with the Creative Commons Attribution Non Commercial (CC BY- NC 4.0) license (© 2015 British Medical Publishing Group).

The Bladder meridian
© 2016 Acupuncture Association of Chartered Physiotherapists54
the treatment of haemorrhoids, although the efficacy of this has not been well researched.
Bladder 40: Weizhong, “Middle of the Crook”Located in the centre of the popliteal crease, BL40 is classified as one of Ma Dan- Yang’s Heavenly Star points. This set of 12 points was named after a famous Jin dynasty acupunctur-ist, and were traditionally thought to be the most useful ones in the body (Nugent- Head 2012). Bladder 40 is particularly beneficial for lumbar spine and knee pain owing to its S1–2 segmental innervation and fascial connections. It is the He- Sea point of the Bladder channel. He- Sea points are traditionally thought to be ones were the Qi of a meridian starts to flow more deeply, and can be used to treat disorders of the corresponding organ; in this case, the bladder (Deadman et al. 2007). From a Western perspective, BL40 shares the same segmental innervation as the parasympathetic nerves to the bladder, which could explain the regulatory effects on bladder function that some authors have reported in protocols including BL40 (Wang et al. 2006). Practitioners should be aware of the proximity of the tibial nerve and pop-liteal artery, which can be reached at a depth of between 2 and 3 cm (Peuker & Cummings 2003c). There have been documented cases of popliteal aneurisms being caused by acupunc-ture to BL40 (Kao & Chang 2002).
Bladder 60: Kunlun, “Kunlun Mountains”Located between the lateral malleolus and the posterior margin of the Achilles tendon, BL60 is another of Ma Dang- Yang’s Heavenly Star points. As the Fire point on the Bladder meridian, it can be used to clear Heat or excess from more proximal parts of the channel, and as such, is useful for occipital headaches, back and leg pain, and eye disorders (Deadman et al. 2007). Kim et al. (2013) found that, when compared with a sham control, acupuncture at BL60 activated specific areas of the brain con-cerned with vision. Empirically, this point is also thought to stimulate labour, alongside points such as SP6, BL32 and Large Intestine 4 (Betts
2009). However, the efficacy of this has yet to be proven (Smith et al. 2013 ). Bladder 60 is tra-ditionally contradicted in pregnancy, and AACP advises against its use (AACP 2012). However, it should be noted that there is no Western evidence or anatomical rationale to suggest that this point is unsafe (Park et al. 2014).
Bladder 67: Zhiyin, “Reaching Yin”Located in the lateral corner of the nail bed of the fifth toe, BL67 is famed for its purported ability to turn breech babies when treated with moxibustion. A recent Cochrane review failed to reach any firm conclusions over the efficacy of this treatment because of the considerable heterogeneity of studies and conflicting out-comes (Coyle et al. 2012). The authors noted large variations in the frequency and length of moxibustion, and gestational age at the commencement of treatment. A more recent sham controlled trial demonstrated a significant decrease in breech presentation at birth when using moxibustion daily for 20 min from week 32 (Vas et al. 2013). The authors suggested that success with this technique may be dependent on early intervention. As the most distal point on the Bladder meridian, BL67 is indicated clas-sically for treating acute disorders at the oppo-site end of the channel, in this case headaches and eye disorders. Cho et al. (1998) found that acupuncture needling at BL67 stimulated the visual cortex on functional magnetic resonance imaging; however, this research was conducted on healthy volunteers, and studies have yet to investigate the clinical effects of this point on symptomatic individuals.
ConclusionsThe Bladder meridian contains many useful points that are frequently employed by physi-otherapists in the treatment of spinal and lower limb disorders, and headaches. However, the use of these points should not be restricted to musculoskeletal pain. Back- Shu points may have an important role to play in the management of significant co- morbidities, such as irritable bowel or bladder syndrome, and asthma. More high- quality research is required into the effects

R. Kyte
© 2016 Acupuncture Association of Chartered Physiotherapists 55
of Bladder points on eye pathologies and preg-nancy, and the mechanisms behind the physi-ological effects of acupuncture in these areas on disorders other than pain.
ReferencesAcupuncture Association of Chartered Physiotherapists
(AACP) (2012) AACP Guidelines for Safe Practice, Version 2. Acupuncture Association of Chartered Physiotherapists, Peterborough.
Betts D. (2009) Inducing labour with acupuncture – crucial considerations. The Journal of Chinese Medicine 90 (June), 20–25.
Cho Z. H., Chung S. C., Jones J. P., et al. (1998) New findings of the correlation between acupoints and corresponding brain cortices using functional MRI. Proceedings of the National Academy of Sciences of the United States of America 95 (5), 2670–2673.
Coyle M. E., Smith C. A. & Peat B. (2012) Cephalic version by moxibustion for breech presentation. Cochrane Database of Systematic Reviews, Issue 5. Art. No.: CD003928. DOI: 10.1002/14651858.CD003928.pub3.
Deadman P., Al- Khafaji M. & Baker K. (2007) A Manual of Acupuncture, 2nd edn. Journal of Chinese Medicine Publications, Hove.
Goadsby P. J. (2005) Migraine, allodynia, sensitisation and all of that. . . European Neurology 53 (Suppl. 1), 10–16.
Haker E., Egekvist H. & Bjerring P. (2000) Effect of sensory stimulation (acupuncture) on sympathetic and parasympathetic activities in healthy subjects. Journal of the Autonomic Nervous System 79 (1), 52–59.
Hinman R. S., McCrory P., Pirotta M., et al. (2012) Efficacy of acupuncture for chronic knee pain: protocol for a randomised controlled trial using a Zelen design. BMC Complementary and Alternative Medicine 12: 161. DOI: DOI: 10.1186/1472- 6882- 12- 161.
Hopwood V. (2004) Acupuncture in Physiotherapy. Butterworth–Heinemann, Oxford.
Hsu C.- C., Weng C.- S., Liu T.- S., Tsai Y.- S. & Chang Y.- S. (2006) Effects of electrical acupuncture on acupoint BL15 evaluated in terms of heart rate variability, pulse rate variability and skin conductance response. The American Journal of Chinese Medicine 34 (1), 23–36.
Kaptchuk T. J. (2000) The Web that Has No Weaver: Understanding Chinese Medicine, 2nd edn. Contemporary Books, Chicago, IL.
Kao C.- L. & Chang J.- P. (2002) Pseudoaneurysm of the popliteal artery: a rare sequela of acupuncture. Texas Heart Institute Journal 29 (2), 126–129.
Karavis M. Y., Argyra E., Segredos V., et al. (2015) Acupuncture- induced haemothorax: a rare iatrogenic complication of acupuncture. Acupuncture in Medicine 33 (3), 237–241.
Kelleher C. J., Filshie J., Burton G., Khullar V. & Cardozo L. D. (1994) Acupuncture and the treatment of
irritative bladder symptoms. Acupuncture in Medicine 12 (1), 9–12.
Keown D. (2014) The Spark in the Machine: How the Science of Acupuncture Explains the Mysteries of Western Medicine. Singing Dragon, London.
Kim N.- H., Cho S.- Y., Jahng G.- H., et al. (2013) Differential localization of pain- related and pain- unrelated neural responses for acupuncture at BL60 using BOLD fMRI. Evidence- Based Complementary and Alternative Medicine 2013: 9. Art. No.: 804696. DOI: 10.1155/2013/804696.
Lee M. S., Shin B.- C., Choi T.- Y. & Ernst E. (2011) Acupuncture for treating dry eye: a systematic review. Acta Ophthalmologica 89 (2), 101–106.
Li Q.- Q., Shi G.- X., Xu Q., et al. (2013) Acupuncture effect and central autonomic regulation. Evidence- Based Complementary and Alternative Medicine 2013: 6. Art. No.: 267959. DOI: 10.1155/2013/267959.
Maciocia G. (2005) The Foundations of Chinese Medicine: A Comprehensive Text for Acupuncturists and Herbalists, 2nd edn. Churchill Livingstone, Edinburgh.
Myers T. W. (2014) Anatomy Trains: Myofascial Meridians for Manual and Movement Therapists, 3rd edn. Churchill Livingstone, Edinburgh.
Nugent- Head A. (2012) The Heavenly Star Points of Ma Danyang. The Journal of Chinese Medicine 98 (February), 5–12.
Paik S.- H., Han S.- R., Kwon O.- J., et al. (2013) Acupuncture for the treatment of urinary incontinence: a review of randomized controlled trials. Experimental and Therapeutic Medicine 6 (3), 773–780.
Park J., Sohn Y., White A. R. & Lee H. (2014) The safety of acupuncture during pregnancy: a systematic review. Acupuncture in Medicine 32 (3), 257–266.
Pearce L. (2013) Fascial connections and acupuncture: the tendino- muscular meridians of TCM and Anatomy Trains. Lecture presented at Moseley Hall Hospital, Birmingham, UK, 24 February 2013.
Peuker E. & Cummings M. (2003a) Anatomy for the acupuncturist – facts & fiction. 1: The head and neck region. Acupuncture in Medicine 21 (1–2), 2–8.
Peuker E. & Cummings M. (2003b) Anatomy for the acupuncturist – facts & fiction. 2: The chest, abdomen, and back. Acupuncture in Medicine 21 (3), 72–79.
Peuker E. & Cummings M. (2003c) Anatomy for the acupuncturist – facts & fiction. 3: Upper & lower extremity. Acupuncture in Medicine 21 (4), 122–132.
Pirog J. E. (1996) The Practical Application of Meridian Style Acupuncture. Pacific View Press, Berkeley, CA.
Smith C. A., Crowther C. A. & Grant S. J. (2013) Acupuncture for induction of labour. Cochrane Database of Systematic Reviews, Issue 8. Art. No.: CD002962. DOI: 10.1002/14651858.CD002962.pub3.
Vas J., Aranda- Regules J. M., Modesto M., et al. (2013) Using moxibustion in primary healthcare to correct non- vertex presentation: a multicentre randomised controlled trial. Acupuncture in Medicine 31 (1), 31–38.

The Bladder meridian
© 2016 Acupuncture Association of Chartered Physiotherapists56
Wang H., Shen G.- M., Liu W.- J., Huang S. & Zhang M.- T. (2013) The neural mechanism by which the dorsal vagal complex mediates the regulation of the gastric motility by Weishu (RN12) and Zhongwan (BL21) stimulation. Evidence- Based Complementary and Alternative Medicine 2013: 7. Art. No.: 291764. DOI: 10.1155/2013/291764.
Wang Y., Li R. & Hua K. (2006) Acupuncture treatment of children nocturnal enuresis – a report of 56 cases. Journal of Traditional Chinese Medicine 26 (2), 106–107.
Yang Y.- Q., Chen H.- P., Wang Y., et al. (2013) Considerations for use of acupuncture as supplemental therapy for patients with allergic asthma. Clinical Reviews in Allergy and Immunology 44 (3), 254–261.
Rachel Kyte is a senior lecturer at the University of Worcester. She trained at Keele University, Staffordshire, UK, qualifying as a physiotherapist in 2000. Since graduating, she has worked in various National Health Service and private settings in both the UK and abroad, specializing in the management of musculoskeletal disorders. Rachel completed her foundation acupunc-ture training in 2003. She was awarded an MSc in Acupuncture from Coventry University, Coventry, UK, in 2009, and became an advanced member of AACP. Rachel is a fellow of the Higher Education Academy and an accredited AACP tutor.

© 2016 Acupuncture Association of Chartered Physiotherapists 57
Acupuncture in Physiotherapy, Volume 28, Number 1, Spring 2016, 57–66
CASE REPORT
Acupuncture for De Quervain’s disorder/tenosynovitis
N. ThompsonOutpatient Physiotherapy Department, Willesden Centre for Health and Care, North West London Healthcare NHS Trust, London, UK
AbstractDe Quervain’s tenosynovitis (DQT) is a disabling condition of the thumb that is caused by thickening and impaired gliding of the thumb extensor and abductor tendons. The subject of this case study was a 28- year- old woman in whom histopathological degenerative changes were found to be more dominant than inflammation. Treatment of DQT with conserva-tive management alone has proved to be difficult. However, there is growing evidence and acceptance of the effectiveness of acupuncture as a treatment for tendon injuries. In this case, the local, segmental and central analgesic effects of acupuncture were employed over five treatment sessions along with night- splinting and exercises. Grip strength, the Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH) questionnaire, and the Numerical Pain Rating Scale (NPRS) were used as outcome measures at baseline and 5 weeks. At 5 weeks, the subject’s grip strength had improved by one point, her QuickDASH score had decreased by 20.5 points, and she experienced only intermittent pain and had stopped tak-ing regular analgesia. Overall, acupuncture only provided partial pain relief and functional improvement. This could be because the subject regularly used her hands in activities of daily living that made the healing time longer. This finding correlates with current clinical research, which has found that acupuncture is almost as effective as corticosteroid injections for the treatment of DQT.
Keywords: acupuncture, de Quervain’s disorder, tenosynovitis.
IntroductionDe Quervain’s tenosynovitis (DQT) is char-acterized by pain or tenderness and swelling on the radial side of the wrist, impairment of thumb function, and thickening of the liga-mentous structure covering the tendons in the first dorsal compartment of the wrist (Moore
1997; Peters- Veluthamaningal et al. 2009). The disorder is caused by impaired gliding of the extensor pollicis brevis (EPB) and abductor pollicis longus (APL) tendons as these pass in the synovial sheath in a fibro- osseous tun-nel; this is a result of thickening of the wrist extensor retinaculum (Peters- Veluthamaningal et al. 2009; Brukner & Khan 2012). The term tenosynovitis is commonly used; however, according to Peters- Veluthamaningal et al. (2009), inflammation is not involved in the pathology of DQT when histopathological degenerative changes are the most predominant feature.
Correspondence: Nora Thompson, Outpatient Physio-therapy Department, Willesden Centre for Health and Care, North West London Healthcare NHS Trust, Robson Avenue, Willesden Green, London NW10 3RY, UK (e- mail: norahorvath75@ yahoo.co.uk).

Acupuncture for De Quervain’s disorder/tenosynovitis
© 2016 Acupuncture Association of Chartered Physiotherapists58
Predisposing movements include forceful grasping with ulnar deviation or repetitive use of the thumb (Howell 2012). De Quervain’s tenosynovitis commonly occurs in people whose job requires repetitive hand movements (Hadianfard et al. 2014), racket sports players, ten- pin bowlers, rowers, canoeists and golfers (Brukner & Khan 2012). Furthermore, it is also frequently diagnosed in pregnant and lactating women (Avci et al. 2002). Other groups of peo-ple who are susceptible to the condition include musicians, assembly workers, game players and people who overuse smartphones (Da Silva & Batigalia 2014).
De Quervain’s tenosynovitis is classified under the umbrella terms repetitive strain injury and work- related musculoskeletal disorders of the upper limb (Peters- Veluthamaningal et al. 2009). Walker- Bone et al. (2004) conducted a large study of the general population in the UK, and found that the incidence of de Quervain’s disease was 0.5% among men and 1.3% among women.
A diagnosis of DQT is mainly made on the basis of past medical history and a physi-cal examination (Moore 1997). The symptoms consist of tenderness at the radial styloid that sometimes radiates to the thumb, forearm and shoulder, and there may be swelling at the radial styloid with tenderness and crepitation on palpation (Peters- Veluthamaningal et al. 2009). A positive Finkelstein’s test is diagnostic of DQT (“The thumb is placed in the palm of the hand with flexion of the metacarpophalangeal and interphalangeal joints while the examiner devi-ates the wrist in the ulnar direction”; Brukner & Khan 2012, p. 427), but it is not a gold standard confirmatory test (Peters- Veluthamaningal et al. 2009).
Conservative treatments include: splinting, local electrotherapeutic modalities, stretches and gradual strengthening (Brukner & Khan 2012); and strapping, transverse friction massage and medication (e.g. non- steroidal anti- inflammatory drugs, NSAIDs) (da Silva & Batigalia 2014). Heat, cold, rest and massage are also commonly used, but these have not been found to be very effective (Moore 1997).
Corticosteroid injections are commonly used to treat DQT if conservative management
has failed. Corticosteroid and local anaesthetic injections into the tendon sheath are usually helpful, and in rare cases, surgical release can also be performed (Brukner & Khan 2012). Peters- Veluthamaningal et al. (2009) found that corticosteroid injections are superior to thumb spica splinting for pain relief in the treatment of DQT. However, this evidence was based on a small clinical trial of poor methodological quality that only included lactating and pregnant women. Kume et al. (2012) concluded that ultrasound- guided injection targets the EPB and is more effective than manual injection. A study by Mehdinasab et al. (2010) included 73 subjects with DQT and randomized them into two groups. These researchers reported success rates of 86.5% with injection and casting (n = 37), and 36.1% with casting alone (n = 36) at a 6- month follow- up. The casting lasted for 1 month. The side effects of the injection included skin hypo-pigmentation (n = 1) and sensory radial nerve impairment (n = 1), and the most common was pain for 1 day after the injection in 40% of the cases (Mehdinasab & Alemohammad 2010). Further potential complications include local infections and local reactions (e.g. swelling, ten-derness, post- injection steroid flare, soft- tissue atrophy and tendon rupture) (Cardone & Tallia 2002). Therefore, some patients are reluctant to receive steroid injections (Hadianfard et al. 2014).
There is growing acceptance of acupuncture as a treatment for musculoskeletal conditions among patients and healthcare professionals (Hadianfard et al. 2014) because of the increas-ing amount of evidence for its effectiveness and safety. Acupuncture can be an effective treatment modality for tendon diseases such as rotator cuff tendinopathy, tennis elbow and Achilles tendinopathy (da Silva & Batigalia 2014). De Almeida et al. (2012) found that the concentration of collagen increased and the molecular organization of the collagen fibres improved during electroacupuncture, which may help the mechanical strength of the tendon to recover after injury. The above authors’ research is promising; however, it must be noted that they used electroacupuncture and that this was actu-ally carried out on rats. In a clinical discussion,
N. Thompson
© 2016 Acupuncture Association of Chartered Physiotherapists 59
Neal & Longbottom (2012) suggested that acupuncture may have a role in treating tendon injuries because of its facilitation of tendon blood flow and fibroblastic activity. To date, there is limited research on this aspect of the use of acupuncture for the treatment of DQT.
Only one randomized controlled trial (RCT) was completed by Hadianfard et al. (2014), who randomly allocated 30 subjects to acupuncture and injection groups. The acupuncture group received five, 30- min treatments within a week [Large Intestine (LI) 5, Lung (LU) 7, LU9 and Ah- Shi points were used], and the injection group received one injection. Both groups were prescribed thumb spica splints. Disability and pain were measured with the Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH) questionnaire and a visual analogue scale at baseline, and 2 and 6 weeks. By 6 weeks, the QuickDASH scores had dropped from 61.2 to 6.1 in the injection group, and from 64.4 to 9.8 in the acupuncture group. These authors found only a small difference between the overall effectiveness of acupuncture and injection for the management of DQT. They concluded that “acupuncture can be considered as an alterna-tive option of treatment of De Quervain’s tenosynovitis” (Hadianfard et al. 2014, p. 116).
Case report
BackgroundThe present subject was a 28- year- old female fashion designer. At the time of her injury, she was employed by a high- street shop. Her job involved drawing sketches, taking manikins apart and knitting to tight deadlines, and required her to use a computer. She was right- handed, and regularly exercised by walking and running.
The subject presented with left thumb pain following a party in January 2015, when she had held a clutch bag for a prolonged period of time. A few days later, she was woken up during the night by a sharp pain in her left thumb and wrist that become a constant ache and worsened after aggravating activities.
Her previous medical history included high blood pressure that was now under control. She was not taking any medication apart from
ibuprofen and paracetamol to control her pain, and was in good general health otherwise.
Clinical examinationThe present subject had left radial- sided wrist and thumb pain at the anatomical snuff box. At times, this pain radiated at the radial aspect of the arm towards the elbow. She also had a con-stant ache that aggravating activity would cause her to score as ≥ 9/10 on the Numerical Pain Rating Scale (NPRS) that took several hours of rest and painkillers to settle to about 4/10.
The subject exhibited normal neck move-ment and neck palpation. There was no pain radiation and numbness, or pins and needles. Her neurological examination was normal. No red flags were identified.
Aggravating factors included picking up objects, gripping, knitting, and using her hands for activities of daily living such as washing dishes, cooking and vacuuming. Painkillers and rest eased the pain.
The initial 24- h pattern was that the pain was worse at night and in the morning, but this changed over time.
At the initial consultation, the subject was not sure that physiotherapy would be of any help. Her general practitioner (GP) had suggested steroid injections, but she wanted to try physio-therapy first because she was not sure about the side effects of these injections.
The differential diagnosis was as follows (Brukner & Khan 2012): (1) carpometacarpal arthritis of the thumb;(2) radiocarpal arthritis;(3) intercarpal instabilities;(4) C6 cervical radiculopathy;(5) intersection syndrome; and(6) trauma- related scaphoid fracture.
Slight swelling was observed on the left ana-tomical snuff box.
On examination, the subject’s forearm prona-tion and supination were fine on both sides. Her wrist range of movement (ROM) was satis-factory in flexion, but she exhibited pain along the radial side of her wrist and thumb on wrist radial and ulnar deviation, and wrist extension. With regard to her thumb ROM, extension and

Acupuncture for De Quervain’s disorder/tenosynovitis
© 2016 Acupuncture Association of Chartered Physiotherapists60
abduction were reduced because of pain, but adduction and flexion were satisfactory. The subject’s grip strength was 5/5 on her right side, but 3/5 on her left because of pain. Resisted thumb extension and abduction were rated as –3/5, and increased pain. Finkelstein’s test was positive on her left side, and negative on her right. Her APL and EPB tendons were tender on palpation, but no muscle tenderness or trig-ger points were identified.
The subject filled out and signed the acu-puncture consent form. There were no con-traindications or precautions for acupuncture, and informed consent gained at all treatment sessions. Verbal and written explanations were given regarding the positive and negative effects of acupuncture.
TreatmentThe treatment rationale was to reduce the pre-sent subject’s pain, improve function, increase grip strength and provide patient education. She was annoyed and frustrated because she had previously attended three physiotherapy sessions within 2 months, but had experienced minimal improvement. Furthermore, her wrist and thumb pain were so bad that she left her job as a fashion designer. She had been advised by a previous physiotherapist to use ice, have regular breaks at work, take anti- inflammatory medications, and perform joint mobilization and wrist/thumb ROM exercises. The subject had also been offered a steroid injection by her GP, but she declined this at the time because of uncertainty about the side effects and opted to try more physiotherapy. Based on the minimal progress made over the course of the previous treatment and the persistence of her symptoms, a decision was made to try acupuncture in order to reduce pain and improve function.
Acupuncture is becoming increasingly popular in the management of tendon injuries. Traditional Chinese medicine (TCM) holds that the needles influence energy called Qi, which flows around the body in meridians. However, in Western medical acupuncture, a medical diagno-sis is made and the needles are used to influence the body’s mechanism, which involves the nerv-ous system and the muscles (White et al. 2008),
and ultimately, reduce pain. Clinical studies have demonstrated that acupuncture improves pain and functional activities in patients with tendon injuries by modulating anti- inflammatory and molecular mechanotransduction pathways that can increase type I collagen synthesis, which is responsible for the tendon’s biomechanical properties (de Almeida et al. 2014).
The consecutive acupuncture sessions and point selections are summarized below.
Session 1. The Large Intestine (yang) and Lung (ying) meridians were chosen initially for local and segmental effects (AACP 2015). Both meridians are on the C6 dermatome, which is where the painful area was located. The LI5 and LU7 acupuncture points were needled locally in order to stimulate the small myelinated Aδ nerve fibres, and the type II and III nerves in the muscles, and to elicit an action potential to induce the release of neuropeptides, which increase blood flow to the area and promote tissue healing (Bradnam 2003, 2007; White et al. 2008). According to de Almeida et al. (2014), it is necessary to use acupuncture points that are anatomically connected to the injured area if the collagen synthesis and reorganization required for tendon healing is to be stimulated. This hypothesis also supported the selection of LI5 and LU7. The LI10 and LI11 points were added to achieve segmental analgesia through the dorsal horn, which continues on a pathway into the anterolateral tract where acupuncture stimulus depresses the response of the substan-tia gelatinosa, leading to pain inhibition (White et al. 2008). Large Intestine 10 and LI11 are part of the same segment as LI5, and share the same nerve supply. The level of segmental analgesia was increased with “layering” (Bradnam 2003, 2007). Large Intestine 4 was initially used on the subject’s left side because it has a strong central effect and is a master point for pain.
The subject was provided with a thumb spica splint, which was mainly for night- time use, and she was encouraged to continue with the ROM exercises as before.
Table 1 outlines the course of treatment and its effects, and Table 2 describes the acupunc-ture point selection.

N. Thompson
© 2016 Acupuncture Association of Chartered Physiotherapists 61
Tab
le 1
. Tr
eatm
ent
and
effe
cts:
(L
I) L
arge
Int
estin
e; (
LU)
Lun
g; (
LR
) L
iver
; (G
B)
Gal
l Bla
dder
; and
(T
E)
Trip
le E
nerg
izer
Trea
tmen
t se
ssio
nA
cupu
nctu
re p
oint
sN
eedl
ing
tech
niqu
e*D
ose
(min
)†N
eedl
e si
ze (
mm
)D
epth
of
inse
rtio
n (c
m)
Trea
tmen
t re
spon
se/a
dver
se r
eact
ions
1
LI4
(le
ft)
LI5
(le
ft)
LI1
0 (le
ft)
LI1
1 (le
ft)
LU7
(left
)
Shal
low,
tap
and
tw
ist
Shal
low,
tap
and
tw
ist
Dee
p, li
ft/t
hrus
t an
d tw
irlD
eep,
lift
/thr
ust
and
twirl
Obl
ique
, sha
llow,
tap
and
tw
ist
10 10 10 10 10
25 25 40 40 25
0.5
0.5
1.0–
2.0
2.0–
3.0
0.5
Goo
d D
e Q
i ach
ieve
dSu
bjec
t re
port
ed h
eavi
ness
of
her
arm
No
othe
r si
de e
ffec
ts
2
LI4
(bi
late
ral)
LI5
(le
ft)
LI1
0 (le
ft)
LI1
1 (le
ft)
LU7
(left
)
As
abov
eA
s ab
ove
As
abov
eA
s ab
ove
As
abov
e
20 20 20 20 20
25 25 40 40 25
0.5
0.5
1.0–
2.0
2.0–
3.0
0.5
Goo
d D
e Q
i ach
ieve
dSu
bjec
t re
port
ed t
hat
she
had
slep
t w
ell a
fter
th
e pr
evio
us s
essi
on
3L
I4 (
bila
tera
l)L
I5 (
left
)L
I10
(left
)L
I11
(left
)LU
7 (le
ft)
LR
3 (b
ilate
ral)
GB
34 (
bila
tera
l)
As
abov
eA
s ab
ove
As
abov
eA
s ab
ove
As
abov
eSh
allo
w, t
ap a
nd t
wis
tD
eep,
lift
/thr
ust
and
twirl
20 20 20 20 20 20 20
25 25 40 40 25 25 40
0.5
0.5
1.0–
2.0
2.0–
3.0
0.5
0.1
1.0–
2.0
Goo
d D
e Q
i ach
ieve
dSu
bjec
t re
port
ed t
hat
she
had
slep
t w
ell a
fter
th
e pr
evio
us s
essi
on
4L
I4 (
bila
tera
l)L
I5 (
left
)L
I10
(left
)L
I11
(left
)LU
7 (le
ft)
GB
34 (
bila
tera
l)LU
9 (le
ft)
As
abov
eA
s ab
ove
As
abov
eA
s ab
ove
As
abov
eA
s ab
ove
Shal
low,
tap
and
tw
ist
20 20 20 20 20 20 20
25 25 40 40 25 40 25
0.5
0.5
1.0–
2.0
2.0–
3.0
0.5
1.0–
2.0
0.5
Goo
d D
e Q
i ach
ieve
dA
litt
le s
ensi
tive
on b
ilate
ral L
I4 a
nd L
I11
5
LI4
(bi
late
ral)
LI5
(le
ft)
LI1
0 (le
ft)
LI1
1 (le
ft)
LU7
(left
) G
B34
(bi
late
ral)
LU9
(left
)
TE
5 (b
ilate
ral)
As
abov
e A
s ab
ove
As
abov
e A
s ab
ove
As
abov
e A
s ab
ove
As
abov
e D
eep,
lift
/thr
ust
and
twirl
20
20
20
20
20
20
20
20
25
25
40
40
25
40
25
40
0.5
0.5
1.0–
2.0
2.0–
3.0
0.5
1.0–
2.0
0.5
1.0–
2.0
Goo
d D
e Q
i ach
ieve
d N
o ad
vers
e ev
ents
*All
perp
endi
cula
r al
ong
the
Lar
ge I
ntes
tine
mer
idia
n.†N
eedl
es o
nly
man
ipul
ated
upo
n in
sert
ion
durin
g se
ssio
n 1.
Nee
dles
man
ipul
ated
upo
n in
sert
ion
and
10 m
in la
ter
durin
g al
l oth
er s
essi
ons.

Acupuncture for De Quervain’s disorder/tenosynovitis
© 2016 Acupuncture Association of Chartered Physiotherapists62
Tab
le 2
. A
cupu
nctu
re p
oint
sel
ectio
n: (
LI)
Lar
ge I
ntes
tine;
(LU
) L
ung;
(L
R)
Liv
er; (
TE
) Tr
iple
Ene
rgiz
er; a
nd (
GB
) G
all B
ladd
er
Clin
ical
rea
soni
ng
Acu
punc
ture
poi
ntN
eedl
ing
tech
niqu
e an
d do
seW
este
rn m
edic
al a
cupu
nctu
re (
Whi
te e
t al.
2008
; AA
CP
2015
)Tr
aditi
onal
Chi
nese
med
icin
e (Y
YH
201
6)
LI4
(H
egu)
Perp
endi
cula
r in
to t
he a
dduc
tor
polli
cis
mus
cle
Dep
th =
1 c
mN
eedl
e =
25
mm
Be
awar
e th
at t
he r
adia
l art
ery
can
caus
e a
stro
ng
vaso
vaga
l res
pons
e, d
o no
t us
e du
ring
preg
nanc
yU
sed
bila
tera
lly
Mas
ter
poin
t fo
r pa
in, h
eada
che
and
rela
xatio
n; b
ilate
rally
co
mbi
ned
with
LR
3C
entr
al e
ffec
tC
8 an
d T
1 m
yoto
mes
(B
radn
am 2
003,
200
7)
Chr
onic
pai
nIn
fluen
ces
the
circ
ulat
ion
of Q
i and
Blo
od:
use
the
Four
Gat
es (
LI4
and
LV
3 bi
late
rally
) to
str
ongl
y m
ove
the
Qi a
nd B
lood
in t
he
body
, cle
arin
g st
agna
tion
and
alle
viat
ing
pain
LI5
(Y
angx
i)Pe
rpen
dicu
lar
into
the
ana
tom
ical
snu
ff b
oxD
epth
= 0
.5 c
mN
eedl
e =
30
mm
Loc
al e
ffec
tC
6/7
myo
tom
es a
nd C
5/6
derm
atom
esW
rist
pain
LI1
0 (S
hous
anli)
Perp
endi
cula
r in
to t
he e
xten
sor
carp
i rad
ialis
long
us o
r su
pina
tor
mus
cles
Dep
th =
1–2
cm
Nee
dle
= 4
0 m
m
Segm
enta
l eff
ect
C5/
6/7
myo
tom
es a
nd C
5/6
derm
atom
esSh
ould
er, e
lbow
and
wris
t pa
in is
sues
, and
ge
nera
l ach
ines
s in
the
se a
reas
Tend
oniti
s
LI1
1 (Q
uchi
)Pe
rpen
dicu
lar
into
the
ext
enso
r ra
dial
is lo
ngus
mus
cle
Dep
th =
2–3
cm
Nee
dle
= 4
0 m
m
Segm
enta
l eff
ect
C5/
6 m
yoto
mes
and
der
mat
omes
Elb
ow a
nd u
pper
lim
b di
sord
ers,
pain
and
in
flam
mat
ion
Tenn
is e
lbow
LU7
(Lie
que)
Obl
ique
pro
xim
ally
Dep
th =
0.5
cm
Nee
dle
= 2
5 m
mPr
ecau
tion:
the
cep
halic
vei
n“[
B]e
twee
n th
e te
ndon
s of
abd
ucto
r po
llici
s lo
ngus
and
br
achi
orad
ialis
” (W
hite
et a
l. 20
08, p
. 197
)
Loc
al e
ffec
tC
7/8
myo
tom
es a
nd C
6 de
rmat
ome
Pain
in t
he t
hum
b
LU9
(Tai
yuan
)Pe
rpen
dicu
lar
Dep
th =
0.5
cm
Nee
dle
= 2
5 m
m
Loc
al e
ffec
tW
rist
pain
, and
arm
pai
n al
ong
the
mer
idia
n.
LR
3 (T
aich
ong)
Perp
endi
cula
r in
to t
he fi
rst
dors
al in
tero
ssei
(pr
ecau
tion:
th
e do
rsal
is p
edis
art
ery)
Dep
th =
1 c
mN
eedl
e =
25
mm
Cen
tral
eff
ects
Com
bine
d w
ith L
I4 b
ilate
rally
, pro
duci
ng a
cal
min
g ef
fect
, us
ed f
or a
nxie
ty a
nd s
tres
s
Cal
min
g po
int,
used
for
ang
er, i
rrita
bilit
y, in
som
nia
and
anxi
ety
With
LI4
, par
t of
“Fo
ur G
ates
” tr
eatm
ent:
pow
erfu
lly a
ffec
ts t
he fl
ow o
f Q
i and
Blo
od
in t
he b
ody
TE
5 (W
aigu
an)
Perp
endi
cula
rD
epth
= 1
–2 c
mN
eedl
e =
40
mm
“[B
]etw
een
radi
us a
nd u
lna,
and
bet
wee
n ex
tens
or in
dici
s an
d ex
tens
or p
ollic
is lo
ngus
” (W
hite
et a
l. 20
08 p
. 197
)
Maj
or p
oint
for
cen
tral
eff
ects
, rel
axes
the
ten
dons
Alle
viat
es p
ain
thro
ugh
the
mer
idia
nC
7/8
myo
tom
esC
6/8
derm
atom
es
Dis
tal p
oint
for
tem
pora
l hea
dach
es, a
nd
rela
xes
the
tend
ons
Use
d fo
r up
per
limb
diso
rder
s
GB
34 (
Yan
glin
gqua
n)
Pe
rpen
dicu
lar
into
the
per
oneu
s lo
ngus
D
epth
= 1
–2 c
m
Nee
dle
= 4
0 m
m
Influ
entia
l poi
nt f
or m
uscl
es a
nd t
endo
n L
5/S1
seg
men
ts a
nd L
5 de
rmat
ome
Influ
entia
l poi
nt f
or m
uscl
es a
nd t
endo
ns
N. Thompson
© 2016 Acupuncture Association of Chartered Physiotherapists 63
Session 2. The subject reported that she had experienced an increase in pain 2 days after the first acupuncture session. However, the pain had later decreased to 0/10 at rest and she had been able to knit for 1 h. After that, the pain had increased to 7/10 and she had had to take painkillers. In spite of this setback, she reported a 30% improvement.
Thumb ROM had increased in both exten-sion and abduction, and the pain had reduced. Wrist ROM was full, with pain only on wrist extension and ulnar deviation. On palpation, the only pain at the radial styloid process was on the APL and EPB tendons, and there was no pain radiation to the forearm. Finkelstein’s test was less painful, and there was slightly increased ulnar deviation.
The acupuncture time was increased to 20 min. The same points were used as before, with one difference: LI4 was employed bilater-ally to enhance the pain- relieving effect. The needles were stimulated once.
The subject was advised to continue with splinting and icing. Thumb ROM and strength-ening exercises were added as pain allowed.
Session 3. The subject reported that she had slept well after the second session, and had experi-enced little increased pain on the following day. After that, the pain was 0/10 at rest, but fluctu-ated between 3/10 and 7/10 with aggravating activities. She was now able to lift up a half- full cup. Overall, she was 40% better.
Acupuncture was again given for 20 min. Large Intestine 4 and LR3 were used together bilaterally. These are considered to be very strong points, and are believed to be able to elicit a strong central effect through the supra-spinal mechanism (Bradnam 2003, 2007). Large Intestine 4 and LR3 are also influential points in TCM, which calls these the “Four Gates”, and are believed to influence the flow of Blood and Qi (YYH 2016). A further reason for this point selection was the fact that the subject had now had the problem for more than 6 months, and therefore, it could now be classified as chronic pain. Bradnam (2003, 2007) recom-mended that chronic pain should be treated by using more needles in the same segment
and choosing a distant point in the disturbed segment.
Based on its use in TCM, Gall Bladder 34 was also added as a distal point because it is an influential point for muscles and tendons (YYH 2016). Furthermore, according to Pearce (2015, p. 66), “Stimulation of the Gall Bladder points can have a profound effect on tendons and muscle tone.” This point is also commonly recommended for musculoskeletal pain.
Session 4. After the third acupuncture session, the subject reported that she had felt slightly more pain for 2 days, but that this had then improved. She had felt so little pain in her left wrist (2–3/10) that she had done 20 min of vacuum cleaning, but this had increased her pain to 8/10 again. However, the pain had reduced to 6/10 a few days later. The subject reported that she had not performed her home exercise programme. Despite the setback, she rated her pain as 40% overall, which was the same as after the second session.
Acupuncture was given for 20 min. The same points were used as before, with the addition of LU9, which was added to increase both local and segmental analgesia. The needles were manipulated twice at insertion and then 10 min later.
Session 5. The subject reported that she had felt increased pain for 2 days after the previous acu-puncture session, but this had then reduced to 3/10. She had avoided all aggravating activities during the period of elevated pain. She was now able to hold a full cup of drink, and reported an overall improvement of 60%.
On assessment, there was no pain on elbow pronation and supination, and full active thumb abduction and extension with pain only in the end range. Her resisted movements were 4/5, and her grip strength was +4/5. Finklestein’s test was still positive, but the subject had more movement on ulnar deviation, and only local tenderness on the radial styloid process.
Acupuncture was given for 20 min. The same points were used with the addition of Triple Energizer 5, which was added bilaterally to increase segmental analgesia. This point is used

Acupuncture for De Quervain’s disorder/tenosynovitis
© 2016 Acupuncture Association of Chartered Physiotherapists64
for upper limb disorders (YYH 2016) and to relax the tendons (AACP 2015). Needles were stimulated on insertion and after every 5 min. No immediate adverse events were reported.
The subject’s exercise programme was reviewed, and eccentric radial deviation exercise with a bottle held in the hand was added. She also continued with self- massage, thumb ROM, and within the pain- free range, resistance exer-cises with a hair band. She also continued using the night- time splint.
The outcome measures were repeated (see Table 3). There was some improvement in hand function and grip strength, as indicated by a 20.5 drop on the QuickDASH and a one- point increase on the Oxford scale, respectively. Overall, the subject’s pain was reduced and intermittent, and she had stopped taking pain-killers regularly.
DiscussionDe Quervain’s tenosynovitis can prove difficult to manage clinically. To some extent, this is because patients regularly use their hands to perform activities of daily living, which prolongs the healing time, and therefore, the condition frequently becomes chronic (Hadianfard et al. 2014). This problem was obvious through-out the present case study: when the subject
experienced some improvements after acupunc-ture treatment, she felt more confident about using her hand, and then setbacks slowed down her recovery. Moreover, the exact pain mecha-nism involved in DQT remains unclear, which poses further problems when selecting the best treatment for this condition (Hadianfard et al. 2014).
The results of the present study were com-pared to Hadianfard et al.’s (2014) RCT. These authors considered an improvement in disability and pain status of ≥ 60% to be a partial suc-cess, failure was defined as an improvement of < 60% and success was represented by an 80% improvement. In the present case, acupuncture treatment resulted in a partial success (i.e. ≥ 60%) according to the patient’s subjective evaluation.
The QuickDASH score dropped by 20.5%, grip strength increased from 3/5 to +4/5 on the Oxford scale, and the NPRS score also improved (see Table 3). During the course of the study, the subject used analgesia as and when it was needed. A thumb spica splint was provided with the advice that it should only be used at night. If splinting had been used during the day, this might have meant that the subject would have avoided aggravating activities, reduc-ing the possibility of flare- ups and improving healing between acupuncture sessions. The effect of treatment was measured over 5 weeks with weekly follow- up sessions. The first acu-puncture session was 45 min long so as to allow enough time to carry out appropriate palpation and needling; the other sessions were 30 min in length.
According to Hadianfard et al. (2014), both acupuncture and corticosteroid injections can be used to treat DQT. Since both treatments significantly ameliorated the condition, it would be interesting to know and compare the cost- effectiveness of the two modalities. However, this was one of the limitations of Hadianfard et al. (2014) study: neither the cost- effectiveness of the one- off injection nor that of the six acupuncture sessions were considered from the perspective of healthcare costs or patient expenditure, such as loss of productivity and travelling expenses (Meals 2014). Calculating the
Table 3. Outcome measure results: (QuickDASH) Quick Disabilities of the Arm, Shoulder and Hand questionnaire*
ResultOutcome measure Baseline 5 weeks
QuickDASH 68.2 47.7Oxford scale (grip strength) 3/5† +4/5Numerical Pain Rating Scale:‡ at worst at best
9/10 4/10§
7/10 0–3/10||
*The QuickDASH is an abbreviated version of the original 30- item out-come measure. It has only 11 items and measures an individual’s ability to complete tasks and absorb forces, and the severity of his or her symptoms. The QuickDASH uses a five- point Likert scale, from which the patient can select an appropriate number corresponding to symptom severity and functional level: the higher the score, the greater the level of disability (reliability = 0.90, validity = 0.70, minimal detectable change = 11.2%). The QuickDASH is a short and clinically applicable fast outcome measure (Wentre 2016).†Pain.‡Used at every session.§Constant with painkillers.||Intermittent with no painkillers.

N. Thompson
© 2016 Acupuncture Association of Chartered Physiotherapists 65
cost- effectiveness of acupuncture and steroid injections would warrant further research.
There were limitations to the present study: only a single case was involved and there was no long- term follow- up, and the author’s knowl-edge of acupuncture was at a foundation level. There is a need for more RCTs investigating the effects of acupuncture treatment, and in particular, in comparison to corticosteroid injec-tions, with a third group using splinting only (Meals 2015).
A different acupuncture approach could have been used; for example, one employing tender muscle points that are non- acupuncture points. Da Silva & Batigalia (2014) suggested that using anatomical knowledge and palpation skills to needle the EPB and APL in addition to LI4, LI10 and LI11 produced a better treat-ment reaction. This was on the basis that, when tendons are primarily damaged, muscles are also involved as painful areas or through muscle spasm. Furthermore, the segmental analgesia effect could have been used differently; for example, by not needling the damaged tissue through TE5, LU9 and LU7, but by applying acupuncture to tissues that were supplied by the same myotome or dermatome (Bradnam 2003, 2007).
Kubo et al. (2011) found that blood flow to the Achilles tendon increased in the side receiv-ing acupuncture during treatment, and then in the contralateral side after the needles had been removed. Therefore, on the basis of the above study, the TE5, LU9 and LU7 points on the contralateral side could have been needled using the central effect of acupuncture through the spinal or supraspinal sympathetic reflexes (Bradnam 2003, 2007; Kubo et al. 2011). This could have reduced tendon soreness during the following day, and might have had a more pronounced pain- relieving effect.
Compared to corticosteroid injections, acupuncture has less side- effects. White et al. (2008) found only a 3% risk of mild and short- lived adverse events (e.g. bleeding, aggravation of symptoms, needling pain, drowsiness and faintness) during acupuncture treatment, and concluded that it presents a negligible risk of serious adverse events. Vas et al. (2008)
described similar findings: no adverse events were reported among the 202 participants who were recruited to their acupuncture group.
At present, rest, NSAIDs and corticosteroid injections are the treatments that are most com-monly used for DQT in clinical practice. The present case study shows that acupuncture could help to reduce thumb and wrist pain, but further research, particularly an RCT, will be necessary to confirm this. However, acupuncture could prove to be a useful tool in the management of DQT.
AcknowledgementsI would like to thank Paul Battersby, whose inspirational tutoring made the AACP founda-tion course very interesting. I would also like to thank my family for supporting me during the course, and my colleagues for giving me clinical advice.
ReferencesAcupuncture Association of Chartered Physiotherapists
(AACP) (2015) Acupuncture Foundation Course Manual, Version 2.4. Acupuncture Association of Chartered Physiotherapists, Peterborough.
Avci S., Yilmaz C. & Sayli U. (2002) Comparison of non-surgical treatment measures for de Quervain’s disease of pregnancy and lactation. The Journal of Hand Surgery 27 (2), 322–324.
Bradnam L. (2003) A proposed clinical reasoning model for western acupuncture. New Zealand Journal of Physiotherapy 31 (1), 40–45.
Bradnam L. (2007) A proposed clinical reasoning model for Western acupuncture. Journal of the Acupuncture Association of Chartered Physiotherapists 2007 (January), 21–30.
Brukner P. & Khan K. (2012) Brukner’ & Khan’s Clinical Sports Medicine, 4th edn. McGraw- Hill Education, North Ryde, NSW.
Cardone D. A. & Tallia A. F. (2002) Joint and soft tissue injection. American Family Physician 66 (2), 283–289.
Da Silva J. B. G. & Batigália F. (2014) Acupuncture in De Quervain’s disease: a treatment proposal. Acupuncture in Medicine 32 (1), 70–72.
De Almeida M. dos S., de Aro A. A., Guerra F. D. R., et al. (2012) Electroacupuncture increases the concentration and organization of collagen in a tendon healing model in rats. Connective Tissue Research 53 (6), 542–547.
De Almeida M. dos S., Guerra F. D. R., de Oliveira L. P., Vieira C. P. & Pimentel E. R. (2014) A hypothesis for the anti- inflammatory and mechanotransduction
Acupuncture for De Quervain’s disorder/tenosynovitis
© 2016 Acupuncture Association of Chartered Physiotherapists66
molecular mechanism underlying acupuncture tendon healing. Acupuncture in Medicine 32 (2), 178–182.
Hadianfard M., Ashraf A., Fakheri M. & Nasiri A. (2014) Efficacy of acupuncture versus local methylpredniso-lone acetate injection in De Quervain’s tenosynovitis: a randomized controlled trial. Journal of Acupuncture and Meridian Studies 7 (3), 115–121.
Howell E. R. (2012) Conservative care of De Quervain’s tenosynovitis/tendinopathy in a warehouse worker and recreational cyclist: a case report. The Journal of the Canadian Chiropractic Association 56 (2), 121–127.
Kubo K., Yajima H., Takayama M., et al. (2011) Changes in blood circulation of the contralateral Achilles tendon during and after acupuncture and heating. International Journal of Sports Medicine 32 (10), 807–813.
Kume K., Amano K., Yamada S., et al. (2012) In de Quervain’s with separate EPB compartment, ultrasound- guided steroid injection is more effec-tive than a clinical injection technique: prospective open- label study. The Journal of Hand Surgery (European Volume) 37 (6), 523–527.
Meals R. A. (2015) Efficacy of acupuncture for De Quervain’s tenosynovitis. [Letter.] Journal of Acupuncture and Meridian Studies 8 (1): 1. DOI: 10.1016/ j.jams.2014.11.006.
Mehdinasab S. A. & Alemohammad S. A. (2010) Methylprednisolone acetate injection plus casting versus casting alone for the treatment of de Quervain’s teno-synovitis. Archives of Iranian Medicine 13 (4), 270–274.
Moore J. S. (1997) De Quervain’s tenosynovitis: stenos-ing tenosynovitis of the first dorsal compartment. Journal of Occupational and Environmental Medicine 39 (10), 990–1002.
Neal B. S. & Longbottom J. (2012) Is there a role for acu-puncture in the treatment of tendinopathy? Acupuncture in Medicine 30 (4), 346–349.
Pearce L. (2015) The Gall Bladder meridian. Acupuncture in Physiotherapy 27 (1), 65–71.
Peters- Veluthamaningal C., van der Windt D. A. W. M., Winters J. C. & Meyboom- de Jong B. (2009) Corticosteroid injection for de Quervain’s tenosynovi-tis. Cochrane Database of Systematic Reviews, Issue 3. Art. No.: CD005616. DOI: 1 0.1002/14651858.CD005616.pub2.
Vas J., Ortega C., Olmo V., et al. (2008) Single- point acupuncture and physiotherapy for the treatment of painful shoulder: a multicentre randomized controlled trial. Rheumatology 47 (6), 887–893.
Walker- Bone K., Palmer K. T., Reading I., Coggon D. & Cooper C. (2004) Prevalence and impact of muscu-loskeletal disorders of the upper limb in the general population. Arthritis and Rheumatism 51 (4), 642–651.
Wentre N. (ed.) (2016) DASH Outcome Measure. [WWW document.] URL http://www.physio- pedia.com/DASH_ Outcome_Measure
White A., Cummings W. & Filshe J. (eds) (2008) An Introduction to Western Medical Acupuncture. Churchill Livingstone, Edinburgh.
Yin Yang House (YYH) (2016) Acupuncture Points. [WWW document.] URL https://theory. yinyanghouse.com/acupuncturepoints/locations_ theory_and_clinical_applications
Following a career change, Nora Thompson studied for her BSc in Physiotherapy at St George’s University Hospitals NHS Foundation Trust in London. After graduating in 2010, she initially worked briefly at Homerton University Hospital in London before spending over 2 years at Central London Community Healthcare NHS Trust. Nora decided to specialize in musculoskeletal physiotherapy, and joined London North West Healthcare NHS Trust in 2014. She currently works as a band 6 physiotherapist, and has completed the AACP Foundation Course.

© 2016 Acupuncture Association of Chartered Physiotherapists 67
Correspondence: Kathryn Fishlock, Centre for Clinical Physiotherapy, St Joseph’s Hospital, Harding Avenue, Malpas, Newport NP20 6ZE, UK (e- mail: [email protected]).
Acupuncture in Physiotherapy, Volume 28, Number 1, Spring 2016, 67–75
CASE REPORT
Acupuncture for plantar fasciitis
K. Fishlock & G. AldridgeCentre for Clinical Physiotherapy, St Joseph’s Hospital, Newport, UK
AbstractPlantar fasciitis is a common musculoskeletal disorder that is frequently treated by physi-otherapists. However, the evidence supporting the appropriate treatment and management of patients with this dysfunction is currently lacking clarity and rigour. This study describes the clinical application of acupuncture for plantar fasciitis in a previously fit and well 57- year- old man exhibiting hyperalgesia of the plantar aspect of his foot. The author reviews the cur-rent literature on treatment approaches and recommendations for physiotherapy manage-ment, examines the principles underpinning the Western medical acupuncture approach to this particular case, and makes recommendations for future research.
Keywords: acupuncture, hyperalgesia, plantar fasciitis.
IntroductionPlantar fasciitis is an inflammatory reaction caused by chronic irritation of the plantar aponeurosis at its origin on the calcaneus (Tortora & Grabowski 2003). It affects approxi-mately 10% of the general population, and is characterized by pain and tenderness upon weight- bearing that is centred on the medial calcaneal tubercle (Zhang et al. 2011). The aponeurosis becomes less elastic with age, and although weight- bearing activities including running, jogging and lifting heavy objects con-tribute to plantar fasciitis, poor biomechanics can also be major factors. For example, flat feet, high arches and an abnormal gait pattern can all cause uneven weight distribution throughout the foot.
The literature provides evidence for an array of conservative treatments for plantar fasciitis,
including: stretching (Dimou et al. 2004); night splints (Batt et al. 1996); taping (Martin 2001); soft- tissue therapy, therapeutic ultrasound and steroid injection (Crawford et al. 1999); heat, ice and extracorporeal shockwave therapy (NICE 2009); and acupuncture (Li et al. 2014). Surgery is recommended as a last resort, usually after multiple failed attempts at conservative manage-ment (Orchard 2012). Although the alleviation of pain is the primary aim of treatment for patients presenting with this dysfunction, it is important to address the causative biomechani-cal influences. Bolgla & Malone (2004) studied the link between plantar fasciitis and the “wind-lass mechanism”, highlighting a biomechanical link to clinical practice. They provided a model that can aid clinicians in formulating a relation-ship between conditions and treatments based on abnormalities of the plantar fascia.
Acupuncture is commonly used to treat mus-culoskeletal pain disorders in clinical settings, and there is published evidence supporting its use in the treatment of plantar fasciitis (Zhang et al. 2011). Some studies have evaluated the

Acupuncture for plantar fasciitis
© 2016 Acupuncture Association of Chartered Physiotherapists68
efficacy and specificity of acupuncture treat-ment by focusing on acupoint selection, while others have compared the effectiveness of myofascial trigger point (MTP) release by dry needling with other treatment modalities. A ran-domized controlled trial (RCT) by Zhang et al. (2011) examined the differences between nee-dling Pericardium (PC) 7 (treatment group) and Large Intestine (LI) 4 (control group) for the treatment of heel pain. Treatment was admin-istered five times a week for a fortnight, and the method used to needle the two acupoints was identical. The results were positive for the treatment of plantar fasciitis with acupuncture, and highlighted that PC7 was significantly more effective at relieving morning pain at 1 month, overall pain and pain on activity, supporting its use as a specific acupoint for heel pain (Zhang et al. 2011).
Cotchett et al. (2010) reviewed the literature on the effectiveness of dry needling and the injection of MTPs associated with plantar heel pain (i.e. plantar fasciitis). This alternative approach involves directly needling the source of pain without reference to the local acupoints mapped on meridians. The inclusion criteria were limited to literature identifying RCTs and non- randomized controlled trials, and included patients diagnosed with plantar heel pain who were treated with dry needling and/or injections alone, or in combination with acupuncture. Only three trials matched the criteria: two of these reported a reduction in pain when MTP dry needling was combined with acupuncture (Tillu & Gupta 1998; Perez- Millan & Foster 2001); and the third found a reduction in pain using 1% lidocaine injections in combination with physical therapy (Imamura et al. 1998). The literature review highlighted that the methodol-ogy of all three studies was poor, and concluded that, because of limited evidence for the effec-tiveness of dry needling and/or injections of MTPs associated with plantar heel pain, further trials were indicated.
The pain- relieving mechanisms of acupunc-ture are well documented, and include centrally mediated opioid pain inhibition, diffuse noxious inhibitory controls and anti- inflammatory effects (White et al. 2008). The rationale for
acupuncture point selection is based on what the clinician is trying to achieve, and can be dependent on patient characteristics rather than the specific type of pain dysfunction. It has been argued that the insertion of a needle into any part of the body may alleviate pain by stimulating the release of opioids or diffuse noxious inhibitory controls, and that the action of anti- inflammatory responses may be general-ized across the whole body (Le Bars et al. 1979). Therefore, this poses the often- asked question: does point selection ultimately have an effect on outcome?
Case reportA previously fit and well 57- year- old man presented with hyperalgesia of the plantar aspect of his foot. The subjective assessment is outlined in Table 1. Further assessment and treatment are detailed in Table 2.
Based on the available evidence, the National Institute for Health and Care Excellence (NICE, formerly the National Institute for Health and Clinical Excellence) produced a clinical knowledge summary of plantar fasciitis in order to provide primary care practitioners with an accessible outline of best practice for its management (NICE 2014). The summary recommends that, initially, patients should be provided with an overview of their presenting condition, and then given self- management advice. This advice should emphasize that most people make a complete recovery within 6 months of beginning conservative treatment. The guidance includes: rest; footwear with a good arch support; orthotics to correct foot pronation; analgesic medications including non- steroidal anti- inflammatory drugs; weight loss; and ice therapy. Once the self- management advice has been issued, NICE (2014) advo-cates self- physiotherapy, and describes a range of stretches for the patient to carry out independently. At no point in the summary are physiotherapy or the use of acupuncture mentioned.
It has been established that there is evidence to support various physiotherapeutic treatment modalities for plantar fasciitis. Because the present subject was not tolerant of manual

K. Fishlock & G. Aldridge
© 2016 Acupuncture Association of Chartered Physiotherapists 69
techniques initially, acupuncture was offered as an adjunct since it has been shown to facilitate improved pain responses. He was screened for contraindications and precautions to needling, an information leaflet was issued and written informed consent was obtained.
Along with other Chinese studies (Wu 2002; Zhu & Zhou 2003), Zhang et al. (2011) have provided evidence to support the use of acu-puncture, and it has been shown to be effective in facilitating physiotherapeutic interventions in the management of specific musculoskeletal dysfunctions (França et al. 2008). Furthermore, a recent study of electroacupuncture in rat models demonstrated that its use produced a central modulating effect on capsaicin- induced central sensitized pain (Kim et al. 2009).
Historically, a great deal of acupuncture research has been supported by systematic reviews of Chinese literature, but a large number of these reviews have been criticized for having extremely poor methodological quality and little scientific grounding. Recently, a review of the reporting characteristics and epidemiological
data of 88 studies found that: 27.3% were written by clinicians; 35.2% were published in speciality journals; and only 36.4% reported any assessment of publication bias (Ma et al. 2012). The above authors noted that the impact fac-tor for how frequently the average article had been cited in a given time period was 0. In the absence of high- quality RCTs of the efficacy of acupuncture in plantar fasciitis, it is important to examine the effects underpinning its use, and also describe the rationale for how it affects pain modulation. Therefore, it is necessary to examine the physiology of stimulation regis-tered at the conscious level of local, segmental and extrasegmental points.
Table 3 provides details of each treatment session, and Table 4 illustrates the principles underpinning each point used in terms of its segmental level. The subject’s pain was located on the plantar aspect of his left foot, and therefore, when considering segmental effects, this region would be largely supplied by the nerve roots L5 and S1 (White et al. 2008). As dermatomal mapping varies significantly in the
Table 1. Patient profile and relevant subjective findings: (VAS) visual analogue scale
Variable Findings
Presenting complaint Chronic left foot pain, medial aspect, improving with the use of an Aircast boot and insolesHistory of presenting complaint
Eight-month history, insidious onset, no traumaGeneral practitioner – pain reliefPrivate consultant – cortisone injection into medial plantar fascia immediately relieved pain, but this only lasted for 4–5 days
Investigations Magnetic resonance imaging – minor oedema within the central band of the plantar fascia in keeping with plantar fasciitis
Previous history NilPrognosis Improving with changes made by consultant – orthotics and Aircast boot (only worn in
evenings)Past medical history Hypertension, otherwise fit and wellDrug history AmlodipineSocial history Work – operational manager, in work, lots of walking
Hobbies – golf, unable to play at presentImpression Plantar fasciitisConcerns Improvements are slowExpectation May helpPrimary problem Medial foot and heel painPain Constant medial pain – VAS = 5/10, worsens to VAS = 8/10Red flags NilNeurology Some numbness bilateral toesAggravating Walking, weight- bearing, plantar flexion with compressionEases Co- dydramol, ibuprofen, stretchesTwenty- four- hour pattern Stiff on rising for 20 min, eases mid- morning, then progressively worsens throughout the daySeverity MildIntensity HighNature Inflammatory nociceptive, mechanical nociceptive, centralized features of hyperalgesia

Acupuncture for plantar fasciitis
© 2016 Acupuncture Association of Chartered Physiotherapists70
Tab
le 2
. A
sses
smen
t an
d tr
eatm
ent:
(VC
G)
verb
al c
onse
nt g
aine
d; (
VA
S) v
isua
l an
alog
ue s
cale
; (L
EFS
) L
ower
Ext
rem
ity F
unct
iona
l Sc
ale;
(PF
) pl
anta
r fa
scia
; (I
SQ)
in s
tatu
s qu
o; (
NA
D)
no
abno
rmal
ities
det
ecte
d; (
R =
L)
right
equ
al t
o le
ft;
(AR
OM
) ac
tive
rang
e of
mov
emen
t; (D
F) d
orsi
flexi
on;
(PG
) pl
anta
rgra
de;
(PF)
pla
ntar
flexi
on;
(GN
) ga
stro
cnem
ius;
and
(B
PI)
Brie
f Pa
in
Inve
ntor
y
Dat
e of
ses
sion
Var
iabl
e20
/01/
1527
/01/
1503
/02/
1506
/02/
1510
/02/
15
Subj
ectiv
e as
sess
men
t
VC
G f
or o
bjec
tive
asse
ssm
ent,
trea
tmen
t
and
plan
L
EFS
= 1
9% (
seve
rely
dis
able
d w
ith
func
tiona
l tas
ks)
VC
GV
AS
= 6
/10
Stre
tche
s he
lp, u
sing
Airc
ast
boot
at
nigh
t to
offl
oad
he
lps,
patie
nt h
as e
aten
VC
GSl
ight
ly im
prov
edN
o ad
vers
e ef
fect
s, im
prov
ed
VA
S 36
h a
fter
tre
atm
ent,
patie
nt h
as e
aten
VC
GN
o ad
vers
e ef
fect
s fr
om
last
tre
atm
ent
sess
ion
VA
S =
5/1
0 (c
onst
ant)
U
nsur
e if
rel
ated
to
plan
tar
fasc
ia s
tret
ches
VC
GN
o ad
vers
e ef
fect
s, pa
tient
fee
ls
a lo
t be
tter
ove
rall
VA
S =
1/1
0
Obs
erva
tions
Patie
nt o
verw
eigh
tR
educ
ed w
eigh
t- be
arin
g in
left
foo
t, m
edia
l as
pect
, inc
reas
ed c
allu
s fo
rmat
ion
on la
tera
l as
pect
of
foot
ISQ
Impr
oved
wei
ght-
bear
ing
in
left
foo
t
Impr
oved
wei
ght-
bear
ing
on
med
ial a
spec
t of
foo
t
Foot
pos
ture
: R =
L in
sta
nce
Neu
rolo
gica
lN
AD
, sen
sory
/mot
or L
3–S2
A
nkle
AR
OM
DF
= P
G –
10°
PF =
PG
+10
°In
eve
rsio
n: R
= L
ISQ
DF
= P
G –
15°
Fu
ll A
RO
M: L
= R
Mid
- foo
t A
RO
M S
ubta
lar
stiff
ness
with
P- A
Mob
ile m
id- f
oot,
no s
tiffn
ess
of t
arsa
lsIS
Q
ISQ
L
ess
stiff
ness
with
PA
at
subt
alar
join
t Sl
ight
sub
tala
r st
iffne
ss, n
ot
tend
erPa
lpat
ion
Incr
ease
d te
nder
ness
of
left
foo
t m
edia
l su
b- m
alle
olus
, dee
p pa
lpat
ion
of P
F pa
in +
+Tr
igge
r po
int
palp
atio
n an
d te
nder
ness
of
med
ial G
N
ISQ
Med
ial a
spec
t of
left
foo
t
less
ten
der
Les
s hy
pers
ensi
tivity
to
light
to
uch
on m
edia
l asp
ect
of
foot
Muc
h im
prov
ed t
oler
ance
to
deep
tou
ch
Gai
t
Red
uced
wei
ght-
bear
ing
on m
edia
l asp
ect
of
left
foo
t
Red
uced
hee
l str
ike
ISQ
Impr
oved
wei
ght-
bear
ing
Im
prov
ed h
eel s
trik
e
NA
D
Mus
cle
leng
thR
educ
ed G
N a
nd P
FIS
QIm
prov
ed G
NIm
prov
ed P
FN
AD
, R =
LTr
eatm
ent
Prog
nosi
s ad
vice
and
rea
ssur
ance
, gai
t re
- edu
catio
nH
ome
exer
cise
pro
gram
me:
sim
ple
AR
OM
ex
erci
ses,
GN
and
PF
stre
tche
sD
iscu
ssed
aim
s an
d be
nefit
s of
acu
punc
ture
, as
wel
l as
adve
rse
effe
cts
and
cont
rain
dica
tions
See
Tab
le 3
Enc
oura
ged
gait
re- e
duca
tion
to a
id c
arry
- ove
r be
twee
n st
retc
hes,
emph
asiz
ing
next
24
h
See
Tab
le 3
Enc
oura
ged
heel
str
ike
on
gait
and
PF s
tret
ches
as
tole
rate
d
See
Tab
le 3
Follo
win
g ac
upun
ctur
e,
gent
le s
oft-
tissu
e m
obili
zatio
n 3
× 3
0 s
to P
F, m
edia
l glid
e
See
Tab
le 3
Follo
win
g ac
upun
ctur
e,
mob
iliza
tion
with
mov
emen
t at
su
btal
ar jo
int,
into
DF,
4 ×
30
s, gr
ade
II
Ana
lysi
s/ou
tcom
e
Plan
tar
fasc
iitis,
hyp
eral
gesi
a, c
entr
al
chan
ges,
biom
echa
nica
l ada
ptat
ions
; not
to
lera
nt o
f m
anua
l tre
atm
ent
Und
erst
ood,
info
rmed
con
sent
gai
ned
for
al
l adv
ised
tre
atm
ents
BPI
= 8
/10
(sev
erity
), 6.
7/10
(inte
rfer
ence
)
No
adve
rse
effe
cts
VA
S =
4/1
0
No
adve
rse
effe
cts,
tole
rate
d in
crea
sed
dose
VA
S =
4/1
0
No
adve
rse
effe
cts,
tole
rate
d do
sePa
in- f
ree
PF p
assi
ve s
tret
ch
follo
win
g tr
eatm
ent
No
adve
rse
effe
cts
BPI
= 3
/10
(sev
erity
), 4.
5/10
(inte
rfer
ence
)L
EFS
= 6
9%
Plan
Tr
ial a
cupu
nctu
re f
or 1
mon
th, w
ritte
n
cons
ent
gain
edG
reat
er d
ose
tole
rabl
e G
reat
er d
ose
tole
rabl
e G
reat
er d
ose
tole
rabl
e C
ontin
ue t
o ad
d lo
ad, m
anua
l tr
eatm
ent

K. Fishlock & G. Aldridge
© 2016 Acupuncture Association of Chartered Physiotherapists 71
literature, White et al.’s (2008) description was applied for the purposes of the present case study, allowing for one level above and below to be classified as segmental. Nerve roots descend-ing from areas more than one level superior or inferior to the affected region were classified as extrasegmental.
The stimulation of local sensory afferent free nerve endings by needle insertion in the skin and nerve fibres in muscle tissue has been shown to elicit an axon reflex. This reflex releases vasoactive neuropeptides, including calcitonin gene- related peptide and histamine, which dilates nearby blood vessels and increases blood flow locally (Sandberg et al. 2003). This has implications for improving the healing
capacity of the underlying tissues in acute and chronic conditions. Both large myelinated Aβ and small myelinated Aδ nerve fibres in the skin, and type II and III nerve fibres within the muscle tissue are stimulated by acupuncture because of its subcutaneous nature (White et al. 2008). In patients whose pain response means that they have a lower tolerance for manual therapy, as in the present case, this method of stimulating these deeper afferent fibres may be more appropriate.
White et al. (2008) described segmental inhibition as the primary mechanism by which acupuncture relieves pain. Segmental stimula-tion of the spinal cord via the afferent fibres of the dorsal horn is thought to depress activity,
Table 3. Acupuncture treatment (patient in prone with feet propped up on three pillows for comfort): (LI) Large Intestine; (LR) Liver; (BL) Bladder; (KI) Kidney; (GB) Gall Bladder; (TE) Triple Energizer; (BPI) Brief Pain Inventory; (VAS) visual analogue scale; (LEFS) Lower Extremity Functional Scale; (AROM) active range of movement; (M/L) muscle length; and (N/A) not applicable
DateAcupuncture points* Depth (cm) Time (min) De Qi
Stimulation time (min)
Outcome measure
Adverse effects
Session 127/01/15
LI4 (bilateral)LR3 (bilateral)BL57 (left)BL60 (left)
1.01.01.0–1.50.5–1.0
20
YesYesYesYes
10
BPIVASLEFS
N/A†
Session 2 03/02/15
LI4 (bilateral)LR3 (bilateral)BL57 (left)BL60 (left)KI3 (left)GB41 (left)
1.01.01.0–1.50.5–1.00.50.5
20
YesYesYesYesYesYes
10
VASAROMM/L
N/A
Session 306/02/15
LI4 (bilateral)LR3 (bilateral)BL57 (left)BL60 (left)KI3 (left)GB41 (left)GB39 (left)
1.01.01.0–1.50.5–1.00.50.50.5
20
YesYesYesYesYesYesYes
5
VASAROMM/L
N/A
Session 4 10/02/15
LI4 (bilateral) LR3 (bilateral) BL57 (left) BL60 (left) KI3 (left) GB41 (left) GB39 (left) TE5 (left)
1.0 1.0 1.0–1.5 0.5–1.0 0.5 0.5 0.5 1.0–2.0
20
Yes Yes Yes Yes Yes Yes Yes Yes
5
BPI LEFS VAS
N/A
*All points perpendicular.†Global relaxation effect.
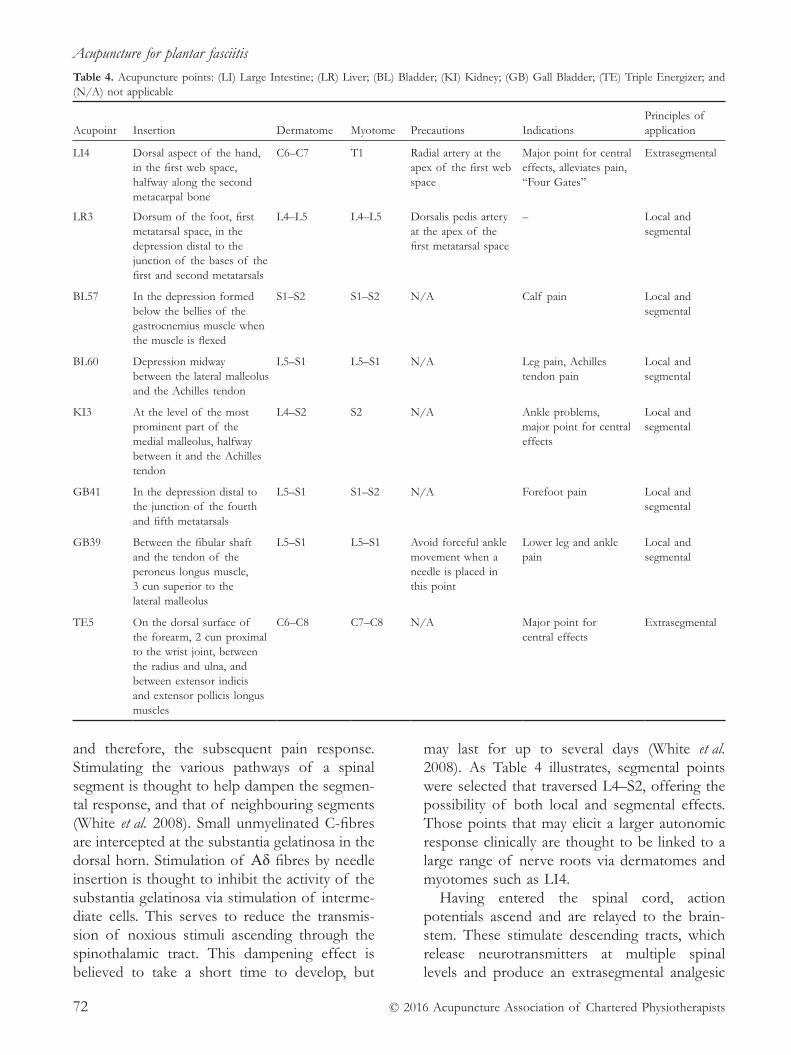
Acupuncture for plantar fasciitis
© 2016 Acupuncture Association of Chartered Physiotherapists72
and therefore, the subsequent pain response. Stimulating the various pathways of a spinal segment is thought to help dampen the segmen-tal response, and that of neighbouring segments (White et al. 2008). Small unmyelinated C- fibres are intercepted at the substantia gelatinosa in the dorsal horn. Stimulation of Aδ fibres by needle insertion is thought to inhibit the activity of the substantia gelatinosa via stimulation of interme-diate cells. This serves to reduce the transmis-sion of noxious stimuli ascending through the spinothalamic tract. This dampening effect is believed to take a short time to develop, but
may last for up to several days (White et al. 2008). As Table 4 illustrates, segmental points were selected that traversed L4–S2, offering the possibility of both local and segmental effects. Those points that may elicit a larger autonomic response clinically are thought to be linked to a large range of nerve roots via dermatomes and myotomes such as LI4.
Having entered the spinal cord, action potentials ascend and are relayed to the brain-stem. These stimulate descending tracts, which release neurotransmitters at multiple spinal levels and produce an extrasegmental analgesic
Table 4. Acupuncture points: (LI) Large Intestine; (LR) Liver; (BL) Bladder; (KI) Kidney; (GB) Gall Bladder; (TE) Triple Energizer; and (N/A) not applicable
Acupoint Insertion Dermatome Myotome Precautions IndicationsPrinciples of application
LI4
Dorsal aspect of the hand, in the first web space, halfway along the second metacarpal bone
C6–C7
T1
Radial artery at the apex of the first web space
Major point for central effects, alleviates pain, “Four Gates”
Extrasegmental
LR3
Dorsum of the foot, first metatarsal space, in the depression distal to the junction of the bases of the first and second metatarsals
L4–L5
L4–L5
Dorsalis pedis artery at the apex of the first metatarsal space
–
Local and segmental
BL57
In the depression formed below the bellies of the gastrocnemius muscle when the muscle is flexed
S1–S2
S1–S2
N/A
Calf pain
Local and segmental
BL60
Depression midway between the lateral malleolus and the Achilles tendon
L5–S1
L5–S1
N/A
Leg pain, Achilles tendon pain
Local and segmental
KI3
At the level of the most prominent part of the medial malleolus, halfway between it and the Achilles tendon
L4–S2
S2
N/A
Ankle problems, major point for central effects
Local and segmental
GB41
In the depression distal to the junction of the fourth and fifth metatarsals
L5–S1 S1–S2
N/A
Forefoot pain
Local and segmental
GB39
Between the fibular shaft and the tendon of the peroneus longus muscle, 3 cun superior to the lateral malleolus
L5–S1
L5–S1
Avoid forceful ankle movement when a needle is placed in this point
Lower leg and ankle pain
Local and segmental
TE5
On the dorsal surface of the forearm, 2 cun proximal to the wrist joint, between the radius and ulna, and between extensor indicis and extensor pollicis longus muscles
C6–C8
C7–C8
N/A
Major point for central effects
Extrasegmental

K. Fishlock & G. Aldridge
© 2016 Acupuncture Association of Chartered Physiotherapists 73
effect (White et al. 2008). Needle insertion has been shown to release naturally occurring neuromodulator peptides including β- endorphin and enkephalin. These act on the midbrain and periaqueductal grey matter, respectively, modify-ing the activity of target cells (White et al. 2008). This modification is thought to dampen noci-ception over a period of time. The extrasegmen-tal points utilized in the present case study were LI4 and Triple Energizer 5. In addition, there may have been greater potential for inhibition from LI4, which spans nerve roots from C6 to T1 and potentially innervates multiple segments.
To accommodate for the potential for adverse sympathetic effects, the present subject was positioned in prone, and his legs were elevated on a pillow for comfort and to reduce tone. Because he did not report any parasympa-thetic relaxation response during the treatment sessions, and no adverse effects were noted at all, the dose was increased at each session (see Table 3). There appears to be a lack of scientific evidence for the number of needles required, but it is thought that between four and six is an appropriate starting point, depend-ing on a patient’s expectations of the technique (White et al. 2008). The depth of needling was selected in order to elicit the desired effect of local stimulation with respect to the underlying anatomy. As the pain response eased in the lat-ter sessions, manual therapy was applied to the plantar fascia, which was not needled because of tenderness.
Needle stimulation, which involved rotation and changing depths, was applied after percep-tion of each needle was normalized, suggesting modulation to the noxious stimulus. This took place at 10 min initially, and then progressed to every 5 min over the course of the treatment sessions. In a small (n = 53), single- blinded cross- over study, Choi et al. (2013) examined the correlation of both needle stimulation (rotation) and depth (0.3 versus 2.0 cm) with analgesic effect, as measured by pressure- pain thresholds in healthy volunteers. The above author’s results demonstrated that stimulation followed by increasing depth was most effec-tive in reducing pressure- pain thresholds. Since the present subject showed no adverse effects
during the early treatment sessions, the dose was further increased by adding both segmental and extrasegmental points, and intensifying the frequency of stimulation. Each treatment ses-sion lasted 20 min since this allowed the present author time to review subjective and objective markers within a total appointment time of 30 min. To facilitate the subject’s recovery and carryover between sessions, he was encour-aged to follow a home programme of gait re- education, active exercise and triceps surae stretches.
Reliable and valid outcome measures are essential to measuring treatment effects accu-rately. In the present clinical scenario, a visual analogue scale (VAS) was used to measure the severity of the subject’s pain. The VAS is widely used as a valid and reliable tool (Revill et al. 1976; Price et al. 1983). The Lower Extremity Functional Scale (Binkley et al. 1999) and Brief Pain Inventory (Cleeland & Ryan 1994) were utilized because these are robust measurements of the impact of plantar fasciitis on a patient’s physical and psychosocial well- being.
DiscussionThe present case study highlights the positive effects of using acupuncture as an adjunct to traditional treatment modalities in the treatment of plantar fasciitis. However, given its single- participant nature, it would be improper to infer that this patient would not have progressed independently without receiving acupuncture. The long- term prognosis for plantar fasciitis is good, with one prospective survey reporting that over 80% of people achieved complete resolu-tion of their symptoms within a year (Wolgin et al. 1994).
The present author was relatively inexpe-rienced in the subtleties of acupuncture as a treatment modality, and although the points employed were thoroughly researched in stand-ard texts and current available evidence, these might have been utilized differently by a clini-cian who was more experienced in this field. For example, it could have been beneficial to utilize MTP principles specifically in those mus-cle groups indicated, such as the palpable tender

Acupuncture for plantar fasciitis
© 2016 Acupuncture Association of Chartered Physiotherapists74
points in the gastrocnemius musculature or the plantar fascia directly, as per Cotchett et al. (2011). It is thought that the axon reflex covers an area of 25 mm (White et al. 2008), and there-fore, local application around affected tissue may stimulate a larger axon reflex. Furthermore, Zhang et al. (2011) advocated the use of PC7 in the treatment of heel pain; however, in the present case, alternative extrasegmental points were used secondary to its proximity with the median nerve (Tortora & Grabowski 2003). These are factors to bear in mind for future clinical practice.
The traditional Chinese medicine rationale for needle use can involve placing further nee-dles along the same meridian in order to rein-force the action of the points. However, from the perspective of Western medicine, there is experimental evidence that suggests that there are fascial links along the meridians (Langevin & Yandow 2002). This application can still be discussed in terms of the nerve roots that sup-ply the region via the dermatomes, myotomes and peripheral nerve roots (White et al. 2008). However, the use of both Bladder (BL) 57 and BL60 could have supported this analgesic effect. This might have been utilized in terms of increasing the dose or working in an area away from the sensitive area, diminishing the likelihood of reinforcing dysfunctional process-ing via excessively noxious stimuli.
It would not be advisable to extrapolate the findings of the present case study to a wider population. However, it serves as an overview of the current evidence base for the treatment of plantar fasciitis with acupuncture as an adjunct to other treatment modalities, par-ticularly when pain is limiting manual therapy. When the evidence base is poor, it is crucial to return to the principles underpinning the use of acupuncture, and the physiological changes that occur as a result of needling in the man-agement of pain.
Future research is required in this area, and participants experiencing heel pain at varying stages of chronicity should be compared. In particular, high- quality RCTs are needed that explore the specifics of: physiotherapeutic inter-ventions; and acupuncture use, both in terms of
the acupoints utilized, and the dose, frequency and timings of sessions.
AcknowledgmentsMany thanks to our families and work colleagues for their continuing support.
ReferencesBatt M. E., Tanji J. L. & Skattum N. (1996) Plantar
fasciitis: a prospective randomized clinical trial of the tension night splint. Clinical Journal of Sport Medicine 6 (3), 158–162.
Binkley J. M., Stratford P. W., Lott S. A. & Riddle D. L. (1999) The Lower Extremity Functional Scale (LEFS): scale development, measurement properties, and clini-cal application. Physical Therapy 79 (4), 371–383.
Bolgla L. A. & Malone T. R. (2004) Plantar fasciitis and the windlass mechanism: a biomechanical link to clini-cal practice. Journal of Athletic Training 39 (1), 77–82.
Choi Y.- J., Lee J.- E., Moon W.- K. & Cho S.- H. (2013) Does the effect of acupuncture depend on needling sensation and manipulation? Complementary Therapies in Medicine 21 (3), 207–214.
Cleeland C. S. & Ryan K. M. (1994) Pain assessment: global use of the Brief Pain Inventory. Annals of the Academy of Medicine, Singapore 23 (2), 129–138.
Cotchett M. P., Landorf K. B., Munteanu S. E. & Raspovic A. (2010) Effectiveness of dry needling and injections of myofascial trigger points associated with plantar heel pain: a systematic review. Journal of Foot and Ankle Research 3: 18. DOI: 10.1186/1757- 1146- 3- 18.
Crawford F., Atkins D., Young P. & Edwards J. (1999) Steroid injection for heel pain: evidence of short- term effectiveness. A randomized controlled trial. Rheumatology 38 (10), 974–977.
Dimou E. S., Brantingham J. W. & Wood T. (2004) A randomized controlled trial (with blinded observer) of chiropractic manipulation and Achilles stretching vs. orthotics for the treatment of plantar fasciitis. Journal of American Chiropractic Association 41 (9), 32–42.
França D. L. M., Senna- Fernandes V., Cortez C. M., et al. (2008) Tension neck syndrome treated by acupuncture combined with physiotherapy: a comparative clinical trial (pilot study). Complementary Therapies in Medicine 16 (5), 268–277.
Imamura M., Fischer A. A., Imamura S. T., et al. (1998) Treatment of myofascial pain components in plantar fasciitis speeds up recovery: documentation by algom-etry. Journal of Musculoskeletal Pain 6 (1), 91–110.
Kim H. Y., Wang J., Lee I., et al. (2009) Electroacupuncture suppresses capsaicin- induced secondary hyperalgesia through an endogenous spinal opioid mechanism. Pain 145 (3), 332–340.

K. Fishlock & G. Aldridge
© 2016 Acupuncture Association of Chartered Physiotherapists 75
Langevin H. M. & Yandow J. A. (2002) Relationship of acupuncture points and meridians to connective tissue planes. The Anatomical Record 269 (6), 257–265.
Le Bars D., Dickenson A. H. & Besson J.- M. (1979) Diffuse noxious inhibitory controls (DNIC). II. Lack of effect on non- convergent neurones, supraspinal involvement and theoretical implications. Pain 6 (3), 305–327.
Li S., Shen T., Liang Y., Zhang Y. & Bai B. (2014) Miniscalpel- needle versus steroid injection for plantar fasciitis: a randomized controlled trial with a 12- month follow- up. Evidence- Based Complementary and Alternative Medicine 2014: 164714. DOI: 10.1155/2014/164714.
Ma B., Qi G.- Q., Lin X.- T., et al. (2012) Epidemiology, quality, and reporting characteristics of systemic reviews of acupuncture interventions published in Chinese journals. The Journal of Alternative and Complementary Medicine 18 (9), 813–817.
Martin J. E., Hosch J. C., Goforth W. P., et al. (2001) Mechanical treatment of plantar fasciitis: a prospective study. Journal of the American Podiatric Medical Association 91 (2), 55–62.
National Institute for Health and Clinical Excellence (NICE) (2009) Extracorporeal Shockwave Therapy for Refractory Plantar Fasciitis. [WWW document.] URL https://www.nice.org.uk/guidance/ipg311
National Institute for Health and Care Excellence (NICE) (2014) Plantar Fasciitis. [WWW document.] URL http://cks.nice.org.uk/plantar- fasciitis#!topicsummary
Orchard J. (2012) Plantar fasciitis. BMJ 345: e6603. DOI: http://dx.doi.org/10.1136/bmj.e6603.
Perez- Millan R. & Foster L. (2001) Low- frequency electroacupuncture in the management of refractory plantar fasciitis. Medical Acupuncture 13 (1), 47–49.
Price D. D., McGrath P. A., Rafii A. & Buckingham B. (1983) The validation of visual analogue scales as ratio scale measures for chronic and experimental pain. Anaesthesia 17 (1), 45–56.
Revill S. I., Robinson J. O., Rosen M. & Hogg M. I. J. (1976) The reliability of a linear analogue for evaluat-ing pain. Anaesthesia 31 (9), 1191–1198.
Sandberg M., Lundeberg T., Lindberg L.- G. & Gerdle B. (2003) Effects of acupuncture on skin and muscle blood flow in healthy subjects. European Journal of Applied Physiology 90 (1–2), 114–119.
Tillu A. & Gupta S. (1998) Effect of acupuncture treat-ment on heel pain due to plantar fasciitis. Acupuncture in Medicine 16 (2), 66–68.
Tortora G. J. & Grabowski S. R. (2003) Principles of Anatomy and Physiology, 10th edn. John Wiley & Sons, Chichester.
White A., Cummings W. & Filshe J. (eds) (2008) An Introduction to Western Medical Acupuncture. Churchill Livingstone, Edinburgh.
Wolgin M., Cook C., Graham C. & Mauldin D. (1994) Conservative treatment of plantar heel pain: long- term follow- up. Foot and Ankle International 15 (3), 97–102.
Wu M. Y. (2002) Special acupuncture methods to treat heel pain. Moderate Rehabilitation 10, 3112–3112.
Zhang S. P., Yip T.- P. & Li Q.- S. (2011) Acupuncture treat-ment for plantar fasciitis: a randomized controlled trial and six months follow- up. Evidence- Based Complementary and Alternative Medicine 2011: 154108. DOI: 10.1093/ecam/nep186.
Zhu G.- X. & Zhou C. (2003) Clinical observations on treatment of 45 heel pain patients by kidney Qi- reinforcing acupuncture technique. Shanghai Journal of Acupuncture and Moxibustion 2003 (12), 23–24.
Kathryn Fishlock graduated from Cardiff University with a degree in physiotherapy in 2008. She went on to work for Aneurin Bevan University Health Board, where she spent over 6 years completing rotations in all core aspects of physiotherapy before specializing in musculoskeletal outpatients. Kathryn now works in the Centre for Clinical Physiotherapy at St Joseph’s Hospital in Newport. Alongside her full- time post, she is the lead physiotherapist for premiership rugby team Crosskeys RFC.
Garry Aldridge graduated from Cardiff University with a degree in physiotherapy in 2008. He also went on to work for Aneurin Bevan University Health Board, where he spent 7 years, which led to him specializing in musculoskeletal outpatients. Garry then moved into the world of professional football as the lead physiotherapist with Newport County FC. He has recently obtained a post at the Centre of Clinical Physiotherapy at St Joseph’s Hospital in Newport.


© 2016 Acupuncture Association of Chartered Physiotherapists 77
Acupuncture in Physiotherapy, Volume 28, Number 1, Spring 2016, 77–84
CASE REPORT
A biopsychosocial approach to chronic mid- portion Achilles tendinopathy
A. M. DavidsonLocomotor Outpatients Department, Homerton University Hospital NHS Foundation Trust, London, UK
AbstractA 37- year- old male runner with a 7- month history of right- sided mid- portion Achilles tendinopathy was treated with physiotherapy and acupuncture in a National Health Service outpatients department. Along with other conservative management options, acupuncture was used as part of a holistic biopsychosocial approach. The treatment ultimately alleviated the pain and improved function, and helped the subject to achieve his agreed goal. New research is emerging that supports the use of acupuncture for tendon disorders; however, the exact treatment mechanism is not yet fully understood. Suggested mechanisms are dis-cussed with reference to relevant literature.
Keywords: Achilles tendinopathy, acupuncture, biopsychosocial model, load management.
IntroductionTendinopathies account for a large proportion of musculoskeletal complaints. These conditions have a high incidence of chronicity and recur-rence, which results in appreciable morbidity and loss of productivity, and represents a major socioeconomic burden (Maffulli et al. 2003). Chronic tendinopathy encompasses a spectrum of disorders.
Tendons are collagenous structures that contain tenocytes, water and ground substance. These structures are surrounded by loose connec-tive tissue, the paratenon, which forms an elastic sleeve that allows free movement of the tendon. Where tendons travel through narrow areas, this tissue becomes a specialized “tenosynovial sheath” that helps to reduce friction between the tendons and the surrounding structures.
The spectrum of disorders involved in tendi-nopathy includes lesions of the tenosynovium, paratenon and enthesis (i.e. the attachment of the tendon to the bone), and the tendon itself. Achilles tendinopathy is very prevalent in both the sporting and recreational communities, and even in the sedentary population. Recent find-ings suggest that up to 20% of running injuries involve the Achilles tendon. As involvement in recreational sports has increased over the past 50 years, so has the incidence of tendon rupture, which is between four and five times more likely among men, and has a peak occur-rence in those between 30 and 40 years of age (Alfredson & Lorentzon 2000).
The onset of pain is often associated with a sudden change in activity rates; for example, from high to low and back again. This is because the time spent resting or in a more sedentary state reduces the tensile strength of the tendon. When individuals return to their previous level of activity after a prolonged rest, they run the risk of exceeding the load- bearing capacity of
Correspondence: Andrew Michael Davidson, Locomotor Outpatients Department, Homerton University Hos-pital NHS Foundation Trust, Homerton Row, London E9 6SR, UK (e- mail: [email protected]).

Chronic mid- portion Achilles tendinopathy
© 2016 Acupuncture Association of Chartered Physiotherapists78
the tendon and producing microtrauma on a cellular level.
The changes apparent in the tendon itself are a sequence of pathological events that begin with upregulation of its cells, the tenocytes. This is followed by a change in the ground substance from proteoglycan to aggrecan, which has a larger molecular weight and binds more water, thereby causing swelling. After this, changes in the collagen cause cleaving or separation of the collagen bundles, as well as degeneration. Finally, there are changes in vascularity: new vessels develop, accompanied by neural ingrowth, which is believed to lead to tendon pain (Alfredson & Lorentzon 2000). Pain and dysfunction are the main clinical signs of a tendinopathy. Other symptoms include swelling or thickening of the tendon. Appreciable weakness and/or a positive squeeze test suggest a torn or ruptured tendon (Douglas et al. 2009).
The present case report suggests that acu-puncture has a role in the treatment of ten-dinopathies as an adjunct to Western medical physiotherapy.
Case report
BackgroundThe present subject was a 37- year- old man with a 7- month history of right- sided mid- portion Achilles tendinopathy pain. His condition was coupled with reduced mobility and strength, and an inability to return to his hobby of run-ning. He was an avid amateur athlete who had taken part in long- distance runs on an annual basis over the past 10 years.
At the time of the injury, the subject was not preparing for any event. He had recently taken a 2- week holiday, which had involved minimal loading, and then returned to his normal sched-ule when he got back. The subject experienced a gradual onset of pain after a run, and this pro-gressed over the next few days; however, there was no clear mechanism of injury or trauma. He attempted to manage his own symptoms with activity modification for 4 months, but this did not have any effect on his symptoms.
The tendinopathy eventually progressed to the point where the subject had to stop all loading
activity because the pain had begun to affect his gait, especially in the morning and after pro-longed sitting. He sought help from his general practitioner, who prescribed non- steroidal anti- inflammatory drugs, and advised him to perform stretches and use ice to reduce his symptoms at rest. The subject’s inability to return to running had a significant impact on his perceived quality of life. The present author’s subjective assess-ment is outlined in “Appendix 1”.
The subject’s main goal was to reduce the pain and return to his previous level of fitness. However, he had developed unhelpful beliefs about his condition. He had been told that he probably had “arthritis” in his tendon because of his age and the amount of running that he had done. He was also concerned that he might suffer a rupture should he return to his previ-ous level of training.
Clinical impressionA thorough subjective history was taken. After ruling out alternative diagnoses such as a stress fracture or retrocalcaneal bursitis, and using ultrasound sonography to confirm the presence of tendinopathic changes (Fig. 1), a diagnosis of mid- portion Achilles tendinopathy in a state of degenerative disrepair was made.
The subject had bilateral pes planus, and a slightly antalgic gait with reduced weight- bearing and heel strike on the right. Although there was no heat or redness in the affected area, a squeeze test of the mid- portion of the tendon was positive for pain. An ultrasound scan showed no evidence of intrasubstance tears.
Figure 1. Doppler ultrasound scan of a mid- portion Achilles tendinopathy. The arrows indicate the presence of neovessels.

A. M. Davidson
© 2016 Acupuncture Association of Chartered Physiotherapists 79
The thickness of the average Achilles tendon is approximately 6 mm. However, at 1.1 cm, the subject’s right Achilles tendon was approximately twice its normal size on pres-entation. There were also moderate signs of mid- substance neovascularity on the ultrasound scan. An Öhberg score of 3+ (Sengkerij et al. 2009) and a visual analogue scale (VAS) score of 8/10 were recorded.
TreatmentThe examination findings were explained to the subject in detail. The intention was to provide him with an understanding of his symptoms, and offer him reassurance about the apparently poor findings of the ultrasound scan. Although there may be a correlation between the presence of neovascularity and pain, there is no estab-lished cause- and- effect relationship at present, and the evidence base remains ambiguous (Rees et al. 2014).
The subject was informed that stress and anxiety can indirectly influence pain by increas-ing neural sensitivity (O’Sullivan 2005). To give his rehabilitation focus and purpose, a long- term SMART (specific, measurable, attainable, relevant and time- bound) goal was mutually agreed. This involved completing a pain- free (or VAS < 3/10) run of 5–8 miles (approximately 8–13 km) at 50% of his normal running pace within 3 months. The initial focus was on improving his distance rather than his speed since tendon pain and flare- ups are associated with sudden increases in load and tension.
The subject was given a 2- week plan, and was asked to avoiding walking barefoot. He was referred to the foot health department for gait and posture assessment, and the fitting of heel lifts. He was also taught an eccentric loading programme because there is evidence to sup-port this as a method of inducing procollagen synthesis within tendons (Öhberg et al. 2004). However, there has also been a recent drive to focus on the concept of load management, which underpinned this exercise plan (Cook & Purdam 2009).
The principle of load management is to determine the level at which the patient can
safely load the affected joint without pain. This is then gradually progressed during rehabilita-tion on the basis of the available biochemical and histological evidence associated with degen-erative tendinopathies. Fu et al. (2010) proposed a combination of theories that indicated that, while trauma might initiate the inflammatory and remodelling phase of healing, multiple intrinsic and extrinsic factors in a poorly suited environ-ment could result in a failed healing response (Fig. 2). Therefore, because a tendinopathy is essentially an overload injury, managing load and stress through the tendon and joint is essential.
The subject was reviewed after 2 weeks. His pain had reduced from 8/10 to an intermittent 5/10 on the VAS. A light jog had caused his symptoms to flare up for several days. He was advised to avoid running and concentrate on non- impact- based forms of exercise to maintain fitness; for example, cycling, swimming, cross- training and rowing. The subject continued to use ice and a non- steroidal anti- inflammatory gel, which seemed to help somewhat. His exer-cise technique was reviewed to ensure that his training was relatively pain- free. The focus was on slow, controlled movements to eccentrically load the tendon, and improve his hip and knee balance.
During his third visit, 2 weeks later, the sub-ject reported that he had again tried to go for a run because his pain was improving. This time, the flare- up was so severe he had had to take a day off work. At this stage, it was deemed appropriate to offer him acupuncture treatment, primarily in order to provide pain relief. After the risks and benefits of acupuncture were explained, the subject gave his consent and was provided with an information form.
In order to support the clinical reasoning for the points selected (Table 1), the present author utilized the “layering method” sug-gested by Bradnam (2001). While not entirely based on clinical research, this approach is based on “an existing knowledge of anatomy, segmental and peripheral nerve innervation of tissues, and the neuroanatomy of the sympa-thetic nervous system” (Bradnam 2003, 2007, p. 21).
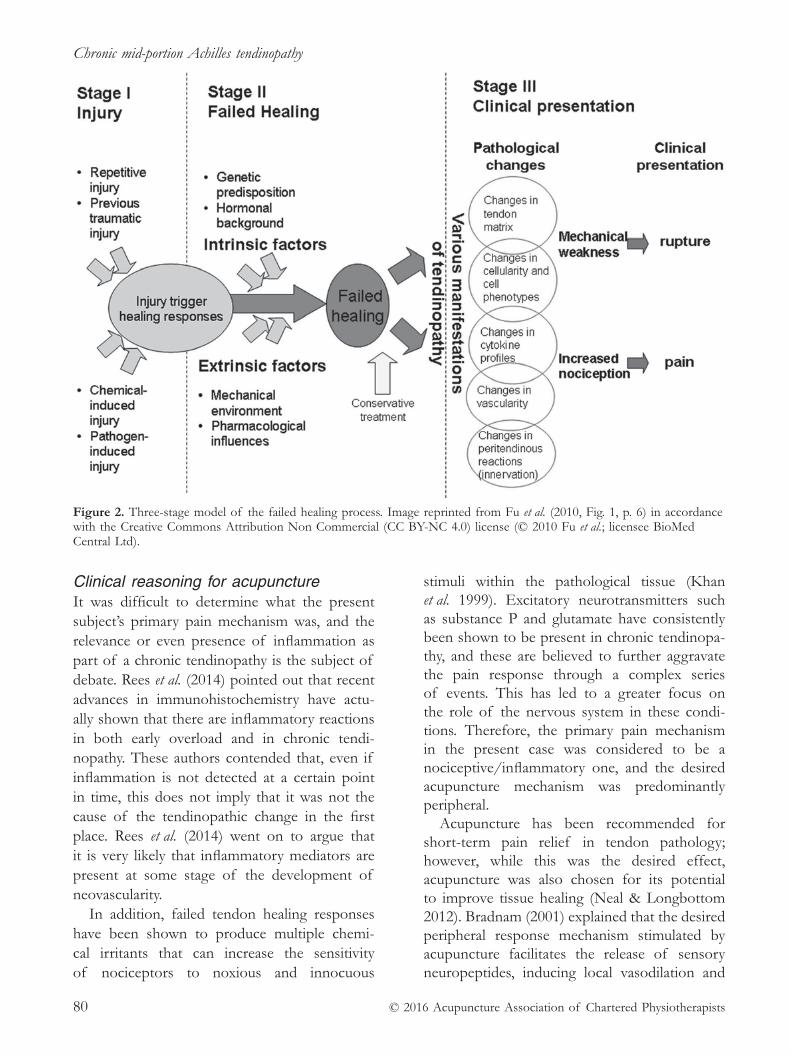
Chronic mid- portion Achilles tendinopathy
© 2016 Acupuncture Association of Chartered Physiotherapists80
Clinical reasoning for acupunctureIt was difficult to determine what the present subject’s primary pain mechanism was, and the relevance or even presence of inflammation as part of a chronic tendinopathy is the subject of debate. Rees et al. (2014) pointed out that recent advances in immunohistochemistry have actu-ally shown that there are inflammatory reactions in both early overload and in chronic tendi-nopathy. These authors contended that, even if inflammation is not detected at a certain point in time, this does not imply that it was not the cause of the tendinopathic change in the first place. Rees et al. (2014) went on to argue that it is very likely that inflammatory mediators are present at some stage of the development of neovascularity.
In addition, failed tendon healing responses have been shown to produce multiple chemi-cal irritants that can increase the sensitivity of nociceptors to noxious and innocuous
stimuli within the pathological tissue (Khan et al. 1999). Excitatory neurotransmitters such as substance P and glutamate have consistently been shown to be present in chronic tendinopa-thy, and these are believed to further aggravate the pain response through a complex series of events. This has led to a greater focus on the role of the nervous system in these condi-tions. Therefore, the primary pain mechanism in the present case was considered to be a nociceptive/inflammatory one, and the desired acupuncture mechanism was predominantly peripheral.
Acupuncture has been recommended for short- term pain relief in tendon pathology; however, while this was the desired effect, acupuncture was also chosen for its potential to improve tissue healing (Neal & Longbottom 2012). Bradnam (2001) explained that the desired peripheral response mechanism stimulated by acupuncture facilitates the release of sensory neuropeptides, inducing local vasodilation and
Figure 2. Three- stage model of the failed healing process. Image reprinted from Fu et al. (2010, Fig. 1, p. 6) in accordance with the Creative Commons Attribution Non Commercial (CC BY- NC 4.0) license (© 2010 Fu et al.; licensee BioMed Central Ltd).

A. M. Davidson
© 2016 Acupuncture Association of Chartered Physiotherapists 81
Table 1. Clinical reasoning for acupuncture: (VAS) visual analogue scale; (VISA- A) Victorian Institute of Sports Assessment – Achilles questionnaire; (N/A) not applicable; (NSAIDs) non- steroidal anti- inflammatory drugs; (SMART) specific, measurable, attainable, relevant, time- bound; (BL) Bladder; (KI) Kidney; (GB) Gall Bladder; and (LI) Large Intestine
Outcome measure
Treatment Acupuncture points Clinical reasoning Response VAS VISA- A
Session 1Advice/educationExercisesIce/NSAIDs
– – – 7/10 39
Session 2Revised exercisesPain managementTapingSoft tissue work
– – – 7/10 N/A
Session 3AcupunctureNon- impact exercisesPain managementReassurance about likely mild flare- up in 24 h
BL60BL61BL62KI3KI4GB34
Prone position, local points to stimulate pain relief and increase blood flow, low initial dose since highly irritableGB34 is an influential point for tendons and a relaxation point
Painful during Relaxed afterErythemaImproved gait
3/10 N/A
Session 4AcupunctureGraded impact exerciseAgreed to start a return to running in 4 weeks
KI3KI4KI5KI6BL58BL60BL62GB34
Prone position, local points for pain relief/circulationIncreased dose since last treatment well tolerated, musculotendinous junction for blood flowHyperstimulation anaesthesia
Painful duringRelief afterErythemaImproved gait
3/10 N/A
Session 5AcupunctureProgress to alternating fast walk and light jogHeel raises with resistance
KI3KI4KI5KI7KI9LI3LI4GB34
Prone position, local points for pain relief/circulationCalming effects for anxiety/stress, try to encourage lasting pain reliefIncreased points into/around tendon to encourage breakdown of dysfunctional collagen to aid tendon remodelling
Painful duringRelief afterErythemaImproved gait
2/10 N/A
Session 6As above As above As above Painful during
Relief afterErythemaImproved gait
2/10 N/A
Session 7AcupunctureProgress to alternating light and regular jog for a maximum of 15 min
As above As above Mild flare- up during jog, eased off after stretches and rest
2/10 N/A
Session 8 Return to run self- management programme Aim to meet SMART goal in 4 weeks
Nil
Minimal symptoms, focus on return to running and improving strength
2/10
64

Chronic mid- portion Achilles tendinopathy
© 2016 Acupuncture Association of Chartered Physiotherapists82
modulating local immune responses. She sug-gested that this is best achieved by needling close to the injured tissue, and using low- intensity stimulation to encourage a peripheral (rather than central) release of neuropeptides (Bradnam 2001).
A healthy tendon requires a strict balance between cell proliferation and death. It is believed that the hypoxic environment present in a tendinopathy may be a primary cause of apoptosis, i.e. programmed cell death. Programmed cell death is the natural elimina-tion of redundant cells; however, it can inter-fere with cell proliferation (Neal & Longbottom 2012). Neovascularity is thought to be the body’s response to this hypoxic state. However, studies have shown that this process does not actually improve tendon vascularity, and as a result, treatments that promote blood flow have been explored for these conditions (Neal & Longbottom 2012). Acupuncture has been shown to improve vasodilation within human tissue, and it may also be able to improve ten-don blood flow.
Since the subject’s ultrasound scan showed a high level of neovascularity, this suggests that hypoxia was a part of his tendon pathology, further supporting the use of acupuncture.
Outcome measuresThe condition- specific Victorian Institute of Sports Assessment – Achilles (VISA- A) questionnaire was used to measure the pre-sent subject’s perceived level of function (Robinson et al. 2001). In addition, a VAS was employed specifically to measure his level of pain. Before the subject underwent acupunc-ture, his VISA- A and VAS scores were 39 and 7/10, respectively. On reflection, it might also have been helpful to use the Patient- Specific Functional Scale, which would have allowed him to choose his own tasks and activities.
DiscussionThe results of the treatment are shown in Table 1. The present subject’s final VISA- A and VAS scores were 64 and 2/10, respectively.
Acupuncture appeared to produce pain relief, improved function, and provided results com-parable to those of other adjunctive treatments (e.g. extracorporeal shockwave therapy, platelet- rich plasma therapy, and autologous blood and corticosteroid injections) without the added risks of rupture or weakening tendon integrity.
A holistic approach was used, and as such, the present results should be interpreted with caution. The subject received treatment that was consistent with a biopsychosocial health-care model, which included the reduction of any health- related stress or anxiety, and the improvement of his sleep pattern. Conservative physiotherapy management was also provided in order to improve his range of movement and strength, and graded load management was used to progress the subject’s return to his previous activity levels. Nevertheless, acupuncture does seem to have played a key role in his recovery, and he subjectively reported a positive response to the treatment.
Further research into the mechanisms under-lying acupuncture would help clinicians to target their interventions more specifically to a condi-tion. However, considering the relatively low risk and potentially significant effects of acupunc-ture, one could defend a more pragmatic view of its use in the UK National Health Service (NHS), especially if the primary outcome is pain relief, which has a stronger evidence base.
LimitationsAlthough the present subject had a chronic tendinopathy, it is not possible to rule out natu-ral regression as the source of his relief. The pathophysiology of tendon pain is complex and multidimensional, and the stages of tendon healing are dynamic and influenced by multiple processes.
No confounding factors were controlled for, such as the subject’s use of or engagement in: medication, anti- inflammatory gel and ice; eccentric loading, exercise and stretches; stress management; improved footwear and an altered running technique; soft- tissue manipulation, education and taping.
In addition, the fact that the present author was a novice must be taken into account.

A. M. Davidson
© 2016 Acupuncture Association of Chartered Physiotherapists 83
Acupuncture points and techniques were altered between and during treatment sessions, affecting reproducibility. It is reasonable to assume that it was the combined effect of the interventions that ultimately led to the subject’s successful rehabilitation.
Future research might benefit from investi-gating a more pragmatic use for acupuncture in the NHS. The Keele STarT Back Screening Tool for back pain is a good analogy: by iden-tifying certain characteristics in a patient, the practitioner can predict what type of treatment the individual will respond to, depending on the psychosocial factors influencing their situation. Similarly, one might be able to identify which tendon stages/patient presentations are more likely to improve with acupuncture, and which ones may not. An ad hoc cost- effectiveness analysis could then determine its viability.
AcknowledgementsI would like to thank the subject of this case study, and my AACP cohort and tutor for help-ing me to develop my acupuncture skills. I am also grateful to Homerton University Hospital NHS Foundation Trust for providing me with supervised training following my completion of the AACP foundation course.
ReferencesAlfredson H. & Lorentzon R. (2000) Chronic Achilles
tendinosis: recommendations for treatment and pre-vention. Sports Medicine 29 (2), 135–146.
Bradnam L. (2001) Western acupuncture point selec-tion: a scientific clinical reasoning model. Meridian Worldwide – Newsletter of the International Acupuncture Association of Physical Therapists 10 (2), 9–18.
Bradnam L. (2003) A proposed clinical reasoning model for western acupuncture. New Zealand Journal of Physiotherapy 31 (1), 40–45.
Bradnam L. (2007) A proposed clinical reasoning model for Western acupuncture. Journal of the Acupuncture Association of Chartered Physiotherapists 2007 (January), 21–30.
Cook J. L. & Purdam C. R. (2009) Is tendon pathology a continuum? A pathology model to explain the clini-cal presentation of load- induced tendinopathy. British Journal of Sports Medicine 43 (6), 409–416.
Douglas J., Kelly M. & Blachut P. (2009) Clarification of the Simmonds–Thompson test for rupture of an Achilles tendon. Canadian Journal of Surgery 52 (2), E40–E41.
Fu S.- C., Rolf C., Cheuk Y.- C., Lui P. P. Y. & Chan K.- M. (2010) Deciphering the pathogenesis of tendinopathy: a three- stages process. Sports Medicine, Arthroscopy, Rehabilitation, Therapy and Technology 2: 30. DOI: 10.1186/1758- 2555- 2- 30.
Khan K. M., Cook J. L., Bonar F., Harcourt P. & Astrom M. (1999) Histopathology of common tendinopathies. Update and implications for clinical management. Sports Medicine 27 (6), 393–408.
Maffulli N., Wong J. & Almekinders L. C. (2003) Types and epidemiology of tendinopathy. Clinics in Sports Medicine 22 (4), 675–692.
Neal B. S. & Longbottom J. (2012) Is there a role for acu-puncture in the treatment of tendinopathy? Acupuncture in Medicine 30 (4), 346–349.
Öhberg L., Lorentzon R. & Alfredson H. (2004) Eccentric training patients in patients with Achilles tendinosis: normalised tendon structure and decreased thickness at follow up. British Journal of Sports Medicine 38 (1), 8–11.
O’Sullivan P. (2005) Diagnosis and classification of chronic low back pain disorders: maladaptive move-ment and motor control impairments as underlying mechanism. Manual Therapy 10 (4), 242–255.
Rees J. D., Stride M. & Scott A. (2014) Tendons – time to revisit inflammation. British Journal of Sports Medicine 48 (21), 1553–1557.
Robinson J. M., Cook J. L., Purdam C.., et al. (2001) The VISA- A questionnaire: a valid and reliable index of the clinical severity of Achilles tendinopathy. British Journal of Sports Medicine 35 (5), 335–341.
Sengkerij P. M., de Vos R.- J., Weir A., van Weelde B. J. G. & Tol J. L. (2009) Interobserver reliability of neovas-cuarization score using power Doppler sonography in midportion Achilles tendinopathy. The American Journal Sports Medicine 37 (8), 1627–1631.
Andrew Davidson works as a senior physiotherapist and part- time researcher in the locomotor outpatient department of Homerton University Hospital NHS Foundation Trust. His speciality is musculoskeletal therapy for persistent pain, and he has a particular interest in the management of tendinopathies.

Chronic mid- portion Achilles tendinopathy
© 2016 Acupuncture Association of Chartered Physiotherapists84
Appendix 1Clinic assessment form
Name: [redacted] DOB: [redacted]
Therapist: LM Andrew Davidson Designation: B6 PT
Date: [redacted] NHS: [redacted] RiO: [redacted]
Occupation/hobbies: Desk- based/running
Main presenting problem: Right- sided posterior heel pain
PC: Posterior heel pain
HPC: Gradual onset; no trauma or direct mechanism of injury over the past 7 months; no swelling, redness or heat
PMH: Nil
DH: Ibuprofen PRN
SH: Lives with partner, full- time employment, office job (seated)
Aggravates: Pain on impact loading and prolonged sitting; some pain in the morning
Eases: Ice, non- steroidal anti- inflammatory drugs, rest
Night pain: Nil
Twenty- four- hour pattern: Increased a.m., decreased p.m.
Numerical Rating Scale score: 7

© 2016 Acupuncture Association of Chartered Physiotherapists 85
Correspondence: Ellen Louise Hellard, Anglian Com-munity Enterprise, Clacton- on- Sea Hospital, Tower Road, Clacton- on- Sea, Essex CO15 1LH, UK (e- mail: [email protected]).
Acupuncture in Physiotherapy, Volume 28, Number 1, Spring 2016, 85–91
CASE REPORT
Acupuncture for pain management of osteoarthritis in the glenohumeral joint
E. L. HellardAnglian Community Enterprise, Clacton- on- Sea, Essex, UK
AbstractThis case report describes acupuncture treatment to manage pain in an 85- year- old woman with a 6- month history of pain and limited function. The subject had severe bilateral osteo-arthritis of the glenohumeral joint with calcific tendinitis. Before acupuncture treatment, she had EuroQuol – five dimensions – five levels (EQ- 5D- 5L), and Shoulder Pain and Disability Index (SPADI) scores of 0.0486 and 80.76%, respectively. Acupuncture was selected for pain management after no success was achieved with conventional physiotherapy and cortisone injections. The patient was a full- time carer for her husband, and therefore, she declined surgical intervention at this time. Treatment consisted of four sessions of acupuncture, and the selected acupoints were used to aid in pain management. The subject responded well to treatment and displayed no adverse effects. Changes after treatment were indicated by EQ- 5D- 5L and SPADI scores of 0.4435 and 75.38%, respectively. These outcomes demonstrated mild improvements in pain and function, showing a change in EQ- 5D- 5L of –0.4386 and a SPADI improvement of 5.38%. The results were limited by disruption to the scheduled sessions, but showed short- term improvements in overall pain and function.
Keywords: acupuncture, glenohumeral joint, osteoarthritis, pain management.
IntroductionGeorge (2008) and Hermoso & Calvo (2009) reported a 21% prevalence of shoulder dis-orders in the elderly community, and that such problems are more commonly seen in women (25%) than men (17%). These findings were supported by Chillemi & Franceschini (2013). The prevalence of shoulder disorders also increases substantially with age (George 2008; Chillemi & Franceschini 2013). Millett et al. (2008) described shoulder osteoarthritis (OA) as the progressive breakdown of articular cartilage
and joint tissue. The erosion of articular carti-lage and the remodelling of subchondral bone eventually results in the loss of joint congruity (Millett et al. 2008), and this increasing instabil-ity results in pain, stiffness and loss of range of movement (ROM).
George (2008) also discussed additional pathological changes linked with OA, ranging from labral degeneration, intra- articular loose bodies and osteophytes. Another major cause of shoulder pain can be linked to calcification of the supraspinatus tendon (Hurt & Baker 2003; Gosens & Hofstee 2009). Gosens & Hofstee (2009) described calcification as a natural cycle of repair, but stated that this can become blocked during one of the healing stages. Hurt & Baker (2003) discussed how

Pain management of osteoarthritis in the glenohumeral joint
© 2016 Acupuncture Association of Chartered Physiotherapists86
the shoulder becomes chronically painful as a result of inflammation around calcium deposits. Green et al. (2005) reported that compromised shoulder mobility results in substantial impair-ment and disability, and is strongly associated with an inability to sleep.
Manyanga et al. (2014) conducted a review and meta- analysis of the use of acupuncture in OA, and concluded that the technique is associated with significant reductions in pain intensity and improvements in functional mobility. Overall, there is little evidence to support the use of acupuncture, especially with regard to OA of the shoulder. The only notably positive results were reported by Green et al. (2005) and Vas et al. (2008), and there has been a distinct lack of research in this area. Nevertheless, Camp (1992) discussed the evidence for the use of acupuncture in pain management, and White & EBAM (2009) described its effects on musculo-skeletal pain through inhibition of nociceptive pathways.
When performing acupuncture, clinicians look for a response called De Qi. Resulting from the stimulation of Aδ, Aβ and C-fibres, this leads to a sensation of heaviness, numb-ness and soreness (Han 2004; Hopwood 2004; White & EBAM 2009). Nociceptive pain signals are transmitted by small- diameter fibres, and acupuncture stimulates large nerve fibres. The signals produced either travel to the cerebral cortex, causing the release of endorphins, or inhibit the nociceptive pathways situated in the dorsal horn, helping to block pain signals (Hopwood 2004).
Furthermore, there is some evidence to sup-port the idea that acupuncture stimulates the healing process. Sandberg et al. (2003) reported that it also has an effect on blood flow to both the skin and the muscles. De Almeida et al. (2015) showed a possible increase in collagen fibres following acupuncture treatment. Henry et al. (2012) stated that there was a very high prevalence of myofascial pain (35–95%) in patients presenting with chronic pain. Henry et al. (2012), Rahbar et al. (2013) and Itoh et al. (2008) described myofascial trigger points (MTPs) as the presence of a hypersensitive palpable taut band within skeletal muscle. Bajaj
et al. (2001) went on to report that MTPs limit joint motion, and lead to an exacerbation of pain and accelerated joint degeneration.
Case reportBackgroundThe present study describes the case of an 85- year- old woman with a 6- month history of pain in her left shoulder. This had begun after she had lifted some shopping out of her car, and had been getting progressively worse. More recently, the subject had also started to experience pain in her right shoulder. She described the pain as a constant dull ache over the shoulder that radiated down over the deltoid muscle and into the biceps, and became sharp on movement. No neurological symptoms were reported.
The subject reported that she had been diagnosed with osteoporosis at 56 years of age, and at that time, she struggled to lift her arms to brush her hair and to stand up straight. She had been advised to improve her posture and exercise. She reported that she had been self- managing her osteoporosis, and had successfully regained full ROM. The subject had had no further problems until this episode of shoul-der pain had begun. She was very dedicated individual to her daily routine, which involved her getting up at 05:00 h every morning to do 30 min of exercises before tending to her hus-band and assisting him with his own functional training.
The subject provided palliative care for her husband. He had cancer, and had also suffered from a stroke a few years ago and was now hemiplegic. She was now struggling with aspects of his daily care: other carers only assisted her three times a day, and she found it difficult to support her husband during standing transfers.
The subject had already undergone six ses-sions of regular physiotherapy, including a home exercise programme. When no improve-ment was seen, she was referred to a Tier II musculoskeletal service and given two cortisone injections without success. The consultant advised her that the best course of action would be surgical intervention involving total

E. L. Hellard
© 2016 Acupuncture Association of Chartered Physiotherapists 87
shoulder replacement. The subject declined this option because she felt that the caring that she had to provide for her husband meant that this was not feasible. She was taking medication for her blood pressure (ramipril) and osteoporosis (alendronate), but had not been prescribed any anticoagulants or steroids. She was also on co- codamol, but would not risk taking anything stronger so as to avoid drowsiness while caring for her husband.
X- rays of the subject’s left shoulder revealed moderate to severe degenerative changes of the glenohumeral joint, and large marginal osteo-phytes at the inferior border of the humeral head. Like the inferior calcific body at the infer-omedial border of the humeral head, these were probably caused by calcific tendinopathy. X- rays of the right shoulder showed hypertrophic changes in the greater tuberosity, and slight sclerosis of the inferior border of the clavicle. The subacromial space was normal. There were moderate degenerative changes in the gleno-humeral joint, and large marginal osteophytes at the inferior border of the humeral head. A large osseous body was seen on the superior border of the glenoid; this was most probably a result of calcific tendinopathy.
Clinical examinationThe subject had poor posture: she was kyphotic with a protracted chin and shoulders.
Her ROM was severely limited in her left shoulder, demonstrating only 40° of flexion and 30° of abduction. Reaching her hand behind her back, the subject was only just able to reach her back pocket, and reaching her hand behind her head, she was only just able to reach the level of her ear.
Her right shoulder demonstrated 70° of flex-ion and 60° of abduction. Reaching her hand behind her back, the subject was only just able to reach her back pocket, and reaching her hand behind her head, she was only just able to reach the level of T1.
For all movements, she reported a pain score of 8/10 on a visual analogue scale. The subject displayed positive painful arc, empty can, Hawkins–Kennedy and lift- off tests, with her pain being greater on her left side than
on her right. She displayed bilateral atrophy of the supraspinatus, infraspinatus and deltoid muscles.
Since all other options had been exhausted, acupuncture was selected for pain management.
Point rationaleLarge Intestine (LI) 4 was employed because it is considered to be the master pain point. Its strong analgesic effects through the release of opioids and descending inhibition have been recognized (Camp 1986; Hansen 1997; Hopwood et al. 1997; Skjodt 2008).
Triple Energizer (TE) 14, the posterior eye of the shoulder, was selected for a number of reasons, not least because it shares the same dermatome as the shoulder (Franklin 2007; Hopwood 2014). Lian et al. (2000), Tas- Cebe & Cummings (2013) and Hopwood (2014) have described the efficacy of TE14 use for shoulder pain and stiffness. Roffey (2009) reported its pain modulating effect on a segmental level via the stimulation of Aβ nerve fibres.
Large Intestine 15, the anterior eye of the shoulder, was used in combination with TE14. This point was described by Stux et al. (2003) and Ahuja (2010) as a key local point for the shoulder, and Roffey (2009) reported that it increased circulatory response.
Gall Bladder (GB) 21 is the meeting point for the Gall Bladder, Triple Energizer and Stomach meridians (Pearce 2015). It was employed because it is used for the treatment of shoulder and neck pain and stiffness (White et al. 2004), particularly in conjunction with Bladder (BL) 12 (Deadman et al. 2007). Furthermore, an MTP is often located at GB21 (Deadman et al. 2007).
Small Intestine (SI) 9 was used because, according to Deadman et al. (2007), it alleviates pain in the shoulder and upper arm, as well as inability to raise the arm.
Small Intestine 10 was selected because Deadman et al. (2007) recommend it as a local point for the shoulder, and especially for acute pain.
Small Intestine 11 was chosen because it has been reported to be efficacious in the treatment of pain and loss of shoulder movement (Hecker et al. 2007).

Pain management of osteoarthritis in the glenohumeral joint
© 2016 Acupuncture Association of Chartered Physiotherapists88
Bladder 11 was used because it has been identified as an influential point for bones and joints (Deadman et al. 2007; Hecker et al. 2007).
Finally, Bladder 12 was selected because Deadman et al. (2007) have described its efficacy in the treatment shoulder pain when it is used in combination with GB21.
TreatmentThe subject was screened for contraindications, and the only precaution highlighted during the subjective assessment was hypertension.
However, she reported that this condition was well controlled by her medication. She gave her informed consent for acupuncture, and the pro-cedure and its possible side effects were fully explained. Five weekly acupuncture sessions were booked.
The dosage during the first session was 10 min (Table 1) because the subject had not previously undergone acupuncture, and the present author was not sure how she would respond. For the same reason, fewer needles were used in the first session. The dosage was then increased to 20 min because it has been
Table 1. Treatment schedule: (MTP) myofascial trigger point; (LI) Large Intestine; (TE) Triple Energizer; (GB) Gall Bladder; (SI) Small Intestine; and (BL) Bladder
Date of treatment*
Acupuncture points†
Active MTP
Time (min)
Needle size (mm)
Depth of insertion (cm)
Needling technique
Adverse response
De Qi
Session 1 09/07/15
LI4LI15TE14GB21SI9 BL11BL12
NoNoNoYesNoNoNo
10
0.25 × 300.25 × 400.25 × 40 0.25 × 30 0.25 × 300.25 × 300.25 × 30
1.02.0–3.01.5–2.01.0–2.52.0–3.00.50.5–1.0
PerpendicularOblique to supraspinatus insertionObliquePinched skin and perpendicularPerpendicularObliqueOblique
None reported
Yes
Session 223/07/15
LI4 LI15 TE14GB21 SI9 SI10SI11BL11BL12
NoNoNoYesNoNoYesNoNo
20
0.25 × 300.25 × 400.25 × 400.25 × 30 0.25 × 300.25 × 300.25 × 400.25 × 300.25 × 30
1.02.0–3.01.5–2.01.0–2.52.0–3.01.0–1.51.0–2.00.50.5–1.0
PerpendicularOblique to supraspinatus insertionObliquePinched skin and perpendicularPerpendicularObliqueOblique laterally towards supraspinatusObliqueOblique
None reported
Yes
Session 319/08/15
LI4 LI15 TE14GB21 SI9 SI10SI11BL11BL12
NoNoNoYesNoNoYesNoNo
20
0.25 × 300.25 × 400.25 × 400.25 × 30 0.25 × 300.25 × 300.25 × 400.25 × 300.25 × 30
1.02.0–3.01.5–2.01.0–2.52.0–3.01.0–1.51.0–2.00.50.5–1.0
PerpendicularOblique to supraspinatus insertionObliquePinched skin and perpendicularPerpendicularObliqueOblique laterally towards supraspinatusObliqueOblique
None reported
Yes
Session 4 26/08/15
LI4 LI15 TE14 GB21 SI9 SI10 BL11 BL12
No No No Yes No No No No
20
0.25 × 30 0.25 × 40 0.25 × 40 0.25 × 30 0.25 × 30 0.25 × 30 0.25 × 30 0.25 × 30
1.0 2.0–3.0 1.5–2.0 1.0–2.5 2.0–3.0 1.0–1.5 0.5 0.5–1.0
Perpendicular Oblique to supraspinatus insertion Oblique Pinched skin and perpendicular Perpendicular Oblique Oblique Oblique
None reported
Yes
*Subject’s consent obtained for all treatments.†All bilateral.

E. L. Hellard
© 2016 Acupuncture Association of Chartered Physiotherapists 89
suggested that a normal dose should be approx-imately 20–30 min (White & EBAM 2009).
Outcome measuresStarting scores. Before acupuncture treatment, the subject had EuroQuol – five dimensions – five levels (EQ- 5D- 5L), and Shoulder Pain and Disability Index (SPADI) scores of 0.0486 and 80.76%, respectively.
Post- treatment scores. After acupuncture treatment, the subject had EQ5D5L and SPADI scores of 0.4435 and 75.38%, respectively. These results demonstrated mild improvements in pain and function, showing a change in EQ- 5D- 5L of –0.4386 and a SPADI improvement of 5.38%.
Following the four sessions of acupuncture, it was decided that the subjects’ husband should to go into residential care, and therefore, she was now able to consider surgery as a viable option.
DiscussionEight acupuncture points were used, and since all were administered bilaterally, this meant that a total of 16 were employed (Table 1). The subject had a mild visual physiological response to treatment and exhibited erythema through-out the sessions. She described De Qi as a heavy, numbing sensation and dull ache. This was always stronger on her left side than her right, and she reported that the level of De Qi increased in the later treatments.
During the second and third sessions, nee-dling of TE14 and SI9 evoked muscle spasms. Myofascial trigger points were noted at GB21 throughout the course of treatment, and at SI11 during the second and third sessions. However, no MTP or tender point was noted at SI11 dur-ing the fourth session, and therefore, this point was not needled.
Unfortunately, as a result of departmental meetings, waiting lists and the subject having to rearrange an appointment, there was a 2- week gap between the first and second treatments, and only four sessions were completed. After this 2- week gap the subject aggravated her
shoulder while carrying out her caring duties during this period, and reported that the pain was so bad that it actually made her feel nau-seous at the time.
Although some small improvements in pain and function were seen, the present author believes that the gap between sessions and the aggravation of the symptoms could well have had a negative effect on the treatment outcomes.
Nevertheless, the subject’s SPADI score showed an improvement of 5.38%. In com-parison, Crespin et al. (2015) reported that acupuncture provided short- term pain relief of approximately 15% when used to treat patients in a total joint replacement programme.
It is difficult to assess the implications of this case study for clinical practice. Even though a patient who had exhausted all other options at the time was afforded some short- term pain relief, the present author believes that, if she had continued to care for her husband at home, then the subject’s pain would have returned to its usual levels soon after the cessation of treatment.
Other acupuncture points that could have been used include LI14, which is located in the insertion of the deltoid muscle, and Stomach (ST) 38, a distal shoulder point for easing stiffness recommended by Tukmachi (1999). A decision was made not to use ST38 because of both its location on the anterior aspect of the calf and time constraints.
Furthermore, the present author stimulated the needles more as she grew increasingly confident with needling, which may explain why a stronger De Qi response was evoked in the later sessions. She believes that the subject could have benefited from further acupuncture treatment. However, despite the proven benefits of acupuncture for pain control and the results of a systematic review by Kim et al. (2012), its use in current practice will be limited by finan-cial constraints.
More high- quality studies that highlight the efficacy of acupuncture for pain control and its cost- effectiveness are needed before it can become a viable treatment option within the National Health Service.

Pain management of osteoarthritis in the glenohumeral joint
© 2016 Acupuncture Association of Chartered Physiotherapists90
AcknowledgementsThanks go to Nigel Hellard, my wonderful husband, for putting up with me.
ReferencesAhuja D. S. (2010) Acupuncture for shoulder pain. Journal
of the Acupuncture Association of Chartered Physiotherapists 2010 (Autumn), 61–70.
Bajaj P., Bajaj P., Graven- Nielsen P. & Arendt- Nielsen L. (2001) Trigger points in patients with lower osteo-arthritis. Journal of Musculoskeletal Pain 9 (3), 17–33.
Camp V. (1986) Acupuncture for shoulder pain. Acupuncture in Medicine 3 (1), 28–32.
Camp V. (1992) Acupuncture of the knee. Acupuncture in Medicine 10 (2), 57–62.
Chillemi C. & Franceschini V. (2013) Shoulder osteo-arthritis. Arthritis 2013: 7. Art. No.: 370231. DOI: 10.1155/2013/370231.
Crespin D. J., Griffin K. H., Johnson J. R., et al. (2015) Acupuncture provides short- term pain relief for patients in a total joint replacement program. Pain Medicine 16 (6), 1195–1203.
Deadman P., Al- Khafaji M. & Baker K. (2007) A Manual of Acupuncture, 2nd edn. Journal of Chinese Medicine Publications, Hove.
De Almeida M. D. S., de Freitas K. M., Oliveira L. P., et al. (2015) Acupuncture increases the diameter and reorganisation of collagen fibrils during rat tendon healing. Acupuncture in Medicine 33 (1), 51–57.
Franklin D. (2007) Acupuncture in the management of shoulder impingement pain. Journal of the Acupuncture Association of Chartered Physiotherapists 2007 (January), 49–55.
George M. S. (2008) Arthroscopic management of shoul-der osteoarthritis. The Open Orthopaedics Journal 2, 23–26.
Gosens T. & Hofstee D.- J. (2009) Calcifying tendinitis of the shoulder: advances in imaging and management. Current Rheumatology Reports 11 (2), 129–134.
Green S., Buchbinder R. & Hetrick S. E. (2005) Acupuncture for shoulder pain. Cochrane Database of Systematic Reviews, Issue 2. Art. No.: CD005319. DOI: 10.1002/14651858.CD005319.
Han J.- S. (2004) Acupuncture and endorphins. Neuroscience Letters 361 (1–3), 258–261.
Hansen J. A. (1997) A comparative study of two methods of acupuncture treatment for neck and shoulder pain. Acupuncture in Medicine 15 (2), 71–73.
Hecker H.- U., Steveling A., Peuker E., Kastner J. & Liebchen K. (2007) Color Atlas of Acupuncture: Body Points – Ear Points – Trigger Points, 2nd edn. Thieme, Stuttgart.
Henry R., Cahill C. M., Wood G., et al. (2012) Myofascial pain in patients waitlisted for total knee arthroplasty. Pain Research and Management 17 (5), 321–327.
Hermoso F. E. & Calvo E. (2009) Shoulder pain in the elderly. Aging Health 5 (5), 711–718.
Hopwood V. (2004) Acupuncture in Physiotherapy. Butterworth–Heinemann, Oxford.
Hopwood V. (2014) The Sanjiao/Triple Energizer meridian, Journal of the Acupuncture Association of Chartered Physiotherapists 2014 (Spring), 41–49.
Hopwood V., Lovesey M. & Mokone S. (1997) Acupuncture and Related Techniques in Physical Therapy. Churchill Livingstone, Edinburgh.
Hurt G. & Baker C. L., Jr (2003) Calcific tendinitis of the shoulder. Orthopaedic Clinics of North America 34 (4), 567–575.
Itoh K., Hirota S., Katsumi Y., Ochi H. & Kitakoji H. (2008) Trigger point acupuncture for treatment of knee osteoarthritis – preliminary RCT for a pragmatic trial. Acupuncture in Medicine 26 (1), 17–26.
Kim S.- Y., Lee H., Chae Y., Park H.- J. & Lee H. (2012) A systematic review of cost- effectiveness analyses alongside randomised controlled trials of acupuncture. Acupuncture in Medicine 30 (4), 273–285.
Lian Y.- L., Chen C.- Y., Hammes M. & Kolster B. C. (2000) The Seirin Pictorial Atlas of Acupuncture: An Illustrated Manual of Acupuncture Points. Konemann, Cologne.
Manyanga T., Froese M., Zarychanski R., et al. (2014) Pain management with acupuncture in osteoarthri-tis: a systematic review and meta- analysis. BMC Complementary and Alternative Medicine 14: 312. DOI: 10.1186/1472- 6882- 14- 312.
Millett P. J., Gobezie R. & Boykin R. E. (2008) Shoulder osteoarthritis: diagnosis and management. American Family Physician 78 (5), 605–611.
Pearce L. (2015) The Gall Bladder meridian. Acupuncture in Physiotherapy 27 (1), 65–71.
Rahbar M., Toopchizadeh V., Eftekharsadat B. & Ganjeifar V. (2013) Therapeutic efficacy of myofascial trigger point therapy in patients with bilateral knee osteoarthritis: a randomised clinical trial. Life Science Journal 10 (6s), 472–478.
Roffey S. (2009) Effects of acupuncture on pain modula-tion in a subject with chronic rotator cuff injury. Journal of the Acupuncture Association of Chartered Physiotherapists 2009 (Spring), 65–72.
Sandberg M., Lundeberg T., Lindbergh L.- G. & Gerdle B. (2003) Effects of acupuncture on skin and muscle blood flow in the healthy subjects. European Journal of Applied Physiology 90 (1–2), 114–119.
Skjodt L. (2008) Treatment of cervical and posterior shoulder pain in a 57- year- old female with conventional physiotherapy and Western acupuncture. Journal of the Acupuncture Association of Chartered Physiotherapists 2008 (Autumn), 53–60.
Stux G., Berman B. & Pomeranz B. (2003) Basics of Acupuncture, 5th edn. Springer- Verlag, Berlin.
Tas- Cebe G. & Cummings S. (2013) A single- blinded controlled trial comparing corticosteroid injection, acu-puncture and home- based exercises for the treatment of primary contracted (frozen) shoulder. Journal of the

E. L. Hellard
© 2016 Acupuncture Association of Chartered Physiotherapists 91
Acupuncture Association of Chartered Physiotherapists 2013 (Autumn), 25–38.
Tukmachi E. S. (1999) Frozen shoulder: a comparison of Western and traditional Chinese approaches and a clinical study of its acupuncture treatment. Acupuncture in Medicine 17 (1), 9–21.
Vas J., Ortega C., Olmo V., et al. (2008) Single- point acupuncture and physiotherapy for the treatment of painful shoulder: a multi- centre randomized controlled trial. Rheumatology 47 (6), 887–893.
White P., Lewith G., Prescott P. & Conway J. (2004) Acupuncture versus placebo for the treatment of chronic mechanical neck pain: a randomized, controlled trial. Annals of Internal Medicine 141 (12), 911–919.
White A. & Editorial Board of Acupuncture in Medicine (EBAM) (2009) Western medical acupuncture: a definition. Acupuncture in Medicine 27 (1), 33–35.
Ellen Louise Hellard graduated from the University of East London in 2010 with a BSc (Hons) in Physiotherapy. She has worked in musculoskeletal physiotherapy for Anglian Community Enterprise for the past 2 years. Ellen completed the AACP Foundation Course under Paul Battersby in 2015, which sparked her interest in acupuncture. She is currently a steward and learning champion with the Chartered Society of Physiotherapy’s East of England regional network.


© 2016 Acupuncture Association of Chartered Physiotherapists 93
Acupuncture in Physiotherapy, Volume 28, Number 1, Spring 2016, 93–98
CASE REPORT
Acupuncture for cancer- related hot flashes and night sweating in a 44- year- old woman with breast cancer
V. RamasamyJohn Taylor Hospice, Birmingham, UK
AbstractThe aim of this study was to assess the effect of acupuncture treatment for cancer- related hot flashes and night sweating. The subject was a 44- year- old woman with a diagnosis of breast cancer who had suffered from intractable hot flashes and night sweating for the past 2 years. Other measures failed to improve her symptoms, but she responded to a course of acupuncture treatment. The subject’s hot flashes and sweating decreased from 9/10 to 2/10, as measured on a visual analogue scale. There was also an improvement in her quality of sleep and overall sense of well- being. Acupuncture may have potential as a treatment modality since the current therapeutic options for hot flashes and night sweating are limited, especially for patients with hormone- sensitive carcinoma.
Keywords: acupuncture, breast cancer, hot flashes, night sweating.
IntroductionSweating is the natural way of lowering body temperature. This is achieved because sweat results in heat loss through the skin. In patients with cancer, sweating may be caused by an infection, a tumour or cancer treatment.
A hot flash is defined as a sudden onset of heat in the upper trunk that spreads to the arms and face, often with subsequent sweating and then a chill. A combination of hot flashes and sweating is frequently the result of vasomotor symptoms, and may occur during the day and also at night (Kronenberg 1990). The severity and frequency of hot flashes vary from person to person, and these can be extreme in patients with breast or prostate cancer who are under-going anticancer therapy (Filshie 2005).
Early research by Carpenter et al. (1998) dem-onstrated that hot flashes are a common and
disruptive clinical problem that affects nearly two- thirds of all breast cancer survivors. These individuals experience hot flashes and sweating more frequently than women undergoing a natural menopause, and cancer- related flashes may be more severe, distressing and of greater duration (Carpenter et al. 2002).
Hot flashes and night sweating may be accompanied by a range of physical sensations, including sweating, flashing or redness, palpita-tions, dizziness, feelings of suffocation, nausea, tingling sensations in the hands, and chills before or after the flash. Associated emotional symptoms may include anxiety, feelings of panic, irritation, annoyance and frustration, and even suicidal ideation. Night sweating disturbs sleep patterns, leading to fatigue and irritability (Miller 2004).
Adjuvant hormonal therapies such as tamox-ifen are an essential part of the treatment regimen for early breast cancer, and are used to prevent recurrence. However, Hunter et al. (2004) mentioned that hot flashes and night
Correspondence: Visweswaran Ramasamy, John Taylor Hospice, 76 Grange Road, Erdington, Birmingham B24 0DF, UK (e- mail: [email protected]).

Cancer- related hot flashes and night sweating
© 2016 Acupuncture Association of Chartered Physiotherapists94
sweating are the most frequently occurring side effects of these interventions, with up to 80% of women taking tamoxifen reporting these as troublesome. Many patients do not wish to expe-rience further side effects of pharmacological preparations during their cancer treatment. For these women, complementary and alternative medicine approaches may offer an alternative (Hunter et al. 2004). Preliminary studies suggest that acupuncture may reduce hot flashes and night sweating in breast cancer survivors, and have fewer side effects than conventional phar-macological therapies (Hervik et al. 2009; Walker et al. 2010).
Mechanism of actionThe specific pathophysiology of acupuncture for hot flashes remains a mystery, although several hypotheses exist. Acupuncture is known to stimulate neuropeptide synthesis, which controls bodily functions such as cardiovascular physiology and hormonal secretions (Omura 1975, cited in Tukmachi 2000). This is believed to activate peripheral nerve endings, muscles and also connective tissue. The stimulation of the nerves produces afferent signals, which increase, for example, central β- endorphins and serotonin, and probably also activate receptors (Guo et al. 2008; Moazzami et al. 2010). Using functional magnetic resonance imaging, Hui et al. (2010) demonstrated that acupuncture decreased activity in the amygdala and hypothalamus. Calcitonin gene- related peptide (CGRP) is a neuropeptide that is released into the circulatory system during a hot flash (Wyon et al. 2000). Acupuncture stimulation causes the release of β- endorphin, which has an inhibitory effect on CGRP. A study by Wyon et al. (1995) showed that urinary excretion of CGRP was reduced following acupuncture. It is possible that neu-ronal activity in the hypothalamus is elevated during hot flashes, and acupuncture may reduce this, perhaps mediated by increased β- endorphin release and decreased noradrenaline activity.
Case reportBackgroundThe present subject was a 44- year- old woman with a diagnosis of breast cancer. She had been
suffering from intractable hot flashes and night sweating for the past 2 years, and this had had a severe impact on her quality of life (QoL). Her sweating was very bad, especially when she tried to sleep. She needed to change her bedclothes several times a night, which had an effect on her sleep and QoL. The subject’s poor sleep pattern impacted on her energy level during the day, leading to fatigue. The hot flashes made her feel uncomfortable when socializing with friends, and increased her anxiety level every time she experienced them. She had tried all other measures, i.e. medications, using a fan, maintaining ambient room temperature, wearing cotton clothing, avoiding caffeine- related drinks, relaxation and listening to music, but these had had very little or no effect on her sweating. Having previously worked as a librarian, she had quit her job because of the increasing side effects of her cancer treatment.
Clinical impressionThe subject was alert and appeared well. Based on the subjective history and objective find-ings, the vasomotor symptoms that she was experiencing were directly linked to her breast cancer diagnosis. Medical assessment ruled out any infection or pyrexia as a cause of sweating. She had begun to have vasomotor symptoms following breast cancer treatment. The subject described her experience of a hot flash as “a sudden warmth all over the body and then accompanied by a feeling of skin peeling from inside”. During hot flashes, she experienced associated symptoms such as palpitation, anxiety, irritability and headaches.
TreatmentPrior to acupuncture treatment, precautions were taken and contraindications were checked. The subject’s left arm was not needled because of axillary clearance. She was given an informa-tion leaflet that explained acupuncture treatment and possible adverse reactions to it. Written informed consent was gained once all the infor-mation had been provided (AACP 2012).
The acupuncture points that were selected are listed in Table 1. The majority of the points used corresponded to those employed in the

V. Ramasamy
© 2016 Acupuncture Association of Chartered Physiotherapists 95
largest trial of acupuncture for hot flashes (Borud et al. (2009). In all treatment sessions, the acupuncture points were stimulated manu-ally, and the needles were left in situ for 30 min. The subject received treatment once a week, and the needles were stimulated manually every 10 min during each session in order to improve the therapeutic effects. The depth of needling was dependent on whether De Qi was elicited. The needles used were all sterile and made of stainless steel (Classic Plus, HMD Europe Ltd, Chipping Norton, Oxfordshire, UK).
The subject did not notice any changes in her symptoms until three sessions of treatment had been completed, after which the frequency and severity of her hot flashes and night sweat-ing reduced slightly. A noticeable reduction in vasomotor symptoms was observed after six sessions of treatment, which had a huge impact on her sleep pattern and psychological well- being. By the end of 8 weeks of acupuncture treatment, the subject reported a significant reduction in both her vasomotor and associated symptoms, including palpitation, anxiety, irrita-bility and headaches. Her hot flashes and sweat-ing decreased from 9/10 to 2/10, as measured on a visual analogue scale (VAS).
DiscussionA significant reduction in the present subject’s hot flashes and night sweating was brought
about by 8 weeks of acupuncture treatment. Prior to this, she had reported between three and four hot flashes every hour, and from four to six incidents of sweating every night. Following the completion of her treatment, she reported that she now only experienced a mild damp feeling two or three times a day, and that her palpitations and feelings of irritabil-ity had considerably improved. Similarly, her night- time sweating had reduced considerably to only one or two incidents a night, and since these were less intense, she could manage the problem without changing her nightclothes. The hot flashes had lessened significantly fol-lowing acupuncture, and the distress caused by these had decreased even more. The outcomes of the acupuncture treatment are detailed in Table 2.
Current treatment options for hot flashes in patients with breast cancer include pharma-cological agents, especially selective serotonin reuptake inhibitors (e.g. venlafaxine and parox-etine), but these have adverse side effects and are considered to be undesirable options for most women (Loprinzi et al. 1998; Nelson et al. 2006). Hormone replacement therapy reduces hot flashes in women by 90–95%, compared to 10–50% with placebo treatment (Carpenter et al. 2007), and may improve QoL (Fahlén et al. 2011), but it also increases the risk of breast cancer (MWSC 2003) and probably that of a recurrence of this form of cancer (Holmberg et al. 2008).
This situation has led to an increasing demand for alternative treatments for hot flashes and night sweating. Although there has been no clearly defined treatment for hot flashes in patients with breast cancer for whom oestrogen replacement is contraindicated (Studdard 1999), alternatives are available. One modality that has only been investigated to a limited extent is acupuncture (Towlerton et al. 1999), possibly because the conclusions of many trials of are not robust enough and are generally incon-sistent. Nevertheless, acupuncture has been shown to be effective for postmenopausal hot flashes, and clinical experience suggests that it is an effective alternative treatment for reduc-ing hot flashes and night sweating, especially
Table 1. Acupuncture points selected: (LI) Large Intestine; (PC) Pericardium; (TE) Triple Energizer; (HT) Heart; (LR) Liver; (SP) Spleen; (ST) Stomach; and (KI) Kidney
Acupuncture point
Size of needle (mm)
Depth of needling (cun)
De Qi
LI4 (right) 0.18 × 25 0.4 YesPC6 (right) 0.18 × 25 0.4 YesPC8 (right) 0.18 × 25 0.4 YesTE5 (right) 0.18 × 25 0.4 YesHT6 (right) 0.18 × 25 0.4 YesHT7 (right) 0.18 × 25 0.4 YesHT8 (right) 0.18 × 25 0.4 YesLI11 (right) 0.25 × 40 0.5 YesLR2 (bilateral) 0.18 × 25 0.4 YesSP6 (bilateral) 0.25 × 40 0.7 YesSP9 (bilateral) 0.25 × 50 1.2 YesST36 (bilateral) 0.25 × 50 1.3 YesKI3 (bilateral) 0.18 × 25 0.4 YesKI6 (bilateral) 0.18 × 25 0.4 YesKI7 (bilateral) 0.18 × 25 0.4 Yes

Cancer- related hot flashes and night sweating
© 2016 Acupuncture Association of Chartered Physiotherapists96
for patients with breast cancer who are seeking non- pharmacological therapies.
There is good evidence that acupuncture can be effective in the treatment of breast- cancer- related hot flashes and night sweating. For example, Walker et al. (2010) demonstrated that 12 weeks of acupuncture is as effective as ven-lafaxine in managing vasomotor symptoms in patients with breast cancer. In addition to this, the above authors demonstrated that hot flashes remained at low levels in the acupuncture group 2 weeks after treatment, whereas the venlafaxine group had experienced significant increases in hot flashes by this time. Positive results were maintained in the acupuncture group 12 weeks after treatment ended. The acupuncture group had the additional benefits of an improvement in their energy levels, and a sense of well- being without any adverse effects. On the other hand, the venlafaxine group experienced side
effects such as nausea, dry mouth, dizziness and anxiety.
Similarly, De Valois et al. (2010) explored the use of traditional acupuncture to manage tamoxifen- related hot flashes and night sweating in women with early breast cancer. Furthermore, they extended the focus of their study to meas-ure physical and emotional well- being using the Women’s Health Questionnaire (WHQ), and the Hot Flashes and Night Sweats Questionnaire. Acupuncture treatment was given on a weekly basis for 8 weeks, and its effects were monitored for up to 30 weeks after treatment. In contrast to Walker et al. (2010), De Valois et al. (2010) reported that a number of participants did not adhere to the weekly acupuncture schedule, and had treatments beyond the allocated 8- week period because of leaving gaps between sessions. This could have influenced both the short- and long- term outcomes of the study. Nevertheless,
Table 2. Treatment outcomes: (LI) Large Intestine; (PC) Pericardium; (HT) Heart; (SP) Spleen; (ST) Stomach; (KI) Kidney; (LR) Liver; and (TE) Triple Energizer
Treatment session (week)
Acupuncture points
Number of hot flashes
Number of night sweats
1
LI4, PC6, HT6, HT7, SP6, SP9, ST36, KI3, KI6, LR2
3–4 every hour, with warmth all over the body and then a feeling of skin peeling from inside
4–6 every night; the subject needed to change her clothes several times
2
LI4, PC6, HT6, HT7, SP6, SP9, ST36, KI3, KI6, LR2, PC8, HT8, LI11
3–4 every hour, with warmth all over the body and then a feeling of skin peeling from inside
4–6 every night; the subject needed to change her nightclothes several times
3
LI4, PC6, HT6, HT7, SP6, SP9, ST36, KI3, KI6, LR2, PC8, HT8, LI11, KI7, TE5
3–4 every hour, with warmth all over the body and then a feeling of skin peeling from inside
4–6 every night; the subject needed to change her nightclothes several times
4
As above
3–4 hot flashes every 2–3 h; a slight reduction in warmth and feeling of skin peeling from inside
4–6 every night, but with less intensity; the subject needed to change her nightclothes at times
5
As above
3–4 hot flashes every 2–3 h with less intensity; no warmth or feeling of skin peeling from inside
3–4 every night, but with less intensity; the subject managed her sweating without any need for a change of nightclothes
6
As above
4–6 hot flashes in a day with less intensity; no warmth or feeling of skin peeling from inside*
3–4 every night but with less intensity; the subject managed sweating without any need for a change of nightclothes
7
As above
2–3 hot flashes in a day with less intensity; no warmth or feeling of skin peeling from inside
1–2 mild ones every night; quality of sleep had improved
8 As above 0; only a damp feeling two or three times a day without any hot flashes
1–2 mild ones every night; overall sense of well- being had improved
*The subject experienced palpitation, anxiety, irritability and headaches at the time of the hot flashes. These associated symptoms began to lessen from week 6 onwards, and a considerable reduction was reported at the end of 8 weeks of treatment.
V. Ramasamy
© 2016 Acupuncture Association of Chartered Physiotherapists 97
the present subject reported improvements in her physical and emotional well- being, as well as reductions in hot flashes and night sweating.
The VAS was used as a subjective outcome measure in the present case study. On reflec-tion, it might have been beneficial to use more- measurable markers (e.g. the WHQ) of the frequency and intensity of hot flashes and night sweating, and health- related QoL. The WHQ subscales focus on aspects of emotional and physical health, such as depression, sleep problems, anxiety and somatic symptoms. Establishing the optimum dose, frequency and duration of acupuncture is an outstanding issue with regard to this form of treatment. It might be worthwhile extending the present subject’s treatment to determine whether her hot flashes and night sweating could be further reduced.
ConclusionsIt would appear that eight sessions of acupunc-ture treatment had a very good effect on the present subject’s hot flashes and night sweating. The symptoms associated with hot flashes and night sweating reduced considerably, and this improved her QoL.
Acupuncture has a good safety profile and a low incidence of side effects, and is a low- risk form of non- pharmacological treatment. On the basis of the present single case study, it is possible that acupuncture may be an accept-able treatment option in the management of hot flashes and night sweating in patients with breast cancer.
AcknowledgementsI would like to thank the subject for consenting to the publication this case study. I would also like to thank Mr Roger Wheelwright, a prostate cancer nurse specialist, for his advice and sup-port during this process.
ReferencesAcupuncture Association of Chartered Physiotherapists
(AACP) (2012) AACP Guidelines for Safe Practice, Version 2. [WWW document.] URL http://www.
aacp.org.uk/member- home/references/guidelines/clinical/239- guidelines- for- safe- practice/file
Borud E. K., Alraek T., White A., et al. (2009) The Acupuncture on Hot Flushes Among Menopausal Women (ACUFLASH) study, a randomized controlled trial. Menopause 16 (3), 484–493.
Carpenter J. S., Andrykowski M. A., Cordova M., et al. (1998) Hot flashes in postmenopausal women treated for breast carcinoma: prevalence, severity, correlates, management, and relation to quality of life. Cancer 82 (9), 1682–1691.
Carpenter J. S., Johnson D. H., Wagner L. J. & Andrykowski M. A. (2002) Hot flashes and related outcomes in breast cancer survivors and matched comparison women. Oncology Nursing Forum 29 (3), E16–E25.
De Valois B. A., Young T. E., Robinson N., McCourt C. & Maher E. J. (2010) Using traditional acupuncture for breast cancer- related hot flashes and night sweats. The Journal of Alternative and Complementary Medicine 16 (10), 1047–1057.
Fahlén M., Wallberg B., von Schoultz E., et al. (2011) Health- related quality of life during hormone therapy after breast cancer: a randomized trial. Climacteric 14 (1), 164–170.
Filshie J., Bolton T., Browne D. & Ashley S. (2005) Acupuncture and self acupuncture for long term treatment of vasomotor symptoms in cancer patients – audit and treatment algorithm. Acupuncture in Medicine 23 (4), 171–180.
Guo Z.- L., Moazzami A. R., Tjen- A- Looi S. & Longhurst J. C. (2008) Responses of opioid and serotonin con-taining medullary raphe neurons to electroacupuncture. Brain Research 1229 (September), 125–136.
Hervik J. & Mjåland O. (2009) Acupuncture for the treatment of hot flashes in breast cancer patients, a randomized, controlled trial. Breast Cancer Research and Treatment 116 (2), 311–316.
Holmberg L., Iversen O.- E., Rudenstam C. M., et al. (2008) Increased risk of recurrence after hormone replacement therapy in breast cancer survivors. Journal of the National Cancer Institute 100 (7), 475–482.
Hui K. K. S., Marina O., Liu J., Rosen B. R. & Kwong K. K. (2010) Acupuncture, the limbic system, and the anticorrelated networks of the brain. Autonomic Neuroscience: Basic and Clinical 157 (1–2), 81–90.
Hunter M. S., Grunfeld E. A., Mittal S., et al. (2004) Menopausal symptoms in women with breast cancer: prevalence and treatment preferences. Psycho- Oncology 13 (11), 769–778.
Kronenberg F. (1990) Hot flashes: epidemiology and physiology. Annals of the New York Academy of Sciences 592 (June), 52–86.
Loprinzi C. L., Pisansky T. M., Fonseca R., et al. (1998) Pilot evaluation of venlafaxine hydrochloride for the therapy of hot flashes in cancer survivors. Journal of Clinical Oncology 16 (7), 2377–2381.

Cancer- related hot flashes and night sweating
© 2016 Acupuncture Association of Chartered Physiotherapists98
Miller H. G. & Li R. M. (2004) Measuring hot flashes: summary of a National Institutes of Health Workshop. Mayo Clinic Proceedings 79 (6), 777–781.
Million Women Study Collaborators (MWSC) (2003) Breast cancer and hormone- replacement therapy in the Million Women Study. Lancet 362 (9382), 419–427.
Moazzami A., Tjen- A- Looi S. C., Guo Z.- L. & Longhurst J. C. (2010) Serotonergic projection from nucleus raphe pallidus to rostral ventrolateral medulla modulates car-diovascular reflex responses during acupuncture. Journal of Applied Physiology 108 (5), 1336–1346.
Nelson H. D., Vesco K. K., Haney E., et al. (2006) Nonhormonal therapies for menopausal hot flashes: systematic review and meta- analysis. JAMA: The Journal of American Medical Association 295 (17), 2057–2071.
Omura Y. (1975) Pathophysiology of acupuncture on cardiovascular and nervous systems. Acupuncture and Electro- Therapeutics Research 1 (2), 55–141.
Studdard J. D. (1999) Patient profile 1: unresolved vaso-motor symptoms with conventional hormone replace-ment therapy. American Journal of Obstetrics and Gynecology 180 (3, Pt 2), S317–S318.
Towlerton G., Filshie J., O’Brien M. & Duncan A. (1999) Acupuncture in the control of vasomotor symptoms caused by tamoxifen. [Letter.] Palliative Medicine 13 (5), 445.
Tukmachi E. (2000) Treatment of hot flushes in breast cancer patients with acupuncture. Acupuncture in Medicine 18 (1), 22–27.
Walker E. M., Rodriguez A. I., Kohn B., et al. (2010) Acupuncture versus venlafaxine for the management of vasomotor symptoms in patients with hormone receptor- positive breast cancer: a randomized con-trolled trial. Journal of Clinical Oncology 28 (4), 634–640.
Wyon Y., Lindgren R., Lundeberg T. & Hammar M. (1995) Effects of acupuncture on climacteric vasomo-tor symptoms, quality of life, and urinary excretion of neuropeptides among postmenopausal women. Menopause 2 (1), 3–12.
Wyon Y. A., Spetz A. C., Theodorsson G. E. & Hammar M. L. (2000) Concentrations of calcitonin gene- related peptide and neuropeptide Y in plasma increase during flushes in postmenopausal women. Menopause 7(1), 25–30.
Visweswaran Ramasamy qualified as a chartered physio-therapist in 2000, and initially worked in India before moving to the UK in 2005. He graduated with an MSc in Musculoskeletal Physiotherapy from Sheffield Hallam University. Visweswaran works as a clinical specialist physiotherapist at John Taylor Hospice in Birmingham. He uses acupuncture for complex pain management, and to treat various cancer- related symptoms.

© 2016 Acupuncture Association of Chartered Physiotherapists 99
Acupuncture in Physiotherapy, Volume 28, Number 1, Spring 2016, 99–102
Book reviews
How the Art of Medicine Makes the Science More Effective: Becoming the Medicine We PracticeBy Claudia WelchSinging Dragon, London, 2015, 256 pages, hardback, £18.99ISBN 978- 1- 84819- 229- 4
“‘[E]vidence- based medicine’ seems an opti-mistic label for medical protocols dictated by study results. When misconduct affects research in every field of medicine, when positive findings are twice as likely to be pub-lished as negative ones, and when 50 percent of all study results are buried, suppressed or go missing [Goldacre 2012], how can we, as doctors, trust the studies we read, or feel confident in the likely effects of the medicine we prescribe?” (p. 33)
How the Art of Medicine Makes the Science More Effective: Becoming the Medicine We Practice is a par-tial answer to the question posed by the passage quoted above. Dr Claudia Welch has prepared an intelligent meditation on the art and science of so- called holistic medicine. Given the pre-sent situation with regard to the publication of new research work and the undoubted neglect of much research in the past – some positive, some negative – complementary medicine in general has not fared well.
The argument runs that emotional contact with, and understanding of, the patient is just as important as the physical application of the therapy. Dr Welch emphasizes the spiritual aspect of the healing arts in the belief that healing can never be truly completed without the spiritual side of medicine. Those familiar with the phi-losophy of traditional Chinese medicine (TCM) will be the least surprised to read this perhaps, since TCM concerns itself very much with how the patient feels, in addition to what they suffer by way of pain or discomfort. However, all of us working in the medical field are aware that we need to take account of the total situation.
The best way to give a flavour of this book is to show the scope of the many topics covered in the five main parts.
The first section, “Excellence in Theoretical Knowledge: How We Know What We Know”, includes a consideration of the sources of knowledge, details of ways to refine our percep-tion and recommendations about how to use it to help with prediction.
A lot more helpful advice follows in the second part, “Extensive Practical Experience: Things We May Not Learn in School”, which contains, for example, chapters entitled: “Don’t Panic. Wait”; “Treat Complicated with Simple”; “When Nothing Is Wrong, Pay Close Attention”; “Turning Away Patients”; “Tell the Truth”; “Mental Illness”; “Domestic Violence”; and “Determining the Severity of a Crisis.”

Book reviews
© 2016 Acupuncture Association of Chartered Physiotherapists100
The third section, “Dexterity: The Value of Flexible Medicine”, covers patients who consist-ently experience odd reactions to remedies, and cause us to explore outside our own fields.
There are some interesting topics to consider in the next part, “Purity: Are We Medicine or Poison?”, which includes chapters on: “Spiritual Powers vs. Effect of Character; “The Mechanics of Emotional Contagion: Who Affects Whom?”; and “Supporting Change Through Appropriate Familiarity, Love, and Focus”.
Part V discusses “The Four Qualities of Effective Medicine”, which are abundance, suit-ability, multiple form and potency.
How the Art of Medicine Makes the Science More Effective will be essential reading for all healthcare practitioners who are interested in understanding the art of their practice, and how it can enhance therapeutic outcomes, including doctors of Ayurveda, TCM and naturopathy, as well as Western medical professionals and other complementary practitioners. Dr Welch also offers practical steps that will help doctors to cultivate their own compassion and further refine their perceptive abilities.
Finally, Dr Welch offers a modern- day ver-sion of the Hippocratic Oath, reminding us that: “we vow to ‘remember that there is art to medicine as well as science, and that warmth, sympathy and understanding may outweigh the surgeon’s knife or the chemist’s drug’” (p. 17).
Val HopwoodClinical Editor
ReferenceGoldacre B. (2012) What Doctors Don’t Know about the Drugs
They Prescribe. [WWW document.] URL https://www.ted.com/talks/ben_goldacre_what_doctors_don_t_know_about_the_drugs_they_prescribe?language=en
Trauma Is Really StrangeBy Steve Haines and Sophie StandingSinging Dragon, London, 2016, 32 pages, paperback, £7.99ISBN 978- 1- 84819- 293- 5
Written by Steve Haines and illustrated by Sophie Standing, this is a small comic book
filled with simple illustrations and complex ideas. The text is pretty basic, but it covers most of the theories associated with the science of trauma. These are presented in a highly abbrevi-ated way, but there is a handy reference list if you want to read more. Trauma Is Really Strange attempts to answer the question of what trauma actually is, and show us how we can overcome it. Surprisingly, the rather simplistic colour illus-trations really do add to the clarity.
This unique format explains the strange nature of trauma, and how it confuses the brain and affects the body. When stressed in this way, human beings tend to dissociate, and our bodies shut down normal processes while the brain is unbalanced by the trauma. This book offers explanations of how our physiology might change following trauma, and describes techniques that could be used to reverse the process:
“The very nature of trauma is that it is overwhelming. It is more than the organism

Book reviews
© 2016 Acupuncture Association of Chartered Physiotherapists 101
can cope with [. . .] [T]rauma takes us to very primitive places of fight or flight or dis-sociation. It is very hard to live fully with our brain screaming ‘danger!’ and generating life or death scenarios at the slightest stimulus.” (p. 31)
Trauma resolution involves conscious techniques that are capable of changing the body’s physiol-ogy, and Trauma Is Really Strange illustrates and briefly describes some of these. The artwork is amusing, using cat and mouse metaphors, and many simple but witty pictures.
According to Joseph (2013): “On average, only 8–12 per cent of people exposed to trau-matic events – and around a fifth to a quarter of those involved in profoundly traumatic experiences – ever reach the diagnostic thresh-old for PTSD.”
It is clear from the above that the lesser symptoms remain largely unreported, and patients may well need help to cope. This is a useful book to keep beside you in the clinic, and could be used to help patients understand the problems that they have after undergoing major trauma, above and beyond those you may be treating. The drawings offer an easy way to understand some of the symptoms of changing physiology. Reflective awareness would appear to be the key. Trauma Is Really Strange mainly seems to be targeting those involved in bodywork, but the techniques described could apply equally to physiotherapists. Trauma- releasing exercises that allow the body to shake away tension, safely releasing deep muscular patterns of stress and trauma, are described briefly, and might well be helpful (Berceli 2008).
This rather unlikely little book could be very useful to therapists and members of the public alike.
Val HopwoodClinical Editor
ReferencesBerceli D. (2008) The Revolutionary Trauma Release Process:
Transcend Your Toughest Times. Namaste Publishing, Vancouver.
Joseph S. (2013) What Doesn’t Kill Us: The New Psychology of Posttraumatic Growth. Basic Books, New York, NY.
Dry Needling for Manual Therapists: Points, Techniques and Treatments, Including Electroacupuncture and Advanced Tendon TechniquesBy Giles Gyer, Jimmy Michael and Ben TolsonSinging Dragon, London, 2016, 315 pages, hardback, £21.99ISBN 978- 1- 84819- 255- 3
Dry Needling for Manual Therapists: Points, Techniques and Treatments, Including Electroacupuncture and Advanced Tendon Techniques is an interesting addi-tion to the extensive literature on trigger point acupuncture. Much of the material in this excel-lent book may be very familiar to members of AACP; however, since it is so comprehensive, they may find plenty of new ideas to stimulate their practice. It seems to be primarily aimed at physical therapists, but could be useful to all therapists who deal with musculoskeletal conditions.
The layout follows that of an introductory text: it is simple and practical, with colour- coded page edges, offering easy reference in the clinic.

Book reviews
© 2016 Acupuncture Association of Chartered Physiotherapists102
There are four main sections: “Background”; “Theories Around Dry Needling and Traditional Chinese Medicine”; “Preparing for Treatment”; and “Needling Techniques”.
The authors have managed to achieve a good mix of traditional Chinese acupuncture (TCA) ideas and the modern techniques of Western medical acupuncture (WMA). The book offers brief but helpful explanations of most of the TCM or WMA theories supporting these acu-puncture techniques. Interestingly, some limited space is also given to Japanese acupuncture. In particular, there are chapters on tendinopathy and tendon techniques, and one section also gives an excellent introduction to electroacu-puncture, which sometimes illustrate the use of cross- patterns of needles.
The anatomical illustrations in the trigger point section are particularly good. There is a useful separation of the diagrams of the areas of referred pain, the colour photographs and the clear illustrations of the actual anatomical structures.
Given that some of readers will have had little or no acupuncture training, it is good to note that the section on safety is comprehensive
and carefully written. The physiological evidence for the actions of the acupuncture stimulus is reasonably well covered, and the better studies establishing the effectiveness of the techniques are described and cited.
In general, this is a well- written text with helpful diagrams and illustrations that will sup-port the use of trigger point acupuncture for both sports injuries and chronic pain.
The closest rival to this volume is Acupuncture, Trigger Points and Musculoskeletal Pain (Baldry 2005), which was last updated over 10 years ago. While the trigger point illustrations are very similar, the research underpinning the WMA theories has obviously moved forward. If you do not already own a copy of Dr Peter Baldry’s classic textbook, then Dry Needling for Manual Therapists would be a very good book to purchase.
Val HopwoodClinical Editor
ReferenceBaldry P. E. (2005) Acupuncture, Trigger Points and
Musculoskeletal Pain, 3rd edn. Churchill Livingstone, Edinburgh.

© 2016 Acupuncture Association of Chartered Physiotherapists 103
Acupuncture in Physiotherapy, Volume 28, Number 1, Spring 2016, 103–104
News, views and interviews
Why publish anyway?We depend heavily on the contributions of our membership when we select the material for each edition of Acupuncture in Physiotherapy. The continuing high quality of this publication is no accident! You may feel that the undeniable effort of writing a case report or a literature review for the journal may not be worth your precious time, but here are some thoughts that may encourage you.
It is recognized that not everybody wants to try their hand at research, many preferring the practical daily use of their hard- won physiother-apy skills, but nonetheless:
• Seeing your name in print is a good experience.
• Both the Health and Care Professions Council, and AACP demand regular continu-ing professional development updates, and this is a useful way of obtaining them.
• It will look impressive on your curriculum vitae.
• Your manager will be pleased.
• Your manager will be even happier if you include him or her as the second author, which you may well do if you have found him or her to be supportive and helpful.
• Publication makes the whole department look good in the eyes of the trust.
All of the above are either necessary or diplo-matic. However, entering the world of research can be very rewarding, and your first publication can set the tone for a return to further study, an MSc or even a PhD! A gentle progression through the possibilities can map out a really interesting future:
• Case studies. Wait for a patient who really inter-ests you. During the first treatment session, decide how you will try to treat the subject, what your rationales for choosing points and techniques will be, and which parameters of recovery you will use to measure progress
over time. Make sure that your approach will be feasible, engage the subject in his or her own treatment, and keep careful notes as you progress.
• Controlled series of case studies. These are similar to single- case studies, but make sure that, even if you individualize your treatments, you are treating the same basic condition and measuring exactly the same outcomes. This allows you some kind of comparison, and will enable you to indicate any trends in the participants’ responses to your treatments. You need around five or six patients for this type of exploratory study. A very good text to help you with organization and planning treatment schedules is Single- Case Research Designs: Methods for Clinical and Applied Settings (Kazdin 2010). This makes it easier to struc-ture both the treatment and non- treatment phases of your studies when your patients are not necessarily beginning at the same time.
• Pragmatic groups. Sometimes you may have uneven referral patterns, and therefore, while you may select from these groups, it would be difficult to control the number of treatments and complete a “tidy” research project. Admitting and providing therapy for appropriate patients who have been accepted for treatment in your centre is quite possible as long as you are clear that there will be poor control over the groups, and while the numbers may be greater, the participants will only provide an indication of trends, as men-tioned above. However, no careful recording of treatment and effect is ever wasted!
• Systematic reviews. A systematic review is a vital step when you are thinking about running a major trial, but this can be done well in advance. If your definition of the topic or question is precise, then all you have to do is read as much as you can get hold of before drawing any conclusions. This is a good way

News, views and interviews
© 2016 Acupuncture Association of Chartered Physiotherapists104
of involving some of your colleagues: if at least three people manage to read all the research papers, you can make a rational deci-sion about the quality of the literature that you will eventually include. This is another way to involve your department!
• Randomized controlled clinical trials. If you are not already working towards a higher degree within a university group, contact AACP directly when you get to the stage of seriously considering a properly controlled clinical trial. There is a lot of expertise avail-able to guide you towards the most effective methods. Make a rough time plan of what you want to investigate, and why. Offer us ideas about prospective patient groups, cases to include and those unsuitable for your techniques. I have no intention of writing
the definitive guide, but would be happy to recommend some really useful books if you would like to contact me (e- mail: [email protected]).
I must add that, when I set out to write this short piece of encouragement, a colleague sug-gested that I offer the opinion that published work makes you quite irresistible to the opposite sex. Since, as far as I’m aware, scientific proof of this is notably absent, perhaps that could be an early project!
Val HopwoodClinical Editor
ReferenceKazdin A. E. (2010) Single- Case Research Designs: Methods for
Clinical and Applied Settings, 2nd edn. Oxford University Press, Oxford.
© 2016 Acupuncture Association of Chartered Physiotherapists 105
Acupuncture in Physiotherapy, Volume 28, Number 1, Spring 2016, 105–107
Guidelines for authors
IntroductionAlways refer to a recent edition of Acupuncture in Physiotherapy. Please follow the style and layout of an article or item that is similar to your own contribution. If something is submitted for publication, then it is implied that it has not been simultaneously submitted to another journal or any other type of publication. Reprints may be considered, but these must be clearly identified as such and permission must be obtained from the original publisher.
Templates for clinical papers and case reports are available on the AACP website (www.aacp.org.uk), or by e-mail on request. These templates should not be deviated from if used. Manuscripts may be returned to authors if they have not adhered to the guidelines. If necessary, the clini- cal editor should be consulted in the initial stages for clarification.
Authors may submit clinical papers, literature reviews, clinical commentaries, case reports, book reviews, course reports, news items, letters or photographs for consideration for inclu- sion in the journal. Academic and clinical papers are subject to review by the editorial committee and may require revision before being accepted.
A Portable Document Format (PDF) file of the final version of any academic article is available free of charge if notice is given to the clinical editor when the article is submitted.
All published material becomes the copyright of the Association.
All submissions should be sent directly to the clinical editor:
Dr Val Hopwood FCSP18 Woodlands CloseDibden PurlieuSouthampton SO45 4JGUK
E-mail: val.hopwood\@btinternet.com
Preparation of manuscriptsAuthors should submit material by e-mail or on CD-ROM. All articles must be typed with wide (3-cm) margins and the pages should be num-bered consecutively. Articles should be a maxi-mum of 7500 words (excluding the abstract, references and tables).
Papers should be arranged as follows:
TitleThe title of the article should be in sentence case, bold and ranged left, as in the main title above: note that there is no full stop and no underlining. The author’s name(s) and institutional affilia-tion(s) should run consecutively below the title. Again, there are no full stops.
Abstract A summary of not more than 250 words outlin-ing the purpose, scope and conclusions of the paper should be submitted. This should be followed by a minimum of three and a maximum of five keywords that best represent the contents.
Text The layout of the journal is that the main heading of each section is in sentence case and bold. Notice that, again, there are no full stops and no underlining.
The first paragraph is left-justified; subsequent paragraphs in the same section are indented, as is this part of the guidelines. When including dia- grams and photographs, these should be num-bered in the order in which they appear in the text, and should be submitted in separate files (do not embed images in the text). Any figure captions should be left-justified and run after the author’s biography at the end of the text. Any tables should come after the figure legends, if there are any. Please indicate placement in the text (e.g. “Fig. 1’’ and “Table 1’’). All figures and tables must be referred to in the text.

Guidelines for authors
© 2016 Acupuncture Association of Chartered Physiotherapists106
When using numbers in the text, these should be written out in words up to and including nine unless these are measurements, numbers in tables or units of time. Always use the Inter-national System of Units (SI).
Clinical papers: referencing All clinical papers must be fully referenced and the citations verified by the author. No excep-tions will be made. The reference list must be arranged alphabetically by the name of the first author or editor, following the Harvard style. In the text, give the author(s) and date of publica-tion in brackets (e.g. “(Smith 1998)’’), or if the main author’s name is part of a sentence, then only the year is in brackets [e.g. “as described by Smith (1998)’’]. For more than one author, reference can be made in the text to “Smith et al. (1998)’’ (note the italics). However, when writ- ing the reference list, the convention is as fol-lows: for up to five authors, write all the authors’ names; for six or more authors, write the first three authors’ names, followed by “et al.”
For journals, give the author’s surname and initials, the year of publication, the title of the paper, the full name of the journal, the volume number, the issue number in brackets, and the first and last page numbers of the article (note the correct use of italic, bold, commas and full stops):
Ceccherelli F., Rigoni M. T., Gagliardi G. & Ruzzante L. (2002) Comparison of superficial and deep acupuncture in the treatment of lumbar myofascial pain: a double-blind randomized controlled study. Clinical Journal of Pain 18 (3), 149–153.
For books, give the author’s/editor’s surname and initials, the year of publication, the book title in italics, and the publisher and city of publication:
Williams P. L. & Warwick R. (eds) (1986) Gray’s Anatomy, 36th edn. Churchill Livingstone, Edinburgh.
For a chapter or section in a book by a named author (who may be one of several contributors), both chapter and book title should be given, along with the editor’s name(s), and the first and last page numbers of the chapter:
Bekkering R. & van Bussel R. (1998) Segmental acupunc-ture. In: Medical Acupuncture: A Western Scientific Approach (eds J. Filshie & A. White), pp. 105–135. Churchill Livingstone, Edinburgh.
For references to documents on the World Wide Web (WWW), give the author’s surname followed by all initials, the year of publication in brackets, the document title in italics, an indica-tion that it is a WWW document in square brackets and the complete Uniform Resource Locator (URL):
List D. (2004) Maximum Variation Sampling for Surveys and Consensus Groups. [WWW document.] URL http://www.audiencedialogue.net/maxvar.html
Please adhere strictly to this style of referencing in any contribution to the journal.
Acknowledgements Please state any funding sources, or companies providing technical or equipment support.
Photographs Photographs may be submitted in colour or black-and-white, but will be printed in mono-chrome. Images must be in sharp focus. Photo-graphs should be numbered and their placing indicated in the text. Digital photographs should be of high resolution (i.e. a minimum of 300 dots per inch).
Line illustrations These should follow the style used in the journal, i.e. any labelling text should be in sentence case (10-point, Arial font), graphs should be two-dimensional and all images must be mono-chrome. As with photographs, line illustrations should be numbered and their placement indi-cated in the text. All images should be of high resolution (i.e. a minimum of 1200 dots per inch).
Case reportsThe journal welcomes case reports of up to 3000 words. These should be structured as follows: title, abstract and keywords, a brief

Guidelines for authors
© 2016 Acupuncture Association of Chartered Physiotherapists 107
introduction, a concise description of the patient and condition, and an explanation of the assess-ment, treatment and progress, followed finally by a discussion and evaluation of the implications for practice. The study must be referenced throughout. Further guidance is available upon request.
Book reviewsAt the beginning of the review, give all details of the book including the title in bold, the author/editor’s full name(s), publisher, city and year of publication, price, whether hardback or paper-back, number of pages, and ISBN number. The reviewer’s name should appear at the end of the review in bold, right-justified, followed by their title and place of work in italics. Reviews of DVDs and DVD-ROMs should follow the same format. Book reviews and reports are normally
no more than 500 words in length; query for longer.
Please contact the clinical editor before writing a review.
General points to notePlease enclose your home, work and e-mail addresses, and telephone number.
It is the author’s responsibility to obtain and acknowledge permission to reproduce any material that has appeared in another journal or textbook.
A brief biographical note about the author(s) should be included at the end of a clinical paper in italics.
All notes and news should have clinical rel-evance to AACP. Please refer at all times to the style and layout of previous issues of the journal for whatever you are writing. Using these guide-lines will save the editorial team time.
Ask your
Physiotherapis
t
about acupunc
ture
and see howit
could help you
Acupuncture ca
n be combined with
other physioth
erapy treatments
such asexercise
, manual therapy
and relaxation tech
niques,to treat
a wide range of
common health
problems and to redu
ce pain.
Acupuncture As
sociation of
Chartered Phys
iotherapists
For more information
about acupunc
ture,
visit www.aacp.
co.uk
AcC

Acupuncture in PhysiotherapyTM
Journal of the Acupuncture Associationof Chartered Physiotherapists
Spring 2016 Volume 28, Number 1
ISSN 2058-3281
Acupuncture in Physiotherapy
TMVolum
e 28, Num
ber 1, Spring 2016


















