
Form !990 Return of Organization Exempt From Income Tax...
12
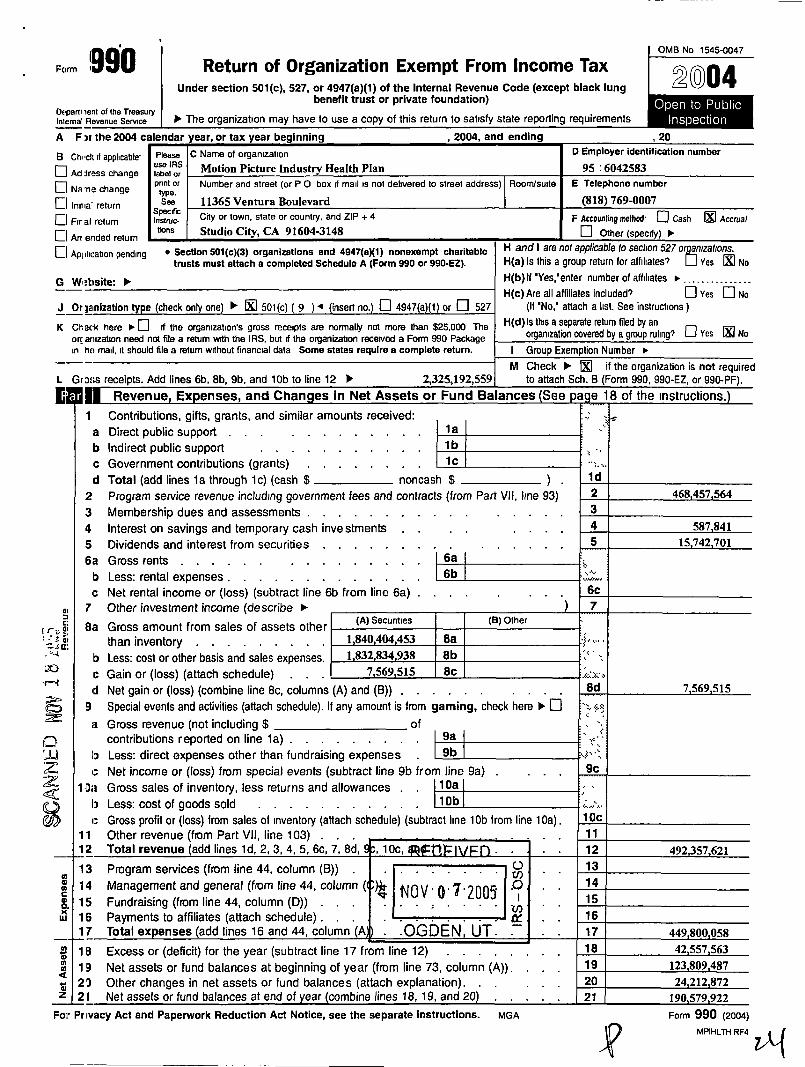
Form !990 Return of Organization Exempt From Income Tax Under section 501(c), 527, or 4947(a)(1) of the Internal Revenue Code (except black lung benefit trust or private foundation) Os~parti lent of the Treasury Internal Revenu e seMce t The organization may have to use a copy of this return to satisfy state r eporting requirements OMB No 1545-0047 2004 A F )r the 2004 calendar year, or tax year beginning , 2004, and ending B Chock ii applicable- Please C Name of organization use ias Motion Picture Industry Health Plan [l Ad ir~sss change label or D Employer identification number 95 :6042583 poor or Number and street (or P O box rf mail is not delivered to street address) RooMswte E Telephone number [l Na ra change [l inoia return See . 11365 Venture Boulevard (818) 769-0007 Specific Cit y or town, state or count ry' and ZIP + 4 F Accounting method 0 Cash 0 Accrual Fir al return ~~s~NC- Art ended return tin. Studio City, CA 91604-3148 ~~ D Other (speedy) [~ 10- Application pending * Section 501(c)(3) organizations end 4947(ex1) nonexempt charitable H and I eke not applicable t0 section 527 orga nizations . H(a) Is this a group return (or affiliates? LJ Yes ibi No H(b) I('Yes,'enter number of affiliates mi~ . .. . . . . . . ..... . H(c) Are all affiliates included O Yes El No (If 'No,' attach a list. See instructions ) H(d) Is this a separate return filed by an organization covered by a group rulings El Yes 0 N o I Group Exemption Number trusts must attach e completed Schedule A (Form 990 or 990-EZ) . J Or ja nization type (check only one) t R1 501(c) ( 9 ) 4 (insert no .) El 4947(a)(1) or El 527 K Ch erk here " D if the organization's gross receipts are normally not more than $25,000 The orr anization need not file a return with the IRS, but rf the organization received a Forth 990 Package in ho mail, it should file a return without financial data Some states require a complete return . --- M Check t Gross receipts . Add lines 6b, 8b, 9b, and 10b to line 12 t 2,325,192,559 to attach Sch . B if the organization is not required (Form 990, 990-EZ, or 990 .PF) . iR of iha inctriirtinnc 1 Revenue Ex p enses, and Chan ges in Net Assets or Fund Balances See 1 Contributions, gifts, grants, and similar amounts received : a Direct public support . . b Indirect public support . c Government contributions (grants) d Total (add lines is through ic) (cash $ noncash $ ) 2 Program service revenue including government fees and contracts (from Part VII, line 93) 3 Membership dues and assessments . . . . . . 4 Interest on savings and temporary cash investments 5 Dividends and interest from securities . . . . 6~a Gross rents . . . . . . . . . . . . , , , 6a b Less : rental expenses . . . . . . . . . . . , , 6b ~c Net rental income or (loss) (subtract line 6b from line 6a) . a, 7 Other investment income (describe 8.a Gross amount from sales of assets other (A) Securities (B) Other than inventory . . . . . . . . 1840 404 453 8a b Less : cost or ocher basis and sales expenses. 1832 834 938 Sb c Gain or (loss) (attach schedule) . . . 7, 569, 515 8c ~d Net gain or (loss) (combine line 8c, columns (A) and (B)) . 9 Special events and activities (attach schedule) . If any amount is from gaming, check here lo. [] ;3 Gross revenue (not including $ of contributions reported on line 1a) . to Less : direct expenses other than fundraising expenses . 9b c Net income or (loss) from special events (subtract line 9b from line 9a) 1 Da Gross sales of inventory, less returns and allowances . . 10a li Less: cost of goods sold . . . . . . . . . . . 10b c Gross profit or (loss) from sales of inventory (attach schedule) (subtract line 10b from line 10a) . 11 Other revenue (from Part VII, line 103) 12 Total revenue (add lines 1d, 2, 3, 4, 5, 6c, 7, 8d, , 10c, q 13 Program services (from line 44, column (B)) . . . . . . . .~ 14 Management and general (from line 44, column ( tr NOV-0-7-200 5 .O . . o, 15 Fundraising (from line 44, column (D)) . . . . , . . . ~ w 16 Payments to affiliates (attach schedule) . . . ~ . . ~ 17 Total ex penses (add lines 16 and 44, column (A .OLDEN UT . 18 Excess or (deficit) for the year (subtract line 17 from line 12) Q 19 Net assets or fund balances at beginning of year (from line 73, column (A)) . m 23 Other changes in net assets or fund balances (attach explanation) . z 21 Net assets or fund balances at end of year (combine lines 18, 19, and 20) Fov Privacy Act and Paperwork Reduction Act Notice, see the separate instructions . MGA 1d 2 3 4 5 6c 7 1 Form 990 (2004) `~ MPIHLTH RF4 ~ G W :tisite : lo- , ., 8d 10c 11 12 492,357 , 621 13 14 15 16 17 449 .800.058 20
Transcript of Form !990 Return of Organization Exempt From Income Tax...
Form !990 Return of Organization Exempt From Income Tax Under section 501(c), 527, or 4947(a)(1) of the Internal Revenue Code (except black lung
benefit trust or private foundation) Os~parti lent of the Treasury Internal Revenu e seMce t The organization may have to use a copy of this return to satisfy state reporting requirements
OMB No 1545-0047
2004
A F )r the 2004 calendar year, or tax year beginning , 2004, and ending
B Chock ii applicable- Please C Name of organization use ias Motion Picture Industry Health Plan [l Ad ir~sss change label or
D Employer identification number
95 :6042583 poor or Number and street (or P O box rf mail is not delivered to street address) RooMswte E Telephone number
[l Na ra change
[l inoia return See.
11365 Venture Boulevard (818) 769-0007 Specific City or town, state or country' and ZIP + 4 F Accounting method 0 Cash 0 Accrual Fir al return ~~s~NC-
Art ended return tin . Studio City, CA 91604-3148
~~ D Other (speedy)
[~
10-
Application pending * Section 501(c)(3) organizations end 4947(ex1) nonexempt charitable H and I eke not applicable t0 section 527 orga nizations . H(a) Is this a group return (or affiliates? LJ Yes ibi No H(b) I('Yes,'enter number of affiliates mi~ . . . . . . . . . . . . . . . H(c) Are all affiliates included O Yes El No
(If 'No,' attach a list. See instructions ) H(d) Is this a separate return filed by an
organization covered by a group rulings El Yes 0 No I Group Exemption Number
trusts must attach e completed Schedule A (Form 990 or 990-EZ).
J Or janization type (check only one) t R1 501(c) ( 9 ) 4 (insert no .) El 4947(a)(1) or El 527
K Ch erk here " D if the organization's gross receipts are normally not more than $25,000 The orr anization need not file a return with the IRS, but rf the organization received a Forth 990 Package in ho mail, it should file a return without financial data Some states require a complete return .
--- M Check t Gross receipts . Add lines 6b, 8b, 9b, and 10b to line 12 t 2,325,192,559 to attach Sch . B
if the organization is not required (Form 990, 990-EZ, or 990.PF) . iR of iha inctriirtinnc 1 Revenue Expenses, and Chan ges in Net Assets or Fund Balances See
1 Contributions, gifts, grants, and similar amounts received : a Direct public support . . b Indirect public support . c Government contributions (grants) d Total (add lines is through ic) (cash $ noncash $ )
2 Program service revenue including government fees and contracts (from Part VII, line 93) 3 Membership dues and assessments . . . . . . 4 Interest on savings and temporary cash investments 5 Dividends and interest from securities . . .
. 6~a Gross rents . . . . . . . . . . . . , , , 6a b Less : rental expenses . . . . . . . . . . . , , 6b ~c Net rental income or (loss) (subtract line 6b from line 6a) .
a, 7 Other investment income (describe
8.a Gross amount from sales of assets other (A) Securities (B) Other
than inventory . . . . . . . . 1840 404 453 8a b Less : cost or ocher basis and sales expenses. 1832 834 938 Sb c Gain or (loss) (attach schedule) . . . 7,569,515 8c ~d Net gain or (loss) (combine line 8c, columns (A) and (B)) .
9 Special events and activities (attach schedule) . If any amount is from gaming, check here lo. [] ;3 Gross revenue (not including $ of
contributions reported on line 1a) . to Less : direct expenses other than fundraising expenses . 9b
c Net income or (loss) from special events (subtract line 9b from line 9a) 1 Da Gross sales of inventory, less returns and allowances . . 10a
li Less: cost of goods sold . . . . . . . . . . . 10b c Gross profit or (loss) from sales of inventory (attach schedule) (subtract line 10b from line 10a) .
11 Other revenue (from Part VII, line 103) 12 Total revenue (add lines 1d, 2, 3, 4, 5, 6c, 7, 8d, , 10c,
q 13 Program services (from line 44, column (B)) . . . . . . . .~ 14 Management and general (from line 44, column ( tr NOV-0-7-200 5 .O . . o, 15 Fundraising (from line 44, column (D)) . . . . , . . . ~
w 16 Payments to affiliates (attach schedule) . . . ~ . . ~ 17 Total expenses (add lines 16 and 44, column (A .OLDEN UT . 18 Excess or (deficit) for the year (subtract line 17 from line 12)
Q 19 Net assets or fund balances at beginning of year (from line 73, column (A)) . m 23 Other changes in net assets or fund balances (attach explanation) . z 21 Net assets or fund balances at end of year (combine lines 18, 19, and 20) Fov Privacy Act and Paperwork Reduction Act Notice, see the separate instructions . MGA
1d 2 3 4 5
6c 7
1
Form 990 (2004) `~ MPIHLTH RF4 ~
G W:tisite : lo-
, ., 8d
10c 11 12 492,357 ,621 13 14 15 16 17 449.800 .058
20
------------------- ----------------------------------------------------------------------------------------------------(Grants and allocations $ )
MPIHLTH RF4
Form 350 (2004) EIIY 95-6042583 Page 2
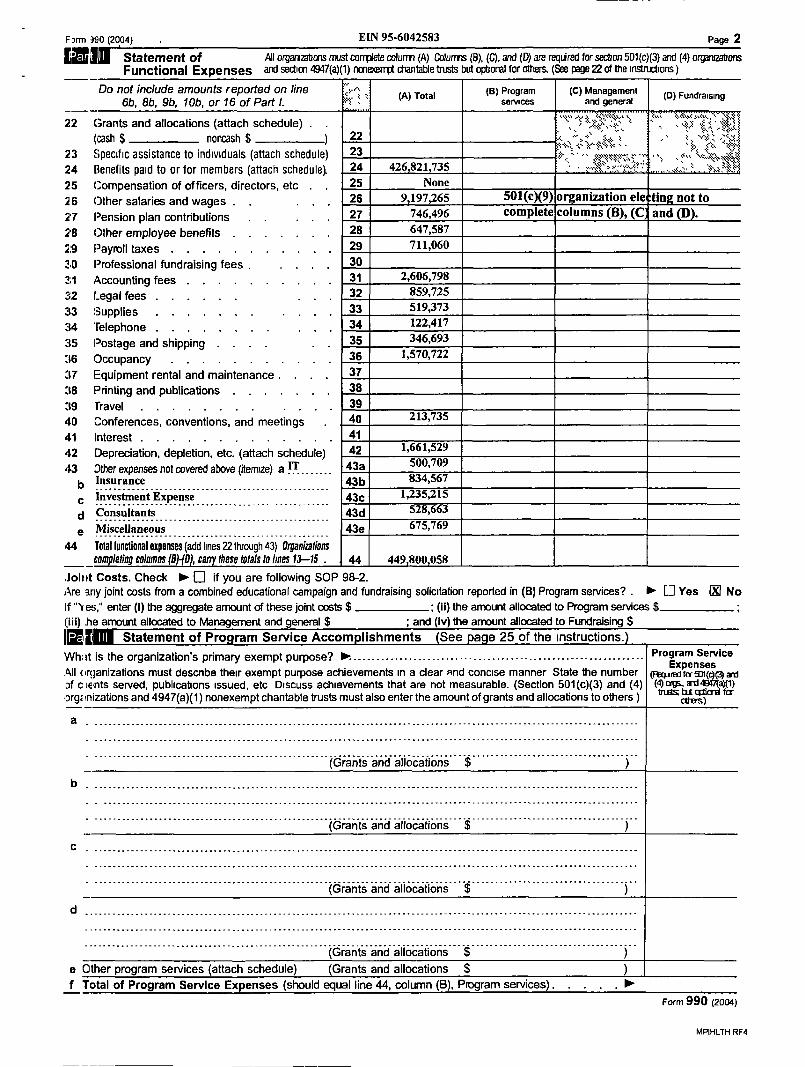
Statement of All organizations must complete column (A) Columns (B), (L), and (D) are required for section 501(c)(3) and (4) org3n¢ahons Functional Expenses and section 4sa7(a)(1) nmexerrFt chantable trusts but optional for omens. (see page 22 of me instructions)
Do not include amounts reported on line {r " (a) Program (c) Management 6b, 8b, 9b, 10b, or 16 of Part l.
(A) Total sennces and general (D) Fundraising
--- y s is;+Yi~,1 v , %1kt ;YS s
22 (rants and allocations (attach schedule) . . v~k, ; ; " , (cash $ noncash $ ~ 22 "" ` ` "' l "',~2
23 Specific assistance to individuals (attach schedule) 23 , ~~<
4 Benefits paid to or for members (attach schedule} 24 426,821,735 25 Compensation of officers, directors, etc . . 25 None 26 ether salaries and wages . . , , , 26 9,197,265 501(c)(9) organization electing not to 2'7 Pension plan contributions . . . , , 27 746,496 complete columns (B), (C and 2'B ether employee benefits . . . . , , , 28 647,587
2:9 Payroll taxes . . . . . . . . . . , 29 711,060
?.0 Professional fundraising fees . . , , , 30
2;1 accounting fees . . . . . . . , , , 31 2,606,798
:c2 Legal fees . . . . . . 32 859,725
:t3 Supplies . . . . . . . . . , , 33 519,373
:t4 'telephone . . . . . 34 122,417
:t5 Postage and shipping . . . . , . 35 346,693
:t6 Occupancy . . . . , . . , . . , 36 1,570,722
;t7 Equipment rental and maintenance . . . . 37
;t8 printing and publications ;t9 Travel . . . . . . . . . . . . 39 <<0 Conferences, conventions, and meetings 40 213,735
41 X41 Interest . . . 42 Depreciation, depletion, etc. (attach schedule) 42 1,661,529
43 Other expenses not covered above (itemize) a IT . . . . . . . 43a 500,709 Insurance 43b 834,567 ------------------------------~-------------------- Investment Expense 43c 1,235,215
-------------------- -----~------ Consultants 43d 528,63
Miscellaneous 43e 675,769
44 Total functional expenses (add lines 22 through 43) Organizations com le6ng columns /9 -/D , ca these totals fu lines 13-15 . 44 449,800,058
,loliit Costs. Check t El if you are following SOP 98-2 . Are any joint costs from a combined educational campaign and fundraising solicitation reported in (B) Program services? . t El Yes (K No If "Y mss;" enter (I) the aggregate amount of these joint costs $ ; (ii) the amount allocated to Program services $ I;iii) he amount allocated to Management and general $ ; and (iv) the amount allocated to Fundraising $
Statement of Program Service Accomplishments See page 25 of the instructions . What is the organization's primary exempt purpose? R . . . . .__ . . . . . . ._ ._ . . . . . ._ . . . . . . . . . . . ._ .__ . . . . . . ._ . . . . . . . . . . . . . . . Program Service
,411 organizations must describe their exempt purpose achievements in a clear and concise manner State the number Expenses
for ~~f c ie~nts served, publications issued, etc Discuss achievements that are not measurable. (Section 501(c)(3) and (4) (~~. ~ff(~) org: inizations and 4947(a)(1) nonexempt charitable trusts must also enter the amount of grants and allocations to others ) °'~ b" C11' 'tr
(Grants and allocations $ )
(Grants and allocations $ )
(Grants and allocations $ )
--------------------------------------------- --------------------------------------------------------------------------
e Other program services (attach schedule) (Grants and allocations $ ) f Total of Program Service Expenses (should equal line 44, column (B), Program services) . . , t
Form 990 (2004)
Form 990 (2004) EIN 95-6042583 Page 3
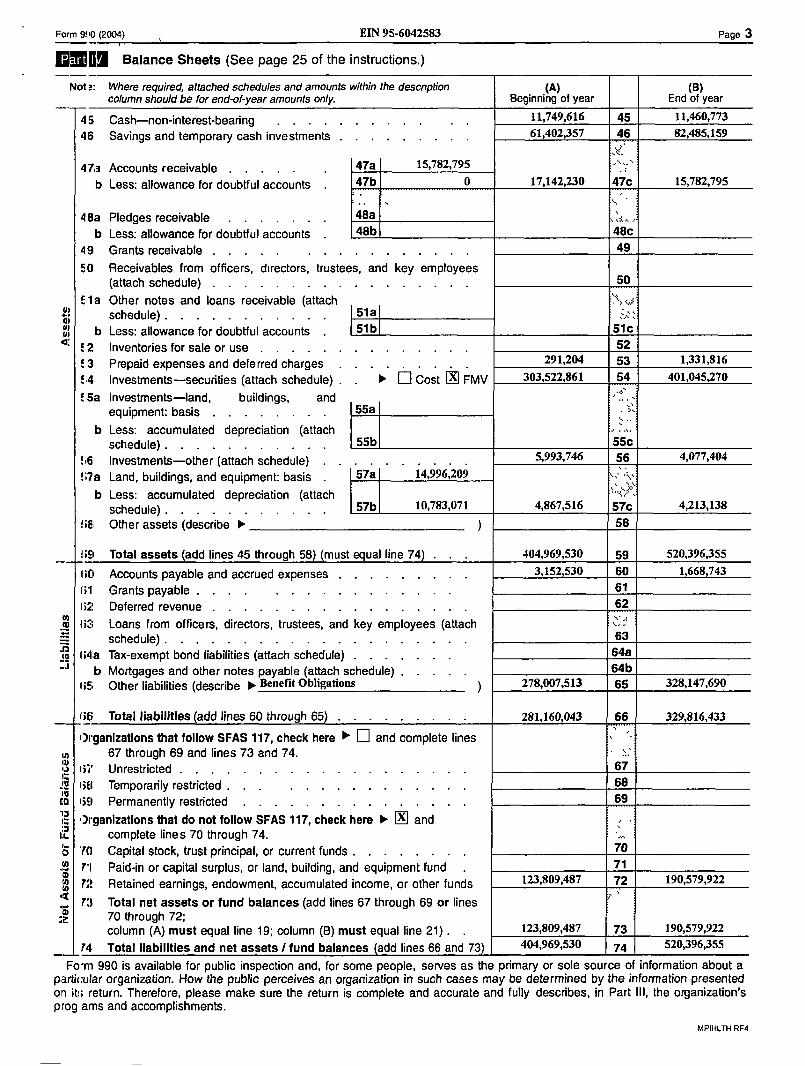
Balance Sheets (See page 25 of the instructions .)
Not' : Where required, attached schedules and amounts within the descnption (A) (B) column should be for end-of-year amounts only. Beginning of year End of year
45 Cash-non-interest-bearing . . . . . . . . . . . . 11,749,616 45 11,460,773
46 Savings and temporary cash investments . . . . . . . . . 61,402,357 46 82,485,159
47.a Accounts receivable . . . . . 47a 15,782,795 _ .
b Less : allowance for doubtful accounts . 47b 0 17,142,230 47c 15,782,795
48a Pledges receivable . . . . . . . 48a s , :k .. .
b Less : allowance for doubtful accounts . 48b 48c 49 Grants receivable . . . . . . . . . . . . . . . . 49 50 Receivables from officers, directors, trustees, and key employees
50 (attach schedule) . . . . . . . f 1 a Other notes and loans receivable (attach
schedule) . 51a a~ . . . . . . . . . . , . b Less : allowance for doubtful accounts . 51b Sic~
.° 2 Inventories for sale or use . . . . E 3 Prepaid expenses and deferred charges . . . . , , 291,204 53 1,331,816
°, 4 Investments-securities (attach schedule) . . t ~ Cost IN FMV 303 ,522,861 54 401,045,270
'.5a Investments-land, buildings, and . . equipment: basis . . . . . . . , 55a
b Less : accumulated depreciation (attach schedule) . . . . . . . . . . , 55b 55c
E,6 Investments-other (attach schedule) . . .
. , , , . . 5,993,746 56 4,077,404
'. .7a Land, buildings, and equipment: basis . 57a 14,996,209
b Less : accumulated depreciation (attach schedule) . . . . . . . . , . , 57b 10,783,071 4,867,516 57c 4,213,138
68 Other assets (describe t ) 58
59 Total assets (add lines 45 through 58 (must equal line 74) . 404,969,530 59 520,396,355
li[i Accounts payable and accrued expenses . . . . . . . . , 3,152,530 60 1,668 743 i;1 Grants payable . . . . . . ire : Deferred revenue . . . . . . .
iu ii2+ Loans from officers, directors, trustees, and key employees (attach =r schedule) . . . . . . . . . . . . . . . . . . . . 63
Io li41a Tax-exempt bond liabilities (attach schedule) . . . . . . . 64a
b Mortgages and other notes payable (attach schedule) . . . . . 64b 65 Other liabilities (describe t Benefit Obligations ~ 278,007,513 65 328,147,690
ii6 Total liabilities add lines 60 through 65) . 281,160,043 66 329,816,433
Organizations that follow SFAS 1'17, check here ~ 0 and complete lines �, 67 through 69 and lines 73 and 74 .
67 ii' Unrestricted . . . . . . . . . a lift Temporarily restricted . . . . 68
ca I iEl Permanently restricted . . . . . . . . . . . . . . . 69
12 Organizations that do not follow SFAS 117, check here t D and complete lines 70 through 74 .
~~ '10 Capital stock, trust principal, or current funds . 70
ail Paid-in or capital surplus, or land, building, and equipment fund 71
14 F:! Retained earnings, endowment, accumulated income, or other funds 123,809,487 72 190,579,922 10 7;f Total net assets or fund balances (add lines 67 through 69 or lines
70 through 72 ; column (A) must equal line 19 ; column (B) must equal line 21) . . 123,809,487 73 190,579,922
ICI Total liabilities and net assets / fund balances add lines 66 and 73 404,969,530 74 520,396,355
Fo~m 990 is available for public inspection and, for some people, serves as the primary or sole source of information about a particular organization . Flow the public perceives an organization in such cases may be determined by the information presented on it, return . Therefore, please make sure the return is complete and accurate and fully describes, in Part III, the organization's prog ams and accomplishments .
MPIHLTH RR
Page 4 EIN 95-6042583 Form 991 (2004)
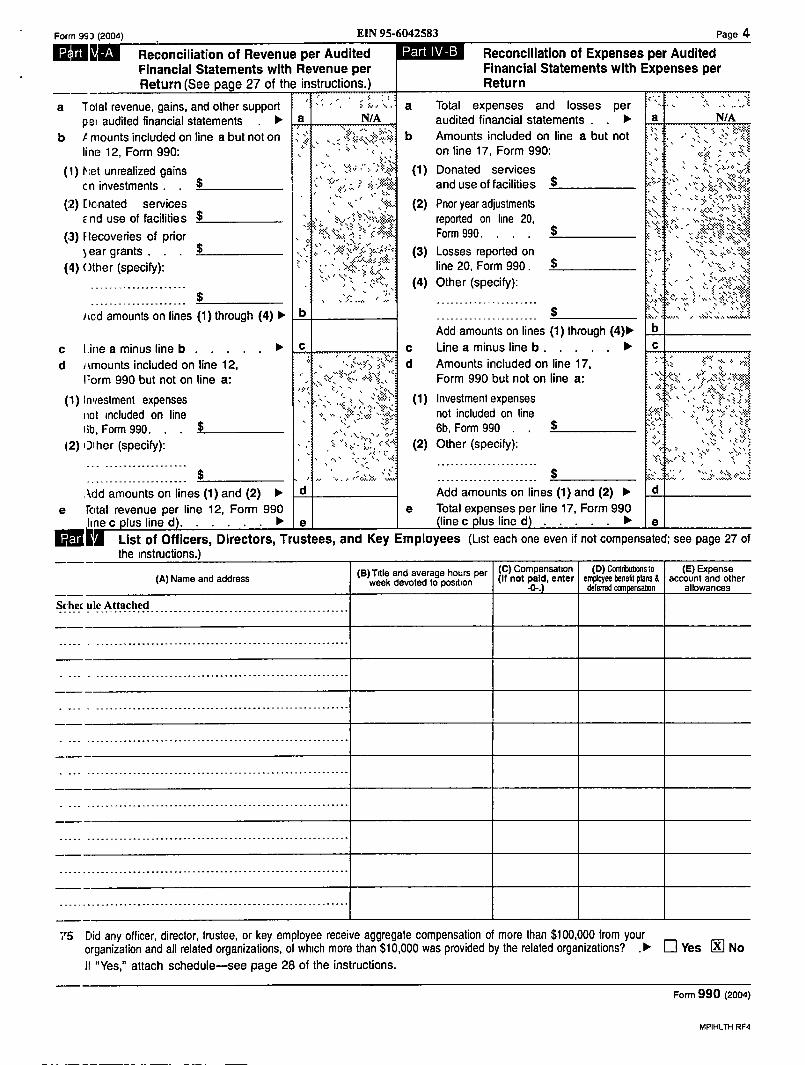
Reconciliation of Revenue per Audited Financial Statements with Revenue per Return (See page 27 of the instructions .)
a 1olal revenue, gains, and other support ` > N " " a peg audited financial statements . t a N/A
b A mounts included on line a but not on ; ~fi " '{{v~vN.` > b li no 12, Form 990 : , ' ` k
( 1 ) Net unrealized gains v c n investments . . $
(2) Donated services " " '7 .,`~hr End use of facilities $
(.3) Fte:coveries of prior % :~~ >" ear grants . . . $ ;{~%' f",; ° :'{
sil\~. (4) ()they (specify) :
--------------------- $ , ,J . k. . ., h .,
Total expenses and losses per audited financial statements . , t a N/A Amounts included on line a but not `" #`k on line 17, Form 990:
(1) Donated services and use of facilities ;
(2) Prior year adjustments '' . . %
reported on line 20, ` ~{sx{n`f ~~ Form 990. . . . ~ ~ ̀~'' `11
(3) Losses reported on ;~. .` line 20, Form 990 . $ " " (4) Other (specify) : , ``fi;;` ti` ; . ~ } .askT~
. . . . . . . . . . . . . . . . . . . . . . srJ\ s\r yr ~ ~%s .'sRsi
----------------------i~cld amounts on lines (1) through (4) lo. b $ ~ } ~ ~ . Add amounts on lines (1) through (4)t yb . `u
c Line a minus line b . . . . . Line a minus line b . . . . . t . `~ ` ' ~~~{ d ikrnounts included on line 12, " d Amounts included on line 17, ; ,
Form 990 but not on line a: ~" r ~.k:;nk~, Form 990 but not on line a: `, s
(1) Investment expenses ; (1) Investment expenses . ..kA. : : iiot included on line °not included on line
y,`'f5 6b, Form 990 $ " ~ :, iib, Form 990 . 12) 0iher (specify) : . , f ..̀.r{r. (2) Other (specify) :
v usss" , _ _ _ _ _ in K ,v " ! bx4\s,i
,acid amounts on lines (1) and (2) t d Add amounts on lines (1) and (2) t e total revenue per line 12, Form 990 e Total expenses per line 17, Form 990
line c plus line d . . . 11', e line c plus line d t e List of Officers, Directors, Trustees, and Key Employees (List each one even if not compensated ; see page 27 of the instructions.)
(B) Tdle and average hours per I (C) Compensation I (D) CoMnbwons to I (E) Expense week devoted to position (11 not paid, enter employee benefd plans d account and other
-0-.) deterred cancensation allowances
MPIHLTH RF4
Reconciliation of Expenses per Audited Financial Statements with Expenses per Return
(A) Name and address
Srhec ule Attached ----- - -------------------------------------------------------
.'S [lid any officer, director, trustee, or key employee receive aggregate compensation of more than $100,000 from your organization and all related organizations, of which more than $10,000 was provided by the related organizations? . 10- 0 Yes Dil No II "Yes," attach schedule-see page 28 of the instructions .
Form 990 (2004)
Fomi 99ii (2004) EIN 95-6042583
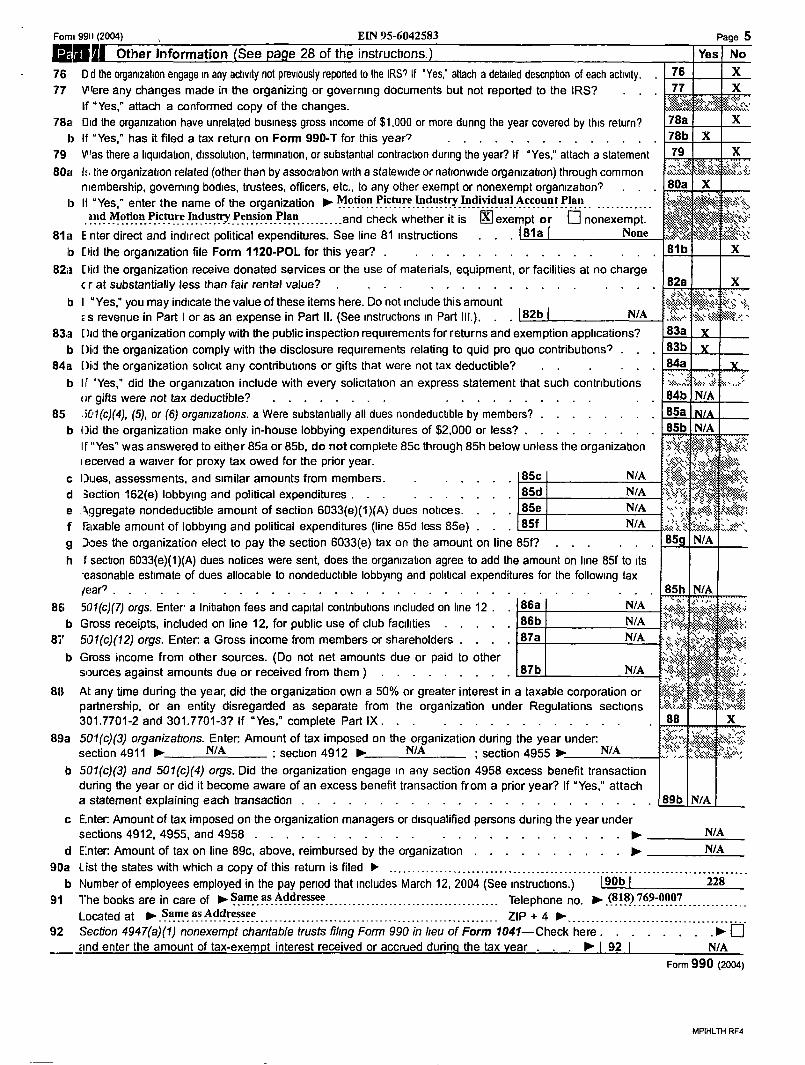
Egli Other Information (See page 28 of the instructions .)
76 D d the organization engage in any activity not previously reported to the IRS If "Yes," attach a detailed description of each activity . 77 Vlere any changes made in the organizing or governing documents but not reported to the IRS?
If "Yes," attach a conformed copy of the changes. 78a Did the organization have unrelated business gross income of $1,000 or more dunng the year covered by this return?
t) If "Yes," has it filed a tax return on Form 990-T for this years . . . 79 Was there a IiqwdaUon, dissolution, termination, or substantial contraction during the yeah? If "Yes ;" attach a statement 80a I: . the organization related (other than by association with a statewide or nationwide organization) through common
membership, governing bodies, trustees, officers, etc., to any other exempt or nonexempt orgarnzahon? 13 11 "Yes," enter the name of the organization t Motion Picrure_Industry Individual Account Plan
and Motion- Picture
- - Indus Pen-- sion -Plan . . . . . . . . . . and check whether it is 0 exempt or [] nonexempt. ---------------- ̀ '=?' - --- - 81a E nter direct and indirect political expenditures. See line 81 instructions . . . 181a I None
to Did the organization file Form 1120-POL for this year? . . . . . 82a Did the organization receive donated services or the use of materials, equipment, or facilities at no charge
c r at substantially less than fair rental value? . . . . . . . b I "Yes," you may indicate the value of these items here . Do not include this amount
s s revenue in Part I or as an expense in Part II . (See instructions m Part III .) . . . I 82b ~ N/A
83,a Did the organization comply with the public inspection requirements for returns and exemption applications? b [)id the organization comply with the disclosure requirements relating to quid pro quo contribudons? .
84a [)id the organization solicit any contributions or gifts that were not tax deductible? b If 'Yes," did the organization include with every solicitation an express statement that such contributions
or gifts were not tax deductible? . . . . . . . . . 85 .iU1(c)(4), (5), or (6) organizations. a Were substantially all dues nondeductible by members? .
b Did the organization make only in-house lobbying expenditures of $2,000 or less? . If "Yes" was answered to either 85a or 85b, do not complete 85c through 85h below unless the organization i eceived a waives for proxy tax owed for the prior year .
c Dues, assessments, and similar amounts from members . . . . , , 85c N/A
d 3ection 162(e) lobbying and political expenditures . . . . . . . . , , 85d N/A
e Aggregate nondeductible amount of section 6033(e)(1)(A) dues notices . . , , 85e N/A
f raxable amount of lobbying and political expenditures (line 85d less 85e) . . , 85f N/A
g does the organization elect to pay the section 6033(e) tax on the amount on line 85f? h f section 6033(e)(1)(A) dues notices were sent, does the organization agree to add the amount on line 85f to its
seasonable estimate of dues allocable to nondeductible lobbying and poliUcal expenditures for the following tax /ear? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
BE ; 501(c)(7) orgs. Enter a Initiation fees and capital contributions included on line 12 . . 86a N/A b Gross receipts, included on line 12, for public use of club facilities . . , , . 86b N/A
81' S01(c)(12) orgs . Enter: a Gross income from members or shareholders . . . . 87a N/A
b Gross income from other sources. (Do not net amounts due or paid to other sources against amounts due or received from them ) . . . . . . . . . 87b N/A
MPIHLTH RF4
Page 5 Yes No
76 X 77 X
78a %X 78b X 79 X
80a / X +
.,,
81b X
82a X
83a .s 83b 84a
84b N/A 85a 85b N/A V~;~ ; s#s~; ,
'` . z~ a:
L,h v\,i~s nvk,;{Sn ss ~ss,
813 At an time during the ear, did the or aniza6on own a 50% or greater interest in a taxable corporation or partnership, or an entity disregarded as separate from the organization under Regulations sections ;":~% 301 .7701-2 and 301 .7701-3? If "Yes," complete Part IX . . . . . . . . . . . . . . . , SB X
89a 501(c)(3) organizations . Enter. Amount of tax imposed on the organization during the year under. section 4911 t NBA ; section 4912 t N/A ; section 4955 t NBA "$``' ̀ ;~~`~~ ` ? J.,
,b 501(c)(3) and 501(c)(4) orgs. Did we organization engage in any section 4958 excess benefit transaction during the year or did it become aware of an excess benefit transaction from a prior year? If "Yes," attach a statement explaining each 6ransac6on . . . . . . . . . . . . . . . . . . . . . . . 89b N/A
c Enter. Amount of tax imposed on the organization managers or disqualified persons during the year under sections 4912, 4955, and 4958 . . . . . . . . . . . . . . . . . . . . . . . ~ N/A
d Enter: Amount of tax on line 89c, above, reimbursed by the organization . . . . . . . . . . 1 N/A 90a List the states with which a copy of this return is filed t __ . .__________, .___ . .__. ._________ ._____ . ._ .__ . . ._____ . ._ . .__. ..___ ._ . . .__ . .,_ b dumber of employees employed in the pay period that includes March 12, 2004 (See instructions .) 190b 1 228
91 The books are in care of t Same as Addressee-------------------- ------------------------------------
_ _ Telephone no . t (g 18)_769-0007 Located at jo. .Same as Addressee -----------------~--------- ZIP + 4 t. .------------------------------------
92 :iection 4947(a)(1) nonexempt charitable trusts filing Form 990 in lieu of Form 7041-Check here . . . . . . . .1 `- rind enter the amount of tax-exempt interest received or accrued during the tax year . . 111". 1 92 1 N/A
Form 990 (2004)
c d e
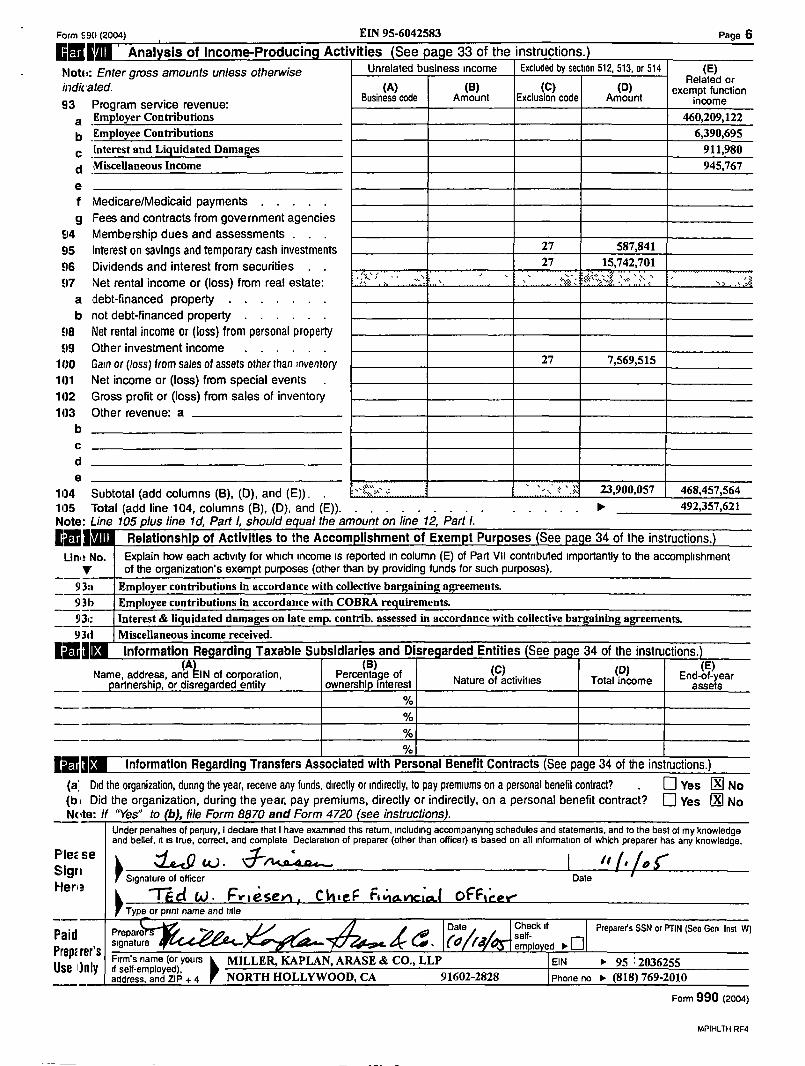
11)4 Subtotal (add columns (B), (D), and (E)) . . 4 . . . . . . . . . . . . ..~ I . . . .~ . . .~. :.~ . .~. .~.~^~ 23,900,057 468,457,564 1i)5 Total (add line 104, columns (B), (D), and (E)) . . . . . . . . . . . . . . t 492,357,621 Note : Line 105 plus line 1d, Part l, should equal the amount on line 12, Part l.
Relationship of Activities to the Accomplishment of Exempt Purposes See page 34 of the instructions .
Llrn : No . Explain how each activity for which income is reported in column (E) of Part VII contributed importantly to the accomplishment of the organization's exempt purposes (other than by providing funds for such purposes) .
93a Employer contributions in accordance with collective bargaining agreements. 931 Employee contributions in accordance with COBRA requirements. 93c Interest & liquidated damages on late emp. contrib . assessed in accordance with collective bargaining agreements. 9311 Miscellaneous income received .
Information Regarding Taxable Subsidiaries and Disregarded Entities See page 34 of the instructions .
Name, address, and EIN of oannershio. or disregard
JZ IM Information Regarding Transfers Associated with Personal Benefit Contracts (See page 34 of the instructions .) (a; Did the organization, during the year, receive any funds, directly or indirectly, to pay premiums on a personal benefit contract? E] Yes IN No (b i Did the organization, during the year, pay premiums, directly or indirectly, on a personal benefit contract? [] Yes N No Note : 11 "Yes" to (b ,file Form 8870 and Form 4720 see instructions).
Under penalties of penury, I declare that I have examined this return, including accompanying schedules and statements, and to the best of my knowledge and belief, d is true, correct, and complete Declaration of preparer (other than officer) is based on all information of which preparer has any knowledge .
.~l n w . ~~~ ReE se ~~cY Sign ' Signature of officer Date
Hen? Td W . Friesev%, C11,eF Ahamiad OFFtcer
Type or print name and idle
Paid Prepare ~r Date Suck signature em'lo~ Prep ~E I~ S Firm's name (or yours' MILLER, KAPLAN, ARASE & CO., LLP
CSC ~hIl JI it self-employed), address, and ZIP + 4 NORTH HOLLYWOOD, CA 91602-2828
Preparers SSN or PTIN (See Gen Inst W)
EIN 11. Phone no 11- (818) 769-2010
MPIHLTH RR
Form f 90 (2004) EIN 95-6042583 Page 6
Analysis of Income-Producing Activities See page 33 of the instructions.
MotEi : Enter gross amounts unless otherwise Unrelated business income Excluded by section 512, 513, or 514 (E) Related or
indicated. (A) (B) (C) (D) exempt function 93 Program service revenue :
Business code Amount Exclusion code Amount income Employer Contributions 460,209,122 Employee Contributions 6,390,695 interest and Liquidated Damages 911,980 Miscellaneous Income 945,767
e f Medicare/Medicaid payments g Fees and contracts from government agencies
94 Membership dues and assessments . E15 Interest on savings and temporary cash investments 27 587,841
fl6 Dividends and interest from securities . . 27 15,742,701
97 Net rental income or (loss) from real estate :
7
a debt-financed property b not debt-financed property
98 Net rental income or (loss) from personal property E19 Other investment income
1()0 Gain or (loss) from sales of assets other than inventory 27 7,569,515
11)1 Net income or (loss) from special events 11)2 Gross profit or (loss) from sales of inventory 11)3 Other revenue: a
b
(C' I (°' of . Nature of activities Total income
Form 990 (2004)
Proceeds From Sale or
Redemption Carry Gain or Value (Loss)
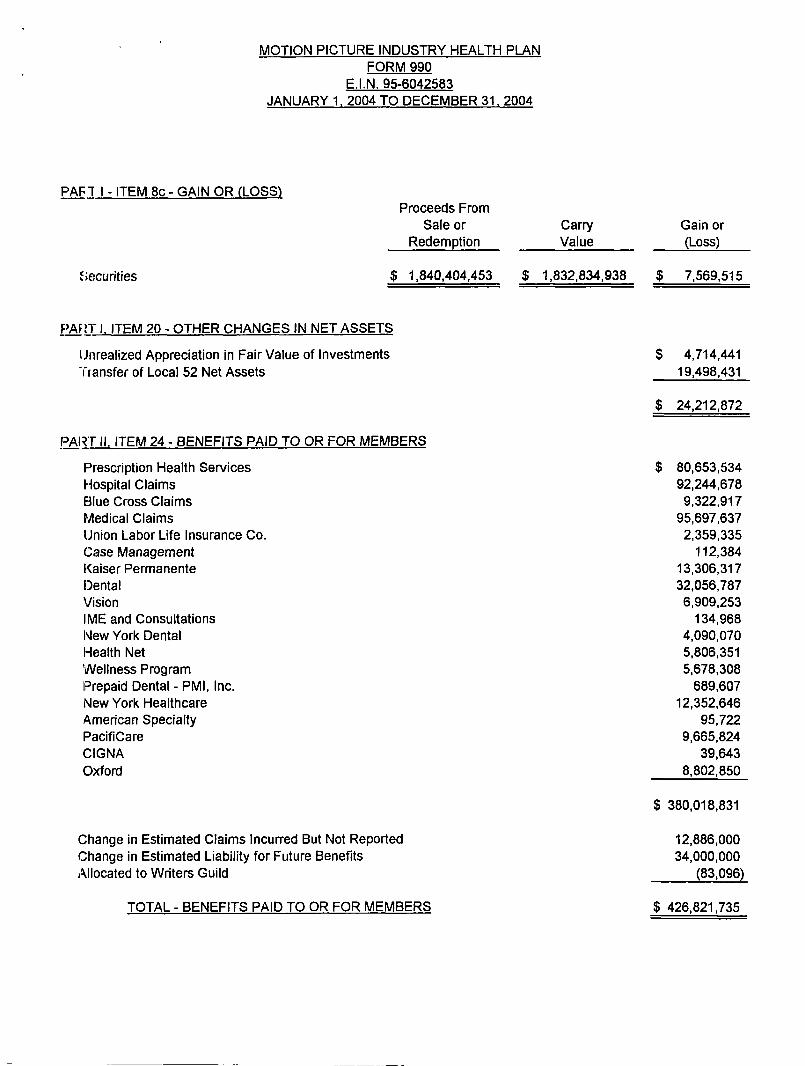
$ 1,840,404,453 $ 1,832,834,938 $ 7,569,515 Se:curities
TOTAL - BENEFITS PAID TO OR FOR MEMBERS $ 426,821,735
MOTION PICTURE INDUSTRY HEALTH PLAN FORM 990
E.I .N . 95-6042583 JANUARY 1, 2004 TO DECEMBER 31, 2004
PAF 7 I - ITEM 8c - GAIN OR (LOSS)
PART l . ITEM 20 - OTHER CHANGES IN NET ASSETS
Unrealized Appreciation in Fair Value of Investments $ 4,714,441 "transfer of Local 52 Net Assets 19,498,431
$ 24,212,872
PART II, ITEM 24 - BENEFITS PAID TO OR FOR MEMBERS
Prescription Health Services $ 80,653,534 Hospital Claims 92,244,678 Blue Cross Claims 9,322,917 Medical Claims 95,697,637 Union Labor Life Insurance Co. 2,359,335 Case Management 112,384 Kaiser Permanente 13,306,317 Dental 32,056,787 Vision 6,909,253 IME and Consultations 134,968 New York Dental 4,090,070 Health Net 5,806,351 Wellness Program 5,678,308 (Prepaid Dental - PMI, Inc. 689,607 New York Healthcare 12,352,646 American Specialty 95,722 PacifiCare 9,665,824 CIGNA 39,643 Oxford 8,802,850
$ 380,018,831
change in Estimated Claims Incurred But Not Reported 12,886,000 Change in Estimated Liability for Future Benefits 34,000,000 Allocated to Writers Guild (83,096)
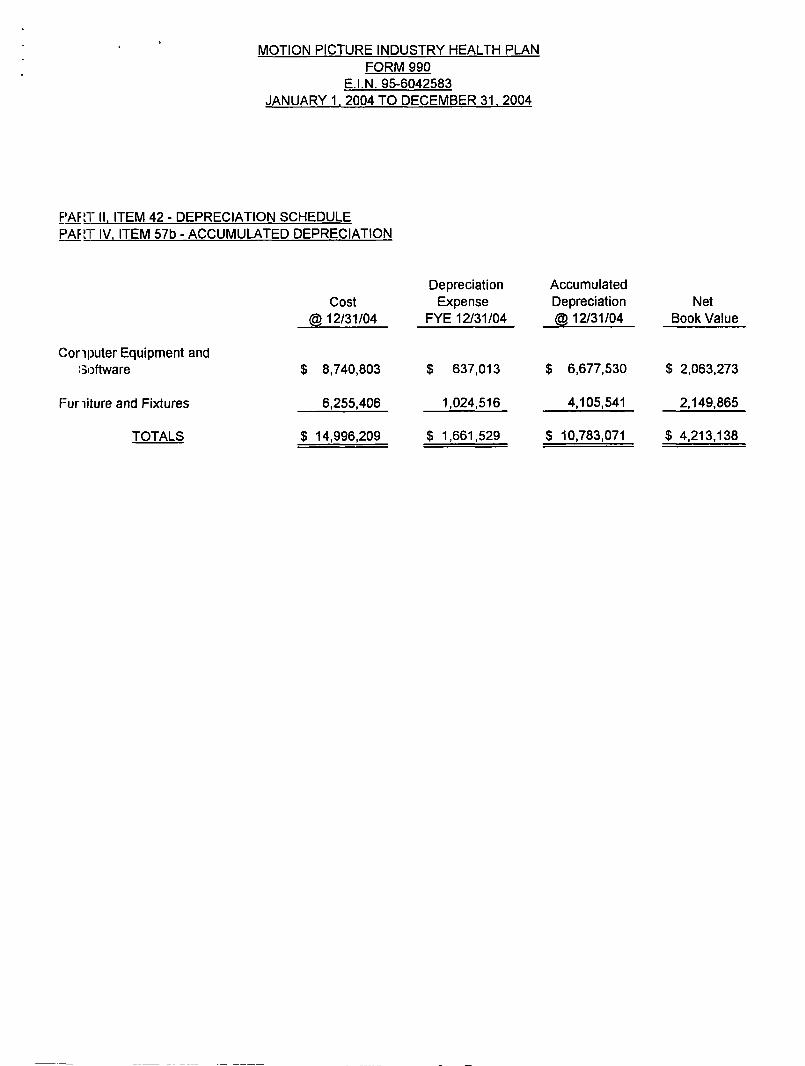
PART II . ITEM 42 - DEPRECIATION SCHEDULE F'AF;1" IV . ITEM 57b - ACCUMULATED DEPRECIATION
1,024,516 4,105,541 2,149,865
$ 1,661,529 $ 10,783,071 $ 4,213,138
F=uriiture and Fixtures 6,255,406
TOTALS $ 14,996,209
MOTION PICTURE INDUSTRY HEALTH PLAN FORM 990
E.I .N . 95-6042583 JANUARY 1, 2004 TO DECEMBER 31, 2004
Cost cGD 12/31/04
C:oriputer Equipment and :3oftware $ 8,740,803
Depreciation Accumulated Expense Depreciation Net
FYE 12/31/04 @ 12/31/04 Book Value
$ 637,013 $ 6,677,530 $ 2,063,273
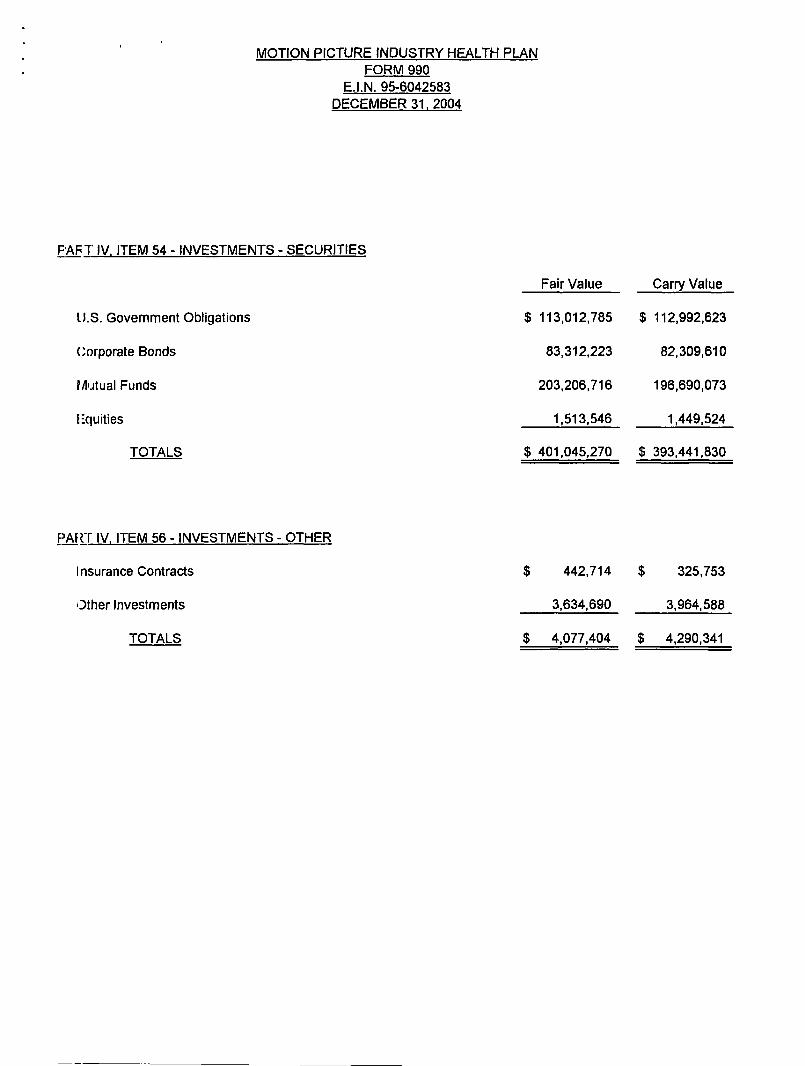
FAIR 7' IV, ITEM 54 - INVESTMENTS - SECURITIES
PAR-f IV . ITEM 56 - INVESTMENTS - OTHER
Insurance Contracts
Other Investments
TOTALS
$ 442,714 $ 325,753
3,634,690 3,964,588
$ 4,077,404 $ 4,290,341
MOTION PICTURE INDUSTRY HEALTH PLAN FORM 990
E.I . N . 95-6042583 DECEMBER 31, 2004
11.S . Government Obligations
Corporate Bonds
PAutual Funds
Equities
TOTALS
Fair Value Carry Value
$ 113,012,785 $ 112,992,623
83,312,223 82,309,610
203,206,716 196,690,073
1,513,546 1,449,524
$ 401,045,270 $ 393,441,830
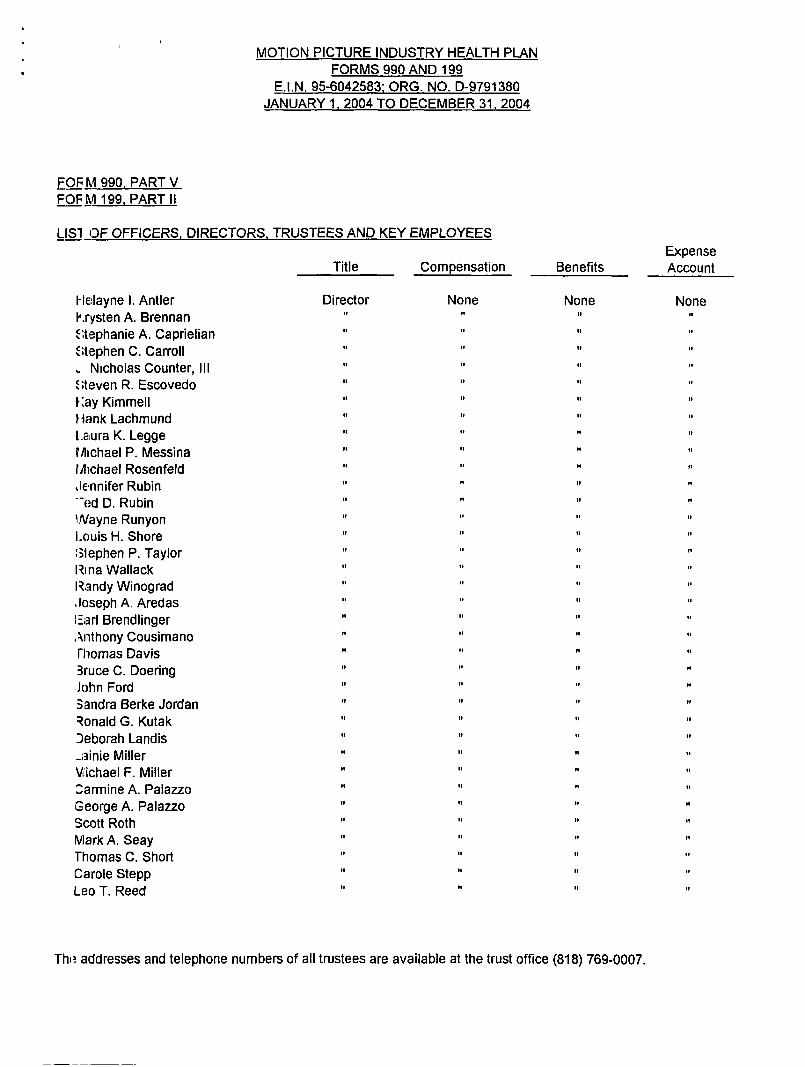
Tho addresses and telephone numbers of all trustees are available at the trust office (818) 769-0007 .
MOTION PICTURE INDUSTRY HEALTH PLAN FORMS 990 AND 199
E.I .N . 95-6042583 ; ORG. NO. D-9791380 JANUARY 1 . 2004 TO DECEMBER 31, 2004
FOF h9 990. PART V FOP M 199, PART I I
LISI OF OFFICERS . DIRECTORS, TRUSTEES AND KEY EMPLOYEES Expense
Title Compensation Benefits Account
Fle:layne I. Antler Director None None None N .rysten A. Brennan It of " :;tephanie A . Caprielian It 11 of " ;;t~ephen C. Carroll
Nicholas Counter, III " ; ;teven R. Escovedo " Kay Kimmell " flank Lachmund Laura K. Legge It
Michael P. Messina 11
Michael Rosenfeld of
Jennifer Rubin It of " -"E:d D. Rubin "
.. .. .. , . Wayne Runyon Louis H . Shore " ;3lephen P. Taylor Rina Wallack Randy Winograd It It
Joseph A. Aredas It 1.
1= ;Rr1 Brendlinger " Anthony Cousimano " fliomas Davis 3UUCe C. Doering .John Ford " Sandra Berke Jordan It It
Donald G. Kutak Deborah Landis _;3inie Miller " Michael F . Miller :.armine A. Palazzo George A. Palazzo Scott Roth Mark A . Seay Thomas C. Short Carole Stepp Leo T. Reed "
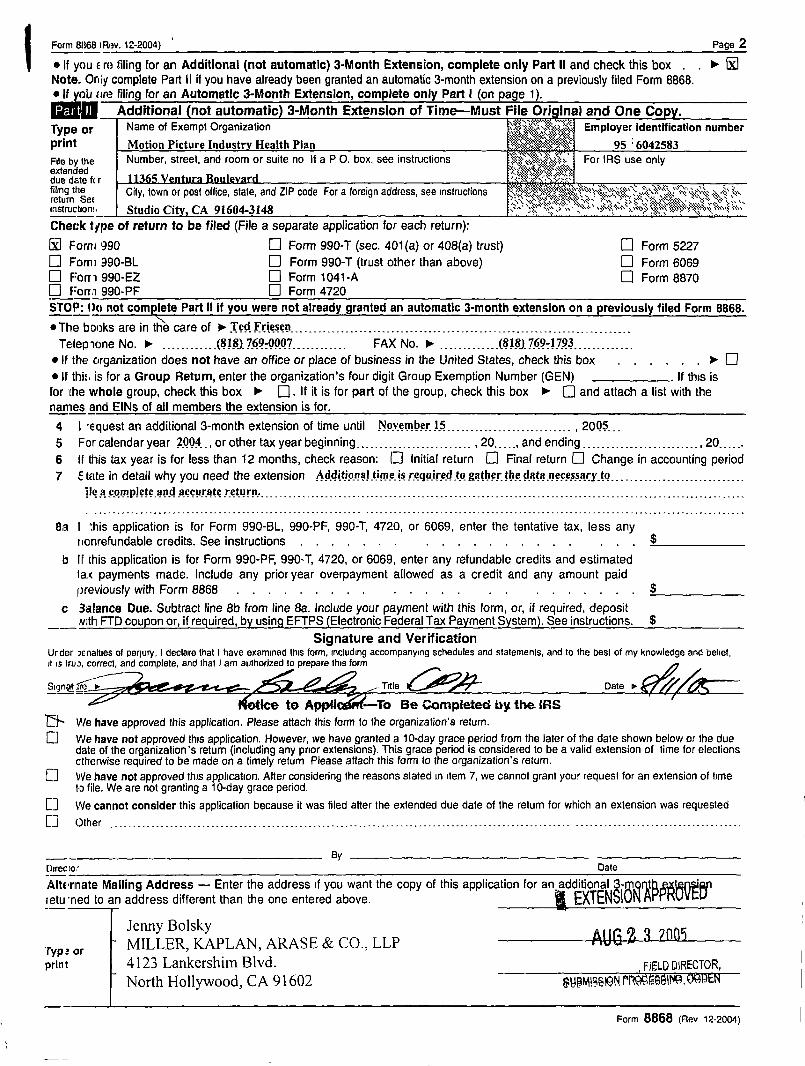
Farm 8068 1 Rav. 12-2004) 2 s If you E rc; filing for an Additional (not automatic) 3-Month Extension, complete only Part 11 and check this box Note . Only complete Part II if you have already been granted an automatic 3-month extension on a previously filed Form 8868. e If yob <<re filing for an Automatic 3-Month Extension, complete only Part I (on page 1) .
Additional not automatic 3-Month Extension of Time-Must File Original and One Co ~~w yam. ; ,K; r~ Type or Name of Exempt Organization ~},}t",;+~~~, Employer identification number print Motion Picture Industry Health Plan 95 :6042583 File by the Number, street, and room or suite no If a P O. box, see instructions jg~~'~~'~" Vjfi ~ .~, " ~"~>v . For IRS use only extened "+S~i
11365 Veotura Boulevard due date f< r '` filing the City, town or post office, state, and ZIP code For a foreign address, see instructions '~,:{ .~~, ~'~~`%k~~ ;~y~;;'~~~~' "~;<w,";`~k return $2E ;k,~a~F.y,..~ti;s}` :s " . ;
v } } , Ss k ~h ~;} V s l \~ instruction:, Studio Citv. CA 91604-3148 ` ' Check type of return to be filed (File a separate application for each return) : [0 Fom+ '390 D Form 990-T (sec . 401(a) or 408(a) trust) [--] Form 5227 El F'omi 990-BL 0 Form 990-T (trust other than above) El Form 6069 D F=orri 990-EZ D Form 1041-A El Form 8870 0 F=orra 990-PF El Form 4720 STOP: Do not complete Part II if you were not already granted an automatic 3-month extension on a previously filed Form 8868 . --- *The books are in the care of t Ted Frieseq______ .___ ._ .___ .__,_. .____ . ._ .__ .___ .___ .____ . . .____ ._ ., .__________ Te;lepicme No . lp~ ------------ (818) 769-0007 ------------ FAX No . " _ . ._, . . . . . . . . (818) 769-1793 .___________ .
" IF the organization does not have an office or place of business in the United States, check this box . . . . . , )- D " If thi :~ is for a Group Return, enter the organization's four digit Group Exemption Number (GEN) . If this is for the whole group, check this box t [] . If it is for part of the group, check this box t Q and attach a list with the names and EINs of all members the extension is for . ---4 I -equest an additional 3-month extension of time until November 15 . . . . . . . . . . . . . . . . . . . . . . . . . . . , 2005--- 5 For calendar year 2004 ., or other tax year beginning . . . . . . . . . --------------- - 20 . . . . ., and ending . . . . . . . . . . . . . . . . . . . . . . . . . . 20 . . . . . . 6 If dais tax year is for less than 12 months, check reason: D Initial return D Final return D Change in accounting period 7 : fate in detail why you need the extension Additional time. is required to gather the data necessary_to. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
file a complete and accurate return .
8a I 'his application is for Form 990-BL, 990-PF, 990-T, 4720, or 6069, enter the tentative tax, less any nonrefundable credits . See instructions . . . . . . . . . .
b If this application is for Form 990-PF, 990-T, 4720, or 6069, enter any refundable credits and estimated 1aK payments made . Include any prior year overpayment allowed as a credit and any amount paid previously with Form 8868 . . . . . . . . . . . . . . . . . . . . . . . $
c 3+31ance Due. Subtract line 8b from line 8a . Include your payment with this form, or, if required, deposit Noth FTD coupon or, if required, by using EFTPS (Electronic Federal Tax Payment System). See instructions . $
Signature and Verification Urder :)enal4es of penury, I declare that I have examined this form, including accompanying schedules and statements, and to the best of my knowledge and belief, it is trua, correct, and complete, and that I am authorized to prepare this form n
SignQ! f3 ~ Title C_oP`- Date s
tics to Appl1 -To Be Completed by the IRS ~~ We have approved this application . Please attach this form to the organization's return . [] We have not approved this application. However, we have granted a 10-day grace period from the later of the date shown below or the due
date of the organization's return (including any prior extensions) . This grace period is considered to be a valid extension of time for elections otherwise required to be made on a timely return Please attach this form to the organization's return .
[] We have not approved this application . After considering the reasons stated m item 7, we cannot grant your request for an extension of time to file . We are not granting a 10-day grace period .
[] we cannot consider this application because it was filed after the extended due date of the return for which an extension was requested
~~ ()flier ---------------~----------------~---~~--------------------------~----------~-----~--------------- --------------~----------~---~-~----
--- BY [hrec to r Date
A1turinate Mailing Address - Enter the address if you want the copy of this application for an additional 3- t retu ~r~ed to an address different than the one entered above. ~ EXTENSI~f~~~~~~
Jenny Bolsky 'ryp : or MILLER, KAPLAN, ARASE & CO ., LLP ~~ If; 2 3 7~Q5
4123 Lankershim Blvd . FIELD DIRECTOR, North Hollywood, CA 91602 SHpMjf~~~lONF .~=.WP+P,09N
Form 8868 (Rev 12-2004)
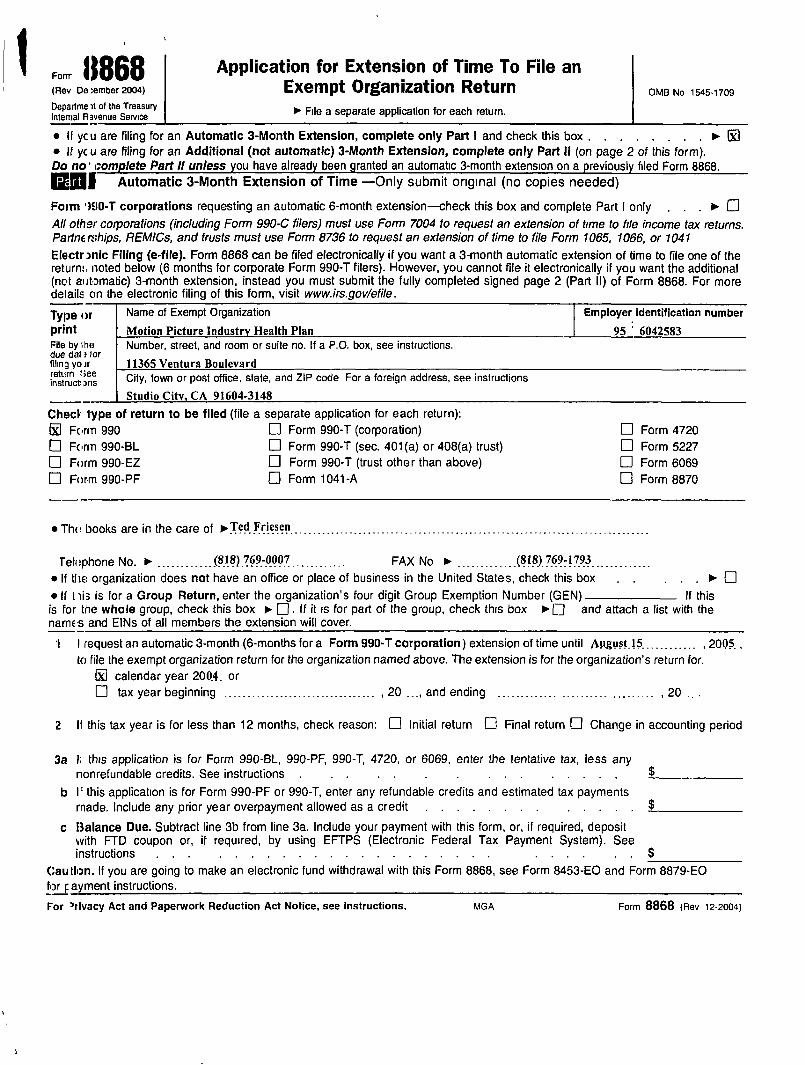
Fomr "868 Application for Extension of Time To File an (Rev De :ember2004) Exempt Organization Return OMB No ,545,,09 Departure it of the Treasury " File a separate application for each return . Internal Rsvenue Service
" If yc u are filing for an Automatic 3-Month Extension, complete only Part 1 and check this box . " If yc u are filing for an Additional (not automatic) 3-Month Extension, complete only Part II (on page 2 of this form). Do no' complete Part 11 unless you have already been granted an automatic 3-month extension on a previously filed Form 8868 . 12-01 Automatic 3-Month Extension of Time -Only submit original (no copies needed)
Form 1EIO-T corporations requesting an automatic 6-month extension heck this box and complete Part I only . . . t D Al! other corporations (including Form 990-C filers) must use Form 7004 to request an extension of time to file income tax returns. PartnE rships, REMICs, and trusts must use Form 8736 to request an extension of time to file Form 1065, 1066, or 1041 Electr 3nic Filing (e-file) . Form 8868 can be filed electronically if you want a 3-month automatic extension of 6me to file one of the return:, noted below (6 months for corporate Form 990-T filers) . However, you cannot file it electronically if you want the additional (not automatic) 3-month extension, instead you must submit the fully completed signed page 2 (Part II) of Form 8868. For more details on the electronic filing of this form, visit www.irs .gov/efile .
Name of Exempt Organization
Motion Picture Industry Health Plan Number, street, and room or suite no. If a P.O . box, see instructions .
Employer identification number Type or print
File by I he due dal ?for filing yo ir retain :See instructs arts City, town or post office, slate, and ZIP code For a foreign address, see instructions
Caution . If you are going to make an electronic fund withdrawal with this Form 8868, see Form 8453-EO and Form 8879-EO for F ayment instructions .
For 'rivacy Act and Paperwork Reduction Act Notice, see Instructions . MGA Form 8868 (Rev i2-2o0a)
Check type of return to be filed (file a separate application for each return) : M Form 990 D Form 990-T (corporation) D Form 4720
Farm 990-BL D Form 990-T (sec . 401(a) or 408(a) trust) 0 Form 5227 D Form 990-EZ D Form 990-T (trust other than above) D Form 6069 O Form 990-PF D Form 1041-A El Form 8870
" They books are in the care of 1Ted Friesen
Telophone No . t . . . . . . . . . . . .(8t8).769.-.0007 . ._,_____ . .__ FAX No t . . . . . . . . . . . . . (815)_769-1793 .______ . .__ ._ " If tlie organization does not have an office or place of business in the United States, check this box " If t His is far a Group Return, enter the organization's four digit Group Exemption Number (GEN) If this is for the whole group, check this box r E] . IF it is for part of the group, check this box t [] and attach a list with the names and EINs of all members the extension will cover.
I I request an automatic 3-month (6-months for a Form 990-T corporation) extension of time until August_15_ . . . . . . . . . . . , 2005_ , to file the exempt organization return for the organization named above. The extension is for the organization's return for.
GYM calendar year 2004 . or [] tax year beginning . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . , 20 . . _, and ending . . . . . . . . . ..-- . . . . . . . . . . . . . . . . . . . . . 20 . . .
2 11 this tax year is for less than 12 months, check reason : D Initial return EJ Final return D Change in accounting period
3a U this application is for Form 990-BL, 990-PF, 990-T, 4720, or 6069, enter the tentative tax, less any nonrefundable credits . See instructions . .
b If this application is for Form 990-PF or 990-T, enter any refundable credits and estimated tax payments made . Include any prior year overpayment allowed as a credit .
c Balance Due. Subtract line 3b from line 3a . Include your payment with this form, or, if required, deposit with FTD coupon or, if required, by using EFTPS (Electronic Federal Tax Payment System). See instructions . . . . . . . . . . . . . . . . . . . . . . . . . . . $


















