Fna Fine Needle Aspiration Cytology and Core Biopsy Guide for Practice

J Clin Pathol 1983;36:1036-1045
Fine needle aspiration biopsy of the thyroid gland: a
study of 304 cases
KENNETH C SUEN, NOEL F QUENVILLE*
From the Department of Pathology, and the *Division ofAnatomical Pathology, Vancouver GeneralHospital, University of British Columbia, Vancouver BC, Canada
SUMMARY We discuss the interpretation of thyroid aspiration cytology in the light of our experi-ence and review the circumstances in which false positives and false negatives may occur. Thetechnique is reliable but by no means infallible and it should not be regarded as a final diagnosticwork-up. Its value lies in selecting patients with thyroid nodules for surgery. In the present seriesof 304 patients, 79 underwent operation and 37 malignancies were found. The incidence ofmalignancy among the surgically excised nodules was 47%, in contrast to 14% in the past. Weestimated that 268 operations would be required to salvage the same number of malignancieswithout the use of fine needle aspiration biopsy.
Whether one should excise a "cold" thyroid noduleor manage it conservatively is a question that con-tinues to provoke controversy.1-3 The main reasonfor such a problem to exist is that thyroid nodulesare common while the incidence of thyroid cancer islow. Based on necropsy data, Sokal estimated thatfewer than 1% of unselected nodular goitres weremalignant.4 On the other hand, in most series ofsurgically excised thyroid nodules about 10% to20% proved to be malignant on histologicalexamination.-7 The higher incidence of malignancyamong the surgically treated patients reflectspreoperative efforts in patient selection and doesnot give a true picture of the natural course of all thethyroid nodules in the general population. Neverthe-less, with a five to one chance that the noduleremoved is benign, there is obviously a need formore precision in the preoperative discriminationbetween malignant and benign thyroid nodules. Wehave been interested in evaluating the fine needleaspiration biopsy (FNAB) in fulfilling this need.This paper reviews our experience with FNAB per-formed at a large municipal hospital during thefour-year period, 1978-1981. Reliable follow-upinformation and sufficient experience have nowaccumulated to answer many of the questionsregarding the advantages and pitfalls of the aspira-tion technique. The literature on this subject is alsoreviewed.
Accepted for publication 20 April 1983
Material and methods
Fine needle aspiration biopsy can be safely per-formed on an outpatient basis. The patient lies com-fortably in a supine position and the neck isextended with a pillow placed under the shouldersand neck. The skin overlying the lesion is cleanedwith an antiseptic. No local anaesthesia is required.The lesion is punctured with a 23 gauge needle con-nected to a 10 ml air-tight plastic syringe. When theneedle has entered the nodule, the plunger is thenretracted to create a vacuum in the syringe. Theneedle is moved back and forth several times withinthe lesion as material is aspirated into the needle bythe negative pressure. Just prior to the withdrawal ofthe needle from the lesion, the plunger is released toeliminate the vacuum, thereby avoiding aspirationof the sample into the syringe barrel. To expel theaspirated material onto the glass slides, the needlecontaining the sample is first detached from thesyringe and the plunger is withdrawn to allow airinto the syringe. The needle is re-attached and theneedle content is ejected on the slides by pushingdown the plunger. Several smears are made andpromptly fixed in 95% ethyl alcohol for haematoxy-lin and eosin or Papanicolaou staining. The needleand syringe are rinsed with physiological saline andthe contents are used for membrane filter prepara-tion. With experience, one can also reliably judgethe adequacy of a sample by naked-eye examinationof the prepared smears. If the sample is considered
1036
copyright. on June 15, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.36.9.1036 on 1 Septem
ber 1983. Dow
nloaded from

Fine needle aspiration biopsy of the thyroid gland: a study of 304 cases
inadequate, aspiration is repeated immediately.Other investigators, particularly those with train-
ing in haematology, have preferred air-dried smearsstained by a Romanovsky method. We have chosenthe haematoxylin and eosin technique partlybecause it is a stain more familiar to tissue patholog-ists and it facilitates morphological correlation bet-ween cells seen in the smears and in the tissue sec-tions. Both the haematoxylin and eosin and thePapanicolaou stains performed on alcohol-fixedsmears provide sharp nuclear detail which is lessevident on Romanovsky-stained smears. However,the latter stain delineates better metachromatic sub-stances such as connective tissue stroma and colloidmaterial. The choice of staining procedures dependson the pathologist's training background and it willnot affect the results so long as he is familiar with thestain and is using the same technique consistently.
During the four-year period from 1978 to 1981,at the Vancouver General Hospital, there was atotal of 331 fine needle aspiration biopsies of thethyroid, of which 27 were subsequently excludedfrom this study for the following reasons: inadequ-ate material for interpretation (15 cases), nofollow-up data available (11 cases) and metastaticcarcinoma from other site (1 case). The remaining304 cases constituted the basis for this study. All thepatients had radioiodine scintiscanning and 96%had ultrasonography. Solitary "cold" nodules andmultinodular goitres with the presence of onedominant "cold" nodule accounted for 235 cases or78% of the total. Ultrasound further divided the"cold" nodules into solid (126 cases), cystic (64cases) and mixed (45 cases). At the time of thebiopsy the patient was examined by the clinician andthe pathologist, and all clinical and laboratory datawere reviewed. The close collaboration between thepathologist and the clinicians has proved to beextremely valuable, not only for the technical prep-aration of the smears but also for the correlation ofthe cytological findings with the clinical and laborat-ory findings.
CYTOLOGICAL INTERPRETATION
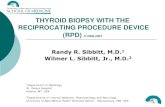
Poorly differentiated carcinomas (Fig. 1)Cytological diagnosis of this group of tumours doesnot pose a problem. The smears contain abundantneoplastic cells which are loosely cohesive. Theusual cellular criteria of malignancy are present,such as anisokaryosis, nuclear hyperchromatism,irregular chromatin clumping and frequently promi-nent nucleoli.
Papillary carcinomaThe aspirated material contains mostly intact tissue
Fig. 1 Poorly differentiated thyroid carcinoma. Note loosecellular cohesion, marked anisokaryosis, andhyperchromatism with coarse clumping and clearing ofchromatin. Haematoxylin and eosin x 520.
fragments rather than free cells. In a typical cellularsample, there are three types of tissue fragments:papillary, monolayered and multilayered. The papil-lary tissue fragment is diagnostic for this tumourtype and it exhibits a stereoscopic configuration bestappreciated by moving the plane of focus of the mic-roscope up and down, a smooth well-definedperipheral outline and a complex ramifying patternreflecting papillary growth (Fig. 2). The constituentcells are crowded and may show nuclear overlappingor moulding, but size variation is usually minimal.The nuclei are characteristically hypochromatic andvesicular or glassy, with a small nucleolus. In someaspirates, only smaller or single papillary fronds arepresent (Fig. 3). A monolayered tissue fragmentdisplays tumour cells in one plane of focus. The lackof a three-dimensional configuration with flatteningof cells in smears probably helps to exaggerate thesize of the tumour cells, which generally appear tobe larger than those in the papillary fragments; nuc-lear pleomorphism is also more evident (Fig. 4a).Sometimes carcinoma cells appear squamoid, with-out signs of keratinisation. The squamoid changesare most often seen in monolayered tissue fragments(Fig. 4b). A multilayered tissue fragment consists ofmarkedly superimposed tumour cells with apparentdisorganisation and the fragment contour exhibitsirregularity (Fig. 5a). Both monolayered and mul-tilayered fragments do not permit accurate typing ofthe cancer unless an additional finding of "ground
1037
copyright. on June 15, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.36.9.1036 on 1 Septem
ber 1983. Dow
nloaded from

Suen, Quenville
..... .. - .. _, W..Fig. 2 A large papillary tissue fragment composed ofnumerous papillary fronds, giving rise to a complexramifying pattern. Haematoxylin and eosin x 125.
glass" nuclei or psammoma bodies is present. Thefinding of multilayered tissue fragments is commonin aspirates of any cellular neoplasms and they arenot necessarily derived from a papillary carcinoma.
In about 50% of our cases, the tumour cellsexhibit intranuclear inclusions of the cytoplasm,so-called pseudonucleoli (Fig. 4a). Although com-monly associated with thyroid papillary carcinoma,these cytoplasmic invaginations have been observedin other lesions including adenocarcinomas andmelanoma.8 9 Twenty per cent of our aspirates con-tain psammoma bodies. These are basophilic, lami-nated spherules measuring 30-100,um in diameter(Fig. 5b), and must not be confused with dystrophiccalcifications which can be seen in involutionalgoitres and occur as irregular, basophilic speckleslacking distinct laminations. In 10% of our cases, agreat number of lymphocytes are admixed with thetumour cells. An erroneous diagnosis of chroniclymphocytic thyroiditis may be made by the unwarybecause the numerous lymphocytes can obscure thepresence of tumour cells.
Follicular carcinomaThe aspirates are hypercellular and contain tumourcells that are dispersed, loosely arranged in follicularformations or grouped in tissue fragments withinwhich a follicular pattern may sometimes be seen.Cellular atypia varies from case to case, depending
. Fig. 3 Small papillary fronds withwell-defined, smooth contour. Theconstituent cells are at different focalplanes, resulting in a stereoscopicconfiguration. Haematoxylin andeosin x 520.
1038
69idLdiLk
A.
copyright. on June 15, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.36.9.1036 on 1 Septem
ber 1983. Dow
nloaded from

Fine needle aspiration biopsy of the thyroid gland: a study of 304 cases
al
I.
p
Jm-W,..0A. 0
Agp-:".t:.. *W",
a .0.
0 :4f. a
0
"A.-Ait
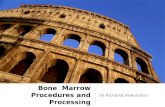
Fig. 4 Monolayered tissue fragments. (a) Note variation in
cell size ground glass vesicularity ofmany nuclei and
intranuclear cytoplasmic inclusions (arrows). (b) Note
squamoid appearance of tumour cells. Haematoxylin and
eosin (a) X 520, (b) X 520.
on the degree of differentiation. Some inves-
tigators"0 have attempted to characterise the
cytological alterations of cells of follicular car-
cinoma. These have included nuclear pleomorphismand overlapping, granular chromatinic pattern, con-
spicuous nucleoli and nuclear size larger than that of
adenoma (Fig. 6). Although these parameters may
have discriminatory value on a statistical basis, they
b
Fig. 5 (a) A group of tightly packed, superimposedtumour cells forming a multilayered iissue fragment. (b)Two psammoma bodies. Haematoxylin and eosin (a) x400, (b) x 520.
are not absolute and we have found them less usefulwhen applied to individual cases of well-differentiated follicular carcinoma whose nuclearfeatures frequently overlap those of adenoma. Mostauthors'2 13 agree that the final diagnosis should reston careful histological examination which permitsevaluation of the entire capsule and inspection forvascular involvement.
Medullary carcinoma (Fig. 7)As with all malignant tumours, the aspirates are cel-lular. The tumour cells are arranged singly and inloosely cohesive groups. The predominant cells arethe small, polyhedral cells with little pleomorphism.The nuclei are round to oval with hyperchromatic,
1039
I.: .L-.Ili-IL.I. lap
V
copyright. on June 15, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.36.9.1036 on 1 Septem
ber 1983. Dow
nloaded from

Suen, Quenville
...
_.i6 AL
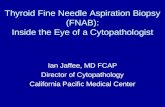
Fig. 6 Follicular carcinoma. Note numerous tumour cellsloosely grouped in a follicular pattern. The cells are largerthan those from adenoma and each nucleus contains a
conspicuous nucleolus. This patient subsequently developeda metastasis in the skull. Haematoxylin and eosin x 400.
chromatin. Nucleoli are not evident. The cytoplasmis usually abundant and many cells contain finecytoplasmic granules. Other cell forms can often beseen in the same smear: spindle-shaped cells,binucleate and multinucleate cells. Not infrequently,the tumour cell nuclei are eccentrically placed, giv-ing rise to a plasmacytoid appearance. No amyloid isseen in our material, but amyloid has been demons-trated in needle aspirates by others with alkalineCongo red stain.'4 Even in the absence of amyl6id,the combination of different cell forms with pre-
dominance of the small polyhedral cells, intracytop-lasmic granulation and plasmacytoid appearance ofsome tumour cells are cytologically suggestive ofmedullary carcinoma.
Follicular adenoma (Fig. 8a & 8b)The aspirates contain many tumour cells occurringin discrete small acinous units or in larger cell sheetswith a follicular pattern. The nuclei are round andregular, usually smaller than those seen in follicularcarcinoma. The chromatin is evenly distributed andthe nucleoli are frequently invisible. However,some cell samples obtained from an atypicaladenoma or an adenoma with retrogressive changesmay reveal cellular atypia that may be confused withcarcinoma. '5
Colloid goitre (Fig. 9)These samples are characteristically hypocellular.
Cyolsmo an el isabnnt an otaisganls
JV4W4
Fig. 7 Medullary carcinoma. Note combinaton ofsmallpolyhedral cells, spindle-shaped cells and binucleate cells.Cytoplasm ofmany cells is abundant and contains granules.Haematoxylin and eosin x 480.
The follicular epithelial cells occur in small mono-layered sheets. The cells are evenly spaced withinthe cell sheets, presenting a monomorphic honey-comb appearance. The nuclei are small, uniform andoval to round with homogeneously dark-stainingchromatin. Nucleoli are absent. Foamy histiocytesand colloid globules are commonly prtsent. In a fewcases of adenomatous goitre, the aspirates areunusually cellular and can be mistaken for a follicu-lar neoplasm. Even histological distinction may be aproblem.
CystsCystic lesions for the most part represent degener-ated involutional goitres with a predominant cysticcomponent. The aspirated fluid ranges from clearyellow to dark brown and typically contains a largenumber of histiocytes, some of which may be ladenwith haemosiderin pigments. A scant number ofbenign-appearing, atrophic follicular epithelial cellsare present.About 3% of the cystic lesions in our series
proved to be derived from cystic papillary car-cinoma. Chu and associates'6 warn that thepathologist should always routinely consider papil-lary carcinoma when examining a cystic lesion eventhough the vast majority of the cysts are benign. Cell
1040
....
XJ'.
Mithombl.
.4 p:0 6: %
v
.:X -kiL 's",
W. :A&.
V4
4 :1w..".A,-kL-. m.
"Wwt Z"imL
u -:11
0i.0i:ss
..'i4 ...
um%
copyright. on June 15, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.36.9.1036 on 1 Septem
ber 1983. Dow
nloaded from

Fine needle aspiration biopsy of the thyroid gland: a study of 304 cases
W
..p. A.J,:-4!$
a
Fig. 9 Colloid goitre. Figure shows a small sheet ofuniform,evenly-spaced follicular epithelial cells. Haematoxylin and eosinx 520.
Fig. 8 Follicular adenomas. (a) Uniform tumour cellsforming discrete follictdlar units. (b) A multilayered tissuefragment within which a follicular pattern is discernible.Haematoxylin and eosin (a) x 400, (b) x 400.
blocks or millipore preparations or both should bemade to minimise the risk of missing the cancercells.
ThyroiditisAspirates of chronic lymphocytic thyroiditis orHashimoto's thyroiditis show abundant small lym-phocytes with variable numbers of plasma cells andhistiocytes. When a germinal centre is aspirated,stimulated lymphocytes at various stages of matura-tion are seen, reminiscent of the cellular content of ahyperactive lymph node. Hurthle cells with pale,oxphilic cytoplasm are frequently present (Fig. 1Oa).The nuclei of the Hurthle cells sometimes can bequite large and atypical, simulating a Hurthle celltumour. In thyroiditis, however, an additional popu-lation of "normal" Hurthle cells with smaller andregular nuclei is also present, giving rise to a cytolog-
ical pattern referred by Nilsson'7 as "discontinuousanisokaryosis" (Fig. 10b). Conversely, smears of aHurthle cell tumour show usually a uniform singlepopulation of neoplastic cells.Other forms of thyroiditis are not specific on aspi-
ration but may be suspected from clinical featurescorrelated with dominant inflammatory cells seen onthe smears, including the multinucleate giant-cellform.'3 On the other hand, Perrson'8 expresses theopinion that different types of thyroiditis can be dis-tinguished on cytological grounds.
Results
The Table shows the results of FNAB and thefollow-up data of the 304 patients. Seventy-onecases were diagnosed by FNAB as neoplastic orprobably neoplastic. Seventy patients underwentsurgical exploration and 65 neoplasms were found(34 carcinomas, 1 lymphoma and 30 adenomas).The remaining five cases proved to be non-neoplastic, including four adenoma-like colloidgoitres and one subacute thyroiditis. One casereported by cytology as "suspicious for lymphoma"did not undergo operation because the clinical pre-sentation was that of chronic lymphocytic thyroiditisand the swelling subsided after thyroid suppressivetherapy. Hence, altogether there were six false posi-tive cytological reports.Follow-up of the 233 cases diagnosed as non-
1041
WM4m
copyright. on June 15, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.36.9.1036 on 1 Septem
ber 1983. Dow
nloaded from

Suen, Quenville
Table Results of304 fine needle aspiration biopsies
Cytological No Surgery withdiagnosis surgery histology
NeoplasmsCarcinoma 16 () Papillary carcinoma 12
Poorly diff carcinoma 2Follicular carcinoma 1Meduilary carcinoma 1
Suspected carcinoma 12 0 Papillary carcinoma 7Follicular carcinoma 3MeduUlary carcinonma 1Subacute thyroiditis 1*
Follicular neoplasm 41 0 Follicular carcinoma 6Papillary carcinoma 1Adenoma 30Colloid goitre 4*
Suspected lymphoma 2 1* Lymphoma 1
Non-neoplasrsCoiloid goitre 133 130 Colloid goitre 3Cysts 59 54 Papillary carcinoma 2t
Benign cystic goitre 3Chronic lymphocytic Chronic lymphocyticthyroiditis 41 40 thyroiditis 1
Total 304 225 79
*False-positive (6 cases).tFalse-negative (2 cases).No of neoplasms = 67.No of malignancies = 37.
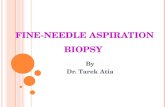
Fig. 10Hashimoto's thyroiditis. (a) Typical aspirate
showing numerous lymphocytes at various stages ofmaturation. A sheet ofHurthle cells is present on the left. (b)
Aspirate showing Huirthle cell hyperplasia. Note admixture
ofnormal-sized Huirthle cells and enlarged atypical Huirthlecells. Haematoxylin and eosin (a) x 400, (b) x 400.
neoplastic by cytology showed that nine nodules had
been treated surgically (Table). The nine cases com-
prised two papillary carcinomas, three benign cystic
goitres, three solid colloid goltres and one chronic
lymphocytic thyroiditis. The first two cases rep-
resented false-negative cytological reports. The
other 224 cytologically benign cases did not show
any clinical justification for operation. The benigndiagnoses were substantiated by a period of follow-
up ranging from one to five years.In the entire series of 304 patients, 79 underwent
operation. The incidence of neoplasms among thesurgically excised nodules was 85% (67 of 79) andthe incidence of malignancy 47% (37 of 79). Sixty-five of the 67 thyroid neoplasms were diagnosed or
suspected on fine needle aspiration biopsy. Twocases were missed. The sensitivity of the aspirationbiopsy (percentage of neoplasms detected by thetest) and the positive predictive value of the test(percentage of correct positive diagnoses) were cal-culated according to Galen and Gambino'smethod'9 as follows:
Sensitivity = true positives x 100true positives + false negatives65
= 2 x 100l= 97%65 + 2
Positive predictive value =
true positivesx 100
true positives + false positives65
= 65 + 6 x 100= 91%
The given number of false-negative cases (2) is a lowestimate, because most of the cytologically "benign"cases were not treated surgically and the period ofclinical follow-up was short (one to five years). Also,we deleted the 15 cases of technical failure fromconsideration in our results. Of these 15 cases,
i...>...
1042
copyright. on June 15, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.36.9.1036 on 1 Septem
ber 1983. Dow
nloaded from

Fine needle aspiration biopsy of the thyroid gland: a study of 304 cases
follow-up showed two Hurthle cell adenomas and ifthese two were included as false-negatives in thecalculation of "sensitivity", the result would beslightly lower-that is, 94%.
Discussion
FNAB is essentially a cytological method and fordiagnosis requires a much smaller sample than thatneeded for histological examination. Many phys-icians who are not aware of the differences betweenFNAB and the histological biopsy obtained by athick-core needle (Tru-Cut or Vim-Silvermanneedle) have unjustifiably regarded FNAB as aneasy and less accurate modification of the histo-logical biopsy. It is important to note that theaccuracy of cytological diagnosis, as far as thyroidaspiration is concerned, compares favourably withthat of the thick-core biopsy.20 21 Among the manyreports that consider the accuracy of FNAB, resultsvary, but in most large series the overall accuracyrate exceeds 90% with a 5 to 10% frequency offalse-positives and false-negatives.12 16 22-24 There areother advantages of fine needle aspiration biopsy. Itis a simple and safe procedure that can be performedon outpatients, with wide patient acceptance. It iscost effective, and can be repeated as necessary.Local anaesthesia, needed for thick-core biopsy, isnot necessary. Complications such as haematomaformation and transitory vocal cord paralysisencountered rarely with the Vim-Silverman orTru-Cut biopsy, are even rarer with the fine needlebiopsy.22-25 Two cases of tumour implantation in theneedle tract following the use of Vim-Silvermanneedle have been recorded in the literature.20 26Recently, Block et a127 reported a subcutaneousimplant of thyroid carcinoma six months aftersurgical excision of the tumour in a patient whosepreoperative assessment included fine needlebiopsy. The authors were careful to point out that itwas difficult to be certain of the origin of the tumourimplant. The large scale use of fine needle aspirationin Scandinavia has yet to result in any reports ofcancer implantation in the needle tract.'2 15 Whilethe rarity of complications and the many advantagesassociated with FNAB have encouraged morephysicians to use the FNAB technique in preferenceto the thick-core biopsy, others still feel that thetechnique has very little value as a routineprocedure in the investigation of thyroid-nodules.3 28 29 Opponents to the FNAB techniqueinsist that accurate diagnosis of a thyroid nodule canonly be ascertained by complete excision of the lesion.
It has been pointed out that the value of a proce-dure must be judged on more than merely correctdiagnosis: the final arbiter is how a technique
influences clinical practice.30 To assess the impact ofFNAB on patient care, we reviewed the pathologicalreports of all thyroidectomies performed between1974 and 1977, the four-year period immediatelypreceding the use of FNAB. Two hundred andforty-seven patients underwent thyroidectomy dur-ing that period and 34 patients (14%) were found tohave malignant lesions. In the aspiration series, 37patients or 47% of the 79 patients who underwentsurgery had malignancies. Two hundred and sixty-eight operations will be required to salvage the samenumber of malignancies if FNAB is not used.
All patients undergoing aspiration biopsy in ourseries were not operated upon and the possibility ofmissing a malignant tumour is not certain. It may bethat the given number of false-negative cases (2) inthe series is a low estimate. The literature indicatesthat the expected incidence of malignancy among"cold" thyroid nodules is between 10% and 20%. Inthe present study, a total of 37 cancers was detected,which represents a figure of 16% malignancy in thetotal number of "cold" nodules (235). This suggeststhat the number of thyroid malignancies that wemay have missed must have been small or negligible.Identification of all cancers is possible only if everynodule is excised. This is obviously impractical andpatient selection is desirable. A low ratio of malig-nant to benign nodules in a surgical series impliesmany unnecessary operations. With judiciouspatient selection, much unnecessary surgery wouldbe saved and most, if not all, cancers would beexcised.
It would be unrealistic to assume that cytologicaldiagnosis of thyroid nodules is simple and infalli-ble. Although cancer cells of the thyroid areabnormal, they often lack fully-developed, malig-nant cytological features. Conceivably, a less-than-certain cytological diagnosis of "suspicious for car-cinoma or neoplasm" is not infrequently made onlesions that subsequently prove to be carcinoma onhistological examination. This does not lessen thevalue of cytology as a screening tool because a "sus-picious" diagnosis is a clear indication of the needfor further investigation or surgical exploration.
False-negative reports can occur in the followingcircumstances:(i) In cystic papillary carcinoma. The two false-negatives in our series belong in this category. Onreview of the aspirates we still could not detect anycancer cells. This could be explained by the scantnumber of tumour cells present whose concentrationwas further diluted by the cystic content. Bothlesions were large cystic masses, measuring 4-5 cmand 5 cm each, and they promptly recurred follow-ing evacuation of the fluid. Walfish et a13' pointedout that although the incidence of malignancy in
1043
copyright. on June 15, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.36.9.1036 on 1 Septem
ber 1983. Dow
nloaded from

1044
small cystic lesions was generally minimal, cysticdegeneration of large malignant lesions could occur.Cysts larger than 4 cm or prompt reaccumulation ofhaemorrhagic fluid after repeated aspirations shouldraise the suspicion of malignancy.(ii) In the presence of chronic thyroiditis. Chroniclymphocytic thyroiditis can coexist with many typesof thyroid cancer. Friedman32 stressed that anincreased ratio of epithelial to lymphoid cells shouldarouse suspicion of an epithelial tumour associatedwith chronic thyroiditis. Hurthle cells ofHashimoto's thyroiditis have to be distinguishedfrom cells derived from a Hurthle cell tumour.Small cell carcinoma or lymphoma can also mimicchronic lymphocytic thyroiditis.32 33 If the diagnosisof thyroiditis is not supported by the patient's clini-cal course, further investigation is needed in anattempt to elucidate the cause of the nodule.(iii) As a result of well-differentiated follicular car-cinoma mistaken for adenoma. Since the distinctionbetween the two conditions requires histologicaldemonstration of capsular or vascular invasion, it isour policy to recommend surgical excision of all fol-licular neoplasms, benign or malignant. Thisapproach is justified not only because it may not befeasible to separate an adenoma from a low-gradecarcinoma on cytological evaluation, but also thereis some evidence to suggest that occasionaladenomas can evolve into carcinomas.3s36(iv) As a result of the needle missing the lesion or aninadequate cell sample. In Varhaug's series24 asmuch as 16% of their samples were unsatisfactory.In Walfish's series3' the unsatisfactory rate was 8%and in Frable's series'3 the rate was 7-5%. Aspeg-ren37 reported that aspiration cytology was found tobe 25% less accurate when various surgeons per-formed the aspiration than when it was performedby trained cytopathologists. Inadequate aspiration,failure in making acceptable smears, or faultyfixation were reasons for this difference. In our mat-erial the unsatisfactory biopsies constituted 5% ofthe total. The same three physicians (two endoc-rinologists and one radiologist) performed 90% ofthe biopsies. For each case, an average of two aspi-rations were performed, and if the biopsy wasjudged inadequate by gross inspection of the smearsit was repeated immediately.The most common causes of false positive cytolog-
ical reports in our study were:(i) Cellular colloid goitre mistaken for neop-lasm. Four such cases of cellular colloid nodule weresurgically treated because they were diagnosed asneoplastic on FNAB.(ii) Thyroiditis mistaken for neoplasm. One case ofchronic lymphocytic thyroiditis was cytologicallylabelled as lymphoma and one case of subacute
Suen, Quenville
thyroiditis diagnosed as "suspected carcinoma"(Table).
In conclusion, we wish to stress that the true valueof fine needle aspiration biopsy lies in patient selec-tion and case identification. In order to maintain ahigh sensitivity (97% in our study) for cancer detec-tion we overdiagnosed some non-neoplasms as neo-plastic, sacrificing somewhat the predictive value ofthe positive reports (91%). We believe that a fewfalse-positive reports are acceptable if one does notwish to miss any of the malignant nodules. Further-more, many more of the benign "cold" noduleswould be operated on if FNAB is not in use. FNABis not a final diagnostic work-up and a conclusivecytological diagnosis is not always required, but eachresult, if suspicious for neoplasm, should lead tofurther investigations that will identify a specificlesion and in most instances this would mean surgi-cal exploration.
References
Degroot U. Most solitary thyroid nodules should be removed.In: Ingelfinger FJ, ed. Controvuersy in internal medicine II.Philadelphia: WB Saunders Co, 1974:421-7.
2 Geer MA. Thyroid nodules. Surgery is usually not necessary. In:Ingelfinger FJ, ed. Controversy in internal medicine 11.Philadelphia: WB Saunders Co, 1974:428-36.
3 Beckers C. Thyroid nodules. Clin Endocrinol Metab1979;8: 181-92.
Sokal JE. The problem of malignancy in nodular goitre. JAMA1959;170:405-12.
Kendall LW, Condon RE. Prediction of malignancy in solitarythyroid nodules. Lancet 1969;i: 1071-3.
6 Knowlson GTG. The solitary thyroid nodule. Br J Surg1971 ;58:253-4.
Katz AD, Zager WJ. The malignant "cold" nodule of thethyroid. Am J Surg 1976;132:459-62.
'Sobel HJ. Cytoplasmic invaginations resembling nuclear inclu-sions. Arch Pathol 1968;85: 114-5.
9 Burns ER, Soloff BL, Hanna C, Buxton DF. Nuclear pocketsassociated with the nucleolus in normal and neoplastic cells.Cancer Res 1971;31:159-61.
10 Lang W, Atay Z, Georgii A. The cytological classification offollicular tumours in the thyroid gland. Virchows Arch (PatholAnat) 1978;378:199-21 1.
"Boon ME, Lbwhagen T, Willems JS. Planimetric studies on fineneedle aspirates from follicular adenoma and follicular car-cinoma of the thyroid. Acta Cytol 1980;24:145-8.
12 Lbwhagen T, Granberg P, Lundell G, Skinnari P, Sundblad R.Wiliems JS. Aspiration biopsy cytology (ABC) in nodules ofthe thyroid gland suspected to be malignant. Surg Clin NorthAm 1979;59:3-18.
3 Frable WJ, Frable MA. Fine needle aspiration biopsy of thethyroid. In: Fenoglio CM, Wolffe M, ed. Progress in surgicalpathology Vol 1. New York: Masson, 1980:105-18.
14 Ljungberg 0. Cytological diagnosis of medullary carcinoma of thethyroid gland. With special regard to the demonstration ofamyloid in smears of fine needle aspirates. Acta Cytol1972;16:253-5.
"Zajicek J. Aspiration biopsy cytology, Part 1. Cytology ofsupradiaphragmatic organs. New York: S Karger, 1974.
16 Chu EW, Hanson TA, Goldman IM, Robbins J. Study of cells infine needle aspirations of the thyroid gland. Acta Cytol1979;23:309-14.
copyright. on June 15, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.36.9.1036 on 1 Septem
ber 1983. Dow
nloaded from

Fine needle aspiration biopsy of the thyroid gland: a study of 304 cases
7 Nilsson G. Nuclear size classes in the follicular epithelium oflymphoid thyroiditis. Acta Pathol Microbiol Scand[A1976;84:165-71.
Persson PS. Cytodiagnosis of thyroiditis. Acta Med Scand (Suppl)1968;483:8-100.
Galen RS, Gambino SR. Beyond normality. The predictive valueand efficiency of medical diagnosis. New York: John Wiley &Sons, 1975.
20 Wang C, Vickery AL, Maloof F. Needle biopsy of the thyroid.Surg Gynecol Obstet 1976;143:365-8.
21 Esselstyn CB Jr, Crile G Jr. Needle aspiration and needle biopsyof the thyroid. World J Surg 1978;2:321-9.
22 Einhorn J, Franzen S. Thin needle biopsy in the diagnosis ofthyroid disease. Acta Radiol 1962;58:321-36.
23 Frable MA. Frable WJ. Thin needle aspiration biopsy of thethyroid gland. Laryngoscope 1980;90:1619-25.
24 Varhaug JE, Segadal E, Heimann P. The utility of fine needleaspiration biopsy cytology in the management of thyroidtumors. World J Surg 1981 ;5:573-7.
25 Friedman M, Shimaoka K, Getaz P. Needle aspiration of 310thyroid lesions. Acta Cytol 1979;23:194-204.
26 Crile G Jr. Management of thyroid disease with particular refer-ence to thyroid nodules. Postgrad Med J 1976;60:105-8.
27 Block MA, Miller JM, Kini SR. The potential impact of needlebiopsy on surgery for thyroid nodules. World J Surg1980;4:737-45.
28 Rosai J. Ackerman's surgical pathology Vol 1. St Louis: CVMosby, 1981:370-1.
29 Dent DM, Miller A, Louw JH. The place of surgery in nodular
thyroid disease. S Afr Med J 1975;49:354-7.30 Anonymous. Utility of needle aspiration of tumours. Br Med J
1978;i: 1507-8.31 Walfish PG, Hazani E, Strawbridge HTG, Miskin M, Rosen IB.
Combined ultrasound and needle aspiration cytology in theassessment and management of hypofunctioning thyroidnodule. Ann Intern Med 1977;87:270-4.
32 Friedman M, Shimaoka K, Rao U, Tsukada Y, Gavigan M,Tamura K. Diagnosis of chronic lymphocytic thyroiditis (nodu-lar presentation) by needle aspiration. Acta Cytol1981;25:513-22.
33 Kini SR, Miller JM, Hamburger JI. Problems in the cytologicdiagnosis of the "cold" thyroid nodule in patients with lym-phocytic thyroiditis. Acta Cytol 1981;25:506-12.
34 Lahey FH, Hare HH. Malignancy in adenomas of the thyroid.JAMA 1951;145:689-95.
35 Silverberg SG, Vidone RA. Adenoma and carcinoma of thethyroid. Cancer 1966;19:1053-62.
36 Meissner WA, Warren S. Tumors of the thyroid gland. Atlas oftumor pathology 2nd series. Washington DC: Armed ForcesInstitute of Pathology, 1969:61-2.
37 Aspegren K, Biorklund A, S6derstrom N, et al. Fine needleaspiration biopsy in thyroid carcinoma. Lakartidningen1976;73:730-2.
Requests for reprints to: Dr KC Suen, Department ofPathology, Vancouver General Hospital, 855 W 12thAvenue, Vancouver, BC, Canada V5Z lM9.
1045
copyright. on June 15, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.36.9.1036 on 1 Septem
ber 1983. Dow
nloaded from