Folic Acid Deficiency.doc
22
Folic Acid Deficiency Author: Angela Gentil i, MD; Chief Edito r: Emmanuel C Besa, MD Background The prevalence of folic acid deficiency has decreased since the nited !tates and Canada introduced a mandatory folic acid food fortification program in "ovem#er $%%&' (eople )ith e*cessive alcohol inta+e and malnutrition are still at high ris+ of folic acid deficiency' istologically, the megalo#lastosis caused #y folic acid deficiency cannot #e differentiated from that o#served )ith vitamin B-$. deficiency' The significance of folic acid deficiency is compounded further #y the follo)ing attri#utes: • An association of folate defi ciency )ith elevated homocystei ne, leading to increased arteriosclerosis ris+s /$0 • The reduced incidence of neural tu#e defects )ith folate supplementation • The role of folate in the occurrence of cancer ence, folic acid clearly is of conse1uence in pu#lic health in the nited !tates, especially #ecause heart disease and cancer constitute the num#er $ and num#er . causes of mortality in the nited !tates' This article e*plores the mechanisms and
-
Upload
pangrum-yongcharoen -
Category
Documents
-
view
227 -
download
0
Transcript of Folic Acid Deficiency.doc

8/14/2019 Folic Acid Deficiency.doc
http://slidepdf.com/reader/full/folic-acid-deficiencydoc 1/22
Folic Acid Deficiency
Author: Angela Gentili, MD; Chief Editor: Emmanuel C Besa, MD
Background
The prevalence of folic acid deficiency has decreased since
the nited !tates and Canada introduced a mandatory folic acid
food fortification program in "ovem#er $%%&' (eople )ith e*cessive
alcohol inta+e and malnutrition are still at high ris+ of folic acid
deficiency'
istologically, the megalo#lastosis caused #y
folic acid deficiency cannot #e differentiated from that o#served )ith
vitamin B-$. deficiency'
The significance of folic acid deficiency is compounded further #y
the follo)ing attri#utes:
• An association of folate deficiency )ith elevated homocysteine,
leading to increased arteriosclerosis ris+s/$0
• The reduced incidence of neural tu#e defects )ith folate
supplementation• The role of folate in the occurrence of cancer
ence, folic acid clearly is of conse1uence in pu#lic health in
the nited !tates, especially #ecause heart disease and cancer
constitute the num#er $ and num#er . causes of mortality in the
nited !tates' This article e*plores the mechanisms and

8/14/2019 Folic Acid Deficiency.doc
http://slidepdf.com/reader/full/folic-acid-deficiencydoc 2/22
manifestations #ehind folate deficiency, as )ell as its ramifications
)ith regard to health and disease at large'
Pathophysiology
2olic acid is composed of a pterin ring connected to p-
amino#en3oic acid 4(ABA5 and con6ugated )ith one or more
glutamate residues' 7t is distri#uted )idely in green leafy vegeta#les,
citrus fruits, and animal products' umans do not generate folate
endogenously #ecause they cannot synthesi3e (ABA, nor can they
con6ugate the first glutamate'
2olates are present in natural foods and tissues as
polyglutamates #ecause these forms serve to +eep the folates
)ithin cells' 7n plasma and urine, they are found as
monoglutamates #ecause this is the only form that can #e
transported across mem#ranes' En3ymes in the lumen of the small
intestine convert the polyglutamate form to the monoglutamate form
of the folate, )hich is a#sor#ed in the pro*imal 6e6unum via #oth
active and passive transport'
8ithin the plasma, folate is present, mostly in the 9-
methyltetrahydrofolate 49-methyl T2A5 form, and is loosely
associated )ith plasma al#umin in circulation' The 9-methyl T2A
enters the cell via a diverse range of folate transporters )ithdiffering affinities and mechanisms 4ie, adenosine triphosphate
/AT(0dependent cotransporter or anion e*changer5' <nce inside,
9-methyl T2A may #e demethylated to T2A, the active form
participating in folate-dependent en3ymatic reactions' Co#alamin 4B-
$.5 is re1uired in this conversion, and in its a#sence, folate is
=trapped= as 9-methyl T2A'

8/14/2019 Folic Acid Deficiency.doc
http://slidepdf.com/reader/full/folic-acid-deficiencydoc 3/22
2rom then on, folate no longer is a#le to participate in its
meta#olic path)ays, and megalo#lastic anemia results' >arge doses
of supplemental folate can #ypass the folate trap, and megalo#lastic
anemia )ill not occur' o)ever, the neurologic?psychiatric
a#normalities associated )ith B-$. deficiency ensue progressively'
The #iologically active form of folic acid is tetrahydrofolic acid
4T2A5, )hich is derived #y the .-step reduction of folate involving
dihydrofolate reductase' T2A plays a +ey role in the transfer of $-
car#on units 4such as methyl, methylene, and formyl groups5 to the
essential su#strates involved in the synthesis of D"A, @"A, and
proteins' More specifically, T2A is involved )ith the en3ymatic
reactions necessary to synthesis of purine, thymidine, and amino
acid' Manifestations of folate deficiency thereafter, not surprisingly,
)ould involve impairment of cell division, accumulation of possi#ly
to*ic meta#olites such as homocysteine, and impairment of
methylation reactions involved in the regulation of gene e*pression,
thus increasing neoplastic ris+s'
A healthy individual has a#out 9-., mcg of folate in
#ody stores' umans need to a#sor# appro*imately 9-$ mcg of
folate per day in order to replenish the daily degradation and loss
through urine and #ile' <ther)ise, signs and symptoms of deficiencycan manifest after months'
Epidemiology
Frequency
United States
The current standard of practice is that serum folate levels
less than ng?m> and a red #lood cell 4@BC5 folate level less than

8/14/2019 Folic Acid Deficiency.doc
http://slidepdf.com/reader/full/folic-acid-deficiencydoc 4/22
$ ng?m> puts an individual at high ris+ of folate deficiency' The
@BC folate level generally indicates folate stored in the #ody,
)hereas the serum folate level tends to reflect acute changes in
folate inta+e'
Data from the "ational ealth and "utrition E*amination
!urvey 4"A"E!5 $%%%-. indicate the prevalence of lo) serum
folate concentrations 4 '& nmol?>5 decreased from $F #efore
folic acid fortification to '9F after folic acid fortification'/.07n elderly
persons, the prevalence of high serum folate concentrations 49'
nmol?>5 increased from HF #efore fortification to &F after
fortification' The latest results from "A"E! are availa#le'/0
International
Countries that do not have a mandatory folic acid food
fortification program have higher rates of folic acid deficiency' 2or
e*ample, a population #ased study in 7ran 4)here there is no
fortification5 sho)ed an age-ad6usted prevalence of
hyperhomocysteinemia 4cy I$9 micromol?>5 of H'$F in men and
$'HF in )omen 4aged .9- y5'
Casey et al e*amined the effects over $ year of a free )ee+ly iron-
folic acid supplementation and de)orming program in 9.,
Jietnamese )omen of child#earing age'
/0
The investigators collecteddemographic data and #lood and stool samples at #aseline and at
and $. months follo)ing the implementation of the program'
2indings included a mean # increase of %' g?> 4( '$5
and a reduction in the presence of anemia from H'9F of the
)omen at #aseline to $%'F at $. months'/07ron deficiency )as
also reduced, from ..'&F at #aseline to %'F #y $. months, as

8/14/2019 Folic Acid Deficiency.doc
http://slidepdf.com/reader/full/folic-acid-deficiencydoc 5/22

8/14/2019 Folic Acid Deficiency.doc
http://slidepdf.com/reader/full/folic-acid-deficiencydoc 6/22
accumulates' !everal recent clinical studies have indicated that mild-
to-moderate hyperhomocystinemia is highly associated )ith
atherosclerotic vascular disease such as coronary artery disease
4CAD5 and stro+e' 7n this case, mild hyperhomocystinemia is
defined as total plasma concentration of $9-.9 mmol?> and
moderate hyperhomocystinemia is defined as .-9 mmol?>'
Genest et al found that a group of $H men )ith premature
coronary artery disease had a significantly higher average level of
homocysteine 4$'H K '5'/07n another study, Coull et al found that
among %% patients )ith stro+e or transient ischemic attac+s 4T7As5,
a#out one third had elevated homocysteine'/H0
Elevated homocysteine levels might act as an atherogenic
factor #y converting a sta#le pla1ue into an unsta#le, potentially
occlusive, lesion' 8ang et al found that in patients )ith acute
coronary syndromes, levels of homocysteine and monocyte
chemoattractant protein-$ 4MC(-$5 )ere significantly higher'/&0MC(-$
is a chemo+ine characteri3ed #y the a#ility to induce migration and
activation of monocytes and therefore may contri#ute to the
pathogenesis of CAD' omocysteine is #elieved to have atherogenic
and prothrom#otic properties via multiple mechanisms'
Bo+hari et al found that among patients )ith CAD, thehomocysteine level correlates independently )ith left ventricular
systolic function'/%0The mechanism is un+no)n, #ut it may #e due to
a direct to*ic effect of homocysteine on myocardial function
separate from its effect on coronary atherosclerosis'
Although in multiple o#servational studies elevated plasma
homocysteine levels have #een positively associated )ith increased

8/14/2019 Folic Acid Deficiency.doc
http://slidepdf.com/reader/full/folic-acid-deficiencydoc 7/22
ris+ of atherosclerosis, randomi3ed trials have not #een a#le to
demonstrate the utility of homocysteine-lo)ering therapy' 7n the
eart <utcomes (revention Evaluation 4<(E5 . trial, supplements
com#ining folic acid and vitamins B and B$. did not reduce the
ris+ of ma6or cardiovascular events in patients )ith vascular
disease'/$0
!imilarly, in the trial of Bonaa et al treatment )ith B
vitamins did not lo)er the ris+ of recurrent cardiovascular disease
after acute myocardial infarction'/$$0
Pregnancy complications
(ossi#le pregnancy complications secondary to maternal folate
status may include spontaneous a#ortion, a#ruption placentae,
congenital malformations 4eg, neural tu#e defect5, and severe
language delay in the offspring' 7n a literature revie), @ay et al
e*amined & studies that demonstrated association #et)een
hyperhomocystinemia and placental a#ruption?infarction'/$.0
2olate
deficiency also )as a ris+ factor for placental a#ruption?infarction,
although less statistically significant'/$0
!everal o#servational and controlled trials have sho)n that
neural tu#e defects can #e reduced #y &F or more )hen folic
acid supplementation is started #efore conception' 7n countries li+e
the nited !tates and Canada, the policy of )idespread fortificationof flour )ith folic acid has proved effective in reducing the num#er
of neural tu#e defects'/$0
Although the e*act mechanism is not understood, a relative
folate shortage may e*acer#ate an underlying genetic predisposition
to neural tu#e defects'

8/14/2019 Folic Acid Deficiency.doc
http://slidepdf.com/reader/full/folic-acid-deficiencydoc 8/22

8/14/2019 Folic Acid Deficiency.doc
http://slidepdf.com/reader/full/folic-acid-deficiencydoc 9/22

8/14/2019 Folic Acid Deficiency.doc
http://slidepdf.com/reader/full/folic-acid-deficiencydoc 10/22
may have chronic hemolytic anemia; or may have underlying
mala#sorption'
!ome patients complain of a sore tongue or pain upon
s)allo)ing' The tongue may appear s)ollen, #eefy, red, or shiny,
usually around the edges and tips initially' Angular stomatitis also
may #e o#served' These oral lesions typically occur at the time
)hen folate depletion is severe enough to cause megalo#lastic
anemia, although, occasionally, lesions may occur #efore the
anemia'
(atients may present )ith G7 symptoms, such as nausea,
vomiting, a#dominal pain, and diarrhea, especially after meals'
Anore*ia also is common and, in com#ination )ith the a#ove
symptoms, may lead to mar+ed )eight loss' o)ever, #e a)are
that an underlying mala#sorption disorder could #e causing these
symptoms, as )ell as folate depletion' The lac+ of folate itself may
not #e the culprit'
Physical
(atients )ith folate deficiency may have dar+ening of the s+in
and mucous mem#ranes, particularly at the dorsal surfaces of the
fingers, toes, and creases of palms and soles' Distri#ution typically
is patchy' 2ortunately, the hyperpigmentation gradually should
resolve after )ee+s or months of folate treatment' A modest
temperature elevation 4 $.N25 is common in patients )ho are
folate deficient, despite the a#sence of any infection' Although the
underlying mechanism is o#scure, the temperature typically falls

8/14/2019 Folic Acid Deficiency.doc
http://slidepdf.com/reader/full/folic-acid-deficiencydoc 11/22
)ithin .-& hours of vitamin treatment and returns to normal )ithin
a fe) days'
%auses
2olate deficiency can result from several possi#le causes,
including inade1uate ingestion, impaired a#sorption, impaired
meta#olism leading to ina#ility to utili3e folate that is a#sor#ed,
increased re1uirement, increased e*cretion, and increased
destruction'
• 7nade1uate ingestion of folate-containing foods: (oor nutrition
is prevalent among people )ith alcoholism and patients )ith
psychiatric mor#idities, as )ell as elderly people 4due to
conditions such as ill-fitting dentures, physical disa#ilities, and
social isolation5' Because folates are destroyed #y prolonged
e*posure to heat, people of certain cultures that involve
traditionally coo+ing food in +ettles of #oiling )ater may #e
predisposed to folate deficiency' Moreover, for patients )ith
renal and liver failure, anore*ia and restriction of foods rich in
protein, potassium, and phosphate contri#ute to decreased
folate inta+e'
• 7mpaired a#sorption
o The limiting factor in folate a#sorption is its transport
across the intestinal )all' 2olate transport across the gut
)all mainly is carrier mediated, satura#le, su#strate
specific, p dependent 4optimal at lo) p5, sodium
dependent, and suscepti#le to meta#olic inhi#itors'
(assive, diffusional a#sorption also occurs, to a minor
8/14/2019 Folic Acid Deficiency.doc
http://slidepdf.com/reader/full/folic-acid-deficiencydoc 12/22
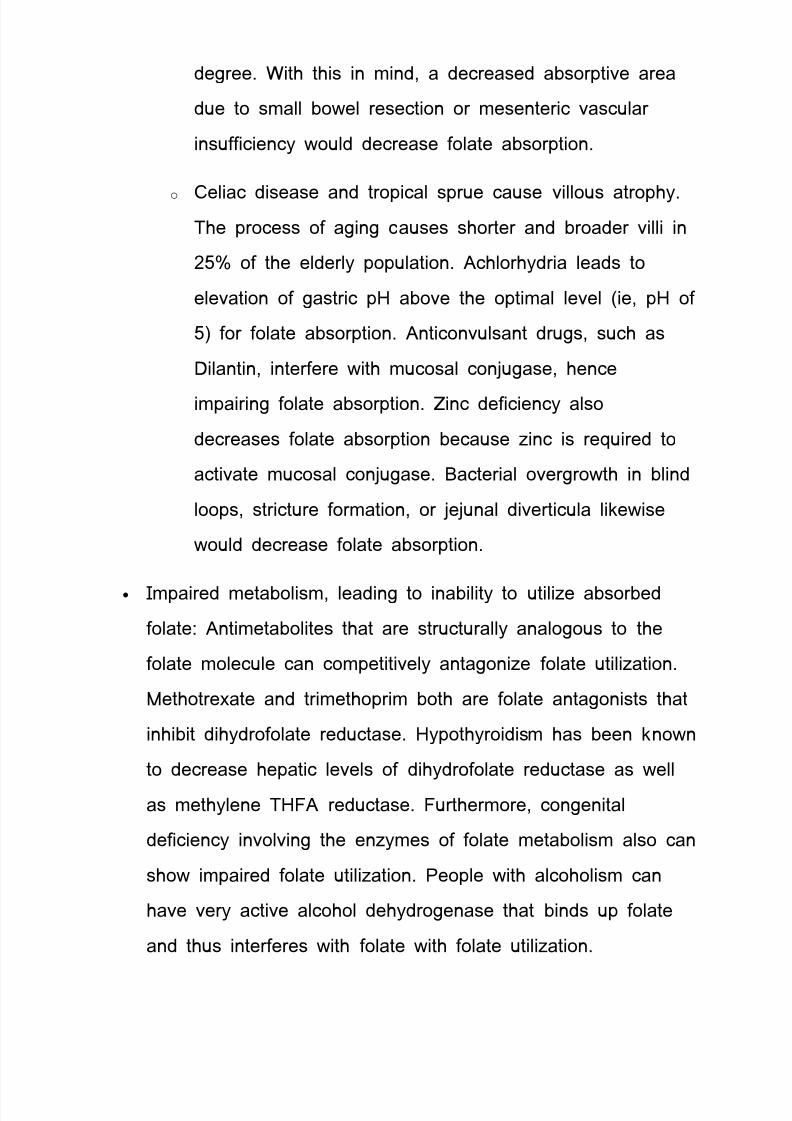
degree' 8ith this in mind, a decreased a#sorptive area
due to small #o)el resection or mesenteric vascular
insufficiency )ould decrease folate a#sorption'
o Celiac disease and tropical sprue cause villous atrophy'
The process of aging causes shorter and #roader villi in
.9F of the elderly population' Achlorhydria leads to
elevation of gastric p a#ove the optimal level 4ie, p of
95 for folate a#sorption' Anticonvulsant drugs, such as
Dilantin, interfere )ith mucosal con6ugase, hence
impairing folate a#sorption' Oinc deficiency also
decreases folate a#sorption #ecause 3inc is re1uired to
activate mucosal con6ugase' Bacterial overgro)th in #lind
loops, stricture formation, or 6e6unal diverticula li+e)ise
)ould decrease folate a#sorption'
• 7mpaired meta#olism, leading to ina#ility to utili3e a#sor#ed
folate: Antimeta#olites that are structurally analogous to the
folate molecule can competitively antagoni3e folate utili3ation'
Methotre*ate and trimethoprim #oth are folate antagonists that
inhi#it dihydrofolate reductase' ypothyroidism has #een +no)n
to decrease hepatic levels of dihydrofolate reductase as )ell
as methylene T2A reductase' 2urthermore, congenital
deficiency involving the en3ymes of folate meta#olism also can
sho) impaired folate utili3ation' (eople )ith alcoholism can
have very active alcohol dehydrogenase that #inds up folate
and thus interferes )ith folate )ith folate utili3ation'

8/14/2019 Folic Acid Deficiency.doc
http://slidepdf.com/reader/full/folic-acid-deficiencydoc 13/22
• 7ncreased re1uirement: 2actors that increase the meta#olic
rate can increase the folic re1uirement' 7nfancy 4a period of
rapid gro)th5, pregnancy 4rapid fetal gro)th5, lactation 4upta+e
of folate into #reast mil+5, malignancy 4increased cell turnover5,
concurrent infection 4immunoproliferative response5, and chronic
hemolytic anemia 4increased hematopoiesis5 all can result in
an increased folate re1uirement'
• 7ncreased e*cretion?loss: 7ncreased e*cretion of folate can
occur su#se1uent to vitamin B-$. deficiency' During the
course of vitamin B-$. deficiency, methylene T2A is +no)n
to accumulate in the serum, )hich is +no)n as the folate trap
phenomenon' 7n turn, large amounts of folate filter through the
glomerulus, and urine e*cretion occurs' Another mechanism of
e*cess e*cretion occurs in people )ith chronic alcoholism )ho
can have increased e*cretion of folate into the #ile' (atientsundergoing hemodialysis also have #een +no)n to have
e*cess folate loss during procedures'
• 7ncreased destruction: !upero*ide, an active meta#olite of
ethanol meta#olism, is +no)n to inactivate folate #y splitting
the folate molecule in half #et)een the C% and "$ position'
The relationship #et)een cigarette smo+ing and lo) folate
levels has #een noted as possi#ly due to folate inactivation in
e*posed tissue'
Differential Diagnoses
• (ernicious Anemia
8/14/2019 Folic Acid Deficiency.doc
http://slidepdf.com/reader/full/folic-acid-deficiencydoc 14/22
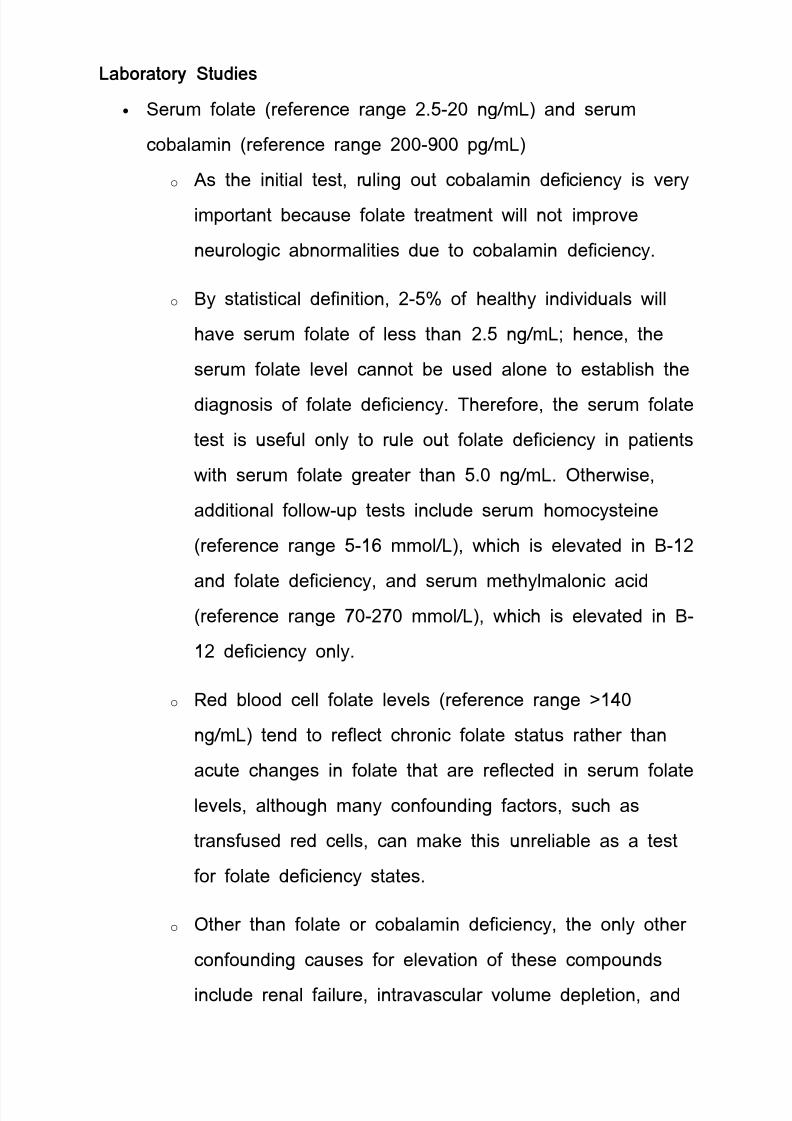
&a!oratory Studies
• !erum folate 4reference range .'9-. ng?m>5 and serum
co#alamin 4reference range .-% pg?m>5
o As the initial test, ruling out co#alamin deficiency is very
important #ecause folate treatment )ill not improve
neurologic a#normalities due to co#alamin deficiency'
o By statistical definition, .-9F of healthy individuals )ill
have serum folate of less than .'9 ng?m>; hence, the
serum folate level cannot #e used alone to esta#lish the
diagnosis of folate deficiency' Therefore, the serum folate
test is useful only to rule out folate deficiency in patients
)ith serum folate greater than 9' ng?m>' <ther)ise,
additional follo)-up tests include serum homocysteine
4reference range 9-$ mmol?>5, )hich is elevated in B-$.
and folate deficiency, and serum methylmalonic acid4reference range H-.H mmol?>5, )hich is elevated in B-
$. deficiency only'
o @ed #lood cell folate levels 4reference range $
ng?m>5 tend to reflect chronic folate status rather than
acute changes in folate that are reflected in serum folate
levels, although many confounding factors, such as
transfused red cells, can ma+e this unrelia#le as a test
for folate deficiency states'
o <ther than folate or co#alamin deficiency, the only other
confounding causes for elevation of these compounds
include renal failure, intravascular volume depletion, and

8/14/2019 Folic Acid Deficiency.doc
http://slidepdf.com/reader/full/folic-acid-deficiencydoc 15/22
some rare in#orn errors of meta#olism involving folate or
co#alamin-dependent en3ymes'
Procedures
Bone marro) #iopsy and aspirate may sho) a hypercellular
#one marro) )ith a megalo#lastic maturation of cells 4see 7mages
- or #elo)5' This cannot #e differentiated from changes o#served
)ith vitamin B-$. deficiency'
istologically, the megalo#lastosis caused #y
folic acid deficiency cannot #e differentiated from that o#served )ith
vitamin B-$. deficiency' (eripheral smear of
#lood in a patient )ith pernicious anemia' Macrocytes are o#served
and some of the red #lood cells sho) ovalocytosis' A -lo#ed
polymorphonuclear leucocyte is present' Bone
marro) aspirate from a patient )ith untreated pernicious anemia'

8/14/2019 Folic Acid Deficiency.doc
http://slidepdf.com/reader/full/folic-acid-deficiencydoc 16/22
Megalo#lastic maturation of erythroid precursors is sho)n' T)o
megalo#lasts occupy the center of the slide )ith a megalo#lastic
normo#last a#ove'
Medical %are
2ruits and vegeta#les constitute the primary dietary source of
folic acid' The minimal daily re1uirement is a#out 9 mcg, #ut this
may #e increased several fold during periods of enhanced meta#olic
demand such as pregnancy'
%onsultations
Consult a dietitian'
Diet
Diet should include fruits and vegeta#les'
Medication Summary
The goals of pharmacotherapy are to eliminate the vitamin
deficiency, reduce mor#idity, and prevent complications'
'itamins
%lass Summary
These agents are essential for normal D"A synthesis and for
the formation of a num#er of coen3ymes in many meta#olic
systems'
Folic acid (Fol#ite)
Cofactor for en3ymes involved in production of red #lood cells'
@eplenishes depleted folate stores consumed during chronic
hemolysis'
Adult Dosing * Uses
Dosing Forms * Strengths

8/14/2019 Folic Acid Deficiency.doc
http://slidepdf.com/reader/full/folic-acid-deficiencydoc 17/22
cream
• '9F
ointment
• '9F
ta#let
• 'mg
• '&mg
• $mg
in6ecta#le solution
• 9mg?m>
+ecommended Daily Allo,ance
Males: mcg?d (<;
2emales: mcg?d (<;
(regnant: mcg?d (<;
"ursing: 9 mcg?d (<;
pper >imit: $ g?d (<
Pre#ention of -eural .u!e Defects
2emales of child#earing potential: mcg?d (<
2emales )? high ris+ or family h* of neural tu#e defects: mg?d
(<
Deficiency
'-$ mg 7J?7M?(< 1D
Methanol .o$icity
9-H9 mg 7J 1hr * . hr
/ther Indications * Uses
Megalo#lastic anemias due to folic acid deficiency 4i'e' sprue5,
anemias of nutritional origin

8/14/2019 Folic Acid Deficiency.doc
http://slidepdf.com/reader/full/folic-acid-deficiencydoc 18/22
"ot effective alone in treatment of pernicious, aplastic, or
normocytic anemias
(regnancy
Elevated serum homocysteine
Pediatric Dosing * Uses
Dosing Forms * Strengths
cream
• '9F
ointment
• '9F
ta#let
• 'mg
• '&mg
• $mg
in6ecta#le solution
• 9mg?m>
+ecommended Daily Allo,ance
- mth: 9 mcg?d (<
H-$. mth: & mcg?d (<
$- years: $9 mcg?d (<
-& years: . mcg?d (<
%-$ years: mcg?d (<
$-$& years: mcg?d (<
pper >imit
• $. mth: "?A
• $- years: mcg?d (<
• -& years: mcg?d (<

8/14/2019 Folic Acid Deficiency.doc
http://slidepdf.com/reader/full/folic-acid-deficiencydoc 19/22
Deficiency
7nfants: $9 mcg?+g?d or 9 mcg?d 7J?(<?7M?!C
$-$ years: $ mg?d 7J?(<?7M?!C initially, then '$-' mg?d
Methanol .o$icity
$ mg?+g 7J 1hr * . hr
/ther Indications * Uses
Megalo#lastic anemias due to folic acid deficiency 4i'e' sprue5,
anemias of nutritional origin
"ot effective alone in treatment of pernicious, aplastic, or
normocytic anemias
(revention of spina #ifida P other congenital neural tu#e
disorders in )omen of child #earing potential
(regnancy
Elevated serum homocysteine
%ontraindications
ypersensitivity
%autions
ndiagnosed anemias
(rotect vials from heat P light
Ad#erse Effects
Frequency -ot Defined
7rrita#ility
Difficulty sleeping
Confusion
Mas+s pernicious anemia
Bronchospasm
@ash

8/14/2019 Folic Acid Deficiency.doc
http://slidepdf.com/reader/full/folic-acid-deficiencydoc 20/22
Can cause deficiency of phenytoin
-utrition
!ources: #lac+ eye peas, pinto #eans, navy #eans, spinach, +idney,
liver, vegeta#les, meats, cereals, fruits, some dar+ green vegeta#les
Function
Enchances elimination of formic acid in methanol to*icity via
provision of coen3yme to folate dehydrogenase
(articipates in D"A synthesis and erythropoiesis
/ther Information
Deficiency: macrocytic anemia; inflammation of tongue; diarrhea
To*icity: mas+ vitamin B$. deficiency; may incr ris+ of sei3ures in
some people
Further /utpatient %are
Treat the underlying disease or condition causing folic acid
deficiency'
DeterrencePre#ention
• (atients )hose folic acid deficiency is related to dietary
factors should #e counseled to include green vegeta#les and
fruit in their diet'
• (rophylactic treatment of pregnant patients and patients )ith
chronic hemolytic anemias can prevent folic acid deficiency
due to the increased re1uirement for folate in these
conditions'
%omplications
• Megalo#lastic anemia
• >eu+openia
• Throm#ocytopenia

8/14/2019 Folic Acid Deficiency.doc
http://slidepdf.com/reader/full/folic-acid-deficiencydoc 21/22
• Angular stomatitis
• Glossitis
• "ausea and vomiting
• Diarrhea
• yperpigmentation
• >o)-grade fever
• Elevated serum homocysteine
Patient Education
• Educate patients regarding proper nutrition, including eating
fruits and vegeta#les'
• Educate patients regarding the need to reduce alcohol
ingestion'
• Discuss the need to ta+e folic acid supplementation'
Medicallegal pitfalls
• 2ailure to provide folic acid supplementation to pregnant
females may lead to spontaneous a#ortion and fetal
a#normalities, including neural tu#e defects and increased ris+
of severe language delay in the child'
• (roviding only folic acid supplementation to a patient )ho has
co#alamin deficiency may lead to development of irreversi#le
neuropathies'• "o randomi3ed clinical trial has proven the efficacy of lo)ering
the homocysteine concentration to improve cognition or to
lo)er the incidence of cardiovascular disease 4CJD5' ntil ne)
evidence is availa#le, clinicians should not promise patients
that folate supplementation )ill improve cognition or decrease
cardiovascular ris+'

8/14/2019 Folic Acid Deficiency.doc
http://slidepdf.com/reader/full/folic-acid-deficiencydoc 22/22





![acid dexaexilcolic,acid folic ]n dezvoltarea creer nn.pdf](https://static.fdocuments.us/doc/165x107/577cb57f1a28aba7118d31d3/acid-dexaexilcolicacid-folic-n-dezvoltarea-creer-nnpdf.jpg)