
Financial Governance Update for Authorisation and ... Clinical Cabinet/Formal... · the Financial...
200
NHS BEXLEY CLINICAL COMMISSIONING GROUP GOVERNING BODY FORMAL MEETING - 25 th October 2012 Financial Governance Update for Authorisation and Financial Management Arrangements Action Required (Approval/information) The CCG Governing Body are requested to; • APPROVE the Financial Management Arrangements document for implementation and circulation immediately following finance handover to the CCG. • NOTE progress on the Financial Governance checklist in respect of requirements for authorisation Executive Summary Appendix 1 is the Financial Management Arrangements document which aims to bring together into one document the following elements: • Overview of arrangements • Standing Orders • Scheme of Reservation and Delegation • Schedule of Matters delegated to officers • Prime Financial Policies • Audit and Integrated Assurance Committee Terms of Reference • Remuneration Committee Terms of Reference • Budget Setting Policy • Sample CCG Financial Report This document should be read in conjunction with the Constitution and the Detailed Financial procedures to complete the overall financial governance arrangements. Appendix 2 is the Financial Governance checklist which details all of the requirements for authorisation and has been annotated for the work undertaken to date. These documents can be used as part of the authorisation process in order to point assessors to the required evidence. At present, all the requirements for application have been met and work is on-going to meet the next deadlines – there are no delays or problems anticipated with complying with these dates. ENCLOSURE: G (xi) Agenda Item : 164/12
Transcript of Financial Governance Update for Authorisation and ... Clinical Cabinet/Formal... · the Financial...

NHS BEXLEY CLINICAL COMMISSIONING GROUP GOVERNING BODY FORMAL MEETING - 25th October 2012
Financial Governance Update for Authorisation and Financial Management Arrangements Action Required (Approval/information) The CCG Governing Body are requested to;
• APPROVE the Financial Management Arrangements document for implementation and circulation immediately following finance handover to the CCG.
• NOTE progress on the Financial Governance checklist in respect of requirements for authorisation
Executive Summary Appendix 1 is the Financial Management Arrangements document which aims to bring together into one document the following elements:
• Overview of arrangements • Standing Orders • Scheme of Reservation and Delegation • Schedule of Matters delegated to officers • Prime Financial Policies • Audit and Integrated Assurance Committee Terms of Reference • Remuneration Committee Terms of Reference • Budget Setting Policy • Sample CCG Financial Report
This document should be read in conjunction with the Constitution and the Detailed Financial procedures to complete the overall financial governance arrangements. Appendix 2 is the Financial Governance checklist which details all of the requirements for authorisation and has been annotated for the work undertaken to date. These documents can be used as part of the authorisation process in order to point assessors to the required evidence. At present, all the requirements for application have been met and work is on-going to meet the next deadlines – there are no delays or problems anticipated with complying with these dates.
ENCLOSURE: G (xi) Agenda Item : 164/12

Organisational implications Financial The Financial Management Arrangements document
provides the framework for the effective functioning of the finance department of the CCG, and puts in one place the required governance documents for all staff, including CSU staff working at the CCG to refer to. The financial governance update document tracks the completion of the requirements for the authorisation process and ensures no items are being omitted.
Equality and Diversity Not applicable Risk (governance and/or clinical)
These documents provide assurance regarding the financial policies of the organisation and the compliance with them, also there is a complete trail which shows the requirements for authorisation and how they are being met.
Patient impact Not applicable NHS constitution Not applicable Which objective does this paper support? Insert
Tick Improve choice and access to integrated health services for Bexley patients Reduce the level of health inequalities across Bexley Improve care for patients with long term conditions & increase the range of services offered within the community
Improving the health & wellbeing for people in Bexley Maximizing the opportunities of joint working (A Picture of Health, Joint Strategy Needs Assessment, Wellness agenda etc)
Using our resources in the most efficient & effective manner (organisational & financial)
Considered/Approved by Other Committees/Groups These documents have not been presented to any other committees Author Julie Witherall Head of Finance and Business Commissioning Support Unit
Executive Sponsor Theresa Osborne Chief Financial Officer
Date 4th October 2012
ENCLOSURE: G (xi) Agenda Item : 164/12

1
APPLICATION FOR AUTHORISATION
FINANCIAL MANAGEMENT ARRANGEMENTS
ENCLOSURE: G (xi) – App1

2
Key Evidence Demonstrated:
EVIDENCE REQUIRED REFERENCE 4.2.1.G CCG has following standard
financial management arrangements in place:
• Internal and external audit Financial Management Arrangements Overview Page 7-8 Section 2.6/2.7 Prime Financial Policies Pages 97/98 sections 2 and 3
• Financial reporting through financial spine
Financial Management Arrangements Overview Pages 8-9 Section 3.0 and 4.0 Prime Financial Policies Pages 96-99 sections 5 to 10
• Audit committee Financial Management Arrangements Overview Page 5 section 2.4 Standing orders pages 36-37 section 4 Audit & Integrated Assurance Committee terms of reference pages 106 to 114
• Standing orders/standing financial instructions
Financial Management Arrangements Overview Page 4 sections 2.1 and 2.3 Standing Orders pages 12 to 38 Prime Financial Policies (SFIs) pages 89 to 103
• Scheme/s of delegation Financial Management Arrangements Overview Page 4 section 2.2 Scheme of Reservation and Delegation pages 41 to 58 Schedule of Matters delegated to officers pages 61 to 86
• Arrangements for management of any charitable funds
Financial Management Arrangements Overview Page 9 section 4.3
• Committee structure including management and audit
Financial Management Arrangements Overview Pages 5-6 2.4 and 2.5 Standing Orders pages 36-37 section 4
• Counter fraud arrangements Financial Management Arrangements Overview page 8 section 2.8 Prime Financial Policies Page 92-93 section 4
• Accounts payable and receivable, cash, fixed assets
Financial Management Arrangements Overview page 9 section 4.1 Prime Financial Policies pages 97-98 section 12, page 101-102 sections 16 and 17
• Payroll and banking facilities Financial Management Arrangements Overview page 9 sections 4.1 and 4.2 Prime Financial Policies page 97 section11
• Appropriate risk sharing arrangements with other CCGs in place and clearly understood by all parties.
Shown in separate document – refer to Financial Governance Update paper

3
APPLICATION FOR AUTHORISATION
FINANCIAL MANAGEMENT ARRANGEMENTS
FINANCIAL MANAGEMENT ARRANGEMENTS
OVERVIEW

4
FINANCIAL MANAGEMENT ARRANGEMENTS 1.0 INTRODUCTION
This document provides a summary of the CCG’s key financial management arrangements. It covers the arrangements for financial governance, financial planning and reporting and its financial systems.
2.0 FINANCIAL GOVERNANCE 2.1 STANDING ORDERS
Whilst the statutory framework for a CCG’s constitution does not prescribe the inclusion of Standing Orders, they are referred to in the NHS Commissioning Board Authority’s Towards Establishment and the CCG has prepared its own Standing Orders based upon the NHSCB model. These can be found at Appendix 1.
2.2 SCHEME OF RESERVATION AND DELEGATION Whilst the statutory framework for a CCG’s constitution does not prescribe the inclusion of a scheme of delegation, they are referred to in the NHS Commissioning Board Authority’s Towards Establishment and the CCG has prepared its own Scheme of Reservation and Delegation based upon the NHSCB model. These can be found at Appendix 2 These are supported by a detailed Schedule of Matters Delegated to Officers which can be found at Appendix 3.
2.3 PRIME FINANCIAL POLICIES (STANDING FINANCIAL INSTRUCTIONS) Whilst the statutory framework for a CCG’s constitution does not prescribe the inclusion of prime financial policies, they are referred to in the NHS Commissioning Board Authority’s Towards Establishment (as ‘standing financial instructions’) and the CCG has prepared its own Prime Financial Policies (Standing Financial Instructions) based upon the NHSCB model. These can be found at Appendix 4. To ensure the Prime Financial Policies remain up-to-date and relevant, the Chief Financial Officer will review them at least annually. Following consultation with the Chief Officer and scrutiny by the CCG’s Audit & Integrated Assurance Committee, the Chief Financial Officer will recommend any amendments, as fitting, to the Governing Body for approval. In support of the Prime Financial Policies, the CCG has prepared more detailed policies, which will be approved by the Chief Officer. These will be known as ‘Detailed Financial Procedures’. The CCG refers to these prime and detailed financial policies together as the CCG’s ‘Financial Policies.

5
2.4 AUDIT & INTEGRATED ASSURANCE COMMITTEE In line with requirements of the NHS Audit Committee Handbook, NHS Codes of Conduct and Accountability, and more recently the Higgs report, an Audit & Integrated Assurance Committee will be established and constituted to provide the group with an independent and objective review of its financial systems, financial information and compliance with laws, guidance, and regulations governing the NHS. The Audit & Integrated Assurance Committee, which is accountable to the group’s governing body, will support the governing body discharge its functions related to overseeing efficiency, effectiveness, economy and governance. The committee shall review the establishment and maintenance of an effective system of integrated governance, risk management and internal control, across the whole of the group’s activities that support the achievement of the group’s objectives.
This will include providing the governing body with an independent and objective view of the group’s financial systems, financial information and compliance with laws, regulations and directions governing the group in so far as they relate to finance. The Committee will comprise two lay members (one of whom, the governance lead, will act as chair) and three clinicians from the governing body, including the nurse and secondary care clinician. It is expected that the Chief Financial Officer and Accountable Officer will attend meetings. Representatives from external audit, internal audit and local counter fraud services will also be in attendance. The Audit Committee will meet a minimum of four times a year. The Committee will meet privately with the external and internal auditors at least once a year. The draft Terms of Reference for the Audit & Integrated Assurance Committee are attached as Appendix 5 and will be approved by the Governing Body and reviewed on a periodic basis.

6
2.5 REMUNERATION COMMITTEE
In line with requirements of the NHS Audit Committee Handbook, NHS Codes of Conduct and Accountability, and more recently the Higgs report, a Remuneration Committee will be established and constituted. The Remuneration Committee’s, which is accountable to the group’s governing body, overall purpose is to:
• ensure that the process of appointing, and if necessary dismissing, the directors are robust, fit for purpose and have been followed;
• oversee and coordinate, through delegation, any elections which may be part of the process of appointment to the governing body;
• oversee the system for all director appointments and agree the parameters for the senior appointments process. The process of all senior executive appointments will be reported back to the Committee in order that the Committee can provide the governing body with assurance;
• agree and review the CCG’s policies on the reward, performance, retention and pension matters for the directors;
• support the board understand and apply Lord Nolan’s ‘Principles of Public Life’ and generally promote transparency and probity.
The Remuneration Committee will meet a minimum of twice a year. The Committee will comprise two lay members (one, the lay member for governance, to act as chair), the CCG Chair and one elected practice member from the governing body. The Chief Officer and Chief Financial Officer will attend Committee meetings, but will not be present for matters involving their personal remuneration. The draft Terms of Reference for the Remuneration Committee are attached as Appendix 6 and will be approved by the Governing Body and reviewed on a periodic basis.
2.6 INTERNAL AUDIT For the first year of operation, the CCG in conjunction with the Commissioning Support Unit (CSU) and the other CCGs in South East London will consider whether it will be feasible to extend the existing arrangements for Internal Audit for one year to allow time for a procurement exercise to be undertaken by the CSU on behalf of the CCGs. . The Audit Committee will monitor the performance of the Internal Audit function, ensuring that it meets mandatory NHS Internal Audit Standards and provides appropriate independent assurance to the Audit Committee, Chief Officer and CCG Governing Body. The audit programme for the forthcoming year is yet to be finalised, but is likely to include:

7
• Internal Financial Controls; • Financial Systems; • Human Resources; • Information Security; • Board Assurance Framework and Risk Management; • Information governance; • Business Continuity; • Governance and CCG delegation; • QIPP management; • Local Financial Reporting; • Acute performance management • 111 Implementation; • Pathway Redesign.
The Internal Auditors will attend Audit & Integrated Committee meetings and will provide reports on audit work undertaken together with management’s response.
2.7 EXTERNAL AUDIT The Department for Communities and Local Governing (DCLG) is due to publish a draft Bill on the future arrangements for local public audit. This Bill will outline how the current audit regime and the Audit Commission will be replaced. Essentially, DCLG have undertaken a procurement exercise to out-source audit work for public bodies. In March 2012, the Audit Commission announced the proposed award of five-year audit contracts to four private firms commencing from 2012/13. It is anticipated that the External Auditor that covers the Bexley geographical areas will be Grant Thornton (UK) LLP. The Audit Commission will remain in place to oversee the contracts and other statutory functions. The external auditor to the CCG will comply with any instructions issued by the Audit Commission when undertaking their audit role. The external auditor will have direct and unrestricted access to audit committee members and the chair of the governing body, accountable officer, and chief finance officer for any significant issues arising from audit work that management cannot resolve, and for all cases of fraud or serious irregularity. External Audit will attend Audit & Integrated Assurance Committee meetings and will provide reports on audit work undertaken together with management’s response.
2.8 COUNTER FRAUD ARRANGEMENTS For the first year of operation, the CCG in conjunction with the Commissioning Support Unit (CSU) and the other CCGs in South East London will consider whether

8
it will be feasible to extend the existing arrangements for Local Counter Fraud Services for one year to allow time for a procurement exercise to be undertaken by the CSU on behalf of the CCGs. Counter Fraud will prepare an annual Counter Fraud work programme which will be approved by the Audit Committee. A representative from the Local Counter Fraud Service will be invited to attend Audit & Integrated Committee meetings.
3.0 FINANCIAL PLANNING AND REPORTING 3.1 FINANCIAL PLANNING
Sound financial planning underpins financial management and control. The CCG will embed strong financial planning throughout its business, and will develop a forward looking financial strategy and budget setting policy. The draft is attached at Appendix 7.
3.2 FINANCIAL REPORTING
Although employed by the South London Commissioning Support Unit, given the importance the CCG places on sound financial management, risk management and financial control, the finance staff will be based within the CCG and report directly to the Chief Financial Officer on a daily basis. This will ensure that its financial management and reporting processes are close to the heart of the CCG’s business and fully understands key challenges and issues. Financial risks will be considered for their probability and impact, and emphasis placed on ownership and action to resolve/mitigate financial risks. The financial reporting will consider differing scenarios and outcomes. Reporting will be transparent, and clear where estimation has been made in making material financial judgements. Monthly financial reports will be prepared for the Finance Working Group and Governing body, describing overall the financial position and key risks, and will make recommendations about mitigating actions that may be required. Financial risks will be considered for their probability and impact. Issues will be escalated to the corporate risk register where appropriate in accordance with the governance framework. An example report is attached at Appendix 8. The CCG will also provide regular reporting information as required by the NHS Commissioning Board. Annual accounts will be prepared in accordance with the published manual for accounts.
4.0 FINANCIAL SYSTEMS 4.1 ACCOUNTS PAYABLE AND RECEIVEABLE, CASH, FIXED ASSETS, PAYROLL

9
The NHS Commissioning Board Authority has signed a contract between the NHSCB and NHS Shared Business Services (SBS) to provide an integrated finance and accounting system to the CCG from April 2013. The SBS solution is already the most widely used finance and accounting system in the NHS and SBS have provided a finance and accounting solution to Bexley for the last year. The CCG will contract with South London CSU for a payroll service. The use of a common system will ensure proper financial and corporate governance, financial consistency, proper risk management relating to the transfer of financial information and the adoption of best practice in business processes. The integrated system will create a basic common infrastructure which will be cost-effective and will save time for organisations in terms of system development.
4.2 CASH AND BANKING FACILITIES Whilst SBS will undertake the transaction processing as described in section 13 above, the CCG plans to secure its remaining financial services including treasury/cash management from its commissioning support service (South London CSU). This will include managing the banking facilities and regular preparation of cash flow forecasts for monitoring purposes. Cash flow forecasting will form part of the financial reporting arrangements within the CCG and will be included in reports to the Governing Body. Procedures for cash and bank are contained within the CCG’s Financial Policies. It is assumed the CCG, through the South London CSU, will be use the government banking service.
4.3 ARRANGEMENTS FOR MANAGEMENT OF CHARITABLE FUNDS As an inherently management organisation, it is not expected that the CCG will hold any charitable funds, and if any such donations should be made, the CCG will liaise with the donator regarding a more appropriate beneficiary.

10
APPLICATION FOR AUTHORISATION
FINANCIAL MANAGEMENT ARRANGEMENTS
APPENDIX 1 STANDING ORDERS
ENCLOSURE: G (xi) – App1

11
APPENDIX 1
STANDING ORDERS

12
STANDING ORDERS
1. STATUTORY FRAMEWORK AND STATUS
1.1. Introduction 1.1.1. Standing orders and other related documents are key components of the
arrangements that an organisation has in place to conduct its business. It is recognised that the authorisation process will require NHS Bexley CCG to clearly demonstrate the arrangements in place to discharge their business. This document brings together the information required by the NHS Commissioning Board to support authorisation. Additionally, it reflects the requirements of relevant regulations regarding procedure for governing bodies, their audit and remuneration committees.
1.1.2. These standing orders have been drawn up to regulate the proceedings of the NHS Bexley Clinical Commissioning Group so that group can fulfil its obligations, as set out largely in the 2006 Act, as amended by the 2012 Act and related regulations. They are effective from the date the group is established.
1.1.3. The standing orders, together with the group’s scheme of reservation and delegation and the group’s prime financial policies, provide a procedural framework within which the group discharges its business. They set out:
1.1.3.1. the arrangements for conducting the business of the group;
1.1.3.2. the appointment of member practice representatives;
1.1.3.3. the procedure to be followed at meetings of the group, the governing body and any committees or sub-committees of the group or the governing body;
1.1.3.4. the process to delegate powers,
1.1.3.5. the declaration of interests and standards of conduct.
1.1.4. These arrangements must comply, and be consistent where applicable, with requirements set out in the 2006 Act (as amended by the 2012 Act) and related regulations and take account as appropriate4 of any relevant guidance.
13
1.1.5. The standing orders, scheme of reservation and delegation and prime financial policies have effect as if incorporated into the group’s constitution. Group members, employees, members of the governing body, members of the governing body’s committees and sub-committees, members of the group’s committees and sub-committees and persons working on behalf of the group should be aware of the existence of these documents and, where necessary, be familiar with their detailed provisions.
1.2. Schedule of matters reserved to the Clinical Commissioning Group and the Scheme of Delegation
1.2.1. The 2006 Act (as amended by the 2012 Act) provides the group with powers to delegate the group’s functions and those of the governing body to certain bodies (such as committees) and certain persons. The group has decided that certain decisions may only be exercised by the group in formal session. These decisions and also those delegated are contained in the group’s scheme of reservation and delegation (see Appendix D).
2. THE CLINICAL COMMISSIONING GROUP (CCG): COMPOSITION OF MEMBERSHIP, KEY ROLES AND APPOINTMENT PROCESS
2.1. Composition of membership of NHS Bexley CCG 2.1.1. Chapter 3 of the group’s constitution provides details of the membership of
the group (see also Appendix B).
2.1.2. The full terms of reference for the NHS Bexley Clinical Commissioning governing body and job role outlined are available on the website at www.bexley.nhs.uk. Other ways of accessing these documents include:
2.1.2.1. by email at [email protected] 2.1.2.2. by post to insert address 221, Erith Road, Bexleyheath, Kent, DA7 6HZ
2.1.3. NHS Bexley CCG has been developed to enable effective participation of each member to exercise its functions.
2.1.4. Chapter 6 of the group’s constitution provides details of the governing structure used in the group’s decision-making processes, whilst Chapter 7 of the constitution outlines certain key roles and responsibilities within the group and its governing body, including the role of practice representatives (section 7.1 of the constitution).
2.1.5. Paragraph 6.6.2 of the group’s constitution sets out the composition of the group’s governing body whilst Chapter 7 of the group’s constitution identifies certain key roles and responsibilities within the group and its governing body.

14
These standing orders set out how the group appoints individuals to these key roles.
2.2. Application to become a Member 2.2.1. Any Eligible Person may apply to become a Member by making a written
application to the Governing Body. Such written application must:
2.2.1.1. specify the name and address of the Eligible Person;
2.2.1.2. confirm that the Eligible Person is a provider of primary medical services pursuant to clause 3.2.1(a) of this Constitution; and
2.2.1.3. confirm that it provides primary medical services from and is situated within the Geographic Area.
2.2.2. Upon receipt by the Governing Body of the application, the Governing Body
2.2.2.1. shall notify the NHS Commissioning Board of the application and request the NHS Commissioning Board’s acknowledgment that the Eligible Person is to become a Member.
2.2.3. Upon receipt by the Governing Body of the acknowledgment by the NHS Commissioning Board pursuant to clause 2.3.2 above (or, if no such acknowledgment is received, within 28 days of the Governing Body’s request for acknowledgment), the Governing Body may declare that the Eligible Person is to become a Member.
2.2.4. Before becoming a Member, the Eligible Person must:
2.2.4.1. sign a copy of this Constitution (as may be varied or amended from time to time pursuant to clause 1.4 of the Constitution); and
2.2.4.2. make a written declaration that it will act consistently with the provisions of this Constitution including, without limitation, the Responsibilities of Members set out at clause 7.1 of the constitution.
2.2.5. An Eligible Person shall be deemed to become a Member on the first day of the month after it has complied with clause 2.3.4 above.
2.2.6. Upon any Eligible Person becoming a Member, the Governing Body shall within 28 days publish an updated list of Members and this Constitution on its website.
2.3. Recommendation to the National Commissioning Board for a Termination of Membership
2.3.1. Any Members membership may be terminated in accordance with a decision of the NHS Commissioning Board and more particularly if that member should cease to be a primary medical services provider in the geographic location defined in section 2 of the constitution.

15
2.3.2. The Governing Board shall, if it believes that a Member no longer satisfies any of the relevant criteria entitling that Member to be a Member of the Group, inform the NHS Commissioning Board.
2.4. Practice Representatives 2.4.1. Chapter 3 of the group’s constitution provides details of the membership of
the group.
2.4.2. Each practice must nominate one representative who will attend locality and Primary Care Advisory Group meetings, who can contribute to strategic discussions and who is authorised to make decisions on behalf of the practice. The practice can also nominate up to two deputies who will substitute for the nominated member when they are unable to attend. Deputies must also be in position to contribute to strategic discussions and make decisions.
2.4.3. Practice representatives will be expected to actively engage in the commissioning work of NHS Bexley CCG. For NHS Bexley CCG to prosper, it is essential all practice representatives engage with each other, their locality and the NHS Bexley CCG governing body.
Nominations: Self-nomination using job description
Eligibility: Applicants must work in a member practice
Appointment process: Nominated by the practice
Term of office: 12 months
Eligibility for reappointment: At the practice’s discretion
Grounds for removal from office:
Material failure to comply with the terms of this constitution and/or as reasonably determined by the chair of the Governing Body
Notice period: This will be determined in light of the need to ensure continuous representation
2.5. GP Locality Leads on the Governing Body 2.5.1. The governing body will have three GP representatives from the localities;
these will be elected by the locality for whom they represent.
2.5.2. Individuals will be eligible for application for election if they meet the following criteria:

16
2.5.2.1. for GP representatives that they work in Bexley as a GP principal or salaried GP (a minimum of two sessions per week in Bexley;
2.5.2.2. an individual shall not be eligible if they are, or subsequently are, retired from the practice or primary care services provider, suspended by either the GMC or the PCT or any other successor body;
2.5.2.3. If the individual is a Sessional GP, they shall not be eligible in the event that they are suspended from their employment or subject to grievance or disciplinary proceedings; and
2.5.2.4. for those individuals (including those stated at (c) above) who are not party to direct contractual arrangements for the provision of primary medical services, they must be on a Performers List.
2.5.3. Applications will be assessed by a panel, convened by the governing body, to assess them against the essential criteria within the person specification. This panel will include a member of the LMC.
2.5.4. Elected NHS Bexley CCG Practice representatives on the governing body will serve a 2-year term from the date of appointment.
2.5.5. Voting: In accordance with the election principles used by the Royal College of GPs, the election will be run on the Single Transferable Vote system (see http://www.electoralreform.org.uk/article.php?id=48 for details of this voting system.)
2.5.6. The Bexley LMC will oversee the entire appointment process to ensure objectivity.
2.5.7. Roles will be funded via an agreed salary remunerated based on the number of sessions worked. Job descriptions for each elected role are available on the website, and specify minimum number of sessions / days required.
2.5.8. Remuneration will be reviewed every 2-years by the Remuneration Committee.
2.5.9. Grounds for removal from office will be considered to be material failure to comply with the terms of this constitution and/or as reasonably determined by the chair of the Governing Body.
2.5.10. Elected members may give 1 months’ notice to retire but are expected to serve full terms (or full years if a part term).
17
2.5.11. Where a member leaves office part way though a year the Governing Body may convene an election or co-opt a member to the Governing Body for the remainder of the year. Any such co-option to be reported to the Council of Members
2.6. Locality Representatives on the Governing Body 2.6.1. The governing body will have three Locality Leads who will be either a GP,
Nurse or practice manager. These will be elected by the locality for whom they represent.
2.6.2. Individuals will be eligible for application for election if they meet the following criteria:
2.6.2.1. for GP representatives that they work in Bexley as a GP principal ,salaried GP, Practice Nurse or Practice Manager;
2.6.2.2. an individual shall not be eligible if they are, or subsequently are, retired from the practice or primary care services provider, suspended by either the GMC or the PCT or any other successor body;
2.6.2.3. If the individual is a Sessional GP, they shall not be eligible in the event that they are suspended from their employment or subject to grievance or disciplinary proceedings; and
2.6.2.4. for those individuals (including those stated at (c) above) who are not party to direct contractual arrangements for the provision of primary medical services, they must be on a Performers List.
2.6.3. Applications will be assessed by a panel, convened by the governing body, to assess them against the essential criteria within the person specification. This panel will include a member of the LMC.
2.6.4. Elected NHS Bexley CCG Practice representatives on the governing body will serve a 2-year term from the date of appointment.
2.6.5. Voting: In accordance with the election principles used by the Royal College of GPs, the election will be run on the Single Transferable Vote system (see http://www.electoralreform.org.uk/article.php?id=48 for details of this voting system.)
2.6.6. The Bexley LMC will oversee the entire appointment process to ensure objectivity.

18
2.6.7. Roles will be funded via an agreed salary remunerated based on the number of sessions worked. Job descriptions for each elected role are available on the website, and specify minimum number of sessions / days required.
2.6.8. Remuneration will be reviewed every 2-years by the Remuneration Committee.
2.6.9. Grounds for removal from office will be considered to be material failure to comply with the terms of this constitution and/or as reasonably determined by the chair of the Governing Body.
2.6.10. Elected members may give 1 months’ notice to retire but are expected to serve full terms (or full years if a part term).
2.6.11. Where a member leaves office part way though a year the Governing Body may convene an election or co-opt a member to the Governing Body for the remainder of the year. Any such co-option to be reported to the Council of Members
2.7. Other GP and Primary Care Health Professionals 2.7.1. The group may identify a number of other GPs / primary care health
professionals from member practices to either support the work of the group and / or represent the group rather than represent their own individual practices.
2.7.2. Nominations / volunteers will be sought for individuals, as required, and eligibility will be based on demonstrated expertise in the specific area required.
2.7.3. Should there be more than one nomination / volunteer, the governing body, will assess the applications and appoint based on their consideration of the applicant most likely to be in a position to best fulfil the role.
2.7.4. These roles will be time limited to the length of the project / task.
2.7.5. Grounds for removal from office will be considered to be material failure to comply with the terms of this constitution and/or as reasonably determined by the chair of the Governing Body.
2.7.6. Notice period –.this will be determined in light of the need to ensure continuous representation.

19
2.8. The Chair of the Governing Body The roles and responsibilities of the NHS Bexley CCG Chair are defined in the Job Description for this role, which is available on the website at www.bexley.nhs.uk.
2.8.1. Chair of the Governing Body is subject to the following appointment process:
Nominations: Selection and interview
Eligibility: GP representatives working in Bexley as a GP principal or salaried GP (a minimum of two sessions per week in Bexley
Appointment process: shortlisted, and elected by member representatives following interview
Term of office: 2 years
Eligibility for reappointment: GP within Bexley and meet the person specification
Grounds for removal from office:
Material failure to comply with the terms of this constitution and/or the passing of a vote of no-confidence vote of no confidence by simple majority of those eligible to vote on Governing Body
Notice period: 6 months
2.9. The Deputy Chair of the Governing Body 2.9.1. The deputy chair will assume responsibility for chair when the CCG is absent
or cannot participate in discussions due to a declared conflict of interest. Nominations: by shortlist and interview. If a GP, by election as above
Eligibility: by meeting job description
Appointment process: as above
Term of office: 2 years
Eligibility for reappointment: as above
Grounds for removal from office:
material failure to comply with the terms of this constitution and/or as reasonably determined by the chair of the Governing Body
Notice period: if employed, as per contract, if elected, 6 months

20
2.10. Accountable Officer 2.10.1. The governing body shall appoint an Accountable Officer.
2.10.2. The Chief Officer shall report directly to the governing body of the Clinical Commissioning Group and to the National Commissioning Board, and is subject to the following appointment process:
2.10.2.1. Nominations: not applicable – appointment by application and assessment centre;
2.10.2.2. Eligibility: Meet Job specification, and assessment centre 2.10.2.3. Appointment process: interview subject to successful competency
assessment; 2.10.2.4. Term of office: for as long as the post holder remains an employee of
Bexley CCG in this role; 2.10.2.5. Grounds for removal from office: material failure to comply with the
terms of this constitution, and/or as reasonably determined by the chair of the Governing Body, and/or the passing of a vote of no-confidence by the Group and in accordance with the Contract of Employment;
2.10.2.6. Notice period: 6 months written notice by the role holder to the chair.
2.11. Chief Financial Officer 2.11.1. The governing body shall appoint a Chief Financial Officer.
2.11.2. The Chief Financial Officer shall report directly to the Chief Officer but with joint accountability to the Chair of the Governing Body and be subject to the following appointment process:
2.11.2.1. Nominations: not applicable – appointment by application and assessment centre;
2.11.2.2. Eligibility: recognised professional accounting qualification 2.11.2.3. Appointment process: interview subject to successful competency
assessment; 2.11.2.4. Term of office: for as long as the post holder remains an employee of
Bexley CCG in this role; 2.11.2.5. Grounds for removal from office: material failure to comply with the
terms of this constitution, and/or as reasonably determined by the chair of the Governing Body, and/or the passing of a vote of no-confidence by the Group and in accordance with the Contract of Employment;
2.11.2.6. Notice period: three months written notice by the role holder to the Accountable Officer and the chair.

21
2.12. The Director of Governance and Quality 2.12.1. The Director of Governance and Quality is subject to the following
appointment process:
2.12.1.1. Nominations: not applicable – appointment by application; 2.12.1.2. Eligibility: recognised professional management experience; 2.12.1.3. Appointment process: appointment by the Governing Body following
open advertisement, and successful competency assessment interview; 2.12.1.4. Term of office: for as long as the post holder remains an employee of
Bexley CCG in this role; 2.12.1.5. Grounds for removal from office: material failure to comply with the
terms of this constitution and/or as reasonably determined by the chair of the Governing Body and in accordance with the Contract of Employment;
2.12.1.6. Notice period: three months written notice by the role holder to the chair and the Accountable Officer.
2.13. The Director of Commissioning 2.13.1. The Director of Commissioning is subject to the following appointment
process:
2.13.1.1. Nominations: not applicable – appointment by application; 2.13.1.2. Eligibility :recognised professional management experience; 2.13.1.3. Appointment process: appointment by the Governing Body following
open advertisement and successful competency assessment interview; 2.13.1.4. Term of office: for as long as the post holder remains an employee of
Bexley CCG in this role; 2.13.1.5. Grounds for removal from office: material failure to comply with the
terms of this constitution and/or as reasonably determined by the chair of the Governing Body and in accordance with the Contract of Employment
2.13.1.6. Notice period: three months written notice by the role holder to the chair and the Accountable Officer.
2.14. The Lay Member 2.14.1. The lay member is subject to the following appointment process:
2.14.1.1. Nominations: not applicable – appointment by application, shortlist and interview;
2.14.1.2. Eligibility: local knowledge of the Bexley healthcare system; 2.14.1.3. Appointment process – open advertisement and appointment by the
Governing Body; 2.14.1.4. Term of office: two years; 2.14.1.5. Eligibility for reappointment: eligible for renewal of one term of the
appointment subject to demonstration of continuing competence;

22
2.14.1.6. Grounds for removal from office: material failure to comply with the terms of this constitution and/or as reasonably determined by the chair of the Governing Body
2.14.1.7. Notice period: six months written notice by the role holder to the chair.
2.15. The Registered Nurse 2.15.1. The registered nurse is subject to the following appointment process:
2.15.1.1. Nominations: not applicable – appointment by application and competitive interview;
2.15.1.2. Eligibility: a registered nurse with local knowledge of the Bexley healthcare system but who is NOT an employee or member (including shareholder) of, or a partner in, any of the following: a person who is a “provider of primary medical services” for the purposes of Chapter A2 of the 2006 Act; or a body which provides any “relevant service” to a person for whom the CCG has responsibility (regulation 12(1) CCG Regulations 2012). ;
2.15.1.3. Appointment process: appointment by the Governing Body following open advertisement and successful interview;
2.15.1.4. Term of office: two years; 2.15.1.5. Eligibility for reappointment :eligible for renewal of one term of the
appointment subject to demonstration of continuing competence; 2.15.1.6. Grounds for removal from office :material failure to comply with the
terms of this constitution and/or as reasonably determined by the chair of the Governing Body;
2.15.1.7. Notice period: six months written notice by the role holder to the chair.
2.16. The secondary care specialist doctor 2.16.1. The secondary care specialist doctor is subject to the following
appointment process:
2.16.1.1. Nominations :not applicable – appointment by application and competitive interview;
2.16.1.2. Eligibility: a secondary care specialist doctor who has local knowledge of the Bexley healthcare system but who is NOT an employee or member (including shareholder) of, or a partner in, any of the following: a person who is a “provider of primary medical services” for the purposes of Chapter A2 of the 2006 Act; or a body which provides any “relevant service” to a person for whom the CCG has responsibility (regulation 12(1) CCG Regulations 2012). ;
2.16.1.3. Appointment process: appointment by the Governing Body following open advertisement and successful interview;
2.16.1.4. Term of office: two years; 2.16.1.5. Eligibility for reappointment : eligible for renewal of one term of the
appointment subject to demonstration of continuing competence;

23
2.16.1.6. Grounds for removal from office: material failure to comply with the terms of this constitution and/or as reasonably determined by the chair of the Governing Body;
2.16.1.7. Notice period: six months written notice by the role holder to the chair.
2.17. DISQUALIFICATION OF MEMBERS OF THE GOVERNING BODY 2.17.1. Elected members of the governing body shall vacate their office:-
2.17.1.1. if any insolvency event or action is made against her or him or s/he makes any arrangement with her/his creditors;
2.17.1.2. if in the opinion of the governing body (having taken appropriate professional advice in cases where it is deemed necessary) s/he becomes or is deemed to have developed mental or physical illness which prohibits or inhibits their ability to undertake their role;
2.17.1.3. if s/he ceases to be a provider of primary medical services, or engaged in or employed to deliver primary + (excluding lay members of the governing body who have been duly appointed by the governing body);
2.17.1.4. if s/he is suspended from providing primary medical services in which case the removal or suspension from the governing body shall be at the discretion of the governing body. The governing body shall take into account the circumstances of any individual before a decision is made;
2.17.1.5. if s/he shall for a period of 5 consecutive meetings of the governing body have been absent and shall at the discretion of the governing body be vacated from her/his office;
2.17.1.6. If s/he shall be convicted of a criminal offence whereby the sentence imposed shall be for a minimum of 6 months imprisonment (whether such sentence is held to be suspended or conditional). The governing body shall take into account the circumstances of the offence in relation to the individual before a decision is made;
2.17.1.7. if s/he shall have behaved in a manner or exhibited conduct which in the opinion of the governing body has or is likely to be detrimental to the honour and interest of the governing body or the Clinical Commissioning Group and is likely to bring the governing body and/or Clinical Commissioning Group into disrepute. This includes but is not limited to dishonesty, misrepresentation (either knowingly or fraudulently), defamation of any member of the governing body (being slander or libel), abuse of position, non-declaration of a known conflicts of interest, seeking to lead or manipulate a decision of the governing body in a manner that would ultimately be in favour of that member whether financially or otherwise;
2.17.1.8. where s/he has become ineligible to stand for a position as a result of the declaration of any Conflicts of Interest under section 8 of the Constitution.
2.17.1.9. they die.

24
3. MEETINGS OF THE CLINICAL COMMISSIONING GROUP (CCG), GOVERNING BODY, COMMITTEES AND SUB-COMMITTEES 3.1. Meetings of the Primary Care Advisory Group and Locality Groups
3.1.1. Calling meetings
3.1.1.1. Primary Care Advisory Group and Locality meetings of the group shall be held at regular intervals at such times and places as the group may determine.
3.1.1.2. One third or more members of the Primary Care Advisory Group or Locality may requisition a meeting in writing. If the chairman refuses, or fails, to call a meeting within seven days of a requisition being presented, the members signing the requisition may forthwith call a meeting
3.1.2. Voting mechanisms at Primary Care Advisory Group and Locality Meetings
3.1.2.1. Voting is by a simple majority. Practices will have one vote per 5000 patient list size (as recorded on 1st April each year)
3.1.2.2. There is no postal voting
3.1.2.3. Proxy voting is not allowed. All votes must be cast when present at a group meeting
3.1.3. Agenda, supporting papers and business to be transacted
3.1.3.1. The agenda will be sent to members seven days before the meeting and supporting papers, whenever possible, shall accompany the agenda but will certainly be despatched no later than three clear days before the meeting, saving in emergency. The Board may determine that certain matters shall appear on every agenda for a meeting and shall be addressed prior to any other business being conducted. Such matters may be identified within this Constitution or following subsequent resolution shall be listed in an appendix to the Constitution.
3.1.3.2. The agenda shall be deemed to be a formal notice specifying the business proposed to be transacted shall be e-mailed or delivered to every member or sent by post to the usual place of residence or work of each member before the meeting. Want of service of such a notice on any member shall not affect the validity of a meeting.
3.1.3.3. In the case of a meeting called by members in default of the Chairman calling the meeting the notice shall be signed by those members.
3.1.3.4. No business shall be transacted at the meeting other than that specified on the agenda or emergency motions allowed under the Standing Order (? – to be checked)

25
3.1.3.5. A member desiring a matter to be included on an agenda shall make his/her request in writing to the Chairman at least 15 clear days before the meeting. The request should state whether the item of business is proposed to be transacted in the presence of the public and should include appropriate supporting information. Requests made less than 15 days before a meeting may be included on the agenda at the discretion of the chairman.
3.1.3.6. The Governing Body will arrange for adequate time to be allocated to each agenda items to allow for appropriate discussion within the planned meeting schedule. Where members require greater time to discuss a matter, they may vote to have an additional meeting or to extend the current meeting to discuss the matter further, provided that enough members commit to the new or extended meeting to allow that meeting to be quorate.
3.1.4. Petitions
3.1.4.1. Where a petition has been received by the CCG the Chair shall include the petition as an item for the agenda of the next meeting.
3.1.5. Chair of meeting
3.1.5.1. At any meeting of the group the Chair, if present, shall preside. If the Chair is absent from the meeting an elected GP from the Governing Body shall preside, if no elected GP members of the Governing Body are able to chair the meeting, a member chosen by the members present, or by a majority of them shall preside.
3.1.5.2. If the Chair is absent temporarily on the grounds of a declared conflict of interest an elected GP from the Governing Body shall preside, if no elected GP members of the Governing Body are able to chair the meeting a. A member chosen by the members present or by a majority of them shall preside.
3.1.6. Chair's ruling
3.1.6.1. The decision of the Chair of the meeting on questions of order, relevancy and regularity and their interpretation of the Constitution, Standing Orders, Scheme of Reservation and Delegation and Prime Financial Policies at the meeting shall be final.
3.1.7. Quorum
3.1.7.1. No business shall be transacted at a meeting unless at least 50% of Members, rounded down to the next whole number are represented
3.1.7.2. If the Chairman or Member has been disqualified from participating in the discussion on any matter and/or from voting on any resolution by reason of a declaration of interest that person shall no longer count

26
towards the quorum. If a quorum is then not available for the discussion and/or the passing of a resolution on any matter, that matter may not be discussed further or voted upon at that meeting. Such a position shall be recorded in the minutes of the meeting. The meeting must then proceed to the next business.
3.1.8. Decision making
3.1.8.1. (Save as provided in these standing orders 3.9 – suspension of constitution and 3.10 variation and amendment of the constitution, every question put to a vote at a meeting shall be determined by a majority of the votes of the members present and voting on the question. In the case of an equal vote, the person presiding i.e. the Chairman of the meeting shall have a second and casting vote.
3.1.8.2. At the discretion of the Chairman, all questions put to the vote shall be determined by oral expression or by a show of hands, unless the Chairman directs otherwise, or it is proposed, seconded and carried that a vote be taken by paper ballot.
3.1.8.3. If at least one third of the members present so request, the voting on any question may be recorded so as to show how each member present voted or did not vote (except when conducted by paper ballot). If a member so requests, their vote shall be requested by name.
3.1.8.4. Absence is normally defined as being absent at the time of the vote. Only in exceptional circumstances may an absent member vote by proxy. In exceptional circumstances the member may request that the Chair of the CCG casts a specified vote or votes on behalf of the member. Where the Chair is unable to cast the proxy vote, due to absence or conflict, the chair shall arrange for the chair of the meeting, or the relevant part of the meeting to cast the specified vote(s) on behalf of the member.
3.1.8.5. A manager who has been formally appointed to act up for an Officer Member during a period of incapacity or temporary absence without formal acting up status may not exercise the voting rights of the Officer Member. An Officer’s status when attending a meeting shall be recorded in the minutes.
3.1.8.6. For the voting rules relating to joint members see Standing Order 5.7.
3.1.9. Emergency powers and urgent decisions
3.1.9.1. Where decisions need to be taken as a matter of urgency the Chair may make decisions on behalf of the CCG or any Committee of the CCG after taking advice and achieving agreement with two of:-
3.1.9.1.1. the Deputy Chair
3.1.9.1.2. the Chair of the Audit Committee

27
3.1.9.1.3. the Chair of the Remuneration Committee
3.1.9.1.4. a GP Member of the Governing Body
3.1.9.2. Such decisions to be reported to the next meeting of the Council of Members, the Governing Body and any relevant committee.
3.2. Governing Body: Calling Meetings 3.2.1. The CCG governing body will meet a minimum of six times per annum.
3.2.2. Formal governing body meetings will be open to the public except where the group considers that it would not be in the public interest to permit members of the public to attend a meeting or part of a meeting. A minimum of 1 meeting per quarter will be held in public regardless.
3.2.3. An annual general meeting of the CCG (AGM) will be held in public once per year.
3.2.4. A minimum of one month’s advance notice will be given for all meetings of the governing body. Dates of public meetings will be advertised on the website: www.bexley.nhs.uk
3.2.5. The Chair or Deputy Chair can call a meeting at any time.
3.2.6. Constituent members are able to call an extraordinary general meeting (EGM) of the governing body, where due process has been followed. In the first instance, constituent members should indicate their reasons for calling a meeting to the locality, and if supported by the locality, the request must be put in writing to the CCG Chair, which must include details of the business to be transacted at that meeting; on receipt of which a meeting will be convened.
3.2.7. An EGM shall take place within 14 days of the governing body receiving the request for the meeting to be held.
3.3. Agenda, supporting papers and business to be transacted 3.3.1. The Chair is responsible for drawing up the agenda for the CCG governing
body meetings.
3.3.2. Items of business to be transacted for inclusion on the agenda of a meeting need to be notified to the Corporate Office Manager at least 10 working days (i.e. excluding weekends and bank holidays) before the meeting takes place.

28
3.3.3. Except in cases of urgency or where circumstances make it impracticable to do so, the agenda will be issued a minimum of five working days before the meeting.
3.3.4. Except in cases of urgency or where circumstances make it impracticable to do so papers will be issued a minimum of five working days before the meeting. At the discretion of the Chair, papers may be tabled where appropriate.
3.3.5. Agendas and papers for the public meetings of the group’s governing body – including minutes and details about meeting dates, times and venues - will be published on the group’s website at www.Bexley.nhs.uk.
3.3.6. Items may be added to the agenda through agreed channels. In the first instance, constituent members should propose the agenda item to the locality. If supported, it will be proposed to the CCG Chair for inclusion as a future agenda item.
3.3.7. For all other of the group’s committees and sub-committees, including the governing body’s committees and sub-committees, the details of how meetings are called are set out in the appropriate terms of reference.
3.4. Petitions 3.4.1. Where a petition has been received from the public, by the CCG, the Chair
shall include the petition as an item for the agenda of the next meeting of the governing body.
3.5. Chair of meeting 3.5.1. At any meeting of the group or its governing body or of a committee or sub-
committee, the chair of the group, governing body, committee or sub-committee, if any and if present, shall preside. If the chair is absent from the meeting, the deputy chair, if any and if present, shall preside.
3.5.2. If the chair is absent temporarily on the grounds of a declared conflict of interest the deputy chair, if present, shall preside. If both the chair and deputy chair are absent, or are disqualified from participating, or there is neither a chair or deputy a member of the group, governing body, committee or sub-committee respectively shall be chosen by the members present, or by a majority of them, and shall preside.

29
3.6. Chair's ruling 3.6.1. The decision of the Chair of the meeting on questions of order, relevancy and
regularity and their interpretation of the constitution, standing orders, scheme of reservation and delegation and prime financial policies at the meeting, shall be final.
3.7. Quorum 3.7.1. The governing body will be quorate if five members are present, made up of
the following members : 3.7.1.1. , two GPs, 3.7.1.2. Chair or a Lay Member, 3.7.1.3. Accountable Officer or Chief Finance Officer, 3.7.1.4. the Specialist Hospital Doctor or Registered Nurse),
3.7.2. Deputies will not generally be allowed but permission can be sought from the Chair.
3.7.3. An employee who has been formally appointed to act up for the Accountable Officer or Chief Financial Officer during a period of incapacity or temporarily to fill a vacancy, shall count towards the quoracy of the meeting.
3.7.4. An employee attending the governing body meeting to represent a governing body member during a period of incapacity or temporary absence without formal acting up status will not count towards the quoracy of the meeting. An employee’s status when attending the meeting shall be recorded in the minutes
3.7.5. If the Chair of the governing body or member has been disqualified from participating in the discussion on any matter and/or from voting on any resolution by reason of a declaration of a conflict of interest (see section 8 of the Constitution), that person shall no longer count towards the quorum. If a quorum is then not available for the discussion and/or the passing of a resolution on any matter, that matter may not be discussed further or voted upon at that meeting. Such a position shall be recorded in the minutes of the meeting. The meeting must then proceed to the next business.
3.7.6. The quorum for Committees and sub-committees of the governing body are as laid out in terms of reference for those groups.
3.7.7. If a quorum is not present within 15 minutes of the time appointed for a meeting to commence, all business which should have been transacted at that meeting shall be held over until the next meeting, unless an EGM is called in the meantime for the transaction of that business.
3.7.8. If, during a meeting, it appears to the Chair that a quorum has ceased to exist, business will be suspended:

30
3.7.9. a quorum exists, the business will proceed; 3.7.10. a quorum does not exist, the meeting will be dissolved and all
remaining business will be adjourned to the next meeting.
3.7.11. If more than half the members of the governing body declare an
interest in a vote or discussion, and quorum is thus lost, the Accountable Officer and the audit chair shall co-opt senior members of the Clinical Commissioning Group officers who do not have an interest to determine the issue.
3.8. Decision making 3.8.1. Generally it is expected that at the governing body’s meetings, decisions will
be reached by consensus. Should this not be possible then a vote of members by show of hands will be required, the process for which is set out below:
3.8.2. Eligibility – voting members of the governing body may vote. Persons acting on behalf of an absent member of the governing body may vote at the discretion of the Chair;
3.8.3. All eligible governing body members have a single vote. A majority vote will be taken as decisive. In the event of a tie, the Chair has the casting vote.
3.8.4. Should a vote be taken, the outcome of the vote, and any dissenting views, must be recorded in the minutes of the meeting.
3.8.5. For all of the governing body’s committees and sub-committee, the details of the process for holding a vote are set out in the appropriate terms of reference.
3.8.6. Decisions excluded from the process set out above will be: 3.8.6.1. any matter delegated by the NHS Bexley CCG governing body to a
named 3.8.6.2. individual or sub-committee.
3.9. Emergency powers and urgent decisions 3.9.1. It is recognised that there will be times when urgent decisions are required.
The Chair has the discretion to define urgent decisions.
3.9.2. In an emergency, where a decision must be made by the governing body before its next meeting, the powers and duties of the governing body may be exercised by the Chair (Emergency Action).

31
3.9.3. or this purpose “emergency” means circumstances in which:-
3.9.4. the governing body will be unable to discharge its statutory functions or be exposed to a significant level of risk if urgent action is not taken; or urgent action must be taken to prevent loss, damage or significant disadvantage to the CCG.
3.9.5. To ensure transparency, any urgent decisions will be recorded and notified in the minutes of the next regular meeting of the CCG governing body.
3.9.6. If decisions have an immediate impact on the wider CCG and constituent members, the locality chairs will be informed at the earliest convenience, so information can be shared with localities.
3.9.7. The Chair and Accountable Officer have the authority to make an urgent decision without consultation with the localities or governing body. Where possible, the Accountable Officer will always discuss decisions with the Chair or Deputy Chair, and in their absence will notify a governing body GP lead.
3.9.8. If chair’s action is required, the chair will consult with at least two other governing body representatives before confirming the action.
3.9.9. The Emergency Action functions of the Chair and Accountable Officer may be exercised by such other persons as the Chair and Accountable Officer may respectively nominate in writing.
3.10. Suspension of Standing Orders 3.10.1. Except where it would contravene any statutory provision or any
direction made by the Secretary of State for Health or the NHS Commissioning Board, any part of these standing orders may be suspended at any meeting, provided 50% of group members are in agreement.
3.10.2. A decision to suspend standing orders together with the reasons for doing so shall be recorded in the minutes of the meeting.
3.10.3. A separate record of matters discussed during the suspension shall be kept. These records shall be made available to the governing body’s Audit and Integrated Assurance Committee for review of the reasonableness of the decision to suspend standing orders.
32
3.11. Application for variation and amendment of the Constitution 3.11.1. Requests by NHS Bexley CCG Members to vary this constitution may
only be made in the following manner:
3.11.1.1. Formal proposals for amendment shall be sent to the Chair of the NHS Bexley CCG governing body via the Locality Group, who shall place them before the governing body members for consideration at the earliest opportunity. The governing body shall not consider the proposal unless members have received at least ten days clear notice of such proposals in advance of the next scheduled meeting;
3.11.1.2. amendments proposed by the governing body shall be put to the next meeting of the Primary Care Advisory Group for decision by vote;
3.11.1.3. a governing body member may invoke an extraordinary meeting to propose an amendment to the constitution at any time; and
3.11.1.4. a constituent practice may invoke an extraordinary NHS Bexley CCG governing body meeting to propose an amendment to the constitution by taking concerns to the locality for referral to discuss at the next meeting of the Primary Care Advisory Group. Where 50% of practices are in support, a formal request can be submitted to the governing body.
3.11.2. This constitution can only be varied in two circumstances:
3.11.2.1. where the group, defined as a minimum of 75% of practice members within the CCG formally applies in writing to the NHS Commissioning Board and that application is granted;
3.11.2.2. where in the circumstances set out in legislation the NHS Commissioning Board varies the group’s constitution other than on application by the group.
3.11.3. In the first instance, the constitution will be subject to formal review after 2 years from the date of commencement. Subsequent to this, they will be reviewed every 4 years unless there are significant concerns raised.
3.11.4. Variations to the constitution will be given to all practice members through accepted communication methods, and more formally through locality and Primary Care Advisory Group meetings.

33
3.12. Record of Attendance 3.12.1. The names and roles (and practices, as appropriate) of all members of
the meeting present at the meeting shall be recorded in the minutes of the group’s meetings. The names of all members of the governing body present shall be recorded in the minutes of the governing body meetings. The names of all members of the governing body’s committees / sub-committees present shall be recorded in the minutes of the respective governing body committee / sub-committee meetings.
3.13. Minutes 3.13.1. For each meeting, an officer will be nominated to draft minutes. These
will be reviewed by the Chair of the meeting, prior to distribution to publication.
3.13.2. Names of individuals and their roles will be recorded within the minutes.
3.13.3. Minutes will be confirmed as a true record through formal acknowledgment at the succeeding meeting that they are indeed a true reflection. Any amendments will be acknowledged and the minutes updated accordingly.
3.13.4. The signed minutes of a meeting shall, unless the contrary is proved, be conclusive proof of the proceedings of that meeting.
3.13.5. Where appropriate, minutes will be made available to constituent members through the GP zone, or accessible to the public on the website: www.bexley.nhs.uk.
3.14. Admission of public and the press 3.14.1. To prevent disruption, discuss a confidential issue or where publicity on
a matter would be prejudicial to the public interest, the CCG Chair or Deputy Chair has the authority to exclude the press or public to a meeting.
3.14.2. The minutes, following exclusions, will be kept separately from the public meeting and only distributed to those individuals with whom the matter concerns.
3.14.3. Where press or public are excluded, members, employees and committee members will not be permitted to disclose confidential contents of papers or minutes, or content of any discussion at meetings on these topics,

34
outside the CCG without express permission of NHS Bexley CCG governing body
3.15. Conduct of meetings 3.15.1. The order of business at a meeting shall follow that set out in the
agenda unless it is varied by the Chair with the consent of the meeting.
3.15.2. A member may only initiate a debate or move a motion on a matter which is not on the agenda with the consent of the meeting.
3.15.3. All motions must relate to matters that are within or related to the functions of the CCG.
3.15.4. Members shall not make derogatory personal references or use offensive expressions or improper language to any other member or any employee of the group.
3.15.5. A member must speak to the subject under discussion. The Chair may call attention to any irrelevance, repetition, unbecoming language or other improper conduct on the part of a member and, where the member persists in that conduct, may direct that member to cease speaking.
3.15.6. A ruling by the Chair on any question of order, whether or not provided for by the Standing Orders, shall be final and shall not be open to debate.
3.15.7. In the event of a disturbance which, in the opinion of the Chair, prevents the orderly conduct of business, the Chair may adjourn the meeting for such period as the Chair considers appropriate.
3.15.8. If a member of the public interrupts the proceedings at any meeting, the Chair may order that person to be removed from the meeting or may order the part of the room which is open to the public to be cleared.
4. APPOINTMENT OF COMMITTEES AND SUB-COMMITTEES
4.1. Appointment of committees and sub-committees 4.1.1. The group may appoint committees and sub-committees of the group, subject
to any regulations made by the Secretary of State, and make provision for the appointment of committees and sub-committees of its governing body.

35
4.1.2. Other than where there are statutory requirements, such as in relation to the governing body’s Audit and Integrated Assurance Committee or remuneration committee, the governing body shall determine the membership and terms of reference of committees and sub-committees and shall, if it requires, receive and consider reports of such committees at governing body meetings.
4.1.3. The provisions of these standing orders shall apply where relevant to the operation of NHS Bexley CCG, the governing body, the governing body’s committees and sub-committee and all committees and sub-committees unless stated otherwise in the committee or sub-committee’s terms of reference.
4.2. Terms of Reference 4.2.1. Terms of reference shall have effect as if incorporated into the constitution
and standing orders.
4.3. Delegation of Powers by Committees to Sub-committees 4.3.1. Where committees are authorised to establish sub-committees they may not
delegate executive powers to the sub-committee unless expressly authorised by the governing body.
4.4. Approval of Appointments to Committees and Sub-Committees 4.4.1. The governing body shall approve the appointments to each of the
committees and sub-committees which it has formally constituted including those of the governing body. Where the governing body determines that persons, who are neither members nor employees, shall be appointed to a committee or sub-committee the terms of such appointment shall be within the powers of the governing body. The governing body shall define the powers of such appointees and shall agree such travelling or other allowances as it considers appropriate.
5. DUTY TO REPORT NON-COMPLIANCE WITH STANDING ORDERS AND PRIME FINANCIAL POLICIES
5.1.1. If for any reason these standing orders are not complied with, full details of the non-compliance and any justification for non-compliance and the circumstances around the non-compliance, shall be reported to the next formal meeting of the governing body for action or ratification. All members of the group and staff have a duty to disclose any non-compliance with these standing orders to the Accountable Officer as soon as possible.

36
6. USE OF SEAL AND AUTHORISATION OF DOCUMENTS
6.1. Clinical Commissioning Group’s seal 6.1.1. The group may have a seal for executing documents where necessary. The
seal shall be kept in safe custody by the Accountable Officer or a person appointed by the Accountable Officer.
6.1.2. The following individuals or officers are authenticate the seal’s use by their signature:
6.1.2.1. The Chief Officer;
6.1.2.2. The Chair of the governing body;
6.1.2.3. The Deputy Chair of the Governing Body
6.1.2.4. The Chief Financial Officer. 6.1.2.5. The Director of Governance and Quality 6.1.2.6. The Director of Commissioning 6.1.2.7. Other individuals may be mandated by the governing body for this
particular purpose. 6.1.2.8.
6.2. Execution of a document by signature 6.2.1. The following individuals are authorised to execute a document on behalf of
the CCG by their signature:
6.2.1.1. The Chief Officer;
6.2.1.2. The Chair of the governing body;
6.2.1.3. The Deputy Chair of the Governing Body
6.2.1.4. The Chief Financial Officer.
6.2.1.5. The Director of Governance and Quality
6.2.1.6. The Director of Commissioning
37
6.2.1.7. Other individuals may be mandated by the governing body for this particular purpose.
7. OVERLAP WITH OTHER CLINICAL COMMISSIONING GROUP POLICY STATEMENTS / PROCEDURES AND REGULATIONS
7.1. Policy statements: general principles 7.1.1. The governing body will from time to time agree and approve policy
statements / procedures which will apply to all or specific groups of staff employed by NHS Bexley Clinical Commissioning Group. The decisions to approve such policies and procedures will be recorded in an appropriate governing body minute and will be deemed where appropriate to be an integral part of the CCG’s standing orders.

38
APPLICATION FOR AUTHORISATION
FINANCIAL MANAGEMENT ARRANGEMENTS
APPENDIX 2 SCHEME OF RESERVATION AND DELEGATION
ENCLOSURE: G (xi) – App1

39
APPENDIX 2
SCHEME OF RESERVATION AND DELEGATION

40
SCHEME OF RESERVATION & DELEGATION 1. SCHEDULE OF MATTERS RESERVED TO THE CLINICAL
COMMISSIONING GROUP AND SCHEME OF DELEGATION 1.1. The arrangements made by the group as set out in this scheme of reservation
and delegation of decisions shall have effect as if incorporated in the CCG’s constitution.
1.2. The clinical commissioning group remains accountable for all of its functions, including those that it has delegated.
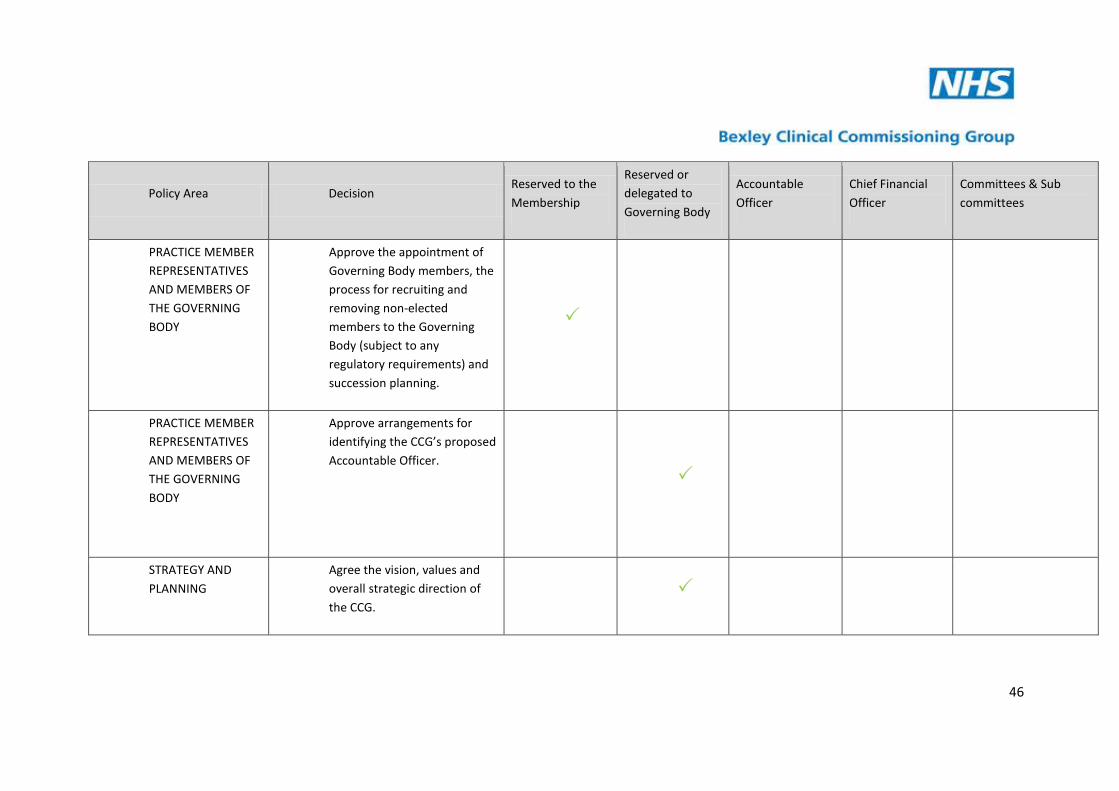
1.3. The following table shows those matters which are reserved and delegated for
the discharge of the groups’ functions.

41
Policy Area Decision Reserved to the Membership
Reserved or delegated to Governing Body
Accountable Officer
Chief Financial Officer
Committees & Sub committees
REGULATION AND CONTROL
Determine the arrangements by which the members of the group approve those decisions that are reserved for the membership.
REGULATION AND CONTROL
Consideration and approval of applications to the NHS Commissioning Board on any matter concerning changes to the group’s constitution, including terms of reference for the group’s governing body, its committees, membership of committees, the overarching scheme of reservation and delegated powers, arrangements for taking urgent decisions, standing orders and prime

42
Policy Area Decision Reserved to the Membership
Reserved or delegated to Governing Body
Accountable Officer
Chief Financial Officer
Committees & Sub committees
financial policies.
REGULATION AND CONTROL
Exercise or delegation of those functions of the clinical commissioning group which have not been retained as reserved by the group, delegated to the governing body or other committee or sub-committee or [specified] member or employee
REGULATION AND CONTROL
Prepare the CCG’s overarching scheme of reservation and delegation, which sets out those decisions of the CCG reserved to the membership

43
Policy Area Decision Reserved to the Membership
Reserved or delegated to Governing Body
Accountable Officer
Chief Financial Officer
Committees & Sub committees
and those delegated to the: CCG’s Governing Body, committees and sub-committees, or its members or employees and sets out those decisions of the Governing Body reserved to the Governing Body and those delegated to the Governing Body’s committees and sub-committees, members of the Governing Body,
an individual who is member of the CCG but not the governing body or a specified person for inclusion in the CCG’s constitution.
REGULATION AND CONTROL
Approval of the CCG’s overarching scheme of reservation and delegation

44
Policy Area Decision Reserved to the Membership
Reserved or delegated to Governing Body
Accountable Officer
Chief Financial Officer
Committees & Sub committees
REGULATION AND CONTROL
Prepare the CCG’s operational scheme of delegation, which sets out those key operational decisions delegated to individual employees of the CCG, not for inclusion in the CCG’s constitution.
REGULATION AND CONTROL
Approval of the CCG’s operational scheme of delegation that underpins the CCG’s ‘overarching scheme of reservation and delegation’ as set out in its constitution.
REGULATION AND CONTROL
Prepare detailed financial policies that underpin the CCG’s prime financial policies.
REGULATION AND CONTROL
Approve detailed financial policies.

45
Policy Area Decision Reserved to the Membership
Reserved or delegated to Governing Body
Accountable Officer
Chief Financial Officer
Committees & Sub committees
REGULATION AND CONTROL
Approve arrangements for managing exceptional funding requests.
REGULATION AND CONTROL
Set out who can execute a document by signature / use of the seal
PRACTICE MEMBER REPRESENTATIVES AND MEMBERS OF THE GOVERNING BODY
Approve the arrangements for:
identifying practice members to represent practices in matters concerning the work of the CCG; and
appointing clinical leaders to represent the CCG’s membership on the CCG’s governing body, for example through election (if desired).
46
Policy Area Decision Reserved to the Membership
Reserved or delegated to Governing Body
Accountable Officer
Chief Financial Officer
Committees & Sub committees
PRACTICE MEMBER REPRESENTATIVES AND MEMBERS OF THE GOVERNING BODY
Approve the appointment of Governing Body members, the process for recruiting and removing non-elected members to the Governing Body (subject to any regulatory requirements) and succession planning.
PRACTICE MEMBER REPRESENTATIVES AND MEMBERS OF THE GOVERNING BODY
Approve arrangements for identifying the CCG’s proposed Accountable Officer.
STRATEGY AND PLANNING
Agree the vision, values and overall strategic direction of the CCG.

47
Policy Area Decision Reserved to the Membership
Reserved or delegated to Governing Body
Accountable Officer
Chief Financial Officer
Committees & Sub committees
STRATEGY AND PLANNING
Approval of the CCG’s operating structure.
STRATEGY AND PLANNING
Approval of the CCG’s commissioning plan.
STRATEGY AND PLANNING
Approval of the CCG’s corporate budgets that meet the financial duties as set out in section 5.3 of the main body of the constitution
STRATEGY AND PLANNING
Approval of variations to the approved budget where variation would have a significant impact on the overall approved levels of income and expenditure or the CCG’s ability to achieve its agreed strategic aims.

48
Policy Area Decision Reserved to the Membership
Reserved or delegated to Governing Body
Accountable Officer
Chief Financial Officer
Committees & Sub committees
ANNUAL REPORTS AND ACCOUNTS
Approval of the CCG’s annual report and annual accounts.
ANNUAL REPORTS AND ACCOUNTS
Approval of the arrangements for discharging the CCG’s statutory financial duties.
HUMAN RESOURCES
Approve the terms and conditions, remuneration and travelling or other allowances for Governing Body members, including pensions and gratuities.
Remuneration
HUMAN RESOURCES
Approve terms and conditions of employment for all employees of the CCG including, pensions, remuneration, fees and travelling or other allowances

49
Policy Area Decision Reserved to the Membership
Reserved or delegated to Governing Body
Accountable Officer
Chief Financial Officer
Committees & Sub committees
payable to employees and to other persons providing services to the CCG.
HUMAN RESOURCES
Approve any other terms and conditions of services for the CCG’s employees.
HUMAN RESOURCES
Determine the terms and conditions of employment for all employees of the CCG
HUMAN RESOURCES
Determine pensions, remuneration, fees and allowances payable to employees and to other persons providing services to the CCG.
Remuneration
HUMAN RESOURCES
Recommend pensions, remuneration, fees and allowances payable to

50
Policy Area Decision Reserved to the Membership
Reserved or delegated to Governing Body
Accountable Officer
Chief Financial Officer
Committees & Sub committees
employees and to other persons providing services to the CCG.
HUMAN RESOURCES
Approve disciplinary arrangements for employees, including the Accountable Officer (where he/she is an employee or member of the CCG) and for other persons working on behalf of the CCG.
HUMAN RESOURCES
Review disciplinary arrangements where the Accountable Officer is an employee or member of another CCG.
HUMAN RESOURCES
Approval of the arrangements for discharging the CCG’s statutory duties as an employer.

51
Policy Area Decision Reserved to the Membership
Reserved or delegated to Governing Body
Accountable Officer
Chief Financial Officer
Committees & Sub committees
HUMAN RESOURCES
Approve human resources policies for employees and for other persons working on behalf of the CCG
QUALITY AND SAFETY
Approve arrangements, including supporting policies, to minimise clinical risk, maximise patient safety and to secure continuous improvement in quality and patient outcomes.
QUALITY AND SAFETY
Approve arrangements for supporting the NHS Commissioning Board in discharging its responsibilities in relation to securing continuous improvement in the quality of general medical services.

52
Policy Area Decision Reserved to the Membership
Reserved or delegated to Governing Body
Accountable Officer
Chief Financial Officer
Committees & Sub committees
OPERATIONAL AND RISK MANAGEMENT
Prepare and recommend an operational scheme of delegation that sets out who has responsibility for operational decisions within the CCG.
OPERATIONAL AND RISK MANAGEMENT
Approve the CCG’s counter fraud and security management arrangements
Audit
OPERATIONAL AND RISK MANAGEMENT
Approval of the CCG’s risk management arrangements.
Audit
OPERATIONAL AND RISK MANAGEMENT
Approve arrangements for risk sharing and or risk pooling with other organisations (for example arrangements for pooled funds with other CCGs or pooled budget arrangements under section

53
Policy Area Decision Reserved to the Membership
Reserved or delegated to Governing Body
Accountable Officer
Chief Financial Officer
Committees & Sub committees
75 of the NHS Act 2006).
OPERATIONAL AND RISK MANAGEMENT
Approval of a comprehensive system of internal control, including budgetary control, that underpin the effective, efficient and economic operation of the CCG
OPERATIONAL AND RISK MANAGEMENT
Approve proposals for action on litigation and claims handling against or on behalf of the CCG.
OPERATIONAL AND RISK MANAGEMENT
Approve the CCG’s arrangements for business continuity and emergency planning.
OPERATIONAL AND RISK MANAGEMENT
Approve the CCG’s arrangements for handling

54
Policy Area Decision Reserved to the Membership
Reserved or delegated to Governing Body
Accountable Officer
Chief Financial Officer
Committees & Sub committees
complaints.
INFORMATION GOVERNANCE
Approval of the arrangements for ensuring appropriate and safekeeping and confidentiality of records and for the storage, management and transfer of information and data.
TENDERING AND CONTRACTING
Approval of the CCG’s contracts for any commissioning support.
TENDERING AND CONTRACTING
Approval of the CCG’s contracts for corporate support (for example finance provision)
PARTNERSHIP WORKING
Approve decisions that individual
members or employees of

55
Policy Area Decision Reserved to the Membership
Reserved or delegated to Governing Body
Accountable Officer
Chief Financial Officer
Committees & Sub committees
the
CCG, participating in joint
arrangements on behalf of the
group can take. Such delegated
decisions must be disclosed in
this scheme of reservation and
delegation. Approve decisions
delegated to joint committees
established under section 75 of
the NHS Act 2006.

56
Policy Area Decision Reserved to the Membership
Reserved or delegated to Governing Body
Accountable Officer
Chief Financial Officer
Committees & Sub committees
COMMISSIONING AND CONTRACTING FOR CLINICAL SERVICES
Approval of the arrangements for discharging the CCG’s statutory duties associated with its commissioning functions, including but not limited to promoting the involvement of each patient, patient choice, reducing inequalities, improvement in the quality of services, obtaining appropriate advice and public engagement and consultation.
COMMISSIONING AND CONTRACTING FOR CLINICAL SERVICES
Approve arrangements for co-ordinating the commissioning of services with other CCGs and or with the local authority(ies), where appropriate

57
Policy Area Decision Reserved to the Membership
Reserved or delegated to Governing Body
Accountable Officer
Chief Financial Officer
Committees & Sub committees
COMMUNICATIONS/ INFORMATION GOVERNANCE
Approving arrangements for handling Freedom of Information requests.
COMMUNICATIONS/ INFORMATION GOVERNANCE
Determining arrangements for handling Freedom of Information requests.
COMMUNICATIONS/ INFORMATION GOVERNANCE
Approving a comprehensive Publication Scheme for the CCG

58
APPLICATION FOR AUTHORISATION
FINANCIAL MANAGEMENT ARRANGEMENTS
APPENDIX 3
SCHEDULE OF MATTERS DELEGATED TO OFFICERS
ENCLOSURE: G (xi) – App1

59
APPENDIX 3
SCHEDULE OF MATTERS DELEGATED TO OFFICERS

60
This Schedule of Matters delegated to officers has been developed in conjunction with the organisation’s Standing Financial Instructions and Standing Orders and will provide guidance for both the CCG and the Commissioning Support Unit, in respect of Bexley CCG. Delegated matters in respect of decisions, which may have a far-reaching effect, must be reported to the Chief Officer. The Delegation shown below is the lowest level to which authority is delegated. Authority can be delegated upwards with no further action being required. However, delegation to lower levels is only permitted with written approval of the Chief Officer who may, before authorising such delegation, consult with other Senior Officers as appropriate. All items concerning Finance must be carried out in accordance with the organisation’s Standing Orders, Standing Financial Instructions and Detailed Financial Procedures. All financial limits in this schedule of matters delegated to officers are subject to sufficient budget being available.

61
REF
DELEGATED MATTERS
AUTHORITY DELEGATED TO
1 Bank Accounts
Maintenance and Operation in accordance with mandates approved by the CCG Governing Body
All banking administered by CSU, but must be managed in accordance with organisational SFIs and SOs. Locally, these are in line with the CCG Detailed Financial Procedures.
2 CCG Budgets
Responsibility for keeping expenditure within budgets
a) At individual budget level (Pay and Non Pay)
b) At service level
c) For the totality of service covered by directorate
a) Budget Manager
b) Head of Service/Departmental Manager
c) Director of Service or equivalent
3
Business Cases/Additional Budgetary Requirements for CCG budgets (the limits below relate to full year costs, not total costs over the life of the project)fiannce committeefi
NB Business cases needing Governing Body approval will need to be approved by those that do not have any declared conflict of interest.

62
REF
DELEGATED MATTERS
AUTHORITY DELEGATED TO
i)
ii)
Developmental Business Cases
a) Up to £100,000
b) £100,001 to £250,000
c) Over £250,001
Mini Business Cases for Clinical Care for services which the CCG is responsible (where patient care must be funded via Health and an urgent decision is required). Funding may be made available or information will be noted as a cost pressure for future years.
The “Mini Business Case” should consist of 2 pages of A4 providing details on the history of patient care, clinical needs which require funding, and the funding required (by component).
a) Up to £100,000
b) Over £100,000
a) Approved by Finance working group, sent to Governing Body for information.
b) Approved by Executive management committee on the recommendation of the Finance working group
c) Approved by Governing Body on the recommendation of the Finance working group
a) Mini business case approved by Finance working group, sent to Governing Body for information.
b) Approved by Executive management committee on the recommendation of the Finance working group
4 Capital Schemes
a) Selection of architects, quantity surveyors, consultant
All capital schemes relating to property will be the responsibility of

63
REF
DELEGATED MATTERS
AUTHORITY DELEGATED TO
engineer and other professional advisors within EU regulations b) Financial monitoring and reporting on all capital scheme
expenditure to Audit Committee (Integrated Governance Committee)
PropCo and therefore the CCG will not have any involvement.
For IT and minor capital schemes, the CCG revenue authorised limits plus detailed financial procedures will be applicable.
5 Charitable and Endowment Funds
Funding Requests (limits per individual request)
a) Up to £1,000
b) Up to £10,000
c) Over £10,000
The CCG does not currently hold any Charitable or Endowment Funds.
6 Clinical Trials
Authorisation of Clinical Trials
Governing Body in conjunction with Director of Governance and Quality, Head of Quality, Clinical Governance and Risk Manager and Corporate Governance and Risk Manager
7
i)
Commissioning Expenditure
Acute Commissioning Expenditure
a) Signing of annual Service Level Agreements with NHS Providers below £5,000,000
b) Signing of annual Service Level Agreements with NHS Providers above £5,000,000
a) Chief Officer and Director of Commissioning
b) Chief Financial Officer and Chief Officer and Director of
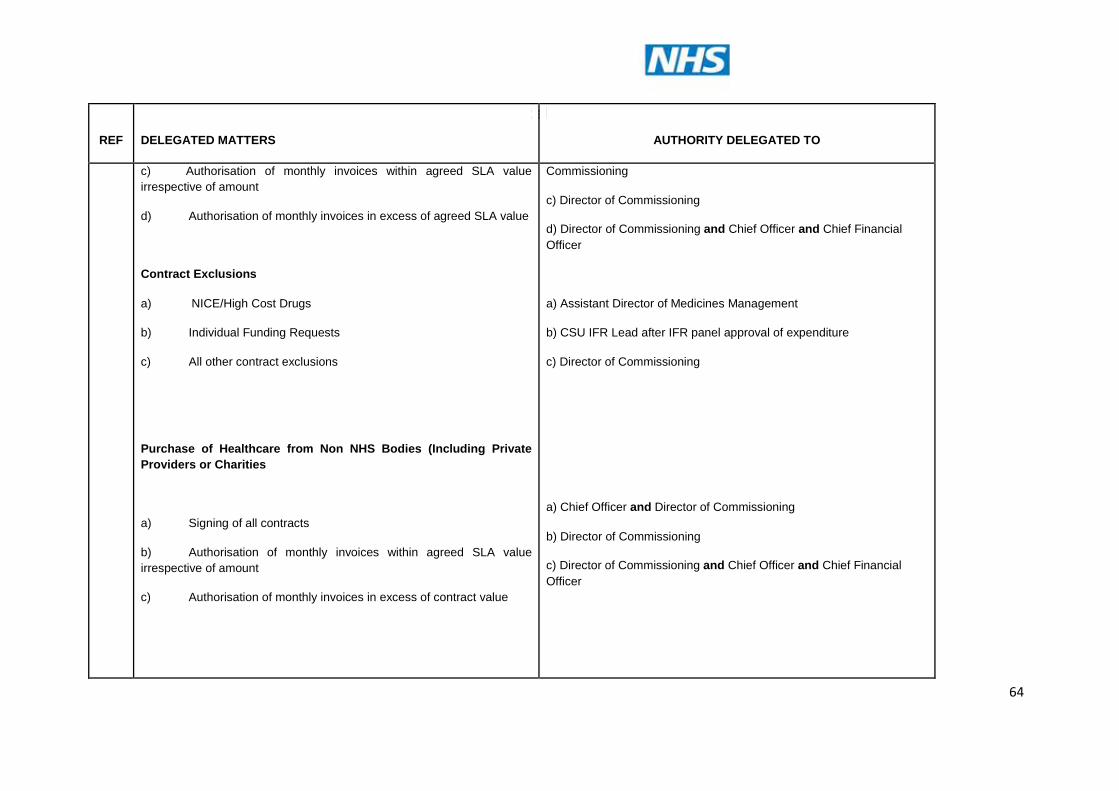
64
REF
DELEGATED MATTERS
AUTHORITY DELEGATED TO
c) Authorisation of monthly invoices within agreed SLA value irrespective of amount
d) Authorisation of monthly invoices in excess of agreed SLA value
Contract Exclusions
a) NICE/High Cost Drugs
b) Individual Funding Requests
c) All other contract exclusions
Purchase of Healthcare from Non NHS Bodies (Including Private Providers or Charities
a) Signing of all contracts
b) Authorisation of monthly invoices within agreed SLA value irrespective of amount
c) Authorisation of monthly invoices in excess of contract value
Commissioning
c) Director of Commissioning
d) Director of Commissioning and Chief Officer and Chief Financial Officer
a) Assistant Director of Medicines Management
b) CSU IFR Lead after IFR panel approval of expenditure
c) Director of Commissioning
a) Chief Officer and Director of Commissioning
b) Director of Commissioning
c) Director of Commissioning and Chief Officer and Chief Financial Officer

65
REF
DELEGATED MATTERS
AUTHORITY DELEGATED TO
ii)
Agreement of Named Placements (not Continuing Care Placements)
a) Up to £50,000 and within approved budget
b) Above £50,000 or in excess of available resources
Non acute and non primary care contracts, such as those for;
Mental Health, Learning Disability and CAMHS Services
Purchase of Healthcare from NHS Bodies
a) Signing of annual Service Level Agreements with NHS Providers below £5,000,000
b) Signing of annual Service Level Agreements with NHS Providers above £5,000,000
c) Authorisation of monthly invoices within agreed SLA value irrespective of amount
d) Authorisation of monthly invoices in excess of agreed SLA value
Contract Exclusions
a) NICE/High Cost Drugs
a) Assistant Director of Commissioning and Contracting
b) Director of Commissioning with Finance working group approval
a) Chief Officer and Director of Commissioning
b) Chief Financial Officer and Chief Officer and Director of Commissioning
c) Director of Commissioning
d) Director of Commissioning and Chief Officer and Chief Financial Officer
a) Assistant Director of Medicines Management

66
REF
DELEGATED MATTERS
AUTHORITY DELEGATED TO
b) Individual Treatments
c) All other contract exclusions (within budget)
Purchase of Healthcare from Non NHS Bodies (Including Private Providers or Charities
a) Signing of all contracts
b) Authorisation of monthly invoices within agreed SLA value irrespective of amount
c) Authorisation of monthly invoices in excess of contract value
Agreement of Named Placements (not Continuing Care Placements)
a) Up to £50,000 and within approved budget
b) Above £50,000 or in excess of available resources
Continuing Care Packages
a) Signing of Contract for placement
b) Authorisation of monthly invoices within agreed contract value irrespective of amount
b) (CSU) IFR Lead after panel decision has been made
c) Director of Commissioning
a) Director of Commissioning
b) Director of Commissioning / AD Commissioning and Contracting
c) Director of Commissioning and Chief Financial Officer
a) AD Commissioning and Contracting
b) Chief Officer and Chief Financial Officer
a) Director of Commissioning
b) AD Commissioning and Contracting after Continuing Care

67
REF
DELEGATED MATTERS
AUTHORITY DELEGATED TO
c) Authorisation of monthly invoices in excess of contract value
Panel assessed and approved NHS funding
c) Director of Commissioning and Chief Financial Officer 8 Complaints (Patients and Relatives)
a) Overall responsibility for ensuring that all complaints are dealt with effectively
b) Responsibility for ensuring complaints relating to a directorate are investigated thoroughly
c) Medico – Legal Complaints
Co-ordination of their management
a) Chief Officer
b) Director of Service in conjunction with Director of Governance and Quality
c) Director of Governance and Quality
9 Condemning & Disposal
a) Items obsolete, obsolescent, redundant, and irreparable or cannot be repaired cost effectively.
i) with current/estimated purchase price up to £49
ii) with current estimated purchase price over £50
b) disposal of mechanical and engineering plant (subject to estimated income of less than £1,000 per sale)
All capital assets relating to property will be the responsibility of PropCo and therefore the CCG will not have any involvement.
However, items held locally such as excess furniture and redundant IT equipment can be approved for disposal by the Chief Officer or Chief Financial Officer

68
REF
DELEGATED MATTERS
AUTHORITY DELEGATED TO
c) disposal of mechanical and engineering plant (subject to estimated income exceeding £1,000 per sale)
d) disposal of excess furniture and redundant IT equipment
10 Contracts with Independent Contractors (GPs, dentists, pharmacists)
a) up to £249,000
b) from £250,000 to £999,000
c) from £1million to £3million
d) over £3million
All Primary Care Contract payments are the responsibility of the National Commissioning Board and therefore the CCG will not have any involvement
11 Drugs
Authorisation of New Drugs
- Estimated total yearly cost up to £50,000
- Estimated total yearly cost above £50,000
Medicines Management Group
Medicines Management Group and Governing Body

69
REF
DELEGATED MATTERS
AUTHORITY DELEGATED TO
12 Engagement of Agency Staff
a) Engagement of Trust’s Solicitors
b)
Booking of Bank or Agency Staff – within budget
- Medical Locums
- Nursing
- Clerical
C) Booking of Bank or Agency Staff – in excess of budget
a) Per LPP agreement and approval of one of the following:
Chief Officer, Chief Financial Officer, Director of Commissioning or Director of Governance and Quality
b)
Director or Assistant Director of Service
Director or Assistant Director of Service
Director or Assistant Director of Service
(with completion of correct HR forms)
C) Finance working group approval required
13 Extended Role Activities
Approval of Nurses to undertake duties/procedures which can properly be described as beyond the normal scope of Nursing Practice
Governing Body

70
REF
DELEGATED MATTERS
AUTHORITY DELEGATED TO
14 Facilities for staff not employed by the Trust to gain practical experience
a) Professional Recognition, Honorary Contracts & Insurance of Medical Staff
b) Non Medical Work experience students
a) Chief Officer and Head of Human Resources (CSU)
b) Chief Officer or Chief Financial Officer or Director of Commissioning or Director of Governance & Quality
15 relates to.
Fees and Charges
a) Private Patients, Overseas Visitors, Income Generation and other patient related services
b) CCG Services
a) Fees and Charges are administered by CSU but must be in compliance with organisational SFIs and SOs and in line with CCG detailed financial procedures
b) Chief Financial Officer
16 Review of fire precautions at CCG site
Corporate Office Manager
17 Hospitality
Applied to both individual and collective hospitality receipt items. In excess of £25 per item received
Declaration required by individual in Hospitality Register

71
REF
DELEGATED MATTERS
AUTHORITY DELEGATED TO
18 Co-ordination of Implementation of Internal and External Audit Recommendations
Internal audit services administered by CSU but must be in compliance with organisational SFIs and SOs and in line with CCG detailed financial procedures. All audit plans will be signed off by the Chief Officer of Chief Financial Officer. External audit will be jointly managed and must be in compliance with organisational SFIs and SOs and in line with CCG detailed financial procedures.
CCG and CSU staff will assist Internal and External auditors in their work and ensure that all audit recommendations are implemented in a timely fashion
19 Insurance Policies including NHSLA
Chief Financial Officer
20 Investment of Funds (Including Charitable & Endowment Funds)
The CCG does not hold any Charitable or Endowment Funds.
21 Invoice request certification for CCG Budgets
Excluding commissioning expenditure covered by section 7
a) Up to £999
a) Budget manager
b) Departmental Heads

72
REF
DELEGATED MATTERS
AUTHORITY DELEGATED TO
b) Up to £4,999
c) From £5,000 to £19,999
d) From £20,000 to £99,999
e) From £100,000 to £250,000
f) Over £250,000
c) Assistant Director of Service
d) Director of Service or equivalent
e) Chief Officer and Chief Financial Officer f) Reserved to the Governing Body
22 Licences/ Agreements
a) Extensions to existing leases
b) Letting of premises to outside organisations
c) Approval of rent based on professional assessment
All capital assets relating to property will be the responsibility of PropCo and therefore it is expected that the CCG will not have any involvement. Further guidance is awaited on head office accommodation.
23 Losses, Write-off & Compensation
a) Losses and Cash due to theft, fraud, overpayment etc
b) Fruitless Payments (including abandoned Capital Schemes).
c) Bad Debts
d) Claims Abandoned.
e) Damage to buildings, fittings, furniture and equipment and loss of equipment and property in stores and in use due to:
Losses and Compensations payments will be administered by the CSU but must be in compliance with organisational SFIs and SOs and in line with CCG detailed financial procedures. All costs to the CCG including write off of bad debts must be approved by the Chief Financial Officer.

73
REF
DELEGATED MATTERS
AUTHORITY DELEGATED TO
Culpable causes (e.g. fraud, theft, arson) or other.
f) Compensation payments made under legal obligation
g) Extra Contractual payments to contractors.
h) Ex-gratia Payments to Patients and staff for loss of personal effects:
i. up to £99
ii. £100-to £499
iii. £500 to £999
iv. £1,000 to £50,000
i) Ex-gratia payments for Clinical negligence(negotiated settlements following legal advice) – up to £250,000 including claimant’s legal costs
j) Ex-gratia payments for personal injury claims involving negligence where legal advice obtained and followed
k) Other ex-gratia payments except cases of maladministration where there is no financial loss by claimant- up to £50,000
l) Write off of NHS Debtors
24 Maintenance & Update of CCG Financial Procedures
Chief Financial Officer

74
REF
DELEGATED MATTERS
AUTHORITY DELEGATED TO
25 Management Consultants within budget
a) Obtaining quotations where aggregate commitment in any one year or total commitment is £4,999 or less
b) Obtaining 3 written quotations where aggregate commitment in any one year is from £5,000 to £24,999
c) Obtaining at least three competitive tenders where aggregate commitment in any one year is £25,000 or more
d) Authorising contracts of engagement following the above
a) Assistant Director of Service
b) Assistant Director of Service or equivalent
c) Director of Service or equivalent and Head of Procurement
d) Director of Service or equivalent and Chief Financial Officer
26 Orders & Requisitions (excluding Commissioning of Healthcare)
a) all orders/requisitions up to £999
all orders/requisitions up to £4,999
all orders/requisitions from £5,000 to £19,999
all orders/requisitions from £20,000 to £99,999
all orders/requisitions from £100,000 to £249,999
all orders/requisitions over £250,000
b) Works orders up to £4,999
Works orders from £5,000 to £19,999
Works orders from £20,000 to £99,999
Works orders from £100,000 to £249,999
a) up to £999 Budget Manager
up to £4,999 Departmental Heads
£5,000 to £19,999 Assistant Director of Service
£20,000 to £99,999 Director of Service or equivalent
£100,000 to £249,999 Chief Officer and Chief Financial Officer
over £250,000 Reserved to the Governing Body
b) up to £4,999 Corporate Office Manager
£5,000 to £19,999 Assistant Director of Service
£20,000 to £99,999 Director of Service or equivalent
100,000 to £249,999 Chief Officer and Chief Financial Officer
over £250,000 Reserved to the Governing Body

75
REF
DELEGATED MATTERS
AUTHORITY DELEGATED TO
Works orders over £250,000
c) Non-Pay Expenditure for which no specific budget has been set up and which is not subject to funding under delegated powers of virement.
Up to £24,999
Over £25,000
d) Orders exceeding 12 month period (including call off orders)
e) All contracts for goods & services and subsequent variations to
contracts
f) Urgent Payments and Orders – exceptional items, goods and services urgently required for an immediate operational need
i) Within budget
a) Up to £19,999
b) £20,000 to £74,999
c) £75,000 to £249,999
d) £250,000+
c)
Up to £24,999 Chief Financial Officer
Over £25,000 Chief Officer and Chief Financial Officer
d) Chief Officer or Chief Financial Officer
e) Chief Officer or Chief Financial Officer for amounts up to £75,000. Above this level Chief Officer and Chief Financial Officer subject to Governing Body approval if over £250,000
f)
i)
a) Director of Service or equivalent
b) Director of Service or equivalent and Chief Financial Officer
c) Chief Financial Officer and Chief Officer
d) Chairs action, Governing Body to ratify

76
REF
DELEGATED MATTERS
AUTHORITY DELEGATED TO
ii) Outside budget
a) Up to £74,999
b) £75,000 to £249,999
c) £250,000+
ii)
a) Director of Service or equivalent and Chief Financial Officer
b) Chief Financial Officer and Chief Officer
c) Chair’s action, Governing Body to ratify
27 Community Services
Variation of operating and clinic sessions within existing numbers
a) Outpatients
b) Other
c) Contract monitoring & reporting
a) Assistant Director of Service or Director of Service or equivalent
b) Assistant Director of Service or Director of Service or equivalent
c) Assistant Director of Service or Director of Service or equivalent
28 Payments to Independent Contractors outside of contract (GPs, dentists, pharmacists)
a) Up to £999 b) Up to £4,999 c) £5,000 to £19,999 d) £20,000 to £99,999 e) £100,000 to £250,000 f) over £250,000
All Primary Care Contract payments are the responsibility of the National Commissioning Board and therefore the CCG will not have any involvement

77
REF
DELEGATED MATTERS
AUTHORITY DELEGATED TO
29 Personnel & Pay
a) Authority to fill funded post on the establishment with permanent staff
b) Authority to appoint staff to post not on the agreed establishment:
c) All requests for upgrading/re-grading (dealt with in accordance with CCG procedures)
d) Approval of the extension of staff on fixed term contracts
e) Pay
i) Authority to complete standing data forms effecting pay, new starters variations and leavers
ii) Authority to complete and authorise positive reporting forms
iii) Authority to authorise overtime/flexi time
iv) Authority to authorise travel & Subsistence expenses up to £250
v) Authority to authorise travel & Subsistence expenses over £250
a) Budget Manager with approval of Director of Service or equivalent and Chief Financial Officer . (CSU) HR to be informed.
b) Director of Service or equivalent and Chief Financial Officer and Finance working group approval. (CSU) HR to be informed.
c) Director of Service or equivalent and Head of Human Resources (CSU) (will be subject to evaluation). Chief Financial Officer to be informed for budgetary purposes.
d) Chief Financial Officer and (CSU) Head of Human Resources to be informed
e)
i) Assistant Director of Service, Director of Service or equivalent and Head of Human Resources (CSU)
ii) Budget Manager
iii) Assistant Director of Service
iv) Budget Manager
v) Assistant Director of Service

78
REF
DELEGATED MATTERS
AUTHORITY DELEGATED TO
f) Leave
i) Approval of Annual Leave
ii) Annual Leave – approval to carry forward (up to maximum of 5 days or in the case of Ancillary & Maintenance Staff as defined in their initial conditions of service
iii) Payment of Annual Leave in exceptional circumstances
iv) Compassionate leave up to 3 days
v) Compassionate leave up to 6 days
vi) Special leave arrangements
- carers leave - up to 3 days in any one year
- up to 6 days in any one year
vii) Leave without pay
viii) Medical staff leave of absence
paid and unpaid leave less than 5 days
paid and unpaid leave more than 5 days
f)
i) Line/Department Manager
ii) Line/Department Manager
iii) Director of Service or equivalent
iv) Assistant Director of Service
v) Director of Service or equivalent
vi)
Assistant Director of Service and Head of Human Resources (CSU)
Director of Service or equivalent and Head of Human Resources (CSU)
vii) Director or Chief Officer
viii)
Chair of Governing Body
Chair of Governing Body and Chief Officer
ix) Director of Service, Chief Officer or Chief Financial Officer
x) Automatic approval with guidance and Head of Human Resources

79
REF
DELEGATED MATTERS
AUTHORITY DELEGATED TO
ix) Time off in lieu
x) Maternity and Paternity Leave – paid and unpaid
g) Sick Leave (in exceptional circumstances)
i) Extension of sick leave
ii) Return to work part-time on full pay to assist recovery
h) Study Leave
i) Study leave outside the UK
ii) Medical staff study leave (UK)
iii) All other study leave (UK)
i) Removal Expenses, Excess Rent and House Purchase
Authorisation of payment of removal expenses incurred by officers taking up new appointments (providing consideration was promised at interview)
i) up to £2,000
ii) over £2,000
j) Grievance Procedure
(CSU)
g)
i) Director or equivalent in conjunction with Head of Human Resources (CSU)
ii) Director or equivalent in conjunction with Head of Human Resources (CSU)
h)
i) Chief Officer
ii) Chief Officer and Chair of Governing Body
iii) Assistant Director of Service
i)
i) Chief Officer and Head of Human Resources (CSU)
ii) Chair of Governing Body and Chief Officer and Head of Human Resources (CSU)
j) See procedure
k)

80
REF
DELEGATED MATTERS
AUTHORITY DELEGATED TO
All grievance cases must be dealt with strictly in accordance with the Grievance Procedure and the advice of Human Resources Directorate
k) Authorised Car & Mobile Phone Users
i) Requests for new posts to be authorised as car users
ii) Requests for new posts to be authorised as mobile telephone users
l) Staff Retirement Policy
Authorisation of extensions of contract beyond normal retirement age in exceptional circumstances
m) Redundancy
Authorisation to agree voluntary redundancy and determine compulsory redundancies in accordance with policy
n) Ill Health Retirement
Decision to pursue retirement on the grounds of ill-health
o) Remuneration for Self-Employed Contractors – must comply
i) Director or equivalent in line with CCG Policy
ii) Director or equivalent in line with CCG Policy
l)
Director of Service or equivalent and Head of Human Resources (CSU)
m)
Director of Service or equivalent and Remuneration Committee with advice from Head of HR (CSS) and appropriate permission as required from National Commissioning Board, Department of Health, Treasury. Chief Financial Officer to be informed prior to offers to ensure available funding.
n)
Director of Service or Chief Officer following advice from Head of Human Resources (CSU) and Occupational Health.
o) Director of Service or equivalent and Chief Financial Officer following receipt of evidence to comply with revenue & customs guidance and employment tests

81
REF
DELEGATED MATTERS
AUTHORITY DELEGATED TO
with Revenue & Customs guidance (and David Nicholson letter) on such employment to ensure correct payment of tax & NI and employment status – preferable to employ or use agency.
p) Employment of voluntary workers
p) Director of Service or equivalent in conjunction with Head of Human Resources (CSU).
30 Petty Cash Disbursements
a) Expenditure up to £50 per item b) Expenditure over £50 per item
The CCG no longer has any petty cash function
31 Quotation, Tendering & Contract Procedures
This section does not apply to Management Consultants (see section 25)
a) Authority to award or sign contracts for goods/services after obtaining at least
i) 1 written quotation for expenditure less than £10,000
ii) At least 3 written quotations from £10,001 to £50,000
iii) At least 3 written competitive tenders from £50,000 to
£60,000
iv) Ideally At least 4 written competitive tenders from £60,001 to
£200,000
a)
i) Budget Holder
ii) Budget Holder up to £15k, Asst Director or equivalent up to £50k
iii) Director of Service or equivalent up to £60k. Use Procurement Manager to tender and procure. All procurement must be authorised by an appropriate CCG Committee or assigned group prior to advertisement.
iv) Director of Service or equivalent up to £100k. Chief Officer and Chief Financial Officer up to £200k. Use Procurement Manager and note OJEU limits for non clinical services. All procurement must be authorised by an appropriate CCG Committee or assigned group prior to advertisement.

82
REF
DELEGATED MATTERS
AUTHORITY DELEGATED TO
v) At least 6 written competitive tenders over £200,000
Following authorisation by an appropriate CCG Committee or assigned group:
b) Issuing of tender
c) Receiving of tender
d) Opening & recording of tender
e) Waiving of Quotations & Tenders subject to SFIs. All to be reported to the Audit Committee (integrated Assurance Committee)
f) Register of tenders received
g) Post tender negotiations - formal record to be kept
h) Approving expenditure in excess of tender price
v) Governing Body Chair and Chief Officer and Chief Financial Officer up to £250k. Over £250k reserved to Governing Body. Use Procurement Manager and note OJEU limits for non clinical services
b) Head of Procurement
c) Head of procurement
d) Two Senior Managers not related to the tender, finance staff involved in costing the tender are not precluded, Directors are also not precluded. If estimated over £100k one must be a Governing Body member
e) Chief Officer and Chief Financial Officer then reported to Audit I Integrated Assurance Committee
f) Chief Officer via Head of Procurement
g) Director or equivalent and Chief Financial Officer
h) Chief Officer and Chief Financial Officer
32 Research Projects

83
REF
DELEGATED MATTERS
AUTHORITY DELEGATED TO
Authorisation of Research Projects
Governing Body in conjunction with Director of Governance and Quality
33 Register of Interests
The keeping of a Declaration of Interests Register
Chief Officer via the Corporate Office Manager
34 Sealing of Documents
2 of the following are required to seal documents:
Chief Officer/Chief Financial Officer/Director of Commissioning/Director of Governance via the Corporate Office Manager
35 Sponsorship
Authorisation of Sponsorship deals
Chief Officer and Governing Body

84
APPLICATION FOR AUTHORISATION
FINANCIAL MANAGEMENT
ARRANGEMENTS APPENDIX 4
PRIME FINANCIAL POLICIES
ENCLOSURE: G (xi) – App1

85
APPENDIX 4
PRIME FINANCIAL POLICIES

86
PRIME FINANCIAL POLICIES
1. INTRODUCTION 1.1. General
1.1.1. These prime financial policies and supporting detailed financial policies shall have effect as if incorporated into the group’s constitution.
1.1.2. The prime financial policies are part of the group’s control environment for managing the organisation’s financial affairs. They contribute to good corporate governance, internal control and managing risks. They enable sound administration, lessen the risk of irregularities and support commissioning and delivery of effective, efficient and economical services. They also help the Accountable Officer and Chief Financial Officer to effectively perform their responsibilities. They should be used in conjunction with the scheme of reservation and delegation adopted by the CCG, at Appendix D. These will be agreed by the Audit and Integrated Assurance Committee and approved by the governing body.
1.1.3. In support of these prime financial policies, the group has prepared more detailed policies, approved by the Accountable Officer and Chief Financial Officer, known as detailed financial policies. The group refers to these prime and detailed financial policies together as the clinical commissioning group’s financial policies.
1.1.4. These prime financial policies identify the financial responsibilities which apply to everyone working for the group and its constituent organisations. They do not provide detailed procedural advice and should be read in conjunction with the detailed financial policies. The Chief Financial Officer is responsible for approving all detailed financial policies. A list of the group’s detailed financial policies will be published and maintained on the group’s website at www.bexley.nhs.uk. They will also be available upon request for inspection at the CCG’s head office.
1.1.5. Should any difficulties arise regarding the interpretation or application of any of the prime financial policies then the advice of the Chief Financial Officer must be sought before acting. The user of these prime financial policies should also be familiar with and comply with the provisions of the CCG’s constitution, Standing Orders and Scheme of Reservation and Delegation.
1.1.6. Failure to comply with prime financial policies and standing orders can in certain circumstances be regarded as a disciplinary matter that could result in dismissal.

87
1.2. Overriding Prime Financial Policies - If for any reason these prime financial policies are not complied with, full details of the non-compliance and any justification for non-compliance and the circumstances around the non-compliance shall be reported to the next formal meeting of the governing body’s Audit and Integrated Assurance Committee for referring action or ratification. All of the CCG’s members and employees have a duty to disclose any non-compliance with these prime financial policies to the Chief Financial Officer as soon as possible.
1.3. Responsibilities and delegation
1.3.1. The roles and responsibilities of the CCG’s members, employees, members of the governing body, its Committees and Sub-Committees and the committees and sub committees of its governing body and persons working on behalf of the group are set out in the main body of this constitution and the group’s Scheme of Reservation and Delegation.
1.3.2. The financial decisions delegated by members of the group are set out in the group’s scheme of reservation and delegation (see Appendix D).
1.4. Contractors and their employees
1.4.1. Any contractor or employee of a contractor who is empowered by the CCG to commit the CCG to expenditure or who is authorised to obtain income shall be covered by these instructions. It is the responsibility of the Accountable Officer to ensure that such persons are made aware of this.
1.5. Amendment of Prime Financial Policies
1.5.1. To ensure that these prime financial policies remain up-to-date and relevant, the Chief Financial Officer will review them at least annually. Following consultation with the Accountable Officer and scrutiny by the governing body’s Audit and Integrated Assurance Committee, the Chief Financial Officer will recommend amendments, as fitting, to the Governing body for approval. As these prime financial policies are an integral part of the group’s constitution, any amendment will not come into force until the group applies to the NHS Commissioning Board and that application is granted.

88
2. INTERNAL CONTROL
2.1. POLICY 2.1.1. the CCG will put in place a suitable control environment and effective
internal controls that provide reasonable assurance of effective and efficient operations, financial stewardship, probity and compliance with laws and policies
2.1.2. The governing body will set up an Audit and Integrated Assurance Committee with terms of reference agreed by the governing body (see paragraph 6.6.4(1) of the group’s constitution.
2.1.3. The Accountable Officer has overall responsibility for the group’s systems of internal control.
2.1.4. The Chief Financial Officer will ensure that:
2.1.4.1. financial policies are considered for review and update annually;
2.1.4.2. a system is in place for proper checking and reporting of all breaches of financial policies; and
2.1.4.3. a proper procedure is in place for regular checking of the adequacy and effectiveness of the control environment.
3. AUDIT
3.1. POLICY 3.1.1. the CCG will keep an effective and independent internal audit function
and fully comply with the requirements of external audit and other statutory reviews
3.1.2. In accordance with the governing body’s Audit and Integrated Assurance Committee terms of reference, the Head of Internal Audit and the Audit Commission appointed external auditor will have direct and unrestricted access to Audit and Integrated Assurance Committee members and the Chair of the governing body, Accountable Officer and Chief Financial Officer for any significant issues arising from audit work that management cannot resolve, and for all cases of fraud or serious irregularity.
3.1.3. The Head of Internal Audit and the external auditor will have access to the Audit and Integrated Assurance Committee and the Accountable
89
Officer to review audit issues as appropriate. All Audit and Integrated Assurance Committee members, the Chair of the governing body and the Accountable Officer will have direct and unrestricted access to the Head of Internal Audit and external auditors.
3.1.4. The Chief Financial Officer will ensure that:
3.1.4.1. the CCG has a professional and technically competent Internal Audit function; and
3.1.4.2. the Audit and Integrated Assurance Committee approves any changes to the provision or delivery of assurance services to the CCG.
4. FRAUD AND CORRUPTION
4.1. POLICY 4.1.1. the CCG requires all staff to always act honestly and with integrity to
safeguard the public resources they are responsible for. The CCG will not tolerate any fraud perpetrated against it and will actively chase any loss suffered
4.1.2. The governing body’s Audit and Integrated Assurance Committee will satisfy itself that the group has adequate arrangements in place for countering fraud and shall review the outcomes of counter fraud work. It shall also approve the counter fraud work programme.
4.1.3. The governing body’s Audit and Integrated Assurance Committee will ensure that the group has arrangements in place to work effectively with NHS Protect.
5. EXPENDITURE CONTROL
5.1.1. The CCG is required by statutory provisions to ensure that its expenditure does not exceed the aggregate of allotments from the NHS Commissioning Board and any other sums it has received and is legally allowed to spend.
5.1.2. The Chief Officer has overall executive responsibility for ensuring that the group complies with certain of its statutory obligations, including its financial and accounting obligations, and that it exercises its functions

90
effectively, efficiently and economically and in a way which provides good value for money.
5.1.3. The Chief Financial Officer will:
5.1.3.1. provide reports in the form required by the NHS Commissioning Board;
5.1.3.2. ensure money drawn from the NHS Commissioning Board is required for approved expenditure only is drawn down only at the time of need and follows best practice;
5.1.3.3. be responsible for ensuring that an adequate system of monitoring financial performance is in place to enable the group to fulfil its statutory responsibility not to exceed its expenditure limits, as set by direction of the NHS Commissioning Board.
6. ALLOTMENTS
6.1.1. The CCG’s Chief Financial Officer will:
6.1.1.1. periodically review the basis and assumptions used by the NHS Commissioning Board for distributing allotments and ensure that these are reasonable and realistic and secure the group’s entitlement to funds;
6.1.1.2. prior to the start of each financial year submit to the CCG governing body for approval a report showing the total allocations received and their proposed distribution including any sums to be held in reserve; and
6.1.1.3. regularly update the governing body on significant changes to the initial allocation and the uses of such funds.
7. COMMISSIONING STRATEGY, BUDGETS, BUDGETARY CONTROL AND MONITORING
7.1. POLICY 7.1.1. the CCG will produce and publish an annual commissioning plan that
explains how it proposes to discharge its financial duties. The CCG will

91
support this with comprehensive medium term financial plans and annual budgets
7.1.2. The Chief Officer will compile and submit to the governing body a commissioning strategy which takes into account financial targets and forecast limits of available resources.
7.1.3. Prior to the start of the financial year the Chief Financial Officer will, on behalf of the Accountable Officer, prepare and submit budgets for approval by the governing body.
7.1.4. The Chief Financial Officer shall monitor financial performance against budget and plan, periodically review them, and report to the governing body. This report should include explanations for variances over 5%. These variances must be based on any significant departures from agreed financial plans or budgets.
7.1.5. The Chief Officer is responsible for ensuring that information relating to the CCG’s accounts or to its income or expenditure, or its use of resources is provided to the NHS Commissioning Board as requested.
7.1.6. The governing body will approve consultation arrangements for the group’s commissioning plan.
8. ANNUAL ACCOUNTS AND REPORTS
8.1. POLICY 8.1.1. the CCG will produce and submit to the NHS Commissioning Board
accounts and reports in accordance with all statutory obligations, relevant accounting standards and accounting best practice in the form and content and at the time required by the NHS Commissioning Board
8.1.2. The Chief Financial Officer will ensure the CCG:
8.1.2.1. prepares a timetable for producing the annual report and accounts and agrees it with external auditors and the Audit and Integrated Assurance Committee;
8.1.2.2. prepares the accounts according to the timetable approved by the Audit and Integrated Assurance Committee;

92
8.1.2.3. complies with statutory requirements and relevant directions for the publication of the annual report;
8.1.2.4. considers the external auditor’s management letter and fully address all issues within agreed timescales; and
8.1.2.5. publishes the external auditor’s management letter on the group’s website at www.bexley.nhs.uk. It will also be available upon request for inspection at the CCG’s head office.
9. INFORMATION TECHNOLOGY
9.1. POLICY 9.1.1. the CCG will ensure the accuracy and security of the group’s
computerised financial data
9.1.2. The Chief Financial Officer is responsible for the accuracy and security of the group’s computerised financial data and shall:
9.1.3. devise and implement any necessary procedures to ensure adequate (reasonable) protection of the group's data, programs and computer hardware from accidental or intentional disclosure to unauthorised persons, deletion or modification, theft or damage, having due regard for the Data Protection Act 1998;
9.1.4. ensure that adequate (reasonable) controls exist over data entry, processing, storage, transmission and output to ensure security, privacy, accuracy, completeness, and timeliness of the data, as well as the efficient and effective operation of the system;
9.1.5. ensure that adequate controls exist such that the computer operation is separated from development, maintenance and amendment;
9.1.6. ensure that an adequate management (audit) trail exists through the computerised system and that such computer audit reviews as the Chief Financial Officer may consider necessary are being carried out.
9.1.7. In addition the Chief Financial Officer shall ensure that new financial systems and amendments to current financial systems are developed in a controlled manner and thoroughly tested prior to implementation.

93
Where this is undertaken by another organisation, assurances of adequacy must be obtained from them prior to implementation.
10. ACCOUNTING SYSTEMS
10.1. POLICY 10.1.1. the CCG will run an accounting system that creates
management and financial accounts
10.1.2. The Chief Financial Officer will ensure:
10.1.2.1. the CCG has suitable financial and other software to enable it to comply with these policies and any consolidation requirements of the NHS Commissioning Board;
10.1.2.2. that contracts for computer services for financial applications with another health organisation or any other agency shall clearly define the responsibility of all parties for the security, privacy, accuracy, completeness, and timeliness of data during processing, transmission and storage. The contract should also ensure rights of access for audit purposes.
10.1.3. Where another health organisation or any other agency provides a computer service for financial applications, the Chief Financial Officer shall periodically seek assurances that adequate controls are in operation.
11. BANK ACCOUNTS
11.1. POLICY 11.1.1. the CCG will keep enough liquidity to meet its current
commitments
11.1.2. The Chief Financial Officer will: 11.1.2.1. review the banking arrangements of the CCG at regular intervals
to ensure they are in accordance with Secretary of State directions, best practice and represent best value for money;
11.1.2.2. manage the CCG's banking arrangements and advise the CCG on the provision of banking services and operation of accounts;
94
11.1.2.3. prepare detailed instructions on the operation of bank accounts.
11.1.3. The Chief Officer shall approve the banking arrangements.
12. INCOME, FEES AND CHARGES AND SECURITY OF CASH, CHEQUES AND OTHER NEGOTIABLE INSTRUMENTS
12.1. POLICY 12.1.1. the CCG will:
12.1.1.1. operate a sound system for prompt recording, invoicing and collection of all monies due;
12.1.1.2. seek to maximise its potential to raise additional income only to the extent that it does not interfere with the performance of the group or its functions
12.1.1.3. ensure its power to make grants and loans is used to discharge its functions effectively
12.1.2. The Chief Financial Officer is responsible for: 12.1.2.1. designing, maintaining and ensuring compliance with systems
for the proper recording, invoicing, and collection and coding of all monies due;
12.1.2.2. establishing and maintaining systems and procedures for the secure handling of cash and other negotiable instruments;
12.1.2.3. approving and regularly reviewing the level of all fees and charges other than those determined by the NHS Commissioning Board or by statute. Independent professional advice on matters of valuation shall be taken as necessary;
12.1.2.4. for developing effective arrangements for making grants or loans.
13. TENDERING AND CONTRACTING PROCEDURE
13.1. POLICY 13.1.1. the CCG:
13.1.1.1. will ensure proper competition that is legally compliant within all purchasing to ensure we incur only budgeted, approved and necessary spending
13.1.1.2. will seek value for money for all goods and services 13.1.1.3. shall ensure that competitive tenders are invited for:
13.1.1.3.1. the supply of goods, materials and manufactured articles;

95
13.1.1.3.2. the tendering of services including all forms of management consultancy services (other than specialised services sought from or provided by the Department of Health); and
13.1.1.4. for the design, construction and maintenance of building and engineering works (including construction and maintenance of grounds and gardens) for disposals
13.1.2. The Public Contracts Regulations 2006 which transpose
European Directives place legal requirement and procedures for awarding contracts above a certain threshold amount. The Department of Health has provided guidance on how these Regulations may be interpreted but this guidance is not binding on CCGs, ultimately it is for CCGs to ensure that they comply with applicable law.
13.1.3. The CCG shall ensure that the firms / individuals invited to tender (and where appropriate, quote) are among those on approved lists or where necessary a framework agreement. Where in the opinion of the Chief Financial Officer it is desirable to seek tenders from firms not on the approved lists, the reason shall be recorded in writing to the Accountable Officer or the CCG’s Audit and Integrated Assurance Committee.
13.1.4. The governing body may only negotiate contracts on behalf of the CCG, and the CCG enter into contracts, within the statutory framework set up by the 2006 Act, as amended by the 2012 Act. Such contracts shall comply with:
13.1.4.1. the CCG’s Standing Orders;
13.1.4.2. the Public Contracts Regulation 2006, any successor legislation and any other applicable law; and
13.1.5. take into account as appropriate any applicable NHS Commissioning Board or the Independent Regulator of NHS Foundation Trusts (Monitor) guidance that does not conflict with (b) above.
13.1.6. In all contracts entered into, the CCG shall endeavour to obtain best value for money. The Accountable Officer shall nominate an individual who shall oversee and manage each contract on behalf of the CCG.

96
13.1.7. The CCG, governing body, and appointed representatives, will work in collaboration with other CCG’s, the National Commissioning Board and Local Authority to commission and contract for services, with joint providers, where it would be beneficial to the local health economy and promote economy, efficiency and effectiveness. Examples of this would be specialist services commissioned by the National and Specialist Commissioning Boards. Where joint arrangements are in place, the CCG will take joint responsibility for commissioning and contracts with partners.
14. COMMISSIONING
14.1. POLICY 14.1.1. working in partnership with relevant national and local
stakeholders, the CCG will commission certain health services to meet the reasonable requirements of the persons for whom it has responsibility
14.1.2. The CCG will coordinate its work with the NHS Commissioning Board, local NHS Trusts, other Clinical Commissioning Groups, other local providers of services, local authority, including through Health & Wellbeing Boards, users, carers and the voluntary sector and others as appropriate to develop robust commissioning plans.
14.1.3. The Chief Officer will establish arrangements to ensure that regular reports are provided to the governing body detailing actual and forecast expenditure and activity for each contract.
14.1.4. Where the CCG makes arrangements for the provision of services by non-NHS providers, it is the Accountable Officer who is responsible for ensuring that the agreements put in place have due regard to the quality and cost-effectiveness of services provided. Before making any agreement with non-NHS providers, the CCG should explore fully the scope to make maximum cost-effective use of NHS facilities.
14.1.5. The Chief Financial Officer will maintain a system of financial monitoring to ensure the effective accounting of expenditure under contracts. This should provide a suitable audit trail for all payments made under the contracts whilst maintaining patient confidentiality.
15. RISK MANAGEMENT AND INSURANCE

97
15.1. POLICY 15.1.1. the CCG will put arrangements in place for evaluation and
management of its risks
15.1.2. The Chief Officer will ensure that appropriate risk management and Assurance framework processes are in place. Risk Management policies and the assurance framework processes will be evaluated by the governing body’s Audit and Integrated Assurance Committee. A local risk management committee will also be in place to support this process.
16. NON-PAY EXPENDITURE
16.1. POLICY 16.1.1. the CCG will seek to obtain the best value for money goods and
services received
16.1.2. The Chief Financial Officer will approve the level of non-pay expenditure on an annual basis and the Chief Officer will determine the level of delegation to budget managers.
16.1.3. The Chief Officer shall set out procedures on the seeking of professional advice regarding the supply of goods and services.
16.1.4. The Chief Financial Officer will:
16.1.4.1. advise the Chief Officer on the setting of thresholds above which quotations (competitive or otherwise) or formal tenders must be obtained; and, once approved, the thresholds should be incorporated in the CCG’s scheme of reservation and delegation;
16.1.4.2. be responsible for the prompt payment of all properly authorised accounts and claims;
16.1.4.3. be responsible for designing and maintaining a system of verification, recording and payment of all amounts payable.
17. CAPITAL INVESTMENT, NON-CURRENT ASSET REGISTERS AND SECURITY OF ASSETS
17.1. POLICY 17.1.1. the CCG will put arrangements in place to manage capital
investment, maintain an asset register recording non-current assets and put in place policies to secure the safe storage of the CCG’s non-current assets
98
17.1.2. The Chief Officer will: 17.1.2.1. ensure that there is an adequate appraisal and approval
processes in place for determining capital expenditure priorities and the effect of each proposal upon plans;
17.1.2.2. be responsible for the management of all stages of capital schemes and for ensuring that schemes are delivered on time and to cost;
17.1.2.3. shall ensure that the capital investment is not undertaken without confirmation of purchaser(s) support and the availability of resources to finance all revenue consequences, including capital charges;
17.1.2.4. be responsible for the maintenance of registers of assets, taking account of the advice of the Chief Financial Officer concerning the form of any register and the method of updating, and arranging for a physical check of assets against the asset register to be conducted once a year.
18. RETENTION OF RECORDS
18.1. POLICY 18.1.1. the CCG will put arrangements in place to retain all records in
accordance with NHS Code of Practice Records Management 2006 and other relevant notified guidance
18.2. The Chief Officer shall: 18.2.1.1. be responsible for maintaining all records required to be retained
in accordance with NHS Code of Practice Records Management 2006 and other relevant notified guidance;
18.2.1.2. ensure that arrangements are in place for effective responses to Freedom of Information requests;
18.2.1.3. publish and maintain a Freedom of Information Publication Scheme.

99
APPLICATION FOR AUTHORISATION
FINANCIAL MANAGEMENT ARRANGEMENTS
APPENDIX 5 AUDIT & INTEGRATED ASSURANCE COMMITTEE TERMS OF REFERENCE
ENCLOSURE: G (xi) – App1

100
APPENDIX 5
AUDIT & INTEGRATED ASSURANCE COMMITTEE TERMS OF
REFERENCE

101
NHS Bexley Clinical Commissioning Group
Governing Body Audit & Integrated Assurance
Committee
Terms of Reference Constitution
The governing body of NHS Bexley CCG has resolved to establish a committee of the Governing Body to be known as the Audit and Integrated Assurance Committee (the Committee). The Committee is a non-executive committee of the Governing Body and has no executive powers, other than those specifically delegated in these terms of reference. These terms of reference can only be amended by the Governing Body.
Purpose
The overall purpose of the Committee is to provide assurance to the Governing Body on:
o the effectiveness of the CCG’s governance, corporate and clinical risk management, performance management, information governance and internal control systems;
o act as an integrated audit committee, taking an overview of finance, quality, risk, safeguarding, patient feedback and internal control to ensure that the governance system is joined up and not siloed;
o the integrity of the financial statements and accounts of the CCG and on the CCG’s Annual Report;
o the work of internal and external audit and any actions arising from their work;
o compliance by the CCG with legal and regulatory requirements. o The Audit and Integrated Assurance Committee will review the findings
of other assurance functions such as external regulators and scrutiny bodies and other committees and sub-committees of the Governing Body.

102
Duties
Governance, risk management, and Internal control
The Committee shall review the establishment and maintenance of an effective system of governance, risk management and internal control, across the whole of the organisation’s activities (both clinical and non-clinical) that supports the achievement of the organisation’s objectives.
In particular, the Committee will review the adequacy and effectiveness of:
o the assurance framework, risk management system, Statement of Internal Control together with an accompanying Head of Internal Audit Statement, external audit opinion or other appropriate independent assurances, prior to discussion by the Governing Body where possible
o the clinical governance system of the CCG, including early warning of
failures in quality and safety
o the information governance system, including requirements under the NHS Information Governance Toolkit
o the research governance system relating to any research activity the
CCG may be engaged with
o the CCGs system for managing conflict of interest, which will include the Committee Chair’s own designated role in the conflict of interest process
o the CCG’s Equality Delivery System (EDS) o the underlying assurance processes that indicate the degree of the
achievement of corporate objectives, the effectiveness of the management of principal risks and the appropriateness of the above disclosure statement
o the policies for ensuring compliance with relevant regulatory, legal and
code of conduct requirements and related reporting and self certification
o the policies and procedures for all work related to fraud and corruption as set out in Secretary of State Directions and as required by the NHS Counter Fraud and Security Management Service

103
o the Committee shall report issues in relation to audit, risk, quality and safety or internal control to the Governing Body on an exception basis in addition to an annual report focused on the effectiveness of the Committee in exercising these duties
o The committee shall take a view about the sufficiency of audit activity in
terms of those providers with which the CCG commissions, and in particular the internal audit and clinical audit of the main organisations form which the CCG commissions patient care services.
o In carrying out this work the Committee will primarily utilise the work of
Internal Audit, External Audit and other assurance functions, but will not be limited to these audit functions. It will also seek reports and assurances from officers as appropriate, concentrating on the overarching systems of governance, risk management and internal control, together with indicators of their effectiveness. This will be evidenced through the Committee’s use of an effective assurance framework to guide its work and that of the audit and assurance functions that report to it.
Internal Audit
o The Committee shall ensure that there is an effective internal audit function established by management that meets mandatory NHS Internal Audit Standards and provides appropriate independent assurance to the Committee, Accountable Officer and the Governing Body. This will be achieved by:
o consideration of the provision of the Internal Audit Service, the cost of
the audit and any questions of resignation and dismissal.
o review and approval of the internal audit strategy, operational plan and more detailed programme of work, ensuring that it is consistent with the audit needs of the organisation as identified in the Assurance Framework.
o review of the major findings of Internal Audit work, management’s response and ensure co-ordination between the Internal and External Auditors to optimise audit resources.
o ensuring that the internal audit function is adequately resourced and
has appropriate standing within the organisation.
o monitoring implementation of audit recommendations.

104
o an annual review of the effectiveness of internal audit.
External audit
The Committee shall review the work and findings of the External Auditors and consider the implications and management’s responses to their work. This will be achieved by:
• consideration of the appointment and performance of the External Auditor as far as the rules governing the appointment permit.
• discussion and agreement with the External Auditor, before the audit commences on the nature and scope of the audit as set out in the Annual Plan, and ensuring co-ordination, as appropriate with other external auditors in the local health economy.
• discussion with the External Auditors of the local evaluation of audit risks and assessment of the CCG and associated impact on the audit fee. review of all external audit reports and appropriateness of management responses agreement of the annual audit letter before it is submitted to the Governing Body agreement of additional work required outside the annual audit plan monitoring implementation of audit recommendations.
Other assurance functions
The Committee shall review the findings of other significant assurance functions, both internal and external to the organisation, and consider the implications for the governance of the organisation.
The Committee will need to include in their considerations reviews of provider functions that may be relevant to the CCG’s role of commissioning safe, effective, quality and cost-effective healthcare services. As such these will need to include but will not be limited to reviews by:
• Department of Health • Care Quality Commission • NHS Litigation Authority

105
• Other regulators and inspectors • Professional bodies with responsibility for performance of staff or
functions including Royal Colleges and accreditation bodies
In addition, the Committee will review the work of any other Committees or task and finish groups established by the Governing Body within the organisation whose work can provide relevant assurance to the Audit and Integrated Assurance Committee’s own scope of work.
Hosted arrangements
The Committee will review and provide assurance to the Governing Body in respect of any hosted arrangements or services, both any services hosted by the CCG and also those services hosted elsewhere but to which the CCG is a party.
Partnership and other inter-organisational arrangements
The Committee shall review and provide assurance to the Governing Body in respect of any formal partnership arrangements or other inter-organisational agreements where the CCG is a party.
Counter Fraud
The Committee shall satisfy itself that the organisation has adequate arrangements in place for countering fraud and shall review the outcomes of Counter Fraud work.
Management
The Committee shall request and review reports and positive assurances from directors and managers on the overall arrangements for governance, risk and internal control.

106
The Committee may also request specific reports from individual functions within the organisation (for example clinical audit) as they may be relevant to the overall arrangements.
Financial reporting
The Committee shall monitor the integrity of the financial systems of the CCG and systems of financial control.
The Committee shall review the Annual Report and Financial Statements before submission to the Governing Body, focusing particularly on:
• the wording in the Statement of Internal Control and other disclosures relevant to the Terms of Reference of the Committee.
• changes in and compliance with accounting policies and practices.
• unadjusted mis-statements in the financial statements.
• significant judgments in preparation of the financial statements.
• significant adjustments resulting from the audit.
The Committee should ensure that the systems for financial reporting to the Governing Body including those concerning budgetary control, are reviewed regularly to ensure completeness and accuracy of the information.
o The Committee shall review and propose changes to the standing orders and standing financial instructions as requested by the Governing Body
Authority/ Delegation
The Committee is authorised by the Governing Body to investigate any activity within its Terms of Reference and in line with the Committee’s prime purpose of providing assurance to the Governing Body.
The Committee is authorised by the Governing Body to obtain outside legal or other independent professional advice and to secure the attendance of outsiders with relevant experience and expertise if it considers this necessary.

107
Membership and attendance
The core membership of the committee will be as follows:
The GP Locality Lead on this committee should not have a place on any other committee of the Governing Body. At least once a year the Committee should meet privately with the internal and external auditors only if possible. The Committee chair may also ask the auditors if they would like a private conversation as an alternative. The Committee should agree and work to an annual programme that takes into account the need to contribute to the timely sign-off of statutory requirements such as the annual accounts.
The Chief Officer and other directors shall be invited to attend particularly when the Committee is discussing areas of risk or operation that are the responsibility of that director.
The Chief Officer shall be invited to attend, at least annually, to discuss with the Committee the process of assurance that supports the Statement of Internal Control.
Quorum
Quorum of the Committee shall be three members.
Clinical Members Non-Clinical Members
1 GP Locality Lead member of the Governing Body (Vice Chair)
Lay Member (Governance) (Committee Chair)
Governing Body Nurse Member • Lay member (PPI)
Governing Body Secondary Care Specialist

108
Decision Making
Where a vote is required to decide a matter each member may cast a single vote, in the event of a tie the Chair of the meeting may cast a second vote. A decision will be made on a simple majority
It may on occasion be necessary for EMC members to make decisions outside formal meetings. The Committee Chair or Vice Chair will decide whether this procedure should be used.
Procedure
The Committee Chair or Vice Chair will arrange for the notice of the business to be determined and any supporting paper, to be sent to members by email. The email will ask for a response to be sent to the Committee Chair or Vice Chair by a stated date. A decision made in this way will only be valid if the same minimum quorum, described in the above paragraph, express by email or signed written communication, by the stated date for response that they are in favour.
The Committee Chair or Vice Chair as appropriate will retain all correspondence pertaining to such a decision for audit purposes and report decisions so made to the next meeting for ratification.
Frequency
Meetings shall be held not less than four times a year and at such other times as the Chair of the Committee shall require. The external auditor or head of internal audit may request a meeting if they consider that one is necessary.
Reporting
The proceedings of each meeting of the Committee shall be reported to the next meeting of the Governing Body.
The minutes of the Committee meeting should be formally recorded by the Governing Body Secretary and submitted to the Governing Body. The Chair

109
shall draw to the attention of the Governing Body any issues that require disclosure to the full Governing Body or require executive action.
The Committee shall be supported administratively by the Corporate Office Manager whose duties in this respect will include:
• agreement of agenda with Chairman and attendees and collation of papers.
• taking the minutes and keeping a record of matters arising and issues to be carried forward.
• enabling the development and training of Committee members.
Review of Arrangements
The Committee shall undertake a self-assessment of its effectiveness on at least an annual basis. This may be facilitated by independent advisors if the Committee considers this appropriate or necessary.
These Terms of Reference shall be reviewed by the Governing Body on at least an annual basis.

110
APPLICATION FOR AUTHORISATION
FINANCIAL MANAGEMENT ARRANGEMENTS
APPENDIX 6
REMUNERATION COMMITTEE TERMS OF REFEFERENCE
ENCLOSURE: G (xi) – App1

111
APPENDIX 6
REMUNERATION COMMITTEE TERMS OF REFERENCE

112
NHS Bexley Clinical Commissioning Group
Governing Body Remuneration Committee
Terms of Reference Constitution
The Governing Body of NHS Bexley Clinical Commission Group hereby resolves to establish a committee of the Governing Body to be known as the Remuneration Committee (“the Committee”). The Committee is a non-executive committee of the Governing Body and has no executive powers other than those specifically delegated in these terms of reference.
Purpose
The overall purpose of the Committee is to:
• ensure that the process of appointing, and if necessary dismissing, the directors are robust, fit for purpose and have been followed
• oversee and coordinate, through delegation, any elections which may be part of the process of appointment to the governing body
• oversee the system for all director appointments and agree the parameters for the senior appointments process. The process of all senior executive appointments will be reported back to the Committee in order that the Committee can provide the governing body with assurance
• agree and review the CCG’s policies on the reward, performance, retention and pension matters for the directors
• support the board understand and apply Lord Nolan’s ‘Principles of Public Life’ and generally promote transparency and probity
Duties
The Committee shall:
o provide assurance to the Governing Body around the process for appointing and dismissing all directors of the governing body, including the Chair and Chief Officer

113
o agree, where there is scope, for recommendation to the Governing Body on the remuneration package, including performance related pay and other terms of service of the Chair, Chief Officer, GP members of the Governing Body, the appointed nursing, consultant and lay members of the Governing Body, including any scheme for performance related pay and any other benefits
o with the Chair and Chief Officer, agree, where there is scope, the
remuneration packages, including the scheme for performance related pay and other terms of service (including severance terms if applicable) of all other executive directors and senior employees
o where there is scope, to review and agree the grading and
remuneration package of any director post that falls vacant, prior to the vacancy being advertised
o to monitor the system to evaluate the performance of the Chief Officer,
the directors and other senior employees as appropriate
o as requested by the governing body, carry out any benchmarking enquiries or other studies to help establish the appropriate terms and conditions for members of the governing body
o ensure that at all times the Governing Body conducts its dealings
around appointment, remuneration and reward with due regard to probity, transparency, the stewardship of public funds and confidentiality due to all employees and officers of the CCG
o ensure that the appraisal and talent management processes within the
CCG are robust and fair
o ensure that access to training and development resources are appropriate and in line with business requirements
o support the board apply Lord Nolan’s ‘Principles of Public Life’
When setting any recommended pay and benefits packages, the guiding principle is that no individual should be involved in the setting of their own remuneration. For this reason, agreeing any pay and benefits packages of the non-executive and GP members without portfolio shall be undertaken by the independent members of the committee in camera. They shall base their recommendations on reasonable benchmark data, market rates and general fairness to both the individuals concerned and the CCG and its membership as a whole. The intention of this mechanism is to

114
preserve the standing of all remunerated members of the CCG from any suggestion of involvement with agreement around their own pay and benefits.
Authority / Delegation
The Committee is authorised by the governing body to investigate any activity within its Terms of Reference. The Committee is authorised by the Governing Body to obtain outside legal or other independent professional advice and to secure the attendance of outsiders with relevant experience and expertise if it considers this necessary.
Membership and attendance
Members of the Committee will be appointed by the CCG Governing Body, who shall identify which member of the Committee shall be the Committee Chair.
Core membership of the Committee will include
The Accountable Officer and any other member of the Governing Body may be I invited to attend as required.
The members of the Committee shall be as follows:
CCG HR Business Manager or equivalent will be responsible for supporting the Chair in the management of Remuneration Committee business and for drawing the Committee’s attention to best practice, national guidance and other relevant documents, as appropriate.
Clinical Members Non-Clinical Members
Chair Lay Member (Governance) (Committee Chair)
1 GP Locality Lead member of the Governing Body
Lay member (PPI)

115
Chief Financial Officer to advise on any matters that have significant financial implications.
Other parties may only attend at the request of the Committee and only to provide advice and information.
The Corporate Office manager shall be secretary to the Committee and shall attend to take minutes of the meeting and provide appropriate support and advice to the Chair and Committee members.
When GP remuneration is being discussed, the Chair and GP members will be replaced by the secondary care and nurse members, or lay members from other South East London CCGs. Staff will not be present for the discussion of matters relating to their own remuneration, performance or terms of service.
Quorum
Quorum shall be three members of the Committee, of which at least one must be one of the independent members.
Decision Making
Where a vote is required to decide a matter each member may cast a single vote, in the event of a tie the Chair of the meeting may cast a second vote. A decision will be made on a simple majority
It may on occasion be necessary for EMC members to make decisions outside formal meetings. The Committee Chair or Vice Chair will decide whether this procedure should be used.
Procedure
The Committee Chair or Vice Chair will arrange for the notice of the business to be determined and any supporting paper, to be sent to members by email. The email will ask for a response to be sent to the Committee Chair or Vice Chair by a stated date. A decision made in this way will only be valid if the same minimum quorum, described in the above paragraph, express by email

116
or signed written communication, by the stated date for response that they are in favour.
The Committee Chair or Vice Chair as appropriate will retain all correspondence pertaining to such a decision for audit purposes and report decisions so made to the next meeting for ratification.
Frequency
Meetings shall be held not less than twice a year and it is at the Governing Body’s discretion as to when they may be called.
Reporting
The proceedings of each meeting of the Committee shall be reported to the next meeting of the governing body unless the business relates to specific individuals. The Chair shall provide a remuneration report for publication with the Annual Report.
The minutes of the Committee meeting should be formally recorded by the Accountable Officer and submitted to the Governing Body. The Chair shall draw to the attention of the governing body any issues that require disclosure to the full Governing Body or require executive action.
The Committee shall be supported administratively by the Accountable Officer whose duties in this respect will include:
• agreement of agenda with Chairman and attendees and collation of papers.
• taking the minutes and keeping a record of matters arising and issues to be carried forward.
• enabling the development and training of Committee members.
Review of Arrangements
The Committee shall undertake a self-assessment of its effectiveness on at least an annual basis. This may be facilitated by independent advisors if the Committee considers this appropriate or necessary.

117
These Terms of Reference shall be reviewed by the Governing Body on at least an annual basis.

118
APPLICATION FOR AUTHORISATION
FINANCIAL MANAGEMENT ARRANGEMENTS
APPENDIX 7
BUDGET SETTING POLICY
ENCLOSURE: G (xi) – App1

119
Appendix 7 Budget Setting Policy
NHS Bexley Clinical Commissioning Group

120
Contents
• Introduction
• Budget Setting Principles
• Allocation/Resources
• Expenditure
• Introduction
121
Introduction
• Budgets are produced annually • Based on the latest Operating Framework, national
planning assumptions and Medium Term Financial Strategy Document
• Covers all revenue operating budgets • Further guidance included in Detailed Financial
Procedures
122
• Budgets to be as realistic as possible • Constructed within CCG Allocation limits • Expenditure on CCG running costs within target set • Reflects required surplus and contingency • Includes expected pay and price changes • National and local investment priorities recognised where affordable • Budget reduction for productivity and efficiency measures • In year changes subject to appropriate authorisation processes • Budget managers to be engaged to ensure understanding of allocated
budgets which secures accountability and facilitates strong financial management
Principles

123
CCG Allocation
• CCG Allocation for 2013/14 estimated to be approx. 80% of PCT budget based upon the national baseline exercise. This includes a share of PCT 12/13 returned surplus
• Need to set aside from this allocation the expected surplus and contingency reserves:
– Surplus target 1% – Contingency 0.5% – Possible additional 0.5% risk share contingency – 2% Non Recurrent reserve
• Includes Running cost allowance • Subject to actual allocation being advised in the
winter of 2012 & 2013/14 Operating Framework

124
Expenditure Plans
• Each year budgets are set using a zero based basis where possible • Reflects full year effect of savings or investments • Review of year end outturn (over or underperformances) • CCG Running costs reflected appropriately • Inflation applied as appropriate (current 2013/14 assumptions
shown in Appendix A) • Demographic & non-demographic increase modelled as
appropriate (see also Appendix A) • Other cost pressures – funding set aside to cover an estimate of
unavoidable pressures where possible • New Investments
– National priorities as per the Operating Framework (13/14 expected priorities listed at Appendix B) – business cases agreed through Finance working group & Executive Management Committee
– Local priorities – as agreed through local management process • Subject to revised planning assumptions from TSA.

125
QIPP Plans
• Budgets adjusted to reflect required savings to achieve surplus and live within CCG Allocation
• QIPP planning through bottom up process • PMO processes incorporating Gateway reviews
embedded within organisation • Reflects opportunities identified through
benchmarking (national and local) • 2013/14 planned QIPP target £3.078m (but
dependant on revised TSA assumptions)

126
2013/14 Assumptions – Appendix A Client Other
BudgetsGroups and
Reserves
Recurrent uplift 2.62%
Demographic Growth 0.43% 0.43% 0.43% 0.00% 0.00% 0.40%
Non-demographic growth 1.55% 1.38% 0.67% 0.00% 0.00% 1.25%
Total population & incidence growth 1.98% 1.81% 1.10% 0.00% 0.00% 1.65%
Prescribing growth 5.00%
Tariff/ Inflation Uplift 2.50% 2.50% 1.50% 2.50% 2.50% 2.24%
Tariff efficiency assumption/ Price Efficiency applied -4.00% -4.00% 0.00% -2.50% -3.01%
Net Tariff inflation uplift -1.50% -1.50% 1.50% 2.50% 0.00% -0.77%
2013/14
Acute Primary Care
Corporate Budgets Total

127
2013/14 National Investments – Appendix B

128
APPLICATION FOR AUTHORISATION
FINANCIAL MANAGEMENT ARRANGEMENTS
APPENDIX 8
SAMPLE CCG FINANCIAL REPORT
ENCLOSURE: G (xi) – App1

129
APPENDIX 8
SAMPLE CCG FINANCIAL REPORT

130
BEXLEY CLINICAL CABINET MEETING 25 SEPTEMBER 2012
Month 4 2012/13 Finance Report
For discussion and information
Executive Summary
The Cluster now prepares a joint Finance report for all six South East London PCTs for the Joint Board. The monthly Bexley position is discussed and agreed between the cluster and the BSU before finalisation. For 2012/13, the BSU is writing a report for the local needs of Bexley Clinical Commissioning Group (CCG). However, this is primarily informed by information provided by Cluster colleagues. Close liaison and communication is therefore vital to ensure robust reporting at a local level. This report provides details for the Clinical Cabinet in respect of the financial position as reported at month 4 2012/13. The report will be developed as the year progresses. For month 4, details of the capital allocation are included; as well as an indication of the split between the CCG responsibilities and those being transferred elsewhere from 1st April 2013.
RECOMMENDATIONS
• DISCUSS & NOTE the Month 4 (July) financial position and forecast outturn detailed in this report;
• NOTE the indicative split of resources between the CCG’s responsibilities and other areas from 1st April 2013.
• DISCUSS & NOTE the key risks and cost pressures identified to achieving the surplus control total in 2012/13 and the management actions being taken to address and mitigate these risks;
• NOTE the revenue and capital resources available to the Care Trust;
• NOTE the month 4 forecast performance against the key national finance targets.

131
Consideration by Other Committees/Groups
Financial updates are also provided at the Programme Management Office (PMO) meetings and Business and Recovery Group meetings.
Organisational implications
Financial The Care Trust has planned for a surplus of 1% (£3,508k) in 2012/13.
To achieve this position, identified QIPP has to be delivered and SLAs need to be delivered within agreed SLA values or with minimum over-performance. At month 4, Bexley Care Trust is forecasting achievement of this position with financial support and return of a proportion of the 2% non-recurrent deduction. The Care Trust / CCG has a plan to achieve a normalised breakeven / 1% surplus position over the 3 years 2012/13-2014/15. However, work with the Trust Special Administrator may revise the planning assumptions used.
Equality and Diversity n/a
Risk (governance and/or clinical)
The risks to breakeven / achieving the control total are outlined in the body of the report and in the organisation’s risk register.
Patient impact n/a
NHS constitution n/a
Which objective does this paper support? Insert Tick )
Improve choice and access to integrated health services for Bexley patients
Reduce the level of health inequalities across Bexley
Improve care for patients with long term conditions & increase the range of services offered within the community
Improving the health & wellbeing for people in Bexley

132
Maximising the opportunities of joint working (A Picture of Health, Joint Strategy Needs Assessment, Wellness agenda etc)
Using our resources in the most efficient & effective manner (organisational & financial)
Author
Theresa Osborne
Chief Financial Officer
Executive Sponsor
Theresa Osborne
Chief Financial Officer
Date 4th September 2012

133
Financial Performance Update as at month 4 (July) 2012/13 1. FINANCIAL KEY INDICATORS 2012/2013 Table 1 below sets out the statutory targets, and progress to date, on which the Care Trust will report to the Department of Health, at the year end, in its Annual Accounts and Annual report.
Table 1: Key Indicators 2012/13
Target Forecast Outturn
Var
% Var Indicator M4
Movement from
previous
Care Trust Statutory Targets:
Achieve Financial Balance – Revenue* £3,508k £3,508k £0k 0 Green =
Remain within Capital Resource Limit (not yet confirmed)
Green =
Remain within Cash Limit# £360,760k £360,760k £0k 0 Green =
Public Sector Payments Compliance – by value
95% 96.42% 1.42% Green
Public Sector Payments Compliance – by count
95% 82.76% (12.24)% Red
* The Care Trust’s statutory financial duty is breakeven and the Care Trust is still forecasting achievement of this at month 2. # Any predicted cash under-utilisation does not result in a breach of the Care trust’s cash limit.
QIPP Target Forecast
Outturn Var % Var Indicator
M3 Movement
from previous
Acute 2,662 1,652 (1,010) 38% Red
Primary Care 1,574 1,574 0 0 Green =
Client groups 2,096 2,074 (22) 1% Amber
Other 1,253 1,203 (50) 4% Red
Total 7,585 6,503 (1,082) 14% Red

134
2. HIGHLIGHTS
• Surplus of £1,150k reported at month 4 against a plan of £1,138k.
• The required 1% surplus of £3,508k has been set aside in reserves and it is currently forecast that this will be achieved in 2012/13. This assumes receipt of £4.8m financial support and return of £4.5m from 2% non-recurrent funding for the South London Healthcare NHS Trust (SLHT) cap and collar contract and Guy’s & St Thomas’ contract transitional costs.
• The financial outlook at this point in the year assumes full utilisation of available reserves and contingencies and delivery of the Quality, Innovation, Productivity & Prevention (QIPP) programme as currently forecast. Whilst overall the position is as expected at month 4 there are significant risks which are explored in the body of the report.
• £2,085k QIPP assessed as achieved at month 4 against a target of £2,527k. £6,503k forecast QIPP achievement against £7,585k plan.
• Acute over-performance of £1,249k reported against all acute contracts at month 4. £4,465k cluster assessed acute over-performance forecast outturn, a deterioration of £1.9m in the month.
• Indicative budgets included of CCG future responsibilities and those being transferred elsewhere.

135
3. BUDGETS
A summary of the 2012/13 budgets showing the approved opening budgets and any movements to 31st July are shown in table 2 below. The month 4 budgets equal the expected Revenue Resource Limit (RRL) shown further on in the report and is as anticipated at year end. The resources shown are net of miscellaneous income that the Care Trust receives for goods/services it provides to other organisations. The resource limit is the allocation that the Care Trust receives from the Department of Health, and this resource limit is the figure that the Care Trust’s net spend is measured against when reviewing its achievement of financial balance. There have been no major budget changes in the month. Table 2: 2012/13 Budget Summary
Directorate Cost Centre - Narrative QIPP / CIP 12/13 Starting Budget
April 2012 - Total
May 2012 - Total
June 2012 - Total
July Budget Changes
July 2012 - Total
TOTAL FOR 20 - BSU HEADQUARTERS 0 10,005,245 10,005,245 10,005,245 10,240,399 95,751 10,336,150TOTAL FOR 20 - FINANCE, BUSINESS & PERFORMANCE 0 3,954,235 3,954,235 3,954,235 3,907,616 -90,042 3,817,574TOTAL FOR 23 - COMMISSIONING, REDESIGN & GOVERNANCE 0 1,924,769 1,924,769 1,924,769 1,900,769 134,544 2,035,313TOTAL FOR 24 - JOINT COMMISSIONING 0 3,489,446 3,489,446 3,489,446 3,455,809 0 3,455,809TOTAL FOR 25 - PUBLIC HEALTH & HEALTH IMPROVEMENT 0 3,826,001 3,826,001 3,826,001 3,829,001 60,874 3,889,875TOTAL FOR 40 - ACUTE SLA 0 175,023,323 175,023,323 175,023,323 179,010,573 0 179,010,573TOTAL FOR 41 - MENTAL HEALTH 0 28,811,505 28,811,505 28,811,505 28,811,505 0 28,811,505TOTAL FOR 42 - SPECIALIST BLOCK 0 14,560,560 14,560,560 14,560,560 14,554,604 0 14,554,604TOTAL FOR 43 - EXCEPTIONAL TREATMENT 0 2,976,546 2,976,546 2,976,546 2,976,546 0 2,976,546TOTAL FOR 44 - LEARNING DISABILITY 0 1,645,090 1,645,090 1,645,090 1,645,090 0 1,645,090TOTAL FOR 45 - COMMUNITY 0 3,260,282 3,260,282 3,260,282 3,272,282 0 3,272,282TOTAL FOR 46 - CONTINUING CARE & NURSING HOMES 0 7,865,436 7,865,436 7,865,436 7,865,436 0 7,865,436TOTAL FOR 47 - NON-CONTRACT ACTIVITY 0 2,053,000 2,053,000 2,053,000 2,053,000 0 2,053,000TOTAL FOR 48 - PROVIDER SLA 0 20,688,716 20,688,716 20,688,716 20,688,716 0 20,688,716TOTAL FOR 49 - PRESCRIBING 0 31,802,217 31,802,217 31,802,217 31,802,217 0 31,802,217TOTAL FOR 70 - PRIMARY CARE (CLOCKTOWER) 0 8,703,757 8,703,757 8,703,757 8,703,757 0 8,703,757TOTAL FOR 72 - PRIMARY CARE (FROGNAL) 0 7,570,502 7,570,502 7,570,502 7,570,502 0 7,570,502TOTAL FOR 74 - PRIMARY CARE (NORTH BEXLEY) 0 9,451,254 9,451,254 9,451,254 9,451,254 0 9,451,254TOTAL FOR 75 - LBB LOCALITY 0 2,354,060 2,354,060 2,354,060 2,354,060 0 2,354,060TOTAL FOR 76 - RESERVES 0 3,338,275 3,338,275 3,338,275 3,338,275 0 3,338,275TOTAL FOR 80 - THIRD SECTOR 0 470,523 470,523 470,523 470,523 0 470,523TOTAL FOR 81 - DENTAL 0 8,367,123 8,367,123 8,367,123 8,367,123 0 8,367,123TOTAL FOR 84 - SERVICE REDESIGN 0 3,942,126 3,942,126 3,942,126 3,795,184 -103,127 3,692,057TOTAL FOR 85 - PHARMACY 0 5,999,587 5,999,587 5,999,587 5,999,587 0 5,999,587TOTAL FOR 86 - OPTOMETRY 0 1,920,000 1,920,000 1,920,000 1,920,000 0 1,920,000TOTAL FOR 90 - RESOURCES 0 -364,003,578 -364,003,578 -364,003,578 -367,983,828 -98,000 -368,081,828

136
4. REVENUE RESOURCE LIMIT (RRL)
The RRL is the allocation that the Care Trust receives from the Department of Health, and this is the figure that the Care Trust’s net spend is measured against when reviewing its achievement of financial balance.
For 2012/13, the anticipated RRL has been included in budgets, as opposed to the actual with anticipated budgets set aside in committed resources. This is in line with other PCTs across South East London.
The RRL confirmed for month 4 and the anticipated adjustments are shown in table 3 below:
Table 3: Month 4 (July) and final expected Revenue Resource Limit (RRL)
Cost centre Month Description BudgetW65631 Initial DEPARTMENT OF HEALTH - PCT04 AWP (340,680,712)W65631 Initial 12/13 growth (9,539,000)W65631 Initial Additional 12/13 reablement (601,000)W65631 Initial Social Care funding (2,306,000)W65631 Initial Primary dental service (8,152,000)W65631 Initial General Ophthalmic service (1,765,000)W65631 Initial Pharmaceutical service (2,824,000)
Initial RRL (365,867,712)W65631 Mth 2 Drugs funding incl DIP &YP (1,028,866)W65631 Mth 2 Cancer drugs fund 561,000W65631 Mth 2 School fruit scheme 168,000W65631 Mth 2 HPV funding through RRL (48,000)
Mth 2 HPV funding through RRL correction 7,000Month 2 RRL (366,208,578)
W65631 Mth 3 PCT recharges 103,000W65631 Mth 3 PCT levies 226,000
Mth 3 Balance of Londonwide activities (39,000)Mth 3 NHS diagnostics refund 11/12 correction (50,000)
W65631 Mth 3 2% resource transfer to SHA 7,017,000Mth 3 2% resource transfer to SHA correction (1,000)Mth 3 Cancer drugs fund adjustment 11/12 correction (25,000)
Month 3 RRL (358,977,578)W65631 Mth4 Point of arrest diversion (58,000)
Month 4 RRL (359,035,578)Expected Adjustment for Cost of Capital (98,000)Expected Balance of Londonwide activities 39,000
W65631 Expected NCG transfer 2,301,000W65631 Expected Mental capacity act (43,000)W65631 Expected Dementia Memory service (38,000)W65631 Expected Dental VTS funding (240,000)W65631 Expected 2011/12 carry forward (2,245,000)W65631 Expected Overseas visitors deduction 212,000W65631 Expected Marginal rate deduction 259,000W65631 Expected NHSE SEL 12/13 loan (4,760,000)
Expected 2% N/R return for SLHT Contract (3,987,250)W65631 Expected 2% N/R return for GSTT transitional costs (522,000)
Expected RRL (368,157,828)Mth 4 adj NHS diagnostics refund 11/12 correction 50,000Mth 4 adj 2% resource transfer to SHA correction 1,000Mth 4 adj Cancer drugs fund adjustment 11/12 correction 25,000
Month 4 Ledger (368,081,828)

137
5. CAPITAL RESOURCE LIMIT (CRL)
The Care Trust has now received the expected £1,625k capital funding for 2012/13 in its CRL.
No Capital expenditure has been reported to date and this is likely to be due to concern that this would not be approved. It is likely that there will be a year-end underspend against the IT allocation. However, discussions with cluster capital colleagues have confirmed that this funding can be used across the cluster.
Table 4 shows details of the Capital allocation for 2012/13 and that proposed for 2013/14 and 2014/15. However, it is currently unknown whether or not CCGs will own fixed assets and therefore need capital from 1st April 2013.
Table 4: Month 4 (July) and final expected Capital Resource Limit (CRL)

138
6. 2012/13 MONTH 4 (JULY) FINANCIAL POSITION Table 5 summarises the financial position, at Directorate level, for the Care Trust at Month 4 (July).
At month 4, the year to date position shows a surplus of £1.150k, £12k above the planned figure of £1,138k. The position was reported to NHS London and the Department of Health in the month 4 FIMs key data return, submitted in line with prescribed deadlines. This key data return is attached at Appendix 1 for information. The BSU Managing Director approved the position and submission for month 4.
The financial position shows the 2012/13 forecast outturn as the expected 1% surplus of £3,508k. This position is constantly reviewed with the expectation that a minimum of breakeven will be met for 2012/13, in line with the Care Trust’s statutory financial breakeven duty.
There are currently some underspends within the corporate and exceptional treatments budgets which are offsetting the overspends in mental health. The overspends in acute and primary care are offset by contingency, reserves and non-recurrent benefit from the Balance Sheet.
The large underspend in BSU headquarters, year to date and forecast outturn, predominantly reflects the £3,508k 1% surplus, set aside and expected as part of financial planning; but also includes the reversal of 2011/12 accruals found not to be needed in the current year (non-recurrent benefit from the Balance Sheet).
The forecast outturn shown against continuing care relates to the expected costs in respect of retrospective reviews, as detailed in the risk schedule further on in the report. At the time of writing 30 cases have been received. This could increase up to the deadline for appeals of 30th September 2012. The appeals will be continually monitored and reviews assessed for liability. A final cost in this respect will not be known until later in the financial year.
The overspend on mental health is being investigated and all clients are being reviewed as part of the residential review being carried out jointly with Oxleas NHS Foundation Trust.
A large QIPP saving is planned within prescribing. At this time in the year this is forecast to be made. However, a specific prescribing reserve has been included within financial plans to mitigate against any under-performance or increased costs as a result of the introduction of new NICE approved drugs for anti coagulation. However, for month 4 this reserve has been played into the forecast position to achieve the required 1% surplus.
Locality primary care budgets are now amalgamated under Primary care – GP to correctly show total GP variances.

139
Table 5: Summary financial position by directorate
Annual Budget
Month 4 Budget
Month 4 Actual
Month 4 Variance YTD Budget YTD Actual YTD
Variance Directorate Code Directorate Description
£000's £000's £000's £000's £000's £000's £000's
YTD Variance
%
Forecast Outturn £000's
Forecast Variance
£000's
Forecast Variance
%
20 BSU Headquarters 10,336 838 94 -744 3,826 2,081 -1,745 -46 4,624 -5,712 -55 22 Finance, Business & Perf Directorate 3,818 296 169 -127 1,273 1,154 -119 -9 3,818 -100 -3 23 Comm, Redesign & Gov'nce Directorate 2,035 203 193 -10 678 623 -56 -8 2,035 0 0 24 Joint Commissioning Directorate 3,456 288 251 -37 1,152 1,158 6 1 3,406 -50 -1
25 Public Health & Health Improve Directorate 3,890 339 433 93 1,297 1,229 -68 -5 3,690 -200 -5
40 Acute SLAs 179,011 14,984 15,714 730 59,139 60,409 1,271 2 183,274 4263 2 41 Mental Health 28,812 2,401 2,488 87 9,604 9,941 337 4 29,328 517 2 42 Specialist Block 14,555 1,213 1,232 19 4,852 4,929 77 2 14,757 202 1 43 Exceptional Treatments 2,977 248 129 -119 992 721 -271 -27 2,977 0 0 44 Learning Disabilities 1,645 137 122 -15 548 570 21 4 1,670 25 2 45 Community 3,272 273 273 1 1,091 1,089 -2 0 3,272 0 0 46 Continuing Care & Nursing Homes 7,865 655 658 3 2,622 2,632 10 0 8,165 300 4 47 Non Contract Activity 2,053 171 219 48 684 857 173 25 2,053 0 0 48 Provider SLA 20,689 1,724 1,744 20 6,896 6,896 0 0 20,689 0 0 49 Local Primary Care 31,802 2,650 2,723 72 10,601 10,720 119 1 31,802 0 0 70 Primary Care - GP 25,726 2,144 2,261 117 8,575 8,913 338 4 26,311 585 2 75 LBB Locality 2,354 196 121 -75 785 630 -155 -20 2,354 0 0 76 Reserves 3,338 278 0 -278 1,113 0 -1,113 -100 0 -3338 -100 80 3rd sector & LBB joint budgets 471 39 52 13 157 158 1 1 471 0 0 81 Dental 8,367 697 697 0 2,789 2,789 0 0 8,367 0 0 84 Service Redesign / Community 3,692 282 308 26 1,231 1,270 39 3 3,692 0 0 85 Pharmacy 6,000 500 537 37 2,000 1,993 -7 0 6,000 0 0 86 Optometry 1,920 160 120 -40 640 632 -8 -1 1,920 0 0
90 Resources -368,082 -30,764 0 30,764 -122,162 0 0 0 -
368,082 0 0 99 Balance Sheet 0 0 -30,538 -30,538 0 -121,393 0 - 0 0 0
Total 0 -48 0 48 381 0 -1,150 -3,408 -3,508 -1

140
7. SUMMARY OF MAIN VARIANCES
• BSU Headquarters
The year to date position is £1,745k underspent. This includes the £1,169k phased 1% surplus, £167k phased prescribing reserve with the balance being the benefit relating to prior year’s unused accruals.
• Finance, Business & Performance
The year to date position shows an under-spend of £119k, compared to an £8k over-spend as at month 3. The large swing is primarily due to the large VAT receipt for BBG LIFT Co invoices, within estates, paid during 2011/12. This was not provided for in the 2011/12 accounts. Three months VAT remains outstanding and this should further improve the position.
• Community Redesign and Governance
Commissioning, Redesign and Governance is £56k underspent as at month 4. Significant under-spends in Medicines Management and Clinical Governance are partially offset by Commissioning, Redesign & QIPP. The Medicines Management variance has increased to a £55k underspend. Income for misattributed prescribing costs for Berkshire West PCT equates to £38k of this. The other significant under-spend of £10k is within the drugs line. There is also a small favourable pay variance.
The Clinical Governance cost centre is £39k under-spent. The pay under-spend has reduced to £8k due to the band 8b Adult safeguarding post being moved out of this cost centre to a new safeguarding cost centre. The band 8b Child safeguarding post will follow in August. The non-pay under-spend of £30k is principally made up of Clinical leads for which there has been no expenditure and a £6k appraiser costs under-spend.
• Joint Commissioning
There is a £6k adverse variance for the year up to July, an improvement of £38k on the previous month. The Continuing Care and Nursing Homes Team is now underspent by just £7k. The Contract Team is £33k

141
overspent. This is due to agency fees for two members of staff being £50k higher than the pay budget vacancies to month 4. The underspend on the Communication and Engagement team budget has reduced to £27k. Expenditure for 12/13 is currently £33k below budget. This is offset by agency fees, which is £6k in excess of the budgeted band 7 post.
• Public Health and Health Improvement
The month 4 position for Public Health and Health Improvement shows an underspend of £68k. The most notable variances are Young Persons Pooled Drug Treatment £34k adverse variance and favourable variances of £39k for Smoking Cessation and £31k for HIV/AIDS. The HIV / AIDS £31k under-spend includes £23k relating to a credit note from Mildmay relating to 2010/11. Some smaller items have not been accrued this month, nominally adding to the positive variance. Given that last year’s West Kent invoice is greater than budget, it is likely that the under-spend will decrease until break-even by year end.
• Acute SLAs
Start contracts with all local providers are agreed and for non-local contracts, most are now agreed and where they are not, due in the main to delays in co-ordinating commissioner agreements with the relevant provider, an assessment of the likely outcome has been included.
Year to date and forecast acute contract positions are showing significant over-performance across the Cluster. The year to date positions and most likely forecast provider contract positions are shown in table 6 below:
Table 6: Acute services (over) / underspend

142
Plan Actual Variance Plan FOT Variance£000s £000s £000s £000s £000s £000s
Commissioning: Acute and Specialist BudgetsGuys & St Thomas' 9,321 9,366 (45) 27,963 29,073 (1,110)Kings 4,190 5,031 (841) 12,570 15,163 (2,593)UHL 1,512 1,525 (13) 4,535 4,457 78SLHT 29,543 29,878 (335) 90,223 91,228 (1,005)Other Acute Service Agreements 3,641 3,749 (109) 10,922 10,747 175London Ambulance 2,174 2,174 0 6,523 6,523 0St George's 151 100 51 454 301 153Darenth Valley 8,333 8,395 (61) 25,000 25,340 (340)
58,865 60,218 (1,353) 178,190 182,831 (4,641)Specialist Services Consortia 4,852 4,929 (77) 14,555 14,757 (202)Other Earmarked Acute budgets 1,950 1,769 181 5,851 5,472 378Sub total - Acute and Specialist Budgets 65,667 66,916 (1,249) 198,595 203,060 (4,465)
YTD Forecast Outurn
These figures are based on:
• Month 3 flex information from Trusts, including adjustments to month 2 information relating to Trust challenges;
• Assessments of un-coded activity that are not yet included in flex data from trusts;
• Adjustments relating to trust-led QIPPs and KEY Performance Indicators (KPIs) not reflected in trust monitoring returns;
• Year-end forecasts are based on a phasing of activity to reflect working days,
seasonality, Refer to Treatment (RTT) and elective trajectories and year-end activity uplifts to meet targets. Further work is being undertaken across all local contracts to ensure a reasonable view of phasing is reflected in monthly reporting.
• There is a lack of clarity on the recurrent nature of some of the activity which has
its roots in a lack of clear intelligence triangulating new demand with activity being performed and reducing waiting times. This represents a risk going forward.
• The Month 4 year to date expenditure position is based on an up-scaling of Month 3 information, adjusted to reflect the above.
• The Cluster is co-ordinating commissioner for the four South East London acute provider contracts (SLHT, Lewisham, King’s and Guy’s).

143
At month 4, the Care Trust is reporting a £1,249k year to date over-performance on acute contracts including £77k on Specialist contracts. The forecast over-performance is £4,465k almost double that reported in month 3. South London Healthcare is now reporting to perform in line with the collar figures in the Cap & Collar agreement, as opposed to the baseline at month 3. A summary of the year to date and forecast outturn position for the four trusts for which cluster is co-ordinating commissioner is shown in table 7 below.
Table 7: Summary YTD and FOT variances for host providers
YTD BudgetAnnual Budget Forecast (Over)/ Under Performance
QIPP Delivery Other Total
QIPP Delivery Other Total
£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000SLHT 29543 0 -335 -335 89423 -674 -331 -1005Lewisham 1512 -13 -13 4535 78 78Guys 9321 -45 -45 27963 -1110 -1110Kings 4190 -841 -841 12570 -2593 -2593Total 44565 0 -1234 -1234 134491 -674 -3956 -4630
YTD (Over)/ Under Performance
An explanation of the key areas of over-performance including mitigating actions is set out below. Further details are within detailed acute contract monitoring reports.

144
South London Healthcare NHS Trust
Key area of over performance
Responsible Director / Manager
Mitigating Action including impact of QIPP
Due Date
Outpatients Christian Adams Outpatient over-performance is significantly influenced by the level of activity that was taken out of the baseline plan in respect of QIPP however there is some evidence of growth. Analysis will be undertaken to assess impact and drivers in both these areas.
Ongoing
Elective Christian Adams After correction for outpatient procedures recorded as daycases residual over performance is £1.6m across the cluster. Initial analysis indicates that around £1m relates to 18-week RTT backlog clearance. This is being reviewed with the Trust to validate and assess future impact.
Further activity relates to colonoscopy activity transferred from InHealth and activity recording errors to be corrected.
August 2012
At month 4 the position is now forecasting in line with the cap and the contracting team is reviewing all activity to ensure that it has been correctly charged. The SLHT cap and collar agreement is across South East London and not by individual PCT. An agreement is yet to be made between PCTs on how the final SLA value will be apportioned and this poses a risk to the Care Trust that the value included as the projected final cap value is understated.

145
Lewisham
Key area of over performance
Responsible Director / Manager
Mitigating Action including impact of QIPP
Due Date
Emergency Neil Stevenson This performance is being reviewed jointly with the trust. Communication has started to mitigate key areas of overspend
September 12
Critical Care Neil Stevenson The increase in activity relates to the over-performance in emergency, as this is high cost low volume activity the position will be reviewed
August 12
Direct Access Neil Stevenson This performance is being reviewed jointly with the trust. Communication has started to mitigate key areas of overspend
September 12

146
Guy’s & St Thomas’
Key area of over performance
Responsible Director / Manager
Mitigating Action including impact of QIPP
Due Date
Emergency Paul Munkenbeck
GSTT continues to over- perform against the emergency Point of Delivery contract plan at month 3. Analysis has recently been completed looking at final 11/12 outturn compared to contract plan (month 8 projected). This revealed significant under purchasing due to an increase in activity at the end of 11/12. There is urgent work ongoing between local BSUs (particularly Southwark and Lambeth), Cluster and the Trust to identify the key emergency drivers and work to reduce demand and activity.
August 2012
Outpatients Paul Munkenbeck
Work is taking place during August between BSUs and the Cluster to analyse variance against QIPP savings plans by speciality to identify key shortfalls in delivery.
August 2012
King’s
Key area of over performance
Responsible Director / Manager
Mitigating Action including impact of QIPP
Due Date
Emergency Rob McCarthy KCH continues to over-perform against the emergency Point of Delivery contract plan at month 3. Analysis has recently been completed looking at final 11/12 outturn compared to contract plan (month 8 projected). This revealed significant under purchasing (over
On-going

147
£1m). There is urgent work ongoing between local BSUs (particularly Southwark and Lambeth), Cluster and the Trust to identify the key emergency drivers and work to reduce demand and activity.
Elective Rob McCarthy Whilst not as significant as the emergency over-performance, there is also large elective over performance at month 3, particularly for the local BSUs. There are several specialties contributing, but 2 key drivers are Clinical Haematology and Medical Oncology. The first was a mid-year transfer from GST to KCH in 11/12, therefore is potentially explained. The second key driver is Medical Oncology, for which there is further investigation ongoing with the Trust to understand. The elective position is likely to deteriorate through the year as KCH works to reduce its RTT backlog however this will be funded by the bid against the Strategic Investment Fund. There was also under purchasing of elective activity when compared to final 11/12 outturn, though not as significant as the level of emergency under purchasing.
On-going
Specialist Commissioning
The annual budget was increased by £42k to a total of £14.6m in month 3 as 2 new services transferred to Specialist Commissioning; these are Cystic Fibrosis Register and Immunology (IVIG). At the end of month 3, the Care Trust was showing an under spend of £200k with a forecast out-turn after applying the risk sharing arrangements of an overspend of £202k which is the same as that predicted at the end of last month. However, a proportion of the projected forecast outturn has been reported at month 4.

148
Specialist commissioning colleagues are continuing to challenge the activity data from Trusts and have a good level of success in this regard. At present, £773k has been challenged with £356k being settled in the specialist commissioning favour, £9k being found against the commissioner and the rest remains yet to be resolved.
The main variances in the month 3 position were Adult BMT £107k underspend (a review of trust waiting lists is currently underway), PICU £121k underspend, Spinal £61k underspend (only 2 months data recd), Haemophilia £35k underspend (a review of clotting factor costs is being undertaken to understand the underspend to date), SCBU £29k which are offsetting overspends in Renal £58k (due to variable activity levels), Neuro-rehab £49k and NICU £43k (which is consistent with previous years).
The performance against areas commissioned by the London Specialist Commissioning group is shown in table 8.

149
Table 8: Specialist Commissioning performance
Category Service Description2 Activity Currency
'Total YTD Activity
YTD Budget Total YTD Actuals (£)
YTD Variance (£)
Total Annual Budget
Forecast Outturn AFTER
Tol/MR AFTER Risk
share
Forecast Variance
AFTER Tol/MR
AFTER Risk share
Existing Adult BMT Transplants 3 242 135 107 968 968 - AIAU N/A - 1 1 - 5 5 - Bowel Screening N/A - 40 40 - 159 159 - Burns HRGs 8 24 25 (1) 94 94 -
OBDs - Child & Young People Oncology Oncology HRG Spells 12 6 31 (24) 25 30 (5)Cleft Lip & Palate Patient Treated 27 37 37 - 149 149 - DSPD N/A 12 12 - 50 50 - Gender Dysphoria Appointment 3 4 1 3 15 12 3 Genetics Outpatient Appointments 309 92 92 - 368 368 - Haemophilia Patients Treated 8 379 344 35 1,516 1,500 16 HAVENS N/A - 13 13 - 51 51 - High Secure Service N/A - 51 51 - 204 204 - HIV Inpatient Spells - 463 443 20 1,853 1,853 0
New Patients 22 Major Trauma N/A - 64 64 - 258 258 - Mental Health for the Deaf OBDs - 2 1 1 8 8 - Neuro Rehabilitation OBDs 518 97 145 (49) 386 386 - Newborn Screening Tests/Blood Spot Cards 748 12 12 - 49 49 - NICU OBDs 293 307 350 (43) 1,226 1,226 - NICU Corporate Cost N/A - 0 - 0 0 0 NICU Local Investment N/A - 1 1 - 3 3 - Paediatric BMT Transplants 1 5 21 (17) 19 19 - PICU OBDs 27 226 106 121 973 973 - Practitioner Health Programme N/A - 6 6 - 25 25 - Renal Sessions 3,810 1,068 1,126 (58) 4,274 4,484 (211)Renal-DAFB Sessions - - - - - - SCBU OBDs 437 252 223 29 1,010 1,010 - SCG Management Costs N/A - 33 33 - 133 133 - Specialised Non Contract Activity N/A - 27 4 23 108 108 0 Specialised Pharmacy N/A - 9 9 - 34 34 - Specialised Psychotherapy Appointment - - - - - - - Spinal Spells - 66 5 61 264 264 - Stereotactic Radiosurgery N/A - 9 12 (3) 35 35 (0)WEMS N/A - 73 73 - 293 293 -
Existing Total 6,226 3,622 3,416 206 14,555 14,751 (197)New Cystic Fibrosis Register - 10 11 (1) 42 42 -
Immunology (IVIG) Drugs - - 5 (5) 5 (5)New Total - 10 16 (6) 42 47 (5)
6,226 3,632 3,433 200 14,596 14,798 (202)
150
• Mental Health
The month 4 position for Mental Health shows an overspend of £337k and is forecast to overspend by £517k at year end.
Adult cost per case continues to overspend by £200k at month 4. Currently there are 10 clients in out of borough placements, against a budget based on 7 clients. In month 4 there has been one discharge, and plans are in place to discharge 2 clients before the handover to Specialist Commissioning planned for September.
The Oxleas contract is overspent by £164k due to having 12 clients in medium secure beds against a contract of 8 beds up to the end of June. 2 clients were discharged at the end of June, so the rate of overspend has decreased. It is anticipated there will be two further discharges by 30th September which will return the Care Trust to the contracted 8 beds. There are no patients waiting for forensic placements. There has also been an under spend (£6k) in the Tilt service as there has been under occupancy during June, although the Care Trust is now back to capacity.
CAMHS cost per case has deteriorated in month to show a £5k overspend, this is due to one admission that has cost £105k over three months, this patient has now been discharged, and it is anticipated that the position will improve in future months.
• Exceptional Treatments
The position for High cost drugs included within this area is showing breakeven for month 4, and it is anticipated that this will continue to year end. The underspend can be attributed to the Home Delivery of Drugs but this is expected to breakeven by year end.
• Learning Disabilities
The Learning Disabilities Directorate is £21k overspent at month 4;
The position is due to an invoice that was not accrued and has since been paid. It relates to legal fees for a client that was admitted last year. The in-month position has improved slightly with one client’s costs coming in lower than forecast in previously.
• Continuing Care & Nursing Homes
Continuing Care has a £10k adverse variance for the year up to July. The forecast outturn is for the directorate to be £300k over spent by year end. This is due to the anticipated levels of retrospective reviews for 2012/13 due to the latest guidance and deadline in this respect.

151
Primary care
The overall primary care position for Bexley excluding practice prescribing is an overspend of £168k (1.2%) to the end of July 2012 (Month 4) and an estimated forecast outturn overspend of £585k. Details are shown in table 9 over the page.
The year to date position on Medical services to the end of July 2012 is an overspend of £183k (2.0%). This is mainly as a result of an overspend on PMS, GMS and APMS contracts of £220k, £40k and £19k respectively, primarily due to 2011/12 QOF achievement being greater than expected, and in previous years.
Bexley GP Practices achieved QOF points which were exceptionally higher than in previous years. The estimated accrual was £404k less than actual and is being phased equally across the 2012/13 financial year. A pro-rata shortfall of £101k has been shown in the month 4 position.
This has also had an impact on the 12/13 budgeted resource of £4,540k, the actual 11/12 outturn position uplifted for the 2.49% 12/13 price increase equates to £4,851k resulting in an anticipated shortfall of £311k.
The total cost pressure in 12/13 amounts to £715k, £241k of which has been shown in the M4 position across PMS, GMS and APMS.
This position has been reduced by releasing the prior year APMS accrual for £357k within LBB Locality; this has been phased across the year, on third being released in month 4.
The month 4 position does not include any anticipated cost pressures relating to the backdated practice payment claims received recently. These have been factored into the forecast outturn, split equally across enhanced services and premises; most likely case £75k and worst case £300k.

152
Table 9: Primary Care position detail
DescriptionBest Case Likely Case
Worst Case
Best Case
Likely Case
Worst Case
£000's £000's £000's £000's £000's £000's £000's £000's £000's £000's £000's £000's
PMS (Excluding NES & LES) 22,781 7,594 6,884 930 7,814 (220) 23,639 23,655 23,727 (645) (736) (1,033)
GMS (Excluding NES & LES) 2,363 788 845 (45) 801 (13) 2,420 2,420 2,425 (40) (40) (45)
APMS (Excluding NES & LES) 497 166 180 (8) 172 (6) 519 519 519 (19) (19) (19)
Out of Hours 1,238 413 603 (191) 413 0 1,238 1,238 1,238 0 0 0
LBB Locality Report 968 323 (728) 994 266 56 626 804 804 342 164 164
NES & LES (To be transferred to BSU) 234 78 27 51 78 (0) 234 234 234 0 0 0
Subtotal: Primary Medical Services 28,080 9,360 7,812 1,731 9,543 (183) 28,674 28,868 28,946 (361) (630) (932)
Dental 8,367 2,789 2,733 56 2,789 0 8,317 8,367 8,403 50 1 (36)
Pharmacy 6,000 2,000 372 1,621 1,993 7 5,980 5,980 6,039 20 20 (39)
Optometry 1,920 640 437 195 632 8 1,895 1,895 1,952 25 25 (32)
Total: Primary Care Services 44,366 14,789 11,353 3,604 14,957 (168) 44,867 45,110 45,340 (267) (585) (1,040)
Forecast Outturn Forecast VarianceYTD
BudgetAnnual Budget
Actual Expenditure
before Manual Accruals
Month End
Manual Accruals
YTD Actual Expenditure
YTD Variance
• Service Redesign / Community
This Directorate has an adverse variance of £39k for the year to July. The GP Anti-coagulation budget over spend of £66k for the year to date is offset by a number of smaller under-spends, most notably Community Dermatology and Minor Oral
153
Surgery. The GP Anti-Coagulation overspend increased by a further £17k during July. This represents a continuation of the over-spending in 2011/12 (72%). No additional funding has been found to bridge the gap but the service is due to be re-tendered BBG wide. Minor Oral Surgery is now showing a £25k favourable variance, due to no expenditure being incurred for the year to date. Given there has been no expenditure since July 2011, no accruals have been made. The Community Dermatology under-spend has increased from £9k to £16k. The £72k increase in budget from last year has not been matched by any substantial increase in expenditure to date. The 2011/12 outturn was £138k against a £119k budget. Forecast outturn for this year is set at break-even.

154
8. Indicative CCG resources From 1st April 2012, Bexley Care Trust’s responsibilities will be primarily transferred to Bexley Clinical Commissioning Group, with other areas being transferred to the National Commissioning Board, the Local Authority, Public Health England and others. Work is ongoing to identify the exact budgets to transfer and to where. However, it is expected that c80% of current budgets will transfer to the CCG and c20% to other areas. This assumption is also being used by the Trust Special Administrator (TSA) in his current work across South East London. Table 10 shows the indicative budgets with this 80:20 split. Table 10: Indicative CCG resources
£000's £000's £000's £000's £000's £000's £000's
80:20 Indicative CCG Budgets 80% 294,465 24,573 24,430 -143 98,034 97,114 -920 291,659 -2,807Indicative Other Budgets 20% 73,616 6,143 6,108 -36 24,509 24,279 -230 72,915 -702Total Budgets 100% 368,082 30,717 30,538 -179 122,543 121,393 -1,150 364,573 -3,508
Indicative CCG Resources 80% -294,465 -24,612 0 24,612 -97,730 0 0 -294,465 0Indicative Other Resources 20% -73,616 -6,153 0 6,153 -24,432 0 0 -73,616 0Total Resources 100% -368,082 -30,764 0 30,764 -122,162 0 0 -368,082 0
Indicative CCG Balance Sheet 80% 0 0 -24,430 -24,430 0 -97,114 0 0 0Indicative Other Balance Sheet 20% 0 0 -6,108 -6,108 0 -24,279 0 0 0Total Balance Sheet 100% 0 0 -30,538 -30,538 0 -121,393 0 0 0
Indicative CCG Total 80% 0 -38 0 38 305 0 -920 -2,807 -2,807Indicative Other Total 20% 0 -10 0 10 76 0 -230 -702 -702Total 100% 0 -48 0 48 381 0 -1,150 -3,508 -3,508
YTD VarianceForecast Outturn £000's
Forecast Variance
£000'sDirectorate Description
Annual Budget In Month Budget In Month Actual In Month Variance YTD Budget YTD Actual
These numbers will be become firmer over the coming months.

155
9. RISKS
Despite currently forecasting achievement of the planned 1% surplus, there are risks to the achievement of this financial position. The main risks and the potential impact on the financial achievement are shown in table 11.
Table 11: Best, Most likely, worst case risks
2012/13 2012/13 2012/13 Notes How they are being managedBest case Most Worst
likely case£m £m £m
Opening (deficit)/surplus after final budgets (with the exception of final acute SLAs)
(9.4) (9.4) (9.4)
RAG rated QIPP included in plans 7.6 7.6 7.6Opening underlying (deficit)/surplus after final budgets (with the exception of final acute SLAs) after QIPP
(1.8) (1.8) (1.8)
Return of 2% N/R for Guy's transitional funding 0.5 0.5 0.5 Expected return to cover transitional Guy's SLA costs
Financial Support 4.8 4.8 4.8 Agreed financial support
Opening (deficit)/surplus after final budgets (with the exception of final acute SLAs) after QIPP and financial support
3.5 3.5 3.5
Further risk / expected movementsIncrease expected for SLHT cap & collar SLA (3.5) (5.5) (5.5) To be covered from
2% N/RUnplanned reductions to RRL (best case based on kn 0.0 (0.2) (0.5) Constant review of RRL. Can be covered by
0.5% contingency & small other reserves.
Acute over-performance (excl SLHT cap & collar) / QIPP under-performance - calculated by cluster colleagues
(2.4) (3.5) (6.0) Contant review and update of position. Most likely case can be covered by contingency and small other reserves. CCG working with GPs to reduce referrals and use of PMC to triage.
Double running costs 0.0 (0.2) (0.5) To be covered from 2% N/R
Anti-coagulation drugs 0.0 (0.5) (1.0) Phased implementation
PPA figures reviewed monthly and over-performance monitored. Active Medicines Management team working with GPs to ensure effective and efficient prescribing as well as use of script switch. £400k prescribing reserve in place.
Increased continuing care and retrospective reviews (0.2) (0.3) (1.0) Monthly review of CHC position. Rigourous review of all cases in place. Can be covered from 0.5% contingency & small other reserves.
Risk assessments for Autism 0.0 0.0 (0.1)(Deficit) / surplus after risks before reserves (2.6) (6.7) (11.1)
General reserve available 1.5 1.5 1.50.5% contingency 1.8 1.8 1.8Prescribing reserve 0.4 0.4 0.4Neuro rehab committed resources 0.4 0.4 0.4Non-recurrent benefit from the Balance Sheet & committed resources released
1.4 1.4 1.4
Other 2% N/R 0.0 0.2 0.5Final (Deficit)/surplus after risks & reserves before 2.9 (1.0) (5.1)Expected 2% N/R return 4.0 4.0 4.0 Expected return to
cover increased SLHT SLA costs
Final (Deficit)/surplus against 1% target surplus 6.9 3.0 (1.1)

156
These risks are continually reviewed and adjusted and the impact on the financial position monitored as they crystallise or circumstances become clearer. At this time in the year because of uncertainty in the level of risks they have not been used to inform the forecast outturn position, which is still predicted to meet the 1% planned surplus position. These risks are in addition to any directorate and primary care overspends, which at this stage in the financial year are expected to be as shown in table 5. The amount included for projected acute over-performance is as provided by cluster colleagues. A summary of acute sector risks, start and in year mitigation and an associated risk rating is set out in table 12. Where the risk is differential across providers, this has also been set out. This is an initial risk assessment and this will be updated as the year progresses. Further details will be provided in monthly acute contract monitoring reports.
Table 12: Acute risk assessment assumptions
Risk Description of risk Start Year Mitigation In year mitigation RAG Status
Activity & Population & Incidence Growth
Acute start contracts have predominantly been based on 2011/12 forecast outturn. This presents two risks: 1. under-purchasing where there is a difference between forecast and actual outturn. 2. in year population & incidence growth.
GSTT - adjustment for potential under-purchasing made; investment in further elective volumes
Monthly robust review and challenge process; use of remaining population & incidence reserves to fund activity growth above contracted levels
King's - contract based on M8 forecast outturn
LHNT – demographics built in to the start contract but high year end outturn has offset some of this growth so start contract values are now only slightly above year end outturn.
SLHT – contract based on M7 FOT

157
Risk Description of risk Start Year Mitigation In year mitigation RAG Status
Delivery of national waiting times targets
Start contracts include commitments to deliver national waiting times targets.
GSTT - start contract includes additional activity to meet jointly assessed required activity to meet 18 weeks targets
Detailed monitoring and assessment of RTT performance completed on a monthly basis. RTT bids against the 2% non-recurrent fund have been approved.
King's - assessment of costs associated with backlog clearance complete and business case to access 2% non-recurrent funds approved
LHNT - start contract volumes and values are considered sufficient to sustain RTT targets
SLHT – start contract based on M7 forecast outturn is considered sufficient to deliver and sustain RTT requirements, noting two specialities will breach targets until September 2012.
QIPP Delivery Start contracts include deductions from forecast outturn to reflect QIPP initiatives
Contracts include terms in respect of the delivery of Trust led KPIs thereby guaranteeing an element of QIPP delivery.
For CCG led initiatives, pre-risk assessed QIPPs have been removed from contracts and risk reserves set aside for the difference between pre-and-post risk assessed QIPPs thereby providing some mitigation against under-delivery.
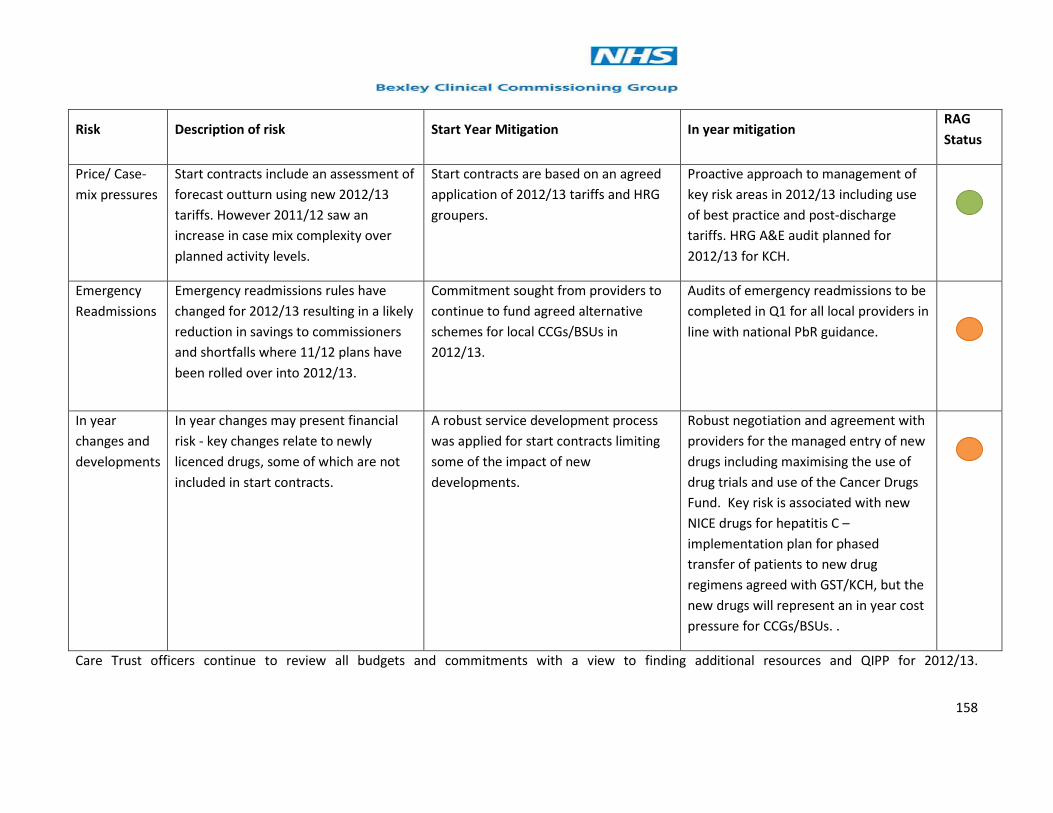
158
Risk Description of risk Start Year Mitigation In year mitigation RAG Status
Price/ Case-mix pressures
Start contracts include an assessment of forecast outturn using new 2012/13 tariffs. However 2011/12 saw an increase in case mix complexity over planned activity levels.
Start contracts are based on an agreed application of 2012/13 tariffs and HRG groupers.
Proactive approach to management of key risk areas in 2012/13 including use of best practice and post-discharge tariffs. HRG A&E audit planned for 2012/13 for KCH.
Emergency Readmissions
Emergency readmissions rules have changed for 2012/13 resulting in a likely reduction in savings to commissioners and shortfalls where 11/12 plans have been rolled over into 2012/13.
Commitment sought from providers to continue to fund agreed alternative schemes for local CCGs/BSUs in 2012/13.
Audits of emergency readmissions to be completed in Q1 for all local providers in line with national PbR guidance.
In year changes and developments
In year changes may present financial risk - key changes relate to newly licenced drugs, some of which are not included in start contracts.
A robust service development process was applied for start contracts limiting some of the impact of new developments.
Robust negotiation and agreement with providers for the managed entry of new drugs including maximising the use of drug trials and use of the Cancer Drugs Fund. Key risk is associated with new NICE drugs for hepatitis C – implementation plan for phased transfer of patients to new drug regimens agreed with GST/KCH, but the new drugs will represent an in year cost pressure for CCGs/BSUs. .
Care Trust officers continue to review all budgets and commitments with a view to finding additional resources and QIPP for 2012/13.
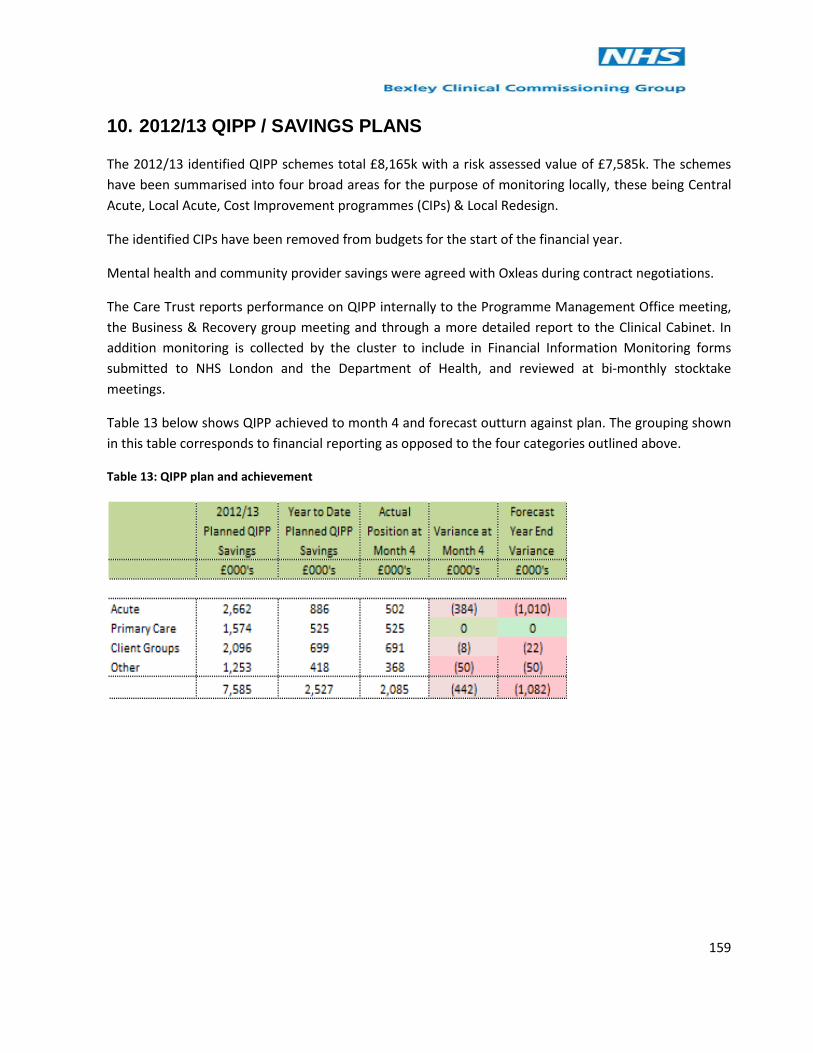
159
10. 2012/13 QIPP / SAVINGS PLANS
The 2012/13 identified QIPP schemes total £8,165k with a risk assessed value of £7,585k. The schemes have been summarised into four broad areas for the purpose of monitoring locally, these being Central Acute, Local Acute, Cost Improvement programmes (CIPs) & Local Redesign.
The identified CIPs have been removed from budgets for the start of the financial year.
Mental health and community provider savings were agreed with Oxleas during contract negotiations.
The Care Trust reports performance on QIPP internally to the Programme Management Office meeting, the Business & Recovery group meeting and through a more detailed report to the Clinical Cabinet. In addition monitoring is collected by the cluster to include in Financial Information Monitoring forms submitted to NHS London and the Department of Health, and reviewed at bi-monthly stocktake meetings.
Table 13 below shows QIPP achieved to month 4 and forecast outturn against plan. The grouping shown in this table corresponds to financial reporting as opposed to the four categories outlined above.
Table 13: QIPP plan and achievement

160
11. FINANCIAL MANAGEMENT
Better Payment Practice Code (BPPC)
Target
One of the Care Trust’s national targets is to ensure that at least 95% of NHS and non-NHS trade creditors are paid within 30 days of receipt of the invoice. Performance against this target is regularly reported to NHS London, and the annual cumulative figure for the year is published in the Annual Accounts and Annual Report.
Table 14: Better Practice Payment Code (BPPC) performance
NHS NON NHS CombinedTarget By Value By Count By Value By Count By Value By Count% % % % % % %
April 95.00% 98.15% 86.54% 85.60% 82.39% 96.94% 83.96%May 95.00% 98.36% 88.45% 87.52% 86.59% 97.31% 87.16%June 95.00% 97.18% 84.12% 82.10% 90.65% 96.28% 88.36%July 95.00% 98.25% 85.19% 84.30% 81.77% 96.42% 82.76%
The numbers have been adjusted from those reported at month 3 as a consequence of a recent review of the reporting algorithm that drives the numbers. The syntax does not account appropriately for invoices that have been part or completely cleared by credit notes. This now requires an additional check each month to identify if this anomaly has arisen and to make an appropriate manual adjustment. The Month 4 figures are accurate and completely consistent with the underlying data, although this has retrospectively changed the past performance figures from previous reports.
Combined NHS and Non-NHS performance by count to the end of July is the lowest it has been this year at 82.76% and is significantly below the 95% target. By value the combined performance is achieving the 95% at 96.42%. This is of concern and budget holders are constantly being asked to approve invoices in a timely manner. However there is concern at the speed with which invoices are being processed by SBS.
Cash Management
Cash Limit
The Care Trust’s cash limit for month 4 was £358.2m as in month 3. The Care Trust is not expecting to significantly under draw its cash in 2012/13.

161
Cash Drawings
Table 15 below shows the year to date cash drawings to Month 4 compared to the planned drawings for the same period. The cash plan anticipates the cash limit at the end of 2012/13 as opposed to the amount confirmed stated above.
Table 15: Planned and actual cash drawings
Actual Cash Drawings 2012/13
Planned Cash Drawings
Cumulative Actual Cash Drawings
Cumulative Planned Cash Drawings
Cash Balance
£m £m £m £m £mApril 28.945 28.945 28.945 28.945 2.295May 28.553 28.553 57.498 57.498 4.591June 28.597 28.597 86.095 86.095 0.151July 27.642 27.642 113.737 113.737 0.040August 30.614 113.737 144.351September 30.614 113.737 174.965October 30.614 113.737 205.579November 30.614 113.737 236.193December 30.614 113.737 266.807January 30.614 113.737 297.421February 30.614 113.737 328.035March 30.626 113.737 358.661Total 113.737 358.661 358.661
The cash balance at the end of April and May was unacceptably high, but this appears
to have been rectified for June and July.
Debtors and Income Collection
Table 16: Aged Debtors Position
Position as at 30
April 2012
Position as at 31
May 2012Position as at 30 June 2012
Position as at 31 July
2012£m £m £m £m
Under 1 Month 0.036 1.418 0.32 0.2111-2 Months 0.476 0.012 0.518 0.8582-3 Months 0.042 0.371 0.379 0.051Over 3 Months 0.283 0.307 0.307 0.583Total 0.837 2.108 1.524 1.703
162
The total value of aged debtors has increased again since June as has the age of debts. This will continue to be monitored to ensure that income is collected in a timely manner. The BSU Finance department is now involved in helping to resolve issues on outstanding invoices in an attempt to improve the position.

163
Statement of Financial Position
The month 3 Statement of Financial Position is presented in table 17 below for information. It is shown in the format required under International Financial Reporting Standards (IFRS). This is only updated on a quarterly basis for the FIMs returns,
Table 17: Statement of Financial Position June 2012

164
12. RECOMMENDATIONS
Members are asked to:
• DISCUSS & NOTE the Month 4 (July) financial position and forecast outturn detailed in this report;
• NOTE the indicative split of resources between the CCG’s responsibilities and other areas from 1st April 2013.
• DISCUSS & NOTE the key risks and cost pressures identified to achieving the surplus control total in 2012/13 and the management actions being taken to address and mitigate these risks;
• NOTE the revenue and capital resources available to the Care Trust;
• NOTE the month 4 forecast performance against the key national finance targets.

165
NHS London Monthly Financial Returns
Collection: Monthly Key Data
Month: 4Organisation Passcode: wa96o5Completed by: J SimpsonDate: 14 August 2012
Business Year & Period: 2012/13 P04Organisation Code: TAKOrganisation Type: POrganisation Name: Bexley Care TrustOrganisation SHA Code: Q36Return E-mail Address: [email protected]
Signed Off by:

166
SummaryBexley Care TrustMonth 4
£000's
% of Planned Revenue
2012/13 Planned Revenue 366,761
2011/12 Surplus/(Deficit) 2,2742012/13 Surplus/(Deficit) -
YTD Planned Surplus/(Deficit) 1,138 0.31%YTD Actual Surplus/(Deficit) 1,150 0.31%YTD Variance 12 0.00%
2012/13 Planned Surplus/(Deficit) 3,508 0.96%2012/13 Forecast Outturn 3,508 0.96%FOT Variance - 0.00%
2011/12 QIPP Target 10,203 2.78%2011/12 QIPP Achievement 8,181 2.23%2012/13 QIPP Target 7,585 2.07%2012/13 QIPP Forecast Achievement 6,511 1.78%
Total Financial Risk Identified 9,187 2.50%Expected Value of Financial Risk (not in FOT) 250 0.07%Total Possible Mitigation 2,004 0.55%Expected Value of Mitigation 250 0.07%
2012/13 Worst Case Forecast Outturn (2,565) -0.70%
SUMMARY UPDATE (must be completed)The PCT is currently forecasting to deliver its planned surplus in 2012/13 but with considerable risks associated with service over-performance and delivery of QIPP savings initiatives. The PCT is assuming access to 2% non-recurrent funding to meet the costs of transformational change, to meet planned non-recurrent RTT costs The PCT is forecasting it will meet the majority of its QIPP savings but this assessment is draft and will be updated as more reliable information is avaliable over the coming months, the QIPP shortfall is built into the financial forecasts in full.

167
TrajectoriesBexley Care TrustMonth 4 4
Month In Month PlanIn Month Actual/
ForecastVariance YTD Plan YTD Actual Variance
£000's £000's £000's £000's £000's £000's4 179 179 (0) 1,138 1,150 125 75 75 (0) 1,213 1,225 126 504 504 (0) 1,718 1,729 117 79 79 (0) 1,797 1,808 118 305 305 (0) 2,102 2,113 119 273 273 (0) 2,375 2,386 11
10 78 78 (0) 2,453 2,464 1111 761 761 (0) 3,214 3,225 1112 294 283 (11) 3,508 3,508 -
Summary of forecast trajectory:Year to date outturn 1,138 1,150 12Forecast for remainder of year 2,370 2,358 (12)Forecast Outturn 3,508 3,508 -
£000s £000s(0) 12
Reasons: Reasons:(119) (442)119 454
Total variance from plan in month 0 Total variance from plan YTD 12FULLY
EXPLAINEDFULLY
EXPLAINED
£000s £000s- 1,150
Reasons: Balance of Plan 2,370(1,074) Change to FCOT from plan -
1,074(12)
Total variance from plan FOT 0 3,508FULLY
EXPLAINEDFULLY
EXPLAINED
Actions to be taken to achieve forecast outturn
CIP Slippage FOT
Expenditure profiling
Actions to recover YTD plan
Reasons for variance between actual and planned YTD
Variance from Plan YTD
Expenditure held in other Budgets
Expenditure held in other budgets
YTD Surplus/(Deficit)
CIP Slippage YTD
Forecast outturn surplus/(deficit)
Reasons for variance between actual and planned in month
Variance from Plan in month
Expenditure held in other BudgetsCIP Slippage in month
Variance from Plan FOT
Reasons for variance between actual and planned FOT
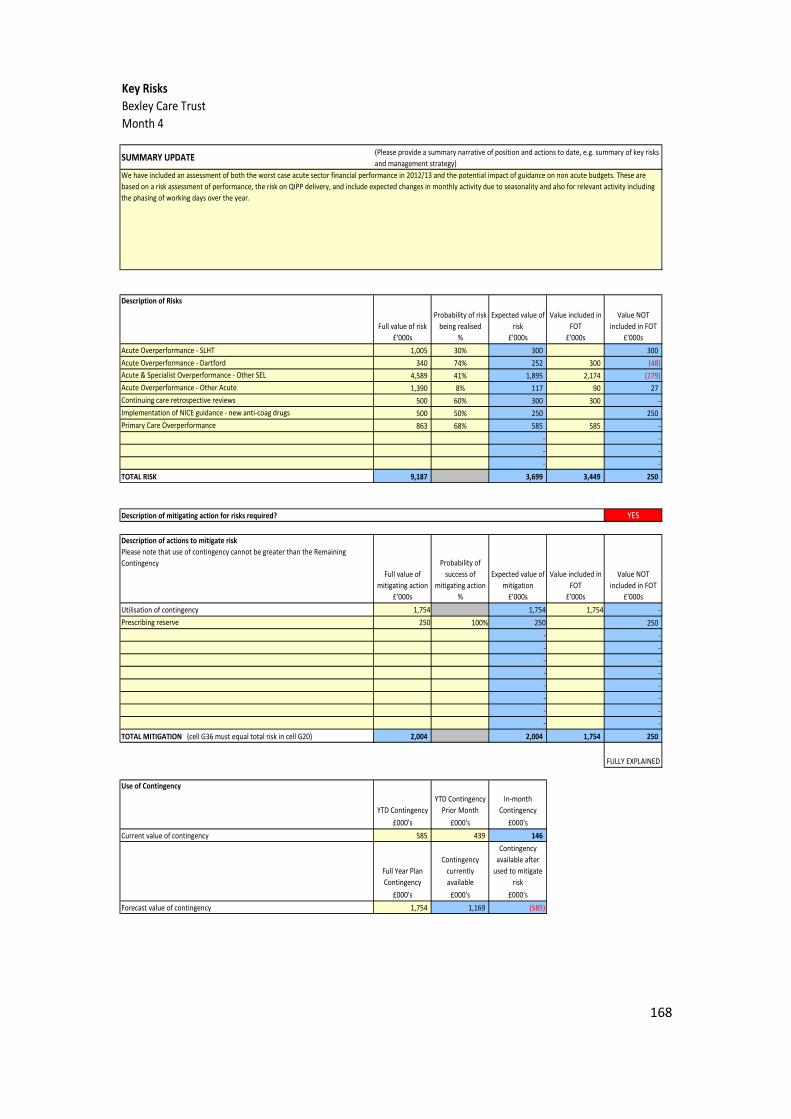
168
Key RisksBexley Care TrustMonth 4
SUMMARY UPDATE
Description of Risks
Full value of risk£'000s
Probability of risk being realised
%
Expected value of risk
£'000s
Value included in FOT
£'000s
Value NOT included in FOT
£'000sAcute Overperformance - SLHT 1,005 30% 300 300Acute Overperformance - Dartford 340 74% 252 300 (48)
4,589 41% 1,895 2,174 (279)1,390 8% 117 90 27
500 60% 300 300 -500 50% 250 250863 68% 585 585 -
- -- -- -
9,187 3,699 3,449 250
YES
Full value of mitigating action
£'000s
Probability of success of
mitigating action %
Expected value of mitigation
£'000s
Value included in FOT
£'000s
Value NOT included in FOT
£'000sUtilisation of contingency 1,754 1,754 1,754 -
250 100% 250 250- -- -- -- -- -- -- -- -
2,004 2,004 1,754 250
FULLY EXPLAINED
Use of Contingency
YTD ContingencyYTD Contingency
Prior MonthIn-month
Contingency£000's £000's £000's
Current value of contingency 585 439 146
Full Year Plan Contingency
Contingency currently available
Contingency available after
used to mitigate risk
£000's £000's £000'sForecast value of contingency 1,754 1,169 (585)
Description of actions to mitigate riskPlease note that use of contingency cannot be greater than the Remaining Contingency
Acute & Specialist Overperformance - Other SEL
(Please provide a summary narrative of position and actions to date, e.g. summary of key risks and management strategy)
We have included an assessment of both the worst case acute sector financial performance in 2012/13 and the potential impact of guidance on non acute budgets. These are based on a risk assessment of performance, the risk on QIPP delivery, and include expected changes in monthly activity due to seasonality and also for relevant activity including the phasing of working days over the year.
Description of mitigating action for risks required?
Acute Overperformance - Other AcuteContinuing care retrospective reviewsImplementation of NICE guidance - new anti-coag drugsPrimary Care Overperformance
Prescribing reserve
TOTAL RISK
TOTAL MITIGATION (cell G36 must equal total risk in cell G20)

169
Underlying PositionBexley Care TrustMonth 4
Non-recurrent items Description YTD FOT£'000s £'000s
Surplus/(Deficit) 1,150 3,508Enter non-recurrent income items Non-recurrent support (1,593) (4,780)(excl CQUIN) as negative values Prior year surplus (758) (2,274)
Total (2,351) (7,054)Enter non-recurrent expenditure items 1% surplus target 1,169 3,508as positive values
Total 1,169 3,508Normalised Surplus/(Deficit) (32) (38)

Appendix 1
170
QIPP AnalysisBexley Care TrustMonth 4
QIPP Local Workstream QIPP Regional Workstream
Total PlanForecast Outturn
Full Year Variance
% Forecast to be
unachieved/(overachieved)
Current Month Plan
Current Month Actual Variance YTD Plan YTD Actual YTD Variance
% Unachvd of FOT
£000s £000s £000s % £000s £000s £000s £000s £000s £000sMental health 976 976 (0) 0% 81 81 - 325 325 (0) 67%Acute Sector 2,317 1,376 (940) 41% 197 109 (88) 771 450 (321) 81%Primary care productivity - - - 0% - - - - - - 0%Community support services 1,147 1,147 - 0% 96 96 - 382 382 - 67%Activity shifts 301 218 (83) 28% 26 7 (18) 100 29 (71) 90%Long Term Conditions - - - 0% - - - - - - 0%Urgent Care - - - 0% - - - - - - 0%Planned Care - - - 0% - - - - - - 0%End of Life Care - - - 0% - - - - - - 0%Prevention - - - 0% - - - - - - 0%Staying Healthy - - - 0% - - - - - - 0%
Procurement Non Clinical Procurement 626 577 (49) 8% 52 40 (12) 209 159 (50) 75%Decommissioning ineffective procedures - - - 0% - - - - - - 0%Enhanced recovery - - - 0% - - - - - - 0%Referral management 18 17 (1) 6% 2 1 (0) 6 6 (0) 69%Back office - - - 0% - - - - - - 0%Estates 626 626 - 0% 52 52 - 209 209 - 67%Staffing - - - 0% - - - - - - 0%Clinical support rationalisation - - - 0% - - - - - - 0%Diagnostics - - - 0% - - - - - - 0%Direct access - - - 0% - - - - - - 0%Medicines use - - - 0% - - - - - - 0%Prescribing 1,574 1,574 - 0% 131 131 - 525 525 - 67%
Unidentified Unidentified - - - 0% - - - - - - 0%
Total 7,585 6,511 (1,074) 14% 636 517 (119) 2,527 2,084 (442) 73%
Productivity
Integrated care
Demand management
Running costs
Clinical overheads
Reducing drug spend

171
Finance & ActivityBexley Care TrustMonth 4
2012/13 Plan 2012/13 FOT Variance2012/13 Plan YTD
2012/13 Actual YTD
Variance
£000's £000's £000's £000's £000's £000'sPbR - Elective 36,718 37,767 1,049 9,073 10,319 1,246PbR - Non-Elective 49,412 50,578 1,166 12,319 12,130 (189)PbR - A&E 6,441 6,311 (130) 1,606 1,607 1PbR - Outpatient 25,301 25,362 61 6,325 6,622 296PbR - Other 102 102 - 26 26 -Non-PbR: critical care 10,086 11,283 1,197 2,513 2,802 289Non-PbR: mental health 31,425 30,925 (500) 7,856 7,774 (83)Non-PbR: community care 23,885 23,885 - 5,971 5,971 0Non-PbR: other 143,373 143,165 (208) 35,846 36,110 265Excluded drugs & devices 7,469 8,975 1,506 1,867 2,087 220Non Contract Activity 2,053 2,053 - 513 513 (0)LSCG 14,555 14,555 - 3,637 3,637 (0)NCG - - - -Transitional funding - - - -Total 350,820 354,961 4,141 87,553 89,597 2,045
Adjustment for block / Cap & Collar Contracts (if applicable) - - - -Revised Total 350,820 354,961 4,141 87,553 89,597 2,045
2012/13 Plan 2012/13 FOT Variance2012/13 Plan YTD
2012/13 Actual YTD
Variance
£000's £000's £000's £000's £000's £000's
In Sector Acute performance
129,023 132,756 3,733 32,118 33,864 1,747Out of Sector London Acute performance 8,484 8,363 (121) 2,112 2,207 95Out of London Acute performance 28,551 29,062 511 7,107 7,309 202Primary Care Contract performance 30,632 31,150 518 7,625 7,710 85Community Services performance 23,885 23,885 - 5,946 5,946 0MH Contract performance 25,675 25,175 (500) 6,391 6,307 (84)Other Contract performance 7,215 7,215 - 1,796 1,797 1Other 97,355 97,355 - 24,458 24,457 (1)Total 350,820 354,961 4,141 87,553 89,597 2,045Must equal row 22 above YES YES YES YES YES YES
2012/13 Plan 2012/13 FOT Variance2012/13 Plan YTD
2012/13 Actual YTD
Variance
PbR - Elective (Spells) 30,487 28,247 (2,239) 7,533 7,062 (471)PbR - Non-Elective (Spells) 27,764 15,376 (12,388) 6,921 4,844 (2,077)PbR - A&E (Attendances) 61,093 35,743 (25,350) 15,273 11,048 (4,225)PbR - Outpatient (Attendances) 197,045 173,791 (23,254) 49,262 45,386 (3,876)PbR - Other - - - -
Year To DateFull Year

Appendix 1
172
Consultancy ServicesBexley Care TrustMonth 4
Total Consultancy
Services Costs in 2011/12
Final Accounts
2011/12 Consultancy
Services Costs that relate to
2011/12 Running Costs
2011/12 Consultancy
Services Costs not part of
2011/12 Running Costs
(i.e. Programme)
Total Consultancy
Services Costs in 2012/13
2012/13 Consultancy
Services Costs that relate to
2012/13 Running Costs
2012/13 Consultancy
Services Costs not part of
2012/13 Running Costs
(i.e. Programme)
Change in Consultancy
Services Costs
Change in Consultancy
Services Costs that relate to Running Costs
Change In Consultancy
Services Costs not related to Running Costs
(i.e. Programme)
Organisation NameOrg type Org code £000s £000s £000s £000s £000s £000s £000s £000s £000s
Bexley Care Trust P TAK 769 24 745 - (769) (24) (745)
2011/12 Consultancy Services Costs 2012/13 Forecast Consultancy Services Costs Change

173
SHA Lodgements & SupportBexley Care TrustMonth 4
2011/12 Final Accounts
Surplus/(Deficit)
Additional Funding to
cover costs of Strategic Change
included in 2011/12 Final
Accounts Surplus/(Defici
t)
Financial Support to
cover deficits included in
2011/12 Final Accounts
Surplus/(Deficit)
Organisation NameOrg type Org code
£000s £000s £000sBexley Care Trust P TAK 2,274 - -

174
2012/13 - 2% Non Recurrent Expenditure - Summary of Spend
TAKBexley Care
Trust
£m
TO PROVIDER ORGANISATIONS
Pump priming QIPP initiatives 1.5
Fixed/Semi fixed costs associated with change, for a time limited period
Redundancy / termination costs
Total to Provider Organisations 1.5
DIRECT PCT EXPENDITURE
QIPP initiatives 0.2
Revenue to capital transfers for capital expenditure that will be completed in 2011/12
Redundancy / termination costs
One off non pay costs related to PCT/SHA close down 0.1
Pump priming costs related to developing the new system 0.1
Total Direct PCT Expenditure 0.4
Total Spend to Date 1.9
TAKBexley Care
Trust
£m
TO PROVIDER ORGANISATIONS
Pump priming QIPP initiatives 3.4
Fixed/Semi fixed costs associated with change, for a time limited period
Redundancy / termination costs
Specific business case (for sign off)
Total to Provider Organisations 3.4
DIRECT PCT EXPENDITURE
QIPP initiatives 0.9
Revenue to capital transfers for capital expenditure that will be completed in 2011/12
Redundancy / termination costs 1.0
One off non pay costs related to PCT/SHA close down 0.7
Pump priming costs related to developing the new system 0.9
Specific business case (for sign off)
Total Direct PCT Expenditure 3.6
Total Spend - Forecast 7.0
Value of 2% (based on PCT 2012/13 Recurrent Allocations) 7.0
Unallocated -
Generic Categories of Expenditure - Year to Date
Generic Categories of Expenditure - Forecast Outturn

Appendix 1
175
Running CostsBexley Care TrustMonth 4
PCT Commissioning Running Costs
Public Health Running Costs
Total 2011/12 Running Costs
PCT Commissioning Running Costs
Public Health Running Costs
Total Forecast 2012/13 Running
Costs
PCT Commissioning Running Costs
Public Health Running Costs
Savings
Total Forecast 2012/13 Running
Costs Savings
£000s £000s £000s £000s £000s £000s £000s £000s £000s
Bexley Care Trust P TAK 6,113 517 6,630 5,950 727 6,676 164 (210) (46)
2011/12 Running Costs 2012/13 Forecast Running Costs 2012/13 Forecast Running Cost Savings
Organisation Name Org type Org code

Appendix 1
176
Capital PositionBexley Care TrustMonth 4
FINANCIAL PERFORMANCE UPDATE - HM Treasury Categories FINANCIAL PERFORMANCE UPDATE - HM Treasury Categories
Type of Spend
Planned Expenditure for
YTD
£000s
Actual Expenditure for YTD
£000s
Variance between actual and planned
for YTD £000s Type of Spend
Full Year Plan
£000s
Full Year Forecast
£000s
Variance between actual and planned
for FYE £000s
New Build - - New Build - -Maintenance 25 25 Maintenance 500 500 -Equipment - - Equipment - -Information Technology - - Information Technology 625 625 -Other - - Other 500 500 -
25 0 25 1,625 1,625 0Disposals & Transfers - - Disposals & Transfers - -Grants & Donations - - Grants & Donations - -Capital Grants - - Capital Grants (500) (500) -Impact of IFRIC 12 - - Impact of IFRIC 12 - -
Total Charge Against CRL 25 0 25 Total Charge Against CRL 1,125 1,125 0
FINANCIAL PERFORMANCE UPDATE - Department of Health Categories FINANCIAL PERFORMANCE UPDATE - Department of Health Categories
Type of Spend
Planned Expenditure for
YTD
£000s
Actual Expenditure for YTD
£000s
Variance between actual and planned
for YTD £000s Type of Spend
Full Year Plan
£000s
Full Year Forecast
£000s
Variance between actual and planned
for FYE £000s
Community Hospitals - - Community Hospitals - -Other Central Programme - - Other Central Programme - -Non Central Programme 25 25 Non Central Programme 1,625 1,625 -
25 0 25 1,625 1,625 0YES YES YES YES YES YES
NO NO(a) Explanation for year to date variance to plan required? (b) Explanation for full year variance to plan required?
Total Gross Capital Expenditure
Total Gross Capital ExpenditureMust equal row 12 above
Total Gross Capital Expenditure
Total Gross Capital ExpenditureMust equal row 12 above

Appendix 1
177
GLOSSARY OF TERMS
APMS ALTERNATIVE PRIMARY MEDICAL SERVICES
BPPC BETTER PAYMENT PRACTICE
CODE
BSU BUSINESS SUPPORT UNIT
CAMHS CHILDREN’S AND ADOLESCENTS MENTAL HEALTH SERVICES
CCG CLINICAL COMMISSIONING GROUP
CIP COST IMPROVEMENT PROGRAMME
CLUSTER NHS SOUTH EAST LONDON
CRL CAPITAL RESOURCE LIMIT
CSS COMMISSIONING SUPPORT SERVICE
FOT FORECAST OUTTURN
GMS GENERAL MEDICAL SERVICES
GSTT GUY’S & ST THOMAS’ NHS FOUNDATION TRUST
HRG HEALTH RESOURCE GROUP
LHNT LEWISHAM HOSPITAL NHS TRUST
LSCG LONDON SEPCIALIST COMMISISONING GROUP
KCH KING’S COLLEGE HOSPITAL NHS FOUNDATION TRUST
KPCA KENT PRIMARY CARE AGENCY
KPI KEY PERFORMANCE INDICATOR

Appendix 1
178
NCB NATIONAL COMMISISONING BOARD
NHSL NHS LONDON
PCT PRIMARY CARE TRUST
PMO PROGRAMME MANAGEMENT OFFICE
PMS PRIMARY MEDICAL SERVICES
QOF QUALITY OUTCOME FRAMEWORK
RTT REFER TO TREATMENT
QIPP QUALITY, INNOVATION, PRODUCTIVITY & PREVENTION
RRL REVENUE RESOURCE LIMIT
SLA SERVICE LEVEL AGREEMENT
SLHT SOUTH LONDON HEALTHCARE NHS TRUST
TSA TRUST SPECIAL ADMINISTRATOR
YTD YEAR TO DATE

Financial governance framework element
An emerging CCG should be in a position to...
Evidence for authorisation
Completed Date
1. The CCG has robust financial procedures and systems and has embedded awareness of financial governance within the CCG. CCGs are expected to promote the effective management of CCG resources and ensure honesty and transparency in their use. Prime financial policies (also known as Standing Financial Instructions) describe financial management arrangements for all areas of CCG expenditure, creditors, debtors, cash and capital assets. If the model constitution is used as a basis, we would expect CCGs to have detailed financial procedures to support their prime financial policies. CCGs will be required to use the integrated finance and accountancy system procured by the NHS Commissioning Board. The system will cover the general ledger, purchase ledger, sales ledger, cash management and management reporting functionality. The cost of providing the integrated finance and accountancy system will be retained by the NHS CB and not passed onto CCGs for the lifetime of the contract.
At point of application
• A) Confirm intention to use financial ledger system procured by the NHSCB.
• B) Confirm intention to use
model CCG prime financial policies (or equivalent), standing orders and scheme of delegation.
• C) Describe proposed
arrangements from April 2013 for financial transaction processing (invoices and payroll), asset management and procurement of non-healthcare goods and services.
• D) Operate in line with PCT
financial procedures and delegated authority.
• E) Describe the components of
their assurance framework.
• F) Describe arrangements for CCG access to adequately
At point of application
• Proposed CCG constitution and any other documents detailing financial governance arrangements
• CCG
organisational structure.
Point of Application – all items completed A, B, C, D E & F) Use of financial ledger, intention to use model CCG prime financial policies, proposals for financial transaction processing from April 13, operate in line with PCT financial procedures, describe the components of assurance framework, arrangements for access to trained finance staff taken to CCG Board 28/06/12 P:\Finance&Info\Financial Planning\Julie work in progress\Authorisation Finance Work\CCG Report on Finance for Authorisation - Front Sheet.doc (Item A, page 1, item a, Item B page 1, item b, Item C, page 1,

CCGs should not keep their own bank accounts or undertake any other separate financial transaction processing in 2012/13 as PCTs will be accountable for the use of NHS resources until April 2013.
CCGs will need their own bank account from April 2013 and requirements for this using the Government Banking Service will be confirmed before 31 March 2013.
resourced and suitably trained finance staff.
After application
• G) Confirm implementation plan in place to ensure ledger system available for use from April 2013 by 31 December 2012.
• H) Confirm arrangements
from April 2013 for financial transaction processing (invoices and payroll) and procurement of non-healthcare goods and services in place including draft service level agreements where required by 28 February 2013.
• I) Full CCG financial
procedures drafted in line with implementation of ledger system by 28 February 2013 for go live in April 2013.
• J) Confirm arrangements for
supporting the Accountable Officer to complete the CCG governance statement.
By 31 March 2013
• Detailed financial procedures.
• Register of
Interests.
item C, Item D, page 2, Item d, Item E, page 2, item e, Item F, page 2, item f) A, C & F supported by CSU document taken to Board on 25/10/2012, page 1 of attachment A supported by Financial Management Arrangements paper to Board 25/10/12, Financial Management Arrangements Overview Pages 8-9 Section 3.0 and 4.0 Prime Financial Policies Pages 96-99 sections 5 to 10 B supported by Financial Management Arrangements paper to Board 25/10/12, Financial Management Arrangements Overview Page 4 sections 2.1 and 2.3 Standing Orders pages

12 to 38 Prime Financial Policies (SFIs) pages 89 to 103 and Financial Management Arrangements Overview Page 4 section 2.2 Scheme of Reservation and Delegation pages 41 to 58 Schedule of Matters delegated to officers pages 61 to 86 C supported by Financial Management Arrangements paper to Board 25/10/12, Financial Management Arrangements Overview page 9 section 4.1 Prime Financial Policies pages 97-98 section 12, page 101-102 sections 16 and 17 and Financial Management Arrangements Overview page 9 sections 4.1 and 4.2 Prime Financial Policies page 97 section11 G & H With regard to

after application tasks, discussions with Cluster colleagues have taken place to request an implementation plan for the ledger, to confirm transaction processing arrangements, these items are now awaited. I) CCG Financial procedures taken to Board meeting on 25/10/2012 – whole document applicable. J) Arrangements for supporting the AO to complete the CCG governance statement remains outstanding at this point.

Financial governance framework element
An emerging CCG should be in a position to...
Evidence for authorisation
Completed Date
2. The CCG has effective financial reporting arrangements. CCGs will need to produce relevant and timely reports on financial performance for stakeholders (internal and external) over the course of the financial year. These reports will be important in helping to ensure that CCGs work within the resources available to them, as well as demonstrating the appropriate use of resources. Whilst CCGs will not produce annual accounts for 2012/13, they will need to demonstrate that they have considered the systems and processes that they will need to ensure that they can produce their annual report and accounts for 2013/14. CCGs will need to be able to produce annual accounts and reports following relevant standards and timetables that the Commissioning Board will set. This is important for transparency at CCG level but also vitally important for the consolidation of CCG financial information into Commissioning Board accounts.
At point of application
• A) Provide the shadow governing body with sample reports on financial performance and activity showing variance against budget and plan, highlighting areas of significant risk and where corrective action is needed.
• B) Provide monthly reports of financial performance against budget for all budgets that have been delegated to them.
• C) Report regularly on the
delivery of their QIPP programme.
• D) Provide details of
arrangements to ensure that all financial reports (internal and external) can be produced in line with relevant statutory and professional reporting requirements in a timely
At point of application
• Constitution and any other documents detailing financial governance arrangements.
A, B & C) Evidence obtained from Board reports;
a) QIPP reports – monthly
b) Finance reports – monthly
D & E) Finance paper for Board on 06/09 regarding production of reports and quality and completeness (Item D – page 1, item a, Item E – page 2, item b) A, D & E supported by CSU document taken to Board on 25/10/2012, page 2 of attachment

manner.
• E) Provide details of the arrangements in place to assure the quality and completeness of finance and performance reports.
By 31 March 2013
• F) Describe the work done (having sought advice as appropriate from PCT clusters on best practice) to ensure that systems and processes are in place to support the production of its annual report and accounts for 2013/14.
• G) Report on local delivery of
QIPP as specified by the NHS Commissioning Board.
F & G) Actions by 31/03/2013 remain outstanding at this time

Financial governance framework element
An emerging CCG should be in a position to...
Evidence for authorisation
Completed Date
3. The CCG has effective financial planning arrangements and a detailed financial plan that is consistent with its commissioning strategy, setting out how it will manage within its management allowance and any other requirements set by the NHSCB. As part of their application for authorisation, CCGs will be expected to demonstrate that their running costs are within £25 per head.
At point of application
• A) Provide a clear operational financial plan developed for 2012/13 that demonstrates delivery of financial balance, cash management, QIPP targets, Operating Framework requirements and other key deliverables.
• B) Provide details of its
planned running costs for 2012/13 .
• C) Provide details of its
strategic planning and prioritisation process and how this relates to the financial planning process.
At point of application
• 2012-13 integrated plan (including a detailed financial plan) and draft commissioning intentions for 2013-14.
A & C) Finance to take MTFS to Board on 06/09 which should cover planning and process A & C) Need to evidence Integrated Plan and CSP for planning as well B) Details of running costs taken to CCG board 28/06/12 P:\Finance&Info\Financial Planning\Julie work in progress\Authorisation Finance Work\CCG Report on Running Costs for next 2 years.docx

Financial governance framework element
An emerging CCG should be in a position to...
Evidence for authorisation
Completed Date
4. CCG has effective financial management arrangements in place.
At point of application
• A) Provide clearly defined financial objectives for the CCG that are approved by the shadow CCG governing body.
• B) Provide clearly defined
shadow governing body level responsibility for financial management that is supported by clear lines of accountability throughout the organisation. This should include financial management processes that will be put in place to ensure QIPP delivery.
• C) Provide details of its
budgetary control framework, including staff establishment control processes.
• D) Provide details of
arrangements to validate provider activity data and information and assess
At point of application
• Constitution and any other documents detailing financial governance arrangements.
A D & E) Finance to take risk sharing paper which is SEL wide to Board on 25/09 (Risk Sharing Paper Item E pages 1-5, no other item included)(Financial Governance Paper, Item D, page 3, item d) Finance to take MTFS to Board on 06/09 which will cover objectives plus constitution C) Finance will outline budgetary control framework in paper for Board on 06/09 (Item C, page 2, item c) B) Please add as evidence the QIPP process (see PMO

implications.
• E) Provide details of the risk sharing arrangements that it has in place with other CCGs.
meetings), CCG structure, CFO and Head of QIPP JDs and CSS finance JDs

Financial governance framework element
An emerging CCG should be in a position to...
Evidence for authorisation
Completed Date
5. The CCG has clear internal audit arrangements. Internal audit is an important element of the financial governance framework that a CCG must put in place. It will provide the CCG with an independent and objective evaluation of the effectiveness of its risk management, control and governance processes and will propose improvements. Advice should be sought from the PCT cluster to help identify an appropriate supplier of internal audit services
At point of application
• A) Provide audit committee terms of reference.
• B) Provide role description for
the chair of the audit committee.
• C) Induction arrangements for
governing body members.
• D) Confirm intentions for obtaining a professional, high quality internal audit service.
By 31 December 2012
• E) Provide details of arrangements to deal with audit recommendations, including how the governing body is assured through monitoring of implementation and arrangements for escalation.
At point of application
• Constitution and any other documents detailing governance arrangements.
A, B and C) Audit committee Tor in draft being led by authorisation team as is the role of the Chair and the induction arrangements A supported by Financial Management Arrangements paper to Board 25/10/12, Financial Management Arrangements Overview Page 5 section 2.4 Standing orders pages 36-37 section 4 Audit & Integrated Assurance Committee terms of reference pages 106 to 114 Otherwise finance actions complete for point of application D) Confirmation of arrangements for internal audit service taken to CCG Board 28/06/12

By 31 March 2013
• F) Provide the draft service level agreement in place for provision of internal audit service.
• G) Provide outline internal
audit plans for 2013/14.
P:\Finance&Info\Financial Planning\Julie work in progress\Authorisation Finance Work\CCG Report on Finance for Authorisation - Front Sheet.doc (Item D, page 2/3, item h) D supported by CSU document taken to Board on 25/10/12, page 2 of attachment and Financial Management Arrangements paper to Board 25/10/12, Financial Management Arrangements Overview Page 7-8 Section 2.6/2.7 Prime Financial Policies Pages 97/98 sections 2 and 3 E) Details of arrangements to deal with audit recommendations to Board 25/09 (pages 1 and 2, no other items included) F and G) By March 2013 actions requested from

Cluster colleagues and information is awaited
6. The CCG has clear external audit arrangements. The Health and Social care Act 2012 (the Act) requires the audit of CCG accounts2. The NHS Commissioning Board will arrange for the Audit Commission to appoint auditors to CCGs. CCGs should make full use of the scope of the audit (which involves a financial statement audit and a value for money review) to help it better exercise its functions effectively, efficiently and economically.
At point of application
A) Provide Audit Committee terms of reference.
B) Provide role description for
the chair of the audit committee.
C) Confirm that they understand
external auditors will be appointed for the CCG by the Audit Commission under the Audit Commission Act 1998.
By 31 March 2013
D) Provide details of arrangements to deal with audit recommendations, including how the governing body is assured through monitoring of implementation and arrangements for escalation.
At point of application
• Constitution and any other documents detailing governance arrangements.
A & B) Audit Committee Tor in draft and being led by authorisation team as is the role of the Chair A supported by Financial Management Arrangements paper to Board 25/10/12, Financial Management Arrangements Overview Page 5 section 2.4 Standing orders pages 36-37 section 4 Audit & Integrated Assurance Committee terms of reference pages 106 to 114 Otherwise finance actions complete for point of application C) Confirmation of arrangements for external audit appointment taken to CCG Board 28/06/12 P:\Finance&Info\Financial Planning\Julie work in

progress\Authorisation Finance Work\CCG Report on Finance for Authorisation - Front Sheet.doc (Item C, page 3, item i) and Financial Management Arrangements paper to Board 25/10/12, Financial Management Arrangements Overview Page 7-8 Section 2.6/2.7 Prime Financial Policies Pages 97/98 sections 2 and 3
D) Details of arrangements to deal with audit recommendations to Board 25/09 (pages 1 and 2, no other items included)

Financial governance framework element
An emerging CCG should be in a position to...
Evidence for authorisation
Completed Date
7. The CCG has established a shadow audit committee and a shadow remuneration committee.
At point of application
• A) Provide shadow audit committee terms of reference.
• B) Provide shadow
remuneration committee terms of reference.
At point of application
• Constitution and any other documents detailing governance arrangements.
A & B) Audit committee Tor and the remuneration committee ToR both in draft and being led by authorisation team A supported by Financial Management Arrangements paper to Board 25/10/12, Financial Management Arrangements Overview Page 5 section 2.4 Standing orders pages 36-37 section 4 Audit & Integrated Assurance Committee terms of reference pages 106 to 114 No other finance input required for

this section
8. The CCG has clear financial arrangements for working with local authorities; and 9. The CCG has clear financial arrangements for handling hosted or shared activity. Domain 5 of the CCG authorisation: Draft guide for applicants sets the clear expectation that CCGs will put in place: “Collaborative arrangements for commissioning with other CCGs, local authorities and the NHS Commissioning Board as well as the appropriate commissioning support”3. The arrangements to support these relationships must include clear and transparent objectives and ways of working, agreed and understood by all parties.
At point of application
• A) List of joint commissioning draft agreements or plans, including pooled budgets and Section 75 agreements where appropriate.
• B) Written agreements in place
detailing the scope of the collaboration with other CCGs, with clear lines of accountability and decision-making processes.
By 31 March 2013
• C) Provide a policy for establishing hosting arrangements.
• D) Provide a policy for CCG
involvement in shared arrangements including specific provision for withdrawal.
• E) Provide a memorandum of
understanding (or equivalent) for hosted/shared activity.
At point of application
• Constitution and any other documents detailing governance arrangements.
• 2012-13
integrated plan and draft commissioning intentions for 2013-14.
• List of
collaborative commissioning arrangements, joint commissioning draft agreements or plans, including pooled budgets, Section 75 agreements where appropriate.
A) Need to add the list held by the authorisation team on Joint arrangements.
B) Need to add
the integrated plan and commissioning intentions (from Mike) as well as the JSNA and JHWS
Otherwise – no financial input required C, D, E & F) By 31/03/2013 arrangements, clarification is being sought as to whether

• F) Provide a risk assessment of
hosted arrangements.
• Draft joint
strategic needs assessment (JSNA).
• Draft joint health
and wellbeing strategy (JHWS).
• Local authority
views.
policies are required if we do not have any such arrangements and if not whether just reporting this fact to the Board would be sufficient to meet the authorisation requirements. A response is awaited. CSU MOU taken to Board 25/10/2012 – whole document applicable.
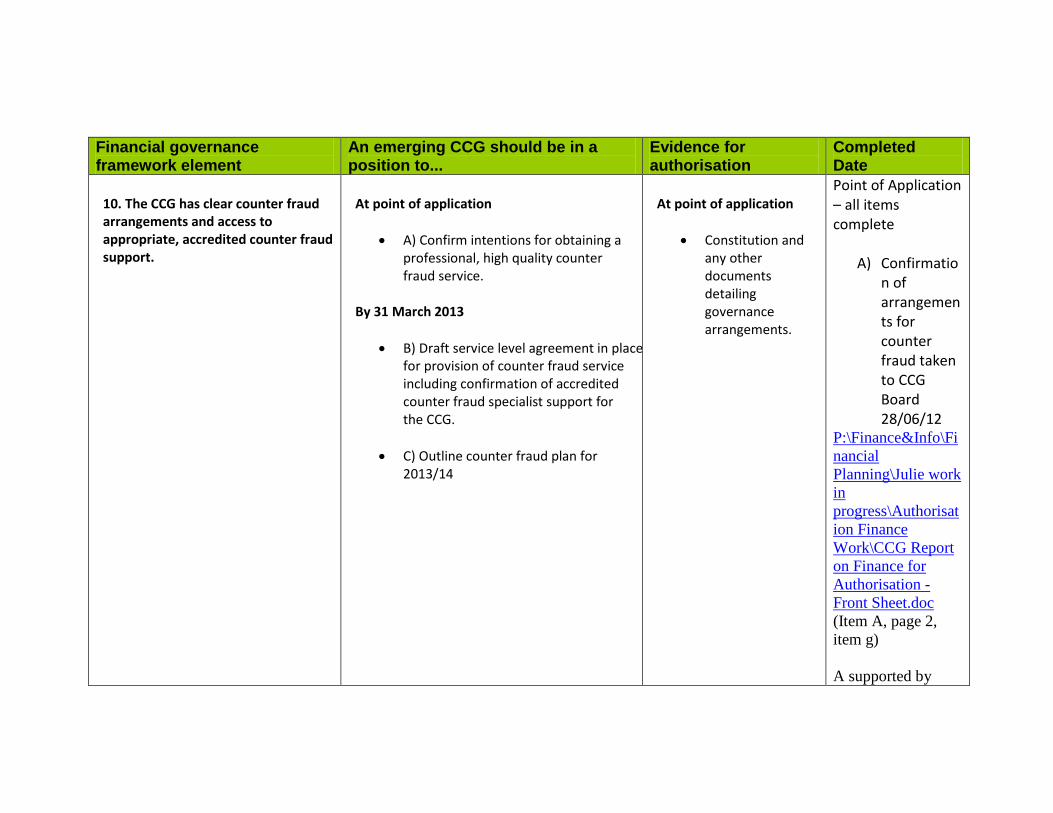
Financial governance framework element
An emerging CCG should be in a position to...
Evidence for authorisation
Completed Date
10. The CCG has clear counter fraud arrangements and access to appropriate, accredited counter fraud support.
At point of application
• A) Confirm intentions for obtaining a professional, high quality counter fraud service.
By 31 March 2013
• B) Draft service level agreement in place for provision of counter fraud service including confirmation of accredited counter fraud specialist support for the CCG.
• C) Outline counter fraud plan for
2013/14
At point of application
• Constitution and any other documents detailing governance arrangements.
Point of Application – all items complete
A) Confirmation of arrangements for counter fraud taken to CCG Board 28/06/12
P:\Finance&Info\Financial Planning\Julie work in progress\Authorisation Finance Work\CCG Report on Finance for Authorisation - Front Sheet.doc (Item A, page 2, item g) A supported by

CSU document taken to Board on 25/10/2012, page 3 of attachment A supported by Financial Management Arrangements paper to Board 25/10/12, Financial Management Arrangements Overview, page 8, section 2.8 plus Prime Financial Policies, page 92-93, section 4 B & C) By March 2013 actions requested from Cluster colleagues and information is awaited
11. The CCG can manage its charitable funds (where held) effectively. Where CCGs expect to hold charitable funds they must ensure they are managed and administered in line with
At point of application
• A) Confirm if the CCG will have any charitable funds and its arrangements for administering them.
At point of application
• Constitution and any other documents
Point of Application – all items completed

guidance issued by the Charities Commission.
detailing governance arrangements.
A) Confirmatio
n of arrangements for charitable funds taken to CCG Board 28/06/12
P:\Finance&Info\Financial Planning\Julie work in progress\Authorisation Finance Work\CCG Report on Finance for Authorisation - Front Sheet.doc (Item A, page 3, item j) Board paper on Financial Management Arrangements 25/10/2012, Financial Management Arrangements

Overview, page 9, section 4.3


















