Flow cytometry as a tool for the prognostic assessment of human neoplasia
12
Inl. J. Rndiarion Oncology Biol. Phys.. Vol. 12, pp. 625-636 0360-3016/86 $3.00 + .I0 Printed in the U.S.A. All rights reserved. Copyright 0 1986 Pergamon Press Ltd. 0 Original Contribution: Biology FLOW CYTOMETRY AS A TOOL FOR THE PROGNOSTIC ASSESSMENT OF HUMAN NEOPLASIA FRANCESCO MAURO, DR. SC.,’ LAURA TEODORI, DR. SC.,’ JOHANNES SCHUMANN, M.D.2 AND WOLFGANG G~HDE, PH.D.~ ‘Division of Physics and Biomedical Sciences, ENEA Casaccia, 00060 Roma, Italy; ‘Fachklinik Homheide, 3Department of Radiobiology, Universitlt Miinster, 4400 Miinster, F.R.G. Flow cytometry permits the quantitative description of neoplastic cell populations from the point of view of their cytogenetic and cytokinetic features. The advances in preparation of cellular monodispersed samples allow the examination not only of in vitro and hematological, but also of surgical, biopsy, endoscopic, and lavage specimens. The analysis of cytometric DNA content has evidenced the importance of (aneu)ploidy as a remarkable tumor marker. Tumors of different sites and, in some cases, stages and/or grades are characterized by a differential occurrence of diploid vs. aneuploid cell subpopulations and by the eventual presence of different stem cell lines within the same tumor. For certain classes of neoplasms, these parameters can be used for the early recognition of neoplasia and related to disease evolution and dissemination and to the results of therapy. Flow cytometry can also be used to evaluate the fraction of (cycling) cells in the S-phase and of proliferating cells (growth fraction). The percent of S cells can be extracted from cytometric DNA content histograms. Furthermore, the method of Bromodeoxyuridine (BrdUrd) incorporation has been recently introduced into flow cytometry. BrdUrd labeling in cycling cells can be detected either by the induction of quenching or enhancement of specific DNAdye fluorescence or by fluorescent anti-BrdUrd monoclonal antibodies. This approach has been confirmed by preliminary comparative tests on cultured cells, normal and malignant bone marrow, and human solid tumor specimens. These parameters, together with other cytometric parameters of potential importance for the cellular characterization of malignancy, offer a reliable and real time-saving tool for the prognostic assessment of human tumors and the predicting and monitoring of the results of therapy. Flow cytometry, Tumor heterogeneity, Tumor markers, Prognostic indicator, Cellular DNA content, Bromodeoxy- uridine incorporation. INTRODUCTION The development of flow cytometry has fostered signifi- cant advances in quantitative cytopathology of neoplastic disease.3,16 In particular, a cell-by-cell description of the cellular heterogeneity in terms of ploidy level(s), occur- rence of multiclonality and proliferative patterns-factors that may account for the diverse clinical course and ther- apeutic results of comuarablv staged and treated neo- piasms-have become -possidle.4,734.38 At present, new cytometric parameters, referring to various cellular con- stituents and properties, are being added to the initial one (cellular DNA content), thus, allowing further recognition and characterization of tumor cell clones.4322 Exciting ap- plications in both basic tumor biology and clinical on- cology are, therefore, possible. In the present investigation, the incidence of aneuploidy, ploidy level(s), multiclonality, and S phase frequency analyzed by flow cytometry in dif- ferent groups of human solid tumors as indicators of the cellular heterogeneity of neoplasms, are reported. Fur- thermore, the prognostic implications of these cellular properties are discussed. METHODS AND MATERIALS A major technical requirement for the use of flow cy- tometry is the preparation of single cell suspensions from solid tissue samples. This problem is not relevant, of Presented at the Third Rome International Symposium, May 1985. Reprints requests to: Dr. Laura Teodori, Laboratory of Do- simetry and Biophysics, ENEA Casaccia, Via Anguillarese 30 1, 00060 Roma, Italy. Part of this work has been partially supported by Deutsche Krebshilfe e.V. Acknowledgments-The authors would like to thank Dr. Mar- 625 cello Span6 for his invaluable help and criticism; Mrs. Ingeberg Spies and Gudrun Striker for their skillful technical assistance. We would also like to thank Dr. Donatella Tirindelli-Danesi for her helpful cooperation in discussing the clinical aspects and Ms. T. Nicola Sinclair, B.A., for her skillful assistance in the preparation of the manuscript. Accepted for publication 27 November 1985.
-
Upload
francesco-mauro -
Category
Documents
-
view
217 -
download
4
Transcript of Flow cytometry as a tool for the prognostic assessment of human neoplasia

Inl. J. Rndiarion Oncology Biol. Phys.. Vol. 12, pp. 625-636 0360-3016/86 $3.00 + .I0 Printed in the U.S.A. All rights reserved. Copyright 0 1986 Pergamon Press Ltd.
0 Original Contribution: Biology
FLOW CYTOMETRY AS A TOOL FOR THE PROGNOSTIC ASSESSMENT OF HUMAN NEOPLASIA
FRANCESCO MAURO, DR. SC.,’ LAURA TEODORI, DR. SC.,’ JOHANNES SCHUMANN, M.D.2 AND WOLFGANG G~HDE, PH.D.~
‘Division of Physics and Biomedical Sciences, ENEA Casaccia, 00060 Roma, Italy; ‘Fachklinik Homheide, 3Department of Radiobiology, Universitlt Miinster, 4400 Miinster, F.R.G.
Flow cytometry permits the quantitative description of neoplastic cell populations from the point of view of their cytogenetic and cytokinetic features. The advances in preparation of cellular monodispersed samples allow the examination not only of in vitro and hematological, but also of surgical, biopsy, endoscopic, and lavage specimens. The analysis of cytometric DNA content has evidenced the importance of (aneu)ploidy as a remarkable tumor marker. Tumors of different sites and, in some cases, stages and/or grades are characterized by a differential occurrence of diploid vs. aneuploid cell subpopulations and by the eventual presence of different stem cell lines within the same tumor. For certain classes of neoplasms, these parameters can be used for the early recognition of neoplasia and related to disease evolution and dissemination and to the results of therapy. Flow cytometry can also be used to evaluate the fraction of (cycling) cells in the S-phase and of proliferating cells (growth fraction). The percent of S cells can be extracted from cytometric DNA content histograms. Furthermore, the method of Bromodeoxyuridine (BrdUrd) incorporation has been recently introduced into flow cytometry. BrdUrd labeling in cycling cells can be detected either by the induction of quenching or enhancement of specific DNAdye fluorescence or by fluorescent anti-BrdUrd monoclonal antibodies. This approach has been confirmed by preliminary comparative tests on cultured cells, normal and malignant bone marrow, and human solid tumor specimens. These parameters, together with other cytometric parameters of potential importance for the cellular characterization of malignancy, offer a reliable and real time-saving tool for the prognostic assessment of human tumors and the predicting and monitoring of the results of therapy.
Flow cytometry, Tumor heterogeneity, Tumor markers, Prognostic indicator, Cellular DNA content, Bromodeoxy- uridine incorporation.
INTRODUCTION
The development of flow cytometry has fostered signifi- cant advances in quantitative cytopathology of neoplastic disease.3,16 In particular, a cell-by-cell description of the cellular heterogeneity in terms of ploidy level(s), occur- rence of multiclonality and proliferative patterns-factors that may account for the diverse clinical course and ther- apeutic results of comuarablv staged and treated neo- piasms-have become -possidle.4,734.38 At present, new cytometric parameters, referring to various cellular con- stituents and properties, are being added to the initial one (cellular DNA content), thus, allowing further recognition and characterization of tumor cell clones.4322 Exciting ap-
plications in both basic tumor biology and clinical on- cology are, therefore, possible. In the present investigation, the incidence of aneuploidy, ploidy level(s), multiclonality, and S phase frequency analyzed by flow cytometry in dif- ferent groups of human solid tumors as indicators of the cellular heterogeneity of neoplasms, are reported. Fur- thermore, the prognostic implications of these cellular properties are discussed.
METHODS AND MATERIALS
A major technical requirement for the use of flow cy- tometry is the preparation of single cell suspensions from solid tissue samples. This problem is not relevant, of
Presented at the Third Rome International Symposium, May 1985.
Reprints requests to: Dr. Laura Teodori, Laboratory of Do- simetry and Biophysics, ENEA Casaccia, Via Anguillarese 30 1, 00060 Roma, Italy.
Part of this work has been partially supported by Deutsche Krebshilfe e.V. Acknowledgments-The authors would like to thank Dr. Mar-
625
cello Span6 for his invaluable help and criticism; Mrs. Ingeberg Spies and Gudrun Striker for their skillful technical assistance. We would also like to thank Dr. Donatella Tirindelli-Danesi for her helpful cooperation in discussing the clinical aspects and Ms. T. Nicola Sinclair, B.A., for her skillful assistance in the preparation of the manuscript.
Accepted for publication 27 November 1985.

626 1. J. Radiation Oncology 0 Biology 0 Physics April 1986, Volume 12, Number 4
course, in the instance of leukemia and other hematolog- ical diseases or when liquid samples of exfoliative materials can be collected. As far as solid tumors are concerned, the preparation procedures presently available, based on mechanical methods and/or the use of enzymes, yield sat- isfactory suspensions of isolated cells or nuclei.34 Unfor- tunately, the question concerning the degree of represen- tativeness of biopsy and even surgical specimens is still open and multiple samples from the same site should be analyzed whenever possible. In fact, it would be safe to assume that the frequency of cytometrically detected aneuploidy may vary according to the accuracy of sam- pling, preparation and measurement, and apparatus res- olution.
Another major requirement concerns the availability of specific, quantitatively binding fluorochromatic probes, which are appropriate to adequately describe the cyto- genetic, phenotypic and proliferative diversity of the can- cer cells.23*35 The search for preparation and staining pro- cedures, such that cells can be analyzed and sorted out while still in viable conditions, is still under way.39
channel number
Furthermore, to perform these kinds of studies, a flow cytometer has to be used routinely and, therefore, should be characterized by an economic performance in terms of effort, time and cost. In the present study, a pulse cy- tophotometer* and, more recently, a flow cytometert- both mercury lamp apparatuses-have been used.
RESULTS
DNA content as a tumor marker After the introduction in flow cytometry of relatively
DNA-specific fluorescent dyes, the measurement of cel- lular relative DNA content has been a main approach for the characterization of human tumors. DNA content ab- normalities, somehow incorrectly, but currently referred to as cytometric aneuploidies, clearly reflecting the pres- ence of chromosomal abnormalities (and not only vari- ations in the chromosome number), have been consis- tently observed in tumor cell populations (e.g., 4,36). On the contrary, cytometric analyses of normal and inflam- matory tissues or of benign tumors all have shown a nor- mal diploid DNA content, with the exception of some “pre-cancerous” conditions, as discussed below. By now, a term defined as DNA index (DI), referring to the ratio of modal DNA fluorescence of abnormal to normal Gi,” cells, is commonly accepted to quantify cytometric ploidy. I9
channel number
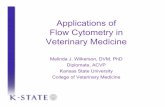
Fig. 1. Representative DNA distribution histograms of a tumor (breast carcinoma) biopsy specimen. Top panel: Mixture of tu- mor and normal cells from the same patient; the first peak on the left represents the diploid population. Bottom panel: Tumor cells only; note the decreased amount of diploid cells.
patient. Human and animal blood mononuclear cell standards can also be used and should be considered mandatory in certain cases.
Tumor samples analyzed in terms of flow cytometri- tally determined DNA content may exhibit the presence of both a diploid and at least one aneuploid cell subpop- ulations. The diploid cell peak can be safely identified by addition of cells from adjacent normal tissue (Fig. 1, top panel) and/or lymphocytes from the blood of the same
The incidence of cytometric aneuploidy in solid tumors of different site and histology has been under study by different groups. In Table 1, we report the data of the two multi-institutional groups represented by the authors of the present paper. These two groups follow a cooperative approach involving the use of the same preparation and staining methods (mithramycin and ethidium bromide
* ICP 22 pulse cytophotometer, Ortho, Westwood, MA. t PAS II flow cytometer, Partec, Arlesheim, Switzerland.

Human neoplasia assessment with flow cytometry 0 F. MAURO et al. 621
Table 1. Incidence of cytometrically determined DNA abnormalities observed in the human solid tumors analyzed
Site
Esophagus Stomach Colon-rectum
Lung (non-small-cell) Lung (microcytoma)
Breast Ovary Cervix Endometrium
Kidney Prostate Bladder Testis
Head and neck Skin (malignant melanoma) Skin (squamous) Skin (basal)
Soft tissue Bone (osteosarcoma)
Total Total (ENEA + Miinster)
Number of cases
11 36 33
98 4
54 4
13 14
16 25 29
9
343 2419
ENEA group Mtinster group
Aneuploid Multiclonal Number Aneuploid MulticlonaI cases (%) cases (%) of cases cases (W) cases (%)
11 (100) 7 (63) 30 (83) 8 (22) 21 (64) 12 (36) 53 43 (81) 15 (28)
92 (94) 49 (50) 3 (75) 2 (50) 41 34 (83) 18 (44)
34 (63) 9 (17) 118 90 (76) 26 (22) (609) 0
9 1 (8) 6 (43) 5 (37)
13 (81) 3 (19) 8 (32) 4 (16)
12 (46) 4 (15) 112 95 (85) 24 (21)
9 (100) 6 (67) 721 548 (76) 94 (13) 298 245 (82) 57 (19) 509 95 (19) 36 (7)
54 51 (95) 16 13 (81)
248 (72) 114 (33) 2076 1241 (58) 270 (13) 1489 (61) 384 (16)
are used as combined fluorescent dyes) and criteria for analysis.43 The incidence of aneuploidy appears to vary among different sites and histologies, from 19% for skin (basal cell carcinoma) to 100% for esophagus and head and neck (squamous cell carcinoma). The data obtained by the two groups are in very good agreement, when tu- mors of the same site are analyzed. A relatively good agreement can also be observed with the data of various authors collected in the most recent review by Barlogie et aL4 the discrepancies (e.g., prostate and bladder) likely resulting from the respective number of cases.
The eventual occurrence of cytometric aneuploidy in “pre-cancerous” conditions is of obvious importance, since it could pinpoint those lesions destined to malignant evolution. At present, as indicated in Table 2, aneuploidy has been observed for some congenital melanocytic nevi, chronic atrophic gastritis, ulcerative colitis, and breast be- nign lesions. With the exceptions of the latter group, cases in which the same patient has exhibited, at a later explo- ration, a definitively neoplastic lesion, have been de- scribed. However, the question whether such aneuploidies refer to actual “pre-cancerous” conditions or to early forms of tumors in situ or just represent instances of er- roneous pathological classification, is still open. Aneuplo- idy has been observed also in pre-leukemia, angioim- munoblastic lymphoadenopathy, and benign monoclonal gammopathy.
Flow cytometrically determined DNA content appears to be a remarkable cellular marker of neoplasia, and, therefore, a potentially important diagnostic tool. Ac- tually, it is the only tumor marker we are aware of that exhibits a false-positive rate close to 0% (the exception being due to sampling errors or to problems about the
Table 2. Incidence of cytometrically determined DNA abnormalities in “pre-cancerous” lesions
Lesion Number Aneuploid of cases cases (a)
Congenital melanocytic 46 4 (9) Miinster group nevi
Acquired nevocellular 376 0 Mtinster group nevi
Various benign skin 207 0 Mtinster group lesions
Breast Benign lesions 16 2 (12) ENEA group Breast benign lesions 18 3 (17) Weiss et aLdl Chronic atrophic 25 9 (36) ENEA group
gastritis Ulcers and other 29 0 ENEA group
benign gastric lesions Ulcerative colitis 51 g (16) Hammarberg
et al. ” Ulcerative colitis 3 1 ENEA group Normal tissue Over 4000 0 Several groups

628 I. J. Radiation Oncology 0 Biology 0 Physics April 1986, Volume 12, Number 4
actual significance of aneuploid “pre-cancerous” condi- tions), even if the false-negative rate can be quite large. This has been well-demonstrated not only by the data of the various groups (Table 1 and Barlogie et d4), but, in particular, by a large screening of bladder irrigation spec- imens carried out at the Memorial Sloan-Kettering Cancer Center.*l Regarding statistics, screening programs based on markers with low rates of false-negatives should be preferred, and not vice versa. Furthermore, the introduc- tion for parameters other than DNA content in two-pa- rameter flow cytometric analysis may well diminish the false-negative rate for certain tumor sites.
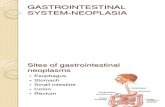
Flow cytometric analysis of DNA content has also shown the occurrence of more than one aneuploid cell subpopulation in the same tumor, that is, the presence of multiple tumor stem cell lines (clones) (Fig. 2). The data are reported also in Table 1 and show a large variability among different tumors, from a very low incidence up to about two-thirds of the total cases (esophagus and head and neck). The technical detection of multiclonality may depend upon the procedure used and the analysis of mul- tiple samples from the same tumor. The number of aneu- ploid clones observed, up to a maximum of five in the instance of non-small-cell carcinoma of the lung and of head and neck, may well represent an index, at the cellular level, of tumor heterogeneity. Tumors with a high fraction of aneuploid cases also exhibit a high fraction of multi- clonal cases (e.g., lung).
The collection of a relatively large number of cases al- lows further analysis of the relative degree of tumor het- erogeneity in terms of DNA content. As indicated in Table 3, the differences of the DNA index (DI) mean and range; the frequency of subcategories of aneuploidy, such as, hy- poploid (DI < 1); and the maximum number of clones observed, are reported.
Clearly, the problem of the evolution of aneuploidy in tumors is strictly linked to that of clonal evolution of neo- plasia. It is difficult to attribute the differences reported above (Tables 1 to 3) to actual intrinsic differences among various tumors and/or to the fact the diseases in different stages of their natural history are being analyzed. The distributions of the DNA indices for the solid tumor clones, analyzed by our two groups, are shown in Figures 3 and 4, respectively. The distributions exhibit the same maximum around diploidy, but differ in the position of the secondary maximum around triploidy or tetraploidy. However, apart from the technical problem of discrimi- nating tetraploid GI,O cells vs. diploid G2/M cells, this discrepancy seems to be a result of the different compo- sition of the overall tumor populations tested (Tables I and 2). Actually, the majority of tumor sites appear char- acterized by DNA indices clustered around subtetraploid values (e.g., testicular tumors in Fig. 5). A similar obser- vation for spontaneous canine tumors has been reported by other authors.20 Our own preliminary studies confirm such an observation as far as small domestic carnivora are concerned, but not for spontaneous tumors in labo-
1 Al
channel number
A2
channel number
Fig. 2. Representative DNA distribution histograms with the presence of more than one aneuploid tumor stem cell line. In both tumors, two aneuploid subpopulations can be observed. The histograms refer to a stomach (top panel) and a colon (bot- tom panel) carcinoma. D represents the diploid peak; Al rep- resents the first aneuploid cell subpopulation and A2 the second aneuploid cell subpopulation.
ratory mice, where the aneuploid cases cluster around tetraploidy.28
Speculation about the development of aneuploidy in transformed cells has produced two main hypotheses. The first is based on the initial occurrence of tetraploidy fol- lowed by a gradual cellular loss of DNA content because of unbalanced losses of chromosomal materia13(j and, eventually, by further endoreduplication to produce clones with higher ploidy levels. The second simply assumes a gradual, variable increase of chromosomal material, lead- ing to conditions of increasing hyperdiploidy (hypodip- loidy being caused by a similar process in the opposite direction). Apart from the oversimplification of these hy- potheses, the problem is difficult to deal with as far as

Site
Human neoplasia assessment with flow cytometry 0 F. MAURO et al.
Table 3. Levels of cytometric aneuploidy observed in the human solid tumors analyzed
Miinster group ENEA group
DNA DNA DNA DNA Aneuploid index index Aneuploid index index Hypoploid
cases mean range cases mean range cases (%)
629
Max no. clones
Esophagus Stomach Colon-rectum
11 1.59 30 1.70 21 1.60
Lung
Breast Gynecologic tumors
Kidney Prostate Bladder Testis
43 1.58 1.06-3.64
34 1.58 0.75-3.40
74 1.67 1.05-2.90
77 1.84
30 1.62 15 1.55
13 1.40 8 1.33
12 1.32
0.75-2.40 0.76-3.13 0.86-2.7 1
0.83-4.9 1
0.82-2.59 0.74-2.2 1
0.60-1.87 0.70-1.87 1.06-2.6 1
78 1.54 1.05-3.00
Head and neck 9 1.86 1.06-8.00
Skin (malignant melanoma) 548 1.65 1.05-4.55 Skin (squamous) 245 1.82 1.05-3.20 Skin (basal) 95 1.95 1.10-2.40
Soft tissue 51 1.68 1.10-2.60 Bone (osteosarcoma) 13 1.70 1.15-3.00
1/t 1 (9) 2 3136 (8) 4 l/33 (3) 3
8142 ( 19) 5
4148 (8) 3 9128 (32) 4
6/16 (22) 5 l/26 (4) 3
0 2
0 5
“spontaneous” human solid tumors are concerned. Our observations on gastric tumors indicate an increase of aneuplo
“0.
30
20
10
0
idy r level (Fig. 6) from (aneuploid) chronic
L_
up to 91
atrophic gastritis to early stages and then to advanced stages of gastric adenocarcinoma.33 These observations appear to favor the second hypothesis. However, both hy-
512 CLONES FROM
SOS DIFFERENT TUMORS
l-4 6 clones at
l-l hlqher indiccc
0 1 2 3
ml\ INOI:X
Fig. 3. Distribution of the DNA indices of all solid tumor clones analyzed by the ENEA group.

630 I. J. Radiation Oncology 0 Biology 0 Physics April 1986, Volume 12, Number 4
Fig. 4. Distribution of the DNA indices of all solid tumor clones analyzed by the Miinster group.
potheses and combinations of the two may be true and have different relevance in various tumors.
The origin, nature, and evolution of DNA abnormal- ities are clearly important to define the cellular basis of the natural history of neoplasia and, in particular, the development of tumor heterogeneity. In this regard, even if the problem is not yet solved, several correlations have been empirically established between cytometric ploidy and clinical parameters of prognostic significance. It is already known that, in solid tumors, survival appears to be adversely affected by increasing DNA index, as reported
for bladder,‘7*2’ prostate,36 and colon cancer.42 In our own experience (Table 4 and Teodori et c~f.~~), we demonstrated a very good correlation, for non-small-cell carcinoma of the lung, between the tumor DNA indices (DI) and the tumor volume doubling time (DT) (as evaluated by serial radiography),24 and between the DNA index (or a com- bination of the latter two parameters) and patient survival. This could be of particular importance to establish the prognosis of those cases where a serial evaluation of the tumor volume is not possible.
The occurrence of cytometric aneuploidy appears to
r N- 66 TLSTXCULAR TUMORS
Fig. 5. Distribution of the DNA indices of all testicular tumors.

Human neoplasia assessment with flow cytometry 0 F. MAURO et al 631
r -- -. I I
I .-- _l
!-‘_‘l
! i I . i
- CHRONIC ATjXf'tilC GASTRITIS
-me STIXACH ADENOCA. (ENDOSCOPY)
_I_'_' STU~H mm0cA, (SURGERY) I i i
~‘-“‘~
! ! i i
a’--; ! i
_._._il ,i._.,! i
I I i
I 1 i I I
i _ --.I
I r-7; I 1
! (!’ f
1.0 1,2 I.4 1.6 1.8 2.0 >2
DNA INOEX
Fig. 6. Frequency of the DNA indices of the aneuploid clones in samples from patients affected by: Chronic atro- phic gastritis (- ); early stages of gastric adenocarcinoma (- - -); advanced stages of gastric adenocarcinoma (-.-.-).
correlate with stage of colon-rectum carcinoma and with the level of invasion, tumor thickness, and the occurrence of metastasis in malignant melanoma.
Table 4. Examples of correlation between cytometric ploidy and clinical parameters
Site Cytometric
ploidy Clinical
parameters P
Lung Dl vs. DT
Dl vs. survival
Dl + DT vs. survival
Colon-rectum Ploidy vs. stage
Melanoma Ploidy vs. invasion
Ploidy vs. metastasis
ForDl>2or<l <0.02 DT ~90 days
ForDl>2or<l <o.o 1 15/18 dead at 18 mo.
For 2 > Dl > 1 1 l/17 alive at 18 mo.
<o.oo 1
Diploid l/5 < 0.01 C+D
Aneuploid 13/I 5 C+D
II 16% aneuploid Ill 35% IV 66% V 85%
Primary 4 1% aneuploid
Metastatic 75% aneuploid
Incorporated BrdUrd as a proliferation marker The attempts to investigate the proliferative character-
istics of tumor cell populations have been a relevant part of cell biology research in the past decades. Determining the parameters describing cell cycle progression and pro- liferative compartments could be important in cancer prognosis (e.g., Tubiana et a13’) and therapy with the purpose of achieving preferential effects on neoplastic cells.
Until recently, both the percent of cells in the S phase and the growth fraction (percent of proliferating cells), together with several cycle-related parameters, have been determined by methods based on DNA incorporation of labeled DNA precursors (H3-thymidine) and autoradio- graphic analysis of labeled cells, a time consuming and delicate method, especially when the percent labeled mi- toses (PLM) is evaluated.
Recently, other in vitro techniques have been devel- oped, such as, the use of the primer-available DNA-de- pendent DNA polymerase (PDP) activity, to determine autoradiographically the proliferative compartment.27,30 However, these techniques are also time consuming and have resolution limits. More recently proposed is the ap- proach based on the incorporation of 5-bromodeoxyuri- dine (BrdUrd), a halogenated analogue of thymidine, pre- viously well-known for its radiosensitizing properties. I3
The detection of cells with BrdUrd-substituted DNA regions can be achieved in two ways. The first is incor- poration of BrdUrd into DNA strands resulting in a modification of DNA-specific dye fluorescence. For

632 I. J. Radiation Oncology 0 Biology ??Physics April 1986, Volume 12, Number 4
example, BrdUrd enhances the fluorescence of DNA stained with chromomycin, olivomycin and mithramycin and quenches the fluorescence of other dyes, such as, ac- ridine orange, ethidium bromide, propidium iodide, and Hoechst 32258.6.8,3’
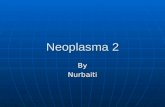
The method based on the monitoring of BrdUrd quenching of acridine orange fluorescence’ has been used by our group to evaluate the proliferative compartment of normal and neoplastic cell populations from human bone marrow aspirates. Particular attention has been paid to the BrdUrd dose-dependence of the effect to achieve a satisfactory fluorescence reduction and a reliable evalu- ation of the amount of cells unexposed and exposed to BrdUrd32 (26 PM, 72 hr of incubation in liquid culture starting immediately after aspiration). In the histograms of Figures 7 and 8, a peak (upper left) is clearly shown and permits a quantitative evaluation of the fraction of BrdUrd-labeled cells. The same results can also be ana- lyzed by a two-parameter display referring to cellular DNA (“green” fluorescence, eventually quenched) on the hor- izontal axis and RNA content (“red” fluorescence) on the vertical axis. In this way, it can be observed that, in this system,” proliferating cells are also characterized by a relatively high amount of RNA. Furthermore, Figures 7
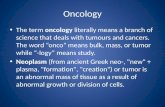
and 8 refer to the same patient on which the Budr tech- nique had been applied before and after chemotherapy treatment (the reduction in the magnitude of the quenched peak indicates an appreciable decrease of the proliferative compartment after chemotherapy). Our data on a first group of patients are shown in Table 5. In spite of the low number of patients, the three groups tested-normal bone marrow; chronic myeloid leukemia; acute myeloid and lymphblastic leukemia-are characterized by signif- icantly different values.
This approach is of extreme interest, but it cannot be used for “pulse” incorporation treatments (since the extent of quenching would be too low to be appreciably detected) and, therefore, for the estimation of the percent S phase cells. Furthermore, this approach cannot be easily applied to samples from solid tumors, because of the difficulties of the relatively long-term in vitro culture.
The second way to detect BrdUrd-labeled cells is by the use of a monoclonal antibody directed against the analogue. I2 The method for producing a FITC (Fluores- cein-isothiocyanate) labeled goat anti-mouse XgG anti- body to fluorescently label the bound anti-BrdUrd probe has‘ been described (such an implement is commercially available.) At present, the technique’2,22 is based on a
Fig. 7. Flow cytometrically determined DNA/RNA content of an untreated human chronic myeloid leukemia after BrdUrd incorporation. Left upper panel: DNA (x axis) vs. RNA (y axis) scattergram. Right upper panel: Channel A shows the DNA distribution and channel B the RNA distribution. Bottom panel: DNA/RNA distribution tridimensional display.

Human neoplasia assessment with flow cytometry 0 F. MAURO ef al 633
Fig. 8. Data similar to those of Figure 7 for the same patient after chemotherapy treatment. The results appear to indicate a decrease in the proliferating cell subpopulation. Note in channel A the presence of both a quenched (left) and a regular (right) peak. In control samples not exposed to BrdUrd, which are not shown here, the regular peak only can be appreciated. The scattergram and the tridimensional display show that quenched cells (left cluster of the scattergram) have the tendency to be characterized by higher cellular RNA content.
“pulse” incorporation of the analogue, followed by ex- posure to the antibody after fixation and DNA denatur- ation. The fraction of labeled cells can be assessed under a fluorescence microscope by one-parameter flow cyto- metry or even by two-parameter flow cytometry in terms of DNA (stained with a specific dye) vs. BrdUrd to eval- uate the growth fraction.
The results obtained following this approach on an in vitro system are shown in Table 6. A comparative analysis indicates a very good agreement in the evaluation of the
Table 5. Percent of proliferating cells in some human bone marrow cases by BrdUrd/acridine orange quenching
Number of patients
Percent P cells + SD
Normal bone marrow (NBM) 4 23.1 + 3.0 Chronic myeloid leukemia
(CML) 3 53.3 + 16.8 Acute myeloid leukemia (AML)
and acute lymphoblastic leukemia (ALL) 4 6.6 +- 2.9
NMB vs. CML: 0.02 > p > 0.01; NBM vs. AML + ALL: p < 0.00 1; CML vs. AML + ALL: 0.0 1 > p > 0.00 1.
percent S phase cells between the methods based on the monoclonal antibody (after 50 PM BrdUrd), Hithymi- dine autoradiographic labeling, and hydroxyurea ( 10
Table 6. Percent of S-phase cells in experimental systems
DNA BrdUrd H3TdR HOU System content monoclonal labeling killing
CHO cells (in vitro)
Log-phase (early)
Log-phase (middle)
Log-phase (late)
Plateau-phase Ehrlich ascite
(in viva) 2 days growth 4 days growth 6 days growth 8 days growth 10 days growth 12 days growth 14 days growth
66.8 57.8 61.7
57.3 55.1 58.0 60.0
38.9 40.2 36.9 26.4 8.7 7.9 10.5
53.5 54.5 51.0 39.8 36.9 35.3 47.8 34.6 34.9 39.1 25.4 30.5 26.0 21.1 23.4 25.3 13.2 12.8 28.0 10.5 10.4

634 1. J. Radiation Oncology 0 Biology 0 Physics April 1986, Volume 12, Number 4
mM), supposedly specific killing of S phase cells. On the contrary, different results are obtained (higher S phase values) for cells in the plateau phase of growth, when a fourth method, based on the estimation of the S phase fraction by analysis of the flow cytometric DNA content distribution, is used. Such an apparent discrepancy can be fully explained on the basis of the occurrence of Q (quiescent) cells arrested in the S phase.1° The results ob- tained on an Ehrlich ascite tumor system in vivo (Table 6) growing with a Gompertzian trend and characterized by a gradual increase of Q cells, fully confirm such an explanation.
Finally, preliminary data on the BrdUrd in vitro label- ing, detected by the monoclonal antibody method of hu- man solid tumor biopsy samples, are presented in Table 7 (unpublished data, Langer and Gohde, 1985). In these tests, the percent of S phase cells has also been compar- atively evaluated on the basis of the DNA content his- togram. The data of Table 7 indicate, once again, that the BrdUrd method yields percentage values lower than those
Table 7. Percent of S-phase cells in the human solid tumors analyzed
Site BrdUrd
monoclonal DNA
content
1. Bladder 17.3 36.5 2. Bladder 19.6 9.1 3. Bladder 24.2 19.7
Mean 20.4 21.8
4. Prostate 4.7 15.8 5. Prostate 4.3 14.0
Mean 4.5 14.9
6. Kidney 13.7 4.0 7. Kidney 1.9 4.4 8. Kidney I.0 26.0 9. Kidney 28.5 38.0
10. Kidney 16.7 24.3
Mean 12.2 19.3
11. Testis 12. Testis (a)
(b) Mean
11.5 15.2 9.6 Il.6
10.3 17.7
10.5 14.8
13. Penis
14. Skin (basal) 15. Skin (basal)
Mean
4.6 14.1
4.7 2.9 3.6 10.7
8.3 6.8
16. ND 1.9 4.4 17. ND (a) 7.8 6.1
(b) 8.5 6.6 18. ND 4.1 26.5 19. ND 10.7 16.8
Mean of all cases 10.0 f 7.6 SD 15.4 f 10.2 SD (p between 0.06 and 0.05).
We recognize the collaboration of Dr. E.M. Langer (Mtinster) for the work reported in this table.
estimated by DNA flow cytometry, but similar to those reported by others (e.g., Stee129) or previously observed by us, for the same tumors with the H3-thymidine method.
DISCUSSION
From the preceding presentation of published and original data, it should be clear that flow cytometry is becoming a powerful tool in the diagnostic and prognostic assessment of neoplasia. The occurrence of abnormalities in cellular DNA content allows early recognition of neo- plastic cell populations, in some cases, and diagnosis of malignancy at tissue level. In the near future, it is likely that the false-negative rate will decrease with the routine use of complementary neoplastic markers in flow cytom- etry. The studies concerning parameters, such as, double- stranded RNA and nucleolar antigen are stil under way, ‘,’ ‘,I4 especially in relation to hematological neoplasia. Perhaps, as far as solid tumors are concerned, some spe- cific monoclonal antibodies can further increase the dis- crimination leve1.2,5,’ ‘*25,26.36.40.42 The practical absence of false-negatives makes cellular DNA content a unique marker. The prognostic implications of the measurement of this marker are still being explored, but are likely to be the most important contribution of quantitative cy- tology to clinical oncology.4%7%‘5,33.38 Several DNA content- parameters, such as. the cytometric aneuploidy level (DNA index), and the presence and number of multiple clones (abnormal DNA stem lines) offer a partial but direct picture of the cellular bases of tumor heterogeneity. The data summarized in Table 7 indicate to what extent these parameters can be considered as adverse prognostic factors for patient survival or disease evolution, at least in some types of human tumors.
The development of cytometric methods for the detec- tion of BrdUrd-labeled cells has offered a new way of measuring the fraction of neoplastic cells in the S phase and/or in the proliferative compartment (growth fraction), thus, definitively re-opening the approach based on the measurement of human tumor cell kinetics. However, the procedures are still being explored and it cannot be decided whether the analogue should be used for in vivo labeling. Apart from future developments concerning the use of DNA and BrdUrd content to estimate cycle-related temporal parameters of tumor kinetics as well, even the S phase percentage should be added to aneuploidy and multiclonality as a predictor of disease evolution.36
The prognostic implications of the results of this kind of study, although needing further validation, especially in terms of inter-laboratory comparison, already suggest two different applications to therapeutic oncology. The first concerns the possibility of patient stratification before assignment to alternative treatments. For instance, in first approximation, tumors with a relatively high percent S phase cells could be candidates for shorter, “compressed” radiotherapy treatment.’ Furthermore, the possibility ex- ists of selecting tumors with a particularly adverse prog-

Human neoplasia assessment with flow cytometry 0 F. MAURO et al. 635
nosis, according to a sort of “cellular staging” (e.g., rela- tively high values of DNA index, percent S phase, number of clones, etc.) for more “radical” forms of treatment.
The second application needs further methodological development since it concerns the analysis of the clonal heterogeneity, also in terms of relative clonogenicity, in- trinsic response to drugs, and drug-induced perturbation of cell cycle progression and recruitment. However, this
approach is, for the moment, hampered by the technical difficulties in adequately sorting the various clones. In our opinion, the main objective of this kind of study should be a more complete monitoring of tumor cell het- erogeneity of prognostic relevance. Unfortunately, in the instance of solid tumors, the problems related to serial sampling make the cytometric monitoring of cell popu- lations, during and after treatment, a difficult objective.
REFERENCES
1. Arcangeli, G., Mauro, F., Morelli, D., Nervi, C.: Multiple daily fractionation in radiotherapy: Biological ratonale and preliminary clinical experiences. Europ. J. Cancer 15: 1077- 1083, 1979.
2. Ashall, F., Bramwell, M.E., Harris, H.: A new marker for human cancer cells. 1. The Ca antigen and the Cal antibody. Lancet ii: 1-6, 1982.
3. Barlogie, B., Drewinko, B., Schumann, J., Giihde, W., Dosik, G., Latreille, J., Johnston, D.A., Freireich, E.J.: Cellular DNA content as a marker of neoplasia in man. Am. J. Med. 69: 195-203, 1980.
4. Barlogie, B., Raber, M.R., Schumann, J., Johnson, T.S., Drewinko, B., Swartzendruber, D.E., GBhde, W., Andreef, M., Freireich, E.J.: Flow cytometry in clinical cancer re- search. Cancer Res. 43: 3982-3997, 1983.
5. Blaszczyk, M., Yan Pak, K., Herlyn, M., Lindgren, J., Pes- sano, S., Steplewski, Z., Koprowski, H.: Characterization of gastrointestinal tumor-associated carcinocmbryonic antigen- related antigens defined by monoclonal antibodies. Cancer Res. 44: 245-253, 1984.
6. Biihmer, R.M.: Flow cytometric cell cycle analysis using the quenching of 33258 Hoechst fluorescence by bromodeoxy- uridine incorporation. Cell Tissue Kinet. 12: 101-l 10, 1979.
7. Biichner, Th., Hiddemann, W., Schumann, J., Gahde, W., WGrmann, B., Ritter, J., Kleinmeier, B., von Bassewitz, D.B., Miiller, K.H., Grundmann, E.: Differential pattern of DNA-aneuploidy in human malignancies. In Tumor Aneu- ploidy. T. Biichner, C.D. Bloomfield, W. Hiddeman, D.K. Hossfeld and J. Schumann (Eds.). New York, Springer-Ver- lag. (In press) 1985.
8. Busch, H., Gyorkey, F., Busch, R.K., Davis, F.M., Yorke, P., Smetana, A.K.: A nucleolar antigen found in a broad range of tumor specimens. Cancer Res. 39: 3024-3030, 1979.
9. Darzynkiewicz, Z., Andreef, M., Traganos, F., Sharpless, T., Melamed, M.R.: Discrimination of cycling and non- cycling lymphocytes by BUdR-suppressed acridine orange fluorescence in a flow cytometric system. Exptl. Cell Res. 115: 31-35, 1978.
10. Darzynkiewicz, Z., Traganos, F., Melamed, M.R.: New cell cycle compartments identified by multiparameter flow cy- tometry. Cytometry 1: 98-108, 1980.
I 1. Davis, F.M., Gyorkey, F., Busch, R.K., Busch, H.: Nucleolar antigen found in several human tumors but not in nontumor tissues studied. Proc. Natl. Acad. Sci. USA 76(2): 892-896, 1979.
12. Dolbeare, F., Gratzner, H., Pallavicini, M.G., Gray, J.W.: Flow cytometric measurement of total DNA content and incorporated bromodeoxyuridine. Proc. Nutl. Acad. Sci. USA 80: 5573-5577, 1983.
13. Elkind, M.M., Whitmore, G.F.: The influence of chemical and physical factors on survival. In The Rabiobiology of Cultured Mammalia Cells. New York, Gordon and Breach Science Publishers. 1979, pp. 145-235.
14. Frankfurt, 0.: Flow cytometric analysis of double-stranded RNA content distributions. J. Histochem. Cytochem. 28: 663-669, 1980.
15. Frankfurt, O.S., Slokum, H.K., Rustum, Y.M., Arbuck S.G., Pavelic, Z.P., Petrelli, N., Huben, R.P., Pontes, E.J., Greco, W.R.: Flow cytometric analysis of DNA aneuploidy in pri- mary and metastatic human solid tumors. Cytometry 5: 7 l- 80, 1984.
16. GGhde, W., Schumann, J., Biichner, T., Otto, F., Barlogie, B.: Pulse cytophotometry. Application in tumor biology and clinical oncology. In Flow Cytometry and Sorting, M.R. Melamed, P.F. Mullaney and M.L. Mendelson (Eds.). New York, John Wiley & Sons. 1979, pp. 599-620.
17. Gustafson, H., Tribukait, B., Esposti, P.L.: DNA pattern, histological grade and multiplicity related to recurrence rate in superficial bladder tumors. Scund. J. Ural. Nephrol. 16: 135-139, 1982.
18. Hammarberg, C., Slezak, P., Tribukait, B.: Early detection of malignancy in ulcerative colitis: A flow-cytometric DNA study. Cancer 53: 291-295, 1984.
19. Hiddemann, W., Schumann, J., Andreef, M., Barlogie, B., Herman, C.J., Leif, R.C., Mayall, B.H., Murphy, R.F., Sandberg, A.A.: Convention on nomenclature for DNA cy- tometry. Cytometry 5: 445-446, 1984.
20. Johnson, T.S., Rao, M.R., Gitman, R.K., Gillete, E.L.: Ploidy and DNA distribution analysis of spontaneous dog tumors by flow cytometry. Cancer Res. 41: 3005-3009, 1981.
21. Klein, F.A., Herr, H.W., Sogani, P.C., Whitmore, W.F., Melamed, M.R.: Detection and follow-up of carcinoma of the urinary bladder by flow cytometry. Cancer 50: 389-395, 1982.
22. Langer, E.M., Riittgers, H.R., Schliermann, M.G., Mitten- burger, H.G., Schumann, J., Giihde, W.: Cycling S-phase cells in animal and spontaneous tumors. Comparison of S- phase frequency estimated with the BrdUrd technique using 3H-thymidine and flow cytometry. Acta Radio/. (In press) 1985.
23. Melamed, M.R., Mullaney, P.F.: An historical review ofthe development of flow cytometry and sorters. In Flow Cytom- etry and Sorting, M.R. Melamed, P.F. Mullaney and M.L. Mendelson (Eds.). New York, John Wiley & Sons. 1979, pp. 3-9.
24. Modini, C., Passariello, R., Loscone, C., Cicconetti, F., Si- monetti, G., Zerilli, M., Tirindelli-Danesi, D., Stipa, S.: TNM staging in lung cancer: Role of computered tomog- raphy. J. Thorac. Cardiovasc. Surg. 84: 569-574, 1982.
25. Rosen, S.T., Mulshine, J.L., Cuttitta, F., Fedorko, J., Camey, D.N., Gazdar, A.F., Minna, J.D.: Analysis of human small cell lung cancer differentiation antigens using a panel of rat monoclonal antibodies. Cancer Res. 44: 2052-206 1, 1984.
26. Rutgers, D.H.: DNA flow cytometry in experimental and clinical oncology. M.D. Thesis, University of Utrecht, 1985.
27. Schiffer, L.M., Marcel, A.M., Nelson, J.S.: Estimation of

636 I. J. Radiation Oncology 0 Biology 0 Physics April 1986, Volume 12, Number 4
28.
29.
30.
31.
32.
33.
34.
tumor growth fraction in murine tumors by DNA-depen- dent DNA polymerase assay. Cancer Res. 36: 2415-2418, 1976. Spano, M., Balduzzi, M., De Vita, R., Pacchierotti, F., Per- retta, G., Teodori, L., Mauro, F.: Interspecific differences in normal and malignant tissues evaluated by flow cyto- metrically determined DNA content. (Abst. D63). X Inter- national Conference on Analytical Cytology, Asilomar, 1984. Steel, G.G.: Cell population kinetics of human tumors. In Growth Kinetics of Tumors. Oxford, Clarendon Press. 1977, pp. 185-216. Stragand, J.J., Bergerat, J.P., White, R.A., Hokanson, J., Drewinko, B.: Biological and cell kinetic properties of a hu- man colonic adenocarcinoma (LoVo) grown in athymic mice. Cancer Res. 40: 2846-2852, 1980. Swartzendruber, D.E.: Microfluorimetric analysis of cellular DNA following incorporation of BUdR. J. Cell Physiol. 90: 445-454, 1976. Teodori, L., Stragrand, J.S., Stettner, S., Barlogie, B.: 5- Bromodeoxyuridine quenching of acridine orange fluores- cence in human bone marrow as a potential probe for growth fraction determination in vitro (Abstract). V International Symposium on Flow Cytometry, Bracciano, Roma, 1980. Teodori, L., Tirindelli-Danesi, D., Cordelli, E., Uccelli, R., Mauro, F., Schillaci, A., Modini, C., Moraldi, A., Capurso, L.: Potential prognostic significance of flow cytometrically determined DNA abnormality in GI tract human tumors. Annals of the New York Academy of Sciences (In press) Teodori, L., Tirindelli-Danesi, D., Mauro, F., De Vita, R.. Uccelli, R., Botti, C., Modini, C., Nervi, C., Stipa, S.: Non- small-cell lung carcinoma: Tumor characterization on the basis of flow cytometrically determined cellular heteroge- neity. Cytometry 4: 174-183, 1983.
35.
36.
37
38.
39.
40.
41.
42.
43.
Traganos, F.: Flow Cytometry: Principles and applications. I Cancer Invest. 2(2): 1949-1963, 1984. Tribukait, B.: Flow cytometry in surgical pathology and cy- tology of tumors of the genito-urinary tract. In Advances in Clinical Cytology, Vol. 2, L.G. Koss and D. Coleman (Eds.). NY, Masson Publishers USA Inc. 1984, pp. 163-l 89. Tubiana, M., Pejovic, M.H., Chavaudra, N., Contesso, G., Malaise, E.P.: The long-term prognostic significance of the thymidine labeling index in breast cancer. Int. J. Cancer 33: 441-445, 1984. Vindelov, L.L., Hansen, H.H., Christensen, I.J., Spang- Thomsen, M., Hirsch, F.R., Hansen, M., Nissen, N.I.: Clonal heterogeneity of small-cell anaplastic carcinoma of the lung demonstrated by flow cytometric DNA analysis. Cancer Res. 40: 4295-4300, 1980. Visser, J.W.M.: Vital staining of haemopoietic cells with the fluorescent bis-bensimidazole derivatives Hoechst 33342 and 33258. O.D. Laerum, T. Lindmo and E. Thorud (Eds.), Universitltsforlaget, Bergen. Flow Cytometry 4: 86-90, 1979. Wagener, C., Petzold, P., Kohler, W., Totovic, V.: Binding of five monoclonal anti-tea antibodies with different epitope specificities to various carcinoma tissues. Int. J. Cancer 33: 469-475, 1984. Weiss, H., Kunde, D., Heinz, U., Schalicke, K.: Sensitivity to heparin in benign, preneoplastic and neoplastic cells of the human breast as revealed by DNA distribution patterns (DNA-DP). Preliminary results. 6th Znternational Sympo- .cium on Flow Cytometry. Schloss Elman, 1982, p. 240. Wolley, R.C., Schreiber, K., Koss, L.G., Karas, M., Sher- man, A.: DNA distribution in human colon carcinoma and its relationship to clinical behavior. J. Natl. Cancer Inst. 69: 15-22, 1982. Zante, J., Schumann, W., Gohde, W., Hacker, U.: DNA- fluorometry of mammalian sperm. Histochemistry 54: l- 7, 1977.