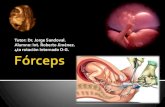
Forceps delivery
26
Forceps Delivery www.freelivedoctor.com
Transcript of Forceps delivery

Forceps Delivery
www.freelivedoctor.com

Obstetric forceps
• Definition:• Obstetric forceps is a double-bladed metal
instrument used for extraction of the foetal head.
www.freelivedoctor.com

Types
• Long curved obstetric forceps• Wrigley’s forceps• Kielland's forceps• Piper’s forceps• Barton's forceps
www.freelivedoctor.com

Action of the Forceps
• Traction: is the main action.• Rotation: in deep transverse arrest, persistent
occipito-posterior and mento-posterior.
www.freelivedoctor.com

Indications of Forceps Delivery
• Prolonged 2nd stage• It is prolongation for more than 1 hour in
primigravidae or 30 minutes in multiparae. This may be due to:
* Inertia and poor voluntary bearing down.* Large foetus. * Rigid perineum.* Malpositions: persistent occipito-posterior and
deep transverse arrest.www.freelivedoctor.com

Maternal indications
* Maternal distress manifested by:>Exhaustion.> Pulse >100 beats / min. > Temperature >38oC .> Signs of dehydration.* Maternal diseases as:> Heart disease. > Pulmonary T.B. > Pre-eclampsia and eclampsia.
www.freelivedoctor.com

Foetal indications
* Foetal distress.* Prolapsed pulsating cord.* Preterm delivery.• After-coming head in breech delivery.• During caesarean sectionOne (used as a lever)
or the two blades may be used to extract the head through the uterine incision.
www.freelivedoctor.com

Type Description
Outlet forceps The foetal head is at the perineum. The scalp is visible at the introitus without separating the labia.Sagital suture is in anteroposterior diameter, right or left occipito-anterior or posterior.Rotation does not exceed 450.
Low forceps The leading point of the skull is at station +2 or more and divided into: i-Rotation ≤450. ii- Rotation >450
Mid forceps The head is engaged, but the leading point is above station +2.
High forceps Not included in the classification. It is abandoned in favour of caesarean section.
www.freelivedoctor.com

Pre-requisites for Forceps Application
* Anaesthesia: general, epidural, spinal or pudendal block.
* Adequate pelvic outlet.* Aseptic measures.* Bladder and Bowel evacuation.* Contractions of the uterus should be present.* Dilatation of the cervix should be fully.* Engaged head.
www.freelivedoctor.com

Pre-requisites for Forceps Application
* Forewater rupture.* Favourable position and presentation:>Occipito-anterior.> Occipito-posterior> Face presentation.>After-coming head in breech.
www.freelivedoctor.com

Types of Forceps Application
* Cephalic application: the forceps is applied on the sides of the foetal head in the mento-vertical diameter so injury of the foetal face, eyes and facial nerve is avoided .
* Pelvic application: The forceps is applied along the maternal pelvic wall irrespective to the position of the head. It is easier for application but carries a great risk of foetal injuries.
* Cephalo-pelvic application: It is the ideal application and possible when the occiput is directly anterior or posterior or in direct mento-anterior position.
www.freelivedoctor.com

How to know Right and Left Blades
• Putting in consideration that the mother is in the lithotomy position, the blade will be applied with the pelvic curve directed anteriorly and the cephalic curve directed medially. If the blade will be applied to the left maternal side it is a left blade and vice versa.
www.freelivedoctor.com

Technique of Forceps Delivery
• In occipito- anterior position* The left blade is applied first. It is held by its handle
between the thumb and fingers of the left hand almost parallel with the right inguinal ligament and passed along the left side of the maternal pelvis between the guiding palm of the right hand and foetal head.
* As the blade passes into the birth canal the handle is carried backwards and towards the midline. It is now the lower blade.
www.freelivedoctor.com

Technique of Forceps Delivery
* The fingers of the left hand are introduced along the right side of the pelvis and the right blade is held and passed in the same manner. It is now the upper blade.
* The 2 blades should be locked easily, if not this means that they were not correctly applied and should be removed and re-assess the position of the head.
www.freelivedoctor.com

Clinical checks for correct forceps application:
* The sagittal suture lies in the midline of the shanks.
* The operator cannot place more than a finger tip between the fenestration of the blade and the foetal head.
* The posterior fontanelle is not more than one finger- breadth above the plane of the shanks.
www.freelivedoctor.com

Traction should be:
* gentle by the force of the arm only,* intermittent with uterine contractions only,* in correct direction i.e. downwards and
backwards till the occiput appears at the vulva, then downwards and forwards.
* The 2 blades are unlocked between contractions to minimise the period of head compression.
www.freelivedoctor.com

Kielland forceps in deep transverse arrest
• The forceps is locked outside with the knobs towards the occiput to know the anterior blade.
• The anterior blade is applied first by one of the following methods:
www.freelivedoctor.com

• The wandering method: The anterior blade is guided into the lateral side of the pelvis with the cephalic curve facing the foetal head. It is then slid over the forehead to fit against the anterior parietal eminence.
• The direct method: when the head is low down in the pelvis, the anterior blade is slid between the head and symphysis pubis with the cephalic curve facing the foetal head.
• The old (classical) method: The anterior blade is applied with the cephalic curve towards the symphysis pubis then it is rotated 1800 to fit with the head. This method is not recommended as the lower uterine segment and bladder may be injured.
www.freelivedoctor.com

• The posterior blade is applied along the concavity of the sacrum.
• The 2 blades are locked, head is rotated and extracted as occipito-anterior.
www.freelivedoctor.com

Complications of Forceps Delivery
• Maternal complications• Foetal complications
www.freelivedoctor.com

Maternal complications
• Complications of anaesthesia.• Lacerations: > Extension of the episiotomy. > Perineal tear. > Vaginal tears. > Cervical lacerations. > Bladder injury. > Ureteric injury. > Rupture uterus.
www.freelivedoctor.com

Maternal complications
• Bone injuries: to pelvic joints, coccyx or symphysis pubis.
• Pelvic nerve injuries.• Postpartum haemorrhage: due to lacerations
or atony.• Puerperal infections.• Remote effects: genital prolapse, stress
incontinence, cervical incompetence and genito-urinary fistulas.
www.freelivedoctor.com

Foetal complications
• Fracture of the skull.• Cephalohaematoma.• Intracranial haemorrhage.• Facial nerve palsy.• Trauma to the face, eyes or scalp.• Asphyxia due to:> intracranial haemorrhage or,> cord compression between the head and the
forceps.www.freelivedoctor.com

FAILED FORCEPS
• Failure to extract the foetus by the forceps which may be due to failure to apply the forceps or to deliver the head with it
www.freelivedoctor.com

FAILED FORCEPS• Causes
* Cephalo-pelvic disproportion.* Contracted outlet. * Incomplete cervical dilatation.* Constriction ring. * Head is not engaged.* Malpositions as persistent occipito-posterior.*Malpresentations as brow.* Foetal congenital anomalies as hydrocephalus, ascitis and
conjoined twins.www.freelivedoctor.com

Management
* Reassessment: The forceps is removed and the patient is re-examined to detect the cause and correct it if possible.
* Caesarean section: is indicated in uncorrectable causes as cephalo-pelvic disproportion, and contracted outlet.
* Exploration of the birth canal: for any injuries.
www.freelivedoctor.com



![Index [ ] · PDF fileDiamond Disc ... Eye Enucleation Forceps ... Kern Bone Holding Forceps](https://static.fdocuments.us/doc/165x107/5aa15ab17f8b9ac67a8baaa4/index-disc-eye-enucleation-forceps-kern-bone-holding-forceps.jpg)