First: What are MDS? David Steensma, MD FACP
7
9/24/2018 1 Myelodysplastic Syndromes (MDS) David Steensma, MD FACP Associate Professor of Medicine, Harvard Medical School Adult Leukemia Program, Dana-Farber Cancer Institute Aplastic Anemia & MDS International Foundation Patient & Family Forum Providence/Warwick - September 2018 First: What are MDS? Four defining features of MDS 1) Marrow failure -> symptoms (low blood counts (=cytopenias) – anemia is most common) 2) Clonal disorders (abnormal chromosomes/ karyotype; acquired DNA mutations) 3) Characteristic “dysplastic” blood and marrow cell appearance (i.e., abnormally formed cells) 4) Instability / tendency to progress to acute myeloid leukemia– formerly “preleukemia” Age-dependent nature of MDS (US) Age at MDS diagnosis (years) *P for trend < .05 0 10 20 30 40 50 < 40 40-49 50-59 60-69 70-79 ≥ 80 0.1 0.7 2.0 7.5 20.9 36.4* Females Males Overall Overall incidence in this analysis: 3.4 per 100,000 SEER registry: ~13,000 new US cases per year Claims-based data: >30,000 US cases per year Rollison DE et al Blood 2008;112:45-52. How do MDS originate? Jean Miélot (d. 1472), Brussels Royal Library DNA replication error rate: ~1 error in 10 8 base pairs (100 million) But 99% of the errors are corrected… So, net: ~1 in 10 10 base pairs (10 billion) Each cell has 3 x 10 9 base pairs (3 billion) So ~1 in 3 chance of an error with each cell division But most (>99%) errors are meaningless What about MDS after chemotherapy or radiation for another disease? (i.e., “therapy-related” or “t-MDS”) TP 53 Diverse bone marrow stem cells A pre-existing TP53 mutant cell exists in some people TP 53 TP 53 TP 53 TP 53 TP 53 Clonal expansion Clonal sweeping (MDS) TP53 mutant cells survive stress better TP 53 TP 53 TP 53 TP 53 TP 53 TP 53 TP 53 TP 53 TP 53 TP 53 TP 53 TP 53 TP53 mutant cells come to dominate; Some have acquired additional mutations Anti-cancer therapy
Transcript of First: What are MDS? David Steensma, MD FACP

9/24/2018
1
Myelodysplastic Syndromes (MDS)
David Steensma, MD FACPAssociate Professor of Medicine, Harvard Medical School
Adult Leukemia Program, Dana-Farber Cancer Institute
Aplastic Anemia & MDS International Foundation Patient & Family Forum
Providence/Warwick - September 2018
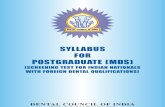
First: What are MDS?
Four defining features of MDS
1) Marrow failure -> symptoms (low blood counts (=cytopenias) – anemia is most common)
2) Clonal disorders (abnormal chromosomes/ karyotype; acquired DNA mutations)
3) Characteristic “dysplastic” blood and marrow cell appearance (i.e., abnormally formed cells)
4) Instability / tendency to progress to acute myeloid leukemia– formerly “preleukemia”
Age-dependent nature of MDS (US)
Age at MDS diagnosis (years)*P for trend < .05
0
10
20
30
40
50
< 40 40-49 50-59 60-69 70-79 ≥ 80
0.1 0.72.0
7.5
20.9
36.4*
FemalesMalesOverall
Overall incidence in this analysis: 3.4 per 100,000
SEER registry: ~13,000 new US cases per year
Claims-based data: >30,000 US cases per year
Rollison DE et al Blood 2008;112:45-52.
How do MDS originate?
Jean Miélot (d. 1472),Brussels Royal Library
DNA replication error rate:~1 error in 108 base pairs (100 million)
But 99% of the errors are corrected…So, net: ~1 in 1010 base pairs (10 billion)
Each cell has 3 x 109 base pairs (3 billion)
So ~1 in 3 chance of an error with each cell divisionBut most (>99%) errors are meaningless
What about MDS after chemotherapy or radiation for another disease?
(i.e., “therapy-related” or “t-MDS”)
TP53
Diverse bone marrowstem cells
A pre-existing TP53 mutant cell exists
in some people
TP53
TP53
TP53
TP53 TP
53
Clonal expansion Clonal sweeping
(MDS)
TP53 mutant cellssurvive stress
better
TP53
TP53
TP53TP
53TP53
TP53
TP53
TP53
TP53
TP53
TP53
TP53
TP53 mutant cellscome to dominate;
Some have acquired additional mutations
Anti-cancer therapy

9/24/2018
2
Parameter Categories and Associated Scores
Cytogenetic risk group
Very good Good Intermediate Poor Very Poor
0 1 2 3 4
Marrow blast proportion
≤2% >2 - <5% 5 - 10% >10%
0 1 2 3
Hemoglobin≥10 g/dL 8 - <10 g/dL <8 g/dL
0 1 1.5
Absolute neutrophil count
≥0.8 x 109/L <0.8 x 109/L
0 0.5
Platelet count≥100 x 109/L 50 - 100 x 109/L <50 x 109/L
0 0.5 1
From: Greenberg P et al Blood 2012 Sep 20;120(12):2454-65. Epub 2012 Jun 27
MDS risk stratification: Revised International Prognostic Scoring System (IPSS-R)
Risk group Points % patientsMedian survival,
years
Median survival for pts under 60
years
Time until 25% of patients develop
AML, years
Very low 0-1.5 19% 8.8 Not reached Not reached
Low 2.0-3.0 38% 5.3 8.8 10.8
Intermediate 3.5-4.5 20% 3.0 5.2 3.2
High 5.0-6.0 13% 1.5 2.1 1.4
Very high >6.0 10% 0.8 0.9 0.7
Why Has Therapy of MDS Been So Challenging?
Unlike leukemia, there are no widely useful MDS “cell lines”.
Several animal models now exist, but may not be
representative. This makes screening targeted agents more
challenging.
Images from medieval Bestiarum Vocabulum
Challenge #1 to narrowly
targeted therapies
Genetically modified mouse for disease modeling
Genomic architecture of MDS. Frequency of driver mutations identified in the sequencing
screen or by cytogenetics in the cohort of 738 patients, broken down by MDS subtype.
Papaemmanuil E et al. Blood 2013;122:3616-3627
Long “tail” of lesions present at
<2% level
Challenge #2 to developing
narrowly targeted therapies
How can MDS be treated?
Goals of Care in MDS

9/24/2018
3
Supportive care(Transfusions,Iron chelation,Growth factors,
etc)
Disease-modifying therapies
(Lenalidomide,Azacitidine,Decitabine;
Clinical trial drugs)
Allogeneic hematopoietic cell
transplant
Supportive care(Transfusions,Iron chelation,Growth factors,
etc)
Transfusion principles
• Whole blood is separated into red blood cells (RBCs), platelets, and plasma
• Red cells: typical volume is 250 mL (a half pint)– 1 Unit raises hemoglobin ~1 g/dL, hematocrit ~3%– Typically given for hemoglobin <8 g/dl or symptoms, hematocrit <24%– Common reactions include fevers, fluid overload, hives; infections very rare today– Irradiated if patient may be transplanted; leukoreduced for all– Special types: HLA matched, washed
• Platelets: typical volume is ~300 mL (6 pooled units or 1 apheresis/single-donor unit)– Typically given for platelet count <10 x 109/L; raises by variable amount (average 30)– Level needs to be 30 x 109/L for mildly invasive procedures, 50 x 109/L for most
surgeries/lumbar puncture, 100 x 109/L for neurosurgery– Common reactions include fevers, hives– Patients can become “immune” (alloimmunized) with time
• White cells (granulocytes) can’t be transfused except under very special circumstances
EPO = erythropoietinProducts in the US: epoetin alfa (Procrit)
darbepoetin alfa (Aranesp)
How does the marrow make red cells?
Who is likely to respond to Erythropoiesis Stimulating Agents (ESAs) in MDS?
Total Score (from below)IWG 2000 erythroid
response rate (patients)
High likelihood of response: > +1 74% (n=34)
Intermediate likelihood: -1 to +1 23% (n=31)
Low likelihood of response: < -1 7% (n=39)
Hellstrom-Lindberg E et al Br J Haem 2003; 120:1037
International Working Group (IWG) 2000 Erythroid Response Criterion: >1.5 g/dL Hb increment, or transfusion independence
Serum EPO level (U/L) RBC transfusion requirement
<100 = +2 pts <2 Units / month = +2 pts
100-500 = +1 pt ≥2 Units / month = -2 pts
>500 = -3 pts
Cumulative probability of survival among 374 MDS patients at Pavia, Italy, 1992–2002 (Transfusion-associated hazard ratio for death, 1.58; P=0.005)
Redrawn by DPS from Cazzola M and Malcovati L NEJM 2005; 352:536-8
“The risk of RBC transfusion dependence in MDS”?implications for iron chelation
% ALIVE
TIME -->
Oxidation (rust!)

9/24/2018
4
Available iron chelators
Deferasirox
Deferiprone –not approved for MDS in US
Deferoxamine Wheatgrass –unapproved supplement
What about platelet growth factors? (“Thrombopoiesis stimulating agents”)
• Goal: reduce need for platelet transfusions and “clinically significant bleeding events”
• Moderately successful in MDS
• Not FDA approved for MDS – Approved for other conditions
• Early studies raised concern about blast growth stimulation– More recent analyses suggest only
modest effect
Why don’t we use white cell growth factors commonly in MDS?
• Cost• Never been shown to improve
survival• Very modest benefit
Neutrophil dysfunction• Side effects (e.g., bone pain,
fevers, spleen rupture, leukemoidreaction)
• Some blasts may use as a growth factor
Disease-modifying therapies
(Lenalidomide,Azacitidine,Decitabine;
Clinical trial drugs)
Lenalidomide in MDSMeasure MDS-003 MDS-004 MDS-002 MDS-005
Transfusion Independence
67% 56% 26% 27%
Complete Cytogenetic
Response45% 29% 9% <10%
Median Response Duration
> 2 years 83 weeks 41 weeks 33 weeks
Del(5q) is the strongest genetic predictor of response for MDS
TP53 mutations are markers of shorter survival/relapse
List A et al NEJM 2005; Raza A et al Blood 2008; Fenaux P et al Blood 2011; Santini V et al JCO 2015
del(5q) Non-del(5q)
AZA-001 survival study (Higher risk MDS):Azacitidine vs “Conventional care”
Log-Rank p=0.0001
HR = 0.58 [95% CI: 0.43, 0.77]
Deaths: Aza = 82, Control = 113
0 5 10 15 20 25 30 35 40
Time (months)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Pro
port
ion s
urv
ivin
g
Control arm(supportive care or chemotherapy)
Azacitidine
Difference: 9.4 months
24.4 months
15 months
Fenaux P, et al. Lancet Oncology 2009 10: 223–232
May be better to give 7 days than <7 daysIV same as SC

9/24/2018
5
Decitabine (D-0007) registration study outcomes
Time to death or AML, all patients (p=0.16)
Time to death or AML, higher-risk patients
(p=0.028)
How do azacitidine or decitabine work? Unknown…
Navada SC et al J Clin Invest. 2014
Is it…• “Hypomethylation” and
reactivation of tumor suppressors?• DNA damage similar to traditional
chemotherapy (nucleoside analogues)?
• Activation of endogenous immunity (eg interferon pathways?)
• Presentation of neo-epitopes/immune response?
Comparison to decitabine failure : median survival 4.3 months, n=87
Outcomes after azacitidine or decitabine failure
Prébet T et al, J Clin Oncol 2011; Aug 20;29(24):3322-7. Epub 2011 Jul 25.Jabbour E et al, Cancer 2010; 116:3830–3834.
Outcomes after failure
Median overall survival after azacitidine fails the patient: 5.6 months
2 year survival: 15%
Favorable factors: female, younger (<60), better risk chromosomes/karyotype, <10% blasts, some response to azacitidine
What Are The Greatest Needs In The MDS Field?
MDS clinical research priorities
• More accurate diagnostic methods– Current techniques are to some extent subjective– Molecular testing is helping in ambiguous cases
• Better prognostication– There are limits to this, but helps decide on therapy
• Better systems of health care delivery– In the US we use our health care dollars poorly /
inefficiently
• Improved therapy
Largest specific unmet therapeutic needs
• Increase proportion of aza/decitabine responders– Current complete response rate 10-20%– Current overall response rate 40-50%– Average duration of response 8-11 months– Need to increase also depth of response and duration
• Treatments for patients after aza/decitabine stop working
• Treatments for “higher” lower risk patients– Defined by molecular genetics or other features
• Who else does lenalidomide work for besides people with del(5q)?
• Other curative therapies besides transplant

9/24/2018
6
What About Stem Cell Transplant?
800 to 1000 transplants in the
US annually for MDS indication
What Is Coming Next?
Predicting the future accurately is notoriously difficult. Where are our robot housekeepers, rocket trains, and flying cars?!
Representative experimental therapies
• Luspatercept– Antibody given every 3 weeks; MEDALIST trial is 48 weeks vs placebo
• Imetelstat– Inhibitor of telomerase
• Oral azacitidine (CC-486), oral decitabine+deaminase inhibitor (cedazuridine/ASTX727)
• SGI-110/guadecitabine• Venetoclax
– Inhibitor of BCL-2; approved for CLL/lymphoma
• Immune checkpoint inhibitors (nivolumab, pembrolizumab, ipilimumab)– Approved for solid tumors; limited activity in MDS alone, but in
combination?
• Chimeric antigen receptor (CAR-T) cells– Need to define ideal target (CD33? CD123?)
An approach to MDS
Cytopenia(s) Disease feature First-line therapy
Anemia only Del (5q) Lenalidomide
No del(5q), serum EPO <500 Erythropoiesis stim. agent
No del(5q), serum EPO >500 ?Immunotherapy
Neutropenia or thrombocytopenia or both
No standard established; observation, growth factors, azacitidine/decitabine
Lower-risk MDS (assessed using IPSS-R, etc.)
Higher-risk MDS
Allogeneic SCT candidate? Therapeutic approach
Yes Proceed to transplant ASAP; azacitidine, decitabine or chemotherapy may be useful as a “bridge”
No Azacitidine; decitabine as alternate
Supportive care for all (transfusions and antimicrobials PRN, ?iron chelation)
Partly based on 2018 NCCN guidelines; see www.nccn.org