
Fourth Annual Healthcare Forum
78
Fourth Annual Healthcare Forum April 11, 2018 McDermott Will & Emery
Transcript of Fourth Annual Healthcare Forum

Fourth Annual Healthcare Forum
April 11, 2018 McDermott Will & Emery

Slide
Agenda • 8:30 Welcome – Roger Waldron
• 8:45 Legislative Outlook – Honorable Jeff Miller
• 9:00 DHA Keynote Address – Guy Kiyokawa
• 9:30 Break
• 9:45 Improving Clinical Input in MSPV – Tammy Czarnecki
• 10:15 VA OSDBU Fair & Reasonable Pricing – Tom Leney
• 11:15 Break
• 11:30 Business Intelligence Sessions
• 12:30 Lunch
• 1:30 MSPV-NG, Formulary, and More – Rick Lemmon & Jaime Friedel

Slide
Forum Sponsor

Slide
Keystone Members

Slide
Executive Members

Slide
Strategic Partners

Legislative Outlook – Congressman Jeff Miller, Senior Legislative Advisor, McDermott Will & Emery
“Medically Ready Force…Ready Medical Force” 1
Military Health System:The Defense Health Agency in 2018
&Acquisition in the DHA
Mr. Guy KiyokawaDeputy Director, Defense Health Agency
April 11, 2018

“Medically Ready Force…Ready Medical Force” 2
… What have we done for them today?

What is the DHA?
“Medically Ready Force…Ready Medical Force” 3
Who we are“ … a joint, integrated Combat Support Agency that enables the Army, Navy, and Air Force medical services to provide a medically ready force and ready medical force to Combatant Commands in both peacetime and wartime.”
What we do Enterprise shared services Standardization and coordination TRICARE health plan NCR Medical Directorate

“Medically Ready Force…Ready Medical Force” 4
Pharmacy Programs Facilities
TRICARE Health Plan Procurement/Contracting
Health Information Technology
Research, Development & Acquisition
Budget & Resource Management Public Health
Medical Logistics Education and Training
Enterprise Activities

MHS Reform
DoD TaskForce on MHS
Governance
September 2011
DEPSECDEFPlanning Memo
March 2012
Directed planning for DHA implementation
March 2013
Directed implementation of
DHA
Dec 2017
Directed implementation of
Broader Responsibilities
DHA PlanningWG Report
November 2012
DHA Shared Services implementation plan
for DEPSECDEF
NDAA 2017
Recommended DHA model for MHS
Governance
September 2013
DODD5136.13
DEPSECDEF“Nine
Commandments”Memo
Establishes the DHA
Global Integration – Enterprise Shared Services – Standardized Processes

FY17 National Defense Authorization ActThe Rationale for MHS Reform
“…a single agency responsible for the administration of all MTFs would: • best improve and sustain operational medical force readiness
and the medical readiness of the Armed Forces, • improve beneficiaries’ access to care, • improve health outcomes, • and lower the total management cost of the military health
system.”
3
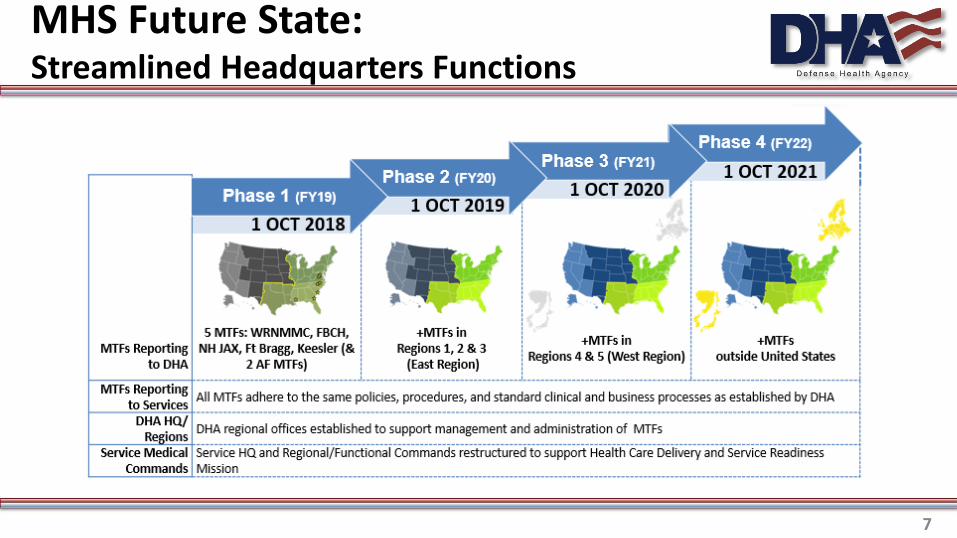
MHS Future State:Streamlined Headquarters Functions
7

MHS reform: DHA and MTFs
“Medically Ready Force…Ready Medical Force” 8

Health IT
“Medically Ready Force…Ready Medical Force” 9

SECDEF Mattis Memo (17 Feb 2017)It’s not just Congress
DoD Deputy Chief Management Officer
“Rebuild”
“Reform”
“Medically Ready Force…Ready Medical Force” 11
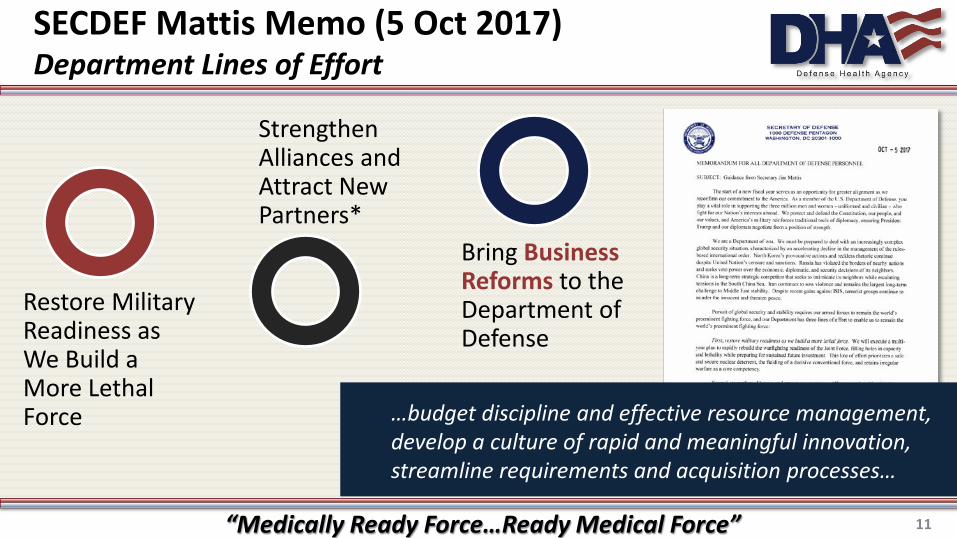
SECDEF Mattis Memo (5 Oct 2017)Department Lines of Effort
…budget discipline and effective resource management, develop a culture of rapid and meaningful innovation, streamline requirements and acquisition processes…
Restore Military Readiness as We Build a More Lethal Force
Strengthen Alliances and Attract New Partners*
Bring Business Reforms to the Department of Defense

“Medically Ready Force…Ready Medical Force” 12
Integrated Health Systems are GrowingHealth insurance plans, hospitals, clinics
Ξ Driven by value-based incentives in medicine with goals to:
Ξ Leading health institutions are expanding geographic reach and standardizing processes
Improve quality
Improve outcomes
Improve efficiency
Reduce costs
Presenter
Presentation Notes
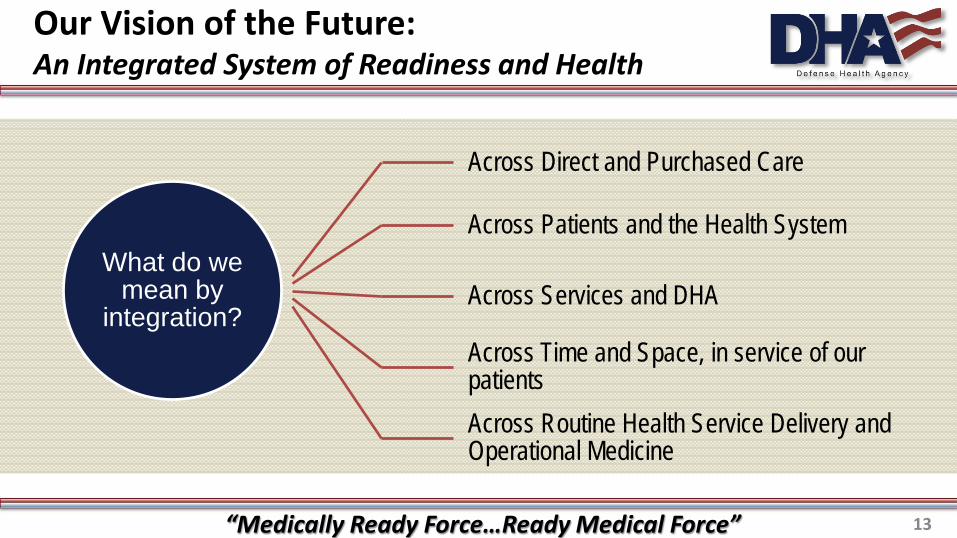
Our Vision of the Future:An Integrated System of Readiness and Health
“Medically Ready Force…Ready Medical Force” 13
What do we mean by
integration?
Across Direct and Purchased Care
Across Patients and the Health System
Across Services and DHA
Across Time and Space, in service of our patientsAcross Routine Health Service Delivery and Operational Medicine

Our Vision of the Future:Enabled through Acquisition
“Medically Ready Force…Ready Medical Force” 14
What do we mean by
integration of Acquisition?
Strategic Sourcing across organizational boundariesSharing agreements enabling patient flow across markets
Dramatic reduction in duplicate contracts
Market focused contracts responsive to regional demand signals
Standardized products and services
VADM Bono: Expectations for our Partners
• Readiness-Focused & Patient-centered
• Agile
• Prepared to support a more integrated future
“Medically Ready Force…Ready Medical Force” 15

16
Connect with Military Medicine
@DHADirector
@DefenseHealthAgency

Networking Break
Improving Clinical Input in MSPV – Tammy Czarnecki, Assistant Deputy Under Secretary of Health for Administrative Operations, VA

VA Fair and Reasonable Pricing – Tom Leney, Executive Director Small and Veteran Business Programs, VA

Networking Break
Defense Health Agency Pharmacy Operations: A Time of Transition
David W. Bobb, RPH, JD Chief, DHA Pharmacy Operations Division
(The information in this briefing is presented by the author/presenter and does not represent the position of the Department of Defense; the data is presented for illustration and may contain estimates and assumptions)
Coalition for Government Procurement Healthcare Forum 11 April 2018
1
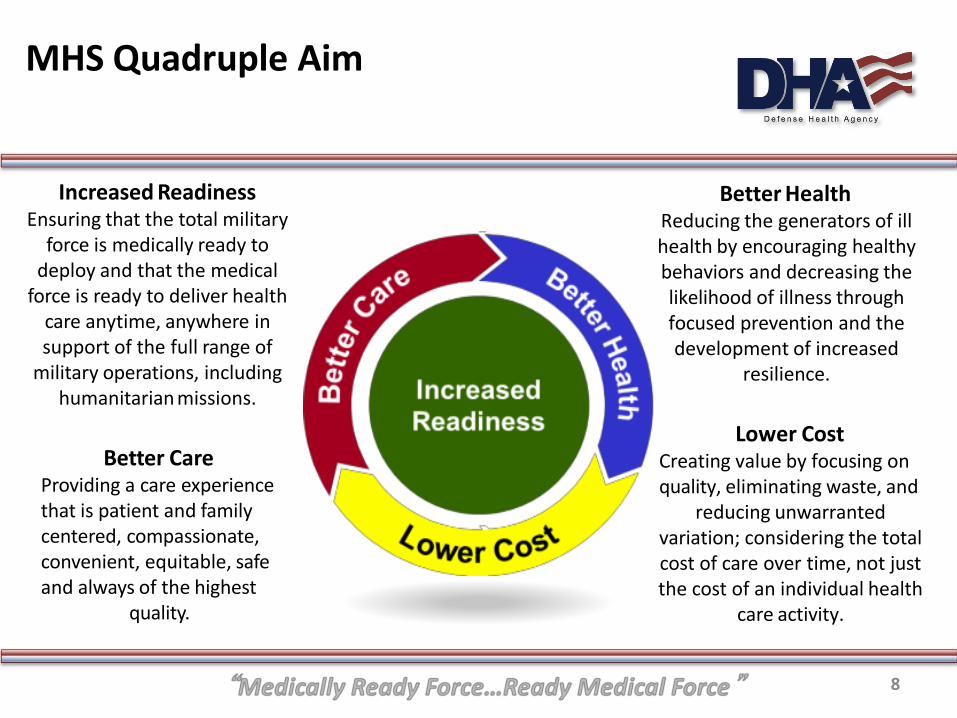
MHS Quadruple Aim
Increased Readiness Ensuring that the total military
force is medically ready to deploy and that the medical
force is ready to deliver health care anytime, anywhere in support of the full range of
military operations, including humanitarian missions.
Better Care
Providing a care experience that is patient and family centered, compassionate, convenient, equitable, safe and always of the highest
quality.
Better Health Reducing the generators of ill health by encouraging healthy behaviors and decreasing the likelihood of illness through focused prevention and the development of increased
resilience.
Lower Cost
Creating value by focusing on quality, eliminating waste, and
reducing unwarranted variation; considering the total cost of care over time, not just the cost of an individual health
care activity.
8

Mission of DHA Pharmacy Operations
“Innovatively manage and standardize the DoD pharmacy benefit in a fiscally
responsible manner to optimize readiness, improve health, and lower costs through
better care”

DHA Pharmacy Operations
Discussion Today: A Brief Look at Pharmacy Spending
Transition Initiatives
Opioid Management
Expanded Formulary Management
Questions
4

Current MHS Outpatient Drug Spend & Offsets (Without Offsets, Drug Spend ~ $2.0B more per year)
$629 $718 $862 $954 $1,046 $1,240 $1,465 $1,787 $2,009 $2,242
$2,852 $3,257
$3,764
$1,615 $1,536 $1,461 $1,407 $1,430 $1,457
$1,498 $1,560
$1,504 $1,569
$1,649
$1,654
$1,762
$3,156
$3,904
$4,182 $4,218
$3,909 $3,844
$3,997 $3,673 $3,365 $3,413
$3,078 $2,317 $2,014
$8 $6 $8
$16 $23
$36 $23 $36
$512
$1,602
$49 $49
$388
$461 $504 $530
$549 $555
$525 $586 $544
$603
$572
$553 $507
$217 $328 $436
$459
$527 $593 $670
$742
$788
$794 $679
$29
$832 $1,137 $1,402
$1,566 $1,449 $1,385
$1,191
$1,067
$881 $840
$0
$1,000
$2,000
$3,000
$4,000
$5,000
$6,000
$7,000
$8,000
$9,000
$10,000
$11,000
$12,000
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
Millio
ns
Retail Refund
OHI
Copay
Compounds
Retail less Compounds
MTFs
$5,794
$6,627
$7,264
$8,281 $8,523
$8,980
$9,614 $9,740
Cost Offsets
Source: Pharmacy Data Transaction Service (PDTS) Data Warehouse; DHA Pharmacy Operations Division (POD) (refunds). Note: 1. Net cost to DoD represents total prescription expenditures minus copays, coverage by other health insurance (OHI), and retail refunds invoiced. 2. Mail Order dispensing fees are included; however, other retail/mail contract costs and MTF cost of dispensing are not included. 3. Retail Refunds are reported on an accrual rather than a cash basis, corresponding to the original prescription claim data & updated refund adjustments. 4. Retail Compound spend, broken out separately, is not adjusted for any recoveries or settlements with compound pharmacies outside of claims reversals
$9,738
$10,272
$11,608
$9,505 $9,615
DoD Net
Costs
Cost Offsets

Defense Health Agency Transition
• Section 702 of the National Defense Authorization Act (NDAA) for 2017 requires that by 1 Oct 2018 the Defense Health Agency (DHA) will assume responsibility for the administration of all MTFs including: • Budget, IT, health care administration and management, policy and procedures,
and medical facility construction
• Readiness is a shared responsibility; DHA supports the Services and Combatant Commands
• Health Affairs, DHA, and Services are working actions to meet Section 702 requirements
• Current Pharmacy Working Group is developing pharmacy-specific solutions for the way ahead

• Implement and Standardize Policies, Procedures, and Models
Goal: Standardize administration of MTFs through the creation of standardized DHA policies.
Rationale: Transform varied Pharmacy operations across the Services into a single, integrated DHA Pharmacy program that standardizes business processes and optimizes pharmacy operations at each MTF.
• Execute Robust and Comprehensive Formulary Management
Goal: Identify and implement best practices for an Enterprise-wide drug formulary
Rationale: Supports readiness, increases cost savings, reduces variance, and improves patient outcomes across each MTF.
• Innovate, Standardize, and Optimize the Pharmacy Experience
Goal: Leverage best practices from within DoD, other Government agencies, and the private sector to improve health outcomes, implement operational efficiencies, and improve the patient experience at all points of service (POS). Fully utilize Pharmacist Clinical Services and integrate MHS GENESIS capabilities to improve patient outcomes.
Rationale: Utilize standardized processes and procedures, increase efficiency in operations, decrease variability in patient care, and improve patient health outcomes
Enterprise Pharmacy Operations Transition Improvement Initiatives

MHS Pain Management and Opioid Reduction Initiatives
“Medically Ready Force…Ready Medical Force” 8
Align DHA Pharmacy with Civilian Standard of Care Develop Prescription Drug Monitoring Program
(PDMP) for bidirectional transparency between DoD controlled substance utilization data and state(s)
Standardize Naloxone prescribing for at risk patients Mirror best industry practice
Continuous MTF Drug Take-back Programs

Prescription Drug Monitoring Program
High degree of Congressional interest currently MTF controlled substance prescription data is not
pushed to state PDMPs, however… Controlled substance prescriptions filled through the
mail or retail venues are reported to state PDMPs MTF providers can see all controlled substance
prescriptions for a patient except if the patient paid cash for a prescription
Operational Security (OPSEC) concerns if data is automatically pushed to all 50+ states

Prescription Drug Monitoring Program
DHA workgroup formed in September 2017 comprised of Pharmacy Operations Division and Health IT Tasked to develop a secure solution for bi-directional sharing (view) of controlled Rx data between MTFs and state PDMPs
Secure Solution Option Create segregated smaller controlled substance database to interface with state PDMPs via portal/hub Available hubs allow providers from one state to view Rx data for patients filling controlled Rxs in another state
U.S. Bureau of Justice Assistance, RxCheck National Assn. of Boards of Pharmacy, InterConnect and Gateway

DoD Tools to Decrease Opioid Use
“Medically Ready Force…Ready Medical Force”
NDAA 18 Copay and Tiers 1 and 4 Changes
“Medically Ready Force…Ready Medical Force” 10
FY18 NDAA creates Tier 4 Allows for exclusion of drugs from benefit
Move select brand name drugs to Tier 1
Evaluate additional discounts with branded pharmaceuticals
Implemented new cost-sharing modifications (copays) on 1 FEB 2018
Value Based Medication Adherence Pilot
11
Determine if lowering copays increases patient medication compliance Pilot began 1 FEB 2018 Two high-impact chronic medications
Oral cholesterol/lipid lowering statin (rosuvastatin) Injectable prefilled insulin pen (Lantus®)
Typical value based incentives increase adherence 2-4% based on $5-10 copay decrease Current MHS adherence rates for Statins is 79% & Antidiabetics is 78% Measure adherence Rates (proportion days covered, refill intensity) For statin, difference in adherence with statins not selected HgA1C Lipid Profiles

“Medically Ready Force…Ready Medical Force” 10
Thank You for Your Time and Attention
Questions???
David W. Bobb, RPh, JD Chief, Pharmacy Operations Division
Defense Health Agency Email: [email protected]
Phone: 703-681-2890

DOD/VA Shared Services
Coalition for Government Procurement Fourth Annual Healthcare Forum
Daniel Keefe and Jody Goldsmith
April 11, 2018
Agenda
• Medical Supply Chain Overview
• Medical/Surgical Prime Vendor Program
• ECAT (Electronic Catalog) Program
• Category Management Initiatives
• Agency Collaboration
2
Every Day Every Crisis
Vision: To provide an integrated and responsive system of choice for delivering consistent, quality medical materiel support for health care providers to perform
their patient care mission
Our Dual Focus
• Ready on day one
• Varied missions & requirements
• Resupply & sustainment
• Control commercial/industrial materiel
• Situational awareness
• Health care economics
• The business of health care
• The cost of medical materiel
• Reliable “next day” support
• Business intelligence
Institutional Operational
3

How DLA Medical Works
• End-to-End, integrated supply chain; from manufacturers to customers
– Just in time support model; providing access to 1.4M medical items
– Electronic interface with DoD customers via: DMLSS (Defense Medical Logistics Standard Support System) TEWLS (Theater Enterprise-Wide Logistics System)
• Extensive use of E-Commerce; satisfies 85% of customer demands utilizing:
– Prime Vendor Programs for Pharmaceuticals and Medical/Surgical items
– Electronic Catalog System for Lab, Optical, Dental, Implants and Equipment
• Readiness Support; Buy access to contingency requirements vice purchase
– CEC (Corporate Exigency Contracts)
– PVWRM (Prime Vendor War Readiness Material)
• Traditional Support; Procurement method of last resort - Includes bulk purchase / depot stocking and manual small purchases
4

Class VIII – Medical
Customers & Items Sales
Inventory Personnel & Vendors
The Big Picture
$5.1 $5.6 $6.3 $6.7 $7.0
0
2
4
6
8
FY13 FY14 FY15 FY16 FY17
Customers: 6,100
Orders: 9.3M annually
Items: 1,414,000
Employees (FY17 Actual):
284 civilian + 11 military
Suppliers: 1,018
$Billions
$120
$88 $82 $105
$92
0
50
100
150
FY13 FY14 FY15 FY16 FY17
$Millions
FY18 Forecast
$7.106B
5

Army
$1.7B
DHA
Order
Pharmac
y $2.8B
Air
Force
$1.0B
Navy
$785M Marine
Corps
$30M Other
$621M
Pharm PV
$4.9B
Med/Surg PV
$614M
Capital
Equipment
$395M
Traditional
Med/Surg
$207M
Traditional
Pharm $380M
ECAT $251M
Hospital
$147M
Medical Business FY 2017
FY17 actual $7.0B
FY18 Forecast $7.106B
6
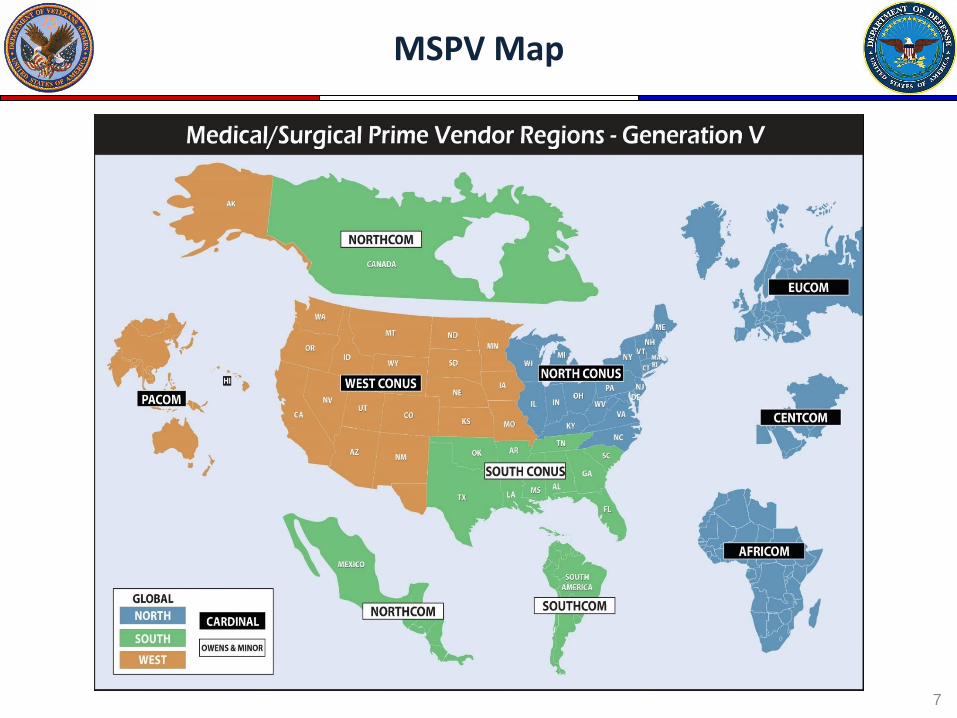
MSPV Map
7

MSPV Product Scope
• Allowable products include: - Medical/Surgical Consumables - Custom Pre-Packs - Low-level Medical Equipment not currently covered by DLA’s ECAT contracts
• MSPV medical products are defined as those used to examine or treat patients, and do not include pharmaceuticals or high-end medical equipment
• Product examples include sutures, bandages, syringes, linens, gowns, stethoscopes, etc…
• Custom Pre-Packs are “Prepackaged” Medical Supplies containing all physician/surgeon selected supplies used to perform a specific medical procedure or operation
8

All Products are priced via Distribution and Pricing Agreements (DAPAs) which must be approved by a DLA Contracting Officer
There are approximately 700 DAPAs with over 340,000 priced items
DAPA Types include:
• Traditional DAPAs Manufacturers/Suppliers: Independent Product Prices
• Incentive Agreement Prices DAPA Discounts resulting from Product Standardization Actions of the DoD Medical Materiel Enterprise Standardization Offices (MMESO)
• PV Branded DAPAs PV’s own brand-name/private-label product lines
Customer Price = DAPA + PV Distribution Fee + DLA Cost Recovery Factor
GEN V Product Pricing MSPV Product Scope cont.
9

• A DAPA is an agreement: - Between a manufacturer/supplier and DLA Troop Support - Which establishes the product selling price - Which establishes the authority allowing PVs to distribute a DAPA-Holder’s products to military and other federal customers
• DAPAs are not contracts and can be dissolved with 30 days notice from either party (DAPA Holder or Government)
• DAPAs are base uncommitted pricing agreements - There is no commitment from the Government to purchase an item just because a DAPA has been established
• DAPA prices are not fixed for an indefinite period - DAPA Holders may request price changes at any time - Approved requests are effective 1st day of following month
Distribution and Pricing Agreement Overview (What is a DAPA?)
10
• Medical/Surgical consumable products only
• Medical products used to examine or treat patients
• Does not include pharmaceuticals or medical equipment
• Product examples… sutures, bandages, syringes, surgical devices, patient gowns, stethoscopes
Med/Surg DAPA Products
11

Step 2: Establish a Distribution Agreement with PVs
Step 3: Obtain Product Liability Insurance
Step 4: Marketing DAPA Products Note: DAPA holders are solely responsible for creating demand for their products through customer-focused marketing efforts
Obtaining a DAPA is only Step One!
12

A Guide to Applying for your DAPA is available on Medical’s website:
www.medical.dla.mil
13
DAPA Management System (DMS)
14

New User Registration
15

If you are interested in establishing a Medical/Surgical DAPA please visit…
www.medical.dla.mil
Or contact us:
Tom Drew DAPA Manager 215-737-2834 [email protected]
Meghan Landry DAPA PCO 215-737-2127 [email protected]
DAPA Team Points of Contact
16
Steve Bollendorf
Medical Surgical Prime Vendor Program Manager
Phone: 215-737-2665
E-mail: [email protected]
Maryann DiMeo
Chief, Medical Surgical Prime Vendor Contracting IST
Phone: 215-737-3201
E-mail: [email protected]
Tom Drew Chief, Med/Surg DAPA Product Support IST Phone: 215-737-2834 E-Mail: [email protected]
MSPV Management Team MSPV Management Team
17
ECAT Agenda
• ECAT Overview
• Program Features
• Customer & Supplier Benefits
• Program Growth
• Customer Satisfaction
• Wrap Up
• Questions?
18

ECAT Overview
• ECAT – An internet solution that uses the latest Electronic Commerce technology for Ordering, Receiving, Management, and Bill Payment of Medical Devices and Supplies
• Provides commodity support for items not available through Med/Surg and Pharmaceutical Prime Vendors
• Emulates Best Commercial Business Practices
• Web-Based Ordering
19

Program Features
• Multiple Catalog Ordering (FAR Part 8)
– Online Comparison Shopping for Best Value – Customer Selects Product and Vendor
• Price • Delivery • Past Performance • Small Business Considerations, etc.
• Suppliers Deliver Direct to Customer • Potential Five (5) Year Contracts
20

Customer & Supplier Benefits
• Customer Benefits
– Stable pricing for all customers based on usage
– B2B e-Business Operating System Interface
– Electronic Commerce solution to local manual purchase
– Robust Search Engines
• Supplier Benefits
– One focal point for contract administration
– 15-Day Payment after Receipt or Invoice
– Paperless Operation = Reduced Administrative Costs
– Electronic Published Catalog Pricing
– Available to all Federal Agencies (DoD, IHS, NIH etc.)
– No Vendor Fee to use ECAT
21

FY17 ECAT Sales by Program
[CATEGORY NAME], [VALUE]
[CATEGORY NAME], [VALUE]
[CATEGORY NAME], [VALUE]
[CATEGORY NAME], [VALUE]
[CATEGORY NAME], [VALUE]
[CATEGORY NAME], [VALUE]
[CATEGORY NAME], [VALUE]
[CATEGORY NAME],
[VALUE]
[CATEGORY NAME], [VALUE]
22

Current Solicitations
• Open Season Solicitations: – The following solicitations are available on the DLA Internet Bid Board
System (DIBBS): https://www.dibbs.bsm.dla.mil
• LAB: SPE2DE-17-R-0001 • DENTAL: SPE2DE-16-R-0004 • OPTICAL: SPM2DE-14-R-0001 (LENSES)
SPM2DE-14-R-0003 (FRAMES) • EQUIPMENT: SPE2DH-16-R-0002
POC: Lab, Dental, Optical Eileen Motta 215-737-3262,[email protected] Equipment: Robert Zalewski 215-737-8712 [email protected]
23
Agency Collaboration (1 of 2)
Eight FY18 Initiatives Potential Effects
1. Identify managed and unmanaged spend within the Health Services Subcategory
2. Expand use of Pharmaceutical Prime Vendor Programs
3. Continue expansion of ECAT (HHS, and BoP)
4. Comprehensive Purchase Card Review to Identify Managed Spend and move towards contracts
1. Q-services could ultimately be standardized and ordered from a platform similar to formulary/catalog
2. More cost avoidance in pharmaceuticals for everyone
3. Could become the Gold Standard of catalogs and considered a best practice
4. Could identify items that need to be added to a catalog and develop joint contracting vehicles with all agencies
24

Agency Collaboration (2 of 2)
Eight FY18 Initiatives Potential Effects
5. Develop replicable demand management strategies for Healthcare Services
6. Leverage medical supply formulary management
7. Develop Online Pricing Portals for price comparison tools
8. Track Small Business Improvement in Health Service Subcategory
5. Decrease the need for HCS contracts, establish locum tenens relationships better than personal services contracts
6. Maximize vendor participation on catalog vehicles towards CA
7. Help identify best prices throughout federal government to be leveraged in vendor negotiations
8. Maximize small business goals
25

Agency Collaboration
• Best In Class (BIC) Vehicles – Joint National Pharmaceuticals
– Hearing Aids
– High Tech Medical Equipment
• Strategic Sourcing – OMB pushing agencies to utilize BICs by requiring exception memorandums
– VA Implementation of ECAT is potential BIC candidate
– DOD/VA developing potential BIC candidate for Healthcare Services
– Congress is pushing towards procurement consolidation (NDAA, GWCM, etc)
26

Questions?
27

U.S. General Services Administration OFFICE OF INFORMATION TECHNOLOGY CATEGORY
www.gsa.gov/itc 1
Health IT Solutions CGP Fourth Annual
Healthcare Forum

www.gsa.gov/itc 2
OFFICE OF INFORMATION TECHNOLOGY CATEGORY
U.S. General Services Administration
John Tenaglia Acting Component Acquisition
Executive and Head of the Contract Activity
Defence Health Agency
Keith Nakasone Deputy Assistant Commissioner,
IT Acquisition Office of Information
Technology Category, GSA
www.gsa.gov/itc 3
OFFICE OF INFORMATION TECHNOLOGY CATEGORY
GSA and DHA Collaboration
U.S. General Services Administration

www.gsa.gov/itc 4
OFFICE OF INFORMATION TECHNOLOGY CATEGORY
Health IT SIN Spend Forecast
U.S. General Services Administration

www.gsa.gov/itc 5
OFFICE OF INFORMATION TECHNOLOGY CATEGORY
Where to Learn More
Acquisition Gateway
hallways.cap.gsa.gov
IT Customer Services Center
Call us at 855-ITaid4u
Sun. 8:00 p.m. to Fri. 8:30 p.m.
GSA Interact
interact.gsa.gov
U.S. General Services Administration

OFFICE OF INFORMATION TECHNOLOGY CATEGORY
U.S. General Services Administration

Slide
Forum Sponsor

Slide
Keystone Members

Slide
Executive Members

MSPV-NG, Formulary, and More – Rick Lemmon & Jaime Friedel


















