
Five cases of suprapubic cystotomy
28
Transcript of Five cases of suprapubic cystotomy

FIVE CASES OF SUPRAPUBIC CYSTOTOMY:
Three for Stone, One for Tumor in the Bladder, and Onefor Exploration with Catheterism of the Ureters;
One Death.
BY
W. W. KEEN, M.D.,PROFESSOR OF THE PRINCIPLES OF SURGERY, JEFFERSON MEDICAL
COLLEGE. PHILADELPHIA.
FROM
THE MEDICAL NEWS,
April iB, 1891.


[Reprinted from The Medical News, April 18, 1891.]
FIVE CASES OF SUPRAPUBIC CYSTOTOMY:Three for Stone, One for Tumor in the Bladder, and One
for Exploration with Catheterism of the Ureters;One Death}
By W. W. KEEN, M.D.,PROFESSOR OF THE PRINCIPLES OF SURGERY, JEFFERSON MEDICAL
COLLEGE,PHILADELPHIA.
Case I. Slone in the bladder; suprapubic cys-totomy; prostatectomy; recovery. —l was called toVineland, N. J., September 12, 1888, by Dr. C. R.Wiley, to see Mr. JB., aged sixty-five. He had hadthe usual symptoms of stone in the bladder for sixyears. A Petersen’s bag was inserted in the rectumand distended with ten ounces of warm water. Thebladder was injected with six ounces of water withfour grains of boric acid to the ounce. Suprapubicdulness then existed to two inches above the pubes.The operation was done by the usual vertical in-cision, and two stones were removed, weighingtogether 763 grains. The prostate projected somuch into the bladder at the mouth of the urethrathat I removed a piece a slarge as the last joint ofthe finger, by the scissors. The bleeding was slight.The bladder was not sutured. A drainage-tube wasinserted and removed on the tenth day: a catheterwas retained in the bladder for four days more.The patient recovered without any trouble, his
1 Read before the Philadelphia Academy of Surgery, April 6,xBqo. '

2 KEEN,
highest temperature being i00.6°, falling to normal,both morning and evening, within a week. Thewound healed entirely in four weeks.
In July, 1889, he had a return of his old symp-toms, and Dr. Joseph W. Hearn, being in Vine-land, was asked by Dr. Wiley to see him again.Dr. Hearn having detected a stone by the sound,reopened the former wound by dilating a smallfistula which had appeared, then crushed and re-moved two stones, weighing 412 grains in all. Afterthat time he was well until his death recently fromanother disease, as Dr. Wiley informs me.
I have no question that the stones removed byDr. Hearn had formed since the first operation, forthe entire interior of the bladder was inspected atthat time and no further stone was detected.
Case 11. Ankylosis of the knee; stone in the blad-der; suprapubic cystotomy; recovery. —R. J. 8., ofBridgeton, N. J., first consulted me June 19, 1888.A tall, spare man, aged forty-three, with ankylosisof the left knee from a white swelling twelve yearsago. Has also suffered considerably from rheumaticgout, and has a deformed right hand following it.There is also considerable ankylosis of both elbows.He passed a stone from the bladder for the firsttime in 1876, and since then has passed dozens ofthem, mostly phosphatic, and he has had also renaltrouble from gravel, attended with hsematuria, sevenor eight years ago. He has passed no stone by theurethra for eighteen months, but his present attackof vesical irritation has existed for three years. Heis obliged to empty the bladder from one to fourtimes an hour. Urine, specific gravity ion, smallamount of pus and albumin, with phosphates; re-action faintly alkaline.

SUPRAPUBIC CYSTOTOMY. 3
Operation, June 4, 1888. The patient desiredthat the “ high operation ” should be done in orderthat the condition of the bladder could be exploredby the eye and the finger at the same time that thestone was removed. The ankylosis of the knee, aswell as his wish, made me decide to do the supra-pubic operation. The rectal bag was distended withten ounces of warm water, and the bladder withsevenounces of water with four grains of boric acid tothe ounce. The dulness of the distended bladderextended two inches above the pubes. An incisiontwo and one-half inches long was made and thebladder easily reached, except for the difficulty withthe anaesthetic, as mentioned later. An incisiontwo inches long was made in the bladder and thestone was extracted. Its shape was that of a flat-tened sphere; it weighed 421 grains when dry, andits surface was quite smooth except at the edges.
The bladder wound was then closed with eightstitches of interrupted fine chromic catgut. Thebladder was now injected with warm water com-bined with the boric acid in order to test the ac-curacy of the closure of the wound. No waterescaped. The wound was then filled with waterand the bladder was injected with nine ounces ofair, when instantly a leak was discovered by the airbubbling up through the water. A stitch closedthis, and made the bladder both air- and water-tight. Six stitches closed the wound in theabdominal wall, which included with care theaponeurosis of the abdominal muscles. The peri-toneum was not recognized during the operation.A flexible catheter was inserted into the bladder,and its end was at first corked up and the bladderemptied every hour ; but, as this caused some pain,the catheter was uncorked and continuous drainageinto a urinal substituted.
4 KEEN,
6th (2d day). He has hid no pain; his highesttemperature is xoo° ; he is hungry, and has sleptwell. The wound was re-dressed yesterday, wheneverything looked well.
Four days after the operation there was con-siderable local tenderness and irritation, and on thesixth day this was so marked that I removed thestitches and evacuated some urineand pus, which hadformed as a result of the giving way of the stitchesin the bladder. The wound was drained for a fewdays and then closed, and he went home on the25th, three weeks after the operation. Since thattime he has had no trouble.
Remarks. —No other operation than the supra-pubic could have been done in this case on accountof the ankylosis of the knee. The operation was anextremely difficult one, because unless he was deeplyanaesthetized he was struggling, with the abdominalwalls as tense as boards, and in order to relax themanaesthesia had to be carried to a point which Ifelt involved serious danger. Between Scylla andCharybdis it was very difficult to steer a safe course.The difficulty was especially great in suturing thebladder. In fact, I think it would have been wiserhad I not attempted to do so, but had simplydrained.
Case 111. Stone in the bladder; surgical kidneys;death from sudden oedema of the lungs. —W. H. C.was referred to me by Dr. Julius A. Johnson, ofEaston, Md., December 11, 1889. His age is fiftynine; his weight two years ago 185pounds; at pres-ent about 135 pounds. Seven to eight years ago hefirst noticed that his water was passed very slowly.Four years ago had a brief attack of apparently acute

SUPRAPUBIC CYSTOTOMY. 5
inflammationof the bladder. Two years ago anotherattack of acute inflammation, with very thick urine,and required catheterization; has used a Nelatoncatheter himself more or less ever since. Passes hiswater about ten times in the twenty-four hours ; hasnever passed any blood, except as a result of the useof the catheter, he thinks. Has no pain in thesmall of the back, but suffers severely in the bladderand perineum, for which he has taken from one-halfto one grain of morphia a day for about two years.In spite of his wasting, his appetite is good, and alsohis sleep, excepting that it is interrupted by thenecessity of passing his water.
Eight years ago, while brushing his teeth, hetouched a nerve, he thinks, and for a few minuteshis face was “drawn.” From one to two yearslater, while going home to dinner, his left arm andleg became weak, and he had no use of them for afew minutes. He did not fall, but sat down, andafter a short time walked home. A few times sincethen he has felt as if a similar weakness was comingon ; seizing his wrist stopped it. In October, 1888,on a Saturday he had a fever and a chill from exposureto cold. On the following Tuesday his wife gavehim a hot toddy. A little while afterward, whilesitting in a chair, a “queer look” came over hisface, so his wife states, and for a few minutes he“talked thick,” but after that had no furthertrouble. He has never had any headache.
He has had at least three considerable haemor-rhages from the bladder. He is not quite sure, butthinks that the haemorrhages came on only at theend of micturition, except the last time, when theurine was uniformly bloody from the beginning.The longest of these haemorrhages continued for twoto three days. By spells the urine has been alter-nately clear and bloody, and its passage attended

6 KEEN,
with considerable soreness, which passed away assoon as the hsemorrhage occurred.
Once he passed a small calculus the size of a pea,and probably one hundred of about the size of apin-head ; these last at varying times.
Operation, December 26, iBBg. I was assistedby Professor Brinton and Drs. Horwitz and Cop-lin. Owing to the bad condition of his kidneys,chloroform was given instead of ether. The fieldof operation was thoroughly prepared the daybefore. Petersen’s bag was inserted into the rectumand distended with twelve ounces of warm water. Ihad not examined his bladder instrumentally before,as it gave him great pain even to introduce a softinstrument, and in view of his general poor healthand the damaged condition of his kidneys, I deter-mined not to give an anaesthetic twice. In orderto fill the bladder as well as to explore it, I nowintroduced a silver catheter. The instant it enteredI struck an evidently large stone. After washingout the bladder, nine ounces of warm, boiled waterwere introduced through the catheter; as soon asthis limit was reached the water began to escapealongside of the catheter, and to prevent its furtherescape, rubber tubing was tied around the penis.Notwithstanding this double dilatation, the bellywas still resonant down to the pubes, though theresonance slightly diminished as the pubes wereapproached. An incision was made in the middleline from the pubes three inches upward. As soonas the belly-wall was cut through, the peritoneumwas encountered, reaching all the way to the pubes.It was readily lifted to the upper end of the incision,but as it was more than usually thin, and requiredan additional assistant, I determined at once to getrid of this necessity and danger, by placing thepatient in Trendelenberg’s position. A tall, stout

SUPRAPUBIC CYSTOTOMY. 7nurse, with his back to the patient’s perineum, tookthe patient’s knees over his shoulders and thus liftedthe pelvis about a foot from the table. The peri-toneum at once disappeared at the upper extremityof the incision. The bladder was still so deep thata possibility, even, of its rupture from the injectionsuggested itself to me. It was found, chiefly by theaid of the catheter which had been placed in it, ata depth of three inches from the skin. Several largeveins were first ligated, both on the bladder-walland in the connective tissue in front of it. Thebladder was then opened, and one large and threesmall stones removed. The small stones were aboutthe size of Lima beans; the large one crumbleddown, under the grasp of the forceps, into a numberof fragments; the stones were phosphatic. Theweight of alj that was recovered was just 600 grains,and I estimated that fifty or sixty grains were lostin the debris in washing out the bladder. Thewall of the bladder was much pocketed, and thethree small stones were found in these pockets,and would almost inevitably have been overlookedhad any other operation than the suprapubic beendone. They were readily extracted by the finger insearching for fragments. The prostate, which hadbeen found but little enlarged toward the rectum,was greatly enlarged on the vesical aspect, the en-largement being chiefly in the middle line and tothe right, forming a uniform, rounded mass, bulginginto the bladder just behind the orifice of theurethra, but not blocking it. Prostatectomy, there-fore, was not done.
The walls of the bladder were rugose and aboutthree times their natural thickness. The wound inthe bladder was not closed. A drainage-tube ofsoft rubber with a bulbous end was introduced intothe bladder. As there was so large a space between

8 K KEN,
the bladder and the abdominal wall, I thought itprudent also to introduce a second drainage-tubefor the first forty-eight hours into the pre-vesicalspace. The abdominal wall was then closed byinterrupted sutures, the two drainage-tubes comingout together at one interspace.
jisf. Reacted very well from the operation. Fortwo days he had slight vomiting, and on the thirdand fourth days considerable hiccough, whichyielded to one-quarter grain doses of cocaine. H;stemperature fluctuated between 97.90 and 99.6°,only once reaching ioo°. The wound was irrigatedthrough the drainage-tube with warm boric acidsolution. The pre-vesical drainage-tube was re-moved at the end of forty-eight hours.
When I left him at 5 p. m. on the 30th (thefourth day) I felt very well satisfied with his condi-tion and quite assured of his recovery. So far ascould be judged, the amount of urine secreted wasample, and there was no danger apparently fromthe kidneys. At 9.30 p. m. on the night of the30th acute oedema of the lungs set in, followed bydeath in S' ven hours. No post-mortem could beobtained.
Remarks. —This operation was only undertakenin view of the urgent symptoms. The bad condi-tion of the kidneys and his serious antecedenthistory of cerebral disturbance of course contra-indicated operation, but his suffering from thestones in the bladder was so intense that relief wasabsolutely neces'ary. That life was terminated bythe sudden oedema is not to be wondered at in viewof the renal complications.
No case ever showed me better the value of Tren-delenberg’s position. The moment he was placed

SUPRAPUBIC CYSTOTOMY. 9in that position, not only did the peritoneum falldown and away, but the bladder was made accessible,although being so deeply placed. Neitherthe rectalbag nor filling the bladder with water raised it tothe abdominal wall, and I was seriously afraid thatthe bladder had been ruptured, although no morewater was injected than the capacity of the bladdereasily permitted.
Case IV. Papillo7na of the bladder; removal bysuprapubic cystotomy; recovery. —Mr. S., aged fifty-seven. (The following history was furnished byDr. Lorini, his medical attendant.) Family historynegative; no cancer. He had malaria in the sixtieswith biliary fever. He had marked trouble withhis gall-bladder from 1878 to 1881, and visitedCarlsbad, since which time he has had no return ofthe trouble. There is no history of urinary calcu-lus or gravel. In 1885 he had an attack of cystitiswith blood in the urine for a few days. He wascircumcised in- 1887. For thirty years he has hada sense of discomfort in the small of the back.About August 1, 1889, after a horseback ride atOcean Beach, N. J., bleeding from the bladderbegan, but yielded to internal remedies after twodays. August 15th, another attack came on andcontinued for a few days, but yielded again to thesame remedies. In January, 1890, a third attacklasted for nine weeks, in spite of internal remediesand the actual cautery over the back. In April andMay his bladder was washed out with boric acid andnitrate of silver solutions of various strengths. Afterfive days the bleeding stopped, but returned againabout the middle of June, and continued up to themiddle of August, in spite of the use of the nitrate ofsilver and boric acid solution. He spent the summer

KEEN,
in Maine and gained greatly in health. The capacityof the bladder was undiminished, and the urinecontained neither casts nor albumin when there wasno blood. There was slight prostatic tenderness.The blood was always thoroughly mixed with theurine from the very start, whether drawn by cathe-ter or voided voluntarily. Clots were passed fromtime to time. These were of irregular shape andseemed to be fewer and smaller when he led an activelife, more numerous and larger when he rested. Noshreds of tissue have ever been found, in spite ofthe most careful watching, except one minute speci-men, which was thought to be papillomatous, andthe deeper cells possibly sarcomatous, by Dr. F. A.Packard.
November ij, ißpo, the haemorrhage returnedmore profusely than ever, and has continued to thepresent time, in spite of internal remedies, washingout the bladder, hypodermics of ergotine, etc.
Status preesens , Dec. /, ißpo. When I saw himfor the first time, at this date, I found a short, stoutman who appeared to be in good health, but with ananaemic, pale skin, and who was evidently sufferingfrom the mental depression incident to the con-tinued haemorrhage. He had lost but little flesh, andhis anaemic appearance, as was stated to me by Dr.Lorini, who had known him for many years, andunder whose care he now was, was habitual and nota result of the bleeding, a rather surprising fact inview of the amount of blood lost. I saw him voidhis urine, which was porter-colored from the firstdrop. There were some small clots of irregularshape, and from the amount of urine passed and itscolor and clots I estimated that the amount of bloodlost was not far from half a pint a day. Dr, CrozerGriffith examined a specimen of the urine for me.It showed no casts; a large amount of blood was
SUPRAPUBIC CYSTOTOMY.
present, with an excess of white blood-cells, whichin some places were adherent to each other inmasses, as in cystitis and other suppurative pro-cesses. No epithelial cells were found. Fragmentsof possible tissue were examined and found to beonly clots which had rested somewhere in theurinary tract sufficiently long to become largelyfibrinous. The urine contained 2 per cent, of urea.The blood count showed 3,890,000 blood cells, 53per cent, of haemoglobin, and no plasmodia. Acareful examination of the region both of thebladder and the kidneys, not only by myself but byDrs. Lorini, W. J. Taylor, J. William White, andWilliam Pepper, was entirely negative. There wasno dulness, no tenderness, no pain, but simplyhaematuria and nothing more. On December 13,1890, I attempted to examine the bladder by thecystoscope, but was unsuccessful in detecting any-thing. The bloody urine was first drawn and re-placed with a warm boric acid solution, but in spiteof the most careful use nothing further could beseen.
The day after the use of the cystoscope he ob-served in urinating that some air or gas bubbledout. I attributed this naturally to some air whichhad been injected into the bladder with the fluid,but he calkd my attention to this difference: thatat the present time the gas produced no pain, butthat when air was injected it produced distinct painas it often had done a year ago when washing outhis bladder. This discharge of air or gas has con-tinued up to the present time. It does not occurwith each act of urination, but occurs at least oncea day, and takes place at the end of urination, notat any other time. It is especially noticed whenhe strains to press out the last few drops from thebladder. So far as he can observe the gas has no

12 KEEN,
odor, and I have observed that the urine has none,nor have the clots that have been passed. He hashad no pain in his bladder or rectum.
His wife tells me that she thinks there is a distinctloss ofstrength in the last few weeks, and also thatfor the last year or more he has been more drowsythan formerly.
Operation, December 2<p, iSgo. Assisted by Drs.J. William White, William J. Taylor, Orville Hor-witz, J. C. Da Costa and Dr. Lorini, his physician.The bladder was first washed out and then filledwith 9 ounces of a boric solution, a drachm to thepint. The Petersen bag in the rectum was then di-lated with warm water, but as soon as the capacity ofeight ounces was reached the resistance became sogreat that I desisted from introducing any more. Anincision in the median line disclosed the bladder,which was secured by two ligatures and then incised.As soon as the finger was introduced I perceived asmall tumor near the right ureter. With the electriclight it was inspected, though with some little diffi-culty. In doing so I used both Watson’s vesicalspeculum and my own, but each had to be sup-plemented by a long pair of forceps to push backthe posterior wall of the bladder. The tumor wasabout the size of the end of the forefinger, say alittle over half an inch in diameter, and about thesame in elevation. It was strawberry-like in itsappearance, though not quite so red. Near to itwere two other small elevations of the size of amoderate pin-head, which were thought possibly tobe the beginning of similar growths. There wereseveral other very minute growths, but so small asto make it doubtful whether they were normal orpathological.
The tumor and the two small elevations near itwere seized by the forceps and drawn forward some-

SUPRAPUBIC CYSTOTOMY. 13
what forcibly, and the mucous membrane for somelittle distance around the base was removed with thetumor by curved scissors. The bleeding was verymoderate and required no special means for its con-trol.
One stitch was put in the wound in the bladderand four stitches in the abdominal wall. Twodrainage-tubes were introduced, one into the pre-vesical space and the other into the bladder, bothsecured in place by stitches in the skin. A largewood-wool dressing was then applied over thewound, and aristol ointment spread over the abdo-men under the dressing. The dressing was to bechanged whenever it was wet, and the bladder tobe washed out with a warm boric acid solution.
He was put to bed in a very fair condition. Dur-ing the operation Trendelenberg’s position was alsotried, but its advantages were not very manifest.Still there was, I think, slightly greater ease of ac-cess to the bladder. The ureters were seen and anattempt was made to catheterize one of them, butwithout obtaining any urine. In justice to the pro-cedure, however, it should be said that we did notpersist long enough, probably, to make the attemptvaluable. We had found sufficient to account forhis condition, and we did not deem it just to himneedlessly to prolong the operation.
No communication was discovered between thebladder and the bowel, though the interior wascarefully examined at every point.
January 1, 189r (the third day). Since theoperation, now three days, he has gone on steadilyimproving. His highest temperature was on thenight following the operation, since which time ithas been 99° and a fraction. The wound looks per-fectly well. On the second day he developed spas-modic pain, which he referred to the prostate, the
KEEN,
attacks of which were quite severe. Thinking that itmight be due to the pressure of the end of thedrainage-tube in the bladder, I removed this rubber tube andreplaced it with a shorter tube of glass, but duringyesterday, his pains being so severe, Dr. White, asI was absent from the city, removed the tube fromthe pre-vesical space. This was not followed byimmediate relief, but with some amelioration ofthe attacks, and finally their disappearance at theend of about twenty-four hours. The tube in thebladder I removed to-day. His appetite is verygood, so that he enjoyed a small chop yesterdayand a small beefsteak to-day. His sleep has beenvery fair.
jd (fifth day). He has had a good deal of vesicaltenesmus, for which I cannot see any reason. Thewound looks well. Two of the four stitches wereremoved to-day; some small shreds of sloughingconnective tissue came away. In examining therectum a few days ago Dr. White thought he de-tected a nipple-like prominence, just as would existif there were a fistulous opening in the rectum, andat the operation a pouch in the posterior wall ofthe bladder was discovered, which possibly corre-sponds to this, although no opening or other lesioncould be detected either at the operation or since.A large enema yesterday emptied the bowels thor-oughly, and there has not been, either from thebladder or from the bowels, any evidence of com-munication between the two.
From this time on he improved very rapidly. Hispain quickly lessened and the wound closed at theend of five weeks. Since that time he has beenperfectly well. There has been no escape of faecesor of gas from the urethra, nor has there been theleast return of the bleeding.
The tumor was examined by Dr. J. P. Crozer Grif-

SUPRAPUBIC CYSTOTOMY. 15
fith and Dr. Burr, and was found, on section, to bea compact sessile form of papilloma without anyfiliform fringes.
Case Y. Possible tumor of bladder; boutonniereoperation; later exploratory suprapubic cystotomy,with catheterism of the ureters by the aid of the elec-tric light; recovery. —M. H., of Mauricetown, N. J.,aged twenty-eight; weight 121 pounds. Was referredto me by Dr. Samuel Butcher, November 22, 1889.Family history negative. No venereal history. OnJune 5, 1887, when he rose from bed he passedclear blood from the bladder without pain andwithout apparent reason, he being then apparentlyin perfect health. The blood was intimately mixedwith the urine from the very first drop. With slightintervals the urine has been bloody ever since. Aweek after the hsematuria he became a little better,when a sudden retention for twenty-four hours wasfollowed by the evacuation of a quantity of clots.There are usually no clots, but the blood and urinewere intimately mixed. For the first year he suf-fered a little pain; since then he has only had slightpain in the loins, possibly more marked on the leftside. In June, 1888, he had bilious fever, and inDecember, 1888, and January, 1889, clots accu-mulated again and required a catheter. He thinksthat occasionally the clots were long and slender,especially when few in number, being one to twoinches long and about the thickness of a pin.
When clots accumulate in the bladder he has con-siderable pain near the anterior superior spine; hiswater then clears up and is apt to be more coloredwhen the pain disappears. No calculus is discov-ered by sounding, and there is no pus in the urine.He passes about the usual quantity and urinates fiveor six times a day. Nothing is found in the urineby microscopic examination but blood. A small

KEEN
amount of albumin is present when there is bloodin the urine, but when there is no blood the urineis absolutely free from albumin.
Dr. Hearn examined the patient some monthsago, and believed that there was a papilloma in thebladder. I admitted him to the Jefferson Hospitalin December, 1889, and watched the urine withgreat care. No long, slender clots were at thattime found, but only irregular-shaped clots. Smallfragments of a possible papilloma were watched forcarefully, but only one or two were found at inter-vals, which were believed by Drs. Longstreth andCoplin to be fragments of a doubtful papilloma.The renal symptoms were practically nil, for thepain in the loin was but slight, and scarcely moremarked on one side than on the other. No increasein the dulness over either kidney was noted, norwas there any tenderness on palpation by one handnor on bimanual examination. The tenderness nearthe anterior superior spine only existed when therewere clots in the bladder, and there is no tender-ness at present.
First operation, January j, ißgo. I explored thebladder by the boutonniere opening. As soon asthe finger entered the bladder, I found at the upperright wall posteriorly a soft, velvety mass. Whetherit was a tumor or the bladder-wall I was not abledefinitely to decide. I introduced a pair of smooth-bladed stone-forceps until the bladder-wall wastouched, then withdrawing them half an inch andclosing the jaws I found that I had grasped some-thing, which by traction gradually yielded with asensation as if thread after thread was being torn.In the jaws of the forceps was a florid mass, lookingnot unlike a blood-clot, but traversed by threadswhich looked like fibrous tissue. Nothing likemucous membrane was seen. A number of small

1 7SUPRAPUBIC CYSTOTOMY.
masses were removed in this way, amounting in allto a mass about twice as large as an English walnut.Twice I tried Sir Henry Thompson’s serrated tumorforceps, but both times, in spite of using every pre-caution, I found that I had caught the bladder-wall,as was manifested by its not yielding after the samegentle traction as before, and by the mucous mem-brane being drawn into the wound. The bleedingwas inconsiderable. Watson’s perineal drainagetube was inserted.
He recovered from the operation without diffi-culty, the wound closing in twenty days, at whichtime he went home. The urine at first cleared up con-siderably, though afterward it again became bloody,but two months later it was almost clear. The massremoved was again submitted to Drs. Longstrethand Coplin, but in spite of careful examination theywere still doubtful whether the masses were blood-clots or fragments of a papillomatous growth,although rather inclined to the latter opinion.
May 2jd. He has gained fifteen pounds inweight, feels much better, and has had no painsince the operation. The urine has generally beenclear until the last two or three weeks, when theblood has reappeared, with small clots. I haverepeatedly seen him pass his water, both before theoperation and since, and it is uniformly bloodyfrom the start.
November ijtk. I examined the bladder by thecystoscope, but could only see a uniformly redand apparently healthy bladder-wall.
Second operation , November 18th, at the Jeffer-son Medical College Hospital. Nine ounces ofwarm boric-acid solution (four grains to the ounce)were injected into the bladder, and eleven ouncesof warm water into the rectal bag. The injectioninto the bladder alone produced dulness of but one

KEEN,
finger’s-breadth above the pubes. This was in-creased, by filling the rectal bag, to 2.5 inches.A three-inch incision in the middle line disclosed
Fig. i.
-FIXEDFIXED
-MOVABLE
the bladder very readily. The peritoneum was notseen. The bladder was opened, and the edges ofthe opening caught with two haemostatic forceps. Aspecial retractor, which I had devised (Fig. 1), was

SUPRAPUBIC CYSTOTOMY. 19
then inserted, in order both to separate the rectimuscles and the edges of the opening in the bladder,and a small, hooded, two-candle power electric lightwas used to examine the bladder. A prior examina-tion by the finger the moment that the bladder wasopened gave an entirely negative result. The ex-amination by the electric light was extremely satis-factory; on the right upper and posterior wall ofthe bladder was seen a scar about one and one-halfinches in diameter, evidently the result of the firstoperation. It was smooth and healthy. I found agood deal of difficulty in examining the posteriorwall, inasmuch as the bladder contracted as soon asthe water escaped, and was thrown into deep folds.By.inserting the angular large haemostatic forceps,or pedicle forceps, and opening the blades, I wasable to push the bladder upward and unfold thecreases in its wall. To obviate this difficulty I havelately devised another instrument (Fig. 2) which asyet I have not had an opportunity to test. I thendiscovered between and above the orifices of theureters a small ulcer, a scant quarter of an inch indiameter, possibly tubercular. A piece of thebottom of it was pinched off for examination micro-scopically, but showed no bacilli.
I found that I could examine the posterior wall ofthe bladder a great deal better when the rectal bagwas removed. The orifices of the two ureters wereseen, and both successfully catheterized. From theleft ureter bloody urine was obtained, and from theright one clear urine.
When the urine escaped into the bladder no dif-ference in the urine from the two ureters was percep-tible, as the red wall of the bladder made both lookalike. But when they were collected in a small glasscup the difference in their appearance was instantlyperceptible.

20 KEEN, SUPRAPUBIC CYSTOTOMY
Fig. 2.
Bladder-dilating instrument.
To facilitate this ureteral catheterism I have de-vised an angular catheter which I believe will be ofservice (Fig. 3).
The opening in the bladder was then stitched,except at its lower end, where a drainage-tube wasinserted. The external wound was partly closed.
December 8 (three weeks). The patient went hometo-day. The drainage-tube was removed on thesecond day after the operation. The rest of thewound healed very well, but the opening in thebladder did not close until two weeks after theoperation. Until that time the urine had beenmuch freer from blood, but it now became muchmore bloody. No especial incident attended hisrecovery. He still has bloody urine. Wheneverhe is ready I intend to explore the left kidney.
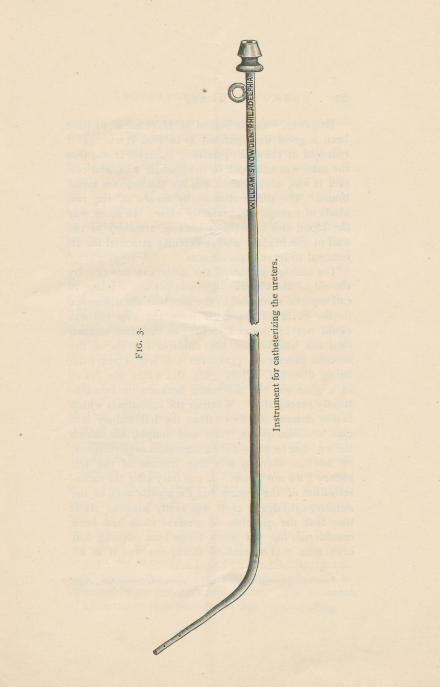
Instrumentforcatheterizingtheureters.
Fig.3,

22 KEEN,
Remarks. —In the case of M. H. (Case V.) I havebeen a good deal puzzled as to what it was that Iremoved at the first operation. Certain it was thatthe mass was adherent to the bladder wall, and cer-tain it was, also, that it was not the mucous mem-brane. The differentiation by means of the twokinds of forceps was perfectly clear. In some waythe blood-clot apparently became attached to thewall of the bladder and sufficiently attached for itsremoval to leave a visible scar.
The catheterization of the ureters in this case bythe aid of the electric light was perfect. I beg tocall especial attention to the fact that the differencein the color of the urine from the two kidneyscould not be noticed so long as the urine escapedinto the bladder, for the uniform redness of themucous membrane prevented the true color frombeing detected. Only when the water was drawnin a glass was the difference between the two dis-tinctly perceptible. Whether the hgematuria whichis now determined to be from the left kidney is acase of haemophilia, pure and simple, for whichBrown 1 has recently done a successful nephrectomy,or whether there is any true disease of the leftkidney Ido not know. It was only after the cathe-terization of the ureters that the significance of theslender, cylindrical clots was really known. It istrue that the question of ureteral clots had beenconsidered, but yet when I saw him nothing hadbeen seen that resembled them, nor was it at all
1 American Journal of the Medical Sciences, November, 1890,p. 522.
SUPRAPUBIC CYSTOTOMY. 23
certain that they were anything more than acci-dental. They were certainly not common.
As a result of my present experience with theboutonniere and the suprapubic operations, Iwould certainly prefer the latter as by far the bet-ter. In view of the persistent haematuria, with itsbaneful effects both on mind and body, I proposeto explore the left kidney whenever the patient isready, and if the indications point that way, to doa nephrectomy.
Case IV. resembles this one in many ways. Inboth the haematuria was the only symptom present,and the diagnosis was correspondingly obscure.Although Mr. S. had the advantage of the mostskilful diagnostic opinions, yet it was with greatdoubt as to whether the papilloma really existed inthe bladder or not, that the operation was begun.It was clear, however, that something ought to bedone, for the disease was making inroads on thepatient’s nervous system quite as much as on hisphysical condition. The kidney was so absolutelyexempt from any indication of disease, that it didnot seem right to explore there; and even if I haddecided to do so, the question which one, was stilla difficult one to solve. I would call especial at-tention to the fact that in both these cases the urinewas uniformly bloody from the beginning of micturi-tion. In the case of M. H. (Case V.) it ought tohave been so, for it came from the kidney, but inthe case of Mr. S. (Case IV.) it ought not to havebeen so, for as a rule a tumor in the bladder bleedsonly toward the end of micturition when it issqueezed by the contracting bladder. The elementof uncertainty thus introduced was very puzzling.


THE MEDICAL NEWS.A National Weekly Medical Periodical, containing 24-28 Double-
Columned Quarto Pages of Reading Matter in EachIssue. $4.00 per annum, post-paid.
That The News fulfils the wants of men in active practice is madeclear by the steady growth of its subscription list. This increase ofreaders has rendered possible a reduction in the price of The News to$4.00 per year, so that it is now by far the cheapest as well as thebest large weekly journalpublished in America.
Every mode of conveying serviceable information is utilized. Theforemost writers, teachers and practitioners of the day furnish originalarticles, clinical lectures and notes on practical advances; the latestmethods in leading hospitals are promptly reported; a condensed sum-mary of progress is gleaned each week from a large exchange list, com-prising the best journals at home and abroad ; a special department isassigned to abstracts requiring full treatment for proper presentation ;editorial articles are secured from writers able to deal instructively withquestions of the day; books are carefully reviewed; society proceedingsare represented by the pith alone; regular correspondence is furnished bygentlemen in position to know all occurrences of importance in the districtsurrounding important medical centres, and minor matters of interest aregrouped each week under news items. Everything is presented with suchbrevity as is compatible with clearness, and in the most attractive manner.In a word, The Medical News is a crisp, fresh, weekly newspaper, andas such occupies a well-marked sphere of usefulness, distinct and comple-mentary to the ideal monthly magazine, The American Journal ofthe Medical Sciences.
The American Journal of the Medical Sciences.Published monthly. Each number contains 112 octavo pages,
illustrated. $4.00 per annum, post-paid.In his contribution to A Century ofAmerican Medicine, published in
1876, Dr. John S. Billings, U. S. A., Librarian of the National MedicalLibrary, Washington, thus graphically outlines the character and servicesofThe American Journal; “The ninety-seven volumes of this Journalneed no eulogy. They contain many original papers of the highest value;nearlyall the real criticisms and reviews which we possess ; and such care-fully prepared summaries of the progress of medical science, and abstractsand notices of foreign works, that from this file alone, were all other pro-ductions of the press for the last fifty years destroyed,it would be possibleto reproduce the great majority of the real contributions of the world tomedical science during that period."
COMMUTATION NATE.—Postage paid.The Medical News, published every Saturday,The American Journal of the Medical
Sciences, monthlyJ
>■ in advance, $7.50j
LEA BROTHERS & CO., 706 and 708 Sansom St, Phi/a.










![YYYYYYYYYYYYYYYYYYYYYYYYYY YYYYYYYYYYYYYYYYYY ... · urinary tract infections 3 diagnosis of utis w ] v [ sample urine collection suprapubic aspiration voided catether infectionif](https://static.fdocuments.us/doc/165x107/602fc10db774850ed7362f07/yyyyyyyyyyyyyyyyyyyyyyyyyy-yyyyyyyyyyyyyyyyyy-urinary-tract-infections-3-diagnosis.jpg)







