Periconceptional daily folic acid (400 µg) supplementation ...
Upload
laura-evansCategory
view
212download
0
www.whijournal.comWomen’s Health Issues 20 (2010) 50–57
FOLIC ACID SUPPLEMENTATION IN YOUNGER AND OLDERNONPREGNANT WOMEN OF REPRODUCTIVE AGE
Findings from the Central Pennsylvania Women’s Health Study(CePAWHS)
Laura Evans* and Carol S. Weisman, PhD
Department of Public Health Sciences, The Pennsylvania State University, College of Medicine, Hershey, Pennsylvania
Received 18 April 2009; revised 14 September 2009; accepted 23 October 2009
Introduction and Background. This study explores variables associated with daily folic acid
Funded, inPennsylvania Ddisclaims respoconclusions.
* Correspondcine, 600 Centerv
E-mail: levan
Copyright � 201Published by Els
supplementation among nonpregnant women ages 18–24, in comparison with women ages25–45. Health-related behaviors, reproductive status, health care access, and sociodemographicvariables are included.
Methods. Data are from a cross-sectional population-based survey of 2,002 women ages 18–45
in the Central Pennsylvania Women’s Health Study. The analytic sample included 246 womenages 18–24 and 1,636 women ages 25–45 who were not pregnant at the time of survey.
Results. Seventeen percent of women ages 18–24 and 27% of women ages 24–45 used daily folicacid supplements. In multiple logistic regression analysis, folic acid use was significantly
associated with only two variables among younger women: fruit consumption at least dailyand regular physical activity levels meeting recommended guidelines. Among older women,folic acid use was associated with these same two health-related behaviors in addition to notsmoking, seeing an obstetrician-gynecologist, receiving diet/nutrition counseling, being
married or living with a partner, and no prior pregnancy. Folic acid use was not associatedwith pregnancy intention in either age group.
Conclusions and Discussion. Women ages 18–24 have significantly lower rates of folic acidsupplementation compared with older women of reproductive age, but fewer variables are
associated with folic acid use among younger women. Missed opportunities to educateyounger women about the benefits of folic acid supplementation are identified.
Introduction
Despite efforts over the years to encourage womenof reproductive age to use folic acid supplements
to prevent birth defects, research shows that supple-mentation is still underutilized by nonpregnantwomen. According to the Centers for Disease Controland Prevention (CDC), all women capable of becomingpregnant should receive 400 mcg of folic acid daily to
part, under grant number 4100020719 with theepartment of Health. The department specificallynsibility for any analyses, interpretations, or
ence to: Laura Evans, Penn State College of Medi-iew Drive, A210, Hershey, PA 17033.
0 by the Jacobs Institute of Women’s Health.evier Inc.
reduce the incidence of neural tube defects (CDC,1992). However, even after the mandated fortificationof food products in 1998, it has been estimated thatwomen consuming a healthy, balanced diet may onlyreceive 25% of the recommended daily amount of folicacid through food alone (Werler, Louik, & Mitchell,1999), and fewer than 10% of all women receive the rec-ommended amount of daily folic acid through theirchosen diet (Yang et al., 2007).
Although there has been a general increase in recentyears in the rate of folic acid supplementation bywomen of all ages, there is still low overall awarenessand usage in younger age groups. According to a recentstudy of nonpregnant women conducted by the Marchof Dimes Foundation and reported by the CDC, 18- to24-year-olds have not only the lowest reported daily
1049-3867/10 $-See front matter.doi:10.1016/j.whi.2009.10.001

L. Evans and C. S. Weisman / Women’s Health Issues 20 (2010) 50–57 51
folic acid use (30% vs. 47% of women ages 25–34 and40% of women ages 35–45), but the younger womenalso have the least amount of knowledge regardingthe importance of supplementation (CDC, 2007).Hilton (2007) found that even women in this youngage group who are seeking a higher level of educationat colleges and universities are unaware of the impor-tance of folic acid, and are therefore not using adequateamounts. Because women aged 18–24 have the highestrate of unplanned pregnancies (Finer & Henshaw,2006), they should be encouraged to use daily folicacid supplements regardless of their pregnancy intent.
Although the CDC’s report calls attention to theneed for increasing awareness in younger women ofchildbearing age, it does not address possible reasonswhy women aged 18–24 are less likely not only touse folic acid, but also to have any knowledge regard-ing the health benefits of folic acid supplementation.Little is known about what motivates young womento become informed about folic acid or to use folicacid supplementation. Because use of a daily multivi-tamin with folic acid is an example of a health-promoting behavior, it seems logical that youngwomen who engage in other healthy behaviors (suchas eating healthy foods, exercising, and not smoking)would be more likely than other women to use folicacid supplements. Similarly, it is likely that youngwomen who come in contact with the health care sys-tem (e.g., for routine or reproductive-related healthcare) would be more likely than other women to be in-formed about folic acid and to use supplements. Fi-nally, young women with higher socioeconomicstatus could be more likely to be better informed abouthealth and health care in general, and possibly morelikely to use folic acid supplements as well.
The present study sought to identify specific repro-ductive, behavioral, health care access, and sociodemo-graphic characteristics that are related to folic acid usein nonpregnant women ages 18–24, compared witholder women of reproductive age (ages 25–45). Al-though some studies have shown maternal education,ethnicity, wantedness of the pregnancy, income, andaccess to prenatal counseling as predictors of folicacid usage (De Jong-van den Berg, Hernandez-Diaz,Werler, Louik, & Mitchell, 2005), none have focusedspecifically on this younger age group.
Methods
SampleThe data are from the Central Pennsylvania Women’sHealth Study, which included a population-based sur-vey of reproductive-age women residing in a 28-county region in central Pennsylvania. The purposeof the survey was to estimate the prevalence of multi-ple risk factors for adverse pregnancy outcomes andidentify the subpopulations at greatest risk. Details of
the study methods have been previously published(Weisman et al., 2006). The study was reviewed andapproved by the Institutional Review Board of thePenn State College of Medicine and a Certificate ofConfidentiality from the National Institutes of Health(CC-HD-04024) was obtained.
A random-digit dial telephone survey of 2,002women was conducted between September 2004 andMarch 2005. Inclusion criteria were female gender,age 18–45 years, residence in the 28-county target re-gion, and English or Spanish speaking. Participantsneeding a proxy or translator to respond to the surveywere excluded. The telephone interview lasted ap-proximately 30 minutes and included questions abouthealth status, pregnancy, health behaviors, stress andexposures, health care access, and sociodemographics.A prenotification letter was sent to sampled house-holds with a small incentive ($2) to encourage partici-pation. The overall response rate calculated using anestimated proportion eligible among households ofunknown eligibility (AAPOR Response Rate 4) was52%, and the cooperation rate among eligible womencontacted was 63%, yielding a sample that was highlyrepresentative of reproductive-age women in centralPennsylvania with regard to age, educational level,race/ethnicity, and poverty (Weisman et al., 2006).
The analytic sample for this study only includedwomen from the Central Pennsylvania Women’sHealth Study sample who met the following criteria:a) provided an age at the time of the survey and/orprovided a birth date and b) were currently nonpreg-nant. This yielded a total sample size of 1,912 women.
Dependent variableThe dependent variable is use of a daily multivitamincontaining folic acid. This variable was measured us-ing two questions: a) ‘‘In the past month how oftenhave you taken a multivitamin: Never, once or twicea week, three or four times a week, five or six timesa week, or every day?’’ and b) ‘‘Does your multivitamincontain folic acid?’’ Women who were unsure if theirmultivitamin contained folic acid were asked to checkthe bottle. One fourth of the sample (n ¼ 489) reportedusing a daily multivitamin that contained folic acid.Although women who take a daily multivitamin arelikely receiving the proper amount of folic acid (mostmultivitamins contain 400 mcg of folic acid), if thewoman was unsure if her daily multivitamin con-tained folic acid, she was coded as a nonuser. In doingso, we conservatively measured folic acid use by defin-ing as nonusers those women who may be ingestingadequate folic acid without their knowledge.
Independent variablesIndependent variables were chosen on the basis oftheir hypothesized relationship to folic acid supple-mentation.

L. Evans and C. S. Weisman / Women’s Health Issues 20 (2010) 50–5752
Reproductive status. Measures of reproductive status in-clude prior pregnancy and whether the woman wasconsidering a pregnancy within the next year. Both ofthese variables were hypothesized to increase the like-lihood of folic acid supplementation because thesewomen would be expected to be more knowledgeableabout folic acid and more motivated to use it. Preg-nancy intendedness within the next year was mea-sured by asking participants: ‘‘Are you consideringbecoming pregnant within the next year, at some othertime in the future, or not at all?’’ Participants could re-spond with any of these provided answers or ‘‘unde-cided.’’ The pregnancy intent variable was thendichotomized into women who were planning on hav-ing a pregnancy within the next year (5.8%) versus allother responses. Women who answered ‘‘undecided’’were grouped into the not-intending category, becausetheir folic acid supplementation habits could not bedue to an intended pregnancy within the next year.Women who reported themselves to be infertile (byhysterectomy, tubal ligation, or other reason) werealso categorized as not considering pregnancy, for thesame reason.
Health-related behaviors. Measures of health-related be-haviors include nutritional intake (fruit, vegetable,and salad consumption), avoiding binge drinking,not smoking, and physical activity level. Healthy be-haviors were hypothesized to be associated with folicacid supplementation, which is also a healthy behav-ior. The measures of nutritional intake were: a) ‘‘Notcounting juice, how often do you eat fruit in a typicalweek?’’ b) ‘‘Not counting carrots, potatoes, or salad,how many times do you eat vegetables in a typicalweek?’’ and c) ‘‘How often do you eat green salad ina typical week?’’ Possible answers were: never, onceor twice a week, three or four times a week, five orsix times a week, once a day, or more than oncea day. Fruit and vegetable intake was categorized asat least daily consumption versus any consumptionthat was less than daily; salad consumption wascategorized as five times a week or more versus anyconsumption less than five times a week. One thirdof women reported consuming fruit at least daily,43% reported consuming vegetables at least daily,and 24% reported consuming green salad at least fivetimes a week.
Binge drinking was measured based on the question:‘‘Considering all types of alcoholic beverages, howmany times during the past month did you have fiveor more drinks on one occasion?’’ One drink was de-fined as 1 can or bottle of beer, 1 glass of wine, 1 canor bottle of wine cooler, 1 cocktail, or 1 shot of liquor.Binge drinkers were defined as those women whohad consumed five or more drinks on one or more oc-casion within the past month (14%). For analysis, bingedrinking was reverse-coded so that avoiding binge
drinking is the variable hypothesized to be associatedwith daily folic acid supplementation.
Smoking was measured with the question: ‘‘Do younow smoke cigarettes every day, some days, or not atall?’’ Women who responded that they currentlysmoke in any quantity (25%) were contrasted withthose who do not smoke. For analysis, not smokingcigarettes was defined as the healthy behavior.
Physical activity level was assessed by asking theparticipants: ‘‘How many days per week do you usu-ally get 30 minutes or more of moderate or strenuousexercise?’’ ‘Moderate’ was defined as physical activitythat was not exhausting, like bowling, golf, walking oryoga; ‘strenuous’ was defined as running, swimming,racquet sports, weight training, or any other activitythat makes the heart beat rapidly. Physical activitylevel was then categorized so as to contrast respon-dents who reported participating in moderate or stren-uous physical activity on at least 4 days per week (25%)versus those who did not exercise at all or did so fewerthan 4 days per week. Physical activity for 30 minutesor more on most days per week was consistent withhealthy lifestyle guidelines at the time of the survey(American College of Sports Medicine, 2000).
Illegal drug use was not included in the analysesbecause too few women reported use of illegal drugs.
Access to health care. Two variables measured women’saccess to health care: a) whether or not the womensee an obstetrician-gynecologist (OB-GYN) and b)whether or not the women had received counselingabout diet and/or nutrition during the past year. Tomeasure OB-GYN use, women were asked: ‘‘Do yousee an OB-GYN for any female-related health care?’’Seeing an OB-GYN was hypothesized to be associatedwith folic acid use because OB-GYNs are the mostlikely health professionals to counsel women aboutpreparing for pregnancy. The women were asked: ‘‘Inthe past 12 months, has a doctor or other health profes-sional asked you or talked to you about diet or nutri-tion?’’ Thirty-seven percent reported talking toa health care provider about this topic in the past12 months. We hypothesized that receiving any coun-seling about diet and nutrition might be associatedwith folic acid supplementation, particularly becausemultivitamins are important in a balanced diet forwomen of reproductive age.
Health insurance status, a common indicator ofaccess to health care, was not included in analyses be-cause folic acid is available over the counter and accesswould not depend on having health insurance.
Sociodemographics. Age was dichotomized to contrastthe two subgroups of interest in this study: 18- to24-year-olds (14%) versus 25- to 45-year-olds (86%).Educational level was measured as a dichotomous var-iable that contrasted women who completed high

L. Evans and C. S. Weisman / Women’s Health Issues 20 (2010) 50–57 53
school or less (41%) versus those who completed somecollege or more (59%). Higher educational level washypothesized to be associated with greater awarenessof folic acid and therefore greater use. Marital statuswas measured as a dichotomous variable contrastingwomen who were married or living with a partner(77%) versus not married or partnered (23%). Beingmarried or living with a partner was hypothesized tobe associated with folic acid supplementation becausewomen in current partnerships might be more likely tobe focused on childbearing.
Location of residence was measured using zip code-based Rural–Urban Commuting Area (RUCA) codes(Hall, Kaufman and Ricketts, 2006; Hart, Larson, &Lishner, 2005). We dichotomized the RUCA codes tocontrast rural versus urban living women. We hypoth-esized that women who lived in an urban area wouldbe more likely to use daily folic acid supplements ow-ing to their greater access to health care providers andinformation regarding its importance.
Other sociodemographic variables considered foranalysis were employment status, race/ethnicity, andpoverty level. Employment status was omitted be-cause it was determined to be an inaccurate measure-ment of potential employment in the younger cohortof women, because many were full-time students. Sim-ilarly, poverty status was omitted because women inthe youngest age group were least likely to report theirhousehold incomes. Race/ethnicity was omitted be-cause the sample of women who were both non-Whiteand using daily folic acid was too small for accurateanalysis.
Data analysisChi-square analysis was used to examine bivariateassociations between age category and all study vari-ables, as well as between folic acid supplementationand all study variables. Because the dependent vari-able (daily folic acid supplementation) is dichotomous,multiple logistic regression was used to examine thepredictors of folic acid use in a multivariable frame-work. The multiple logistic regression was preformedon the entire sample of nonpregnant women and onage-stratified subgroups. In these analyses, the ad-justed odds ratio indicates the odds that a woman in-cluded in the category for the given independentvariable uses a daily multivitamin containing folicacid, and the effect of all other independent variablesis held constant. A significance level of p , .05 isused in all analyses. SPSS 16.0.1 (SPSS, Inc., Chicago,IL) was used for data analysis.
Results
Table 1 shows the frequencies of all study variables inthe total analytic sample and by age subgroup; thetable also shows which variables differ significantly
between age groups. Use of daily folic acid supplemen-tation is significantly lower among 18- to 24-year-olds(16.7%) than among 25- to 45-year-olds (27.1%). Addi-tionally, the older women were significantly morelikely to have had a prior pregnancy and to consumevegetables daily, and they were less likely to bingedrink and smoke. With regard to sociodemographics,older women were significantly more likely to havecompleted some college or higher education, morelikely to be married or living with a partner, and lesslikely to reside in an urban area, compared withyounger women.
Table 2 displays bivariate associations between theindependent variables and daily folic acid supplemen-tation, stratified by age group. Among women ages 18–24, those who consumed fruit daily and who partici-pated in moderate or strenuous physical activity atleast 4 days per week were significantly more likelyto supplement with daily folic acid than those whodid not participate in these healthy behaviors. Similarto the younger age group, women ages 25–45 were sig-nificantly more likely to supplement with daily folicacid if they consumed fruit daily or if they participatedin physical activity at least four days per week. Unlikefor younger women, not having had a prior pregnancy,pregnancy intent within the next year, salad consump-tion at least five times a week, daily vegetableconsumption, not smoking regularly, visiting an OB-GYN, talking to a physician about diet/nutrition, com-pletion of college or more higher education, and beingmarried or living with a partner were significantly as-sociated with daily folic acid consumption in the 25- to45-year-old group.
Table 3 shows the results of the multiple logistic re-gression analysis for the full sample. Age is significant,with older women (25–45) nearly twice as likely to usefolic acid supplements, controlling for other variables.Additional significant indicators of folic acid use in theentire sample include having had no prior pregnancy,daily fruit consumption, not smoking, physical activityat least 4 days per week, visiting an OB-GYN, speakingwith a doctor about diet/nutrition within the past year,being married or living with a partner and residing ina nonurban area.
Table 4 shows the results of multiple logistic regres-sion analyses, stratified by age group. Consistent withthe bivariate results, for women ages 18–24, the onlysignificant predictors of folic acid supplementationare two health behaviors: daily fruit consumptionand moderate or strenuous physical activity at least4 days per week. Women age 18–24 who consumedfruit daily were 2.7 times more likely to supplementwith daily folic acid, whereas women who participatedin physical activity were 2.2 times more likely to takedaily supplements. For women ages 25–45, seven vari-ables significantly predict folic acid supplementation:having a prior pregnancy reduces the odds of folic

Table 1. Study Variables by Age Group
Total Sample(n ¼ 1,912)
18- to 24-Year-Olds(n ¼ 276)
25- to 45-Year-Olds(n ¼ 1,636) p-Value*
Dependent variableDaily folic acid supplementation 25.6% 16.7% 27.1% .000**
Reproductive statusPrior pregnancy 76.6% 35.5% 83.6% .000**Pregnancy intent within the next year 5.8% 7.2% 5.6% .333
Health-related behaviorsDaily fruit consumption 33.1% 31.2% 33.4% .505Salad consumption �5 times a week 24.0% 23.6% 24.0% .950Daily vegetable consumption 43.0% 37.0% 44.0% .034**Binge drinking 14.4% 24.6% 12.7% .000**Smoking 25.6% 31.9% 24.5% .012**Physical activity 24.9% 26.4% 24.7% .584
Access to health careVisits an obstetrician-gynecologist 70.1% 65.5% 70.8% .090Spoken with a doctor about diet/nutrition 36.7% 40.9% 36.0% .132
SociodemographicsCompleted some college or morey 59.4% 48.6% 61.2% .000**Married or living with a partner 77.0% 41.7% 82.8% .000**Urban area 61.3% 69.2% 60.0% .005**
* Based on c2 tests of associations for comparisons between age groups.** p , .05.y The group of 18- to 24-year olds includes women not yet in college.
L. Evans and C. S. Weisman / Women’s Health Issues 20 (2010) 50–5754
acid use, and daily fruit consumption, not smoking,higher physical activity level, seeing an OB-GYN,receiving diet/nutrition counseling in the past12 months, and being married or partnered increasethe odds of folic acid use.
Discussion
These findings confirm prior research showing thatwomen ages 18–24 are less likely than older womenof reproductive age to use daily folic acid supplements,despite the well-documented health benefits such sup-plementation can have for both the woman and anychildren she conceives. Levels of folic acid use in thisstudy are lower than those found in previous research,including the recent report by the CDC (2007). Thiscould be because of our more restrictive measure offolic acid use, as described earlier, but may also reflectlower levels of folic acid supplementation in CentralPennsylvania. An objective of Healthy People 2010 isthat 80% of nonpregnant women meet the guidelinesfor adequate daily folic acid consumption by 2010(U.S. Department of Health and Human Services,2000); currently, the number of women receivingenough folic acid is still much lower than desired.
We were particularly interested in contributing tounderstanding of the use of folic acid supplementsamong women ages 18–24. Of all of the predictorsexamined, only daily fruit consumption and physicalactivity at least 4 days per week predicted folic aciduse in women ages 18–24. It is possible that these twohealthy behaviors are markers for overall healthylifestyle in this younger age group, and that young
women who engage in these behaviors may also main-tain health through multivitamin use. It is particularlynoteworthy that considering becoming pregnant in thenext year and receiving diet/nutrition counseling froma health professional—both of which were more likelyamong younger women than older women in our sam-ple—failed to predict folic acid use by youngerwomen. This suggests that preconceptional healthservices may be failing younger women.
In older women (ages 25–45), prior pregnancy, threehealth-related behaviors, namely, seeing an OB-GYN,receiving diet/nutrition counseling, and marital statuspredicted folic acid use. All predictors operated in theexpected direction except for prior pregnancy: havinghad a prior pregnancy reduced, rather than increased,the odds of folic acid use in older women. Althoughthis finding seems counterintuitive, it is possible olderwomen, particularly those who have ended childbear-ing, are no longer basing their health-related decisionson their potential to become pregnant. Nonetheless,our conceptual framework for understanding folicacid use was more successful in predicting supplemen-tation by older women than by younger women.
The main limitation of our study was the relativelysmall sample size of women ages 18–24. Variables thatwe were forced to omit from the multivariate analysisowing to the small sample size in the younger age groupmay have provided more insight into behaviors andcharacteristics that are associated with folic acid use.
Daily folic acid intake is important in all women ofchildbearing age because it is most effective at prevent-ing negative outcomes in the early stages of pregnancy;neural tube defects occur within the first 21 days after
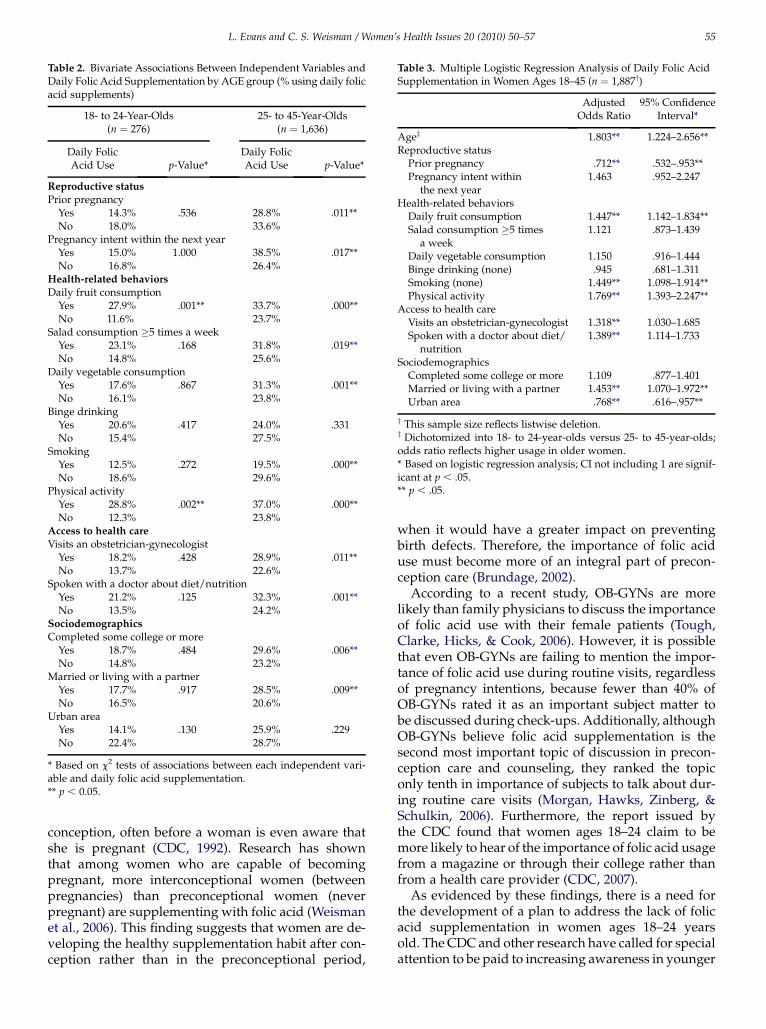
Table 2. Bivariate Associations Between Independent Variables andDaily Folic Acid Supplementation by AGE group (% using daily folicacid supplements)
18- to 24-Year-Olds(n ¼ 276)
25- to 45-Year-Olds(n ¼ 1,636)
Daily FolicAcid Use p-Value*
Daily FolicAcid Use p-Value*
Reproductive status
Prior pregnancyYes 14.3% .536 28.8% .011**No 18.0% 33.6%
Pregnancy intent within the next yearYes 15.0% 1.000 38.5% .017**No 16.8% 26.4%
Health-related behaviors
Daily fruit consumptionYes 27.9% .001** 33.7% .000**No 11.6% 23.7%
Salad consumption �5 times a weekYes 23.1% .168 31.8% .019**No 14.8% 25.6%
Daily vegetable consumptionYes 17.6% .867 31.3% .001**No 16.1% 23.8%
Binge drinkingYes 20.6% .417 24.0% .331No 15.4% 27.5%
SmokingYes 12.5% .272 19.5% .000**No 18.6% 29.6%
Physical activityYes 28.8% .002** 37.0% .000**No 12.3% 23.8%
Access to health care
Visits an obstetrician-gynecologistYes 18.2% .428 28.9% .011**No 13.7% 22.6%
Spoken with a doctor about diet/nutritionYes 21.2% .125 32.3% .001**No 13.5% 24.2%
Sociodemographics
Completed some college or moreYes 18.7% .484 29.6% .006**No 14.8% 23.2%
Married or living with a partnerYes 17.7% .917 28.5% .009**No 16.5% 20.6%
Urban areaYes 14.1% .130 25.9% .229No 22.4% 28.7%
* Based on c2 tests of associations between each independent vari-able and daily folic acid supplementation.** p , 0.05.
Table 3. Multiple Logistic Regression Analysis of Daily Folic AcidSupplementation in Women Ages 18–45 (n ¼ 1,887y)
AdjustedOdds Ratio
95% ConfidenceInterval*
Agez 1.803** 1.224–2.656**Reproductive status
Prior pregnancy .712** .532–.953**Pregnancy intent within
the next year1.463 .952–2.247
Health-related behaviorsDaily fruit consumption 1.447** 1.142–1.834**Salad consumption �5 times
a week1.121 .873–1.439
Daily vegetable consumption 1.150 .916–1.444Binge drinking (none) .945 .681–1.311Smoking (none) 1.449** 1.098–1.914**Physical activity 1.769** 1.393–2.247**
Access to health careVisits an obstetrician-gynecologist 1.318** 1.030–1.685Spoken with a doctor about diet/
nutrition1.389** 1.114–1.733
SociodemographicsCompleted some college or more 1.109 .877–1.401Married or living with a partner 1.453** 1.070–1.972**Urban area .768** .616–.957**
y This sample size reflects listwise deletion.z Dichotomized into 18- to 24-year-olds versus 25- to 45-year-olds;odds ratio reflects higher usage in older women.* Based on logistic regression analysis; CI not including 1 are signif-icant at p , .05.** p , .05.
L. Evans and C. S. Weisman / Women’s Health Issues 20 (2010) 50–57 55
conception, often before a woman is even aware thatshe is pregnant (CDC, 1992). Research has shownthat among women who are capable of becomingpregnant, more interconceptional women (betweenpregnancies) than preconceptional women (neverpregnant) are supplementing with folic acid (Weismanet al., 2006). This finding suggests that women are de-veloping the healthy supplementation habit after con-ception rather than in the preconceptional period,
when it would have a greater impact on preventingbirth defects. Therefore, the importance of folic aciduse must become more of an integral part of precon-ception care (Brundage, 2002).
According to a recent study, OB-GYNs are morelikely than family physicians to discuss the importanceof folic acid use with their female patients (Tough,Clarke, Hicks, & Cook, 2006). However, it is possiblethat even OB-GYNs are failing to mention the impor-tance of folic acid use during routine visits, regardlessof pregnancy intentions, because fewer than 40% ofOB-GYNs rated it as an important subject matter tobe discussed during check-ups. Additionally, althoughOB-GYNs believe folic acid supplementation is thesecond most important topic of discussion in precon-ception care and counseling, they ranked the topiconly tenth in importance of subjects to talk about dur-ing routine care visits (Morgan, Hawks, Zinberg, &Schulkin, 2006). Furthermore, the report issued bythe CDC found that women ages 18–24 claim to bemore likely to hear of the importance of folic acid usagefrom a magazine or through their college rather thanfrom a health care provider (CDC, 2007).
As evidenced by these findings, there is a need forthe development of a plan to address the lack of folicacid supplementation in women ages 18–24 yearsold. The CDC and other research have called for specialattention to be paid to increasing awareness in younger
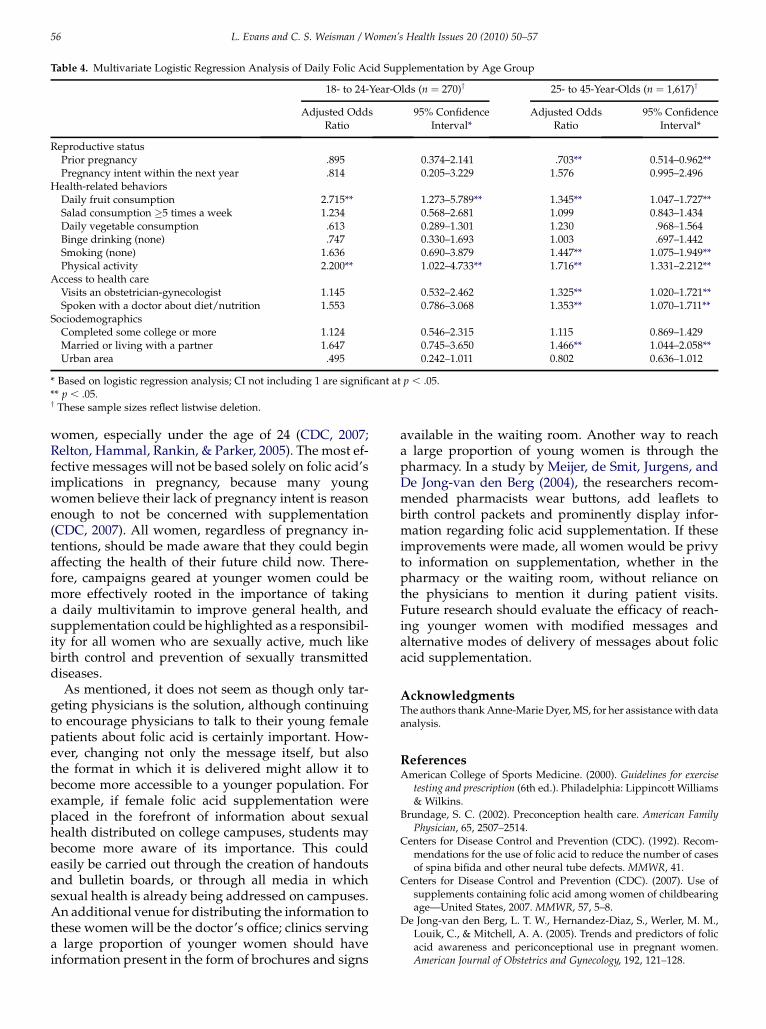
Table 4. Multivariate Logistic Regression Analysis of Daily Folic Acid Supplementation by Age Group
18- to 24-Year-Olds (n ¼ 270)y 25- to 45-Year-Olds (n ¼ 1,617)y
Adjusted OddsRatio
95% ConfidenceInterval*
Adjusted OddsRatio
95% ConfidenceInterval*
Reproductive statusPrior pregnancy .895 0.374–2.141 .703** 0.514–0.962**Pregnancy intent within the next year .814 0.205–3.229 1.576 0.995–2.496
Health-related behaviorsDaily fruit consumption 2.715** 1.273–5.789** 1.345** 1.047–1.727**Salad consumption �5 times a week 1.234 0.568–2.681 1.099 0.843–1.434Daily vegetable consumption .613 0.289–1.301 1.230 .968–1.564Binge drinking (none) .747 0.330–1.693 1.003 .697–1.442Smoking (none) 1.636 0.690–3.879 1.447** 1.075–1.949**Physical activity 2.200** 1.022–4.733** 1.716** 1.331–2.212**
Access to health careVisits an obstetrician-gynecologist 1.145 0.532–2.462 1.325** 1.020–1.721**Spoken with a doctor about diet/nutrition 1.553 0.786–3.068 1.353** 1.070–1.711**
SociodemographicsCompleted some college or more 1.124 0.546–2.315 1.115 0.869–1.429Married or living with a partner 1.647 0.745–3.650 1.466** 1.044–2.058**Urban area .495 0.242–1.011 0.802 0.636–1.012
* Based on logistic regression analysis; CI not including 1 are significant at p , .05.** p , .05.y These sample sizes reflect listwise deletion.
L. Evans and C. S. Weisman / Women’s Health Issues 20 (2010) 50–5756
women, especially under the age of 24 (CDC, 2007;Relton, Hammal, Rankin, & Parker, 2005). The most ef-fective messages will not be based solely on folic acid’simplications in pregnancy, because many youngwomen believe their lack of pregnancy intent is reasonenough to not be concerned with supplementation(CDC, 2007). All women, regardless of pregnancy in-tentions, should be made aware that they could beginaffecting the health of their future child now. There-fore, campaigns geared at younger women could bemore effectively rooted in the importance of takinga daily multivitamin to improve general health, andsupplementation could be highlighted as a responsibil-ity for all women who are sexually active, much likebirth control and prevention of sexually transmitteddiseases.
As mentioned, it does not seem as though only tar-geting physicians is the solution, although continuingto encourage physicians to talk to their young femalepatients about folic acid is certainly important. How-ever, changing not only the message itself, but alsothe format in which it is delivered might allow it tobecome more accessible to a younger population. Forexample, if female folic acid supplementation wereplaced in the forefront of information about sexualhealth distributed on college campuses, students maybecome more aware of its importance. This couldeasily be carried out through the creation of handoutsand bulletin boards, or through all media in whichsexual health is already being addressed on campuses.An additional venue for distributing the information tothese women will be the doctor’s office; clinics servinga large proportion of younger women should haveinformation present in the form of brochures and signs
available in the waiting room. Another way to reacha large proportion of young women is through thepharmacy. In a study by Meijer, de Smit, Jurgens, andDe Jong-van den Berg (2004), the researchers recom-mended pharmacists wear buttons, add leaflets tobirth control packets and prominently display infor-mation regarding folic acid supplementation. If theseimprovements were made, all women would be privyto information on supplementation, whether in thepharmacy or the waiting room, without reliance onthe physicians to mention it during patient visits.Future research should evaluate the efficacy of reach-ing younger women with modified messages andalternative modes of delivery of messages about folicacid supplementation.
AcknowledgmentsThe authors thank Anne-Marie Dyer, MS, for her assistance with dataanalysis.
ReferencesAmerican College of Sports Medicine. (2000). Guidelines for exercise
testing and prescription (6th ed.). Philadelphia: Lippincott Williams& Wilkins.
Brundage, S. C. (2002). Preconception health care. American Family
Physician, 65, 2507–2514.Centers for Disease Control and Prevention (CDC). (1992). Recom-
mendations for the use of folic acid to reduce the number of casesof spina bifida and other neural tube defects. MMWR, 41.
Centers for Disease Control and Prevention (CDC). (2007). Use ofsupplements containing folic acid among women of childbearingage—United States, 2007. MMWR, 57, 5–8.
De Jong-van den Berg, L. T. W., Hernandez-Diaz, S., Werler, M. M.,Louik, C., & Mitchell, A. A. (2005). Trends and predictors of folicacid awareness and periconceptional use in pregnant women.American Journal of Obstetrics and Gynecology, 192, 121–128.

L. Evans and C. S. Weisman / Women’s Health Issues 20 (2010) 50–57 57
Finer, L. B., & Henshaw, S. K. (2006). Disparities in rates of unin-tended pregnancy in the United States, 1994 and 2001. Perspectives
on Sexual and Reproductive Health, 38, 90–96.Hall, S. A., Kaufman, J. S., & Ricketts, T. C. (2006). Defining urban and
rural areas in US epidemiologic studies. Journal of Urban Health, 83,162–175.
Hart, L. G., Larson, E. H., & Lishner, D. M. (2005). Rural definitionsfor health policy and research. American Journal of Public Health,95, 1149–1155.
Hilton, J. J. (2007). A comparison of folic acid awareness and intakeamong young women aged 18-24 years. Journal of the AmericanAcademy of Nurse Practitioners, 19, 516–522.
Meijer, W. M., de Smit, D. J., Jurgens, R. A., & De Jong-van denBerg, L. T. W. (2004). Pharmacists’ role in improving awarenessabout folic acid: a pilot study on the process of introducing an in-tervention in pharmacy practice. International Journal of Pharmacy
Practice, 12, 29–35.Morgan, M. A., Hawks, D., Zinberg, S., & Schulkin, J. (2006). What
obstetrician-gynecologists think of preconception care. Maternal
and Child Health Journal, 10, S59–S65.Relton, C. L., Hammal, D. M., Rankin, J., & Parker, L. (2005). Folic acid
supplementation and social deprivation. Public Health Nutrition, 8,338–340.
Tough, S. C., Clarke, M., Hicks, M., & Cook, J. (2006). Pre-conceptionpractices among family physicians and obstetrician-gynaecolo-gists: Results from a national survey. Journal of Obstetrics andGynaecology Canada, 28, 780–788.
U.S. Department of Health and Human Services. (2000). Healthy peo-
ple 2010. 2nd ed. Vol I. Washington, DC: Author.
Weisman, C. S., Hillemeier, M. M., Chase, G. A., Dyer, A. M.,Baker, S. A., Feinberg, M., et al. (2006). Preconceptional health:risks of adverse pregnancy outcomes by reproductive life stagein the Central Pennsylvania Women’s Health Study (CePAWHS).Women’s Health Issues, 16, 216–224.
Werler, M. M., Louik, C., & Mitchell, A. A. (1999). Achieving a publichealth recommendation for preventing neural tube defects withfolic acid. American Journal of Public Health, 89, 1637–1640.
Yang, Q., Carter, H. K., Mulinare, J., Berry, R. J., Friedman, J. M., &Erickson, J. D. (2007). Race-ethnicity differences in folic acid intakeamong women of childbearing age in the United States after folicacid fortification: Findings from the National Health and Nutri-tion Examination Survey, 2001-2002. American Journal of Clinical
Nutrition, 85, 1409–1416.
Author DescriptionsLaura Evans is a third year medical student at the
Pennsylvania State University College of Medicine.She has a particular interest in women’s health and Ob-stetrics and Gynecology. She received her Bachelor ofArts degree from Franklin and Marshall College.
Carol S. Weisman, PhD, is a sociologist and healthservices researcher with a principal interest inwomen’s health. Her current research focuses on pre-conception health, women’s access to cancer screeningservices, and quality of women’s primary care.