
for building climate resilient health systems
56
Operational framework for building climate resilient health systems H E A L T H & C LI M A T E R E S E A R C H I N F R A S T R U C T U R E , TE C H N O L O G I E S A N D PR O D U C TS T O E N H A N C E C LI M A T E R E SILIE N C E M A N A G E M E N T O F E N V I R O N M E N T A L D E T E R M I N A N T S O F H E A L T H C L I M A T E I N F O R M E D H E A L T H P R O G R A M M E S & M A N A G E M E N T P R E P A R E D N E S S E M E R G E N C Y I N T E G R A T E D R I S K M O N I T O R I N G & E A R L Y W A R N I N G A S S E S S M E N T A D A P T A T I O N C A P A C I T Y & V U L N E R A B I L I T Y , W O R K F O R C E H E A L T H G O V E R N A N C E L E A D E R S H I P & H E A L T H F I N A N C I N G C L I M A T E &
Transcript of for building climate resilient health systems
Operational frameworkfor building climate resilient
health systems
HEALTH &
CLIMATE RESEARCH
INFRASTRUCTURE, TECHNOLOGIES AND
PRODUCTS TO ENHANCE
CLIMATE RESILIENCE
MANAGEMENT OF
ENVIRONMENTAL
DETERMINANTS
OF HEALTH
CLIM
ATEINFO
RMED
HEA
LTH PRO
GRAM
MES
& M
AN
AGEM
ENT
PREP
ARE
DN
ESS
EMER
GEN
CY
INTE
GRA
TED
RIS
KM
ON
ITO
RIN
G &
EARL
Y W
ARN
ING
ASSESSMEN
TADAPTATIO
NCAPACITY &
VULNERA
BILITY,
WORKFORCE
HEALTH
GOVERNANCE LEADERSHIP &
HEALTH FINANCING
CLIM
ATE &
Operational framew
ork for building climate resilient health system
s

WHO Library Cataloguing-in-Publication Data
Operational framework for building climate resilient health systems.
I.World Health Organization.
ISBN 978 92 4 156507 3 Subject headings are available from WHO institutional repository
© World Health Organization 2015
All rights reserved. Publications of the World Health Organization are available on the WHO web site (www.who.int) or can be purchased from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]).
Requests for permission to reproduce or translate WHO publications –whether for sale or for non-commercial distribution– should be addressed to WHO Press through the WHO website (www.who.int/about/licensing/copyright_form/en/index.html).
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use.
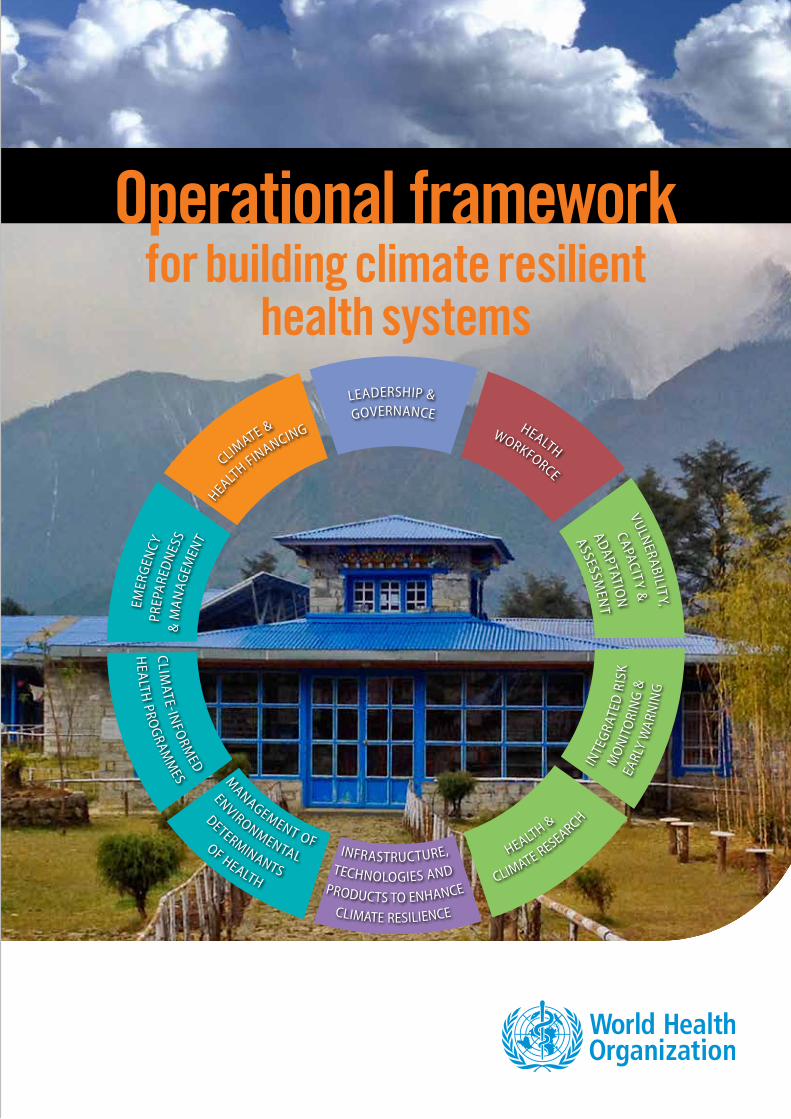
Cover illustration: Building climate resilience requires strengthening of a range of health system functions, from disease surveillance, to enhanced health action in emergencies. Health facilities are at the front line. The photograph shows a health clinic in Nepal, which uses solar panels to ensure reliable energy access to provide essential medical services, including during extreme weather events.
Printed in Geneva, Switzerland.

Operational framework for building climate resilient health systems

AcknowledgementsPrepared by Joy Shumake-Guillemot (World Meteorological Organization (WMO)/World Health Organization (WHO) Joint Office), Elena Villalobos-Prats, Diarmid Campbell-Lendrum (WHO Public health, environmental and social determinants of health (PHE)).
WHO gratefully acknowledges the financial support provided by the Department for International Development (DFID), United Kingdom and comments and technical inputs from Guy Howard and Alexandra Chittenden at DFID.
This framework builds on relevant frameworks and work plans on climate change and health adopted across WHO regions such as the WHO Regional Office for Africa (AFRO) “Adaptation to climate change in Africa: Plan of action 2012–2016”; the WHO Regional Office for the Americas (AMRO) “Strategy and plan of action on climate change”; the WHO Regional Office for Europe (EURO) “Protecting health in an environment challenged by climate change: European regional framework for action”; the WHO Regional Office for South-East Asia (SEARO) “Regional strategy for protecting health from climate change”; and guidance given in resolutions on climate change and health by the WHO Regional Office for the Eastern Mediterranean (EMRO) and WHO Regional Office for the Western Pacific (WPRO).
It also benefits from the experience gained in country projects funded by Norway, Deutsche Gesellschaft für Internationale Zusammenarbeit (GIZ), the German Federal Ministry for the Environment, Nature Conservation and Nuclear Safety (BMU), Spain through the Millennium Development Goals Fund (MDG-F), and the Global Environment Facility (GEF).
WHO also wishes to extend its gratitude to the following reviewers within WHO:
Jonathan Abrahams, Magaran Bagayoko, Mariam Otmani del Barrio, Hamed Bakir, Carlos Corvalan, Nasir Hassan, Rokho Kim, Waltaji Terfa Kutane, Marina Maiero, Bettina Menne, Maria Neira and Jung Sub Yeom.
Furthermore, WHO acknowledges the insightful comments and contributions provided by the par-ticipants of the inception meeting of the DFID-funded project on “Building adaptation to climate change in health in least developed countries through resilient WASH”, held in Geneva, Switzerland in October 2013, and the final meeting of the GEF/UNDP/WHO Project Managers and International Project Board for the Global Project “Piloting health adaptation to climate change”, held in Bridgetown, Barbados in May 2015, who provided insightful inputs for the finalization of the framework. Participants of the first meeting were: Elias Bartholomew Maiga Chinamo, Semunesh Golla, AM Zakir Hussain, Iqbal Kabir, Neema Minja Kileo, Waltaji Terfa Kutane, Shamsul Gafur Mahmud, Abadh Kishore Mishra, Abul Khair Mohammad, Dorisia Mulashani, Sudan Raj Panthi, Badri Pokhrel, Khom Bahadur Subedi and Dangew Tadesse. Participants of the second meeting were: Tonya Brathwaite, Lester Cumberbatch, Steve Daniel, Rada Dukpa, Kris Ebi, Sally Edwards, Guto Galvao, Winfred Austin Greaves, Simon Hales, Joy St. John, Vladimir Kendrovski, Desmond King, Mazen Malkawi, Sonia Nurse, Kepha Ombacho, MeciuselaTuicakau, Dorji Wangchuk and Nima Wangchuk.

Acronyms and abbreviations _________________________________________________________ iv
1. Introduction _____________________________________________________________________1
2. Background ____________________________________________________________________ 22.1 Public health rationale _________________________________________________________ 2
2.2 Policy context _________________________________________________________________5
3. Applying a resilience approach to health systems ______________________________________ 63.1 Goal and objectives ____________________________________________________________ 6
3.2 Introducing a resilience approach ________________________________________________ 6
3.3 Applying a resilience approach to health systems _____________________________________ 8
3.4 Overarching considerations in building resilience ____________________________________ 9
3.5 Connecting to the “building blocks” of health systems ________________________________ 10
3.6 Ten components for building climate resilience ______________________________________ 12
3.7 How to use the framework ______________________________________________________ 13
Components ______________________________________________________________________144.1 Component 1: Leadership and governance __________________________________________ 14
4.2 Component 2: Health workforce _________________________________________________ 16
4.3 Component 3: Vulnerability, capacity and adaptation assessment ________________________ 19
4.4 Component 4: Integrated risk monitoring and early warning ___________________________ 21
4.5 Component 5: Health and climate research _________________________________________23
4.6 Component 6: Climate resilient and sustainable technologies and infrastructure ____________25
4.7 Component 7: Management of environmental determinants of health ____________________27
4.8 Component 8: Climate-informed health programmes _________________________________29
4.9 Component 9: Emergency preparedness and management _____________________________32
4.10 Component 10: Climate and health financing _______________________________________34
5. Monitoring progress ____________________________________________________________ 36
6. Conclusions ___________________________________________________________________ 43
Terminology _____________________________________________________________________ 44
References _______________________________________________________________________ 47
Contents

iv Operational framework for building climate resilient health systems
Acronyms and abbreviationsCOP Conference of the Parties
DFID Department for International Development
EDRM-H Emergency and Disaster Risk Management for Health
GEF Global Environmental Facility
GFATM Global Fund to Fight AIDS, Tuberculosis and Malaria
H-NAP health component of NAP
IPCC Intergovernmental Panel on Climate Change
NAP National Adaptation Plan
UNFCCC United Nations Framework Convention on Climate Change
V&A vulnerability and adaptation
WHA World Health Assembly
WHO World Health Organization

Introduction 1
IntroductionThis document presents the World Health Organization (WHO) Operational framework for building climate resilient health systems. The framework responds to the demand from Member States and partners for guidance on how the health sector and its operational basis in health systems can systematically and effectively address the challenges increasingly presented by climate variability and change. This framework has been designed in light of the increasing evidence of climate change and its associated health risks (1); global, regional and national policy mandates to protect population health (2); and a rapidly emerging body of practical experience in building health resilience to climate change (3).
Primarily intended for public health professionals and health managers, this framework would also help guide decision-makers in other health-determining sectors, such as nutrition, water and sanitation, and emergency management. International development agencies could use this framework to focus investments and country support for public health, health system strengthening and climate change adaptation.
The objective of this framework is to provide guidance for health systems and public health programming to increase their capacity for protecting health in an unstable and changing climate. By implementing the 10 key components laid out in this framework, health organizations, authorities and programmes will be better able to anticipate, prevent, prepare for and manage climate-related health risks. Least developed countries and countries in the process of developing the health components of National Adaptation Plans (NAPs) under the UN Framework Convention on Climate Change (UNFCCC) (4) may find this document particularly useful in their efforts to design a comprehensive response to the risks presented by short-term climate variability and long-term climate change.
1

2 Operational framework for building climate resilient health systems
Background
2.1 Public health rationale
There is clear evidence that human actions, principally the burning of fossil fuels and associated release of climate pollutants, are causing significant changes in global climate. This in turn is creating observed consequences in environmental and social conditions across all continents (5). As many of the largest health concerns are strongly influenced by weather and climate conditions, this inevitably presents risks for human health that can be grouped into:
• Direct impacts, such as those arising from damages and illness due to increased frequency and severity of extreme weather events.
• Environmental system mediated impacts, such as rising air pollution and changing patterns of vector-, food- and water-borne diseases.
• Socially mediated effects that occur via effect of climate change on social and human systems, such as health effects resulting from undernutrition, occupational heat stress and mental illness, as well as potential increases in population displacement, slowing of economic growth and poverty aggravation.
Table 1 shows some of the main climate-related health risks, that have been assessed as having medium-to-strong evidence by the Intergovernmental Panel on Climate Change (IPCC). In addition, the IPCC identifies a series of key reasons for concern with regard to effects of climate change which are either particularly severe or irreversible (5). This includes the potential: (i) increase in severity and frequency of extreme weather events, such as storms and floods causing mass displacement and disruption of livelihoods in low-lying coastal zones and small island states due to storm surges and rise in sea level; (ii) breakdown of food systems resulting in food shortages and volatile prices, particularly in low- and middle-income countries; (iii) potential increase in risk of violent conflict associated with resource scarcity and population movements; and (iv) slowing down of economic growth and exacerbation of poverty, with associated reversal of global health progress, achievement of the Millennium Development Goals, and the objectives of the forthcoming post-2015 development agenda.
Overall, climate change is expected to significantly increase health risks, particularly in low- and middle-income countries and populations. They will also disproportionately affect vulnerable groups within each country, including the poor, children, the elderly and those with pre-existing medical conditions.
Despite these challenges, a lot can be done to protect deterioration of health due to climatic conditions. Over the long term, mitigation is necessary to avoid continued degradation of the environmental determinants of health. In the short-to-medium term (i.e. up to the next 20–30 years) well-planned adaptation measures can avoid much of the projected health impacts.
2

Background 3
TABlE 1: Summary of the main expected health impacts of climate variability and climate change globally by the middle of the current century
Climate change effects
Health risks Health impacts Confidence rating
Direct effects
Increased number of warm days and nights; increased frequency and intensity of heat waves; increased fire risk in low rainfall conditions
Excess heat-related mortality; increased incidence of heat exhaustion and heat stroke, particularly for outdoor labourers, athletes, the elderly; exacerbated circulatory, cardiovascular, respiratory and kidney diseases; increased premature mortality related to ozone and air pollution produced by fires, particularly during heat waves
Increased risk of injury, disease and death due to more intense heat waves and fires
Very high
Decreased number of cold days and nights
Lower cold-related mortality and reduced cardiovascular and respiratory diseases particularly for the elderly in cold and temperate climates
Modest improvements in cold-related mortality and morbidity
low
Effects mediated through natural systems
Higher temperatures and humidity; changing and increasingly variable precipitation; higher sea surface and freshwater temperatures
Accelerated microbial growth, survival, persistence, transmission, virulence of pathogens; shifting geographic and seasonal distribution of diseases (e.g. cholera, schistosomiasis) and ecological changes (e.g. harmful algal blooms); lack of water leading to poor hygiene; flood damage to water and sanitation infrastructures; contamination of water sources through overflow
Increased risks of food- and water-borne diseases
Very high
Higher temperatures and humidity; changing and increasingly variable precipitation
Accelerated parasite replication and increased biting rates; prolonged transmission seasons; re-emergence of formerly prevalent diseases; changing distribution and abundance of disease vectors; reduced effectiveness of vector control interventions
Increased risks of vector-borne diseases
Medium
Effects heavily mediated by human systems
Higher temperatures and changes in precipitation
Lower food production in the tropics; lower access to food due to reduced supply and higher prices; combined effects of undernutrition and infectious diseases; chronic effects of stunting and wasting in children
Increased risk of undernutrition resulting from diminished food production in poor regions
High
Higher temperatures and humidity
Outdoor and unprotected workers obliged to work either in physiologically unsafe conditions or to lose income and livelihood opportunities
Consequences on workers’ health include lost work capacity and reduced labour productivity in vulnerable populations
High
Combined effect
Overall climate change
Combination of above risks Negative health effects would outweigh positive effects worldwide
High
Note: The final column refers to the level of confidence in the evidence for expected health impacts, as presented in the Fifth assessment report of the IPCC (1). Other health impacts are possible (see text), but were not assigned evidence grading by the IPCC.

4 Operational framework for building climate resilient health systems
Potential for adaptation to
reduce risk
Risk level withcurrent adaptation
Risk level withhigh adaptation
Risk and potential for adaptation
2080–2100 "Era of climate options"
+ 4°C
Present
+ 1.5°C
2030–2040 "Era of committed climate change"
Vector-bornediseases
Undernutrition
Heat
Food- and water-borneinfections
Air quality
Extreme weatherevents
Mental healthand violence
Occupational health
Vector-bornediseases
Undernutrition
Heat
Food- and water-borneinfections
Air quality
Extreme weatherevents
Mental healthand violence
Occupational health
Vector-bornediseases
Undernutrition
Heat
Food- and water-borneinfections
Air quality
Extreme weatherevents
Mental healthand violence
Occupational health
FIGURE 1: Conceptual presentation of health risks due to climate change and the potential for risk reduction through adaptation
Note: The width of the slices gives a qualitative indication of the relative burden of ill health at the global level. For each timeframe, impact levels are estimated for the current state of adaptation and for a hypothetical highly adapted state, indicated by different colours.Source: Reproduced from the health chapter, Working group II of the IPCC Fifth assessment report (1).
Figure 1 provides a qualitative assessment of the future burden (for the period 2030–2040)of ill-health due to current climate change, in which the world will inevitably experience approximately 1.5 °C of warming due to past and present greenhouse gas emissions (1,5). Figure 1 also presents the period 2080–2100, for which the global mean temperature is expected to increase by approximately 4 °C above preindustrial levels, unless vigorous mitigation efforts are undertaken soon (1,5). The different colours indicate the extent to which disease burdens could be avoided by effective adaptation measures in each period.

Background 5
This operational framework can be used by all health systems, but is particularly oriented to support those in low- and middle-income countries, which often already face challenges to adequately prepare for health emergencies and control disease burdens, provide coverage of basic healthcare and public health services, manage inequity, and use resources in a cost-effective way. Health systems with such challenges are at particularly high risk for future setbacks and losses in health achievements gained. And, in these locations building of resilience would need to start with reducing existing health system vulnerabilities.
2.2 Policy context
The operational framework responds to policy mandates at global, regional and (increasingly at) national levels. It includes the World Health Assembly (WHA) and WHO regional committee resolutions on health protection from climate change, strengthening national health emergency and disaster management capacities for managing the risks of meteorological and other extreme events, health system strengthening and implementation of International Health Regulations (2,7). It also responds to the requests by parties to the UNFCCC regarding provision of support in planning adaptation to climate change in key sectors, including health. Additionally, it responds to the post-2015 development agenda and associated Sustainable Development Goals and the Sendai framework for disaster risk reduction.
This document therefore aims to support national ministries of health and their partners to identify the key functions that need to be strengthened in order to provide a comprehensive public health response to climate change, within an overall intersectoral NAP (4).

6 Operational framework for building climate resilient health systems
Applying a resilience approach to health systems
3.1 Goal and objectives
Framework goal
The goal is to enhance the capacity of health systems to protect and improve population health in an unstable and changing climate. Ultimately, health systems should be increasingly strengthened and continue to be efficient and responsive to improve health, reduce inequities and vulnerability, and provide adequate social and financial protection, in light of the shocks and stresses they may face from climate variability and change. The framework therefore aims to achieve its goal through activities that build capacity to effectively monitor, anticipate, manage and adapt to the health risks associated with climate variability and change.
Framework objectives
Specifically, this framework aims to:
• guide professionals working in health systems, and in health determining sectors (e.g. water and sanitation, food and agriculture, energy, urban planning) to understand and effectively prepare for the additional health risks posed by climate variability and change, through a resilience approach;
• identify the main health functions that need to be strengthened to build up climate resilience, and use these as the basis for developing a comprehensive and practical plan (e.g. as the health component of NAP (H-NAP)) (4); and
• support health decision-makers to identify roles and responsibilities to implement this plan, for actors both within and outside the formal health sector.
3.2 Introducing a resilience approach
What is resilience?
IPCC defines ‘resilience’ as the “capacity of a social-ecological system to cope with a hazardous event or disturbance, responding or reorganizing in ways that maintain its essential function, identity, and structure, while also maintaining the capacity for adaptation, learning and transformation.” (6)
3

Applying a resilience approach to health systems 7
In the simplest terms, resilience refers to the holistic ability and agility of a system to change and flex – according to circumstances – and continue to function under stress, while undergoing change. Resilience is much more than just the absence of vulnerability; it is about whole system capacity.
Adaptations to climate change and climate resilience building are closely related, but not synonymous. ‘Adaptation’, as defined by the IPCC in its Fifth assessment report, is the “process of adjustment to actual or expected climate and its effects. In human systems, adaptation seeks to moderate harm or exploit beneficial opportunities. In natural systems, human intervention may facilitate adjustment to expected climate and its effects” (6).
With regard to health, resilience relates to the capacity of the system itself to cope with and manage health risks in a way that the essential functions, identity and structure of health systems are maintained. While health adaptation seeks to moderate harm or exploit beneficial opportunities, the preservation of a certain level of quality and sustainable performance of the system itself is not ensured. The incorporation of a climate-resilient approach to health systems contributes to assuring the performance of the system, and therefore, the sustainability and maximization of value for money of health investments. However, it is important to remember that maintaining system resilience may not always be possible. The magnitude of climate-induced changes or shocks may be so significant that it is outside human abilities to maintain its essential functions, and thus the system may collapse or fail.
Figure 2 shows the conceptual framework of a resilient system, which can be applied to communities, organizations, or other systems, including health systems.
Resilience =
+Decreased vulnerability
Increased capacity.Improved choices & opportunities
1CONTEXT
2CHALLENGE/
DISTURBANCE
3CAPACITY TO DEAL
WITH DISTURBANCE
4CHOICES &
OPPORTUNITIES
5OUTCOMEOPTIONS
Stresses
Vulnerability Transform
Recover better than before
Recover to pre-event state
Recover but worse than before
Collapse
Exposure
Sensitivity
Adaptive capacity
Shock
Created by Seán Mongeyfrom the Noun Project
Created by Muneer A.Safiahfrom the Noun Project
HealthSystem
Source: Adapted from Defining disaster resilience: a DFID approach paper (8).
FIGURE 2: Conceptual framework for resilience

8 Operational framework for building climate resilient health systems
The degree of resilience a system possesses largely manifests in step 4 (choices and opportunities; see Figure 2). Low levels of resilience may result in the system collapsing (health operations cease) or experiencing setbacks (limited health service delivery capacity due to stock losses or staff shortages) that put them in a worse position than before the adverse events.
3.3 Applying a resilience approach to health systems
Building health system resilience to climate change is a cumulative process. It begins with making resilience a goal, in addition to current goals of improving population health, being responsive and efficient and providing social and financial protection.
This entails building capacity to: recognize, monitor, anticipate, communicate and prepare for changing climate-related health risks; prevent, respond to, manage, and cope with uncertainty, adversity and stress; adapt operations to changing risk conditions; recover from crisis and setbacks with minimal outside support; and learn from experience and improve system capacity for the future.
WHO working definition of a climate resilient health system
A climate resilient health system is one that is capable to anticipate, respond to, cope with, recover from and adapt to climate-related shocks and stress, so as to bring sustained improvements in population health, despite an unstable climate.
For the whole health system to become more climate-resilient, its independent building blocks (i.e. leadership and governance, health workforce, health information systems, essential medical products and technologies, service delivery and financing) have to also become climate resilient.
Furthermore, in order to effectively protect the health of the population, the health sector should strengthen and extend its sphere of influence and operations beyond itself mainly in relation to health-determining sectors (e.g. water, energy, food and agriculture and urban planning). While it is clear that the management of these sectors is not directly under the control of the health sector, the development of normative guidance to determine acceptable levels of exposure to risks for health (e.g. water and air quality guidelines) is a core health role. In the same way, the role of monitoring health outcomes in relation to the operations of these sectors is usually the responsibility of the health sector.
Ultimately, the health sector should effectively extend into the community level if the health system is to protect health and facilitate community resilience. Local level dialogue, two-way information exchange, and community mobilization should be considered essential functions of the health system. Community empowerment can activate local capacity, increase the scope of available information, improve understanding of vulnerability and build foundations for local resilience.

Applying a resilience approach to health systems 9
3.4 Overarching considerations in building resilience
Building climate resilience is a process of teaching the health system to more effectively adapt to change, particularly changing health risks due to climate change. The process of building resilience occurs in two principle ways: (i) reducing overall vulnerability, and (ii) developing specific system capacities. Incorporating these considerations when applying the operational framework is important to integrating climate perspectives to health policy and operations.
Reduce vulnerability
A healthier population and stronger health system will be more resilient to climate change. In order to reduce vulnerability and create resilient health systems and healthier populations that are able to respond to potential health effects from climate change, the following measures are recommended:
• Continued investments to reduce poverty and inequity.• Universal access to essential services, such as health, education, clean water and adequate
food.
For health system strengthening the following measures are recommended:
• An adequate workforce and climate-proofed infrastructure in local facilities to control climate-sensitive diseases and improve response to local emergencies.
• Surveillance systems to monitor population health and environmental exposure.• Good practices of health governance.
Develop capacities
Addressing current gaps and improving the current health system or programme performance is not enough to prepare a health system to tackle climate change. Health systems should increasingly take steps to understand how climate change will affect their population and service delivery, evaluate the effectiveness of their interventions and systems under diverse climatic conditions, and enhance their institutional capacity accordingly. To do this, public health and health system capacities that are attuned to climate realities are needed.
Add long-term perspectives for actions to be put in place today
Climate related health risks occur at multiple timescales, from short-term climate variability (such as heat waves and storms that can trigger health emergencies over timescales from days to weeks), to long-term climate change (such as timing of the onset of seasons and average number of hot days and nights over decades). The implementation of each component should therefore consider decisions with the aim to improve service delivery and health system performance in the short- (days to years), medium- (5–10 years) as well as long-term (decades) perspectives.

10 Operational framework for building climate resilient health systems
Ensure adaptive management approaches exist
Adaptive management is a structured and iterative process of decision-making and implementation that is especially useful in the context of uncertainty. Adaptive management processes and approaches use active learning methods to help accrue multiple perspectives of information that can reduce uncertainty over time and adjust the system according to changes (9). In general, using tools and approaches that seek and apply feedback and new information to decision-making facilitates adaptive management. For example, risk assessments clarify the scale of local needs; clients, staff and partners surveys provide insights on effectiveness; monitoring identifies stepwise changes in conditions; scenario-planning of project performance and failure under diverse conditions identifies limitations; and pilot projects or pretesting helps improve project or process design before scaling up. Each of these processes or tools provides ways of introducing phased implementation and allowing for adjustments and modifications to be made based on early lessons and available information. This framework encourages adaptive management approaches and processes.
Ensure community approaches and voices to strengthen health action
Community action is critical to achieve climate-resilience relevant to each of the 10 components listed below. The health impacts of climate change on individuals and communities are determined at the local level by changes in local conditions and health behaviours from available information. Thus partnerships of government, academic institutions and civil society with communities are key to understanding the nature of local risks and vulnerability, and to developing appropriate solutions to protect health. Communities can play important roles in improving the quality of assessments, risk monitoring, communications, capacity building and programming. Community-based action is a principal mechanism for ensuring that people themselves are informed, educated and able to take appropriate action to protect and maintain their individual and families’ health. Resilience can be strategically built through good development policy and practices that take climate change into consideration and empower communities.
3.5 Connecting to the “building blocks” of health systems
Health systems vary around the world, but all share some common features in their ultimate goals and general functions. WHO has identified six common “building blocks” (10) that are necessary to support the delivery of Universal Health Coverage and improved outcomes (Figure 3). To ensure that climate resilience builds on and strengthens existing health systems, these building blocks are taken as a starting point for the expansion of primary components that specifically enhance climate resilience.
Features of Adaptive Management
• Risk-informed
• Iterative processes
• Flexible
• Information seeking for learning
• Nonlinear
• Uses models and scenarios to understand future context
• Embraces risk and uncertainty as a way to increase learning

Applying a resilience approach to health systems 11
1. Leadership and governance. In addition to the core functions of ensuring good governance, evidence-informed policy and accountability within the traditional health system itself, the climate resilience approach requires leadership and strategic planning to address the complex and long-term nature of climate change risks. It particularly calls for collaboration to develop a shared vision among diverse stakeholders, and coordinated cross-sectoral planning to ensure that policies are coherent and health promoting, particularly in sectors that have a strong influence on health, such as water and sanitation, nutrition, energy and urban planning.
2. Health workforce. Overall, health system functioning relies on a sufficient number of trained and resourceful staff, working within an organizational structure that allows the health system to effectively identify, prevent and manage health risks. Building climate resilience requires additional professional training in linking climate change to health, and an investment in the organizational capacity to work flexibly and effectively in response to other conditions affected by climate change. It also requires raising the awareness of links between climate and health with key audiences (including but not limited to health policy makers, senior staff, the media), and in particular empowering affected communities to take ownership of their own response to new health challenges.
3. Health information systems. This building block focuses particularly on health information systems, including disease surveillance, as well as the research that is required to continue to make health-related progress against persistent and emerging threats. In the context of climate change, there is a specific need for: (i) information on vulnerability to climate risks, existing and expected future capacity of the system to respond, and identification of adaptations; (ii) integration of climate information into disease surveillance, providing an opportunity to develop early warning systems and more accurate target interventions; and (iii) guidance and utilization of the rapidly emerging body of research on health and climate change.
4. Essential medical products and technologies. This traditionally aims to ensure provision of proven, safe and cost-effective healthcare interventions. The challenge of climate change requires a wider perspective, which includes the selection of more climate-resilient intervention options both within the healthcare and in health-determining sectors, from renewable energy in health facilities to climate resilient water and sanitation infrastructure. It requires attention to utilization of innovative technologies (such as remote sensing for disease surveillance) and involves reducing the environmental impact of healthcare as a means to long-term sustainability.
5. Service delivery. Building and expanding traditional systems of healthcare delivery to enhance climate resilience includes attention to: (i) the integration of climate change considerations, particularly the use of meteorological information, into existing programmes for control of climate-sensitive diseases (e.g. vector-borne diseases); (ii) improved management of the environmental determinants of health, such as water and sanitation, nutrition and air quality, taking into account the modifying effect of socioeconomic conditions; and (iii) disaster risk reduction, emergency preparedness and management, in relation to the health consequences of extreme weather events, such as heat waves, floods and droughts.
6. Financing. In addition to meeting the existing large demand of financing curative interventions within healthcare systems, there is a need to consider a potential increase

12 Operational framework for building climate resilient health systems
in healthcare costs due to climate-sensitive diseases, and develop new models to finance preventive intersectoral approaches. This can include leveraging climate change specific funding streams.
3.6 Ten components for building climate resilience
In order to provide a comprehensive health response to climate change, health decision makers need to consider the full range of functions that need to be strengthened to increase climate resilience.
Starting from health sector building blocks, and taking into account existing global and regional mandates, the operational framework elaborates on 10 components that together provide a comprehensive approach to integrating climate resilience into existing health systems. These can provide the structure for a health adaptation plan, including the allocation of roles and responsibilities, as well as human and financial resources.
FIGURE 3: Ten components comprising the WHO operational framework for building climate resilient health systems, and the main connections to the building blocks of health systems
C L I M AT E R E S I L I E N C E
Bu
ilding blocks
of health system
s Health information systems
Service delivery
Financing
Leadership & governance
Essential medical
products & technologies
Health workforce
HEALTH &
CLIMATE RESEARCH
CLIMATE RESILIENT
& SUSTAINABLE
TECHNOLOGIES AND INFRASTRUCTURE
MANAGEMENT OF
ENVIRONMENTAL
DETERMINANTS
OF HEALTH
CLIM
ATEINFO
RMED
HEA
LTH PRO
GRAM
MES
& M
AN
AGEM
ENT
PREP
ARE
DN
ESS
EMER
GEN
CY
INTE
GRA
TED
RIS
KM
ON
ITO
RIN
G &
EARL
Y W
ARN
ING
ASSESSMEN
TADAPTATIO
NCAPACITY &
VULN
ERABILITY,
WORKFORCE
HEALTH
GOVERNANCE LEADERSHIP &
HEALTH FINANCING
CLIM
ATE &
10 components to build climate resilient health systems

Applying a resilience approach to health systems 13
3.7 How to use the framework
The framework components should be used to mainstream climate change into sector-wide or vertical programmes, as well as guide the holistic design of NAPs. Each component plays an important role in strengthening system capacity to address climate change. As a systemic approach, there are strong connections between the various components that serve to reinforce one another. A sound climate adaptation plan will therefore include many, if not all, of the 10 components.
Health systems vary, as do the scale and nature of the challenges with which they are faced. Therefore, the framework is not to be used as a definitive and rigid structure, but as a flexible approach that should be adapted to the national and local context.
The following sections provide a description of the main issues to consider under each component, along with proposed objectives and examples of measurable outputs to enhance climate resilience.

14 Operational framework for building climate resilient health systems
Components
4.1 COMPONENT 1: leadership and governance
This component refers to the strategic consideration and management of the scope and magnitude of climate related stress and shocks to health systems now and in the future, and their incorporation into strategic health policy, both within the formal health system and in health-determining sectors.
Within the formal health sector, political leadership and the will to address the health risks of climate change are essential to ensure implementation across the full range of programmes for climate-sensitive health risks. This includes ensuring collaboration between all relevant health divisions, such as environmental health; vector control; water, sanitation and hygiene; disaster management; health information systems; policy; and finance.
At the same time, an effective response to climate change implies assessment, monitoring, regulation and management of climate-related health risks that originate in other sectors. These sectors include agriculture and food; water; waste; energy; transport; labour and industry; land planning; housing and infrastructure; and disaster management. At the national level, these sectors in most countries have active programmes to respond to the impacts of climate change. With adequate coordination, investments in these sectors can be leveraged to also maximize health protection.
Accountability is an integral part of health governance. This therefore also requires engagement with, and accountability to, the wider community that are affected by the decisions taken on their behalf.
Objectives for the implementation of this component
Governance: specific responsibility and accountability mechanisms on climate change and health established within the health ministry.
Policy: climate variability and change considerations reflected in main health policies and programmes.
4GOVERNANCE
LEADERSHIP & W
ORKFO
RCEH
EALTH
OF
HEA
LTH
DET
ERM
INA
NTS
EN
VIRO
NM
ENTA
L M
ANAG
EMEN
T O
F
PRO
GRAM
MES
HEA
LTH
CLIM
ATE
INFO
RMED
& MANAGEMENT
PREPAREDNESS
EMERGENCY FINANCING
CLIMATE & HEALTH
ASSESSMENT
ADAPTATION
CAPACITY &
VULN
ERABILITY, EARLY WARNING
MONITORING &
INTEGRATED RISK
RESEARCHCLIMATE
HEALTH &
INFRASTRUCTURE
TECHNOLOGIE
S &
& SUSTAINABLE
CLIMATE RESILI
ENT
Political commitment and effective leadership to build climate resilience
• Policy prioritization and planning to address climate risks
• Inclusive policies encouraging high degree of social and economic equity
• Legal and regulatory systems which protect health and emergency policies and planning
• Institutional mechanisms, capacities and structures, and allocation of responsibilities to address climate
• Partnerships
• Accountability and community participation.

Components 15
Cross-sectoral collaboration: cross-sectoral collaboration strengthened and synergies maximized to ensure that decisions taken in other sectors protect and promote health.
Examples of measurable outputs
Governance
• Climate change and health focal points designated within the health ministry with specific programme of action and budget allocated.
• Climate change and health focal points or units, working in collaboration with relevant climate-sensitive health programmes (e.g. vector-borne diseases, nutrition, infectious diseases, disaster risk reduction) to build resilience of programmes.
Policy
• National strategy on health and climate change and/or H-NAP developed.
Cross-sectoral collaboration
• Agreements (e.g. Memoranda of Understanding) established between the health ministry and main stakeholders at the national level (e.g. meteorological services, ministries of environment, food and agriculture, energy, transport, planning), include specific roles and responsibilities in relation to protecting health from climate change.
• Health representation ensured in main climate change processes at national, regional and global levels (e.g. UNFCCC meetings and Conference of the Parties (COP), NAP, national communications to the UNFCCC).
• Main policies and strategies from health-determining sectors reflect climate change and health considerations both in relation to adaptation (e.g. climate-resilient water safety plans) and mitigation (e.g. health cobenefits in transport policies).
• Health impact assessments conducted for new mitigation and adaptation policies and programmes in all health-determining sectors, in accordance with article 4.1.f of the UNFCCC.

16 Operational framework for building climate resilient health systems
4.2 COMPONENT 2: Health workforce
This component refers to strengthening of technical and professional capacity of health personnel, the organizational capacity of health systems, and their institutional capacity to work with others.
Development of capacities specifically for climate change and health should build upon and support the more general effort to ensure adequate baseline levels of health competencies in health policy and management, research and analysis, healthcare and public health service delivery.
A health system relies upon an effective health workforce to achieve the best health outcomes possible, given available resources and circumstances. Climate variability and change may increase local demand for services, thus potentially altering the number of health workers and staff required, the type of health workers, as well as their level of training.
Technical and professional capacity of health staff can be developed through training, education, mentoring as well as experiential trial and error to: understand and use climate information for health decision-making, engage in cross-sectoral monitoring, conduct research and interventions, and effectively manage changing risks to health and health system performance. In addition, a range of competencies would become increasingly important, such as the ability to effectively work and communicate across disciplines, analytical skills to interpret and use nonhealth information for decision-making, and the ability to communicate climate risks to health actors and the public.
Organizational capacity refers to the availability of sufficient financial and human resources to cope with the health threats of climate change. This includes the efficient and targeted use of resources, information, knowledge and processes employed by the organization (such as resource mobilization and income generation, human resources and staffing, programme and process management), which enhance the resilience and adaptive capacity of a health system to address risks associated with climate change.
It is also strategically important to develop institutional capacity, including the ability of health systems to partner with other actors. This involves the ability to define and fulfil responsibilities in collaboration with other sectors, and communicate with the
public, including through the media. It is therefore important to build awareness and media capacity to effectively and responsibly communicate climate risks and associated
Guiding principles for capacity building on climate change and health
• Build on existing efforts, standards and best practices undertaken at all levels
• Focus on actors’ needs. In order to ensure the implementation of accurate interventions, any initiative on capacity development at any level should start by a capacity assessment of the corresponding health system
• Foster collaboration and partnerships, especially with and between countries and regions, and within and between related departments and units
• Enhance the sustainability of capacity building efforts by integrating climate change at early stages of professional health training
• Engage with wider audiences outside of the core health community, including other sectors, the media and community groups.
GO
VERN
AN
CELE
AD
ERSH
IP &
W
ORKFORCE
HEALTH
OF HEALTH
DETERMINANTS
ENVIRONMENTAL
MANAGEM
ENT OF PROGRAMMES HEALTH
CLIMATEINFORMED
& MANAGEMENT
PREPAREDNESS
EMERGENCY
FINANCI
NG
CLIMATE
& H
EALT
H
ASSESSMENTADAPTATION CAPACITY & VULNERABILITY,
EARLY WARNING
MONITORING &
INTEGRATED RISK
RESEARCHCLIM
ATE HEALTH &
INFRASTRUCTURETECH
NO
LOG
IES & &
SUSTA
INA
BLE CLIM
ATE RESILIENT

Components 17
uncertainty, as well as identify how to best disseminate appropriate and constructive public service announcements.
Communities need to be aware of the challenges around them, involved in risk identification and decision-making, and empowered to effectively protect themselves. Community groups and leaders need to be prepared for local risks, know what role they play in prevention and response, and be aware of potential effective solutions and resources available to them. Communities also often have rich local information about risks, community capacity and vulnerability that can help to guide the formulation of responses. Outreach, partnerships, stakeholder engagement, and effective two-way dialogue are vital to improving how the health system works with the community.
Other sectors need to be aware of the scope and scale of health risks that originate within their sectors; and the need for effective dialogue to enable effective collaborative planning, policy and implementation of actions with cobenefits to health.
Objectives for the implementation of this component
Human resources: sufficient number of health workers with the required technical capacity available to deal with the health risks posed by climate variability and change.
Organizational capacity development: resources, information, knowledge and processes employed by health organizations used in an efficient and targeted manner in the face of additional risks posed by climate variability and change.
Communications and awareness raising: raise awareness of the link between climate variability/climate change and health outcomes among different target audiences (e.g. policy makers, senior staff, media and communities).
Examples of measurable outputs
Human resource skill building, training and education
• Training courses on climate change and health topics targeting health personnel conducted.
• Curricula on climate change and health developed and imparted at secondary and/or tertiary levels.
Organizational capacity development
• Contingency plans for the deployment of sufficient health personnel in case of acute shocks, such as extreme weather events and outbreaks developed at the relevant level (i.e. national, provincial, local).
• Realistic and innovative capacity-building plans (e.g. from capacity or vulnerability and adaptation assessments) developed to address identified human resources and institutional capacity gaps.

18 Operational framework for building climate resilient health systems
• Contingencies, adaptation costs and potential losses and damages from climate change incorporated by management staff into investment plans.
Communications and awareness raising
• Development and implementation of internal and external communication plans (including the development of knowledge products) to raise awareness of health and climate change, and response options targeting key audiences, such as health professionals and decision-makers, communities, the media and other sectors.
• Health professionals, the media and community leaders trained in risk communication, including communication of uncertainty.
• Stakeholder forum on protecting health from climate change established as a way to engage health-determining sectors and the community.

Components 19
4.3 COMPONENT 3: Vulnerability, capacity and adaptation assessment
This component includes the range of assessments that can be used to generate policy-relevant evidence on the scale and nature of health risks, and the most vulnerable populations, taking into account the local circumstances.
Health risks vary depending on the nature of the exposure (e.g. if the location of a population makes it prone to drought or to flooding), the projected changes in climatic conditions and associated hazards (e.g. projected change in precipitation patterns or climate suitability for infectious disease transmission), socioeconomic and environmental determinants at the population and individual level (e.g. age, gender, coverage of water, sanitation and hygiene systems), and the capacity of health systems to protect from current and future risks (e.g. the effectiveness of disease surveillance systems and the degree to which they are flexible to sudden shocks or to gradually changing patterns of disease risk). Similarly, the scope of available adaptation options will depend on the governance and institutional arrangements within the country, and the availability of human and financial resources, among other factors.
Climate vulnerability and adaptation (V&A) assessments are an essential tool for health policy and programmatic planning (11). Their objective is to assess which populations are most vulnerable to different kinds of health effects, to identify weaknesses in the systems that should protect them, and to specify interventions to respond. Assessments can also improve evidence and understanding of the linkages between climate and health, serve as a baseline analysis against which changes in disease risk and protective measures can be monitored, identify knowledge gaps, provide the opportunity for building capacity, and strengthen the case for investment in health protection. V&A assessments are not one-time studies, but iterative processes that involve phased investigation, periodic review, additional studies and assessments to update with new information, and active stakeholder communication.
Successful V&A assessment processes will often include inputs from academic experts, to ensure high quality evidence, as well as managerial and operational personnel to ensure relevance to policy and practice. The studies will examine health risks, such as heat stress, nutrition and vector-borne diseases separately, and consider how they interact with each other and with changes in other determinants, such as ageing and urbanization. Assessment teams will consider opportunities and constraints for responses throughout the causal pathway, from managing environmental health determinants, to disease surveillance, to control and treatment of specific diseases. Critically, the process will involve a range of stakeholders and use information from a variety of sources, including health and nonhealth scientific information, as well as community knowledge and feedback.
WORKFORCE
HEALTH
OF HEALTHDETERMINANTS
ENVIRONMENTAL
MANAGEMENT OF
PROGRAMM
ES
HEALTH
CLIMATEINFORM
ED
& M
ANAG
EMEN
TPR
EPAR
EDN
ESS
EMER
GEN
CY
FIN
ANCI
NG
CLIM
ATE
& HEA
LTH
ASSESSMENT
ADAPTATION
CAPACITY &
VULNERABILITY,
EARLY WA
RNIN
GM
ON
ITORIN
G &
IN
TEGRATED
RISK
RESEARCH
CLIMATE
HEALTH & INFRASTRUCTURE
TECHNOLOGIES &
& SUSTAINABLE
CLIMATE RESILIENT
GOVERNANCE
LEADERSHIP &
Steps of vulnerability and adaptation (V&A) assessments
• Assess frame and scope
• Establish baseline conditions
• Assess the potential health impacts of future climate change
• Identify adaptation options
• Assess resources
• Ensure synergies and optimize trade-offs with other objectives
• Establish an iterative process for monitoring changes in health risks associated with climate change, and review adaptation options.

20 Operational framework for building climate resilient health systems
Throughout the V&A assessment process a range of additional studies, analytical exercises and tools may be used to gain a more holistic perspective of health vulnerability to climate. These include:
• Vulnerability and risk mapping• Modelling• Scenario development• Health system capacity and performance assessments• Economic assessments• Health impact assessments of decisions in other sectors• Specific risk, events and hazard assessments.
Objectives for the implementation of this component
Vulnerability: a sound understanding of the main health risks posed by climate vulnerability and change, and of the most vulnerable population groups available in the country or region.
Capacity: baseline information on capacities and gaps within the health system to face the challenges posed by climate change.
Adaptation options: information on the main adaptation options available, including their comparative advantages, potential costs and efficiency, available for selection by health system decision makers.
Examples of measurable outputs
Vulnerability
• Baseline rates and climate sensitivity of health conditions, allowing selection of priority risks, and continuous monitoring of changing risk conditions and health status assessed.
• Most vulnerable populations and areas prone to health risks of climate change identified.• Health impact assessments for key adaptation and mitigation policies and programmes
of health-determining sectors conducted.
Capacity
• Baselines on existing human resources, technical and health service delivery capacity established, with identification of weaknesses.
• Recommendations made for addressing gaps and building health system capacity.
Adaptation options
• Assessment results used to prioritize allocation of resources and effective interventions in health and related sectors for high risk and vulnerable populations.
• Plan defined and mechanism established for iterative review of health vulnerability and adaptation options.

Components 21
4.4 COMPONENT 4: Integrated risk monitoring and early warning
Climate change is altering the incidence and distribution of many important health risks including the occurrence of extreme weather events, and the transmission of vector-, water- and food-borne diseases. Building climate resilience entails: (i) developing adequate capacity and flexibility to understand how climatic conditions influence health outcomes; (ii) being able to anticipate changing health risks; and (iii) informing preparedness, surveillance and response to needs in a timely manner.
The objective of integrated risk monitoring is to generate a holistic perspective of health risks with real-time information. It uses a set of diverse instruments to bring together information about climatic and environmental conditions, health conditions and response capacity. It is the basis for establishing early warning systems to identify, forecast and communicate high-risk conditions.
Integrated risk monitoring refers to the use of early detection tools and epidemiological surveillance used in conjunction with direct and remote sensing technologies for surveillance of environmental determinants of health (e.g. water and air quality, variability in ambient temperature and humidity, or incidence of extreme weather events). Monitoring a broad range of signals around a health risk can allow changing conditions to be identified more quickly in order to anticipate outbreaks and emergencies related to weather and climatic conditions. One advantage of integrated monitoring is that environmental data may be more standardized and readily available than population health data.
Tracking qualitative and quantitative information about community and health system vulnerability, preparedness and response capacity levels are also important components of risk monitoring. For example, it is important to maintain up-to-date information on: whether high-risk regions have adequate staff and supplies during cyclone season; whether certain areas have high concentrations of vulnerable groups; and to identify regions and/or health facilities that could be more vulnerable to extreme events due to setbacks caused by recent disasters, loss of leadership or resources.
Health early warning systems are designed to anticipate and alert the public and health professionals that a rapid-onset emergency, such as an extreme weather event or disease outbreak, is expected. This advanced alert can provide additional lead-time to deploy appropriate preparedness measures and responses. Effective monitoring and early warning systems can prevent avoidable illness, injury and death when coupled with adequate response capacity.
WORKFORCEHEALTH
OF HEALTH
DETERMINANTS
ENVIRONMENTAL
MANAGEMENT OF
PROGRAMMES
HEALTH CLIMATEINFORMED
& MANAGEMEN
T
PREPAREDNESS
EMERGENCY FI
NAN
CIN
GCL
IMAT
E &
HEA
LTH
ASSESSMENT
ADAPTATION
CAPACITY &
VULNERABILITY,
EARLY WARNING
MONITORING &
INTEGRATED RISK
RESEARCH
CLIMATE
HEALTH
&
INFRASTRUCTURE
TECHN
OLOGIES &
& SU
STAINABLE
CLIMATE RESILIENT
GO
VERN
ANCE
LEAD
ERSH
IP &
Key environmental risks to monitor
• Extreme weather events, e.g. heavy rainfall, wind and sandstorms
• Temperatures known to induce heat or cold stress
• Air quality
• UV radiation
• Rainfall and humidity levels that favour or restrict vector abundance
• El Niño/La Niña years
• Seasonal allergen loads and occurrences
• Water availability and quality
• Water and sanitation infrastructure preparedness for extreme events.

22 Operational framework for building climate resilient health systems
Information sources on climate-risks may originate from local community knowledge, as well as multiple fields of scientific and practice-based knowledge (epidemiology, meteorology and climate, environment, agriculture, water resource management, etc.). Relevant information may be qualitative or quantitative, as well as observational or modelled. Because information on environmental and climate conditions are generally best collected and analysed by their respective authorities, health authorities are not always expected to collect these additional data. It is recommended to establish partnerships with meteorological agencies, hydrological services, or others to access and appropriately interpret nonhealth information.
Objectives for the implementation of this component
Integrated disease surveillance and early warnings: data on climate-sensitive environmental risks and epidemiological trends collected, analysed and interpreted on a continual basis and timely response to risks promoted.
Monitoring: information on climate change impacts, vulnerability, response capacity and emergency preparedness capacity reported over time.
Communication: timely warnings communicated to health decision-makers, the media and the public and translated into effective action to prevent negative health outcomes.
Examples of measurable outputs
Integrated disease surveillance and early warnings
• Early detection tools (e.g. rapid diagnostics, syndromic surveillance) used to identify changing incidence and early action triggered.
• Geographic and seasonal distribution of health risks and outcomes (i.e. risk mapping) tracked.
• Early warning systems for relevant extreme weather events and climate-sensitive diseases (e.g. heat-stress, zoonotic diseases, undernutrition) established.
Monitoring
• Indicators on climate change impacts, vulnerability, response capacity and emergency preparedness capacity, as well as climate and environmental variables included in relevant monitoring systems at national level and reported over time.
• Periodic reviews for improvements or deterioration of capacities identified in V&A assessments.
• Impacts of main environmental determinants of health monitored by the health sector.
Communication
• Communication strategy on climate risks to health developed and implemented, outlining the scope of information for diverse audiences (e.g. media, public, health personnel and other sectors) and events, including who should communicate, and the means of communication.
• Community engagement and feedback mechanisms established to empower affected populations to respond to warnings, and to guide future development of monitoring and warning systems.
Vertical spacing
adjusted

Components 23
4.5 COMPONENT 5: Health and climate research
Building climate resilience calls for both basic and applied research so as to reduce uncertainty about how local conditions may be affected, gain insight into local solutions and capacities, and build evidence to strengthen decision-making.
Research from global to local level can be used to gather knowledge on climate risks to health; the modulating effect of social and environmental determinants; climate-sensitivity of diseases and risks; how communities and health systems currently understand and cope with climate risks; how local conditions and vulnerabilities are connected to broader determinants; and the degree to which communities and local health services are prepared to cope with climate-related changes and shocks. Applied research that can develop and test new technologies, data tools and instruments, and strategies for risk management are also critical to evidence-based decision-making.
Research should inform existing knowledge management platforms, be effectively communicated, and find opportunities to be translated to practice. Guidance on priority knowledge gaps and ideas to shape national research can be found in global and regional level research agendas, such as those led by WHO (12). These may be made more relevant through adaptation to the specific national or subnational context.
Objectives for the implementation of this component
Research agenda: multidisciplinary national research agenda on climate change and health defined and endorsed by stakeholders.
Support for research: research capacity on climate change and health built by supporting relevant multidisciplinary networks, making available financial resources and creating training opportunities.
Connect to policy: research findings on climate change and health disseminated to and used by policy makers.
Examples of measurable outputs
Research agenda
• National research agenda on climate change and health defined through the organization of a stakeholder forum involving representatives from health and other government ministries, research institutions, nongovernmental organizations, the private sector and vulnerable populations.
WO
RKFO
RCE
HEAL
TH
OF HEALTH
DETERM
INANTS
ENVIRO
NMENTAL
MAN
AGEMENT OF PROGRAMMES
HEALTH
CLIMATEINFORMED
& MANAGEMENT
PREPAREDNESS
EMERGENCY
FINANCING
CLIMATE &
HEA
LTH
ASSESSMENTADAPTATION
CAPACITY &
VULNERABILITY,
EARLY WARNING
MONITORING &
INTEGRATED RISK
RESEARCH
CLIMATE
HEALTH &
INFRASTRUCTURETECH
NO
LOG
IES &
& SUSTA
INA
BLE CLIM
ATE RESILIENT
GOVE
RNA
NCE
LEAD
ERSH
IP &

24 Operational framework for building climate resilient health systems
Support research
• Access to and linkage of data on meteorological information, health determinants and outcomes enabled.
• Multidisciplinary research partnerships, knowledge management networks and rosters of local experts established.
• Financial backing mechanisms to support research programmes and postgraduate training programmes established.
Connect to policy
• Mechanism established for researchers to inform planning, policy and stakeholder groups.• Policy makers included in the definition and review of research agendas.

Components 25
4.6 COMPONENT 6: Climate resilient and sustainable technologies and infrastructure
Health system resilience to climate risks builds on provision of essential preventive and curative health products, from vaccines for climate-sensitive diseases to surgical equipment. It can be further enhanced through investment in specific technologies that can reduce vulnerability to climate risks, both within and outside the traditional health sector.
One important component is the provision of climate resilient health infrastructure and services. This includes ensuring that the siting of health facilities and the building codes that are applied account for current and projected future climate risks, such as the potential for increased frequency and intensity of heat waves, cyclones or storm surges. It also includes consideration of climate resilience of essential environmental services to health facilities, such as water and sanitation services which may be compromised by flood or drought, and electricity supply that may be cut off during extreme weather events (13). Changing climatic conditions can also influence the effectiveness of specific medical products. For example, antidepressants, antihistamines, antipsychotics and diuretics may predispose their users to heat stroke or heat stress when temperatures are high.
Climate resilience can also be enhanced through the use of new technologies or approaches for better delivery of health interventions, particularly through the use of information technology. Satellite-based remote sensing of meteorology and environmental conditions on the ground have proven effective in improving the reliability of weather warnings, monitoring, surveillance and risk mapping the probability of transmission of water-borne and vector-borne diseases. Mobile communications have increased the speed and volume of health data collection while reducing costs and improving emergency response. Advances in information management technologies have greatly enhanced capacity to analyse connections between environmental and health data. Systematic integration of these technologies into disease surveillance systems can support vulnerability and adaptation assessment, as well as surveillance and early warning.
Selection of medical technologies and products with lower environmental footprint can also contribute to climate resilience and long-term sustainability. Processes and technologies such as solar-powered photovoltaics, water pumps and vaccine chains can enhance resilience by ensuring independent water and energy supplies to remote rural facilities, and for health operations during emergencies. Use of technologies with lower energy demand can simultaneously increase resilience and decrease the impact of the health sector on the environment, such as reduced emissions of climate-altering pollutants associated with energy generation. Health systems constitute a significant share of many national economies (14). They can therefore make an important contribution to overall sustainability by taking into account environmental impacts in relation to their procurement of medical technologies, as well as energy, water, buildings, transport, food, waste disposal and management.
WORKFORCE HEALTH
OF HEALTHDETERMINANTS ENVIRONMENTAL MANAGEMENT OF
PROGRAMMES
HEALTH
CLIMATEINFORMED
& MANAGEM
ENT
PREPAREDNESS
EMERGENCY
FINA
NCIN
GCLIM
ATE & H
EALTH
ASSESSMENT
ADAPTATION
CAPACITY &
VULNERABILITY,
EARLY W
ARN
ING
MONIT
ORING
&
INTEG
RATE
D RI
SK
RESE
ARC
HCL
IMAT
E H
EALT
H &
INFR
ASTRUCTURE
TECH
NOLOGIES &
& SUSTAIN
ABLE
CLIM
ATE RESILIENT
GOVERNANCE
LEADERSHIP &

26 Operational framework for building climate resilient health systems
Objectives for the implementation of this component
Adaptation of current infrastructures, technologies and processes: future climate risks systematically considered with regard to revision or upgrading of technologies, products and procedures for health system service delivery.
Promotion of new technologies: new technologies, processes and products selected and deployed to increase climate resilience through enhanced health service delivery.
Sustainability of health operations: low environmental impact technologies procured and promoted by the health sector to enhance resilience to climate and contribute to long-term sustainability.
Examples of measurable outputs
Adaptation of current infrastructures, technologies and processes
• Specifications for siting and construction of health facilities, and energy, water and sanitation provisions revised in line with projected climate risks.
• Training and recommendations for prescription of pharmaceuticals during extreme heat conditions revised.
Promotion of new technologies
• New technologies such as eHealth or satellite imagery used to improve health system performance.
Sustainability of health operations
• Impact of health sector on the environment assessed, and appropriate mechanisms to monitor carbon emissions and environmental impacts developed.
• Sustainability in selection of products and procurement of services including energy, water, transport and waste management assessed and prioritized by health facilities.

Components 27
4.7 COMPONENT 7: Management of environmental determinants of health
Climate change threatens health through environmental determinants, strongly mediated by social conditions. For this reason, some of the most effective actions that can be taken by health systems are in collaboration with other sectors, i.e. through promoting a “Health in all policies” approach.
Scaling up multisectoral public health prevention programmes can avoid negative health outcomes at their source and facilitate timely and increasingly effective responses to changing environmental and climate-related risk conditions. Health-related policies and programmes in sectors, such as agriculture, transport, housing and energy can lead to reduced health risks and improved health practices, behaviours and processes.
While the health sector does not usually have direct control over environmental determinants, they have essential roles to play at both policy and programmatic levels in providing evidence and raising awareness, joint monitoring of environmental exposures and outcomes, defining regulatory standards and management of health risks. This requires active coordination and intersectoral planning.
TABlE 2: Examples of joint actions between ministries of health and other sectors to manage the environmental determinants of health
Environmental determinants of health
Important collaborating sectors
Examples of joint action
Air quality Industry and labour
Energy
Transport
Definition and monitoring of air quality standards, worker safety standards for heat
Promotion of energy-efficient heating and cooking
Joint implementation of health impact assessments for key transport programmes
Water quantity and quality
Water resources Integration of health in water resources management policy
Implementation of climate resilient water safety plans
Definition and monitoring or water quality standards
Food and nutrition security
Agriculture and food safety
Food security forecasting and nutritional screening
Integrated vector management
Housing Land planning
Housing and infrastructure
Disaster management
Zoning and building regulations for health and other infrastructure taking account of flood and storm risks
Ventilation standards and improved housing and building design
Health and public safety plans and training for extreme weather events
Waste management Municipal services Waste minimization, safe disposal and recycling
WORKFORCE
HEALTH
OF H
EALTH
DETERMINANTS
ENVIR
ONMENTAL
MANAGEMENT OF
PROGRAMMESHEALTH CLIMATEINFORMED
& MANAGEMENT
PREPAREDNESS
EMERGENCY
FINANCING
CLIMATE & H
EALTH
ASSESSMENT ADAPTATION CAPACITY & VULNERABILITY,
RESE
ARCH
CLIM
ATE
HEALT
H &
INFR
ASTR
UCTU
RE
TECH
NO
LOG
IES
&
& S
UST
AIN
ABLE
CLIM
ATE
RESI
LIEN
T
GO
VERNAN
CE
LEAD
ERSHIP &
EARLY WARNING
MONITORING &
INTEGRATED RISK

28 Operational framework for building climate resilient health systems
Objectives for the implementation of this component
Monitoring: joint monitoring of climate-sensitive environmental risks against evidence-based standards.
Regulation: regulatory policies protecting populations against climate-sensitive environmental risks defined, revised and enforced.
Coordinated management: environmental determinants of health jointly managed, with clear roles and responsibilities defined across sectors.
Examples of measurable outputs
Monitoring
• Integrated monitoring systems allowing collection and analysis of data on environmental hazards, socioeconomic factors and health outcomes established.
• Evidence-based quality standards for climate-sensitive environmental conditions defined.
Regulation
• Regulations on key environmental determinants of health (air quality, water quality, food quality, housing safety, waste management) revised and enforced to reflect broader ranges of expected climatic conditions.
• Building regulations and waste management infrastructure, environmentally sustainable and resistant to likely local extreme events promoted.
Coordinated management
• Health impact assessments for policy and programmes in sectors such as transport, agriculture and energy, implemented.
• Joint multisectoral risk management approaches to health risks related to disasters, water, waste, food and air pollution (e.g. food safety, diarrhoeal disease control, integrated vector management, joined-up risk communication) undertaken.

Components 29
4.8 COMPONENT 8: Climate-informed health programmes
Health programming and operations should consider climate risks and vulnerability and increasingly become climate-resilient through assessment, programming and implementation.
In addition to collaboration with other actors, the health sector is also often directly responsible for programmes that address climate-sensitive health risks (such as vector-borne and water-borne diseases), health response during extreme weather events and nutritional crises.
Health programming and operations should increasingly be designed and implemented taking into account both current climate variability and projected future climate change. In combination with other factors, these will influence the geographical distribution, timing of occurrence and intensity of burden of these climate-sensitive diseases.
Existing efforts in disaster risk reduction, public health preparedness, and several vertical programmes for communicable and noncommunicable diseases may either not be adequate, be rendered ineffective or unsustainable, or not be needed. Such programmes can become climate resilient by using information about current and projected future climate conditions to identify capacity gaps and inform policy, strategic investment and planning decisions.
Specific health programmes can use information gathered through the implementation of the component related to “information and early warning systems” (e.g. V&A assessments, research, integrated risk monitoring and early warning systems) to improve their decision-making capabilities and adjust the scale of intervention accordingly. For example, health programming informed by early warnings about a potential outbreak or heat wave can use time wisely to prepare operations for increased patient loads and special needs. Climate-informed programming will continually review and adjust service delivery according to new information.
WORKFORCE
HEALTH
PROGRAMM
ES
HEALTH
INFORMED
CLIMATE& M
ANAG
EMEN
TPREPARED
NESS
EMERG
ENCY
FINANCING
CLIMATE & HEALTH ASSESSM
ENT
ADAPTATIO
N
CAPACITY &
VULNERABILITY
, RE
SEAR
CH
CLIM
ATE
HEA
LTH &
INFRASTRUCTURE
TECHNOLOGIES &
& SUSTAINABLE
CLIMATE RESILIENT
GOVERNANCE
LEADERSHIP &
EARL
Y W
ARN
ING
MO
NIT
ORI
NG
&
INTE
GRA
TED
RIS
K
OF HEALTHDETERMINANTS
ENVIRONMENTAL
MANAGEMENT OF
Departments and programmes that can become climate-informed
• Communicable diseases control (particularly by zoonotic and vector-borne disease control units)
• Noncommunicable diseases
• Water and sanitation
• Nutrition, food hygiene and safety
• Occupational health
• Environmental health
• Maternal and child health
• Geriatrics
• Mental health
• Disasters and emergency management
• Facilities management
• Health statistics and information
• Pharmacies.

30 Operational framework for building climate resilient health systems
TABlE 3: Examples of climate-informed health interventions
Climate-related health risks and mechanisms
Example of interventions
Extreme heat and thermal stress
•Establish occupational health exposure standards
•Improve health facility design, energy efficient cooling and heating systems
•Ensure public education to promote behaviour change, e.g. in relation to clothing, ventilation, etc.
•Develop heat-health action plans, including early warning, public communication, and responses, such as cooling centres for high-risk populations
Water-borne and food-borne diseases
•Enhance disease surveillance systems during high-risk seasons/periods
•Strengthen food and water quality control
Zoonotic and vector-borne diseases
•Expand the scope of diseases monitored, and monitor at the margins of current geographic distributions to detect spread
•Establish early warning systems if appropriate
•Establish vector/pest control
•Enhance diagnostic and treatment options in high-risk regions/periods
•Ensure adequate animal and human vaccination coverage
Allergic diseases and cardiopulmonary health
•Develop exposure forecasts – air quality, allergens, dust
•Enforce stricter air quality standards for pollution
•Establish allergen management
•Plan for increased demand for treatment during high-risk seasons or weather conditions
Nutrition •Perform seasonal nutritional screening in high-risk communities
•Scale up integrated food security, nutrition and health programming in fragile zones
•Promote public education and food hygiene
Storms and floods •Include climate risk in siting, designing or retrofitting health infrastructure
•Establish early warning and early action systems, including education and community mobilization
•Assess and retrofit or construct public health infrastructure (e.g. health facilities in flood-prone areas) to sustain increased extreme weather conditions, warmer temperatures, environmental changes
Mental health and disability
•Address special needs of mental health patients (as well as other disabilities) by developing emergency preparedness plans
•Address mental health needs of disaster- and trauma-exposed populations
•Establish community watch for people with mental illness during extreme weather conditions

Components 31
Objectives for the implementation of this component
Health programming: information on current and projected (future) climatic conditions integrated into strategic planning of health programmes for climate-sensitive diseases.
Delivery of interventions: public health programmes revise their standard operating procedures to respond to climate risks in delivery of interventions.
Examples of measurable outputs
Health programming
• Medium- and long-term plans for disease control programmes revised to consider capacities that may be stressed or exceeded by climate change.
• Investment plans defined to address identified capacity gaps.
Delivery of interventions
• Risk maps and analysis of seasonal trends in diseases used to target resources and preventive measures for those most at risk.
• Contingency plans for healthcare provision in extreme weather events, or delivery of interventions to control outbreaks of infectious diseases in new locations, developed and tested.

32 Operational framework for building climate resilient health systems
4.9 COMPONENT 9: Emergency preparedness and management
Outbreaks and health emergencies triggered by climate variability are primary concerns of climate change. Climate-informed preparedness plans, emergency systems, and community-based disaster and emergency management are essential for building climate resilience. Thus, health systems and communities should aim to holistically manage overall public health risks and emphasize preparedness in addition to the usual focus on response capacity. Responses are often late and dominated by ‘emergency’ programming and crisis response, which are resource intensive and not effective in building resilience.
Health operations including healthcare and public health infrastructure should be increasingly prepared to address changing population catchments, service demands, increase emergency response and operate under diverse environmental conditions. For example, new facilities and service routes should be appropriately located and adequately robust to be safe and remain functional during the type of extreme weather events projected for a particular area. This includes infrastructure for water supplies, drainage, waste disposal and sanitation, as well as telecommunications, energy supplies and medical transport. Another example is that pharmacies should have protocols and practices for safe storage and transport of pharmaceuticals, vaccines and medical equipment in extreme heat conditions.
Community-based actions are at the forefront of protecting health in emergencies. Community knowledge of local risks and vulnerable groups is essential to identify and address actual needs of the community. A prepared, active and well-organized community can reduce risks, save lives and minimize the impact of emergencies.
WHO is in the process of developing an Emergency and Disaster Risk Management for Health (EDRM-H) Policy Framework, which includes principles, programmes and activities for effective management of risks (15).
WORKFO
RCEHEALTH
FINANCINGCLIMATE & HEALTH
ASSESSM
ENT
AD
APTATIO
N
CAPACITY &
VULN
ERABILITY,
RESEARCH CLIMATE HEALTH &
INFRASTRUCTURE
TECHNOLOGIES &
& SUSTAINABLE
CLIMATE RESILIENT
GOVERNANCE
LEADERSHIP &
EARLY WARNING
MONITORING &
INTEGRATED RISK
OF HEA
LTH
DETER
MIN
ANTS
ENVIRONM
ENTA
L
MANAGEM
ENT
OF
PRO
GRA
MM
ES
HEA
LTH
CL
IMAT
EIN
FORM
ED & M
ANAGEMENT
PREPAREDNESS
EMERGENCY
Managing changing risks of climate extremes and disasters
IPCC, special report on managing the risks of extreme events and disasters to advance climate change adaptation
• Measures that provide benefits under current climate and a range of future climate change scenarios, called low-regrets measures, are available starting points for addressing projected trends in exposure, vulnerability and climate extremes
• Effective risk management generally involves a portfolio of actions to reduce and transfer risk and to respond to events and disasters, as opposed to a singular focus on any one action or type of action
• Multihazard risk management approaches provide opportunities to reduce complex and compound hazards
• Opportunities exist to create synergies in international finance for disaster risk management and adaptation to climate change, but these have not yet been fully realized
• Stronger efforts at the international level do not necessarily lead to substantive and rapid results at the local level
• Integration of local knowledge with additional scientific and technical knowledge can improve disaster risk reduction and climate change
• Appropriate and timely risk communication is critical for effective adaptation and disaster risk management
• An iterative process of monitoring, research, evaluation, learning and innovation can reduce disaster risk and promote adaptive management in the context of climate extremes.

Components 33
Operational guidance is available for emergency managers to enhance capacity to manage the health risks associated with emergencies and disasters.
Objectives for the implementation of this component
Inform policies and protocols: emergency and disaster risk management protocols and policies adequately informed by current and likely future climatic conditions.
Risk management: strengthen health system capacity to manage risks so that overall vulnerability and exposure to hazards are reduced and residual risks and uncertainties effectively managed.
Empowerment of communities: empower communities to effectively prevent and respond to the health risks posed by extreme weather events.
Examples of measurable outputs
Inform policies and protocols
• Climate-sensitive health risks included under national disaster reduction strategy and plans, and wider development processes.
Risk management
• Risk assessments for current and projected future exposure to extreme weather events routinely used to inform health sector strategic development plans.
• Health sector contingency plans for extreme weather events developed, including risk reduction, preparedness and response, in line with the WHO emergency response framework.
• Emergency response plans for individual health facilities defined and implemented in case of need.
Community empowerment
• Stakeholder mechanism to support participation, dialogue and information exchange, to empower civil society and community groups as primary actors in emergency preparedness and response established.
• Capacity development programmes implemented to identify and support the roles of local communities to identify risks, prevent exposure to hazards and take action to save lives in extreme weather events.

34 Operational framework for building climate resilient health systems
4.10 COMPONENT 10: Climate and health financing
Effectively protecting health from climate change will incur financial costs for health systems. For example, health systems may need to expend resources to expand the geographic or seasonal range or population coverage of surveillance and control programmes for climate-sensitive infectious diseases, or to retrofit health facilities to withstand more extreme weather events. Additional investment may also be needed in other sectors to achieve health goals, such as implementing climate resilient water safety plans, or enhanced food security forecasting and nutritional screening during droughts.
In order to mobilize and apply resources to these issues, assessments of resource requirements, available finance, finance gaps and opportunities to fill them, are all needed. Resource requirements can be assessed through budgeting of interventions selected in the previously described components, and compared with existing budgets and funding sources to identify shortfalls that need to be addressed through mobilization of new resources. For example, if an increase in extreme weather events is predicted, then resources will need to be mobilized for contingencies or to cover the costs of insurance or replacement costs for damaged health facilities, and lost or damaged uninsured equipment in extreme weather events. Planning and management teams should consider that in addition to adequate development funds to maintain core healthcare and public health services (i.e. water/sanitation/environmental hygiene/disaster and health emergency preparedness), climate change-specific funding mechanisms should be accessed so as to effectively build the resilience of the system.
A comprehensive approach to financing health protection from climate change will first build on core investments in the health sector, such as investments to ensure adequate numbers of trained health personnel, and basic health infrastructure and services, which also help to address climate change risks. This can be from national resources or external donors. For example, the Bill and Melinda Gates Foundation provides significant support to combat diarrhoeal diseases and malaria, as well as for emergency response, which simultaneously improves health and decreases vulnerability to climate change. The Global Fund to Fight AIDS, Tuberculosis and Malaria (GFATM) supports overall malaria control, including some investments specifically in collection of meteorological data, to predict and manage seasonal and inter-annual variations in malaria transmission.
Resources can also be mobilized by combining climate change and health considerations in investments in key health determining sectors. For example, national governments and donors make very large investments in water and sanitation, which improve health and generally reduce climate vulnerability. Adding criteria for climate resilience and health promotion to investment strategies can ensure that these investments bring the greatest
WORKFORCE
HEALTH
FINANCIN
G
CLIM
ATE &
HEALTH
ASSESSMEN
T
ADAPTATION
CAPACITY &
VULNERABILITY,
RESEARCH
CLIMATE
HEALTH & INFRASTRUCTURE TECHNOLOGIES & & SUSTAINABLE CLIMATE RESILIENT
GOVERNANCELEADERSHIP &
EARLY W
ARN
ING
MO
NITO
RING
&
INTEG
RATED RISK
OF HEALTH
DETERMINANTS
ENVIRONMENTAL
MANAGEMENT OF
PROGRAM
MES
HEALT
H
CLIMATE
INFO
RMED
&
MA
NAG
EMEN
T
PREP
ARE
DN
ESS
EMER
GEN
CY
Main climate change funding mechanisms
Global Environmental Facility• Least Developed Countries Fund:
http://www.thegef.org/gef/ldcf
• Special Climate Change Fund: http://www.thegef.org/gef/sccf
Kyoto Protocol• Adaptation Fund:
https://www.adaptation-fund.org/
UNFCCC• Green Climate Fund:
http://www.gcfund.org/home.html

Components 35
possible benefits in terms of human health, climate adaptation and social return on investment over the long term. This approach applies to international as well as national financing streams. For example, the Global Facility for Disaster Reduction and Recovery has funding streams on both adaptation and mitigation. Investments for risk reduction in sectors ranging from water resources to food and nutrition security can protect and promote health.
Opportunities are now becoming available to mobilize additional resources specifically to address additional risks presented by climate change, including for health. At the international level, the main multilateral mechanisms are mandated under the UNFCCC and the Kyoto Protocol, promoting financial assistance from more developed parties to those countries deemed more vulnerable and with fewer resources available to adapt to climate change. Parties to the UNFCCC have mandated the Global Environmental Facility (GEF) to manage the Special Climate Change Fund and the Least Developed Countries Fund, established the Adaptation Fund under the Kyoto Protocol and recently the Green Climate Fund (16). Further guidance on entry points for health under each of these funding streams is provided by WHO (17). In addition to the main international climate change specific funding mechanisms, funding is also available through bilateral and regional channels.
Objectives for the implementation of this component
Health-specific funding mechanisms: climate change considerations included in proposals related to climate-sensitive diseases submitted to and funded by health funding mechanisms.
Funding for sectors influencing health: health and climate change considerations incorporated in projects and programmes supported through development funding available for main health determining sectors.
Climate change funding streams: climate change funding mechanisms available at national level accessed.
Examples of measurable outputs
Health-specific funding mechanisms
• Resources to increase resilience to climate variability and climate change included as a line item in national or subnational health investment plans.
• Proposals to external donors to support control of climate-sensitive diseases (e.g. GFATM on malaria control) included climate variability and change.
Development funding in sectors influencing health
• Screening for climate variability, climate change risks and health protection, included as a criteria for selecting investments in key health determining sectors, such as water and sanitation, and food and nutrition security.
• Health impacts of climate change monitored in programmes funded through financial mechanisms specific to health-determining sectors.
Climate change funding streams
• Projects and programmes on building health system resilience submitted to and granted by the main international climate change funds (e.g. the GEF, Adaptation Fund, bilateral donors).
Vertical spacing
adjusted

36 Operational framework for building climate resilient health systems
Monitoring progressMonitoring of both the implementation of this framework and the extent to which its aim to build climate resilient health systems is achieved, is fundamental for it to be effective.
The intended ultimate impact of implementing the operational framework will be a decrease in the burden of climate-sensitive diseases, and a strengthening in the overall resilience of the health system. The following table includes proposed indicators of progress at the outcome level for each of the six building blocks of health systems. The examples of measurable outputs proposed for each of the components above has also been added to the table so as to provide a comprehensive monitoring framework.
5

Monitoring progress 37
TABl
E 4:
Exa
mpl
e in
dica
tors
for
mon
itori
ng th
e im
plem
enta
tion
of th
e W
HO
oper
atio
nal f
ram
ewor
k on
bui
ldin
g cl
imat
e-re
silie
nt h
ealth
sys
tem
s
Six
build
ing
bloc
ks o
f he
alth
sys
tem
s
Exam
ple
indi
cato
rs
at o
utco
me
leve
lTe
n co
mpo
nent
s of
the
oper
atio
nal
fram
ewor
k
Exam
ples
of m
easu
rabl
e ou
tput
s to
enh
ance
clim
ate
resi
lienc
e
lead
ersh
ip a
nd
gove
rnan
ceM
ain
polic
ies
and
stra
tegi
es f
or c
limat
e ch
ange
, he
alth
and
he
alth
-det
erm
inin
g se
ctor
s (e
.g. w
ater
an
d sa
nita
tion
, fo
od
and
nutr
itio
n se
curi
ty)
refle
ct c
limat
e ch
ange
and
hea
lth
conn
ecti
ons
lead
ersh
ip a
nd
gove
rnan
ceGo
vern
ance
•C
limat
e ch
ange
and
hea
lth
foca
l poi
nts
desi
gnat
ed w
ithi
n th
e he
alth
min
istr
y, w
ith
spec
ific
prog
ram
me
of
acti
on a
nd b
udge
t al
loca
ted.
•C
limat
e ch
ange
and
hea
lth
foca
l poi
nts
or u
nits
, w
ork
in c
olla
bora
tion
wit
h re
leva
nt c
limat
e-se
nsit
ive
heal
th
prog
ram
mes
(e.
g. v
ecto
r-bo
rne
dise
ases
, in
fect
ious
dis
ease
s, n
utri
tion
, di
sast
er r
isk
redu
ctio
n) t
o bu
ild
resi
lienc
e of
pro
gram
mes
.
Polic
y
•N
atio
nal s
trat
egy
on h
ealt
h an
d cl
imat
e ch
ange
and
/or
H-N
AP
dev
elop
ed.
Cros
s-se
ctor
al c
olla
bora
tion
•A
gree
men
ts (
e.g.
Mem
oran
da o
f U
nder
stan
ding
) be
twee
n th
e he
alth
min
istr
y an
d m
ain
stak
ehol
ders
at
nati
onal
leve
l sig
ned,
whi
ch in
clud
e sp
ecifi
c ro
les
and
resp
onsi
bilit
ies
in r
elat
ion
to p
rote
ctin
g he
alth
fro
m
clim
ate
chan
ge.
•H
ealt
h re
pres
enta
tion
ens
ured
in m
ain
clim
ate
chan
ge p
roce
sses
at
nati
onal
, re
gion
al a
nd g
loba
l lev
els
(e.g
. U
NFC
CC
mee
ting
s an
d C
OP,
NA
P, n
atio
nal c
omm
unic
atio
ns t
o th
e U
NFC
CC
).
•M
ain
polic
ies
and
stra
tegi
es f
rom
hea
lth-
dete
rmin
ing
sect
ors
refle
ct c
limat
e ch
ange
and
hea
lth
cons
ider
atio
ns b
oth
in r
elat
ion
to a
dapt
atio
n (e
.g. cl
imat
e-re
silie
nt w
ater
saf
ety
plan
s) a
nd m
itig
atio
n (e
.g.
heal
th c
oben
efits
in t
rans
port
pol
icie
s).
•H
ealt
h im
pact
ass
essm
ents
con
duct
ed f
or n
ew m
itig
atio
n an
d ad
apta
tion
pol
icie
s an
d pr
ogra
mm
es in
all
heal
th d
eter
min
ing
sect
ors
(in
acco
rdan
ce w
ith
arti
cle
4.1
.f o
f th
e U
NFC
CC
).
Hea
lth w
orkf
orce
Per
cent
age
of
heal
thca
re p
erso
nnel
w
ith
info
rmat
ion
and
trai
ning
to
addr
ess
clim
ate
chan
ge
and
heal
th li
nks,
ap
prop
riat
e to
the
ir
role
and
fun
ctio
n (a
s de
term
ined
by
a su
rvey
)
Hea
lth w
orkf
orce
Hum
an r
esou
rces
•Tr
aini
ng c
ours
es o
n cl
imat
e ch
ange
and
hea
lth
topi
cs t
arge
ting
hea
lth
pers
onne
l con
duct
ed.
•C
urri
cula
on
clim
ate
chan
ge a
nd h
ealt
h de
velo
ped
and
impa
rted
at
seco
ndar
y an
d/or
ter
tiar
y le
vels
.
Orga
niza
tiona
l cap
acity
dev
elop
men
t
•C
onti
ngen
cy p
lans
for
the
dep
loym
ent
of s
uffic
ient
hea
lth
pers
onne
l in
case
of
acut
e sh
ocks
, su
ch a
s ex
trem
e w
eath
er e
vent
s an
d ou
tbre
aks
deve
lope
d at
the
rel
evan
t le
vel (
i.e. na
tion
al, pr
ovin
cial
, lo
cal)
.
•R
ealis
tic
and
inno
vati
ve c
apac
ity-
build
ing
plan
s (e
.g. fr
om c
apac
ity
or v
ulne
rabi
lity
and
adap
tati
on
asse
ssm
ents
), d
evel
oped
to
addr
ess
iden
tifie
d hu
man
res
ourc
es a
nd in
stit
utio
nal c
apac
ity
gaps
.
•C
onti
ngen
cies
, ad
apta
tion
cos
ts a
nd p
oten
tial
loss
es a
nd d
amag
es f
rom
clim
ate
chan
ge in
corp
orat
ed b
y m
anag
emen
t st
aff
into
inve
stm
ent
plan
s.

38 Operational framework for building climate resilient health systems
Six
build
ing
bloc
ks o
f he
alth
sys
tem
s
Exam
ple
indi
cato
rs
at o
utco
me
leve
lTe
n co
mpo
nent
s of
the
oper
atio
nal
fram
ewor
k
Exam
ples
of m
easu
rabl
e ou
tput
s to
enh
ance
clim
ate
resi
lienc
e
Com
mun
icat
ions
and
aw
aren
ess
rais
ing
•D
evel
opm
ent
and
impl
emen
tati
on o
f in
tern
al a
nd e
xter
nal c
omm
unic
atio
n pl
ans
(inc
ludi
ng t
he d
evel
opm
ent
of k
now
ledg
e pr
oduc
ts)
to r
aise
aw
aren
ess
of h
ealt
h an
d cl
imat
e ch
ange
and
res
pons
e op
tion
s ta
rget
ing
key
audi
ence
s, s
uch
as h
ealt
h pr
ofes
sion
als
and
deci
sion
-mak
ers,
com
mun
itie
s, t
he m
edia
and
oth
er s
ecto
rs.
•H
ealt
h pr
ofes
sion
als,
the
med
ia a
nd c
omm
unit
y le
ader
s tr
aine
d in
ris
k co
mm
unic
atio
n, in
clud
ing
com
mun
icat
ion
of u
ncer
tain
ty.
•S
take
hold
er f
orum
on
prot
ecti
ng h
ealt
h fr
om c
limat
e ch
ange
est
ablis
hed
as a
way
to
enga
ge h
ealt
h-de
term
inin
g se
ctor
s an
d th
e co
mm
unit
y.
Hea
lth
info
rmat
ion
syst
ems
Num
ber
of c
limat
e-se
nsit
ive
dise
ases
fo
r w
hich
the
re a
re
mon
itor
ing
syst
ems
that
are
abl
e to
fo
reca
st a
nd m
onit
or
risk
s an
d/or
to
mon
itor
di
seas
e ri
sks
pose
d by
cl
imat
e va
riab
ility
and
ch
ange
Vuln
erab
ility
, ca
paci
ty a
nd
adap
tatio
n as
sess
men
t
Vuln
erab
ility
•B
asel
ine
rate
s, a
nd c
limat
e se
nsit
ivit
y of
hea
lth
cond
itio
ns, al
low
ing
sele
ctio
n of
pri
orit
y ri
sks,
and
co
ntin
uous
mon
itor
ing
of c
hang
ing
risk
con
diti
ons
and
heal
th s
tatu
s as
sess
ed.
•M
ost
vuln
erab
le p
opul
atio
ns a
nd a
reas
pro
ne t
o he
alth
ris
ks o
f cl
imat
e ch
ange
iden
tifie
d.
•H
ealt
h im
pact
ass
essm
ents
for
key
ada
ptat
ion
and
mit
igat
ion
polic
ies
and
prog
ram
mes
of
heal
th-
dete
rmin
ing
sect
ors
cond
ucte
d.
Capa
city
•B
asel
ines
on
exis
ting
hum
an r
esou
rces
, te
chni
cal a
nd h
ealt
h se
rvic
e de
liver
y ca
paci
ty e
stab
lishe
d, w
ith
iden
tific
atio
n of
wea
knes
ses.
•R
ecom
men
dati
ons
mad
e fo
r ad
dres
sing
gap
s an
d bu
ildin
g he
alth
sys
tem
s ca
paci
ty.
Adap
tatio
n op
tions
•A
sses
smen
t re
sult
s us
ed t
o pr
iori
tize
allo
cati
on o
f re
sour
ces
and
effe
ctiv
e in
terv
enti
ons
in h
ealt
h an
d re
late
d-se
ctor
s fo
r hi
gh r
isk
and
vuln
erab
le p
opul
atio
ns.
•P
lan
defin
ed a
nd m
echa
nism
est
ablis
hed
for
iter
ativ
e re
view
of
heal
th v
ulne
rabi
lity
and
adap
tati
on o
ptio
ns.

Monitoring progress 39
Six
build
ing
bloc
ks o
f he
alth
sys
tem
s
Exam
ple
indi
cato
rs
at o
utco
me
leve
lTe
n co
mpo
nent
s of
the
oper
atio
nal
fram
ewor
k
Exam
ples
of m
easu
rabl
e ou
tput
s to
enh
ance
clim
ate
resi
lienc
e
Inte
grat
ed r
isk
mon
itori
ng a
nd
earl
y w
arni
ng
Inte
grat
ed d
isea
se s
urve
illan
ce a
nd e
arly
war
ning
•E
arly
det
ecti
on t
ools
(e.
g. r
apid
dia
gnos
tics
, sy
ndro
mic
sur
veill
ance
) us
ed t
o id
enti
fy c
hang
ing
inci
denc
e an
d ea
rly
acti
on t
rigg
ered
.
•G
eogr
aphi
c an
d se
ason
al d
istr
ibut
ion
of h
ealt
h ri
sks
and
outc
omes
(i.e
. ri
sk m
appi
ng)
trac
ked.
•E
arly
war
ning
sys
tem
s fo
r re
leva
nt e
xtre
me
wea
ther
eve
nts
and
clim
ate-
sens
itiv
e di
seas
es (
e.g.
hea
t st
ress
, zo
onot
ic d
isea
ses,
und
ernu
trit
ion)
est
ablis
hed.
Mon
itori
ng
•In
dica
tors
on
clim
ate
chan
ge im
pact
s, v
ulne
rabi
lity,
res
pons
e ca
paci
ty a
nd e
mer
genc
y pr
epar
edne
ss
capa
city
, as
wel
l as
clim
ate
and
envi
ronm
enta
l var
iabl
es in
clud
ed in
rel
evan
t m
onit
orin
g sy
stem
s at
nat
iona
l le
vel a
nd r
epor
ted
over
tim
e.
•P
erio
dic
revi
ews
for
impr
ovem
ents
or
dete
rior
atio
n of
cap
acit
ies
iden
tifie
d in
V&
A a
sses
smen
ts.
•Im
pact
s of
mai
n en
viro
nmen
tal d
eter
min
ants
of
heal
th m
onit
ored
by
the
heal
th s
ecto
r.
Com
mun
icat
ion
•C
omm
unic
atio
n st
rate
gy o
n cl
imat
e ri
sks
to h
ealt
h de
velo
ped
and
impl
emen
ted,
out
linin
g th
e sc
ope
of
info
rmat
ion
for
dive
rse
audi
ence
s (e
.g. m
edia
, pu
blic
, he
alth
per
sonn
el a
nd o
ther
sec
tors
) an
d ev
ents
, in
clud
ing
who
sho
uld
com
mun
icat
e an
d th
e m
eans
of
com
mun
icat
ion.
•C
omm
unit
y en
gage
men
t an
d fe
edba
ck m
echa
nism
s es
tabl
ishe
d to
em
pow
er a
ffec
ted
popu
lati
ons
to r
espo
nd
to w
arni
ngs,
and
to
guid
e fu
ture
dev
elop
men
t of
mon
itor
ing
and
war
ning
sys
tem
s.
Hea
lth a
nd c
limat
e re
sear
chRe
sear
ch a
gend
a
•N
atio
nal r
esea
rch
agen
da o
n cl
imat
e ch
ange
and
hea
lth
defin
ed t
hrou
gh t
he o
rgan
izat
ion
of a
sta
keho
lder
fo
rum
invo
lvin
g re
pres
enta
tive
s fr
om h
ealt
h an
d ot
her
gove
rnm
ent
min
istr
ies,
res
earc
h in
stit
utio
ns,
nong
over
nmen
tal o
rgan
izat
ions
, th
e pr
ivat
e se
ctor
and
vul
nera
ble
popu
lati
ons.
Supp
ort r
esea
rch
•A
cces
s to
, an
d lin
kage
of,
dat
a on
met
eoro
logi
cal i
nfor
mat
ion,
hea
lth
dete
rmin
ants
and
out
com
es e
nabl
ed.
•M
ulti
disc
iplin
ary
rese
arch
par
tner
ship
s, k
now
ledg
e m
anag
emen
t ne
twor
ks a
nd r
oste
rs o
f lo
cal e
xper
ts
esta
blis
hed.
•Fi
nanc
ial b
acki
ng m
echa
nism
s to
sup
port
res
earc
h pr
ogra
mm
es a
nd p
ostg
radu
ate
trai
ning
pro
gram
mes
es
tabl
ishe
d.
•Co
nnec
t to
polic
y
•M
echa
nism
est
ablis
hed
for
rese
arch
ers
to in
form
pla
nnin
g, p
olic
y an
d st
akeh
olde
r gr
oups
.
•P
olic
y m
aker
s in
clud
ed in
the
defi
niti
on a
nd r
evie
w o
f re
sear
ch a
gend
as.

40 Operational framework for building climate resilient health systems
Six
build
ing
bloc
ks o
f he
alth
sys
tem
s
Exam
ple
indi
cato
rs
at o
utco
me
leve
lTe
n co
mpo
nent
s of
the
oper
atio
nal
fram
ewor
k
Exam
ples
of m
easu
rabl
e ou
tput
s to
enh
ance
clim
ate
resi
lienc
e
Esse
ntia
l m
edic
al p
rodu
cts
and
tech
nolo
gies
Per
cent
age
of
heal
thca
re f
acili
ties
in
corp
orat
ing
clim
ate
vari
abili
ty
and
chan
ge in
si
ting
, co
nstr
ucti
on,
tech
nolo
gies
and
pr
oced
ures
to
ensu
re
prov
isio
n of
bas
ic
serv
ices
(in
clud
ing
ener
gy, w
ater
and
sa
nita
tion
).
Clim
ate
resi
lient
an
d su
stai
nabl
e te
chno
logi
es a
nd
infr
astr
uctu
re
Adap
tatio
n of
cur
rent
tech
nolo
gies
and
pro
cess
es
•S
peci
ficat
ions
for
sit
ing
and
cons
truc
tion
of
heal
th f
acili
ties
, an
d en
ergy
, w
ater
and
san
itat
ion
prov
isio
ns
revi
sed
in li
ne w
ith
proj
ecte
d cl
imat
e ri
sks.
•Tr
aini
ng a
nd r
ecom
men
dati
ons
for
pres
crip
tion
of
phar
mac
euti
cals
dur
ing
extr
eme
heat
con
diti
ons
revi
sed.
Prom
otio
n of
new
tech
nolo
gies
•N
ew t
echn
olog
ies
such
as
eHea
lth
or s
atel
lite
imag
ery
used
to
impr
ove
heal
th s
yste
m p
erfo
rman
ce.
Sust
aina
bilit
y of
hea
lth o
pera
tions
•Im
pact
of
heal
th s
ecto
r on
the
env
iron
men
t as
sess
ed, an
d ap
prop
riat
e m
echa
nism
s to
mon
itor
car
bon
emis
sion
s an
d en
viro
nmen
tal i
mpa
cts
deve
lope
d.
•S
usta
inab
ility
in s
elec
tion
of
prod
ucts
and
pro
cure
men
t of
ser
vice
s in
clud
ing
ener
gy, w
ater
, tr
ansp
ort
and
was
te m
anag
emen
t as
sess
ed a
nd p
rior
itiz
ed b
y he
alth
fac
iliti
es.
Serv
ice
deliv
ery
Per
cent
age
of
med
ium
- an
d lo
ng-
term
pla
ns f
or
cont
rol p
rogr
amm
es
for
clim
ate-
sens
itiv
e di
seas
es
and
emer
genc
y m
anag
emen
t th
at
incl
ude
cons
ider
atio
n of
clim
ate
chan
ge
risk
s.
Man
agem
ent o
f en
viro
nmen
tal
dete
rmin
ants
of
heal
th
Mon
itori
ng
•In
tegr
ated
mon
itor
ing
syst
ems
allo
win
g co
llect
ion
and
anal
ysis
of
data
on
envi
ronm
enta
l haz
ards
, so
cioe
cono
mic
fac
tors
and
hea
lth
outc
omes
exi
st.
•E
vide
nce-
base
d qu
alit
y st
anda
rds
for
clim
ate-
sens
itiv
e en
viro
nmen
tal c
ondi
tion
s de
fined
.
Regu
latio
n
•R
egul
atio
ns o
n ke
y en
viro
nmen
tal d
eter
min
ants
of
heal
th (
air
qual
ity,
wat
er q
ualit
y, f
ood
qual
ity,
hou
sing
sa
fety
, w
aste
man
agem
ent)
rev
ised
and
enf
orce
d to
refl
ect
broa
der
rang
e of
exp
ecte
d cl
imat
ic c
ondi
tion
s.
•B
uild
ing
regu
lati
ons
and
was
te m
anag
emen
t in
fras
truc
ture
, en
viro
nmen
tally
sus
tain
able
and
res
ista
nt t
o lik
ely
loca
l ext
rem
e ev
ents
pro
mot
ed.
Coor
dina
ted
man
agem
ent
•H
ealt
h im
pact
ass
essm
ents
for
pol
icy
and
prog
ram
mes
in s
ecto
rs s
uch
as t
rans
port
, ag
ricu
ltur
e an
d en
ergy
, im
plem
ente
d.
•Jo
int
mul
tise
ctor
al r
isk
man
agem
ent
appr
oach
es t
o he
alth
ris
ks r
elat
ed t
o di
sast
ers,
wat
er, w
aste
, fo
od a
nd
air
pollu
tion
(e.
g. f
ood
safe
ty, di
arrh
oeal
dis
ease
con
trol
, in
tegr
ated
vec
tor
man
agem
ent,
join
ed u
p ri
sk
com
mun
icat
ion)
und
erta
ken.

Monitoring progress 41
Six
build
ing
bloc
ks o
f he
alth
sys
tem
s
Exam
ple
indi
cato
rs
at o
utco
me
leve
lTe
n co
mpo
nent
s of
the
oper
atio
nal
fram
ewor
k
Exam
ples
of m
easu
rabl
e ou
tput
s to
enh
ance
clim
ate
resi
lienc
e
Clim
ate-
info
rmed
he
alth
pro
gram
mes
H
ealth
pro
gram
min
g
•M
ediu
m-
and
long
-ter
m p
lans
for
dis
ease
con
trol
pro
gram
mes
rev
ised
to
cons
ider
cap
acit
ies
that
may
be
stre
ssed
or
exce
eded
by
clim
ate
chan
ge.
•In
vest
men
t pl
ans
defin
ed t
o ad
dres
s id
enti
fied
capa
city
gap
s.
Deliv
ery
of in
terv
entio
ns
•R
isk
map
s an
d an
alys
is o
f se
ason
al t
rend
s in
dis
ease
s us
ed t
o ta
rget
res
ourc
es a
nd p
reve
ntiv
e m
easu
res
for
thos
e m
ost
at r
isk.
•C
onti
ngen
cy p
lans
for
hea
lthc
are
prov
isio
n in
ext
rem
e w
eath
er e
vent
s, o
r de
liver
y of
inte
rven
tion
s to
con
trol
ou
tbre
aks
of in
fect
ious
dis
ease
in n
ew lo
cati
ons
deve
lope
d an
d te
sted
.
Emer
genc
y pr
epar
edne
ss a
nd
man
agem
ent
Polic
ies
and
prot
ocol
s
•C
limat
e-se
nsit
ive
heal
th r
isks
incl
uded
und
er n
atio
nal d
isas
ter
redu
ctio
n st
rate
gy a
nd p
lans
, an
d w
ider
de
velo
pmen
t pr
oces
ses.
Risk
man
agem
ent
•R
isk
asse
ssm
ents
for
cur
rent
and
pro
ject
ed f
utur
e ex
posu
re t
o ex
trem
e w
eath
er e
vent
s ro
utin
ely
used
to
info
rm h
ealt
h se
ctor
str
ateg
ic d
evel
opm
ent
plan
s.
•H
ealt
h se
ctor
con
ting
ency
pla
ns f
or e
xtre
me
wea
ther
eve
nts
deve
lope
d, in
clud
ing
risk
red
ucti
on,
prep
ared
ness
and
res
pons
e, in
line
wit
h th
e W
HO
em
erge
ncy
resp
onse
fra
mew
ork.
•E
mer
genc
y re
spon
se p
lans
for
indi
vidu
al h
ealt
h fa
cilit
ies
defin
ed a
nd im
plem
ente
d in
cas
e of
nee
d.
Com
mun
ity e
mpo
wer
men
t
•E
stab
lishm
ent
of s
take
hold
er m
echa
nism
s to
sup
port
par
tici
pati
on, di
alog
ue a
nd in
form
atio
n ex
chan
ge, to
em
pow
er c
ivil
soci
ety
and
com
mun
ity
grou
ps a
s pr
imar
y ac
tors
in e
mer
genc
y pr
epar
edne
ss a
nd r
espo
nse.
•Im
plem
enta
tion
of
capa
city
dev
elop
men
t pr
ogra
mm
es t
o id
enti
fy a
nd s
uppo
rt t
he r
oles
of
loca
l com
mun
itie
s to
det
erm
ine
risk
s, p
reve
nt e
xpos
ure
to h
azar
ds a
nd t
ake
acti
on t
o sa
ve li
ves
in e
xtre
me
wea
ther
eve
nts.

42 Operational framework for building climate resilient health systems
Six
build
ing
bloc
ks o
f he
alth
sys
tem
s
Exam
ple
indi
cato
rs
at o
utco
me
leve
lTe
n co
mpo
nent
s of
the
oper
atio
nal
fram
ewor
k
Exam
ples
of m
easu
rabl
e ou
tput
s to
enh
ance
clim
ate
resi
lienc
e
Fina
ncin
gP
erce
ntag
e of
the
na
tion
al h
ealt
h bu
dget
tha
t ad
dres
ses
risk
s po
sed
by c
limat
e va
riab
ility
and
cha
nge
Clim
ate
and
heal
th
finan
cing
Hea
lth-s
peci
fic fu
ndin
g m
echa
nism
s
•R
esou
rces
to
incr
ease
res
ilien
ce t
o cl
imat
e va
riab
ility
and
clim
ate
chan
ge in
clud
ed a
s a
line
item
in
nati
onal
and
/or
subn
atio
nal h
ealt
h in
vest
men
t pl
ans.
•P
ropo
sals
to
exte
rnal
don
ors
to s
uppo
rt c
ontr
ol o
f cl
imat
e-se
nsit
ive
dise
ases
(e.
g. G
FATM
on
mal
aria
co
ntro
l), in
clud
ed c
limat
e va
riab
ility
and
cha
nge.
Deve
lopm
ent f
undi
ng in
sec
tors
influ
enci
ng h
ealth
•S
cree
ning
for
clim
ate
vari
abili
ty, cl
imat
e ch
ange
ris
ks a
nd h
ealt
h pr
otec
tion
, in
clud
ed a
s a
crit
eria
for
se
lect
ing
inve
stm
ents
in k
ey h
ealt
h de
term
inin
g se
ctor
s, s
uch
as w
ater
and
san
itat
ion,
and
foo
d an
d nu
trit
ion
secu
rity
.
•H
ealt
h im
pact
s of
clim
ate
chan
ge m
onit
ored
in p
rogr
amm
es f
unde
d th
roug
h fin
anci
al m
echa
nism
s sp
ecifi
c to
hea
lth-
dete
rmin
ing
sect
ors.
Clim
ate
chan
ge fu
ndin
g st
ream
s
•P
roje
cts
and
prog
ram
mes
on
build
ing
heal
th s
yste
m r
esili
ence
sub
mit
ted
to a
nd g
rant
ed b
y th
e m
ain
inte
rnat
iona
l clim
ate
chan
ge f
unds
(e.
g. t
he G
EF,
Ada
ptat
ion
Fund
, bi
late
ral d
onor
s).
Not
e: A
s he
alth
sys
tem
s va
ry, th
e fin
al d
efini
tion
of
indi
cato
rs w
ill b
e co
ntex
t sp
ecifi
c. T
he t
able
giv
es p
ropo
sed
exam
ples
of
mea
sura
ble
indi
cato
rs o
f pr
ogre
ss in
impl
emen
tati
on
of “
build
ing
bloc
ks”
in h
ealt
h sy
stem
s ov
eral
l, i.e
. th
e co
mbi
ned
effe
ct o
f im
plem
enta
tion
of
the
vari
ous
com
pone
nts
desc
ribe
d ab
ove.
It
also
giv
es e
xam
ples
of
spec
ific
outp
uts
that
con
trib
ute
to t
hese
com
pone
nts.

Conclusions 43
ConclusionsClimate change, interacting with a range of other factors, places increasing stress on health. The structured framework presented here aims to ensure that health systems provide a comprehensive, efficient and equitable response, and ultimately continue to protect and improve population health in light of the varied current and future risks presented by climate variability and climate change. This approach is grounded in the core functions of the health sector, but linked to the wider environmental and social determinants of health.
In addition to changes in climate and other environmental and social determinants of health, health systems themselves are also changing rapidly. For this reason, the framework should be implemented in a flexible way to take into account different country contexts, and iteratively, take advantage of new evidence, experience and lessons learned from within and outside the country, as well as changing circumstances. Applied in this way, climate resilient health systems can help to promote and safeguard the provision of Universal Health Coverage, and make an important contribution to overall sustainable development.
6

44 Operational framework for building climate resilient health systems
TerminologyThis section draws upon glossaries and definitions provided by the IPCC (5), the International Strategy for Disaster Reduction (18), and WHO (19) .
Adaptation: refers to the process of adjustment to actual or expected climate and its effects. In human systems, adaptation seeks to moderate harm or exploit beneficial opportunities. In natural systems, human interventions may facilitate adjustment to expected climate and its effects. In public health, the analogous term is “prevention”. Various types of adaptations exist, including anticipatory and reactive, private and public, autonomous and planned. Adaptation responds to immediate threats of climate vulnerability (commonly addressed with disaster risk reduction, emergency response and epidemic management), but primarily seeks to identify and plan for large-scale risks and trends posed by long-term environmental and climatic changes such as sea-level rise, changing ground and surface water availability, changes in disease vector distribution and crop pests, changes in air quality, glacial retreat, UV exposures, and extreme and increasing temperatures. Resilience to climate change usually requires a capacity to anticipate climate change and plan needed adaptations.
Adaptive capacity is the ability of a system to adjust to climate change, to moderate potential damages, to take advantage of opportunities, or to cope with the consequences.
Climate change refers to any change in the climate over time, generally decades or longer, whether due to natural variability or as a result of human activity.
Climate variability refers to trends in variation in the mean state and other statistics of the climate on all temporal and spatial scales beyond that of individual weather events. Extreme weather (storms, extreme temperatures) and climate events (drought) are part of climate variability trends.
Climate-resilient health systems have the ability to anticipate, respond to, cope with, recover from and adapt to climate-related shocks and stresses, so as to bring sustained improvements in population health, despite an unstable climate.
Climate-sensitive health outcome is any health outcome whose geographic range, incidence or intensity of transmission is directly or indirectly associated with weather or climate.
Climate-related risks are additional (exacerbated) risks that people and their livelihoods and assets face due to climate change. These risks can be direct, such as in exposure to more frequent heat waves or floods; or indirect, such as when a drought negatively impacts food supplies (and prices) and in effect livelihoods and nutrition. Certain groups may also face increased risks from measures taken in response to climate change (such as adaptation measures that protect certain areas of a city from flooding but increase flood-risks in other areas) or for mitigation (such as new hydropower schemes displacing populations or increasing malaria vector breeding sites).

Terminology 45
Exposure is the amount of a factor to which a group or individual is exposed; sometimes contrasted with dose (the amount that enters or interacts with the organism). Exposures may be either beneficial or harmful. Exposure to climatic conditions that affect health is heavily influenced by location, socioeconomic conditions and human behaviour.
Climate risk management is an approach to identify hazards and impacts associated with both climate variability and climate change, and provides tools for decision-making in response. Climate risk management aims to reduce negative impacts through “climate informed decisions” which couple information about the climate system and meteorological conditions along with the known associations to health outcomes, and incorporates this knowledge into decision-making on planning, forecasting, systems management and geographic or spatial targeting, or risk management interventions. Climate risk management encourages handling of current climate-related risks as a basis for managing and building capacity to address more complex, long-term risks associated with climate change.
Climate change mitigation refers to policies and measures used to reduce greenhouse gas emissions (carbon) and/or enhance sinks such as forests, as a means to slow down and reduce future and more dangerous climate change. Climate change mitigation is primary prevention of future harm for decades in the future and necessitates public education and awareness along with use of low-carbon technology.
A disaster is a serious disruption of the functioning of a community or a society involving widespread human, material, economic or environmental losses and impacts, which exceeds the ability of the affected community or society to cope using its own resources.
Disaster risk is the potential loss expressed in lives, health status, livelihoods, assets and services, which could occur in a particular community or a society due to the impact of a natural hazard.
Disaster risk reduction is a systematic approach to identifying, assessing and reducing disaster risk. Specifically, disaster risk reduction aims to minimize vulnerabilities and disaster risks throughout a society in order to avoid (prevent) or limit (mitigate and prepare for) the adverse impacts of natural hazards, and facilitate sustainable development. Disaster risk reduction addresses climate-related disasters (drought, extreme weather events such as floods, cyclones, and storms) and encompasses nonclimatic hazards, such as tsunamis, volcanoes and earthquakes.
A health system comprises all the organizations, institutions and resources that are devoted to producing actions principally aimed at improving, maintaining or restoring health. Health systems involve numerous stakeholders from individual and community to government, at local, subnational and national levels. The health system is recognized by WHO to be made up of six key building blocks: (i) leadership and governance; (ii) health workforce; (iii) health information systems; (iv) essential medical products and technologies; (v) financing; all of which lead to (vi) service delivery. The goal of a health system is to deliver effective preventive and curative health services to the full population, equitably and efficiently, while protecting individuals from catastrophic healthcare costs.

46 Operational framework for building climate resilient health systems
Health system strengthening refers to improving the six health system building blocks and managing their interactions in ways that achieve more equitable and sustained improvements across health services and health outcomes, requiring both technical and political knowledge as well as action.
Resilience is the capacity of a social-ecological system to cope with a hazardous event or disturbance, responding or reorganizing in ways that maintain its essential function, identity and structure, while also maintaining the capacity for adaptation, learning and transformation.
Vulnerability is the degree to which individuals and systems are susceptible to or unable to cope with adverse effects of climate change including climate variability and extremes. The vulnerability and coping capacity of particular populations to changing meteorological conditions and its human and social consequences is influenced by a variety of factors. These include biological factors, sociocultural factors and access to and control over resources.

References 47
References1. Smith KR, Woodward A, Campbell-Lendrum DD, Chadee Y, Honda Q, Liu JM, et al. Human health: impacts,
adaptation, and co-benefits. In: Field CB, Barros VR, Dokken DJ, Mach KJ, Mastrandrea MD, Bilir TE, et al., editors. Climate change 2014: impacts, adaptation, and vulnerability. Part A: global and sectoral aspects. Contribution of Working Group II to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change. Cambridge, UK and New York, USA: Cambridge University Press; 2014 (https://ipcc-wg2.gov/AR5/images/uploads/WGIIAR5-Chap11_FINAL.pdf, accessed 26 July 2015).
2. Climate change and health. Resolution of the Sixty-First World Health Assembly. Geneva: World Health Organization; 2008 (http://www.who.int/gb/ebwha/pdf_files/A61/A61_R19-en.pdf, accessed 26 July 2015).
3. Climate change and human health: projects. In: WHO/Geneva programmes [website] Geneva: World Health Organization; 2015 (www.who.int/globalchange/projects accessed 26 July 2015).
4. WHO guidance to protect health from climate change through health adaptation planning. Geneva: World Health Organization; 2014 (http://apps.who.int/iris/bitstream/10665/137383/1/9789241508001_eng.pdf?ua=1, accessed 26 July 2015).
5. IPCC. Summary for policymakers. In: Stocker TF, Qin D, Plattner,GK, Tignor M, Allen SK, Boschung J, et al., editors. Climate Change 2013: the physical science basis. Contribution of Working Group I to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change. Cambridge, UK and New York, USA: Cambridge University Press; 2013 (https://www.ipcc.ch/report/ar5/wg1/citation/WGIAR5_Citations_FinalRev1.pdf, accessed 26 July 2015).
6. IPCC. Glossary. In: Field CB, Barros VR, Dokken DJ, Mach KJ, Mastrandrea MD, Bilir TE, et al., editors. Climate change 2014: impacts, adaptation, and vulnerability. Part A: Global and Sectoral Aspects Contribution of Working Group II to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change. Cambridge, UK and New York, USA: Cambridge University Press; 2014.
7. International health regulations. WHO/Geneva health topics [website] Geneva: World Health Organization; 2007 (http://www.who.int/topics/international_health_regulations/en/, accessed 26 July 2015).
8. Defining disaster resilience: a DFID approach paper. UK: Department for International Development; 2011 (https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/186874/defining-disaster-resilience-approach-paper.pdf, accessed 26 July 2015).
9. Hess JJ, McDowell JZ, Luber G. Integrating climate change adaptation into public health practice: using adaptive management to increase adaptive capacity and build resilience. Environmental Health Perspectives 2012;120(2):171–9.
10. Monitoring the building blocks of health systems: a handbook of indicators and their measurement strategies. Geneva: World Health Organization; 2010 (http://www.who.int/healthinfo/systems/monitoring/en/, accessed 26 July 2015).
11. Protecting health from climate change: vulnerability and adaptation assessment. Geneva: World Health Organization; 2013 (http://apps.who.int/iris/bitstream/10665/104200/1/9789241564687_eng.pdf?ua=1, accessed 26 July 2015).
12. Protecting health from climate change: global research priorities. Geneva: World Health Organization; 2009 (http://www.who.int/phe/news/madrid_report_661_final_lowres.pdf, accessed 26 July 2015).
13. Vision 2030: the resilience of water supply and sanitation in the face of climate change. Summary and policy implications. Geneva: World Health Organization; 2009 (https://extranet.who.int/iris/restricted/handle/10665/44172, accessed 26 July 2015).
14. Chung JW, Meltzer DO. Estimate of the carbon footprint of the US health care sector. Journal of the American Medical Association 2009;302(18):1970–2.
15. Meeting report on the consultation on the health emergency risk management framework and improving public health preparedness, 21–23 November 2012. Geneva: World Health Organization; 2013 (http://apps.who.int/iris/bitstream/10665/78359/1/WHO_HSE_HEA_HSP_2013.1_eng.pdf, accessed 24 August 2015).
16. Climate finance. United Nations Framework Convention of Climate Change [website] 2015 (http://unfccc.int/cooperation_and_support/financial_mechanism/items/2807.php, accessed 26 July 2015).
17. Financial resources for implementation of adaptation. WHO/Climate change and human health [website]. Geneva: World Health Organization; 2015 (http://www.who.int/globalchange/financial_sources_adaptation_implementation/en/, accessed 26 July 2015).
18. Terminology on disaster risk reduction. The United Nations Office for Disaster Risk Reduction/Terminology [website]; 2015 (http://www.unisdr.org/we/inform/terminology, accessed 26 July 2015).
19. Everybody’s business: strengthening health systems to improve health outcomes. WHO’s framework for action. Geneva: World Health Organization; 2007 (http://www.who.int/healthsystems/strategy/everybodys_business.pdf, accessed 26 July 2015).



PUBLIC HEALTH AND ENVIRONMENT
Operational framew
ork for building climate resilient health system
s
Public Health & Environment Department (PHE)
Health Security & Environment Cluster (HSE)
World Health Organization (WHO)
Avenue Appia 20 – CH-1211 Geneva 27 – Switzerland
www.who.int/phe/en/
http://www.who.int/globalchange/en/
E-mail: [email protected]
This document presents the World Health Organization (WHO) Operational framework for
building climate resilient health systems. The framework responds to the demand from
Member States and partners for guidance on how the health sector and its operational basis
and health systems can systematically and effectively address the challenges increasingly
presented by climate variability and change.
Primarily intended for public health professionals and health managers, this framework
would also help guide decision-makers in other health-determining sectors, such as
nutrition, water and sanitation, and emergency management. International development
agencies could use this framework to focus investments and country support for public
health, health system strengthening and climate change adaptation.
The objective of this framework is to provide guidance for health systems and public health
programming to increase their capacity for protecting health in an unstable and changing
climate. By implementing the 10 key components laid out in this framework, health
organizations, authorities and programmes will be better able to anticipate, prevent, prepare
for and manage climate-related health risks. Least developed countries and countries in the
process of developing the health components of National Adaptation Plans (NAPs) under
the UN Framework Convention on Climate Change (UNFCCC) may fi nd this document
particularly useful in their efforts to design a comprehensive response to the risks presented
by short-term climate variability and long-term climate change.


















