Female Urinary Incontinence Dr Ida Mah Specialist in Urology Hong Kong Urology Clinic Pedder Street,...
80
Female Urinary Incontinence Dr Ida Mah Specialist in Urology Hong Kong Urology Clinic Pedder Street, Central Hong Kong
-
Upload
shauna-scott -
Category
Documents
-
view
226 -
download
0
Transcript of Female Urinary Incontinence Dr Ida Mah Specialist in Urology Hong Kong Urology Clinic Pedder Street,...

Female Urinary Incontinence
Dr Ida MahSpecialist in UrologyHong Kong Urology ClinicPedder Street, CentralHong Kong

Urinary Incontinence
The involuntary loss of urine per urethra

Prevalence
Depends on diagnostic criteria and studied population
34% in Hong Kong women aged 18 and above reported urinary incontinence– Ma SS, Urogynecol J Pelvic Floor Dysfunct. 1997; 8 (6): 327-31
49% of female aged 18 and above have urinary incontinence– Ngan et al, the Hong Kong Practitioner 2006 vol 28
34% of female age 10-90 experienced stress incontience– Pang MW et al, Hong Kong Med J 2005 Jun; 11(3): 158-63

Urinary Incontinence

Urinary Incontinence

Types of Urinary Incontinence
Stress Urinary Incontinence Urge Urinary Incontinence Mixed Urinary Incontinence Overflow Urinary Incontinence

Stress Urinary Incontinence
Definition: the involuntary loss of urine per urethra caused by an increase in intra-abdominal pressure

Continence Mechanism
Anatomical support– Intact pelvic floor that hold the bladder
neck and urethra in place Intrinsic urethral mechanisms:
– Coaptation Mucosa Submucosa
– Compression Submucosa Internal sphincter External sphincter

Causes of SUI
Pelvic floor laxity due to childbirth Damage to the urethra due to
– Radiation– Surgery (hx of urethral surgery)– Neurological– Trauma
History
SUI is a clinical diagnosis Association activities childbirth history Hx of surgery or injury to the
urethra Effect on Quality of Life

Physical Examination
Abdominal, rectal, vaginal examination– Look for presence of stress urinary
incontinence– Look for coexisting pelvic organ
prolapse– Assess pelvic floor muscle tone
Pad test
Semi-qualitative assessment of the severity of leakage
1 hour, 2 hours or 24 hours 1 hour:
– Patient is asked to drink 500cc of water– Then perform a series of standard exercise
like climbing stairs and walking– Weight gain of pad is then measured– Significant if >2gm
Management of SUI
Conservative
Surgical
How to decide plan of treatment?
Severity of patients’ symptoms– Subjective and objective
Fitness for operation Presence of other pathology Complications or morbidity of
treatment
Conservative Management
Behavioral Modification
Pharmacotherapy??
Pelvic floor exercise

Behavioral Modification
Diet and lifestyle changes: avoidance of caffeine, stop smoking etc
Fluid management
Timed voiding Bowel habit:
avoid constipation

Pharmacotherapy
Estrogen– Subjective but no objective
improvement Serotonin(5-HT) and
noradrenaline reuptake inhibitor (Duloxetine)

Duloxetine
Significantly reduces incontinence frequency and improve the patient’s QOL
Significant side effects of nausea,dry mouth, fatique, insomnia & constipation (11-23%)
Approved for use in patients with moderate to severe SUI in Europe
Not approved in the States for use in SUI by the FDA because of several suicidal deaths associated with withdrawal of the drug
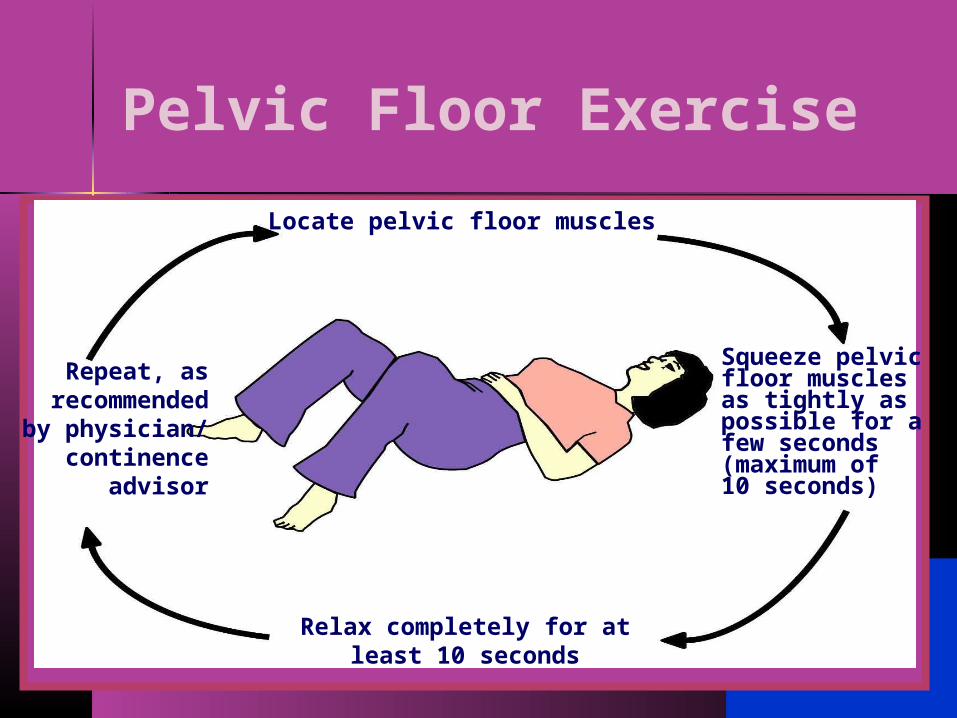
Locate pelvic floor muscles
Squeeze pelvicfloor musclesas tightly aspossible for afew seconds(maximum of10 seconds)
Relax completely for atleast 10 seconds
Repeat, asrecommendedby physician/
continenceadvisor
Pelvic Floor Exercise

Pelvic Floor Exercise Make sure
patients contract the appropriate muscle
Biofeedback– Vaginal cone– Perineometer

Pelvic Floor Exercise
Need a dedicated therapist to supervise the therapy and follow up the patients

Surgical Treatment for SUI

Goal of Surgery for SUI
Prevention of urethral descent– Retropubic Suspension
To provide a backboard against which the bladder neck and proximal urethra can be compressed during increases in intra-abdominal pressure– Sling Procedure

Surgical Rx of SUI
Retropubic Suspensions Sling Procedures Injection therapy

Burch Colposuspension
Described in 1961 Lateral fixation of
urethrovaginal tissue to the Cooper’s ligament
Complications:– Enterocoele (5-10%)
Disadvantage: requirement of an abdominal incision

Surgical Rx of SUI
Retropubic Suspensions Sling Procedures Injection therapy

Sling Procedure
Autologous Sling– Rectus Fascia– Fascia Lata
Synthetic Sling– Polypropylene
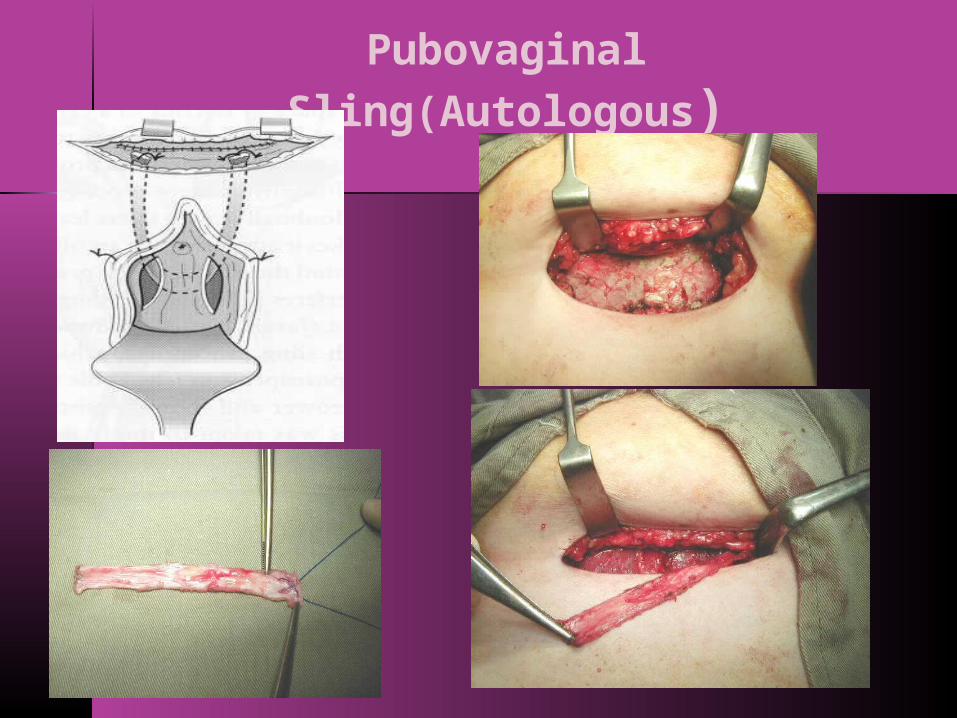
Pubovaginal Sling(Autologous)

Tension Free Vaginal Tape First described by
Ulmsten in 1996 A polypropylene
tape placed at mid-urethra
Tension free urethral support
Minimal invasive Short hospital stay Quick return to
normal daily activities
> 1 million tapes have been implanted worldwide

Tension Free Vaginal Tape

Transobturator Tape

Results of Urethral Tape 85% cure rate at 1-3 year follow-
up– Ulmsten U et al Br J Obstet Gynaecol 1999;106:345-350– Olsson I et al Gynecol Obstet Invest 1999;48:267-269
85% cure rate at 5 year follow-up– Nilson et al Inter Urogyne Journal 2001(suppl 2): S5-S8
TVT vs Colposuspension: similar success rate but TVT provides shorter hospital stay and less days off from work

Urge Incontinence
Urge incontinence is the involuntary loss of urine associated with or preceded by urgency
Caused by involuntary detrusor contraction (detrusor overactivity) during the filling phase

Definition
Detrusor overactivity is a urodynamic observation characterised by involuntary detrusor contractions during the filling phase which may be spontaneous or provoked– Neurogenic detrusor overactivity– Idiopathic detrusor overactivity
International Continence Society 2002
Symptom-based definition of Overactive Bladder OAB is a syndrome referring to
the symptoms of frequency, urgency, urge incontinence, either single or in any combination, when appearing in the absence of local pathologic or metabolic factors explaining these symptoms
Abrams P and Wein AJ: Urology 51(6):1062
Prevalence of OAB
8-35%, depends of studied population and methods of evaluation
13.7% in Hong Kong More commonly in the elderly Urge incontinence affects at least
13 million Americans at a cost to the economy of $16 billion annually

Bladder Filling & Emptying Cycle
The cycle ofbladder fillingand emptying
1. Bladder fills
2. First desire tourinate (bladder
half full)
Urination 3. Urinationvoluntarily inhibiteduntil time and place
are right
Detrusor musclecontracts
Detrusor muscle relaxes
Urethralsphinctercontracts
Urethralsphincterrelaxes

Pathophysiology of OAB Involuntary
detrusor contractions occur during the filling phase which cause the sensation of urgency
Etiology of Detrusor Overactivity Neurogenic
– Spinal cord disorder, DM Local bladder irritation
– Stones, infection, tumour, foreign body
Bladder outlet obstruction– BPH
Aging Idiopathic (OAB)
Etiology of Idiopathic OAB Disorder of the micturition reflex
– Loss of cortical or peripheral inhibition
Disorder of neurotransmission Myogenic disorder
– Structural changes cause increased sensitivity to stimulation
Behavioral / psychological

Etiology of OAB
No single theory explains the pathophysiology of OAB
Significant advances have been made but still a long way to go to
Symptoms of OAB
Frequency (85%) Urgency (54%) Urge incontinence (36%) Nocturia
• Milsom et al 1999
Goals of Evaluations
Rule out local pathologic and metabolic factors
Identify other treatable / curable conditions
Identify other serious underlying conditions
Initial Evaluation
History Physical Examination Voiding diary

Evaluation: History
Identify the symptoms of OAB– Frequency, urgency, urge incontinence,
nocturia Symptoms suggestive of underlying
causes– Haematuria– Hx of urinary tract stones
Hx suggestive of outlet obstruction Medical and neurological history

Evaluation: Physical Examiantion General Examination (including
bladder palpation) Digital rectal examinatioin in
males Pelvic examination in females
(observe for SUI and prolapse Neurological examination

Evaluation: Voiding Diary
Evaluation: Lab tests
Urinalysis– MSU to rule out haematuria, pyuria,
bacteruriaand glucosuria– Urine for cytology
Blood tests– Fasting blood glucose– Renal function

Evaluation: Radiology
KUB– To rule out underlying urinary tract
especially bladder stones USG kidneys and bladder
– To detect bladder pathology– To detect upper tract damage in
patients with neurogenic bladder
Urodynamic Study
Filling cystometry
Involuntary detrusor contraction
? >15cm water Associated
with symptoms Spontaneous
or provoked Bladder
capacity Assess outlet
obstruction

UD tracing : detrusor overactivity

Urodynamic Study
False Positives– 60% of normal volunteers
False Negatives– 10-40% with negative UDS have
positive ambulatory UDS

Indications for UDS
Treatment failure Suspect outlet obstruction Association with stress
incontinence Suspect neurogenic bladder Consideration of surgery
Indications for referral to urologists Evidence of bladder outlet
obstruction Haematuria (? Underlying
carcinoma) Associated with neurological
disease Bladder stones Associated with stress
incontinence or pelvic prolapse Failed medical
treatment/consideration of surgical Rx

Management of OAB
Behavioral therapy Pharmacologic therapy Surgery

Behavioral Therapy
Education Voiding diaries Fluid/dietary management Bladder training/timed
voiding/delayed voiding Pelvic floor training/biofeedback

Education
Education on the normal bladder physiology and pathophysiology of OAB

Dietary advice
Fluid management
Avoid stimulants like coffee, tea and alcohol

Behavioral Therapy
Bladder training Timed voiding/delayed voiding No standard protocol, teaching
material or technique Efficacy: low cure rates, improve
efficacy if combined with drug Rx Results better in urodynamically
stable patients
Pelvic Floor Training
Competent pelvic floor muscles make the difference between wet and dry OAB
Indicated in patients with urge incontinence and weak pelvic floor muscle
Pharmacologic Therapy Muscarinic cholinergic receptors
located on detrusor muscle respond to parasympathetic mediated release of acetylcholine to stimulate detrusor contraction
5 muscarinic receptors have been described
M3 responsible for activating detrusor contraction
M3 receptors also mediate salivary secretions and bowel contraction (ie. Side effects)
Side Effects of Drug Rx
Mainly due to their anticholinergic action
Dry mouth Blurred vision Constipation Tachycardia Drowsiness

Contraindication and precaution
Contraindicated in patients with narrow angle glaucoma
Use with caution in patients with outlet obstruction as the drugs may precipitate retention

Oxybutynin (ditropan)
Binds to M2 and M3 receptors Dosage: 2.5mg bd to 5mg tds Significant side effects: dry
mouth, decreased gastric motility 18% patients remain on Rx for
over 6 months Less side effects in children
Tolterodine (detrusitol)
Not receptor selective but selective for bladder tissue over salivary tissue
Efficacy similar to oxybutynin but less dry mouth and less withdrawals from drug Rx
Dosage: 2mg bd

Solifenacin (Vesicare)
Slow release Plasma level rise over 4-6 hours ,
then steady over 24 hours Demonstrated efficacy at a lower
steady level to reduce side effects

Tricyclic Antideprssants Imipramine most commonly used Central and peripheral anticholinergic
effects Block norepinephrine and serotonin re-
uptake thereby causing a direct inhibition of normal excitatory pathways
Sedative Dosage: 10mg QD to 25mg QID Side effects: anti-cholinergic side
effects, weakness, fatigue

Acupuncture
Endorphinergic effects at the sacral spinal cord level or above
Inhibit somatovesical reflexes Increase in peripheral circulation Need randomised control studies

Surgical Treatment for OAB Bladder overdistension Supratrigonal transection of
bladder Bladder denervation Neuromodulation: Interstim BOTOX injection Augmentation enterocystoplasty

Surgical Treatment for OAB Bladder overdistension Supratrigonal transection of
bladder Bladder denervation Neuromodulation: Interstim BOTOX injection Augmentation enterocystoplasty
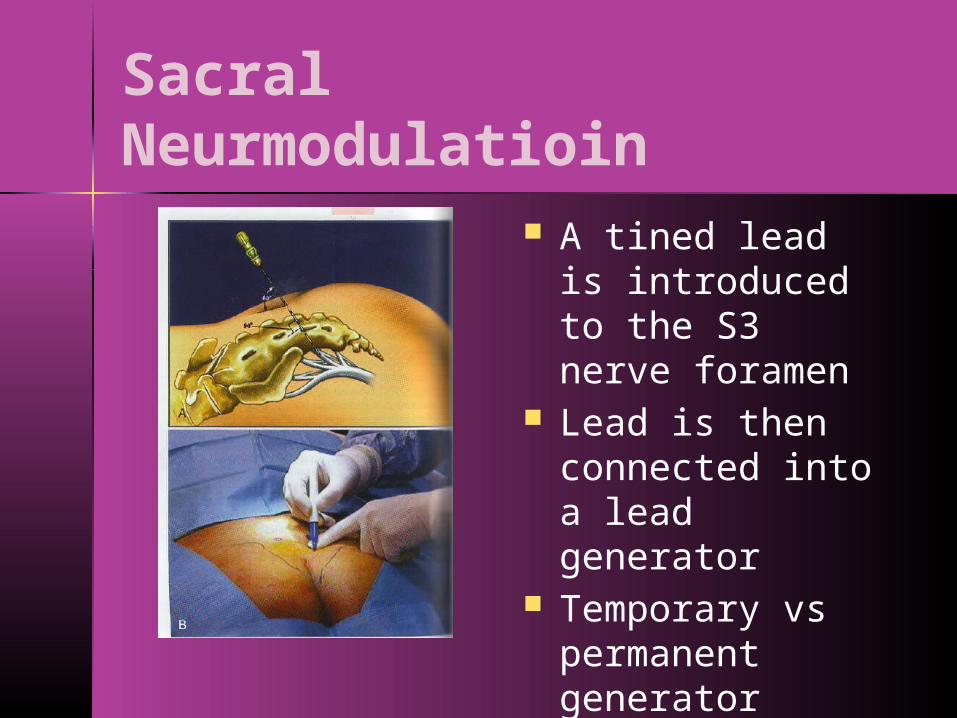
Sacral Neurmodulatioin
A tined lead is introduced to the S3 nerve foramen
Lead is then connected into a lead generator
Temporary vs permanent generator

Sacral Neuromodulation Outcome
– 47% dry– 29% improved
Side effects:– Pain (16%)– Implant infection (19%)– Lead migration (7%)
Cost
Surgical Treatment for OAB Bladder overdistension Supratrigonal transection of
bladder Bladder denervation Neuromodulation: Interstim BOTOX injection Augmentation enterocystoplasty

Injection of BOTOX BOTOX A blocks
acetylcholine release at the neuromuscular junction
Injection of BOTOX at suburothelial space modulates the release of neurotransmitters from sensory nerve endings, thus inhibiting the occurrence of bladder overactivity

Injection Site
Generally distributed around bladder–Avoid dome
Potential for intraperitoneal injection
Difficulty of injection
* ** * *** **** ****
* * * * * ** * * * * *
****

Injection of BOTOX
Advantage:– Effective– Effect last for 6-8
months– Minimal invasive– Outpatient
procedure
Disadvantage– Effect last for 6-8
months only– Risk of retention
of urine (10%)– Limb weakness
Surgical Treatment
Bladder overdistension Supratrigonal transection of
bladder Bladder denervation Neuromodulation: Interstim Injection of BOTOX Augmentation enterocystoplasty

Augmentation Enterocystoplasty
Clam cystoplasty Up to 90%
success rate in DI and neurogenic bladder
Increase the bladder capacity and abolish the unstable contraction

Side Effects of Cystoplasty Retention of urine Mucus plug retention Stone formation Electrolyte disturbance Malignancy
Reserved for patients who have intractable symptoms and are willing to accept the possible side effects

Conclusions
Urinary incontinence is a common problem Treatment depends on the nature and
severity of the condition OAB: important to identify treatable
underlying factors Patients should be provided with information
on various choices of Rx (conservative & operative)
With appropriate Rx patients could be cured of the incontinence and thus improving the quality of life