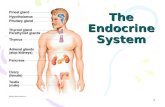
Endocrine & Cell Communication Part II: The Endocrine System.

of 17
Upload
andriyoethCategory
view
217download
08/13/2019 Focused Endocrine Assessment2004
1/17
Presented by:RN.com
12400 High Bluff DriveSan Diego, CA 92130
This course has been approved for one (1) contact hour.
This course expires on September 28, 2006.Copyright 2004 by RN.com.
All Rights Reserved. Reproduction and distributionof these materials are prohibited without the
express written authorization of RN.com.
First Published: September 28, 2004
RN.coms Assessment Series: Focused Endocrine Assessment
8/13/2019 Focused Endocrine Assessment2004
2/17
1
Acknowledgements________________________________________________________________________ 2
Purpose & Objectives _____________________________________________________________________ 3
Introduction _____________________________________________________________________________ 4
Assessing Common Endocrine Abnormalities__________________________________________________ 5
Pituitary Disorders______________________________________________________________________ 6
Thyroid Disorders ______________________________________________________________________ 7
Adrenal Disorders ______________________________________________________________________ 9
Pancreatic Disorders ___________________________________________________________________ 11
Conclusion______________________________________________________________________________ 14
References______________________________________________________________________________ 15
Post Test Viewing Instructions _____________________________________________________________ 16
8/13/2019 Focused Endocrine Assessment2004
3/17
2
ACKNOWLEDGEMENTS
RN.com acknowledges the valuable contributions of
Lori Constantine MSN, RN, C-FNP , author of Focused Endocrine Assessment . Lori has been a nurse for nineyears and has a broad range of clinical experience. She has worked as a staff nurse, charge nurse, and nurse
preceptor on many different medical surgical units including vascular, neurology, neurosurgery, urology,gynecology, ENT, general medicine, geriatrics, oncology, and blood and marrow transplantation. She receivedher Bachelors in Nursing in 1994 and a Masters in Nursing in 1998, both from West Virginia University.Additionally, in 1998, she was certified as a Family Nurse Practitioner. She has worked in staff development asa Nurse Clinician and Education Specialist since 1999 at West Virginia University Hospitals, Morgantown, WV.
8/13/2019 Focused Endocrine Assessment2004
4/17
3
PURPOSE & OBJECTIVES
The purpose of this article is to familiarize you with conducting a focused endocrine assessment. This willallow you to hone in on your patients endocrine signs and symptoms and intervene effectively. Ultimately, thehormones secreted by your endocrine organs execute their effects on specific cells and tissues to maintainhomeostasis within the body. If there is an overproduction or underproduction of these hormones, the patient
usually presents with symptoms. It is your duty as the patients nurse to recognize these symptoms and to actupon them as needed.
After successful completion of this course, you will be able to:
1. Identify assessment findings in common endocrine abnormalities.
2. Briefly discuss the role specific hormones play in selected disease processes.
8/13/2019 Focused Endocrine Assessment2004
5/17
8/13/2019 Focused Endocrine Assessment2004
6/17
5
ASSESSING COMMON ENDOCRINE ABNORMALITIES
When conducting a focused endocrine assessment on your patient, begin with a thorough history of their chiefcomplaints. You will need to elicit information about any experienced signs or symptoms of endocrine diseaseor disorders. Endocrine disorders and diseases usually manifest according to which endocrine hormone is beingoverproduced and secreted or underproduced and secreted. The key to discovering the nature of the symptoms
lies in your understanding of the functions of the endocrine hormones.
When assessing the endocrine system you most likely will perform a problem-focused assessment. The problem-focused endocrine assessment is necessary after a comprehensive assessment indicates a potentialendocrine abnormality. This assessment may also be necessary when an interval or abbreviated assessmentshows a change in status from your last assessment or report you received. When a new symptom emerges orthe patient develops some distress also consider a focused endocrine assessment. The advantage of thisassessment is that it allows you to ask about symptoms and move quickly to conducting a focused physicalexam.
Physical exam techniques used in your focused endocrine assessment are the same techniques used in yourgeneral exam; inspection, auscultation, percussion, and palpation. During inspection, you are looking for things
you can observe with your eyes, ears or nose. Examples of what to inspect related to endocrine abnormalitiesare skin color, location of lesions, bruises or rashes, symmetry, size of body parts, and abnormal sounds orodors.
Auscultation is used in your focused endocrine assessment before percussion or palpation. Examples of examfindings you will auscultate during your focused endocrine assessment include:
Murmurs. Cardiac irregularities. Adventitious breath sounds. Alterations in bowel sounds.
Palpation is another physical exam technique you will use in your focused endocrine assessment. During light palpation, you press the skin about inch to 3/4 inch with the pads of your fingers. When using deep palpation,use your finger pads and compress the skin about 1 inches to 2 inches. Palpation allows you to assess fortexture, tenderness, temperature, moisture, pulsations, masses, and internal organs (Shaw, 1998).
Finally, percussion is used in your focused endocrine assessment to allow you to elicit tenderness or sounds that point to underlying problems. When percussing directly over suspected areas of tenderness, monitor the patientfor signs of discomfort. Examples of endocrine abnormalities you may percuss are an enlarged pancreas, a
pleural effusion associated with specific endocrine abnormalities, or a hormone-secreting tumor.
Assessing endocrine abnormalities requires strong history and physical exam skills. Depending upon your patients chief complaint, specific parts of each body system will be assessed. It requires skill and knowledgeon your behalf to focus your assessment and hone in on the suspected endocrine abnormality. Therefore, it isuseful to review the possible endocrine disorders and their associated pathology, signs, and symptoms. If youunderstand these, you will be able to rapidly focus your assessment to pinpoint the endocrine disease or disorderaffecting your patient.
8/13/2019 Focused Endocrine Assessment2004
7/17
6
Pituitary Disorders
The pituitary gland, also known as the hypophysis, is located atthe base of the brain. It is actually two very different glands; theanterior pituitary and the posterior pituitary. Each gland has aunique link to the hypothalamus. Antidiuretic hormone (ADH),or vasopressin, is the major hormone secreted by the posterior
pituitary. The anterior pituitarys major hormones are growthhormone (GR), thyroid stimulating hormone (TSH), andadrenocorticotropin (ACTH) (Sherwood, 1997).
The hypothalamus, also known as the master gland, producesand releases hormones that stimulate the pituitary gland, namelygrowth hormone releasing hormone (GRH), thyrotropic-releasinghormone (TRH), and corticotropin releasing hormone (CRH)(Sherwood, 1997). The following table summarizes keyassessment findings and their associated disorder or disease,aberrant hormone, potential causes of the disorder or disease, andkey subjective and objective assessment findings.
Syndrome of Inappropriate ADH (SIADH) - Above normal ADH release
Possible Cause ofAbnormality
Key Assessment Findings -Subjective Key Assessment Findings - Objective
ADH secreting tumor Chemotherapy Oat cell carcinoma
Anorexia Nausea Headache Fatigue Irritability
Weight gain Vomiting Muscle weakness Muscle spasms or cramps Possible coma Hallucinations Decreased LOC Confusion Low serum sodium Low serum osmolarity High urine osmolarity Normal urine sodium excretion Low edema
(Pathophysiology: A 2-in-1 reference, 2004)
Diabetes Insipidus (DI) - Below normal ADH release
Possible Cause of AbnormalityKey Assessment Findings -
SubjectiveKey Assessment Findings -
Objective CVA Hypothalamic-pituitary tumors Cranial trauma or surgeries Hereditary Drugs (lithium and phenytoin
[Dilantin]) Alcohol (transient DI)
Abrupt onset of polydipsiaand polyuria
Nocturia Sleep disturbances related
to nocturia Fatigue Headache Visual disturbances
Fluid intake 5-20 liters/day Urine output of 2-20 liters/day
of dilute urine Urine specific gravity < 1.006 Fever Changes in LOC Hypotension Tachycardia
(American Association of Critical Care Nurses, 1998; Pathophysiology: A 2-in-1 reference, 2004)
PituitaryGland Hypothalamus
8/13/2019 Focused Endocrine Assessment2004
8/17
7
Thyroid Disorders
The thyroid gland lies in the anterior portion of the neck andstraddles the trachea. It secretes two hormones that play amajor role in the bodys metabolism, thyroxine (T4) &triiodothyronine (T3). Absence of these hormones maydecrease the bodys basal metabolic rate by 60% and excess ofthese hormones may increase the bodys basal metabolic rate
by 100% (American Association of Critical Care Nurses,1998 ). The following tables summarize key assessmentfindings and their associated disorder or disease, aberranthormone, potential causes of the disorder or disease, and keysubjective and objective assessment findings.
Hypothyroidism - Chronic deficiency of T4 & T3
Possible Cause of Abnormality Key AssessmentFindings - Subjective
Key Assessment Findings - Objective
Thyroid gland dysfunction Inadequate release of TRH or
TSH from the hypothalamic- pituitary axis(hypophysectomy or pituitaryradiation)
Surgical removal orradioiodine ablation withhyperthyroidism
Hashimotos thyroiditis(chronic inflammation of thethyroid)
Diminished hearing Cold intolerance Fatigue Lethargy Complaints of
constipation
Bradycardia Decreased LOC Hypothermia Hypoventilation Hypoactive bowel sounds Weight gain Elevated TSH Free T4 decreased Elevated CK-MB T3, T4 decreased pCO2 increased pO2 decreased pH decreased Hypoglycemia
(American Association of Critical Care Nurses, 1998; Pathophysiology: A 2-in-1 reference, 2004)
Myxedema Coma - Acute deficiency of T4 & T3
Possible Cause of Abnormality Key AssessmentFindings - Subjective
Key Assessment Findings - Objective
Insufficient thyroid
supplementation Increased stressors in patientswith hypothyroidism (trauma,cold, anesthesia, infection)
Subjective findings
associated withhypothyroidism
Similar S/S of hypothyroidism but even
more pronounced, anasarca, hoarseness, pericardial & pleural effusions,diminished hearing, paralytic ileus,unresponsiveness, decreased breathing,low blood pressure, low blood sugar, and
below normal temperature ACUTE SITUATION
(American Association of Critical Care Nurses, 1998; Nurse's Assessment video series: Endocrine signs andsymptoms, 2002)
Thyroid
8/13/2019 Focused Endocrine Assessment2004
9/17
8
Hyperthyroidism - Chronic increase in T4 & T3
Possible Cause ofAbnormality
Key AssessmentFindings - Subjective Key Assessment Findings - Objective
Adenoma Thyroiditis Overtreatment of
hypothyroidism Discontinuation of
thyroid supplements Stress Iodine load with pre-
existing hyperthyroidstate
Pituitary tumor
Irritability Restlessness Heat intolerance Complaints of
diarrhea Insomnia
Tachycardia Atrial arrhythmias PVCs PACs Dyspnea Palpitations Weight loss Hyperthermia Elevated T4 & T3, Decreased TSH Increased TSH if from a TSH secreting
tumor (in pituitary) (+) Test for thyroid antibodies (Graves
Disease)
Hyperglycemia Diaphoresis
(American Association of Critical Care Nurses, 1998; Nurse's Assessment video series: Endocrine signs andsymptoms, 2002; Pathophysiology: A 2-in-1 reference, 2004)
Thyrotoxicosis or Thyroid Storm - Acute increase in T4 & T3
Possible Cause of AbnormalityKey Assessment
Findings - SubjectiveKey Assessment Findings - Objective
Decompensation of pre-existinghyperthyroid state after stressor
(surgery, anesthesia, infection,trauma)
Restlessness Agitation changes in LOC
Same as for hyperthyroidism but more pronounced: tachycardia, diaphoresis,
fever, diarrhea, confusion, signs andsymptoms associated with CHF and
pulmonary edemaCRITICAL SITUATION
(American Association of Critical Care Nurses, 1998; Nurse's Assessment video series: Endocrine signs andsymptoms, 2002)
Sick Euthyroid Syndrome - Underproduction of TSH from the anterior pituitary, which stimulates the production and release of T4 & T3.
Possible Cause of Abnormality Key AssessmentFindings - Subjective
Key Assessment Findings - Objective
Common in acutely ill Abnormalities in thyroid
function occur in patients withserious illness not caused by
primary thyroid or pituitarydysfunction.
May be absent Normal or low TSH Abnormal T4 (low or high) T3 may be low Absence of thyroid symptoms The degree of reduction in thyroid
hormone levels appears to becorrelated with the severity ofnonthyroidal illness
(American Association of Critical Care Nurses, 1998)
8/13/2019 Focused Endocrine Assessment2004
10/17
9
Adrenal Disorders
The adrenal glands are two organs located atop of each kidney.They are responsible for the secretion of mineralocorticoids,glucocorticoids and the corticosteriods, epinephrine andnorepinephrine. Aldosterone accounts for 95% of allmineralocorticoids produced and secreted by the adrenal cortex.Cortisol is the primary glucocorticoid secreted by the adrenalcortex. Epinephrine and norepinephrine are hormones secretedfrom the adrenal medulla (Sherwood, 1997). The following tablesummarizes key assessment findings and their associated disorderor disease, aberrant hormone, potential causes of the disorder ordisease, and key subjective and objective assessment findings.
Primary Adrenal Insufficiency or Addisons Disease - Chronic deficiency or secretion of cortisol (fromadrenal cortex) (Aldosterone is usually unaffected)
Secondary Adrenal Insufficiency - Chronic deficiency of ACTH (from the anterior pituitary), which stimulatescortisol release from the adrenal cortex
Possible Cause ofAbnormality
Key Assessment Findings- Subjective
Key Assessment Findings - Objective
Autoimmune destructionof the adrenal gland
Adrenal destructionfrom surgery, trauma,sepsis, suppression ofgland related to drugs(ketoconazole [Nizoral],rifampin [Rifadin],
phenytoin [Dilantin]),infection, Tuberculosis,hemorrhage, or bilateraladrenelectomy
Pituitary hypofunction(surgery, trauma,ischemia)
Nausea Abdominal pain Fatigue Malaise Weakness
Hyperpigmentation (only in primaryadrenal insufficiency)
Orthostatic hypotension Decreased cardiac size and output Weak & irregular pulse X-rays may show adrenal calcification
(only in primary adrenal insufficiency) Decreased cortisol levels Elevated plasma ACTH levels (in primary
adrenal insufficiency due to disorder ofthe adrenal gland)
Decreased plasma ACTH (whendysfunction is a result of thehypothalamic-pituitary axis)
Other endocrine abnormalities (insecondary adrenal insufficiency due to
pituitary abnormality)(American Association of Critical Care Nurses, 1998; Nurse's Assessment video series: Endocrine signs andsymptoms, 2002; Pathophysiology: A 2-in-1 reference, 2004.)
AdrenalGlands
8/13/2019 Focused Endocrine Assessment2004
11/17
8/13/2019 Focused Endocrine Assessment2004
12/17
11
Pheochromocytoma (Adrenal Neoplasm) - Increase epinephrine & norepinephrine (from adrenal medulla)
Possible Cause of AbnormalityKey Assessment Findings
SubjectiveKey Assessment Findings -
Objective
Tumor of the adrenal medulla Headache Palpitations Dizziness Complaints of constipation Anxiety
Hypertension Hyperglycemia Dyslipidemia Irregular heart rate Diaphoresis Syncope
(Pathophysiology: A 2-in-1 reference, 2004).
Primary Aldosteronism - Increase in production and secretion of aldosterone (from adrenal cortex)
Possible Cause of Abnormality Key Assessment Findings Subjective
Key Assessment Findings -Objective
Most cases of primary
hyperaldosteronism resultfrom a benign tumor of theadrenal gland and occur in
people between 30 and 50years old.
Headache
Muscle weakness Fatigue Numbness
Hypernatremia
Hypervolemia Hypertension Hypokalemia Elevated plasma & elevated
urinary aldosteronism(Pathophysiology: A 2-in-1 reference, 2004)
Pancreatic DisordersThe endocrine pancreas produces and secretes insulin, glucagon,and somatostatin. All three of these hormones play a significantrole in carbohydrate, fat, and protein metabolism (American
Association of Critical Care Nurses, 1998). The following tablesummarizes key assessment findings and their associated disorderor disease, aberrant hormone, potential causes of the disorder ordisease, and key subjective and objective assessment findings.
Diabetes Mellitus - Absolute decreased production of insulin (Type I) OR resistance of cells to circulatinginsulin (Type II)
Possible Cause ofAbnormality
Key Assessment Findings -Subjective
Key Assessment Findings - Objective
Type I: Genetics,autoimmune disease,
viral infections Type II: Genetic factors,
obesity Gestational: Pregnancy
induced
Headaches Fatigue Lethargy Reduced energy levels Irritability Emotional lability Vision changes Numbness Tingling
Hyperglycemia Polyuria Polydipsia Polyphagia Anorexia Muscle cramps Type I presents usually emergently Type II presents insidiously
(Diabetes mellitus: pathophysiology for nurses video series, 2000; Pathophysiology: A 2-in-1 reference, 2004)
Pancreas
8/13/2019 Focused Endocrine Assessment2004
13/17
12
Pancreatic Neoplasms Insulin production and secretion may be impaired
Possible Cause ofAbnormality
Key Assessment Findings -Subjective Key Assessment Findings - Objective
Benign or malignant tumorof the pancreas
Anorexia Nausea Malaise Abdominal or back pain
Jaundice Clay-colored stool Vomiting Weight loss Blood in stool Hypoglycemia or hyperglycemia
(Pathophysiology: A 2-in-1 reference, 2004)
Pancreatitis Insulin production and secreting may be impaired. Inflammation of the pancreas occurs due toedema, hemorrhage, or necrosis.
Possible Cause of Abnormality Key Assessment Findings Subjective
Key Assessment Findings -Objective
Alcoholism
Trauma Peptic ulcer disease Biliary tract disease Pancreatic cysts or tumors Drugs (sulfonomides, thiazides,
birth control pills, NSAIDs) Kidney failure Organ transplantation Endoscopic exam of the biliary tree
Severe, knife-like mid-
epigastric abdominal pain, which can radiateto the back
Mottled skin
Tachycardia Dehydration Hypovolemia Hemodynamic instability Abdominal distention Crackles in lung bases Pleural effusions Increased serum amylase,
lipase, and glucose(Pathophysiology: A 2-in-1 reference, 2004)
Hypoglycemia - Increased insulin production, secretion, and/or administration
Possible Cause ofAbnormality
Key Assessment Findings- Subjective
Key Assessment Findings - Objective
Overproduction,secretion oradministration ofinsulin
Dizziness Weakness Nervousness Agitation Headache Mental dullness
Pallor Cool, clammy skin Diaphoretic Polyphagia Tachycardia Palpitations Confusion Blurred vision
Paresthesias Seizures Coma Decreased blood glucose level (
8/13/2019 Focused Endocrine Assessment2004
14/17
13
Diabetic Ketoacidosis (DKA) - Decreased insulin administration in Type I Diabetics
Possible Cause of Abnormality Key Assessment Findings Subjective
Key Assessment Findings -Objective
Lack of circulating insulin in Type IDiabetics leading to a hyperosmolarand hyperglycemic state with ketone
production New onset diabetes Inadequate insulin use in a known
diabetic patient Stress (MI, CVA, trauma, surgery,
emotional upset) in a known Type Idiabetic
Medications (steroids, beta blockers,thiazide diuretics)
Alcohol use
Myalgias Flu-like signs and
symptoms Lethargy Nausea Decreased level of
consciousness Coma
Warm, dry skin Increased blood glucose
levels (approximately 300-700mg/dL)
Polydipsia Polyuria (due to osmotic
diuresis) Dehydration Increased BUN, HCT,
HGB, acetone breath(exhalation of ketones)
(+) Urine & serum ketones Metabolic acidosis Kussmauls respirations
Increased serum osmolarity
(Diabetes mellitus: pathophysiology for nurses video series, 2000; Pathophysiology: A 2-in-1 reference, 2004;Shaw, 1998)
Hyperosmolar, Hyperglycemic, Non-ketotic Syndrome (HHNKS) - - Increased blood glucose levels in TypeII Diabetics
Possible Cause ofAbnormality
Key Assessment Findings- Subjective
Key Assessment Findings - Objective
Lack of circulating insulinin Type II Diabetics
leading to a hyperosmolarand hyperglycemic statewithout ketone production
Myalgias Flu-like signs and
symptoms Lethargy Nausea Decreased level of
consciousness Coma
Warm, dry skin Increased blood glucose levels
(approximately 400-2,000mg/dL) Polydipsia, polyuria (due to osmotic
diuresis) Severe dehydration Increased BUN, HCT, HGB (-) Urine & serum ketones Absence of acetone breath (no ketones,
no acidosis) Increased serum osmolarity (> 315
mOsm/kg) Wider variety of mental status changes
including hallucinations, seizures,aphasia
(Diabetes mellitus: pathophysiology for nurses video series, 2000; Pathophysiology: A 2-in-1 reference, 2004;Shaw, 1998)
8/13/2019 Focused Endocrine Assessment2004
15/17
14
CONCLUSION
Integrating the health history and physical exam in a focused endocrine assessment takes experience, and moreimportantly, practice. It is not enough to simply ask the right questions and perform the physical exam. As thenurse, you must critically analyze all of the data you obtain, synthesize the data into a relevant problem focus,and then identify a plan of care for your patient based upon this synthesis. As the plan of care is being carried
out, reassessments must occur on a periodic basis. How often these reassessments occur is unique to each patient, based upon their specific endocrine disorder.
8/13/2019 Focused Endocrine Assessment2004
16/17
15
REFERENCES
American Association of Critical Care Nurses (1998). The Endocrine System. In J. Alspach (Ed.), Core curriculum forcritical care nursing (5th ed., Rev., pp. 565-577). Philadelphia: Saunders.
Diabetes mellitus: pathophysiology for nurses video series . (2000). Blanchard & Loeb.
Nurse's Assessment video series: Endocrine signs and symptoms . (2002). Blanchard & Loeb.
Pathophysiology: A 2-in-1 reference . (2004). Philadelphia: Lippincott, Williams & Wilkins.
Shaw, M. (Ed.). (1998). Pathophysiology Made Incredibly Easy. Springhouse, PA: Springhouse.
Sherwood, L. (Ed.). (1997). Human physiology: From cells to systems (3rd ed.). Belmont, California: Wadsworth.
8/13/2019 Focused Endocrine Assessment2004
17/17
16
POST TEST VIEWING INSTRUCTIONS
In order to view the post test you may need to minimize this window and click TAKE TEST. You can thenrestore the window in order to review the course material if needed.