Financing of Health Systems: restrictions and opportunities International Conference on Innovations...
37
Financing of Health Systems: restrictions and opportunities International Conference on Innovations in Health Financing Mexico City, April 2004 Carlos Noriega
-
Upload
buddy-barnett -
Category
Documents
-
view
213 -
download
0
Transcript of Financing of Health Systems: restrictions and opportunities International Conference on Innovations...

Financing of Health Systems:
restrictions and opportunities
International Conference on Innovations
in Health Financing
Mexico City, April 2004
Carlos Noriega

Financing of Health Systems: restrictions and opportunities
1. Introduction
2. Objectives
3. Health expenditures: need and demand
4. Health financing:
a. Collection
b. Risk - Pooling
c. Contracting
5. Policy Options and Opportunities
Mexico faces critical public health challenges in the near term:
Improving health status
Reducing health inequalities
Demographic transition
• Some of the challenges emerged as a consequence of deficiencies in the national health system.
• Despite recent reforms, some issues remain to be defined.
• How should the national health system be financed?
• Conceptual analysis and international experience should bear on the policy response.

In designing a national health system the following issues need to be addressed:
• How much financing is required?
• From what sources?
• What is the role of government?
• Which services are to be included?
In strengthening an existing national health system the questions are inverted:
• What can be done with available financing?
• Is the structure of financing adequate?
• Can the government do any better?
• Should the basket of services be modified?

Financing of Health Systems: restrictions and opportunities
1. Introduction
2. Objectives
3. Health expenditures: need and demand
4. Health financing:
a. Collection
b. Risk - Pooling
c. Contracting
5. Policy Options and Opportunities

Set guiding principles for financing a national health system
Hypothesis
It is as important the amount of financing as the structure of
collection and the mechanism for allocating the resources
Two major premises
1. The financing scheme is, simultaneously, a major instrument of economic and social policies.
2. Principles cannot ignore the current economic, social and
political environment

Financing of Health Systems: restrictions and opportunities
1. Introduction
2. Objectives
3. Health expenditures: need and demand
4. Health financing:
a. Collection
b. Risk - Pooling
c. Contracting
5. Policy Options and Opportunities
How much to spend?
The gap between need and demand for health services may be explained by:
• Legal and regulatory framework
• Budget restrictions
• Market failure
• Information costs and asymmetries
• Financial market costs
• Externalities

Health expenditures
•Form of investment in human capital
•Impact welfare and economic growth
Health expenditures should respond to health considerations as well as to overall economic growth and development goals

EVISA VS. HEALTH EXPENDITURE AS % OF GDP
Health expenditure as % of GDP
EV
ISA
0 3 6 9 12 15
28
38
48
58
68
78
México
EVISA VS. HEALTH EXPENDITURE PER CAPITA (US$)
Health expenditure per capita (US$)
EV
ISA
0 1 2 3 4 5(X 1000)
28
38
48
58
68
78
México
DALY´s

LIFE EXPECTANCY VS. HEALTH EXPENDITURE AS % OF GDP
Health expenditure as % of GDP
Lif
e ex
pect
ancy
0 3 6 9 12 15
34
44
54
64
74
84
México
LIFE EXPECTANCY VS. HEALTH EXPENDITURE PER CAPITA (US$)
Health expenditure per capita (US$)
Lif
e ex
pect
ancy
0 1 2 3 4 5(X 1000)
34
44
54
64
74
84
México
Life Expectancy
• México spends relatively little in health as compared to other countries with similar income per capita in the
region
• Daly´s in Mexico are relatively higher as compared to other countries with similar levels of health expenditures
(% of GDP and $/pc)
• At low levels of expenditure more spending contributes to a higher health level
• At higher levels of expenditure more spending contributes marginally or even negatively to the health level
• México still can improve health levels by spending more
Developing countries need to confer a higher priority to health expenditures to promote welfare and growth.

Financing of Health Systems: restrictions and opportunities
1. Introduction
2. Objectives
3. Health expenditures: need and demand
4. Health financing:
a. Collection
b. Risk - Pooling
c. Contracting
5. Policy Options and Opportunities

From the point of view of efficiency
Moral Hazard
Once insured, there are incentives to engage in a more risky behaviour and to use in excess health services
Adverse Selection
Asymmetric information may lead riskier households/persons to seek affiliation
Rule of thumb: control population in order to charge according to risk
I. Sources of financing

From the point of view of equity
Individual Society-Pooling
Financing Out of pocket General Revenue
Risk burden Pay per event Social Insurance
Inequitable Equitable
Rule of thumb: favor pooling of risks and of financing
Dilemma: is there a conflict between efficiency and equity?

EVISA VS. OUT OF POCKET HEALTH EXPENDITURE AS % OF TOTAL HEALTH EXPENDITURE
Out of pocket health expenditure as % of total health expenditure
EV
ISA
0 20 40 60 80 100
28
38
48
58
68
78
México
DALY´s vs Out-of-pocket expenditures as % of total health expenditures

GDP per capita
com
pone
nt e
ffec
t
0 1 2 3 4 5(X 10000)
-29
-19
-9
1
11
21
Out of pocket health expenditure as % of total health expenditure
com
pone
nt e
ffec
t
0 20 40 60 80 100
-25
-15
-5
5
15
GDPpc has a positive impact on DALY´s
Out-of-pocket expenditures have a negative impact on DALY´s
Source: WHO, Sample of 191 countries, 2002

International evidence does not support the dilemma
• More equitable financing reinforce efficiency of health systems
• Equity goals may be pursued as part of the financing scheme
• Equity goals should be made transparent to ensure they are effectively achieved

II. Federal-Local
Federal financingEquity: Inter-regional transfersEfficiency: More effective risk-pooling
Local financing
Alignment of incentivesTransparency and accountability
Closer links expenditure / collection
Challenges for local operation
• Increase coverage
• Autonomy for managing programs
• Flexibility to adapt content of basic package of services
• Responsibility in a decentralized financing scheme

0.00 4.00 8.00 12.00
POBLACION ABIERTA
400.00
800.00
1200.00
1600.00
GA
ST
O P
ER
CA
PIT
A E
N S
AL
UD
Ags
BC
BCS
Camp
Coah
Col
Chis
Chih
DF
Dgo
Gto
Gro
Hgo
Jal MexMichMor
Nay
NLOax
Pue
Qro
Q.Roo
SLP
Sin
Son
Tabs
Tamps
Tlax
Ver
Yuc
Zac
Local financing for open population (% of total public spending, 2002)
0
10
20
30
40
50
60
Tabasc
o
Distrit
o Fed
eral
Veracru
z
Chihuah
ua
Sinaloa
Tamau
lipas
Nuevo L
eón
Mor
elos
Nayarit
Chiapas
Tlaxca
la
Mich
oacán
Queré
taro
Colima
Durang
o
Baja C
alifo
rnia
%
Local governments differ greatly in their contribution to health financing of open population

To improve efficiency incentives need to be realigned:
• Increase local financing
• Provide operational autonomy to local governments
Health programs for open population:
• Federal in nature,• Operated by local governments• Financed mostly by federal government
Financing of Health Systems: restrictions and opportunities
1. Introduction
2. Objectives
3. Health expenditures: need and demand
4. Health financing:
a. Collection
b. Risk - pooling
c. Contracting
5. Policy Options and Opportunities
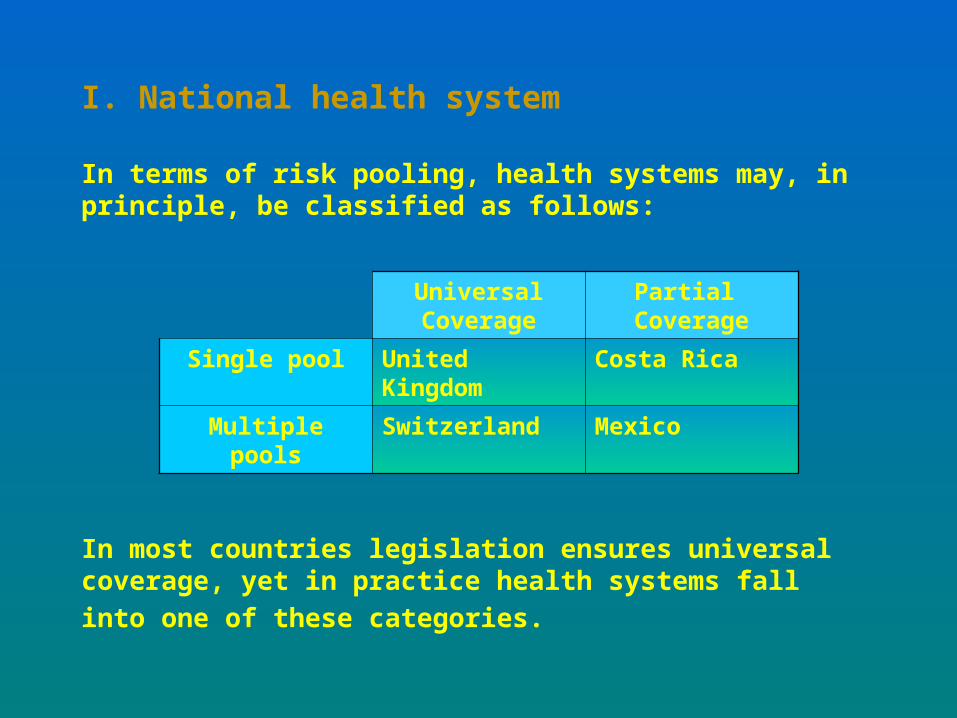
I. National health system
In terms of risk pooling, health systems may, in principle, be classified as follows:
In most countries legislation ensures universal coverage, yet
in practice health systems fall into one of these categories.
Universal Coverage
Partial Coverage
Single pool United Kingdom Costa Rica
Multiple pools Switzerland Mexico

Advantages of a single pool of risks:
• Better compensation of risks
• More transparency for pooling financial resources
• Reduce administrative costs
• Centralized contracting of inputs and services
Advantages of multiple pools of risk:
• Decentralization stimulates standardization
• Efficiency gains of adecentralized scheme
• Marginal compensation gains for very large populations
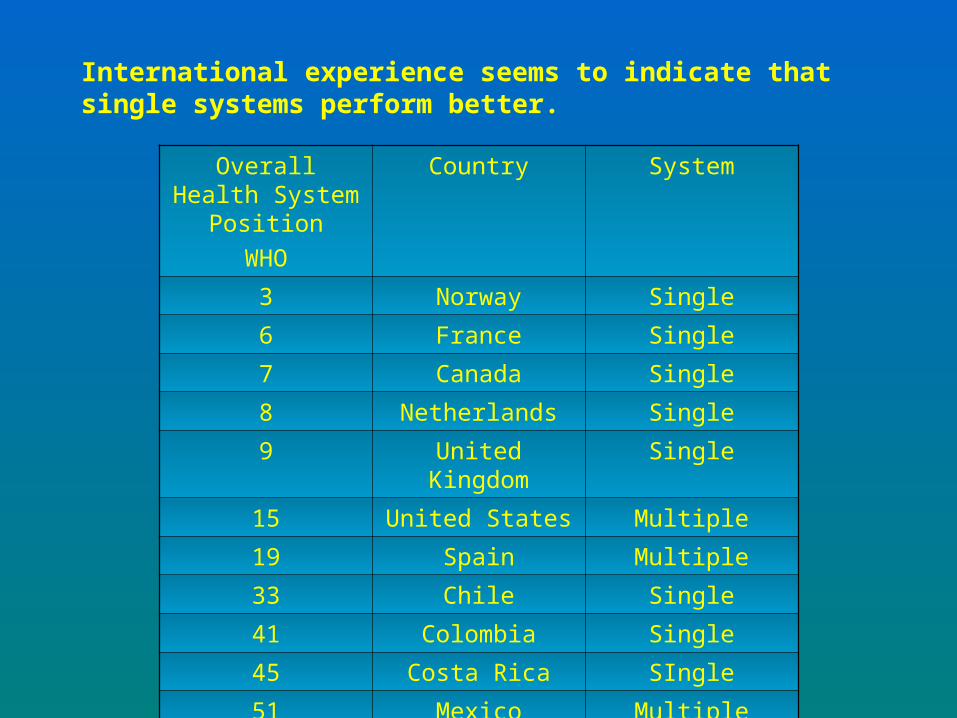
Overall Health System Position
WHO
Country System
3 Norway Single
6 France Single
7 Canada Single
8 Netherlands Single
9 United Kingdom Single
15 United States Multiple
19 Spain Multiple
33 Chile Single
41 Colombia Single
45 Costa Rica SIngle
51 Mexico Multiple
65 Venezuela Multiple
International experience seems to indicate that single systems perform better.

Challenges to implement effective risk-pooling in the presence of various national health institutions:
• Portability of rights
• Standardization of public contributions
• Management of financial reserves
• Standardization of services
• Standardization of quality of services
Recommendation:
• Migrate to a single health system with effective financing and risk pooling,
• In the short run implement a gradual process of separation of financing/provision in existing public health institutions

II. Public-Private Two major issues need to be answered: 1. Nature of the service
PUBLIC (?) PRIVATE (?)
Compulsory affiliation Voluntary affiliation
Non-profitable Profitable
Centralized De-centralized
Comprehensive coverage Partial coverage
Regulated Non-regulated
Risk-pooling Health-services provision
The false debate

GOAL INSTRUMENT ACTION
Long term perspective Compulsory affiliation Creation of operative and actuarial reserves
Universal coverage Public contribution (subsidies for the poorest and worst risks)
Regulation for “bad risks” (pre-existencias)
Efficiency and Quality of health services
Competition in the provision of services
Cost containment Competition Hard budget restriction
• International experience shows a variety of solutions
• Services not necessarily have to be provided by the public sector.
Ultimate criterion: allow private participation on efficiency grounds making use of available instruments

2. Co-existence of providers: substitute vs. complement
Role Condition Mechanism
Substitute Large group Capitated reversal of contributions
Complement Nature of risk not prioritary for public health
None
Basic Package Complementary Package
Basic care Public
Secondary care
Tertiary care Private
This outcome enhances efficiency in the system and allows for public resources to be focused where they cannot be
substituted by the private sector.

Financing of Health Systems: restrictions and opportunities
1. Introduction
2. Objectives
3. Health expenditures: need and demand
4. Health financing:
a. Collection
b. Risk - Pooling
c. Contracting
5. Policy Options and Opportunities

Basic services provided
Classical Universalism: Provide and finance everything for everybody
New Universalism: If services are to be provided for all, then not all services can be provided.
Defined basket of basic services
Gains in efficiency:
• Costs: standardization allows for economies of scale
• Simplification of processes: planning, training, monitoring, supervision
• Certainty on rights of affiliates
• Sharpening the scope of public responsibilities
Gains in equity:
• Affiliates receive similar benefits (avoids undue transfers)
• Increase coverage

Constraints:
• Budget Restriction
• Extend coverage
Recommendations:
• Reach a consensus on public health priorities
• Establish cost-effectiveness criteria to define a basket of basic services
• Coordinate among existing public health institutions to transit to that basket of basic services

Financing of Health Systems: restrictions and opportunities
1. Introduction
2. Objectives
3. Health expenditures: need and demand
4. Health financing:
a. Collection
b. Risk - Pooling
c. Contracting
5. Policy Options and Opportunities
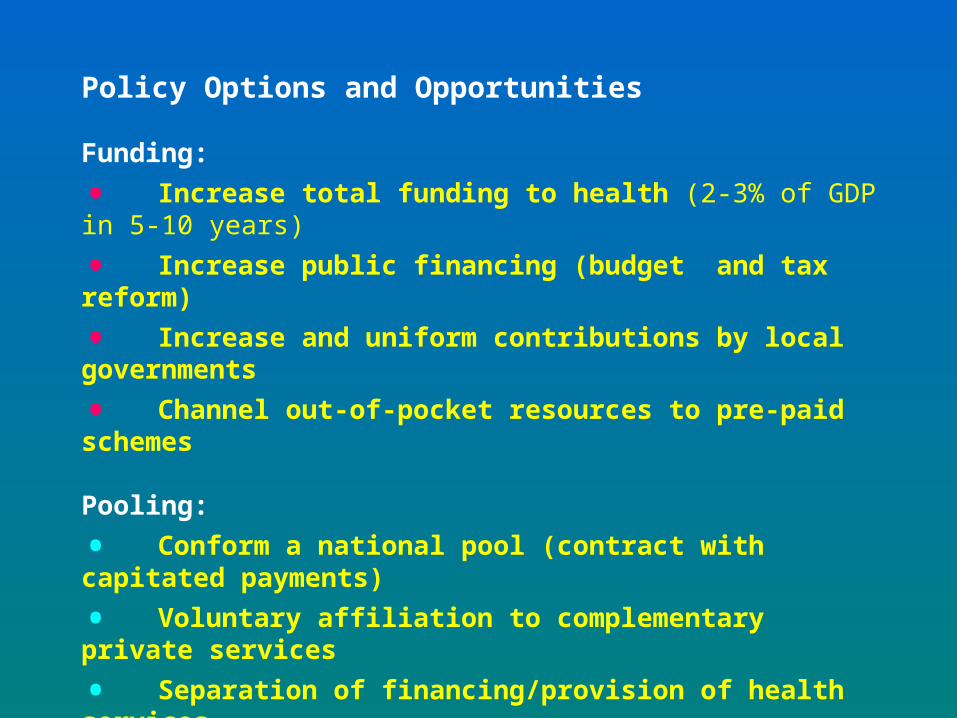
Policy Options and Opportunities
Funding:
• Increase total funding to health (2-3% of GDP in 5-10 years)
• Increase public financing (budget and tax reform)
• Increase and uniform contributions by local governments
• Channel out-of-pocket resources to pre-paid schemes Pooling:
• Conform a national pool (contract with capitated payments)
• Voluntary affiliation to complementary private services
• Separation of financing/provision of health services
• Allow private participation in complementary services
Contracting:
• Move towards a basket of basic services

Consensus on public health priorities
and health financing
Collection Riks-Pooling Contracting
Efficiency Equity Universal Coverage

Goal Instrument Actions
Funding
Increase total resources by 2-3% of GDP in 5-10 years
Federal Government raises contributions and explicit subsidies
Tax and budget reform
Local governments increase contributions and uniform them across regions
Tax and budget reform
Channel out-of-pocket resources into a pre-paid scheme
Transform current assistance programs into insurance programs
Seguro popular de salud, Seguro de salud de familia, voluntary affiliation (IMSS, ISSSTE)
Pooling
Establishment of a single national pool
Pool contributions and subsidies
Coordinate (merge) existing national and local social security institutions (IMSS, ISSSTE, ISSSTESON, ISSSTELEON, etc.)
Split funding and provisioning Contract through capitated payments
Internal reforms of existing national and local social security institutions
Allow private participation for complementary services
Legal and regulatory reforms
Contracting
Define a basic package of services
Legal and regulatory reforms Define services based on cost-effectiveness criteria

Financing of Health Systems:
restrictions and opportunities
International Conference on Innovations
in Health Financing
Mexico City, April 2004
Carlos Noriega