Food allergy in children
22
Food allergy in children Hugo Van Bever Department of Pediatrics National University Singapore APAPARI Workshop, Hanoi, May 200
description
Food allergy in children. Hugo Van Bever Department of Pediatrics National University Singapore. APAPARI Workshop, Hanoi, May 2008. Food Allergy… Fact or Fiction?. 1. Difficult problem group of diseases - PowerPoint PPT Presentation
Transcript of Food allergy in children

Food allergy in children
Hugo Van BeverDepartment of Pediatrics
National University Singapore
APAPARI Workshop, Hanoi, May 2008

Food Allergy…Fact or Fiction?
1. Difficult problem group of diseases
2. Lot of non-scientific data … opinions… truths… tradition… stories.
3. Food other types of reaction (intolerance, intoxication, etc…)
4. Too many children are labeled as being “food-allergic”

Food allergy = an immunologically-mediated reaction
against food 1. IgE-mediated 2. Cell-mediated reactions (T lymphocytes - delayed onset) 3. Mixed types (atopic dermatitis)
4. Other mechanisms ( unknown - CIC – complement – etc…)

Prevalence of food allergy
1. General population: 2 % 2. Young children (< 3 yrs): 8 % 3. Singapore children: 4 – 5 %
SPECIFIC GROUPS
4. Young children with severe eczema: 90 % 5. Children with asthma: < 10 %

Manifestations of food allergy
1. SKIN: urticaria – angioedema > eczema 2. RESPIRATORY: rhinitis – asthma 3. GI TRACT: diarrhea – vomiting – FTT - eosinophilic gastroenteritis - enterocolitis 4. GENERAL: anaphylactic shock 5. OTHER: migraine, hyperactivity, sleep disturbances etc… ?

Foods triggering anaphylaxis in Singaporean children (1992 – 1996)
124 children with acute anaphylaxis at NUH mean age (yrs) 1. Egg and milk 11 % 0.7 2. Bird’s nest 27 % 4.5 3. Chinese herbs 7 % 5.0 4. Crustacean seafood 24 % 11.0 5. Others * 30 % 7.0
* Chicken, duck, ham, fruits (banana, rambutan), cereals, gelatin and spices
Goh et al. Allergy 54, 1999, 78-92.

Every food has its own story…
cow’s milkhen’s eggpeanuts, fish, seafood, …
prevalence
age3 yrs 5 yrs6 months

SensitizationSensitization to food… to food…
sensitization to allergens…sensitization to allergens…
1. prenatal sensitization
2. postnatal sensitization

Sensitization to food…
eating, touching and
smelling…
peanutsfishhen's egg

Allergy to cow’s milk proteins in mother’s milk or in hydrolyzed cow’s milk infant
formulas assessed by intestinal permeability measurements.
ovalbuminovalbuminpeanut proteinpeanut protein
cow’s milk proteincow’s milk protein
mother’s milkmother’s milk

Prenatal sensitization to allergens…does it exist?
1. clinical evidence (peanuts – ovalbumine – pollen – house dust mite – cat - dog)
2. allergens in amniotic fluid & cord blood
3. active transport through placenta

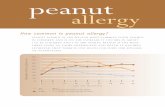
Exposure to peanuts in utero and in infancy and the development of sensitization to peanut allergens in young children.
Frank L, Marian A, Visser M, Weinberg E, Potter PC. Pediatr Allergy Immunol 1999, 10, 27-32.
… mothers who consumed peanuts more than once a week during pregnancy were more likely to have a peanut-allergic child than mothers who consumed peanuts less than once a week (odds ratio=3.97, 98% confidence interval 0.73-24).

Allergic sensitization during pregnancy influences the offspring’s immune reactions. A study in a mouse model
(H. Renz, 1999).
study group
control group
Ovalbumin challenge (every second day)
decreased INF-
( x 8 – 9 )
PREGNANCY BIRTH

Direct evidence for transplacental allergen Direct evidence for transplacental allergen transfer.transfer.
Szépfalusi et al. Pediatr Res 2000, 48, 404-7. Szépfalusi et al. Pediatr Res 2000, 48, 404-7.
maternal side fetal side
BLG 8 8
Bet v1 10 2
Human IgG = increase
= Ig receptor involvement

Diagnosis of food allergy
1. IgE-mediated food allergy - SPT – IgE
2. Non-IgE-mediated food allergy- patch test- in vitro: LTT (cytokine profile?)
GOLDEN STANDARD = DBPCFC
research …

Utility of food-specific IgE concentrations in predicting symptomatic food allergy. Hugh A. Sampson. JACI 2001,
107, 891.
Diagnostic decision points of 95%
- cow’s milk 15 kU/L - egg 7 kU/L - peanut 14 kU/L - fish 20 kU/L
n = 100, mean age = 3.8 yrs

Future immunomodulatory therapies for food allergy
1. Humanized monoclonal anti-IgE 2. Mutated allergen protein immunotherapy 3. Peptide immunotherapy 4. Immuno-stimulatory sequences 5. Probiotics (?) no effect on allergic reactions

Alternative feedings in case of CMA
1. Breast milk 2. Soy formulas (?) 3. Goat formulas (?) 4. Hypoallergenic formulas ( partial hydrolysate formulas) 5. Amino acid-based formulas (complete hydrolysate formulas

Primary prevention of atopy: food allergen avoidance
-- BREAST FEEDINGSaarinen AM, Kajosaari M. Breastfeeding as prophylaxis
against atopic disease: prospective follow-up study until 17 years old. Lancet 1995; 346: 1065 - 1069.
-- HYPO-ALLERGENIC MILKVandenplas Y et al. The long-term effect of a partial whey hydrolysate formula on the prophylaxis of atopic disease.
Eur J Pediatr 1995; 154: 488 - 494.

The long-term effect of a partial whey hydrolysate formula on the prophylaxis of atopic disease.
Vandenplas et al. Eur J Ped 1995, 154, 488.
prevalence of CMP sensitivity

Conclusion: Food Allergy…Fact or Fiction?
… a lot of non-scientific data … opinions… truths… tradition…
stories … etc …
scientific data
… A fact… surrounded with lot’s of fiction

Conclusion…
Still … breast is best
…but… impossible to study
… no contra-indications…