Bioanalytical methods for food allergy diagnosis, allergen detection ...

Food Allergy – Diagnosis, Management & Considerations for College Campuses
S. Shahzad Mustafa, MD, FAAAAI

Disclosures Speaker’s bureau Genentech, Teva
Consultant Genentech, Teva

Outline Definitions Diagnosis Management Considerations for college campuses

James Daly - Author
“You cannot be distracted by the noise of misinformation.”

Definition of a Food Allergy “An adverse health effect arising from a specific immune
response that occurs reproducibly on exposure to a specific food.”
Boyce. JACI 2010; 126: 1105.

Allergy Versus Intolerance
Allergy IntoleranceRequires sensitization Can occur in absence of sensitization
Validated diagnostic testing Minimal validated diagnostic testing
Reproducible reactions Reactions can occur inconsistently
Dose independent Frequently dose dependent
Caused by an individual allergen Can be caused by a class effect
Cannot block with pre-treatment Validated pre-treatment regimens
Desensitization protocols Desensitization not possible
Can lead to death Typically very little mortality

Prevalence Food allergy affects 3-6% of children and ~3% of adults in
the United States Self reported prevalence ranges from 20-35% Over-diagnosis by physicians as high as 80%
Rona. JACI 2007; 120: 638.

Over-Diagnosis of Food Allergy
Fleischer. J Peds 2011; 158(4): 578.

Quality of Life Associated with Food Allergy 70% reported significant effects on social events 60% reported significant effects on meal preparation 40% reported a significant increase in overall stress levels 34% reported an effect on school attendance 10% chose to home school their children
Bollinger. Ann All Asthma Imunol 2006. 96: 415. Springston. Ann All Asthma Immunol 2010. 105: 287.

Diagnosis
Oral FoodChallenge

Diagnosis - History Common complaints NOT
suggestive of an IgE mediated mechanism Isolated rhinitis Isolated cough/asthma Chronic abdominal discomfort Isolated reflux/heartburn Chronic urticaria Fatigue Reactions occur inconsistently Reactions occur only with
larger doses Ongoing mild to moderate
atopic dermatitis/eczema

Food Allergy & Atopic Dermatitis
Boyce. JACI 2010; 126: 1105.

Common Food Allergens
Pediatrics AdultsFood %
Cow’s milk 2.5
Egg white 1.5
Peanut 1.0
Tree nuts 0.5
Wheat 0.4
Soy 0.4
Shellfish 0.1
Finned fish 0.1
Sesame 0.1*
Food %
Peanut 0.6
Tree nuts 0.6
Shellfish 2.0
Finned fish 0.4
Sesame 0.1*
Boyce. JACI 2010; 126: 1105.

Diagnostic Tools Skin prick testing and specific IgE testing (RAST,
ImmunoCAP, etc) indicate the presence of IgE antibody Skin prick testing and specific IgE testing do NOT prove
clinical reactivity Food allergy requires the presence of IgE antibody AND
clinical reactivity Upwards of 50-60% of individuals have presence of IgE in
the absence of clinical reactivity
Celik-Bilgli. Clin Exp All 2005; 35(3): 268.

Skin Prick Testing
A negative skin test makes allergy very unlikely Less than 5%
The likelihood of a true allergy increases with the size of the reactions > 8 mm wheal = > 95% likelihood of allergy
Sampson. JACI 2001; 107: 891., Image from WebMD.com,

Specific IgE Testing
Sampson. JACI 2001; 107: 891.

Unproven Diagnostic Testing Intradermal skin testing Atopy patch testing Food IgG or IgG4
Basophil activation testing Lymphocyte stimulation testing Applied kinesiology Hair analysis Electrodermal testing Cytotoxic tests Ordering food panels of specific IgE testing is not
recommended

Diagnosis
Oral FoodChallenge

Oral Food Challenges• Performed to confirm or refute IgE mediated food allergy
or to evaluate resolution of IgE mediated food allergy Skin prick tests commonly remains reactive despite resolution
of allergy
Van Der Velde. JACI 2012; 130(5): 1136.

Safety of Oral Food Challenges Jaffe Food Allergy Institute, 2008-2010 Patients aged 8 months – 21 years of age
Lieberman J. JACI 2011; 128(5); 1120.
Total Challenges 701
Failed challenges 132 (18.8%)
Reactions limited to skin symptoms 75 (10.7%)
Reactions requiring epinephrine 12 (1.7%)
Reactions requiring 2+ doses of epinephrine 1 (0.14%)
Reactions requiring treatment in ED 1 (0.14%)

Food Pollen Syndrome Presents with oropharyngeal itching and discomfort
typically with fresh fruits and vegetables in individuals allergic to environmental allergens

Food Pollen Syndrome Mechanism is local IgE production Minimal if any risk of anaphylaxis
Clinical diagnosis Management Avoid culprit food Continue to consume culprit food Pre-treat with antihistamine Cook/heat culprit food Allergen immunotherapy to environmental allergens

Special Considerations Cow’s milk allergy Roughly 70% will tolerate baked milk products Alternatives include soy milk, coconut milk, almond milk, rice
milk Cannot safely consume goat’s milk
Egg allergy Roughly 70% will tolerate baked egg products Safe to administer influenza and MMR vaccines
Shellfish and finned fish allergy Safe to receive contrast for radiographic studies Systemic reactions with airborne exposure have been reported

Special Considerations (cont’d) Soy allergy Safe to consume soy lecithin
Tree nut allergy Nearly all will tolerate coconut No cross reactivity with seeds Reasonable to avoid certain tree nuts but consume others
Peanut allergy 95%+ will tolerate other legumes Nearly all will tolerate highly refined peanut oil Minimal if any risk with airborne exposure

Airborne Peanut Allergen
Participants consumed peanuts to simulate various conditions Cafeteria setting Sporting event Commercial airliner
Participants measured airborne protein via personal air monitors during the eating sessions with room ventilation turned off
Perry. JACI 2004; 113(5): 973.

Rick of Airborne & Contact Exposure to Peanut
Simonte. JACI 2003; 112(1): 180.

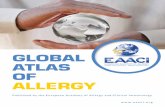
Precautionary Labeling
Hefle. JACI 2007; 120(1): 171.

Precautionary Labeling
Percentage of Products with Detectable Allergen
Hefle. JACI 2007; 120(1): 171.

Food Allergy Guidelines
Boyce. JACI 2010; 126(6): S1.

Mortality Associated with Food Allergy
Umasunthar. Clin Exp All 2013; 43: 1333.

Management Strict food avoidance Ensure nutritional needs are being met Minimize risk of reaction while maintaining adequate
quality of life Be aware of emergency action plan Carry epinephrine at all times Periodically reevaluate for tolerance

Points to Consider Unifying factors in nearly all deaths from food allergy Peanut and/or tree nut allergy Sub-optimally controlled asthma Delayed or no administration of epinephrine
Previous reactions do NOT predict future reactions No diagnostic tools to predict the severity of reactions Adolescents and college-aged students at higher risk of
reactions due to risk-taking behavior

College Survey
Greenhawt. JACI 2009; 124: 323.

Management in School and Higher Education
http://www.cdc.gov, http://www.foodallergy.org

CDC Guidelines
“A positive psychosocial climate – coupled with food allergy education and awareness
for all children, families, and staff members –can help remove feelings of anxiety and alienation
among children with food allergies.”

Communication
Student/Patient
Parents
Campus StaffAllergist
Primary Care Physician

Consensus Best Practices for Campus Collaborative, campus-wide approach Transparent and flexible process capable of meeting
student needs without being burdensome For student and campus staff
Comprehensive food allergy policy Emergency response plan Emergency response training for staff Confidentiality
http://www.foodallergy.org

Pilot Guidelines for Higher Education
http://www.foodallergy.org

Education of School Personnel Research from Houston Independent School District 62 school nurses responsible for ~61,000 students
Compared school data from 2010 and 2012 Intervention: single educational session on food allergy provide
to all personnel in 2011 Results Decreased frequency of reactions Improved availability of epi devices
Epi device/allergic child ratio = 0.185 in 2010, 0.77 in 2012
Conclusion: a single education session for school personnel was highly successful in improving the management of food allergies in the school setting
Houston Independent School District Experience.

Example Policy
Adapted from policy statement at Siena College.

Summary Although food allergies have increased in prevalence, they
are often misdiagnosed, and this has serious implications on quality of life
Management is based on food avoidance and appropriate treatment of accidental reactions with epinephrine
Management must account for unique properties of individual food allergens
Management on campus should be based upon risk assessment, communication, education, and cooperation