
Food Intake and nutritional Status of Children … Intake and nutritional Status of Children ......
65
0 Akhoni Shomay Formative Research Project CARE Bangladesh Food Intake and nutritional Status of Children Under the Age of Two By Thérèse Blanchet and Drishti Research Centre Dhaka, May 2010
Transcript of Food Intake and nutritional Status of Children … Intake and nutritional Status of Children ......

0
Akhoni Shomay Formative Research Project CARE Bangladesh
Food Intake and nutritional Status of Children
Under the Age of Two
By
Thérèse Blanchet
and Drishti Research Centre
Dhaka, May 2010

1
Table of Content Acronyms…………………………………………………………………………………………………………….2 Lexicon……………………………………………………………………………………………………………......3 1. Introduction:..........................................................................................................6 1.1 Purpose of the research: ............................................................................................................................6 1.2 Selection of sites and duration of field work:....................................................................................6 1.3 Constitution of a purposive sample: .....................................................................................................7 1.4 Informants and research methods.........................................................................................................8 1.5 Problems encountered and limitations of the study:..................................................................10 2. Socio‐economic characteristics of households:.....................................................12 2.1 Family structure and child nutritional status: ...............................................................................12 2.2 Literacy level of parents:.........................................................................................................................13 2.3 Parents’ occupations and income generating activities:............................................................14 2.4 Impact of father’s migration on family food supply and child nutrition:............................16 2.5 Household socio‐economic level: ........................................................................................................19 3. Mothers’ health history and indicators: ...............................................................21 3.1 Mothers’ age at marriage and at first pregnancy:.........................................................................21 3.2 Ante‐natal care and child birth.............................................................................................................21 3.3 Number of children and use of contraception: ..............................................................................26 4. Breastfeeding:......................................................................................................30 4.1 Feeding Colostrums: .................................................................................................................................30 4.2 The first food: ..............................................................................................................................................32 4.3 Fathers’ limited role: ................................................................................................................................33 4.4 Complete or partial failure to breast feed: ......................................................................................34 4.2.1 Caesarian cases: ..............................................................................................................................................35 4.2.2 The baby does not have its fill: .................................................................................................................37
5. Complementary foods:.........................................................................................38 5.1 Luta and suji: ................................................................................................................................................38 5.2 Boiled rice: .....................................................................................................................................................39 5.3 Fish: ..................................................................................................................................................................40 5.4 Eggs, pulses (dal) and other proteinrich food: ................................................................................41 5.5 Vegetables and fruits: ................................................................................................................................41 5.6 Ulofa (snack foods): ....................................................................................................................................42 5.7 Khichuri: .........................................................................................................................................................44 6. Babies who ‘dry up’ because of bad spirits: traditional beliefs and treatments....46 6.1 Conditions for which kobiraj treatment is preferred:.................................................................46 6.2 Mothers clients of kobiraj:......................................................................................................................48 6.3 Child with kuiya rog: Exemplary story of failed treatment of a malnourished child:... 48 7. Conclusion: ..........................................................................................................51 Appendix 1: Complementary Food and Age When Initiated………………………….……………….. 54 Appendix 2: Weight for Age and Nutritional Status……………………………………….……………….. 55 Appendix 3:Age wise mean weight, minimum weight and maximum weight ……….………… .56 Appendix 4:Information about Households (Dehunda Union)…………………………………….……58

2
Appendix 5:Information About Households (Sutarpara Union)…………………………………….….60 Appendix 6: Information about children (Dehunda Union)……………….……………………….…….62 Appendix 7: Information about Children (Sutarpara)………………………………………….…...………64

3
Acronyms ANC Ante Natal Care ASFR Akhoni Shomay Formative Research Project CARE Cooperative for Assistance and Relief Everywhere EPI Expanded Program on Immunization FPI Family Planning Inspectors FSUP Food Security for Ultra‐Poor FWA, Family Welfare Assistant FWC Family Welfare Centre FWV, Family Welfare Visitor HA Health Assistant HH-MC Household with Malnourished Child HH‐WC Household with Well nourished Child MBBS Bachelor of Medicine and Bachelor of Science MC Malnourished Child NGO Non‐Government Organization SACMO Sub‐Assistant Community Medical Officer SHOUHARDO Strengthening Household Ability to Respond to Development
Opportunities TBA Traditional Birth Attendant THC Thana (Sub‐district) Health Complex TT Tetanus Toxoid UNICEF UN Children’s Fund WC Well‐nourished Child WFP World Food Program

4
LEXICON ayah health assistant (female) at FWC and hospital; child care
minder in private homes bel wood apple bhalobasha love, doughnut popular amongst children bhat boiled rice bhatsunni traditional rite when a baby eats rice for the first time
(Hindu); bhaji fried or roasted vegetables bhorta pureed or mashed foods; dish eaten with boiled rice chanatchur crisp snack with fried and spicy pulse paste, peanuts , etc. chowkidar village police employed by local government; guard dais traditional birth attendants dal lentil gomosta farm labour contracted for 8 months in the haor region;
tied (bandha muni) contractual employee who receives an advance payment.
ghalshia mortar and pestle to husk rice grammer daktar rural health parishioner; peddler haor geographical milieu constituted of low land that floods and
can support only one rice crop a year hayat shesh baby’s days were counted and it would die holdi beran turmeric fried with spices hozur religious person usually who leads prayers in a mosque jhal strong/hot jharphuk ‘power’ of mantra or magic blow kobiraj traditional healer who treats by means of herbal medicine,
amulets, mantra and other means to placate spirits kali zeera bhorta puree of black cumin kanda rog baby crying abnormally kobiraji traditional healing methods khichuri popular food prepared with rice, pulse, spices, oil or ghee
vegetables or meat khir or payash homemade sweet prepared with milk, sugar and fine rice. kuiya/ hugna rog baby not gaining weight and drying up lactogen infant formula most widely available luta rice porridge prepared with ground rice flour boiled in water magga beta derogatory word denoting a man who pokes his nose in
women’s affairs or rituals matree sodon government maternity home in district towns mash kalai dal variety of lentil costing half the price of the more prestigious kind moa proshad food offerings presented to a deity misri white sugar candy misripani water sweetened with white sugar candy moshuri dal red lentil (expensive) mukhebhat ceremony when a child is fed rice for the first time
(Muslim) murobbi senior & respected women/men panta bhat rice leftover from the previous night often preserved in water pet bhora to fill one’s stomach; to eat aplenty pet bhore na not to fill one’s stomach pet kamrano baby suffering diarrhea, dysentery

5
pir Muslim saint polli chikitshok rural health practitioner pushti nutrition; nourishment; locally understood as synonym of
relief food given for free and coming from foreign countries
shaldud colostrums shondesh sweet prepared with milk, sugar and little flour shorir boncorano close off the body suji wheat porridge, coarsely ground wheat flour sold in shops talmisry sugar derived from the sap of a palm tree called talmisri thana sub‐district. police station torcari curry with juice ulofa cheap snack foods; junk foods popular with children union parishod local government body composed of elected chairman and
members upordosh malevolent spirits that attack pregnant women who just
give birth and small babies

6
1. Introduction:
1.1 Purpose of the research: The study documents the feeding patterns of children up to the age of two in a rural
population of Karimgonj, Kishorganj district, Bangladesh. Weight for age as
indicator of nutritional status is taken to have sufficient merit and the growth chart
standardized by the World Health Organization (and utilized in the Shouhardo
programme conducted by CARE) is used to define categories or well‐nourished and
moderately and severely malnourished children. Initially, the objective was to
collect information on 75 children, 50 malnourished and 25 well nourished. The
sample was later increased to 119 children of whom 87 (73 percent) were
underweight and considered malnourished.
1.2 Selection of sites and duration of field work: Fieldwork was conducted in two unions, Sutar Para and Dehunda, selected following
a reconnaissance tour and consultation with CARE. Each union presents different
traits. Sutar Para is partly in the haor, a geographical milieu constituted of low land
that floods heavily and can support only one rice crop a year with risk of flood even
for that single crop (it flooded in April 2010). Fishing constitutes the second most
important source of food and income. Dwellings are crowded on land that rises
above water level and needs protection against erosion. Government services are
especially poor and Sutar Para is the only union out of the 11 unions of Karimgonj
sub‐district not having a Family Welfare Centre (FWC). Part of Suttar Para union
was included in the Shouhardo project, one component of which distributed
nutritive food, known as ‘pushti packets’, and dispensed teaching on child and
mother nutrition. A food security programme for the poor is another component of
the Shouhardo project.

7
Dehunda union is well connected with Karimgonj town and has better access to
markets, doctors and hospital. It has one Family Welfare Centre. However, services
are quite poor. Dehunda union was not included in any recent governmental or non
governmental nutritional programme although UNICEF in 2004‐2005 distributed
‘pushti (nourishing) packages’ for pregnant and lactating women and mothers with
children under the age of two. NGO activities are sparse. Dehunda has an
important male out migration to urban centres. Adolescent girls migrate to work in
garment factories and to a lesser extent domestic work. To be married or to bring
up their children, many return to the village. Others keep on working leaving their
children to be cared for by family members in the village. This temporary urban
migration influences outlooks and consumption styles and one can find evidence of
this in children’s feeding patterns.
A five‐member research team participated in the inquiry. Two women and two men
completed a two‐week fieldwork in February 2010 and three women and two men
completed a one‐week fieldwork in the first week of April of the same year. The
research was completed in four months.
1.3 Constitution of a purposive sample: Well‐nourished and malnourished children were identified from EPI centres, after
consultation with health practitioners (HAs, FWAs, TBAs) and simply circulating in
villages. The criteria for the selection were that the children should be between 2
and 24 months of age, be comprised of an equal number of boys and girls and come
from a range of socio‐economic backgrounds and not be limited to the poor. The
mothers should also be available for the interview. Once contact was established
with the mother, the child and the mother were weighed and qualitative
information was gathered regarding pregnancy, birth circumstances and feeding
patterns at different stages. The second visit augmented the population from 6 to
21 months to provide more children for the MicroNutrient project.

8
Health Assistants responsible for child immunization recognized only a few
malnourished children among the population they served. “Malnutrition is a
problem of the past”, said one, “the situation is much improved now. Here, mothers
are small and it is only normal that their babies should be light‐weight.” Such views
were found to be widespread. The high levels of malnutrition prevailing in the
1970’s and 1980’s may have contributed to set standards low. When a scale was
brought and children’s weights were plotted against the growth chart, most children
fell in the moderately to severely malnourished category. This came as a surprise to
many parents who did not see their children as malnourished. Most were
unfamiliar with a growth chart and the very concept of a normative weight for age is
very loose. Finding well‐nourished children above the age of 6 months required
time and searching over a wider area.
It should be clear from the above that conventional methods for the constitution of a
random sample were not applied. This was not the objective and the result of this
research should not be interpreted as a measure of the incidence of malnourished
children in the selected unions.
1.4 Informants and research methods
Mothers of children under the age of two were invited to narrate their experience of
pregnancy, childbirth, income, role and decision‐making in the family, work load
cooking patterns and food habits. They were asked to recall the food fed to the child
and eaten by themselves in the last 24 hours. Senior women (mothers‐in‐laws,
mothers and grand‐mothers) were also interviewed in joint family households and
elsewhere. An attempt was made to reach fathers and other male caretakers but
many were working away during the day or had migrated and were unavailable.
Members of the research team spent time at tea stalls and village shops where

9
observation was made and information collected on ulofa, a local term referring to
cakes, biscuits, doughnuts and other snack foods much appreciated by children and
fed to babies under the age of two. Team members visited two local bakeries to find
out the mode of preparing these snack foods. Traditional health practitioners, HAs,
FWA, FWV, SACMO and MBBS doctors were interviewed and a few consultations
were observed. To further test the advice health practitioners give to parents, one
field worker dressed as a peasant visited three ‘doctors’ complaining that his wife
did not have enough breast milk and what should he do. These methods allowed to
crosscheck some of the information obtained through interviews.
Sets of questions were prepared beforehand for each type of informant (Tools 1‐5 in
the Appendix) but printed forms were not taken to the interview which could
intimidate the informant. The information obtained was jotted in a notebook and
written up later. Tape recorders were also used.
Table 1: Respondents Mothers 115 Fathers 45 Grandmothers 8 Grandfathers 5 Traditional Birth Practitioners 14 Aunts/uncles 15 Rural Health Practitioners 13 Homeopaths 2 Traditional Healers (Kobiraj) 4 Health Assistants (HA) 4 Family Planning Inspectors (FPI) 2 Family Welfare Assistants (FWA) 5 Family Welfare Visitors (FWV) 2 SACMO 2 MBBS Doctors 3 Local Elected Representatives 8 Union Parishod Secretaries 5 Chowkidar/Village Police 5 Shop Owners (sell junk foods) 13 Bakers and helpers 3 Medicine shop owners/assistants 3 Pharmaceutical Representatives 2

10
1.5 Problems encountered and limitations of the study: Child feeding practices is a topic more complex than it appears. The time devoted in
this research was short and opportunities to observe behaviour limited. In Sutar
Para where the Shouhardo project had been implemented, mothers ‘knew’ the right
answers. This applies to Dehunda as well to the extent that messages about good
nutrition from different sources are mechanically repetitive. Several mothers
mentioned that they introduced khichuri as complementary food from the age of 6
months as advised by doctors and educators. However, the 24‐hour recall and
observations in the field showed that such food was rarely given and mothers did
not do what they said they did.
The focus being on very young children, there were few mothers on their own
without support. One unsupported mother had gone to beg in Dhaka leaving
behind a 2‐month‐old baby who died after “8 tins of Lactogen”, the mother said. The
child having died, this mother did not fit our criteria for selection. Family crisis that
have negative impacts on childcare were an important issue for investigation but
not much could be heard in one visit. In one household that was visited twice, it was
observed that the condition of a severely malnourished child had worsened. The
mother said that she had not cooked for 3 days. A neighbour explained that she had
learned that her husband had taken a second wife and ‐ as if this was not enough ‐
the rice crop had just been destroyed by flood (this was the second week of April).
The flood had entered this mother’s heart and washed away her ability to care for
her children. Another mother who held a severely malnourished 18‐month old child
complained that the child was demanding too much of her and she was getting
impatient. She had missed the potato harvest season, her main source of income for
the year, and her husband, a migrant worker, did not remit enough money to
support the family. A third mother had a bald patch on top of her head. Asked what
was the cause, a neighbour commented that her husband had beaten her causing an
injury that needed to be stitched. She was a battered wife. With more time, such

11
situations that impact on childcare and nutrition could have been better
investigated.
Many mothers were keen to ‘enlist’ their babies in the expectation that they would
benefit from future donation of food. Expectation of free gifts opened many doors
but it also potentially biased the information given. In both unions, people were
familiar with the free gift of food to improve nutrition and the word pushti
(nourishment, nutrition) was associated with pushti packets. Asked why he (his
wife) did not feed his child khichuri as taught by the Shouhardo program, a father
replied that they did not get American oil anymore, that is why. The common
understanding of pushti, as a food packet given for free to the poor (but often
misappropriated by the rich) is strong and will be difficult to erase. Past programs
have created expectations and also – which is possibly more damaging ‐
misapprehension on the meaning of pushti. This legacy must be recognized. Akhoni
Shomay project may decide to replace pushti with a more neutral term less loaded
with expectations of free gift, a word that invites to think anew about the food a
child needs to grow healthy.
Mothers listed types of complementary foods and the age at which they were
introduced; they described the food given to the child in the last 24 hours.
Unfortunately, there is no precision on quantities. The absence of measurement of
quantity of food fed to the child is a major limitation of the study. Only observations
made in the field can be give a hint. The Child’s Individual Sheet given in the
Appendix lists the foods mothers said they fed to their babies but when mealtime
was witnessed, the quantities of non‐rice items were very small, sometimes so small
that their nutritional value would be insignificant. The discrepancy between what
mothers said they fed to the child and what the child actually ate must be
underlined. In their replies, the mothers wanted to give a good impression to the
investigation team (often taken to be CARE staff).

12
Many issues could have been investigated with greater depth if more time had been
available. In spite of its limitation, let us hope the information collected here will
be useful for the formative research.
2. Socio‐economic characteristics of households:
2.1 Family structure and child nutritional status: Information was collected on 119 children belonging to 115 households.
Table 2 shows the type of family (nuclear, joint or extended) of the well‐nourished
and malnourished children. Slightly more malnourished children are found in
nuclear families as opposed to joint families.
Table 2: Family Patterns by Nutrition Status
Dehunda Union Sutarpara Union Family Pattern MC WC MC WC
Total
Nuclear 31 13 27 8 79 Joint 12 3 12 8 35 Extended 0 0 1 0 1 Total 43 16 40 16 115
Case histories illustrate well the advantages and disadvantages of living in different
types of family structures for the child and its mother. In one case, a 28‐year‐old
woman has 4 children and lives in a joint family that has a good amount of land. The
family is solvent but the youngest child is severely malnourished. The mother
admits that she is tired and overworked and she cannot take proper care of her
youngest child who is 18 months old. She says that her mother‐in‐law also shows
little interest in the child – a girl born after two daughters when a son was expected.
The young mother expressed her frustration about the little support she gets from a
husband who increases her workload instead of supporting her. This educated
mother (she had a Secondary School Certificate) was shocked to learn that her child
fell in the severely malnourished category. In another case, a woman with two well‐
nourished children had just separated from her in‐laws. She explains that she can

13
manage more efficiently since her migrant husband, who is a goldsmith, sends
remittances directly to her. She can give undivided attention to her children who
look healthy and well nourished.
Household composition undoubtedly influences childcare and the food intake of
small children but conclusions as to which type of household presents the best
advantage are not obvious. In a joint family, the mother has many obligations and
decision‐making power but other caretakers are present who sometimes support
the mother and care for the child. A mother said that her 22‐month old son was
healthy because everybody ‘loved’ and fed him. In such case, the joint family
benefits the child. But the question can be raised as to whether a sickly baby who
often cries gets the same loving attention. Some children are attractive, others less
so. The joint family environment is not always supportive for the mother and her
sick baby.
2.2 Literacy level of parents:
Table 3 shows the literacy levels of mothers and fathers, which is lower than the
national average: 52 percent of the mothers and 58 percent of the fathers are
illiterate. As expected, literacy levels are lower for the parents of malnourished
children. However, malnourished children are also found among mothers and
fathers with secondary education suggesting that child nutrition is a complex issue.
Table ‐ 3: Father and mother’s level of schooling
Father of Mother Educational level MC WC Total MC WC Total No Schooling 53 13 66 48 12 60 I to II 2 1 3 3 2 5 III to V 11 8 19 16 8 24 VI to VIII 12 5 17 6 6 12 IX to X 4 4 7 4 11 SSC 2 1 3 3 3 HSC & Above 2 2 Total 82 32 114 83 32 115

14
2.3 Parents’ occupations and income generating activities: Table 4 gives the father’s main occupation. The table reflects a mixed economy
with agriculture and fishing being the most important activities. Few fathers have
only one occupation and these vary seasonally and from one year to the next. As
mentioned, the economy of Dehunda is oriented more towards urban migration and
Sutar Para more towards fishing as complement to agriculture. No clear pattern
emerges relating child nutritional status to the father’s occupation.
Table 4: Father’s occupations and child nutritional status.
Occupation/activities Father of
MC Father of
WC Total
Engaged in agricultural work only 18 7 25 Agricultural work + Day labour + seasonal fishing 18 4 22 Day Labour (incl. Gomosta or tied seasonal labour) 13 6 19 Rickshaw Puller 7 3 10 Petty trader 9 5 14 Bamboo basket maker 3 1 4 Job holder (Driver, garment & other factory worker) 3 2 5 Rural health practitioner (Polli Chikitshok) 1 2 3 Boatman 2 2 Primary school teacher 1 1 Furniture maker 1 1 Goldsmith 2 2 Mason helper 1 1 Others (barber, 3 3 Sick/Inactive 2 2
Total 82 32 114 Opportunities to earn an income for women are very limited (Table 5). Two thirds
of the mothers declared having no income of their own which renders them totally
dependent on husbands, in‐laws or other family members.

15
Table 5: Mothers' Occupations and Income Generating Activities
Occupation/activities Mother of
MC Mother of
WC Total
Bamboo basket maker 6 2 8 Day Labour/ maid 2 1 3 Hen & duck rearing 5 2 7 Cattle, Hen & duck rearing 3 3 6 Fishing net maker 3 1 4 Earth worker (incl. FSUP) 4 4 Moneylender 1 1 2 Garment worker (Dhaka) 1 1 Tailor 1 1 2 Beggar 1 1 Total 27 11 38 (33.0) Not engaged in income generating activity 56 21
77 (67.0)
Interestingly, malnourished children are found in equal proportion among mothers
with income and mothers without income of their own. Some occupations, such as
raising calves, hens or ducks or lending money can be practiced ‘inside’ and do not
jeopardize social rank. Women of solvent families also practice such activities.
Other activities are clearly associated with poverty and low status such as
earthwork and begging. Earthwork employed 4 women of Sutar Para. Tree worked
under the Food Security for Ultra Poor (FSUP) project run by CARE and the fourth
was employed on a local government project. These mothers were given work on
the ground of their high level of poverty and all their children were malnourished.
They said they were not given any facility to breastfeed their babies while at work.
The one mother employed on a local government scheme lost her job because she
took time to breastfeed her 6‐month‐old baby and delayed the completion of the
teamwork. The one mother sent to beg by her husband is also very poor. It should
be pointed out that Bengali mothers do not carry their babies on their back while
working outside. This is not the practice. These mothers left their babies behind for
several hours everyday and combining work with breastfeeding was not facilitated.
One 17‐year‐old girl currently employed in a garment factory was met as she came
to remit money to her mother who is the caretaker of her child. The baby was
breastfed for two months only. At 8 months, the baby was severely malnourished.
16
The working mother remits a third of her salary (1,200 taka per month) ‐ quite a
large sum of money ‐ but the child is fed on the cheapest food ‐ boiled rice flour with
sugar and, occasionally, a little milk. The young mother said her mother is old
fashioned and does not ‘understand’ how to feed the child. The grandmother has no
other source of income and her ‘old fashioned’ ways probably reflect her economic
limitation as much as her ignorance. This case is exceptional. The babies of other
garment workers were not undernourished. Some were fed on abundant fresh or
powder cows milk and their roundedness stood out in relation to other babies the
same age. One grandmother caretaker explained that she had worked for 20 years
as a maid in Dhaka city and she ‘knew’ how to care of a child. Her model was the
middle class women she worked for. They did not breastfeed, or did not breastfeed
for long and quickly introduced complementary and substitute foods. Garment
workers being mostly absent mothers, only one was included in the sample.
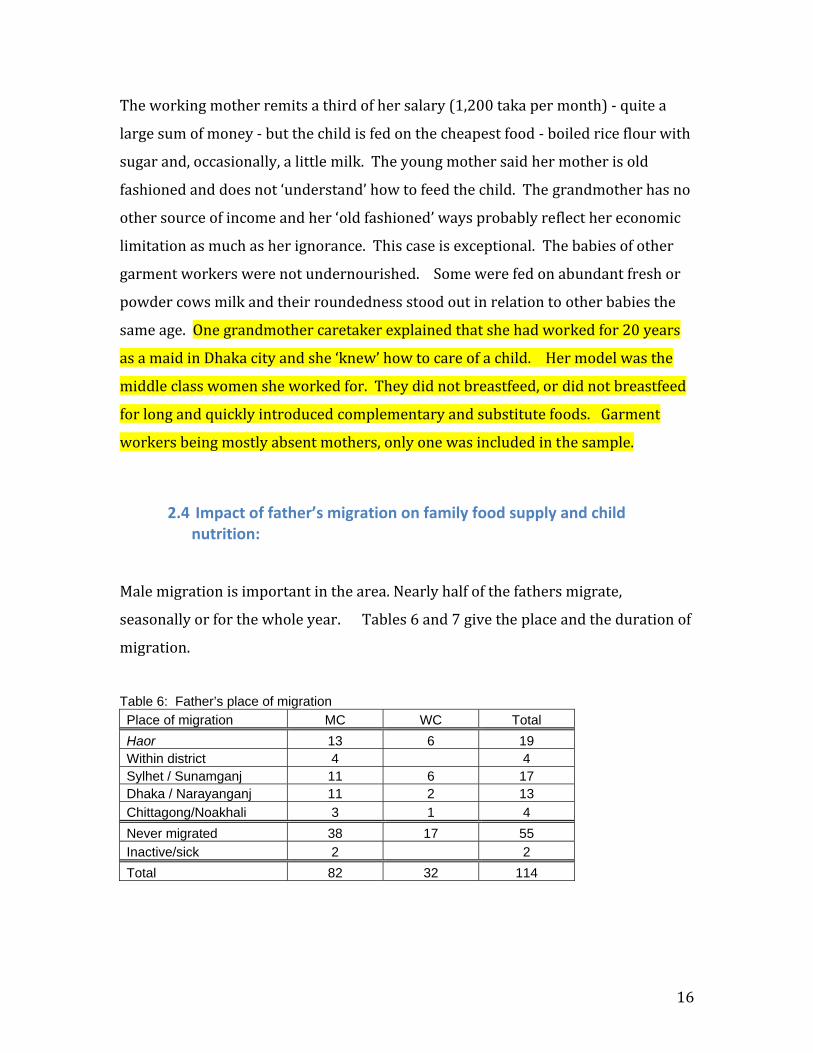
2.4 Impact of father’s migration on family food supply and child nutrition:
Male migration is important in the area. Nearly half of the fathers migrate,
seasonally or for the whole year. Tables 6 and 7 give the place and the duration of
migration.
Table 6: Father’s place of migration Place of migration MC WC Total Haor 13 6 19 Within district 4 4 Sylhet / Sunamganj 11 6 17 Dhaka / Narayanganj 11 2 13 Chittagong/Noakhali 3 1 4 Never migrated 38 17 55 Inactive/sick 2 2 Total 82 32 114

17
Table 7: Father’s duration of migration
Duration of migration
MC
WC Total
Up to 3 Months 22 4 26 Up to 6 Months 5 5 10 Up to 9 Months 5 2 7 Up to 12 Months 6 4 10 Total 38 15 53
Migration provides an income when local employment is unavailable, which is
positive. But remittances are often irregular and uncertain and wives who stay
behind with the children – by far the most common situation ‐ must ensure that the
food reserve lasts. Some husbands do not entrust their wives with money. Others
hold money but are not allowed to spend as they think fit and must account to the
husband when he returns. Some husbands complain that their wives spend too
much in their absence – it could be on credit at the local shop ‐ and wives retort that
their husbands underestimate the family food requirement in their absence. One
woman and her malnourished child were weighted at 25 days interval and both had
lost weight. The mother commented. “All family members lost weight since my
husband (a rickshaw puller) left. There is no one to purchase the little extra he used
to bring home: we have not eaten fish, we don’t get fresh vegetables and I don’t buy
milk. The husband had left a supply of rice, oil and lentil before he left but his wife
made a conservative usage of it. For this family, food has gone down in both, quality
and quantity.
Are wives as resource‐less in the absence of their husbands as they pretend to be?
To what extent does this discourse simply reproduces the norm that men provide
and wives and children depend on them? More time would have been needed to
read the sub‐text. But on the surface, mothers do not appear much empowered in
the absence of their husbands although some spoke of the greater freedom they
enjoyed. One mother said that when her husband was away she replaced ulofa with
homemade food. She did not think that ulofa was good for the children but when
her husband brought them, she could not intervene. Some mothers said they

18
cooked once instead of twice a day and the meals were less elaborate. This is not
necessarily good for the children.
Sometimes, entire families migrate. One mother with a severely malnourished child
opted not to migrate to Narayangonj brickfield this year to take better care of her
baby. The husband and the mother‐in‐law migrated alone.
A young father who worked as a day labourer said he would not migrate because he
had no capital to buy a reserve of food prior to departure and he was not sure he
could send regular remittances. This man tried hard, to the extent of his ability, to
feed his family and in spite of his meager income, his children were in relatively
good health.
What to make of these stories and impressions regarding migration? For the
Akhoni Shomoy Programme, migration in its many forms is a reality that must be
reckoned with. Populations are mobile, and especially the poor. Although, this is
not easy, a special effort should be made to reach migrant fathers. They should be
more aware about the nutritional needs of family members, especially their
pregnant or lactating wife and their small children. Feeding children adequately
should not be a matter of dispute between husband and wife.
Fathers’ migration creates rhythms of food deprivation followed by feast and plenty.
One can see that both can be problematic. When migrant fathers return home with
their savings, there is the prospect of eating better food but also junk food of the
ulofa category. Migrant fathers are generous with the latter. Wanting to please
their children, they offer them food, which is damaging to their health.

19
2.5 Household socio‐economic level: Table 8 gives the per‐capita income for households with mal and well‐nourished
children and Figure 1 presents the same data in terms of Extremely Poor, Poor and
Solvent households.
Table 8: Per‐Capita Income for Households with Mal and Well‐Nourished Children Per-Capita Income (BDT) HH-MC HH-WC Total HH-MC (%) HH-WC (%) Below 300 2 2 2.41 300-499 8 8 9.64 500-699 13 6 19 15.66 18.75 700-999 32 10 42 38.55 31.25 1000 -1499 21 7 28 25.30 21.88 1500-1999 2 2 4 2.41 6.25 2000-2499 3 2 5 3.61 6.25 2500-2999 2 2 0.00 6.25 3000+ 2 3 5 2.41 9.38 83 32 115 100.00 100.00 Figure 1: Economic Level of Households with Mal and Well Nourished Children
0
5
10
15
20
25
30
35
HH. with Malnourished Child 27 33 23
HH. with Well-Nourished Child 5 13 14
Extreme poor Poor Solvent

20
The economic level of households bears a strong relationship with the nutritional
status of the child, the extreme poor having the highest percentage of malnourished
children, which is hardly surprising. It is more puzzling to see that 62 percent of the
children in solvent households are malnourished. Economic wealth and the ability
to access food do not ensure that children are well fed, again pointing out to a
multiplicity of factors in malnutrition. In solvent households, one sees young
mothers saddled with heavy work and not having power and control. Also within
large solvent families, all are not equal. A wife whose husband is sick or
unemployed may have to serve everyone else while she and her children’s needs are
not given importance. The young age of the mother and her inability to express
herself and be heard are also factors. Parul is 18 years old and her 4‐month‐old
baby is severely malnourished although it was born healthy. She says she does not
have enough breast milk, yet her in‐laws are a solvent family. The young mother
looks depressed. She says that when her time comes to eat – after everyone else, ‐
the vegetables and the fish in the torcari are gone and only juice is left. Her husband
migrates the year around. He also earns less than her two brothers‐in‐law. Parul’s
distress is hidden behind the wall of an affluent family. Mothers and mothers‐in‐
law may be unaware about child nutritional requirements in solvent and in poor
families but it is more difficult for the richer people to admit that a child is
malnourished as it hurt rank and status. Some mothers‐in‐law in solvent families
are particularly stubborn about their ways saying they have nothing to learn from
anyone. The ‘know’ what a child needs.

21
3. Mothers’ health history and indicators: The answers mothers gave to the questionnaire are presented here. Although
differences between mothers of well and malnourished children are not
considerable, it is interesting to note what appears meaningful.
3.1 Mothers’ age at marriage and at first pregnancy: On the whole, mothers were married very young ‐ 42 percent before the age of 16 –
and most had their first pregnancy between 16 and 18. One finds a slight difference
between mothers of malnourished and well‐nourished children, the latter having
begun their childbearing period a little later.
Table 9: Mother's present age and age at marriage
Present Age Age at Marriage Age at first pregnancy Age MC WC MC WC MC WC Up to 15 years 36 12 6 2 16 to 18 6 1 37 11 54 14 19 to 21 19 4 10 9 20 15 22 to 24 15 9 3 1 25 to 27 22 10 28 to 30 7 1 31 to 33 4 5 34 & above 10 2 Total 83 32 83 32 83 32
3.2 Ante‐natal care and child birth
Apart from receiving tetanus toxoid (TT) injections, most mothers did not get any
antenatal care (tables 10 and 11). Only 10 percent of the mothers‐to‐be visited a
satellite clinic, which should provide antenatal care according to government plan.

22
Some mothers believe that going to a satellite clinic is a waste of time and they will
not learn anything that they do not already know. Others are frustrated by the long
wait for staff that do not turn up or turn up late (they do not live locally) and rush
through consultations. It must be said that satellite clinics are multi‐purposes and
the staff (FWV, FWA and ayah) have little time for pregnant women. There are no
facilities for check ups. Nutrition is not given importance.
Married at 14, Anju gave birth to her first child at 15. She did not breastfeed
because, during pregnancy, her breasts secreted a liquid and sores developed under
her tight blouse. Both, her mother and her aunt (the birth attendant) told her not to
breastfeed. Her first child survived on Lactogen and on cow’s milk – her brother
offered her a cow ‐ but the second child died 16 day after birth. Fed sweetened
water and diluted cow’s milk by bottle, it “dried up”. It was taken to a kobiraj1 first,
then to a doctor shortly before it died. Seeing the bottle, the doctor got angry and
asked her why she did not breastfeed. Anju’s third pregnancy ended in a stillbirth.
When she got pregnant a 4th time, Anhu got determined to seek advice about her
ability to breastfeed. She waited at the satellite clinic to get the attention of the FWV.
The latter told her that there was no reason why she could not breastfeed. She
should wash her breast with soap regularly and stop wearing the tight and dirty
blouse. Anju’s confidence was boosted and she successfully breastfed her fourth
child.
Anju received assistance at the satellite clinic, but what wastage before it happened.
Her young age and her lack of knowledge and her following the advice of her mother
and her aunt who were not trained dais (traditional birth attendants) did not help.
The latter may have interpreted her symptoms as signs that she suffered upordosh
and was possessed by some kind of spirit that ‘ate’ her babies (these beliefs will be
discussed below). As a mother undergoing her 4th pregnancy, she had more say
1 We shall see below that such condition often leads to seek treatment from traditional doctors as the cause is assumed to be spiritual.

23
and more mobility and it is then that she made the choice to consult the FWV who
was experienced and most helpful.
On the day she was interviewed, the FWV said she did not have enough time to see
pregnant women. This is hardly surprising. The clinic opened at 11 o’clock when it
should have opened 2 hours earlier. The deterioration of health and family planning
services is increasingly discussed at national level and in the media. This study can
only concur with the conclusion that services are poor. The satellite clinic does not
attract pregnant women and in Sutar Para, as mention, the union has no clinic and
the staff (SACMO, FWV, FWA) sits at Niamatpur market, which is far away. In these
circumstances, one cannot be surprised that ancestral beliefs survive.
Anju’s story is a good illustration of the lack of mobility and the lack of experience of
of adolescent mothers expecting their first child. They are under the influence and
authority of the senior women (murobbi) who often favour the traditional treatment
of kobiraj to ‘close off the body’ (shorir bon corano) which is explained below.
Women who face problems during pregnancy are more likely to visit government
facilities at sub‐district and at district levels (thana health complex, district sadar
hospital and matree sodon). Together with private clinics, such facilities were
availed by 20 percent of the women during pregnancy. These visits are costly and
women go with their husband or other caretaker. The main purpose of the visit is
often unrelated to the pregnancy. They go for the treatment for ‘gastric’, ‘headache’
or other problem. One may say that many receive ante‐natal check ups by chance.
Parents strongly desiring a son also visit doctors to get an ultra‐sonogram to know
the sex of the baby. The practice has recently increased in Karimganj . We have not
heard of sex selective abortion. Doctors are cautious not to announce a daughter
arguing that the picture is not clear.
When doctors examine a pregnant woman, they reportedly give advise about
nutrition. These are mechanically repeated and do not seem to impact much on the

24
recipient. In any case, patients go to doctors to get ‘medicines’ and this is what they
mostly remember.
A majority of mothers did not take iron and calcium tablets while pregnant. Those
who took them got them from doctors consulted at sub‐district or at district levels
and not from the satellite clinic. In Dehunda, a peddler ‘daktar’ cultivates a
clientele of pregnant women and sells iron and calcium tablets for 60 taka accepting
credit if need be. This ‘daktar’ has good selling skill, far better than the government
health staff.
About two thirds of the mothers‐to‐be (64.3 percent) had no antenatal care (if one
excludes kobiraji and other traditional methods). Here, one notes an important
difference between the mothers of malnourished and well‐nourished children, the
latter being twice as likely to have consulted and received antenatal care. This
suggests more receptivity to health messages and better trust in ‘modern’ health
practitioners (for lack of a better term). A quarter of the women (25.5 percent)
sought protection from kobirajs who dispense amulets and thread to wear, oil to rub
on the body. These precautions constitute a kind of antenatal care in the eyes of
those who believe in malevolent spirits (upordosh). With girls undergoing a first
pregnancy, mothers who lost a succession of babies through spontaneous abortion,
stillbirth or early death are good clients of the traditional practitioners.
Mothers of well‐nourished children were more likely to deliver at their natal home
where they reportedly received better care and attention. There is little difference
in the kind of birth attendant assisting the mother in home deliveries. Ten mothers
(8.5 percent) had hospital deliveries and these were all cases with complications
(high pressure, oedema, bleeding, etc). Five mothers (4.3 percent) received the
assistance of a nurse midwife for a home delivery (table 13).

25
Table 10: Antenatal care MC-Mother WC-Mother Total Never visit doctor, clinic or hospital 62 12 74 Mother received ANC in Satellite clinic 5 7 12 Mother herself visit doctor or THC due to complication 7 6 13 Zila Sadar Hospital or Zila FWC (Matree Sodon) 3 1 4 Private Clinic 4 3 7 Others (Homeopath, Smiling Sun, Village doctor) 2 2 4 Missing information 1 1 Total 83 32 115 Table 11: Tetanus Toxoid Vaccination
MC-Mother WC-Mother Total TT vaccine not receive 10 3 13 TT vaccine receive 72 30 102 Total 82 33 115 Table 12: Place of birth MC-Mother WC-Mother Total Given birth the last child at marital home 49 15 64 Given birth the last child at natal home 27 15 42 Hospital 7 2 9 Total 83 32 115 Table 13: Birth Attendant MC-Mother WC-Mother Total Trained TBA 19 8 27 Untrained TBA 35 13 48 Relatives 17 8 25 At hospital 8 2 10 Nurse-midwife for a home delivery 4 1 5 Total 83 32 115 Table 14: Assessment of newborn’s health and weight MC-Mother WC-Mother Total Normal in size and weight 45 31 76 Underweight 29 0 29 Premature baby 6 1 7 Early complications (pneumonia, cough, jaundice) 7 0 7 Total 87 32 119

26
Mothers of malnourished children were more likely to report that the baby was
small at birth2 and/or had suffered complications such as respiratory disease or
jaundice (table 14).
3.3 Number of children and use of contraception:
Tables 15, 16 show that 115 mothers have 308 living children for a total of 369
pregnancies.
Table 15: Number of Living Children by mothers of well and malnourished child
No. of living children MC - Mother WC - Mother
No. of Mother (%)
No. of Total Living Children
1 22 7 29 (25.2) 29 2 24 14 38 (33.0) 76 3 14 5 19 (16.5) 57 4 8 3 11 (9.6) 44 5 9 1 10 (8.7) 50 6 3 1 4 (3.5) 24 7 3 1 4 (3.5) 28 83 32 115 (100.0) 308
Table 16: Number of pregnancies by mothers of well and malnourished child No. of Total Pregnancies MC-Mother
WC-Mother Total
Total Pregnancies
1 20 6 26 26 2 19 9 28 56 3 10 8 18 54 4 12 2 14 56 5 7 3 10 50 6 8 1 9 54 7 5 2 7 49 8 2 1 3 24
Total 83 32 115 369 The time gap between pregnancies is often small (Table 17). Nearly half of second
and subsequent children were conceived before the previous child reached one
2 These are the perceptions of the mothers and other close relatives. No precise measure of birth weight exists with home delivered babies.

27
year. In such cases, the mother is likely to breastfeed throughout her pregnancy
and up to, and even beyond, the birth of the second child.
Table 17: Gap between pregnancies Gap between child Dehunda Sutarpara Total % Within 1 year 33 22 55 47.8 Within 2 year 57 40 97 84.3 Within 3 year 36 11 47 40.9 Within 4 year 15 11 26 22.6 Within 5 year 8 5 13 11.3 Above 5 year 7 5 12 10.4 Interestingly, the first child born to a mother is the most likely to be malnourished
(table 18). This situation may relate to child marriage, early pregnancy and the low
status of the young wife in her in‐law’s home. Inexperience, lack of mobility and
sometimes psychological distress could be factors. A woman’s third child is the least
likely to be malnourished and this could relate to the growing confidence and
progressive assertion of the young woman as she gains status as a mother of several
children. Case histories exemplify these changes. The chances of a 4th, 5th or 6th
child being malnourished increases again but the number of children is here so
small, one should not venture an interpretation.
Table 18: Rank of the Malnourished/Well‐Nourished Child among a Mother’s Children
Rank of the MC/WC Child
Malnourished Child
Well-Nourished Child
Malnourished (%)
Well nourished (%)
1st 22 7 25.3 21.9 2nd 18 8 20.7 25.0 3rd 11 8 12.6 25.0 4th 13 3 14.9 9.4 5th 6 2 6.9 6.3 6th 10 1 11.5 3.1 7th 5 2 5.7 6.3 8th 2 1 2.3 3.1
Total 87 32 100.0 100.0

28
Figure 3: Rank of the Well / Malnourished Child among siblings
Figure: Rank of the Mal/Well-Nourished Children
0.0
5.0
10.0
15.0
20.0
25.0
30.0
1st 2nd 3rd 4th 5th 6th 7th 8th
Perc
ent
Malnourished (%)
Wellnourished (%)
Table 19 shows that 71.4 percent of the women and 2.7 percent of the men use a
contraceptive method. Most of those who do not use contraceptives want a child or
believe they will not get pregnant (table 20). Here only a small number of women
admitted wanting contraceptives but not having access to them. Male use of
contraceptive is abysmally low. Table 19: Contraceptive Use
MC WC Total Type of Method Father Mother Father Mother Father Mother
Vasectomy (NSV) 2 2 Ligation 3 3 Pill 33 16 49 Injection 8 4 12 Condom 1 1 Taking herbal medicine from Kobiraj 3 3 Nothing 33 12 45 Total 2 80 1 32 3 112
Table 20: Mothers’ reasons for not using contraceptive (multiple answers) MC- Mother WC- Mother Total Wants to have another baby 9 9 Pregnant 1 1 2 Husband lives elsewhere 2 2 4 Bad side effects 5 1 6 Menstruation not yet begun 8 5 13 Menstrual problem 1 1 Husband wants son 2 2 4 Too old to be pregnant again/no need 3 1 4 Wants to use/ no access 2 2 Total 33 12 45

29
Children were weighted with and without their mothers. Table 21 and Figure 2
give mother’s weight in relation to the child nutritional status. That mothers of well‐
nourished children, on average, have higher weights is, as one would expect.
Table 21: Mothers’ Weight and Child Nutritional Status Weight
(In Kilogram) Mother of Mal-Child
Mother of Well-Child Total
% of MC Mother
% of WC Mother
Below 35 7 0 7 8.4 35 – 39 20 1 21 24.1 3.1 40 – 44 30 14 44 36.1 43.8 45 – 49 12 14 26 14.5 43.8 50 – 54 9 2 11 10.8 6.3 55 + 5 1 6 6.0 3.1 Total 83 32 115 100.0 100.0
Figure 4: Mothers’ Weight & Nutritional Status of Child
Figure: Mother's Weight & Nutritional Status of Child
0.05.0
10.015.020.025.030.035.040.045.050.0
Below 35 35 - 39 40 - 44 45 - 49 50 - 54 55 +
Weight in KG
Perc
ent MC (%)
WC (%)
These data provide a timely reminder that the child’s health begins with the
mother’s health during, and even before, pregnancy, her physical and emotional
maturity, her ability to carry, sustain and care for the baby. That is why the locking
up of adolescent girls in marriage and their bearing children too early, together with
the low status accorded in their in‐laws home are factors contributing to the
malnutrition of babies. Mothers’ low weight, their inability to space pregnancies for

30
different reasons, their lack of income and control over resources, these and other
problems exposed in this section are well known. Yet, they persist. A broad
perspective needs to be kept in mind when addressing child nutrition.
4. Breastfeeding:
4.1 Feeding Colostrums: Widely disseminated messages regarding the benefits of feeding colostrums
(shaldud) have been heard and have changed behaviours to some extent.
Discarding colostrums used to be common practice, the substance being associated
with the pollution of childbirth, compared with pus, and considered harmful to the
baby3. In this investigation, only 3 mothers unambiguously stated getting rid of the
colostrums before putting the baby to the breast: one mother breastfed her baby on
the third day; another breastfed on the fifth day after carefully removing the thick
yellowish substance. Excluding mothers who did not breastfeed because of delivery
by caesarian, breast infection or nipple problems, all others declared putting the
baby to the breast soon after birth. However, actual behaviour is more complicated.
A mother declared that she did not discard colostrums. Yet, she was observed falling
a few drops of the thick substance before getting her 4‐day‐old baby to suck because
“this is the custom”. She added that this ‘milk’ accumulated during pregnancy and it
had gone stale (bad). Upon probing, several mothers admitted doing the same.
The table below shows separately the results obtained for Sutar Para and Dehunda
unions. The difference for the two unions is probably due to the different
interpretations of the research teams on the importance of discarding a few drops of
colostrums. Should it be interpreted as a mere ritual gesture without nutritional
consequences? How to assess the quantity discarded? Both results are presented
here to illustrate the difficulty of the investigation and interpretation.
3 See Blanchet, T. Meanings and Rituals of Birth, University Press Limited, Dhaka, 1984

31
Table 22: Union-wise reporting on the feeding of colostrums Colostrums Fed Dehunda Sutarpara Total Fully 16 (26.7) 36 (61.0) 52 (43.7) Partly 42 (70.0) 17 (28.8) 59 (49.6) None 2 (3.3) 6 (10.2) 8 (6.72) Total 60 (100.0) 59 (100.0) 119 (100.0) Figure 3: Colostrums fed:
Colostrums Fed
44%
49%
7%
Fully Partly None
The message that colostrums is good for the baby and should not be discarded has
been heard, no doubt. Yet, the belief that the parturient remains in a state of
pollution for a set number of days after birth, and that her colostrums is a dangerous
substance for the child persists.4 If 44 percent of the mothers confirmed fully
feeding the colostrums, a higher percentage still settled for a compromise feeding
colostrums but getting rid of the first secretions, which are the richest part. One
must conclude that, although progress has been achieved, much remains to be done
to realize the full benefits of breastfeeding.
Some mothers continued breastfeeding a child while pregnant with another and,
after the birth, they breastfed two babies. Such mothers are not aware of producing
colostrums. Whatever colostrums are produced in such circumstances, the older
child gets the greatest part of it.
4 See Blanchet, T. 1984

32
4.2 The first food: In assessing exclusive breastfeeding, the first week of life has been set apart: 44.3
percent of the mothers did not exclusively breastfeed their baby during this time.
Water, water sweetened with misri5, honey or diluted cow’s milk were fed with a
spoon, a shell or by getting the baby to suck a cloth imbibed with the substance.
Reasons given for administering these elements are:
1) The mother does not produce ‘milk’ yet,
2) The baby is in danger of de‐hydratation,
3) Swallowing something ‘pure’ clears the mucus (polluted substance) that
remains in the baby’s orifices.
4) Misri protects against ‘pneumonia’ (a generic term referring to respiratory
infections).
5) This is our tradition. It needs not be explained.
6) The baby should start life with the taste of sweetness
Senior women (and not the parturient) generally feed water, water with misri or
other substance to the child. In some families, the issue as to whether the baby
should be fed in this way opposes two generations of women. A young wife not
listening to her mother‐in‐law in this matter would be held responsible should her
baby get sick later on. The issue can also divide in‐laws. A young woman delivered
her first baby at her mother’s home. The mother‐in‐law who came to visit accused
her of ‘killing’ the baby as she insisted on exclusive breastfeeding. The mother‐in‐
law was honoured – the baby belongs to the patri‐linage ‐ and, in her presence, the
baby was fed water with misri. After she left, the new mother discarded the water
and carried on only breastfeeding. These contested issues are also the stuff of
family politics.
5 Misri is a white sugar derived from the sap of a palm tree called talmisri

33
Tables 23 shows that mothers of well‐nourished children are almost twice as likely
to have breastfed their babies soon after birth and to have abstained from feeding
water and sweeteners. Babies who were not breastfed all fall in the malnourished
category together with babies who were put to the breast two days or more after
the birth. There is no surprise here (table 24). Such data should be shared with
those who advise mothers not to breastfeed their babies for a variety of reasons.
Table 23 :The first food fed to the child after birth
Type of food Malnourished
Child (%) Well nourished
Child (%) Total (%) Breast milk 30 (34.5) 20 (62.5) 50 (42.0) Water 17 (19.5) 4 (12.5) 21 (17.6) Misri with water 30 (34.5) 5 (15.63) 35 (29.4) Honey 3 (3.4) 2 (6.25) 5 (4.2) Cow’s milk 7 (8.0) 1 (3.125) 8 (6.72) Total 87 (100.0) 32 (100.0) 119 (100.0) Table 24: How long after birth the baby is put to the breast
Time Malnourished
Child (%) Well nourished
Child (%) Within 1 hour 24 (27.6) 20 (32.3) Within 2 hours 16 6 Within 6 hours 11 3 Within 12 hours 6 2 Within 24 hours 2 1 Within 2 days 6 Within 3 days 11 Within 4 days 1 Within 5 days 2 Never breastfed 8 Total 87 32
4.3 Fathers’ limited role: In a group discussion with men, one participant – father of 7 children ‐ stated that
shaldud is sold at shops in tins. An older man immediately rebuked him saying that
this is mother’s milk. It used to be discarded but now doctors say it is good and it

34
should be fed to the baby. Many fathers had heard about the benefits of feeding
colostrums from TV, radio and elsewhere, but very few could tell whether their own
wives had actually fed it to their children. Fathers are not invited in the house of
birth and most do not regard these matters as part of their domain.
I never told the mother to breastfeed or not to breastfeed. This is her body.
This is women’s work. If a man pokes his nose into the affairs of women, people will laugh. They will call him ‘magga beti’ (effeminate man). For men, this is shameful. Beside, I know nothing about this.
The father takes on an active role when it is declared that the mother cannot
breastfeed and infant formula or other food should be purchased from the market.
Fathers are well aware of the commercial product available as substitute to breast
milk (the most common being Lactogen 1) and many knew accurately how much it
costs. It should be said that men of the household generally are not involved in
deciding whether the mother has the ability to breastfeed or not. They often act
upon the recommendations of the senior women (mother, mother‐in‐law or other
relative).
4.4 Complete or partial failure to breast feed: The cultural and the religious injunction to breastfeed remains strong in Karimganj,
as in most of Bangladesh, and the decision not to breastfeed is never expressed as a
matter of individual choice. Mothers who do not breastfeed invoke causes beyond
their control. These fall into 4 types: (1) caesarian case, (2) breast infection (3)
nipple problem and (4) a fear that the baby does not get its fill.

35
4.2.1 Caesarian cases:
A 16‐year‐old girl was delivered by caesarian as she showed signs of eclampsia. The
nurse at Kishorgonj district hospital helped the adolescent girl to breastfeed her
baby for the first 15 days but when a second hospitalization was required to a more
distant hospital, the mother was separated from the child and breastfeeding was
discontinued. All family attention was directed to the young mother whose life was
in danger. She survived. When she returned home, the baby had grown
accustomed to bottle‐feeding and did not suck its mother’s breast. The young
mother and her caretakers at home received no advice on the management of such
situation. At 14 month, the baby is severely malnourished.
One can understand that when the mother’s life is in danger, all attention should be
on her and breastfeeding becomes secondary. Yet, breastfeeding is critical as
failure to breastfeed effectively leads to malnutrition as the study clearly shows.
Beliefs associated with surgical ‘operation’ need addressing. Mothers who were
delivered by caesarian section are convinced that their bodies are not fit to
breastfeed and their entourage sustains such view. Such women ingurgitated
dangerous medicines that could poison the baby. More over, ‘operations’ weaken
the body and if the baby sucks its mother’s milk, the mother will not recover her
strength. Pheana had two operations. She was delivered by caesarian section and
had a second operation later because she could not urinate (she had eclampsia). She
had plenty of breast milk when she returned home two weeks after the birth but her
husband, her mother‐in‐law and her mother forbade her to breastfeed. The mother
fully recovered but her child is now severely malnourished.
In private and in government hospitals, breastfeeding is largely recognized as
beneficial and we have evidence that assistance is given to the mother. There has
been a marked improvement in the last two decades on this matter even though the
handling of some cases remains questionable. Angura had 7 pregnancies and 5 of
her children are alive. She and her husband are day labourers and they are very

36
poor. She had a breast infection while pregnant with her last child. After the birth,
she went to see a doctor in Karimgonj regarding this problem and he gave her
medicines. He also told her not to breastfeed from the infected breast and
prescribed Lactogen 1 for the baby. The 4‐month‐old baby is already malnourished.
Angura explained:
I bought 3 tins of Lactogen. I cannot afford to spend so much and the baby cannot have its fill.
I am a workingwoman. How can I hold her in my arms all the time? Lactogen is like water. She urinates right away. Nothing stays inside.
When she gets 5 month old, I will feed her ‘luta’ (boiled rice flour with sugar). That will fill her stomach and she will sleep. I will then be able to work without tension.
This baby had no luck. I breastfed my other children for one year and I had no problem.
Doctors should realize that many of their patients cannot afford to buy several tins
of Lactogen and would only give very diluted portions, not to mention the difficulty
of keeping the bottle clean (as these babies are fed with bottle). The infant formula
is prescribed like a ‘medicine’ and is often understood as such. What is ‘medicine’,
what is ‘food’ and how do food and medicine relate to health? This is a critical
question.
The first tin of Lactogen is ‘medicine’. It is bought without hesitation and even very
poor parents find the money to pay for it but purchasing subsequent tins is a
different matter. This is so because of the prohibitive cost but also because of
misapprehension on the need for continuous quality feeding for the child to grow
healthy. When interpreted as ‘medicine’ with magical power, the prescription of
Lactogen is dangerous and is hardly better than the amulet of the kobiraj.

37
4.2.2 The baby does not have its fill:
Angura says she cannot keep the baby at the breast all day long. She wants a
content baby with a full stomach who will sleep and allow her to work. She says
that her baby does not have its fill ‐ pet bhore na.
This assessment – pet bhore na is made by mothers in very different circumstances.
Healthy mothers in affluent households who do not lack breast milk evoke it, and
poor mothers and malnourished also claim it. A 22‐year‐old mother was visiting
her father’s home with her 2‐month‐old baby ‐ the first grandchild of the family. She
and the child received much love and her father attentively listened to his daughter.
She said she did not have enough breast milk and the baby was hungry. She ‘knew’
this because the baby cried a lot. This educated mother whose husband was on a
mission abroad with the army had developed an outlook shared by several middle
class mothers. They want ‘the best’ for their children and this ‘best’ is associated
with (prestigious, superior) infant formula.
Poor mothers lacking energy also introduce complementary food early because,
arguably, the baby does not have its fill. Anwara is 32 year old. Married at the
age of 13, she had 7 pregnancies. Four children are alive and they are all daughters.
She does not use a family planning method because her husband wants a son. With
her last child, Anwara felt that her breast milk did not suffice and she began feeding
bottles of water with sugar15 days after the birth. She considers water with sugar
to be ‘food’ in the sense that it fills the baby’s stomach. If she had not fed this ‘food’,
her daughter would be worst off, she thinks. Under this regime of sweetened water,
the baby was certainly less hungry and sucked the breast less. This was the
mother’s intention.
Anwara did not do this for her other children but this time she felt tired and ‘old’.
At the interview, her poor health was obvious and her ‘tiredness’ was both physical
and psychological. She talked about the pressure to produce a son and to arrange

38
the marriage of 4 daughters in the future. This weighed heavily on her. Her 7
months old daughter was moderately malnourished. The 24 hour recall mentions
that she had eaten half a pushti biscuit distributed in schools6 and brought home by
her sister. Not intended for babies under two, these pushti biscuits constitute
nonetheless an important complementary food. Interestingly, they are not classified
as belonging to the class of ulofa.
The subjective elements in the perception that one’s breast milk is inadequate need
careful attention. Doctors and health advisors brush aside as false consciousness,
laziness or ‘superstitions’ the reasons invoked by mothers. But women are not only
their bodies and the common assumption that mothers ‘naturally’ breastfeed is
simplistic and reductive of the values humans invest in their actions. Much has been
written elsewhere on the reasons why mothers breastfeed or do not breastfeed
their babies but very little has been done in Bangladesh. This is a complex issue
that deserves research.
5. Complementary foods:
5.1 Luta and suji:
The first complementary food given is usually luta, which is home‐ground rice
boiled in water to which sugar is added or, less often, milk and sugar, or salt. It is
cooked to different consistencies depending on the age of the child and the mode of
feeding (bottle, spoon or hand). Paddy husked at home with mortar and pestle
(ghalshia) produces rice which is not entirely polished. However, rice purchased on
the market is totally polished. A coarsely ground wheat flour (suji) is also cooked in
the same way. Luta and suji are nutritionally poor, especially when no milk is 6 The World Food Programme distributes the pushti biscuits to primary school children. Each child gets a packet containing 8 biscuits. Teachers are instructed to ensure that the 8 biscuits are eaten on the school premises but we found many pushti biscuits brought home and fed to pre‐school children. In Sutar Para, the school teacher attributed increased school attendance to the distribution of the pushti biscuits.

39
added. They have the advantage of being widely available and easily prepared. The
first complementary food is generally sweetened and even poor families spend a
substantial amount of money on white sugar. The baby is accustomed to sugar
early, and this makes the introduction of non‐sweetened food problematic. The
assumption that a baby’s food should be sweetened should be addressed
Luta is introduced when the mother believes the baby does not have its fill and this
perception, as seen above, is highly variable. A mother introduced luta for her 2‐
month old baby but most mothers introduce it much later. Table 17 shows that
more that a quarter of the mothers introduced luta from 9 months onward, that is at
least 3 months later than the WHO recommendation. (see also Child’s Individual
Sheet in Appendix).
Table 17: Age when Luta or suji were initiated
Malnourished
Child Well nourished
Child Total
Below 6 months 7 3 10 6-8 months 23 11 34 9-11 months 13 2 15 Above 12 months 3 3 Total 46 16 62
5.2 Boiled rice:
The introduction of boiled rice (bhat) marks a life stage, which, traditionally, has
been ritualized at about 9 months. The Borman (Hindu fishermen) in Sutar Para call
the ceremony bhatsuni. Food offerings are made to a deity (moa proshad) , after
which the maternal uncle (mama) feeds the child a shondesh made of milk and sugar
before introducing a few grains of rice in its mouth. Similar practices are observed
among Muslims who cook sweet rice with milk and spices (khir or payash) and
introduce rice in a ritual called mukhebhat. Relatives offer gifts and the event is the

40
object of a feast. These rituals underline the central place of rice as ‘food’ and as
symbol of wealth and prosperity.
The Bengalis are known to eat largest quantities of rice – the largest amount per
capita in the world according to a report. Rice is cooked without salt and is
flavoured with the bhorta, bhaji, torcari and other accompanying dishes, the variety
evidently depending on the socio‐economic level of the household. A common
practice is rural households is to prepare the accompanying dish(es) with much chili
and salt. In this way, much rice can be consumed but, for small children, this is truly
problematic.
Boiled rice is first served to small children with salt and mustard oil. The oil makes
the rice soft and tasty; it also accustoms the child to food which is a little hot (jhal)
and salty after eating sweetened food. Mustard oil is believed to have positive
properties protecting against cold and cough. Progressively, the child is fed a little
of the family main dish which contains much chilly and salt. A pinch to give taste to
the rice is all that is given.
5.3 Fish:
Feeding fish to children, even among fishermen, is delayed. It will be done when the
child is ‘old enough’, when it can speak and is able to complain of a fish bone stuck in
its throat, for example. Feeding fish to small children causes worms, says a
proverb. It may also be the instrument of malevolent spirits (upordosh). In one
family, it was observed that, from a dish containing small fish, tomatoes and
potatoes, only a piece of potato with some of the juice was given to the 20‐month‐
old child.
Mothers’ answers reported on the Child’s Individual sheet should be interpreted
with caution. If a mother answered that she fed some of the family dish containing
fish to the child, it does not mean that the child ate a piece fish.

41
5.4 Eggs, pulses (dal) and other protein‐rich food:
The same applies to other protein‐rich foods, which are occasionally fed to the child
but in very small quantities. A shop owner pointed out how little dal he sold. Dal is
said to be costly but this is a matter of perception. When one sees how much
families spend on junk food, replacing the latter with dal would be considerably
cheaper.
5.5 Vegetables and fruits:
The first round of the investigation was conducted in February, a time when many
vegetables (tomato, potato, bean, cabbage, cauliflower, bitter gourd) were abundant
and cheap. Karimgonj is a vegetable garden for Dhaka and the local population
benefits from this production. Tomatoes, potatoes and beans were regularly
consumed but, for some reason, cabbage and cauliflowers were not found on the
menu. A survey conducted during the monsoon would give quite different results
with a much lower consumption of vegetables. It is important to take into account
seasonal variations in the advice given to mothers about good nutrition. Rigidly
uniform menus that cannot be realized the year around should not be suggested.
Fruit trees are rare in the crowded villages and purchased fruits are expensive. To
feed a child (imported) grapes and oranges would be a rare and memorable event.
Perhaps this is why it was reported as a food given to the child in the questionnaire.
Fruits are not regularly eaten and many mothers said that they could not afford to
feed ‘fruit’ to their children. Again, messages about good nutrition should only
propose what is possible to realize, less mothers feel alienated or unconcerned.
Some fruits available in April (e.g. bel) were not fed to children. Others (e.g.
banana) are not particularly rich in nutritive value.

42
5.6 Ulofa (snack foods):
Ancestral rules concerning rice and fish fed to small children are still followed. Yet,
there is no taboo concerning ulofa which refers to snack foods such as cake, biscuit,
doughnut, crisps, chips and chanatchur purchased from shops. They come in
different shapes and colours and sometimes bear attractive names such as
bhalobasha (love) and are highly appreciated by children. Bhalobasha (love) is the
name of a popular doughnut that sells for 1.50 taka.
Most parents believe that ulofa is good for small children. Babies as young as three
months old are fed the soft cake. No danger is perceived in feeding this food. As the
child gets older, biscuits, doughnuts and other snack foods are given, in some
families without restraint. As one mother said: “Two kinds of foods are good for
babies: milk and ulofa”. Ulofa foods were not sold in villages 10‐15 years ago but
only in larger markets that were visited once a week. Nowadays little shops have
sprung up everywhere even in remote villages. Two shop owners interviewed
stated that ulofa was what they sold the most and it was their main source of profit.
One of them stopped selling bananas, potatoes, onions and other perishables to
concentrate on ulofa. Twelve different kinds of cakes, biscuits, doughnuts and other
ulofa hung in open bags attracting child customers (and flies). Mothers came to
pacify a baby with a bhalobasha doughnut and 3‐4 year old boys came by
themselves several times a day to buy on credit cakes and biscuits of their choice.
Fathers who ‘love’ their children paid the bill at the end of the week.
The association of ulofa with bhalobasha is not fortuitous. Parents, and especially
fathers, manifest care and affection to their children through the procurement of
ulofa food. Few parents wish to refuse a child bhalobasha (love and doughnut).

43
Costly biscuits with attractive packaging (Energy Plus, Olympics, etc) and advertized
on TV (with older children as consumers) are also available in village shops. But the
most widely consumed ulofa foods are the cheap ones produced in the district that
are not individually wrapped. A visit to two bakeries gave some idea of the
fabrication process. In one of them, hair and flies were seen plowed into the dough
in front of our eyes not to mention the sweat running from the baker’s arms in the
extremely hot place. Oil that had been used to fry several batches of food the
previous day was poured as ingredient for the cake baked on that day. “This is good
oil, we re‐use it before it gets too dark”, explained the assistant. Food inspectors
visit the bakery but only to collect bribes, confirmed one of the bakers. Although it
was not possible to check more bakeries, serious questions can be raised on the
quality of these products.
Table 18 shows the age at which ulofa was introduced for 64 children. Unlike luta
or suji, the consumption of ulofa does not end at the stage when the child is ready to
eat rice but it continues and often increases to the point of replacing rice.
Table 18: Age when Ulufa foods are introduced
Malnourished
Child Well nourished
Child Total At 3 months 1 1 4 months 2 2 5 months 1 1 6 months 5 5 7 months 9 1 10 8 months 9 3 12 9 months 6 2 8 10 months 8 8 11 months 3 2 5 13 months 3 1 4 16 months 6 6 18 months 1 1 19 months 1 1 Total 53 11 64

44
The enthusiasm with which ulofa foods are fed to children – including children
considered too young to eat rice, vegetable and fish ‐ in a matter of concern.
Awareness of the harm done by eating these foods was found among parents of
children who, at the age of 3 ‐ 5 refused to eat anything but ulofa and were stunted,
often sick and generally in poor health. Then, may began a cycle of visits to
‘doctors’ who prescribe B Complex vitamins, Zinc supplement or de‐worming
medicine all of which come in a syrupy form that reminds children of ulofa. A child
was observed demanding syrupy medicine three times during a one hour interview
and the mother obliged being unable to refuse. Behind these consumptions, lie
important business interests. Movements for the protection of consumers are
beginning to surface in Bangladesh but there was no sign of them in the study area.
Pre‐school children do not get the pushti biscuits. Anyway, children brought up on
ulofa tend not to appreciate pushti biscuits that are not sweet to their taste.
5.7 Khichuri:
For several years and through different programmes, mothers have been advised to
prepare khichuri and feed it as complementary or weaning food to children.
Khichuri contains rice, lentils, oil, vegetables cooked long enough to be soft. It is a
prestigious restaurant food when cooked with meat. The dish is attractive and the
name seems appropriate to convey a message about the nutritive requirements of
children. Yet, it has not achieved the desired purpose. In the study area, most
mothers heard that khichuri is good for children. A kind of festival was organized
under the Shouhardo project when a large amount of khitchuri was prepared and
distributed to members. The joyous event is still remembered. Yet, hardly any
mother was found to prepare khichuri after the project closed down.
The reasons given for not preparing khichuri were:
• The ingredients are not available (pushti packets are no longer distributed).

45
• It is troublesome to prepare. It requires time, fuel, and additional cooking
pot (which are scarce). The ingredients are not at hand.
• The child does not like it.
• Babies eat very little. Why go to the trouble of cooking a separate dish when,
in the end, older children eat it. They can eat like adults.
• It is simply not worth the trouble (there is no fridge in the village).
The arguments given – lack of time, fuel, cooking pot, unavailability of the
ingredients and uncertain results ‐ should be taken seriously. Village conditions
differ from the city. Cooked food must be eaten before it gets spoiled. The dish is to
be cooked with a lentil (moshuri dal) which is twice as costly as the one more
commonly used in the village (mash kalai dal), so getting the ingredient is seen as a
problem.
Advocated by government, NGOs, medical practitioners as the panacea to combat
child malnutrition, the word khichuri has lost credentials and probably should be
abandoned. It suffers three major faults:
1. Like ‘pushti packets’, it has been associated with the free gift of food from
foreign countries entertaining an unhealthy dependency.
2. It is associated with relief goods raising resentment regarding past
corruption and injustice of distribution when those most in need did not get
their share.
3. The remedy has been prescribed without explaining the food value of each
ingredient. Hence, a rigid interpretation of the ‘cure’ and when the
ingredients cannot be obtained, it is rejected en bloc.
Lessons should be drawn from the failure of the khichuri campaigns. It did not
promote self‐reliance and resourcefulness based on the acquisition of adequate and
applicable knowledge regarding a child’s nutritional needs.

46
6. Babies who ‘dry up’ because of bad spirits: traditional beliefs and treatments
Many mothers consulted a kobiraj while pregnant and wore an amulet and a thread
invested with the ‘power’ of mantra or magic blow (jharphuk). After birth, the baby
was given the same protective elements. In serious conditions, kobiraj apply more
drastic and highly imaginative treatments, which would be too long to describe
here. In a sample of 51 mothers, 13 (25.5 percent) sought kobiraj treatment while
pregnant and, in addition, 7 (13.7 percent) did so specifically for a sick child. In
other words, at least 4 out of 10 mothers were under kobiraj protection or
treatment. Many mothers and children were seen wearing one or several amulets
and the intervention of kobiraj (pir and hozur) frequently appeared in case histories.
It was not a major focus of the research and data are fragmentary. Yet, the study
would be defective if it did not include a discussion of the practices of traditional
practitioners and of the beliefs on which they are based and the influence it has
particularly in interpreting and treating the symptoms of malnutrition.
6.1 Conditions for which kobiraj treatment is preferred: While doctor treatment is believed to be good for certain illnesses such as
‘pneumonia’ (respiratory diseases), many hold that kobiraj treatment is best for the
following conditions:
1. a baby not gaining weight and drying up: kuiya/hugna rog
2. a baby crying abnormally: kanda rog
3. a baby suffering diarrhea, dysentery: pet kamrano
4. a baby refusing to suck the breast:
There is good chance that the above conditions relate to malnutrition in their causes
or in their effects, or in both. This is what ‘scientific’ medicine is likely to conclude

47
but kobiraj theories and treatments do not make such links and can be highly
damaging by simply ignoring the importance of food intake. Begum’s 6‐month‐old
baby had severe diarrhea (condition 3) and she consulted 3 kobirajs. One of them
told her that her baby’s days were counted and it would die soon (hayat shesh).
Nonetheless, her neighbours convinced her to consult a doctor at the thana health
complex. When the doctor saw the baby, she admonished the mother. Why did she
waste time with kobirajs. Why did she not come to the doctor earlier? The doctor
decided to hospitalize the baby but Begum took it home. She explained that she did
so for 3 reasons: (1) Her husband, a migrant worker, was away and she did not
have his permission, (2) she had no money and (3) the kobiraj who said that her
baby would die cultivated doubt in her mind. If this was so, why stay in hospital.
The baby died the next day and the father arrived for the burial.
This story is exemplary. Doctors often complain of being the last one to be
consulted when saving the child may not be possible. The advantage of consulting
kobirajs is their accessibility and their social proximity. Case histories confirm that
they are often consulted first. Going to a kobiraj is an initiative that can be taken by
women alone. It does not require that the husband be involved. Kobirajs can be
paid in kind with rice, banana, oil or other common goods that are not difficult to
find. They can be paid later unlike doctors who demand cash payment at the visit.
Kobiraj theory is not ‘foreign’ to the local people and many are convinced that
harmful spirits inhabit their universe. These spirits (which are dangerous to name
individually and are collectively referred to as upordosh) are known to be particular
fond of new wives, pregnant women, women who have just given birth and small
children. Kobirajs build their practice on these beliefs and, clearly, in 2010 in
Karimganj, and no doubt in many parts of Bangladesh, they have not lost their
clientele even though some conditions such as neo‐natal tetanus – manifest in
symptoms 1 and 4 ‐ have almost disappeared with TT injections.

48
6.2 Mothers clients of kobiraj: The clients of kobirajs are many but among them are young wives pregnant for the
first time. Mothers‐in‐law advise them to ‘close their bodies (shorir boncora)’ to
prevent attacks by upordosh. Also, mothers who have lost babies already seek the
treatment of kobirajs. The malevolent spirits gazed at them once (drishti or nozor
dawa) and darted their poison, so they may well do it again. A mother who lost
babies supposes that the spirits are attracted to her. Under pressure from elders or
of their own accord, such women follow proscriptions and observe taboos more
strictly than others. They abstain from eating many kinds of fish during pregnancy‐
mrigel, boal, shoal, gozar, tsikra ‐ and in the house of birth, they do not eat fish at all
and stick to dry food ‐ turmeric fried with spices (holdi beran), puree of black cumin
(kali zeera borta), flat bread and ulofa. Following these rules generally result in a
diet poor in protein. Other restrictions ‐ avoiding going out at certain times and
avoiding passing under neat fishing nets while pregnant instill caution and fear.
Such women may not be receptive to messages about the need for pregnant and
lactating mothers to improve their diet. A mother explained that as a young wife
under the control of her mother‐in‐law, she had been careful and her babies lived,
but when she established her own households, she had been ‘lazy’ and negligent and
this is why two of her babies died. At her next pregnancy, she deliberately adhered
to the old proscriptions again and was sorry for her past bravery.
6.3 Child with kuiya rog: An exemplary story of failed treatment of a malnourished child:
Rahima had four children. The eldest is 8 years old, the second died at the age of 6
months from pneumonia, the third and the fourth are 3 years and 18 months and
are severely malnourished. Rahima struggled with malnutrition with all her
children. Presently, Hakim weighs 6 kg at the age of 3 years and Okia weighs 5.2 kg
at 18 months. We got interested in Rahima’s last two children. While Hakim is

49
considered a clear case of kuiya rog (condition 1) ‐ the worst case of malnutrition
found during fieldwork ‐, , the parents do not recognize Okia as a cause of alarm.
This family history will be reviewed, as there are important lessons to be drawn.
Rahima’s family has suffered chronic poverty. Her husband used to migrate to
work in Comilla leaving insufficient food and Rahima had no other source of income
at the time. Three years ago, the husband stopped work migration as his health
had deteriorated. Presently, husband and wife weave bamboo baskets for a living.
They work at home and can look after their children at the same time. They have an
arrangement with a businessman who gave them an advance payment and now
buys their baskets at a cheap rate. Together, husband and wife earn 70 to 80 taka a
day and, with this income, they support a family of 5.
Rahima’s 2nd, 3rd and 4th child were born in the span of 4 years. Not surprisingly,
Rahima is in poor health. When she was pregnant with the 4th child, her body
swelled and her head ‘spinned’. Rahima says she had little breastmilk from the 3rd
child onward. She believes that the death of the second child and the continuous
secretion of breast milk that could not be sucked caused an obstruction of the milk
conducts. In any case, Hakim was born small and, at 3 months, he was hospitalized
for malnutrition for 12 days. The doctor said that the baby did not get enough
breast milk and the mother should eat better and larger quantities of food. The
husband commented: “We are a poor family. Where can we get additional food
(shongshare obhab. Barti khabar kothai pabo?)” This exchange between doctor
and patient is a well‐rehearsed discourse. What is being communicated here, or
rather, why is the message back and forth not taken? Hakim returned home and his
condition continued to be poor. When he was 9 months, his mother got pregnant
again. She breastfed throughout the pregnancy. Hakim lost his mother’s milk at 18
months. His condition rapidly deteriorated.
One year ago, Rahima sought help for her son from a rich family of the village now
living in Dhaka. They gave 4,000 taka to treat Hakim. The money was entrusted to

50
one of their relatives. Hakim was taken to Kishorganj district hospital and a battery
of tests was done on him. Then, the money was gone and Hakim was returned
home. The large amount of money spent on their son impressed the parents. They
retain that doctor treatment is very costly but it is ineffective to treat certain
diseases (e.g. kuiya rog) which are better left to the kobiraj. According to Rahima,
the doctor said nothing about feeding her son. After this episode, the parents placed
all their hopes in kobirajs. At present, Hakim is massaged everyday with special oil
and ghee obtained from a woman kobiraj. The two bottles must be replenished
before getting empty and the healing property of the substance will not be lost. The
parents are doing something for their extremely weak child who, age 3, cannot walk
and the rest is in god’s hand. Rahima, on whose shoulders fall the heaviest
responsibilities, is clearly an exhausted mother.
The 4th child, Okia, was included in the study and we have data on colostrums and
complementary foods. Okia did not get full colostrums as a baby. It was fed
sweetened water first and was put to the breast on the 2nd day (we do not know
whether Hakim, the 3rd child, was still breastfed then). Okia was fed breast milk up
to 10 months complemented with luta and salt only from 11 months onwards. At 16
months, rice with mustard oil was introduced. The 24‐hour recall reveals that the
18‐month‐old baby was fed breast milk in the morning, rice with mustard oil at
noon, a cake in the afternoon and a biscuit and breast milk at night. The mother ate
rice with mixed vegetables three times. The portions were small and she may not
have had her fill but a little of the beans, tomato and potato dish could have been fed
to Okia. The mother did not think fit to do so. To sum up, complementary food was
introduced late and its nutritive value is very poor. Even in this poor family , we
discover that ulofa foods are fed to small children.
If Rahima did not learn about nutrition and still invest all her hope in the treatment
of a kobirajs, after such history, then questions must be raised. This is a case of
repeated failures with a malnourished mother giving birth to underweight babies
and raising malnourished children, one of who dies, while the others survive

51
stunted and damaged for life. Poverty and ignorance combine with inadequate
health services. What did the 3rd child get from a battery of tests at the district
hospital? Nothing. Here we see that good intention – giving 4,000 taka to a poor
family – can also have damaging effects since it sent the family back to kobirajs.
And these advices about good care and nutrition – vague and non‐specific words
mechanically pronounced by doctors belonging to another world ‐ in what way do
they help?
This is the failure of individuals but of an entire health system unable to tackle
problem of child malnutrition. Blaming the ‘superstitions’ of parents and the villain
kobirajs is too easy. What about the missed opportunities, the inappropriate
treatments and the ineffective advices received from the representatives of
‘scientific’ medicines. Poverty does not explain (or excuse) everything either. In
any case, poverty is not a fatality.
7. Conclusion:
Child nutrition has been a neglected problem. With an appropriate approach,
prospects for success are high even the issue is not simple. There is an urgency to
stop a damage, which in some families, has been perpetrated from one generation to
the next due to faulty understanding of what a child needs to grow.
The problems are complex. The Aknoni Shomoy project must limit its action to
what is possible but it should strive to keep a vision wide enough to encompass the
economic, the social, the cultural and situate actors ‐ primarily mothers – in the
contexts in which their actions take meaning and value.

52
Mothers should be taught about the nutritional needs of their babies and the values
of foods normally available and which they can afford. With complementary and
weaning foods, teaching should insist on variety, on quantity and the regularity of
food intake which a baby needs. Food, not only of the kind that ‘fills the stomach’
but also build ‘strength’ should be well identified.
Fathers need to be reached and convinced that nutrition is important. It requires a
few items to be made available. These are costly, but less so than ulofa foods. How
can father please their children and manifest their ‘love’ through other means than
junk food. There should be campaign to limit the unrestrained consumption of
these items. Ulofa, syrupy medicines, sweetened food, tought should be given on
how to reverse these trends.
The practices of the numerous ‘daktar’ having a shop or peddling also needs
addressing. The prescription of ‘Domperidone’ to increase breast milk is a
widespread practice that is harmful and needs to be stopped.
Some of the advices given by kobirajs are highly detrimental. For example, mothers
that have lost babies before are told to discard the first milk and throw it in a river.
The substance is believed to be so harmful, it may hurt even for domestic animals.
Restrictions of food intake and on movement recommended by kobiraj are
appreciated by others as well. At a focus group discussion, elderly women
expressed their dislike of messages advising pregnant and lactating women to eat
more and better food, and refrain from too heavy work. They argued that today
young women are ‘weak’ and are made even weaker by following such messages.
Mothers need to be reached early and for those who are convinced success should
be visible and demonstrable.

53
Again, resourcefulness and intelligence in adapting imaginatively and simply the
food normally available for the family should be encouraged. This should be
completed with the creation of vegetable gardens as encouraged by the Shouhardo
project.
The idea that good nutrition will come through food packet distributed by foreign
donors should definitely be abandoned. And for good nutrition to be ensured there
is no magic ‘medicine’, only good habits
Better health services would provide a healthy competition to kobiraj treatment.

54
Appendix 1: Complementary food and age when initiated (multiple count as different foods were fed at different ages) Complementary food Age
2 Month
3 Month
4 Month
5 Month
6 Month
7 Month
8 Month
9 Month
10 Month
11 Month
12 Month
13 Month
14 Month
15 Month
16 Month
17 Month
18 Month Total
Luta-1 (rice porridge with sugar) 3 3 4 1 2 2 15 Luta-2 (rice porridge with sugar & milk) 1 5 1 3 2 12 Luta-3 (rice porridge with salt) 2 3 1 2 1 2 11 Suji -1 (Wheat porridge with sugar) 1 1 2 2 6 Suji -2 (Wheat porridge with sugar & milk) 1 1 1 3 Jau (rice or wheat light porridge) 1 3 4 Khichuri (rice+dal+vegetable+salt+e.oil) 3 3 3 1 2 2 14 Bhat with KhasToil (rice+salt+mustard oil) 2 2 2 1 4 3 4 4 3 7 4 7 43 Fish Salun Bhat (rice, vegetable and fish) 2 5 5 2 3 8 1 9 4 5 16 60 Salun Bhat (rice and vegetable) 1 2 6 8 9 4 6 36 Dud Bhat (rice and cow milk) 2 1 1 1 5 Dal Bhat (rice, Lentil) 1 1 1 2 3 4 4 16 Cow milk 5 5 1 2 13 Powder milk 2 1 2 1 6 Lactogen + Cow milk 1 1 2 Ulufa (industrial and non-industrial dry food items) 1 1 9 11 5 3 6 5 6 6 10 9 11 15 11 109 Hand made bread (wheat/rice flour) 1 1 Rice/Taler Pitha (rice flour, with palm juice) 2 1 2 5 Fruits (banana, orange, grapes) 4 1 2 1 8 Sago 1 2 3 School biscuit (WFP) 1 1 3 1 2 2 10 Total 2 1 12 10 36 33 33 16 21 17 24 14 21 38 31 35 38 382

55
Appendix 2: Weight for Age and Nutritional Status
Sl.No. Age
(Month) S.M.C Sl. No. Age
(Month) S.M.C Age
(Month) M.M.C Age
(Month)
Mildly Under Weight
Age (Month)
Well nourished
Weight 1 2.5 2 33 14 6.6 3 3.8 4 5.2 2 5.4 2 2.5 2.4 34 14 6.2 6 6.1 5 5.3 2 6.1 3 5.5 3.1 35 14 6.1 6 5.2 6 6.3 2 4.5 4 5.5 2.7 36 15 7.7 8 5.8 10 7.2 2 4.7 5 5 4.2 37 15 7.3 9 6.5 11 8.8 2.5 6 6 5 4.8 38 16 6.9 15 7.8 11 8 4 6 7 5 4.1 39 16 8.4 16 8.6 11 7.6 4 6.8 8 6 5.5 40 16 7 16 8 12 8.4 4 6.2 9 6 3.4 41 16 8.2 17 9.2 12 9.2 5 6 10 6 5 42 17 7.4 19 8.4 14 8.5 5 6.6 11 7 3.5 43 17 8 20 8.8 24 10.3 5.5 6.9 12 8 4.5 44 18 8.2 21 8.9 6 6.5 13 8 5.7 45 18 6.7 6 8.1 14 8 5.1 46 18 8 6 6.5 15 9 5.4 47 18 7.7 7 8.2 16 9 6.3 48 18 8.6 7 7.8 17 11 6.5 49 18 6.3 7 7.4 18 11 6.7 50 18 5.7 8 8 19 11 7.2 51 18 5.2 8 7.9 20 12 7 52 18 8 9 10 21 12 5 53 19 7.8 9 8.3 22 12 6.7 54 19 8.1 9 8.6 23 12 6.5 55 20 7.8 10 9.2 24 12 6 56 22 8.4 11 8.9 25 12 7.3 57 23 5.8 12 8.8 26 12 6.2 58 23 7.1 13 8.9 27 13 6.7 59 23 7 14 9.1 28 13 6 60 24 8.2 14 9.1 29 13 6.6 61 24 8.4 18 10.1 30 13 6.9 62 24 8.3 19 11.5 31 13 4.5 63 24 9 22 11 32 14 6.6 64 24 8.6 23 10.9
Note: S.M.C = Severely Malnourished Child, M.M.C = Moderately Malnourished Child. Total Infants = 119

56
Appendix 3: Age wise mean weight, minimum weight and maximum weight
Age in Month Total
Children
Mean weight of both sexes
(K.G)
Infant (G) minimum
weight (K.G)
Infant (G) maximum
weight (K.G)
Infant (B) minimum
weight (K.G)
Infant (B) maximum
weight (K.G) 2 7 4.44 2.0 4.5 2.4 6.1 3 1 3.80 3.8 4 4 6.05 5.2 6.8 6.0 6.2 5 9 4.56 3.1 6.0 2.7 6.9 6 9 5.84 3.4 6.5 5.0 8.1 7 4 6.73 3.5 8.2 7.4 7.8 8 6 6.17 4.5 7.9 8.0 9 6 7.52 5.4 8.3 8.6 10.0
10 2 8.20 7.2 9.2 11 7 7.67 6.5 8.9 6.7 8.8 12 10 7.05 5.4 8.8 5.0 9.2
13 6 6.60 6.0 8.9 4.5 6.9 14 7 7.46 6.6 8.9 6.2 7.7 15 3 7.60 7.3 7.8 7.7 16 6 7.85 6.9 8.0 7.0 8.6 17 3 8.20 7.4 9.2 18 10 7.45 5.2 10.1 5.7 8.2 19 4 8.95 7.8 11.5 8.1 20 2 8.30 7.8 8.8 21 1 8.90 8.9 22 2 9.70 11.0 8.4 23 4 7.70 5.8 10.9 7.0 24 6 8.80 8.2 8.3 10.3
119 Note: Infant (G) =Girl Infant, Infant (B) =Boy Infant

57
Appendix 4: Information about Households (Dehunda Union)
Sl. No.
Mother's name
Mother's present age
Father's Name
Father's present
age Child's Name Sex Village Name
Ward No. HH. ID
Family Pattern
No. of total
Pregnancy
Total Living
children 1 Shorufa 35 Soltu 46 Hridoy M Bhatia Gangpara (Purbo) 7 H - 183 Nuclear 7 7 2 Morzina 19 Humayun 25 Treesha F Bhatia Gangpara (Purbo) 7 H - 32 Nuclear 2 2 3 Piana 25 Joj Mia 43 Kaifa F Khamar Dehunda 1 H - 840 Nuclear 3 3 4 Ajifa 30 Miraj Uddin 38 Noyon M Khamar Dehunda 1 H - 844 Nuclear 4 2 5 Happy 29 Sonju Mia 36 Lamia F Khamar Dehunda 1 H - 839 Nuclear 5 4 6 Asma 28 Shamsuddin 32 Lamia F Khamar Dehunda 1 H - 705 Nuclear 6 5 7 Orbula 28 Abul Bashar 32 Rashid M Chor Dehunda 2 H - 29 Nuclear 6 4 Khurshid M 8 Parvina 38 Died ** Rabbi M Khamar Dehunda 2 H - 147 Nuclear 7 7 9 Halima 18 Shafiqul 25 Rubel M Khamar Dehunda 2 H - 149 Nuclear 1 1
10 Rahima 27 Monzil 34 Okia F Khamar Dehunda 2 H - 148 Nuclear 4 3 11 Shabana 24 Suruj Mia 35 Tayeba F Khamar Dehunda 2 H - 99 Nuclear 2 2 12 Bedana 25 Zahed 37 Rumi F Shakoa Namapara 9 H - 535 Nuclear 2 2 13 Halima 35 Hares Mia 42 Rafia F Shakoa Namapara 9 H - 572 Nuclear 8 5 14 Kolpona 24 Borzu Mia 35 Al-Ismail M Shakoa Namapara 9 H - 553 Joint 4 3 15 Juena 22 A. Rahim 25 Shakibur M Shakoa Namapara 9 H - 558 Nuclear 4 3 16 Salma 24 Edris Ali 30 Sharmin F Shakoa Namapara 9 H - 557-X Joint 3 2 17 Maksuda 20 Sumon 25 Sadia F Shakoa Namapara 9 H - 404 Joint 1 1 18 Asma 25 Ripon 28 Rahat M Bhatia Gangpara (Poshchim) 5 H - 1284 Joint 2 2 19 Bedena 34 Wahed Mia 44 Jubayer M Bhatia Gangpara (Poshchim) 5 H - 1532 Nuclear 6 4 20 Ambia 30 Rashed 40 Tanzina F Bhatia Gangpara (Poshchim) 5 H - 1186 Nuclear 8 6 21 Piana 24 Junu Mia 38 Razia F Bhatia Gangpara (Poshchim) 5 H - 1139 Joint 4 4 22 Halima 24 Sonju 30 Mushahid M Chor Dehunda (Dokkhinpara) 3 H - 71 Nuclear 2 2 23 Zahura 23 Abu Kalam 32 Maruf M Chor Dehunda (Dokkhinpara) 3 H - 44 Nuclear 1 1 24 Lolita 22 Aftab 27 Rafiq M Chor Dehunda (Dokkhinpara) 3 H - 9 Nuclear 5 3 25 Haresa 20 Wahab 28 Ramzan M Chor Dehunda 3 H - 61 Joint 2 2 26 Hawa 27 Kamrul 36 Raqib M Chor Dehunda 3 H - 67 Nuclear 3 3 27 Asia 22 Karim 32 Ashadul M Shakoa Namapara 9 H - 515 Nuclear 6 4 28 Jahanara 27 Anisur 34 Mohima F Chor Dehunda 3 H - 292 Nuclear 4 3 29 Ambia 25 Saiduzzaman 28 Nabila F Chor Dehunda 3 H - 299 Joint 4 3 30 Nargis 20 Rafiqul 28 Jannatul F Shakoa Namapara 9 H - 575 Nuclear 2 2 31 Rubina 22 Sirazul 38 Rubima F Chor Dehunda 3 H - 260 Nuclear 2 2

58
32 Sheuli 23 Fozlul Karim 34 Aqib M Chor Dehunda 3 H - 295 Nuclear 4 2 33 Shoma 22 Kabir 26 Lamia F Bhatia Gangpara (Purbo) 7 H - 028 Nuclear 2 2 34 Rupa 25 Hadich Mia 38 Maisha F Bhatia Gangpara (Purbo) 7 H - 187 Joint 3 3 35 Sarjahan 35 Golap Mia 55 Ashiqul M Dehunda Gudaraghat 3 H - 282 Joint 5 3
36 Rekha 22 Mokles 25 Sujon M Chor Dehunda (Dokkhinpara) 3 H - 28 Nuclear 3 2
37 Jebunnesa 31 Rojob Ali 36 Arafat M Bhatia Gangpara (Poshchim) 5 H - 1289 Nuclear 5 4
38 Begum 31 Chunnu Mia 40 Sadia F Bhatia Gangpara (Poshchim) 5 H - 1201 Nuclear 5 4
39 Anura 32 Mojibor 42 Shipu F Khamar Dehunda 1 H - 95 Nuclear 7 4 40 Parvin 33 Helal 43 Rubaiya F Khamar Dehunda 1 H - 90 Nuclear 7 6 41 Parvin 20 Jalal 30 Suraiya F Chor Dehunda 1 H - 683 Joint 1 1 42 Ruma 20 Matiur 28 Rea F Chor Dehunda 1 H - 23 Nuclear 1 1 43 Amina 17 Hanif 22 Meem F Chor Dehunda 1 H - 27 Joint 1 1 44 Zinnata 20 Faruk 29 Emon M Chor Dehunda 1 H - 231 Nuclear 1 1 45 Zulekha 17 Khairul 27 Nuha F Chor Dehunda 1 H - 861 Joint 1 1 46 Modina 27 Abu Taher 44 Tofazzol M Shakoa Poshchimpara 8 H - 275 Nuclear 2 2 47 Rahima 38 Siraj 45 Reza F Shakoa Poshchimpara 8 H - 223 Joint 8 7 48 Nazma 20 Tara Mia 42 Zeesan M Shakoa Poshchimpara 8 H - 277 Joint 2 1 49 Zahura 35 Hadich Mia 26 Abdullah M Shakoa Poshchimpara 8 H - 209 Nuclear 6 5 50 Morzina 17 Montaz 38 Emon M Shakoa Poshchimpara 8 H - 276 Nuclear 1 1 51 Lovely 23 Saiful 42 Nuween F Shakoa Namapara 9 H - 1013 Nuclear 2 2 52 Hafsa 27 Rukku Mia 40 Nazmul M Shakoa Namapara 9 H - 407 Nuclear 4 4 53 Shukia 22 Kajol 30 Afsana F Shakoa Namapara 9 H - 536 Nuclear 5 2 54 Aklima 21 Faruk 32 Ashamoni F Shakoa Namapara 9 H - 406 Nuclear 2 2 55 Angura 34 Roton 45 Taiba F Shakoa Namapara 9 H - 533 Nuclear 7 5 56 Begum 21 Borju 35 Shamim M Shakoa Namapara 9 H - 885 Joint 2 2 57 Sabina 19 A. Hashem 27 Jakia F Shakoa Namapara 9 H - 885 Joint 1 1 58 Mina 27 Idu Mia 42 Mustakim M Shakoa Namapara 9 H - 578-X Nuclear 4 3
59 Shoma 26 Abu Taher (Dakter) 40 Mim F Shakoa Poshchimpara 8 H - 265 Nuclear 2 2

59
Appendix 5: Information about Households (Sutarpara Union)
Sl. No. Mother's name
Mother's present
age Father's Name
Father's present
age Child's Name Sex Village Name Ward HH. ID Family Pattern
No. of total
Pregnancy
Total Living
chikdren 1 Saleha 25 Alaudduin 30 Lailu F Puran Chamta 2 H-345 Joint 4 2 2 Masuda 26 Milon 28 Mahin M Puran Chamta 2 H - 308 Joint 1 1 3 Asma 22 Ab. Kaiyum 25 Noman M Sutarpara 5 H - 915 Nuclear 3 3 4 Sharaswati Barman 34 Niranjan Barman 48 Tisa moni F Sutarpara 5 H - 986 Joint 6 5 5 Hena 21 Anju Mian 25 Ahsanullah M Sutarpara 5 H - 607 Extended 1 1 6 Raj Bahar 26 Kobir Mian 28 Tamim M Khakshri 4 H - 4 Nuclear 2 2 7 Asma Begum 24 Renu Mian 30 Wasim M Chong Noagaon 9 New Nuclear 3 2 8 Anwara 22 Joidhar 25 Zihad M Chong Noagaon 9 New Nuclear 1 1 9 Fatema 26 Asad 40 Shofiqul Islam M Sutarpara 5 H - 4560 Nuclear 4 3 10 Rekha Akhter 27 Zahed Mian 40 Tahmina Shanta F Sutarpara 5 H - 889 Nuclear 7 6 11 Joshna 30 Fazlu 35 Sonia F Sutarpara 5 H - 576 Nuclear 4 4 12 Sahana Khatun 24 Zahed Mian 26 Ratul M Sutarpara 5 H - 870 Nuclear 2 2 13 Rupa 20 Nazrul Islam 26 Enayetullah M Sutarpara 5 H - 878 Joint 1 1 14 Rehana 32 Anam Mian 45 Kohinoor F Chong Noagaon 8 H - 308 Nuclear 6 6 15 Zulekha 20 Sonju 25 Zihad M Chong Noagaon 8 H - 309 Joint 2 2 16 Eron 24 Khaleque Mian 30 Sajon M Chong Noagaon 8 H - 321 Nuclear 3 3 17 Mahmuda 30 Bacchu Mian 40 Sadia F Chong Noagaon 9 H - 80 Nuclear 5 5 18 Sabina 20 Mahbul 35 Faisal M Chong Noagaon 9 H - 79 Nuclear 1 1 19 Shakina 29 Babul 37 Munna Hussain M Chong Noagaon 9 H - 131 Nuclear 4 5
Munir Hussain M Chong Noagaon 9 H - 131 Nuclear 20 Rozina 26 Habibur Rahman 29 Motahar Hussain M Chong Noagaon 9 H - 130 Nuclear 3 3 21 Ruma 28 Awal Mian 39 Ramin M Chong Noagaon 9 H - 135 Joint 3 3 22 Nadira 18 Habibullah 22 Nadir Mian M Chong Noagaon 9 H - 2 Nuclear 2 1 23 Sheuli 17 Rahat Mian 25 Eva F Uttar Goneshpur 1 H - 305 Joint 1 2
Shimanto M Uttar Goneshpur 1 H - 305 Joint 24 Rotna 24 Habibur 32 Rafi M Uttar Goneshpur 1 H - 241 Joint 3 3 25 Sathi 18 Kobir Mian 25 Suborna F Uttar Goneshpur 1 H - 328 Nuclear 1 1 26 Shopna 24 Kashem Ali 35 Shourav M Uttar Goneshpur 1 H - 278 Joint 2 2 27 Ruby Sharkar 20 Ismail Sarkar 27 Eva F Sutarpara 6 H - 674 Joint 1 1 28 Lolita 40 Ab. Rahman 47 Hadisa F Sutarpara 6 H - 665 Nuclear 7 6 29 Majeda 20 Al Amin 25 Suraiya F Sutarpara 6 H - 640 Nuclear 1 1

60
30 Sharifa 20 Habibur 28 Mim F Sutarpara 6 New Joint 3 2 31 Asma 20 Abul 30 Shojol M Sutarpara 6 H - 585 Nuclear 3 3 32 Shakibun Nahar 21 Roton 27 Shahin M Sutarpara 6 H - 544 Nuclear 2 2 33 Marufa 21 Motiur 35 Mohona F Sutarpara 6 H - 741 Joint 3 1 34 Masuda 20 Joshim uddin 28 Maisa F Uttar Goneshpur 1 H - 539 Nuclear 3 2 35 Ripa 27 Habibur 34 Mim F Uttar Goneshpur 1 H - 419 Nuclear 3 3 36 Sahida 21 Mubarak 25 Shafayatullah M Sutarpara 5 H - 833 Joint 1 1 37 Kitabjan 20 Sobuj 25 Hamim M Sutarpara 5 H - 835 Joint 2 1 38 Jhuma 19 Shah Alam 25 Suchona F Sutarpara 5 H - 858 Joint 1 1 39 Sudina 25 Ansar Ali 35 Imran M Sutarpara 5 H - 847 Nuclear 6 2 40 Asiya Begum 35 Bazlu Mia 50 Sharmin F Uttar Goneshpur 1 H - 284 Nuclear 3 2 41 Rizia Akter 18 Ziaur Rahman 27 Robin M Khakshri 4 H - 219 Nuclear 1 1 42 Salma 25 Qutubuddin 32 Konika F Khakshri 4 H - 214 Nuclear 2 2 43 Sikha Rani 22 Sumon Das 28 Poja Rani F Khakshri 4 H - 174 Joint 1 1 44 Salma 31 Jalal 38 Nafisa F Khakshri 4 H - 129 Joint 5 5 45 Rokeya 26 Belal 40 Jannatul F Sutarpara 5 H - 632 Nuclear 5 5 46 Anjona 20 Fardin 26 Nupur F Chong Noagaon 9 H - 359 Nuclear 2 2 47 Asma 18 Roton Mia 26 Amir Hamja M Chong Noagaon 9 H - 215 Nuclear 2 2 48 Asma 32 Shah Alam 38 Mojahid M Chong Noagaon 9 H - 236 Nuclear 6 5 49 Fatema Akter Honey 21 Quader bhuiyan 28 Anika F Chong Noagaon 9 H - 509 Joint 1 1 50 Salma 21 Bokul 27 Ar Rahman M Sutarpara 5 H - 1029 Nuclear 2 2 51 Bokula 22 Khokon Mia 26 Liya F Sutarpara 5 H - 1027 Nuclear 2 1 52 Noyon 19 Helal 24 Mir Hussain M Sutarpara 5 H - 1031 Nuclear 2 2 53 Salma 20 Renu Mian 26 Tamanna F Sutarpara 5 N/A Joint 1 1 54 Masuma 22 Johurul Islam 27 Eti F Uttar Goneshpur 1 H - 260 Joint 1 2
Shriti F Uttar Goneshpur 1 55 Juena 26 Ujjal 27 Rifat M Uttar Goneshpur 1 H - 292 Nuclear 2 2 56 Hosna 30 Shahjahan 40 Rabbi M Chong Noagaon 9 H - 331 Nuclear 5 4

61
Appendix 6: Information about children (Dehunda Union)
Sl. No. Mother's
name Child's Name Sex
Child Age
(month)
Weight of Child
(KG) MUAC (CM)
Mother's Weight
(KG) Remarks Level of Nutrition
1 Shorufa Hridoy M 22 8.4 13.3 31.1 M.C. Severe 2 Morzina Treesha F 14 9.1 15.0 41.0 W.C. Wel 3 Piana Kaifa F 19 7.8 13.5 41.6 M.C. Severe 4 Ajifa Noyon M 5.5 6.9 15.5 38.7 W.C. Wel 5 Happy Lamia F 24 8.2 14.0 56.9 M.C. Severe 6 Asma Lamia F 16 8.0 13.0 41.4 M.C. Moderate7 Orbula Rashid M 18 6.3 11.0 37.8 M.C. Severe (Twins) Khurshid M 18 5.7 10.8 M.C. Severe 8 Parvina Rabbi M 12 6.2 11.0 44.6 M.C. Severe 9 Halima Rubel M 24 8.4 11.8 40.8 M.C. Severe
10 Rahima Okia F 18 5.2 8.7 34.0 M.C. Severe 11 Shabana Tayeba F 23 10.9 14.3 50.2 W.C. Wel 12 Bedana Rumi F 16 6.9 11.5 39.8 M.C. Severe 13 Halima Rafia F 19 8.4 12.6 47.2 M.C. Moderate14 Kolpona Al-Ismail M 15 7.7 12.5 44.9 M.C. Severe 15 Juena Shakibur M 2 5.4 12.0 39.3 W.C. Wel 16 Salma Sharmin F 18 8.0 12.4 46.3 M.C. Severe 17 Maksuda Sadia F 23 5.8 10.9 37.9 M.C. Severe 18 Asma Rahat M 10 9.2 12.0 43.3 W.C. Wel 19 Bedena Jubayer M 23 7.1 13.5 53.8 M.C. Severe 20 Ambia Tanzina F 5.5 3.1 9 57.7 M.C. Severe 21 Piana Razia F 9 5.4 10.9 50.1 M.C. Severe 22 Halima Mushahid M 12 7.0 13.5 42.6 M.C. Severe 23 Zahura Maruf M 5.5 2.7 9.0 38.7 M.C. Severe 24 Lolita Rafiq M 4 6.0 12.5 45.8 W.C. Wel 25 Haresa Ramzan M 6 6.1 12.8 43.8 M.C. Moderate26 Hawa Raqib M 24 10.3 15.0 41.9 M.C. Mc-mild 27 Asia Ashadul M 2 6.1 14.0 43.8 W.C. Wel 28 Jahanara Mohima F 14 6.6 12.9 48.3 M.C. Severe 29 Ambia Nabila F 14 8.5 14.0 60.5 M.C. Mc-mild 30 Nargis Jannatul F 7 8.2 13.2 47.2 W.C. Wel 31 Rubina Rubima F 5 5.3 12.0 43.7 M.C. Mc-mild 32 Sheuli Aqib M 9 10 14.0 48.5 W.C. Wel 33 Shoma Lamia F 22 11.0 15.0 47.2 W.C. Wel 34 Rupa Maisha F 21 8.9 13.0 48.0 M.C. Moderate35 Sarjahan Ashiqul M 12 5.0 10.0 37.6 M.C. Severe 36 Rekha Sujon M 17 7.4 10.0 41.4 M.C. Severe 37 Jebunnesa Arafat M 12 6.7 11.0 38.8 M.C. Severe 38 Begum Sadia F 6 6.5 13.2 44.0 W.C. Wel 39 Anura Shipu F 5 6.0 12.7 42.3 WC Wel 40 Parvin Rubaiya F 13 8.9 13.5 46.0 WC Wel 41 Parvin Suraiya F 5 4.2 11.8 45.7 MC Severe

62
42 Ruma Rea F 11 6.5 11.0 38.0 MC Severe 43 Amina Meem F 8 4.5 10.6 38.4 MC Severe 44 Zinnata Emon M 11 6.7 11.0 42.4 MC Severe 45 Zulekha Nuha F 9 6.3 10.6 42.6 MC Severe 46 Modina Tofazzol M 14 6.6 10.8 40.3 MC Severe 47 Rahima Reza F 9 8.3 11.0 47.0 WC Wel 48 Nazma Zeesan M 6 5.5 11.0 45.1 MC Severe 49 Zahura Abdullah M 12 6.5 11.4 43.0 MC Severe 50 Morzina Emon M 6 8.1 12.6 41.9 WC Wel 51 Lovely Nuween F 8 5.8 10.4 50.5 MC Moderate52 Hafsa Nazmul M 11 8.8 14.5 48.8 MC Mild 53 Shukia Afsana F 20 7.8 13.5 45.0 MC Severe 54 Aklima Ashamoni F 11 8.0 13.5 46.6 MC Mild 55 Angura Taiba F 4 5.2 10.6 50.6 MC Mild 56 Begum Shamim M 12 8.4 13.0 43.0 MC Mild 57 Sabina Jakia F 12 8.8 12.8 40.7 W.C. Wel 58 Mina Mustakim M 24 8.3 11.7 38.9 MC Severe 59 Shoma Mim F 10 7.2 11.5 59.7 MC Mild
Note on remarks & nutrition level columns: Severe or M.C. = Severely Malnourished Child, Wel or W.C = Well nourished Child, Moderate = Moderately Malnourished Child, Mild = Mildly Malnourished Child

63
Appendix 7: Information about children (Sutarpara Union)
Sl. No. Mother's name Child's Name Sex Child Age (month)
Weight of Child (KG)
MUAC (CM)
Mother's weight Remarks
Level of Nutrition
1 Saleha Lailu F 15 7.8 11.5 40.3 MC Moderate2 Masuda Mahin M 23 7.0 12.5 40.4 MC Severe3 Asma Noman M 2 4.7 47.6 WC Wel 4 Sharaswati Barman Tisa moni F 15 7.3 12.3 38.4 MC Severe5 Hena Ahsanullah M 19 8.1 12.0 41.6 MC Severe6 Raj Bahar Tamim M 13 4.5 12.5 30.4 MC Severe7 Asma Begum Wasim M 5 6.6 13.4 42 WC Wel 8 Anwara Zihad M 3 3.8 12.6 41.8 MC Moderate9 Fatema Shofiqul Islam M 24 9.0 14.0 35.5 MC Severe10 Rekha Akhter Tahmina Shanta F 12 6.0 13.4 41.4 MC Severe11 Joshna Sonia F 8 5.7 11.9 34.5 MC Severe12 Sahana Khatun Ratul M 5 4.8 13.2 38.9 MC Severe13 Rupa Enayetullah M 24 8.6 15.2 35.2 MC Severe14 Rehana Kohinoor F 6 3.4 10.0 35.6 MC Severe15 Zulekha Zihad M 18 8.2 14.0 41.5 MC Severe16 Eron Sajon M 11 7.2 13.6 34.3 MC Severe17 Mahmuda Sadia F 2 4.5 11.8 46.3 WC Wel 18 Sabina Faisal M 17 8.0 14.2 35.1 MC Severe
19 Shakina Munna Hussain M 14 6.2 14.0 41.6 MC Severe
Munir Hussain M 14 6.1 14.0 MC Severe20 Rozina Motahar Hussain M 17 9.2 13.2 48.5 MC Moderate21 Ruma Ramin M 9 8.6 14.0 46.3 WC Wel 22 Nadira Nadir Mian M 16 8.6 14.6 41.4 MC Moderate23 Sheuli Eva F 2.5 2.0 8.8 37.1 MC Severe
Shimanto M 2.5 2.4 9.0 MC Severe24 Rotna Rafi M 8 8.0 15.2 71.5 WC Wel 25 Sathi Suborna F 14 9.1 15.0 45 WC Wel 26 Shopna Shourav M 2.5 6.0 49 WC Wel 27 Ruby Sharkar Eva F 19 11.5 16.4 47.1 WC Wel 28 Lolita Hadisa F 18 6.7 13.8 38.8 MC Severe29 Majeda Suraiya F 18 8.0 15.6 43.2 MC Severe30 Sharifa Mim F 11 8.9 14.2 42.2 WC Wel 31 Asma Shojol M 12 7.3 13.2 33.1 MC Severe32 Shakibun Nahar Shahin M 7 7.8 15.6 37.5 WC Wel 33 Marufa Mohona F 4 6.8 14.2 48.1 WC Wel 34 Masuda Maisa F 6 6.5 13.6 39.6 WC Wel 35 Ripa Mim F 8 5.1 12.0 65.4 MC Severe36 Sahida Shafayatullah M 4 6.2 15.0 43.7 WC Wel 37 Kitabjan Hamim M 5 4.1 41.2 MC Severe38 Jhuma Suchona F 8 7.9 14.4 47 WC Wel 39 Sudina Imran M 6 5.0 12.6 41.1 MC Severe40 Asiya Begum Sharmin F 13 6.6 134 38.9 MC Severe41 Rizia Akter Robin M 12 9.2 142 50 MC Mild

64
42 Salma Konika F 18 10.1 52.1 WC Wel 43 Sikha Rani Poja Rani F 7 3.5 102 40.8 MC Severe44 Salma Nafisa F 18 7.7 50.4 MC Severe45 Rokeya Jannatul F 6 5.2 110 44.9 MC Moderate46 Anjona Nupur F 6 6.3 134 39.4 MC Mild 47 Asma Amir Hamja M 13 6.9 124 30.4 MC Severe48 Asma Mojahid M 16 7 116 40.2 MC Severe49 Fatema Akter Anika F 11 7.6 128 43.9 MC Mild 50 Salma AR Rahman M 16 8.4 138 40.1 MC Severe51 Bokula Liya F 9 6.5 124 39.2 MC Moderate52 Noyon Mir Hussain M 7 7.4 134 49.1 WC Wel 53 Salma Tamanna F 18 8.6 136 52 MC Severe54 Masuma Eti F 13 6.7 52.3 MC Severe
Shriti F 6 MC Severe55 Juena Rifat M 16 8.2 40.5 MC Severe56 Hosna Rabbi M 20 8.8 134 55.7 MC Moderate
Note on remarks & nutrition level columns: Severe or M.C. = Severely Malnourished Child, Wel or W.C = Well nourished Child, Moderate = Moderately Malnourished Child, Mild = Mildly Malnourished Child


















