Fetal Hydrocephalus: Surgical Treatment · Abstract Fetal hydrocephalus continues to present a...
18
Fetal Hydrocephalus: Surgical Treatment Sergio Cavalheiro, Antonio Fernandes Moron, Marcos Devanir Silva da Costa, Patricia Alessandra Dastoli, and Jardel Mendonça Nicacio Contents Introduction .............................................................................. 2 Epidemiology ............................................................................ 3 Diagnostic ................................................................................ 3 Experimental Studies and Natural History ........................................... 5 Etiology and Classification ............................................................. 6 Twin Gestation ........................................................................... 7 Surgical Approaches .................................................................... 7 Technical Notes .......................................................................... 10 Cephalocentesis ........................................................................... 10 Ventriculoamniotic Shunting ........................................................... 11 Third Ventriculostomy .................................................................. 11 Open Surgery for Intrauterine Repair for Myelomeningocele ...................... 11 Illustrative Cases ........................................................................ 13 Case 1 ..................................................................................... 13 Case 2 ..................................................................................... 13 Conclusion ............................................................................... 15 References ................................................................................ 16 S. Cavalheiro (*) · A. F. Moron · M. D. S. da Costa · P. A. Dastoli · J. Mendonça Nicacio Department of Neurosurgery, Hospital and Maternity Santa Joana, Sao Paulo, SP, Brazil Federal University of Sao Paulo, Sao Paulo, SP, Brazil e-mail: [email protected]; [email protected]; marcoscostaneuro@gmail. com; [email protected]; paty.dastoli@uol. com.br; [email protected] # Springer Nature Switzerland AG 2019 G. Cinalli et al. (eds.), Pediatric Hydrocephalus, https://doi.org/10.1007/978-3-319-31889-9_70-1 1
Transcript of Fetal Hydrocephalus: Surgical Treatment · Abstract Fetal hydrocephalus continues to present a...
Fetal Hydrocephalus: SurgicalTreatment
Sergio Cavalheiro, Antonio Fernandes Moron,Marcos Devanir Silva da Costa, Patricia Alessandra Dastoli, andJardel Mendonça Nicacio
ContentsIntroduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Epidemiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Diagnostic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Experimental Studies and Natural History . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Etiology and Classification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Twin Gestation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Surgical Approaches . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Technical Notes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10Cephalocentesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Ventriculoamniotic Shunting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Third Ventriculostomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Open Surgery for Intrauterine Repair for Myelomeningocele . . . . . . . . . . . . . . . . . . . . . . 11
Illustrative Cases . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Case 1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Case 2 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
S. Cavalheiro (*) · A. F. Moron · M. D. S. da Costa · P. A.Dastoli · J. Mendonça NicacioDepartment of Neurosurgery, Hospital andMaternity SantaJoana, Sao Paulo, SP, Brazil
Federal University of Sao Paulo, Sao Paulo, SP, Brazile-mail: [email protected];[email protected]; [email protected]; [email protected]; [email protected]; [email protected]
# Springer Nature Switzerland AG 2019G. Cinalli et al. (eds.), Pediatric Hydrocephalus,https://doi.org/10.1007/978-3-319-31889-9_70-1
1
AbstractFetal hydrocephalus continues to presenta challenge, not only for neurosurgeons butalso for obstetricians and the entire communityinvolved in the medical, religious, ethical, andlegal aspects related to this condition. In theearly twentieth century, fetal hydrocephaluswas a cause of maternal mortality due touterine rupture (Feeney and Barry, J ObstetGynaecol Br Emp 61:652–656, 1954). Cur-rently, however, with the use of diagnostictools such as ultrasonography and magneticresonance imaging (MRI), a pregnant womanhas the option to terminate her pregnancy,especially in countries where abortion is legal.
KeywordsFetal hydrocephalus · Obstrutivehydrocephalus · Endoscopic thirdventriculostomy · Cephalocentesis ·Myelomeningocele · Ventriculomegaly
Introduction
Fetal hydrocephalus continues to present a chal-lenge, not only for neurosurgeons but also forobstetricians and the entire community involvedin the medical, religious, ethical, and legal aspectsrelated to this condition. In the early twentiethcentury, fetal hydrocephalus was a cause of mater-nal mortality due to uterine rupture (Feeney andBarry 1954). Currently, however, with the useof diagnostic tools such as ultrasonography andmagnetic resonance imaging (MRI), a pregnantwoman has the option to terminate her pregnancy,especially in countries where abortion is legal.
Following results obtained from amanagementof myelomeningocele study (MOMS), a random-ized trial of prenatal versus postnatal repairof myelomeningocele, which demonstrated thatantenatal surgery outcomes are superior than post-natal ones; several centers worldwide beganperforming fetal surgery to treat disease (Adzicket al. 2011). However, the same results were notobtained in studies of fetal hydrocephalus. Thelast study on this condition, conducted 30 yearsago (International Register of Fetal Surgery
1982), showed that intrauterine surgery did notlead to better outcomes than treatment afterbirth, thereby contraindicating any fetal neurosur-gical procedure for the treatment of hydrocepha-lus. However, unlike the myelomeningocele trial,the fetal cooperative study had several biases: thechoice of hydrocephalus etiology was not uni-form, and imaging tests, comparing the differentetiologies of hydrocephalus, were not in highdefinition (Manning et al. 1986).
Fetal hydrocephalus is a serious malformation,which may, alongside the resultant ventricu-lomegaly, hide a large number of different defects,each with a different evolution, depending onthe etiology of the hydrocephaly. Other malfor-mations associated with hydrocephalus may occurin up to 75% of cases, providing a strong influenceon the prognosis of fetuses affected by this disease.
With recent technological development,especially with regards to diagnosis, fetal neuro-surgery has been privileged with the evolutionof ultrasonography (US), the complementationof ultrasound with magnetic resonance imaging(MRI), and a huge library of laboratory tests. Safediagnosis is assured for central nervous systemdiseases, including genetic, malformative, andinfectious processes affecting the fetus. The useof MRI with a T2-weighted sequence is mostsatisfactory, as it is too fast to be affected by thefetal movements and allows accurate observation,mainly of the posterior fossa structures such as thebrainstem and the cerebellum, thus increasingdiagnostic possibilities. Small intraventricularhemorrhages formerly not visualized by ultraso-nography can now bemore easily detected by fetalMRI (Benacerraf et al. 2007; Dill et al. 2009;Jeanty et al. 1981; Leidig et al. 1988; Levineet al. 2002; Manning et al. 1986).
The fetal moment, characterized as the periodduring which the fetus suffers the insult culminat-ing in hydrocephalus, is also one of the mostimportant factors to consider when establishinga prenatal prognosis. Fetal hydrocephalies begin-ning in the last trimester of gestation have betteroutcomes than those diagnosed at the beginningof gestation.
One of the key points of prenatal diagnosis is thedifferentiation between fetal hydrocephalus and
2 S. Cavalheiro et al.
non-hypertensive ventriculomegaly. The former iseligible for intrauterine treatment with good results.The latter, however, may result in either a favorableor catastrophic outcome through a destructive eti-ology, as seen in viral infections such as the Zikavirus. Therefore, non-hypertensive ventriculo-megalies are typically not eligible for intrauterinetreatment (Cavalheiro et al. 2016).
Epidemiology
The real incidence of fetal hydrocephalus is proba-bly underestimated because many cases of fetaldeath early in gestation are often not studied.In fact, it is not even known how often abortionsare performed among mothers of hydrocephalicfetuses. It is believed that the incidence rate ofsuch cases varies between 0.2 and 1.5 per 1000live births (Alter 1962; Cavalheiro et al. 1992,2002; Malpas 1937; Nomura et al. 2010; Steinet al. 1981). The incidence varies significantlyaccording to different authors and locations. Thehighest incidences were found in the city of Liver-pool, with 4.2 per 1000 live births (Malpas 1937)and Dublin, with 3.5 per 1000 live births (Coffeyand Jessop 1955), while in the United States theincidence was 0.96 per 1000 (Alter 1962). Cochraneet al. (1985) and Prata-Martins et al. (1985) foundthat multiparous women more often carried a fetuswith hydrocephalus, while Cavalheiro et al. foundthat primiparous women presented with a higherincidence of a fetus with hydrocephalus. Further-more, the predisposition is greater for fetuses of themale sex (Cavalheiro et al. 1992).
Diagnostic
Obstetric ultrasonography as part of routineprenatal monitoring is the standard method fordiagnosing intrauterine ventriculomegaly. Fetalventriculomegaly or hydrocephalus are complexdefinitions and are often difficult to differentiateand accurately identify.
Before the ready availability of ultrasonogra-phy, fetal hydrocephalus diagnoses were basedon x-rays of the maternal abdomen and
identification of fetal macrocrania (Lorber 1961).In 1966, Barke et al. were the first to confirm thepresence of ventriculomegaly by performingintrauterine gaseous ventriculography (Barkeet al. 1966). Advances in ultrasonography causeda revolution in the practice of obstetrics. Espe-cially when used after the 15th week of preg-nancy, ultrasound allowed the easy diagnosis ofnumerous malformations.
Clinically, most cases of fetal hydrocephalusare accompanied by polyhydramnios, a fact thatmay lead the obstetrician into a false diagnosisand suspicion of an error in the gestational age.An ultrasonographic image is then requested forclarification and the hydrocephalus is finallydiagnosed.
At the beginning of gestation, the ventricularcavities are large and the echogenicity of theventricle walls is not very clear, so diagnosis isdifficult. As gestation continues, the ventricularcavities decrease in size and echogenicity of theventricle wall increases. In some cases, the down-sizing of the ventricular cavities only occurs bythe end of gestation, which may lead to a falsediagnosis of hydrocephalus. In 1981, Jeanty et al.(1981) described a relationship between the lateralventricle and the cerebral hemi-hemisphere(LV/CHH) based on the study of 200 normalfetuses. The graphical representation of this rela-tionship permits ventriculomegaly to be diag-nosed at an early gestational age, much earlierthan any increase in the biparietal diameter. Inmany cases, the cranial circumference and thebiparietal diameter only increase near the end ofthe gestational period. Huge ventriculomegalyoften occurs without any increase in the cephalicperimeter. Ventriculomegaly is identified whenthe LV/CHH ratio is greater than 0.5 after the15th week of gestation. During the fetal period,an atrial width <10 mm is considered normal;between 10 and 15 mm, the ventriculomegaly isclassified as mild to moderate, whereas a measure-ment >15 mm is graded as severe (Garel 2005).
In addition to ultrasonography, other tests cancontribute to the diagnosis of ventriculomegaly,such as a Doppler ultrasound scan of the cranialarteries, mainly the middle and anterior cerebralarteries. Alterations of cerebral hemodynamics in
Fetal Hydrocephalus: Surgical Treatment 3
fetuses with ventriculomegaly have been studiedusing this method. Gosling and King (1974) andPourcelot (1974) used Doppler ultrasound toestablish two indices better evaluate the obtainedwave: the pulsatility index (PI) and resistanceindex (RI).
Using animal hydrocephalic models andmeasuring the intracranial pressure (ICP) witha Camino optic fiber monitor and Doppler ultra-sound, Seibert et al. (1989) found a direct corre-lation between the ICP (cerebral perfusionpressure) and RI. The ratio between ventriculardilation and PI has been largely discussed inthe literature. Many studies suggest that a stableventriculomegaly is associated with a normal IP.Lui et al. (1990) described increased RIcorresponding to increased dilation of the ventri-cle, and its return to normality after ventricularshunting. Chadduck and Seibert (1989) founda mean RI of 0.84 in 46 newborn infants pre-senting with symptoms of progressive ventricu-lomegaly or hydrocephalus. After shunting, themean decreased to 0.72. Nishimaki et al. (1991)and Goh et al. (1991) found similar values andbelieved that any RI values above 0.8 in newborninfants and 0.65 in older children indicated theneed for shunting. A high resistance in the dia-stolic component may be directly associated withthe severity of the hydrocephalus because of theincrease in intracranial pressure.
Another imaging method contributing to ante-natal practice is fetal magnetic resonance imaging(MRI). However, MRI is subject to artifacts dueto movements of the fetus. Multiple reportshave confirmed that fetal MRI is a valuable andimportant adjunct to Ultrasound in a multitude offetal brain pathologies (Huisman 2008; Huismanet al. 2002).
Fetal MRI is better suited than ultrasonographywhen evaluating processes of maturation and neu-ronal myelination. It is also not affected by issuessuch as acoustic shadowing in the evaluation of thecerebral cortex as well as during the differentiationof brain tissues. High-resolution images and ultra-fast single-shot T2-weighted or half-Fourier single-shot turbo spin-echo (HASTE) sequences allow theinvestigation to be performed without the need forsedation of the fetus and are sufficiently precise to
allow for analysis of the fetal anatomy. The use ofgadolinium should be avoided, since the gadolin-ium will pass into the fetal circulation, be elimi-nated into the amniotic fluid via renal excretion,and return to the fetal circulation after deglutition.Thus, the elimination of gadolinium occurs veryslowly in the fetus. Small foci of intraventricularand intraparenchymal hemorrhages are also moreeasily detected by MRI than via ultrasonography.
Biochemical tests may contribute to differentdiagnoses that may be associated with a fetalhydrocephalus. Alpha fetal protein (AFP) is afetal glycoprotein synthesized at the level of thevitelline sac, which can be found in the gastroin-testinal tract and in the liver during intrauterine life.In 1972, Brock and Sutcliffe (1972) showed that ahigh concentration of AFP protein is found in theamniotic fluid in cases of defective closure of theneural tube. One year later, the same authors real-ized that a higher concentration of protein can befound not only in the amniotic fluid but also in thematernal blood in cases of open pathologies of theneural tube. However, they have demonstrated thatthis high concentration in the serum also occurredin other malformations, such as digestive atresia,isolated hydrocephaly, defective closure of theabdominal wall, congenital nephrotic syndrome,sacral teratomas, and also in cases of fetus-mothertransfusions and maternal obesity. A high concen-tration is also observed in 15% of individuals of theblack race. Acetylcholinesterase electrophoresis isa qualitative assay specific for open pathologies ofthe neural tube. However, in practice, it is seldomcarried out because it is difficult to perform.
With a view to enabling prognosis and possibleintrauterine treatment, blood tests of both themother and the fetus are necessary in addition tothe hydrocephalus diagnosis. The analysesshould include the study of congenital infectionsacquired during gestation as well as a study ofthe fetal karyotype. Cordocentesis should beperformed as a matter of routine before any clin-ical decision regarding treatment. However, theassociation of fetal hydrocephalus with congenitalinfection or chromosomopathy contraindicatesintrauterine therapeutic procedures.
In contrast to the development of treatmentdevices, technological progress improved the
4 S. Cavalheiro et al.

techniques allowing diagnosis of hydrocephaly.Today, tridimensional ultrasound, fetal MRI,Doppler ultrasound, serology, and tests for infec-tion and chromosomopathies have made diagno-sis almost as simple as if a physician could“look” directly into a woman’s womb.
Experimental Studies and NaturalHistory
It is difficult to study the natural history of fetalhydrocephaly considering the great variabilityof factors involved. Several researchers began todevelop experimental animal models. Their unan-imous belief is that the best results are obtainedfrom the most precocious intrauterine treatment ofhydrocephalus.
Nakayama et al. (1983) proposed an experi-mental model based on the injection of kaolininto the fetal cisterna magna of ewes and monkeysin order to produce obstructive hydrocephalus.From the results, they concluded that the cerebralgray matter is preserved whereas the white matteris undoubtedly damaged. They recommendeda precocious in utero treatment, before neuralnecrosis, gliosis, and axonal dystrophy makehydrocephalic lesions irreversible.
Michejda and Hodgen (1981) induced fetalhydrocephalus in rhesus monkeys by administ-ering endovenous injections of triamcinoloneacetamide to the mother. It became evident thatmonkeys that did not undergo ventriculoamnioticshunting had delayed intrauterine growth, muscu-lar changes with motor deficits, and frequentlyexperienced convulsive crises accompaniedby pulmonary and gastrointestinal disturbances,dying generally within a period of 10–14 daysafter birth. On the contrary, the monkeys treatedusing ventriculoamniotic shunts had normal intra-uterine growth and development and did notdie after birth. The authors concluded that fetalhydrocephalus can be successfully diagnosed andtreated in utero.
Edwards et al. (1984) studied 17 ewes and10 monkeys with congenital hydrocephalus pro-duced by the injection of silicone oil or kaolin.Antenatal ultrasound was used to record the
progressive course of ventriculomegaly. The cere-bral mantle of the animals became markedly thin-ner, with relative preservation of the cerebralcortex and severe reduction of the white matter.The gray matter cytoarchitecture remained nor-mal, while there was moderate gliosis in the sub-cortical white matter and in the corpus callosum. Itwas concluded that structural changes produced infetal hydrocephalus may be reversible, especiallyby virtue of the plasticity of the immature nervoussystem, and consequently ventriculoamnioticshunting is more efficient in establishing thisreversion to normality than postnatal shunting.The authors believe that cerebral changes of thehydrocephalic fetus may become irreversibleif they are just observed throughout the wholegestational period. Gupta et al. (1995) reviewed266 published cases of isolated ventriculomegalyin the literature. Out of these, 175 cases survived,40 cases were interrupted, and 51 patients diedafter birth. Out of those who survived, 63%presented with normal mental development; 11%presented with mild, 12% moderate, and 14%severe handicaps. Of these cases, 111 presentedwith mild stable ventriculomegaly. Cavalheiroet al. (2003) analyzed 39 patients with progressivehydrocephalus with no other associated severemalformations who received intrauterine treat-ment and found that 26 patients were considerednormal, i.e., with an IQ higher than 70, in follow-ups that ranged from 1 to 14 years of age.
Edwards (1986) emphasized that the difficultyin identifying isolated cases of hydrocephaluswithout associated anomalies may influence theresults. Although results obtained in animal stud-ies were encouraging, these results are not trans-ferable to humans. The issue lies in the correctidentification of cases which might benefit fromreceiving intrauterine treatment.
Experimental studies in animal models havedemonstrated that the earlier the treatment forfetal hydrocephalus is given, the greater efficacyit has. This type of result is not verified in dailyclinical practice due to the large variety of dis-eases a fetus may present with. In the case ofmalformative hydrocephalus, many patients pre-sent with multiple associated malformations,which compromise a good outcome (Chervenak
Fetal Hydrocephalus: Surgical Treatment 5

et al. 1984; Clark and Milhorat 1970; Edwardset al. 1984; Stein et al. 1981).
Etiology and Classification
Congenital hydrocephalus is one of the mostcommon congenital anomalies affecting the cen-tral nervous system and results from an imbalanceof CSF formation and absorption. This imbalanceresults in the accumulation of CSF, increased ICP,and dilation of the ventricles (Milhorat 1978; VonKoch et al. 2003).
In fetal ventricular dilatation, it is very impor-tant to differentiate between ventriculomegalyand hydrocephalus. Ventriculomegaly may bethe result of atrophy or hypoplasia of the centralnervous system or malformation associated withagenesis of the corpus callosum, while in hydro-cephalus the ventriculomegaly is hypertensive.It can be very difficult to differentiate betweenthe two conditions. In hydrocephalus, there isoften a decrease in the subarachnoid space anddangling of the choroid plexus. The angle formedbetween the wall of the ventricle and the choroidplexus is increased. In ventriculomegaly, onthe other hand, the subarachnoid space and cho-roid plexus are preserved (Pooh et al. 2003).Cavalheiro et al. (2003) reported the results from36 intrauterine treated fetuses and found that allthose that presented levels of intracranial pressureabove 20 cm H2O had a better cognitive andmotor development than those that presentedlow levels of intracranial pressure.
Ventriculomegaly may be “isolated” or part ofa syndrome. In addition, ventriculomegaly may bea complication of an intrauterine infection or hem-orrhage. A correct differentiation between thevarious etiologies of ventriculomegaly is essentialto predict outcome and to guide the varioustreatment options which may start as early asthe antenatal period (Huisman 2011). It is well-known that an isolated mild to moderate ventricu-lomegaly is linked to an abnormal outcome in10–20% of children, whereas ventriculomegalywith associated anomalies or as part of a complexsyndrome is characterized by an abnormal out-come in up to 40–50% of children (Bulas 2007).
The most frequently seen associated malfor-mation is myelomeningocele, with an incidenceof 25–30%. Cardiac, renal, and gastrointestinalabnormalities have an incidence of approximately7–15%. A quarter of associated anomalies arenot diagnosed before birth. Hereditary hydroceph-alus is rare and represents 3–10% of cases offetal hydrocephalus. Its diagnosis is importantfor genetic counseling for the couple. Bicker-Adams syndrome is characterized by hydroceph-alus linked to the long arm of the X chromosomein Xq28. Patients present with stenosis ofthe cerebral aqueduct, spasticity, severe mentalretardation, adducted thumbs, and hypoplasiaof the corpus callosum (Chervenak et al. 1984;Nicolaides et al. 1990; Vintzileos et al. 1987).
Ventriculomegaly is classified from mildto moderate if it measures between 10 mm and15 mm and severe if greater than 15 mm. Inthe group with mild and moderate ventricu-lomegaly, only 14% develop progressive hydro-cephalus, 57% are stable, and in 29% regressionoccurs spontaneously (Kelly et al. 2001). Mildventriculomegaly is often associated with othermalformations, such as cerebral hypoplasia, intra-ventricular hemorrhage, brain tumor, craniosyn-ostosis, and vein of Galen aneurysms. They maybe associated with chromosomal alterationsand infections such as rubella, cytomegalovirus,Coxsackie virus, toxoplasmosis, parvovirus, andZika virus among others. In the Pooh and Pooh(2009) series, all patients with intrauterine resolu-tion of ventriculomegaly had a favorable short-term prognosis.
Oi (2003) classifies hydrocephalus into threemajor categories:
1. Primary hydrocephalus, including communi-cating or noncomplicated hydrocephalus,aqueductal stenosis, foramen atresia, andothers.
2. Dysgenetic hydrocephalus, including hydro-cephalus with spina bifida, bifid cranium,Dandy-Walker cyst, holoprosencephaly,hydranencephaly, lissencephaly, congenitalcyst, and others.
3. Secondary hydrocephalus, hydrocephalus dueto brain tumor, hemorrhagic or other vascular
6 S. Cavalheiro et al.

disease(s), infection, trauma, subdural fluidcollection, and others.
After several years treating and monitoringfetuses with fetal hydrocephalus, we can say thatwhen facing a case of evolving acute hydroceph-alus without other associated malformations,intrauterine procedures can be beneficial.
Twin Gestation
In face of a twin gestation in which both fetusespresent with hydrocephalus, the process is uni-form, and both fetuses can be treated with thesame protocol. However, it is more common foronly one of the twins to present with hydroceph-alus. Termination is impracticable and any fetalsurgery procedure might mean a risk to the normalfetus.
Earlier delivery after confirmation of lungmaturity becomes the choice procedure. When atwin gestation is carried to term and one of thefetuses would typically present with a voluminousmacrocranium, cephalocentesis, and removal oflarge quantities of liquor are indicated to facilitatechildbirth. It is most remarkable that sometimesonly one of the fetuses is affected despite theinfectious origin of the fetal hydrocephalus,Fig. 1.
Surgical Approaches
Liley (1963) was the first to inject blood into theperitoneal cavity of a 32-week-old fetus affectedby Rh isoimmunization. The fetus had a goodoutcome and this case was the initial milestonefor fetal surgery. Kellner et al. (1980) diagnosedhydrocephaly in a 33-week-old fetus and per-formed a gaseous fetal ventriculography todetermine the thickness of the cerebral cortex,which measured less than 10 mm. Having optedfor vaginal delivery, they performed a trans-abdominal fetal cephalocentesis to avoid dystociaand drained 1200 ml of liquor. This provedinsufficient. A transvaginal ventricular puncturefollowed and an additional 700 ml of liquor was
drained. Stenosis of the cerebral aqueduct wasrevealed following autopsy.
Birnholz and Frigoletto (1981) used repeatedcephalocentesis in a hydrocephalic 25-week fetus,performing six ultrasound-guided transabdominalpunctures. The volume of drained liquor variedbetween 40 and 180 ml. The ultrasonographicseries showed a decrease in the ventricularcavity and increase in the cortical thickness. At34 weeks’ gestation, a caesarean section tookplace and the infant was born in good condition.After birth, computed tomography of the newborninfant’s brain revealed an asymmetric hydroceph-alus with the presence of a posterior cyst inthe midline and absence of the corpus callosum.There was no evidence of intracranial hemor-rhage. A ventriculoperitoneal shunt was placed,but the child’s development was retarded andassociated with convulsive crises. A muscularbiopsy revealed Becker’s muscular dystrophy.
It has been accepted that cephalocentesis isan effective method of helping hydrocephalicchildren achieve better outcomes. Clewell et al.(1982) described the first ventriculoamnioticshunt performed on a 24-week-old fetus, whichwas effective until the 32nd week of gestationwhen a caesarean section was performed. Thenewborn infant subsequently underwent ventricu-loperitoneal shunting. In the follow-up, neuro-psychomotor development was compromised,though somewhat improved by physiotherapy.
Frigoletto et al. (1982) described the insertionof a ventriculoamniotic shunt in a 24-week-oldfetus. Three attempts had to be made in order tomaintain the shunt. The first valve was lost in themother’s abdominal cavity during the procedure,the second one proved ineffective, and the thirdtime a multiperforated silicone tube without avalve was placed. Ten days after the final proce-dure, i.e., 28 weeks into the pregnancy, laborstarted and the mother underwent a caesareansection. The infant had a safe delivery, withApgar scores of 8 and 9. Later the infant’s clinicalstate declined and death occurred 5.5 weeks afterbirth.
The following prerequisites have been pro-posed for in utero shunting to be considereda viable procedure:
Fetal Hydrocephalus: Surgical Treatment 7
1. Hydrocephaly should be diagnosed at an earlystage of gestation.
2. It should not be associated with othermalformations.
3. A karyotypic study should be performed in allcases.
4. Ventricular dilatation should be progressive.5. The treatment should be managed by a multi-
disciplinary team comprising specialists inperinatology, ultrasonography, obstetrics, neu-rosurgery, and genetics.
Michejda et al. (1986) reported the resultsat the Second Meeting of the Fetal Medicine
Society, which justified the establishment of thefollowing criteria for fetal treatment: ultrasonog-raphy, amniocentesis to provide material for kar-yotypic study, acetylcholinesterase and/or AFPdosage, viral culture, all with the family’s consent.Specific criteria for treatment of fetal hydroceph-aly were given as ventriculomegaly without evi-dence of multiple associated malformations, earlydiagnosis (before the 30th week of gestation),ultrasonographic evidence of increased ventricu-lar size and decreased cerebral mantle, single ges-tation, and the mother’s consent. For surgery,a high-risk obstetric unit is required, as well asavailable access to several different specialties,
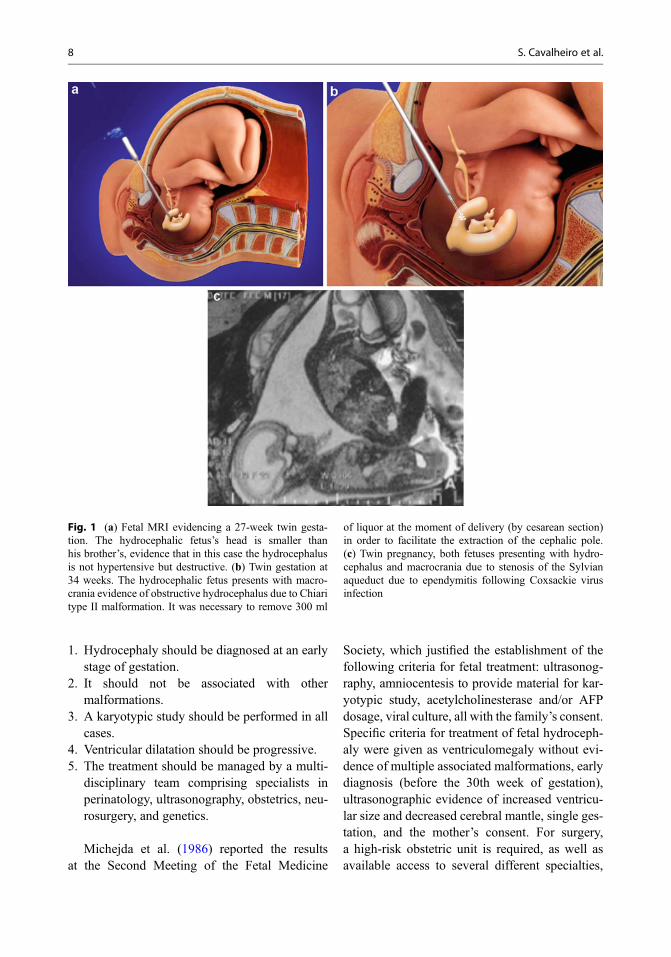
Fig. 1 (a) Fetal MRI evidencing a 27-week twin gesta-tion. The hydrocephalic fetus’s head is smaller thanhis brother’s, evidence that in this case the hydrocephalusis not hypertensive but destructive. (b) Twin gestation at34 weeks. The hydrocephalic fetus presents with macro-crania evidence of obstructive hydrocephalus due to Chiaritype II malformation. It was necessary to remove 300 ml
of liquor at the moment of delivery (by cesarean section)in order to facilitate the extraction of the cephalic pole.(c) Twin pregnancy, both fetuses presenting with hydro-cephalus and macrocrania due to stenosis of the Sylvianaqueduct due to ependymitis following Coxsackie virusinfection
8 S. Cavalheiro et al.

such as an obstetrician skilled in fetal blood trans-fusion, a pediatric neurosurgeon, a neonatal pedi-atric surgeon, a geneticist, a neonatalanesthesiologist, and a neonatologist.
Forty-four human fetuses diagnosed withhydrocephaly were treated with ventricu-loamniotic shunts. There were eight deaths, fourof which were as a direct consequence of thesurgical intervention. The follow-up showedthat 12 of the survivors were normal, 6 had milddeficits, while 18 had severe deficits associatedwith other malformations of the central nervoussystem. The authors’ conclusion was that hydro-cephaly can be successfully treated in utero, buta better option might be hysterotomy, to preventdisplacement of the shunt.
Manning et al. (1986) described the resultsof the “International Fetal Surgery Registry.”In terms of fetal hydrocephalus, 25 fetuses under-going ventriculoamniotic shunting had been reg-istered by June 1983. There were sufficient dataavailable to permit evaluation in only 19 of thesecases: 13 had aqueductal stenosis, three had mul-tiple anomalies, one had holoprosencephaly,one had a Chiari II malformation, and onehad a Dandy-Walker malformation. Four of the19 fetuses died during or after the shunting pro-cedure. Seven of the survivors had normal devel-opment and eight had either a mild or severehandicap. In view of such results, many medicalcenters decided against the provision of intrauter-ine treatments. Consequently, new techniques forthe fetal treatment of hydrocephaly, such as newvalves for ventriculoamniotic shunts, have notbeen developed. As of 1986, practically allmedical centers had discontinued in uterointerventions.
Cavalheiro et al. (2003) described the first fetalthird ventriculostomy in 2003 and Bruner et al.(2001) presented four cases of ventriculoamnioticshunting using open surgery. However, progressin the treatment of fetal hydrocephalus has beenpoor. Reverting ventriculomegaly does not lead toa reversal of the devastating effects already causedby hydrocephalus and not even of those caused bythe associated malformation. Although diagnosesof fetal malformations have improved duringthe last few years, the same improvement has not
been seen in surgical techniques for the treatmentof hydrocephalus. Surgical options include littlemore than cephalocentesis, which consist of mul-tiple ventricular punctures in order to removeliquor, and ventriculoamniotic shunts, which pro-vide a fast decrease in the volume of the ventric-ular cavity, but often migrate into either theventricular or the uterine cavities.
As yet, there are no drainage systems thatcan be placed percutaneously and fixed on theskin of the fetus that might be performed withopen surgery. Fetal neuroendoscopy is feasiblebut technically very difficult because the fetusis seldom in a position that permits the surgeonto reach Kocher’s point and perform the proce-dure. Neuroendoscope procedures in fetuses andnewborns are most complicated because theLilequist membrane is too detached from thetuber cinereum at that age. For the procedure tobe successful, it is necessary to open both mem-branes, which sometimes becomes very difficultin utero (Buxton et al. 1998; Gorayeb et al. 2004).
Neuroendoscopic procedures have beenattempted three times, and in only one case itwas effective. Furthermore, the authors are notunanimous over whether neuroendoscopic proce-dures are as effective in newborns as they arewhen performed after the first year of life, whichcauses doubt about the convenience of performingfetal endoscopic third ventriculostomy.
Bruner et al. (2001) at Vanderbilt Universityconducted fourth ventriculoperitoneal shunts infetuses with progressive hydrocephalus, macro-cephaly, and progressive increase of the lateralventricles greater than 1.5 mm/week. Gestationalage ranged from 23 to 26 weeks. All fetuses werediagnosed with Sylvian aqueduct stenosis as eval-uated through MRI and ultrasonography andinfection frames were excluded. The procedureswere performed through hysterotomy. No benefitfor the fetus was found in any of the cases. Recentdevelopments in fetal imaging and moleculargenetics have not improved the selection ofcases that may benefit from fetal surgery.
The most developed surgical technique is inutero correction of myelomeningocele by opensurgery, although it is not used as a treatment butin prevention of fetal hydrocephalus. A
Fetal Hydrocephalus: Surgical Treatment 9
randomized trial of prenatal versus postnatalrepair of myelomeningocele has shown thatwhen the myelomeningocele is repaired beforethe 26th gestational week, shunting after birthis only required in 40% of cases. Whenmyelomeningocele is treated only after birth,shunting is required in 82% of cases. Furthermore,the cases treated in utero had considerable motorgains (Adzick et al. 2011). From 2011 to 2016, weoperated on 186 fetuses with myelomeningoceleand a gestational age of less than 27 weeks, usingthe same technique proposed by MOMS, withminor variations. Out of the 186 cases, shuntplacement was necessary in 10 (5.4%).
We were able to utilize essentially four differ-ent techniques to treat fetal hydrocephalus:
1. Repeated cephalocentesis2. Amniotic ventricle derivations3. Endoscopic third ventriculostomy4. Open Fetal Ventriculoamniotic Shunting.
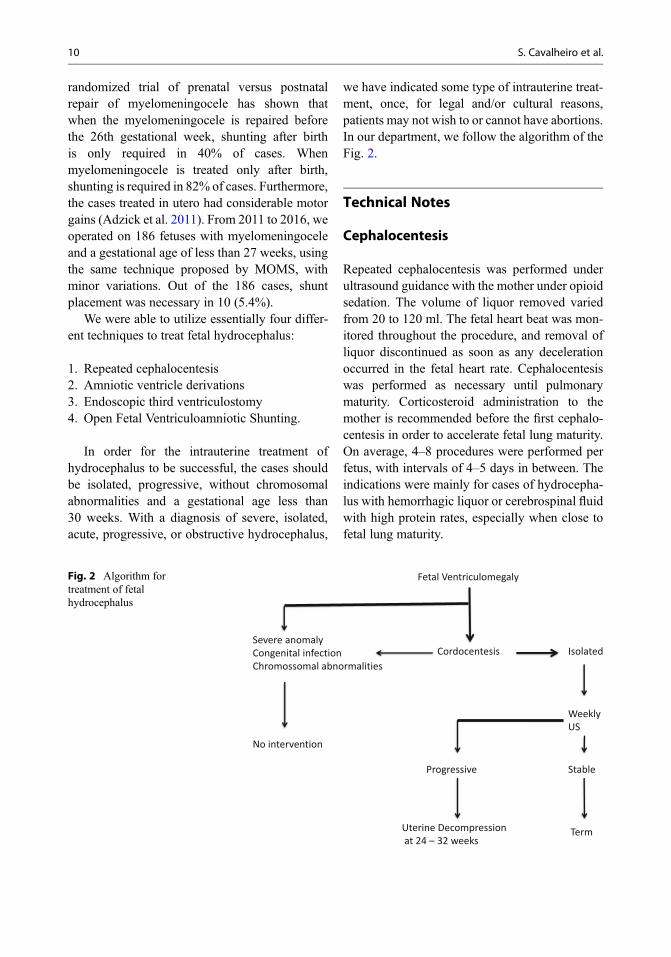
In order for the intrauterine treatment ofhydrocephalus to be successful, the cases shouldbe isolated, progressive, without chromosomalabnormalities and a gestational age less than30 weeks. With a diagnosis of severe, isolated,acute, progressive, or obstructive hydrocephalus,
we have indicated some type of intrauterine treat-ment, once, for legal and/or cultural reasons,patients may not wish to or cannot have abortions.In our department, we follow the algorithm of theFig. 2.
Technical Notes
Cephalocentesis
Repeated cephalocentesis was performed underultrasound guidance with the mother under opioidsedation. The volume of liquor removed variedfrom 20 to 120 ml. The fetal heart beat was mon-itored throughout the procedure, and removal ofliquor discontinued as soon as any decelerationoccurred in the fetal heart rate. Cephalocentesiswas performed as necessary until pulmonarymaturity. Corticosteroid administration to themother is recommended before the first cephalo-centesis in order to accelerate fetal lung maturity.On average, 4–8 procedures were performed perfetus, with intervals of 4–5 days in between. Theindications were mainly for cases of hydrocepha-lus with hemorrhagic liquor or cerebrospinal fluidwith high protein rates, especially when close tofetal lung maturity.
Fetal Ventriculomegaly
CordocentesisSevere anomalyCongenital infectionChromossomal abnormalities
No intervention
Isolated
Weekly US
Progressive Stable
Uterine Decompressionat 24 – 32 weeks
Term
Fig. 2 Algorithm fortreatment of fetalhydrocephalus
10 S. Cavalheiro et al.

Ventriculoamniotic Shunting
Ventriculoamniotic shunting was performedpercutaneously under ultrasound guidance, anda pigtail catheter (KCH-Rocket Medical PLC,New England) was inserted. One tip of the cathe-ter was left in the fetal lateral ventricle and theother in the amniotic cavity, Fig. 3.
Third Ventriculostomy
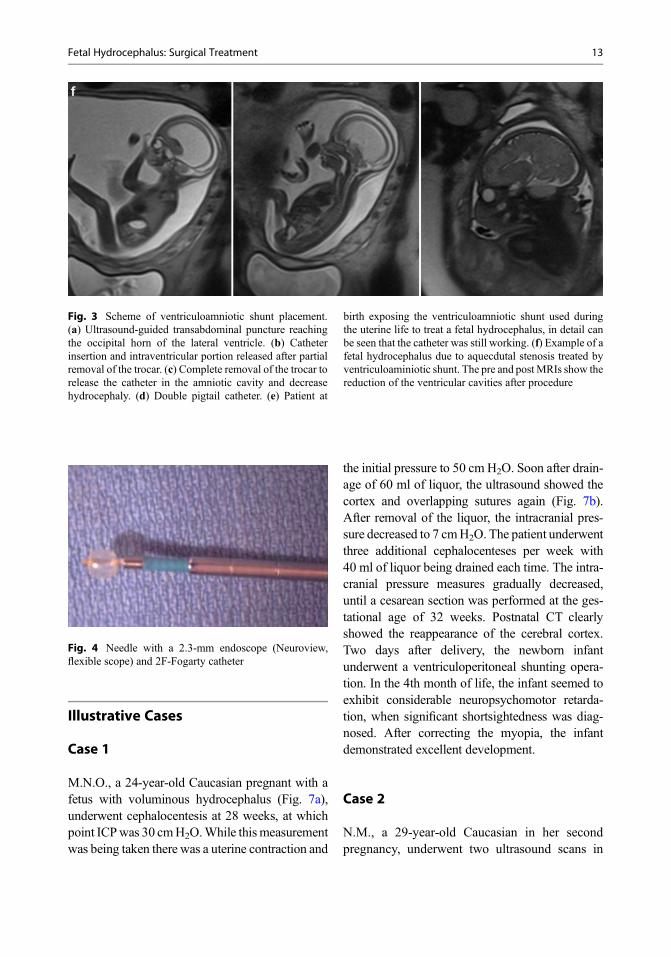
Third ventriculostomy was performed underfetal anesthesia. Always under ultrasound guid-ance, the umbilical cord was punctured with athin needle, the umbilical vein catheterized, anda total dose of 5 μg/kg of fentanyl citrate and0.1 mg/kg pancuronium bromide was adminis-tered. Five minutes after fetal anesthesia, a smallincision was made in the mother’s abdominalskin with an 11-blade scalpel. Again, underultrasound guidance, the fetal skull was punc-tured with a 2.5-mm-diameter needle on thebrim of the bregmatic fontanelle, providingaccess to the lateral ventricle. As soon asthe mandrel was withdrawn, liquor exitedunder increased pressure. A 2.3-mm-diameterneuroendoscope (Neuroview, flexible scope,25C, Traatek, USA) was inserted through theneedle, as well as a 1 mm working channelconnected to a 300 W xenon lighting system.Monro’s foramen could be identified and theendoscope was inserted into the third ventricle,its floor was opened, and the fetal basilar arterycould be visualized. The opening was suffi-ciently enlarged with a 2-Fr Fogarty catheter,and the endoscope was withdrawn along withthe needle (Fig. 4). A small occlusive dressingwas applied to the mother’s abdomen.
Open Surgery for Intrauterine Repairfor Myelomeningocele
After the publication of the results fromthe Myelomeningocele Management Study(MOMS), by Adzick et al. (2011), we began to
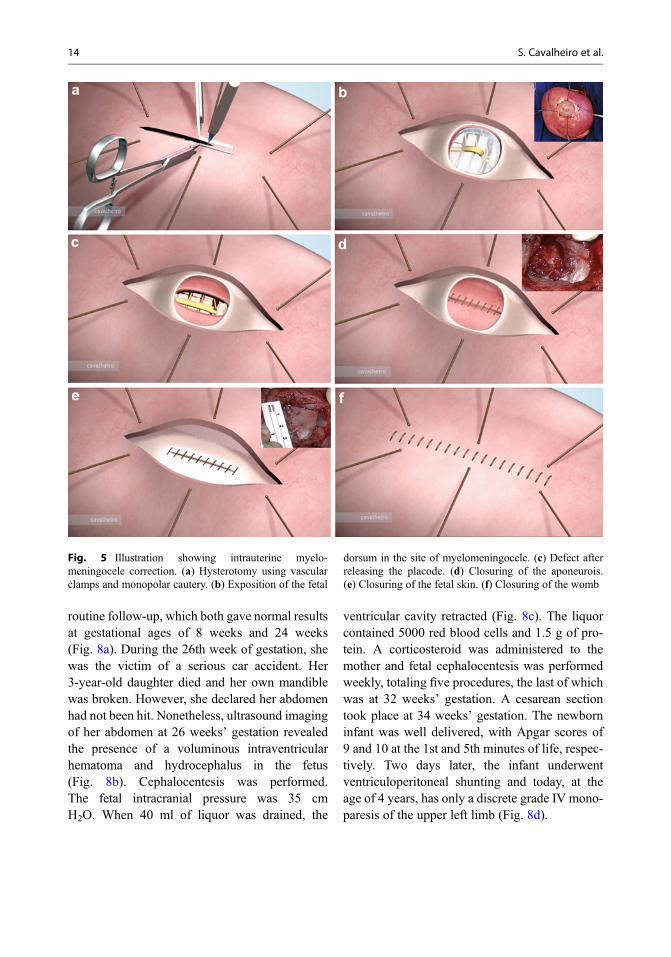
perform the same procedure in our department.During this period, we performed 186 open fetalsurgeries to treat fetal myelomeningocele. Thetechnique that we used consisted of opening theabdominal wall (extended Pfannenstiel incision),removing the uterus from the abdominal cavity,detailed mapping of the placental location, andidentification of fetal body parts and the umbilicalcord through intraoperative ultrasonography.A median longitudinal hysterotomy of approxi-mately 5 cm long was performed on the contralat-eral uterine wall to placental insertion usingelectrocautery and De Bakey vascular clamps. Inorder to avoid bleeding and lacerations of theamniotic membrane, a continuous suture was car-ried out using Vycril 0 around the entire uterineopening involving the amnion membrane andmyometrium layer. The dorsal region of the fetuswas positioned at the site of uterine opening andthe myelomeningocele was closed in three planes:dura mater, aponeurosis, and skin. Before theclosing of the dura mater, the placode wasreleased and tunneled. The entire procedure wasperformed using a microscope or magnifyingglass. The uterine closure was performed in threeplanes: continuous suture of the amnion mem-brane and myometrium layer with monocryl 4-0,continuous suture of the myometrium layerwith Vicryl 2-0, and interrupted sutures of themyometrium layer with Vicryl 0 (Figs. 5 and 6).The patient was hospitalized on average from 5 to6 days, treated with medications in order to pre-vent preterm labor, and was monitored for fetalwell-being and maternal clinical picture.
After discharge, a weekly outpatient follow-upwas conducted in order to monitor the followingfactors: fetal growth and vitality, degree ofherniation of the brain stem (assess reversal ofbrainstem), measurement of the lateral ventriclesof the brain, fetal scarring and aspects of the lowerlimbs, and characteristics of the uterine scar. Themode of delivery was cesarean section. Whencomparing our results with postnatal and prenatalsurgeries, shunt placement rate varied from 86%to 5.4%, respectively, confirming that in uterocorrection of myelomeningocele prevents postna-tal hydrocephalus.
Fetal Hydrocephalus: Surgical Treatment 11
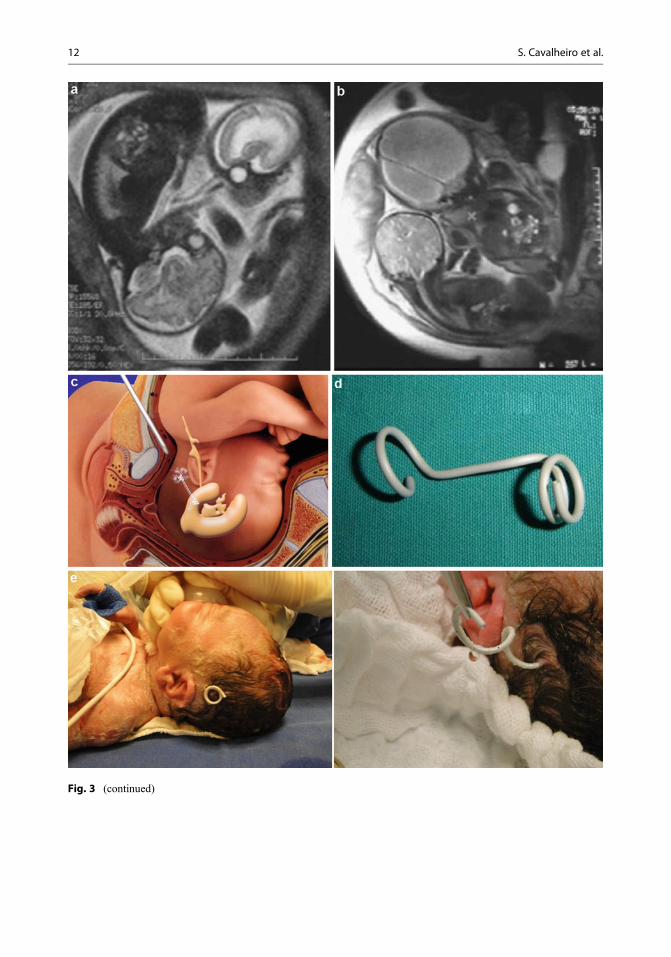
Fig. 3 (continued)
12 S. Cavalheiro et al.
Illustrative Cases
Case 1
M.N.O., a 24-year-old Caucasian pregnant with afetus with voluminous hydrocephalus (Fig. 7a),underwent cephalocentesis at 28 weeks, at whichpoint ICPwas 30 cmH2O.While this measurementwas being taken there was a uterine contraction and
the initial pressure to 50 cm H2O. Soon after drain-age of 60 ml of liquor, the ultrasound showed thecortex and overlapping sutures again (Fig. 7b).After removal of the liquor, the intracranial pres-sure decreased to 7 cmH2O. The patient underwentthree additional cephalocenteses per week with40 ml of liquor being drained each time. The intra-cranial pressure measures gradually decreased,until a cesarean section was performed at the ges-tational age of 32 weeks. Postnatal CT clearlyshowed the reappearance of the cerebral cortex.Two days after delivery, the newborn infantunderwent a ventriculoperitoneal shunting opera-tion. In the 4th month of life, the infant seemed toexhibit considerable neuropsychomotor retarda-tion, when significant shortsightedness was diag-nosed. After correcting the myopia, the infantdemonstrated excellent development.
Case 2
N.M., a 29-year-old Caucasian in her secondpregnancy, underwent two ultrasound scans in
Fig. 3 Scheme of ventriculoamniotic shunt placement.(a) Ultrasound-guided transabdominal puncture reachingthe occipital horn of the lateral ventricle. (b) Catheterinsertion and intraventricular portion released after partialremoval of the trocar. (c) Complete removal of the trocar torelease the catheter in the amniotic cavity and decreasehydrocephaly. (d) Double pigtail catheter. (e) Patient at
birth exposing the ventriculoamniotic shunt used duringthe uterine life to treat a fetal hydrocephalus, in detail canbe seen that the catheter was still working. (f) Example of afetal hydrocephalus due to aquecdutal stenosis treated byventriculoaminiotic shunt. The pre and post MRIs show thereduction of the ventricular cavities after procedure
Fig. 4 Needle with a 2.3-mm endoscope (Neuroview,flexible scope) and 2F-Fogarty catheter
Fetal Hydrocephalus: Surgical Treatment 13
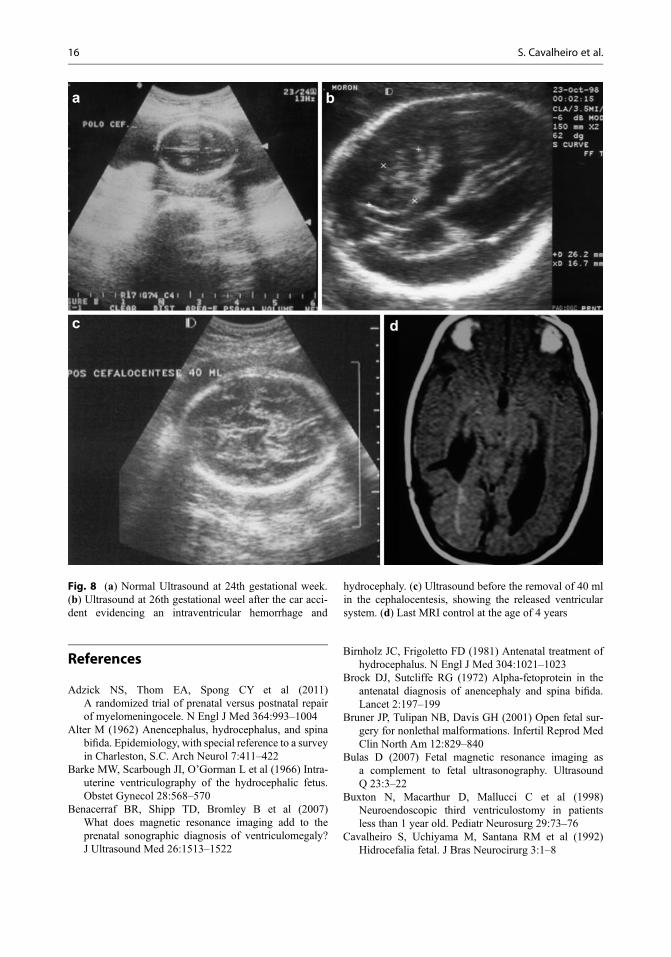
routine follow-up, which both gave normal resultsat gestational ages of 8 weeks and 24 weeks(Fig. 8a). During the 26th week of gestation, shewas the victim of a serious car accident. Her3-year-old daughter died and her own mandiblewas broken. However, she declared her abdomenhad not been hit. Nonetheless, ultrasound imagingof her abdomen at 26 weeks’ gestation revealedthe presence of a voluminous intraventricularhematoma and hydrocephalus in the fetus(Fig. 8b). Cephalocentesis was performed.The fetal intracranial pressure was 35 cmH2O. When 40 ml of liquor was drained, the
ventricular cavity retracted (Fig. 8c). The liquorcontained 5000 red blood cells and 1.5 g of pro-tein. A corticosteroid was administered to themother and fetal cephalocentesis was performedweekly, totaling five procedures, the last of whichwas at 32 weeks’ gestation. A cesarean sectiontook place at 34 weeks’ gestation. The newborninfant was well delivered, with Apgar scores of9 and 10 at the 1st and 5th minutes of life, respec-tively. Two days later, the infant underwentventriculoperitoneal shunting and today, at theage of 4 years, has only a discrete grade IV mono-paresis of the upper left limb (Fig. 8d).
Fig. 5 Illustration showing intrauterine myelo-meningocele correction. (a) Hysterotomy using vascularclamps and monopolar cautery. (b) Exposition of the fetal
dorsum in the site of myelomeningocele. (c) Defect afterreleasing the placode. (d) Closuring of the aponeurois.(e) Closuring of the fetal skin. (f) Closuring of the womb
14 S. Cavalheiro et al.
Conclusion
Thirty years after the first in utero procedurefor the treatment of fetal hydrocephalus, littleprogress has been made with respect to the neu-rosurgical techniques for the management of thatdisease during the gestational period. Diagnostictechniques have improved vastly and we nowhave a better ability to evaluate cases of fetal
hydrocephalus and associated malformationsof the central nervous system. We believe thatin utero fetal procedures should be performedin cases of acute instances of evolving butnondestructive hydrocephaly without any otherassociated malformation. Procedures to preventhydrocephalus, such as closure of myelomening-oceles in fetuses before the 26th gestational week,should be encouraged.
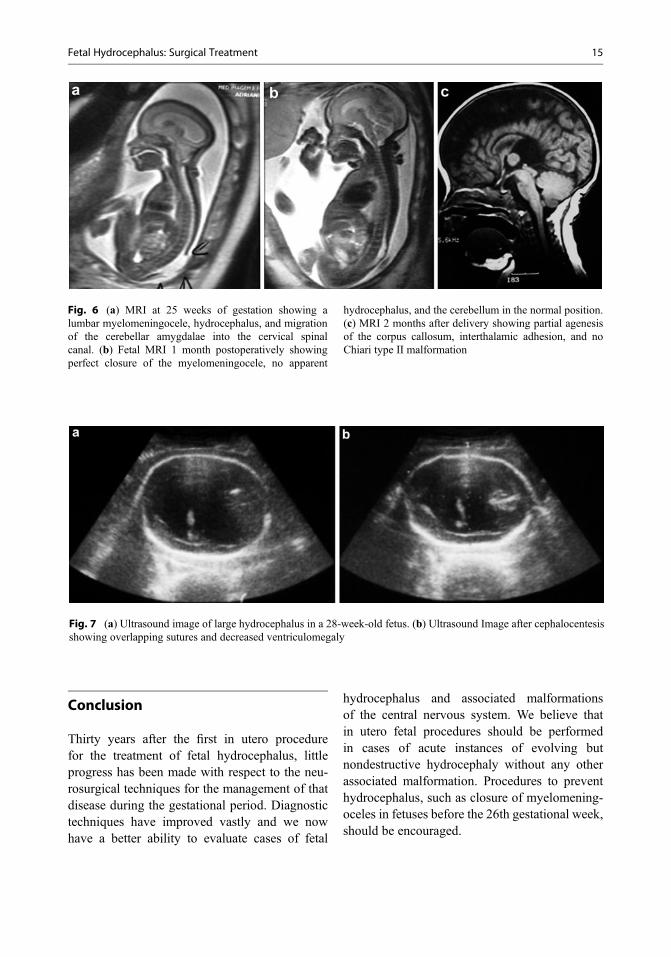
Fig. 6 (a) MRI at 25 weeks of gestation showing alumbar myelomeningocele, hydrocephalus, and migrationof the cerebellar amygdalae into the cervical spinalcanal. (b) Fetal MRI 1 month postoperatively showingperfect closure of the myelomeningocele, no apparent
hydrocephalus, and the cerebellum in the normal position.(c) MRI 2 months after delivery showing partial agenesisof the corpus callosum, interthalamic adhesion, and noChiari type II malformation
Fig. 7 (a) Ultrasound image of large hydrocephalus in a 28-week-old fetus. (b) Ultrasound Image after cephalocentesisshowing overlapping sutures and decreased ventriculomegaly
Fetal Hydrocephalus: Surgical Treatment 15
References
Adzick NS, Thom EA, Spong CY et al (2011)A randomized trial of prenatal versus postnatal repairof myelomeningocele. N Engl J Med 364:993–1004
Alter M (1962) Anencephalus, hydrocephalus, and spinabifida. Epidemiology, with special reference to a surveyin Charleston, S.C. Arch Neurol 7:411–422
Barke MW, Scarbough JI, O’Gorman L et al (1966) Intra-uterine ventriculography of the hydrocephalic fetus.Obstet Gynecol 28:568–570
Benacerraf BR, Shipp TD, Bromley B et al (2007)What does magnetic resonance imaging add to theprenatal sonographic diagnosis of ventriculomegaly?J Ultrasound Med 26:1513–1522
Birnholz JC, Frigoletto FD (1981) Antenatal treatment ofhydrocephalus. N Engl J Med 304:1021–1023
Brock DJ, Sutcliffe RG (1972) Alpha-fetoprotein in theantenatal diagnosis of anencephaly and spina bifida.Lancet 2:197–199
Bruner JP, Tulipan NB, Davis GH (2001) Open fetal sur-gery for nonlethal malformations. Infertil Reprod MedClin North Am 12:829–840
Bulas D (2007) Fetal magnetic resonance imaging asa complement to fetal ultrasonography. UltrasoundQ 23:3–22
Buxton N, Macarthur D, Mallucci C et al (1998)Neuroendoscopic third ventriculostomy in patientsless than 1 year old. Pediatr Neurosurg 29:73–76
Cavalheiro S, Uchiyama M, Santana RM et al (1992)Hidrocefalia fetal. J Bras Neurocirurg 3:1–8
Fig. 8 (a) Normal Ultrasound at 24th gestational week.(b) Ultrasound at 26th gestational weel after the car acci-dent evidencing an intraventricular hemorrhage and
hydrocephaly. (c) Ultrasound before the removal of 40 mlin the cephalocentesis, showing the released ventricularsystem. (d) Last MRI control at the age of 4 years
16 S. Cavalheiro et al.
Cavalheiro S, Sparapani FV, Moron AF et al (2002)Fetal meningeal hemangiopericytoma. Case report.J Neurosurg 97:1217–1220
Cavalheiro S, Moron AF, Zymberg ST et al (2003) Fetalhydrocephalus – prenatal treatment. Childs Nerv Syst19:561–573
Cavalheiro S, Lopez A, Serra S et al (2016) Microcephalyand Zika virus: neonatal neuroradiological aspects.Childs Nerv Syst 32:1057
Chadduck WM, Seibert JJ (1989) Intracranial duplexDoppler: practical uses in pediatric neurology and neu-rosurgery. J Child Neurol 4(Suppl):S77–S86
Chervenak FA, Duncan C, Ment LR et al (1984) Outcomeof fetal ventriculomegaly. Lancet 2:179–181
Clark RG, Milhorat TH (1970) Experimental hydrocepha-lus. 3. Light microscopic findings in acute and subacuteobstructive hydrocephalus in the monkey. J Neurosurg32:400–413
Clewell WH, Johnson ML, Meier PR et al (1982) A surgi-cal approach to the treatment of fetal hydrocephalus.N Engl J Med 306:1320–1325
Cochrane DD, Myles ST, Nimrod C et al (1985) Intrauter-ine hydrocepahlus associated abnormalities and fetaloutcome. Can J Neurol Sci 12:51–59
Coffey VP, Jessop WJ (1955) Congenital abnormalities.Ir J Med Sci 349:30–48
Dill P, Poretti A, Boltshauser E et al (2009) Fetal magneticresonance imaging in midline malformations of thecentral nervous system and review of the literature.J Neuroradiol 36:138–146
Edwards MS (1986) An evaluation of the in utero neuro-surgical treatment of ventriculomegaly. Clin Neurosurg33:347–357
Edwards MS, Harrison MR, Halks-Miller M et al (1984)Kaolin-induced congenital hydrocephalus in utero infetal lambs and rhesus monkeys. J Neurosurg 60:115–122
Feeney JK, Barry AP (1954) Hydrocephaly as a cause ofmaternal mortality and morbidity; a clinical study of304 cases. J Obstet Gynaecol Br Emp 61:652–656
Frigoletto FD Jr, Birnholz JC, GreeneMF (1982) Antenataltreatment of hydrocephalus by ventriculoamnioticshunting. JAMA 248:2496–2497
Garel C (2005) Fetal cerebral biometry: normal paren-chymal findings and ventricular size. Eur Radiol15:809–813
Goh D, Minns RA, Pye SD (1991) Transcranial Doppler(TCD) ultrasound as a noninvasive means of monitor-ing cerebrohaemodynamic change in hydrocephalus.Eur J Pediatr Surg 1(Suppl 1):14–17
Gorayeb RP, Cavalheiro S, Zymberg ST (2004) Endo-scopic third ventriculostomy in children younger than1 year of age. J Neurosurg 100:427–429
Gosling H, King DH (1974) Continuous wave ultrasoundas an alternative and complement to X-ray in vascularexamination. In: Reneman RS (ed) Cardiovascularapplication of ultrasound. Elsevier, New York,pp 266–282
Gupta JK, Bryce FC, Lilford RJ (1995) Assessment andmanagement of fetal ventriculomegaly and other asso-ciated congenital anomalies. In: Levene MI, Lilford RJ(eds) Fetal and neonatal neurology and neurosurgery.Churchill Livingstone, Edinburgh, pp 215–230
Huisman TA (2008) Fetal magnetic resonance imaging.Semin Roentgenol 43:314–336
Huisman TA (2011) Fetal magnetic resonance imaging ofthe brain: is ventriculomegaly the tip of the syndromaliceberg? Semin Ultrasound CT MR 32:491–509
Huisman TA, Martin E, Kubik-Huch R et al (2002) Fetalmagnetic resonance imaging of the brain: technicalconsiderations and normal brain development. EurRadiol 12:1941–1951
Jeanty P, Dramaix-Wilmet M, Delbeke D et al (1981)Ultrasonic evaluation of fetal ventricular growth.Neuroradiology 21:127–131
Kellner KR, Cruz AC, Gelman SR et al (1980) Percutane-ous fetal ventriculography: a simplified technique to aidin management of the hydrocephalic fetus. J ReprodMed 24:225–228
Kelly EN, Allen VM, Seaward G et al (2001) Mildventriculomegaly in the fetus, natural history, associ-ated findings and outcome of isolated mild ventricu-lomegaly: a literature review. Prenat Diagn 21:697–700
Leidig E, Dannecker G, Pfeiffer KH et al (1988) Intrauter-ine development of posthaemorrhagic hydrocephalus.Eur J Pediatr 147:26–29
Levine D, Trop I, Mehta TS et al (2002) MR imagingappearance of fetal cerebral ventricular morphology.Radiology 223:652–660
Liley AW (1963) Intrauterine transfusion of foetus inhaemolytic disease. Br Med J 2:1107–1109
Lorber J (1961) Systematic ventriculographic studiesin infants born with meningomyelocele and encephalo-cele. The incidence and development of hydrocephalus.Arch Dis Child 36:381–389
Lui K, Hellmann J, Sprigg A et al (1990) Cerebral blood-flow velocity patterns in post-hemorrhagic ventriculardilation. Childs Nerv Syst 6:250–253
Malpas P (1937) The incidence of human malformationsand the significance of changes in the maternal envi-ronment in the causation. J Obstet Gynaecol Br Emp44:434–438
Manning FA, Harrison MR, Rodeck C (1986) Cathetershunts for fetal hydronephrosis and hydrocephalus.Report of the International Fetal Surgery Registry.N Engl J Med 315:336–340
Michejda M, Hodgen GD (1981) In utero diagnosis andtreatment of non-human primate fetal skeletal anoma-lies. I. Hydrocephalus. JAMA 246:1093–1097
Michejda M, Queenan JT, Mccullough D (1986) Presentstatus of intrauterine treatment of hydrocephalus and itsfuture. Am J Obstet Gynecol 155:873–882
Milhorat TH (1978) Hydrocephalus. In: Plum F,McDowell FH (eds) Pediatric neurosurgery.F.A. Davis Company, Philadelphia, pp 91–135
Nakayama DK, Harrison MR, Berger MS et al (1983)Correction of congenital hydrocephalus in utero
Fetal Hydrocephalus: Surgical Treatment 17
I. Themodel: intracisternal kaolin produces hydroceph-alus in fetal lambs and rhesus monkeys. J Pediatr Surg18:331–338
Nicolaides KH, Berry S, Sniiders RJM et al (1990)Fetal lateral cerebral ventriculomegaly: associatedmalformations and chromosomal defects. Fetal DiagnTher 5:5–14
Nishimaki S, Kawakami T, Akamatsu H et al (1991)Cerebral blood flow velocities in the anterior cerebralarteries and basilar artery. III. Investigation in hydro-cephalus (Part 2). No To Hattatsu 23:560–566
Nomura ML, Barini R, De Andrade KC et al (2010)Congenital hydrocephalus: gestational and neonataloutcomes. Arch Gynecol Obstet 282:607–611
Oi S (2003) Diagnosis, outcome, and management of fetalabnormalities: fetal hydrocephalus. Childs Nerv Syst19:508–516
Pooh RH, Pooh KH (2009) Antenatal assessmentof CNS anomalies, including neural tube defects.In: Levene MI, Chervenak FA (eds) Fetal and neonatalneurology and neurosurgery. Elsevier, Edinburgh,pp 291–337
Pooh RK, Maeda K, Pooh KH (2003) An atlas of fetalcentral nervous system disease. In: Diagnosis and man-agement. Parthenon CRC, London
Pourcelot L (1974) Applications cliniques de L’examenDoppler transcutané. In: Peroneal P (ed) Velocimetreultrasonore Doppler. Inserm, Paris, pp 213–240
Prata-Martins JA, Diegoli MSC, Diegoli CA et al (1985)Conduta obstétrica e prognóstico da hidrocefalia.Ginecol Obstet Bras 8:195–201
Seibert JJ, Mccowan TC, Chadduck WM et al (1989)Duplex pulsed Doppler US versus intracranial pressurein the neonate: clinical and experimental studies.Radiology 171:155–159
Stein SC, Feldman JG, Apfel S et al (1981) Theepidemiology of congenital hydrocephalus. A study inBrooklyn, N.Y. 1968–1976. Childs Brain 8:253–262
Vintzileos AM, Campbell WA, Weinbaum PJ et al (1987)Perinatal management and outcome of fetal ventricu-lomegaly. Obstet Gynecol 69:5–11
Von Koch CS, Gupta N, Sutton LN et al (2003) In uterosurgery for hydrocephalus. Childs Nerv Syst 19:574–586
18 S. Cavalheiro et al.