
Forward Momentum: It’s time for an Age Friendly Health System€¦ · It’s time for an...
56
Forward Momentum: It’s time for an Age- Friendly Health System Kedar S. Mate, MD Chief Innovation Officer, IHI October 19, 2017
-
Upload
hoangduong -
Category
Documents
-
view
214 -
download
1
Transcript of Forward Momentum: It’s time for an Age Friendly Health System€¦ · It’s time for an...

Forward Momentum: It’s time for an Age-Friendly Health SystemKedar S. Mate, MDChief Innovation Officer, IHI
October 19, 2017

Situation (1):
Older adults:
• do not reliably receive necessary and evidence-based care;
• routinely receive unwanted care and treatment when we don’t know
what matters to;
• are needlessly harmed by inappropriate medications; .
• are vulnerable to falls when we don’t encourage mobility;
• experience avoidable delirium and cognitive decline.

4©2015
Source:
SEMCOG 2040 Forecast-14.0% -11.4% -11.0%
85.5%
-20.0%
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
0-17 18-24 25-64 65+
Population Growth by Age Group 2010-2040
Counties Included
in Data Set:
• Livingston
• Macomb
• Monroe
• Oakland
• Washtenaw
• Wayne
Situation (2):

Situation (3):
• We have lots of evidence-based geriatric-care models of
care that have proven very effective

Bettercareplaybook.org 6
Situation (3):
• We have lots of evidence-based geriatric-care models of
care that have proven very effective
• Yet, most reach only a portion of those who could benefit
– Difficult to disseminate and scale
– Difficult to reproduce in settings with less resources
– Most don’t translate across care settings
• 4m of 46m

The Know-Do Gap
Yesterday Today Tomorrow
What we
know
What we
do

“The First Law of Improvement”
Every system is perfectly designed to
achieve exactly the results it gets.
Dr. Paul Batalden
To get a different result, we must
change the system

Model I: Bad Apples
The
Problem
Quality
Frequency
Better

The Simple, Wrong Answer
Name, Shame & Blame
Somebody

The Cycle of Fear
Engender
Fear
Micromanage Kill the
Messenger
Filter the
Information

Model 2: Continuous Improvement
“All teach, All learn”
Quality
Fre
qu
en
cy



“…98,000 people die in
hospitals each year as
a result of medical
errors that could have
been prevented.”
Institute of Medicine,
November 1999
Origins of the 100,000 Lives Campaign
• By 2004, as a country we had made little progress
• The science was available, our implementation was
unreliable
• Variability in the quality of care was persistent &
entrenched
• There were isolated islands of excellence in patient
safety
• We believed that our sense of urgency was shared by
leaders and providers everywhere in healthcare

100,000 Lives Campaign Objectives (December 2004 – June 2006)
• Save 100,000 Lives
• Enroll more than 2,000 hospitals in the initiative
• Build a national infrastructure for change
• Raise the profile of the problem - and our
proactive response

Six Changes That Save Lives
• Rapid Response Teams
• Evidence-Based Care for Acute Myocardial
Infarction
• Medication Reconciliation to prevent Adverse
Drug Events (ADEs)
• Apply Central Line Infection Bundle
• Prevent Surgical Site Infections
• Apply Ventilator-Associated Pneumonia Bundle
Over 3,100 Hospitals Enrolled
78% of all acute care beds


“When we talk of social
change, we talk of
movements, a word that
suggests vast groups of
people walking together,
leaving behind one way and
traveling toward another.”
Rebecca Solnit

Roadmap for a movement
• Will for change
• Aim & Purpose
• Evidence-based
interventions
• Technical method
for change
• Social system for
spread

Roadmap for a movement
• Will for change
• Aim & Purpose
• Evidence-based
interventions
• Technical method
for change
• Social system for
spread

What is our aim?
The John A. Hartford Foundation and IHI have
adopted the bold and important aim of establishing
Age-Friendly Care in 20 percent of US hospitals
and health systems by 2020
An Age-Friendly Health system is one where every
older adult:
• Gets the best care possible;
• Experiences no healthcare-related harms; and
• Is satisfied with the health care they receive.
Roadmap for a movement
• Will for change
• Aim & Purpose
• Evidence-based
interventions
• Technical method
for change
• Social system for
spread
Deriving the Evidence-based interventions
• Reviewed 17 evidence-based models and
programs serving older adults:
– What population is served?
– What outcomes were achieved?
– What are the core features of the model?

July – August 2016
90 discrete core features identified by model experts in pre-
work
Redundant/similar concepts removed
and 13 core features synthesized by IHI
team
Expert Meeting led to the selection of the “vital few”: the 4Ms
29

The Four M’s
• What Matters: Knowing and acting on each
patient’s specific health goals and care preferences
• Medication: Optimizing medication use to reduce
harm and burden, focused on medications affecting
mobility, mentation, and what matters
• Mentation: Identifying and managing depression,
dementia and delirium across care settings
• Mobility: Maintaining mobility and function and
preventing complications of immobility

Evidence-base
• What Matters:– Asking what matters and developing an integrated systems to address it lowers
inpatient utilization (54% dec), ICU stays (80% dec), while increasing hospice use (47.2%) and pt satisfaction (AHRQ 2013)
• Medications:– Older adults suffering an adverse drug event have higher rates of morbidity, hospital
admission and costs (Field 2005)
– 1500 hospitals in HEN 2.0 reduced 15,611 adverse drug events saving $78m across 34 states (HRET 2017)
• Mentation: – Depression in ambulatory care doubles cost of care across the board (Unutzer 2009)
– 16:1 ROI on delirium detection and treatment programs (Rubin 2013)
• Mobility: – Older adults who sustain a serious fall-related injury required an additional $13,316 in
hospital operating cost and had an increased LOS of 6.3 days compared to controls (Wong 2011)
– 30+% reduction in direct, indirect, and total hospital costs among patients who receive care to improve mobility (Klein 2015)
References at end of slides
31
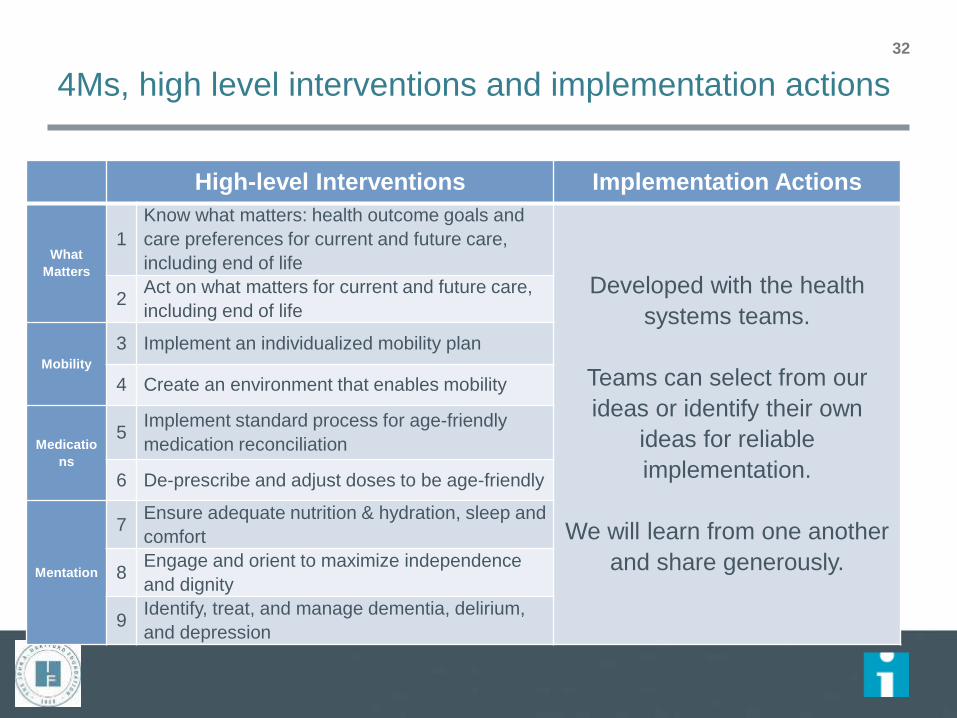
4Ms, high level interventions and implementation actions
32
High-level Interventions Implementation Actions
What
Matters
1
Know what matters: health outcome goals and
care preferences for current and future care,
including end of life
Developed with the health
systems teams.
Teams can select from our
ideas or identify their own
ideas for reliable
implementation.
We will learn from one another
and share generously.
2Act on what matters for current and future care,
including end of life
Mobility
3 Implement an individualized mobility plan
4 Create an environment that enables mobility
Medicatio
ns
5Implement standard process for age-friendly
medication reconciliation
6 De-prescribe and adjust doses to be age-friendly
Mentation
7Ensure adequate nutrition & hydration, sleep and
comfort
8Engage and orient to maximize independence
and dignity
9Identify, treat, and manage dementia, delirium,
and depression

Roadmap for a movement
• Will for change
• Aim & Purpose
• Evidence-based
interventions
• Technical method
for change
• Social system for
spread

The Model for Improvement

Roadmap for a movement
• Will for change
• Aim & Purpose
• Evidence-based
interventions
• Technical method
for change
• Social system for
spread


Design to Achieve National Scale
Stage 0:
Developin
g the
Prototype
Activity: Literature
review & Expert
meeting
Output: Age
Friendly Prototype
Stage 1:
Testing
the
Prototype
Activity: Prototype
testing with five
systems & scaling
within those five
Output: Age Friendly
Model & Scale-up
Guidance
Stage 2
Scale-Up
Activity: Campaign
spreads to 1000+ care sites
Output: 1000+ Age Friendly
Health Systems with
evidence of improved
outcomes for older adults
Testing the Prototype for refinement
(3/17 – 2/18)
Scaling up the Prototype in the five
prototyping systems (1/18 – 12/18)

Where are we now?
38
By the numbers…
• 5 systems actively testing across 26 sites (primary care, PACE, outpt hospice, SNF, inpatient acute, rehab, CCRC, senior ED) in 8 states
• 17 Advisory Group members (chaired by Mary Tinetti & Ann Hendrich)
• 9 expert geriatric faculty – the leaders of the field
• 60+ active tests executing now of age-friendly
• 214 members of AFHS list-servs (US and abroad)
• “Thousands” of lives improved…our most recent estimate was over 3500 in early testing
A 95 year old woman
40

Developing “change packages” for Age-Friendly Care
M Prevent Assess Treat
What
MattersDocument health care
agent
Ask What Matters
questions and document
responses; Ask for
presence of health care
agent
Apply What Matters in
treatment
Medication
Remove in-hospital meds
from discharge med list;
Send updated med list to
primary care physician;
change order sets
Screen for high-risk
meds
De-prescribe or dose
adjust high-risk meds
(especially opiates,
insulin, sleepers)
Mentation
De-prescribe meds
known to cause delirium;
Ensure sufficient
hydration; Support
sufficient sleep
Screen for delirium
(e.g., 2 questions)
Identify and reverse
causes of delirium (non-
pharmacologic); plus
Prevention
Mobility Mobilize patients (if
ambulatory; if not
ambulatory)
Conduct mobility test
(e.g., TUG)
Create mobility plan; plus
Prevention
If found
If positive
If positive

A sample of tests being run by our
health system teams1. Glacier Hills: Moving to single document, work flow,
documentation of What Matters conversation
2. Glacier Hills: Education of providers about asking What Matters
questions using Being Mortal film
3. St. Alphonsus: What Matters Most to You flyer
4. St. Alphonsus: Testing Serious Illness Conversation Guide
questions
5. St. Alphonsus: Asking What Matters questions in Assessment
Bundle
6. St. Alphonsus: Moving advance care planning documents/
advanced directives to the next level/site of care or provider at
discharge
7. St. Mary Mercy: Integrate What Matters questions into geriatrics
assessment
8. Providence: Testing Scotland What Matters questions
9. KP: Knowing older adults through “My Care My Life” binder
10. Ascension: Assessing caregiver burden with caregivers and
patients
11. Ascension: Information on website about services and to enable
self-referral
12. Ascension: Streamlined patient access Referral and intact process
13. St. Alphonsus: Bring home med containers to AWV for better med
rec
14. St. Alphonsus: Checking home meds with provider profile in EMR
with every admit
15. St. Alphonsus: Obtaining med list from pharmacy to review for
deprescribing
16. St. Alphonsus: Education guide based on Med Rec Guide
17. St. Mary Mercy: Medication review for pill burden and sending
deprescribing recommendations to pharmacy
18. Providence: PharmD reviews med list for high risk meds and
recommends de-prescribing to PCP
19. PACE: Pharmacovigilance review with ER/hospital utilization
review
20. Anne Arundel: Established an Age-Friendly prescribing “culture”;
Looking for opportunities to scale-up to other units
21. KP: Patients encouraged to bring personal items to hospital to
create a “Just like home” environment
22. KP: Coaching for staff to develop personal relationship with pts
23. KP: Educate providers re medication issues for deprescribing and
treatment of delirium
24. KP: Self-care plan for high-risk patients, case manager creates
plan to include hydration and nutrition
25. Glacier Hills: Screening (bCAM), standard intervention for
delirium
26. St. Alphonsus: Assessment with mini-cog and PHQ2
27. St. Mary Mercy: Communication re 3D delirium assessment
28. St. Mary Mercy: Assessment with family member involvement
29. Anne Arundel: Hydration- geriatric cups
30. Glacier Hills: Assessment tool with what matters most about
mobility
31. Glacier Hills: Workflow, PT referral to wellness center, education
32. St. Alphonsus: Timed Get Up and Go assessment
33. St. Mary Mercy: Matter of balance, check your risk for falling
(CDC) plus meds
34. St. Mary Mercy: Story book, shorts, What Matters document,
thank you letters, MOVE (mobility optimizes virtually everything)
35. Providence: STEADI results at annual wellness visit, patient who
has fallen or with specific STEADI score has follow up visit with
RN to address risk factors
36. Providence: Measure mobility with STEADI scores at AWV year-
over-year
37. Providence: Patient who has fallen or with specific STEADI score
participate in a shared medical appointment; PharmD reviews
med list for high risk meds and recommends deprescribing to
PCP
38. KP: Patient-initiated patient mobilization, MD's provide 1-page
prompt with exercises (includes exercises for patients in bed and
wheelchair)
39. Anne Arundel: Mobility/quality tech
40. Anne Arundel: 6-clicks, refer to PT

Practical ideas for changing the system of production43
0
500
1000
1500
2000
2500
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53
Hydration
Water Intake w/ Old Pitcher Median
73% increase

Knowing & Acting on What Matters44
Reduced
falls by 18%

Mobility: Empowering older adults 45
Reduce Length of
Stay;
Go home not rehab

FY18 APPROVED System Level Performance Measures / Metrics
Goal Area/Weight Measures Level* Threshold Target Maximum Comments
1. Community Health & WellBeing (CHWB) / 20%
75% of the 20% weight (i.e., 15%):Clinical Services: Tobacco and BMIScreening and Referral Improvement (2points available)Clinical Transformation Portfolio (8 pointsavailable)
System Level 4+ points 7+ points 9+ points Clinical Services: Each ministry has an individual baseline and individual targets. Points earned based on improvement.Clinical Transformation Portfolio: Five policy, system and environmental change strategy initiatives
25% of the 20% weight (i.e., 5%) Growth
System Level TBD TBD TBD New dimension for FY18 to be developed
2. Clinical Care / 20% Reduction of unplanned 30 dayreadmissions to acute inpatient TrinityHealth facilities
(50% of the 20% weight)
System Level 40% of ministries at Target or better
50% of ministries at Target or better
60% of ministries at Target or better
For reference, FY17 = 30/40/50 % of ministries at threshold or better
Reduction of Hospital Acquired Infections(50% of the 20% weight)
System Level 40% of ministries at Target or better
50% of ministries at Target or better
60% of ministries at Target or better
For reference, FY17 = 30/40/50 % of ministries at threshold or better
3. Patient Experience / 20% Willingness to Recommend:Acute Care (34% of 20% weight)Emergency Care (33% of 20% weight)Owned physician practice groups CG-CAHPs (33% of 20% weight)
System Level 30% of ministries at Threshold or
better
40% of ministries at Threshold or
better
50% of ministries at Threshold or better
For reference, FY17 = 30/40/50 % of ministries at threshold or better
4. Colleague Engagement /20%
Colleague Engagement Score System Level 4.06 4.08 4.09 For reference, FY17 = system level score of 4.03/4.05/4.09
5. Financial Stewardship /20%
Operating Margin (OM) (50% of the 20% weight) Cost Per Case Mix-Adjusted Equivalent
Discharge (CMAED)(50% of the 20% weight)**
System Level
System Level
OM: 1.5%
Cost Per CMAED: $7,806
OM: 2.1%
Cost Per CMAED: $7,729
OM: 2.6%
Cost Per CMAED: $7,652
For reference, FY17: 1.2/2.2/3.0 % OM
For reference, FY17: $7,720/$7,645/$7,570 Cost Per CMAED
**Reflects our overall cost position and actions to improve this cost position to move on glide path to be profitable under Medicare. This Cost per CMAED is based on Regional Health Ministries (RHMs) only. For National Health Ministries and Mission Health Ministries, cost per unit metrics will be:Trinity Health Senior Communities (THSC): Cost per DayTrinity Health at Home (THAH): Cost per AdmissionTrinity Health PACE: Cost per Member per MonthPittsburgh Mercy Health Services: Cost per Outpatient UnitAll other Mission Health Ministries: No cost metric; Operating Margin used as the sole measure of financial stewardship Note: The same spread applies to National Health Ministries and Mission Health Ministries
*For RHM executives, weight on objectives is split between an RHM (70%) and System (30%) Components
46©2017 Trinity Health
FY 18 Priority Strategic Aims – These are the priorities!
↑ mob, ↓ hi risk meds & know what matters ↓ ADEs,
right-siting care, ↑ functional status ↓ unplanned
admissions
↑ mob & know what matters
↑ functional status, ↑ d/c to home, ↑ HCAPHS
↑ willingness to recommend
Mechanism varies by discounted FFS, Per case (DRG),
APM (provider at risk)

The business case
Make a sustainable
business case for age-friendly care
Reduce costs associated with
poor quality care
Reduce harm that results in use of higher level of care settings, longer inpatient LOS, ED visits,
readmissions to inpatient settings
Reduce risk of malpractice claims
Improve care transitions, discharge planning, and care coordination
Increase utilization of cost-effective
services
Increase consistent use of underused, evidence-based services and practices
Reduce over-utilization of unnecessary care
Optimize site of care (shift care to lower cost care settings)
Enhance revenue and market share
Increase staff productivity and decrease turnover
Increase bed capacity
Improve reputation as an AFHS to attract patients

The risk…and the opportunity
• Motion…
• Or we could get what Elon Musk described as
“the sum of all vectors”—what you call
FORWARD motion
48
“Every person in your
company is a vector.
Your progress is
determined by the sum
of all vectors.” —
Elon Musk

• Build a shared understanding of the problem
• Set “winnable milestones”
• Design approaches that will work at massive scale
• Drive (rather than assume) demand
• Embrace course corrections
Forward
Motion

What can we do by next Tuesday?50

What can we do by next Tuesday?51
This is our moment. It is time for an Age-Friendly system of care that touches every single older adult in this country.
• Talk to your local hospital CEO or Board chairperson about what it would take to become Age-Friendly
• Ask them to commit to one action—to one “M”—to becoming more Age-Friendly starting next month
• Tell them you will support them to realize it
• And…tell us about it so we can learn with you

Hope is not a plan
52
But, there is no plan without hope



Kedar S. Mate, MDChief Innovation & Education OfficerInstitute for Healthcare Improvement20 University Road, 7th FloorCambridge, MA
Department of MedicineWeill Cornell Medical College
[email protected] @KedarMate
Thank you

Citations
• AHRQ Health Care innovations Exchange. System-integrated program coordinates care for people with advanced illness, leading to greater use of hospice services, lower utilization and costs and high satisfaction. 2013. Available from: https://innovations.ahrq.gov/profiles/system-integrated-program-coordinates-care-people-advanced-illness-leading-greater-use
• Riley GF, Lubitz JD. Long-Term Trends in Medicare Payments in the Last Year of Life. Health Services Research. 2010; 45(2):565-576
• Field, Terry S., et al. "The costs associated with adverse drug events among older adults in the ambulatory setting." Medical care 43.12 (2005): 1171-1176.
• Health Research & Educational Trust (February 2017). Adverse Drug Events Change Package: 2017 Update. Chicago, IL: Health Research & Educational Trust. Accessed at www.hret-hiin.org
• Unutzer J et al. Healthcare costs associated with depression in medically ill fee-for-service Medicare participants. Journal of the American Geriatrics Society. 2009 Mar;57(3):506-10
• Rubin FH et al. Sustainability and scalability of the Hospital Elder Life Program (HELP) at a community hospital. Journal of the American Geriatric Society. 2013 Mar; 59(2): 359-365
• Wong et al. The cost of serious fall-related injuries at three midwestern hospitals. Joint Commission Journal on Quality and Patient Safety. 2011 Feb; 37(2): 81-87.
• Klein K, Bena JF, Albert NM. Impact Of Early Mobilization On Mechanical Ventilation And Cost In Neurological ICU. 2015 American Thoracic Society International Conference Abstracts.
56


















