FINAL BURN CD-TYPHOID FEVA

of 68
Transcript of FINAL BURN CD-TYPHOID FEVA
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
1/68
I. Introduction
Typhoid fever was not well understood in the ancient world, probably because its
symptoms are not primarily diarrheal, but rather systemic and non-specific. It was only inthe mid-19th century that physicians began to distinguish it from typhus and malaria.
Typhoid or enteric fever is an ancient disease, which has afflicted mankind since human
populations grew large enough to contaminate their water and food supplies. Practicality
has always been an attribute of the typical Filipino. It is a trait that has been embedded
into the very fabric of our lives as we bid to make the best out of what we have. We
exploit and utilize our resources to the maximum possible extent in an effort to limit
whatever goes to waste as a result of our actions. Kyle is one example of a very practical
person. Everyday before going to school in his hometown of Malugong Tboli, South
Cotabato, he chooses to make the nearby river useful and chooses to bathe in it rather
than use the water that his father had fetched from the community reservoir.
Unfortunately for him, other practical persons (and even animals) also exhibit
practicality by using the river as a site for disposing bodily waste, turning the natural
body of water into a medium for spread of infection and disease.
One week prior to admission, Kyle began to have persistent fever then after few
days he started to vomit everything that he eats. Initially, they thought that it was caused
by mosquito bite. Unbeknownst to him and his family, Kevin had contracted an infection
from his daily swimming sessions in the river. He was taken to the Davao Medical Center
on November 24, 2007 when he was no longer able to tolerate the symptoms especially
the vomiting episodes. After undergoing laboratory tests and diagnostic exams, Kevin
was diagnosed of having Typhoid fever.
In the United States alone, about 400 cases of typhoid fever occur each year, and
70% of these are acquired while traveling internationally. Typhoid fever is still commonin the developing world, where it affects about 12.5 million persons each year. In the
Philippines, the Department of Health estimated that in the year 2002 alone, there were
13,661 cases of typhoid and paratyphoid fever in the country, of which 990 were reported
from Region11. Typhoid is now regarded as a disease of history by many people living in
developed countries. However, WHO estimates that globally there are still more than 17
1
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
2/68
million typhoid cases annually and that these infections areassociated with about 600 000
deaths.
Our group was able to handle the case of Kyle when we were assigned for duty at
the Pediatric Ward of the Davao Medical Center on November 9, 2007. After we were
given consent by his parents, we decided to take Kevins case as a subject for study in
order to expand our knowledge regarding his disease and be able to collect additional
data that we deem necessary for us to progress in our quest to become effective nurses in
the future.
2
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
3/68
II. OBJECTIVES
-During our four weeks of exposure in the clinical area, from November 15-
December 1, 2007, the group will be able to achieve the following:
General Objectives:
1. To be able to choose a case study for our case presentation.
2. To have a case study related to our concepts in lecture regarding
communicable diseases and oxygenation.
3. To be able to apply our learnings from our lectures to our case study.4. To learn further regarding on our concepts in lecture.
Specific Objectives:
1. To gather enough and credible data for our case study and be
able to prevent it.
2. To be able to establish rapport to our patient and his family in
order to gain their cooperation for the interview and therapeutic
processes.
3. To be able to know our patients Family background and Health
history in order to trace past and present health condition.
4. To be able to assess our patients developmental stages in life
into three theories namely: Havighurts, Freud, Erikson, or
Piaget.
5. To be able to define Typhoid fever along with the patients
complete diagnosis in at least three sources from any medical
surgical textbooks.
6. To be able to assess our patient physically and cephalocaudally.
3
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
4/68
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
5/68
III. PATIENTS DATAPatients code name: Kyle
Age: 8 years old Nationality: Filipino
Civil status: Single
Occupation: Student
Ward: Pedia
Room: IMCU
Bed no. : 4
Religion: Roman Catholic
Educal attainment: grade 1
Date of admission: November 24, 2007
V/S on admission:
T: 39. 8 C CR: 145 bpm
RR: 34 cpm BP: 90/70 mmhg
Chief Complaints: Fever
Admitting diagnosis: Enteric Fever t/c Typhoid fever
Final diagnosis: Thyphoid fever r/o intestinal perforation
Source of information: Patients Chart
5
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
6/68
IV. HEALTH HISTORY
Family Health history
There is no history of any diseases in the family of Kyles Mother, the Gaway clan.
However, in the paternal line, a history of Heart diseases and Hypertension is present.
Marilou, his fathers eldest sibling and Robert Nelson, the fifth of the six siblings has
hypertension and heart disease while Anabelle, the second sibling and Gladys, the
youngest among has hypertension. Meanwhile, Wilfredo, Kyles father did not acquire
any from the two disease nor have any disease.
Effects and expectations of the illness to self and famil y
Of course, the first effect of Kyle being ill is that both of his parents and as well as
his lola and younger sibling, of which he is the eldest, they worry so much of Kyle. The
effect was emotional. His father became so worried and problematic. He said that he
cant sleep very well because he is too concerned for his child. Also, there was a big
effect on financial, the family needs to spend a lot of money for the medications which is
so expensive but they are so thankful that there is the Lingap which helped them in
their hospital finances. Her mother is also worried that she would always call from Jeda
for Kyle. Also Kyles brothers misses him so much and so is he that he will always cry
and wants to see his siblings who are in South Cotabato. Kyle is a grade 1 student from
Malugong Elementary school. There was a big effect on his studies because he has been
absent for about 3 weeks but with the permission from his teacher because Kyle is a very
diligent student. Also, because of the sickness Kyle sufferes both mental, physiological
and emotional. He wasnt able to do his usual routines at home like playing with his
playmates, watching TV and swimming in the pool when he was still not sick. These are
very important for a child of 8 years old.
6
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
7/68
The Family expects a lot that Kyle would recover from the illness and that he
would go back to his old strength and go to school and do his usual routines. The Family
expects that they will become more careful in their diets or in the food hygiene in order to
prevent having the disease because hospitalization is expensive.
Past Health History
a. History of past illness
Kyle havent had any kind of diseases or illnesses since he was a
baby until this year. The only illnesses that he will have are just mild fever,
coughs and colds but nothing more severe.
b. History of present illness
Kyles lifestyle is so active. Before going to school, he takes a bathin the Malugong River which is near their house. Then, as a child, he loves to eat
junk foods like Mr. chips and drink sodas. He has a good academic performance
in school. As what his father says he would sometimes be the leader in some
schoolworks. When he arrives from school he plays with his playmates from the
neighborhood. If not playing outside and not swimming in the river with friends
and especially if its weekend he watches cartoons from morning till evening. His
usual diet are vegetables but eats slowly and his favorite foods are pork sausage,
salted foods and okras. He always skips breakfast especially during schooldays
because he wokes up late in the morning so there are no time for it and then he
usually have a dinner heavier than his lunch.
7
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
8/68
On the month of November Kyle got sick. He had a fever for eight
day. Usually the fevers are high and is lowered by taking paracetamol which
offered a temporary relief then followed by loss of appetite. There are no medical
consultation made. There was an onset of soft and watery stools for five days but
still no consultation done and no meds given. The patient had anorexia and will
vomit everything that he will swallow along with his fever and diarrhea and this
prompted his father to consult medical help at Davao Medical Center.
8
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
9/68
V. DEVELOPMENTAL DATA
Moral Development Theory (Lawrence Kohlberg)
Moral development, a complex process not fulkly understood, involves learning
what ought to be and what ought to be done. It is more than imprinting that parents rule
and virtues or values of children. The term moral means relating to right and wrong.
The terms Morality, Moral behavior, and Moral Development nedd to be distinguished
from each other. Morality refers to the requirements necessary for people to live in a
societry; Moral behavior is the way a person perceives those requirements and responds
to them; Moral development is the pattern of change in moral behavior with age.
At the meantime, the children lives with their lola at Malugong and their Father
lives their temporarily. Kyle, as a child perceives punishment as the sign that he dis
something wrong or what hes doing is wrong. He avoids punishment and consequences
which are either set by his father or authorities and so he does things that he thinks are
right by which he cant be punished. He follows what his Lola, mother and Father wants
him to do as having good grades at school and being a good and unbully child. Also, Hedoes what he wants to do or what interest him which tells that what his doing is actually
right(at his own view of what is right). Like he goes to swimming in the river, play with
playmates and watch TV a lot. This is his routine and what he likes to do and also his
father doesnt prohibit him from doing so.
9
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
10/68
Psychosocial Development (Erik Erikson)
This theory refers to the development of personality. Personality is a complex that
is difficult to define. It can be considered as the outward (interpersonal) expression of theinner(intrapersonal) self. It compasses a persons temperament, feeling, character traits,
independence, self-esteem, self-concept, behavior, ability to interact with others and
ability to adapt to life changes.
The patient is an eight-years old child. He belongs in the stage of Industry vs.
Inferiority. Industry here refers to purposeful or meaningful activity. It's the development
of competence and skills, and a confidence to use a 'method', and is a crucial aspect of
school years experience. Erikson described this stage as a sort of 'entrance to life'. A child
who experiences the satisfaction of achievement - of anything positive - will move
towards successful negotiation of this crisis stage. A child who experiences failure at
school tasks and work, or worse still who is denied the opportunity to discover and
develop their own capabilities and strengths and unique potential, quite naturally is prone
to feeling inferior and useless. Engaging with others and using tools or technology are
also important aspects of this stage. It is like a rehearsal for being productive and being
valued at work in later life. Inferiority is feeling useless; unable to contribute, unable tocooperate or work in a team to create something, with the low self-esteem that
accompanies such feelings
Kyle is a productive student at school and an active child in the village. He has a
lot of friends and plays with them after school or on weekend when it does not interrupt
in his school works. He enjoys playing and swimming with his friends. He doesnt miss
his schooldays and he doesnt want to be absent in school. After playing and watching TV
during schooldays, he would now study his lessons for school. Kyle knows when to do
things and has his method of doing it by setting his priorities and what needs to be
attended first and whats more important. He is confident in his self as evidenced by
being a good leader at school. He also have a positive comments from his teachers.
10
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
11/68
Cognitive Theory (Jean Piaget)
This theory refers to the manner in which people learn to think, reason,
and use language. It involves a persons intelligence, perceptual ability, and ability to process information. Cognitive development represents a progression of mental abilities
from illogical to logical thinking, from simple to complex problem solving, and from
understanding concrete iseas to understand abstract concepts.
Our Patient, Kyle is on Concrete Stage. During this stage, accommodation
increases. The child develops an ability to think abstractly and to make rational
judgements about concrete or observable phenomena, which in the past he needed to
manipulate physically to understand. In teaching this child, giving him the opportunity to
ask questions and to explain things back to you allows him to mentally manipulate
information.
Our patient is a grade 1 student from Malugong Elementary highschool in
South Cotabato. His favorite subjects are Math and Filipino. He likes to read short stories
like Fables and Filipino folklores.
He is practical. He thinks for what is important and what could he done.He follows his therapeutic regime i.e. NPO in which after knowing, he does not insists on
eating or drinking because it was the instruction. He knows how to reason and answers
question concretely and coherently. He follows our instructions or what we tells him to
do like, when he was lying on bed, we asked him to sit in order for us to auscultate his
lungs eventhough he has body malaise. We also observed that he knows how to reason
for things while were conversing with him.
As what we observed, Kyle is a smart boy. He knows what he should do
and what to say and reasons. At his age, He could comprehend his present condition and
follows instructions given to him by the medical staffs.
11
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
12/68
DEFINITION OF COMPLETE DIAGNOSIS
Typhoid Fever r/o Intestinal Perforation
Typhoid Fever
Typhoid fever is a bacterial infection of the intestinal tract and occasionally the
bloodstream. It is an uncommon disease with only 30-50 cases occurring in New York
each year. Most of the cases are acquired during foreign travel to underdeveloped
countries. The germ that causes typhoid is a unique human strain of Salmonella calledSalmonella typhi . Outbreaks are rare
Source:
http://www.health.state.ny.us/diseases/communicable/typhoid_fever/fact_sheet.htm
An acute illness associated with fever caused by the Salmonellae Typhi bacteria. The
bacteria is deposited in water or food by a human carrier, and is then spread to other
people in the area. The incidence of the illness in the United States has markedly
decreased since the early 1900's. This improvement is the result of improved
environmental sanitation. Mexico and South America are the most common areas for
U.S. citizens to contract typhoid fever. India, Pakistan and Egypt are also known high risk
areas for developing this disease.
Source: http://www.medicinenet.com/typhoid_fever/article.htm
Typhoid fever is a potentially life-threatening illness that is caused by the bacteria
Salmonella typhi (S. typhi) . Persons with typhoid fever carry the bacteria in their bloodstream
and intestinal tract and can spread the infection directly to other people by contaminating
12
http://www.health.state.ny.us/diseases/communicable/typhoid_fever/fact_sheet.htmhttp://www.medicinenet.com/typhoid_fever/article.htmhttp://www.health.state.ny.us/diseases/communicable/typhoid_fever/fact_sheet.htmhttp://www.medicinenet.com/typhoid_fever/article.htm -
8/14/2019 FINAL BURN CD-TYPHOID FEVA
13/68
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
14/68
This surgical emergency involves rupture of the wall of the intestine . intestinal
perforation results in severe abdominal pain intensified by movement . Later symptoms
include fever and chills.
Source: http://www.medhelp.org/HealthTopics/H.html
14
http://www.bio-medicine.org/Medicine-Dictionary/emergency/http://www.bio-medicine.org/Medicine-Dictionary/rupture/http://www.bio-medicine.org/Medicine-Dictionary/intestine/http://www.bio-medicine.org/Medicine-Dictionary/abdominal_pain/http://www.bio-medicine.org/Medicine-Dictionary/movement/http://www.bio-medicine.org/Medicine-Dictionary/fever/http://www.bio-medicine.org/Medicine-Dictionary/chills/http://www.medhelp.org/HealthTopics/H.htmlhttp://www.bio-medicine.org/Medicine-Dictionary/emergency/http://www.bio-medicine.org/Medicine-Dictionary/rupture/http://www.bio-medicine.org/Medicine-Dictionary/intestine/http://www.bio-medicine.org/Medicine-Dictionary/abdominal_pain/http://www.bio-medicine.org/Medicine-Dictionary/movement/http://www.bio-medicine.org/Medicine-Dictionary/fever/http://www.bio-medicine.org/Medicine-Dictionary/chills/http://www.medhelp.org/HealthTopics/H.html -
8/14/2019 FINAL BURN CD-TYPHOID FEVA
15/68
VII. PHYSICAL ASSESSMENT
1. Vital signs
BP: 110/90 (sitting)
TEMP: 39. 7 C
RR: 42 bpm (shallow and fast)
PR: 112 bpm
2. General Survey
Weight remains the same since admission, 17 kg. The head
circumference is . He appears to have signs of distress, pain and anxietyand talks limitedly. He is conscious, alert, coherent and oriented. He is
ectomorphic, well developed and looks according to age. He is poorly
nourished as evidenced by very thin body structure, dry skin and reported
that he only eats a little and his usual diet is vegetables but his favorite is
pork sausage and salted foods. However at the onset of his symptoms, he
started to loss his appetite. His emotional state is that he appears to be
worried, restless and has grimaced face and also cries due to
homesickness.
3. Skin
Texture of skin is smooth and is hot to touch. Turgor is good. Scars
and allergies are noted on both lower legs. Pitting edema is noted on
both arms and feet. Pallor is present on palms and soles of feet.
4. Head
Configuration of the head is normocephalic with fontanels
closed and no masses or lesions are present. Facial movements are
symmetrical. Hair is evenly distributed and scalp is clean.
15
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
16/68
5. Eyes
Lids are symmetrical but swelling. Edema is evident on
both periorbital regions but more severe on the right side. No lesions.
Conjunctiva is pale in color and sclera is anicteric but light red in color.
Visual acuity is glossy normal and peripheral vision is intact and full.
6. Ears
Has normoset of external pinnae and are symmetrical.
Hearing is symmetrical with cerumen on the external canal but without
discharges and foul smell.
7. Nose
Septum is midline. No discharges, no lesions and masses. Both
are patent.
8. Mouth
Lips are cracked and dry with presence of bleeding lesions.
Mucosa and gums are pale in color and tongue is at midline and intact speech.
Cavities are present on molars and premolars on both upper and lower teeth.
9. Pharynx
Uvula is at midline with mucusa pinkish in color. Tonsils are
not inflamed.
10. Neck
Trachea is at midline. No tenderness at cervical lymph nodes
upon palpation and thyroid is not enlarged.
16
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
17/68
11. Chest and Lungs
Breathing is irregular and is having shallow and fast breathing
with use of accessory muscles. Lung expansion is symmetrical with no adventitious
lung sounds upon auscultation.
12. Heart
Palpitation is present. Bleeding tendencies for lesions on lips and
gastrointestinal tract. There is a presence of a heart sound upon palpation.
13. Breast and axillae
Both breast are equal in shape and symmetrical. Surface is smooth and
no dimpling, edema or retractions. No masses and tenderness.
14. Abdomen
By inspection, there are presence of visible veins but no lesions and
scars. Abdomen is globular in configuration with absent bowel sounds upon
auscultation. Tenderness is evident during palpation with presence of guarding
behavior. Abdominal pain is felt on the left hypochondriac region.
15. Back and extremities
Peripheral pulses are symmetrical. nail beds pale in color. ROM full
and symmetrical and muscle tone is equally strong and symmetrical muscle size with
coordinated gait.
17
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
18/68
VIII. ANATOMY PHYSIOLOGY
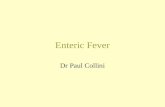
The human digestive system is a complex series of organs and glands that processes food.
In order to use the food we eat, our body has to break the food down into smaller
molecules that it can process; it also has to excrete waste.
Most of the digestive organs (like the stomach and intestines) are tube-like and contain
the food as it makes its way through the body. The digestive system is essentially a long,
twisting tube that runs from the mouth to the anus, plus a few other organs (like the liver
and pancreas) that produce or store digestive chemicals.
TheDigestiveProcess :
The start of the process - the mouth: The digestive process begins in the mouth. Food
is partly broken down by the process of chewing and by the chemical action of salivary
enzymes (these enzymes are produced by the salivary glands and break down starches
into smaller molecules).
On the way to the stomach: the esophagus - After being chewed and swallowed, the
food enters the esophagus. The esophagus is a long tube that runs from the mouth to the
stomach. It uses rhythmic, wave-like muscle movements (called peristalsis) to force food
from the throat into the stomach. This muscle movement gives us the ability to eat or
drink even when we're upside-down.
Human Digestive System
18
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
19/68
In the stomach - The stomach is a large, sack-like organ that churns the food and bathes
it in a very strong acid (gastric acid). Food in the stomach that is partly digested and
mixed with stomach acids is called chyme.
In the small intestine - After being in the stomach, food enters the duodenum, the first
part of the small intestine. It then enters the jejunum and then the ileum (the final part of
the small intestine). In the small intestine, bile (produced in the liver and stored in the gall
bladder), pancreatic enzymes, and other digestive enzymes produced by the inner wall of
the small intestine help in the breakdown of food.
In the large intestine - After passing through the small intestine, food passes into the
large intestine. In the large intestine, some of the water and electrolytes (chemicals like
sodium) are removed from the food. Many microbes (bacteria like Bacteroides ,
Lactobacillus acidophilus , Escherichia coli , and Klebsiella ) in the large intestine help in
the digestion process. The first part of the large intestine is called the cecum (the
appendix is connected to the cecum). Food then travels upward in the ascending colon.
The food travels across the abdomen in the transverse colon, goes back down the other
side of the body in the descending colon, and then through the sigmoid colon.
The end of the process - Solid waste is then stored in the rectum until it is excreted viathe anus.
Digestive System Glossary :
anus - the opening at the end of the digestive system from which feces (waste) exits the
body.
appendix - a small sac located on the cecum.
ascending colon - the part of the large intestine that run upwards; it is located after the
cecum.bile - a digestive chemical that is produced in the liver, stored in the gall bladder, and
secreted into the small intestine.
cecum - the first part of the large intestine; the appendix is connected to the cecum.
chyme - food in the stomach that is partly digested and mixed with stomach acids.
19
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
20/68
Chyme goes on to the small intestine for further digestion.
descending colon - the part of the large intestine that run downwards after the transverse
colon and before the sigmoid colon.
duodenum - the first part of the small intestine; it is C-shaped and runs from the stomach
to the jejunum.
epiglottis - the flap at the back of the tongue that keeps chewed food from going down
the windpipe to the lungs . When you swallow, the epiglottis automatically closes. When
you breathe, the epiglottis opens so that air can go in and out of the windpipe.
esophagus - the long tube between the mouth and the stomach. It uses rhythmic muscle
movements (called peristalsis) to force food from the throat into the stomach.
gall bladder - a small, sac-like organ located by the duodenum. It stores and releases bile
(a digestive chemical which is produced in the liver) into the small intestine.
ileum - the last part of the small intestine before the large intestine begins.
jejunum - the long, coiled mid-section of the small intestine; it is between the duodenum
and the ileum.
liver - a large organ located above and in front of the stomach. It filters toxins from the
blood, and makes bile (which breaks down fats) and some blood proteins.
mouth - the first part of the digestive system, where food enters the body. Chewing and
salivary enzymes in the mouth are the beginning of the digestive process (breaking down
the food).
pancreas - an enzyme-producing gland located below the stomach and above the
intestines. Enzymes from the pancreas help in the digestion of carbohydrates, fats and
proteins in the small intestine.
peristalsis - rhythmic muscle movements that force food in the esophagus from the throat
into the stomach. Peristalsis is involuntary - you cannot control it. It is also what allows
you to eat and drink while upside-down.
rectum - the lower part of the large intestine, where feces are stored before they are
excreted.
salivary glands - glands located in the mouth that produce saliva. Saliva contains
enzymes that break down carbohydrates (starch) into smaller molecules.
sigmoid colon - the part of the large intestine between the descending colon and the
20
http://www.enchantedlearning.com/subjects/anatomy/lungs/label/http://www.enchantedlearning.com/subjects/anatomy/lungs/label/http://www.enchantedlearning.com/subjects/anatomy/lungs/label/ -
8/14/2019 FINAL BURN CD-TYPHOID FEVA
21/68
rectum.
stomach - a sack-like, muscular organ that is attached to the esophagus. Both chemical
and mechanical digestion takes place in the stomach. When food enters the stomach, it is
churned in a bath of acids and enzymes.
transverse colon - the part of the large intestine that runs horizontally across the
abdomen.
Functions of the Digestive System
The digestive system includes the digestive tract and its
accessory organs, which process food into molecules that can
be absorbed and utilized by the cells of the body. Food is
broken down, bit by bit, until the molecules are small enough
to be absorbed and the waste products are eliminated. The
digestive tract, also called the alimentary canal or gastrointestinal (GI) tract, consists of a
long continuous tube that extends from the mouth to the anus. It includes the mouth,
pharynx, esophagus, stomach, small intestine, and large intestine. The tongue and teeth
are accessory structures located in the mouth. The salivary glands, liver, gallbladder, and pancreas are major accessory organs that have a role in digestion. These organs secrete
fluids into the digestive tract.
Food undergoes three types of processes in the body:
Digestion
Absorption
Elimination
Digestion and absorption occur in the digestive tract. After the nutrients are absorbed,
they are available to all cells in the body and are utilized by the body cells in metabolism.
21
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
22/68
The digestive system prepares nutrients for utilization by body cells through six
activities, or functions.
Ingestion . The first activity of the digestive system is to take in food through the mouth.
This process, called ingestion, has to take place before anything else can happen.
Mechanical Digestion . The large pieces of food that are ingested have to be broken into
smaller particles that can be acted upon by various enzymes . This is mechanical
digestion, which begins in the mouth with chewing or mastication and continues with
churning and mixing actions in the stomach.
Chemical Digestion The complex
molecules of carbohydrates, proteins, and
fats are transformed by chemical digestion
into smaller molecules that can be absorbed
and utilized by the cells. Chemical
digestion, through a process called
hydrolysis, uses water and digestive
enzymes to break down the complex
molecules. Digestive enzymes speed up thehydrolysis process, which is otherwise very
slow.
Movements . After ingestion and mastication, the food particles move from the mouth
into the pharynx, then into the esophagus. This movement is deglutition, or swallowing.
Mixing movements occur in the stomach as a result of smooth muscle contraction. These
repetitive contractions usually occur in small segments of the digestive tract and mix the
food particles with enzymes and other fluids. The movements that propel the food
particles through the digestive tract are called peristalsis. These are rhythmic waves of
contractions that move the food particles through the various regions in which
mechanical and chemical digestion takes place.
22
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
23/68
Absorption . The simple molecules that result from chemical digestion pass through cell
membranes of the lining in the small intestine into the blood or lymph capillaries. This
process is called absorption .
Elimination . The food molecules that cannot be digested or absorbed need to be
eliminated from the body. The removal of indigestible wastes through the anus, in the
form of feces, is defecation or elimination.
General Structure of the Digestive System
The long continuous tube that is the digestive tract is about 9 meters in length. It opens to
the outside at both ends, through the mouth at one end and through the anus at the other.
Although there are variations in each region, the basic structure of the wall is the same
throughout the entire length of the tube.
The wall of the digestive tract has four layers or tunics:
Mucosa
Submucosa
Muscular layer
Serous layer or serosa
The mucosa, or mucous membrane layer, is the innermost tunic of the wall. It lines the
lumen of the digestive tract. The mucosa consists of epithelium, an underlying loose
connective tissue layer called lamina propria , and a thin layer of smooth muscle called
the muscularis mucosa. In certain regions, the mucosa develops folds that increase the
surface area. Certain cells in the mucosa secrete mucus, digestive enzymes, and
hormones. Ducts from other glands pass through the mucosa to the lumen. In the mouth
and anus, where thickness for protection against abrasion is needed, the epithelium is
stratified squamous tissue. The stomach and intestines have a thin simple columnar
epithelial layer for secretion and absorption.
23
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
24/68
The submucosa is a thick layer of loose connective tissue that surrounds the mucosa. This
layer also contains blood vessels, lymphatic vessels, and nerves. Glands may be
embedded in this layer.
The smooth muscle responsible for movements of the digestive tract is arranged in two
layers, an inner circular layer and an outer longitudinal layer. The myenteric plexus is
between the two muscle layers.
Above the diaphragm , the outermost layer of the digestive tract is a connective tissue
called adventitia. Below the diaphragm, it is called serosa.
Organs of the Digestive System
At its simplest, the digestive system is a tube running from mouth to anus. Its chief goal
is to break down huge macromolecules (proteins, fats and starch), which cannot be
absorbed intact, into smaller molecules (amino acids, fatty acids and glucose) that can be
absorbed across the wall of the tube, and into the circulatory system for dissemination
throughout the body.
24
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
25/68
Regions of the digestive system can be divided into two main parts: the alimentary tract
and accessory organs. The alimentary tract of the digestive system is composed of the
mouth, pharynx, esophagus, stomach, small and large intestines, rectum and anus.
Associated with the alimentary tract are the following accessory organs: salivary glands,
liver, gallbladder, and pancreas.
Mouth
he mouth, or oral cavity, is the first part of the digestive tract. It is
dapted to receive food by ingestion, break it into small particles
y mastication, and mix it with saliva. The lips, cheeks, and palate
orm the boundaries. The oral cavity contains the teeth and tongue
nd receives the secretions from the salivary glands.
Lips and Cheeks
The lips and cheeks help hold food in the mouth and keep it in place for chewing. They
are also used in the formation of words for speech. The lips contain numerous sensory
receptors that are useful for judging the temperature and texture of foods.
Palate
The palate is the roof of the oral cavity. It separates the oral cavity from the nasal cavity.
The anterior portion, the hard palate, is supported by bone. The posterior portion, the soft
palate, is skeletal muscle and connective tissue. Posteriorly, the soft palate ends in a
25
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
26/68
projection called the uvula. During swallowing, the soft palate and uvula move upward to
direct food away from the nasal cavity and into the oropharynx.
Tongue
The tongue manipulates food in the mouth and is used in speech. The surface is covered
with papillae that provide friction and contain the taste buds.
Teeth
A complete set of deciduous (primary) teeth contains 20 teeth. There are 32 teeth in a
complete permanent (secondary) set. The shape of each tooth type corresponds to the way
it handles food.
Pharynx and Esophagus
Pharynx
The pharynx is a fibromuscular passageway that connects the nasal and oral cavities to
the larynx and esophagus. It serves both the respiratory and digestive systems as a
channel for air and food. The upper region, the nasopharynx, is posterior to the nasal
cavity. It contains the pharyngeal tonsils, or adenoids, functions as a passageway for air,
and has no function in the digestive system. The middle region posterior to the oral cavity
is the oropharynx. This is the first region food enters when it is swallowed. The opening
from the oral cavity into the oropharynx is called the fauces. Masses of lymphoid tissue,
the palatine tonsils, are near the fauces. The lower region, posterior to the larynx, is the
laryngopharynx, or hypopharynx. The laryngopharynx opens into both the esophagus and
the larynx.
26
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
27/68
Food is forced into the pharynx by the tongue.
When food reaches the opening, sensory receptors
around the fauces respond and initiate an
involuntary swallowing reflex. This reflex action
has several parts. The uvula is elevated to prevent
food from entering the nasopharynx. The
epiglottis drops downward to prevent food from
entering the larynx and trachea in order to direct
the food into the esophagus. Peristaltic
movements propel the food from the pharynx into
the esophagus.
Esophagus
The esophagus is a collapsible muscular tube that serves as a passageway between the
pharynx and stomach. As it descends, it is posterior to the trachea and anterior to the
vertebral column. It passes through an opening in the diaphragm, called the esophageal
hiatus, and then empties into the stomach. The mucosa has glands that secrete mucus to
keep the lining moist and well lubricated to ease the passage of food. Upper and lower
esophageal sphincters control the movement of food into and out of the esophagus. Thelower esophageal sphincter is sometimes called the cardiac sphincter and resides at the
esophagogastric junction.
Stomach
The stomach, which receives food from the esophagus, is located in the upper left
quadrant of the abdomen. The stomach is divided into the fundic, cardiac, body, and
pyloric regions. The lesser and greater curvatures are on the right and left sides,
respectively, of the stomach.
27
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
28/68
Gastric Secretions
The mucosal lining of the stomach is simple columnar epithelium with numerous tubular
gastric glands. The gastric glands open to the surface of the mucosa through tiny holes
called gastric pits. Four different types of cells make up the gastric glands:
Mucous cells
Parietal cells
Chief cells
Endocrine cells
The secretions of the exocrine gastric glands - composed of the mucous, parietal, and
chief cells - make up the gastric juice. The products of the endocrine cells are secreted
directly into the bloodstream and are not a part of the gastric juice. The endocrine cells
secrete the hormone gastrin, which functions in the regulation of gastric activity.
Regulation of Gastric Secretions
28
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
29/68
The regulation of gastric secretion is accomplished through neural and hormonal
mechanisms. Gastric juice is produced all the time but the amount varies subject to the
regulatory factors. Regulation of gastric secretions may be divided into cephalic , gastric,
and intestinal phases. Thoughts and smells of food start the cephalic phase of gastric
secretion; the presence of food in the stomach initiates the gastric phase; and the presence
of acid chyme in the small intestine begins the intestinal phase.
Stomach Emptying
Relaxation of the pyloric sphincter allows chyme to pass from the stomach into the small
intestine. The rate of which this occurs depends on the nature of the chyme and the
receptivity of the small intestine.
Small and Large Intestine
Small Intestine
The small intestine extends from the pyloric sphincter to the ileocecal valve, where it
empties into the large intestine. The small intestine finishes the process of digestion,
absorbs the nutrients, and passes the residue on to the large intestine. The liver,
gallbladder, and pancreas are accessory organs of the digestive system that are closely
associated with the small intestine.
The small intestine is divided into the duodenum, jejunum, and ileum. The small intestine
follows the general structure of the digestive tract in that the wall has a mucosa withsimple columnar epithelium, submucosa, smooth muscle with inner circular and outer
longitudinal layers, and serosa. The absorptive surface area of the small intestine is
increased by plicae circulares , villi, and microvilli.
29
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
30/68
Exocrine cells in the mucosa of the small intestine secrete mucus, peptidase, sucrase,
maltase, lactase, lipase, and enterokinase. Endocrine cells secrete cholecystokinin and
secretin.
The most important factor for regulating secretions in the small intestine is the presence
of chyme. This is largely a local reflex action in response to chemical and mechanical
irritation from the chyme and in response to distention of the intestinal wall. This is a
direct reflex action, thus the greater the amount of chyme, the greater the secretion.
Large Intestine
The large intestine is larger in diameter than the small intestine. It begins at the ileocecal
junction, where the ileum enters the large intestine, and ends at the anus. The large
intestine consists of the colon, rectum, and anal canal.
The wall of the large intestine has the same types of tissue that are found in other parts of
the digestive tract but there are some distinguishing characteristics. The mucosa has a
large number of goblet cells but does not have any villi. The longitudinal muscle layer,
although present, is incomplete. The longitudinal muscle is limited to three distinct bands,
called teniae coli, that run the entire length of the colon. Contraction of the teniae coli
30
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
31/68
exerts pressure on the wall and creates a series of pouches, called haustra, along the
colon. Epiploic appendages, pieces of fat-filled connective tissue, are attached to the
outer surface of the colon.
Unlike the small intestine, the large intestine produces no digestive enzymes. Chemical
digestion is completed in the small intestine before the chyme reaches the large intestine.
Functions of the large intestine include the absorption of water and electrolytes and the
elimination of feces.
Rectum and Anus
The rectum continues from the signoid colon to the anal canal and has a thick muscular
layer. It follows the curvature of the sacrum and is firmly attached to it by connective
tissue. The rectum and ends about 5 cm below the tip of the coccyx, at the beginning of
the anal canal.
The last 2 to 3 cm of the digestive tract is the anal canal, which continues from the
rectum and opens to the outside at the anus. The mucosa of the rectum is folded to form
longitudinal anal columns. The smooth muscle layer is thick and forms the internal anal
sphincter at the superior end of the anal canal. This sphincter is under involuntary control.
There is an external anal sphincter at the inferior end of the anal canal. This sphincter is
composed of skeletal muscle and is under voluntary control.
Accessory Organs
The salivary glands, liver, gallbladder, and pancreas are not part of the digestive tract, but
they have a role in digestive activities and are considered accessory organs.
Salivary Glands
Three pairs of major salivary glands (parotid, submandibular, and sublingual glands) and
numerous smaller ones secrete saliva into the oral cavity, where it is mixed with food
31
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
32/68
during mastication. Saliva contains water, mucus, and enzyme amylase . Functions of
saliva include the following:
o It has a cleansing action on the teeth.
o It moistens and lubricates food during mastication and swallowing.
o It dissolves certain molecules so that food can be tasted.
o It begins the chemical digestion of starches through the action of amylase,
which breaks down polysaccharides into disaccharides.
Liver
The liver is located primarily in the right hypochondriac and epigastric regions of the
abdomen, just beneath the diaphragm. It is the largest gland in the body. On the surface,
the liver is divided into two major lobes and two smaller lobes. The functional units of
the liver are lobules with sinusoids that carry blood from the periphery to the central vein
of the lobule.
The liver receives blood from two sources. Freshly oxygenated blood is brought to the
liver by the common hepatic artery, a branch of the celiac trunk from the abdominal
aorta. Blood that is rich in nutrients from the digestive tract is carried to the liver by the
hepatic portal vein.
The liver has a wide variety of functions and many of these are vital to life. Hepatocytes
perform most of the functions attributed to the liver, but the phagocytic Kupffer cells that
line the sinusoids are responsible for cleansing the blood.
Liver functions include the following:
secretion synthesis of bile salts
synthesis of plasma protein
storage
detoxification
32
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
33/68
excretion
carbohyrate metabolism
lipid metabolism
protein metabolism
filtering
Gallbladder
The gallbladder is a pear-shaped sac that is attached to the visceral surface of the liver bythe cystic duct. The principal function of the gallbladder is to serve as a storage reservoir
for bile. Bile is a yellowish-green fluid produced by liver cells. The main components of
bile are water, bile salts, bile pigments, and cholesterol.
Bile salts act as emulsifying agents in the digestion and absorption of fats. Cholesterol
and bile pigments from the breakdown of hemoglobin are excreted from the body in the
bile.
Pancreas
The pancreas has both endocrine and exocrine functions. The endocrine portion consists
of the scattered islets of Langerhans , which secrete the hormones insulin and glucagon
into the blood. The exocrine portion is the major part of the gland. It consists of
pancreatic acinar cells that secrete digestive enzymes into tiny ducts interwoven between
the cells. Pancreatic enzymes include anylase, trypsin, peptidase, and lipase. Pancreatic
secretions are controlled by the hormones secretin and cholecystokinin.
33
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
34/68
IX Etiology
Predisposing Factors:
factor actual rationaleGenes X Salmonella typhi is shed
only in human feces and istransmitted via the fecal-oral route of infection. It istherefore a non-hereditarydisease.
Age X There is no specific agegroup within which thedisease is most dangerous.However, traditionally theage range considered to beat greatest risk was 5-25years but typhoid fever canaffect any person from anyage group who ingests thesalmonella typhi bacteria.
Sex X Both sexes can acquiretyphoid fever through theingestion of contaminatedfood or water.
Socio-Economic Status The Family is not sofinancially well off.However, the mother isworking in Jeda as aDomestic Helper and thefather is unemployed. Thefamilys income is notsufficient to finance all their
34
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
35/68
needs in order for the livingto be more comfortable andto buy all the medicinesneeded.
Precipitating Factors:
Environment The family at the momentlived at a village near aRiver where Kyle and his
siblings usually takes a bath.Also it is where thecarabaos are bathing and thefather also said that maybetheir neighbors defecatethere.Typhoid is common in poor andtropical areas of theworld where sanitation isinadequate and the water supply not effectively
purified.Source:www.ptolemy.ca.pdf Unsanitary food handling The Family does practice
good sanitation in handlingfoods. They dining table isalways left uncleanedespecially the 3 youngsibling are the only oneeating together. Also,Unwashed plates are alwaysleft in their lavatory until it
accumulates. Sometimesleft-over foods are also leftuncovered in the diningtable.
Ingestion of ContaminatedFoods.
Kyle is always swimmingthe contaminated river.There is a possibility that heingested water from the
35
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
36/68
river even at minimumamount. S typhi istransmitted via the fecal-oral route. The infectiousdose is between 105 and
109. The dose is lower if the bacteria are given withsodium bicarbonate,suggesting that a proportionof the ingested bacteria aredestroyed by the acidenvironment in the stomach.
Source: www.ptolemy.ca
Unsanitary preparation of
food
The father said that there are
a lot of food flies, rats andcockroaches in their kitchenthat must have contaminatedthe prepared food.
36
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
37/68
X. Symptomatology
symptoms actual rationale
1. Fever Because of the presence of
Salmonella typhi on his blood thethe body releases pyrogeneswhich are abnormal proteins. The
body increases temperature toincrease oxygen uptake whichresults to increased respiratoryrate and renders WBC moreaggressive against bacteria andthis increases there phagocyticactivity. Endotoxins released bythe gram-negative bacteria whichelicits a antigenic response thatresults to increased intemperature.
2. Burning Micturition X Not Present.
3. Gastroenteritis S.typhi, which is present withinhis stomach, elicits aninflammatory reaction as the bodytries to combat the infection.
4. Diarrhea Diarrhea is one of the bodysmethods of releasing infectious
bacteria before it gets a chance to proliferate.
5. Headache X Not Present.
6. Abdominal Pain Frequent contact of the stomachlining with the S.typhi bacteriaresults in constant inflammation,especially in areas of greatestmacrophage concentration, whichin turn causes tissue necrosis,hence, the abdominal pain.
7. Body Ache X Not Present.
8. Dry Cough Bacteria can reach the lungs ascontaminated blood enters the
37
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
38/68
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
39/68
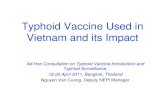
XI. Pathophysiology
39
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
40/68
S.typhi is shed inhuman feces
Contamination of food
and water
Ingestion of contaminatedfood or water by humans
S.typhi tries to survive in acidicenvironment of the stomach
Remaining bacteria invadeepithelial cells in the intestine
Macrophages from Peyers patches engulf bacteria
S.typhi injects effector proteins into macrophage
Normal cellular activities arediverted
Bacteria survives andmultiplies within
macrophage
Macrophages carrying bacteria
accumulate in Peyers patches
Phagocytes undergo lyses and release bacteria into nearby lymphatic ducts
Constant exposure to bacteria
Inflammation
Necrosis
Bowel perforation
Intestinal bleeding
-Blood in vomitus-Abdominal pain-Gastroenteritis
Bacteria disseminate to regional lymphnodes
Bacteria passes through thoracicduct and enters the bloodstream
Primary Bacteremia(Asymptomatic)
40
Predisposing Factors:
o Geneso Ageo Sexo Socio-economic
Status
Precipitating Factors:
o Environmento Unsanitary Food
Handlingo Ingestion of
ContaminatedFood
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
41/68
Changes brought about by sepsisaccumulate in the heart, brain, andkidneys
IF NOTTREATED: IF TREATED:
Infection spreads to other systems
-Endocarditis-Renal Failure-Brain Infxn
41
-Fever -Headache-Abdominal Pain
Overwhelmingsepsis
Circulatory Failure
DEATH!
Antibiotic Therapy
-Elimination/decrease in number of S.typhi
-Alleviation of signsand symptoms-Recovery fromcondition
Bacteria spread to other cells of reticuloendothelial system (including
spleen, liver, and gallbladder)
Bacterial growthwithin spleen and liver
-Splenomegaly-Hepatomegaly
Bacteria is shed into the bloodstream
Secondary Bacteremia
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
42/68
XII. Doctors Order
42
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
43/68
Date Order Rationale Remarks11/25/07 >Pls. admit to SVI, level 2, red2
>DAT except for DCF>Dxs:
CBC, platelet count
UA
Blood GS/CS Urine GS/CS
Typhidot IgM and IgB
>IVF: D5LR 1L to run @56cc/h
>Meds: Ranitidine 20mg/ IVTTq8h prn for abdominal pain,
>Chloramphenicol565mg/IVTT q8h
>VSq4h with BP monitoring,WOF unusualities: bleeding andhypotension, refer
>To assess the patient for infection, anemia and anydisorders.
>To assess for anyabnormalities within theurinary system as well as for systemic problems that maymanifest symptoms throughthe urinary tract.
>To detect Typhoid fever andany other salmonellainfection.
>To prevent patient fromdehydration and maintainadequate electrolyte and fluid
balance.
>To relief Patients abdominal pain.
>Use to treat infetctionspecifically salmonellaspecies.
>To monitor the patientscondition and monitor for anyunusualties in the patient such
bleeding and hypotension.
DONE
DONE
DONE
DONE
DONE
DONE
DONE
DONE
11/26/079:30am
9:45pm
>Still for UA, blood GS/CS,urine GS/CS>Cont. IVF @ SR >Cont. meds
>VSq4h
>I&OqS
>To monitor patientscondition and assess for anyabnormalities in the patientsVS.
> To determine if the kidneysfunction is now affected
because Typhoid fever iscomplicated by AcuteOliguric Renal Failure.
43
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
44/68
XIII. Diagnostic and L abor atory Exams
Date Diagnostic Exam Rationale Normalvalue
Result Clini cal significance Nursingconsiderations
11/24/07 COMPLETE BLOODCOUNT
Hgb
Hct
RBC count
To evaluate blood loss,erythropoieticability,anemia, andresponse totherapy.
To evaluate blood loss,anemia, bloodreplacementtherapy, andfluid balance,and screensred blood cellstatus. Also toevaluatedehydration
andhypervolemia.
To evaluateanemia andother conditions
135-175
0.40-0.52
4.20-6.10
L71 g/L
L0.20
L2.78x10^6/uL
Increased: Congenital heart disease Hemoconcentration Congestive heart failure Chronic obstructive
pulmonary disease
DehydrationDecreased: Anemia Hemolysis Severe hemorrhage Cancer Kidney disease Chronic hemorrhage Nutritional deficiency Lymphoma Hemoglobinopathies
Increased: Congestive heart disease Hemoconcentration Severe dehydration Shock Severe diarrheaDecreased: Anemia Cirrhosis Hemolytic reaction Dietary deficiency Malnutrition Hemorrhage
Increased: Congenital heart disease Polycythemia
vera/hemoconcentration
The CBC requiresa sample of bloodcollected from avein. The nurse or
phlebotomistinserting the needshould clean theskin first. Thetourniquet should
be removed fromthe arm as soon asthe blood flows. Ia fingerstick isused to collect the
blood, care must btaken to wipe awathe first drop, andnot to squeeze thefinger excessivelyas this causes the
blood to be diluted by tissue fluid.
Many drugs affecthe results bycausing increasedor decreased RBCWBC, and/or
platelet productionMedications shou
be taken intoaccount wheninterpreting result
Discomfort or bruising may occu
at the puncture sitApplying pressureto the puncture situntil the bleedingstops helps toreduce bruising;warm packs relievdiscomfort. Some
people feel dizzy faint after blood
44
http://www.labtestsonline.org/understanding/conditions/anemia.htmlhttp://www.labtestsonline.org/understanding/conditions/bone_marrow_disorders.htmlhttp://www.labtestsonline.org/understanding/conditions/anemia.htmlhttp://www.labtestsonline.org/understanding/conditions/bone_marrow_disorders.htmlhttp://www.labtestsonline.org/understanding/conditions/anemia.htmlhttp://www.labtestsonline.org/understanding/conditions/anemia.htmlhttp://www.labtestsonline.org/understanding/conditions/bone_marrow_disorders.htmlhttp://www.labtestsonline.org/understanding/conditions/bone_marrow_disorders.htmlhttp://www.labtestsonline.org/understanding/conditions/bone_marrow_disorders.htmlhttp://www.labtestsonline.org/understanding/conditions/bone_marrow_disorders.htmlhttp://www.labtestsonline.org/understanding/conditions/bone_marrow_disorders.htmlhttp://www.labtestsonline.org/understanding/conditions/anemia.htmlhttp://www.labtestsonline.org/understanding/conditions/bone_marrow_disorders.html -
8/14/2019 FINAL BURN CD-TYPHOID FEVA
45/68
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
46/68
Lymphocytes
Monocytes
Eosinophils
20-35
2-10
1-6
29
7
L0
Measles Rubella Mononucleosis or
tularemia SLE Aplastic anemia
Increased: Viral infection including
TB, hepatitis, mumps pertussis, syphilis,rubella,mononucleosis,cytomegalovirus, or other viral illnesses,lymphocytic leukemia,ulcerative colitis
chronic infection or animmune disease
Decreased: defective lymphatic
circulation chronic debilitating
conditions such as CHF,renal failure, or advancedTB
Hodgkins disease or burns
Increased: TB Hepatitis
Malaria Rocky mountain spotted
fever SLE Monocytic leukemia Lymphomas Chronic ulcerative colitis
Decreased: Does not have clinical
significance related todisease; it may indicate
positive response to prednisone treatment.
Increased: Allergic response Serum sickness Parasitic infection
including hookworm,roundworm, amebiasis, or trichonosis.
Skin disorder
46
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
47/68
Basophils
Platelet CountTo assist inthe diagnosisof bleedingdisorders
0-1
150-400
0
L125
Neoplastic disorder Ulcerative colitis Pernicious anemia Scarlet fever Autoimmune disease Splenectomy
Decreased: Cushings syndrome Trauma Burns Shock Surgery CHF Aplastic anemia Pernicious anemia
Increased: Chronic myelocytic
leukemia Polycythemia vera Hodgkins disease Ulcerative colitis Nephrosis Chronic hemolytic anemia
Decreased: Hyperthyroidism Pregnancy Stress response Anaphylactic reactions Steroid therapy
An abnormally low platelet level(thrombocytopenia) is acondition that may resultfrom increaseddestruction of platelets,decreased production, or increased usage of
platelets. In idiopathicthrombocytopenicpurpura (ITP), plateletsare destroyed atabnormally high rates.Another cause of a low
platelet count is anenlarged spleen.Hypersplenism ischaracterized by thecollection (sequestration)of platelets in the spleen.
47
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
48/68
Disseminatedintravascular coagulation(DIC) is a condition inwhich blood clots occur within blood vessels in anumber of tissues.
Leukemia and aplasticanemia can result in a low platelet count because of decreased production of
platelets in the bonemarrow. All of thesediseases produce reduced
platelet counts.
Abnormally high plateletlevels (thrombocytosis)may indicate either a
benign reaction to aninfection, surgery, or certain medications; or adisease like polycythemiavera, in which the bonemarrow produces toomany platelets tooquickly.
48
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
49/68
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
50/68
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
51/68
Date Diagnostic Exam Rationale Normalvalue
Result Clinical significance Nursingconsiderations
11/28/-7 Serology Typhidot
It is a dot ELISAkit which detects
IgM and IgGantibodies againstS. Typhi. It uses aspecific antigen onthe outer membrane of S.Typhi dotted onnitrocellulose stripsand for detectingthe resultingantigen antibodycomplex,
peroxidaseconjugated antihuman IgG andIgM and achromogenicsubstrate areemployed.
IgM
IgG
+
+
Positive control gives bluecolour dots,
- blood culture positive for salmonella agglutinating bodies, indicative of salmenonella infection
51
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
52/68
XIV. Drug Study
52
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
53/68
XV. Nursing Theories
Nightingales Environmental Theory
Florence Nightingale, often considered the first nurse theorist, defined nursingover 100 years ago as "the act of utilizing the environment of the patient to assist him in
his recovery". She linked health with five environmental factors: pure or fresh air , pure
water ,efficient drainage , cleanliness , light, especially direct sunlight. Nightingale's
environmental factors attain significance when one considers that sanitation conditions in
hospitals of the mid-1800s were extremely poor and that women working in the hospitals
were often unreliable, uneducated, and incompetent to care for the ill. In addition to those
factors, Nightingale also stressed the importance of keeping the client warm, maintaining
a noise-free environment, and attending to the client's diet in terms of assessing intake,
timeliness of the food, and its effect on the person. Nightingale set the stage for further
work in the development of nursing theories. Her general concepts about ventilation,
cleanliness, quiet, warmth, and diet remain integral parts of nursing and health care today.
53
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
54/68
The case of our patient is Typhoid fever. The cause of Typhoid is Salmonella. The
mode of acquiring the bacteria and so as the disease itself is through fecal-oral mode of
transmission. The bacteria is easily transmitted especially to unsanitary places or objects.
In order to provide care for our patient, we need to eradicate its reservoir in order to
prevent the bacterias survival and stop or prevent its transmission and so as help the
affected clients recover from the infection and also protecting his family. We need to
promote and maintain a clean environment conducive for a healthy living and not for
bacteria. We need to provide clean water and foods. Proper food handling and washing
before and after every procedure done should be well observed and maintained and so as
for the patient and family. They should practice having a safe food and safe eating and
living environment. Also, we need to provide a well balanced diet for the patient in order
to hydrate and fulfill the metabolic demands. Good ventilation and comfort should also be promoted so that our patient will feel quite relaxed and have a happy and healthy
disposition. All in all, this sums up to promoting wellness.
Dorothy Johnson Behavioral System (JBS) Model
Johnson states that a nurse should use the behavioral system as their knowledge base, comparable to the biological system that physicians use as their base of knowledge.
The reason Johnson chose the behavioral system model is the idea that "all the patterned,
repetitive, purposeful ways of behaving that characterize each person's life make up an
organized and integrated whole, or a system". Johnson states that by categorizing
behaviors, they can be predicted and ordered. Johnson categorized all human behavior
into seven subsystems: Attachment, Achievement, Aggressive, Dependence, Sexual,
Ingestive, and Eliminative. Each subsystem is composed of a set of behavioral responses
or tendencies that share a common goal. These responses are developed through
experience and learning and are determined by numerous physical, biological,
psychological, and social factors. Four assumptions are made about the structure and
function of each subsystems. These four assumptions are the "structural elements"
common to each of the seven Subsystems. The first assumption is "from the form the
54
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
55/68
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
56/68
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
57/68
Seventh, engaging in genuine teaching-learning experience that attends to the
patients health care needs.
Eight, creating healing environment at all levels, physical, social, emotional,
mental, spiritual, and consciousness. Thereby, wholeness, beauty, comfort, dignity, and
peace must be enhanced.
Ninth, assisting with basic needs, with an intentional caring consciousness,
administering human care essentials' and examples of needs maybe according to
Maslows hierarchy of needs.
Tenth, Opening and attending to spiritual-mysterious and existential dimensionsof one's own life-death, soul care for self and the one-being-cared-for and so in attending
to the patient we should be open-minded regarding the patients beliefs.
57
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
58/68
XVI. Nursing Care Plans
58
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
59/68
XVII. Health Teachings
1. Wash your hands. Frequent hand washing is the best way to control infection.
Wash your hands thoroughly with hot, soapy water, especially before eating or
preparing food and after using the toilet. Carry an alcohol-based hand rub for times
when water isn't available.
2. Avoid untreated water. Contaminated drinking water is a particular problem in
areas where typhoid is endemic. For that reason, drink only bottled water or canned
or bottled carbonated beverages, wine and beer. Carbonated bottled water is safer
than still water is. Wipe the outside of all bottles and cans before you open them.
Ask for drinks without ice. Use bottled water to brush your teeth, and try not to
swallow water in the shower.
3. Avoid raw fruits and vegetables. Because raw produce may have been washed in
unsafe water, avoid fruits and vegetables that you can't peel, especially lettuce. To
be absolutely safe, you may want to avoid raw foods entirely.
4. Choose hot foods. Avoid food that's stored or served at room temperature.
Steaming hot foods are best. And although there's no guarantee that meals served at
59
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
60/68
the finest restaurants are safe, it's best to avoid food from street vendors it's
more likely to be contaminated.
5. Get Vaccinated- Typhoid fever vaccine. one is injected in a single dose, and the
other is administered orally over a period of days. Neither is 100 percent effective,and both require repeat vaccinations.
6. Appropriate systems for human waste disposal must be available. S.typhi can
only be shed through human feces. It is therefore of utmost importance that human
waste be disposed in a most appropriate manner to avoid spread of bacteria.
To prevent infecting others
If you're recovering from typhoid or paratyphoid, these measures can help keep others
safe:
1. Wash your hands often. This is the single most important thing you can do to keep
from spreading the infection to others. Use plenty of hot, soapy water and scrub
thoroughly for at least 30 seconds, especially before eating and after using the
toilet.
2. Clean household items daily. Clean toilets, door handles, telephone receivers and
taps at least once a day with a household cleaner and paper towels or disposable
cloths.
3. Avoid handling food. Avoid preparing food for others until your doctor says you're
no longer contagious. If you work in the food service industry or a health care
facility, you won't be allowed to return to work until tests show that you're no
longer shedding typhoid bacteria.
4. Keep personal items separate. Set aside towels, bed linen and utensils for your own use and wash them frequently in hot, soapy water. Heavily soiled items can be
soaked first in disinfectant.
60
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
61/68
XVIII. DISCHARGE PLAN
Medication
*Cephalosporins (sef-a-loe-SPOR-ins) are used in the treatment of
infections caused by bacteria. They work by killing
bacteria or preventing their growth.
-Cephalosporins may be taken on a full or empty stomach. If
this medicine upsets your stomach, it may help to take it
with food.
* Ampicillin are used to reduce the development of drug-resistant bacteria
and maintain the effectiveness of Ampicillin and other antibacterial drugs, Ampicillin
should be used only to treat or prevent infections that are proven or strongly suspected to be caused by bacteria.
*Ciprofloxacin is used to treat bacterial infections in many different parts of
the body. They work by killing bacteria or preventing their growth.
61
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
62/68
Exercise
*Regular exercises aides in achieving and maintaining an optimum level of wellness and health. This may help in avoiding diseases and disorders.
Treatment/therapy
*Water therapy helps in recovery from the illness.
Hygiene
*S.typhi is shed in human feces. Advise the patient to maintain proper hygiene, especially after voiding to avoid spreading the disease.
*Advise the patient not to handle food or participate in food preparation.
*Educate significant others on importance of sanitary food preparation.
Outpatient
1. Water must be properly filtered and boiled before drinking if it is from an
unreliable source.
2. Food must be properly washed and then cooked3. One must not eat or drink in suspected unhygienic or unreliable places.
4. Express importance of compliance to prescribed mediations.
Diet
Diet: Rich in Carbohydrates, proteins and fats
1. Food must be simple and easy to digest, avoid all kinds of spices on food.
2. Food should be cooked well, but not overcooked as that would make it difficult todigest.
3. If diarrheas develop in typhoid increase fluid intake such as soups, curries, gravies
and fruit juice. Vitamin B and C foods must be consumed in order to compensate
for the losses of those vitamins.
4. Eggs and milks are suitable proteins that can be consumed during typhoid fever.
62
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
63/68
5. Vegetables oils and milk products such as butter, cheese, cream and emulsified
fats can be consumed. Wheat, rice, potatoes and other foods that are high in
carbohydrates are advised
XIX. PrognosisCRITERIA POOR FAIR GOOD JUSTIFICATION
1.Onset of
illness
The progression of thypoid fever
includes an incubation period of 2-3
weeks, in which the first week isasymptomatic. This explains why the
client sought admission only when
symptoms began to appear and the
bacteria were already in systemic
circulation.2. Duration of
illness
As of the writing of this study, the
client has had the illness for almost 3
weeks. He began proper treatment 9
days after the appearance of symptoms,
which would suggest that the disease is
already in its second week of
progression. We rated this parameter
63
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
64/68
fair because proper treatment was given
at just the right time, although the
patient could have sought professional
help sooner.3. Precipitating
factors
Health teachings were given to the
patient and his family regarding the
causes of the disease. The precipitating
factors of this case were highly
modifiable and so we gave this
parameter a good rating.4. Attitude and
willingness to
take medication
Kyle was very willing to take his
medications and he and his family were
observed to have complied with the
treatment regimen being given. As for
this reason, we rated this parameter as
good.5. Family
Support
Kyles family is very supportive as
provided whatever they could to help in
their sons recovery. They also listened
intently when health teachings were being given to prevent reoccurrence of
the disease.6. Age Tyhpoid fever does not affect a specific
age group. It can be acquired by anyone
who accidentally ingests the S.typhi
bacteria.7. Environment The familys house is situated near a
river wherein which carabaos bathe andother humans defecate. Kyle is fond of
swimming in the river which may cause
infection due to the contaminated water.
POOR: Onset of Illness, Environment
64
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
65/68
FAIR: Duration of Illness, Age
GOOD: Precipitating Factors, Attitude & Willingness to Take Medication, Family
Support
Computation:
Number of categories rated POOR x1 + Number of categories rated FAIR x2 +
Number of categories GOOD x3 divided by TOTAL number of categories = score of
general prognosis.
= 2 + 2(2) + 3(3)
= 2 + 4 + 9
= 15/7
= 2.1 (Good)
Scoring for general Prognosis:
1 1.6 = POOR
1.7 2.3 = FAIR
2.4 3.0 = GOOD
General Prognosis:
Based on above criteria, our patient Kyle has a good prognosis.
65
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
66/68
I. References
Marilynn E. Doenges, Mary Frances Moorhouse, Alice C. Geissler-Murr, Nursing
Care Plans Guidelines for Individualizing Nursing Care, 6 th Edition, Copyright
2002 F.A. Davis Company
Suzanne C. Smeltzer, Brenda G. Bare, Brunner and Suddharts Textbook of
Maedical-Surgical Nursing, 10 th Edition, Copyright by Lippincott William and
Wilkins, 2004
Barbara Kozier, Glenora Erb, Audrey Berman, Shirlee Snyder, Fundamentals of
Nursing, Concepts, Procxess and Practice, 7th
Edition, Philippine Edition
published by PEARSON EDUCATION SOUTH ASIA LTD., Copyright 2004
66
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
67/68
Marrilynn E. Doenges, Mary Frances Moorhouse, Alice C. Geissler-Murr, Nurses
Pocket Guide, Diagnoses, Interventions and Rationales, 9 th Edition, Copyright
2004 by F.A. Davis Company
Sylvia A. Price, Lorraine M. Wilson, Pathophysiology, Clinical Concepts of
Disease Process, 4 th Edition, Copyright 1992 by Mosby-Year Book, Inc.
Wilson, Shannon, Stang, Prentice Hall, Nurses Drug Guide 2005, Copyright
2005 by Pearson Education, Inc., Upper Saddle River, NJ 07458
Amy M. Karch, 2003 Lippincotts Nursing Drug Guide, Copyright 2003 by
Lippincott Williams and Wilkins
Rick Daniek, Nursing fundamentals, Caring and Clinical Decision Making,
Thanson Asian Edition, Copyright 2004 by Delmar, a division of Thomsom
Learning, Copyright 2002 by F.A. Davis Company
Marilyn E. Doenges, Macy Frances Moorhouse, Nurses Pocket Guide: Nursing
Diagnoses with interventions, 3 rd Edition, Copyright 1991 by F.A. Davis
Company
67
-
8/14/2019 FINAL BURN CD-TYPHOID FEVA
68/68
Edited by: William A. Sodeman, Pathologic Physiology Mechanisms of Disease,
Illustrated, 2 nd Edition, Copyright, 150, by W.B. Saunders Company
Internet Sources:
- http://www.metagenics.com/ADAM/41/024200.html
- http://en.wikipedia.org/wiki/Typhoid_fever
- http://www.ecureme.com/emyhealth/data/Enteric_Fever.asp
http://www.metagenics.com/ADAM/41/024200.htmlhttp://en.wikipedia.org/wiki/Typhoid_feverhttp://www.metagenics.com/ADAM/41/024200.htmlhttp://en.wikipedia.org/wiki/Typhoid_fever