The Reptilian Brain The Mammalian Brain The Thinking Brain The Triune Brain.

Few Mets in the Brain
Salvador Villà
ICO HUGTIP Badalona
IOT Barcelona Acadèmia, desembre 2014

Patient...
Age: 56 yo Middle Favorable
Performance status: KPS 90 (or less...?) (and after
corticosteroids!) Favorable!
Extracranial disease: No. Favorable!
Activity of primary tumor: No. Favorable!
Number of mets: 1, Size 13mm Favorable!
Histology (primary tumor): Lung ca,
Adenocarcinoma. Unfavorable!

KARNOFSKY PERFORMANCE STATUS SCALE DEFINITIONS RATING (%) CRITERIA 100 Normal no complaints; no evidence of disease.
90 Able to carry on normal activity; minor signs or symptoms of
disease.
80 Normal activity with effort; some signs or symptoms of disease.
70 Cares for self; unable to carry on normal activity or to do active
work.
60 Requires occasional assistance, but is able to care for most of his
personal needs.
50 Requires considerable assistance and frequent medical care.
40 Disabled; requires special care and assistance.
30 Severely disabled; hospital admission is indicated although death
not imminent.
20 Very sick; hospital admission necessary; active supportive
treatment necessary.
10 Moribund; fatal processes progressing rapidly.
0 Dead
Karnofsky Performance Status

Memory
loss?
MRI better than
CT
Neurocognitive
evaluation?
Dexamethasone and mets Vecht et al, Neurology 94
• Convencional dosage 16 mg/d
• 2 double blind trials: 4 mg vs. 8 mg and 4
mg vs. 16 mg
• Kf > 80, 96 p recuited
• Improvement of KPS: no changes
• Side effects: dosis dependent

Sarin (Lancet Neurol 2003)
• 1. Starting total dose with 4mg/24h
• 2. If after 72h clinical improvement is not observed, adding 8mg/24h
• 3. If after next 72h clinical improvement is not observed, it was advised to increase doses 4 mg every 6h till to reach 24mg/24h.
• 4. If stabilization or improvement of symptoms and signs were observed, decreasing of 4 mg every 72 h was recommended.
• 5. In case of getting worse, starting as scheduled above.
• 6. If high endocranial pressure or consciousness were altered, starting with 24 mg/24h of dexamethasone and manitol.
• Taking of pills could be done at the morning 2/3 of total doses, and at the evening 1/3 of total dose.

Treat the patient!
Do not treat the image!

Tom Nikkelsen et al, J of Neurooncol 2010
Forsyth et al 2003

Variables RPA Rotterdam SIR BSBM GPA Rades1-2 DS-GPA
PS KPS ECOG KPS KPS KPS KPS KPS
Age <65 NA <50, 51-59 >59 NA <50, 51-59, >59 <70 <50, 51-59, >59
ECM No vs yesLimited
activityNo vs yes No vs yes No vs yes No vs yes No vs yes
Control
PTNo vs yes
Limited
activityPD vs no PD NA NA NA NA
Steroids NAType of
responseNA NA NA NA NA
N of BM NA NA 1,2-3,>3 NA 1, 2-3, >3 1, 2-3, >3 1, 2-3, >3
Vol of BM NA NA Yes NA NA NA NA
Interval
to BMNA NA NA NA NA <8m vs >8m NA
Histology NA NA NA NA NA NA Yes

Sperduto et al, 2008
GPA: 3.5, MST 11 months
(Prospectively validated, Villà et al 2011)

Sperduto et al, 2011
MST 14.8
For RPA class 1: 7.1 m

There are limitations in the ability
of physicians to accurately predict
patient survival (Tsao et al,
ASTRO 2012)
Kondziolka et al , J Neurosurg 2014
All p
A-B
C- lung
D- breast

• Large oedema in single BM: best prognostic prognostic (Spanberger
13)
• Central necrosis and patterns of enhancement: negative factor
(2001, Xu 2012). Hypofractionated RT, better (Tomas-Dasu 14)
• Cystic BM: similar LC compared to noncystic BM (Ebinu 2013)
• High DWI and low ADC indicated poor OS (Berghoff 13)
• Total tumour volume of BM: factor (Baschnagel 2013, Hartford
2013)
• No differences between supratentorial lobes and infratentorial region
(EORTC 22952)
• Radiation necrosis: spectroscopy MRI, PET MET, surgery
Imaging factors

PF and histology, Lung Ca
• NSCLC: Adenoca and large-cell ca had a higher chance of BM (Shi
2006)
• Radio-resistant tumor (NSCLC) and poor response to WBI alone vs.
S and WBI (Mintz 1996).
• Focused RT dose and EGR mutation influence outcome (Lee 12)
• NSCLC with unique mets: 3 different situations and many
interpretations in the literature
• NSCLC: high Ki-67 expression and low p53 expression predicted
poor OS and correlation with BM
• NSCLC: Ki67 index, microvascular density and hypoxia-inducible
factor 1 alpha as promising prognostic value (Berghoff 14)
• ALK gene (anaplastic lymphoma kinase) translocations and
amplifications: constant incidence between PTs and BM (Preusser
13)
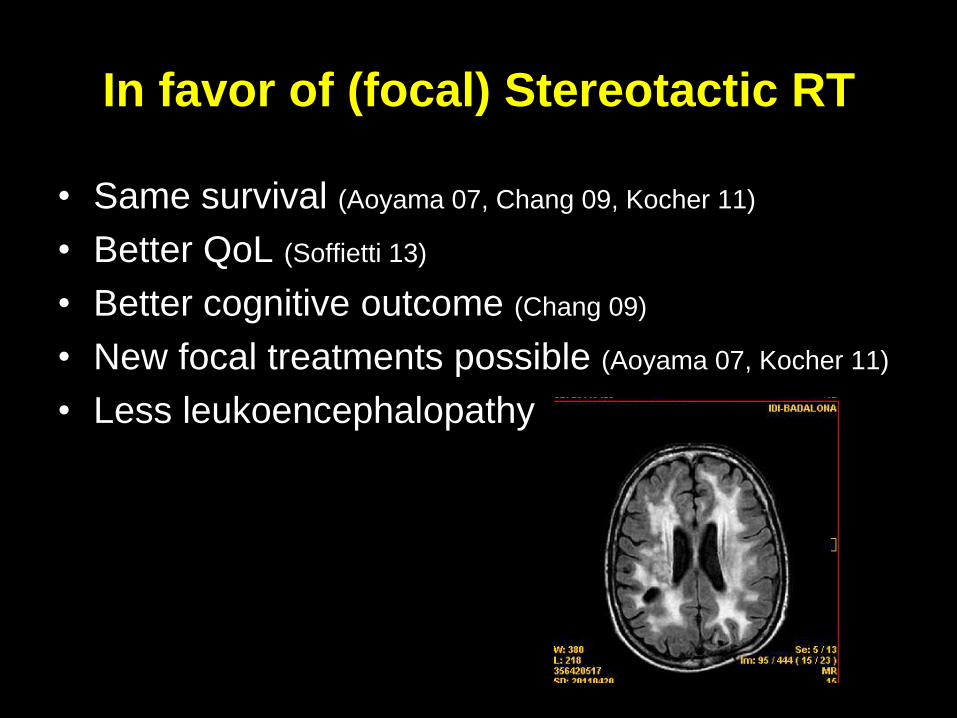
In favor of (focal) Stereotactic RT
• Same survival (Aoyama 07, Chang 09, Kocher 11)
• Better QoL (Soffietti 13)
• Better cognitive outcome (Chang 09)
• New focal treatments possible (Aoyama 07, Kocher 11)
• Less leukoencephalopathy
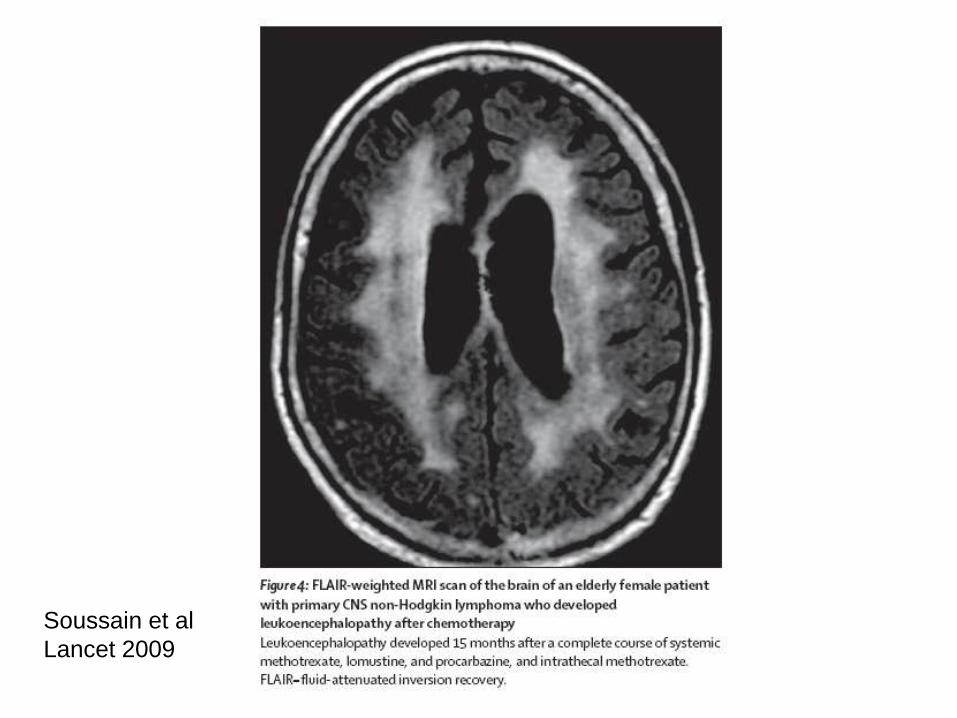
Soussain et al
Lancet 2009

SRS, exactrac
Conventional arctherapy with
asymmetric isocenter

In favor of WBI
• Less progression in the brain (Aoyama 07, Kocher 11)
• Drugs to prevention cognitive damage (RTOG trial,
memantine, Brown 13)
• New techniques to reduce dose in whole brain areas
• New techniques to protect hipocampus
Phase 2 RTOG trial 0933,
Gondi et al JCO 2014

Dose distribution for the higher dose regions
using WBRT+SIB
WBRT with conventional SRT
where the combined dose is not taken into account
Baumert et al 2013 Figure 1: WBRT /SIB: low (green) and high dose (red) levels delivered synchronously

Surgery for BM
• Accessible, no eloquent area?
• In posterior fossa
• More than one mets?
• No evidence that Surgery is better than
SRT

Well-demarcated
NSCLC
Vascular co-option
Melanoma
Diffuse invasion
SCLC
Influenced by expression of alfa v integrins complexes
Neuro-Oncol 2013


Conclusions
• To be careful with corticosteroids
• Try to avoid Whole Brain Irradiation
• Focal treatment!
• Close Follow-Up
• MRIs needed
• Prophylaxis in NSCLC?




Subclassification Class 2 (Yamamoto 2012)
• 4 factors:
KPS: 90 to 100 vs. 70 to 80
Number of BM: 1 vs. multiple
ECM: yes vs. no
PT status: controlled vs. not controlled
Class IIa, IIb, IIc (3753 GKRS patients)

Niwinska et al, 2012. Breast ca

Nomogram (Barnholtz-Sloan et al, 2012)

Nomogram from Rotterdam after SRS (Rodrigues 2014)
(PF related to TX) German group have added PT and ECM (Huttenlocher 2014)


Nieder et al Cancer 2011


Comparison of median survival in 7 studies using the recursive
partitioning analyses (RPA) classes (treatment was WBRT with or
without local measures, none of the studies is limited to one
particular cancer type).
Nieder and Mehta 2009

Carsten and Mehta 2009

Rades 2: scoring systems for irradiated patients,
Rades et al 2011

Marko et al, 2012. Breast cancer

Nomogram from Rotterdam after SRS (PF related
to TX) (Rodrigues 2014)

Table 7: Advantages and Disadvantages of Brain Metastases Prognostic Indices
Prognostic Index Statistical Validation Advantages Disadvantages
RTOG RPA large prospectively collected RTOG clinical trial primary
dataset, multiple validation investigations
well-known and described classification
system, frequently utilized in clinical care
and clinical trials moderate OC with low PPG PPV, some validation
studies suggest high PPG MMR
ROTTERDAM large primary dataset, no validation investigations*
good OR for both PPG and GPG
classifications, high PPG PPV, low PPG
MMR small GPG (<10%) in primary validation, use of
subjective steroid response, moderate GPG PPV
SIR very small primary dataset, large validation dataset confirming
OC derived from whole brain plus SRS
population small GPG (10%) in primary validation, moderate
OC with very low PPG PPV
BS-BM small primary dataset, validation datasets do not confirm high
OC seen in primary report derived from various SRS populations,
simple scoring system small (3%) PPG group with low PPV, high GPG
MMR
GPA very large prospective RTOG clinical trial primary dataset,
moderate sized validation cohorts derived from WBRT and SRS patient
populations, good GPG OC small GPG cohorts in primary and validation
datasets, low PPG PPV, high GPG MMR
RADES I large primary dataset, no validation investigations*
balanced proportions of patients in each of
four groups, overall good OC and PPG
MMR low PPG PPV
GGS moderate size primary dataset, no validation investigations* straightforward index construction, overall
good OC small (3%) PPG group with low PPV, high PPG
MMR
DS-GPA large primary dataset, no validation investigations*
disease-specific scoring integrated into
index, balanced proportions of patients in
each of four groups complex index construction, OC could not be
calculated from published reports
RADES II large primary dataset, no validation investigations* good OC, well balanced groups patient population not well reported in manuscript
* no validation studies that meet systematic review eligibility criteria (see methods section)
PPV = Positive Predictive Value; PPG = Poor Prognostic Group; GPG = Good Prognostic Group; OR = Operating Characteristics; SRS =
Stereotactic Radiosurgery; MMR = Major Misclassification Rate
Systemic review of scores Rodrigues et al 2013


Nieder et al Cancer 2011

Nieder et al Cancer 2011

Review Nieder et al Cancer 2011-1
• Mets USA: 170,000 per year
• Cost of care: 43,955 euros
• Management approaches: supportive
care, surgery, RT
• TX alghoritmes: based on patients’
prognosis and aim (palliation, prolongation
of survival, or both)

Review Nieder et al Cancer 2011-2
• Retrospective study
• 2 equally sized groups of patients
• 1- contemporary: 2005-2009 (103 p)
• 2- historical: 1983-1989 (103 p)
• Matching: diff in sex, colorectal ca (more in contemporary), no extracranial mets (less in contemporary group), single brain (less contemporary group), syncrhonous (less historical), interval (shorter in historical), RPA class (poorer in historical), and GPA score 0-1 (poorer in contemporary)

Nieder et al Cancer 2011

Nieder et al Cancer 2011



Review: Nieder et al, Cancer 2011

Diagnosis-specific GPA

Nieder et al, Cancer 2011


Villà et al, 2011

1-4 BM, max diameter 30 mm Aoyama 2006




An EORTC Phase III trial of Adjuvant Whole
Brain Radiotherapy Versus Observation in
patient with 1 to 3 Brain Metastases From
Solid Tumor After Surgical Resection or
Radiosurgery: Quality-of-Life analysis
R. Soffietti1, M. Kocher2, M. U. Abacioglu3, S. Villa4, F. Fauchon5,
B. G. Baumert6, L. Fariselli7, T. Tzuk-Shina8,R-D Kortmann9, C.
Carrie10, M. Ben Hassel11, M.Kouri12, E.Valeinis13, D. van den
Berge14, R. P. Mueller2, G. Tridello15,16, L. Collette16, A.
Bottomley8 on behalf of EORTC Radiation Oncology and Brain
Tumor Groups
Soffietti et al, 2011 (submitted)

Conclusion Adjuvant WBRT after surgery or radiosurgery of
a limited number of brain metastases from solid
tumors may negatively impact some aspects of
HRQOL, even if these effects are transitory.
Consequently, observation with close monitoring
with MRI (as done in the EORTC trial) is not
detrimental for HRQOL.
Soffietti et al, 2011 (submitted)

Lung cancer 1993.Solitary Brain mets Surgery + WBI 1996
MRI scan
4/2011


Figure 1: WBRT /SIB: low (green) and high dose (red) levels delivered synchronously
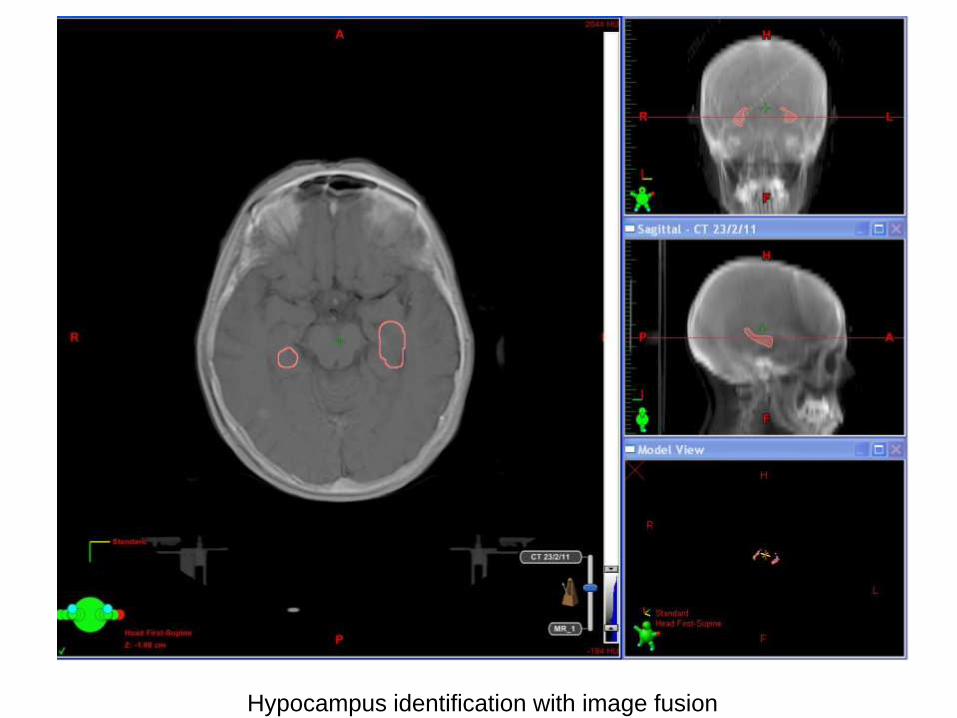
Hypocampus identification with image fusion

SRS for brain mets

Sperduto et al, 2008

Conventional arctherapy with asymmetric isocenter
Brain mets