Football and Traumatic Head Injuries; Research and...
67
Football and Traumatic Head Injuries; Research and Clinical Implications P. Gunnar Brolinson, DO, FAOASM, FAAFP, FACOFP Professor and Discipline Chair, Sports Medicine Director, Primary Care Sports Med Fellowship Team Physician, Virginia Tech Team Physician, US Ski Team Stefan Duma, PhD Steve Rowson PhD Virginia Tech –Wake Forest School of Biomedical Engineering AAO Convocation March 23rd, 2014
Transcript of Football and Traumatic Head Injuries; Research and...
Football and Traumatic Head Injuries;
Research and Clinical Implications
P. Gunnar Brolinson, DO, FAOASM, FAAFP, FACOFP
Professor and Discipline Chair, Sports Medicine
Director, Primary Care Sports Med Fellowship
Team Physician, Virginia Tech
Team Physician, US Ski Team
Stefan Duma, PhD
Steve Rowson PhD
Virginia Tech –Wake Forest School of Biomedical Engineering
AAO Convocation March 23rd, 2014
Funding and Disclaimer
DOT: National Highway Traffic Safety Administration
Toyota Central Research and Development Labs, Inc
NIH: R01HD048638
I do not have any relevant financial relationships to be discussed, directly or
indirectly, referred to or illustrated with or without recognition within this
presentation.

Congratulations!
13 ACC Players in Super Bowl
Kam Chancellor, Virginia Tech

No health topic in recent memory has captured the
public’s attention as much as the debate on sports
related traumatic brain injury.
The deal calls for the NFL to pay $765 million to fund medical exams, concussion-related compensation, medical research for retired NFL players
and their families, and litigation expenses, according to a court document filed in U.S. District Court in Philadelphia.
Presentation Outline Part 1: STAR Helmet Rating Update
– Review Data and Validation Studies
– Adding Rotational Acceleration
Part 2: Brain Strain During Impact
Part 3: Head Impact Sensor Evaluation
– Accuracy and Exposure Comparisons
Part 4: Clinical Implications and Challenges
Questions and Discussion
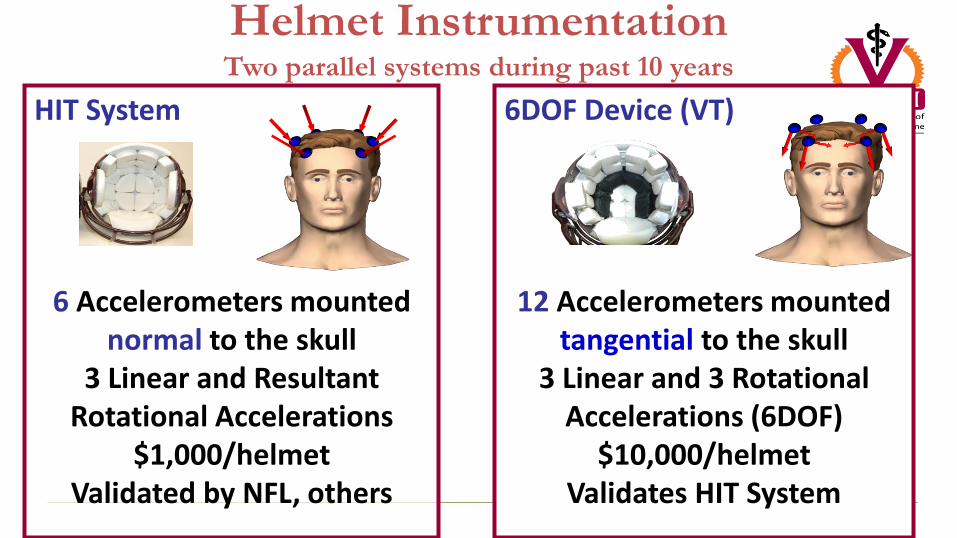
HIT System
6 Accelerometers mounted normal to the skull
3 Linear and Resultant Rotational Accelerations
$1,000/helmet Validated by NFL, others
6DOF Device (VT)
12 Accelerometers mounted tangential to the skull
3 Linear and 3 Rotational Accelerations (6DOF)
$10,000/helmet Validates HIT System
Helmet Instrumentation Two parallel systems during past 10 years
0
20,000
40,000
60,000
80,000
100,000
120,000
140,000
160,000
180,000
200,000
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Tota
l Num
ber
of Im
pact
s C
olle
cted
at V
irgi
nia
Tech
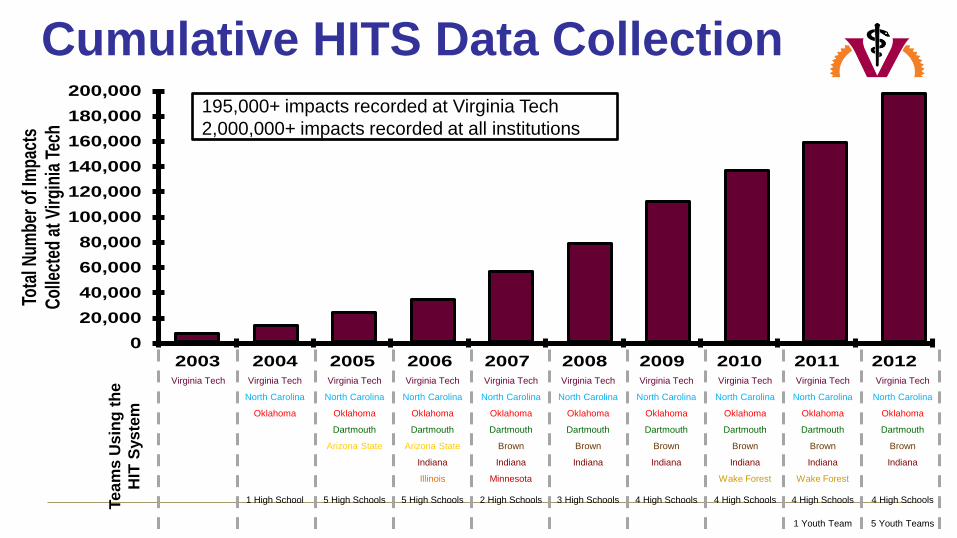
Cumulative HITS Data Collection
Virginia Tech Virginia Tech
North Carolina
Oklahoma
1 High School
Virginia Tech
North Carolina
Oklahoma
Dartmouth
Arizona State
5 High Schools
Virginia Tech
North Carolina
Oklahoma
Dartmouth
Brown
Minnesota
Indiana
2 High Schools
Virginia Tech
North Carolina
Oklahoma
Dartmouth
Arizona State
Illinois
Indiana
5 High Schools
Virginia Tech
North Carolina
Oklahoma
Dartmouth
Brown
Indiana
3 High Schools
Virginia Tech
North Carolina
Oklahoma
Dartmouth
Brown
Indiana
4 High Schools
Virginia Tech
North Carolina
Oklahoma
Dartmouth
Brown
Wake Forest
Indiana
4 High Schools
Virginia Tech
North Carolina
Oklahoma
Dartmouth
Brown
Wake Forest
Indiana
4 High Schools
1 Youth Team
Virginia Tech
North Carolina
Oklahoma
Dartmouth
Brown
Indiana
4 High Schools
5 Youth Teams
Te
am
s U
sin
g t
he
HIT
Sys
tem
195,000+ impacts recorded at Virginia Tech
2,000,000+ impacts recorded at all institutions

STAR Rating System for Football Helmets
STAR: Summation of Tests for the Analysis of Risk
4
1
6
1L H
aRhESTAR
Combines true impact exposure with an unbiased risk analysis using real world biomechanical data to assess
helmet safety for consumers.
(Rowson and Duma, 2011)

0
200
400
600
800
1000
1200
1400
1 2
1134
416
NOCSAE Pass / Fail Threshold
Adams A2000
Severity Index
Riddell 360 0
20
40
60
80
100
120
140
160
180
200
1 2
190
84
Peak Acceleration (g)
Adams A2000 Riddell 360
Adams A2000 Riddell 360
VS
Helmet Comparison: Top Impact from 60 inch Drop
Height

Consider Two Helmets
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0 50 100 150 200 250 300 350
Pro
babi
lity
of M
TBI
Linear Acceleration (g)
Which helmet would you choose?
Helmet A
Helmet B For Identical Impacts:
Helmet A 90 g 1% risk of concussion
Helmet B 200 g 59% risk of concussion

Journal of Neurosurgery 2014
Data compiled from 8 collegiate football teams
1833 players over 6 years
Exposure controlled
Clinical Evidence

Riddell Revolution reduces risk of concussion by 53.9% compared to Riddell VSR4 (p=0.03)
(STAR Equation predicts 54.2% reduction)
Journal of Neurosurgery 2014

Institute of Medicine Committee on Sports-Related Concussions in Youth
The National Academies Press 2013
• “The STAR system is theoretically grounded and represents an intriguing approach to how the injury mitigation properties of a helmet could be assessed.”
• “The STAR system is based on sound principles…”
• Adding rotational acceleration and youth specific data would increase wide-spread application of the STAR system
NFL Developed a Poster from the Virginia Tech Helmet Ratings Posted in all 32 Locker Rooms

Rotational Acceleration Comparison
NFL
Volunteer
DAI Concussion
DAI

Linear Acceleration (g)
Rot
atio
nal A
ccel
erat
ion
(rad
/s/s
)
0 50 100 150 2000
2000
4000
6000
8000
10000
Combined Linear and Rotational Risk ROC Curves
0 0.5 10
0.2
0.4
0.6
0.8
1
False Positive Rate
Tru
e P
osit
ive
Rat
e
0 0.5 10
0.2
0.4
0.6
0.8
1
False Positive Rate
Tru
e P
osit
ive
Rat
e
NFL Data
58 Impacts
25 Concussions
0 0.5 10
0.2
0.4
0.6
0.8
1
False Positive Rate
Tru
e P
osit
ive
Rat
e
0 0.5 10
0.2
0.4
0.6
0.8
1
False Positive Rate
Tru
e P
osit
ive
Rat
e
HITS Data
63,011 Impacts
244 Concussions
Risk Contours
10% 25%
50%
75% 90%
5%
1%
𝑅𝑖𝑠𝑘 =1
1 + 𝑒−(−10.2+0.0433𝑎+0.000873∝−0.00000092𝑎∝
AUC = 0.982
AUC = 0.892
(Rowson and Duma, ABME, 2013)
Volunteer Data

Pneumatic Linear Impactor
Pressure Vessel
Solenoid Valve
5DOF Linear Slide Table
Piston 14 kg Impacting Ram
Hybrid III Head

Implications of Helmet Fit • Upper skull is very similar between
headforms
• Substantial differences are noted in: – Nape of neck – Chin – Jaw
Differences can have
profound effect on
helmet fit
Hybrid III NOCSAE
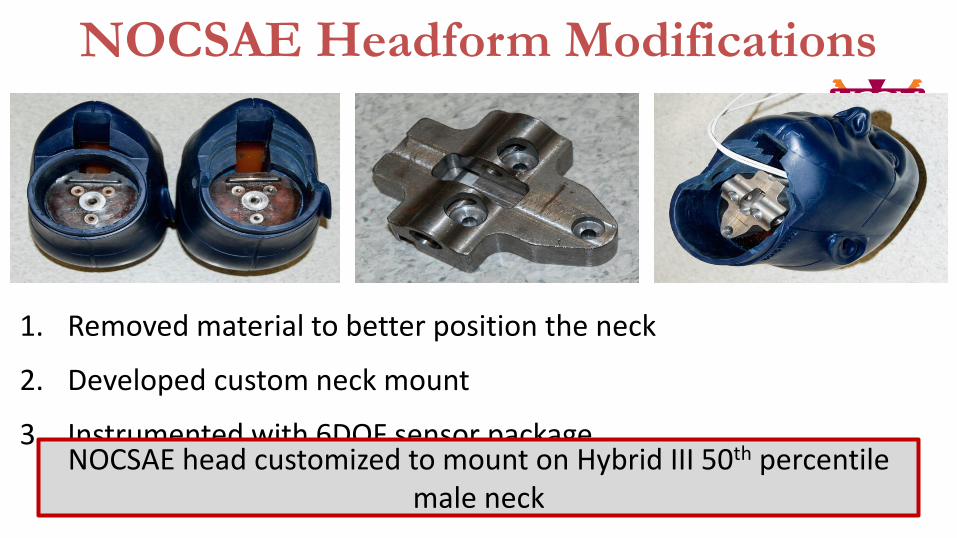
NOCSAE Headform Modifications
1. Removed material to better position the neck
2. Developed custom neck mount
3. Instrumented with 6DOF sensor package NOCSAE head customized to mount on Hybrid III 50th percentile
male neck
Presentation Outline Part 1: STAR Helmet Rating Update
– Review Data and Validation Studies
– Adding Rotational Acceleration
Part 2: Brain Strain During Impact
Part 3: Head Impact Sensor Evaluation
– Accuracy and Exposure Comparisons
Questions and Discussion
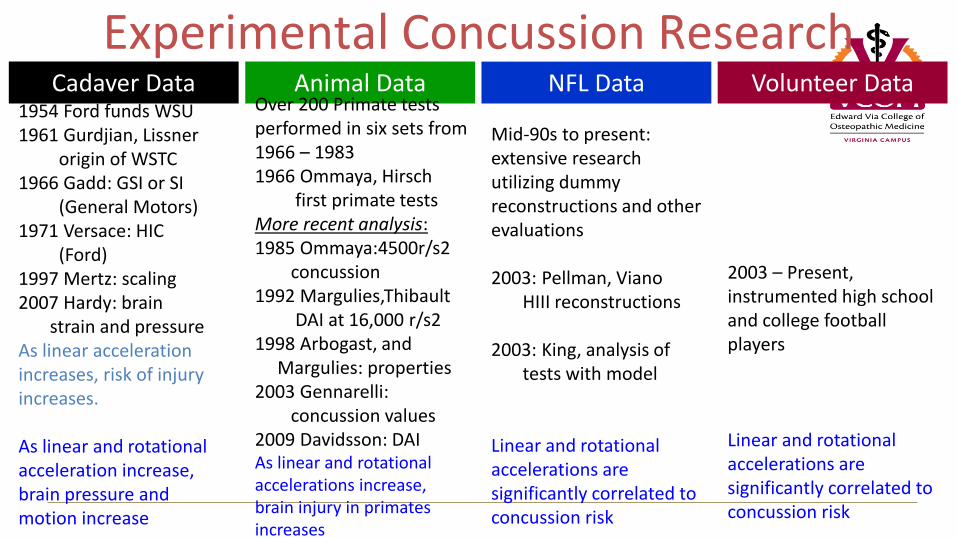
Cadaver Data NFL Data Volunteer Data Animal Data
Experimental Concussion Research
1954 Ford funds WSU 1961 Gurdjian, Lissner origin of WSTC 1966 Gadd: GSI or SI (General Motors) 1971 Versace: HIC (Ford) 1997 Mertz: scaling 2007 Hardy: brain strain and pressure As linear acceleration increases, risk of injury increases. As linear and rotational acceleration increase, brain pressure and motion increase
Over 200 Primate tests performed in six sets from 1966 – 1983 1966 Ommaya, Hirsch first primate tests More recent analysis: 1985 Ommaya:4500r/s2 concussion 1992 Margulies,Thibault DAI at 16,000 r/s2 1998 Arbogast, and Margulies: properties 2003 Gennarelli: concussion values 2009 Davidsson: DAI As linear and rotational accelerations increase, brain injury in primates increases
Mid-90s to present: extensive research utilizing dummy reconstructions and other evaluations 2003: Pellman, Viano HIII reconstructions 2003: King, analysis of tests with model Linear and rotational accelerations are significantly correlated to concussion risk
2003 – Present, instrumented high school and college football players Linear and rotational accelerations are significantly correlated to concussion risk

In Situ Brain Strain
1. Effect of linear and rotational acceleration
2. Effect of helmet on brain strain
Hardy et al (2007)

Specimen Preparation
5 mm
Neutral Density Targets
3
mm
Cranial Pressure Transducer

Head Impact Testing
• High-speed bi-planar x-ray
• Riddell VSR4 Helmet
Hardy et al (2007)

Example Motion Patterns
1
2
3 4
5
6
9
8
11
10
13
12 14 7
C2 C1
25
50
75
100
-75 -50 -25 0 25 50 75
PA-X (mm)
IS-Z
(m
m)
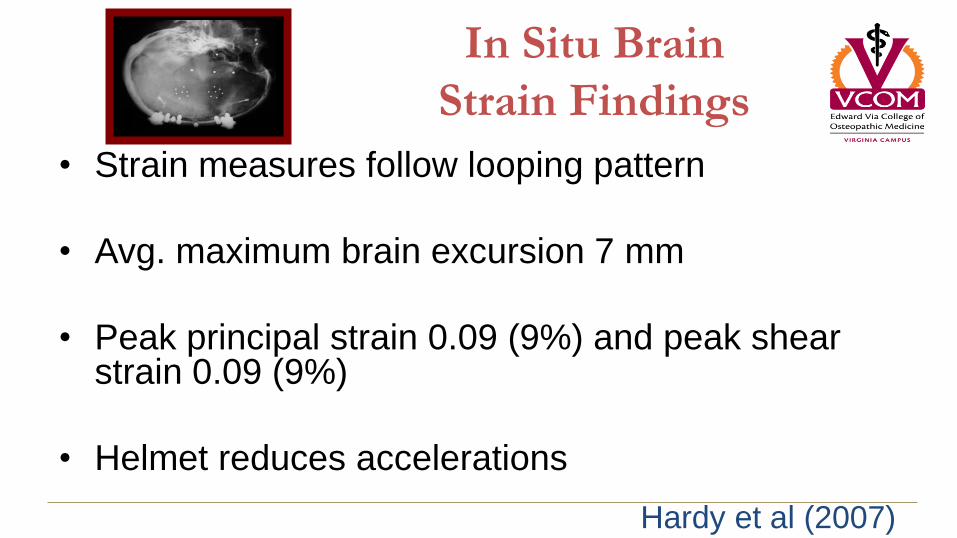
In Situ Brain
Strain Findings
• Strain measures follow looping pattern
• Avg. maximum brain excursion 7 mm
• Peak principal strain 0.09 (9%) and peak shear strain 0.09 (9%)
• Helmet reduces accelerations
Hardy et al (2007)
Presentation Outline
Part 1: STAR Helmet Rating Update
– Review Data and Validation Studies
– Adding Rotational Acceleration
Part 2: Brain Strain During Impact
Part 3: Head Impact Sensor Evaluation
– Accuracy and Exposure Comparisons

New Sensors – New Opportunities
Triax
MC10 CheckLight
Riddell Insite
X2 Patch
Careful of Comparisons • Published studies ~10/14g threshold
• If higher trigger, 20g or 30g, exposure data will be very
different

Sensor Validation Studies:
Acceleration Correlation

Sensor Validation Studies: Impact Detection
New Sensors – New Questions
Triax
MC10 CheckLight
Riddell Insite
X2 Patch • Linear and/or Rotational Acceleration
• Validation, Methods, Publication
• Private or Public Data
–Visible player lights
–Sideline trainer/coach alert
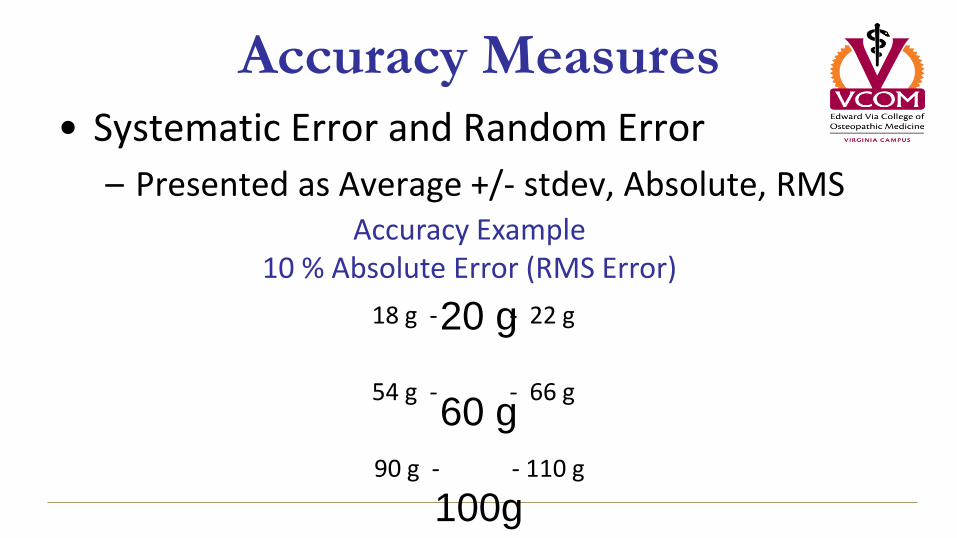
Accuracy Measures
20 g
60 g
100g
• Systematic Error and Random Error
– Presented as Average +/- stdev, Absolute, RMS Accuracy Example
10 % Absolute Error (RMS Error)
18 g - - 22 g
54 g - - 66 g
90 g - - 110 g

Presentation Outline Part 1: STAR Helmet Rating Update
– Review Data and Validation Studies
– Adding Rotational Acceleration
Part 2: Brain Strain During Impact
Part 3: Head Impact Sensor Evaluation
– Accuracy and Exposure Comparisons
Part 4: Clinical implications and Challenges
Questions and Discussion

Review of all of the evidence based scientific
literature related to athletes with multiple
concussions and return to play…
• There isn’t any…
• “Studies of management of concussion were so poor…”
• So what do we do?
• Rely on “Expert Opinion” based on clinical practice, the relevant available medical and scientific literature and currently available diagnostic testing.
Schneider KJ, Iverson GL, Emery CA, et al. The effects of rest and treatment following sport-related concussion: a systematic review of the literature. Br J Sports Med. 2013;47:304–307.

53% of concussions are unreported
(McCrea et al. 2004)

MTBI Event – The Next Play
Another Example MTBI Event

Peak G = 139 G
Another Example MTBI Event
Clinically diagnosed concussion
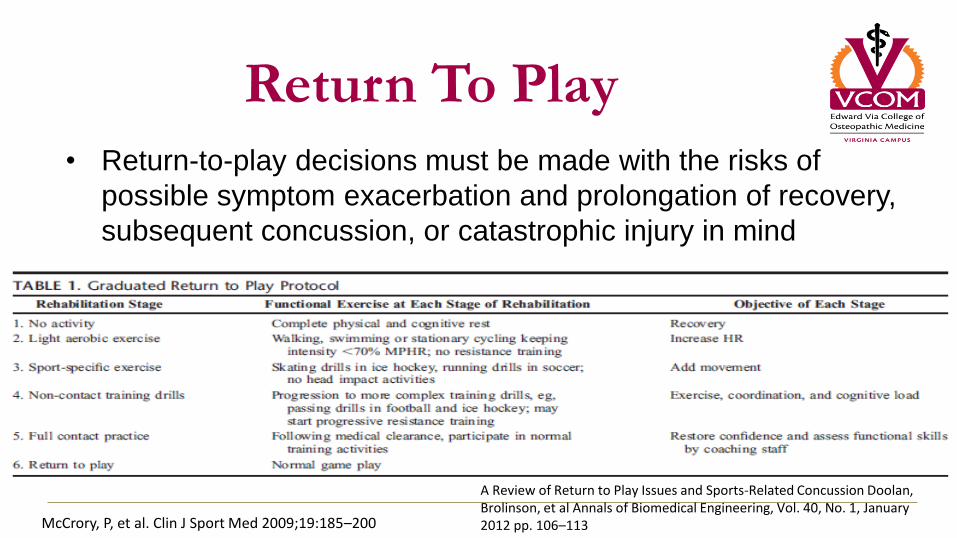
Return To Play
• Return-to-play decisions must be made with the risks of
possible symptom exacerbation and prolongation of recovery,
subsequent concussion, or catastrophic injury in mind
McCrory, P, et al. Clin J Sport Med 2009;19:185–200
A Review of Return to Play Issues and Sports-Related Concussion Doolan, Brolinson, et al Annals of Biomedical Engineering, Vol. 40, No. 1, January 2012 pp. 106–113

RTP…Other Considerations • Age
– discussed above…generally more conservative with younger athletes
• Must rely more on input from parents and coaches
• Social Pressure – Teammates, coaches and parents
• Multiple Concussions – No specific number has been established to mandate season ending injury or retirement.
– Worrisome group
• Decreased time between concussions
• More prolonged recovery from each subsequent concussion
• Concussions resulting from progressively decreased biomechanical forces
• Persistent Headache – Must differentiate “post concussive” from “cervicogenic” or “cranial” dysfunction
– Consider PT/OMT to address cervical and upper thoracic dysfunction
• With these last two groups may need to consider full neuropsych evaluation as well as other
diagnostic testing as indicated

Risk of Recurrence • Significantly increased risk of sustaining a concussion when an athlete is
still recovering from a previous concussive injury
– A second impact, often of less or even minimal force, then produces signs and symptoms that are severe enough to be observed directly
– In extreme cases, it is likely that this same scenario produces the ‘‘second impact syndrome’’
• Guskiewicz et al. showed that high school football players who suffered a concussion were three times more likely to sustain a second concussion during the same season
• Delaney, et al. showed that athletes who experienced concussion with a loss of consciousness were six times more likely to sustain another concussion than those who had been concussed but never lost consciousness
Guskiewicz K, et al. Am. J. Sports Med. 2000; 28:643-50 Delaney J,et al. Clin. J. Sport Med. 2000; 10:9-14

Post Concussion Syndrome • A function of the length of
symptom persistence
– 3 months duration of 3 or more
symptoms
• Of retired NFL players who were
diagnosed with post-concussion
related depression, 87% continued
to have lifelong symptoms
• Medications that address
symptoms may be considered in
the treatment of PCS
– Dosing should begin low and
titrated upward slowly
Jotwani, V et al. Curr. Sports Med. Rep.; 2010; 9 (1): 21-26 Halsted, M and K Walter. Pediatrics, 2010; 126 (3): 597-615

Summary of Gunnar’s clinical
treatment Pearls for PCS • Remember that dx and tx is a “team
event” – Psychologists, neurologists, PM&R, PT’s
and ATC’s can all be involved
• You are treating “symptoms”
• Evaluate and treat cranial, cervical and thoracic somatic dysfuntion
• For mild insomnia with head/neck pain – Flexeril 10mg at hs
– Elavil 10-25mg at hs
• For headache – NSAIDs
– Topamax 25-50mg BID
• For depression with diffuse “body pain” – Effexor and Cymbalta (SNRI’s)
– Tricyclics
– SSRI’s don’t seem to work well
• For “fogginess” – Omega 3 supplements
– Antioxidants • Alpha Lipoic Acid 100mg QD
• B Complex
– Amantadine • 100-200mg BID
• Remember to include physical therapy and neurocognitive rehab as appropriate
• In general avoid narcotics
Placebo-Controlled Trial of Amantadine for Severe Traumatic Brain Injury; Gianco et al; N Engl J Med 2012; 366:819-826March 1, 2012DOI: 10.1056/NEJMoa1102609

Clinical Considerations for Athletes
with Multiple Concussions • To date, no specific number of concussions has been established to
mandate season ending injury or retirement.
• Experts understand that repetitive concussions can be associated with significant and prolonged neurocognitive deficits – decreased time between concussions
– increased recovery time
– concussions resulting from decreased biomechanical forces
• Clinicians may wish to consider a full neuropsychological evaluation and the use of advanced diagnostics and imaging techniques in these athletes.
A Review of Return to Play Issues and Sports-Related Concussion Doolan, Brolinson, et al Annals of Biomedical Engineering, Vol. 40, No. 1, January 2012 pp. 106–113
Clinical Considerations for Athletes
with Multiple Concussions • When to remove an athlete from the competitive season or
recommend permanent retirement from competition? – Must be managed in on individualized basis and multiple factors taken
into account
– Utilize the sports medicine team and appropriate diagnostic modalities • “One opinion is no opinion”
“The current literature is unclear and contradictory regarding specific therapeutic approaches. Sports clinicians are left to develop an approach to management of concussion that is based on currently available best practices that have little scientific evidence to support them.”
P.G. Brolinson; management of sport related concussion review and commentary; Clin J Sport Med Journal Club issue 24(1) -Jan 2014.

Clinical Considerations for Athletes
with Multiple Concussions
Remove for Season • Prolonged post concussive
symptoms
• 3 “simple” concussions in a single season
• 2 or more “complex” concussions in a single season
• decreased academic and athletic performance
• clinically relevant imaging abnormality.
Career Ending • Pathologic abnormality such as Chiari
malformation
• Intracranial hemorrhage
• Clinically relevant imaging abnormality
• Diminished academic performance or cognitive abilities
• Persistent prolonged post-concussion syndrome
• Decreased threshold for concussion
• 3 or more “complex” concussions during career
• Persistent neuropsychiatic symptoms
A Review of Return to Play Issues and Sports-Related Concussion Doolan, Brolinson, et al Annals of Biomedical Engineering, Vol. 40, No. 1, January 2012 pp. 106–113
What about repetitive “sub concussive” impacts?
• Millions of individuals have played contact sports for many years without obvious functionally significant adverse effects, and without developing progressive neurodegenerative disorders.
• Nevertheless, we are concerned that repetitive head impacts may have an adverse effect on some athletes.
– It is reasonable to speculate that individual differences such as polymorphisms in genes modulating response to neurotrauma39 (e.g., APOE, BDNF, ANKK1) or other host factors may play a role
– it is tempting to hypothesize that risk of chronic traumatic encephalopathy or other long term effects of contact sports may represent a gene–environment interaction between repetitive mild neurotrauma and genetic vulnerability to heightened injury response or attenuated neural repair.
McAllister TW, Flashman LA, Maerlender AC, Greenwald RM, Beckwith JG, Tosteson TD, Crisco JJ, Brolinson PG, Duma SM, Duhaime AC, Grove MR and Turco JH. “Cognitive Effects of One Season of Head Impacts in a Cohort of Collegiate Contact Sport”. Neuro. 2012 May 29;78(22):1777-84.

What is Chronic Traumatic
Encephalopathy???
• A progressive neurodegenerative syndrome
• Dementia Pugilistica… – “Punch Drunk Syndrome”
• Accumulation of Tau Protein in neurologic tissue – Genetically determined?
– Head trauma triggered?
– “Over-production” vs “Inadequate Clearance”?
• Presents clinically after a prolonged latent period
• A composite syndrome of mood disorders – associated neuropshychiatric and cognitive
impairments
• Definitive diagnosis is by direct tissue analysis post mortem
BU Center for the Study of Traumatic Encephalopathy
Brain tissue from 18-year-old multi-sport athlete

What is Post Traumatic Encephalopathy?
• A clinicopathologic syndrome that follows focal
or diffuse brain trauma
– Associated with gross or microspcopic
destruction of brain tissue
– Lacerations, contusions, hemorrhages, etc
• Not neurodegenerative and not progressive
• Can co-exist with CTE
HS Football and Risk of
Neurodegenerative Disease • To assess whether high school football played between
1946 and 1956, when headgear was less protective than today, was associated with development of neurodegenerative diseases later in life.
• Compared 438 FB players to 140 non FB players from HS in Rochester, MN
• High school students who played American football from 1946 to 1956 did not have an increased risk of later developing dementia, PD, or ALS compared with non–football-playing high school males, despite poorer equipment and less regard for concussions compared with today and no rules prohibiting head-first tackling (spearing).
• These results should be somewhat reassuring to high school players from 50 years ago, they should give no reassurance to today’s players.
High School Football and Risk of Neurodegeneration: A Community-Based Study; Savica, Parisi et al; Mayo Clin Proc. 2012;87(4):335-340

Legislating Risk
• Former British prime minister Harold Macmillan said, "To be alive at all involves some risk."
• Yet, some lawmakers on this side of the Atlantic want to remove all risks for high school athletes through restrictive legislation, with concussions being the flavor of the month.
• The Federal Government has also gotten involved in the concussion debate and the Government Accountability Office (GAO) published its report on the testimony given before the committee on education and labor of the House of Representatives on May 20th 2010.
• Texas (2007), Washington and Oregon (2009) passed the first concussion-specific laws addressing scholastic sports.
• Washington’s law was named after Zackery Lystedt, a teenager who in 2006 sustained a serious brain injury while playing football.
• One problem with this legislation are the costs of implementing such a program which would include athletic trainers present at all practices and games as well as physician coverage for games.
Erik Simpson and Brent Crane Posted 04/26/2011 08:21:41 PM | USA Today

Legislating Risk
• Since 2009 44 Sates and DC have enacted youth sports TBI laws aimed at increasing awareness or reducing risk of repeat injury or both.
• These laws represent a uniform but not scientifically proven consensus about the minimum time a young athlete should refrain from reentering contact sports activities.
• Also exhibit divergence regarding the health care professional best qualified to make the RTP decision.
• Existing youth TBI laws are not designed to reduce initial TBIs. Continued research and evaluation of existing laws will be needed to develop a more comprehensive risk reduction program.
Harvey, H; American Journal of Public Health: May 16, 2013
NCAA • “Institutions shall have a concussion management plan on file such that a
student-athlete who exhibits signs, symptoms or behaviors consistent with a concussion shall be removed from practice or competition and evaluated by an athletics healthcare provider with experience in the evaluation and management of concussion. Student-athletes diagnosed with a concussion shall not return to activity for the remainder of that day. Medical clearance shall be determined by the team physician or their designee according to the concussion management plan.
• In addition, student-athletes must sign a statement in which they accept the responsibility for reporting their injuries and illnesses to the institutional medical staff, including signs and symptoms of concussions. During the review and signing process student-athletes should be presented with educational material on concussions.”
-- NCAA Memorandum
April, 2010
www.ncaa.org/health-safety
Thoughts on Rules Changes,
Technique and “The Game” • "I sent those plays to make
that statement," Carroll said. "Let's demonstrate that guys like that are turning the corner and do get it. That message should go throughout pro football, throughout college football and down to the young kids playing so they can see the game can be played differently."

Thoughts on Rules Changes,
Technique and “The Game” • "There's still the warrior mentality of the
players, which we can relate to," Carroll said. "But through proper education and awareness, the way they play is shifting. It's clear our game is not the same as it was, but it's still OK. It's fine.
• "And guys like [Seahawks safety] Kam Chancellor can be as physical and tough as anybody in football and still make the right decisions on hitting guys to keep the game safe. I would have never thought I would be saying this; I see the game different now."

Multiple Concussions and Future
Diagnostic Considerations
• Biomarkers – term often used to refer to a protein
measured in blood whose concentration reflects the severity or presence of some disease state.
– Troponin is a biomarker used to diagnose acute myocardial infarction (AMI) in Emergency Rooms
• Advanced Imaging – fMRI and DTI
• Improved point of care diagnostics and technology
• Head acceleration sensing systems
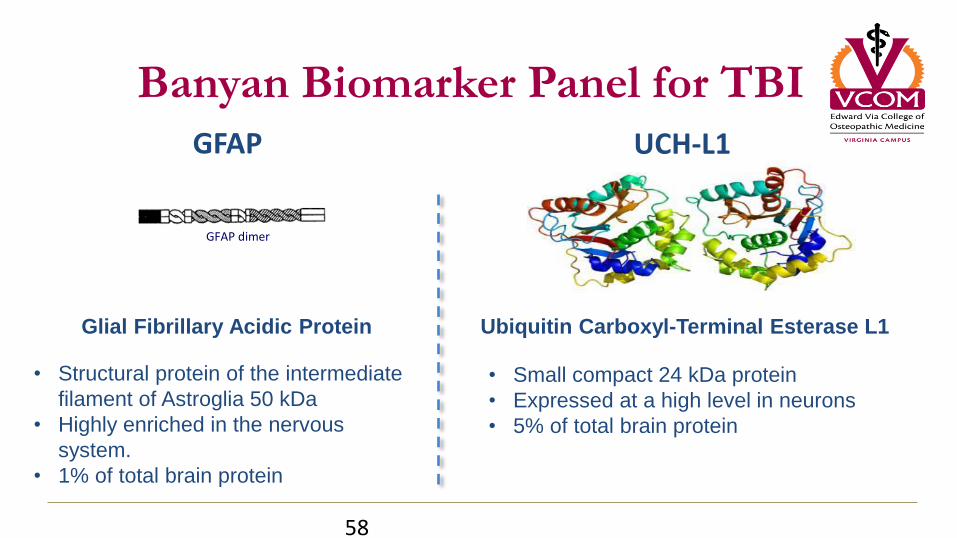
Banyan Biomarker Panel for TBI
58
Glial Fibrillary Acidic Protein Ubiquitin Carboxyl-Terminal Esterase L1
• Structural protein of the intermediate
filament of Astroglia 50 kDa
• Highly enriched in the nervous
system.
• 1% of total brain protein
• Small compact 24 kDa protein
• Expressed at a high level in neurons
• 5% of total brain protein
GFAP UCH-L1
GFAP dimer

Mild and moderate TBI study (GFAP)
59
Annals of Emergency Medicine
May 29, 2011
Elevated Levels of Serum Glial Fibrillary Acidic Protein Breakdown Products in
Mild and Moderate Traumatic Brain Injury Are Associated With Intracranial
Lesions and Neurosurgical Intervention
SUMMARY:
GFAP-BDP is detectable in serum within an
hour of injury
It is associated with measures of injury severity,
including the GCS score, CT lesions, and
neurosurgical intervention.
Further study is required to validate these
findings before clinical application.

Mild and moderate TBI Study (UCHL-1)
60
Journal of Neurotrauma
July, 2011
Serum levels of UCHL-1 distinguishes mild and moderate traumatic brain
injury from trauma controls and is associated with lesions on computed
tomography.
SUMMARY:
UCHL-1 was detected in the serum of mild and
moderate TBI (MMTBI) patients within an hour of
injury

Biomarkers
• Swedish researchers say they have devised a blood test that could better diagnose sports-related brain injuries and prevent American football, rugby and ice hockey players returning to the field in danger.
• Zetterberg's team examined all the players in the Swedish Hockey League and found that between September and December of the 2012/2013 season alone, 35 of 288 players had had a concussion. In three cases, it was so severe that the player was knocked unconscious.
• The results were compared with the pre-season samples from two full teams, and the scientists found that having raised levels of a nerve cell protein called tau in the blood was a marker of concussion.
http://www.chicagotribune.com/sports/sns-rt-uk-concussion-20140313,0,2665158.story
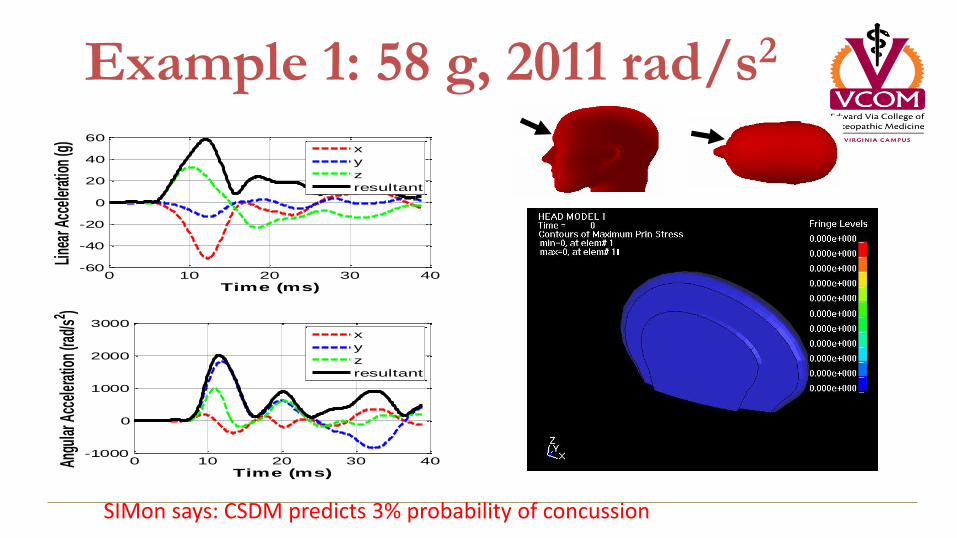
Example 1: 58 g, 2011 rad/s2
0 10 20 30 40-60
-40
-20
0
20
40
60
Time (ms)
Line
ar A
ccel
erat
ion
(g)
x
y
z
resultant
0 10 20 30 40-1000
0
1000
2000
3000
Time (ms)
Angu
lar A
ccel
erat
ion
(rad/
s2 )
x
y
z
resultant
SIMon says: CSDM predicts 3% probability of concussion

Example 2: 83 g, 9922 rad/s2
0 10 20 30 40-100
-50
0
50
100
Time (ms)
Line
ar A
ccele
ratio
n (g
)
x
y
z
resultant
0 10 20 30 40-1
-0.5
0
0.5
1x 10
4
Time (ms)
Angu
lar A
ccel
erat
ion
(rad/
s2 )
x
y
z
resultant
SIMon says: CSDM predicts 14% probability of concussion
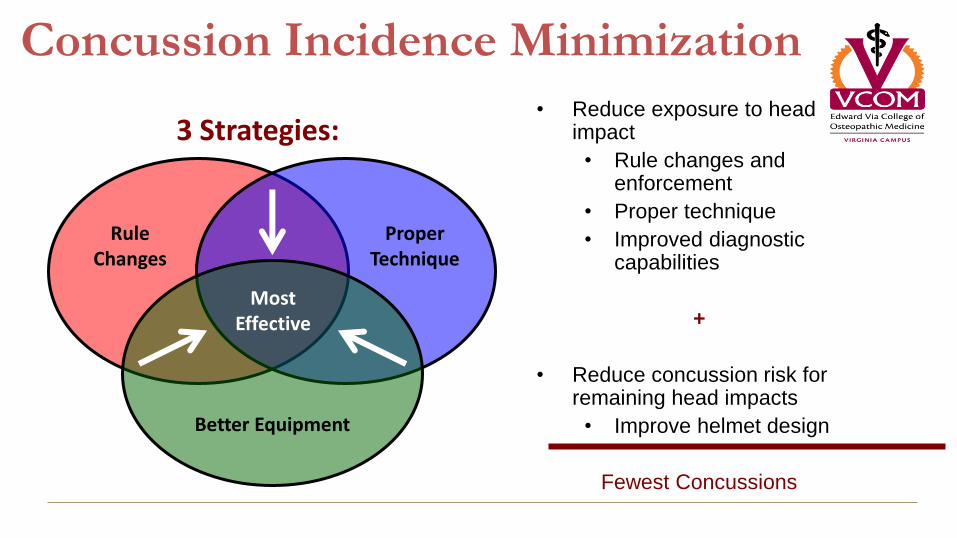
Concussion Incidence Minimization
Rule Changes
Proper Technique
Better Equipment
Most Effective
3 Strategies: • Reduce exposure to head
impact
• Rule changes and enforcement
• Proper technique
• Improved diagnostic capabilities
+
• Reduce concussion risk for remaining head impacts
• Improve helmet design
Fewest Concussions

Summary • Data suggest that female athletes may have a higher incidence of concussion and experience
more severe concussive symptoms
• We are just now beginning to research and understand risk and clinical implications for concussion in youth sports
• The presence of preexisting mood or learning disorders can confound pre-injury baseline testing as well as concussion diagnosis and management
• Multiple concussions are associated with increased risk of: – Mood disorders (anxiety and depression)
– Cognitive dysfunction
• Migraine headache and concussion have similar presentations – Athletes who have migraines also may be at a higher risk of being concussed but not know if this is a “cause and effect”
relationship
• The genetics of concussion remain a mystery, and the role of factors such as the ApoE promoter gene are being investigated
• Brain Biomarkers and Advanced Imaging Technologies are an emerging area of research for enhancing our clinical diagnostic capability
• There are some data to suggest that concussion risk may increase as an athlete fatigues or if he or she continues to participate in the sport after sustaining an initial mild traumatic injury
• Regarding helmets…more padding is more better!

All Data and Reports Online
http://www.vcom.vt.edu/sportsmed/

We choose to do these things, “not because they are easy, but because they are hard, because that goal will serve to organize and measure the best of our energies and skills, because that challenge is one that we are willing to accept, one we are unwilling to postpone, and one which we intend to win.” John F. Kennedy