
Final Report for PROJECT FOR IMPROVEMENT OF ...i Final Report for PROJECT FOR IMPROVEMENT OF HEALTH...
132
i Final Report for PROJECT FOR IMPROVEMENT OF HEALTH SERVICE WITH A FOCUS ON SAFE MOTHERHOOD IN KISII AND KERICHO DISTRICTS March 2008 Submitted by HANDS (Health and Development Service) Report No. HANDS/ XIII / 2008 Period covered from 24 th March 2005 to 31 st March 2008
Transcript of Final Report for PROJECT FOR IMPROVEMENT OF ...i Final Report for PROJECT FOR IMPROVEMENT OF HEALTH...
i
Final Report for PROJECT FOR IMPROVEMENT OF
HEALTH SERVICE WITH A FOCUS ON SAFE MOTHERHOOD IN
KISII AND KERICHO DISTRICTS
March 2008
Submitted by
HANDS
(Health and Development Service)
� � � �
Report No. HANDS/ XIII / 2008 Period covered from 24th March 2005 to 31st March 2008
Final Report SAMOKIKE March 2008
iii
CONTENTS
INTRODUCTION..........................................................................................................................................�MAPS ..............................................................................................................................................................�PROJECT SITE .............................................................................................................................................�PROJECT PHOTOS......................................................................................................................................�LIST OF ABBREVIATONS .........................................................................................................................xi
EXECUTIVE SUMMARY............................................................................................................................1
CHAPTER 1. OVERVIEW OF THE PROJECT .......................................................................................3
� 1.1 Background................................................................................................................................... 3 � 1.2 Target Population, Implementation Period, and Activities ...................................................... 3 � � 1.2.1 Target Population.................................................................................................................. 3 1.2.2 Implementation Period ................................................................................................................. 4 1.3 Organizational Structure................................................................................................................. 5 1.3.1 Project Counterpart ...................................................................................................................... 5 1.3.2 Office Management ....................................................................................................................... 6 1.3.3 Networking..................................................................................................................................... 8
Chapter 2. Project Achievements..................................................................................................................10
2.1 Survey Conducted by the Project ...........................................................................................................10 2.2 Outputs of the Project ............................................................................................................................11 2.2.1 Output 1 .................................................................................................................................................12 2.2.2 Output 2 .................................................................................................................................................18 2.2.3 Output 3 .................................................................................................................................................29 2.2.4 Output 4 .................................................................................................................................................32 2.2.5 Output 5 .................................................................................................................................................37 2.3 Project Input.............................................................................................................................................39 2.3.1 Expenditure of Project..........................................................................................................................392.3.3 Provision of Equipment ........................................................................................................................40 2.3.4 Facilities .................................................................................................................................................41 2.4 Achievement of Overall Goal ..................................................................................................................42 2.4.1 Factors Contributed to Achieve the Project Purpose.........................................................................42 2.4.2 Achievement of Project Purpose ..........................................................................................................43 2.4.3 Towards the Achievement of Overall Goal .........................................................................................43
Chapter 3. Recommendations and Lessons Learned for Future ...............................................................44
3.1 Recommendations and Lessons Learned ...............................................................................................44 3.2 Way Forward............................................................................................................................................45
Chapter 4. History of Project Design Matrix...............................................................................................47
Chapter 5. Appendices...................................................................................................................................49

Final Report SAMOKIKE March 2008
i
INTRODUCTION�
Health and Development Service (HANDS) in collaboration with the Japan International Cooperation Agency(JICA) and the Ministry of Health (MoH) of Republic of Kenya, initiated the “Project for Improvement of Health Services with a Focus on Safe Motherhood in Kisii and Kericho Districts”; SAveMOthers in KIsii and KEricho (SAMOKIKE Project). The Project was implemented for three years from March 2005 to March 2008.
Under its “National Health Sector Strategic Plan (1999-2000)”, the MoH had aimed to establish the referral system from the primary health facilities such as Health Centre (HC) to the secondary health facilities such as District Hospitals. Then, the MoH planned “The Second National Health Sector Strategic Plan (2001-2005)” to reducing the maternal mortality rate, increasing the skilled birth attendance rate, and improving the antenatal care with emphasis on the primary health facilities near the community. In Japan, on the other hand, “Healthcare and Development Initiative (HDI)” was announced in June 2005 emphasizing MDGs relating health. This was aimed to support the development of infrastructure for healthcare management, with special emphasis on strengthening the healthcare system, developing and strengthening of the healthcare facilities, and assisting the capacity building of health workers.
Since 2000, JICA has been extending support to western Kenya such as rehabilitation program at District Hospitals and HCs. SAMOKIE project has been positioned as the extension of JICA initiatives mentioned above to strengthening the healthcare services.
The Project can be distinguished from other technical assistance projects by several characteristics. First, this is a PROTECO (Proposed-Type Technical Cooperation Project�that incorporates strength of both JICA and NGO creating synergy between the government policy and the grass-root activity. In addition, this Project has attempted to achieve the synergy by combining the horizontal approach of improving HC system and the vertical approach of improving maternal care services.
It has been a challenge to achieve these broad goals in three years. The social confusion after the presidential election of December 2007 had significantly affected SAMOKIKE project activities in its final phase. Still, in the final evaluation, lessons learned from the Project were strongly recommended as meaningful to the foregoing policy-making in the community-led improvement of the quality of healthcare system.
Next year, Kisii and Kericho District Hospitals are scheduled to be renovated for better functionality financially supported by JICA donation. We believe further activities creating synergies will continue towards the future.
Tamayo Haraguchi Chief Advisor
JICA/HANDS/MOH SAMOKIKE Project

Final Report SAMOKIKE March 2008
ii
MAPS
Final Report SAMOKIKE March 2008
iii
Project Site
Map: Kisii District, Nyanza Province
�
�

Final Report SAMOKIKE March 2008
iv
�
Map: Kericho District, Rift Valley Province �

Final Report SAMOKIKE March 2008
v
Project Photos
1. Maternal Care
1. HC Renovation�Supplying water tanks � � � �
Ibeno HC, Kisii��
2. Provision of medical equipment�Adult weighing scaleChepkemel HC,Kericho�
�
3. Essential Obstetric Care Training�Professionalmaternal care trainings for midwife (Kisii DH)
4. Kakamega Study Tour�Studying referral system in Kakamega District
5. Partners Workshop�Group work of HC staff, community representativesKisii�
�Partners Workshop�Pregnant woman experienceKericho��
Final Report SAMOKIKE March 2008
vii
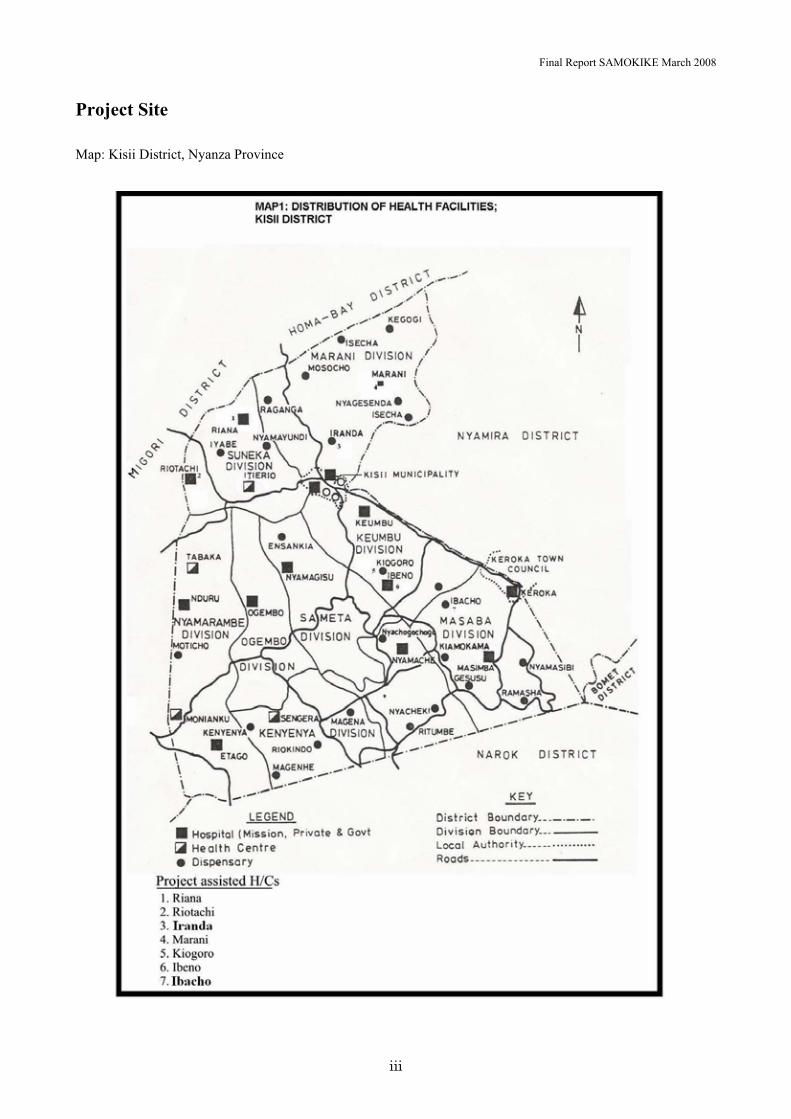
2. Health Centre Management
1. Provison of multi-purpose vehicles to Kisii and Kericho districts
2. Study tour to TanzaniaMorogoro region�participated by DHMT members of Kisii and Kericho districts
3. Monitoring of 5S1K impelmenation by DHMT member (Riana HC, Kisii�
4. 5S1K Workshop at pilot HC (Chepkemel HC, Kericho�
5. Utilizaion of HIS Board Riana HC, Kisii�
6. Supervison to HCs for HIS improvement by DMRIOsSigowet HC, Kericho�

Final Report SAMOKIKE March 2008
ix
3.Community Activities
1. Community Activity Meeting�Discussion of Action Plan by HC staff and Community RepresentativesKericho�
2. Community Led Community Meetings at HCRiotanchi HC, Kisii�
�
�
3. Community Campaign�Procession(Kipkelion HC, Kericho��
4. Community Campaign � A man wearing Maternity Jacket (Riana HC, Kisii�
5. Community phones managed by the communityRiotanchi HC, Kisii�
6. IGA�Planting corn within the empty space of the HC (Kipkelion HC, Kericho�
Final Report SAMOKIKE March 2008
xi
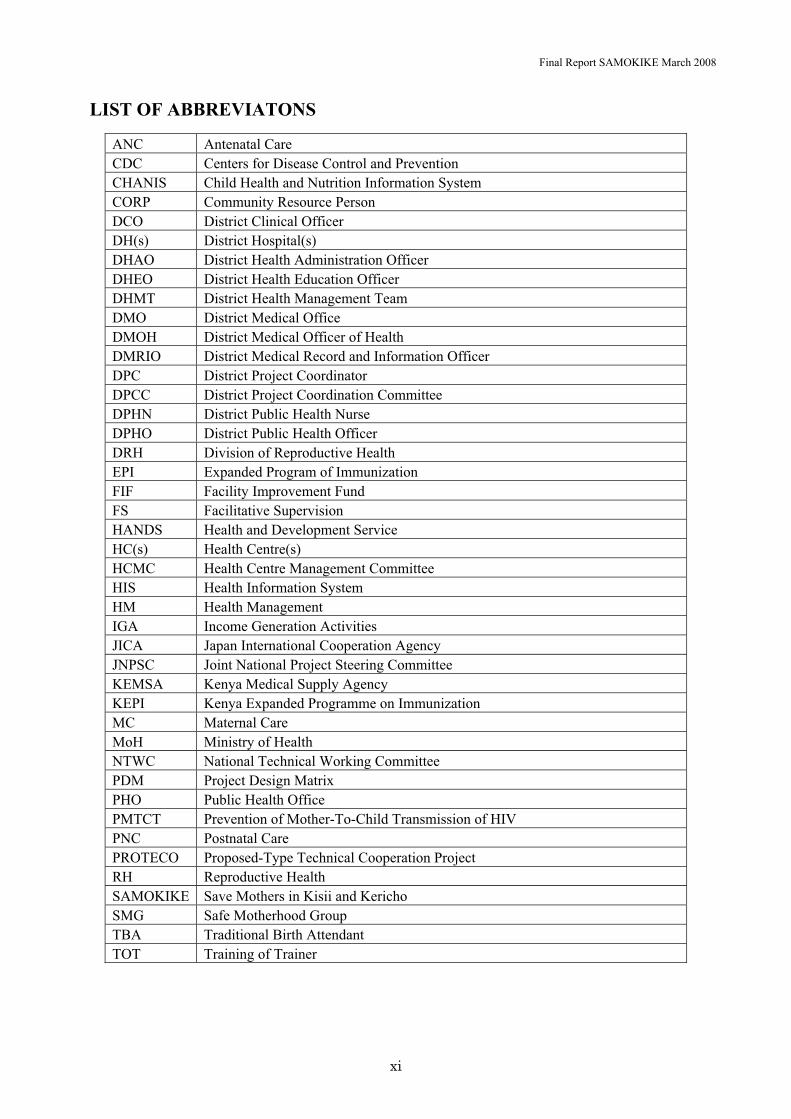
� LIST OF ABBREVIATONS
ANC Antenatal Care CDC Centers for Disease Control and Prevention CHANIS Child Health and Nutrition Information System CORP Community Resource Person DCO District Clinical Officer DH(s) District Hospital(s) DHAO District Health Administration Officer DHEO District Health Education Officer DHMT District Health Management Team DMO District Medical Office DMOH District Medical Officer of Health DMRIO District Medical Record and Information Officer DPC District Project Coordinator DPCC District Project Coordination Committee DPHN District Public Health Nurse DPHO District Public Health Officer DRH Division of Reproductive Health EPI Expanded Program of Immunization FIF Facility Improvement Fund FS Facilitative Supervision HANDS Health and Development Service HC(s) Health Centre(s) HCMC Health Centre Management Committee HIS Health Information System HM Health Management IGA Income Generation Activities JICA Japan International Cooperation Agency JNPSC Joint National Project Steering Committee KEMSA Kenya Medical Supply Agency KEPI Kenya Expanded Programme on Immunization MC Maternal Care MoH Ministry of Health NTWC National Technical Working Committee PDM Project Design Matrix PHO Public Health Office PMTCT Prevention of Mother-To-Child Transmission of HIV PNC Postnatal Care PROTECO Proposed-Type Technical Cooperation Project RH Reproductive Health SAMOKIKE Save Mothers in Kisii and Kericho SMG Safe Motherhood Group TBA Traditional Birth Attendant TOT Training of Trainer

Final Report SAMOKIKE March 2008
1
Executive Summary
The overall goal of the Project was to improve the health condition, particularly the maternal health in the Kisii and Kericho Districts. The Project purpose was to improve the maternal care in the project areas with a focus on health centres (HCs) and communities and the Project activities were planned to achieve the following five outputs; � Output 1: Maternal care services at the HCs are upgraded. � Output 2: Management support in the HCs is improved � Output 3: District Health Management Teams (DHMTs)’ system for their supportive
supervision for HCs is strengthened. � Output 4: Maternal care at the community level is improved � Output 5: A referral system is arranged and functioning between communities, HCs and �
District Hospitals (DHs).
In order to achieve broad aspects of outputs, the Project activities was implemented within three different target levels; District Medical Office (DMO), HC, and community. Through the three-year activities, we conducted minor renovation of HC facilities, provided medical equipment for maternal care, and built the capacity of health staff. In addition, SAMOKIKE project strengthened cooperation among community and health facilities, organizing role building at the three target levels. As a result, it has led to achieve improved health care service at HCs and communities focusing on maternal care.
Especially, implementation of Partners Workshop, 5S1K trainings at HCs, and Community Campaign were the activities that have achieved highest impacts. For example, Partners Workshop was epoch-making that it has provided training opportunity simultaneously to both HC workers and the community, resulting in strengthening mutual understanding and coordination between community and HC staffs. Staffs of DMO, DH, and HC learned together the basic methodology of 5S1K as a tool for understanding basic management of healthcare system, and its activities were implemented at all HCs under the supervision of DMO. In addition, through the series of community activities, HC staff and community members cooperated and organized successful Community Campaign in the final year.
In the final evaluation, SAMOKIKE project results was highly regarded for creating positive impacts among different levels, which lesson can be disseminated to other projects. However, the Project did not have enough time and resources to fully achieve all the various goals set up in PDM. Especially, the supervision of DMO and the improvement of referral system remain unfulfilled because of limited human resources in health facilities and government budget.
Unfortunately, the Project in its last half of the final year was affected by the social confusion after the presidential election. Western Kenya, project’s target region, was restricted from transportation, and Japanese staff could not operate. As a result, dissemination seminar was cancelled which was aimed to promote impacts of the achievements of the Project to other region in order to maintain its sustainability. Despite the influence of external conditions, however, SAMOKIKE project produced a technical report on

Final Report SAMOKIKE March 2008
2
the achievements and lessons learned and conducted Dissemination Preparation Training so that when the confusion is resolved, the MOH may utilize and take initiative to conduct dissemination seminars.

Final Report SAMOKIKE March 2008
3
CHAPTER 1. OVERVIEW OF THE PROJECT
1.1 Background
Western Kenya (Nyanza province and part of Rift Valley Province) is challenged by high prevalence of infectious diseases including malaria and HIV/AIDS, low social capital compared to a large population, and the deterioration of health facilities. Under these conditions, Kenyan government established “The National Health Sector Strategic Plan 1999-2004”. This Plan prioritized on decentralization and appropriate allocation of human resources, aiming to improve health service at the regional level by establishing referral system from the primary health facilities such as Health Centres (HCs) to the secondary health facilities such as District Hospitals (DH), as well as strengthening management capacity of medical supplies and equipment usage.
The maternal mortality rate in Kenya is reported to be 1,000 per 100,000 births (WHO, UNICEF, UNFPA. 2000), among the highest in the world. The causes of high maternal mortality rate result from pregnancy-related complication such as postpartum hemorrhage. These are due to the inappropriate awareness of a pregnant woman or a traditional birth attendant (TBA) to detect danger signs, lack of basic maternal care (MC) service or referral system at the primary health facilities such as HCs, and the inability of the hospitals to offer speedy and appropriate maternal care.
No data on the maternal mortality rate of the project target region is available, but data indicates that in-facility delivery of the two target Provinces is 36.0%, which is lower than the national average of 40.1% (Kenya Demographic and Health Survey 2003). Given that more than 50% of deliveries take place at home, the need is high in increasing the delivery rate at the facility attended by medical certificate holders (doctors, clinical officers, and nurses/midwives) and in strengthening the linkage between communities and primary health facilities.
SAMOKIKE Project was initiated in western Kenya (Kisii District, Nyanza Province and Kericho District, Rift Valley Province) to improve maternal care in the target regions through strengthening HC management, upgrading maternal care at the HC and community levels, and encouraging community involvement, thereby ultimately contributing to the health of pregnant women and their community.
1.2 Target Population, Implementation Period, and Activities
1.2.1 Target Population
The total population of Kisii and Kericho Districts was approximately 1,000,000 (Kisii 500,000, Kericho 500,000). In particular, SAMOKIKE project targeted 7 HCs in each District, total of 14 HCs, and surrounding residents of approximately 260,000.
In 2007, some of the target HCs became under the administrative rule of new Districts due to a governmental
Final Report SAMOKIKE March 2008
4
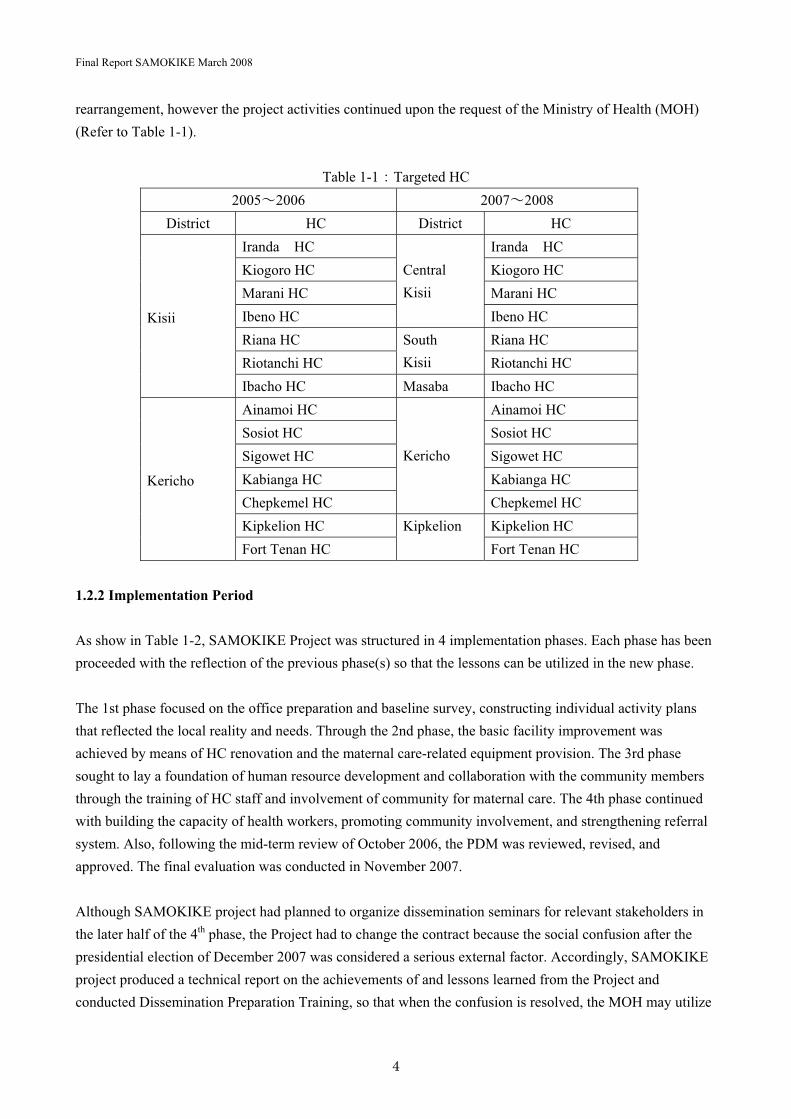
rearrangement, however the project activities continued upon the request of the Ministry of Health (MOH) (Refer to Table 1-1).
Table 1-1�Targeted HC 2005�2006 2007�2008
District HC District HC Iranda� HC Iranda� HCKiogoro HC Kiogoro HC Marani HC Marani HC Ibeno HC
�
CentralKisii� Ibeno HC
Riana HC Riana HC Riotanchi HC
SouthKisii Riotanchi HC
�
�
�
Kisii�
�
� Ibacho HC Masaba Ibacho HC Ainamoi HC Ainamoi HC Sosiot HC Sosiot HC Sigowet HC Sigowet HC Kabianga HC Kabianga HC Chepkemel HC
�
�
Kericho�
� Chepkemel HC Kipkelion HC Kipkelion HC
�
�
Kericho�
�
� Fort Tenan HC Kipkelion
Fort Tenan HC
1.2.2 Implementation Period
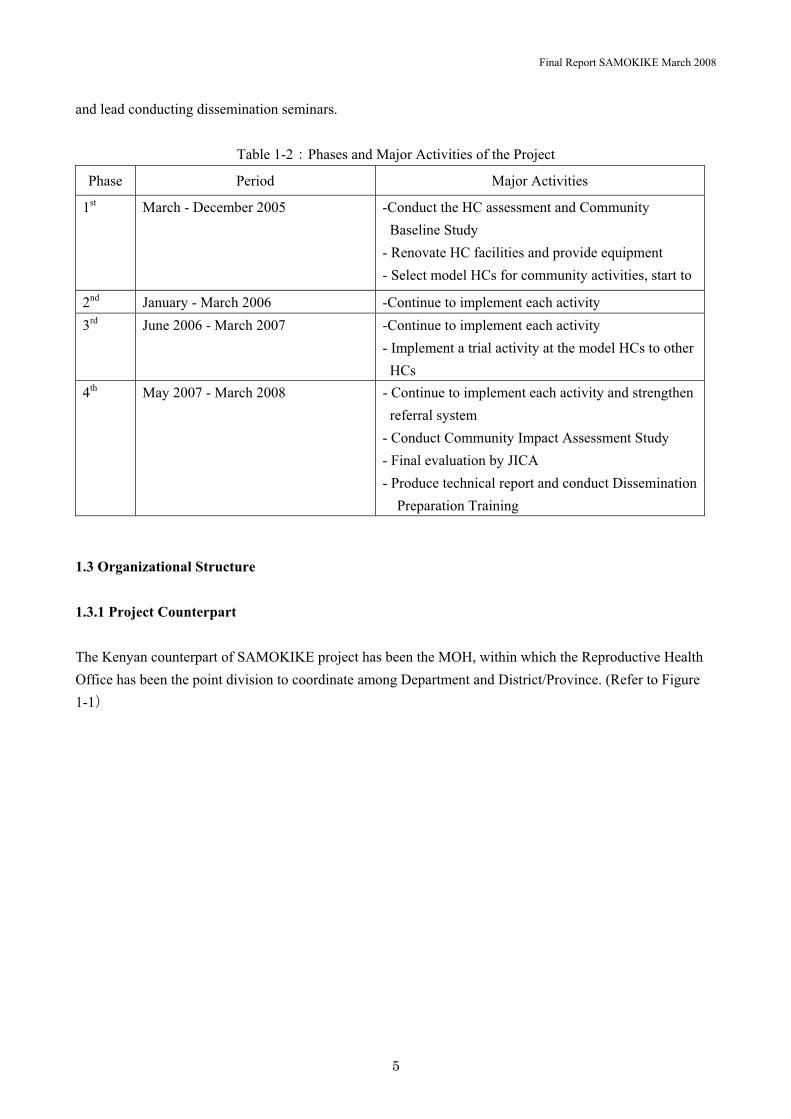
As show in Table 1-2, SAMOKIKE Project was structured in 4 implementation phases. Each phase has been proceeded with the reflection of the previous phase(s) so that the lessons can be utilized in the new phase.
The 1st phase focused on the office preparation and baseline survey, constructing individual activity plans that reflected the local reality and needs. Through the 2nd phase, the basic facility improvement was achieved by means of HC renovation and the maternal care-related equipment provision. The 3rd phase sought to lay a foundation of human resource development and collaboration with the community members through the training of HC staff and involvement of community for maternal care. The 4th phase continued with building the capacity of health workers, promoting community involvement, and strengthening referral system. Also, following the mid-term review of October 2006, the PDM was reviewed, revised, and approved. The final evaluation was conducted in November 2007.
Although SAMOKIKE project had planned to organize dissemination seminars for relevant stakeholders in the later half of the 4th phase, the Project had to change the contract because the social confusion after the presidential election of December 2007 was considered a serious external factor. Accordingly, SAMOKIKE project produced a technical report on the achievements of and lessons learned from the Project and conducted Dissemination Preparation Training, so that when the confusion is resolved, the MOH may utilize
Final Report SAMOKIKE March 2008
5
and lead conducting dissemination seminars.
Table 1-2�Phases and Major Activities of the Project
Phase Period Major Activities
1st March - December 2005 -Conduct the HC assessment and Community Baseline Study
- Renovate HC facilities and provide equipment - Select model HCs for community activities, start to
2nd January - March 2006 -Continue to implement each activity 3rd June 2006 - March 2007 -Continue to implement each activity
- Implement a trial activity at the model HCs to other HCs
4th May 2007 - March 2008 - Continue to implement each activity and strengthen referral system
- Conduct Community Impact Assessment Study - Final evaluation by JICA - Produce technical report and conduct Dissemination
Preparation Training
1.3 Organizational Structure
1.3.1 Project Counterpart
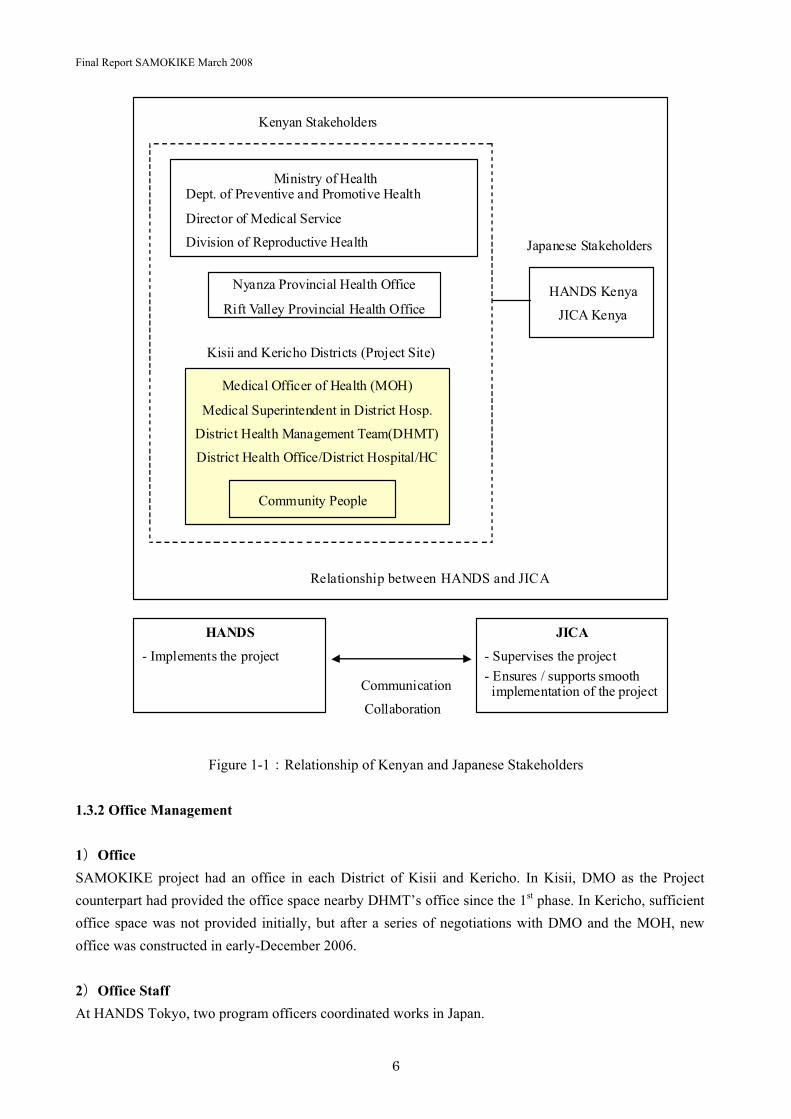
The Kenyan counterpart of SAMOKIKE project has been the MOH, within which the Reproductive Health Office has been the point division to coordinate among Department and District/Province. (Refer to Figure 1-1�
Final Report SAMOKIKE March 2008
6
Figure 1-1�Relationship of Kenyan and Japanese Stakeholders
1.3.2 Office Management
1�OfficeSAMOKIKE project had an office in each District of Kisii and Kericho. In Kisii, DMO as the Project counterpart had provided the office space nearby DHMT’s office since the 1st phase. In Kericho, sufficient office space was not provided initially, but after a series of negotiations with DMO and the MOH, new office was constructed in early-December 2006.
2�Office Staff At HANDS Tokyo, two program officers coordinated works in Japan.
Ministry of HealthDept. of Preventive and Promotive Health
Director of Medical Service
Division of Reproductive Health
Medical Officer of Health (MOH)
Medical Superintendent in District Hosp.
District Health Management Team(DHMT)
District Health Office/District Hospital/HC
Community People
HANDS Kenya
JICA Kenya
HANDS
- Implements the project
JICA
- Supervises the project - Ensures / supports smooth
implementation of the project
Kisii and Kericho Districts (Project Site)
Kenyan Stakeholders
Japanese Stakeholders
Nyanza Provincial Health Office
Rift Valley Provincial Health Office
Communication
� Collaboration
Relationship between HANDS and JICA

Final Report SAMOKIKE March 2008
7
In Kisii office, in addition to one Japanese coordinator since the 2nd phase, there was four to five Kenyan staff. In Kericho office, there was a total of five to six Japanese staff including a chief advisor, an administrative coordinator, and three or four technical experts, and four to six Kenyan staff. (Refer to Table 1-3, Figure 1-2�
Two technical assistants who were seconded to this Project each from DMO of Kisii and Kericho continued their duties at the Project offices while Japanese experts did not reside.
In the small cities of Kisii and Kericho where recruitment was usually difficult, SAMOKIKE project extended hiring efficient staff from the previous phase for the smooth project implementation.
In each phase, the Kenyan Labor Law was respected in every step of the hiring process with every employee, with the assistance from the legal team of JICA Kenya in reviewing employment agreements. Two of these employees had been seconded from DMO of Kisii and Kericho since the 1st phase.
Table1-3�List of HANDS Kenyan Staff Total Number of Staff
Position1st Phase 2nd Phase 3rd Phase 4th Phase
Kericho Office - Technical Assistant 1 1 3 3 - Secretary 2 1 1 0 - Assistant Coordinator 0 0 0 1 - Driver 1 2 2 2 - Technical Assistant on Community
Phone0 0 0 1
Kisii Office - Technical Assistant 1 1 2 2 - Secretary 1 1 1 1 - Driver 1 1 1 1 - Technical Assistant on Community
Phone0 0 0 1

Final Report SAMOKIKE March 2008
8
Figure 1-2�Project Team Organization
1.3.3 Networking
As mentioned before, SAMOIKIE project worked in a partnership with the MoH. The Project had organized Project Steering Committee together with the MoH for information sharing and discussions to organize, plan, and implement the Project (Refer to Appendix 1-3). In each phase, the Project presented its plan and activity report to the MoH, whose opinions were reflected to the next phase (Refer to Appendix 6). After 2007, amidst the decentralization movement, the Project sought to strengthen the coordination with
������������� ��
������������ ��
������ �������� ���
�����������
������������� ��
!�����������"#�$
!���� ���
"��%��
������� &������
������������� �� ��
������� ������
�������%����
'�(������)(�� � ������� ���
*�+"!��,���
������ �������� ��
������ �������� ��-
�������������
����� �� �������� ��
������������� ��
������������ ��
����������%������
#� ���������#��.����
����������%������
*�� �#���/����
����������%������"��/
#���/����
����������%������
������� �*�� �
������������� ��
!�����������"#�$
������������� �� ��
������� ������
"��%��
�*�+"!&������
"��%��
������� &�������

Final Report SAMOKIKE March 2008
9
the Districts and started producing Project Monthly Report in the 4th phase and visiting MoH office at Provincial and National level regularly. In Nyanza Province, the Stakeholder Meeting requested the Project to present its activities, contributing to the dissemination of the Project achievements.
1) Meeting led by the MoH a)� Joint National Project Steering Committee (JNPSC): 5 times
-A committee to discuss mainly management and policy issues. -Members consisted of the Ministry of Finance, Permanent Secretary in MoH, Director of
Medical Service, Head of Promotion and Prevention department, Head of Division of Reproductive Health, JICA representative, and HANDS representative
b)� National Technical Working Committee (NTWC): 6 times -A committee to discuss mainly planning of project implementation. -Members consisted of Head of Promotion and Prevention Department, Head of Division of
Reproductive, Provincial Medical Officer of Health (Nyanza Province, Rift Valley Province), District Medical Officer of Health (Kisii Districts, Kericho Districts), JICA project manager, and HANDS project staff
2) Meeting led by the Project a)� District Project Coordination Committee (DPCC): 12 times
� -A committee to discuss mainly project activities. -Members consisted of DHMT (Kisii Districts, Kericho Districts), and HANDS project staff
HANDS also established a strong network with other organizations and have built capacity development through conducting trainings facilitated by local NGOs such as Aga Khan Health Services and Engender.
Final Report SAMOKIKE March 2008
10
Chapter 2. Project Achievements
SAMOKIKE Project used the Project Design Matrix (PDM) to design goals to which activities were planned and implemented. This chapter first gives the overview of the surveys SAMOKIKE project conducted (Refer to session 2-1). Next it describes for each targeted output as follows; a) summary of relevant activities, b) achievements of indicators, c) review and recommendations (Refer to session 2-2). Then, the list of equipment and facilities that SAMOKIKE project provided are mentioned (Refer to session 2-3).Finally, achievements of the Project’s overall goal and purposes are discussed (Refer to session 2-4).
2.1 Survey Conducted by the Project
SAMOKIKE project conducted surveys at the 1st phase and at the middle-to-end of the 4th phase on each area of Maternal Care (MC), Health Management (HM), and Community Activities (CA). Major surveys were as shown in Table 2-1. The results of these surveys were very useful when it was necessary to review and evaluated activities of SAMOKIKE project.
Table 2-1�Summary of Project Surveys
Year Survey Content Target/Method
Maternal Care Related 2005 � HC Assessment
Survey� Types of services � Amount and condition of
medical equipments
� Amount and condition of storage
� Maternal record keeping
� Visits by HANDS experts � Interview with HC staff by
HANDS experts.
� Interview with DHMT members
2007 � Assessment on Emergency Preparedness
� Delivery kit maintenance at HC delivery room
� Visit by HANDS experts, Kenyan staffs
2007 � Assessment on staff allocation
� Number of staff at each HC
� HC staff completing a survey form� Interview with DPHN
2007 � Maternal care Follow up
� Maternal care training evaluation
� Delivery kit maintenance at HC delivery room
� Campaign evaluation
� Visit by HANDS experts, Kenyan staffs, and DPHN
2007 � Case study on Referral cases
� Utilization and evaluation of referral form
� Review of referral form at DH/HC and interview with nurse
Health Management Related
2005 � HC Assessment � HC Generally � Visit by HANDS experts
Final Report SAMOKIKE March 2008
11
2007 Survey � HC facilities generally � HCMC activities � Referral generally � HIS status at HC � Maintenance of drug and
medical supplies
� Status of DHMT supervision
� Interview by HANDS experts with HC staff
� Interview with DHMT members
2007 � 5S1K Performance Assessment
� Status of 5S1K within HC using checklist
� Visit by DPHN to HC � Visit and interview by DPHN with
HC staff
2007 � HISPerformance Assessment
� Quality of 5 Monthly Reports using checklist
� Status of HIS at HC (mainly filing, utilization of HIS board and referral stamp)
� Confirmation of DMRIO report using checklist
� Visit HC by DMRIO
Community Activity Related
2005 � Community Assessment Survey
2007 � Community Impact Assessment Survey
� Opinion and knowledge of community member on delivery and child care
� Satisfaction on ANC, delivery service at HC and utilization
� Ability towards SMG by other community members, capacity ability of HC
� Interview with key informant � Household interview � Focus group discussion � Direct observation
(By Almaco Management Consultants Ltd�
2007 � Interview on HCMATERNAL CARE and SMG
� Status of HCMC, SMG, activities,
� changes before and after SAMOKIKE project
� Interview by HANDS experts, with HC staff and HCMC
2.2 Outputs of the Project
The following sections summarize the Project’s outputs, their relevant activities, achievements, and review and recommendations. Refer to Appendix 1 for details about the program and the number of participants for the training, workshop and meetings. (Appendix 1-1.“Training and Workshop”, Appendix 1-2. “Community Meeting and Campaign”, Appendix 1-3. “Maternal Care and Stakeholder Meeting”). 2.2.1 Output 1
Final Report SAMOKIKE March 2008
12
Output 1 “Maternal Care at the HCs are Upgraded” Indicators�� Increase in the number of HC and HC staff (rate) providing skilled delivery attendance � Number of Maternal Death Review (MDR) � Number of staff completed training within each HC � Number of follow-ups, staff receiving follow-ups, and evaluation of work performed by trained
staff.� Communities satisfaction level of the quality of care � Number of HC maintaining facilities and equipment 1and 2 years after their installation � Number of staff attended maintenance training and the frequency of regular maintenance Related Project Activities�� HC Renovation � Medical equipment provision � Essential obstetric care training (National Package training) � Maternal care training (Partners Workshop) � Medical equipment training
Summary of related activities 1) HC Renovation1st and 2nd phases�SAMOKIKE project renovated 10 out of 14 HCs which had not been renovated previously by JICA. The renovations included reconstructions of broken walls, making drainage trenches, supplying water tanks and generators. These renovations were essential for providing maternal care especially delivery services. The Project involved Community Representatives, who monitored the process of the renovations.
2) Providing medical and non-medical equipment (2nd phase) Medical equipment necessary for maternal care was provided to the targeted HC and DH, including diagnostic set (sphygmomanometer, thermometer, weighing scale, and fetoscope), delivery set (kidney dishes, forceps, cord scissors), and other equipment (delivery bed, sterilizer, and oxygen concentrator). The type and amount of equipment were decided on the result of the baseline survey and discussions with DHMT members.
3) Essential Obstetric Care Training (National Package Training) (3rd phase) SAMOKIKE project conducted the training in collaboration with Reproductive Health Team (RHT) members from central, provincial and district levels. Central MOH provided the training materials such as Power Point (PPT) and textbooks, and the representative of RHT members from two provinces and two districts facilitated the training. The training was held for 10 days covering broad maternal care skills including ANC, delivery care, PNC, neonatal care, management of complications of pregnancy, and infection prevention (including HIV/AIDS). Totally 24 midwives from 14 HCs, District Hospitals and Sub District Hospitals were trained.
Final Report SAMOKIKE March 2008
13
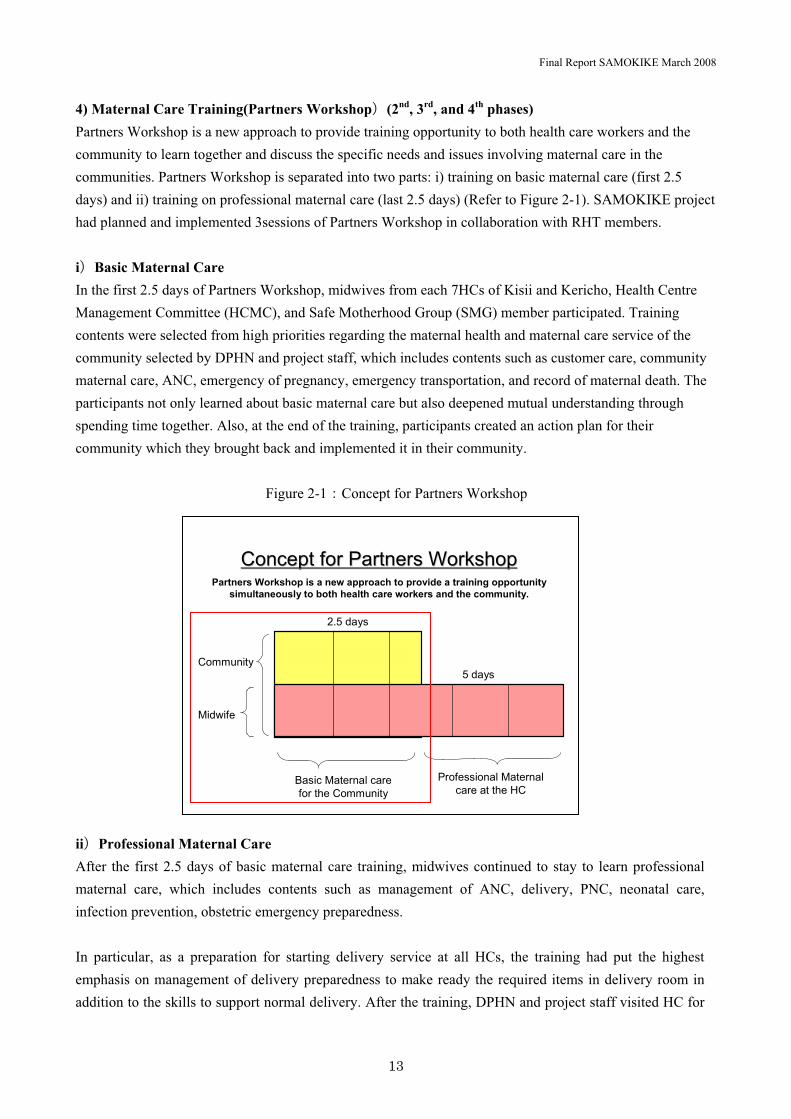
4) Maternal Care Training(Partners Workshop�(2nd, 3rd, and 4th phases) Partners Workshop is a new approach to provide training opportunity to both health care workers and the community to learn together and discuss the specific needs and issues involving maternal care in the communities. Partners Workshop is separated into two parts: i) training on basic maternal care (first 2.5 days) and ii) training on professional maternal care (last 2.5 days) (Refer to Figure 2-1). SAMOKIKE project had planned and implemented 3sessions of Partners Workshop in collaboration with RHT members.
i�Basic Maternal Care In the first 2.5 days of Partners Workshop, midwives from each 7HCs of Kisii and Kericho, Health Centre Management Committee (HCMC), and Safe Motherhood Group (SMG) member participated. Training contents were selected from high priorities regarding the maternal health and maternal care service of the community selected by DPHN and project staff, which includes contents such as customer care, community maternal care, ANC, emergency of pregnancy, emergency transportation, and record of maternal death. The participants not only learned about basic maternal care but also deepened mutual understanding through spending time together. Also, at the end of the training, participants created an action plan for their community which they brought back and implemented it in their community.
Figure 2-1�Concept for Partners Workshop
ii�Professional Maternal Care After the first 2.5 days of basic maternal care training, midwives continued to stay to learn professional maternal care, which includes contents such as management of ANC, delivery, PNC, neonatal care, infection prevention, obstetric emergency preparedness.
In particular, as a preparation for starting delivery service at all HCs, the training had put the highest emphasis on management of delivery preparedness to make ready the required items in delivery room in addition to the skills to support normal delivery. After the training, DPHN and project staff visited HC for
Community
Midwife
Basic Maternal care for the Community
Professional Maternal care at the HC
2.5 days
5 days
Concept for Partners WorkshopConcept for Partners WorkshopPartners Workshop is a new approach to provide a training opportunity
simultaneously to both health care workers and the community.

Final Report SAMOKIKE March 2008
14
follow-ups.
5) Medical Equipment Training (4th phase)In the 2nd phase, SAMOKIKE project provided medical equipment required for maternal care to each HC and DH. In addition, in the 4th phase, the Project conducted training on equipment which requires maintenance such as adult and child weighing scale, oxygen concentrator, autoclave, sphygmomanometer (BP machine) and electric fetoscope The Project invited a facilitator from a company based in Nairobi (CROWN Health Care) from which SAMOKIKE project bought these equipment. The training covered purposes, basic usage, and maintenance of equipment.
Achievement of indicators 1) Number of HC and HC staff (rate) providing skilled delivery attendanceThere were 5 HCs that began to provide delivery services during the Project, and now all 14 HCs are ready to provide delivery services. In addition, 13 out of 14 HCs presently are capable of 24 hour delivery service. According to pre and post test from all three Partners Workshop conducted, every participant (HC midwives) got higher score compared to the pre test. (Refer to Table 2-2). In addition, the number of skilled midwives in the 4th phase increased from the average of 4.8 to 5.1 in Kisii and remained flat at 3.6 in Kericho from the survey. Despite the increase in Kisii, this number far lags the minimum of 8 staff per HC which the Kenyan government specifies and further improvement is required. (Refer to Table 2-3).
Table 2-2�Results of Pre-post tests of Partners Workshop (Professional Maternal Care)

Final Report SAMOKIKE March 2008
15
�� ID 1 2 3 4 5 6 7 8 9 10 11 12 Average Highest Lowest
Pre % 49 39 44 50 59 50 63 59 61 44 56 54 52 63 39Post % 75 70 66 76 71 71 68 77 82 74 80 79 74 82 66Balance 26 31 23 26 12 20 5 18 21 30 24 25 22 19 28Pre % 51 63 54 56 59 40 51 61 50 60 54 56 54 63 40
Post % 67 71 79 66 71 74 62 78 65 88 79 75 73 88 62Balance �0 1 -2 �� �3 34 �� �5 �2 -1 -2 �6 �1 -2 --
-��ID 1 2 3 4 5 6 7 8 9 10 11 12 Average Highest Lowest
Pre % 0� 0- 17 5� 46 04 51 01 24 21 0- 53 65 80 49Post % 79 77 85 84 82 80 80 78 67 68 77 77 78 85 67Balance 18 14 5 13 33 16 2 9 13 11 14 4 13 5 18Pre % 52 46 53 -6 34 51 53 22 24 20 24 57 78 29
Post % 51 17 54 07 25 64 52 06 5� 55 5- 73 94 57Balance 3 3� � 3� -3 �0 - �4 �5 -� �1 �0 �0 -1
3��ID 1 2 3 4 5 6 7 Average Highest Lowest
Pre % 57 22 26 42 07 07 51 0� 51 42Post % 14 50 10 1- 13 1- 60 14 60 50Balance �4 -� -5 35 -3 -- �1 -3 �1 3�Pre % 63 77 56 33 65 56 21 55 33Post % 75 85 71 56 78 78 54 12 20Balance �- 1 �2 -3 �3 -- �0 1 -3
���
���������
���
���������
���
���������
Table 2-3�Number of Midwife at Target HC
Kisii Kericho
2005 2007 Increase or decrease 2005 2007 Increase or
decrease Ibacho HC 3 4 � Ainamoi HC 6 6 �Ibeno HC 7 6 � Chepkemel HC 3 3 �Iranda HC 3 5 � Fort TernanHC 2 2 �
Kiogoro HC 4 5 � Kabianga HC 1 2 �Marani HC 8 7 � Kipkelion HC 3 2 �Riana HC 6 5 � Sigowet HC 6 6 �
Riotanchi HC 3 4 � Sosiot HC 4 4 �average 4.8 5.1 � average 3.6 3.6 �
2) Maternal Death Review (MDR) At Partners Workshop, SAMOKIKE project addressed MDR to HC staff and community members. Although it was difficult to assess death at the community, the staff of HANDS and DPHN visited the area of reported maternal death and discussed with HC staff and community members.
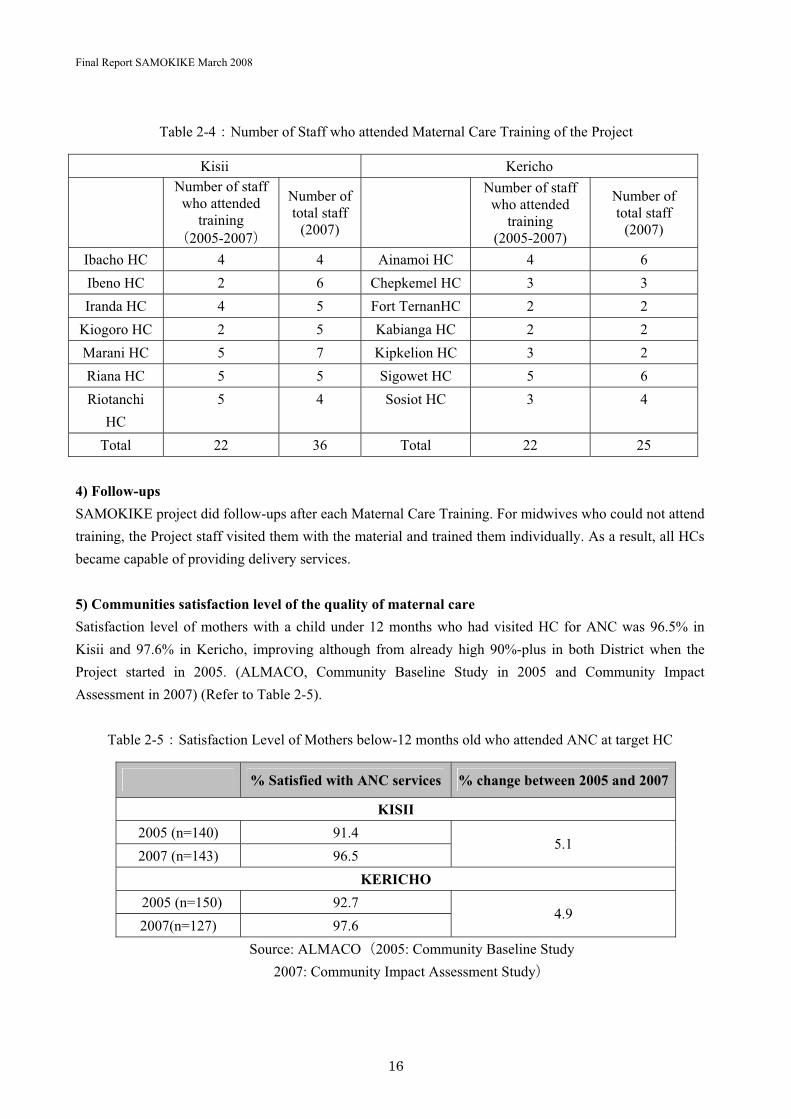
3) Number of staff completed training within each HC The number of midwives who attended maternal care trainingNational Package, Partners Workshop�was 22 from each District and total of 44. Based on the survey, these numbers were equivalent to 61% midwives in Kisii and 88% midwives in Kericho (Refer to Table 2-4). Due to relocation of HC staff, some midwives who attended training may have had to move away from the target HC.
Final Report SAMOKIKE March 2008
16
Table 2-4�Number of Staff who attended Maternal Care Training of the Project
Kisii Kericho Number of staff
who attended training
2005-2007�
Number of total staff
(2007)
Number of staff who attended
training(2005-2007)
Number of total staff
(2007)
Ibacho HC 4 4 Ainamoi HC 4 6Ibeno HC 2 6 Chepkemel HC 3 3Iranda HC 4 5 Fort TernanHC 2 2
Kiogoro HC 2 5 Kabianga HC 2 2Marani HC 5 7 Kipkelion HC 3 2Riana HC 5 5 Sigowet HC 5 6Riotanchi
HC5 4 Sosiot HC 3 4
Total 22 36 Total 22 25
4) Follow-ups SAMOKIKE project did follow-ups after each Maternal Care Training. For midwives who could not attend training, the Project staff visited them with the material and trained them individually. As a result, all HCs became capable of providing delivery services.
5) Communities satisfaction level of the quality of maternal care Satisfaction level of mothers with a child under 12 months who had visited HC for ANC was 96.5% in Kisii and 97.6% in Kericho, improving although from already high 90%-plus in both District when the Project started in 2005. (ALMACO, Community Baseline Study in 2005 and Community Impact Assessment in 2007) (Refer to Table 2-5).
Table 2-5�Satisfaction Level of Mothers below-12 months old who attended ANC at target HC
� % Satisfied with ANC services % change between 2005 and 2007
KISII 2005 (n=140) 91.42007 (n=143) 96.5
5.1
KERICHO 2005 (n=150) 92.72007(n=127) 97.6
4.9
Source: ALMACO2005: Community Baseline Study 2007: Community Impact Assessment Study�

Final Report SAMOKIKE March 2008
17
Also, the survey in 2005 resulted in satisfaction levels of delivery at HC as low as 12.9� in Kisii and 42.1� in Kericho, which improved significantly in the survey in 2007 as high as 98.7� in Kisii and 97.3� in Kericho. (Refer to Table 2-6)
Table 2-6�Satisfaction Level of Delivery at Target HC
�% Satisfied with delivery
services last delivery % change between 2005 and
2007
KISII 2005 (n=139) 12.92007 (n=143) 98.7
85.8
KERICHO 2005 (n=159) 42.12007 (n=139) 97.2
55.1
Source: ALMACO, 2005: Community Baseline Study 2007: Community Impact Assessment Study�
6) Number of HC maintaining facilities and equipment 1and 2 years after their installation All HCs could offer services using the provided equipment, however, some equipment could not be used temporarily because HC ran out of fuel of the generator or battery for the electric fetoscope. Currently, all HCs in Kericho and Kisii have one or more Income Generating Activities (IGA) going on, hence, we expect the community to continue to better manage its HC by supplementing the necessary equipments from IGA.
7) Number of staff attended maintenance training and the frequency of regular maintenance A total of 27 staff from both Districts attended the Medical Equipment Training. In addition, technicians from DH who are in charge of maintenance for HC equipment participated. Although regular maintenance at HCs was not conducted, technicians from DH provided services to HC when requested.
Discussion and lesson learnt 1) Setting up better environment for qualitative improvement in maternal care services After implementation of three year project, all HCs could provide delivery service now and the level of community satisfaction has risen. However, the average number of skilled midwives at each HC is 5.2 in Kisii and 3.6 in Kericho, which far lags the minimum of 8 per HC that the Kenyan government specifies. Also, dormitories are not sufficiently established for health staff at HC and better environment are necessary to be provided. In the aspect of the qualitative improvement in maternal care services, SAMOKIKE project recommends increase number of midwives and improvement in the HC environment such as staff dormitories.
2) Involving community and HC staff in the management of HC facility and medical equipment SAMOKIKE project has involved community to HC renovation and such community involvement will
Final Report SAMOKIKE March 2008
18
continue to be the key to maintaining and managing HC. In addition, supplies such as fuel and batteries for medical equipment should be afforded by funds raised through IGA. It is desirable that HC staff coordinate with the community to maintain and manage the facilities and medical equipment.
3) Enhancing collaboration between community and HC SAMOKIKE project has involved community to many of its activities. In particular, Partners Workshop was epoch-making that it provided training opportunity simultaneously to both HC workers and the community. As a result, Partner Workshop and other various activities resulted in strengthening mutual understanding and coordination between community and HC. SAMOKIKE project highly recommends disseminating these activities to the other regions.
2.2.2 Output 2
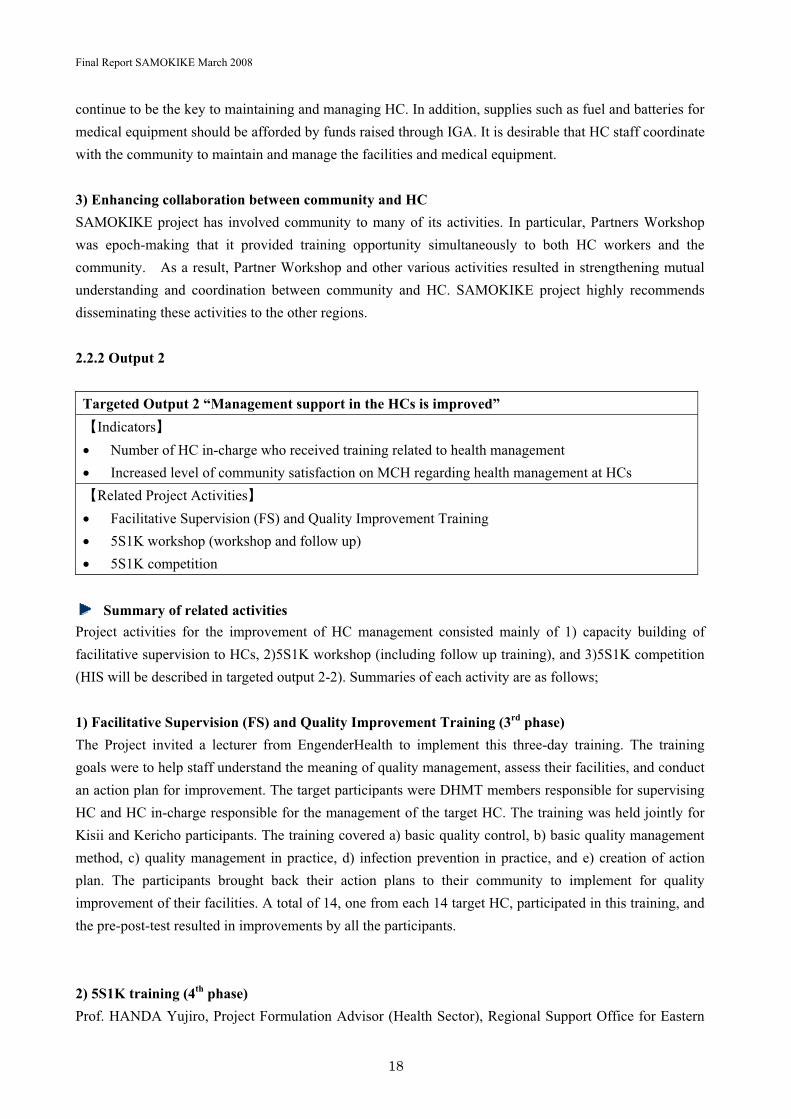
Targeted Output 2 “Management support in the HCs is improved” Indicators�� Number of HC in-charge who received training related to health management � Increased level of community satisfaction on MCH regarding health management at HCs Related Project Activities�� Facilitative Supervision (FS) and Quality Improvement Training � 5S1K workshop (workshop and follow up) � 5S1K competition
Summary of related activities Project activities for the improvement of HC management consisted mainly of 1) capacity building of facilitative supervision to HCs, 2)5S1K workshop (including follow up training), and 3)5S1K competition (HIS will be described in targeted output 2-2). Summaries of each activity are as follows;
1) Facilitative Supervision (FS) and Quality Improvement Training (3rd phase) The Project invited a lecturer from EngenderHealth to implement this three-day training. The training goals were to help staff understand the meaning of quality management, assess their facilities, and conduct an action plan for improvement. The target participants were DHMT members responsible for supervising HC and HC in-charge responsible for the management of the target HC. The training was held jointly for Kisii and Kericho participants. The training covered a) basic quality control, b) basic quality management method, c) quality management in practice, d) infection prevention in practice, and e) creation of action plan. The participants brought back their action plans to their community to implement for quality improvement of their facilities. A total of 14, one from each 14 target HC, participated in this training, and the pre-post-test resulted in improvements by all the participants.
2) 5S1K training (4th phase) Prof. HANDA Yujiro, Project Formulation Advisor (Health Sector), Regional Support Office for Eastern
Final Report SAMOKIKE March 2008
19
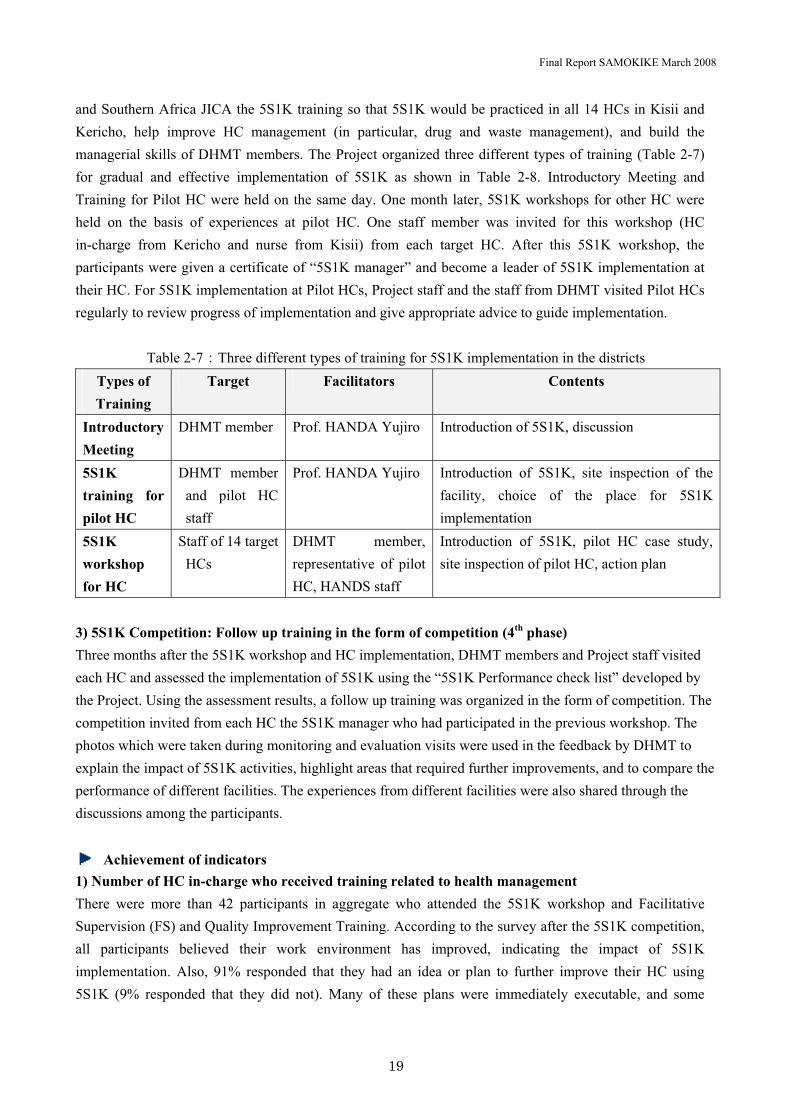
and Southern Africa JICA the 5S1K training so that 5S1K would be practiced in all 14 HCs in Kisii and Kericho, help improve HC management (in particular, drug and waste management), and build the managerial skills of DHMT members. The Project organized three different types of training (Table 2-7) for gradual and effective implementation of 5S1K as shown in Table 2-8. Introductory Meeting and Training for Pilot HC were held on the same day. One month later, 5S1K workshops for other HC were held on the basis of experiences at pilot HC. One staff member was invited for this workshop (HC in-charge from Kericho and nurse from Kisii) from each target HC. After this 5S1K workshop, the participants were given a certificate of “5S1K manager” and become a leader of 5S1K implementation at their HC. For 5S1K implementation at Pilot HCs, Project staff and the staff from DHMT visited Pilot HCs regularly to review progress of implementation and give appropriate advice to guide implementation.
Table 2-7�Three different types of training for 5S1K implementation in the districts Types of Training
Target Facilitators Contents
IntroductoryMeeting
DHMT member Prof. HANDA Yujiro Introduction of 5S1K, discussion
5S1Ktraining for pilot HC
DHMT member and pilot HC staff
Prof. HANDA Yujiro Introduction of 5S1K, site inspection of the facility, choice of the place for 5S1K implementation
5S1Kworkshopfor HC
Staff of 14 target HCs
DHMT member, representative of pilot HC, HANDS staff
Introduction of 5S1K, pilot HC case study, site inspection of pilot HC, action plan
3) 5S1K Competition: Follow up training in the form of competition (4th phase) Three months after the 5S1K workshop and HC implementation, DHMT members and Project staff visited each HC and assessed the implementation of 5S1K using the “5S1K Performance check list” developed by the Project. Using the assessment results, a follow up training was organized in the form of competition. The competition invited from each HC the 5S1K manager who had participated in the previous workshop. The photos which were taken during monitoring and evaluation visits were used in the feedback by DHMT to explain the impact of 5S1K activities, highlight areas that required further improvements, and to compare the performance of different facilities. The experiences from different facilities were also shared through the discussions among the participants.
Achievement of indicators 1) Number of HC in-charge who received training related to health management There were more than 42 participants in aggregate who attended the 5S1K workshop and Facilitative Supervision (FS) and Quality Improvement Training. According to the survey after the 5S1K competition, all participants believed their work environment has improved, indicating the impact of 5S1K implementation. Also, 91% responded that they had an idea or plan to further improve their HC using 5S1K (9% responded that they did not). Many of these plans were immediately executable, and some

Final Report SAMOKIKE March 2008
20
getting a hint from other HC during the training. These indicate HC managers’ growing skills and confidence as a result of the training that the Project organized.
2) Increased level of community satisfaction on MCH regarding health management at HCs Interviews with HCMC: representative in communities, and Assistant Chief (Refer to Table 2-8) resulted in increased level of satisfaction on maternal care service related to community management.
Table 2-88Results of Interview with Community Representatives9HCMC and Assistant Chief:
Y 2005 Y 2007 Availability of facility 65.6% 46.9%Medicine and medical
supply 37.5% 9.4%
Appropriateness of facility
37.5% 9.4%
Healthcare education 34.3% 28.1% Water supply 15.6% 3.1%
Electricity supply 12.5% 0% Services 6.2% 0%
*Rate of respondents who though they needed an improvement (the lower percentage indicates an improvement)
Source8Almaco 2007
In the improved areas (availability of facilities, appropriateness of facilities), in addition to contribution by training and Project’s equipment provision, it is also important that HC management generally improved as facilities are properly being managed. Also, the improved supply of service can be seen to be in turn contributing to the improvement of management capacity.
Discussion and lesson learnt 1) Introducing and implementing 5S1K gradually To improve the management skills of HC managers, the Project first hosted workshop on basic concept of HC management in the 3rd phase, and as an advanced step conducted more practical 5S1K workshop in the 4th phase. It could be recognized that achievements of the training were put into the practice, owing to such process of training implementation. Such gradual implementation not only increased knowledge of HC staff but also improved HC management in practice. These results are recognized by community representatives and would lead to further utilization of HC.

Final Report SAMOKIKE March 2008
21
2) Capacity building of HC managers Although leaving a room for improvement, the Project has succeeded in laying the groundwork for building the skills of HC managers. It is most important for the managers to continue to work on their skills and recognize that they can improve further. The Project recommends HC staff and DHMT as supervisor of medical facilities generally to continue to support HC managers.
Targeted Output 2-2�Health Information System (HIS) and record keeping system at HCs is functioning and is utilized for service and management at the HCs Indicators�� Number of training sessions for HIS and trainees � Efficiency of recording and reporting � Use of HIS for care and management at HCs and DHMT � Use of HIS for monitoring and evaluation � HIS study tour (for DMRIO) � HIS training and follow up training � HIS Board and Referral Stamp � HIS competition
Summary of related activities Health Information System (HIS) is essential to any program for improvement of health management. Project activities for the improvement of HIS included; 1) The study tour for capacity improvement of District Medical Record and Information Officer (DMRIO), 2) HIS training and follow-up training, 3) Introduction of HIS Board and Referral Stamps as tools for practical use of HIS; and 4) Competition for sustainable HIS improvement.
1) HIS Study Tour (3rd phase) The Project organized a study tour to Mombasa District, Coast Province in Tanzania, for Kisii and Kericho DMRIO for HIS improvement. In Mombasa, The Aga Khan Health Services, in collaboration with Provincial Health Office was operating the HIS and Health Report Improvement project which has shown some positive improvement of HIS in the province. The tour was organized with site visits in the project area and discussions with project related personnel. By this study tour, DMRIOs could acquire practical knowledge to identify and analyze the main challenges and also how to address them in Kisii and Kericho.
2) HIS training (3rd phase) and follow up training (4th phase) After the study tour to Mombasa, HIS training was conducted by DMRIOs with technical support from Aga Khan Health Services for 2.5 days. The main targets for this training were HC staff responsible for health information reports from HC to the districts in both Kisii and Kericho. One HC staff (Recording officer or Nurse) was invited as a participant from each target HC. Management Information System Consultant from Aga Khan Health Services invited as a trainer to facilitate the whole training with DMRIOs. The following contents were covered during the training.
Final Report SAMOKIKE March 2008
22
- Overview of HIS - Detailed guidelines for Monthly Summary Reports from HC to the Districts - Discussion on importance o HIS and quality of data and information - Discussion on how to overcome challenges of HIS, especially quality of data
HIS follow up training was conducted in the 4th phase as one-day training and was meant to follow up HIS related activities at HCs and to identify ways to improve HIS. In preparation for this training, DMRIOs assessed the 5 monthly summary reports which were submitted to the district by HC.
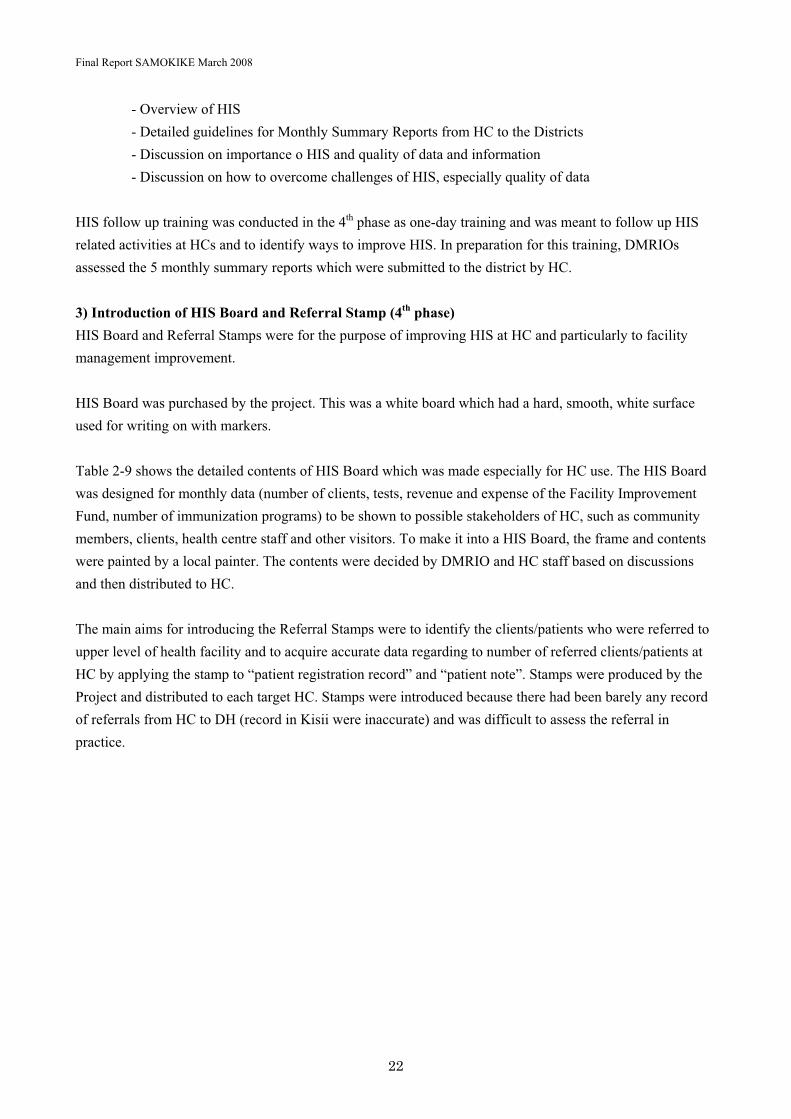
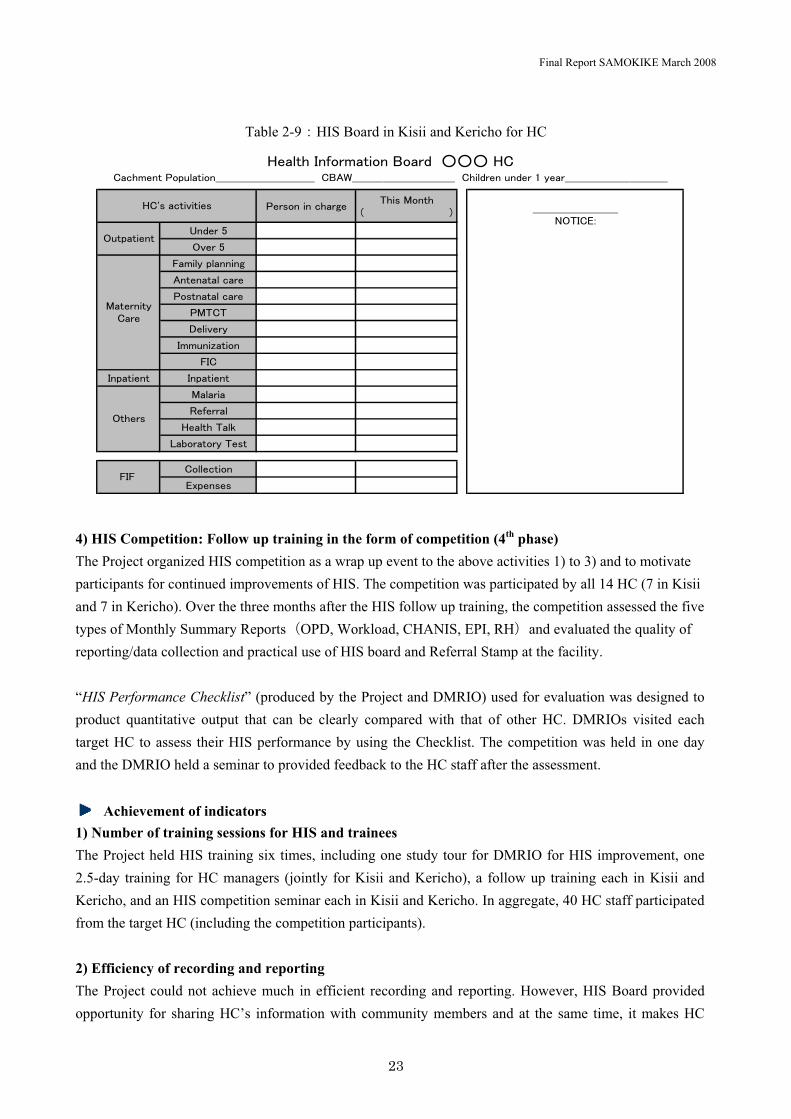
3) Introduction of HIS Board and Referral Stamp (4th phase) HIS Board and Referral Stamps were for the purpose of improving HIS at HC and particularly to facility management improvement.
HIS Board was purchased by the project. This was a white board which had a hard, smooth, white surface used for writing on with markers.
Table 2-9 shows the detailed contents of HIS Board which was made especially for HC use. The HIS Board was designed for monthly data (number of clients, tests, revenue and expense of the Facility Improvement Fund, number of immunization programs) to be shown to possible stakeholders of HC, such as community members, clients, health centre staff and other visitors. To make it into a HIS Board, the frame and contents were painted by a local painter. The contents were decided by DMRIO and HC staff based on discussions and then distributed to HC.
The main aims for introducing the Referral Stamps were to identify the clients/patients who were referred to upper level of health facility and to acquire accurate data regarding to number of referred clients/patients at HC by applying the stamp to “patient registration record” and “patient note”. Stamps were produced by the Project and distributed to each target HC. Stamps were introduced because there had been barely any record of referrals from HC to DH (record in Kisii were inaccurate) and was difficult to assess the referral in practice.
Final Report SAMOKIKE March 2008
23
Table 2-9�HIS Board in Kisii and Kericho for HC
������������/�����#�� �
$
;����2
�%��2
<����(�����/
�� ��� �����
��� �� �����
�#���
"��%���
������=� ���
<��
��(� ��� ��(� ���
#�����
>������
*�� ���,
?�@��� ������
���� ���
�)(�����
*�� �������� ���A����BBB*�������� ��(�� ���CCCCCCCCCCCCCCCCCCCCCCCCCCCCC�A�DCCCCCCCCCCCCCCCCCCCCCCCCCCCCCC�����������������CCCCCCCCCCCCCCCCCCCCCCCCCCCCCC
*�E��� �%� ���
CCCCCCCCCCCCCCCCCCCCCCCCC+�����F
�� (� ���
#� ���� �����
� ����
<�<
4) HIS Competition: Follow up training in the form of competition (4th phase) The Project organized HIS competition as a wrap up event to the above activities 1) to 3) and to motivate participants for continued improvements of HIS. The competition was participated by all 14 HC (7 in Kisii and 7 in Kericho). Over the three months after the HIS follow up training, the competition assessed the five types of Monthly Summary ReportsOPD, Workload, CHANIS, EPI, RH�and evaluated the quality of reporting/data collection and practical use of HIS board and Referral Stamp at the facility.
“HIS Performance Checklist” (produced by the Project and DMRIO) used for evaluation was designed to product quantitative output that can be clearly compared with that of other HC. DMRIOs visited each target HC to assess their HIS performance by using the Checklist. The competition was held in one day and the DMRIO held a seminar to provided feedback to the HC staff after the assessment.
Achievement of indicators 1) Number of training sessions for HIS and trainees The Project held HIS training six times, including one study tour for DMRIO for HIS improvement, one 2.5-day training for HC managers (jointly for Kisii and Kericho), a follow up training each in Kisii and Kericho, and an HIS competition seminar each in Kisii and Kericho. In aggregate, 40 HC staff participated from the target HC (including the competition participants).
2) Efficiency of recording and reporting The Project could not achieve much in efficient recording and reporting. However, HIS Board provided opportunity for sharing HC’s information with community members and at the same time, it makes HC
Final Report SAMOKIKE March 2008
24
staff to review the health information even after monthly reports were submitted to the district (before introducing HIS Board, most of HC staff did not have interest for own HC’s information and never review the data which was submitted to the district).The Referral Stamp made it much easier to count the number of referred patients. In these respects, the Project made some contribution to efficient recording and reporting.
3) Use of HIS for care and management at HCs and DHMT HC only recently started utilizing HIS such as HIS Board, and it is too soon to evaluate its impact on the improvement of facility management and services. The Project considers HIS Board the first step. Also, as DMRIO builds up capacity, DHMT members started to share monthly information with each other. Improvements are gradual if not sufficient. For example, in the month of a maternal death at one HC, DHMT shared this information among its members and appropriately followed up with this HC (Refer to Maternal Death Review).
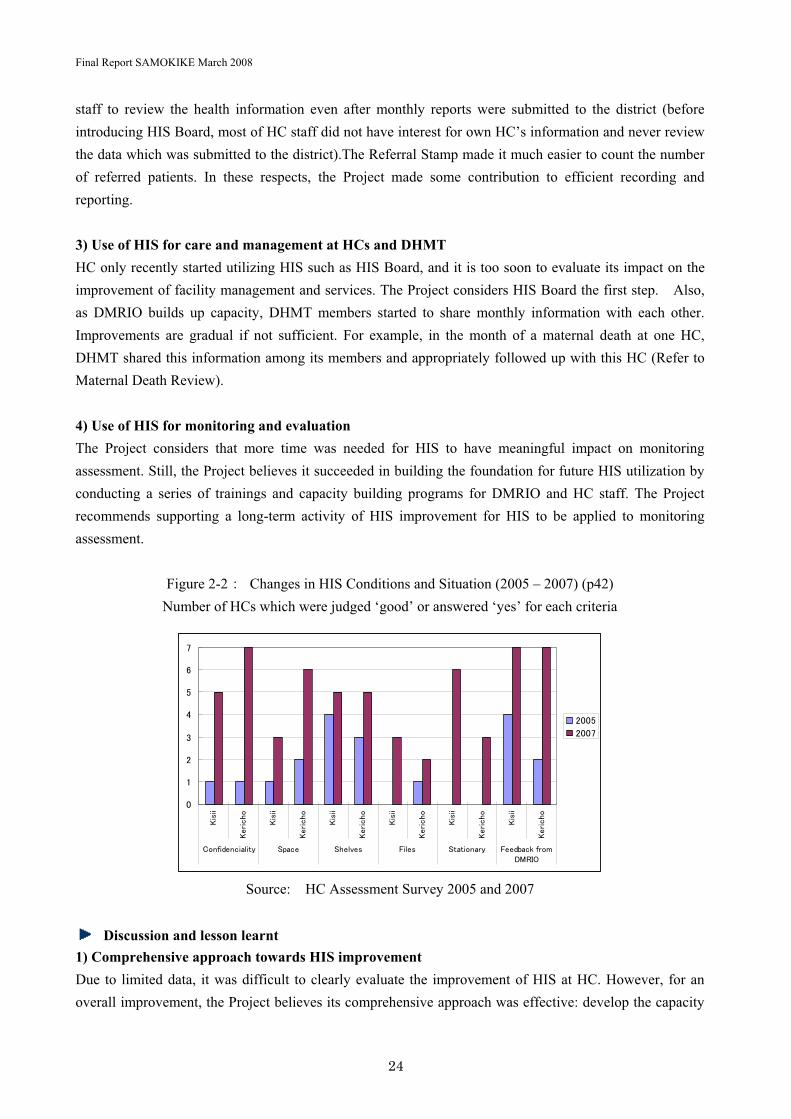
4) Use of HIS for monitoring and evaluation The Project considers that more time was needed for HIS to have meaningful impact on monitoring assessment. Still, the Project believes it succeeded in building the foundation for future HIS utilization by conducting a series of trainings and capacity building programs for DMRIO and HC staff. The Project recommends supporting a long-term activity of HIS improvement for HIS to be applied to monitoring assessment.
Figure 2-2� Changes in HIS Conditions and Situation (2005 – 2007) (p42) Number of HCs which were judged ‘good’ or answered ‘yes’ for each criteria
7
�
-
3
4
2
0
5
���
��
����
���
���
��
����
���
���
��
����
���
���
��
����
���
���
��
����
���
���
��
����
���
������������ � !(��� !��%�� <��� ! � ������ <���@��,����"#>��
-772
-775
Source:� HC Assessment Survey 2005 and 2007
Discussion and lesson learnt 1) Comprehensive approach towards HIS improvement Due to limited data, it was difficult to clearly evaluate the improvement of HIS at HC. However, for an overall improvement, the Project believes its comprehensive approach was effective: develop the capacity

Final Report SAMOKIKE March 2008
25
of DMRIO as leaders of HIS improvement in their District; train HC staff; offer follow up training; introduce HIS Board as a new tool; introduce Referral Stamp; and evaluate results and reflect to future planning. The Project believes such comprehensive approach was effective towards the direction of overall improvement.
2) DMRIO to lead further HIS improvement Since the 4th phase, DMRIO has taken initiatives of interventions and trainings. DMRIO has developed a capacity to lead activities in their District for HIS improvement. The Project recommends DMRIO to continue to work on HIS improvement at target HC or other medical facilities such as dispensaries. Budgeting should be discussed for these purposes.
3) Challenges while promoting HIS Kisii District (Nyanza Province) was in the process of implementing a new pilot system of HIS while Kericho District (Rift Valley Province) was not. Such discrepancy made it difficult to execute a joint training for these two Districts, which was one of the most difficult issues to resolve.
Targeted Output 2-3:�Management capability for drugs and medical supplies at the HCs are improved.”
Indicators�� Reduced stock-out time for drugs and medical supplies. � Improved basic drug and medical supplies management of HCs. � Rational use of medicines based on guidelines at HCs
Relevant Project Activities�� Drug management training � 5S1K training � 5S1K competition
Summary of related activities 1) Drug management training (3rd phase) HANDS technical advisor led the training on drug management for HC staff to learn the basic knowledge about drug management. Training was held for three days each in Kisii and Kericho, and one participant (nurse, HC in-charge) from each HC, or a total of 13 participants, were invited. This training also introduced the basic concepts of 5S1K, which was more formally introduced in the 4th
phase.
2) 5S1K trainings, 5S1K competition: Please refer to output 2-1.
Achievement of indicators 1) Reduced stock-out time for drugs and medical supplies (records and condition of drugs and medical supplies) Drug management training resulted in some improvement; however, improvements varied from one HC to

Final Report SAMOKIKE March 2008
26
another. After the 5S1K training and competition of the 4th phase, HC showed significant improvements.
Also, according to the HC Assessment Survey that compared 2005 with 2007, both Kisii and Kericho improved in all assessment areas including space, alignment, darkness, shelves, and security (Refer to Figure 2-3).
� � �
Photo�� Store room before (left) and after (right) 5S1K; Chepkemel HC, Kericho
Figure 2-3�Pharmacy Store Management Change (2005 - 2007) (p31) Number of HCs which was judged ‘good’ for each criteria
7
�
-
3
4
2
0
5
����� ������� ����� ������� ����� ������� ����� ������� ����� �������
!(��� ��/���� "��,���� !��%�� !����� �
-772
-775
Source:� HC Assessment Survey 2005 and 2007
2) Decrease in shortage of medical supply inventory 2007 HC Assessment Survey results show that as of December 2007, there were fewer days of medical supply store shortages (from the high of 43 days on average in 2005 to the low of 20 days on average in 2007).However, this seemed to have resulted from the change in supply system (formerly central to district to HC; now central to HC), and not fully explained by the impact of the Project activities.
3) Rate of prescriptions based on HC treatment guidelines There is no data on the rate of prescriptions that were based on HC treatment guidelines. However, Table 2-10 shows that more guidelines were used at HC in 2007 compared with 2005 in both Kisii and Kericho.
Final Report SAMOKIKE March 2008
27
Apparently, guidelines were used effectively for treatment. However, these guidelines were not a tool that the Project provided and encouraged, and therefore this cannot be seen as an achievement of the Project. However, it can be said that the various Project training helped HC staff develop skills to utilize these guidelines.
Table 2-10� Number of Guidelines Used at HC (Average)
2005 2007 Kisii 2.57 3.57
Kericho 2 3
Average 2.29 3.29
Source:� HC Assessment Survey 2005 and 2007
Discussion and lesson learnt1) Positive impact of external conditions on drug management Generally, medical supply management has improved. There were changes in external conditions that contributed to this progress (e.g. Change in supply system).The Project contributed much to the improvement in store management. The improvements varied across different HC, so the Project recommends DHMT to regularly support less developed HC to work hard to catch up.
2) Promoting 5S1K as preparation for the transitioning of the medical supply system The MOH is planning to transition from its current PUSH system to a PULL system regarding the medical supply distribution. Prior to 5S1K, store management was barely functioning (see Photo), and HC could not have appropriately managed supply if converted to a PULL system. Most, if not all, HC have improved store management and started to record supply more properly. In these respects, the Project recommends introducing 5S1K as preparation for the change to the PULL system and for further improvement in medical store management in medical facilities of Kisii and Kericho that had not been the target of the Project.
Targeted Output 2-4: “To improve waste management system.” Indicators�� Number of HC staff who received the basics of waste management � Number of HCs which undertake waste management according to the MOH standard � Improvement behavior regarding waste management among HC for improvement Relevant Project Activities�� 5S1K training� 5S1K competition
Summary of related activities Interventions for waste management improvement were also attempted through 5S1K activities which led to cost-effective improvements in facility environment improvement as well as sanitary conditions by such instructions as burning rubbish regularly, separating refuse purposely, and fencing the refuse pit. Proper

Final Report SAMOKIKE March 2008
28
way of using Safety Box was also given to HC staff. For other relevant activities, please refer to targeted output 2-1.
Achievement of indicators 1) Number of HC staff attending waste management training In aggregate, over 30 participated in the waste management training as a part of 5S1K training and competition.
2) Number of HC that follows the MOH waste management guidelines Since the MOH has not standardized the requirements for waste management at HC level, the Project cannot make this assessment quantitatively. However, 2007 HC Assessment Survey results showed improvements in the use of refuse pit and Safety Box as shown in Figure 2-4.Safety Box has become available in all 14 target HCs. More HCs in Kisii responded refuse pits were “good”, but there was no change in the response from HCs in Kericho.
3) Improvement in attitude and behavior of staff towards waste management For general waste, the Project had since its inception believed that each HC should have its own incinerator to prevent infection and improve sanitary conditions. However, purchasing a new incinerator was financially not possible either at HC or by the MOH; therefore, this need was converted into making another effort within available resources, such as burning rubbish regularly (around two times per week) using paraffin and managing the capacity of a refuse pit. Such improvements were seen in almost all HCs (both in Kishii and Kericho). Also, pits were properly fenced for the safety measure for children.
Figure 2-4� Waste Management Change (2005 - 2007) Number of HCs which was judged ‘good’ for each criteria
7
�
-
3
4
2
0
5
����� ������� ����� �������
!��� �@�) >�����(�
-772
-775
Source:� HC Assessment Survey 2005 and 2007

Final Report SAMOKIKE March 2008
29
� � �
Photo:� � Refuse pit before (left) and after 5S1K (right)
Discussion and lesson learnt 1) Improvement in waste management Project has observed improvements in waste management, which has a room for further improvement. In particular for Safety Boxes, burning those in a refuse pit by using paraffin won’t be sufficient for both reasons; infectious prevention and environment protection. Those are needed to be burned in an incinerator. However, in current circumstances, there is no fund to set incinerator at each HC and no system to collect Safety Boxes from each HC to burn those at District Hospital. Accordingly, a new standard needs to be established to determine and promote appropriate levels of waste management given the distant locations and limitations in purchasing an incinerator. In these respects, the Project recommends that DHMT guides HC.
2.2.3 Output 3
Targeted Output 3 “District Health Management Teams(DHMTs) system for their supportive supervision for HCs is strengthened”
Indicators�� Number of DHMT members involved in supervision of HCs. � Number of v supervision at each HC. � Level of satisfaction by HC in charges with supportive supervision Relevant Project Activities�� Supervision check list � Study tour to Tanzania � DPCC meetings� Provision of Multi Purpose vehicles: one for Kisii and one for Kericho � Other joint activities
Summary of related activities 1) Supervision check listDue to the lack of comprehensive and standardized check list on DPCC, Supervision to HC by DPCC was insufficient and lack of consistency each HC. The Project developed the supervision check list through the discussion with DPCC. In the 2nd phase, DPCC revised it with HC managers.

Final Report SAMOKIKE March 2008
30
2) Study tour to Tanzania (3rd phase) A study tour to Tanzania was aimed at enhancing the knowledge base of DHMT members through technical discussions with the Ministry of Healthcare of Tanzania and The Project for Strengthening District Health Services in Morogoro Region (Morogoro Health Project).This one-week tour was participated by DMOH and DPHN of both Districts of Kisii and Kericho. The tour members actively discussed with the Project for Strengthening District Health Services in Morogoro Region (Morogoro Health Project), which was a project in many ways similar to the SAMOKIKE Project that worked to improve health system of Tanzanian districts and provinces.
3) DPCC meetings (1st to 4th phase) DPCC (District Project Coordination Committee) has promoted information sharing and discussion between Kisii and Kericho for the purposes of effective Project management and capacity building of DHMT members. DPCC meetings were organized as shown in Table 2-11.
Table 2-11�DPCC held in each phase
Number of DPCC meetings
Phase 1 5Phase 2 2Phase 3 3Phase 4 2
In the 4th phase, DPCC met twice because the first half of this phase was devoted to follow up trainings and because DPCC had to cancel its scheduled meeting in the second half due to the turmoil after the presidential election.
4) Provision of Multi Purpose Vehicles: one for Kisii and one for Kericho (1st phase) The Project provided one vehicle to each Kisii and Kericho in the middle of the 1st phase. These were Multi Purpose cars that were used for ambulance to strengthen the referral system or for building the capacity of DHMT to support and supervise HCs. At each DPCC meeting, the status of the usage of the vehicles was updated and maintenance and other related issues were discussed. Nowadays, the Multi Purpose cars are used as not only a referral but also regular supervision by DHMT.
5) Other joint activities The Project had aimed for a sustained development of its activities and to this goal coordinated all Project activities with DHMT. In particular, the Project organized DHMT-led training and other activities and contributed to build the capacity of DHMT members.

Final Report SAMOKIKE March 2008
31
6) Dissemination Preparation Training The Project planned Dissemination Seminar in the last half of 4th phase, however, political and social confusion in Kenya affected by the result of Kenyan presidential election made it impossible to be held it in the phase. Therefore, the Project rearranged the four-day training for the purpose of reviewing and sharing the project achievements and planning the continued activities with DHMT members. The training included the session of the preparation of dissemination seminar, (when safety condition become better) as a part of technical transformation.
Achievement of indicators 1) Number of DHMT who supervised each HC The members of District Health Office who supervised each HC included District Medical Officer of Health (DMOH), District Public Health Nurse (DPHN), District Clinical Officer (DCO), District Public Health Officer (DPHO), District Medical Record and Information Officer (DMRIO), District Health Administration Officer (DHAO), together with other members as necessary. The total team members were between eight and ten in Kisii District and normally between four and five in Kisii District, who visited their relevant HC for supervision.
2) Number of visits to HC for supervision In Kisii, normally two days of a week were regular visit days, but this was subject to change due to scheduling conflicts. Also, the target HC of the Project was only few of the all HC that DHMT supervised. As a result, actual visits to each HC were 1-3 times per month. There were no regular visit days in Kericho. However, HC recognized more number of visits by DHMT members than before. The new DMOH (in position since March 2007) has initiated building a new system, which progress the Project expects to continue.
3) Level of satisfaction of HC managers for DHMT supervision The level of satisfaction of HC managers for DHMT supervision has improved from “rather dissatisfied to satisfied” (average) of 2005 to “satisfied to very satisfied” (average) of 2007 (HC Assessment Survey). The reasons for the improvement were 1) DHMT members gave advance notices to HC before a visit, 2) DHMT members were more cooperative than before, 3) DHMT members identified issues unnoticed by HC staff and helped solve problems, and 4) DHMT members were more attentive to HC requests.
Discussion and lesson learnt 1) Strengthening support and supervision for medical facilities The Project in its 1st phase developed the checklist for medical facility supervision to improve the quality of support of HC by DHMT. However, in reality, the check list had not been utilized because DHMT could not allocate resources and because DHMT could not financially afford to establish means of transportation to visit HC. Later, DHMT better recognized the effectiveness of the checklist after the implementation of 5S1K and HIS competitions, which gave opportunities for DHMT members to learn how to assess HC conditions using tools similar to the checklist. It is desirable that each Kisii and Kericho develops its own methods – e.g. incorporating 5S1K concepts as a standard of support/supervision of medical facilities – to

Final Report SAMOKIKE March 2008
32
improve their system. The Project recommends each District to ensure budget and staff allocations for further progress and improvement in quality (e.g. more frequent visits, accurate recording of advice, etc).
2.2.4 Output 4
Targeted Output 4 “Maternal Care at the community level is improved” Indicators�� Number of community people seeking maternal care services in target health facility. � Increased knowledge regarding maternal care among people � Number of maternal care health learning sessions held and its participants regarding maternal care. � Number of peer learning workshops and exchange visits � Number of communities replicating activities Relevant Project Activities�� Monitoring HC renovation � Selecting pilot HC � Involvement of community (e.g; Community Activity Meeting, Community Campaign)
Summary of related activities SAMOKIKE project adopted a “two-way approach” in implementing community activities since we believe that the interaction between the HC and the community is the key to improve health service at the HCs as well as to promote the health of the community. This principle was applied for conducting following activities during the Project.
Figure 2-5�“Two-Way approach” between HC and Community Activities
1) Monitoring HC renovation (1st and 2nd phases) SAMOKIKE project considered HC renovation an opportunity to strengthen the relationship between the
SAMOKIKE
DHMT
Health Centre Community
• Monitoring process of the HC renovation
• Attending the same workshop e.t.c…
Final Report SAMOKIKE March 2008
33
HCs and communities by involving the Community Representatives in the process of renovations. Community Representatives made a team and monitored the process of the renovations by local agencies. In addition, Community Representatives reported the progress of the renovations to HC staff, HANDS staff, and DHMT and issues that each party found were shared together.
2) Selecting model HC (2nd phase) The Project selected Chepkemel HC (Kericho district) and Iranda HC (Kisii district) as a model HC. The following three points were considered as criteria for selection; a) the extent of community participation to HC (especially women’s participation), b) appropriateness of recording and record-keeping of the minutes of meetings and c) relationship between the HC and community. SAMOKIKE project in its 1st phase provided to these pilot HC generators that enabled them 24 hour delivery service. Upon providing the generators, the Project conducted management training for maintenance to the Community Representatives.
3) Involvement of community (Community Activity Meeting, community Campaign) (2nd, 3rd, and 4th
phase)SAMOKIKE project implemented the following activities towards improving maternal care and healthcare in Kisii and Kericho districts: a) Conducted Community Activities Meetings (CAM): Trainings for Community Representatives, b) Held Community led Community Meetings at HCs: Trainings for Community Leaders, and c) Implemented Community Campaigns.
a) Community Activity Meeting (CAM) The overall purpose of Community Activity Meeting was to provide an opportunity for discussions between HC staff and Community Representatives and to encourage them working together. CAM invited three participants; 1 staff from HC (normally clinical officer), 1 HCMC member and 1 SMG members each from all targeted HCs. Every year CAM was held and agenda� was decided according to current demands. During the 2nd phase, the meeting focused on reporting the progress of HC renovation, sharing the issues still to be solved. In the 3rd phase, action plan to promote HC involvement was developed, and action plan to organize Community Campaign was discussed in the 4th phase.
b) Community Led Community Meeting at HC (2nd, 3rd, and 4th phases)Community Led Community Meeting at HC was organized in second year of the project and 3meetings at each HC were conducted during the Project. While CAM was mainly organized by SAMOKIKE project and DHMTs, Community Representatives (HCMC and SMG members) mainly organized Community Meetings. In the 3rd phase, the main objectives of the meeting were to provide basic information about Safe Motherhood to other community members and to prepare for Community Campaigns in the 4th phase. Each meeting helped involve more community people to the community activities and SAMOKIKE project succeeded in improving the knowledge of maternal care at the community.
Final Report SAMOKIKE March 2008
34
Figure 2-6�Four Main Actors of SAMOKIKE Community Activities
SMG
Mem
bers HC Staff
HCMC
Mem
bers Comm
unity
lead
ers
COMMUNITY ACTIVITIES
SMG
Mem
bers HC Staff
HCMC
Mem
bers Comm
unity
lead
ers
SMG
Mem
bers HC Staff
HCMC
Mem
bers Comm
unity
lead
ers
COMMUNITY ACTIVITIES
c) Community Campaign (4th phase) SAMOKIKE project organized Community Campaign to raise further awareness to promote Safe Motherhood in its 4th phase. In order to reach mass population, two approaches were used: a) the first campaign targeting community people “broadly”, and b) the second campaign targeting pregnant woman and mothers “specifically”.
i�First Campaign (Mass Campaign) The first Campaign was targeted to community people aimed a)to promote importance of community support in saving mothers and newborns and b)to inform community about the importance of father’s participation. Campaigns were held for a half day to one full day, mainly organized by Community Representative and Community Leaders who had attended Campaign Pre-Meetings at each HC. The details of the Campaign was unique at each HC, including a) procession by Community Representatives and Community Leaders and HC staff who wore the campaign T-shirts and carried the campaign banner within the catchment area of HC, b) getting together at an open space in the community providing entertainments such as dramas and songs prepared by local school children and women’s group and c) promotion of the key message “Mama Mwenye Afya Jamii Yenye Afya (Healthy Mothers, Healthy Community)” which emphasize the importance of Safe Motherhood in the community. In addition, comments from mothers who had experienced delivery at HC helped community to understand services at HC.
ii�Second Campaign The second Campaign was aimed to educate pregnant women about Safe Motherhood and to promote the importance of ANC and PNC at HCs. Brochures were provided to encourage attendance of ANC at least 4 times, to get assistance of skilled midwife at delivery, and to promote the importance of attending PNC. Afterwards, baby shawls were given as presents to women who gave birth at HC and to those who wanted to deliver at HC but could not for specific reasons. (Refer to Table 2-12 for detail).
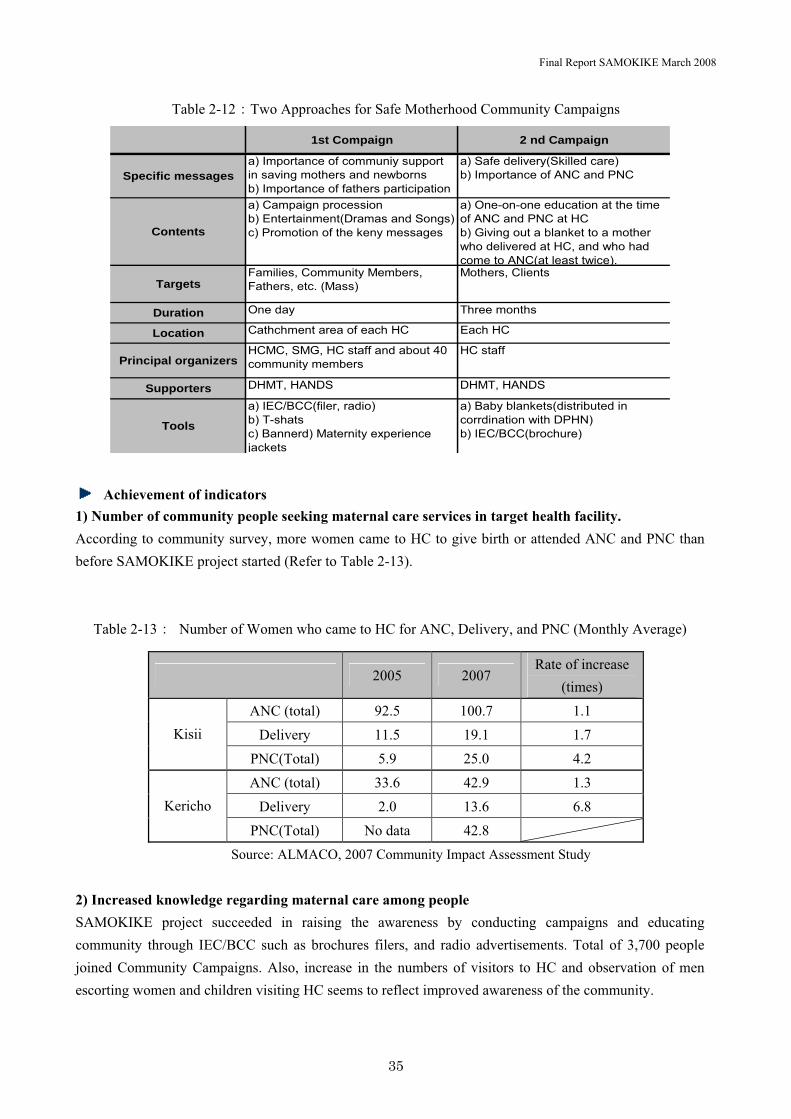
Final Report SAMOKIKE March 2008
35
Table 2-12�Two Approaches for Safe Motherhood Community Campaigns
1st Compaign 2 nd Campaign
Specific messagesa) Importance of communiy supportin saving mothers and newbornsb) Importance of fathers participation
a) Safe delivery(Skilled care)b) Importance of ANC and PNC
Contents
a) Campaign processionb) Entertainment(Dramas and Songs)c) Promotion of the keny messages
a) One-on-one education at the timeof ANC and PNC at HCb) Giving out a blanket to a motherwho delivered at HC, and who hadcome to ANC(at least twice).
TargetsFamilies, Community Members,Fathers, etc. (Mass)
Mothers, Clients
Duration One day Three months
Location Cathchment area of each HC Each HC
Principal organizersHCMC, SMG, HC staff and about 40community members
HC staff
Supporters DHMT, HANDS DHMT, HANDS
Toolsa) IEC/BCC(filer, radio)b) T-shatsc) Bannerd) Maternity experiencejackets
a) Baby blankets(distributed incorrdination with DPHN)b) IEC/BCC(brochure)
Achievement of indicators1) Number of community people seeking maternal care services in target health facility. According to community survey, more women came to HC to give birth or attended ANC and PNC than before SAMOKIKE project started (Refer to Table 2-13).
Table 2-13� Number of Women who came to HC for ANC, Delivery, and PNC (Monthly Average)
� 2005 2007Rate of increase
(times) ANC (total) 92.5 100.7 1.1
Delivery 11.5 19.1 1.7 Kisii
PNC(Total) 5.9 25.0 4.2 ANC (total) 33.6 42.9 1.3
Delivery 2.0 13.6 6.8 Kericho
PNC(Total) No data 42.8 �
Source: ALMACO, 2007 Community Impact Assessment Study
2) Increased knowledge regarding maternal care among people SAMOKIKE project succeeded in raising the awareness by conducting campaigns and educating community through IEC/BCC such as brochures filers, and radio advertisements. Total of 3,700 people joined Community Campaigns. Also, increase in the numbers of visitors to HC and observation of men escorting women and children visiting HC seems to reflect improved awareness of the community.

Final Report SAMOKIKE March 2008
36
3) Number of maternal care health learning sessions held and its participants regarding maternal care.
SAMOKIKE project conducted a total of 6 maternal care health learning sessions (Partners Workshop), 3 times in each District. A total of 140 people or 70 people in each District attended. Also, the Project organized Community Led Community Meetings at each HC to discuss maternal care with Community Representatives
4) Number of peer learning workshops and exchange visits During Partners Workshop, the program introduced particularly active HC and its communities. For example, the Workshop highlighted one community that made an empty space of HC a farm for IGA
5) Number of communities replicating activities Currently, all 14HCs are implementing IGA. Activities such as SMG escorting pregnant women in labor to HC are reported. In addition, within 3 targeted HCs, new midwives were hired by the community to resolve shortage of staffing issue.
Discussion and lesson learnt 1) Sustainability of the ongoing community activities SAMOKIKE projects believe that active involvement of community is crucial to effectively improve maternal care of the community. Better achievements were observed after active community involvement; therefore, the Project recommends encouraging community involvement to sustain further improvement. In particular, we believe that IGA by the community will continue to help improve maternal care services at each HC. Also, community involvement is necessary to extend catchment area for promoting maternal care of the community.
2) Promoting participation of family, husband, and men Promoting women to come to HC requires understanding of social, financial, cultural, and geographical conditions surrounding women. SAMOKIKE project organized activities to educate men about assisting pregnant mothers, which effort will need to be continued. It is expected that men who joined these activities will proactively support pregnant women and mothers.

Final Report SAMOKIKE March 2008
37
2.2.5 Output 5
Targeted Output 5 “A referral system is arranged and functioning between communities, HCs and District Hospitals” Indicators�� Number of appropriate referral cases of maternal complications � Types and number of record of communication, transportation and maintenance � Utilization of referral guidelines � Number of meetings reviewing referral cases Relevant Project Activities�� Kakamega study tour � Installation of community phones � Implementation of referral form and provision of referral stamp � Training and Refresher Course on Referral
Summary of related activities 1) Kakamega Study Tour (3rd phase) SAMOKIKE project organized a three-day tour to Kakamega District in Western Province of Kenya, where a maternal healthcare project had been implemented, to study their referral forms. The contents of the program were about expenses, communication and transportation tool, recording and management system of their referral system. Photocopies of Kakamega District’s referral forms were brought back for discussions with DHMT of Kisii and Kericho, and these forms were revised and implemented at all HCs and DH.
2) Installation of community phones (4th phase) Given the importance of timely referral in case of obstetric emergency, SAMOKIKE project installed community phone (Simu Ya Jamii) and other accessories to all target HCs. Community phones can be a source of IGA as 45% of the charge of the usage will be received by the phone owner. Such profit is expected to be utilized for emergency purposes within the community. HCMC was appointed as a manager of community phones, and methods to manage community phones were decided at each HC. Community phones were used mainly for emergency at night time but were placed in a convenient location for community people to utilize during the day and to promote as IGA. The Project conducted technical training to the manager, HCMC, and HC staffs, and introduced the installation and its benefits to the community during Community Campaigns.
3) Implementation of referral form and provision of referral stamp (3rd and 4th phases) Referral forms are necessary for effective information sharing between the facilities when transporting patients in emergency. Photocopies of Kakamega’s referral forms were brought back for discussions with DHMT of Kisii and Kericho, revised and implemented after the training with midwives. Referral Stamp had been introduced to HC for tracking the record of patients and pregnant women referred from HC to DH (Refer to Session 2-2).

Final Report SAMOKIKE March 2008
38
4) Trainings and Refresher Course (Follow-up) on Community Phone (4th phase) Trainings on procedure and management of community phones and Refresher Course were held after the installation. During the Refresher Course, technical training was conducted for midwives who require sophisticated skills in times of emergency. The technical training covered knowledge about management of obstetric emergency such as pregnancy induced hypertension (PIH), obstructed labor, fetal distress and postpartum hemorrhage which are typical obstetric emergency.
Achievement of indicators 1) Number of appropriate referral cases of maternal complications The multi-purpose vehicle provided by SAMOKIKE project in its 1st phase enabled effective transportation of patients in emergency. As a result, the percentage of referral cases at all HCs rose from the low of 13% (13 out of 101patients) in August 2006 to the high of 19% (28 out of 144 patients) in August 2007. There is not enough information to evaluate the appropriateness of referral; however, referral forms and delivery records had been utilized properly to record diagnosis and referral case such as saving lives of both mothers and babies had been reported.
2) Types and number of record of communication, transportation and maintenance Although the frequency of the usage of community phone vary depending on HC and its number of delivery, community phones are used approximately one to four times every month at each target HC. In addition, HCs and DHs have been utilizing referral forms which were introduced in the 4th phase to manage an emergency case effectively.
3) Utilization of referral guidelines In the 4th phase, SAMOKIKE project implemented technical training for midwives, covering management of obstetric emergency such as Pregnancy Induced Hypertension (PIH), obstructed labor, fetal distress, and postpartum hemorrhage. The participants brought back copies of the training material to their HC to put into practice. Also, guidelines to promote the procedure in referral case such as ways to contact DH, to complete referral form and register book were distributed to each HC. It has been reported that they are now implementing the procedures.
4) Number of meetings reviewing referral cases At DPCC, SAMOKIKE project reviewed referral cases with member of DHMT of Kisii and Kericho using actual referral forms and delivery records of DH. Also, all cases that was required to be shared was discussed with DHMT.
Discussion and lesson learnt 1) External factors and community involvement SAMOKIKE project had faced difficult challenges such as poor geographical conditions (e.g., unpaved roads) and financial issues (e.g., cost of fuel for transportation and maintenance of multi-purpose vehicle) against its goal of strengthening referral system from HC to DH. Although these hurdles were too
Final Report SAMOKIKE March 2008
39
significant to be resolved in three year project, supporting community-led emergency support system (e.g.,human resources, expense support, or lending of vehicles) enabled to strengthen the network of the community. Through sustaining community involvement, we hope such external factors will be resolved step by step.
2) Preparedness for emergency at HC Not all HCs are actually prepared for emergency at HC. In addition to normal delivery, HC should develop capacity for dealing with obstetric complications. SAMOKIKE project recommends that DPHN as supervisor of HC continue to review referral cases and level up the skill and knowledge of each midwives.
3) Preparedness of DH There were occasions in which patients were referred from HC to DH but DH could not fully accommodate to an emergency due to shortage of ambulance or fuel for transportation. Also, HC may not always afford an escort of its nurse or midwife due to capacity limitation. In regards for strengthening effective referral system, the Project recommends to establish support system where escort support from the DH would be provided.
2.3 Project Input
2.3.1 Expenditure of Project
The following table summarizes the contracted amount of SAMOKIKE project over three years.
Table 2-14�Contract amount of the SAMOKIKE Project (by phase) 1st Phase 2nd Phase 3rd Phase 4th Phase Total
Contract amount (yen) 94,102 33,033 80,687 89,523 297,345
� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � In 1000 yen�
2.3.2 Dispatch of Japanese Experts The list of Japanese experts (HANDS project members) is shown in Table2-15
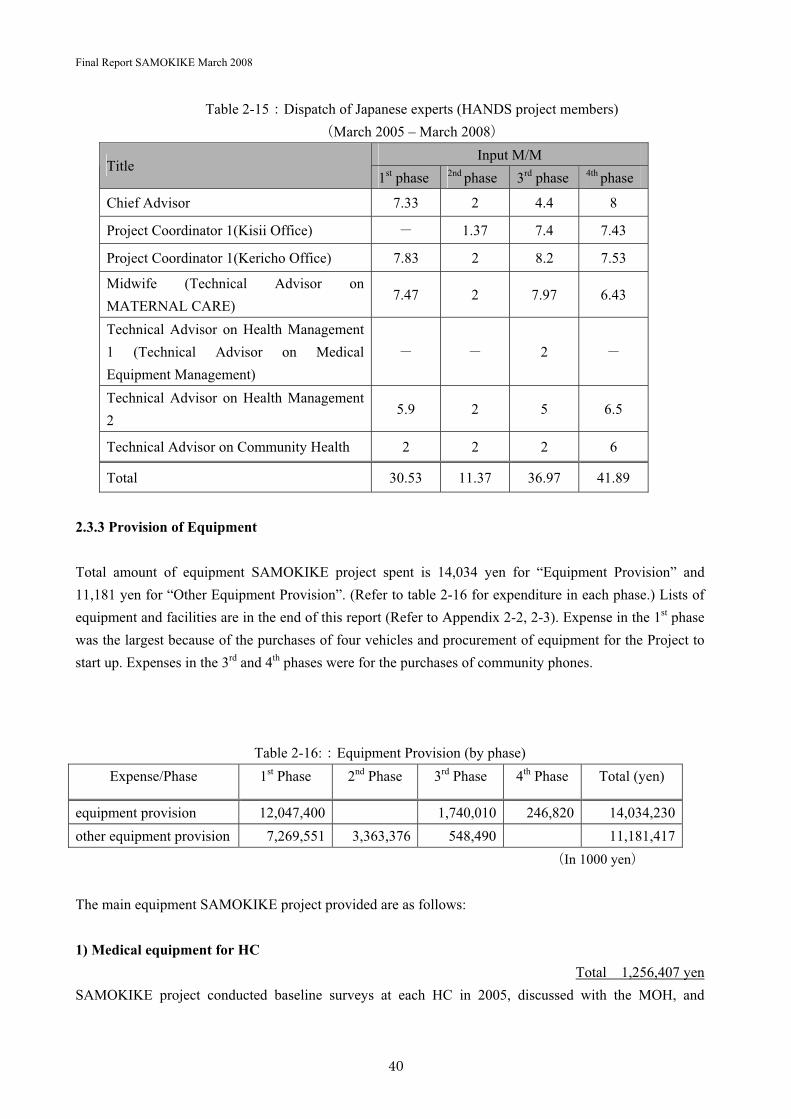
Final Report SAMOKIKE March 2008
40
Table 2-15�Dispatch of Japanese experts (HANDS project members) March 2005 – March 2008�
Input M/M Title
1st phase 2nd phase 3rd phase 4th phase
Chief Advisor 7.33 2 4.4 8
Project Coordinator 1(Kisii Office) � 1.37 7.4 7.43
Project Coordinator 1(Kericho Office) 7.83 2 8.2 7.53
Midwife (Technical Advisor on MATERNAL CARE)
7.47 2 7.97 6.43
Technical Advisor on Health Management 1 (Technical Advisor on Medical Equipment Management)
� � 2 �
Technical Advisor on Health Management 2
5.9 2 5 6.5
Technical Advisor on Community Health 2 2 2 6
Total 30.53 11.37 36.97 41.89
2.3.3 Provision of Equipment
Total amount of equipment SAMOKIKE project spent is 14,034 yen for “Equipment Provision” and 11,181 yen for “Other Equipment Provision”. (Refer to table 2-16 for expenditure in each phase.) Lists of equipment and facilities are in the end of this report (Refer to Appendix 2-2, 2-3). Expense in the 1st phase was the largest because of the purchases of four vehicles and procurement of equipment for the Project to start up. Expenses in the 3rd and 4th phases were for the purchases of community phones.
Table 2-16:�Equipment Provision (by phase) Expense/Phase 1st Phase 2nd Phase 3rd Phase 4th Phase Total (yen)
equipment provision 12,047,400 1,740,010 246,820 14,034,230other equipment provision 7,269,551 3,363,376 548,490 11,181,417� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � In 1000 yen�
The main equipment SAMOKIKE project provided are as follows:
1) Medical equipment for HC Total� 1,256,407 yen
SAMOKIKE project conducted baseline surveys at each HC in 2005, discussed with the MOH, and
Final Report SAMOKIKE March 2008
41
decided a list of equipment to provide. The list covered minimal requirements for maternal care services at HC (ANC, delivery, PNC), and equipment was provided to each HC by February 2006. Equipment can be categorized as maternal care purpose, record keeping purpose, and drug and medical supply management purpose. For details, refer to Appendix 2-2 “List of Equipment provided to Kisii and Kericho through JICA” and 2-3 “List of Equipment provided to Kisii and Kericho through HANDS”.
2) Community phone for HC Total� 1,986,830 yen
To strengthen referral system, community phones powered by solar-panel battery were provided to 14 HCs. In the 3rd phase, main components were procured, and additional equipment was gathered, assembled, put to training, and installed in the 4th phase,.
3) Vehicles for District Medical Office Total� 12,047,400 yen
In the 1st phase, SAMOKIKE project provided to each District Health Office of Kisii and Kericho a multi-purpose vehicle for their supervision of HC, referral transportation, and delivery of medical supplies. The vehicles were utilized flexibly during the implementation of SAMOKIKE project. In addition, two 4WD vehicles were purchased for the project activities that were provided to DMO of Kisii and Kericho after the closure of SAMOKIKE project.
2.3.4 Facilities SAMOKIKE project conducted the following facility construction and renovation:
1) HC renovation Total� 7,603,864 yenKisii�5,120,824�Kericho�2,483,040�
Based on the results of baseline surveys on the facilities of targeted HCs in the 1st phase, SAMOKIKE project renovated 4HCs in Kericho and 6HCs in Kisii. Renovation covered facilities, water supply, fences, space for medical supply and health record keeping. For details, refer to Appendix 2-4 “Cost of Health centre renovation in Kisii and Kericho through JICA.”
2) Construction of Kericho office Total�1,000,000 KESKenya Schilling) � 1,728,000 yen
SAMOKIKE project had temporarily used a storage space of Kericho DH as office space since the 1st
phase. In the 3rd phase, a new office was constructed within Kericho DH. This construction was fully financed by the MOH. In addition, the Project offered 1 million KES (1,728,000 yen) for security replenishment (e.g., fencing, window, etc�.

Final Report SAMOKIKE March 2008
42
2.4 Achievement of Overall Goal
Overall Goal : “Health condition, particularly the maternal health, in Kisii and Kericho Districts is improved ”
Indicators�� Maternal mortality (rate) in the Districts � Case fatality rate due to maternal complications � Infant mortality rate and malaria fatality rate Project Purpose�“Maternal care in the Project are with a focus on HCs and communities is improved” Indicators�� Skilled birth attendance rate of in the Districts � Delivery rate and ANC rate at HCs � Success rate in meeting the needs of women with maternal complications � HC utilization rate and client satisfaction
2.4.1 Factors Contributed to Achieve the Project Purpose
To achieve the Project Purpose of “Maternal care in the Project are with a focus on HCs and communities is improved”, SAMOKIKE project implemented the following three approaches: a) upgrading maternity care (targeted outputs 1, 2, 5); b) strengthening HC management (targeted outputs 2, 3); and c) encouraging community involvement (targeted output 4). These three approaches were interdependent and only together could achieve SAMOKIKE project’s overall goal. Japanese Experts worked together to coordinate these approaches to pursue the goal of the Project.
Figure 2-7:�SAMOKIKE Project Approach
Upgrading Upgrading MaternityMaternity CareCare
Encouraging Encouraging Community Community InvolvementInvolvement
Strengthening Strengthening Health Centre Health Centre ManagementManagement
Where good maternity care at Where good maternity care at HC should beHC should be
Final Report SAMOKIKE March 2008
43
2.4.2 Achievement of Project Purpose
As discussed section 2-2, most targeted outputs were achieved to a large extent even not perfectly. In this respect, it can be expected that the Project Purposes were reasonably fulfilled. However, SAMOKIKE project could not obtain data on “Skilled birth attendance rate of in the Districts”, which was one of the indicators of Project Purpose that SAMOKIKE project could not evaluate. However, the number of ANC and deliveries at the target HCs increased significantly after SAMOKIKE project compared to before (Refer to Table 2-13), which should be considered as a positive impact of the Project. In addition, the level of community’s satisfaction towards HC services has improved (Refer to Tables 2-5 and 2-6). SAMOKIKE project was reported several cases of successful treatments meeting the needs of pregnant women with complications. In particular, at meetings reviewing referral cases, participants have started to report more cases including a referral from HC to DH that utilized a multi-purpose vehicle of SAMOKIKE project and saved the lives of both the mother and the child.Refer to Section 2-2-5�
2.4.3 Towards the Achievement of Overall Goal
The Overall Goal of SAMOKIKE project was “Health condition, particularly the maternal health, in Kisii and Kericho Districts is improved”. The indicators measuring Overall Goal were maternal mortality rate in the Districts, case fatality rate due to maternal complications, infant mortality rate, and malaria fatality rate. Unfortunately, accurate and comparable data could not be obtained at the end of SAMOKIKE project, since these indicators need to be observed and compared in a longer span of 5-10 years. However, factors for achieving the Overall Goal and Project Purpose– “upgrading maternal care”, “strengthening HC management”, “encouraging community involvement” - were mostly achieved and therefore SAMOKIKE project can be considered to have succeeded in building the foundation for a further achievements.
Final Report SAMOKIKE March 2008
44
Chapter 3. Recommendations and Lessons Learned for Future
3.1 Recommendations and Lessons Learned
1) Basic investments for improving maternal care services To improve maternal care, it is most important to strengthen the capability of facilities nearest to community, which means building HC’s capability to provide normal delivery services.� To this goal, SAMOKIKE project recommends promoting ANC and investing facilities capable of 24-hour normal delivery services at the HC level.
2) Strengthening relationship between community and HC SAMOKIKE project resulted in the increased number of people coming to HC for maternal care thanks to the strong relationship between community and HC based on the key concept of Safe Motherhood. In particular, the following two factors contributed to the effective relationship building in the short-term:
First, there was a basis for building relationship between community and HC because it was widely recognized by people in Kenya that HCs are for community and managed and operated by community. SAMOKIKE project saw this as an example of government policy to effectively impact improvements at the grass-root level. Second, Partner’s Workshop was implemented as a unique method for capacity development, unlike TOT. This new approach was effective because community members spent days and nights with HC staffs (midwives) to not only learn the technical issues at the workshop but also to develop mutual understanding between each other.
3) Synergy effect of 5S1K in educating basic(minimal )health management 5S1K training as means to educate basic health management resulted in an additional impact of strengthening leadership skills among HC staff. Given the all-time shortage of resources, 5S1K is a concept easily understood and executed at all levels, well regarded by MoH in District as well as MoH in Province SAMOKIKE project recommends them to sustain disseminating the concept of 5S1K.
4) Role allocation of building referral system People tend to think that building referral system involves large scale initiatives such as infrastructure building, logistics, and strong management system by the government, although they are barely achievable. Therefore, collaboration between the public sector (central and local government) and the private sector (NGO, company, community, and community people) is essential. Under the limited resource, SAMOKIKE project recommended each community, HC, District Hospital, and District Health Office to proactively think and execute what each can do within their power to improve the referral system which we believe to continue to be a more practical approach.
5) Combining the horizontal approach with the vertical approach By combining the horizontal goal of improving health services with the vertical goal of improving maternal
Final Report SAMOKIKE March 2008
45
care, SAMOKIKE project enabled counterpart, HC staff and community to clearly understand the direction of the project, encouraged actions, therefore result in reaping an immediate impact. SAMOKIKE project recommends sustaining the development of basic health management focusing with the issue of maternal care at community.
6) Motivation programs at the HC level Organizing minimal HC management contest under the supervision of DHMT largely influenced the behaviors of HC staff. In particular, DHMT has reported that it has greatly contributed to the improvement of the environment of administration of HCs and changed HC staffs behaviors such as submitting HIS accurately and punctually. Certificate award of the contest is displayed at both the HC and the office of DMO and many HCs anticipate such contest to be continued every year to motivate their activities. SAMOKIKE project recommends similar programs as cost efficient means to motivate DMO people and to promote the supervision of HC.
7) Utilizing Safe Motherhood Group activities Safe Motherhood Group (SMG) who were educated through SAMOKIKE project are capable resources who could serve as role models for other communities. SAMOKIKE project recommends appointing SMG for educating Community Health Worker which is a part of the government strategy to develop community-led healthcare services.
8) Cost sharing activities of health service In some HCs, Community Representatives have approved to hire midwives to enable 24 hour delivery service using Facility Improvement Fund (FIF). Efficient utilization of FIF at the HC has greatly contributed to improve the health service of HC. We believe, at least, minimum cost sharing from the health service in the community will be necessary.
3.2 Way Forward
1) Budgeting gap to be resolved with the counterpart SAMOKIKE project had not been designed in the scope of annual budgeting of Kenya and therefore may not be financially sustainable. In the future, it is important to minimize the budgeting gap by reflecting the capacity of the counterpart from the initial project planning.
2) Predicting external factors � The social confusion in the final year of SAMOKIKE project was an external factor quite unexpected. In the future, it is important to predict and prepare for risks, especially those associated with tensions between different tribes.
3) PROTECO Despite rooms for improvements for both JICA and NGO, after three years of experience in PROTECO,

Final Report SAMOKIKE March 2008
46
SAMOIKIKE project recommends PROTECO to progress as a collaborated program between JICA and NGO to each exercise their strength. This is expected to also create examples of synergy between the government policy and the grass-root activity. Since HANDS had committed since from the pre-project survey, SAMOKIKE project has benefited from building network with related Kenyan stakeholders from the beginning and presence of collaboration with JICA contributed hugely to appeal to Kenyan government. Furthermore, JICA’s presence helped SAMOKIKE project to be well recognized by the Kenyan government. We strongly believe that this indicates a possibility for a grass-root achievements to be reflected in government policy making.
Final Report SAMOKIKE March 2008
47
Chapter 4. History of Project Design Matrix
As a result of three changes in the policies of Health Program and after the review of the Project mid-term evaluation, the SAMOKIKE project needed to change its indicators and activities on the later half of 2006. Following the discussions at the NTWC meeting of July 2007, revised PDM was approved by the head of Reproductive Health Office, and finalized for M/M in September 2007.
First, indicators and activities related to drug and supply management was changed. This was due to the transition in the Kenyan drug and supply distribution system that had previously been PUSH system, in which MOH supply fixed amount of drug and supply. However, the system is now transitioning gradually at various District and Provincial levels to PULL system in which health facilities order the required amount. It is anticipated that some more time is required before the change to become effect at HC level.
Second, indicators and activities related to HMIS improvement was changed. This was because DANIDA (Danish International Development Agency) has started to test a new form of HMISHealth Management Information System�in certain Districts, which included one of SAMOIKIE project’s target District. However, it has not been decided whether the MOH might change its HMIS policy throughout all the Districts.
Third, indicators related to improvement in the capacity of Community Health Workers (CHWs) were changed. This was because the MOH announced its new guidelines regarding community healthcare activities in 2006, which clarified requirements, roles, and activities of CHWs.
After the mid-term evaluation, it was pointed out that the correlation of the SAMOIKE project’s activities and their outcomes were unclear. Therefore, the Project regrouped the target outputs and related activities so that hey are measurable. In addition, SAMOKIKE project added the activities of capacity building of HC managers and education on waste management to improve health management as based on the baseline surveys. Moreover, the mid-term evaluation team and NTWC had mentioned that the indicators were abstract and not easily measured in PDM0. Therefore, the amended PDM1 contains indicators that are more specific. Further details are shown in Appendix 4-3.�

Final Report SAMOKIKE March 2008
49
Chapter 5. Appendices
Appendix 1� Activity summary � Appendix 1-1� Training and Workshop � Appendix 1-2� Community meeting and Campaign � Appendix 1-3� Maternal care and Stakeholder Meeting Appendix 2� Donation list � Appendix 2-1� Equipment list � Appendix 2-2� List of Equipment provided through JICA � Appendix 2-3� List of Equipment provided through HANDS � Appendix 2-4� Renovation of facility Appendix 3� SAMOKIKE Project PO Appendix 4� PDM
Appendix 4-1� PDM02005�Appendix 4-2� PDM12007�Appendix 4-3� PDM changes
Appendix 5� IEC material Appendix 6� Minutes of JNPSC/NTWC meeting
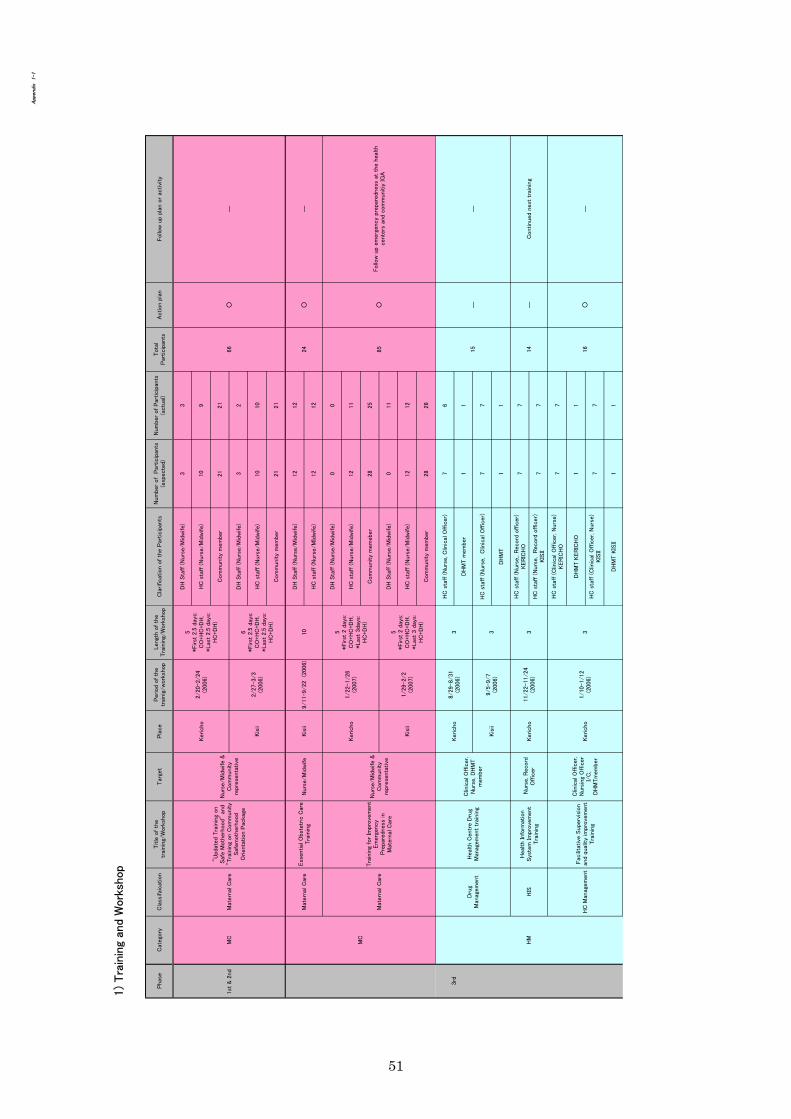
51

52
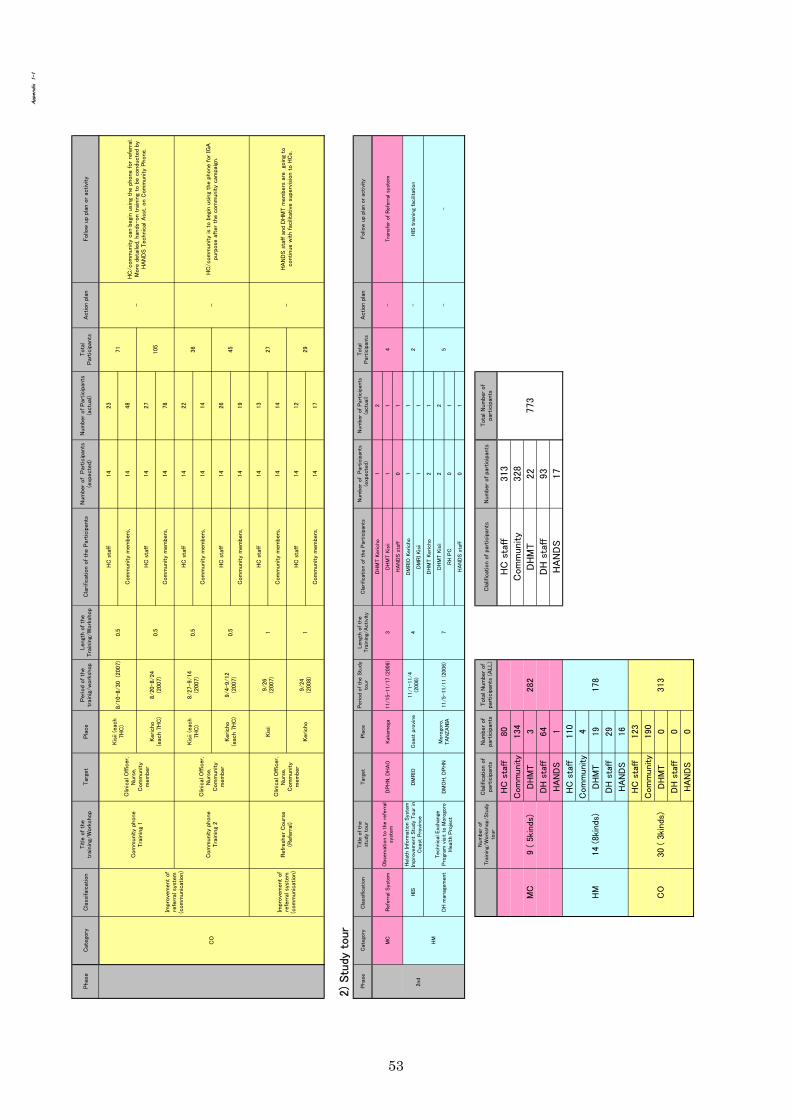
53
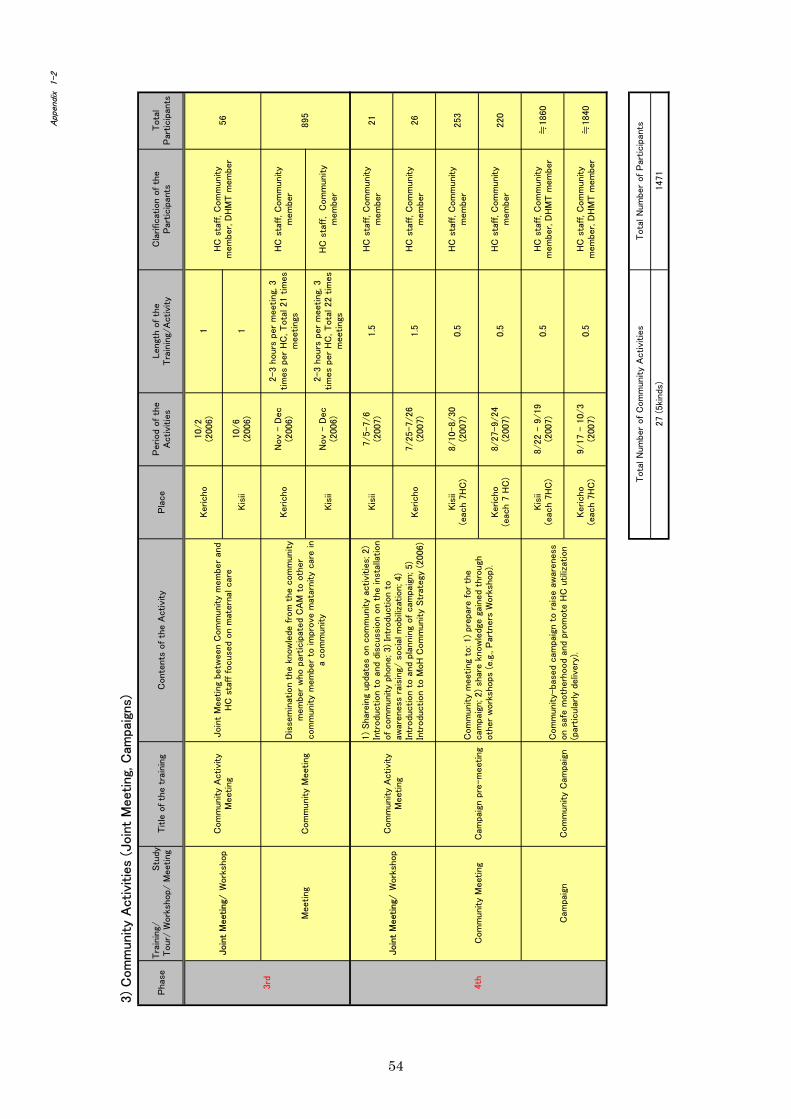
54

55

Equ
ipm
ent L
ist
Safe
Mot
herh
ood
Proj
ect i
n K
isii
and
Ker
icho
(SA
MO
KIK
E) JI
CA
-HA
ND
S-M
oH 2
005-
2008
#D
eliv
ery
date
Item
Mod
el/T
ype
etc.
unit
Am
ount
(KSH
)D
eliv
ery
com
pany
Allo
catio
nM
anag
emen
t in
char
ge(M
oH)
Rem
arks
1st P
hase
(200
5.M
arch
-Dec
embe
r)1
2005
-03-
28V
ideo
cam
era
DC
R-H
C42
E JE
31s
et57
,547
Japa
npu
rcha
seK
isii
DM
OH
220
05-0
3-28
Dig
ital c
amer
aPo
wer
shor
t A52
01
37,8
61Ja
pan
purc
hase
Ker
icho
DM
OH
320
05-0
3-28
Com
pute
rpro
ject
orEM
O-7
451
212,
292
Japa
npu
rcha
seK
eric
hoD
MO
H4
2005
-04-
18In
k-je
tprin
ter
HP
Des
kjet
3845
210
,000
INTE
LLI S
OLU
TIO
NS
Kis
ii &
Ker
icho
DM
OH
520
05-0
5-03
Lase
r prin
ter
HP1
010
126
,000
Nak
umat
tK
isii
DM
OH
2005
-05-
03La
ser p
rinte
rH
P102
026
,000
Nak
umat
tD
RH
DR
H6
2005
-06-
07C
opie
rN
ASH
UA
TEC
Cop
ier 5
16P
117
4,00
0TH
E C
OPY
CA
TK
eric
hoD
MO
H7
2005
-06-
16La
ptop
Com
pute
rTO
SHIB
Asa
telli
tepr
o A
602
378,
160
INTE
LLI S
OLU
TIO
NS
Kis
ii &
Ker
icho
DM
OH
820
05-0
9-24
Fax
tele
phon
ePa
naso
nic
KX
342
238
,000
MIB
NK
isii
& K
eric
hoD
MO
H9
2005
-10-
06C
upbo
ard
Loca
l man
ufac
ture
d16
33,2
80G
.G.K
AR
IUK
IK
isii
& K
eric
hoD
MO
H10
2005
-10-
14V
inyl
Pel
vic
Mod
el S
et1s
et63
,849
Japa
npu
rcha
seK
eric
hoD
MO
H
1120
05-1
0-27
Pow
er g
ener
ator
SH32
00EX
Ele
max
Hon
da 2
.6K
VA
Gen
erat
or S
.No.
1123
119.
1123
093
212
2,96
0Pr
otec
h In
dust
rial
E qui
pmen
tIr
anda
,C
hepk
emel
HC
DM
OH
1220
05-1
1-01
Com
pute
rpro
ject
orEP
SON
PR
OJE
CT
EMP-
TW10
199
,011
Off
ice
Mar
tK
isii
DM
OH
1320
05-1
1-01
Cop
ier
Can
non
FC12
01
37,8
16D
elig
htK
isii
DM
OH
1420
05-1
1-01
Scan
ner
HP
Scan
njet
2400
17,
888
Del
ight
Ker
icho
DM
OH
1520
05-1
1-03
Lapt
op C
ompu
ter
Tosh
iba
Tecr
a A
5S41
65
815,
000
INTE
LLI S
OLU
TIO
NS
DR
H(1
),Kis
ii2
,Ker
icho
(2)
DR
H/D
MO
H
1720
05-1
1-18
Whe
elch
air
1616
8,00
0B
IO-Z
EQ K
ENY
AK
isii
& K
eric
hoD
MO
H
1820
05 Ju
ne-O
ct.
Off
ice
furn
iture
(Det
ail i
s sho
wn
in b
elow
)14
582,
080
Loca
l man
ufac
ture
d an
dot
hers
Kis
ii &
Ker
icho
DM
OH
1920
05-1
0-31
Toyo
ta L
andc
ruis
er H
ard
Stat
ionw
agon
Std
.H
ZJ10
5R-G
CM
RS
Engi
ne: 4
164c
c di
esel
eng
ine
Tran
smis
sion
: 5 sp
eed
man
ual g
earb
ox@
2,72
3,70
02
5,44
7,40
0TO
YO
TA E
ast A
fric
aLt
d.K
isii
& K
eric
hoD
MO
H
2020
05-1
1-02
Toyo
ta L
andc
ruis
er H
ardt
opA
mbu
lanc
eH
ZJ78
R-R
JMR
S
Engi
ne: 4
164c
c di
esel
eng
ine
Tran
smis
sion
: 5 sp
eed
man
ual g
earb
ox@
3,30
0,00
02
6,60
0,00
0TO
YO
TA E
ast A
fric
aLt
d.K
isii
& K
eric
hoD
MO
H
56

#D
eliv
ery
date
Item
Mod
el/T
ype
etc.
unit
Am
ount
(KSH
)D
eliv
ery
com
pany
Allo
catio
nM
anag
emen
t in
char
ge(M
oH)
Rem
arks
2nd
Phas
e (2
006.
Janu
ary-
Mar
ch)
120
06-0
2-22
Shre
dder
CO
MX
Stra
ight
cut
TLH
320
121
,599
Off
ice
Mar
tK
eric
hoD
MO
H20
06-0
2-22
Lam
inat
or25
,000
Off
ice
Mar
tK
isii
& K
eric
hoD
MO
H
220
06-0
3-10
Mat
erni
ty c
are
mat
eria
ls(S
tep
Stoo
l, In
stru
men
t Tro
lley
with
1dr
awer
, Drip
stan
d, E
xam
inat
ion
couc
hes
1453
2,40
0C
RO
WN
HEA
LTH
CA
RE
Kis
ii &
Ker
icho
DM
OH
320
06-0
3-15
Mic
roph
one
BO
SS/M
EGA
139
,000
ECO
TEC
HK
eric
hoD
MO
H5
2006
-03-
20La
ptop
Com
pute
rTo
shib
a Te
cra
A5S
416
119
1,40
0IN
TELL
I SO
LUTI
ON
SD
RH
DR
H7
2006
-03-
20B
inde
rLo
calp
urch
ase
120
,995
Off
ice
Mar
tK
eric
hoD
MO
H
820
06-0
3-21
Pow
er g
ener
ator
ELEM
AX
/HO
ND
A E
NG
INE
GEN
ETR
ATO
RS
SH46
00 E
X-R
220
0,00
0Pr
otec
hR
iota
nchi
,K
abia
n ga
HC
DM
OH
3rd
Phas
e (2
006.
July
-200
7.M
arch
)1
2007
-01-
18M
ater
nity
Exp
erie
nce
jack
etJa
pane
sepu
rcha
se2
77,8
62K
ubot
a ed
ucat
ion
Kis
ii &
Ker
icho
DM
OH
220
07-0
2-12
Del
iver
y be
dLo
calp
urch
ase
136
,000
CR
OW
NK
abia
nga
HC
DM
OH
320
07-0
2-19
Whi
te b
oard
Loca
lpur
chas
e16
142,
400
VA
NG
UA
RD
Kis
ii &
Ker
icho
DM
OH
420
07-0
3-09
Cae
sare
an o
pera
tion
char
tLo
cal p
urch
ase
1656
,272
CR
OW
NK
isii
& K
eric
hoD
MO
H5
2007
/3/
"Sim
u ya
Jam
ii" S
olae
pan
elK
yose
ra K
C40
T-1
1425
2,00
0Te
lesa
les s
olar
Kis
ii &
Ker
icho
DM
OH
620
07/3
/"S
imu
ya Ja
mii"
Sol
a-ba
ttery
Vol
tmas
ter 1
00A
mp
Bat
tery
(3un
its/H
C)
Bat
ter y
aci
d (4
bottl
esx2
0L/H
C)
4233
4,95
0Te
lesa
les s
olar
Kis
ii &
Ker
icho
DM
OH
720
07/3
/"S
imu
ya Ja
mii"
tel
epho
neA
dond
GA
18-6
08(B
G)
1442
0,00
0A
dtel
Kis
ii &
Ker
icho
DM
OH
4th
Phas
e (2
007.
Mey
-200
8.M
arch
)
120
07-0
8-09
"Sim
u ya
Jam
ii" S
trand
cab
les
Twin
& e
arth
cab
le 6
mm
(280
m)
56,0
00K
halu
mbu
s ele
ctric
al &
Elec
troni
csK
isii
& K
eric
hoD
MO
H
220
07-0
8-09
"Sim
uya
Jam
ii"B
atte
rych
arge
rcon
trolle
rSo
llate
k Su
npow
er 6
1449
,000
Kha
lum
bus e
lect
rical
&El
ectro
nics
Kis
ii &
Ker
icho
DM
OH
320
07-0
8-10
"Sim
u ya
Jam
ii" S
olae
pan
elB
rack
et53
x65.
5x4
cm w
ith st
and
1435
,000
Kha
lum
bus e
lect
rical
&El
ectro
nics
Kis
ii &
Ker
icho
DM
OH
57

Ker
icho
/Kis
ii of
fice
furn
iture
(Del
iver
ed 2
005-
2006
)Ite
mU
nit
Inst
alle
d1
Des
k(Im
port)
6K
eric
ho o
ffic
e2
Des
k(Lo
cal m
ade)
3K
eric
ho o
ffic
e3
Cha
ir(C
aste
r)6
Ker
icho
off
ice
4C
hair(
Pipe
)6
Ker
icho
off
ice
5C
hair(
Fold
type
)6
Ker
icho
off
ice
6B
ook
Shel
f3
Ker
icho
off
ice
7C
abin
etLa
rge
1K
eric
ho o
ffic
e8
Side
cab
inet
2K
eric
ho o
ffic
e9
Com
pute
tabl
e1
Ker
icho
off
ice
10Ta
ble
3K
eric
ho o
ffic
e11
Mee
ting
tabl
e se
t1
Ker
icho
off
ice
12Sa
fe1
Ker
icho
off
ice
13D
esk
4K
isii
offic
e14
Cha
ir(C
aste
r)5
Kis
ii of
fice
15C
hair(
Fold
type
)3
Kis
ii of
fice
16C
abin
et3
Kis
ii of
fice
17Ta
ble
2K
isii
offic
e
58

Item
Kis
iiK
eric
hoR
emar
ks
IM
ED
ICA
L E
QU
IPM
EN
T
AD
EL
IVE
RY
SE
T1
Kid
ney
Dis
h (L
arge
)10
55
35
85
546
00
33
20
54
172
Kid
ney
Dis
h (M
ediu
m)
148
81
56
88
588
63
20
28
534
3A
rtery
For
ceps
95
55
56
55
456
54
57
05
537
4G
allip
ot8
55
33
65
540
60
05
10
53
205
Cor
d Sc
isso
r9
53
55
85
545
104
55
55
35
426
Epis
ioto
my
Scis
sor
94
35
46
54
405
53
24
42
429
7C
ord
Cla
mp
1810
109
1010
1010
8716
1010
610
1010
577
8D
isse
ctin
g Fo
rcep
s Too
thed
105
55
51
55
4110
55
05
05
535
9D
isse
ctin
g Fo
rcep
s Non
Too
thed
105
55
57
55
476
55
45
15
536
10B
owl
100
40
38
55
350
51
50
05
218
11Sp
onge
Hol
ding
For
ceps
81
01
10
55
218
00
10
02
011
12N
eedl
e H
olde
r4
33
33
13
323
30
30
31
33
1613
Scis
sor
53
33
33
33
265
33
33
33
326
14Sp
ecul
um4
32
13
03
319
20
00
00
30
5
BD
IAG
NO
STIC
SE
T1
Clin
ical
The
rmom
eter
55
05
05
525
05
05
05
015
2Sy
phig
nom
anom
eter
12
31
01
210
02
03
12
08
3A
dult
Wei
ghin
g Sc
ale
11
01
00
14
11
01
01
04
4B
aby
wei
ghin
g sc
ale
11
11
01
16
11
01
01
04
5St
etho
scop
e1
31
10
22
101
00
21
20
66
Tape
Mea
sure
22
12
12
212
11
11
12
18
7Pr
egna
ncy
Cal
cula
tor
52
22
22
22
194
22
22
22
218
CM
AC
HIN
ER
Y
1El
ectri
c Fo
etos
cope
21
11
11
11
92
11
11
11
19
#2: T
wo
(2) t
o ea
ch D
istri
ct H
ospi
tal a
nd o
ne(1
) to
each
Hea
lth C
entre
(HC
)2
Aut
ocla
ve1
12
11
23
Oxy
gen
gene
rato
r1
11
1
DO
TH
ER
ME
DIC
AL
EQ
UIP
ME
NT
1W
heel
Cha
ir fo
r Adu
lt1
01
11
11
17
10
11
11
11
72
Step
Sto
ol0
00
00
00
60
01
11
11
16
3B
aby
Cot
11
11
01
16
01
01
01
03
4Tr
olly
with
One
Dra
wer
64
Sam
e as
#1
Sam
e as
#1
#3: A
lloca
tion
will
be
dete
rmin
ed b
y th
eD
istri
ct.
Kis
iiK
eric
ho
#1: T
he q
uant
ity o
f the
equ
ipm
ent t
o be
dona
ted
was
det
erm
ined
by
Tech
nica
l Adv
isor
on M
ater
nal C
are
base
d on
the
faci
lity
asse
ssm
ent.
Don
atio
n L
ist (
Dom
ain
of M
ater
nal C
are)
JIC
A /
HA
ND
S / M
oH S
afe
Mot
herh
ood
Proj
ect
59

5D
rip S
tand
74
6Ex
amin
atio
n C
ouch
31
7Ex
amin
atio
n La
mp
on C
asto
rs6
3
EE
QU
IPM
EN
T F
OR
INFE
CT
ION
PR
EV
EN
TIO
N
1D
ust B
ox1
11
11
11
71
11
11
11
7#4
: One
(1) f
or e
ach
HC
2G
um B
oots
22
22
22
214
22
22
22
214
#5: T
wo
(2) f
or e
ach
HC
3Pe
dal B
in2
22
22
212
22
22
84
Rub
ber M
acki
ntos
h5
33
33
33
326
53
33
33
33
265
Gre
en T
owel
(Lar
ge)
331
124
6G
reen
Tow
el (M
ediu
m /
Smal
l)58
238
7C
over
for S
teril
e C
hettl
e Fo
rcep
Con
tain
er84
8M
othe
r's G
own
3821
9M
idw
ife's
Gow
n 38
IIT
RA
ININ
G M
OD
EL
1V
inyl
Pel
vic
Mod
el S
et1
11
12
New
born
Bab
y M
odel
11
11
#7: D
onat
ed to
the
Dis
trict
Rep
rodu
ctiv
eH
ealth
Tea
ms
Sam
e as
#1
#6: T
he sa
me
budg
et w
as a
lloca
ted
to tw
odi
stric
t to
mak
e gr
een
tow
els a
nd o
ther
s. Th
ety
pes a
nd q
uant
ity o
f the
se g
oods
wer
e ba
sed
on th
e pr
opos
al fr
om e
ach
dist
rict.
60
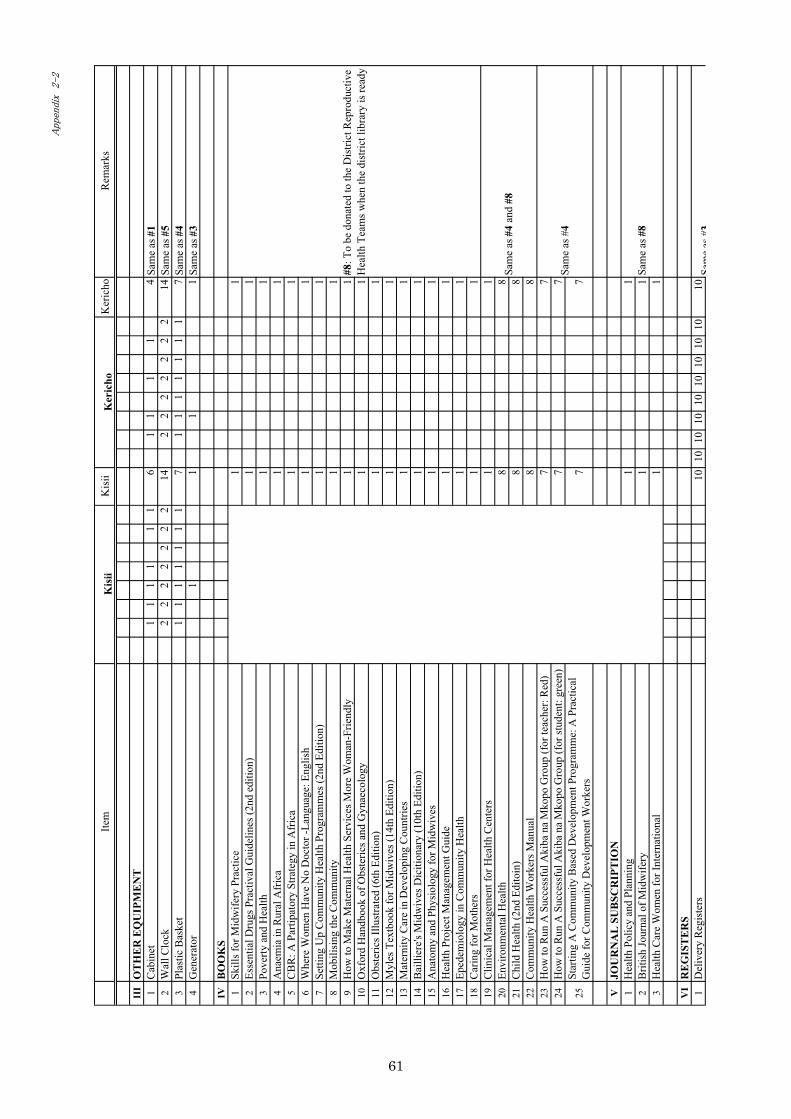
Item
Kis
iiK
eric
hoR
emar
ks
III
OT
HE
R E
QU
IPM
EN
T1
Cab
inet
11
11
11
61
11
14
Sam
e as
#1
2W
all C
lock
22
22
22
214
22
22
22
214
Sam
e as
#5
3Pl
astic
Bas
ket
11
11
11
17
11
11
11
17
Sam
e as
#4
4G
ener
ator
11
11
Sam
e as
#3
IVB
OO
KS
1Sk
ills f
or M
idw
ifery
Pra
ctic
e1
12
Esse
ntia
l Dru
gs P
ract
ival
Gui
delin
es (2
nd e
ditio
n)1
13
Pove
rty a
nd H
ealth
11
4A
naem
ia in
Rur
al A
fric
a1
15
CB
R: A
Par
tipat
ory
Stra
tegy
in A
fric
a1
16
Whe
re W
omen
Hav
e N
o D
octo
r -La
ngua
ge: E
nglis
h1
17
Setti
ng U
p C
omm
unity
Hea
lth P
rogr
amm
es (2
nd E
ditio
n)1
18
Mob
ilisi
ng th
e C
omm
unity
11
9H
ow to
Mak
e M
ater
nal H
ealth
Ser
vice
s Mor
e W
oman
-Frie
ndly
11
10O
xfor
d H
andb
ook
of O
bste
rics a
nd G
ynae
colo
gy1
111
Obs
teric
s Illu
stra
ted
(6th
Edi
tion)
11
12M
yles
Tex
tboo
k fo
r Mid
wiv
es (1
4th
Editi
on)
11
13M
ater
nity
Car
e in
Dev
elop
ing
Cou
ntrie
s1
114
Bai
llier
e's M
idw
ives
Dic
ition
ary
(10t
h Ed
ition
)1
115
Ana
tom
y an
d Ph
ysio
logy
for M
idw
ives
11
16H
ealth
Pro
ject
Man
agem
ent G
uide
11
17Ep
edem
iolo
gy in
Com
mun
ity H
ealth
11
18C
arin
g fo
r Mot
hers
11
19C
linic
al M
anag
emen
t for
Hea
lth C
ente
rs1
120
Envi
ronm
enta
l Hea
lth8
821
Chi
ld H
ealth
(2nd
Edi
toin
)8
822
Com
mun
ity H
ealth
Wor
kers
Man
ual
88
23H
ow to
Run
A S
ucce
ssfu
l Aki
ba n
a M
kopo
Gro
up (f
or te
ache
r: R
ed)
77
24H
ow to
Run
A S
ucce
ssfu
l Aki
ba n
a M
kopo
Gro
up (f
or st
uden
t: gr
een)
77
25St
artin
g A
Com
mun
ity B
ased
Dev
elop
men
t Pro
gram
me:
A P
ract
ical
Gui
de fo
r Com
mun
ity D
evel
opm
ent W
orke
rs7
7
VJO
UR
NA
L S
UB
SCR
IPT
ION
1H
ealth
Pol
icy
and
Plan
ning
11
2B
ritis
h Jo
urna
l of M
idw
ifery
11
3H
ealth
Car
e W
omen
for I
nter
natio
nal
11
VI
RE
GIS
TE
RS
1D
eliv
ery
Reg
iste
rs10
1010
1010
1010
1010
10
Kis
iiK
eric
ho
#8: T
o be
don
ated
to th
e D
istri
ct R
epro
duct
ive
Hea
lth T
eam
s whe
n th
e di
stric
t lib
rary
is re
ady
Sam
e as
#4
and
#8
Sam
e as
#8
Sam
eas
#3
Sam
e as
#4
61
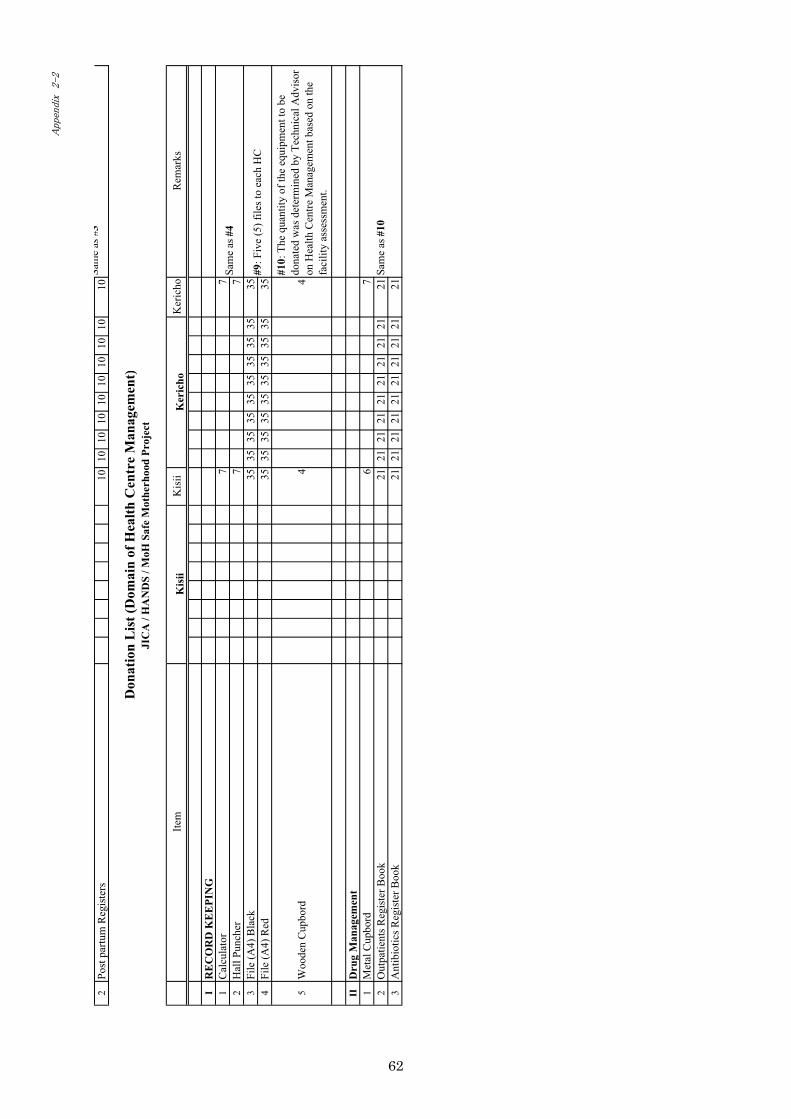
2Po
st p
artu
m R
egis
ters
1010
1010
1010
1010
1010
Item
Kis
iiK
eric
hoR
emar
ks
IR
EC
OR
D K
EE
PIN
G1
Cal
cula
tor
77
2H
all P
unch
er7
73
File
(A4)
Bla
ck35
3535
3535
3535
3535
354
File
(A4)
Red
3535
3535
3535
3535
3535
5W
oode
n C
upbo
rd4
4
#10:
The
qua
ntity
of t
he e
quip
men
t to
bedo
nate
d w
as d
eter
min
ed b
y Te
chni
cal A
dvis
oron
Hea
lth C
entre
Man
agem
ent b
ased
on
the
faci
lity
asse
ssm
ent.
IID
rug
Man
agem
ent
1M
etal
Cup
bord
67
2O
utpa
tient
s Reg
iste
r Boo
k21
2121
2121
2121
2121
213
Ant
ibio
tics R
egis
ter B
ook
2121
2121
2121
2121
2121
Sam
e as
#10
Sam
e as
#4
#9: F
ive
(5) f
iles t
o ea
ch H
C
Don
atio
n L
ist (
Dom
ain
of H
ealth
Cen
tre
Man
agem
ent)
JIC
A /
HA
ND
S / M
oH S
afe
Mot
herh
ood
Proj
ect
Kis
iiK
eric
ho
Sam
eas
#3
62
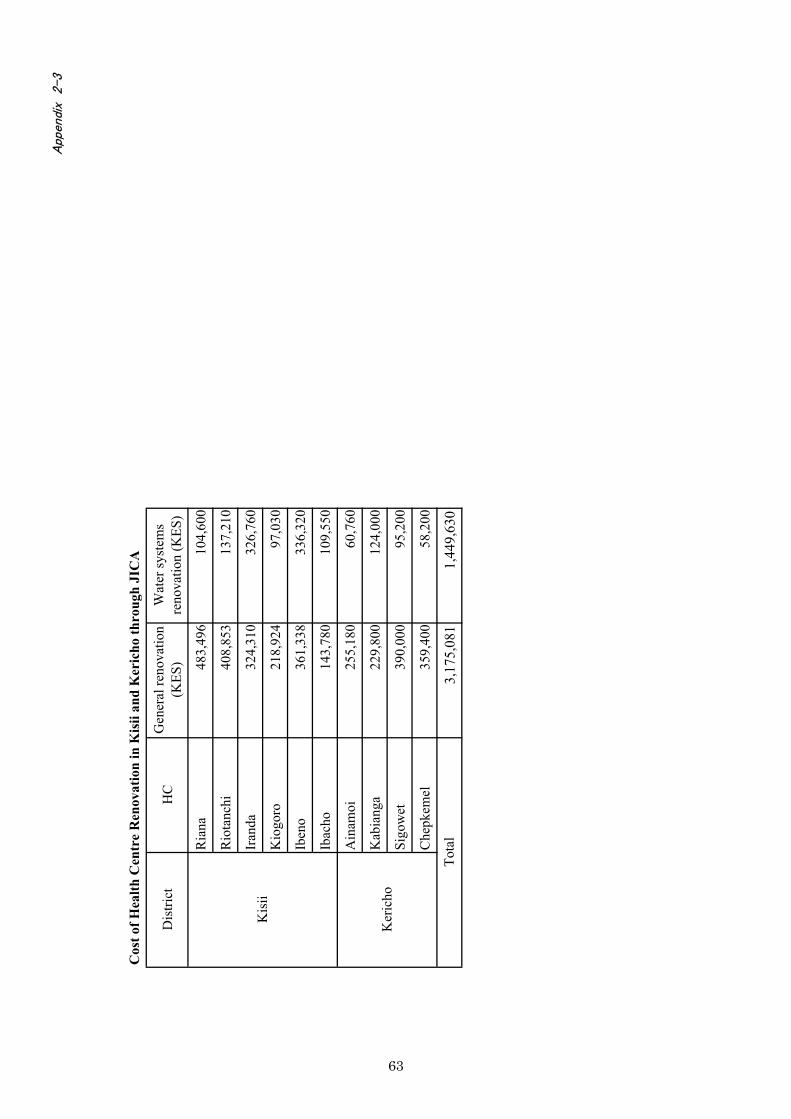
Cos
t of H
ealth
Cen
tre
Ren
ovat
ion
in K
isii
and
Ker
icho
thro
ugh
JIC
A
Dis
trict
HC
Gen
eral
reno
vatio
n(K
ES)
Wat
er sy
stem
sre
nova
tion
(KES
)
Ria
na48
3,49
610
4,60
0
Rio
tanc
hi40
8,85
313
7,21
0
Iran
da32
4,31
032
6,76
0
Kio
goro
218,
924
97,0
30
Iben
o36
1,33
833
6,32
0
Ibac
ho14
3,78
010
9,55
0
Ain
amoi
255,
180
60,7
60
Kab
iang
a22
9,80
012
4,00
0
Sigo
wet
390,
000
95,2
00
Che
pkem
el35
9,40
058
,200
3,17
5,08
11,
449,
630
Kis
ii
Ker
icho
Tota
l
63

Ann
ex 3
���������
�� ����������
����� � ����������������
�����
����������
���������
���� �
����
!"!
�����
���� �
����
�������#
���� �
���$��
!��%����&
���� �
����
�%����&
���� �
���'�(�!��%����)
������� ��
������� � ���
����
������
��� �
�
������
��� �
�
������
��� �
�
������� � ���
����
������
��� �
�
������
��� �
�
������
��� �
�
������� � ���
����
������� � ���
����
������
��� �
�
������
��� �
�
������
��� �
�
������� � ���
����
������
��� �
�
������
��� �
�
������
��� �
�
������� � ���
����
������
��� �
�
������
��� �
�
������
��� �
�
������� � ���
����
������
��� �
�
������
��� �
�
������� � ���
����
������
��� �
�
������� � ���
����
������
��� �
�
������
��� �
�
������� � ���
����
������
��� �
�
������� � ���
����
������
��� �
�
������� � ���
����
������
��� �
�
������� � ���
����
������
��� �
�
������
��� �
�
������� � ���
* ���
��
��������
�+������
�
,,
���&
-����������
��� ������.
���!�� %�/��� �
���)
������ �.������� ����
����
���#
�, ����
��
-����������
� �� �0�
�����12�
���"3
+,�
-����������
� �� �4��.5.���!�� %6
������ �.������� ������$�
��
.��������
� ��
-���������
��� ������7
�!"����
�"����
-����������
��� �������
� ������.
����0���8���3
+#
�&
9,�
,)
������ �.������� ���,
-���������
��� ������/
��� ���
���"
����
-����������
� �� �07
�!"����
�"���� 6
*
�!(�
�� ���
�0:�������� !
� ��
;�<
=�� �3
.���!�� %�>�
����
��� !�%
7�!"��!���%
*,�
&,
�)
+,�
#&
)9
,�
,,
9
-����������
� �� �0�
��������%
��3
�#
*�
�+
,,
,�
,
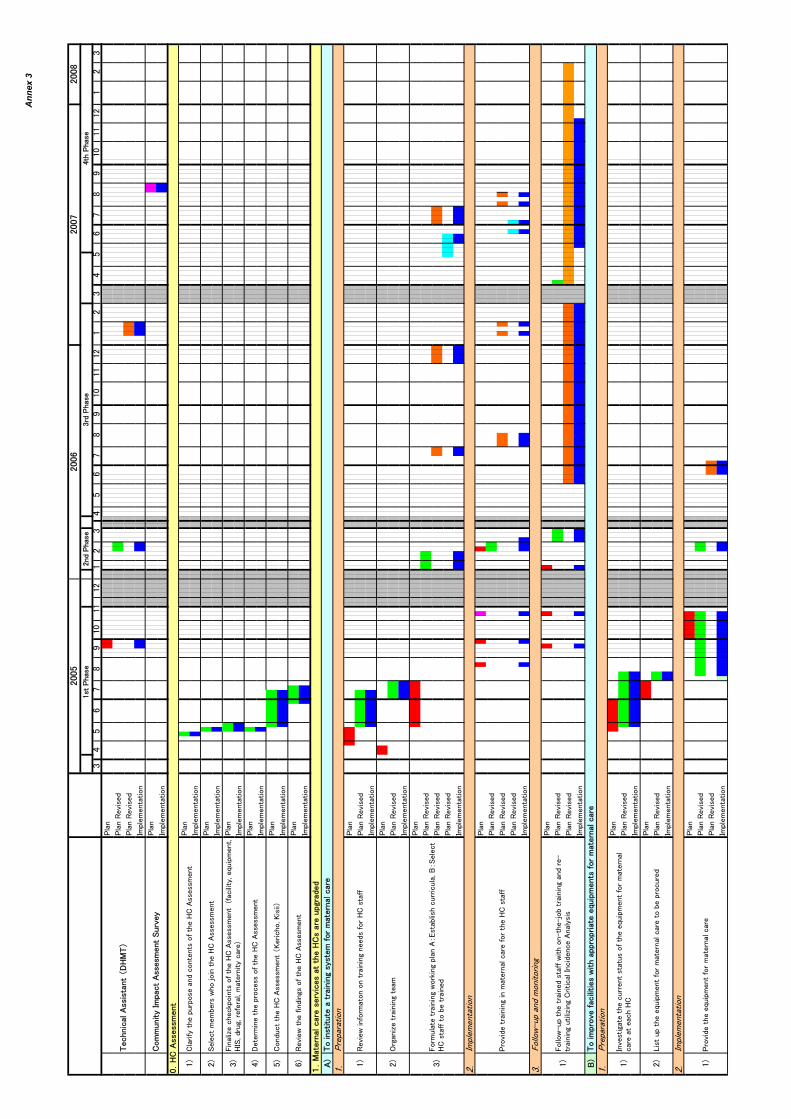
Ann
ex 3
* ���
��
��������
�+������
�
,,
���&
���)
����
���#
�, ����
��
+,�
+#
�&
9,�
,)
**
,�
&,
�)
+,�
#&
)9
,�
,,
9�
#*
��
+,,
,�
,����
������
��� �
�
������
��� �
�
������� � ���
����
������� � ���
����
������� � ���
����
������� � ���
����
������� � ���
����
������� � ���
����
������� � ���
����
������� � ���
�3
,?����
������
��� �
�
������� � ���
����
������
��� �
�
������� � ���
����
������
��� �
�
������
��� �
�
������
��� �
�
������� � ���
�?����
������
��� �
�
������
��� �
�
������
��� �
�
������� � ���
+?����
������
��� �
�
������
��� �
�
������� � ���
>3
,?����
������
��� �
�
������� � ���
����
������
��� �
�
������� � ���
�?����
������
��� �
�
������
��� �
�
������� � ���
-����������
� �� �47/�-6
:� �!� ����@!
���� ������� ����������� ��(�����!���
,3
.���!�� %���
�� ��
� �
�� ��!���%
�3
�"��
�A�� ������"� ���
'����81!
���
�����
� ����"
,3
'����
81!� ��� ������� ����8� ����1 ��1��(� ������"���
����1
������"�! ���A��"�.�� ����������������
���%
�
����
�� ���
,3
����
�"� �� ����!���� � � ! ���� ����@!
���� ������� �����
������ ����
��/
.
,3
#3
�����8� ���������" ���� ���/
.��
� �
��
�3
'���
!�� �� ������"�8��2��"������
B� �(
�� ���!����!��;�>B�����
/.� ���� ��(�� ������
�����
�� � ���
�����8�������
� ������ ������"�����
�����/.� ���
�3
����� ����(�
� �8
�������� ���/
.��
� ���
�3
.���!� � ���/
.��
�
��� �4�������;��� ��6
.�����%� ���!�� �
�������� �� ���� ���/
.��
� ���
+3
+3
'�����A������2
��� ���� ���/
.��
� ��� ��0������ %;��@!
���� ;
/��;���!";��������;��� ���� %�����3
*3
7� ���
���� ������� ���� ���/
.��
� ���
�C/.��
�
���
,3
DC�� ����������� ������ �� � ���/
. �����!"���
��
����
�� ���
�����
�� � ���
-���� � ! ���� ������"� %
��������� ����������
�������
� ������"�����
� ��������������� ���/
.� ���
�������
� ����@!
���� ������� ����������
-��������
����
��� �� �8� ���
����� ���@!
���� ������� ����������

Ann
ex 3
* ���
��
��������
�+������
�
,,
���&
���)
����
���#
�, ����
��
+,�
+#
�&
9,�
,)
**
,�
&,
�)
+,�
#&
)9
,�
,,
9�
#*
��
+,,
,�
,����
������
��� �
�
������� � ���
����
������
��� �
�
������
��� �
�
������� � ���
����
������
��� �
�
������
��� �
�
������� � ���
+?
����
������
��� �
�
������
��� �
�
������� � ���
.3
����
������� � ���
����
������� � ���
����
������� � ���
����
������� � ���
73
����
������� � ���
����
������� � ���
����
������
��� �
�
������� � ���
����
������
��� �
�
������� � ���
����
������
��� �
�
������� � ���
�3
����
������
��� �
�
������� � ���
����
������
��� �
�
������� � ���
����
������� � ���
����
������
��� �
�
������� � ���
���� �
� ��������� �������
� � ���
� ����������
*3
�������
� ��� ������"� ��/
.� ������� ���(�
��������!"���
��������
� !
��� ����
�"����
�3
+3
*3
�������
� ������"��(
�! ���
��%��������� ����@!
���� ������� �����
�����0�?"?� �����A� ���;����
�"���� ���� ����@!
���� 3
�3
'����81!
���
�����
� ����"
,3
'����
81!���
������ ��� ���/
.�������
���
7���
�������
� ��%�����
���� ����@!
���� ������� ����������
'����
81!���
������ ��� ������ ���! ���
����
��� ���� ���@!��� %
�����!"����
�"����
+3
�� ���!
������� �
�������� � ��� ����/.
,3
'����
81!���
������ ���������12�
���"������� ����������
�3
�� ���!
������� �
�������� � �� ����
���
��/. ��
��� ����
,3
7���
�������
� ��%�����
������!"���
���������� !
���
���
�"���� �(�
������ ���/
.��
� ���
�3
� �(
�� ���
���"
���� � %
���������!" ������������� !
���
+3
7���
���������� �
��"!
������� ������
����� ��! �
������!" ����
�������� !
���
,3
,3
,3
,3
+3
.���!
� ���"!
�������� ����
������ ����@!
���� ������� �����
����
7���
���"!
������� ��(
�! ���
��%��������� ����@!
���� ����
�� ����������
������
��8
� ��� !
�%� %
���� � ���/
.
'����81!
���
�����
� ����"
'���
!�� ��������
������� �(�
������ ���/
.��
� ���
-��������
�������12�
���"������� ����������
-��������
�����
��� �� ���� ���/
. �������
� � ���
� ����������
-��������
���!"���
���������� !
��� ����
�"���� ������� ����������
������
�� ���/
.����
��� �� ��E�
� ����� ���8
� ��� !
�%� %
��
(� �
����� ���/
.��
� ���
'����81!
���
�����
� ����"
'����81!
���
�����
� ����"
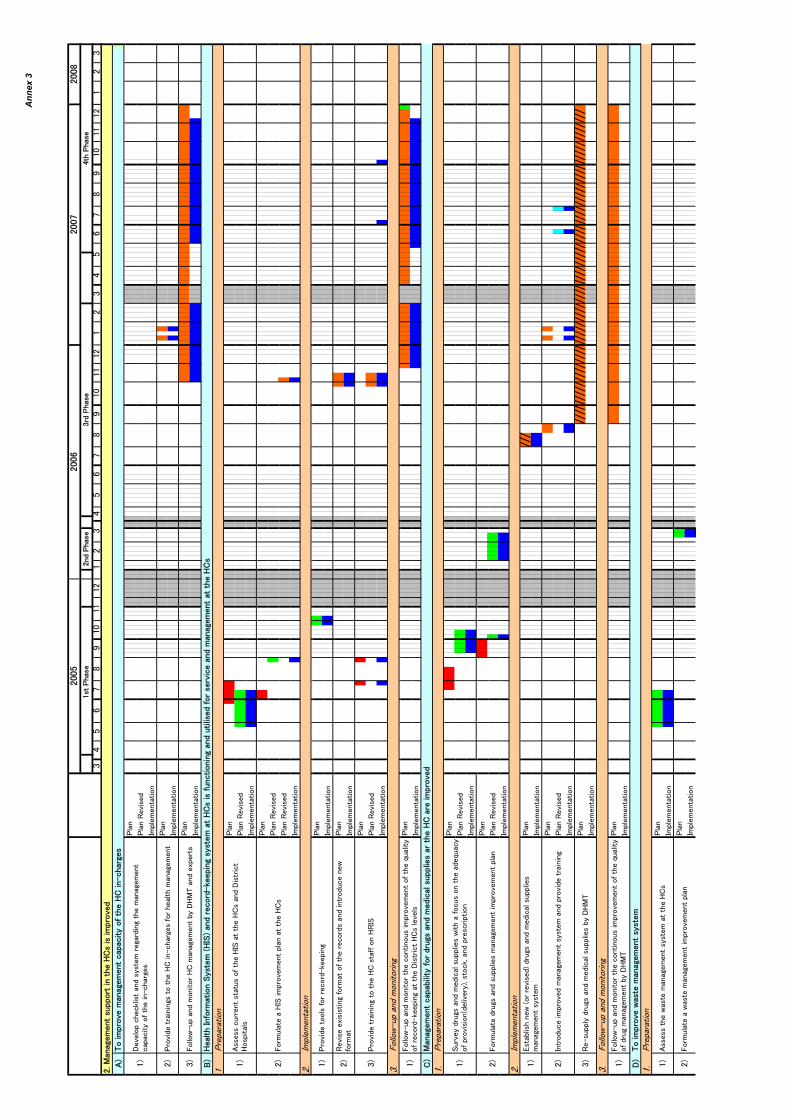
Ann
ex 3
* ���
��
��������
�+������
�
,,
���&
���)
����
���#
�, ����
��
+,�
+#
�&
9,�
,)
**
,�
&,
�)
+,�
#&
)9
,�
,,
9�
#*
��
+,,
,�
,
�3
����
������
��� �
�
������� � ���
����
������� � ���
����
������� � ���
>3
,����
�� ���
����
������
��� �
�
������� � ���
����
������
��� �
�
������
��� �
�
������� � ���
�?����
������� � ���
����
������� � ���
����
������
��� �
�
������� � ���
+?����
������� � ���
.3
,?����
������
��� �
�
������� � ���
����
������
��� �
�
������� � ���
�?����
������� � ���
����
������
��� �
�
������� � ���
����
������� � ���
+?����
������� � ���
73
,?����
������� � ���
����
������� � ���
'����
81!���
������ ��� ������ ���! ���
����
��� ���� ���@!��� %
�����!"����
�"���� �(%
�7/�-
'����81!
���
�����
� ����"
����
�� ���
���� �
��E� � ��"�����
� ���� ��������� ���
���� ���!
�����8
����
�
����
�� ���
,3
,3
� � � ���8
� ���
���"
���� � %
���� � ���/
.
� �(
�� ����8�0������� �
�3���!" ������������� !
���
���
�"���� � %
��
'���
!�� ����!" ����� !
��� ����
�"���� ���
����
��� ����
�3
,3
�3
�?����
�"���� � !
�� ���� ���/
. �� �������
�
�������
� ������" � �� ���/
.���1����"�
��������� ���
���"
����
7���
�������2�� ���
�� %
�����"�
����"� ����
���"
����
��
��� %���� �����1����"�
�3
+3
�������
� ������"� �� ���/
.� �������/
���
'����81!
���
�����
� ����"
,3
'����
81!���
������ ��� ������ ���! ���
����
��� ���� ���@!��� %
���������12�
���"�� � ���7
� ��� �/. �����
�
,3
�������
� ��� �����������12�
���"
'����
81!���
������ ���/.��
���"
���� �(%
�7/�-������E
��
,3
� � ��!���� � � ! ���� ���/
���� � ���/
. ���
��7� ���
/�
� ��
+3
�3
'���
!�� ����/
���������
��� ����
�� � ���/
.
,3
�����
�� � ���
�3
,3
+3
��1 !
�%���!" ������������� !
��� �(%
�7/�-
�� ���!
���������
�����
�"���� � %
�������������
� ������"
-��������
�8�
���
���"
���� � %
��
/��� ��������
� �����%
���0/��3���
��������12�
���"� %
���� �/. �� ��!�� �����"���
��! ��� ������� �
�������������
�"���� �� � ���/.
���
�"���� ���
�(��� %�������!"
������������� !
��� ���� ���/
.�����������
�
�����
�� � ���
�!���%���!" ������������� !
��� �8� �������! ���� ������
@!��
%������� ���0�������%3;� ��2;������� �
�� ���
�3
'���
!�� ����8
� ���
���"
���� ���
����
��� ����
-��������
����
�"���� ���
��� %���� ���/
.���1����"�
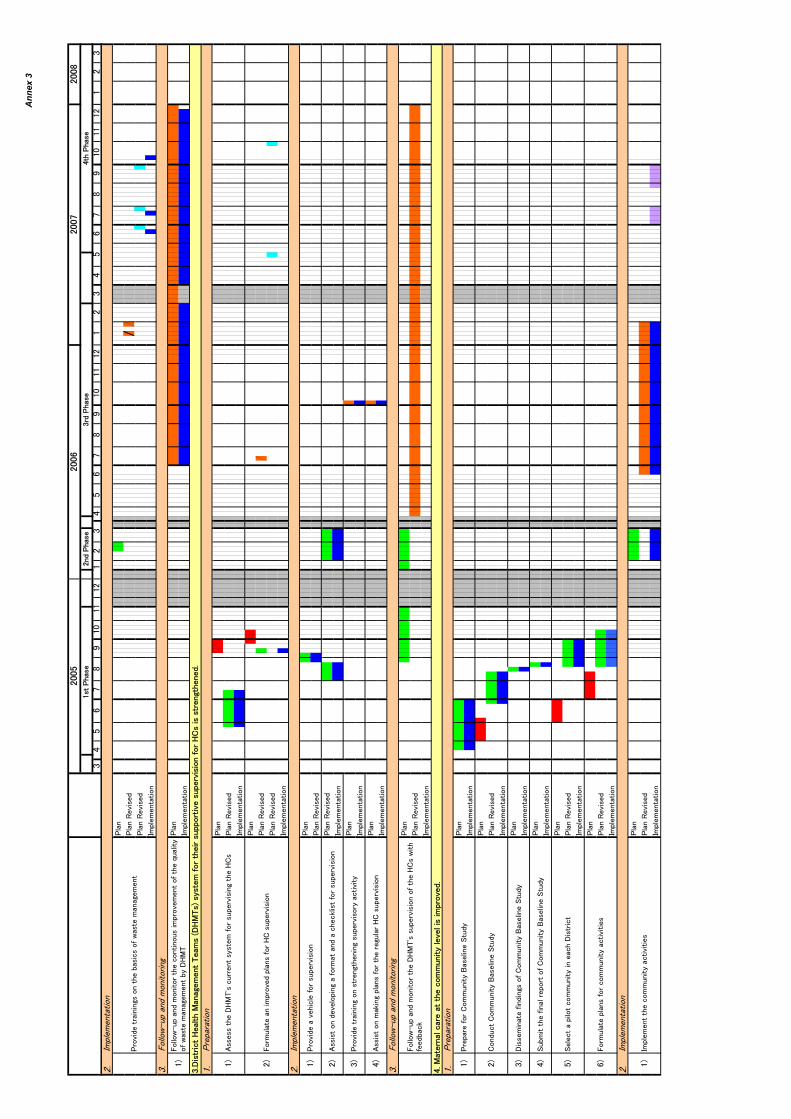
Ann
ex 3
* ���
��
��������
�+������
�
,,
���&
���)
����
���#
�, ����
��
+,�
+#
�&
9,�
,)
**
,�
&,
�)
+,�
#&
)9
,�
,,
9�
#*
��
+,,
,�
,�?
����
������
��� �
�
������
��� �
�
������� � ���
+?����
������� � ���
,?����
������
��� �
�
������� � ���
����
������
��� �
�
������
��� �
�
������� � ���
�?����
������
��� �
�
������
��� �
�
������� � ���
����
������� � ���
����
������� � ���
+?����
������
��� �
�
������� � ���
*?��� ������������ � �������!�� %�����
��� �������
�?
,?����
������� � ���
����
������
��� �
�
������� � ���
����
������� � ���
����
������� � ���
����
������
��� �
�
������� � ���
����
������
��� �
�
������� � ���
�?����
������
��� �
�
������� � ���
'����
81!���
������ ��� ���7
/�-F � !�
��� ������� ���/
. �8� �
����(
��2
����
�� ���
,3
�3
#3
'���
!�� ����� ���������!�� %���
��� ��
������� � �������!�� %���
��� ��
����
�� ���
'����81!
���
�����
� ����"
,3
.���!
� �.���!�� %�>�
������� !�%
*3
����� ������ �����!�� %�������
��7
� ���
�3
�3
'���
!�� �����������
�����
�����/.� !�
��� ���
+3
7� �
���� ��������" ����.���!�� %�>�
������� !�%
�����
�� � ���
,3
����
�������.���!�� %�>�
������� !�%
�3
*3
� � �����
�2��"����
����� �����"!
����/.� !�
��� ���
�������
� ������"���� ���" �����"� !
���� ��%��� ��� %
+3
�!(�
� � ������������
� ����.���!�� %�>�
������� !�%
,3
�������
��������������� !
���� ���
� � ��������
����"�������
� �����������2�� ����� !
���� ���
�����
�� � ���
� � � ���7
/�-F ��!���� � %
������� !
���� ��"� ���/
.
�����
�� � ���
'����81!
���
�����
� ����"
'����
81!���
������ ��� ������ ���! ���
����
��� ���� ���@!��� %
���8�
���
���"
���� �(%
�7/�-
+?7� ��� �/��� ���
���"
���� �-���
�07
/�- 3� %
������� ����� !
�� ���� !�
��� ��������/. �� � ���" �����?
,3
�������
� ������" ���� ���(�
�� ����8�
���
���"
����

Ann
ex 3
* ���
��
��������
�+������
�
,,
���&
���)
����
���#
�, ����
��
+,�
+#
�&
9,�
,)
**
,�
&,
�)
+,�
#&
)9
,�
,,
9�
#*
��
+,,
,�
,
,?����
������
��� �
�
������� � ���
����
������
��� �
�
������� � ���
����
������
��� �
�
������� � ���
����
������
��� �
�
������
��� �
�
������
��� �
�
������� � ���
�?����
������
��� �
�
������
��� �
�
������
��� �
�
������� � ���
����
������
��� �
�
������� � ���
����
������
��� �
�
������
��� �
�
������
��� �
�
������
��� �
�
������� � ���
+?����
������
��� �
�
������
��� �
�
������� � ���
����
������
��� �
�
������� � ���
����
������
��� �
�
������
��� �
�
������
��� �
�
������� � ���
����
������
��� �
�
������
��� �
�
������
��� �
�
������
��� �
�
������� � ���
����
������
��� �
�
������� � ���
-������"�/.� ������� ���"!�������
$��� �<� ������������ �� �����"�.���� ��
<� ������-���������G
��2��"�.���� ��
7� ��� ������� �.������� ����.
���� ��
,3
�3
������ �.���� ��
�� �!�����!���� �����@!
���� �� �/
. ���
��7� ��� �/�
� ��
� � ���� ��!���"� ���
�� � ����(%����
����"��E� ��"���
����� ���
�������"���8���������� �7� ��� �/�
� ��
�3
D3
.���!
� ���"!
�����!
�� ���������������
�
'����81!
���
�����
� ����"
(3�'���
!�� �����������"!������� ����� ���/
. ���
��7� ���
/�
� ��
�3
+3
,3
�?������������ %
���� ������"�
����
���!�� ������(�
8��������!�� �� ;�/
. ���
��7� ��� �/�
� �� ?
.���!
� ����� ����
���������!���� �������� ���
�� � ���
�3�'���
!�� ��������!���� �������� ���
�� � �����������
���������� �/. ���
��7� ��� �/�
� ��
�����
�� � ���
����
�� ���
� � � ����!���� ���������� %
��
'���
!�� ������������� %
���������
��� ����
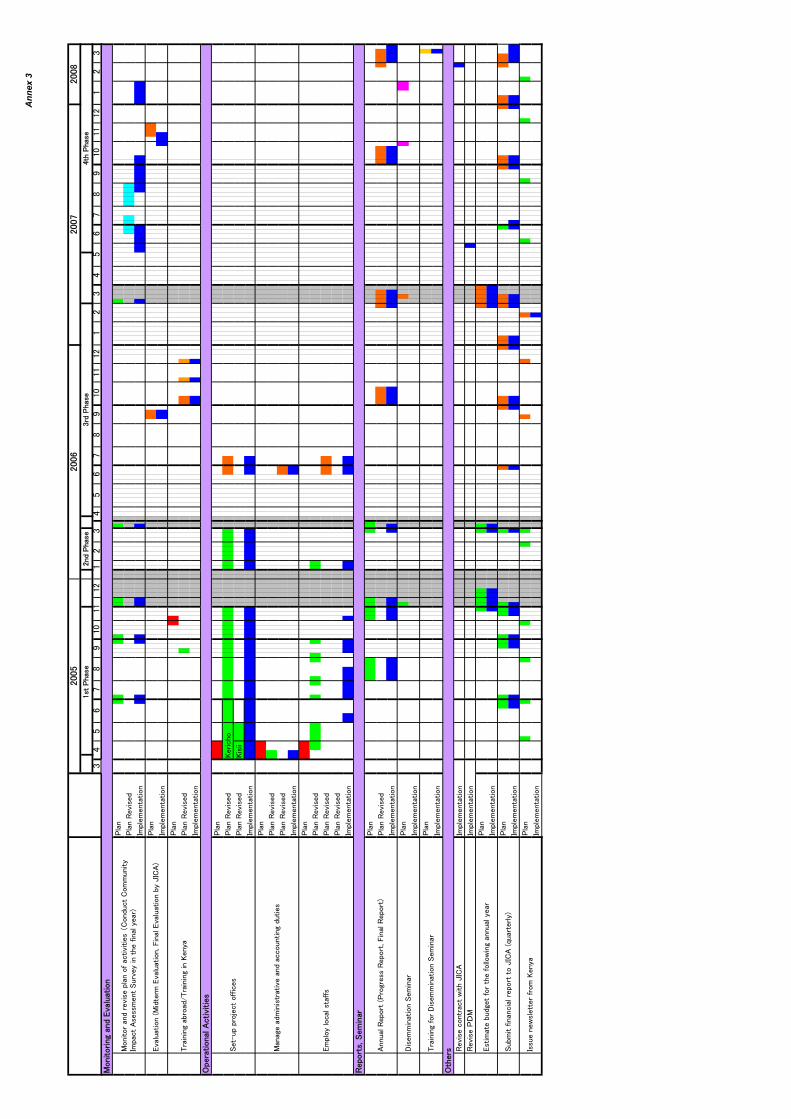
Ann
ex 3
* ���
��
��������
�+������
�
,,
���&
���)
����
���#
�, ����
��
+,�
+#
�&
9,�
,)
**
,�
&,
�)
+,�
#&
)9
,�
,,
9�
#*
��
+,,
,�
,
����
������
��� �
�
������� � ���
����
������� � ���
����
������
��� �
�
������� � ���
����
������
��� �
��������
������
��� �
��� ��
������� � ���
����
������
��� �
�
������
��� �
�
������� � ���
����
������
��� �
�
������
��� �
�
������
��� �
�
������� � ���
����
������
��� �
�
������� � ���
����
������� � ���
����
������� � ���
������� � ���
������� � ���
����
������� � ���
����
������� � ���
����
������� � ���
���� �
�HI�
���!����
��
� �0���"�� ��
��
� ;�'������
��
� 3
� ��
� ��(!�"
� ����� ��������
8��"���
�!���%���
7� ������ �����������
-������"�����7� ������ �����������
���� �
���� ���
�8� ��$�.�
���� �����
������ �
����������
��� �� �4.���!
� �.���!�� %
���
� �� �
��� ��!���%���� ���������%���3
� !
����8 �� �����������%�
�!(�
� ������
��������
� � ��$�.��0@!
�� ���%3
���
�!� ����0��� ���
����
�!� ���;�'��������
�!� ����(%�$�.�3
-������"��(
����
5-������"�������%�
���
� ;��������
����%������� ���
���
�
�� �������
� ��� ��
�� 1!������ �������
���
�"�����
��� �� ����������
��!� ��"��!
��
���� ����"���
�����
�!� ���

Proj
ect D
esig
n M
atrix
Pr
ojec
t Nam
e: P
roje
ct fo
r the
Impr
ovem
ent o
f Hea
lth S
ervi
ce w
ith a
focu
s on
Safe
Mot
herh
ood
in th
e K
isii
and
Ker
icho
Dis
trict
sPr
ojec
t Per
iod:
Mar
ch 2
005
to 2
008
(3 y
ears
)Im
plem
entin
g O
rgan
isat
ions
: Dis
trict
Hea
lth M
anag
emen
t Tea
ms (
DH
MTs
), D
ivis
ion
of R
epro
duct
ive
Hea
lth (D
RH
), D
epar
tmen
t of P
reve
ntiv
e an
d Pr
omot
ive
Hea
lth S
ervi
ce, M
inis
try o
f Hea
lth
Targ
et G
roup
s: D
HM
Ts, H
ealth
car
e pr
ovid
ers,
HC
adm
inis
tratio
n st
aff,
and
com
mun
ities
in th
e K
isii
and
Ker
icho
Dis
trict
s B
enef
icia
ries:
Peo
ple
in th
e K
isii
and
Ker
icho
Dis
trict
s, pa
rticu
larly
wom
en o
f rep
rodu
ctiv
e ag
e.
PDM
0 (A
pril
2005
, Pro
ject
Doc
umen
t)N
arra
tive
Sum
mar
y O
bjec
tivel
y V
erifi
able
Indi
cato
rs *
1M
eans
of V
erifi
catio
nIm
port
ant A
ssum
ptio
ns[O
vera
ll G
oal]
Mat
erna
l mor
talit
y (r
ate)
in th
e D
istri
ct
Cas
e fa
talit
y ra
te d
ue to
mat
erna
l com
plic
atio
ns
Infa
nt m
orta
lity
rate
and
mal
aria
fata
lity
rate
[P
roje
ct P
urpo
se]
Skill
ed b
irth
atte
ndan
ce ra
te in
Dis
trict
Del
iver
y ra
te a
nd A
NC
rate
at H
Cs
HC
util
izat
ion
rate
and
clie
nt sa
tisfa
ctio
n [O
utpu
ts]
Com
pone
nt 1
. Mat
erna
l car
e in
the
Proj
ect a
rea
is im
prov
ed.
1%
of H
Cs p
rovi
ding
skill
ed b
irth
atte
ndan
ce (S
BA
)1.
Mat
erna
l car
e se
rvic
es a
t the
HC
s are
upg
rade
d.
% o
f clin
ical
staf
f mee
ting
the
defin
ition
of S
BA
1-1
Com
plet
ion
of tr
aini
ng w
orkp
lan,
No.
of s
taff
trai
ned
(into
tal a
nd b
y H
C),
No.
of f
ollo
w-u
ps fo
r tra
inin
g, N
o. o
fst
aff r
ecei
ving
the
follo
w-u
ps, E
valu
atio
n of
wor
kpe
rfor
med
by
train
ed st
aff,
Clie
nts s
atis
fact
ion
with
the
qual
ity o
f car
e.
Rec
ords
on
mee
tings
, Tr
aini
ngre
cord
s and
repo
rts, M
onito
ring
reco
rds
1-2.
No.
of H
Cs m
aint
aini
ng fa
cilit
y an
d eq
uipm
ent
prov
ided
1an
d 2
year
s afte
r ins
talla
tion,
No.
of s
taff
trai
ned
for
mai
nten
ance
.
Mon
itorin
g re
cord
s,C
omm
unity
surv
ey,
Mai
nten
ance
reco
rds
2. M
ater
nal c
are
at th
e co
mm
unity
leve
l is i
mpr
oved
. 2
No.
of C
OR
Ps tr
aine
d, N
o. o
f CO
RPs
atte
ndin
g A
NC
s and
deliv
erie
s in
pilo
t com
mun
ities
Patie
nt c
harts
at H
Cs a
ndH
ospi
tals
No.
of H
ealth
lear
ning
sess
ions
, No.
of p
artic
ipan
ts,
Cha
nges
in a
war
enes
s and
hea
lth b
ehav
iour
am
ong
peop
le.
For s
calin
g-up
to o
ther
com
mun
ities
, Tr
aini
ng re
cord
s/re
port
No.
of p
eer l
earn
ing
wor
ksho
ps a
nd e
xcha
nge
visi
ts
Com
mun
ity su
rvey
N
o. o
f com
mun
ities
repl
icat
ing
activ
ities
Cen
sus (
DH
S), M
DR
, Hea
lthSt
atis
tics
Patie
nt c
harts
at h
ospi
tals
and
HC
s, D
HS,
Hea
lth S
tatis
tics,
Com
mun
ity S
urve
ys, E
xit
Inte
rvie
ws
Hea
lth c
ondi
tion,
par
ticul
arly
the
mat
erna
l hea
lth, i
n th
e K
isii
and
Ker
icho
Dis
trict
s is i
mpr
oved
.
Mat
erna
l car
e in
the
Proj
ect a
rea
with
a fo
cus o
n he
alth
cen
tres a
ndco
mm
uniti
es is
impr
oved
.Su
cces
s rat
e in
mee
ting
the
need
s of w
omen
with
mat
erna
lco
mpl
icat
ions
No
sign
ifica
nt c
hang
es in
the
patte
rn o
f dis
ease
,M
OH
pol
icy,
or
econ
omic
or p
oliti
cal
cond
ition
s.
Trai
ning
reco
rds,
Rep
orts
by
train
ees
Rec
urre
nt c
osts
are
prov
ided
for h
ospi
tals
,H
Cs,
and
com
mun
ities
by
the
Ken
yan
side
.
71

Nar
rativ
e Su
mm
ary
Obj
ectiv
ely
Ver
ifiab
le In
dica
tors
*1
Mea
ns o
f Ver
ifica
tion
Impo
rtan
t Ass
umpt
ions
Com
pone
nt 2
. Man
agem
ent s
uppo
rt in
the
HC
s is i
mpr
oved
. 3
No.
of p
rope
r ref
erra
l cas
es o
f mat
erna
l com
plic
atio
ns
Cas
e re
view
reco
rdU
se o
f com
mun
icat
ion
& tr
ansp
orta
tion
Patie
nt c
hart
(Hos
pita
l, H
C)
No.
of t
rain
ing
sess
ions
for r
efer
ral a
nd N
o. o
f par
ticip
ants
U
se o
f ref
erra
l gui
delin
e N
o. o
f mee
tings
for r
evie
win
g re
ferr
al c
ases
4N
o. o
f tra
inin
g se
ssio
ns fo
r HIS
and
trai
nees
Com
mun
ity su
rvey
sR
edun
danc
y of
reco
rds a
nd re
porti
ng
Cas
e re
view
mee
tings
Use
of H
IS fo
r car
e an
d m
anag
emen
t at H
Cs
Adm
inis
tratio
n re
cord
s at H
Cs
Use
of H
IS fo
r mon
itorin
g an
d ev
alua
tion
Mon
itorin
g re
cord
sTr
aini
ng re
cord
s/re
ports
5St
ock-
out d
rugs
and
med
ical
supp
lies
Stoc
k/in
vent
ory
reco
rds
Use
of l
ogbo
oks f
or in
vent
ory
and
pres
crip
tion
Del
iver
y re
cord
sFr
eque
ncy
of d
rug
deliv
ery
to H
Cs
Logb
ooks
Rat
iona
l use
of m
edic
ines
bas
ed o
n gu
idel
ines
at H
Cs
Trai
ning
reco
rds/
repo
rtsPa
tient
cha
rts a
t HC
s Pr
escr
iptio
n re
cord
s6
No.
of D
HM
T m
embe
rs su
perv
isin
g H
Cs.
DH
MT
repo
rtsQ
ualit
y of
supe
rvis
ion
DH
MT
mee
ting
reco
rds
Qua
lity
assu
ranc
e of
HC
man
agem
ent
HC
C, H
FMT
mee
ting
reco
rds
4. H
ealth
Info
rmat
ion
Syst
em (H
IS) a
nd re
cord
kee
ping
syst
em a
t HC
sis
func
tioni
ng a
nd is
util
ised
for s
ervi
ce a
nd m
anag
emen
t at t
he H
Cs.
5. M
anag
emen
t cap
abili
ty fo
r dru
gs a
nd m
edic
al su
pplie
s at t
he H
Cs a
reim
prov
ed.
6. D
istri
ct H
ealth
Man
agem
ent T
eam
s (D
HM
Ts)'
syst
em fo
r the
irsu
ppor
tive
supe
rvis
ion
for H
Cs i
s stre
ngth
ened
.
3. A
refe
rral
syst
em is
arr
ange
d an
d fu
nctio
ning
bet
wee
n co
mm
uniti
es,
HC
s and
Dis
trict
Hos
pita
ls.
72

Nar
rativ
e Su
mm
ary
Obj
ectiv
ely
Ver
ifiab
le In
dica
tors
*1
Mea
ns o
f Ver
ifica
tion
Impo
rtan
t Ass
umpt
ions
(Act
iviti
es)
(Inp
uts)
Inpu
ts)
Out
com
e 1.
Mat
erna
l car
e se
rvic
es in
the
HC
s are
upg
rade
d.
Japa
nese
side
Ken
yan
side
A) T
o in
stitu
te a
trai
ning
syst
em fo
r mat
erna
l car
e [H
uman
Res
ourc
es]
[Ass
ignm
ents
of c
ount
erpa
rts]
1. P
repa
ratio
n (L
ong-
or sh
ort t
erm
exp
erts
or c
onsu
ltant
s)
Min
istry
of H
ealth
1) O
rgan
izin
g tra
inin
g te
am w
ithin
DH
MT
1. C
hief
Adv
isor
or T
echn
ical
Adv
isor
DR
H2)
Rev
iew
ing
info
rmat
ion
on tr
aini
ng n
eeds
for H
C st
aff
2. P
roje
ct M
anag
erO
ther
rele
vant
dep
artm
ents
3) E
stab
lishi
ng c
urric
ula
3. P
roje
ct C
oord
inat
orD
HM
T (K
isii
& K
eric
ho)
4) S
elec
ting
heal
th st
aff t
o be
trai
ned.
4.
Mid
wife
ryPM
O5)
For
mul
atin
g tra
inin
g w
ork-
plan
5. C
omm
unity
-bas
ed h
ealth
H
C st
aff
2. Im
plem
enta
tion
[Pro
visi
on o
f Equ
ipm
ent]
HFM
T (H
CC
)1.
Equ
ipm
ent f
or M
ater
nal c
are
at H
Cs
2. M
ater
nal c
are
equi
pmen
t for
trai
ning
at H
ospi
tals
[A
ccom
odat
ions
]3.
Fol
low
-up
or M
onito
ring
3. L
eani
ng m
ater
ials
nec
essa
ry fo
r tra
inin
g Sa
lary
for t
he st
aff
4. C
omm
unic
atio
n eq
uipm
ent
Faci
litie
s5.
Equ
ipm
ent f
or P
roje
ct O
pera
tion
Proj
ect O
ffic
e2)
Con
duct
ing
Mat
erna
l Dea
th R
evie
w (M
DR
)[F
acili
ty R
enov
atio
n ]
Off
ice
secr
etar
ies
i.e. W
ater
supp
ly fa
cilit
y at
HC
, Sol
ar sy
stem
for H
CD
river
sTr
aini
ng si
tes
1. P
repa
ratio
n
[Cou
nter
part
train
ing]
Trai
ning
in Ja
pan
and/
or th
ird c
ount
ries,
Acc
epta
nce
of tr
aine
es1.
Mid
wife
ry2.
Impl
emen
tatio
n 2.
Dis
trict
Hea
lth M
anag
emen
t 1)
Ren
ovat
ing
faci
litie
s and
pro
vidi
ng e
quip
men
t 3.
Oth
ers
2) D
evel
opin
g m
anua
ls fo
r ope
ratio
n an
d m
aint
enan
ce.
[Pro
ject
Ope
ratio
nal C
ost]
3. F
ollo
win
g-up
and
Mon
itorin
g 1.
Tra
inin
gC
ondu
ctin
g re
gula
r mai
nten
ance
for e
quip
men
t and
faci
litie
s 2.
Em
ploy
men
t of l
ocal
con
sulta
nts (
incl
udin
g su
b-co
ntra
ctin
g)
Tra
inin
g in
mat
erna
l car
e fo
r HC
staf
f, in
clud
ing
esse
ntia
l& e
mer
genc
yob
stet
ric c
are,
AN
C, P
AC
with
clie
nt-c
entre
d ca
re.
1) F
ollo
w-u
p fo
r the
trai
ned
staf
f with
on-
the-
job
train
ing
and
re-tr
aini
ngut
ilizi
ng C
ritic
al In
cide
nce
Ana
lysi
s *2
B) T
o es
tabl
ish
a sy
stem
for r
enov
atin
g fa
cilit
ies a
nd p
rovi
ding
equ
ipm
ent
with
thei
r mai
nten
ance
.
1) In
vest
igat
ing
the
curr
ent s
tatu
s of t
he fa
cilit
ies a
nd e
quip
men
t at e
ach
HC
.2)
Det
erm
inin
g th
e re
quire
d re
nova
tion
and
sele
ctin
g eq
uipm
ent f
orm
ater
nal c
are.
Dec
isio
ns o
n re
nova
tion
and
equi
pmen
t pro
visi
on w
ill b
e m
ade
base
d on
furt
her s
urve
ys, i
nclu
ding
an
asse
ssm
ent o
f the
cond
ition
of e
quip
men
t pro
vide
d by
Jap
anes
e G
rant
Aid
.R
ecur
rent
cos
ts fo
r ite
ms s
uch
as v
ehic
le fu
el a
nd e
quip
men
t
73
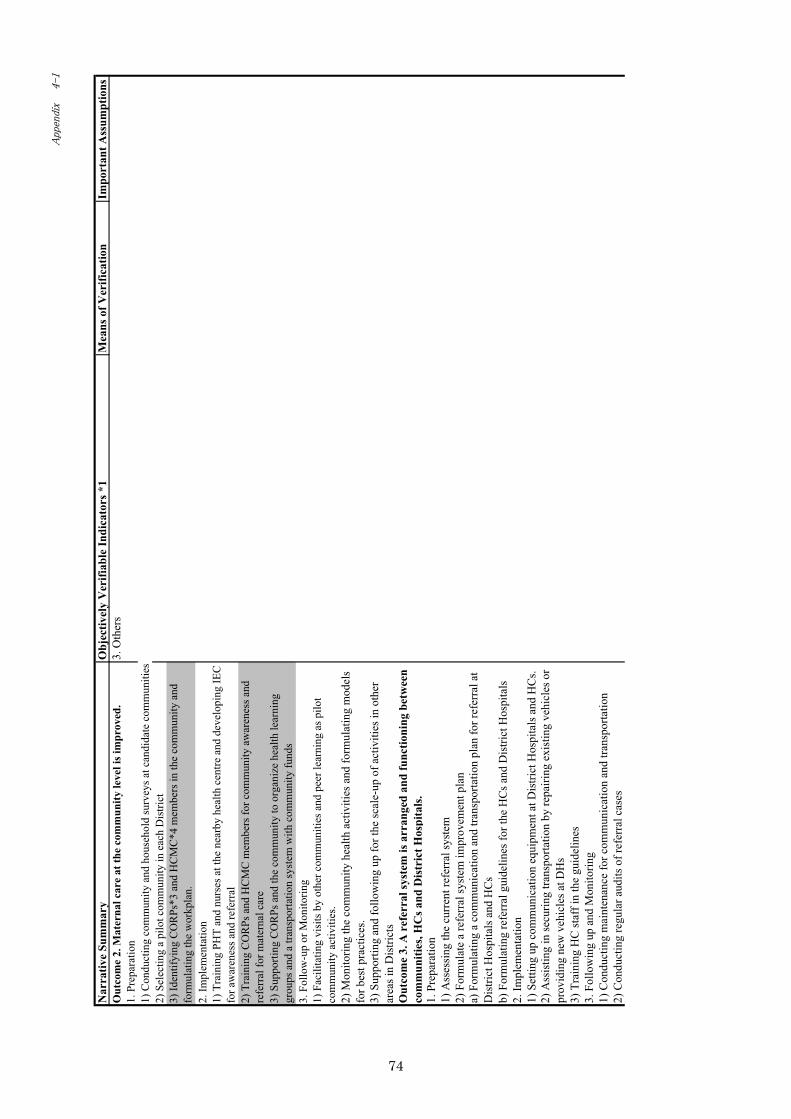
Nar
rativ
e Su
mm
ary
Obj
ectiv
ely
Ver
ifiab
le In
dica
tors
*1
Mea
ns o
f Ver
ifica
tion
Impo
rtan
t Ass
umpt
ions
Out
com
e 2.
Mat
erna
l car
e at
the
com
mun
ity le
vel i
s im
prov
ed.
3. O
ther
s 1.
Pre
para
tion
1) C
ondu
ctin
g co
mm
unity
and
hou
seho
ld su
rvey
s at c
andi
date
com
mun
ities
2)
Sel
ectin
g a
pilo
t com
mun
ity in
eac
h D
istri
ct
2. Im
plem
enta
tion
3. F
ollo
w-u
p or
Mon
itorin
g
Out
com
e 3.
A r
efer
ral s
yste
m is
arr
ange
d an
d fu
nctio
ning
bet
wee
nco
mm
uniti
es, H
Cs a
nd D
istr
ict H
ospi
tals
.1.
Pre
para
tion
1) A
sses
sing
the
curr
ent r
efer
ral s
yste
m
2) F
orm
ulat
e a
refe
rral
syst
em im
prov
emen
t pla
n
b) F
orm
ulat
ing
refe
rral
gui
delin
es fo
r the
HC
s and
Dis
trict
Hos
pita
ls
2. Im
plem
enta
tion
1) S
ettin
g up
com
mun
icat
ion
equi
pmen
t at D
istri
ct H
ospi
tals
and
HC
s.
3) T
rain
ing
HC
staf
f in
the
guid
elin
es3.
Fol
low
ing
up a
nd M
onito
ring
1) C
ondu
ctin
g m
aint
enan
ce fo
r com
mun
icat
ion
and
trans
porta
tion
2) C
ondu
ctin
g re
gula
r aud
its o
f ref
erra
l cas
es
3) Id
entif
ying
CO
RPs
*3 a
nd H
CM
C*4
mem
bers
in th
e co
mm
unity
and
form
ulat
ing
the
wor
kpla
n.
1) T
rain
ing
PHT
and
nurs
es a
t the
nea
rby
heal
th c
entre
and
dev
elop
ing
IEC
for a
war
enes
s and
refe
rral
2) T
rain
ing
CO
RPs
and
HC
MC
mem
bers
for c
omm
unity
aw
aren
ess a
ndre
ferr
al fo
r mat
erna
l car
e
a) F
orm
ulat
ing
a co
mm
unic
atio
n an
d tra
nspo
rtatio
n pl
an fo
r ref
erra
l at
Dis
trict
Hos
pita
ls a
nd H
Cs
2) A
ssis
ting
in se
curin
g tra
nspo
rtatio
n by
repa
iring
exi
stin
g ve
hicl
es o
rpr
ovid
ing
new
veh
icle
s at D
Hs
3) S
uppo
rting
CO
RPs
and
the
com
mun
ity to
org
aniz
e he
alth
lear
ning
grou
ps a
nd a
tran
spor
tatio
n sy
stem
with
com
mun
ity fu
nds
1) F
acili
tatin
g vi
sits
by
othe
r com
mun
ities
and
pee
r lea
rnin
g as
pilo
tco
mm
unity
act
iviti
es.
2) M
onito
ring
the
com
mun
ity h
ealth
act
iviti
es a
nd fo
rmul
atin
g m
odel
sfo
r bes
t pra
ctic
es.
3) S
uppo
rting
and
follo
win
g up
for t
he sc
ale-
up o
f act
iviti
es in
oth
erar
eas i
n D
istri
cts
74

Nar
rativ
e Su
mm
ary
Obj
ectiv
ely
Ver
ifiab
le In
dica
tors
*1
Mea
ns o
f Ver
ifica
tion
Impo
rtan
t Ass
umpt
ions
Out
com
e 4.
Hea
lth In
form
atio
n Sy
stem
(HIS
) and
rec
ord
keep
ing
syst
em a
t HC
s is f
unct
ioni
ng a
nd is
util
ised
for
serv
ice
and
man
a gem
ent a
t the
HC
s.1.
Pre
para
tion
1) A
sses
sing
the
curr
ent s
tatu
s of t
he H
IS a
t the
HC
s and
Dis
trict
Hos
pita
ls2)
For
mul
atin
g a
HIS
impr
ovem
ent p
lan
at th
e H
Cs
2. Im
plem
enta
tion
1) T
rain
ing
Dis
trict
MR
IO fo
r im
prov
emen
t pla
n fo
r HIS
2) T
rain
ing
HC
staf
f in
reco
rd-k
eepi
ng
3. F
ollo
win
g up
and
Mon
itorin
g C
ontin
uous
ly im
prov
ing
the
qual
ity o
f rec
ord-
keep
ing
at th
e D
istri
ctan
d H
C le
vels
Out
com
e 5.
Man
agem
ent c
apab
ility
for
drug
s and
med
ical
supp
lies
at th
e H
Cs a
re im
prov
ed.
1. P
repa
ratio
n1)
Sur
veyi
ng d
rugs
and
med
ical
supp
lies w
ith a
focu
s on
the
adeq
uacy
ofpr
ovis
ion
(del
iver
y), s
tock
, and
pre
scrip
tion
2) F
orm
ulat
ing
a dr
ug m
anag
emen
t im
prov
emen
t pla
n at
the
HC
s2.
Impl
emen
tatio
n1)
Intro
duci
ng lo
gboo
ks fo
r inv
ento
ry, s
tore
-kee
ping
and
pre
scrip
tion;
train
ing
HC
staf
f to
use
the
log
book
s2)
Tra
inin
g H
C st
aff o
n th
e ca
se m
anag
emen
t gui
delin
es a
t the
HC
s to
ensu
re th
e ra
tiona
l use
of d
rugs
3) M
aint
aini
ng a
nd st
reng
then
ing
the
logi
stic
s sys
tem
for d
rug
deliv
ery
in c
oord
inat
ion
with
HIS
3. F
ollo
win
g up
and
Mon
itorin
gC
ontin
uous
ly im
prov
ing
the
qual
ity o
f dru
g m
anag
emen
t.O
utco
me
6. D
istr
ict H
ealth
Man
agem
ent T
eam
s (D
HM
Ts)
' sys
tem
for
thei
r su
ppor
tive
supe
rvis
ion
for
HC
s is s
tren
gthe
ned.
1. P
repa
ratio
n 1)
Ass
essi
ng th
e D
HM
T's c
urre
nt sy
stem
for s
uper
visi
ng th
e H
Cs
2) F
orm
ulat
ing
thei
r pla
n fo
r HC
supe
rvis
ion
2. Im
plem
enta
tion
Impl
emen
ting
the
supe
rvis
ory
plan
3.
Fol
low
ing
up a
nd M
onito
ring
Mon
itorin
g th
e D
HM
T's s
uper
visi
on o
f the
HC
s with
feed
back
.
*2 C
ritic
al In
cide
nce
Ana
lysi
s: T
o as
sess
the
effe
cts o
f tra
inin
g by
exa
min
ing
reco
rds o
n th
e m
anag
emen
t of c
ases
han
dled
by
the
train
ees a
fter t
he tr
aini
ng.
*3 C
OR
Ps in
clud
e co
mm
unity
lead
ers,
tradi
tiona
l birt
h at
tend
ants
(TB
As)
and
com
mun
ity h
ealth
wor
kers
(CH
Ws)
. *4
The
Hea
th C
entre
Man
agem
ent C
omm
ittee
(HC
MC
) is a
com
mun
ity-b
ased
com
mitt
ee re
spon
sibl
e fo
r man
agem
ent o
f the
HC
s.
*1 T
he o
bjec
tivel
y ve
rifia
ble
indi
cato
rs u
sed
for t
he p
urpo
se a
nd o
utpu
ts a
re a
ccor
ded
to th
ose
esta
blis
hed
in th
e D
istri
ct P
lan.
Oth
erw
ise,
eff
orts
will
be
mad
e to
det
erm
ine
impo
rtant
indi
cato
rssu
ch a
s Mat
erna
l Mor
talit
y (r
ate)
in th
e ar
ea b
y ba
selin
e s
75

Proj
ect D
esig
n M
atrix
Pr
ojec
t Nam
e: P
roje
ct fo
r the
Impr
ovem
ent o
f Hea
lth S
ervi
ce w
ith a
focu
s on
Safe
Mot
herh
ood
in th
e K
isii
and
Ker
icho
Dis
trict
sPr
ojec
t Per
iod:
Mar
ch 2
005
to 2
008
(3 y
ears
)Im
plem
entin
g O
rgan
isat
ions
: Dis
trict
Hea
lth M
anag
emen
t Tea
ms (
DH
MTs
), D
ivis
ion
of R
epro
duct
ive
Hea
lth (D
RH
), D
epar
tmen
t of P
reve
ntiv
e an
d Pr
omot
ive
Hea
lth S
ervi
ce, M
inis
try o
f Hea
lth
Targ
et G
roup
s: D
HM
Ts, H
ealth
car
e pr
ovid
ers,
HC
adm
inis
tratio
n st
aff,
and
com
mun
ities
in th
e K
isii
and
Ker
icho
Dis
trict
s B
enef
icia
ries:
Peo
ple
in th
e K
isii
and
Ker
icho
Dis
trict
s, pa
rticu
larly
wom
en o
f rep
rodu
ctiv
e ag
e.
PDM
1 (M
ay 2
007)
Nar
rativ
e Su
mm
ary
Obj
ectiv
ely
Ver
ifiab
le In
dica
tors
*1M
eans
of V
erifi
catio
nIm
port
ant A
ssum
ptio
ns[O
vera
ll G
oal]
Mat
erna
l mor
talit
y (r
ate)
in th
e D
istri
ct
Cas
e fa
talit
y ra
te d
ue to
mat
erna
l com
plic
atio
ns
Infa
nt m
orta
lity
rate
and
mal
aria
fata
lity
rate
[P
roje
ct P
urpo
se]
Skill
ed b
irth
atte
ndan
ce ra
te in
Dis
trict
Del
iver
y ra
te a
nd A
NC
rate
at H
Cs
HC
util
izat
ion
rate
and
clie
nt sa
tisfa
ctio
n [O
utpu
ts]
Out
put 1
. Mat
erna
l car
e se
rvic
es a
t the
HC
s are
upg
rade
d.
Incr
ease
in th
e N
o. o
f HC
s pro
vidi
ng sk
illed
birt
h at
tend
ance
(SB
Incr
ease
in th
e N
o. o
f clin
ical
staf
f mee
ting
the
defin
ition
of S
BA
Rec
ords
on
mee
tings
, Tr
aini
ngre
cord
s and
repo
rts, M
onito
ring
reco
rds
Mon
itorin
g re
cord
s, C
omm
unity
surv
ey, M
aint
enan
ce re
cord
s
Out
put 2
. Man
agem
ent s
uppo
rt in
the
HC
s is i
mpr
oved
. 2-
1. T
o im
prov
e m
anag
emen
t cap
acity
of t
he H
C in
-cha
rges
HC
C,H
FMT
mee
ting
reco
rds
Mon
itorin
g re
cord
s,C
omm
unity
Sur
vey
(Exi
tin
terv
iew
s)D
HM
Tre
ports
No.
of t
rain
ing
sess
ions
for H
IS a
nd tr
aine
esTr
aini
ng re
ports
Use
of H
IS fo
r car
e an
d m
anag
emen
t at H
Cs a
nd D
HM
TU
se o
f HIS
for m
onito
ring
and
eval
uatio
n
2-2.
Hea
lth In
form
atio
n Sy
stem
(HIS
) and
reco
rd k
eepi
ng sy
stem
at H
Cs i
sfu
nctio
ning
and
is u
tilis
ed fo
r ser
vice
and
man
agem
ent a
t the
HC
s.G
ood
scor
e in
the
HIS
perf
orm
ance
che
cklis
t on
reco
rdin
g an
d re
porti
ngA
dmin
istra
tion
reco
rds a
t HC
sM
onito
ring
reco
rds
No.
of H
C in
-cha
rge
who
rece
ived
trai
ning
rela
ted
to h
ealth
man
agem
ent
Incr
ease
d le
vel o
f com
mun
ity sa
tisfa
ctio
n on
MC
H re
gard
ing
heal
th m
anag
emen
t at H
Cs
Effic
ienc
y of
reco
rdin
g an
d re
porti
ng
Cen
sus (
DH
S), M
DR
, Hea
lthSt
atis
tics
Patie
nt c
harts
at h
ospi
tals
and
HC
s, D
HS,
Hea
lth S
tatis
tics,
Com
mun
ity S
urve
ys, E
xit
Inte
rvie
ws
Hea
lth c
ondi
tion,
par
ticul
arly
the
mat
erna
l hea
lth, i
n th
e K
isii
and
Ker
icho
Dis
trict
s is i
mpr
oved
.
Mat
erna
l car
e in
the
Proj
ect a
rea
with
a fo
cus o
n he
alth
cen
tres a
ndco
mm
uniti
es is
impr
oved
.Su
cces
s rat
e in
mee
ting
the
need
s of w
omen
with
mat
erna
lco
mpl
icat
ions
No
sign
ifica
nt c
hang
es in
the
patte
rn o
f dis
ease
,M
OH
pol
icy,
or e
cono
mic
or p
oliti
cal c
ondi
tions
.
Trai
ning
reco
rds,
Rep
orts
by
train
ees
Rec
urre
nt c
osts
are
prov
ided
for h
ospi
tals
,H
Cs,
and
com
mun
ities
by
the
Ken
yan
side
.C
ompl
etio
n of
trai
ning
wor
kpla
n, N
o. o
f sta
ff tr
aine
d (in
tota
lan
d by
HC
), N
o. o
f fol
low
-ups
for t
rain
ing,
No.
of s
taff
rece
ivin
gth
e fo
llow
-ups
, Eva
luat
ion
of w
ork
perf
orm
ed b
y tra
ined
staf
f,C
lient
s' sa
tisfa
ctio
n w
ith th
e qu
ality
of c
are.
No.
of H
Cs m
aint
aini
ng fa
cilit
y an
d eq
uipm
ent 1
and
2 y
ears
afte
r the
ir in
stal
latio
n, N
o. o
f sta
ff tr
aine
d fo
r mai
nten
ance
.
76
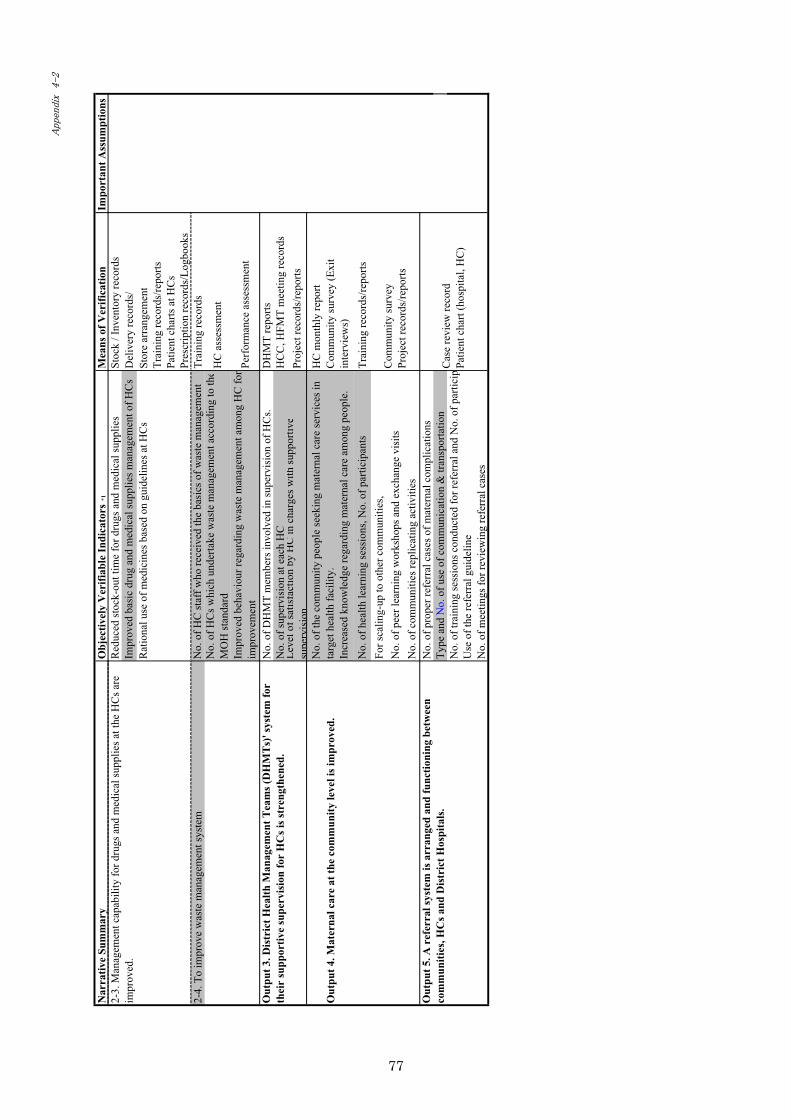
Nar
rativ
e Su
mm
ary
Obj
ectiv
ely
Ver
ifiab
le In
dica
tors
*1M
eans
of V
erifi
catio
nIm
port
ant A
ssum
ptio
nsR
educ
ed st
ock-
out t
ime
for d
rugs
and
med
ical
supp
lies
Stoc
k / I
nven
tory
reco
rds
Del
iver
y re
cord
s/St
ore
arra
ngem
ent
Trai
ning
reco
rds/
repo
rtsPa
tient
cha
rts a
t HC
s Pr
escr
iptio
n re
cord
s/Lo
gboo
ks2-
4. T
o im
prov
e w
aste
man
agem
ent s
yste
mTr
aini
ng re
cord
s
HC
ass
essm
ent
Perf
orm
ance
ass
essm
ent
No.
of D
HM
T m
embe
rs in
volv
ed in
supe
rvis
ion
of H
Cs.
DH
MT
repo
rtsN
o. o
f sup
ervi
sion
at e
ach
HC
H
CC
, HFM
T m
eetin
g re
cord
sPr
ojec
t rec
ords
/repo
rts
Out
put 4
. Mat
erna
l car
e at
the
com
mun
ity le
vel i
s im
prov
ed.
HC
mon
thly
repo
rtC
omm
unity
surv
ey (E
xit
inte
rvie
ws)
Trai
ning
reco
rds/
repo
rts
No.
of c
omm
uniti
es re
plic
atin
g ac
tiviti
es
No.
of p
rope
r ref
erra
l cas
es o
f mat
erna
l com
plic
atio
ns
Type
and
No.
of u
se o
f com
mun
icat
ion
& tr
ansp
orta
tion
No.
of t
rain
ing
sess
ions
con
duct
ed fo
r ref
erra
l and
No.
of p
artic
ipU
se o
f the
refe
rral
gui
delin
eN
o. o
f mee
tings
for r
evie
win
g re
ferr
al c
ases
2-3.
Man
agem
ent c
apab
ility
for d
rugs
and
med
ical
supp
lies a
t the
HC
s are
impr
oved
.
Cas
e re
view
reco
rdPa
tient
cha
rt (h
ospi
tal,
HC
)
For s
calin
g-up
to o
ther
com
mun
ities
,N
o. o
f pee
r lea
rnin
g w
orks
hops
and
exc
hang
e vi
sits
Rat
iona
l use
of m
edic
ines
bas
ed o
n gu
idel
ines
at H
Cs
Leve
l of s
atis
fact
ion
byH
Cin
cha
rges
with
supp
ortiv
esu
perv
isio
n
No.
of H
C st
aff w
ho re
ceiv
ed th
e ba
sics
of w
aste
man
agem
ent
No.
of H
Cs w
hich
und
erta
ke w
aste
man
agem
ent a
ccor
ding
to th
eM
OH
stan
dard
Out
put 5
. A r
efer
ral s
yste
m is
arr
ange
d an
d fu
nctio
ning
bet
wee
nco
mm
uniti
es, H
Cs a
nd D
istr
ict H
ospi
tals
.
Out
put 3
. Dis
tric
t Hea
lth M
anag
emen
t Tea
ms (
DH
MT
s)' s
yste
m fo
rth
eir
supp
ortiv
e su
perv
isio
n fo
r H
Cs i
s str
engt
hene
d.
No.
of t
he c
omm
unity
peo
ple
seek
ing
mat
erna
l car
e se
rvic
es in
targ
et h
ealth
faci
lity.
Incr
ease
d kn
owle
dge
rega
rdin
g m
ater
nal c
are
amon
g pe
ople
.
No.
of h
ealth
lear
ning
sess
ions
, No.
of p
artic
ipan
ts
Impr
oved
bas
ic d
rug
and
med
ical
supp
lies m
anag
emen
t of H
Cs
Impr
oved
beh
avio
ur re
gard
ing
was
te m
anag
emen
t am
ong
HC
for
impr
ovem
ent
Com
mun
ity su
rvey
Proj
ect r
ecor
ds/re
ports
77

Nar
rativ
e Su
mm
ary
Obj
ectiv
ely
Ver
ifiab
le In
dica
tors
*1M
eans
of V
erifi
catio
nIm
port
ant A
ssum
ptio
ns(A
ctiv
ities
)(I
nput
s)In
puts
)O
utco
me
1. M
ater
nal c
are
serv
ices
at t
he H
Cs a
re u
pgra
ded.
Ja
pane
se si
deK
enya
n si
deA
. To
inst
itute
a tr
aini
ng sy
stem
for m
ater
nal c
are
[Hum
an R
esou
rces
][A
ssig
nmen
ts o
f cou
nter
parts
]A
-1. P
repa
ratio
n (L
ong-
or sh
ort t
erm
exp
erts
or c
onsu
ltant
s)
Min
istry
of H
ealth
1) O
rgan
izin
g tra
inin
g te
am w
ithin
DH
MT
1. C
hief
Adv
isor
or T
echn
ical
Adv
isor
DR
H2)
Rev
iew
ing
info
rmat
ion
on tr
aini
ng n
eeds
for H
C st
aff
2. P
roje
ct M
anag
erO
ther
rele
vant
dep
artm
ents
3) E
stab
lishi
ng c
urric
ula
3. P
roje
ct C
oord
inat
orD
HM
T (K
isii
& K
eric
ho)
4) S
elec
ting
heal
th st
aff t
o be
trai
ned.
4.
Mid
wife
ryPM
O5)
For
mul
atin
g tra
inin
g w
ork-
plan
5. C
omm
unity
-bas
ed h
ealth
H
C st
aff
A-2
. Im
plem
enta
tion
[Pro
visi
on o
f Equ
ipm
ent]
HFM
T (H
CC
)1.
Equ
ipm
ent f
or M
ater
nal c
are
at H
Cs
2. M
ater
nal c
are
equi
pmen
t for
trai
ning
at H
ospi
tals
[A
ccom
mod
atio
ns]
A-3
. Fol
low
-up
or M
onito
ring
3. L
eani
ng m
ater
ials
nec
essa
ry fo
r tra
inin
g Sa
lary
for t
he st
aff
4. C
omm
unic
atio
n eq
uipm
ent
Faci
litie
s5.
Equ
ipm
ent f
or P
roje
ct O
pera
tion
Proj
ect O
ffic
e2)
. Con
duct
ing
Mat
erna
l Dea
th R
evie
w (M
DR
)[F
acili
ty R
enov
atio
n ]
Off
ice
secr
etar
ies
i.e. W
ater
supp
ly fa
cilit
y at
HC
, Sol
ar sy
stem
for H
CD
river
sTr
aini
ng si
tes
B-1
. Pre
para
tion
[Cou
nter
part
train
ing]
Trai
ning
in Ja
pan
and/
or th
ird c
ount
ries,
Acc
epta
nce
of tr
aine
es1.
Mid
wife
ryB
-2. I
mpl
emen
tatio
n 2.
Dis
trict
Hea
lth M
anag
emen
t 1)
. Ren
ovat
ing
faci
litie
s and
pro
vidi
ng e
quip
men
t 3.
Oth
ers
2). D
evel
opin
g m
anua
ls fo
r ope
ratio
n an
d m
aint
enan
ce.
[Pro
ject
Ope
ratio
nal C
ost]
B-3
. Fol
low
ing-
up a
nd M
onito
ring
1. T
rain
ing
1). C
ondu
ctin
g re
gula
r mai
nten
ance
for e
quip
men
t and
faci
litie
s 2.
Em
ploy
men
t of l
ocal
con
sulta
nts (
incl
udin
g su
b-co
ntra
ctin
g)O
utco
me
2. M
anag
emen
t sup
port
in th
e H
Cs i
s im
prov
ed.
3. O
ther
s 2-
1. T
o im
prov
e m
anag
emen
t cap
acity
of t
he H
C in
-cha
rges
1. P
repa
ratio
n 1)
. Ass
essi
ng th
e cu
rren
t iss
ues r
egar
ding
the
man
agem
ent c
apac
ity o
f the
HC
in-c
harg
es2.
Impl
emen
tatio
n ).
Trai
ning
HC
in-c
harg
es o
n th
e he
alth
man
agem
ent
1). T
rain
ing
in m
ater
nal c
are
for H
C st
aff,
incl
udin
g es
sent
ial&
em
erge
ncy
obst
etric
car
e, A
NC
, PA
C w
ith c
lient
-cen
tred
care
.
B. T
o es
tabl
ish
a sy
stem
for r
enov
atin
g fa
cilit
ies a
nd p
rovi
ding
equ
ipm
ent w
ithth
eir m
aint
enan
ce.
1). I
nves
tigat
ing
the
curr
ent s
tatu
s of t
he fa
cilit
ies a
nd e
quip
men
t at e
ach
HC
.
2). D
eter
min
ing
the
requ
ired
reno
vatio
n an
d se
lect
ing
equi
pmen
t for
mat
erna
lca
re.
Rec
urre
nt c
osts
for i
tem
s suc
h as
vehi
cle
fuel
and
equ
ipm
ent
1). F
ollo
w-u
p fo
r the
trai
ned
staf
f with
on-
the-
job
train
ing
and
re-tr
aini
ngut
ilizi
ng C
ritic
al In
cide
nce
Ana
lysi
s *2
Dec
isio
ns o
n re
nova
tion
and
equi
pmen
t pro
visi
on w
ill b
e m
ade
base
d on
furt
her s
urve
ys, i
nclu
ding
an
asse
ssm
ent o
f the
cond
ition
of e
quip
men
t pro
vide
d by
Jap
anes
e G
rant
Aid
.
78

Nar
rativ
e Su
mm
ary
Obj
ectiv
ely
Ver
ifiab
le In
dica
tors
*1M
eans
of V
erifi
catio
nIm
port
ant A
ssum
ptio
ns2-
2. H
ealth
Info
rmat
ion
Syst
em (H
IS) a
nd r
ecor
d ke
epin
g sy
stem
at H
Cs i
sfu
nctio
ning
and
is u
tilis
ed fo
r se
rvic
e an
d m
anag
emen
t at t
he H
Cs.
1. P
repa
ratio
n 1)
. Ass
essi
ng th
e cu
rren
t sta
tus o
f the
HIS
at t
he H
Cs a
nd D
istri
ct H
ospi
tals
2). F
orm
ulat
ing
a H
IS im
prov
emen
t pla
n at
the
HC
s2.
Impl
emen
tatio
n 1)
. Tra
inin
g D
istri
ct M
RIO
for i
mpr
ovem
ent p
lan
for H
IS2)
. Tra
inin
g H
C st
aff i
n re
cord
-kee
ping
3.
Fol
low
ing
up a
nd M
onito
ring
1). C
ontin
uous
ly im
prov
ing
the
qual
ity o
f rec
ord-
keep
ing
at th
e D
istri
ct a
ndH
C le
vels
2-3.
Man
agem
ent c
apab
ility
for
drug
s and
med
ical
supp
lies a
t the
HC
sar
e im
prov
ed.
1. P
repa
ratio
n1)
. Sur
veyi
ng d
rugs
and
med
ical
supp
lies w
ith a
focu
s on
the
adeq
uacy
of
prov
isio
n (d
eliv
ery)
, sto
ck, a
nd p
resc
riptio
n2)
. For
mul
atin
g a
drug
and
supp
lies m
anag
emen
t im
prov
emen
t pla
n at
the
2. Im
plem
enta
tion
1). T
rain
ing
of H
C st
aff o
n th
e ba
sics
of d
rug
and
med
ical
supp
lies
man
agem
ent
2). T
rain
ing
HC
staf
f on
the
case
man
agem
ent g
uide
lines
at t
he H
Cs t
o en
sure
the
ratio
nal u
se o
f dru
gs3.
Fol
low
ing
up a
nd M
onito
ring
1). C
ontin
uous
ly im
prov
ing
the
qual
ity o
f dru
g m
anag
emen
t. 2-
4. T
o im
prov
e w
aste
man
agem
ent s
yste
m
1. P
repa
ratio
n 1)
. Ass
essi
ng th
e w
aste
man
agem
ent s
yste
m a
t the
HC
s2.
Impl
emen
tatio
n 1)
.Tra
inin
g H
C st
aff o
n th
e ba
sics
of w
aste
man
agem
ent
3. F
ollo
win
g up
and
Mon
itorin
g 1)
. Con
tinuo
usly
impr
ovin
g th
e w
aste
man
agem
ent
Out
com
e 3.
Dis
tric
t Hea
lth M
anag
emen
t Tea
ms (
DH
MT
s)' s
yste
m fo
rth
eir
supp
ortiv
e su
perv
isio
n fo
r H
Cs i
s str
engt
hene
d.1.
Pre
para
tion
1). A
sses
sing
the
DH
MT'
s cur
rent
syst
em fo
r sup
ervi
sing
the
HC
s2)
. For
mul
atin
g an
impr
oved
pla
n fo
r HC
supe
rvis
ion
2. Im
plem
enta
tion
1). I
mpl
emen
tatio
n of
the
supe
rvis
ory
plan
3. F
ollo
win
g up
and
Mon
itorin
g 1)
. Mon
itorin
g th
e D
HM
T's s
uper
visi
on o
f the
HC
s with
feed
back
.
79

Nar
rativ
e Su
mm
ary
Obj
ectiv
ely
Ver
ifiab
le In
dica
tors
*1M
eans
of V
erifi
catio
nIm
port
ant A
ssum
ptio
nsO
utco
me
4. M
ater
nal c
are
at th
e co
mm
unity
leve
l is i
mpr
oved
. 1.
Pre
para
tion
1). C
ondu
ctin
g co
mm
unity
and
hou
seho
ld su
rvey
s at c
andi
date
com
mun
ities
2)
. Sel
ectin
g a
pilo
t com
mun
ity in
eac
h D
istri
ct
2. Im
plem
enta
tion
3. F
ollo
w-u
p or
Mon
itorin
g
Out
com
e 5.
A r
efer
ral s
yste
m is
arr
ange
d an
d fu
nctio
ning
bet
wee
nco
mm
uniti
es, H
Cs a
nd D
istr
ict H
ospi
tals
.1.
Pre
para
tion
1). A
sses
sing
the
curr
ent r
efer
ral s
yste
m
2). F
orm
ulat
e a
refe
rral
syst
em im
prov
emen
t pla
n
b). F
orm
ulat
ing
refe
rral
gui
delin
es fo
r the
HC
s and
Dis
trict
Hos
pita
ls
2. Im
plem
enta
tion
1). S
ettin
g up
com
mun
icat
ion
equi
pmen
t at D
istri
ct H
ospi
tals
and
HC
s.
3). T
rain
ing
HC
staf
f in
the
guid
elin
es3.
Fol
low
ing
up a
nd M
onito
ring
1). C
ondu
ctin
g m
aint
enan
ce fo
r com
mun
icat
ion
and
trans
porta
tion
2). C
ondu
ctin
g re
gula
r aud
its o
f ref
erra
l cas
es*1
The
obj
ectiv
ely
verif
iabl
e in
dica
tors
use
d fo
r the
pur
pose
and
out
puts
are
acco
rded
to th
ose
esta
blis
hed
in th
e D
istri
ct P
lan.
Oth
erw
ise,
eff
orts
will
be
mad
e to
det
erm
ine
impo
rtant
indi
cato
rs su
ch a
s Mat
erna
l Mor
talit
y (r
ate)
inth
e ar
ea b
y ba
selin
e*2
Crit
ical
Inci
denc
e A
naly
sis:
To
asse
ss th
e ef
fect
s of t
rain
ing
by e
xam
inin
g re
cord
s on
the
man
agem
ent o
f cas
es h
andl
ed b
y th
e tra
inee
s afte
r the
trai
ning
.
*4 T
he H
eath
Cen
tre M
anag
emen
t Com
mitt
ee (H
CM
C) i
s a c
omm
unity
-bas
ed c
omm
ittee
resp
onsi
ble
for m
anag
emen
t of t
he H
Cs.
*3 C
HW
s who
are
Ex-
CO
RPs
incl
ude
com
mun
ity le
ader
s, tra
ditio
nal b
irth
atte
ndan
ts (T
BA
s) a
nd c
omm
unity
hea
lth w
orke
rs.
2). A
ssis
ting
in se
curin
g tra
nspo
rtatio
n by
repa
iring
exi
stin
g ve
hicl
es o
rpr
ovid
ing
new
veh
icle
s at D
Hs
3). S
uppo
rting
and
follo
win
g up
for t
he sc
ale-
up o
f act
iviti
es in
oth
er a
reas
inD
istri
cts
a). F
orm
ulat
ing
a co
mm
unic
atio
n an
d tra
nspo
rtatio
n pl
an fo
r ref
erra
l at
Dis
trict
Hos
pita
ls a
nd H
Cs
2). M
onito
ring
the
com
mun
ity h
ealth
act
iviti
es a
nd fo
rmul
atin
g m
odel
s for
best
pra
ctic
es.
2). T
rain
ing
CH
Ws a
nd H
CM
C m
embe
rs o
n co
mm
unity
aw
aren
ess a
nd re
ferr
alfo
r mat
erna
l car
e3)
. Sup
porti
ng C
HW
s and
the
com
mun
ity to
org
aniz
e he
alth
lear
ning
gro
ups a
nda
trans
porta
tion
syst
em w
ith c
omm
unity
fund
s
1). F
acili
tatin
g vi
sits
by
othe
r com
mun
ities
and
pee
r lea
rnin
g as
pilo
t com
mun
ityac
tiviti
es.
1). T
rain
ing
PHT
and
nurs
es a
t the
link
hea
lth c
entre
and
dev
elop
ing
IEC
for
awar
enes
s and
refe
rral
3). I
dent
ifyin
g C
HW
s*3
and
CH
IC*4
mem
bers
in th
e co
mm
unity
and
form
ulat
ing
the
wor
kpla
n.
80
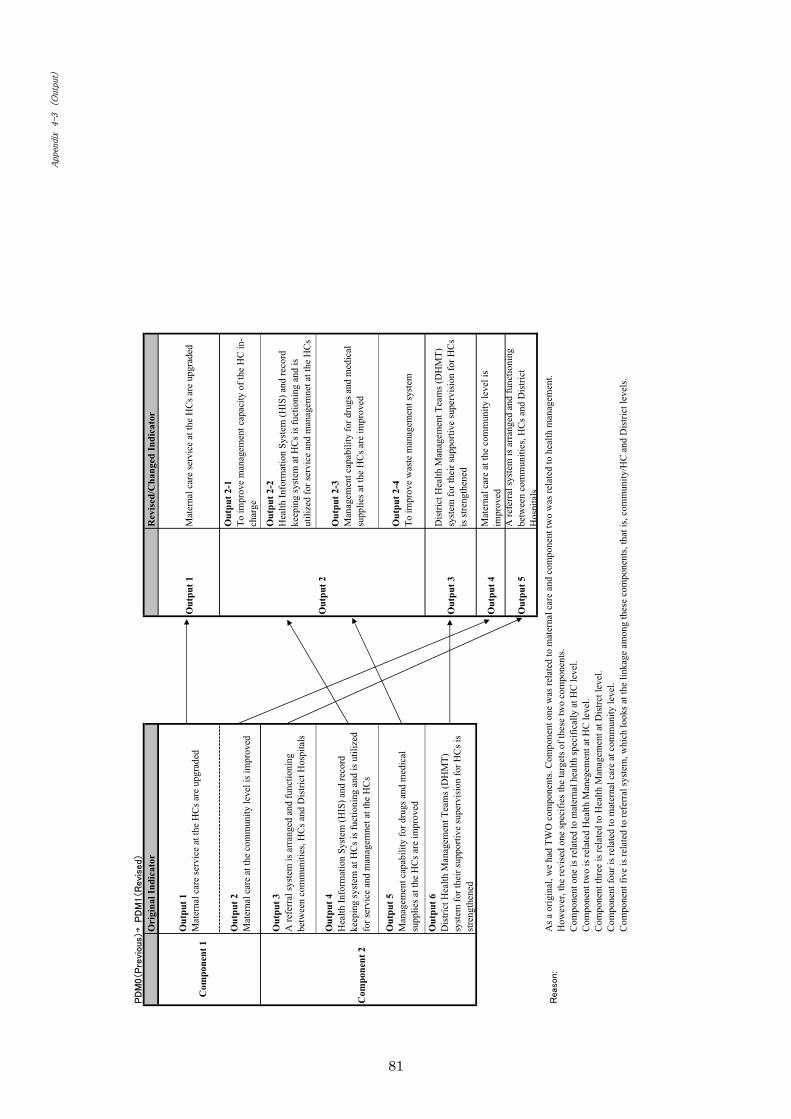
→ Ori
gina
l Ind
icat
orR
evis
ed/C
hang
ed In
dica
tor
Out
put 1
Mat
erna
l car
e se
rvic
e at
the
HC
s are
upg
rade
dO
utpu
t 1M
ater
nal c
are
serv
ice
at th
e H
Cs a
re u
pgra
ded
Out
put 2
Mat
erna
l car
e at
the
com
mun
ity le
vel i
s im
prov
ed
Out
put 2
-1To
impr
ove
man
agem
ent c
apac
ity o
f the
HC
in-
char
ge
Out
put 3
A re
ferr
al sy
stem
is a
rran
ged
and
func
tioni
ngbe
twee
n co
mm
uniti
es, H
Cs a
nd D
istri
ct H
ospi
tals
Out
put 2
-2H
ealth
Info
rmat
ion
Syst
em (H
IS) a
nd re
cord
keep
ing
syst
em a
t HC
s is f
uctio
ning
and
isut
ilize
d fo
r ser
vice
and
man
agem
net a
t the
HC
s
Out
put 4
Hea
lth In
form
atio
n Sy
stem
(HIS
) and
reco
rdke
epin
g sy
stem
at H
Cs i
s fuc
tioni
ng a
nd is
util
ized
for s
ervi
ce a
nd m
anag
emne
t at t
he H
Cs
Out
put 2
-3M
anag
emen
t cap
abili
ty fo
r dru
gs a
nd m
edic
alsu
pplie
s at t
he H
Cs a
re im
prov
ed
Out
put 5
Man
agem
ent c
apab
ility
for d
rugs
and
med
ical
supp
lies a
t the
HC
s are
impr
oved
Out
put 2
-4To
impr
ove
was
te m
anag
emen
t sys
tem
Out
put 6
Dis
trict
Hea
lth M
anag
emen
t Tea
ms (
DH
MT)
syst
em fo
r the
ir su
ppor
tive
supe
rvis
ion
for H
Cs i
sst
reng
then
ed
Out
put 3
Dis
trict
Hea
lth M
anag
emen
t Tea
ms (
DH
MT)
syst
em fo
r the
ir su
ppor
tive
supe
rvis
ion
for H
Cs
is st
reng
then
ed
Out
put 4
Mat
erna
l car
e at
the
com
mun
ity le
vel i
sim
prov
ed
Out
put 5
A re
ferr
al sy
stem
is a
rran
ged
and
func
tioni
ngbe
twee
n co
mm
uniti
es, H
Cs a
nd D
istri
ctH
ospi
tals
Out
put 2
Com
pone
nt 1
Com
pone
nt 2
As a
orig
inal
, we
had
TWO
com
pone
nts.
Com
pone
nt o
ne w
as re
late
d to
mat
erna
l car
e an
d co
mpo
nent
two
was
rela
ted
to h
ealth
man
agem
ent.
How
ever
, the
revi
sed
one
spec
ifies
the
targ
ets o
f the
se tw
o co
mpo
nent
s.C
ompo
nent
one
is re
late
d to
mat
erna
l hea
lth sp
ecifi
cally
at H
C le
vel.
Com
pone
nt tw
o is
rela
ted
Hea
lth M
aneg
emen
t at H
C le
vel.
Com
pone
nt th
ree
is re
late
d to
Hea
lth M
anag
emen
t at D
istrc
t lev
el.
Com
pone
nt fo
ur is
rela
ted
to m
ater
nal c
are
at c
omm
unity
leve
l.C
ompo
nent
five
is re
late
d to
refe
rral
syst
em, w
hich
look
s at t
he li
nkag
e am
ong
thes
e co
mpo
nent
s, th
at is
, com
mun
ity/H
C a
nd D
istri
ct le
vels
.
81
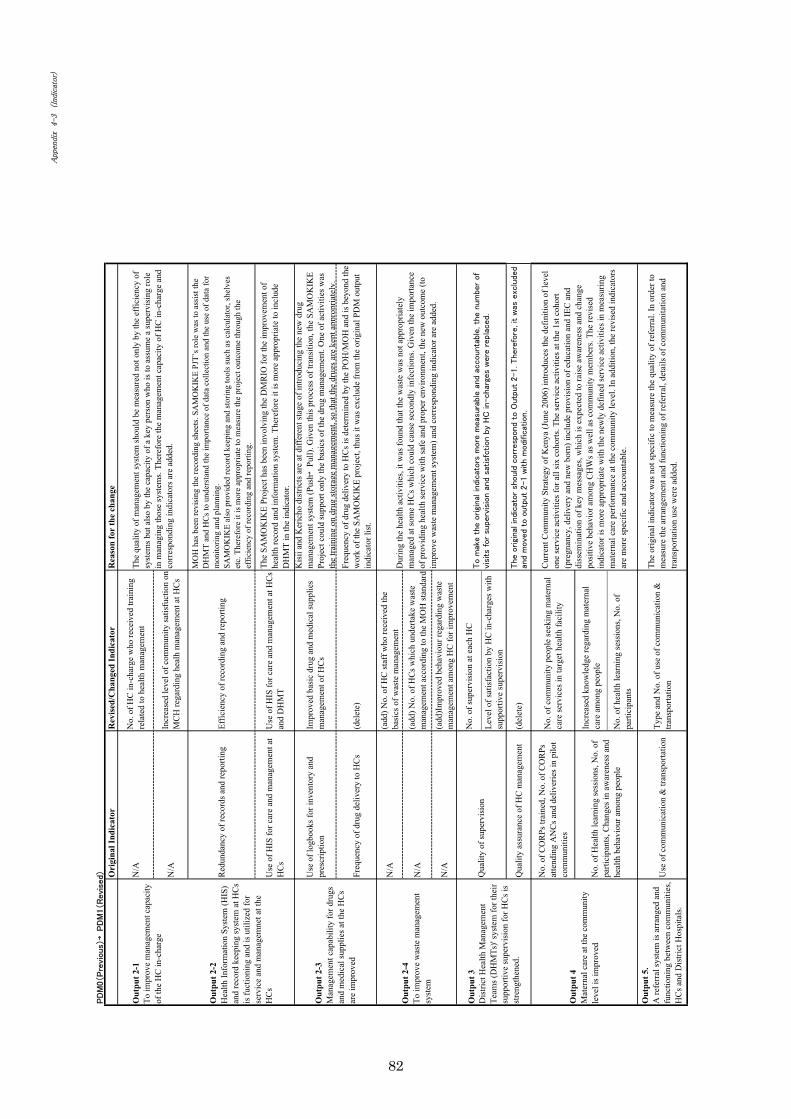
→O
rigi
nal I
ndic
ator
Rev
ised
/Cha
nged
Indi
cato
rR
easo
n fo
r th
e ch
ange
N/A
No.
of H
C in
-cha
rge
who
rece
ived
trai
ning
rela
ted
to h
ealth
man
agem
ent
N/A
Incr
ease
d le
vel o
f com
mun
ity sa
tisfu
ctio
n on
MC
H re
gard
ing
heal
h m
anag
emen
t at H
Cs
Red
unda
ncy
of re
cord
s and
repo
rting
Effic
ienc
y of
reco
rdin
g an
d re
porti
ng
MO
H h
as b
een
revi
sing
the
reco
rdin
g sh
eets
. SA
MO
KIK
E PJ
T’s r
ole
was
to a
ssis
t the
DH
MT
and
HC
s to
unde
rsta
nd th
e im
porta
nce
of d
ata
colle
ctio
n an
d th
e us
e of
dat
a fo
rm
onito
ring
and
plan
ning
.SA
MO
KIK
E al
so p
rovi
ded
reco
rd k
eepi
ng a
nd st
orin
g to
ols s
uch
as c
alcu
lato
r, sh
elve
set
c. T
here
fore
it is
mor
e ap
prop
riate
to m
easu
re th
e pr
ojec
t out
com
e th
roug
h th
eef
ficie
ncy
of re
cord
ing
and
repo
rting
.
Use
of H
IS fo
r car
e an
d m
anag
emen
t at
HC
sU
se o
f HIS
for c
are
and
man
agem
ent a
t HC
san
d D
HM
T
The
SAM
OK
IKE
Proj
ect h
as b
een
invo
lvin
g th
e D
MR
IO fo
r the
impr
ovem
ent o
fhe
alth
reco
rd a
nd in
form
atio
n sy
stem
. The
refo
re it
is m
ore
appr
opria
te to
incl
ude
DH
MT
in th
e in
dica
tor.
Use
of l
ogbo
oks f
or in
vent
ory
and
pres
crip
tion
Impr
oved
bas
ic d
rug
and
med
ical
supp
lies
man
agem
ent o
f HC
s
Kis
ii an
d K
eric
ho d
istri
cts a
re a
t diff
eren
t sta
ge o
f int
rodu
cing
the
new
dru
gm
anag
emen
t sys
tem
(Pus
h →Pu
ll). G
iven
this
pro
cess
of t
rans
ition
, the
SA
MO
KIK
EPr
ojec
t cou
ld su
ppor
t onl
y th
e ba
sics
of t
he d
rug
man
agem
ent.
One
of a
ctiv
ities
was
the
train
ing
on d
rug
stor
age
man
agem
ent,
so th
at th
e dr
ugs a
re k
ept a
ppro
pria
tely
.
Freq
uenc
y of
dru
g de
liver
y to
HC
s(d
elet
e)Fr
eque
ncy
of d
rug
deliv
ery
to H
Cs i
s det
erm
ined
by
the
POH
/MO
H a
nd is
bey
ond
the
wor
k of
the
SAM
OK
IKE
proj
ect,
thus
it w
as e
xclu
de fr
om th
e or
igin
al P
DM
out
put
indi
cato
r lis
t.
N/A
(add
) No.
of H
C st
aff w
ho re
ceiv
ed th
eba
sics
of w
aste
man
agem
ent
N/A
(add
) No.
of H
Cs w
hich
und
erta
ke w
aste
man
agem
ent a
ccor
ding
to th
e M
OH
stan
dard
N/A
(add
)Im
prov
ed b
ehav
iour
rega
rdin
g w
aste
man
agem
ent a
mon
g H
C fo
r im
prov
emen
t
No.
of s
uper
visi
on a
t eac
h H
C
Leve
l of s
atis
fact
ion
by H
C in
-cha
rges
with
supp
ortiv
e su
perv
isio
n
Qua
lity
assu
ranc
e of
HC
man
agem
ent
(del
ete)
No.
of C
OR
Ps tr
aine
d, N
o. o
f CO
RPs
atte
ndin
g A
NC
s and
del
iver
ies i
n pi
lot
com
mun
ities
No.
of c
omm
unity
peo
ple
seek
ing
mat
erna
lca
re se
rvic
es in
targ
et h
ealth
faci
lity
Incr
ease
d kn
owle
dge
rega
rdin
g m
ater
nal
care
am
ong
peop
le
No.
of h
ealth
lear
ning
sess
ions
, No.
of
parti
cipa
nts
Use
of c
omm
unic
atio
n &
tran
spor
tatio
nTy
pe a
nd N
o. o
f use
of c
omm
unic
atio
n &
trans
porta
tion
The
orig
inal
indi
cato
r was
not
spec
ific
to m
easu
re th
e qu
ality
of r
efer
ral.
In o
rder
tom
easu
re th
e ar
rang
emen
t and
func
tioni
ng o
f ref
erra
l, de
tails
of c
omm
unita
tion
and
trans
porta
tion
use
wer
e ad
ded.
Dur
ing
the
heal
th a
ctiv
ities
, it w
as fo
und
that
the
was
te w
as n
ot a
ppro
pria
tely
man
aged
at s
ome
HC
s whi
ch c
ould
cau
se se
cond
ly in
fect
ions
. Giv
en th
e im
porta
nce
of p
rovi
ding
hea
lth se
rvic
e w
ith sa
fe a
nd p
rope
r env
ironm
ent,
the
new
out
com
e (to
impr
ove
was
te m
anag
emen
t sys
tem
) and
cor
resp
ondi
ng in
dica
tor a
re a
dded
.
Cur
rent
Com
mun
ity S
trate
gy o
f Ken
ya (J
une
2006
) int
rodu
ces t
he d
efin
ition
of l
evel
one
serv
ice
activ
ities
for a
ll si
x co
horts
. The
serv
ice
activ
ities
at t
he 1
st c
ohor
t(p
regn
ancy
, del
iver
y an
d ne
w b
orn)
incl
ude
prov
isio
n of
edu
catio
n an
d IE
C a
nddi
ssem
inat
ion
of k
ey m
essa
ges,
whi
ch is
exp
ecte
d to
rais
e aw
aren
ess a
nd c
hang
epo
sitiv
e be
havi
or a
mon
g C
HW
s as w
ell a
s com
mun
ity m
embe
rs. T
he re
vise
din
dica
tor i
s mor
e ap
prop
riate
with
the
new
ly d
efin
ed se
rvic
e ac
tiviti
es in
mea
surin
gm
ater
nal c
are
perf
orm
ance
at t
he c
omm
unity
leve
l. In
add
ition
, the
revi
sed
indi
cato
rsar
e m
ore
spec
ific
and
acco
unta
ble.
Qua
lity
of su
perv
isio
n
Out
put 4
Mat
erna
l car
e at
the
com
mun
ityle
vel i
s im
prov
edN
o. o
f Hea
lth le
arni
ng se
ssio
ns, N
o. o
fpa
rtici
pant
s, C
hang
es in
aw
aren
ess a
ndhe
alth
beh
avio
ur a
mon
g pe
ople
Out
put 3
Dis
trict
Hea
lth M
anag
emen
tTe
ams (
DH
MTs
)' sy
stem
for t
heir
supp
ortiv
e su
perv
isio
n fo
r HC
s is
stre
ngth
ened
.
Out
put 5
.A
refe
rral
syst
em is
arr
ange
d an
dfu
nctio
ning
bet
wee
n co
mm
uniti
es,
HC
s and
Dis
trict
Hos
pita
ls.
Out
put 2
-3M
anag
emen
t cap
abili
ty fo
r dru
gsan
d m
edic
al su
pplie
s at t
he H
Cs
are
impr
oved
Out
put 2
-4To
impr
ove
was
te m
anag
emen
tsy
stem
The
qual
ity o
f man
agem
ent s
yste
m sh
ould
be
mea
sure
d no
t onl
y by
the
effic
ienc
y of
syst
ems b
ut a
lso
by th
e ca
paci
ty o
f a k
ey p
erso
n w
ho is
to a
ssum
e a
supe
rvis
ing
role
in m
anag
ing
thos
e sy
stem
s. Th
eref
ore
the
man
agem
ent c
apac
ity o
f HC
in-c
harg
e an
dco
rres
pond
ing
indi
cato
rs a
re a
dded
.
Out
put 2
-1To
impr
ove
man
agem
ent c
apac
ityof
the
HC
in-c
harg
e
Out
put 2
-2H
ealth
Info
rmat
ion
Syst
em (H
IS)
and
reco
rd k
eepi
ng sy
stem
at H
Cs
is fu
ctio
ning
and
is u
tiliz
ed fo
rse
rvic
e an
d m
anag
emne
t at t
heH
Cs
82
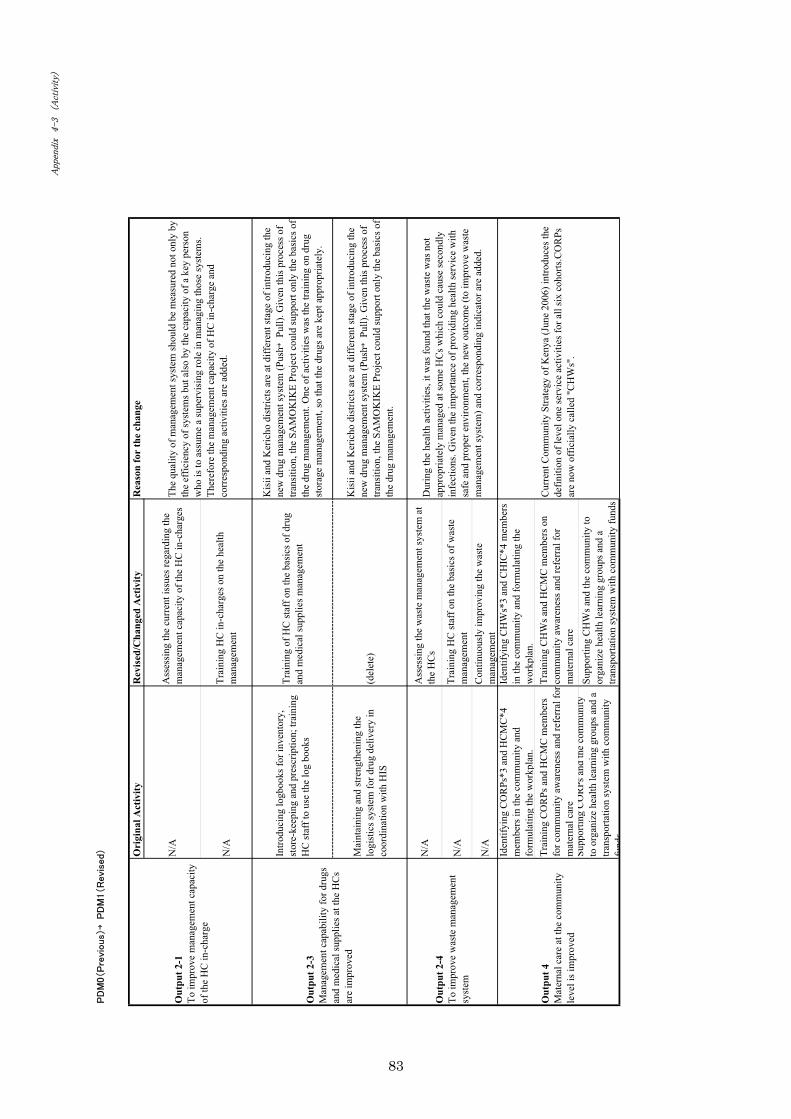
→
Ori
gina
l Act
ivity
Rev
ised
/Cha
nged
Act
ivity
Rea
son
for
the
chan
ge
N/A
Ass
essi
ng th
e cu
rren
t iss
ues r
egar
ding
the
man
agem
ent c
apac
ity o
f the
HC
in-c
harg
es
N/A
Trai
ning
HC
in-c
harg
es o
n th
e he
alth
man
agem
ent
Intro
duci
ng lo
gboo
ks fo
r inv
ento
ry,
stor
e-ke
epin
g an
d pr
escr
iptio
n; tr
aini
ngH
C st
aff t
o us
e th
e lo
g bo
oks
Trai
ning
of H
C st
aff o
n th
e ba
sics
of d
rug
and
med
ical
supp
lies m
anag
emen
t
Kis
ii an
d K
eric
ho d
istri
cts a
re a
t diff
eren
t sta
ge o
f int
rodu
cing
the
new
dru
g m
anag
emen
t sys
tem
(Pus
h →Pu
ll). G
iven
this
pro
cess
of
trans
ition
, the
SA
MO
KIK
E Pr
ojec
t cou
ld su
ppor
t onl
y th
e ba
sics
of
the
drug
man
agem
ent.
One
of a
ctiv
ities
was
the
train
ing
on d
rug
stor
age
man
agem
ent,
so th
at th
e dr
ugs a
re k
ept a
ppro
pria
tely
.
Mai
ntai
ning
and
stre
ngth
enin
g th
elo
gist
ics s
yste
m fo
r dru
g de
liver
y in
coor
dina
tion
with
HIS
(del
ete)
Kis
ii an
d K
eric
ho d
istri
cts a
re a
t diff
eren
t sta
ge o
f int
rodu
cing
the
new
dru
g m
anag
emen
t sys
tem
(Pus
h →Pu
ll). G
iven
this
pro
cess
of
trans
ition
, the
SA
MO
KIK
E Pr
ojec
t cou
ld su
ppor
t onl
y th
e ba
sics
of
the
drug
man
agem
ent.
N/A
Ass
essi
ng th
e w
aste
man
agem
ent s
yste
m a
tth
e H
Cs
N/A
Trai
ning
HC
staf
f on
the
basi
cs o
f was
tem
anag
emen
t
N/A
Con
tinuo
usly
impr
ovin
g th
e w
aste
man
agem
ent
Iden
tifyi
ng C
OR
Ps*3
and
HC
MC
*4m
embe
rs in
the
com
mun
ity a
ndfo
rmul
atin
g th
e w
orkp
lan.
Iden
tifyi
ng C
HW
s*3
and
CH
IC*4
mem
bers
in th
e co
mm
unity
and
form
ulat
ing
the
wor
kpla
n.Tr
aini
ng C
OR
Ps a
nd H
CM
C m
embe
rsfo
r com
mun
ity a
war
enes
s and
refe
rral
for
mat
erna
l car
e
Trai
ning
CH
Ws a
nd H
CM
C m
embe
rs o
nco
mm
unity
aw
aren
ess a
nd re
ferr
al fo
rm
ater
nal c
are
Supp
ortin
gC
OR
Psan
dth
eco
mm
unity
to o
rgan
ize
heal
th le
arni
ng g
roup
s and
atra
nspo
rtatio
n sy
stem
with
com
mun
ityfu
nds
Supp
ortin
g C
HW
s and
the
com
mun
ity to
orga
nize
hea
lth le
arni
ng g
roup
s and
atra
nspo
rtatio
n sy
stem
with
com
mun
ity fu
nds
Out
put 2
-3M
anag
emen
t cap
abili
ty fo
r dru
gsan
d m
edic
al su
pplie
s at t
he H
Cs
are
impr
oved
The
qual
ity o
f man
agem
ent s
yste
m sh
ould
be
mea
sure
d no
t onl
y by
the
effic
ienc
y of
syst
ems b
ut a
lso
by th
e ca
paci
ty o
f a k
ey p
erso
nw
ho is
to a
ssum
e a
supe
rvis
ing
role
in m
anag
ing
thos
e sy
stem
s.Th
eref
ore
the
man
agem
ent c
apac
ity o
f HC
in-c
harg
e an
dco
rres
pond
ing
activ
ities
are
add
ed.
Out
put 2
-1To
impr
ove
man
agem
ent c
apac
ityof
the
HC
in-c
harg
e
Cur
rent
Com
mun
ity S
trate
gy o
f Ken
ya (J
une
2006
) int
rodu
ces t
hede
finiti
on o
f lev
el o
ne se
rvic
e ac
tiviti
es fo
r all
six
coho
rts.C
OR
Psar
e no
w o
ffic
ially
cal
led
"CH
Ws"
.
Out
put 4
Mat
erna
l car
e at
the
com
mun
ityle
vel i
s im
prov
ed
Out
put 2
-4To
impr
ove
was
te m
anag
emen
tsy
stem
Dur
ing
the
heal
th a
ctiv
ities
, it w
as fo
und
that
the
was
te w
as n
otap
prop
riate
ly m
anag
ed a
t som
e H
Cs w
hich
cou
ld c
ause
seco
ndly
infe
ctio
ns. G
iven
the
impo
rtanc
e of
pro
vidi
ng h
ealth
serv
ice
with
safe
and
pro
per e
nviro
nmen
t, th
e ne
w o
utco
me
(to im
prov
e w
aste
man
agem
ent s
yste
m) a
nd c
orre
spon
ding
indi
cato
r are
add
ed.
83

App
endi
x�5
Lis
t of I
EC
/BC
C m
ater
ials
pro
vide
d by
SA
MO
KIK
E p
roje
ct
No
IEC
/BC
CTa
rget
O
bjec
tive
Maj
or C
onte
nt
Dis
trib
utio
n M
etho
d
1
Post
er o
f Mod
el o
n
Goo
d C
usto
mer
Car
e
HC
staf
f To
im
prov
e cu
stom
er c
are
at
the
HC
s.
-
Idea
l atti
tude
of H
C st
aff t
owar
d cl
ient
s D
istri
bute
d on
e po
ster
for
eac
h
HC
.
MC
2
Post
er o
f R
efer
ral
Proc
edur
e on
Mat
erna
l
Emer
genc
y
HC
staf
f To
le
ad
the
HC
st
aff
to
appr
opria
te
refe
rral
pr
oced
ure
in c
ase
of e
mer
genc
y.
-
Ref
erra
l Pro
cedu
res
Dis
tribu
ted
one
post
er f
or e
ach
HC
.
3
5S a
pron
H
C st
aff
To sh
ow 5
S1K
prin
cipl
es to
ever
ybod
y in
HC
(Sta
ff,
clie
nts)
.
To g
et a
n at
tent
ion
abou
t 5S1
K
activ
ities
-5S
mar
k
-C
onte
nts
of 5
S1K
(So
rt, S
et,
Shin
e, S
tand
ardi
ze,
Sust
ain,
and
Kee
p it
up)
Giv
en
one
apro
n to
5S
1K
man
ager
on
the
day
of tr
aini
ng
4
5S1K
ToT
mat
eria
ls
HC
staf
f and
com
mun
ity m
embe
rs
To te
ach
5S1K
prin
cipl
es to
HC
staf
f and
com
mun
ity m
embe
rs
-Pu
rpos
e of
5S1
K
-M
eani
ng o
f 5S1
K
-Ex
ampl
e of
5S1
K a
ctiv
ities
-Ex
ampl
e of
5S1
K (b
efor
e an
d af
ter)
Giv
en o
n se
t of
mat
eria
l (1
0
slid
es w
ith la
min
atio
n) to
5S1
K
man
ager
(one
set p
er e
ach
HC
)
HM
5
5S1K
man
ager
badg
e
5S1K
man
ager
(HC
staf
f)
To e
ncou
rage
5S1
K m
anag
er to
act a
s man
ager
of 5
S1K
-N
ame
of th
e pe
rson
-M
eani
ng o
f 5S1
K
-Ph
oto
of th
e pe
rson
with
5S
apro
n
Giv
en o
n th
e da
y of
trai
ning
for
5S1K
man
ager
.
�
84
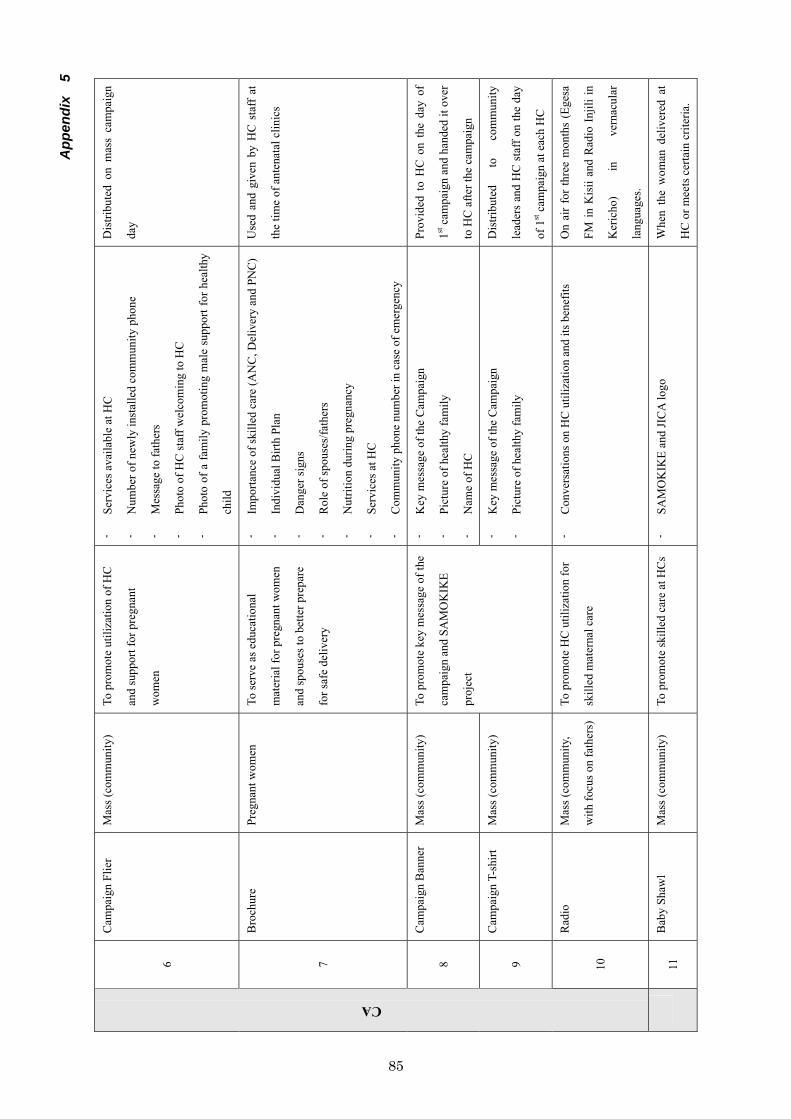
App
endi
x�5
6
Cam
paig
n Fl
ier
Mas
s (co
mm
unity
) To
pro
mot
e ut
iliza
tion
of H
C
and
supp
ort f
or p
regn
ant
wom
en
-Se
rvic
es a
vaila
ble
at H
C
-N
umbe
r of n
ewly
inst
alle
d co
mm
unity
pho
ne
-M
essa
ge to
fath
ers
-Ph
oto
of H
C st
aff w
elco
min
g to
HC
-Ph
oto
of a
fam
ily p
rom
otin
g m
ale
supp
ort f
or h
ealth
y
child
Dis
tribu
ted
on m
ass
cam
paig
n
day
7
Bro
chur
e Pr
egna
nt w
omen
To
serv
e as
edu
catio
nal
mat
eria
l for
pre
gnan
t wom
en
and
spou
ses t
o be
tter p
repa
re
for s
afe
deliv
ery
-Im
porta
nce
of sk
illed
car
e (A
NC
, Del
iver
y an
d PN
C)
-In
divi
dual
Birt
h Pl
an
-D
ange
r sig
ns
-R
ole
of sp
ouse
s/fa
ther
s
-N
utrit
ion
durin
g pr
egna
ncy
-Se
rvic
es a
t HC
-C
omm
unity
pho
ne n
umbe
r in
case
of e
mer
genc
y
Use
d an
d gi
ven
by H
C s
taff
at
the
time
of a
nten
atal
clin
ics
8
Cam
paig
n B
anne
r M
ass (
com
mun
ity)
-K
ey m
essa
ge o
f the
Cam
paig
n
-Pi
ctur
e of
hea
lthy
fam
ily
-N
ame
of H
C
Prov
ided
to
HC
on
the
day
of
1st c
ampa
ign
and
hand
ed it
ove
r
to H
C a
fter t
he c
ampa
ign
9
Cam
paig
n T-
shirt
M
ass (
com
mun
ity)
To p
rom
ote
key
mes
sage
of t
he
cam
paig
n an
d SA
MO
KIK
E
proj
ect
-K
ey m
essa
ge o
f the
Cam
paig
n
-Pi
ctur
e of
hea
lthy
fam
ily
Dis
tribu
ted
to
com
mun
ity
lead
ers
and
HC
sta
ff on
the
day
of 1
st c
ampa
ign
at e
ach
HC
CA
10
Rad
io
Mas
s (co
mm
unity
,
with
focu
s on
fath
ers)
To p
rom
ote
HC
util
izat
ion
for
skill
ed m
ater
nal c
are
-C
onve
rsat
ions
on
HC
util
izat
ion
and
its b
enef
its
On
air
for
thre
e m
onth
s (E
gesa
FM in
Kis
ii an
d R
adio
Inj
ili in
Ker
icho
) in
ve
rnac
ular
lang
uage
s.
11
Bab
y Sh
awl
Mas
s (co
mm
unity
) To
pro
mot
e sk
illed
car
e at
HC
s-
SAM
OK
IKE
and
JIC
A lo
go
Whe
n th
e w
oman
del
iver
ed a
t
HC
or m
eets
cer
tain
crit
eria
.
�
85

IEC
Imag
es
1.Po
ster
of M
odel
on
Goo
d C
usto
mer
Car
e2.
Pos
ter
of R
efer
ral P
roce
dure
on
Mat
erna
l Em
erge
ncy
3. “
5S a
pron
”
4. “
5S1K
ToT
mat
eria
ls “
5. 5
S1K
man
ager
bad
ges
6. C
ampa
ign
Flie
r
86

Appe
ndix
5
7. B
roch
ure
8. C
ampa
ign
Ban
ner
9. C
ampa
ign
T-sh
irt
11. B
aby
Shaw
l
87

Appendix 6
JOINT NATIONAL PROJECT STEERING COMMITTEE MEETING HELD ON 14/9/05 IN AFYA HOUSE.
Attendants.1. Mr. Zacharia Ogongo P/S MOH 2. Ms Naoko Fujita Hands chief advisor/project manager 3. Ms Masayo Nonoguchi Hands project coordinator 4. Dr Yasuhiko Kamiya Hands Technical Advisor 5. Dr Kemboi C.K DMOH –Kericho 6. Dr E.S Abunga DMOH-Kisii 7. Joseph N Neya DS/DIV-MOH 8. Ms Yumiko Igarashi JICA 9. Dr Willi Nyambati JICA Kenya office 10.Mr. Jiro Inamura DRR, JICA Kenya office 11.Dr Marsden Solomon Deputy Head, DRH 12.Mr. Daniel Sande DRH-National coordinator
ApologyDr Misore Head PPHS
The meeting started at 9.30am after handing over ceremony of two ambulances to Kisii and Kericho DMOHs.
Min 1/9/05: Welcome Remarks. The P/S chaired the meeting. He welcomed members and requested them to introduce themselves.
Min 2/9/05: Issues arising Office in Kericho is to be put up now awaiting AIE to avail funds, details of this will be reported in the next meeting by P/S office. The P/S requested for early ownership of the project by the concerned districts.
Min 3/9/05: Achievements April to August Operational and Technical achievements were presented. This was the project progress report in the last 4 months since its commencement in April 2005.
89

Appendix 6
The project has held several meetings at different levels, NTWC 2 meetings, DPCC 3 meetings in Kisii and Kericho, JNPSC it was the first meeting.Office set up in Kisii had been done. Fixing and ordering vehicles for the project (two ambulances for Kisii and Kericho have been handed over) Community Based Study had been done which included Dissemination workshop at Kericho on 12/8/05. Facility Based Study was done including feedback workshop 4 times, this necessitated rescheduling of some planned project activities.
Min 4/9/05: Constraints, Challenges and Concerns. Temporary project office issue in Kericho Project counterparts-budgetary and secondment issues. Coordination of the project with the District, GOK and JICA.
Min5/9/05: Progress report on HC renovation. HANDS decided minor renovations for 10 HCs based on the HC assessment. Total budget for renovation for the project Kshs.4, 060,000/= Renovation points include; water supply system, fencing and gate, drainage and partitioning. There is good community participation in monitoring the progress of HC renovation.
Min 6/9/05: Provision of medical equipments for maternal care. The process of procurement is as follows; HC assessment was conducted in june/july, and request for RH equipments from DRHT in Kisii and Kericho was received in August. The DRH gave standardized RH equipment list on 2/9/05.During HC assessment a lot of donated equips were found in good condition but not in use, while some HCs offering delivery services lacked equipments.
Min7/5/09: Procurement Policy. The project will;
- Provide medical equipments following the national guideline. - Consider making full use of existing facilities and equipments and
proper maintenance through the assistance of the two trained medical engineering personnel.
- Redistribution of donated equipments under supervision of DMOH in Kisii and Kericho-this will be realistically done at the end of the project.
90

Appendix 6
- Consider provision of other equipments as per HC individual needs. GOK funds in the two districts have been factored in the New District Health Plan to assist in procurement of equipments and renovations
Min 8/9/05 Any Other Business. HANDS/JICA expressed concern on counterpart funding from the MOH in relation to the project. In response, the PS said he would look into the matter and give feedback in subsequent meetings. It was agreed that there is need to enhance service demand seeking behavior by:--sensitizing the community on the services available. -enhancing quality maternal services -renovating of the existing HCs -strengthening referral systems (project ambulances in place) By addressing above issues members felt the communities’ confidence will be enhanced and this will increase number of client seeking behavior. The P/S emphasized on interaction and involvement of other community development projects i.e. CDF, LATIFA etc
There being no other business JICA country representative appreciated the presence of P/S who then thanked members for attending the meeting. Next meeting to be held on 16/11/05. Meeting closed at 11.30am
Sign………………….. Date…………………………….
Chairman.
Sign…………………. Date…………………………….
Secretary.
91
Appendix 6
MINUTES OF THE JOINT NATIONAL PROJECT STEERING COMMITTEE MEETING ON 16TH NOV, 2005 BETWEEN MOH AND JICA/HANDS AT AFYA HOUSE.
MEMBERS PRESENT. 1. Mr.Zachariah Ogongo Permanent Secretary-MoH –Chairman. 2. Dr Ambrose Misore Head PPHS-MoH 3. Dr Eric Abunga DMOH – Kisii 4. Dr Kemboi C K DMOH – Kericho 5. Dr M.M Solomon DRH –MoH 6. Mr J.M Gitonga PHO/D 7. Dr Were S.N ADMS, HSRS8. Mr Daniel Sande DRH-MoH 9. Ms Naoko FUJITA HANDS –Project Manager 10. Ms Yoko SUZUKI HANDS –Tokyo Officer 11. Dr Willie Nyambati Jica Kenya Office 12. Ms Yumiko Igarashi Jica 13. Mr Jiro Inamura Jica Kenya Office.
ABSENT WITH APOLOGY.1. Dr J.Nyikal DMS2. Dr I. Amira PMO Rift Valley 3. Dr J Gesami PMO Nyanza 4. Mr Charles Mutiso Rep.Ministry of Finance
The meeting started at 9.30am.
Min 1/11/05 Welcome Remarks Welcome remarks from the Permanent Secretary and self introduction of members.Remarks from Jica’s country representative and briefing on project progress to P/S and members.
Min 2/11/05 Achievements in the 1st term.HANDS representative took members through the projects’ achievements in the 1st term which included; Maternal Care –she told members preparation for the training for next year were on going, printing of the ANC/Delivery /PNC registers to be finalized in January 2006.
92

Appendix 6
JICAs’Kenya office in process of procuring equipments worth approximately Kshs. 4,500,000/= which will be distributed in Health Centers (HCs) in Feb 2006, HANDS Kenya has purchased equipments/materials worth approximately Kshs 1300, 000/= and had done distribution more distribution will be in Feb, 2006.
Health Management –procurement and handover of vehicles (two ambulances) to DHMT Kisii and Kericho had been done, procurement of drug storage and record keeping cabinet was in process. Printing of registers was in process and distribution will be early next year.
Health Centre renovation-Minor HC renovation had been done in 5 HCsin Kisii, 4 HCs in Kericho.Total renovation budget Kshs 4,060,000/=
Community Activities included involvement in the HC renovation, and establishment of women groups. Training of the community on maternal issues targeted both men and women.
Operational Achievements-this included office set up in Kisii and Kericho and hiring of staff. Construction of new office in Kericho to start early 2006. In summary effects of these years activities were geared towards improving Safe Motherhood(SM) services in HC and the community.
Plans for 2006 Jan-March included;Maternal Care-distribution of MC medical equipments, training of staff
and community members. Health Management –drug management plan development and training,
strengthening MC record keeping system and finalizing supervision list with DHMT,Community Activities-training of women and men in SM and
strengthening relationship between HC and community.
-HANDS /JICA to contribute Kshs300, 000/= towards Kericho office construction while GoK-MoH to fund the construction.
-consideration for spacious cabinets for drug storage during renovation to be done since the revised drug kit is bulky-there is need to lias with HC management during this activity. -consider purchasing solar panels in sunny areas since generators are costly.
93
Appendix 6
-Community involvement is important and that the process of strengthening HC management was underway where each HC is expected to open an account and revive HC management committees that are gender sensitive. -Male involvement in maternal health services is necessary. -Need to improve security and maintenance of HC through community involvement. Appropriate location and standardizing of drug stores is necessary. -Need to strengthen HC management since present health needs are demanding, it is necessary to know what modern health facility constitutes,ie hospital, HC or dispensary levels, and upgrading of facilities should be done appropriately.-Need to have close monitoring of drugs and other commodities through use of standardized tools/registers.
Min3/11/2005 Constraints and Challenges.Concerns on Counterpart budget –this was being worked on and it will be reflected in Feb/March 2006 revised estimates, since treasury had agreed to incorporate the 3 year JICA/ HANDS project
Staff shortage –there was on going recruitment and the head of PPHS promised to act through CNOs’ office depending on staff returns from the two districts.
-In Kericho staff redistribution was in process. -There is need to address post basic and other training related matters by the facility management i.e. by not allowing all staff to go for training at the same time, management to consider facility needs first.
Min 4/11/05 A O B -HANDS team leaves on 18/11/2005 to JAPAN for holidays, to be back mid January 2006 (project will continue running while they are away) -HANDS expressed need to have an office in Nairobi to assist in streamlining coordination of project activities. -Members agreed to have the national team visiting the project sites before the next meeting. -There is need to make arrangements for official handing over of the JICA and BELGIUM projects in Kisii and Nyamira districts. -Need to have deeper involvement in the project through emulatinglesions learnt in other facilities and replicating them in the project.
94

Appendix 6
-Need to have issues taken to the ground and involve the community while handling the matters rather than having issues handled in boardrooms
With no other business, the P/S thanked the JICA/HANDS team for there commendable work and wished them safe journey to Japan.
Next JNPSC 19/1/2006, DPCC 27/1/2006, NTWC date to be fixed. There will be project progress meeting on 9/3/2006 Meeting closed at 10.30am.
Chairman………………………….. Date……………………….
Secretary…………………………… Date………………………..
95

Appendix 6
MINUTES OF THE THIRD JOINT NATIONAL PROJECT STEERING COMMITTEE MEETING ON 29TH SEPT, 2006 BETWEEN MOH AND JICA/HANDS AT AFYA HOUSE
MEMBERS PRESENT 1. Mr.Hezron Nyangito Permanent Secretary-MoH –Chairman. 2. Dr S K Sharrif Head PPHS-MoH 3. Dr Josephine Kibaru Head-DRH –MoH 4. Dr Eric Abunga DMOH – Kisii 5. Dr Kemboi C.K. DMOH – Kericho 6. Mr F.M Ombwori Personal Assistant/PS 7. Prof.Handa Y Regional formulation Advisor, JICA 8. Mr. Daniel Sande DRH-MoH 9. Yumiko Kitagawa HANDS –Technical advisor MC 10. Mamoru Shimamoto HANDS –Project Manager 11. Kazuhiko Tokuhashi DRR-JICA Kenya Office 12. Ms Yumiko Igarashi JICA Project formulation Advisor 13. Keiko Takahashi HANDS. 14. Kiyomi Yamamoto HANDS 15. Yoshiki Ehare JICA Kenya 16. E Kinyangi JICA Prog. Officer
ABSENT WITH APOLOGY.1. DMS 2. PMO Rift Valley 3. PMO Nyanza 4. Rep. Ministry of Finance
The meeting started at 9.15am.
Min 1/9 Welcome Remarks - Welcome remarks from the Permanent Secretary and self introduction of
members.- Safe Motherhood is a key area in health and there is need to focus on it
due to challenges facing it. - He Called for duplication of Samokike Project in other parts of the country
and urged the involved parties to scale up the project - He commented on evaluation of the project and said it was crucial for the
purpose of prioritization of project activities, and emphasized on need for integration of health services.
- With maternal health being one of the MDGs, all efforts to improve the project outcome were welcome.
96
Appendix 6
Min. 2/9 Address from DRR JICA Office Kenya
- Thanked MOH for cooperation and mentioned achievements due to cooperation
- Emphasized on need to have strong health system to address health challenges; Malaria, HIV/AIDS, TB and said that with this in place safe motherhood will be achieved.
- Said JICA was willing to support MOH activities in other districts. - Mentioned JICA had sent 16 experts from HANDS to the project. - Commented on the trainings and the benefits to the HC staff and the
community.- He said that the project mid-term evaluation was one of the 3rd phase
agenda and he looked forward for cooperation/participation from MOH/JICA and HANDS. Prof. Handa would lead the evaluation team from JICA side.
- Called for support from MOH to the implementing organization HANDS.
Min: 3/9 Presentation on Mid-term Evaluation SAMOKIKE Project
- Emphasis on joint evaluation process and report writing MOH/JICA and HANDS was made.
- Role of evaluation was to acknowledge the evidence of project progress in terms of assessing how much more input was required and other positive project performance policy aspect and for betterment of health services.
- Members were shown and explained to the project design matrix format that was used in the project.
- 5 projects outputs were mentioned to members. - He mentioned that HANDS used integrated approach in implementation of
the 5 outputs and this was in collaboration with MOH (DMOH). - He mentioned expected efficiency based on the project outputs, with
emphasis to HC and communities. - More indicators were required for the evaluation process, which was being
worked on, and the outcome was necessary and essential evidence to be shown to MOH, JICA Kenya office and Japan Government.
- Evaluation report was necessary in determining project progress. - He said project design was relevant since it is in line with local demand,
the project goal being health issues especially maternal health is improved. - Members were reminded that no short comings in terms of efficiency in
the project activities had occurred. - He mentioned that there was effectiveness in the project, how the 5
outputs were contributing to the project outputs. - Despite staff shortage, the ones in health facilities were motivated
especially due to project works, and they require acknowledgement and support.
97

Appendix 6
- The project has a positive impact since it addresses maternal health care issues.
- On sustainability, he mentioned that retention of trained staff was crucial since it could assist in measuring project sustainability.
- He called for active participation and collaboration from Kenyan side both MoH/DMoH and locals (community),
- He had high expectation in the project as JICA/Japanese government would like to use the evaluation report in other sub-Saharan countries of Africa.
- The PS thanked Prof. Handa and assured him of total support and contribution in the project especially during mid-term evaluation.
- He added MOH was shifting its priorities towards community approach, and he looked forward to having the report as it could assist in improving the health status of the communities and else where.
DMOH – Kericho
- He commended the project especially the renovations in the 7 health centers. He added there was increase in maternal services due to improved services and availability of referral services. Supervision was being done in good time using the developed checklist and he looked forward to the mid-term evaluation exercise.
DMOH – Kisii
- Commended the project and said there was full community participation and involvement.
- Repairs were being done with focus to reproductive health. - Ambulance had improved referral services - Number of deliveries had increased through improved maternal care - Checklist was assisting in the joint supervision - Commented on the current staff training and added it was possible to
sustain the project. - On staff shortage he assured members of balancing staff in the health
centers following the recent MOH posting.
Min: 4/9 AOB- PS told the DMOHs to redistribute staff for balance - Members were informed of the uniqueness of the project as it was being
implemented by Japan NGO. - It is important that the evaluation should have the report and the costs of
the project as it was being implemented by NGO. - DPPHs emphasized on community participation, and that evaluation
should measure community involvement.
98
Appendix 6
- He called for additional indicators i.e. to address community and maternal care i.e. number of deliveries with skilled birth attendants.
- All activities done at community level that had led to increase to number of deliveries could be copied elsewhere as lessons learnt.
- It was important for the community people to be organized and educated by HC staff before the exercise.
- Evaluation was scheduled for October whereas report writing was scheduled for November.
- PS assured cooperation and support from MOH side.
With no other business, the meeting ended at 10.15 am.
Chairman………………………………….Date……………………….
Secretary…………………………………..Date……………………….
99

Appendix 6
MINUTES OF THE TECHNICAL COMMITTEE MEETING HELD ON APRIL 28, 2OO5
BETWEEN, MOH AND JICA (HANDS) AT AFYA HOUSE
MEMBERS PRESENT
1. Dr. A.O. Misore - Head, PPHS - Chairman 2. Dr. J. Kibaru - Head, DRH 3. Dr. E.S. Abunga - DMOH, Kisii 4. Dr. Kemboi C.K. - DMOH, Kericho 5. Kano Yoshiaki - Resident Representative, JICA 6. Nyambati Willie - JICA 7. Daniel E. Sande - DRH 8. Kanenawa Tomaki - JICA 9. Ehala Yoshiko - JICA 10.Fujita Naoko - HANDS 11.Kamiya Yasuniko - HANDS 12.Chiba Yoko - HANDS 13.Nonoguchi Masayo - HANDS
ABSENT WITH APOLOGY
1. Dr. James Nyikal - DMS
AGENDA
1. Welcome and introduction2. Review of the previous minutes 3. Matters arising 4. Any Other Business
� Dr. Misore who was chairing the meeting welcomed those present and asked them to introduce themselves.
� He thanked JICA and HANDS for their effort towards improving health care services in the two districts (Kisii and Kericho) focusing on Safe Motherhood and systems support for the 3 years they will be running the project.
100
Appendix 6
� JICA countries resident representative called for support from MOH and other teams working in the area and added that this will in turn encourage Japan Government’s effort in funding the project.
� Head, DRH gave an overview of the current maternal situation in the country. She mentioned causes of maternal death, direct and indirect causes contraceptives use, among women of reproductive age, in Kenya and mentioned that factors that led to increase in maternal death included poor referral system, poor infrastructure, inadequate health management and information systems, incompetent health provisions among other factors.
� She said, improving these factors would decrease maternal mortality in Kenya.
� HANDS Chief Advisor made a presentation on the overview of the project, its mission being working with people in improving their health status and added that it’s a non-profit making.
� MOH-Kisii made a presentation on the district plan, focusing on improving maternal health.
� He mentioned training activities for service health provider that will improve quality of care towards Safe Motherhood.
� Other matters discussed were: purchase of delivery equipments, PAC equipments and initiation of youth friendly activities.
� Improving communication both transport means and telephones� Need for clear policy from DRH on training of CORPS instead of TBAs. � Need to train Kericho DHMT on maternal health and prioritize community
activities. � Schedule of project was discussed and agreed that a project
implementation schedule should be made showing flow of activities. � It was agreed that regular meetings should be held in respect to the project.
Any Other Business
� Need to standardize equipment using rapid assessment tool was discussed and strict adherence to time frame to enable mid term evaluation of the project to be done at appropriate time.
� Proper arrangement be made to minimize interferance of the project with normal health services in the institutions owing to inadequate staff in the facilities especially in relation to training.
� Renovation and furnishing the Kisii/Kericho office was found necessary.
101

Appendix 6
� The committee agree that the National Steering Committee meeting be held on 25th August 2005 at 2.30 p.m. and Technical Committee meeting be held on 28th July 2005 from 9.00 a.m at Afya House.
� 1st District Committee meeting was scheduled on 6th May 2005 at Kericho Tea Hotel where head-DRH will chair the Meeting.
� With no other business Dr. Misore declared the meeting officially ended at 4.30 p.m.
Sign ……………………………………………… Date ………… Chairman
Sign ………………………………………………. Date………… Secretary
102
Appendix 6
NATIONAL TECHNICAL WORKING GROUP MEETING, MOH-JICA/HANDS SAFE MOTHERHOOD PROJECT IN AFYA HOUSE ON 4/8/2005.
IN ATTENDANCE
1. Dr. Kemboi C. K. DMOH/KERICHO 2. Dr. Josephine Kibaru Head – DRH/MOH 3. Adangah Ageism Policy & Planning Div. 4. Dr. E.S. Abunga DMOH Kisii 5. J. Inamura JICA Kenya 6. Tonoki Kanenawa JICA 7. Mamoru Shimamoto HANDS Kenya 8. Mayo Nonoguchi HANDS Kenya 9. Naoko Fujita HANDS Kenya 10.Yoko Chiba HANDS Kenya 11.Yauhiko Kamiya HANDS Kenya 12.Leonard Mauti DDPHN/ District Co-ord. 13.Mary Cheuiyot DDPHN/District Co-ord. 14.Mabwai Daudi HANDS 15.Sylvia Kimaru HANDS 16.Daniel Sande DRH/MOH
Absent with Apology1. Dr. Nyikal DMS
The meeting started at 9.00a.m.
Min. 1/8/05: Welcome Remarks
Dr. Misore chaired the meeting. He welcomed members, and requested them to introduce themselves. He took the group over the previous minutes. No issues arose after previous minute’s overview.
He introduced a new project member Mr.Shimamoto, and embarked on the agenda of the days meeting.
Min.2/8/05: Overall project progress This was the project progress report in the last 4 months since its commencement on 1st April 2005. Hands project manager took members through the overall project progress.
103

Appendix 6
Min. 3/8/05: Operational progress Staff recruitment for project operation had been done following advertisement on the daily newspaper though they (HANDS) require more staff to improve the project.Office set up for Kisii was done and completed in May 2005, though in Kericho they lacked a proper office and there is need to have a well-constructed office.She requested the MOH to construct a new building for them to get an office since the cost of renovating the current office was almost equivalent. She awaits feedback from MOH.
The hands project coordinator said on purchase of equipments including vehicles (2 ambulances and 2 project cars) said they were handling technical issues on importation. She said on 10th August the supervision vehicles will be at the Mombasa Port and will be in Nairobi by end of August. Supervision vehicle for hands will be available– end of September. She went ahead to show the group the type of vehicles they had purchased.
On networking a couple of meetings had been held previously and that meetings involving hands and local authority were on going.
Min. 4/08/05: Technical Progress
Facility assessment survey had been done by HANDS; these took one month.Community baseline study took 2 months, it was done by a private consultant firm (Almaco) ended July and that HANDS were expecting 1st draft of the report on baseline survey study in due course.
Members were shown major activity plan for 3 years with proper divisions, which included both original schedule vs. the re-schedule plan The said preparation period may take a bit longer than the expected, same to baseline survey and needs assessment – she said the delay was caused by the rescheduling of events/activities of the project.
Equipment purchase was in preparation period (September/October) since the equipments were already available in the country, while vehicles will be available by end of August.
Staff training is to be done next year2006 Health centre renovation was to be in 2006 but with re-scheduling, minor renovation will be commenced this year. Improving referral system and renovation of District Hospital will be done next year 2006. On community activities, the new project community technical adviser will work in collaboration with DHMT
104

Appendix 6
Monitoring and evaluation remains unchanged She reminded members that despite the alterations the project had not changed much.
Technical advisor on health management took the group on overall technical progressHe said the project had been divided in 4 phases and named them i.e.
(i)Introductory phase, (1st April-6th May) Involved;
– Introduction of Japanese Staff/DHMT –Introduction of the project
(ii) Preparatory phase (7th-30th May) – Involved confirmation of donors involvement in Kisii and Kericho
(iii) Health centre assessment phase (31stMay-12thJuly)–Involved Hands technical advisor and DHMT members in Kisii/Kericho
H/Cs(iv) Post H/C assessment phase(13th-July-Now)
- Involved data entry and analysis and schedule of meetings at various levels.
On health centre assessment findings he said two areas had been involved i.e. maternal care and Health management He discussed the findings of ANC, PNC, PMTC, FP and KEPI, and mentioned that TBAs practiced secretly by seeking help from private/mission hospitals.
He touched on facility equipment materials and spelled out some of challenges that exists i.e. lack of basic equipment and poor maintenance of existing equipments, poor record keeping, IP lacking etc He went ahead and showed pictures of H/C visited and renovated by JICA in 2003, and compared to the ones not renovated at all. The discrepancy was quite visible. From the assessment, it was found necessary to compare quality of service to quality of planning and management.
Other issues mentioned included need for proper renovations, availability of water supply and drainage systems, proper record keeping and management. DHMT supervision findings in health centers for both Kisii and Kericho were presented, and it emerged that most HCMCs were active.
Technical advisor on maternal care presented the community baseline study where she said improved maternal care at community level was the expected output from the community activities and that the purpose of study was to
105

Appendix 6
obtain people’s perspectives, knowledge, attitude and practice of pregnancy and childbirth. She said that ALMACO management consultants Ltd. Based in Nairobi had been subcontracted for the implementation of the project and that targeted communities were those ones within 1 kilometer from the 14 H/Centers targeted by the project.
She spelled out summary of observations and findings of community baseline study and gave out the way forward – that the project activities will be designed in collaboration with the representatives from the communities, H/Centre staff, DHMT members and HANDS TA on community activities.
Min. 5/8/05: Re-scheduling of project activitiesShe told members, that trainings were postponed since during assessment there was a problem with basic infrastructure therefore, DHMT/HANDS and communities found it necessary to start with renovations first.
This meant proper planning should be done before commencing the renovations. The current renovations were minor and that renovated H/Centers in 2002 by JICA were not to be considered.
She told members that 4M was available for the project and was to be spent by the end of October, 2005. Transparency of expenditure was mandatory and each H/Centre should write and handover proposal for renovation, regular reporting on progress and monitoring and evaluation by DHMT/HANDS will be continuous.
29/8/05 there will be a counterpart meeting for both districts, followed by regular meetings in Kisii and Kericho in respect to project progress. Members were shown procedures of H/C renovations and need for teamwork between H/Cs and the community. Responding to the presentations, the chairman told members that re-scheduling of project will not interfere with project process and that vehicles that are being purchased are not ambulances but for routine procedures.
He said there was need to find out basic equipments lacking in H/Cs and that some of donated equipments were not functioning but there was need to ensure proper maintenance of equipments the H/Cs are having. He assured members that there was adequate drug supply till September, 2006 and there was need to streamline drug use. He emphasized that currently drugs will be delivered to facilities not in the district depot allocation for the exercise is available.
He said money for Kericho hospital administration block was available and that further discussion on its utility was necessary before the construction works.
106
Appendix 6
He wanted to know what JICA/HANDS intended to do in Kericho in regard to construction/renovation, and cautioned the DMOH against giving out land to any other group since there is to save available land for expansion of the facility in future. He assured HANDS that Kericho would renovate one of the buildings to create an office for them.
Head-DRH wanted the vehicles to be modified to have all the facilities for ambulance services. She said registers were available i.e. ANC, PMTCT and PNC and suggested that the project can fund printing and distribution. On IP, she instructed DMOH Kericho to ensure that before equipments are purchased IP practice should be in place. Since government buys equipments for health facilities, HANDS should find out what’s lacking so that they don’t buy equipments already available.
The chairman wanted to know from HANDS whether the 4M was based on needs assessment findings and told members that each district has allocation of 6M for rural health facilities development and that HANDS should discuss with DHMT on necessary renovations, then with DHMT to choose the facilities that require renovation to enable merging of the funds in order to carry out reasonable work. He insisted on proposal submission by H/C and that only priority areas were to be chosen.
Min 6/8/05: Printed Estimates Head-DRH assured JICA/HANDS that their JICA project would appear on counterpart budget contribution by the MOH on the revised estimates of March 2006.Therefore the Kisii/Kericho DMOH should give their contributions.
JICA representative assure members that by end of this year the renovations will be done and that trainings will be on as from 2006.
Min.7/8/05: Project Collaboration On collaboration with counterparts, Technical advisor or maternal issues said the MOH staff lacked enough time to participate in working with them (HANDS) but after discussion the issues had been solved. She called for more MOH workers to assist with more information and organogram. Therefore there was need to second a DHMT member – Dr. Misore responded by urging the DMOH to expand activities in the district by allocating more staff from clinical area for these activities and proper coordination for office continuity. DMOH Kisii confirmed to members that he had already assigned a DHMT staff fully to the project and that DMOH Kericho was to do the same. The chairman urged members on prior planning of activities to avoid project activities clashing with normal daily activities.
107
Appendix 6
Min. 8/08/05: Schedule of other meetings � CBS – Dissemination by workshop 12/8/05 � 2nd JNPSC 25/8/05 2.30p.m. � 4th DPCC 16/9/05 � NTWC quarterly 3/11/05 subject to change
The chair thanked participants and said it was a good start with no other matters arising meeting ended at 11.30a.m.
Sign……………………………. Date………………………….
Chairman
Sign……………………………. Date…………………………..
Secretary.
108

Appendix 6
NATIONAL TECHNICAL WORKING COMMITTEE FOR MOH/HANDS/JICA SAFE MOTHERHOOD (SAMOKIKE) PROJECT ON 3
RD NOVEMBER, 2005
Members Present
1. Dr. J. Kibaru - Head DRH 2. Ms Naoko Fujita - HANDS Chief Advisor 3. Ms Yoko Chiba - HANDS Technical Advisor 4. Ms Masayo Nonoguchi - HANDS Project Coordinator 5. Ms Yoko Suzuki - HANDS Program Officer 6. Dr. Kemboi C. K. - DMOH Kericho 7. Ms. Yumiko Igarashi - JICA PA 8. Dr. E. S. Abunga - DMOH Kisii 9. Mr. Daniel Sande - DRH MoH 10. Dr. Willie Nyambati - JICA SPO 11. Mr. Jiro Inamura - PRR/JICA Kenya 12. Mr. Stephen Cheruiyot - Economist/Planning Officer – MoH
Absent with Apology Dr. A. O. Misore - Head PPHS
Meeting started at 9.00 a.m.
Min 1/11/05 Welcome Remarks Welcome and introductory remarks by DRH Head and Deputy Resident Representative, JICA Kenya Office.
Min 2/11/05 Presentation of Achievements in the 1st term
(March – November, 2005) HANDS
(i) Summary of achievements � Operational achievements included – Office setting
for Kisii and Kericho and staff recruitment/secondment. o Networking – meetings at National Level JNPSC
and NTWC at district level DPCC including meetings with other stakeholders and News letters.
o Technical achievements including baseline study and needs assessment, equipment provision, community involvement and HC renovations.
109
Appendix 6
(i) Achievement by each activity where issues on the following were discussed; � Maternal care at the health centres � Management at the health centres � District health management teams supervision � Maternal care at the communities
(ii) Provision of project equipment
� Multipurpose vehicles for districts use purchased and were handed over in September 2005 at Afya House other two project vehicles purchased for HANDS use in Kisii and Kericho. Details of multipurpose vehicles use explained.
� Medical equipment for Maternal care following guidelines from MoH-DRH, record keeping, and drug management were purchased, other equipments pending purchase by the SAMOKIKE budget while others by JICA.
(iii) Minor change on Project Design Matrix � Explanation on original project output and activities
against new project output and activities was given in details this included the old version i.e. Maternal Care Services at the Health Centres are upgraded against new version i.e. To improve maternal care at the health centres. This change came as a result of the Needs Assessment performed in the two districts (Kisii and Kericho).
Min 3/11/05 Constraints and Challenges
On office building in Kericho, the budgetary allocation of � 1.5M still pending awaiting financial release from the Ministry. On issues of counterpart budget, it was discussed that this budgetary allocation will be available by Feb/March 2006 approximately 10M. On weak participation by the DHMT members-it was discussed that prior activities planning and communication should be done on time while strengthening RH teams in the districts and delegation of duties will enhance full participation. On lack of H/C staff the MOH to address the issue.
110
Appendix 6
Min 4/11/05 Summary by DMOH � Establishment of supervision checklist for Kisii and
Kericho� Improvement of supervision activities in the health
facilities due to availability of supervision vehicles. � The SAMOKIKE project by HANDS is a ‘hands on’
project in comparison to other counterparts.
Presentation of Plan for 2nd term
Min 5/11/05 Plan of each activity
Outline of plans of each activity for the second phase was presented.
� Maternal care at the health centres, rough schedule of the SAMOKIKE project including training with proposed training program, delivery of donated equipments and joint meeting between HANDS and DRHT in Kisii and Kericho
Min 6/11/05 Brief Reports by DMOHS
� Health Centre management: - Management/staff/service issues in terms of the role of the district in improving management/staff/service issues.
� Maintenance of facility/equipment in terms of the district role in maintaining the facility equipment properly.
� Record keeping and the role of the district in provision of equipment and stationeries for record keeping
� Waste management following recommendation from the GoK guidelines
� Drug management � DHMT supervision. � Plan for community activity includes-training women group
leaders on SM with H/C staff o Installation of a generator to the model HC – Iranda HC o Follow up of the result of HC renovation o Collection of voices from community and reflection to
the SAMOKIKE Project.
111
Appendix 6
Min 7/11/05 AOB � HANDS and DRH can be accessed on internet through their
website www.hands.or.jp and www.drh.go.ke� DMOHs to have data of the project- will help in determine
project impact.� DMOHs to monitor the use of vehicles and equipment in the
districts. � HANDS presented (Logo mark design) meaning “lets work
together” this was approved by the DHMT in last 4th DPCC in Kericho
� Installation of generator in model H/C – Iranda, The DMOH/Community to agree on use, maintenance and fuelling this should be minuted.
� Through Rapid Result Initiative (RRI) the DMOHs of Kisii and Kericho should improve other SM issues especially FP uptake by improving their data through HMIS, distribution of commodities, supervision activities and other services in their districts with the presence of counterparts in their districts.
� District personnel to sustain the project while experts are away on holidays
� Need to share SM training schedule for the districts through the national coordinator.
� Need to integrate and coordinate activities in the districts-this will assist in identifying existing gaps in the districts that need to be addressed.
� For the purpose of project sustainability the GoK personnel need to participate fully rather than the community although the involvement of the community is important to enhance community ownership and uptake of services.
� Districts to order guidelines from DRH as other necessary arrangements for library are being mad- for the training models there is need to add others such as “madam Zoë” model.
With no other business meeting ended at 1 p.m. Next meeting date was scheduled for Feb. 2006.
Chairman --------------------------------------- Date ------------
Secretary --------------------------------------- Date ------------
112

Appendix 6
4TH NATIONAL TECHNICAL WORKING COMMITTEE MEETING FOR MOH/JICA/HANDS SAFE MOTHERHOOD (SAMOKIKE) PROJECT ON 15TH MARCH 2006
Members Present1. Dr. A. Misore -Head PPHS 2. Dr. J. Kibaru -Head DRH 3. Ms Yoko Chiba -HANDS Technical Advisor MC 4. Mr.Mamoru Shimamoto -Chief advisor HANDS Project 5. Ms Kyoko Koto -HANDS Program Officer 6. Dr. Kemboi C. K. -DMoH Kericho 7. Ms.Yumiko Igarashi -Project formulation advisor JICA 8. Dr. E. S. Abunga -DMoH Kisii 9. Mr. Daniel Sande -DRH MoH 10. Dr. Willie Nyambati -JICA SPO
Absent with Apology Mr. Kazuhiko Tokuhashi Deputy Resident Representative JICA
Meeting started at 9.00 a.m.
Min 1/03/06 Welcome Remarks Welcome and introductory remarks by Head PPHS.
Min 2/03/06 Address by DRR JICA. JICA Kenya office lost a member of staff hence Mr. Kazuhiko could not avail.
Min 3/03/06 Technical Activities in Second Phase Second phase had 60 days starting 22/1/2006 to 21/3/2006. Activities undertaken include office opening in Kisii and Kericho, highering of new local staff, holding of several meetings and implementing of activities including training of staff on matters concerning equipment and drug management, record keeping, follow ups and improving staff capacity in order to deliver quality MC services. All activities undertaken were based on action plan.
113
Appendix 6
Upgrading Maternal Care in HCs.One week orientation training on MC was contacted in Kisii and Kericho where service providers and 42 CORPS attended.
Improving management systems at HCs.Training curriculum already developed, training will be contacted in the 3rd phase, it includes waste management (Infection prevention and control)
Strengthening supervision capacity of the DHMTs. Supervisory checklist draft in place, management team working on the final supervisory checklist that will assist them during their supervisory visits in HCs.
Improving maternal care at the community. Orientation training of CORPS on MC, renovations of HCs and installation of generators in two model HCs in two 2 districts done.
Results of HC renovation. � Improved Water and Drainage systems, fence, gates, partitioning and
ceilings etc. Night duty in the two model HCs has improved due to operating generators installed by the project.
� Slides on training session and equipment handover were shown tomembers.
� Equipments included those purchased by JICA budget and HANDS, where HANDS provided training models, books, journals and registers to each district.
� Equipment distribution based on individual HC needs. � Water provided is tank water not piped. � Register printing was limited since DRH was in its final stages of
reviewing and standardizing the registers. � Madam Zoe is an essential training model for the two districts,
HANDS to include it in the models. � A comprehensive skills training for purposes of competency is
necessary after the orientation training. TOTs at divisional level should train CORPs using community orientation package.
� Participants during training session on full board booking to be provided with out of pocket (500/=), and that if the project cannot provide, the DMOH to source for funds else where for the participants allowances.
114
Appendix 6
� Project to continue its operations in the absence of experts and on their return, they will receive reports on equipment and commodity maintenance.
� Reflection of money spent by HANDS in the budget was necessary which is 100M although a 3o% budget cut was expected, since most of activities had been done.
Min 4/03/06 Plan of activities in the 3rd phase � HANDS promotion video was shown to members on maternal
services in Kisii, Kericho and other parts of the world and brief historical explanation on why JAPAN is working for SM in Kenya and other parts of the world given.
� Activities of 3rd phase were not mentioned due to anticipated budget cut by 30%. This would too result in having less HANDS technical staff.
� Although project was 3years,budget allocation was on yearly basis. � HANDS wished to continue working in Kenya after the project
term, and added that, often breaks and travels to Japan interfered with project operations. They called on MOH and GOK to negotiate for their continuous stay for the interest of the project, though it was clear that JAPAN Govt controlled their schedule in Kenya through JICA.
� Official project evaluation by JICA in cooperation with MOH will be done in Aug/Nov, 2006.
� There was need for discussions between MOH/JICA/HANDS on project consistence, expert’s breaks among other issues. Breaks cause wastage of time and resources. The frequent local staff highering and termination of their contracts had negative impact on the project, hence need to have them working in experts absence for the project continuity and sustainability.
� HANDS operation in Kenya would be possible after their project term ended only if they negotiated with GOK for registration licensing as an international NGO.
� DMOHS of Kisii and Kericho commented HANDS for the renovations, equipments and vehicles and added that health services had improved greatly. Communities were positive and supportive to the project. Although 2nd phase was short they promised to sustain the project during experts absence.
115
Appendix 6
� Availability of multipurpose vehicles made referral services effective, though there is need to strengthen communication by availing mobile phones and airtime to HC in charges.
� DMOHs were urged to ensure availability of functional kitchens, food and charcoal in HCs for mothers who seek delivery services.
� Construction of HANDS office in Kericho commenced in March, 06.JICA to contribute Kshs.300, 000/=towards the construction, in Kisii JICA will put up modern structures late this year to enable HANDS have a spacious office.
Min 4/03/06 AOB.� HANDS team to visit head of PPHS office before their departure to
Japan.� Project vehicles to be packed in Afya House compound while experts
are away. � There is need for project trends to be standardized since staff in the
two districts maybe transferred to other districts to offer similar services.
� HANDS requested DRH for official training proposal for district RH teams.
� Head PPHS thanked JICA/HANDS for their good work, and emphasized on community involvement with focus to reducing maternal mortality rates through offering preventive health services, rather than curative services and added that MOH would make follow up visits to facilities to assess utility. He hoped talks between HANDS and JAPAN govt will be done in goodtime to facilitate their early return.
� With no other business meeting ended at 11.30am.
Chairman…………………………………. Date…………………..
Secretary…………………………………. Date………………….
116

Appendix 6
5TH NATIONAL TECHNICAL WORKING COMMITTEE MEETING FOR MOH/JICA/HANDS SAFE MOTHERHOOD SAMOKIKE PROJECT ON 17TH
JULY 2006.
Members Present.
1. Dr J K Kibaru -Head DRH 2. Mr E Kinyangi -Programme Officer JICA 3. Dr E S Abunga -DMOH Kisii 4. Dr Kemboi C K -DMOH Kericho 5. Kiyomi Yamamoto -PC HANDS 6. Yumiko Kitagawa -MC Expert HANDS 8. Mamoru Shimamoto -PM HANDS 9. Daniel Sande -Programme Officer DRH MOH
Absent with apology Dr SK Sharrif HPPHS Mr. Kazuhiko Tokuhashi deputy resident Representative JICA Ms Yumiko Igarasshi Project Formulation Advisor JICA
Meeting started at 9.15am
Min 1/07/06 Opening Remarks.Welcome and introductory remarks by head-DRH
Min 2/07/06 Address from JICA DRR JICA Kenya office Mr. Kazuhiko Tokuhashi was unwell, while Ms Yumiko Igarashi was on leave. Mr. Kinyangi replaced Dr Willie Nyambati as JICA health representative.
Min 3/07/06 Introduction of new experts in the project New project members were introduced four long-term experts who were to stay during the project 3rd phase –Project Manager, Technical advisor on Maternal Care, Project coordinator for Kisii and Kericho. 5 short term experts were expected to the project-they were to go back to Japan before end of 3rd term.
Min 4/07/06 Review of previous activities in 2nd phase.Provision of equipments for maternal care to HCs Conducted SM training to service providers and community resource persons. Conducted DHMT supervision to HCs using checklist. Installation of generators to the two model HCs in Kisii and Kericho. Due to above activities, the number of deliveries in HCs had increased and clean water supply is adequate. Maternal emergencies are well addressed through improved communication and referral system.
117

Appendix 6
Two generators were purchased, although there was need for all HCs to have generators. For maintenance there is need to use other resources i.e. CDF and community involvement. The issue of solar use for power provision was raised, members felt it was important and needed to be discussed in subsequent meetings.
Min 5/07/06 Plan of activities in the 3rd phase 7/06 to 2/07 5 major activities to be undertaken.
� Upgrading MC in HCs through equipment maintenance, staff trainings, monitoring and evaluation activities and record keeping.
� Improving of management system in HCs � Strengthening supervision capacities of DHMTs � Improving MC in communities � Strengthening referral system
Nine trainings were to be carried out 3rd phase beginning with maternal care-2 week course in Essential Obstetric Care. Comments on trainings, -there is need to involve DHMT members in selection of participants in order to get the right staff and community members. Need to standardize the trainings by use of standardized training manuals. On essential obstetric training it was agreed that the DMOHs for the districts to provide funds for participants, out of pocket and facilitation fee for facilitators. This was to be discussed on 20th July 2006 in DPCC meeting in Kisii. HANDS wished to take four DHMT members for an exchange programme in Tanzania,-members discussed and it was agreed that HANDS was to meet all the costs involved.
Min 6/07/06 AOB There was need for HANDS experts to serve for longer period in the project. Construction of Kericho office was complete although the building had not dried up due to rains. Kisii office to be expanded in October 06, while JICA project in Kisii awaits design mission to give design report-this was expected in August 06. Mid term evaluation by Dr Handa to be done on 25-26 July 06, evaluation workshop to be held on 27-28 July 06 in Kericho.Evaluation will end in September 2006.MOH required early communication to enable participation in the evaluation exercise. MOH promised support to the project, HANDS urged to work closely with DMOHs to achieve better results. With no other issues arising members agreed that JPSC was to be held on 29/9/06 after projects’ midterm evaluation. Meeting ended 11am.
Chairman…………………………………………………Date……………………….
Secretary…………………………………………………Date………………………..
118

Appendix 6
6TH MEETING OF THE NATIONAL TECHNICAL WORKING COMMITTEE (NTWC) FOR THE MOH/JICA-HANDS SAFE MOTHERHOOD (SAMOKIKE) PROJECT
DATE: 26/02/2007
VENUE: DRH BOARDROOM
Members Present: Organization 1. Dr. J. Kibaru Head-DRH 2. Yumiko Igarashi JICA 3. Adangah Agisu MOH 4. Elijah Kinyangi JICA 5. Daniel Sande DRH/MOH 6. Dr. F. S. Abunga DMOH - Kisii 7. Dr. A. K. Rotich DMOH – Kericho 8. MS. Junko Kato HANDS 9. Kiyomi Yamamoto HANDS 10. Dr. Kitetu R.N MOH/HSRS 11. Yumiko Kitagawa HANDS 12. Akiko Matsumoto HANDS
Absent with apology Dr. S K Sharrif HPPHS Deputy Country Representative-JICA
Meeting started at 10.15am
Min 1/02/06 Opening remarks Welcome and introductory remarks by the head-DRH.She called for feedback of the activities in 3rd phase of the project from the experts.
Min 2/02/06 Address from JICA DRR JICA Kenya office Deputy Country Representative sent apology. Igarashi – feedback report on Midterm evaluation to be released soon.
Min 3/02/07 Review of Technical Activities in the 3rd Phase Summary of activities: 3rd phase Had several training i.e.
� Maternal Care � Health facility management � Training included health personnel and community members
Summary of other trainings
� Health Centre drug management- basic training on drug management � Health Information System improvement training-used new tools in the training
119

Appendix 6
� Facilitative supervision done, which targeted Health Centers I/C in collaboration with Engender Health.
Activities in 3rd Phase - 3 study tours
� HIS program study tour to Coast Province � Technical exchange program visit to Morogoro Health project (MHP) � Observation of the referral system – Kakamega PGH supported the study tour (DHMT
Kakamega discussed referral system)
Community Activity in 3rd Phase
� Joint meeting, community and targeted health center staff � Community meeting at targeted health centers-had 956 participants for community
activities� Generators provided, delivery beds replaced in Kabianga H/C
Comments
� DMOH Kisii - The slight reduction in number of clients was due to lack of staff to cover night duty. With new staff employed the number is expected to rise.
� DMOH Kericho – Same as above, staff shortage resulted in reduction in number of clients.
� Dr. Kibaru –being a project district, skilled care is required to scale up the number of deliveries.
� New MOH strategy is to make use of the retired/unemployed midwives working in the villages, for them to give skilled delivery care-Can deliver women at home then bring them to post natal for care.
� Record keeping training will enable staff to report clearly
� Most women still make use of TBA but the retired midwives approach will improve delivery services as FP and immunization have picked up
� HMIS – partners to print standardized tools/registers for facilities. (DMOHs to facilitate the process)
� Training – as MOHs we need to use facilitators from the ministry for the purpose of standardizing the trainings, therefore provincial TOTs should be used in trainings.
� Study tours –all members were asked to submit their reports
120

Appendix 6
Min 4/02/07 Plan of Activities for the 4th Phase
� Need to conduct MC training and need for the staff to know how to care for mothers especially attitude – customer care
� Use of incentives i.e. provision of baby shawls to cover baby and cover materials for mothers.
� Focus on improving the referral system – will provide each health center with phone to enable them call the district hospitals and support referral system.
Comments – Dr. Kibaru
� Community dialogue for the purpose of scaling up the services – use of community RH package
� Need to have a broad approach and involve the men
� Community RH package to be applied in Kisii and Kericho
� Community health extension workers are part of the strategy and are being trained
� On sustainability of trainings offered to health workers, facilitators from the districts should use participants’ performance sheet which will be evaluated in the subsequent trainings.
� Need for Clinical Training Skills for the purpose of teaching. CTS for the district TOTs to be considered by HANDS.
� Mr.Kinyangi – elaborated on referral, roads status -need to have collaboration in terms of road repair – during community RH forums, issues of relationship between pregnant mothers and good roads should come up - advocacy to be done.
� Kisii referral improved – standby driver available
� Kericho- some parts not accessible arrangements in place to facilitate easy referral system.
� Need to have standby ambulances in the districts to facilitate easy referral.
� Need to improve capacity of the newly employed staff to enable them be able to run the health centers
� Tools to be printed and distributed to facilities in the project districts.
� Provision of drug management manuals to enable non-trained staff read and apply.
121
Appendix 6
Min 5/02/07 AOB
� Changes to be made on Project Design Matrix and indicators. � Need to focus on the MDGs to meet our objectives. � Baseline survey is required in Gucha and Nyamira districts and there is need to
develop TOR tools to support the selection of these districts. The purpose of the survey is to assess future expansion of the project.
� Results of final project evaluation report are expected.
Previous Meeting
� Counter part funds required for the purpose of supporting facilitative supervision activities in the districts (JICA to facilitate).
� Mid-term evaluation report required in the next meeting, it will enable DMOH/HANDS evaluate project progress.
� Need for a stakeholders forum to have feedback of mid-term report.
Sign…………………………. Date…………………………
Chairman.
Sign………………………….. Date………………………….
Secretary
122

Appendix 6
7TH NATIONAL TECHNICAL WORKING COMMITTEE MEETING FOR MOH/JICA/HANDS SAFE MOTHERHOOD (SAMOKIKE) PROJECT ON 17TH JULY 2007
Members Present1. Dr. S.K Sharif -Head PPHS 2. Dr. J. Kibaru -Head DRH 3. Ikuko Shimizu -HANDS 4. Tamayo Haraguchi -HANDS 5. Yumiko Kitagawa -HANDS 6. Dr. Ambrose K Rotich -DMoH Kericho 7. Ms.Yumiko Igarashi -Project formulation advisor JICA8. Dr. E. S. Abunga -DMoH Kisii 9. Mr. Daniel Sande -DRH MoH 10. Mr. Elijah Kinyangi -JICA SPO 11. Professor Handa Yujiro -JICA 12. Nancy Chelule -MOH-PMO-RVP
Absent with Apology Mr. Kazuhiko Tokuhashi Deputy Resident Representative JICA
Meeting started at 10.00 a.m.
Min 1/07/07 Welcome Remarks Welcome and introductory remarks by Head PPHS.
Min 2/07/07 Address by DRR JICA. Apologies from JICA country representative.
� Activities started in the 4th phase � JICA to give a report of mid term evaluation
Terminal evaluation of the project will be done in October 2007.
Min 3/07/07 Results of the Mid Term Evaluation by JICA Professor Handa a Japanese expert, and a member of evaluation team gave summary of the mid term evaluation report to members, which he classified as typical semi internal evaluation. In evaluation, 5 evaluation criteria were used which included relevance, effectiveness, efficiency, impact and sustainability. He looked at the 6 project components where he explained that the sixth component was broken down in smaller units. As much as evaluation was to route out positive issues, the team came up with various recommendations, which included;
� Monitoring of the justified activities � Referral activities to be looked into through proper decision making in referral of
cases� Capacity strengthening of health workers. � Decongestion of district hospitals through transfer of health services to health
centers.
123
Appendix 6
� Introduction of work empowerment project in health centers by use of 5S1K i.e. Sorting, Setting, Shining, and Standardizing, Sustain and Keep it up, to improve quality of services at the health centers.
� Maintenance of project managers for longer period � Staffing more qualified staff to health centers � Managerial skills to be improved through 5S1K� Advocacy and support supervision by DHMT should be regular especially to health
centers far away from accessible roads.
Lessons Learnt during mid term evaluation. � Utilization of the CBOs, improving status of health centers and working with
district hospitals would improve maternal health services � That the districts work closely with community people � That the community was cooperative to the evaluation team who were able to
collect information from the community.� Signing of the evaluation report done by JICA, and Dr. Kibaru
Min 4/07/07 – PDM (change amendments) Chief Advisor, HANDS explained to members the meaning of SAMOKIKE project, and added that it was a 3-year project that started in March 2005. She explained activities of 1st and 2nd year and emphasized that activities of 2007 were the focus. PDM Amendment She explained that PDM is a tool used for project management, which was revised in Feb 2007.Refer at annex 3.1
� Members looked at the amendments made to the PDM document. This helped in understanding clearly the project targets and achievements.
Dr. Kibaru told the members that it was important to have measurable indicators. JICA was requested to print the new revised registers, which should be disseminatedonce they are available in the two districts, Dr. Kibaru was requested to send a request letter to JICA for printing to be done.
� There is need to address issues revised in the PDM, – including change of indicators to be specific. Time frame for finalization of the document was given a deadline of July 2007, of which confirmation of the PDM changes and minutes of the meeting was to be signed, followed by a written letter to PS for signature, for approval of the PDM document.
Min 5/07/07 Plan of activities for 4th phase Divided activities into 3 categories
1. Capacity building2. Community mobilization3. Information sharing and coordination among MOH/JICA, HANDS, PMOH, MOH and
health centers.
124
Appendix 6
- Went through the yearly operational schedule-activities to go up to mid March, 2008
- Final evaluation of project will be done in October, 2007 - Final evaluation should be conducted 6½ months before the project
ends to allow any changes to be incorporated. - 3 years after the end of the project, impact assessment will be done
Min 6/07/07 AOB
- Adoption of the mid term evaluation report by JICA, HANDS and MOH (PS)
- Final evaluation to be conducted in early October, 2007 through a joint team
- TOR to be made following PDM change.
Min 7/07/07 Closing Remarks DMOH Kisii said there was improvement in hospital deliveries and referrals in targetedhealth centers. DMOH Kericho said project helped in achieving some of the indicators i.e. increased deliveries in health facilities, he added that project vehicle had an accident and was under repair but referral still continues with another vehicle.
The head-DRH (Dr. Kibaru) said maternal mortality rate cannot be reduced unless there is skilled health care provision and added that supervision will be done in the province soon.
PNO R/Valley � Thanked HANDS for the work they are doing in Kisii/Kericho.� To continue working together to improve morbidity and mortality � Referral system was impressive and should be rolled out to other facilities � Possibilities of extending the project from HC to dispensaries since they are near
communities. The head DPPHS (Dr. Sharif), thanked professor Handa and evaluation team for the mid term evaluation and promised to look at it and address issues coming up especially those under control of the DHMT.
� With no other business meeting ended at 12 pm.
Chairman…………………………………. Date…………………..
Secretary…………………………………. Date………………….
125


















