Formulation Development and Evaluation of Gastro...
12
Journal of Pharmacy Research Vol.11 Issue 2 February 2017 Raghavendra Kumar Gunda et al. / Journal of Pharmacy Research 2017,11(2),167-178 167-178 Review Article ISSN: 0974-6943 Available online through http://jprsolutions.info *Corresponding author. Mr.Raghavendra Kumar Gunda M.Pharm Research Scholar, School of Pharmaceutical Sciences, VISTAS, Vels University, Pallavaram, Chennai, Tamilnadu, India- 600117. Formulation Development and Evaluation of Gastro Retentive Drug Delivery Systems- A Review Raghavendra Kumar Gunda *1 , A.Vijayalakshmi 2 1 Research Scholar, School of Pharmaceutical Sciences, VISTAS, Vels University, Pallavaram, Chennai, Tamilnadu, India- 600117. 2 School of Pharmaceutical Sciences, VISTAS, Vels University, Pallavaram, Chennai, Tamilnadu, India- 600117. Received on:12-01-2017; Revised on: 19-02-2017; Accepted on: 27-02-2017 ABSTRACT In recent years many advancement has been made in research and development of Oral Drug Delivery System. Concept of Novel Drug Delivery System arose to overcome the certain aspect related to physicochemical properties of drug molecule and the related formulations. Purpose of this review is to compile the recent literature with special focus on Gastro Retentive Drug Delivery Systems to give an update on pharmaceutical approaches used in enhancing the Gastric Residence Time (GRT). Various approaches are currently used including Gastro Retentive Floating Drug Delivery Systems(GRFDDS),swelling and expanding system, polymeric bioadhesive systems, modified- shape systems, high density system and other delayed gastric emptying devices. These systems are very helpful to different problem solve during the formulation of different dosage form. The present work also focuses on the polymers used in floating drug delivery systems mostly from natural origin. Floating drug delivery systems are less dense than gastric fluids; hence remain buoyant in the upper GIT for a prolonged period, releasing the drug at the desired/ predeterminedrate. This review article focuses on the recent technological development in floating drug delivery systems with special emphasis on the principal mechanism of floatation and advantages of achieving gastric retention, brief collection on various polymers employed for floating drug delivery systems etc. In addition this review also summarizes the In –Vitro and In -Vivo studies to evaluate their performance and also their future potential. KEY WORDS: Controlled release, Floating lag time, Floating duration/ Gastric residence time, Gastro retentive drug delivery systems, Natural gums, Bioadhesive. INTRODUCTION Oral administration is the most convenient andpreferred means of any drug delivery to thesystemic circulation.The effective oral drugdelivery practice depends on various factors like gastricemptying process, gastrointestinal transit time of dosageform, drug release from dosage form and site ofabsorption of drug [1-3] . Gastric emptying of dosage forms is an extremely variable process and ability to prolong and control the emptying time is a valuable asset for dosage forms, which reside in the stomach for a longer period of time than conventional dosage forms.It has been frequently observed thatmany drugs which are easily absorbed at uppergastrointestinal tract (GIT), eliminated quickly in to lowerGIT because of the peristaltic movement. So it leads toincomplete absorption of drugs from upper part of GIT. To overcome this limitation, the development of oralgastro retentive sustained or controlled releaseformulations is an attempt to release the drug slowly atupper GIT to maintain effective drug concentration insystemic circulation for a prolonged period [3] . Several difficulties are faced in designing controlled release systems for better absorption and enhanced bioavailability [4] . Gastroretentive systems can remain in the gastric region for several hours and hence significantly prolong the gastric residence time of drugs. Prolonged gastric retention improves bioavailability, reduces drug waste, and improves solubility for drugs that are less soluble in a high pH environment. It has applications also for local drug delivery to the stomach and proximal small intestines.Gastric retention helps to provide better availability of new products with new therapeutic possibilities and substantial benefits for patients. The controlled gastric retention of solid dosage forms may be achieved by the mechanisms of mucoadhesion, flotation,
-
Upload
phunghuong -
Category
Documents
-
view
229 -
download
5
Transcript of Formulation Development and Evaluation of Gastro...

Journal of Pharmacy Research Vol.11 Issue 2 February 2017
Raghavendra Kumar Gunda et al. / Journal of Pharmacy Research 2017,11(2),167-178
167-178
Review Article
ISSN: 0974-6943
Available online throughhttp://jprsolutions.info
*Corresponding author.
Mr.Raghavendra Kumar Gunda M.Pharm
Research Scholar,
School of Pharmaceutical Sciences,
VISTAS, Vels University,
Pallavaram, Chennai,
Tamilnadu, India- 600117.
Formulation Development and Evaluation of
Gastro Retentive Drug Delivery Systems- A Review
Raghavendra Kumar Gunda*1, A.Vijayalakshmi 2
1Research Scholar, School of Pharmaceutical Sciences, VISTAS, Vels University, Pallavaram, Chennai, Tamilnadu, India- 600117.2School of Pharmaceutical Sciences, VISTAS, Vels University, Pallavaram, Chennai, Tamilnadu, India- 600117.
Received on:12-01-2017; Revised on: 19-02-2017; Accepted on: 27-02-2017
ABSTRACT
In recent years many advancement has been made in research and development of Oral Drug Delivery System. Concept of Novel Drug
Delivery System arose to overcome the certain aspect related to physicochemical properties of drug molecule and the related formulations.
Purpose of this review is to compile the recent literature with special focus on Gastro Retentive Drug Delivery Systems to give an update
on pharmaceutical approaches used in enhancing the Gastric Residence Time (GRT). Various approaches are currently used including
Gastro Retentive Floating Drug Delivery Systems(GRFDDS),swelling and expanding system, polymeric bioadhesive systems, modified-
shape systems, high density system and other delayed gastric emptying devices. These systems are very helpful to different problem solve
during the formulation of different dosage form. The present work also focuses on the polymers used in floating drug delivery systems
mostly from natural origin. Floating drug delivery systems are less dense than gastric fluids; hence remain buoyant in the upper GIT for a
prolonged period, releasing the drug at the desired/ predeterminedrate. This review article focuses on the recent technological development
in floating drug delivery systems with special emphasis on the principal mechanism of floatation and advantages of achieving gastric
retention, brief collection on various polymers employed for floating drug delivery systems etc. In addition this review also summarizes the
In –Vitro and In -Vivo studies to evaluate their performance and also their future potential.
KEY WORDS: Controlled release, Floating lag time, Floating duration/ Gastric residence time, Gastro retentive drug delivery systems,
Natural gums, Bioadhesive.
INTRODUCTIONOral administration is the most convenient andpreferred means ofany drug delivery to thesystemic circulation.The effective oraldrugdelivery practice depends on various factors like gastricemptyingprocess, gastrointestinal transit time of dosageform, drug releasefrom dosage form and site ofabsorption of drug[1-3].
Gastric emptying of dosage forms is an extremely variable processand ability to prolong and control the emptying time is a valuableasset for dosage forms, which reside in the stomach for a longerperiod of time than conventional dosage forms.It has been frequentlyobserved thatmany drugs which are easily absorbed atuppergastrointestinal tract (GIT), eliminated quickly in to lowerGIT
because of the peristaltic movement. So it leads toincompleteabsorption of drugs from upper part of GIT. To overcome thislimitation, the development of oralgastro retentive sustained orcontrolled releaseformulations is an attempt to release the drug slowlyatupper GIT to maintain effective drug concentration insystemiccirculation for a prolonged period[3]. Several difficulties are faced indesigning controlled release systems for better absorption and
enhanced bioavailability[4].
Gastroretentive systems can remain in the gastric region for severalhours and hence significantly prolong the gastric residence time ofdrugs. Prolonged gastric retention improves bioavailability, reducesdrug waste, and improves solubility for drugs that are less soluble ina high pH environment. It has applications also for local drug deliveryto the stomach and proximal small intestines.Gastric retention helpsto provide better availability of new products with new therapeuticpossibilities and substantial benefits for patients.
The controlled gastric retention of solid dosage forms may be
achieved by the mechanisms of mucoadhesion, flotation,

Journal of Pharmacy Research Vol.11 Issue 2 February 2017
Raghavendra Kumar Gunda et al. / Journal of Pharmacy Research 2017,11(2),167-178
167-178
sedimentation (High density), expansion, modified shape systems,or by the simultaneous administration of pharmacological agents
that delay gastric emptying.Several recent examples have beenreported showing the efficiency of such systems for drugs withbioavailability problems[4-6].
Approaches to increase gastric residence time include
High-density systems Bioadhesive or Mucoadhesive systems Swelling and Expanding Systems Superporous Hydrogels Ion Exchange Resins Bioadhesive Liposomal Systems
Raft-forming systems Gas-generating systems Low-density systems (Floating systems /
Hydrodynamically Balanced Systems )
Floating Drug Delivery Systems (GRFDDS)These are the low density systems having their density lesser thanthe gastric fluid (1.004 gm/cm3) and thus remain buoyant in thestomach without affecting the gastric emptying rate for a prolongedperiod. GRFDDS are classified into two major categories[7-13]
.
Effervescent systems/ Gas generating systems
In this system floatability can be achieved by the generation of gasbubbles. They are formulated in such a way that when in contactwith the acidic gastric contents, CO
2 is liberated and gets entrapped
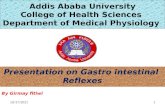
in swollen hydrocolloids, which provides buoyancy to the dosageforms. In vitro, the lag time before the unit floats is < l minute andbuoyancy is prolonged for 8-10 hours. Bilayer or multilayer systemshave also been designed in which drug and excipients can beformulated independently, and the gas generating unit can beincorporated into any of the layers of multiple unit systems, whichavoids the ‘all-or-nothing’ emptying process encountered in singleunit systems[14-15]. It must form a cohesive gel barrier. It should releasecontents slowly to serve as a reservoir[16].
Gas-generating (Effervescent) systems.(a) Bilayer gas-generating systems, with(c) or without (b) semi permeable membrane.
Hydrodynamically balance systems are best suited for drugs havinga better solubility in acidic environment and also for the drugs havingspecific site of absorption in the upper part of the small intestine.To remain in the stomach for a prolonged period of time the dosageform must have a bulk density of less than 1. It should stay in thestomach, maintain its structural integrity, and release drug constantlyfrom the dosage form. HBS are single-unit dosage form, containingone or more gel-forming hydrophilic polymers. Hydroxypropylmethylcellulose (HPMC), hydroxethyl cellulose (HEC), hydroxypropylcellulose (HPC), sodium carboxymethyl cellulose (NaCMC),polycarbophil, polyacrylate, polystyrene, agar, carrageenans or alginicacid are commonly used excipients to develop these systems[17-18].The polymer is mixed with drug and usually administered in a gelatincapsule. The capsule rapidly dissolves in the gastric fluid at bodytemperature and hydration.
Table 1:Polymers and other ingredients used for increasing GRT [19]
Polymers and other ingredients Example
Hydrocolloids (20%-75%) Acacia, Pectin, Chitosan, Agar, Casein, Bentonite,Veegum, HPMC (K4M, K100M and K15M),Gellan gum, Sodium CMC, MC, Calcium alginate,Eudragit S100, Eudragit RL, Propylene foam,Eudragit RS,ethyl cellulose, Polyethylene oxide,β Cyclodextrin, CMC, Polyethylene glycol,polycarbonate, PVA, Sodium alginate, HPC-L,CP 934P, HPC, Eudragit S, Metolose S.M. 100,PVP, HPC-H, HPC-M, HPMC K15, Acrylicpolymer, E4 M and Carbopol.
Inert fatty materials (5%- 75%) Beeswax, fatty acids, long chain fatty alcohols,Gelucires® 39/01 and 43/01.
Effervescent agents Sodium bicarbonate, citric acid, tartaric acid, Di-SGC (Di-Sodium Glycine Carbonate), CG(Citroglycine).
Release rate accelerants (5%-60%) Lactose, MannitolRelease rate retardants (5%-60%) Dicalcium phosphate, Talc, Magnesium stearateBuoyancy increasing agents (upto80%) Ethyl celluloseLow density material Polypropylene foam powder (Accurel MP
1000®).
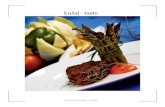
Effervesant Layers(Inner and outer sublayer)
Conventional sustainrelease pills)
Swelable membrane layer
H2O
A
B(A) Multiple-unit oral floating drug delivery system.
(B) Working principle of effervescent floating drug delivery

Journal of Pharmacy Research Vol.11 Issue 2 February 2017
Raghavendra Kumar Gunda et al. / Journal of Pharmacy Research 2017,11(2),167-178
167-178
High-density systems
These systems, which have a density of ~3 g/cm3, are retained in the
rugae of the stomach and are capable of withstanding its peristaltic
movements. Above a threshold density of 2.4–2.8 g/cm3, such
systems can be retained in the lower part of the stomach.
Sedimentation has been employed as a retention mechanism for
pellets that are small enough to be retained in the rugae or folds of
the stomach body near the pyloric region, which is the part of the
organ with the lowest position in an upright posture. Dense pellets
(approximately 3g/cm3) trapped in rugae also tend to withstand the
peristaltic movements of the stomach wall. With pellets, the GI transit
time can be extended from an average of 5.8–25 hours, depending
more on density than on the diameter of the pellets. A density close
to threshold density seems necessary for significant prolongation
of gastric residence time. Commonly used excipients are barium
sulphate, zinc oxide, titanium dioxide and iron powder, etc. These
materials increase density by up to 1.5–2.4g/cm3 [20-23].
Swelling and Expanding Systems
Swelling and expanding systems are dosage forms that, after
swallowing, swell to an extent that prevents their exit from the
pylorus[24]. As a result, the dosage form is retained in the stomach
for a long period. These systems may be called ‘plug type systems’,
since they exhibit a tendency to be logged at the pyloric sphincter.
Swelling and controlled release of the drug may be achieved on
contact of the drug delivery system with gastric fluid; the polymer
imbibes water and swells. Extensive swelling of the polymer is the
result of the presence of physical-chemical crosslinks in the
hydrophilic polymer network. The bulk enables gastric retention and
maintains the stomach in a ‘fed’ state, suppressing housekeeper
waves[25,26]. Medicated polymer sheets or swelling balloon hydrogels
are examples of such delivery systems. A balance between the rate
and extent of swelling and the rate of erosion of the polymer is
crucial to achieve optimum benefit and to avoid adverse effects.
They are explained as follows (Non-Effervescent systems)[27].
Colloidal gel barrier systems
These systems incorporate a high level (20-75% w/w) of one or more
gel forming, highly swellable,cellulose type hydrocolloids,
polysaccharides and matrix forming polymers. On coming in contact
withgastric fluid, the hydrocolloids in the system hydrate and form a
colloidal gel barrier around its surface.This gel barrier controls the
rate of fluid penetration into the device and consequent release of
the drug[27].
inside a micro-porous compartment with apertures along its top and
bottom walls. The peripheral walls of the drug reservoir compartment
are completelysealed to prevent any direct contact of the gastric
mucosal surface with the undissolved drug.
Multiparticulate system Floating Beads
In these systems, the dosage of the drug substances is divided on a
plurality of subunit, typically consisting ofthousands of spherical
particles with diameter of 0.05-2.00 mm. Thus multi particulate dosage
forms arepharmaceutical formulations in which the active substance
is present as a number of small independent subunits.To deliver the
recommended total dose, these subunits are filled into a sachet.
Microballons
various approaches are made in delivering substances to the target
site in a controlled release fashion. Oneof such approach is using
polymeric microballoons as carrier for drugs. Hollow microspheres
are known as themicroballoons. Microballoons were floatable in vitro
for 12 hrs, when immersed in aqueous media. Radio graphicalstudies
proved that microballoons orally administered to human were
dispersed in the upper part of stomach andretained there for three hr
against peristaltic movements.
Super porous Hydrogels
In this approach to improve gastric retention time (GRT) super porous
hydrogels of average pore size >100 micro meter, swell to equilibrium
size within a minute due to rapid water uptake by capillary wetting
through numerous interconnected open pores. They swell to a large
size (swelling ratio: 100 or more) and are intended to have sufficient
mechanical strength to withstand pressure by gastric contraction.
This is achieved by co-processing with a hydrophilic particulate
material, croscarmellose sodium. Which forms a dispersed phase
within the continuous polymer matrix during the synthesis
(‘superporous hydrogel composites’). The superporous hydrogel
composites stay in the upper GIT for >24 hours. Recent advances in
the field have led to “superporous hydrogel hybrids”, which are
prepared by adding a hydrophillic or water dispersible polymer that
can be cross-linked after the superporous hydrogel is formed.
Examples of hybrid agents include polysaccharides such as sodium
alginate, pectin and chitosan[28-30].
Ion-Exchange Resins
A coated ion exchange resin bead formulation has been shown to
have gastric retentive properties, which was loaded with bicarbonates.
Ion exchange resins are loaded with bicarbonate and a negatively
charged drug is bound to the resin, resultant beads were thenThis technology is based on the encapsulation of a drug reservoirMicro porous compartment systems

Journal of Pharmacy Research Vol.11 Issue 2 February 2017
Raghavendra Kumar Gunda et al. / Journal of Pharmacy Research 2017,11(2),167-178
167-178
encapsulated in a semipermeable membrane to overcome the rapid
loss of carbon dioxide. Upon arrival in the acidic environment of the
stomach and exchange of chloride and bicarbonate ions take place.
As a result of this reaction carbon dioxide was released and trapped
in a membrane thereby carrying beads towards the top of gastric
content and producing a floating layer of resin beads in contrast the
uncoated beads, which will sink quickly[31-34].
Bioadhesive or Mucoadhesive Systems
The term “mucoadhesion” is commonly used to describe an
interaction between the mucin layer that lines the entire GIT and a
bioadhesive polymer. Bioadhesive drug delivery systems (BDDS)
are used as a delivery device within the lumen to enhance
drugabsorption in a site specific manner. This approach involves the
use of bioadhesive polymers, which can adhere to the epithelial
surface in the stomach. Thus, they prolong the gastric retention
time[35-36].
Bioadhesion can be explained by[37-38]
The absorption theory
The electron theory
The wetting theory
The diffusion theory
Bioadhesive mechanism
Bioadhesive liposomal Systems
Mucoadhesive liposomal systems are formulated by coating a
polymer to facilitate enteral absorption of poorly absorbed drugs.
Liposomes are generally coated with mucoadhesivepolymers such
as chitosan, carbopol, Carboxymethyl chitin and carboxymethyl
chitosan. The mucoadhesion of the resultant liposomes leads to an
enhanced GRT of the dosage forms[39-40].
Raft forming systems
Raft forming systems have received much attention for the drug
delivery for gastrointestinal infections and disorders. Floating Rafts
have been used in the treatment of Gastric esophageal reflux disease
(GERD). The mechanism involved in the raft formation includes the
formation of viscous cohesive gel in contact with gastric fluids,
where in each portion of the liquid swells forming a continuous layer
called a raft. This raft floats on gastric fluids because of low bulk
density created by the formation of CO2. Usually, the system
ingredients includes a gel forming agent and alkaline bicarbonates
or carbonates responsible for the formation of CO2 to make the system
less dense and float on the gastric fluids . Jorgen et al described an
antacid raft forming floating system. The system contains a gel
forming agent (e.g. sodium alginate), sodium bicarbonate and acid
neutralizer, which forms a foaming sodium alginate gel (raft), which
when comes in contact with gastric fluids, the raft floats on the
gastric fluids and prevents the reflux of the gastric contents (i.e.
gastric acid) into the esophagus by acting as a barrier between the
stomach and esophagus[41-42].
FACTORS AFFECTING Gastro Retention Time of Floating Drug
Delivery Systems
The various factors which influence the efficacy of Gastro Retentive
Drug Formulation‘s as a gastro-retentive systems are:
Formulation Factors and Idiosyncratic Factors[27,43]
Formulation Factors
Density
GRT is a function of dosage form buoyancy that is dependent on the
density. The density of a dosage form also affects the gastric emptying
rate. A buoyant dosage form having a density of less than that of the
gastric fluids floats. Since it is away from the pyloric sphincter, the
dosage unit is retained in the stomach for a prolonged period. Drug
floatation is a function of time and it could least until hydrodynamic
equilibrium is achieved. Dosage forms having larger density then
the gastric content sink at the bottom of the atrium where they settle
and release the active compound in a controlled manner over a
prolonged period of time.
Size
Dosage form units with a diameter of more than 7.5 mm are reported
to have an increased GRT compared with those with a diameter of 9.9
mm. Larger dosage forms tend to have longer gastric retention time
than smaller ones because they are emptied in the digestive phase
(weaker MMC) and also because their passage through the pyloric
sphincter into the small intestine is hindered.
Shape of dosage form:
Tetrahedron and ring shaped devices with a flexural modulus of 48
and 22.5 kilo pounds per square inch (KSI) are reported to have

Journal of Pharmacy Research Vol.11 Issue 2 February 2017
Raghavendra Kumar Gunda et al. / Journal of Pharmacy Research 2017,11(2),167-178
167-178
better GRT = 90% to100% retention at 24 hours compared with other
shapes.
Under fasting conditions, the GI motility is characterized by periods
of strong motor activity or the MMC that occurs every 1.5 to 2
hours. The MMC sweeps undigested material from the stomach and,
if the timing of administration of the formulation coincides with that
of the MMC, the GRT of the unit can be expected to be very short.
However, in the fed state, MMC is delayed and GRT is considerably
longer.
Viscosity Grade of Polymer:
Drug release and floating properties of GRFDDS are greatly affected
by viscosityof polymers and their interaction. Low viscosity polymers
(e.g., HPMC K100 LV) were found to be morebeneficial than high
viscosity polymers (e.g., HPMC K4M) in improving floating
properties. In addition, adecrease in the release rate was observed
with an increase in polymer viscosity.
Nature of meal
Feeding of indigestible polymers or fatty acids salts can change the
motility pattern of the stomach to a fed state, thus decreasing the
gastric emptying rate and prolonging drug release. Type of meal and
its caloric content, volume, viscosity and co-administered drugs affect
gastric secretions and gastric emptying time. The rate of emptying
primarily depends on caloric contents of the ingested meal. It does
not differ for proteins, fats and carbohydrates as longas their caloric
contents are the same. Generally gastric emptying is slowed down
because of increased acidity, osmolarity and calorific values.Gastric
residence time increases in the presence of food, leading to increased
drug dissolution of the dosage form at the most favorable site of
absorption. A GRT of 4-10 hours has been reported after a meal of
fats and proteins.
Frequency of feed
The GRT can be increased by over 400 minutes when successive
meals are given compared with a single meal due to the low frequency
of MMC.
Idiosyncratic Factors
Idiosyncrasy is genetically determined abnormality to a chemical.
The drug interacts with some unique feature of theindividual, not
found in majority of subjects, and produces the uncharacteristic
reaction. The type of reaction isrestricted to individuals with a
particular genotype. It may also depends on-
Gender
their age and race matched female counterparts (4.6±1.2 hours),
regardless of theweight, height and body surface.Mean ambulatory
GRT in males (3.4 ± 0.6 hours) is less compared with their age and
race matched female counter parts (4.6 ± 1.2 hours) regardless of the
weight, height and body surface.
Age
Low gastric emptying time is observed in elderly than do in younger
subjects. Intra subject and inter subjectvariations also are observed
in gastric and intestinal transit time. Elderly people, especially those
over 70 years havea significantly longer GRT. Elderly people,
especially those above 70, have a significantly longer GRT.
Posture
GRT can vary between supine and upright ambulatory states of the
patient
Upright Position:
An upright position protects floating forms against postprandial
emptying because the floatingform remains above the gastric
contents irrespective of its size. Floating dosage forms show
prolonged and morereproducible GRTs while the conventional dosage
form sink to the lower part of the distal stomach from wherethey are
expelled through the pylorus by astral peristaltic movements.
Supine Position:
This position offers no reliable protection against early and erratic
emptying. In supine subjectslarge dosage forms (both conventional
and floating) experience prolonged retention. The gastric retention
offloating forms appear to remain buoyant anywhere between the
lesser and greater curvature of the stomach.
On moving distally, these units may be swept away by the peristaltic
movements that propel the gastric contentstowards the pylorus,
leading to significant reduction in GRT compared with upright
subjects.
Concomitant Intake of Drugs:
Drugs such as prokinetic agents (e.g., metoclopramide and cisapride),
anticholinergics (e.g., atropine or propantheline), opiates (e.g.,
codeine) may affect the performance of GRFDDS. The co-
administration of GI-motility decreasing drugs can increase gastric
emptying time.
Biological factors
Diseases like gastroenteritis, gastric ulcer, pyloric stenosis, diabetes
and hypothyroidism retard gastric emptying. Partial or total
gastrectomy, duodenal ulcer and hypothyroidism promote gastric
emptying rate.Women have slower gastric emptying time than men. Mean
ambulatory GRT in meals (3.4±0.4 hours) is less as compared with

Journal of Pharmacy Research Vol.11 Issue 2 February 2017
Raghavendra Kumar Gunda et al. / Journal of Pharmacy Research 2017,11(2),167-178
167-178
Advantages of GRFDDS
Increasing the GRT with either of the approaches offers several
advantages such as:
Acidic drug substances like aspirin cause irritation on the
stomach wall when come in to contact with it. Hence HBS
formulation may be useful for the administration of aspirin
and other similar drugs.
The Floating systems are advantageous for drugs meant
for local action in the stomach. e.g., antacids.
The GRFDDS are advantageous for drugs absorbed through
the stomach ex: Ferrous salts, Antacids. Improved drug
absorption, because of increased GRT and more time spent
by the dosage form at its absorption site.
Controlled delivery of drugs.Minimizing the mucosal
irritation due to drugs, by drug releasing slowly at controlled
rate.The controlled, slow delivery of drug to the stomach
provides sufficient local therapeutic levels and limits the
systemic exposure to the drug. This reduces side effects
that are caused by the drug in the blood circulation. In
addition the prolonged gastric availability from a site directed
delivery system may also reduce the dosing frequency.
Administration of prolongs release floating dosage forms,
tablet or capsules, will results in dissolution of the drug in
the gastric fluid. They dissolve in the gastric fluid would be
available for absorption in the small intestine after emptying
of the stomach contents. It is therefore expected that a drug
will be fully absorbed from the floating dosage forms if it
remains in the solution form even at the alkaline pH of the
intestine.
When there is vigorous intestinal movement and a shorted
transit time as might occur in certain type of diarrhea, poor
absorption is expected. Under such circumstances it may
be advantageous to keep the drug in floating condition in
stomach to get a relatively better response.
As sustained release systems, floating dosage forms offer
various potential advantages. Drugs that have poor
bioavailability because their absorption is limited to upper
GI tract can be delivered efficiently thereby maximizing their
absorption and improving their absolute bioavailability.
Floating dosage forms with SR characteristics can also be
expected to reduce the variability in transit performance. In
addition, it might provide a beneficial strategy for gastric
and duodenal cancer treatment.
The concept of GRFDDS has also been utilized in the development
of various anti- reflux formulations
Disadvantages/Limitations of GRFDDS:
Floating system is not feasible for those drugs that have
solubility or stability problem in G.I. tract.
These systems require a high level of fluid in the stomach
for drug delivery to float and work efficiently.
Drugs showing absorption window at stomach region are
only considered to be better candidates.
Drugs such as Nifedipine, which is well absorbed along the
entire GI tract and also undergo significant first-pass
metabolism, may not be suitable candidates for increasing
the GRT since the slow gastric emptying may lead to reduced
systemic bioavailability. Also there are limitations to the
applicability of GRFDDS for drugs that are irritant to gastric
mucosa.
The dosage form should be administered with a full glass of
water (200-250 ml).
These systems do not offer significant advantages over
the conventional dosage forms for drugs, which are
absorbed throughout the gastrointestinal tract.
The use of large single-unit dosage forms sometimes poses
a problem of permanent retention of rigid large-sized single-
unit forms especially in patients with bowel obstruction,
intestinal adhesion, gastropathy, or a narrow pyloric
opening (mean resting pyloric diameter 12.8 ± 7.0 mm)
POTENTIAL DRUG CANDIDATE FOR GRFDDS
GRFDDS is beneficial for drug candidate which have
stability problems at alkaline pH (captopril, ranitidine HCl,
metronidazole)
Drugs having narrow absorption window in stomach, or
upper part of small intestine
(L-DOPA, p- aminobenzoic acid, furosemide, riboflavin)

Journal of Pharmacy Research Vol.11 Issue 2 February 2017
Raghavendra Kumar Gunda et al. / Journal of Pharmacy Research 2017,11(2),167-178
167-178
Drugs those are locally active in the stomach (misroprostol,
antacids)
Drugs that exhibit low solubility at high pH values (e.g.,
diazepam, chlordiazepoxide, verapamil)
Drugs that disturb normal colonic microbes (e.g., antibiotics
used for the eradication of Helicobacter pylori, suchas
tetracycline, clarithromycin, amoxicillin)
Table 2: The Potential Candidates for GRFDDS
Formulation Drug candidates
Floating microspheres Aspirin, Griseofulvin, p-nitroaniline,
Ibuprofen, Ketoprofen , Piroxicam,
Verapamil, Cholestyramine,
Theophylline, Nifedipine, Nicardipine,
Dipyridamol , Tranilast and Terfinadine
Floating granules Diclofenac sodium, Indomethacin and
Prednisolone
Films Cinnarizine, Albendazole
Floating tablets and PillsAcetaminophen, Acetylsalicylic acid,
Ampicillin, Amoxycillintrihydrate,
Atenolol, Fluorouracil, Isosorbide
mononitrate, Para- aminobenzoic acid,
Piretanide, Theophylline, Verapamil
hydrochloride, Chlorpheniramine
maleate, Aspirin, Calcium Carbonate,
Fluorouracil, Prednisolone, Sotalol ,
pentoxyfilline and DiltiazemHCl,
Atenolol, ciprofloxacin.
Floating Capsules Chlordiazepoxide hydrogen chloride,
Diazepam , Furosemide, Misoprostol, L-
Dopa, Benserazide, Ursodeoxycholic
acid and Pepstatin, and Propranolol
Formulation of Floating Dosage Form
The following types of the ingredients can be incorporated in to
GRFDDS
Hydrocolloids
Inert fatty materials
Release rate accelerants
Release rate retardant
Buoyancy increasing agents
Miscellaneous
Hydrocolloids:
Suitable hydrocolloids are synthetic, anionic or non-ionic like
hydrophilic gums, modifiedcellulose derivatives. e.g., Acacia, pectin,
agar, alginates, gelatin, casein, bentonite, veegum, MC, HPC, HEC,
and SCMC can be used. The hydrocolloids must hydrate in acidic
medium i.e., gastric fluid is having pH 1.2.Althoughthe bulk density
of the formulation may initially be more than one, but when gastric
fluid is enter in the system, itshould be hydro-dynamically balanced
to have a bulk density of less than one to assure buoyancy.
Table 3: Polymers and their Applications in GRFDDS19,27
Name of Pharmaceutical A Application in GRFDDSthe polymer pplications
Pec tin Adsorbent, Pectin gel beads have beenemulsifying agent, shown to be an effectiveGelling agent, medium for controlling thethickening agent, release of a drug within thestabilizing agent. gastrointestinal (GI) tract.
Acacia Emulsifying and Used in novel tabletsuspending agent, formulations and modifiedbinder, viscosity- release tabletsenhancer
Agar Emulsifying agent, It has been investigated in astabilizing agent, number of experimentalsuppository base, pharmaceutical applicationssuspending agent, including as a Sustainedtablet binder, release agent in gels, beads,thickening agent, microspheres, and tablets.viscosity-increasingagent
Ge la t in Coating agent, Low-molecular-weightfilm-former, gelatin has been investigatedGelling agent, for its ability to enhance thesuspending agent, dissolution of orallytablet binder, ingested drugs. Ibuprofen–viscosity-increasing gelatin micro pellets haveagent. been prepared for the
controlled release of thedrug.
Alginic Acid Stabilizing agent, Alginate gel beads capablesuspending agent, of floating in the gastricsustained release cavity have been prepared,adjuvant, tablet binder, the release properties oftablet disintegrant, which were reported to beViscosity increasing applicable for sustainedagent release of drugs, and for
targeting the gastric mucosa.C hito s an Coating agent, Chitosan has been processed
disintegrant, into several pharmaceuticalfilmformer, forms including gels, films,mucoadhesive, binder, beads, microspheres, tabletsviscosity-increasing and coatings for liposomes.agent.
Ethylcellulose Coating agent, Studies have also suggestedflavoring fixative, ethylcellulose for use inTablet binder, floating microparticlestablet filler, viscosity- Based on low-density foamIncreasing agent. powder, for gastro retentive
drug delivery systemsPolycarbophil Adsorbent, Floating-bioadhesive
bioadhesive, microspheres coated withControlled release poly carbophil have beentablet binder, found to be a useful gastroemulsifying agent, retentive drug deliverythickening agent, system for the treatment ofsuspending agent. Helicobacter pylori.
So d ium Alkalizing agent, Sodium bicarbonate hasbicarbonate therapeutic agent. been used as a gas-forming
agent in alginate raftsystems and in floating,controlled-release oraldosage forms of furosemideand cisapride.
Inert fatty materials:Edible, pharmaceutical inert fatty material, having a specific gravity

Journal of Pharmacy Research Vol.11 Issue 2 February 2017
Raghavendra Kumar Gunda et al. / Journal of Pharmacy Research 2017,11(2),167-178
167-178
less than one can beadded to the formulation to decrease the
hydrophilic property of formulation and hence increases the
buoyancy e.g.Purified grades of beeswax, fatty acids, long chain
alcohols, glycerides, and mineral oils can be used.
Release rate accelerant:
The release rate of the medicament from the formulation can be
modified by includingexcipient like lactose and/or mannitol. These
may be present from about 5-60 % by weight. (Super Disintegrant)
Release rate retardants:
Insoluble substances such as di-calcium phosphate, talc, magnesium
stearate decreases thesolubility and hence retard the release of
medicaments.
Buoyancy Increasing agents:
Materials like ethyl cellulose, which has bulk density less than one,
can be used forenhancing the buoyancy of the formulation. It may
be adapted up to 80 % by weight.
Table 4: List of Marketed Products with increased GRT44
Brand name Drug (dose) Company, country Dosage form
Madopar® Levodopa(l00mg), benserazide(25mg) Roche Products, US Floating controlled release capsuleValrelease® Diazepam (15mg) Hoffmann-La Roche, US Floating capsuleLiquid Gaviscon® Al. hydroxide (95mg), Mg. carbonate (358mg) GlaxoSmithKline, India Raft-forming liquid alginate preparationTopalkan® Aluminium-magnesium antacid Pierre Fabre Drug, France Floating liquid alginate preparationConviron® Ferrous sulphate Ranbaxy, India gel-forming floating systemCifran OD® Ciprofioxacin (500mg & 1g) Ranbaxy, India Gas-generating floating tabletOflin OD® Ofloxacin (400mg) Ranbaxy, India Gas-generating floating tabletCytotec® Misoprostol (100ng) Pharmacia, US Bilayer floating capsule
Miscellaneous:
Pharmaceutically acceptable adjuvant like preservatives, stabilizers,
and lubricants can beincorporates in the dosage forms as per the
requirements. They do not adversely affect the hydrodynamic balance
of the systems. A list of Polymers and their Applications in GRFDDS
are given in Table 3.
Evaluation of Floating Drug Delivery System:
Evaluation of a formulation and parameters to be evaluated is a critical
aspect in formulation technology. Aschematic on evaluation of
GRFDDS is shown as in Schematic Diagram.
Evaluation of Powder Blend as per general Pharmacopoeial
specifications such as Angle of Repose, Bulk Density, Tapped
Density, Hausners Ratio, Compressibility Index etc.
Evaluation of Floating Tablets
Pharmacopoeial Tests
Hardness[46]
The hardness of the tablets was tested by diametric compression
using a Monsanto Hardness Tester. A tablet hardness of about 2-4
Kg/cm2 is considered adequate for mechanical stability.
Friability[46]
The friability of the tablets was measured in a Roche Friabilator. 20
Tablets were taken, Weighed and Initial weight was noted (W0) are
dedusted in a drum for a fixed time (100 Freefalls, in a Roche Friabilator)
and weighed (W) again. Percentage friability was calculated from the
loss in weight as given in equation as below. The weight loss should
not be more than 1 %
Friability (%) = [(Initial weight- Final weight) / (Initial weight)] x
100
Content Uniformity[46]
In this test, 20 tablets were randomly selected and the percent drug
content was determined, the tablets contained not less than 85% or
not more than 115% (100±15%) of the labeled drug content can be
considered as the test was passed.Schematic Diagram of Evaluation of Floating Drug Delivery System

Journal of Pharmacy Research Vol.11 Issue 2 February 2017
Raghavendra Kumar Gunda et al. / Journal of Pharmacy Research 2017,11(2),167-178
167-178
Assay[47]
The drug content in each formulation was determined by triturating
20 tablets and powder equivalent to average weight was dissolved
in 100ml of 0.1N Hydrochloric acid by sonication for 30 min. The
solution was filtered through a 0.45μ membrane filter, diluted suitably
and the absorbance of resultant solution was measured
spectrophotometrically at λmax of API( nm) using 0.1 N Hydrochloric
acid as blank .
Thickness[46]
Thickness of the all tablet formulations were measured using
verniercalipers by placing tablet between two arms of the
verniercalipers.
In-Vitro Buoyancy Studies[48-49]
The tablets were placed in a 100-mL beaker containing 0.1N HCl. The
time required for the tablet to rise to the surface and float was
determined as floating lag time.
Buoyancy (%) = Wf /W
f+W
s*100
Where, Wfand W
s are the weights of floating and settled
microspheres respectively.
In-Vitro Dissolution Study[50-51]
The In-vitro dissolution study for the Floating tablets were carried
out in USP XXIII type-II dissolution test apparatus (Paddle type)
using 900 ml of 0.1 N HCl as dissolution medium at 50 rpm and
temperature 37±0.5°C. At predetermined time intervals, 5 ml of the
samples were withdrawn by means of a syringe fitted with a pre-filter,
the volume withdrawn at each interval was replaced with same
quantity of fresh dissolution medium. The resultant samples were
analyzed for the presence of the drug release by measuring the
absorbance at λmax of API( nm) using UV Visible spectrophotometer
after suitable dilutions. The determinations were performed in
triplicate (n=3)
Kinetic modelling of drug release[52-57]
The dissolution profile of all the formulations was fitted in to zero-
order, first-order, Higuchi and Korsmeyer-peppas models to ascertain
the kinetic modelling of drug release.
In-Vivo Evaluation for Gastro-Retention:
X-ray/ Gamma Scintigraphy:
X ray/Gamma Scintigraphy is a very popular evaluation parameter
for floatingdosage form nowadays. It helps to locate dosage form in
the gastrointestinal tract (GIT), by which one can predictand correlate
the gastric emptying time and the passage of dosage form in the GIT.
Here the inclusion of aradio opaque material into a solid dosage form
enables it to be visualized by X rays. Similarly, the inclusion of a
emitting radionuclide in a formulation allows indirect external
observation using a camera or scintiscanner. Incase of scintigraphy,
the rays emitted by the radionuclide are focused on a camera,
which helps to monitor thelocation of the dosage form in the GIT.
TheFormulated Tablets (TranilastEudragit S (BaSO4) Isardipine
(HPMC) system)and for In-Vivo studies two healthy male volunteers
administered hard gelatin capsules packed with microballons (1000
mg) with 100 mL water. X-ray photographs at suitable intervals were
taken[58-60].
Two phases: Phase I (fasted conditions): Five healthy volunteers
(3 males and 2 females) in an open randomized crossover design,
capsules ingested in sitting position with 100 mL of tap water.
Phase II (fed states): Four subjects received normal or MR capsules
in a crossover design after standard breakfast. Venous blood samples
were taken in heparinized tubes at predetermined time intervals after
dosing.
In-Vivo behavior of coated and uncoated beads, prepared floating
beads was monitored using a single channel analyzing study in 12
healthy human volunteers of mean age 34 yrs by Gamma
scintigraphy[31].
Tablet density
Tablet density is an important parameter for floating tablets. The
tablet would floats only when its density is less than that of gastric
fluid (1.004). The density is determined using following
relationship[61]
V = r2hd =m/v
v = volume of tablet (cc)
r = radius of tablet (cm)
h = crown thickness of tablet (g/cc)
m = mass of tablet
FOR MULTIPLE UNIT DOSAGE FORMS (MICROSPHERES/
MICROBALLONS) [60]
In case of multiparticulate drug delivery systems, differential scanning
calorimeter (DSC), particle size analysis, flow properties, surface
morphology, mechanical properties and x-ray diffraction studies are
performed.
Size and shape evaluation
The particle size and shape plays a major role in determining solubility
rate of the drugs and thus potentially its bioavailability. The particle
size of the formulation can be determined using Sieve analysis, Air
elutriation analysis, Photo analysis, Optical microscope, Electro

Journal of Pharmacy Research Vol.11 Issue 2 February 2017
Raghavendra Kumar Gunda et al. / Journal of Pharmacy Research 2017,11(2),167-178
167-178
résistance counting methods, Sedimentation techniques, Laser
diffraction methods[31,62].
Morphology and surface topographyThe surface topography and structures were determined usingscanning electron microscope (SEM) operated with an accelerationvoltage of 10k.v, Contact angle meter, Atomic force microscopy
(AFM), Contact profiliometer[62].
Percentage drug entrapment
Percentage entrapment efficiency was reliable for quantifying the
phase distribution of drug in the pre-pared formulations. The drug is
extracted by a suitable method, analyzed and is calculated from:
PDE = Practical Drug Loading /Theoretical Drug Loading * 100
FUTURE POTENTIAL AND CONCLUSION
The development of GRFDDS products is currently one of the most
important challenges in pharmaceutical research. From the above
review we conclude that GRFDDS products by virtue of formulation
and product design provide drug release in a modified form distinct
from that of the conventional dosage forms mainly at stomach region,
aptly applicably to drugs showing absorption at stomach site. The
physicochemical properties of the drug, polymer and the drug to
polymer ratio govern the release of drug from the formulation. The
use of one kind of polymer or another can affect the release kinetics,
the presence of burst effect and the mechanisms involved in the
release. Natural polymers have been used significantly in designing
and synthesis of novel drug delivery systems because of their
biodegradable, biocompatible, ecofriendly nature and vast
availability. Hence these natural polymers will expand the scope of
new drug delivery systems in the future. With proper selection of
natural polymers and their blending with other polymers better
floating dosage forms with improved floating lag time, floating
duration and drug release can be achieved. The use of Natural
Polymers can be a good replacement for synthetic polymers in the
Formulation development of controlled release floating dosage forms,
Formulations prepared by such renewable and eco-friendly plant
resources can be considered as promising floating matrix forming
agents to bring about sustained release action with site specific
delivery for improved bioavailability. FDDS approach may be used
for various potential active agents with narrow absorption window,
e.g. antiviral, antifungal and antibiotic agents (sulphonamides,
quinolones, penicillins, cephalosporins, aminoglycosides and
tetracyclines).
The kinetic study of drug release helps in obtaining meaningful
parameters which are employed for comparative purposes and relating
the release parameter with important parameters such as
bioavailability which further aids in studying the influence of
formulation factors on the drug release for optimization.
REFERENCES
1. Praveen N, Mahant S, Sharma D, Floating systems: A novel
approach towards gastro retentive drug delivery systems,
Int J Pharm PharmSci, 2(2), 2010, 3-15.
2. Sonia D, Singh TG, Kumar AR, Sood S, Arora S, Gastro
retentive: controlled release drug delivery system, Asian J
Pharm Clin Res,4(1), 2011, 5-13.
3. Satyajit Panda, NeerajaSukanyaSailada, Bandaru Devi,
SnigdhaPattnaik, LaxmidharMaharana. Design of Floating
Drug Delivery Systems: An Update on Polymeric
Advancements with Special Reference from Natural Origin.
Int. J. Pharm. Sci. Rev. Res., 39(1), July – August 2016; Article
No. 26, Pages: 125-132.
4. Hirtz J. The git absorption of drugs in man: a review of
current concepts and methods of investigation. Br J
ClinPharmacol. 1985; 19: 77-83.
5. Arora, S., Ali, J., Ahuja, A., Khar, R.K., Baboota, S., Floating
drug delivery systems: A Review, AAPS Pharmscitech, 2005,
372-390.
6. Jain, S. K., Agrawal, G. P., Jain, N. K., Floating microspheres
as drug delivery system: Newer Approaches, evaluation of
porous carrier-based floating or list at microspheres for
gastric delivery, AAPS Pharmascitech, 2006, 7, 54-62.
7. Kumar AJ, Senthilanthan B, Ravichandiran V, A review
article on different types of floating drug delivery systems,
Int J PharmPharmSci, 4(1), 2012, 45-50.
8. Arunachalam A, Karthikeyan K, Kishore K, Prasad PH,
Sethuraman S, Ashuthoshkumar S, Manidipa S, Floating
drug delivery systems: A review, Int J Res Pharm Sci, 2(1),
2011, 76-83.
9. Yeole PG, Khan S, Patel VF, Floating drug delivery systems:
Need and development, Indian J Pharm Sci, 67(3), 2005, 265-
272.
10. Pattan SR, Wani NP, Shelar MU, Nirmal SA, Chaudhari PD,
Gude RS, Scope and significance of floating drug delivery
system, Indian Drugs, 49(10), 2012, 5-12.
11. Shweta A, Ali J, Ahuja A, Khar RK, Baboota S, Floating
drug delivery systems: Review, AAPS PharmSciTech, 6(3),
2005, E372- E390.
12. Shah SH, Patel JK, Patel NV, Stomach specific floating drug
delivery system: A review, Int J PharmTech Res, 1, 2009,
623–33.

Journal of Pharmacy Research Vol.11 Issue 2 February 2017
Raghavendra Kumar Gunda et al. / Journal of Pharmacy Research 2017,11(2),167-178
167-178
13. Prasad G, Rao GC, Studies on development and
characterization of gastro retentive drug delivery system
for antibiotics: Cefdinir, J Pharm Res, 6, 2013, 836-844.
14. Hasim H., Li W.P. A. Improving the release characteristics
of water-soluble drugs from hydrophilic sustained release
matrices by in situ gas generation. Inl J Pharm. 1987; 35,
201-206.
15. Krogel I., Bodlmeier R. Floating or pulsatile drug delivery
systems based on coated effervescent cores. Int J Pharm.
1999; 187(2), 175-184.
16. Srikanth MV, Vanitha A, Weeliang PH, Dharmalingam SR,
Ravi S, Adinarayana G, Preparation and in vitro
characterization of noneffervescent floating drug delivery
system of poorly soluble drugcarvedilol phosphate, Acta
Pharm, 64, 2014, 485-494.
17. Sato Y., Kawashima Y., Takeuchi H. In vitro and in vivo
evaluation of riboflavin-containing microballoons for a
floating controlled drug delivery systems in healthy humans.
Int J Pharm. 2004; 275, 97-107.
18. Kawashima, Y., Niwa, T., Takeuchi, H., Hino, T., Itoh, Y.,
Hollow microspheres: for use as a floating controlled drug
delivery system in the stomach, J Pharm Sci, 1992, 81, 135-
140.
19. Reddy LH, Murthy RS. Floating dosage system in drug
delivery. Crit Rev Ther Drug Carrier Syst 2002; 19(6): 553-
85.
20. Peppas N. A., Bures P., Leobandung W. Hydrogel in
pharmaceutical formulations. Eur J Pharm Sci. 2000; 50, 27-
46.
21. Oarke G. M., Newton J. M., Shon M. B. Comparative
gastrointestinal transit of pellet systems of varying density.
Int J Pharm. I995; 114 (1), 1-11.
22. Riner J. L., Byford R. L., Stratton L. G. Influence of density
and location on degradation of sustained-release boluses
given to cattle. Am J Vet Res. 1982; 43(ll), 2028-2030.
23. Seth, P.R., Tossounian, J., The hydrodynamically balanced
system: a novel drug delivery system for oral use, Drug
Dev Ind Pharm, 1984, 10, 313-339.
24. Wang K, He Z, Alginate konjacglucomannan chitosan beads
as controlled release matrix, Inter J Pharm, 244(1-2), 2002,
117-126.
25. Gupia P.,Vermani K., Garg S. Hydrogels from controlled
release to pH-responsive drug delivery. Drug Discov Today.
2002; 10, 369-379.
26. Klausner E. A., Lavy E., Friedman M. Expandable
gastroretentive dosage forms. J Cont Rel. 2003: 90, 14-62.
27. P. N. Murthy, Anjan K. Mahapatra, Tapan Kumar Nayak
and DiptanuDey. Formulation, characterization and drug
release kinetics of floating drug delivery systems. J. Chem.
Pharm. Res., 2015, 7(6):781-792.
28. Chen J., Blevins W. E., Park H. Gastric retention properties
of Superporous hydrogel composites. J Cont Rel. 2000; 64,
39-51.
29. Chen J., Park K. Synthesis and characterization of
superporous hydrogel composites. J Cont Rel. 2000; 65 (1-
2), 73-82.
30. Chavda H, Patel C, Chitosan super porous hydrogel
compositebased floating drug delivery system: A newer
formulation approach, J Pharm BioalliedSci, 2(2), 2010, 124–
131.
31. Atyabi F., Sharma H. L., Mohammad H. A. H. In vivo
evaluation of a novel gastric retentive formulation ba.sed
on ion exchange resins. J Cont Rel. 1996; 42 (2), 105-113.
32. Spandana ADS, Neelofar SS, Sabiya SS, Ramana BV,
Nagarajan G, Formulation and evaluation of bilayer floating
tablets of simvastatin and lovastatin, J Chem Pharm Res,
6(12), 2014, 186- 197.
33. Shaheen S, Sushma T, Devender S, Ahmad R, Venu M,
Aseem B, Ahmad FJ, An approach for lacidipine loaded
gastro retentive formulation prepared by different methods
for gastroparesis in diabetic patients, Saudi Pharm J, 21,
2013, 293-304.
34. Mina IT, Controlled-release effervescent floating matrix
tablets of ciprofloxacin hydrochloride: Development,
optimization and in vitro–in vivo evaluation in healthy
human volunteers, Europ J Pharm Biopharm, 74, 2010, 332-
339.
35. Harrigan, R.M., Drug delivery device for preventing contact
of un-dissolved drug with the stomach lining, US Patent
4,1977, 055, 178.
36. Rajamma AJ, Yoogesh HN, Sateesha SB, Natural gums as
sustained release carriers: development of gastro retentive
drug delivery system of ziprasidone HCl, DARU J Pharm
Sci, 20(1), 2012, 58.
37. Lehr C. M., Hass J. Development in the area of bio adhesive
drug delivery systems. Expert OpinBiolTher. 2002; 2, 287-
98.
38. Ponchel G., Irache J. M. Specific and non-specific
bioadhesive particulate systems for oral delivery to the
gastrointestinal tract. Adv Drug Del Rev. 1998; 34, 191-219.
39. Takeucbi H., Yamamoio H., Niwa T. Mucoadhesion of
polymer-coated liposomes to rat intestine in vitro. Chem
Pharm Bull. 1999; 42, 1954-1956.

Journal of Pharmacy Research Vol.11 Issue 2 February 2017
Raghavendra Kumar Gunda et al. / Journal of Pharmacy Research 2017,11(2),167-178
167-178
Source of support: nil ;Conflict of interest: None Declared
40. Arnold S. C., Ferritto M. S., Lenz R. W. PH dependent
modification of phospholipid vesicle membrane by poly
(carboxylic acid) bearing pendant cholesteryl esters. Poly
Prep. 1986; 27, 42-43.
41. Fabregas J., Claramunt J., Cucala J. In vitro testing of an
antacid formulation with prolonged gastric residence time
(AlmagateFlot-Coat). Drug Dev Ind Pharm. 1994; 20, 1199-
1212.
42. Washington N., Greaves J. L., Wilson C. G. Effect of time of
dosing relative to a meal on the raft formation anti-reflux
agenl. J Pharm Pharmacol. 1990; 42, 50-53.
43. Chaturvedi Shashank, KumariPrabha, Singh Sunil,
AgrawalVipinKumar.Approaches to increase the gastric
residence time: floating drug delivery systems- a review.
Asian j pharm clin res, 2013; 6(3):1-9.
44. Ushimaru K, Nakamichi K & Saito H, Pharmaceutical
preparations and a method of manufacturing them, US Pat
4, 702, 918, October 27, 1987.
45. Ozdemir N, Ordu S, Ozkan Y. Studies of floating dosage
forms of Furosemide: In- vitro and In vivo evaluations of
bilayer tablet formulations. Drug. Dev. Ind. Pharm. 2000;
857- 66.
46. Raghavendra Kumar Gunda. Formulation development and
evaluation of rosiglitazone maleate sustained release tablets
using 32factorial design. International J of PharmTech
Research, 2015; 8(4): 713-724.
47. HumeraAnjum, P. Sandhya, Shama Sultana, K. Someshwar.
Enhancement of Solubility of Poorly Soluble Drug Using
Drug Solution Dropping Technique.Int J Sci Res Pub, 2014;
Vol.4(2): 1-6 .
48. Rosa M, Zia H, Rhodes T. Dosing and testing In-Vitro of a
bioadhesive and floating drug delivery system for oral
application. Int J Pharm. 1994;105:65-70.
49. Brijesh S. Dave, Avani F. Amin,1 and Madhabhai M. Patel.
Gastroretentive Drug Delivery System of Ranitidine
Hydrochloride: Formulation and In Vitro Evaluation. AAPS
PharmSciTech2004; 5 (2) Article 34.
50. Raghavendra Kumar Gunda, J. N. Suresh Kumar, Chandan
Kumar Brahma, V. Satyanarayana, K. Naga Prashant.
Design, Formulation and Evaluation of Atenolol Gastro
Retentive Floating Tablets. Asian Journal of Pharmaceutics
2015 9 (4) (Suppl) S34-S42.
51. Raghavendra Kumar Gunda, J. N. Suresh Kumar, V.
Satyanarayana, K. V.Ramananjaneyulu, B.satyprasad.
Formulation Development and Evaluation of Carvedilol
Phopsphate Gastro Retentive Floating Tablets. International
Research Journal of Pharmacy 2016 7 (1) 44-51.
52. K.P.R.chowdary, optimization of valsartan tablet formulation
by 23 factorial design, J Glob Tren Pham Sci, 2014; 5(1):
1374-1379 .
53. Notari RE. Biopharmaceutics and clinical pharmacokinetics.
4th ed. New York: Marcel Dekker Inc; 1987. p. 6-21.
54. Higuchi T. Mechanism of sustained-action medication.
Theoretical analysis of rate of release of solid drugs
dispersed in solid matrices. J Pharm Sci 1963; 51:1145-9.
55. Peppas NA. Analysis of Fickian and non-Fickian drug release
from polymers. Pharm ActaHelv 1985; 60:110-1.
56. GundaRaghavendra Kumar, J.N.Suresh Kumar,
V.Satyanarayana, G.Swarupa Rani, B.Satya Prasad.
Formulation Development and Evaluation of Clopidogrel
Fast Dissolving Tablets. Iranian Journal of Pharmaceutical
Sciences, 2016: 12 (2): 61-74.
57. Raghavendra Kumar Gunda, J.N.Suresh Kumar, S.Jayakumari
,A.Vijayalakshmi, V.Satyanarayana. Formulation
Development and Evaluation of Risperidone Fast
Dissolving Tablets. Journal of Pharmacy Research,
2016,10(9):579-588.
58. Sato Y., Kawashima Y., Takeuchi H. In vitro and in vivo
evaluation of riboflavin-containing microballoons for a
floating controlled drug delivery systems in healthy humans.
Int J Pharm. 2004; 275, 97-107.
59. Kawashima, Y., Niwa, T., Takeuchi, H., Hino, T., Itoh, Y.,
Hollow microspheres: for use as a floating controlled drug
delivery system in the stomach, J Pharm Sci, 1992, 81, 135-
140.60. Kawashima Y, Niwa T, Takeuchi H, Hino T, Ito Y. Preparation
of multiple unit hollow microspheres (microballoons) withacrylic resins containing tranilast and their drug releasecharacteristics (in vivo). J Control Release. 1991; 16: 279-290.
61. Shah, S.H., Patel, J.K., Patel, N.V., Stomach specific floating
drug delivery system: a review, Int J PharmTech , 2009, 1(3),
628-629.
62. Narang N., An Updated Review On: Floating Drug Delivery
System (FDDS), Int J Advance Pharm, 2011, 3(1), 1-7.