Fluoroscopic Anatomy of Left-Sided Heart Structures for...
11
STATE-OF-THE-ART REVIEW Fluoroscopic Anatomy of Left-Sided Heart Structures for Transcatheter Interventions Insight From Multislice Computed Tomography Pascal Thériault-Lauzier, PHD,* Ali Andalib, MD,* Giuseppe Martucci, MD,* Darren Mylotte, MD,* Renzo Cecere, MD,y Rüediger Lange, MD, PHD,z Didier Tchétché, MD,x Thomas Modine, MD, PHD,k Nicolas van Mieghem, MD,{ Stephan Windecker, MD,# Jean Buithieu, MD,* Nicolo Piazza, MD, PHD*z ABSTRACT With the introduction of transcatheter structural heart therapies, cardiologists are increasingly aware of the importance of understanding anatomical details of left-sided heart structures. Understanding fluoroscopic cardiac anatomy can facilitate optimal positioning and deployment of prostheses during transcatheter valve repair/replacement, left atrial appendage occlusion, septal defect closure, and paravalvular leak closure. It is possible to use multislice computed to- mography to determine optimal fluoroscopic viewing angles for such transcatheter therapies. The purpose of this paper is to describe how optimal fluoroscopic viewing angles of left-sided heart structures can be obtained using computed tomography. Two- and 3-chamber views are described and may become standard in the context of transcatheter structural heart interventions. (J Am Coll Cardiol Intv 2014;7:947–57) © 2014 by the American College of Cardiology Foundation. S ince the introduction of transcatheter struc- tural heart therapies, cardiologists have become increasingly aware of the importance of understanding anatomical details of left-sided car- diac structures (1). Many critical anatomical struc- tures comprise several components and are arranged in a complex tridimensional geometry. Even though these anatomical and functional components have been the topic of numerous publications (1,2), little consideration has been given to understanding their configuration as appreciated under fluoroscopy (3). Understanding fluoroscopic cardiac anatomy can facilitate optimal positioning and deployment of prostheses during transcatheter valve repair/replace- ment, left atrial appendage occlusion, septal defect closure, and paravalvular leak closure. Commonly, these therapies are conducted using standard fluoro- scopic angulations irrespective of variations in anat- omy. It is possible that patient-specific fluoroscopic viewing angles can improve procedural safety and efficacy. Multislice computed tomography (MSCT) multi- planar reconstruction of the aortic valvular complex has enhanced patient selection and procedural planning for transcatheter aortic valve replacement (4). For example, MSCT affords physicians the From the *Department of Medicine, Division of Cardiology, McGill University Health Centre, Montreal, Quebec, Canada; yDepartment of Surgery, Division of Cardiovascular Surgery, McGill University Health Centre, Montreal, Quebec, Canada; zDepartment of Cardiovascular Surgery, German Heart Centre Munich, Munich, Germany; xDepartment of Interventional Cardi- ology, Clinique Pasteur, Toulouse, France; kDepartment of Cardiovascular Surgery, University Hospital of Lille, Lille, France; {Department of Cardiology, Thoraxcentre, Erasmus Medical Centre, Rotterdam, the Netherlands; and the #Department of Interventional Cardiology, University Hospital, Bern, Switzerland. Dr. Martucci is a proctor for Medtronic. Dr. Lange receives consulting and lecture fees from Medtronic. Dr. Modine receives consulting fees from Medtronic. Dr. van Mieghem receives consulting fees from Medtronic and Boston Scientific. Dr. Windecker has received institutional research grants from Biotronik and St. Jude Medical; and serves on the scientific advisory board of Cardialysis BV. Dr. Piazza is a proctor for and receives consulting fees from Medtronic. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose. Manuscript received March 12, 2014; revised manuscript received May 2, 2014, accepted June 4, 2014. JACC: CARDIOVASCULAR INTERVENTIONS VOL. 7, NO. 9, 2014 ª 2014 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/$36.00 PUBLISHED BY ELSEVIER INC. http://dx.doi.org/10.1016/j.jcin.2014.06.002
Transcript of Fluoroscopic Anatomy of Left-Sided Heart Structures for...

J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 7 , N O . 9 , 2 0 1 4
ª 2 0 1 4 B Y T H E A M E R I C A N CO L L E G E O F C A R D I O L O G Y F O U N D A T I O N I S S N 1 9 3 6 - 8 7 9 8 / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R I N C . h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j c i n . 2 0 1 4 . 0 6 . 0 0 2
STATE-OF-THE-ART REVIEW
Fluoroscopic Anatomy of Left-Sided HeartStructures for Transcatheter InterventionsInsight From Multislice Computed Tomography
Pascal Thériault-Lauzier, PHD,* Ali Andalib, MD,* Giuseppe Martucci, MD,* Darren Mylotte, MD,* Renzo Cecere, MD,yRüediger Lange, MD, PHD,z Didier Tchétché, MD,x Thomas Modine, MD, PHD,k Nicolas van Mieghem, MD,{Stephan Windecker, MD,# Jean Buithieu, MD,* Nicolo Piazza, MD, PHD*z
ABSTRACT
Fro
yDzDolo
{DInt
con
con
St.
fee
dis
Ma
With the introduction of transcatheter structural heart therapies, cardiologists are increasingly aware of the importance
of understanding anatomical details of left-sided heart structures. Understanding fluoroscopic cardiac anatomy can
facilitate optimal positioning and deployment of prostheses during transcatheter valve repair/replacement, left atrial
appendage occlusion, septal defect closure, and paravalvular leak closure. It is possible to use multislice computed to-
mography to determine optimal fluoroscopic viewing angles for such transcatheter therapies. The purpose of this paper is
to describe how optimal fluoroscopic viewing angles of left-sided heart structures can be obtained using computed
tomography. Two- and 3-chamber views are described and may become standard in the context of transcatheter
structural heart interventions. (J Am Coll Cardiol Intv 2014;7:947–57) © 2014 by the American College of Cardiology
Foundation.
S ince the introduction of transcatheter struc-tural heart therapies, cardiologists havebecome increasingly aware of the importance
of understanding anatomical details of left-sided car-diac structures (1). Many critical anatomical struc-tures comprise several components and are arrangedin a complex tridimensional geometry. Even thoughthese anatomical and functional components havebeen the topic of numerous publications (1,2), littleconsideration has been given to understanding theirconfiguration as appreciated under fluoroscopy (3).Understanding fluoroscopic cardiac anatomy canfacilitate optimal positioning and deployment of
m the *Department of Medicine, Division of Cardiology, McGill Univ
epartment of Surgery, Division of Cardiovascular Surgery, McGill Uni
epartment of Cardiovascular Surgery, German Heart Centre Munich, Mun
gy, Clinique Pasteur, Toulouse, France; kDepartment of Cardiovascular
epartment of Cardiology, Thoraxcentre, Erasmus Medical Centre, Rott
erventional Cardiology, University Hospital, Bern, Switzerland. Dr. Mart
sulting and lecture fees from Medtronic. Dr. Modine receives consultin
sulting fees from Medtronic and Boston Scientific. Dr. Windecker has rece
Jude Medical; and serves on the scientific advisory board of Cardialysis B
s from Medtronic. All other authors have reported that they have no rel
close.
nuscript received March 12, 2014; revised manuscript received May 2, 20
prostheses during transcatheter valve repair/replace-ment, left atrial appendage occlusion, septal defectclosure, and paravalvular leak closure. Commonly,these therapies are conducted using standard fluoro-scopic angulations irrespective of variations in anat-omy. It is possible that patient-specific fluoroscopicviewing angles can improve procedural safety andefficacy.
Multislice computed tomography (MSCT) multi-planar reconstruction of the aortic valvular complexhas enhanced patient selection and proceduralplanning for transcatheter aortic valve replacement(4). For example, MSCT affords physicians the
ersity Health Centre, Montreal, Quebec, Canada;
versity Health Centre, Montreal, Quebec, Canada;
ich, Germany; xDepartment of Interventional Cardi-
Surgery, University Hospital of Lille, Lille, France;
erdam, the Netherlands; and the #Department of
ucci is a proctor for Medtronic. Dr. Lange receives
g fees from Medtronic. Dr. van Mieghem receives
ived institutional research grants from Biotronik and
V. Dr. Piazza is a proctor for and receives consulting
ationships relevant to the contents of this paper to
14, accepted June 4, 2014.

FIGUR
The ve
(A and
is desc
angles
ABBR EV I A T I ON S
AND ACRONYMS
CAU = caudal
CRA = cranial
LAO = left-anterior oblique
MSCT = multislice computed
tomography
RAO = right-anterior oblique
Thériault-Lauzier et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 7 , N O . 9 , 2 0 1 4
Cardiac Fluoroscopic Anatomy Using MSCT S E P T E M B E R 2 0 1 4 : 9 4 7 – 5 7
948
opportunity to pre-select optimal x-ray fluo-roscopic viewing angles for deployment ofthe valve prosthesis (5–15). Such angle opti-mization may decrease procedure time, ra-diation exposure, and injected contrast agentvolume (15). It may reduce the risk of acutekidney injury (15) and paravalvular regurgi-tation (14). MSCT can also be used to deter-mine optimal fluoroscopic viewing angles for
transcatheter therapies targeting the mitral valvularcomplex, the left atrial appendage, the pulmonaryveins, and the atrial septum.
Therefore, the purpose of this paper is to describehow optimal fluoroscopic viewing angles of left-sidedheart structures can be obtained using computed to-mography (CT). We describe 2- and 3-chamber viewsthat may become standard in the context of left-sidedstructural heart interventions.
ATTITUDINAL DESCRIPTION OF ANATOMY
In our discussion, structures will be termed accordingto their attitudinally correct anatomical position (16).
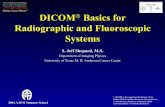
E 1 Geometry of the Optimal Projection Curve
ctor joining the x-ray source and the center point of the detector is d
B) The angular system (cranial [CRA]/caudal [CAU] and right anterio
ribed. (C) All vectors vd perpendicular to vector vs are optimal view
of all vectors vd for a particular structure of interest. (D) The optim
This implies that the subject is facing the observer andstanding upright. Thus, structures closer to theobserver are described as being anterior and thoserelatively farther away within the body are posterior.Components lying closer to the head are superior(i.e., cranial [CRA]) and those toward the feet are saidto be inferior (i.e., caudal [CAU]). Structures to theleft-hand side of the observer are right-sided andthose to the observer’s right are left-sided. Discussingheart structures in their attitudinal position is in per-fect agreement with nomenclatures used for CT andx-ray fluoroscopic imaging; this is not necessarily truewith echocardiography. The fluoroscopic screen por-trays the thorax in an upright orientation despite thepatient being in a supine position. Superior and infe-rior structures are appreciated in the upper and lowerhalves of the screen. The direction of fluoroscopicprojections is described based on 2 conventional an-gles, CRA/CAU and left anterior oblique (LAO)/rightanterior oblique (RAO) (Figures 1A and 1B). In theanteroposterior viewing angle (CRA/CAU 0�, LAO/RAO0�), right- and left-sided structures are found on theleft and right sides of the screen, respectively.
esignated vd, and the vector pointing along a structure of interest is vs.
r oblique [RAO]/left anterior oblique [LAO] angles) used influoroscopy
ing angles. The optimal projection curve is the plot of the fluoroscopic
al projection curve is shown for different cardiac structures.

FIGURE 2 Aortic Valve Sinuses
Multislice computed tomography (MSCT) double-oblique reslices are shown parallel to the aortic annulus at the level of the aortic sinus (A), just
above the aortic annulus (B), and at the annulus (C). The eye symbols describe the position of the x-ray detector in the corresponding
fluoroscopic view: blue corresponds to F and red to G. (D) The MSCT reslice is in the same orientation as the fluoroscopic view in F and shows
the right coronary aortic sinus (RCAS) between the noncoronary aortic sinus (NCAS) and left coronary aortic sinus (LCAS). (E) The MSCT reslice
is in the same orientation as the fluoroscopic view in G and shows the NCAS between RCAS and LCAS. The fluoroscopic angulations are indicated
in the figures. AR ¼ anterior-right; IL ¼ inferior-left; IR ¼ inferior-right; LA ¼ left-anterior; PL ¼ posterior-left; RP ¼ right-posterior; SL ¼superior-left; SR ¼ superior-right; other abbreviations as in Figure 1.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 7 , N O . 9 , 2 0 1 4 Thériault-Lauzier et al.S E P T E M B E R 2 0 1 4 : 9 4 7 – 5 7 Cardiac Fluoroscopic Anatomy Using MSCT
949
FLUOROSCOPIC ANATOMY USING MSCT
Fluoroscopy is used to guide the vast majority oftranscatheter cardiac procedures. Inherently, it is a2-dimensional imaging modality that requires theuser to select a viewing angle that provides accurateinformation on device positioning. For a particularstructure, an optimal viewing angle should minimizepositioning errors due to parallax. The goal of manytranscatheter procedures—such as valve implanta-tions, left-atrial appendage occlusions, septal defectclosures, and paravalvular leak occlusions—is toimplant a quasicylindrical device inside a highlyvariable anatomical structure. The fluoroscopic pro-jection that minimizes parallax during deploymentis such that the source-to-detector direction isorthogonal to the axis of symmetry of the anatomicalfeature of interest (Figure 1C). Based on this criterion,it is possible to determine an optimal CRA/CAU anglefor any given LAO/RAO angle. The plot of theoptimal combinations is called the optimal projection
curve (7,8,10–12,15). MSCT is a 3-dimensional imag-ing modality that is not affected by parallax. MSCTimages can be used to define the direction of struc-tures and produce an optimal projection curve(Figure 1D).
In addition to parallax errors, optimal viewangles should also minimize the overlap of anatomicstructures, a problem that also stems from the2-dimensional nature of fluoroscopy. In the contextof transcatheter interventions, some cardiac struc-tures must be distinguished in order to accuratelyimplant devices. The overlap of a highly attenuatinganatomical structure with the region of implantationmay reduce the contrast-to-noise ratio and com-promise visualization. Therefore, it is crucial to un-derstand which fluoroscopic angulations providemaximal separation between structures of interest.This understanding can be obtained from MSCTangiography, which depicts cardiac structures withrelatively high soft-tissue contrast, as well as hightemporal and spatial resolution.

FIGURE 3 Aortic Annulus
(A) The MSCT double-oblique reslice is at the level of the aortic annulus. The 2 eye symbols describe the position of the x-ray detector
in the corresponding fluoroscopic view: blue corresponds to B and red to E. (B) The MSCT reslice is in the same orientation as the
fluoroscopic view in C and shows the maximal annulus diameter (DMAX) in plane. (D) The MSCT reslice is in the same orientation as the view
in E and shows the minimal annulus diameter (DMIN) in plane. The fluoroscopic angulations are indicated in the figures. Abbreviations as
in Figures 1 and 2.
Thériault-Lauzier et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 7 , N O . 9 , 2 0 1 4
Cardiac Fluoroscopic Anatomy Using MSCT S E P T E M B E R 2 0 1 4 : 9 4 7 – 5 7
950
Fluoroscopy and MSCT share a common imagecontrast mechanism: x-ray attenuation. Conse-quently, it is possible to use MSCT volumetric data tosimulate fluoroscopic images. A ray-casting methodbased on this principle was used to generate thefluoroscopic images presented in this paper. Todemonstrate how MSCT may provide optimal fluo-roscopic viewing angles for left-sided heart struc-tures, we used an MSCT scan from a 66-year-oldmale patient with moderate functional mitralregurgitation. It is important to note that fluoro-scopic angulations are dependent on the specificorientation of the heart within the thorax, a param-eter that may vary considerably between patients(7,8,10–12,15). Although we describe general angula-tions, exact angulations may be determined for aspecific patient prior to an intervention. Measure-ment of fluoroscopic angulation from MSCT data canbe done with visualization software packages thatoffer double-oblique multiplanar reconstruction; theexact CRA/CAU and RAO/LAO angulations for aparticular structure can be obtained by analyzing theoblique sagittal and oblique transverse views,respectively.
AORTIC ROOT, VALVE, AND
LEFT VENTRICULAR OUTFLOW TRACT
The aortic root extends from the basal attachmentpoints of the aortic valve leaflets to their superiorattachment at the level of the sinotubular junction(17). The 3 leaflets form the limits of the right, left,and noncoronary aortic sinuses. Optimal fluoroscopicviews of the aortic root can be selected such that theview is perpendicular to the plane of the aorticannulus (Figures 2A to 2C). During transcatheter aorticvalve replacements, physicians often select a viewthat shows the right coronary sinus between thenoncoronary and left coronary sinuses (Figures 2Dand 2F). In the current patient, this view is obtainedusing a mild LAO and mild CAU angulation. Alterna-tively, a view with the noncoronary or left coronarysinus in the central position can also be obtained(Figures 2E and 2G). In this case, an LAO and CRAangulation is selected.
The aortic valve annulus is defined as the planarring of tissue that unites the most proximal point ofeach leaflet attachment line. The annulus is rarelycircular (18). Rather, it has a long and a short axis that

FIGURE 4 Mitral Valve Leaflets
(A) The MSCT double-oblique reslice is parallel to the mitral annulus best-fit plane and intersects the leaflets of the valve. The 2 eye symbols
describe the position of the x-ray detector in the corresponding fluoroscopic view: blue corresponds to C and red to F. (B) The MSCT reslice is in
the same orientation as the fluoroscopic view in C, which shows the aortic (A) and mural (P) leaflets without overlap. This view results in an
overlap of the 3 segments (1,2,3). The MSCT reslices show the mural (D) and aortic (E) leaflets, respectively. D and E are in the same orientation
as the fluoroscopic view in F, which shows the leaflet segments (1,2,3) without overlap, but results in an overlap of the A and P leaflets. The
fluoroscopic angulations are indicated in the figures. Abbreviations as in Figures 1 and 2.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 7 , N O . 9 , 2 0 1 4 Thériault-Lauzier et al.S E P T E M B E R 2 0 1 4 : 9 4 7 – 5 7 Cardiac Fluoroscopic Anatomy Using MSCT
951
can be appreciated using MSCT (19). Under fluoros-copy, the aortic annulus’s apparent diameter variesdepending on the view angle (Figure 3A). In the cur-rent patient, a mild LAO projection with minimalCRA/CAU angulation provides a view of the maximumdiameter (Figures 3B and 3D), whereas an extremeRAO and CAU view shows the minimum diameter(Figures 3C and 3E).
MITRAL VALVE
The mitral valve has 2 major leaflets commonlydescribed as being anterior and posterior. Relative tothe anatomical axes of the body, however, the leafletsare in an anterosuperior and posteroinferior orienta-tion. For simplicity, we describe these leaflets asaortic and mural, respectively. The Carpentier clas-sification recognizes 3 scallops in the mural leaflet(P1 to P3) and 3 corresponding segments in the aorticleaflet (A1 to A3) (20). A1P1 and A3P3 segments arelocated superoposterior and inferoanterior, respec-tively, with respect to A2P2 (Figure 4A). Emergingtranscatheter interventions require the positioning
of the delivery catheter in a precise position relativeto each leaflet and each segment. Understanding theleaflet configuration under fluoroscopy may easethis process. In the patient studied, an extreme RAOand CAU view can be used to maximally separate themural and aortic leaflets of the mitral valve(Figures 4B and 4C). In this view, however, the aorticsegments A1,2,3 overlap one another; such an overlapalso exists for mural segments P1,2,3. To separate theleaflet segment (1,2,3), we use an RAO and CRA pro-jection. In this view, mural and aortic leaflets overlapsuch that A1 overlaps P1, A2 overlaps P2, and A3
overlaps P3 (Figures 4D to 4F).The fibrous ring of the mitral valve annulus ex-
tends from the right and left trigones and encirclesthe mural leaflet of the mitral valve. The area offibrous continuity between trigones is commonlyreferred to as the aortic-mitral curtain (Figure 5A).Some designs of transcatheter mitral valve replace-ment devices are not axially symmetric and must bepositioned at a particular angle relative to themitral commissure. In the patient studied, the inter-commissural diameter of the mitral annulus, which

FIGURE 5 Mitral Valve Annulus
(A) The MSCT double-oblique reslice in is parallel to the mitral annulus best-fit plane. The 2 eye symbols describe the position of the x-ray
detector in the corresponding fluoroscopic view: red corresponds to C and blue to E. (B) The MSCT reslice is in the same orientation as the
fluoroscopic view in C, which shows the intercommissural diameter (DCC) of the mitral valve annulus and the right and left trigones maximally
separated. The MSCT reslice in B is in the same orientation as the view in C, which shows the aortomural diameter (DAM) of the annulus,
overlapping right (RTr) and left (LTr) trigones, and the aortic-mitral curtain (AMC) fully separated from the root of the aorta. The fluoroscopic
angulations are indicated in the figures. Abbreviations as in Figures 1 and 2.
Thériault-Lauzier et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 7 , N O . 9 , 2 0 1 4
Cardiac Fluoroscopic Anatomy Using MSCT S E P T E M B E R 2 0 1 4 : 9 4 7 – 5 7
952
is often the maximum diameter of the annulus, canbe appreciated using a mild RAO and CRA angu-lation (Figure 5B). This angulation is analogous to anechocardiographic 2-chamber view. Also in the pa-tient studied, an extreme RAO and CAU viewshows the aortomural diameter of the mitralannulus—often considered to be the minimumdiameter of the annulus (Figure 5C). This view isanalogous to a 3-chamber echocardiographic view.The aortic-mitral curtain is observed perpendicularlyand clearly separated from the left atrium and theaortic root. This view may be of particular interest tothose implanting transcatheter mitral valve bio-prostheses. Indeed, it can be used to assess theinteraction of the prosthesis with the left ventricularoutflow tract and could potentially reveal anobstruction or a deformation of the aortic-mitralcurtain.
PAPILLARY MUSCLES
Two papillary muscle divisions arise adjacent toeach other within the left ventricular cavity. Using
attitudinal description, it is illogical to describe thesedivisions as being either posteromedial or antero-lateral (16); in the vast majority of cases, the papillarymuscles lie in the posterior one-half of the left ven-tricular cavity and are relatively inferoanterior andposterosuperior to each other (Figure 6A).
The exact number, positioning, morphology, andthickness of papillary muscles can vary considerably(21). They are considered to be potential obstaclesto the deployment of transcatheter devices that pro-trude into the left ventricle such as mitral valveprostheses or ventricular septal defect closure de-vices. Therefore, it is important to understand theirconfiguration as observed under fluoroscopy. In thesubject studied, the papillary muscle divisions can bemaximally separated in a mild CRA projection withor without mild left or right angulation (Figures 6Band 6C) (2-chamber view). An extreme RAO and CAUprojection creates an overlap between the papillarymuscles (Figures 6D to 6F) (3-chamber view). Themural attachment of the papillary muscles is dia-metrically opposed to the anteriorly located leftventricular outflow tract.

FIGURE 6 Papillary Muscles
(A) The MSCT double-oblique reslice cuts through the longitudinal axis of the left ventricle. The 2 eye symbols describe the position of the
x-ray detector in the corresponding fluoroscopic view: red corresponds to C and blue to F. (B) The MSCT reslice is in the same orientation as the
fluoroscopic view in C, which shows a maximal separation between the superoposterior papillary muscles (SPPM) and the inferoanterior
papillary muscles (IAPM). The MSCT reslices show the SPPM (D) and IAPM (E), respectively. D and E are in the same orientation as the
fluoroscopic view in F, which shows an overlap between the SPPM and the IAPM. The fluoroscopic angulations are indicated in the figures.
Abbreviations as in Figures 1 and 2.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 7 , N O . 9 , 2 0 1 4 Thériault-Lauzier et al.S E P T E M B E R 2 0 1 4 : 9 4 7 – 5 7 Cardiac Fluoroscopic Anatomy Using MSCT
953
LEFT ATRIAL APPENDAGE
The left atrial appendage is a contractile extension ofthe left atrium that lies in its anterior, superior, andleft aspect. It varies considerably in shape and size, aswell as in the number of lobes formed within itslumen (22). The orifice of the left atrial appendage isoval (Figure 7A) and opens in the left atrium adjacentto and at an oblique angle with the mitral valveannulus (23). Transcatheter left atrial appendageclosure devices are deployed in the orifice of theappendage to prevent thrombus formation in patientswith atrial fibrillation. Some physicians size thesedevices based on fluoroscopic images acquired instandard angulations such as CRA 25� and RAO 25�. Inthe subject studied, the orifice of the appendage isappreciated en face in a highly LAO and CRA fluoro-scopic projection (Figures 7B and 7C). The minimumdiameter of the appendage orifice is appreciated in anRAO and mild cranial fluoroscopic view (Figures 7Dto 7F). This angulation can also be used to visualizethe ridge of tissue that separates the left atrialappendage orifice from the left superior pulmonaryvein ostium. The long diameter of the appendage
orifice can be appreciated in an LAO and CAU pro-jection (Figures 7G to 7I). This angulation results in anoverlap of the proximal segment of the left superiorpulmonary vein with the left atrial appendage.
ATRIAL SEPTUM
The atrial septum is a tissue partition betweenthe right and left atria. In a majority of patients, theperiphery of the septum is constantly thick andbecomes thin toward its center at the fossa ovalis,the embryologic remnant of the foramen ovale(24). In normal individuals, the septum is orientedobliquely with the right atrium lying anterior, right,and inferior to the left atrium (25) (Figure 8A). Theaortic root lies left and anterior to the atrial septum.In many procedures, a transseptal puncture is used togain access to the left atrium from the right atrium.An RAO view shows the septum with minimal overlapwith the aortic root. Having said this, a standardCRA/CAU 0� RAO 30� view is often used to confirmthat the puncture needle is positioned over theseptum and not the aortic root. In the subject studied,CRA/CAU 0� RAO 35� achieves minimal overlap

FIGURE 7 Left Atrial Appendage
(A and B) The MSCT double-oblique reslices are in the same orientation as the fluoroscopic view in C, which shows the left atrial
appendage (LAA) orifice en face and its proximity to the left superior pulmonary vein (LSPV). (D and E) The MSCT reslices are in the same
orientation as the view in F, which shows DMIN and maximally separates the appendage and the LSPV. (G and H) The MSCT reslices
are in the same orientation as the view in I, which shows DMAX and an overlap between the LAA and the LSPV. The eye symbols describe
the position of the x-ray detector in the corresponding fluoroscopic view: blue corresponds to C, red to F, and green to I. The fluoroscopic
angulations are indicated in the figures. IPR ¼ inferior-posterior-right; LA ¼ left atrium; SAL ¼ superior-anterior-left; other abbreviations
as in Figures 1 to 3.
Thériault-Lauzier et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 7 , N O . 9 , 2 0 1 4
Cardiac Fluoroscopic Anatomy Using MSCT S E P T E M B E R 2 0 1 4 : 9 4 7 – 5 7
954
(Figures 8G to 8I). An RAO and CAU angulation isselected to view the septum en face (Figures 8Band 8C). A puncture needle would point toward theimage in this angulation. In an LAO view (Figures 8Dto 8F), the septum is seen perpendicularly but over-laps the aortic root. In this view angle, the curvatureof a puncture needle would appear maximal becauseit would point directly to the right of the image.
DISCUSSION
The spatial configuration of cardiac anatomy asdepicted using fluoroscopy is difficult to understand.In effect, physicians often rely on pattern recognitionrather than tridimensional mental visualization
when performing image-guided interventions. Fluo-roscopic cardiac anatomy has been previouslydescribed in the context of electrophysiological in-terventions (26–28). This paper also describes fluo-roscopic cardiac anatomy, but it focuses on anatomyrelevant for structural heart interventions. This topichas not previously been covered in a systematicfashion.
As noted throughout the paper, several fluoro-scopic views may be particularly relevant for trans-catheter therapies. Among the different projectionsdescribed, 2 angulations are particularly noteworthy:1) the extreme RAO and CAU view, which we call3-chamber view; and 2) the mild RAO and CRA view,which we refer to as 2-chamber view. Figure 9

FIGURE 8 Atrial Septum
(A) The MSCT axial slice simultaneously cuts through the left ventricle (LV), left atrium (LA), right ventricle (RV), and right atrium (RA). It also
shows a cut through the atrial septum (AS). (B) The MSCT double oblique slice is in the same orientation as the fluoroscopic view in C and shows
the AS en face. (D, E, G, H) The MSCT slices show the relationship of the AS with the ascending aorta (Ao), superior vena cava (SVC), and the
inferior vena cava (IVC). (F) The view is in the same orientation as D and E and shows the overlap of the Ao and the SVC. (I) The view is in the
same orientation as G and H and shows that AS is posterior with respect to the aortic root (AR). The eye symbols describe the position of the
x-ray detector in the corresponding fluoroscopic view: blue corresponds to C, red to F, and green to I. The fluoroscopic angulations are
indicated in the figures. C/C ¼ cranial/caudal; other abbreviations as in Figures 1 and 2.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 7 , N O . 9 , 2 0 1 4 Thériault-Lauzier et al.S E P T E M B E R 2 0 1 4 : 9 4 7 – 5 7 Cardiac Fluoroscopic Anatomy Using MSCT
955
summarizes the anatomical structures that can bevisualized in these 2 fluoroscopic views. We believethat these 2 angulations may become a standardin the context of left-sided structural heart in-terventions, and in particular, transcatheter mitralvalve therapies.STUDY LIMITATIONS. In particular, a single MSCTscan in diastole was used, which explains why onlyapproximate angulations were described. Normalanatomical variations as well as pathological statescan have a strong influence on optimal viewing angles.In particular, ventricular hypertrophy, ventricular oratrial dilation, pulmonary hyperinflation, pulmonaryobstructive disease, obesity, and changes associated
with aging are among potential factors influencingfluoroscopic angulations. Furthermore, the use of apre-operative MSCT scan may not accurately reflectthe spatial position of anatomical structures once inthe catheterization laboratory. Respiratory motionmay affect the orientation of the heart. The patient’sarm position also differs between the 2 procedures;the arms are generally placed overhead duringMSCT scanning, whereas they are placed along thebody during the intervention. New technology suchas intraoperative C-arm cone-beam CT, also knownas rotational angiography, might alleviate theselimitations. Furthermore, tridimensional renderingsmay be overlaid over planar fluoroscopic images to

FIGURE 9 Standard Viewing Angles
Summary of anatomic structures as visualized under fluoroscopy in 2-chamber view (A) and 3-chamber view (B). Abbreviations as in Figure 4.
Thériault-Lauzier et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 7 , N O . 9 , 2 0 1 4
Cardiac Fluoroscopic Anatomy Using MSCT S E P T E M B E R 2 0 1 4 : 9 4 7 – 5 7
956
visualize the anatomy of structures targeted by trans-catheter therapies. In the future, the conceptof CT-based fluoroscopic viewing angles can be appliedto images obtained using these new technologies.
CONCLUSIONS
Herein we present a review of the fluoroscopic anat-omy of left-sided heart structures relevant for trans-catheter therapies. Optimal fluoroscopic angulations,which minimize parallax or overlap with other
clinically relevant structures, were described for theaortic valve, the mitral valve, papillary muscles, andthe atrial septum.
REPRINT REQUESTS AND CORRESPONDENCE: Dr.Nicolo Piazza, Division of Cardiology, Departmentof Medicine, McGill University Health Centre, TheRoyal Victoria Hospital, 687 Pine Avenue West, Mon-treal, Quebec H3A 1A1, Canada. E-mail: [email protected].
RE F E RENCE S
1. Van Mieghem NM, Piazza N, Anderson RH, et al.Anatomy of the mitral valvular complex and itsimplications for transcatheter interventions formitral regurgitation. J Am Coll Cardiol 2010;56:617–26.
2. Anderson RH, Ho SY, Becker AE. Anatomy of thehuman atrioventricular junctions revisited. AnatRec 2000;260:81–91.
3. Cosio FG, Anderson RH, Becker A, et al. Livinganatomy of the atrioventricular junctions: a guideto electrophysiological mapping. A ConsensusStatement from the Cardiac Nomenclature Study
Group, Working Group of Arrhythmias, EuropeanSociety of Cardiology, and the Task Force onCardiac Nomenclature from NASPE: North Amer-ican Society of Pacing and Electrophysiology. EurHeart J 1999;20:1068–75.
4. Schultz C, Moelker A, Tzikas A, et al. The use ofMSCT for the evaluation of the aortic root beforetranscutaneous aortic valve implantation: theRotterdam approach. EuroIntervention 2010;6:505–11.
5. Kempfert J, Falk V, Schuler G, et al. Dyna-CTduring minimally invasive off-pump transapical
aortic valve implantation. Ann Thorac Surg 2009;88:2041.
6. Dvir D, Kornowski R. Percutaneous aortic valveimplantation using novel imaging guidance.Catheter Cardiovasc Interv 2010;76:450–4.
7. Gurvitch R, Wood DA, Leipsic J, et al. Multislicecomputed tomography for prediction of optimalangiographic deployment projections duringtranscatheter aortic valve implantation. J Am CollCardiol Intv 2010;3:1157–65.
8. Kurra V, Kapadia SR, Tuzcu EM, et al. Pre-pro-cedural imaging of aortic root orientation and

J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 7 , N O . 9 , 2 0 1 4 Thériault-Lauzier et al.S E P T E M B E R 2 0 1 4 : 9 4 7 – 5 7 Cardiac Fluoroscopic Anatomy Using MSCT
957
dimensions: comparison between x-ray angio-graphic planar imaging and 3-dimensional multi-detector row computed tomography. J Am CollCardiol Intv 2010;3:105–13.
9. Tzikas A, Schultz C, Van Mieghem NM, deJaegere PP, Serruys PW. Optimal projection esti-mation for transcatheter aortic valve implantationbased on contrast-aortography: validation of aPrototype Software. Catheter Cardiovasc Interv2010;76:602–7.
10. Leipsic J, Gurvitch R, Labounty TM, et al.Multidetector computed tomography in trans-catheter aortic valve implantation. J Am CollCardiol Img 2011;4:416–29.
11. Arnold M, Achenbach S, Pfeiffer I, et al.A method to determine suitable fluoroscopicprojections for transcatheter aortic valve implan-tation by computed tomography. J CardiovascComput Tomogr 2012;6:422–8.
12. Binder RK, Leipsic J, Wood D, et al. Predic-tion of optimal deployment projection fortranscatheter aortic valve replacement:angiographic 3-dimensional reconstructionof the aortic root versus multidetectorcomputed tomography. Circ CardiovascInterv 2012;5:247–52.
13. Cockburn J, Trivedi U, de Belder A, Hildick-Smith D. Optimal projection for transcatheteraortic valve implantation determined from thereference projection angles. Catheter CardiovascInterv 2012;80:973–7.
14. Poon KK, Crowhurst J, James C, et al. Impact ofoptimising fluoroscopic implant angles onparavalvular regurgitation in transcatheter aortic
valve replacements–utility of three-dimensionalrotational angiography. EuroIntervention 2012;8:538–45.
15. Samim M, Stella PR, Agostoni P, et al. Auto-mated 3D analysis of pre-procedural MDCT to pre-dict annulus plane angulation and C-arm positioning:benefit on procedural outcome in patients referredfor TAVR. J Am Coll Cardiol Img 2013;6:238–48.
16. Anderson RH, Loukas M. The importance ofattitudinally appropriate description of cardiacanatomy. Clin Anat 2009;22:47–51.
17. Anderson RH. The surgical anatomy of theaortic root. Multimed Man Cardiothorac Surg2007 Jan 1;2007(102):mmcts.2006.002527.doi:10.1510/mmcts.2006.002527.
18. Piazza N, de Jaegere P, Schultz C, Becker AE,Serruys PW, Anderson RH. Anatomy of the aorticvalvar complex and its implications for trans-catheter implantation of the aortic valve. CircCardiovasc Interv 2008;1:74–81.
19. Schultz CJ, Moelker A, Piazza N, et al. Threedimensional evaluation of the aortic annulus usingmultislice computer tomography: are manufac-turer’s guidelines for sizing for percutaneousaortic valve replacement helpful? Eur Heart J2010;31:849–56.
20. Carpentier A. Cardiac valve surgery–the“French correction.” J Thorac Cardiovasc Surg1983;86:323–37.
21. Delgado V, Kapadia S, Marsan NA, Schalij MJ,Tuzcu EM, Bax JJ. Multimodality imaging before,during, and after percutaneous mitral valve repair.Heart 2011;97:1704–14.
22. Veinot JP, Harrity PJ, Gentile F, et al. Anatomyof the normal left atrial appendage: a quantitativestudy of age-related changes in 500 autopsyhearts: implications for echocardiographic exami-nation. Circulation 1997;96:3112–5.
23. Su P, McCarthy KP, Ho SY. Occluding the leftatrial appendage: anatomical considerations.Heart 2008;94:1166–70.
24. Schwinger ME, Gindea AJ, Freedberg RS,Kronzon I. The anatomy of the interatrial septum:a transesophageal echocardiographic study. AmHeart J 1990;119:1401–5.
25. Ho SY, McCarthy KP, Faletra FF. Anatomy ofthe left atrium for interventional echocardiogra-phy. Eur J Echocardiogr 2011;12:i11–5.
26. Farre J, Anderson RH, Cabrera JA, et al.Fluoroscopic cardiac anatomy for catheter ablationof tachycardia. Pacing Clin Electrophysiol 2002;25:76–94.
27. Farre J, Anderson RH, Cabrera JA, et al. Car-diac anatomy for the interventional arrhythmolo-gist: I. Terminology and fluoroscopic projections.Pacing Clin Electrophysiol 2010;33:497–507.
28. Wright M, Knecht S, Jaïs P. Intra-proceduraltechniques: fluoroscopy and angiography. In:Auricchio A, Singh J, Rademakers FE, editors.Cardiac Imaging in Electrophysiology. London:Springer, 2012:105–31.
KEY WORDS cardiac imaging, fluoroscopicanatomy, interventional imaging, multislicecomputed tomography, transcatheter cardiacintervention