
Four Paradigms of Recovery A Criterion Counseling Model for Successfully Overcoming Addiction H....
96
Four Paradigms of Recovery A Criterion Counseling Model for Successfully Overcoming Addiction H. Gray Otis, PhD, CMHC, DCMHS-T Clinical Director, The Phoenix Recovery Center [email protected] www.ThePhoenixRC.com 801-885-8585
-
Upload
maximillian-barton -
Category
Documents
-
view
214 -
download
0
Transcript of Four Paradigms of Recovery A Criterion Counseling Model for Successfully Overcoming Addiction H....
Four Paradigms of Recovery A Criterion Counseling Model for Successfully Overcoming Addiction
H. Gray Otis, PhD, CMHC, DCMHS-TClinical Director, The Phoenix Recovery Center
www.ThePhoenixRC.com
801-885-8585

Copyright H. Gray Otis, PhD, CMHC, 2013
Clinical Director, Clinical Mental Health Specialist - Trauma
The Phoenix Recovery Center
Residential recovery treatment for men & women
The Phoenix Counseling Center
Intensive outpatient recovery treatment
General outpatient – adults, couples, families
Professional Background

Copyright H. Gray Otis, PhD, CMHC, 2013
How do we assess successful recovery?
We know the criteria in order to diagnose substance dependence
Do we know what recovery is? What are the criteria?
What does “dual diagnosis” recovery mean?
Can we define behavioral health by the absence of symptoms?
Genesis

Copyright H. Gray Otis, PhD, CMHC, 2013
My clinical concentration is on abstinence but there are other options Focus of treatment
Addiction recovery Trauma & chronic distress resolution Health and strength development
Medications alleviate symptoms – but – do not resolve underlying causal factors
Substance dependence is a biological disease with underlying psychological origins – thus – dual diagnosis
Bias – Up Front Presumptions

Copyright H. Gray Otis, PhD, CMHC, 2013
Recovery Perspective
Treat the Addictions• Consider the symptoms of addictions – substance & behavioral• Could an addiction be symptomatic?
Treat the Underlying Causal Factors• Understand the unseen factors that created the addiction• These are often based in trauma or chronic distress
Encourage health & strength development

Copyright H. Gray Otis, PhD, CMHC, 2013
RESEARCHWhat are the percentage of clients that as teens experimented with drugs or alcohol and then got hooked?
Is this primary basis that explains why they became addicted?
Does the public believe that drug experimentation is the reason teens become addicted?

Copyright H. Gray Otis, PhD, CMHC, 2013
CURRENT RESEARCHWhat are the percentage of clients that as teens experimented with drugs or alcohol and then got hooked?
Is this primary basis that they became addicted?
Does the public believe that drug experimentation is the reason teens become addicted?
Current research addiction is based on:
1. Exposure
2. Vulnerability of the individual – genetic predisposition, past distress
3. Current situation of the individual – present distress

Copyright H. Gray Otis, PhD, CMHC, 2013
Factors of Psychological Health
Those who are generally healthy have:1. Positive Self-beliefs
2. An Internal Sense of:
• Emotional self-regulation
• Nurturing self-care
3. Effective Interpersonal Relationships
4. Perspective of Purpose and Meaning

Copyright H. Gray Otis, PhD, CMHC, 2013
Those in long-term recovery exhibit:1. Positive Self-beliefs
Believe
2. An Internal Sense of:Understand
• Emotional self-regulation
• Nurturing self-care
3. Effective Interpersonal Relationships Connect
4. Perspective of Purpose and Meaning Imagineer
Four Paradigms of Recovery
Copyright H. Gray Otis, PhD, CMHC, 2013
Believe – Understand – Connect – Imagineer
The Four Paradigms of Recovery serve as a model to
integrate clients’ positive experiences which they had before their addiction with
current constructive recovery experiences.
This model correlates with Twelve Step principles.
Synopsis

BelieveOur Self-Beliefs Govern Life Choices & Outcomes

Copyright H. Gray Otis, PhD, CMHC, 2013
“I am unworthy to be loved”
Virtually everyone in initial recovery does not accept that they are worthy of being loved .
In many cases, this is the underlying reason for their dependence.
BELIEVE

Copyright H. Gray Otis, PhD, CMHC, 2013
“I am unworthy to be loved”
Virtually everyone in initial recovery does not accept that they are worthy of being loved .
In many cases, this is the underlying reason for their dependence.
Substance or Behavioral Dependence
Shame Self-Beliefs
BELIEVE

Copyright H. Gray Otis, PhD, CMHC, 2013
DEFINING SELF-BELIEFSM
ore than persistent personality traits
How the person experiences self - for exam
ple;
You alone see through your eyes and only you interpret w
hat you perceive
No one w
ill ever experience what
you have – your unique com
bination of experiences
You daily construct your own
unique world
This always links to w
hat you believe about your self
Our self-beliefs essentially shape who we are

Copyright H. Gray Otis, PhD, CMHC, 2013
Individuals fall into one of two groups
Those individuals who deeply
believe:
“I am unw
orthy to be loved”
‘I am not enough and never will be.’
‘I am asham
ed of myself’
‘I cannot stand who I am so I num
b m
yself with food, addictions, ‘right’ thinking, m
eds, anger, etc.
How
does this correlate with those
who suffer from
substance addiction?
RESILIENCE RESEARCH

Copyright H. Gray Otis, PhD, CMHC, 2013
Other Shame Self-BeliefsI don’t deserve love
I am a bad
I am worthless
I deserve bad things
I am damaged, broken
I am ugly
I am stupid, not smart enough
I don’t matter
I don’t belong, I am different
I am irresponsible
I cannot be trusted, trust myself
I cannot trust others
I am weak, not in control
I am a failure
I am imperfect, flawed, I must please

Copyright H. Gray Otis, PhD, CMHC, 2013
UNDERSTANDING SHAME•
Shame self-beliefs distort and
disfigure how individuals
perceive themselves.
•Evidence is accum
ulated that
the shame beliefs are true
•The psychic pain of sham
e
dominates consciously and
subconsciously e.g.
destructively disparaging self-
talk
Shame is the petri dish in
which the bacteria of
addiction thrive

Copyright H. Gray Otis, PhD, CMHC, 2013
Distinguishing between guilt and shame
Guilt:
“I did something wrong or bad,” “I did something dumb,” “I acted carelessly,” etc.
Guilt motivates us to change
SHAME SELF-BELIEF QUALITIES

Copyright H. Gray Otis, PhD, CMHC, 2013
Distinguishing between guilt and shame
Guilt:
“I did something wrong or bad,” “I did something dumb,” “I acted carelessly,” etc.
Guilt motivates us to change
Shame:
“There is something wrong with me – I am bad,” “I am dumb,” “I am careless,” etc.
Shame beliefs lead us to accept the lie that we cannot change
SHAME SELF-BELIEF QUALITIES

Copyright H. Gray Otis, PhD, CMHC, 2013
Distinguishing between guilt and shame
Guilt:
“I did something wrong or bad,” “I did something dumb,” “I acted carelessly,” etc.
Guilt motivates us to change
Shame:
“There is something wrong with me – I am bad,” “I am dumb,” “I am careless,” etc.
Shame beliefs lead us to accept the lie that we cannot change
Counselors must be skilled in shame resolution
SHAME SELF-BELIEF QUALITIES
Copyright H. Gray Otis, PhD, CMHC, 2013
THE SELF-BELIEF CONTINUUM Fear/Sham
e
Love/Empathy
1 2 3
4 5 6
7
On a scale from
1 to 7, how much
of the individual’s life is
lived with love and empathy?
Low scores correlates with shame
self-beliefs & addictions

Copyright H. Gray Otis, PhD, CMHC, 2013
ORIGINS OF SHAME SELF-BELIEFShame self-belief arises from emotionally charged events (trauma) as well as other disturbing experiences (small t trauma, chronic distress, developmental trauma)
The individual lives with distress such as a loss of attachment, fear for the safety of self or others, chronic low-grade anxieties, cultural conflicts, feelings of inadequacy, etc.
There is often a sense of terrible helplessness
These deep seated emotions may be manifested in almost any DSM disorder and all substance dependence disorders
In order to blunt the high level of fear & shame, individuals use coping mechanisms that provide instant, temporary relief – most commonly substance or behavioral addictions

Copyright H. Gray Otis, PhD, CMHC, 2013
SHAME SELF-BELIEF RESULTSShame self-belief induces negative coping mechanisms
In addition to drugs and alcohol, individuals may turn to sex, gambling, working, religion, blaming, exercise, politics, eating disorders, or any other addiction patterned behaviors
Shame Self-Beliefs most often lie in the subconscious
Self-beliefs trump everything else mentally & emotionally – they color are decision making
We must go beyond cognitive-behavioral therapy
’Counselors can create the pre-conditions for transforming Shame Self-Beliefs into Positive Self-Beliefs

Copyright H. Gray Otis, PhD, CMHC, 2013
The second of the two groups :
Those individuals who
predominantly believe:
“I am w
orthy to be loved”
How many individuals with
addictions have this self-belief?
What can w
e learn from this?
POSITIVE SELF-BELIEFS
Copyright H. Gray Otis, PhD, CMHC, 2013
Counselors need an evidenced-based m
odel to understand the underlying basis of m
ental disorders including substance dependence:
“Client sham
e self-beliefs relate to attachm
ent, abandonm
ent, and trauma”
Shame Self-beliefs can be
transformed into Positive
Self-beliefs
Outcom
e research shows that addressing underlying sham
e is a critical aspect dependence recovery.
THE TRANSFORMATIONAL APPROACH

Copyright H. Gray Otis, PhD, CMHC, 2013
“I am evil”“I am acceptable!”
Shame self-belief example:
‘I am evil’ replaced with:
What are the chances for his recovery?
TRANSFORMATIONAL SELF-BELIEFS

Copyright H. Gray Otis, PhD, CMHC, 2013
TRANSFORMATIONAL APPROACHShow clients how to transform ‘Shame Self-Beliefs’
1. Develop Client Emotional Regulation
2. Treat Trauma
3. Promote Positive Self-Beliefs
4. Support Forgiveness, No Use of Labels, Self-Change, Addiction Recovery
Which comes first?

Copyright H. Gray Otis, PhD, CMHC, 2013
THERAPEUTIC CONSIDERATIONSSeek out shame beliefs:
“What are you ashamed of?” “What traumatic or chronic distress experiences have you had?” (e.g. abuse,
accidents, injuries, combat, learning difficulties, bullying, alcoholic caregiver, etc.) “What negative beliefs do you have about yourself starting with the words; ‘I am. . .’?
(e.g. “I am unsafe,” “I’m stupid,” “I am out of control,” I’m a terrible parent,” etc.)
Distinguish for the client the difference between guilt and shame
Help clients transform shame self-beliefs into positive self-beliefs – Brene Brown (TED Talk - Vulnerability, etc.)

Copyright H. Gray Otis, PhD, CMHC, 2013
TREAT TRAUMA & CHRONIC DISTRESS
Trauma & attachment are at the center of shame self-belief - understand GAD, PTSD, small t trauma, mTBI, developmental trauma
Know how to help client’s effectively process trauma – evidenced based optionsBody workEMDRSand tray, play therapyThought Field Therapy, Acupressure Tapping, (Instant Emotional Healing, Lambrou & Pratt), Affirmations Cognitive Processing TherapyTrauma Focused CBTStress Inoculation TherapyOthers?
Ethical responsibility to effectively treat or to refer
Copyright H. Gray Otis, PhD, CMHC, 2013
EFFECTIVE TREATMENTResults – positive self-beliefs become dominant
1. Individuals convert shame self-beliefs to positive self-beliefs and they know it
2. Triggers are no longer experienced
3. The shame experiences are integrated in memory
4. The results are permanent
The impact of life-threatening industrial accident on Nate
Chronic distress or trauma is more difficult for many clients to resolve – Belinda’s story

Copyright H. Gray Otis, PhD, CMHC, 2013
STRENGTHENING SELFPracticed 12-15 times a day for 7 weeks
Positive Self-Belief elements:
1. Strong positive emotional memory visualization
2. Body memory sensation
3. Belief: “I am worthy to be loved!”
4. Finger to thumb connection
Demonstrated by the counselor – five iterations
Client logging method
Client preparation: “The toughest experiment you will ever do”
Client reports back at the next session

Copyright H. Gray Otis, PhD, CMHC, 2013
OUTCOMES OF POSITIVE BELIEF Alleviation of root source of substance dependence
Enhanced emotional resilience
Better physical well-being
Improved relationships
Increased appreciation, enjoyment, & meaning
Lasting recovery outcomes

Understand• Emotional self-regulation
• Nurturing self-care
Copyright H. Gray Otis, PhD, CMHC, 2013
EMOTIONAL SELF-REGULATIONVirtually all people afflicted with dependence have used substances and behaviors to numb out painful emotionsWithdrawal usually brings an immense increased of often overwhelming
emotions and feelings
Most do not have a vocabulary to describe what they are experiencing
They feel flooded with unwanted emotional pain
“We are swimming in a sea of our own emotions”

Copyright H. Gray Otis, PhD, CMHC, 2013
THERAPEUTIC CONSIDERATIONSTeach an easy-to-understand emotional vocabulary
Distinguish between secondary emotions (e.g. “I am mad”) from primary
feelings (e.g. I feel Accused, Guilty, Rejected, Unlovable, and/or Powerless)
so that the client can identify and discuss their emotions and feelings
Focus on their emotional experience (e.g. What emotions are you
experiencing now. What are your feelings?)

Copyright H. Gray Otis, PhD, CMHC, 2013
DEVELOP EMOTIONAL REGULATION
I am Mad – Sad - AnxiousI feel:• Accused • Guilty• Rejected • Unlovable• Powerless
“When I am out of WAC – I feel AGRUP” “However, I can regulate how I feel”
I am GladI feel:• Worthy• Acceptable• Capable
Help clients understand their emotions and feelings:
Fear/Shame Love/Empathy 1 2 3 4 5 6 7

Copyright H. Gray Otis, PhD, CMHC, 2013
THERAPEUTIC CONSIDERATIONSHelp them learn principles of emotional intelligence particularly how to
regulate their emotions.
Clients rarely know how to perceive the balance that is needed for recovery?
They seldom recognize how the 12 Steps integrate the key elements of
successful living.
Help them daily review their well-being.

Understand• Emotional self-regulation
• Nurturing self-care

Copyright H. Gray Otis, PhD, CMHC, 2013
NURTURING SELF-CARE
Clients hardly ever know how to perceive the balance needed for recovery
They seldom recognize how the 12 Steps integrate the key elements of
successful living
Help them daily review their well-being.

Copyright H. Gray Otis, PhD, CMHC, 2013
THERAPEUTIC CONSIDERATIONSA new approach to a greeting
Instead of; “Hi, how are you?”

Copyright H. Gray Otis, PhD, CMHC, 2013
THERAPEUTIC CONSIDERATIONSA new approach to a greeting
Instead of; “Hi, how are you?”
How goes your H E A R T? How is your Health? How are your Emotions? How is your Awareness? How are your Relationships? How is your Transcendent spirituality

Copyright H. Gray Otis, PhD, CMHC, 2013
HEALTHHow is your Health?
Sleep 7 to 8 hours Eat well Drink enough water Exercise regularly * Take care of health needs
Nurture your well-being Stop smoking * Take a supplement if needed Limit caffeine, sodas, & sugar
Which of these lower the risk for relapse?Which of these are you modeling for your clients?

Copyright H. Gray Otis, PhD, CMHC, 2013
EMOTIONSHow are your Emotions?
Recognize emotions & feelings
Regulate & soothe yourself
Appreciate positive feelings
Practice appreciating
Understand yourself
Use empathy to understand others
Emotional mindfulness is prerequisite to emotional intelligence We cannot control emotions but we can regulate them & soothe ourselves

Copyright H. Gray Otis, PhD, CMHC, 2013
AWARENESSHow is your Awareness?
Know what you are focusing on
Use your mind to resolve shame
Work through guilt
Value the worth of others & self
Realize that you are becoming more
Worthy, Acceptable, and Capable
Cognitive awareness is central to reason, logic, and effective actionThe ability to focus our mind changes our brain

Copyright H. Gray Otis, PhD, CMHC, 2013
RELATIONSHIPSHow are your Relationships? Clean up your side of the street
(& only your side)
Work through resentments
Practice forgiveness
Support the “Five Positives to One
Negative Interactions”
Sit as an adult not as a parent or
child
Know your family constellationsAlmost every person with an addiction as been the ‘victim’ of othersContinuing to blame is almost a sure sign of relapse – How come?

Copyright H. Gray Otis, PhD, CMHC, 2013
TRANSCENDENT SPIRITUALITYHow is your Transcendent Spirituality?
Find the joy in enjoyment and the
heart of courage in encouragement
Become open to ‘Coincidences’
How many of your clients have ‘religion problems’Many have not understood their spiritual experiences
(e.g. nature, caring, connection, wonder, etc.)
Develop your own sense of the
spiritual
Tap into the energy of your higher
power
Copyright H. Gray Otis, PhD, CMHC, 2013
SELF-CARE
The Self-care Imperative for RecoveryRecovery is not a simplistic formula
However, there are factors that greatly decrease risk factors
Most clients do not understand these concepts on first hearing
Seeking a balance in
health, emotions, awareness, relationships, and spirituality
is an ongoing, life-long journey

Factoids

Copyright H. Gray Otis, PhD, CMHC, 2013
What is the new pain med that will hit the streets next month?
Additional Job Security

Copyright H. Gray Otis, PhD, CMHC, 2013
What is the new pain med that will hit the streets next month? FDA approved in record time FDA advisory panel voted 11 to 2 against approval Alleviates chronic pain Better than Hydrocodone 5 – 10 mg
Additional Job Security

Copyright H. Gray Otis, PhD, CMHC, 2013
What is the new pain med that will hit the streets next month? FDA approved in record time FDA advisory panel voted 11 to 2 against approval Alleviates chronic pain Better than Hydrocodone 5 – 10 mg
Here comes Zohydro ER 50 mg
Additional Job Security

Copyright H. Gray Otis, PhD, CMHC, 2013
LIMITATIONS
“Because of the risks of addiction, abuse, and misuse with opioids,
even at recommended doses, and because of the greater risks of
overdose and death with extended-release opioid formulations, reserve
Zohydro ER for use in patients for whom alternative treatment options
are ineffective, not tolerated, or would be otherwise inadequate”

Copyright H. Gray Otis, PhD, CMHC, 2013
COUNTER POINT
We need effective pain medications
Physicians must assess for risks1. Exposure
2. Vulnerability of the individual
3. Current situation of the individual
There usually are options for those at risk of dependency

Factoids
Copyright H. Gray Otis, PhD, CMHC, 2013
Best predictor of successful therapy outcomes?
Considerations
Copyright H. Gray Otis, PhD, CMHC, 2013
Best predictor of successful therapy outcomes?
Counselors who ask their clients how they can be more effective.
Considerations

ConnectIsolation is the common thread in substance or behavioral addictions
Copyright H. Gray Otis, PhD, CMHC, 2013
PROBLEMATIC RELATIONSHIPS
They have poor relational conceptualizations
Expectations are high & acceptance is low
There is little ‘friendship’ in their relationships

Copyright H. Gray Otis, PhD, CMHC, 2013
THE POWER OF FRIENDSHIP
When individuals rediscover how to be friends:
Relationships start to heal & then flourish
The pieces fit
How does this happen?
Copyright H. Gray Otis, PhD, CMHC, 2013
Every friendship is composed of two separate relationships.
For example;
I have a relationship with Mark, my colleague at work
But Mark has a different perspective about his relationship with me
THERAPEUTIC CONSIDERATIONS

Copyright H. Gray Otis, PhD, CMHC, 2013
RECALL A CLOSE FRIENDExamples, a grandparent, a favorite friend growing up, a current BFF,
anyone you felt very close to (but not your spouse)
Think about how well you related to this friend
Then estimate how well they related to you
There are five qualities of interactions which summarize the closeness &
the effectiveness of the relationship between any two people. They are:

Copyright H. Gray Otis, PhD, CMHC, 2013
G R E A T FRIENDSHIPSAsk: Am I really . . .
• Genuine? Do I demonstrate that I am genuine by being honest, sincere, open, truth full, & transparent so
that others can be at ease with me?
• Respectful? Do I respect the ability of every adult to make their own choices even when I disagree? Do I
allow them to be responsible for the results of their decisions?
• Empathetic? Do I express through empathy that I care enough to listen, understand, and want the best for
the other person? Do I understand what others are saying, their feelings, their fears & their caring love?
• Accepting? Do I fully accept the other person as they are. Even when I disagree with them, can I express
my thoughts without ‘constructive criticism’ or imposing my values and expectations on them?
• Trustful? Do I believe in the basic good-hearted nature of the other person by acknowledging the best
about them? Am I trustful of their intentions?
Copyright H. Gray Otis, PhD, CMHC, 2013
AM I GENUINE?Do I demonstrate that I am genuine by being honest, sincere, open, truth
full, & transparent so that others can be at ease with me?
‘Are you honest, truthful, and open with your friend?’
‘Is it easy to be sincerely yourself?’
‘How do you encourage your friend to be comfortable with you?’
‘Does this work for both you and your friend?’

Copyright H. Gray Otis, PhD, CMHC, 2013
AM I RESPECTFUL?Do I respect the ability of every adult to make their own choices even when I
disagree? Do I allow them to be responsible for the results of their decisions?
‘Do you consent that your friend has the right to make their own decisions, even
when you differ with them?’
‘Does your friend allow you to do the same?’
‘Does this work for both of you?’

Copyright H. Gray Otis, PhD, CMHC, 2013
AM I EMPATHETIC?Do I express through empathy that I care enough to listen, understand, and want
the best for the other person? Do I understand what they are saying, their
feelings, their fears & their caring love?
‘Do you really try to understand your friend?’
‘Is it important for you to work ‘as a team’ and to be concerned about each
other’s best interests?’
‘Do both of you strive to understand the others perspectives and feelings?’

Copyright H. Gray Otis, PhD, CMHC, 2013
AM I ACCEPTING?Do I fully accept the other person as they are. Even when I disagree
with them, can I express my thoughts without ‘constructive criticism’ or
imposing my values and expectations on them?
‘Do you accept your friend, the good and not so good?’
‘Do you almost always refrain from criticizing them?’
‘Do you refrain from requiring your friend to meet your expectations?’
‘Are both you and your friend accepting of each other without feeling
submissive or compliant?’

Copyright H. Gray Otis, PhD, CMHC, 2013
AM I TRUSTFUL?
Do I believe in the basic good-hearted nature of the other person by
acknowledging the best about them? Am I trustful of their intentions?
‘Do you consistently see your friend as ‘well-intentioned?’
‘Generally, do you assume the best about your friend?’
‘Are you both trustful that each of you are good-hearted?’

Copyright H. Gray Otis, PhD, CMHC, 2013
If you are almost always . . .
Genuine Respectful Empathetic Accepting Trustful
Your relationship with your friend might look something like the
following slide:
G R E A T FRIENDSHIPS

Copyright H. Gray Otis, PhD, CMHC, 2013
MEASURING G R E A T:
GENUINE RESPECTFUL EMPATHETIC ACCEPTING TRUSTFUL
10
9
8
7
6
5
4
3
2
1
0
_
_
_
_
_
_
_
_
_
_
10
9
8
7
6
5
4
3
2
1
_
_
_
_
_
_
_
_
_
_
10
9
8
7
6
5
4
3
2
1
_
_
_
_
_
_
_
_
_
_
10
9
8
7
6
5
4
3
2
1
_
_
_
_
_
_
_
_
_
_
10
9
8
7
6
5
4
3
2
1
_
_
_
_
_
_
_
_
_
_

Copyright H. Gray Otis, PhD, CMHC, 2013
If your friend is almost always . . .
Genuine Respectful Empathetic Accepting Trustful
You can estimate that your friend’s relationship with you might look
like the following slide:
G R E A T FRIENDSHIPS
Copyright H. Gray Otis, PhD, CMHC, 2013
G R E A T RELATIONSHIPS
GENUINE RESPECTFUL EMPATHETIC ACCEPTING TRUSTFUL
10
9
8
7
6
5
4
3
2
1
0
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
10
9
8
7
6
5
4
3
2
1
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
10
9
8
7
6
5
4
3
2
1
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
10
9
8
7
6
5
4
3
2
1
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
10
9
8
7
6
5
4
3
2
1
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
Copyright H. Gray Otis, PhD, CMHC, 2013
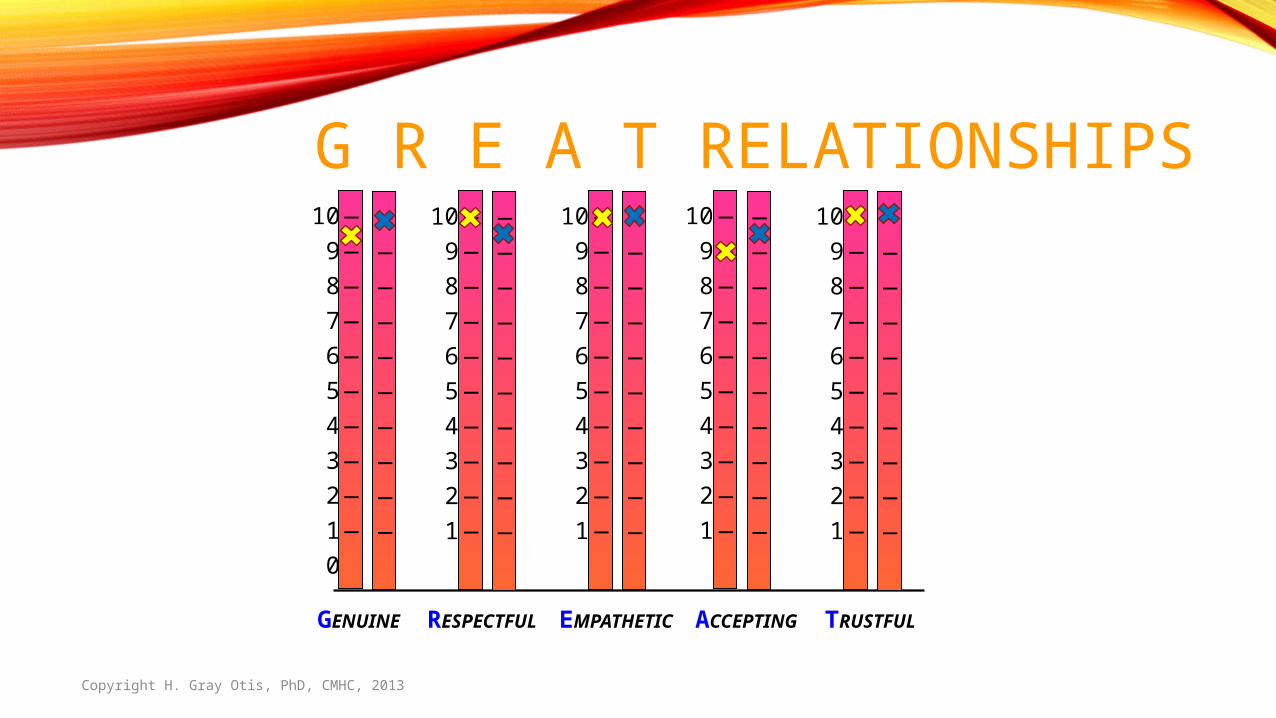
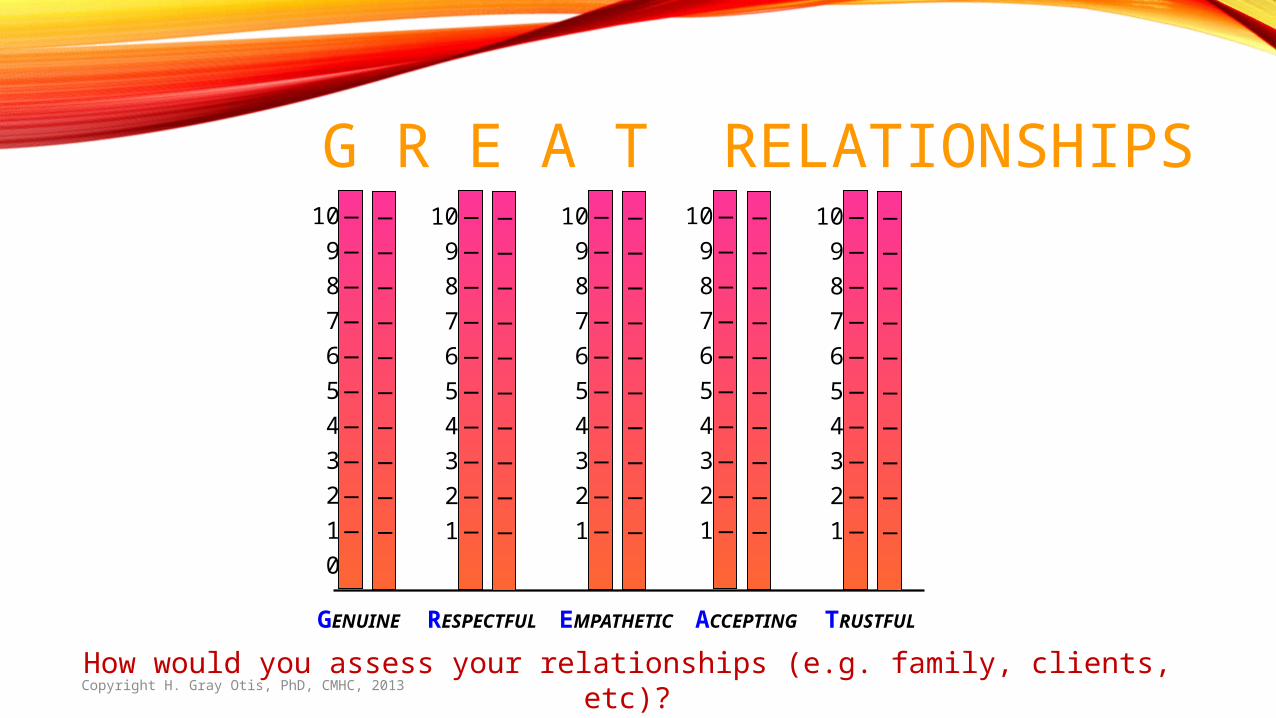
G R E A T RELATIONSHIPS
GENUINE RESPECTFUL EMPATHETIC ACCEPTING TRUSTFUL
10
9
8
7
6
5
4
3
2
1
0
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
10
9
8
7
6
5
4
3
2
1
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
10
9
8
7
6
5
4
3
2
1
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
10
9
8
7
6
5
4
3
2
1
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
10
9
8
7
6
5
4
3
2
1
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
_
How would you assess your relationships (e.g. family, clients, etc)?
Copyright H. Gray Otis, PhD, CMHC, 2013
CREATING ‘G R E A T’Focus on ‘what works’ and ‘what doesn’t work’
Ask yourself to do more of ‘what works’
Do G R E A T experiments
Observe how you feel, think, & act
Observe the results
Report how it works
As we model a G R E A T friendships we grow in our abilities

Copyright H. Gray Otis, PhD, CMHC, 2013
YOUR FRIEND
Empathetic
Accepting
TrustfulGenuine
Respectful
G R E A T FRIENDS
YOU
Empathetic
Accepting
TrustfulGenuine
Respectful

Copyright H. Gray Otis, PhD, CMHC, 2013
THE POWER OF FORGIVENESSResolving the imbedded resentment of trauma & chronic distress
Forgiving is not: Forgetting Excusing Trusting Continuing relationship

Copyright H. Gray Otis, PhD, CMHC, 2013
THE POWER OF FORGIVENESSResolving the imbedded resentment of trauma & chronic distress
Forgiving is not: Forgetting Excusing Trusting Continuing relationship
Forgiving lets go of the need for another to suffer for my sake
Resolved resentment alleviates triggers & frees the forgiver

Copyright H. Gray Otis, PhD, CMHC, 2013
BUILD GREAT CONNECTIONSOvercoming addiction’s isolation
Work through passed relationships concernsFamily conflicts
Prior injurious relationships
The impact of the addiction on loved ones Build functional, fun relationships – 12 steps, friends, etc. Learn how to trust & rely on others Develop a “Cone of Support” – Self, Reliable Others, H P

Copyright H. Gray Otis, PhD, CMHC, 2013
We all want to be heard, understood, and accepted
When we practice hearing, understanding, & accepting others – we become more
Worthy
Acceptable
Capable
THE POWER OF CONNECTION

Factoids

Copyright H. Gray Otis, PhD, CMHC, 2013
Testosterone levels decrease with opioid use
Considerations

Copyright H. Gray Otis, PhD, CMHC, 2013
Testosterone levels decrease with opioid use
Consider testosterone hormone replacement therapy after three months of abstinence & not feeling normal
Considerations

Copyright H. Gray Otis, PhD, CMHC, 2013
Testosterone levels decrease with opioid use
Consider testosterone hormone replacement therapy after three months of abstinence & not feeling normal
ADD, ADHD can interfere with recovery
Considerations
Copyright H. Gray Otis, PhD, CMHC, 2013
Testosterone levels decrease with opioid use
Consider testosterone hormone replacement therapy after three months of abstinence & not feeling normal
ADD, ADHD can interfere with recovery
Consider Strattera (non-stimulant) medication
Considerations

ImagineerHelping those recovering to visualize and create meaningful, enjoyable lives

Copyright H. Gray Otis, PhD, CMHC, 2013
THE CRUCIAL QUESTION
“What are you going to do with the rest of your life?”
In addiction, creativity is focused on obtaining, using, & hiding the use of substances
There is little or no effort concentrating on obtaining enjoyment, meaning, or fulfillment
Those caught up in dependence fear the responsibility & opportunity to create their own life
In recovery, sobriety is never enough – it is fundamental but each person has to envision their life as satisfying & worthwhile

Copyright H. Gray Otis, PhD, CMHC, 2013
WALT DISNEY’S DILEMMA: Many of his staff were talented artists – he valued their creative
imaginations
But in developing Disneyland, he needed engineers to turn
imagination into reality
How could he combine the best of both?
Today’s most coveted work title for Disney employees

Copyright H. Gray Otis, PhD, CMHC, 2013
WALT DISNEY’S DILEMMA: Many of his staff were talented artists – he valued their creative
imaginations
But in developing Disneyland, he needed engineers to turn
imagination into reality
How could he combine the best of both?
Today’s most coveted work title for Disney employees
Imagineer
Copyright H. Gray Otis, PhD, CMHC, 2013
THERAPEUTIC CONSIDERATIONS
Engage the client in identifying their values: Many do not know their values
Many are conflicted between their held values & behaviors
Listing values by each person in a group is value provoking
Individuals can track their own reliability
Self-trust is dependent upon consistency at 97%

Copyright H. Gray Otis, PhD, CMHC, 2013
WHAT R U 4?
Identify aspirations (We are what we desire to be) Show how unproductive it is to focus on what they do not want
Help them focus on the desires they want in their life Teach them to use the power of visualization
Demonstrate how to daily engineer the creation of their desires
Create a wheel of good fortune

Factoids
Copyright H. Gray Otis, PhD, CMHC, 2013
If an individual smokes within one hour of wakening there
is a significantly greater risk of addiction
What does this mean for those who are in recovery?
Consider

Bringing it Home
Copyright H. Gray Otis, PhD, CMHC, 2013
THE FOUR PARADIGMS OF RECOVERY: 1.Integrate withTwelve Steps programs
2.Address the underlying distress sources of addictions
3. Help clients build their life’s path & their own program of recovery
4. Are based on holistic health principles utilizing individual skill development
5. Positive reinforcement is a natural effect of using these skills
6. Clients learn how to put into practice these skills & achieve better outcomes
7. It is imperative that we also attend to taking care of ourselves by practicing these skills with our clients, those whom we work with, as well as our family and friends
Copyright H. Gray Otis, PhD, CMHC, 2013
Those in long-term recovery meet the following criteria:1. Believe They exhibit positive self-beliefs
2. Understand They show an internal sense of
Emotional self-regulation
Nurturing self-care
3. Connect They achieve effective interpersonal relationships
4. Imagineer They realize their own purpose and meaning
Four Paradigms of Recovery

Questions?

Four Paradigms of Recovery A Criterion Counseling Model for Successfully Overcoming Addiction
H. Gray Otis, PhD, CMHC, DCMHS-TClinical Director, The Phoenix Recovery Center
www.ThePhoenixRC.com
801-885-8585


















