First International Conference on Evidence- based healthcare (Pre-Conference Workshops on Topics...
30
First International Conference on Evidence- based healthcare (Pre-Conference Workshops on Topics related to Evidence Based Medicine) The Inaugural Conference of the International Society of Evidence-based Health Care When and Where? Workshops: 06 October 2012 Conference: 07 – 08 October 2012 Venue: India International Centre, New Delhi Contact email: [email protected]
-
Upload
rebecca-carlson -
Category
Documents
-
view
217 -
download
1
Transcript of First International Conference on Evidence- based healthcare (Pre-Conference Workshops on Topics...

First International Conference on
Evidence- based healthcare(Pre-Conference Workshops on Topics related to Evidence Based Medicine)
The Inaugural Conference of the International Society of Evidence-based Health Care
When and Where?Workshops: 06 October 2012Conference: 07 – 08 October 2012Venue: India International Centre, New
DelhiContact email:[email protected]

Who should attend?
• Physicians, Nurses, medical students involved in the implementation of evidence including frontline healthcare professionals
• Educators involved in teaching and training in evidence based healthcare
Speakers
• Tony Dans, Kameshwar Prasad, Paul Glasziou• Chile, Pakistan, Peru, Taiwan

Contact address:“ISEHCON 2012”Clinical Epidemiology Unit Room No-91, Near Examination Section,All India Institute of Medical SciencesAnsari Nagar, New Delhi-110029, IndiaPhone: +91-11-26594436/26588434Email: [email protected]

The First International Conference for Evidence-based Healthcare

Evidence-based personalized medicine: Plan for talk
subgroup effects
varying baseline risk
values and preferences
trial of therapy

Is there true variation in effects?
Patients• Severity/stage
Intervention• intensity/timing?
Outcome?• Short versus long-term

RR 0.67RD 10%
RR 0.67RD 3.3%
RR 0.67RD 1%

Subgroup Analysis: The ISIS-2 Study
ASAASA
N=8587N=8587PlaceboPlacebo
N=8800N=8800
Overall MortalityOverall Mortality 9.4%9.4% 11.8%11.8%
11.1%11.1% 10.3%10.3%
9.26%9.26% 12%12%
-23%
+9%
-28%
Subgroup 1Subgroup 1
Subroup 2Subroup 2

Subgroup Analysis: The ISIS-2 Study
ASAASA
N=8587N=8587PlaceboPlacebo
N=8800N=8800
Overall MortalityOverall Mortality 9.4%9.4% 11.8%11.8%
11.1%11.1% 10.3%10.3%
9.26%9.26% 12%12%
-23%
+9%
-28%
Gemini or LibraGemini or Libra
Other astrological Other astrological signssigns

Sub-group hypotheses disproved Aspirin ineffective in secondary prevention of stroke in women
Antihypertensives for primary prevention ineffective in women
Antihypertensive treatment ineffective or harmful in elderly
ACEI don’t reduce mortality in CHF patients taking ASA
ß blockers are ineffective after acute MI in elderly
Thrombolysis for acute MI ineffective in previous MI
Tamoxifen ineffective in breast cancer aged <50 years High-dose ASA better than low dose in carotid endarterectomy
Amlodipine reduces deaths in non-ischaemic but not ischemic cardiomyopathy
Platelet-activating factor receptor antagonist reduces mortality in gram-negative sepsis but not in other sepsis
Ticlopidine better than ASA for recurrent stroke in blacks but not whites
Valsartan reduces deaths in patients not receiving ACEI and beta blockers, but not in those who are

Patient presents with tibial fracture
reaming, big nails• more stable
no reaming, small nails• maintains blood supply
could effect differ with fracture severity?• open versus closed

Large RCT: SPRINT
some patient open, some closed
randomized to reamed/unreamed
differences from prior trials• concealed randomization• blinded adjudication of outcomes• proscription from re-operation for delayed union
for six months
1319 randomized, 1226 (93%) followed 1 yr

SPRINT (stratified RRs)
1 20.5
Reamed Nonreamed Relative Risk (95% CI)
Closed Fractures 45/416 68/410 0.67 (0.47, 0.96)
Open Fractures 60/206 46/194 1.27 (0.91, 1.78)
All Patients 105/622 114/604 0.90 (0.71, 1.15)

Believe sub-group analysis – open vs closed tibial fractures?
• within-study comparison? yes
• large difference in effect yes
• unlikely chance p = 0.01
• consistent across studies no
• a priori hypothesis yes
• one of small number hypotheses yes
• biologically compelling yes

Patients with atrial fibrillation
risk of stroke varies• CHADS2: congestive heart failure; hypertension; age
>75; diabetes; prior stroke
risk of stroke varies• CHADs2 0: 8 per 1,000 per year• CHADs2 1: 22 per 1,000 per year• CHADS2: 45 per 1,000 per year• CHADS3: 96 per 1,000 per year
Warfarin 2/3 relative risk reduction• CHADs2 0: 5 per 1,000 per year• CHADs2 1: 14 per 1,000 per year• CHADS2: 40 per 1,000 per year• CHADS3: 64 per 1,000 per year

Comparison of patient and Comparison of patient and physician valuesphysician values
• to anticoagulate or not to anticoagulate to anticoagulate or not to anticoagulate patients with atrial fibrillation: differences patients with atrial fibrillation: differences between physician and patient perspectivesbetween physician and patient perspectives– Devereaux PJ et. al., BMJ, 2001Devereaux PJ et. al., BMJ, 2001
• face to face interview of 63 physicians and face to face interview of 63 physicians and 61 patients61 patients
• probability trade-off tool to determine and probability trade-off tool to determine and compare physician and patient thresholds compare physician and patient thresholds for how much stroke reduction is necessary for how much stroke reduction is necessary and how much bleeding risk is acceptable and how much bleeding risk is acceptable for antithrombotic therapy in atrial for antithrombotic therapy in atrial fibrillationfibrillation

Devereaux et. al., 2001Devereaux et. al., 2001
• patients with atrial fibrillation at high risk of strokepatients with atrial fibrillation at high risk of stroke
• warfarin decreases risk at cost of increased gi warfarin decreases risk at cost of increased gi bleedsbleeds
• without treatment 100 patients will suffer:without treatment 100 patients will suffer:– 12 strokes (six major, six minor), 3 serious gi bleeds in 2 12 strokes (six major, six minor), 3 serious gi bleeds in 2
yearsyears
• warfarin would decrease strokes in 100 patients to warfarin would decrease strokes in 100 patients to 4 per 2 years (8 fewer strokes, 4 major, minor)4 per 2 years (8 fewer strokes, 4 major, minor)
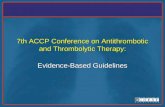
• how many bleeds would you accept in 100 patients how many bleeds would you accept in 100 patients over a year, and still be willing to administer/take over a year, and still be willing to administer/take warfarin?warfarin?

Devereaux et. al., 2001Devereaux et. al., 2001• patients with to atrial fibrillation at high risk of patients with to atrial fibrillation at high risk of
strokestroke
• warfarin decreases risk at cost of increased gi bleedswarfarin decreases risk at cost of increased gi bleeds
• without treatment 100 patients will suffer:without treatment 100 patients will suffer:– 12 strokes (six major, six minor), 3 serious gi bleeds in 2 12 strokes (six major, six minor), 3 serious gi bleeds in 2
yearsyears
• warfarin would decrease strokes in 100 patients to 4 warfarin would decrease strokes in 100 patients to 4 per 2 years (8 fewer strokes, 4 major, minor)per 2 years (8 fewer strokes, 4 major, minor)
• how many bleeds would you accept in 100 patients how many bleeds would you accept in 100 patients over a year, and still be willing to administer/take over a year, and still be willing to administer/take warfarin?warfarin?

0
5
10
15
20
25
30
35
40
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22
MAXIMUM NUMBER OF ACCEPTABLE EXCESS BLEEDS
NU
MB
ER
OF
PH
YS
ICIA
NS
/PA
TIE
NT
S
Physicians N=63
Patients N=61
PHYSICIAN AND PATIENT BLEEDING THRESHOLDS FOR WARFARIN

Limitations of RCTs variable response
• if it worked, likely not in all•didn’t work, subgroup of responders
with binary outcomes, most subgroup hypotheses (relative effects) spurious
but symptomatic treatment presents opportunity

Conventional trial of therapy
give medication, do you feel better?
what are the problems?•natural history•placebo effects•patient and physician expectations•desire to please

R R
INDIVIDUAL PATIENT
PRN
REGULAR MONITORING OF TREATMENT TARGET
ACTIVE TREATMENT
PLACEBO
OR ALTERNATIVE
A P
R R
INDIVIDUAL PATIENT
PRN
REGULAR MONITORING OF TREATMENT TARGET
ACTIVE TREATMENT
PLACEBO
OR ALTERNATIVE
RR RR
INDIVIDUAL PATIENT
INDIVIDUAL PATIENT
PRN
REGULAR MONITORING OF TREATMENT TARGET
ACTIVE TREATMENT
PLACEBO
OR ALTERNATIVE
A P

Fibromyalgia
chronic condition
aches and pains
fatigue
sleep disturbance
irritable bowel syndrome


N of 1 RCT – Ms. M.P.N of 1 RCT – Ms. M.P.
Amitriptyline 20 mg. o.d.Amitriptyline 20 mg. o.d.
Duration of periods: 4 weeksDuration of periods: 4 weeks
3 pairs3 pairs
Outcomes:Outcomes:– weekly rating of symptomsweekly rating of symptoms
• energy level, tirednessenergy level, tiredness
• aches and painsaches and pains• morning stiffnessmorning stiffness• sleep disturbancesleep disturbance• headachesheadaches• bowel disturbancebowel disturbance

How much energy have you had in the last week?
1.1. No energy at allNo energy at all
2.2. A little energyA little energy
3.3. Some energySome energy
4.4. Moderately energeticModerately energetic
5.5. Quite a bit of energyQuite a bit of energy
6.6. Very energeticVery energetic
7.7. Full of energyFull of energy



When is N of 1 appropriate? you have a cold – N of 1? too short, not important enough
you have appendicitis – N of 1? only once
you have depression – N of 1? treatment takes too long
chronic lung disease, bronchodilator – N of 1? chronic condition, symptoms important, medication acts fast, variable
response

Personalizing EBM
different relative effects (rarely)
different absolute effects (usually)
applying N of 1 principle (sometimes)
individualized values and preferences (always)• only the patient can tell you his/her values