FORECASTING EMERGENCY ADMISSIONS IN DEVON - THE...
12
FORECASTING EMERGENCY ADMISSIONS IN DEVON - THE DEVON PREDICTIVE MODEL Todd Chenore Senior information analyst NHS Devon
Transcript of FORECASTING EMERGENCY ADMISSIONS IN DEVON - THE...

FORECASTING EMERGENCY ADMISSIONS IN DEVON - THE DEVON PREDICTIVE MODEL
Todd ChenoreSenior information analystNHS Devon

PREDICTIVE MODELLING IN UK HEALTHCARE
Ò Predictive risk models are used for predicting events such as unplanned hospital admissions, which are undesirable, costly and potentially preventable.
Ò Such models have been shown to be superior to other ‘case finding’ approaches, including threshold models and clinical opinion (Curry N. et al. 2005, Allaudeen N. et al. 2011).
Ò Predictive risk models can help the NHS manage: 1. ageing populations2. increasing numbers of people living with long-term
conditions3. rising rates of emergency hospital admissions4. financial pressures

HISTORY OF PREDICTIVE MODELLING IN NHS
Ò Case finding and/or risk stratificationÒ Condition specific models (COPD, falls, etc.)
Ò PARR++ – Inpatient data, readmissions onlyÒ CPM – all emergency admissions, 4 datasetsÒ PRISM – Welsh model Ò SPARRA – Scottish model

KAISER PYRAMID
Relative Risk Population% Emergency admits OP visits A&E visits Interventions
Very High Relative Risk 0.5% 18.6 X average 5.8 X average 8.5 X average Case Management High Relative Risk 0.6% - 5% 5.5 X average 3.8 X average 2.9 X average Disease ManagementModerate Relative Risk 6% - 20% 1.7 X average 1.9 X average 1.4 X average Supported Self Care Low Relative Risk 21% - 100% 0.5 X average 0.6 X average 0.8 X average Prevention & Promotion

5
FREQUENTLY-ADMITTED PATIENTS
0
5
10
15
20
25
30
35
40
45
50
- 5 - 4 - 3 - 2 - 1 Intense year
+ 1 + 2 + 3 + 4
Aver
age
num
ber o
f em
erge
ncy
bed
days
Source: Ann Rowe / Roger HallidayDepartment of Health

6
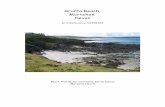
REACTIVE CASE MANAGEMENT REGRESSION TO THE MEAN
0
5
10
15
20
25
30
35
40
45
50
Aver
age
num
ber o
f em
erge
ncy
bed
days
- 5 - 4 - 3 - 2 - 1 Intense year + 1 + 2 + 3 + 4

7
EMERGING RISKPROACTIVE CASE MANAGEMENT
0
5
10
15
20
25
30
35
40
45
50
Aver
age
num
ber o
f em
erge
ncy
bed
days
- 5 - 4 - 3 - 2 - 1 Intense year
+ 1 + 2 + 3 + 4

DPM - A LOCAL MODEL
Ò Variables chosen from CPM, literature search, and local clinical suggestions
Ò Employed local datasets to capture more riskÒ Employed binary logistic regression
É University of Westminster studyÒ Many variables
É Good for clinical use but not parsimoniousÒ Used significant variables only
É Appropriate?Ò Split sample validationÒ Low cost

NUMBER (%) PATIENTS IN ‘AT RISK’ GROUP PREDICTED BY THEMODEL WHO HAD AN EMERGENCY ADMISSION WITHIN 12 MONTHS
‘At risk’ sub-group Combined Predictive Model (CPM)
Devon Predictive Model (DPM)
200 top-ranked patients (0·03% of registered population) 143/200 (71.5%) 173/200 (86.5%)
1000 top-ranked patients (0·13% of registered population) 605/1000 (60.5%) 742/1000 (74.2%)
3800 top-ranked patients (0·5% of registered population) 1843/3800 (48.5%) 2286/3800 (60.2%)
7000 top-ranked patients (0·92% of registered population) 2639/7000 (37.7%) 3708/7000 (53.0%)
16000 top-ranked patients (2·1% of registered population) 4896/16000 (30.6%) 6877/16000 (43.1%)

10
Monthly Data extract from Practice
Secure transfer to PCT Data Warehouse
Generation of Predictive Risk score using DPMData from Secondary Care, DDOC, SWAST, Exeter system, etc.
Identification of Top At-Risk Patients for Admission to Community Virtual Ward
Initial Visit, Consent and Assessment by Community Matron
Areas for action identified and discussed at Complex Care Team Weekly Meeting
and with Patients Own GP etc.
On-going review by the Community Matron as dictated by Predictive Risk
and Current Clinical and Social need -including either Daily/Weekly/Monthly
planned visits
Actions and involvement as necessary by the
Complex Care Team/ GP /Practice, Secondary Care,
Nurse Specialists etc. –Co-ordinated by the
Community Matron for each patient
Patient discharged from CVW if Predictive Risk falls out of top-40/50 – Follow-up via ongoing regular review by
Patients Own GP/Practice and Complex Care Team etc as necessary
Patient and Carers given details for contacting Virtual Ward Office if any problems/early clinical need
Daily communication with Secondary Care, DDOC, SWAST etc - informed of
status and presence of Yellow Folder and Escalation Plan for
each patient in their home and help with crisis
management, admission avoidance and early discharge

Locality Average VW occupancy
Average VW occupancy
chosen from top 0.5% risk
Average VW occupancy
chosen from low risk
Percentage of practices hitting 2011 DPM LES
targets
First quarter net admission
change 2009 to 2011 for top 0.5% cohort*
Change in actual PbR cost associated with net admission
change*
Locality A 107.4% 45.2% 15.5% 65.5% -22.06% -£845,310
Locality B 98.8% 37.8% 21.6% 42.9% -14.24% -£210,758
Locality C 90.3% 28.7% 26.4% 19.2% 3.91% £151,742
Devon Evaluation

ON THE HORIZON
Ò Impactability modelsÉMany not appropriate (refusal, mental health, etc.)É ACS admissionsÉGaps in care
Ò Emerging risk models