
FEMA CONTRACTOR - American Medical Response · Proprietary and Confidential. Do not reproduce...
143
Proprietary and Confidential. Do not reproduce without permission of American Medical Response. AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 1 FEMA CONTRACTOR Revised 4/5/2016
Transcript of FEMA CONTRACTOR - American Medical Response · Proprietary and Confidential. Do not reproduce...

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
1
FEMA CONTRACTOR
Revised 4/5/2016

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
(Revised 4/5/2016)
Emergency Responder, To participate in a disaster response or other Federal event is a privilege and represents one of the higher callings within the field of emergency medical services (EMS). The purpose of this handbook is to answer questions and provide basic information common to most AMR/FEMA responses in order to lay the foundation for a successful deployment. The responder is reminded that deployments are high-profile events that may present challenges not common in day-to-day operations. It is incumbent upon all participants to reflect the highest levels of professionalism, duty and understanding as they are mobilized from around the country to support communities in need. Maintaining a confident as well as professional mindset as challenges arise will most certainly allow for a positive deployment experience thus bringing great credit upon you, your company, the EMS profession, and the United States of America. ______________________________________ ________________________________ Steve Delahousey RN, NREMT-P, ADLS® Don S. Harvey Vice President of Emergency Management AMR Chief of Emergency Management Federal Liaison / Project Director NATCOM Incident Commander

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 3
TABLE OF CONTENTS
Overview of FEMA/AMR Federal National Ambulance Service Support ............................................... 5
Situation and Assumptions (Key Concepts) ............................................................................................ 5
Organization and Assignment of Responsibilities .................................................................................. 5
Office of Emergency Management (OEM) ............................................................................................. 5
National Command Center (NATCOM) .................................................................................................. 9
AMR Liaison Agency Representative .................................................................................................. 11
AMR Forward Command .......................................................................................................................... 11
AMR Forward Operating Base (FOB) .................................................................................................. 11
Unity of Command .................................................................................................................................... 12
First Line Supervision .............................................................................................................................. 12
Significant Incident ................................................................................................................................... 12
Mission Assignments to Support State and Local EMS ....................................................................... 13
Vehicle Operations .................................................................................................................................... 14
Safety .......................................................................................................................................................... 19
Shift Lengths ............................................................................................................................................. 20
Conduct ...................................................................................................................................................... 20
Discrimination ........................................................................................................................................... 21
Accountability ........................................................................................................................................... 21
Uniform, Identification and Appearance ................................................................................................. 22
Deployment Instructions .......................................................................................................................... 22
Flying ....................................................................................................................................................... 22
Driving ..................................................................................................................................................... 23
Check-In Process ...................................................................................................................................... 23
Demobilization ........................................................................................................................................... 24
Operational Documentation ..................................................................................................................... 24
Billing for services .................................................................................................................................... 25
Reimbursement and expense .................................................................................................................. 25
Credentials and Identification Badges .................................................................................................... 25
Release of Information for AMR/FEMA Federal EMS Activities ........................................................... 25
EMS Scope of Practice, Protocols, Reciprocity, and Medical Control and Direction ........................ 28
Appendix 1 Shift and Safety Management Plan ......................................................................................... 29
Appendix 2 Deployment Uniform Policy ...................................................................................................... 33
Appendix 3 Deployment Check-In Forms ................................................................................................... 35
Appendix 4 Deployment Documentation ..................................................................................................... 39
Appendix 5 Credentials and Identification Badges ..................................................................................... 47
Appendix 6 Scope of Practice ..................................................................................................................... 49
Appendix 7 Hazard Based Guidelines ........................................................................................................ 63
Appendix 8 Critical and Specialty Care Patient Transport .......................................................................... 68

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 4
Appendix 9 Specialty Ambulance ............................................................................................................... 73
Appendix 10 Air Medical Support ................................................................................................................ 74
Appendix 11 DHS Non-Disclosure Agreement ......................................................................................... 101
Appendix 12 Equipment for Ground Ambulances ..................................................................................... 105
Appendix 13 Non-Ambulance Medical Support by Fixed Site EMS Personnel ........................................ 114

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 5
Purpose This guide describes the systems and processes used during a federal activation of the FEMA federal EMS contract as well as a non-federal activation of the American Medical Response (AMR) Emergency Response Team (ERT). The parent company of AMR is Envision Healthcare Holdings, Inc. (EVHC). While the guide is written primarily for AMR, it may be expanded to include other EVHC subsidiaries and departments. The organizational structure identifies key leadership positions and establishes chains of command in reference to, AMR’s Office of Emergency Management (OEM), the National Command Center (NATCOM), Area Command, and Forward Operating Base with single or multiple incidents. Emergency management and incident response refer to the broad spectrum of activities and entities providing effective and efficient operations, coordination, and support. Incident management, by distinction, includes directing specific incident operations; acquiring, coordinating, and delivering resources to incident sites; and sharing information about the incident with appropriate parties. Taken together, these elements of Command and Management are the most visible aspects of incident management, typically executed with a sense of urgency. Situation and Assumptions (Key Concepts) Most incidents are managed locally and are typically handled by local EMS and emergency management personnel within a single jurisdiction. In other instances, incidents that begin with a single jurisdictional response rapidly expand to multidisciplinary, multijurisdictional levels requiring significant additional resources and operational support. This guide, using ICS, provides a flexible core mechanism for coordinated and collaborative incident response, whether for incidents where additional resources are required or are provided from different entities outside the jurisdiction, or for complex incidents with national implications. Effective cross-jurisdictional coordination using processes and systems is absolutely critical in this situation. National Standards and Credentials AMR, the OEM, and NATCOM have existing organizational structures in place. AMR uses the following federal guidelines for minimum standards of disaster management and credentialing of its incident management team (IMT) members.
National Incident Management System (NIMS)
FEMA’s Incident Command System (ICS)
FEMA’s Designing a National Emergency Responder Credentialing System
FEMA’s EMS Typed Resource Definitions The AMR IMT is composed of individuals who are proven leaders and whom the NATCOM Incident Commander and AMR/FEMA Project Director have determined would best position the team for success. A copy of the AMR IMT roster is maintained by the OEM National Emergency Management Planning Manager. Organization and Assignment of Responsibilities Office of Emergency Management (OEM)—The AMR OEM is the Company’s lead agency that oversees all matters related to emergency management, mitigation, response and recovery when they involve Federal agencies or in response to emergency situations that exceed the capacity of local operations. The OEM is under the overall direction of the EVHC Chief of Emergency Management (CEM) and the day-to-day direction and leadership of the AMR Vice

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 6
President of Emergency Management (VPEM). The OEM provides strategic direction, oversight, and coordination of the Federal EMS Contract and supports both routine maintenance and continuous refinement of the contract and its components. This includes regular consultation with Federal agencies, AMR departments and other stakeholders. This office is also responsible for: developing and articulating the AMR key policies, positions and strategies for dealing with federal emergencies; implementing, coordinating, and enforcing policies across multiple departments and jurisdictions; executing interagency agreements; developing training standards; and analyzing effective disaster management services. It oversees the development, implementation and evaluation of the Company’s disaster planning efforts through its National Emergency Operations Plan (NEOP). For non-Federally declared disasters, the OEM may provide guidance, support, and coordination to AMR jurisdictions as long as there is no conflict with Federal responsibilities. The OEM provides oversight, review and certification of IMT members who may respond during Federal deployments. AMR’s Office of Emergency Management (OEM) is tasked with management of all aspects of the Federal EMS Contract. The OEM is responsible for contract maintenance, subcontracting of all disciplines, deployment operations, and the Emergency Response Team. OEM associates include the following positions.
Chief of Emergency Management
Vice President of Emergency Management
National Emergency Management Planning Manager
National Ground Ambulance Emergency Manager
National Paratransit Emergency Manager
National Air Ambulance Emergency Manager
National Emergency Response Team Manager/Coordinator
Chief of Emergency Management and Special Projects (CEM) -The EVHC CEM is appointed by the EVHC President and CEO and provides executive direction to the OEM. He also serves as the NATCOM Incident Commander and is responsible for all deployments. The

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 7
CEM has full authority to act and speak on behalf of EVHC in all matters related to disaster deployments. As an EVHC executive, the CEM may include other EVHC departments or subsidiaries, e.g., EmCare, to participate in the NEOP. Vice President of Emergency Management (VPEM) — Under the CEM’s direction, the VPEM oversees the OEM and all matters related to emergency management, mitigation, response and recovery. The VPEM serves as the senior advisor to the CEM in matters of emergency management. This position is responsible for: developing and articulating the EVHC and AMR key policies, positions and strategies for dealing with emergencies; interpreting and applying state and federal legal requirements; implementing, coordinating, and enforcing policies across multiple departments and jurisdictions; overseeing the development, implementation and evaluation of the Company’s Incident Action Plan; executing interagency agreements; developing training standards; and analyzing effective disaster management services. At the direction of the CEM, coordinates the Company’s Incident Action Plan, i.e., response to emergency situations that exceed the capacity of local operations. The VPEM is responsible for coordinating the Company’s involvement in the full range of events within which domestic incident management activities occur, including awareness, prevention, management, response and recovery to emergencies, disasters and other significant events as defined by national and state response plans. National Planning Emergency Manager — The AMR National Emergency Management Planning Manager (“Planner”) is a primary management position responsible for providing planning services to the OEM. These services include collecting and analyzing intelligence and information, as well as developing policies, plans, procedures, network provider agreements, mutual aid and assistance agreements, strategies, and other arrangements to perform missions and tasks. The Planner prepares and documents the Company’s actions in response to Federal disaster deployments and major events and develops unified action, contingency, long-term, and other plans related to the Company’s NEOP. The Planner provides information on overall disaster planning issues and progress/status of responses from a regional or national perspective. The Planner also performs executive job duties as they pertain to disaster planning. National Ground Ambulance Emergency Manager — AMR’s contract with FEMA requires us to provide ground ambulance services in the event of a national disaster. Vast internal and external (network subcontractors) resources are required. This position will coordinate and manage all aspects of the ground ambulance disaster program. The National Ground Ambulance Emergency Manager manages, coordinates, and directs the actions of the ground ambulance disaster response. This includes maintaining all required records, and ensuring the logistical needs of all assigned personnel are met during the entire activation. For day-to-day operations, the National Ground Ambulance Emergency Manager reports work progress, resources status, and other important information to the VPEM. During deployments and/or NATCOM activation, s/he reports to the NATCOM Operations Section Chief. National Paratransit Emergency Manager — AMR’s contract with FEMA requires us to provide Paratransit services in the event of a national disaster. Vast internal and external (network subcontractors) resources are required. This position will coordinate and manage all aspects of the Paratransit disaster program. The National Paratransit Emergency Manager manages, coordinates, and directs the actions of the Paratransit emergency response. This includes maintaining all required records, and ensuring the logistical needs of all assigned personnel are met during the entire activation. For day-to-day operations, the National Paratransit Emergency Manager reports work progress, resources status, and other important
Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 8
information to the VPEM. During deployments and/or NATCOM activation, s/he reports to the NATCOM Operations Section Chief. National Air Ambulance and Logistics Emergency Manager — AMR’s contract with FEMA requires us to provide air ambulance services in the event of a national disaster. Vast internal and external (network subcontractors) resources are required. This position will coordinate and manage all aspects of the air ambulance disaster program. The National Air Ambulance Emergency Manager coordinates the actions of the air ambulance disaster response. This includes maintaining all required records, and ensuring the logistical needs of all assigned personnel are met during the entire activation. For day-to-day operations, the National Air Ambulance Emergency Manager reports work progress, resources status, and other important information to the VPEM. During deployments and/or NATCOM activation, s/he reports to the NATCOM Operations Section Chief and works in collaboration with the Air Ambulance Specialists, Inc. (AASI) leadership. The National Air Ambulance Manager will also act as the OEM’s Logistics Manager and will collaborate with the AMR logistics, fleet and procurement teams for planning, development, implementation, organizing, coordinating and auditing of materials and purchasing within the OEM. National Emergency Response Team (ERT) Manager/Coordinator — The AMR National ERT Manager/Coordinator (“ERT Manager”), will coordinate and manage all aspects of the ERT program. This includes maintaining all required records, and ensuring the logistical needs of all assigned personnel are met during the entire activation. For day-to-day operations, the ERT Manager reports work progress, resources status, and other important information to the VPEM. During deployments and/or NATCOM activations s/he reports to the Planning Section Chief. The ERT manager will be responsible for obtaining and maintaining personnel credentialing criteria for AMR for disaster management to meet the requirements under the FEMA Federal EMS Contract. This position also administers the PCard and reconciliation process post-activation.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 9
National Command Center (NATCOM) NATCOM serves as the Emergency Operations Center (EOC), Area Command and functional command center for EVHC and its subsidiaries in any and all Federal deployments or other significant incidents. It provides coordination, direction, and support during major incidents, Federal deployments or when resource needs exceed local capabilities. It serves as the interface between the Company’s ongoing operations and the emergency operations it is supporting. During Federal deployments it also serves as the interface between EVHC and government agencies. NATCOM will usually be activated to provide incident management oversight to AMR in times of disaster, however it may be expanded to include other EVHC subsidiaries and departments, e.g., EmCare. The core functions of NATCOM include:
Coordination
Communications
Resource allocation and tracking
Information collection, analysis, and dissemination NATCOM is organized much the same as NIMS ICS Area Command, i.e., to oversee management of multiple incidents handled individually by separate ICS organizations or to oversee the management of a very large or evolving incident engaging multiple IMTs. The EVHC Chief of Emergency Management makes the decision to establish Command through

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 10
NATCOM. It is activated only if necessary, depending on the complexity of the incident and incident management span-of-control considerations. For incidents under its authority, NATCOM Command has the following responsibilities:
Develop broad objectives for the impacted area(s).
Coordinate the development of individual incident objectives and strategies.
Allocate or reallocate resources as the established priorities change.
Ensure that incidents are properly managed.
Ensure effective communications.
Ensure that incident management objectives are met and do not conflict with each other or with Company policies.
Identify critical resource needs then approve, commit, and make optimal use of assigned resources.
Ensure that joint planning for tactical activities is accomplished in accordance with approved incident objectives.
Ensure the integration of tactical operations. NATCOM utilizes the principles of ICS Unified Command which consists of senior leadership from various departments and jurisdictions operating together to form a single command structure. Other departments and entities have key responsibilities to support NATCOM activations and field deployments. The NATCOM General Staff and Command Staff, which bring together AMR senior leadership and other department heads as necessary, provide national strategic and policy advice to the NATCOM Incident Commander (NIC) during large-scale incidents that affect the Company. The size, complexity, duration and location of an incident will influence NATCOM staffing. It may be organized by major discipline; by emergency support function; by jurisdiction; or, more likely, by some combination thereof. NATCOM is activated to support the on-scene response during an escalating incident by relieving the burden of external coordination and securing additional resources. It is staffed with personnel trained and authorized to represent their department/discipline. It is equipped with mechanisms for communicating with the incident site and obtaining resources and potential resources. Upon activation of NATCOM, communications and coordination must be established between FOB IC and NATCOM. In addition all functional sections and departments within AMR must be capable of communicating appropriately with NATCOM. Multi-departmental coordination system is the process we use to allow all levels of EVHC companies, subsidiaries and departments to work together more efficiently and effectively. All EVHC departments with jurisdictional authority or functional responsibility for any or all aspects of an incident may be asked to participate in the NATCOM Unified Command structure. The exact composition of the NATCOM Unified Command structure will depend on size of the incident, the location(s) of the incident (i.e., which geographical administrative jurisdictions are involved) and the type of incident (i.e., which functional agencies and departments of the involved jurisdiction(s) are required). The designation of a single NATCOM Incident Commander (NIC) is used to promote greater unity of effort and efficiency. Together with the NIC, the General Staff and Command Staff, and their deputies, make up the NATCOM Unified Command. NATCOM is a functional entity comprised of IMT staff, and not a physical structure
Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 11
necessarily. While the NATCOM facility (building) is strategically located and designed to accommodate all General Staff and Command Staff positions, it may also be partially activated by the NIC and located at alternate strategic sites depending upon the size, complexity and duration of the incident. In addition to the Command function, other functions and activities of the NATCOM IMT staff include:
To delegate authority and to provide a separate organizational level within the NATCOM ICS structure with sole responsibility for the tactical direction and control of resources.
To provide logistical support to the incident organization.
To provide planning services for both current and future activities.
To provide cost assessment, time recording, and procurement control necessary to support the incident and the managing of claims.
To promptly and effectively interact with the media, and provide informational services for the incident, involved agencies, and the public.
To provide a safe operating environment within all parts of the incident organization.
To ensure that assisting and cooperating agencies’ needs are met, and to see that they are used in an effective manner.
AMR Liaison Agency Representative The AMR Liaison Agency Representative is also called the AMR Liaison Officer or AMR LNO. The FEMA ICS definition of Agency Representative is “an individual assigned to an incident for an assisting or cooperating agency who has been delegated authority to make decisions on matters affecting that agency’s participation at the incident.” As part of the AMR NATCOM Incident Command Staff, the AMR LNO will provide communication and coordination with the Regional Chief Executive Officers (CEOs), or their designees, during all phases of a response. Only one AMR LNO will be assigned for each incident, including incidents operating under Unified Command and multi-jurisdiction incidents. The AMR LNO may have assistants as necessary, and the assistants may also represent assisting agencies or jurisdictions. The AMR LNO is the point of contact for other Agency Representatives that may be assigned to the incident by assisting or cooperating agencies/providers. AMR Forward Operating Base (FOB) AMR Forward Operating Base has overall incident management responsibility for the designated command jurisdiction and reports directly to AMR NATCOM Operations Section Chief.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 12
Unity of Command The Unity of Command concept is fundamental to the ICS command structure. Each individual participating in a deployment reports to only one supervisor. This eliminates the potential for individuals to receive conflicting orders from a variety of supervisors, thus increasing accountability, preventing freelancing, improving the flow of information, helping with the coordination of operational efforts, and enhancing operational safety. First Line Supervision Emergency Response Team members will be assigned to report to a single supervisor. Usually, this supervisor will be a Strike Team Leader (STL) or other designated supervisor. The STL or other supervisor manages, coordinates, and directs the actions of the resource based on directions from operational leadership. The first line supervisor must maintain all appropriate records while ensuring the logistical needs of all assigned personnel are met during the period of the assignment. Significant Incident NATCOM may be activated for federal deployments or other significant incidents. Significant incident is defined as an occurrence or event, natural or man-made, that requires a multi-departmental or multi-jurisdictional response to protect life or property or to lessen or avert the

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 13
threat of a catastrophe. Incidents can, for example, include major disasters, emergencies, terrorist attacks, terrorist threats, civil unrest, wildland and urban fires, floods, hazardous materials spills, nuclear accidents, aircraft accidents, earthquakes, hurricanes, tornadoes, tropical storms, tsunamis, war-related disasters, public health and medical emergencies, national security events and other occurrences requiring a coordinated response. Significant Incidents require responses well beyond “business as usual.” They have some or all of the following characteristics:
Involve more than one agency and/or political jurisdiction.
Involve complex management and communication issues.
Require experienced, highly qualified supervisory personnel.
Require numerous tactical and support resources.
Involve multiple victims with injuries, fatalities, or illnesses.
Include widespread damage to property/environment.
Result in psychological threat/trauma.
Span multiple operational periods (days, weeks).
Are costly to control and mitigate.
Require extensive recovery efforts.
Draw national media interest.
Mission Assignments to Support State and Local EMS Oversight of AMR Federally contracted EMS assets while enroute to the disaster theater of operations (TOO) will be managed by AMR NATCOM. Once the AMR Federal EMS assets arrive at the Federally-designated check-in site, they will be officially checked-in and inventoried by Government and AMR representatives. State EMS officials may also perform check-in procedures. The AMR Disaster Resources will then likely be assigned to various state and local EMS jurisdictions and given various mission types. In the conduct of these missions a resource may or may not be directly reporting to AMR IMT. If AMR’s Federal disaster response assets are assigned to local jurisdictions to be assimilated into their existing EMS system, it is expected that the Incident Command structure of the local jurisdiction will also be used. Whenever possible, the local jurisdiction is also expected to provide ongoing resources to sustain the Federal assets assigned to them, e.g., fuel, food, lodging, etc. If this is not possible, the Federal assets will remain under the logistical control of AMR’s IMT. Missions are assigned by the FEMA or U.S. Dept. of Health and Human Services (HHS) field representative at the FOB. Missions may include, but are not limited to, evacuation assistance, augmenting local EMS/911 system, triage and treating casualties, inter-facility transports, on-scene stand-by, search and rescue support, and hospital or shelter staffing. Individual call assignment and dispatch is usually the responsibility of the local EMS authorities who have been granted access to AMR Federally contracted EMS assets. FEMA or HHS will monitor and direct the appropriateness of mission activities. Example: A mission for AMR Federally contracted EMS may be to assist a local EMS agency in evacuating a local hospital. FEMA or HHS would assign the AMR Federal assets and the local EMS agencies would direct/dispatch the individual calls. FEMA or HHS would monitor the appropriateness of the activities being requested and intervene if the activities were inappropriate for the mission assignment, e.g., rather than evacuating the hospital, the ambulances were assigned by local EMS to assist in distribution of food and water. Detailed direction on how to perform the work and the supervision of responders is the sole responsibility of AMR in collaboration with local jurisdictions. AMR shall provide management

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 14
and assure that communications are in place to successfully provide services and reports. When a resource is assigned by AMR leadership to a State or Local Organization, the AMR Disaster Response resource will report to, follow direction and become an assimilated component of the host organization. An Operational Unity of Command relationship shall then exist between the AMR Resource and the host organization. AMR’s Forward Command will remain in contact with deployed operational units to provide for any unmet logistics needs and obtain information necessary for Operational Status reports. All applicable AMR policies, including the Emergency Response guidance covered in this publication, shall remain in effect. Vehicle Operations Vehicle Identification: All deployed Ground Ambulances and Paratransit vehicles shall display FEMA-approved placards on driver’s side front and rear windows with the FEMA Placard Number legibly written and clearly visible. Each vehicle shall have only one unique FEMA Placard Number assigned to it for the duration of an event. These Placard Numbers are not to be removed, modified, exchanged, or otherwise altered by any entity unless authorized by the specific Group Director located at NATCOM. Placard # Issuing Placard numbers are designed for the purpose of identifying a VEHICLE asset. Placard numbers are unique and issued sequentially, without repetition of numerical digits. Placard numbers are generated and assigned through the Rapid Electronic Deployment System (REDS). All responding agencies should download and print assigned FEMA Placards through REDS. If for any reason an agency is unable to download and print their FEMA placards they should print blank placards (available on REDS) and fill in their applicable placard number as assigned by REDS or the AMR Office of Emergency Management (OEM). If it is not possible to print placards, agencies SHOULD NOT delay response. Placards will be available at the check-in site. Once a vehicle is assigned a placard number they will keep that number for the duration of the deployment regardless of change of personnel, equipment, or vehicle operational status. If, due to extenuating circumstances, a placard number needs to be changed it must be authorized and performed through NATCOM dispatch or the discipline manager. Additionally, if a vehicle is placed out of service and another unit is assigned in its place, the new unit should receive its own unique placard number designation. The placard number assigned to the out-of-service vehicle should be suspended until such time as the vehicle is repaired and placed back in service or taken out of service entirely. There are only three authorized methods of issuing and distributing vehicle placard numbers.
1. Discipline Representative (i.e. Ground Ambulance or Paratransit Managers) (REDS) 2. NATCOM (Dispatch) 3. Forward Operating Base (This is the last resort method. Forward Operating Base will be
supplied with blank placards and a pre-designated bank of numbers to use should resources arrive without placards).
Vehicle Type Identification: Since ambulances look similar on the outside, the Vehicle Type Identification was developed so various officials could readily identify the level of service provided by a resource. At the end of each FEMA Placard Number will be a Vehicle Type Identifier. It is imperative that the vehicle type displayed on the placard matches with the personnel and equipment of the actual resource.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 15
Placard # Description
1 0 1 1 A A This is a sequential, four-digit identification number assigned to specific vehicles. The numbers begin at 0001 and progress through 9999.
This letter designates whether the resource is an AMR unit “A” or a Network Provider “N”.
This letter indicates what type of resource the vehicle is (see chart below).
In this example this four digit number is designated as an AMR vehicle from the Northeast Division.
In this example, this is an AMR vehicle.
In this example, this is an ALS vehicle.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 16
AMR/FEMA Vehicle Placard - Example
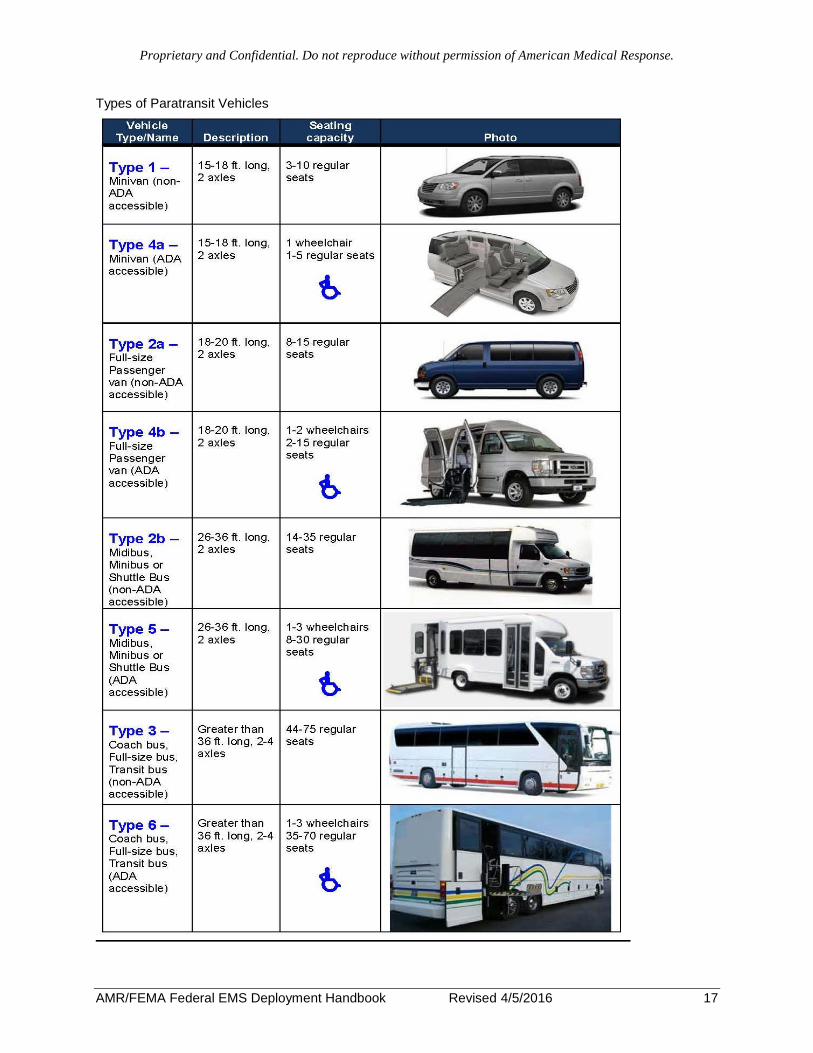
PROVIDER A = AMR vehicle N = Network provider vehicle VEHICLE TYPES A = ALS Ground Ambulance B = BLS Ground Ambulance C = ALS Bariatric Ground Ambulance D = ALS Med-Evac Bus (4 or more ALS patient stretcher positions) G = Paratransit Type 1: Minivan - 3-10 regular seats H = Paratransit Type 2b: Minibus/Midibus/Shuttle bus – 14-35 regular seats J = Paratransit Type 3: Coach/transit bus – 44-75 regular seats K = Paratransit Type 4b: ADA Full size passenger van – 1-2 wheelchairs, 2-15 regular seats L = Paratransit Type 5: ADA Minibus/Midibus/Shuttle bus – 1-3 wheelchairs, 8-30 regular seats M = Paratransit Type 6: ADA Coach/transit bus – 1-3 wheelchairs, 35-70 regular seats N = Paratransit Type 2a: Full size passenger van – 8-15 regular seats P = Paratransit Type 4a: ADA Minivan – 1 wheelchair, 1-5 regular seats F = Air Ambulance Fixed Wing R = Air Ambulance Rotor Wing X = Support Vehicle
Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 17
Types of Paratransit Vehicles
Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 18
Federal EMS FEMA Contractor Decal: Once a resource has completed the check-In process and is cleared to enter the theater of operations a Federal EMS decal will be adhered to the driver’s side upper front windshield. The application of the Federal EMS FEMA Contractor decal represents that the resource meets or exceeds the minimum standards for the Resource Vehicle Type as identified on the FEMA placard. Driving Requirements: Emergency Vehicle Operations Course (EVOC), or Coaching the Emergency Vehicle Operator (CEVO), or Defensive Driving Course IV (DDC4), or equivalent and valid driver’s license is required for the operation of Emergency Response Network resource vehicles. In the course of a disaster response a large fleet of vehicles will be utilized. Given the risk of collisions or accidents while functioning in disaster conditions all personnel are reminded that all vehicles must be operated in a manner that provides for due regard and the safety of all persons and property. Components of the AMR Vehicle Safety Policy include and are not limited to:
Basic Defensive Driving Practices
Safety Belts & Other Restraint Devices
Backing & Tight –Quarters Maneuvering
Parking & Securing the Vehicle
Emergency Vehicle Operations
Use of Emergency Warning Devices
Post-Collision Guidelines
AMR leadership is expected to implement and enforce all AMR Vehicle Safety Policies for AMR and subcontractor resources. Regardless of circumstances or unit status, vehicles shall not be driven faster than a safe speed for the current road, weather, and traffic conditions. Check the vehicle’s fuel gauge frequently and make every effort to assure the fuel tank is “topped off” whenever possible. Remember that service stations may be closed during emergencies or may be unable to pump fuel during power outages. Monitor the local Emergency Broadcast System radio frequency for helpful news, weather condition, and traffic reports. If long distance driving is involved, individuals will trade off driving as necessary (8-12 hours maximum) to assure the driver is alert and rested. If transport time or the destination point is excessive, arrangements will be made for the crews to stay for the night. Fixed Site Personnel Fixed Site Personnel shall be either EMTs or Paramedics with the required certification. They may be stationed at shelters, airheads, triage centers, or other fixed location sites. EMS personnel at fixed sites will be equipped with portable and disposable medical supplies and equipment comparable to that which is required on ambulances commensurate with their level of certification, i.e., EMT equipment—BLS ambulance, Paramedic equipment—ALS ambulance. This equipment will exclude ambulance equipment such as extrication equipment, patient transportation devices, traffic safety equipment, and other equipment or supplies that are commonly used on vehicles rather than fixed sites.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 19
For a more detailed description, please see Appendix 13: Non-Ambulance Medical Support by Fixed Site Personnel Personal 72-hour Go-Kit Unless otherwise indicated by AMR, all EMS responders will be required to carry their own equipment and supplies to be self-sufficient for 72 hours. The following is a suggested list of personal items that each individual ERT member should include as part of their response. You should include enough items to be completely self-sustainable for a minimum of 72 Hours. These items are for emergency responders, not patients or victims.
Safety boots
Sunglasses
Climate appropriate clothing
Uniforms
Rain gear
Undergarments
Individual personal maintenance medications
Aspirin, Tylenol, or Ibuprofen
Waterproof matches
12 hr. light sticks
Flashlight (wind-up power or extra batteries)
Portable AM/FM radio with NOAA weather freq.
Cell phone with charger and/or pager (optional)
Nextel radio with DC and AC charger (optional)
Portable GPS (optional)
Drinking Water – 1 gal. per person per day min.
Water purification tablets or household chlorine bleach and medicine dropper
Bedding (Sleeping bag, pillow)
Toiletries / Sundries
Toilet paper
Non-perishable food items for self (Protein bars, canned fruit, high caloric bars, etc.)
Spending money
Driver’s license
EMS credentials (state, national, CPR, ACLS certification cards)
Company ID badge
ERT – FEMA ID badge
Insect repellent
Large duffel bag
Hearing protection
Hand sanitizer or anti-bacterial wipes
Work gloves
Swiss Army-style knife with tools, etc.
Compass with whistle
Map of disaster area
Safety Safety for crews is always the number one priority. All assets will be available for response for around-the-clock operations, and assigned crewmembers must not be fatigued to the extent that their safety, the safety of others, or the mission is compromised. An example of an asset would be a fully staffed and equipped ALS ambulance. This asset shall be available 24/7. This does not mean that the original crewmembers assigned to the asset must be available 24/7. The crew may be replaced after 12 hours of continuous duty but the asset remains available 24/7. The very nature of a disaster deployment means that an event has happened or may happen that warrants action to protect life, property, or the environment. In all probability, the disaster area will contain certain hazards that are not incumbent to routine daily operations. These hazards include and are not limited to:
Operating in inclement or rapidly changing weather conditions
Night-time or limited visibility operations
Austere living conditions
Poor road conditions
Debris
Flooding
Power outages, downed power lines
Extended operational shifts with limited rest breaks
High-stress environment

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 20
For a more detailed description, please see Appendix 1: Shift and Safety Management Plan See also Appendix 7: Hazard Based Guidelines, Protective Equipment for Workers in Hurricane Flood Response.
Shift Lengths Typical shifts for EMS personnel in disaster situations are 12 hrs., 24 hrs., 36 hrs. or even 48 hrs. Shift lengths longer than 12 hrs. must include rest periods. The shift lengths are usually based on work load (type of work and volume). According to FEMA Typed Resource Definitions – EMS, the recommended shift lengths for Ambulance Strike Team personnel is 12 – 24 hrs., depending on the number of ambulances needed, and they should be self-sufficient for 72 hrs. Disaster responders should be healthy enough to function under austere field conditions (possibly no showers, housing in tents, portable toilets, extreme weather conditions and long periods of standing). Disaster responders must make provision for their personal health care plans concerning prescription or routine medications. There is a possibility that pharmacy services may not be available. Bring adequate supplies of maintenance medications and assure that the medications can withstand being stored in temperature extremes. Shift lengths will be based on disaster criteria and environment, i.e., transferring patients from one facility to another versus transferring patients from the field to an emergency department or staging area; long distance versus local travel destinations. Weather conditions could also play a factor in shift lengths as well. EMS disasters assets, e.g. ambulances, shall not be taken out of services for crew rest. If fatigued, the crewmembers will be allowed to rest, and replaced if needed, but the asset should remain in service. 24-hour shifts carry the expectation that crewmembers have time during the shift to rest, but remain available for immediate response to an emergency. Regardless of the shift length, if any crewmember, Strike Team Leader, Task Force Leader, Safety Officer or other appropriate AMR or government representative believes that a team member is fatigued to the point they cannot safely carry out a mission, the fatigued individual should be relieved from duty and replaced with rested personnel. Team members shall remain safety conscious at all times during a deployment. Any individual safety concerns may be routed through the formal chain of command. All individuals are instructed that if they feel their safety is in question, they may contact the local Safety Officer to discuss relative options to ensure their well-being. Any individual may intervene to prevent an unsafe or life-threatening act from occurring. For a more detailed description, please see Appendix 1: Shift and Safety Management Plan
Conduct Emergency Response Team members are required to act in a lawful, professional manner at all times and shall not reflect discredit upon AMR, FEMA, the Department of Homeland Security, the United States or any Federal agency. The Government may direct AMR to remove any ERT member, subcontractor, or other employees from the deployment area for misconduct or security reasons. AMR Standards of Conduct remain in effect throughout the entirety of a deployment. This includes while traveling to and from the deployment area, on shift as well as off shift.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 21
The following are prohibited activities: (not intended to be an exhaustive list)
Theft or attempted theft
Dishonesty
Misappropriation of AMR or Government funds or AMR or Government property
Destruction or unauthorized use of AMR or Government equipment or property
Use of language or action that is inappropriate in the workplace whether racial, sexual or of a general offensive nature
Rude or discourteous behavior
Falsification of documents
Fighting, threatening, assaulting or abusing another individual
Illegal activities such as fraud, kickbacks, or falsifying expense accounts
Carrying, possessing, or using a firearm or any dangerous weapon
Use, sale, possession, or functioning under the influence of alcohol or unlawful drugs
Gambling
Insubordination, including refusal to follow work directions or instructions
Violation of safety rules/regulations
Conducting unapproved media interviews Discrimination Emergency planning, response, and recovery efforts include persons who may be members of an at-risk or special needs population. These individuals may have a need for assistance in a certain area, such as medical care, transportation, maintaining independence for daily living, supervision, or communication. Persons with special needs or who are at risk in an emergency can include children, elderly persons, persons from diverse cultural origins, individuals with disabilities, individuals who are limited English speaking, persons who live in institutionalized settings and persons who do not have access to transportation, among others. Federal laws prohibit discrimination against individuals on the basis of race, color, national origin, disability, or age. AMR policy also prohibits discrimination. Accountability Team members shall be accounted for throughout the entire length of a deployment. Check-in and check-out procedures shall be followed as directed by the IMT when entering and leaving the TOO. While deployed it is imperative that each responder assures that their leader knows their location while on and off any active shifts. In order to be located without delay, team members should keep leadership updated as to their specific location, routes that they will utilize, and the specific spot that they will be sleeping. Just as it is important to be accountable for one’s self during a deployment it is important to be accountable for the equipment and other assigned resources. Items such as two-way radios, wireless phones, GPS navigation devices, or any other item assigned to an individual during a deployment are the property of either American Medical Response or the Government of the United States. As such, these items must be returned as directed to the appropriate AMR representative. Marking, defacing, damaging, writing or drawing on or upon assigned property, including equipment, vehicles and facilities is not allowed. Use of materials or facilities for purposes not directly related to the deployment effort, including neglect, misuse or waste of materials, tools or equipment, inflicting damage to, or failure to properly safeguard or protect property is deemed as unprofessional conduct.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 22
All members of the ERT should make every effort to report on-time and ready for duty for whatever task, work shift or mission they have been assigned to. Lack of accountability, punctuality, or preparedness disrupts workflow and increases the workload of others. Team members risk disciplinary action for accountability failures and punctuality and preparedness issues.
Uniform, Identification and Appearance The identification and appearance of all personnel involved in a disaster response is an important concern. Whether dealing with government officials, other disaster response professionals or the public in a direct or indirect manner, it is essential that all team members project a professional image and are clearly identified. Please refer to Appendix 2 for a detailed description of the AMR Deployment Uniform Policy. Deployment Instructions Flying Those that are traveling by air are reminded that all applicable rules concerning conduct remain in effect throughout a deployment. Paramedics should not carry personal issue narcotics with them while traveling via air. The same rules for the general public concerning what may be carried on planes apply for ERT members. Those that are flying are encouraged to be familiar with the documentation needed and prohibited items in order to be processed through airport checkpoints quickly and without incident. Adult passengers (18 and over) are required to show a valid U.S. federal or state-issued photo ID in order to be allowed to go through the checkpoint and onto their flight.
Acceptable IDs include:
U.S. passport
U.S. passport card
DHS "Trusted Traveler" cards (Global Entry, NEXUS, SENTRI, FAST)
U.S. Military ID (active duty or retired military and their dependents, and DOD civilians)
Permanent Resident Card
Border Crossing Card
DHS-designated enhanced driver's license
Driver's Licenses or other state photo identity cards issued by Department of Motor
Vehicles (or equivalent)
Native American Tribal Photo ID
HSPD-12 PIV Card
An airline or airport-issued ID (if issued under a TSA-approved security plan)
A foreign government-issued passport
Canadian provincial driver's license or Indian and Northern Affairs Canada (INAC) card
Transportation Worker Identification Credential (TWIC)
Non-US/Canadian citizens are not required to carry their passports if they have documents
issued by the U.S. government such as Permanent Resident Cards. Those who do not
should be carrying their passports while visiting the U.S.
When processing through a screening checkpoint, each traveler is allowed one bag in order to
limit the total volume of liquids, aerosols and gels. Consolidating products into one bag and X-
raying them separately from the carry-on bag enables security officers to quickly clear all items.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 23
3-1-1 for carry-ons = 3.4 ounce (100ml) bottle or less (by volume); 1 quart-sized, clear, plastic,
zip-top bag; 1 bag per passenger placed in screening bin. One-quart bag per person limits the
total liquid volume each traveler can bring. 3.4 ounce (100ml) container size is a security
measure.
Be prepared. Each time TSA searches a carry-on it slows down the line. Practicing 3-1-1 will
ensure a faster and easier checkpoint experience.
3-1-1 is for short trips. If in doubt, consider putting your liquids in checked luggage.
Declare larger liquids. Medications, baby formula and food, and breast milk are allowed in
reasonable quantities exceeding three ounces and are not required to be in the zip-top bag.
Declare these items for inspection at the checkpoint. Officers may need to open these items to
conduct additional screening.
Before you fly, understand everything you can and cannot bring when you travel by air by reading the list of permitted and prohibited items available at: http://www.tsa.gov/traveler-information/prohibited-items Driving When departing aboard a vehicle from home base or from a pre-designated AMR/FEMA reserve cache site, personnel shall call NATCOM dispatch at 866.219.9253 (or other designated number) so they can be entered into the NATCOM CAD. Network Provider should provide AMR’s National Command Center (NATCOM) an estimated time of arrival (ETA) to the official check-in location. While enroute to check-in, Network Provider should give periodic progress updates every 2 hours with status and location of deployed units. If any problems are encountered along the way, call NATCOM dispatch at 866-219-9253 (or other designated number). Vehicles shall not be driven faster than the legal, safe speed for the current road, weather, and traffic conditions. NATCOM will make the decision and advise if driving in emergency mode (lights and siren) is authorized. Company policies and procedures remain enforce during the entire deployment. All breakdowns while traveling to the check-in site should be reported to NATCOM dispatch at 866.219.9253 (or other designated number). If you are driving in a convoy and one unit breaks down, it is not necessary for all the other ambulances to stay with that unit. Other vehicles should continue to the check-in site once the disabled unit is secure. Personnel from the disabled unit should board another vehicle and continue on to the check-in with the rest of the team. Check-In Process Prior to entering the TOO you must be formally checked-in. This is a formal process during which time you will officially check-in your vehicle (if applicable) and when you will officially register yourself as an event responder. If on a vehicle you may also receive equipment such as a two-way radio/phone, GPS navigator or a transponder. A technical specialist will install any equipment needed for the deployment. As a responder you will be classified as one of the following:
Ground Ambulance responder

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 24
Paratransit responder
Air Ambulance responder
Air Medical Support Team
Fixed Site Personnel
Incident Management Team
Operations Support Team
Communications Support Team
As stated above, you will be required to officially check-in using the appropriate check-in sheet and the Responder Registration Form. Examples of all check-in forms and the Responder Registration Form can be found in Appendix 3: Deployment Check-In Forms. Be prepared to produce copies of all credentials that demonstrate deployment eligibility. Demobilization Check out process—Prior to leaving for your home base you must be formally checked out and demobilized. This is a formal process during which you will be required to turn in the AMR/FEMA Radio/Phone, GPS navigator, and any other equipment you were issued. A
company specialist will remove any equipment that has been temporarily installed for this
deployment. Check‐out/demobilization personnel will notify the AMR National Emergency
Communications Center that you have been officially checked out. On your way home—You will be called by NATCOM dispatch approximately every three hours. If you do not hear from a NATCOM dispatcher after three hours, please call in to NATCOM dispatch at 866‐219‐9253 and check‐in. If you have ANY problem along the way, call NATCOM
dispatch at 866‐219‐9253. Under no circumstances should any units return home in the emergency mode (lights and siren). Company policies and procedures remain enforce when returning home, including use of alcohol and harassment. Receipts for food, fuel and lodging are required for reimbursement. You should return directly home using the fastest route. Only stops for fuel and food are authorized. Any exceptions must be approved by AMR NATCOM. Arrival at home base
Driving home—When you arrive back at your home base it will be your responsibility to report your arrival to NATCOM dispatch at 866‐219‐9253. If for some reason you do not return
directly home, you must inform the Demobilization Officer at the time you check‐out. Any units that are traveling great distances and plan to stop for sleep/rest, should inform the Demobilization Officer. Lodging needs should be discussed with your manager. Flying home—If you are driving a company vehicle to a staging/storage area and then flying home, you should notify NATCOM dispatch when you drop off your vehicle. You do not need to notify them when you arrive home from your flight. Documentation Accurate and timely documentation aids in the tracking and accountability of resources, provides information on the type and quantity of services delivered, and creates an historical record that can be used to validate services rendered and improve future responses.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 25
The two primary forms that will be utilized by crewmembers will be the Unit Activity Log (ICS-214 Ground Ambulance, ICS-214 Paratransit, ICS 214 Fixed Site Support and ICS-214 Miscellaneous) and the Disaster Patient Encounter Form. The ICS-214 must be completed for each operational period for each resource vehicle or crew and submitted to leadership as instructed. A Disaster Patient Encounter Form must be completed by all ground ambulance crews anytime that a caregiver-patient relationship is established. This includes patients that refuse medical care or transportation. AMR documentation must be completed in addition to whatever forms are required by the host organization. AMR documents are legal property of AMR and are to be submitted to AMR authorized leadership only. Examples of ICS 214 forms and Disaster Patient Encounter form can be found in Appendix 4: Deployment Documentation. Billing for services AMR is contracted with the United States Government under the Federal EMS Contract. Ground Ambulance, Air Ambulance, Paratransit resources, or individuals shall not under any circumstances bill or charge for services. Reimbursement and expense It is advised to keep all receipts for expenses incurred during a deployment especially receipts associated with meals, lodging, and travel expenses. Remember an original supplier receipt showing company name, address, date of transaction, each item purchased, cost and form of payment must be obtained and retained for every expense submitted. Emergency Response Team members are expected to use good judgment before incurring any expense during a deployment and “do the right thing” if a situation arises that is not covered by policy. Contact the appropriate AMR Incident Management Team member or NATCOM if questioning a potential expense. AMR assumes no obligation to reimburse employees for expenses NOT in compliance with policy or deemed unnecessary. Credentials and Identification Badges
EMS personnel participating in a deployment shall be appropriately licensed or credentialed in their state of origin to function at that skill level within the TOOs. Caregivers shall keep copies of their credentials readily available at all times during a deployment should they need to be verified. For a more detailed description of Credentialing, see Appendix 5: Credentials and Identification Badges. Release of Information for AMR/FEMA Federal EMS Activities
Confidentiality and Non-Disclosure - Subcontractors To the extent that work under AMR/FEMA Federal EMS Contract may provide Subcontractors with sensitive or proprietary business, technical, or financial information belonging to the Government, AMR and its Subcontractors shall, after receipt thereof, treat such information as confidential and not secure such information for its own use or disclose such information to third parties unless specifically authorized by AMR and the Government in writing. DHS Non-Disclosure Agreement As a federal contractor and authorized entity, AMR and its subcontractors are bound by the U.S. Department of Homeland Security (DHS) regulations that govern the release of certain

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 26
information. The DHS requires that subcontractors sign a “Non-Disclosure Agreement”, DHS Form 11000-6(08-04). This document defines three categories of information that may not routinely disclosed. This information includes, but is not limited to the following: A) protected critical infrastructure information (PCII), B) sensitive security information (SSI), and C) other sensitive but unclassified information (SBU). The United States Government has placed special confidence and trust in those who perform pursuant to the Federal EMS Contract and they are obligated to protect this information from unauthorized disclosure, in accordance with the laws, regulations, and directives applicable to the specific categories of information to which they are granted access. Federal EMS contractors and subcontractors will not disclose or release any information provided to them without authorization. Should situations arise that warrant the disclosure or release of such information, they will do so only under approved circumstances in accordance with laws, regulations, or directives applicable to the specific categories of information. They will honor and comply with any dissemination restrictions cited or verbally relayed to them by the proper authority. Any materials in their possession containing information covered by this Position Statement, will be handled and safeguarded in a manner that affords sufficient protection to prevent the unauthorized disclosure of or inadvertent access to such information. Federal EMS contractors and subcontractors shall return all information to which they have had access or which is in their possession 1) upon demand by an authorized individual; and/or 2) upon the conclusion of their duties, association, or support to the Department of Homeland Security; and/or 3) upon determination that their official duties do not require further access to such information. They shall report any loss, theft, misuse, misplacement, unauthorized disclosure, or other security violation, they have knowledge of and whether or not they are personally involved. Administratively Confidential Information The contractor and its subcontractors shall not publish or otherwise disclose, except to the Government and except matters of public record any information or data obtained hereunder from private individuals, organizations, or public agencies in a publication whereby the information or data furnished by any particular person or establishment can be identified, except with the consent of such person or establishment. Confidentiality of Information To the extent that the work under this contract requires that the Contractor may be given access to sensitive or proprietary business, technical, or financial information belonging to the Government or other companies, the Contractor shall, after receipt thereof, treat such information as confidential and not appropriate such information to its own use or disclose such information to third parties unless specifically authorized by the Contracting Officer in writing. The foregoing obligations, however, shall not apply to information that —
At the time of receipt by the Contractor, is in the public domain
Is published by others after receipt thereof by the Contractor or otherwise becomes part of the public domain through no fault of the Contractor
The Contractor can demonstrate was already in its possession at the time of receipt thereof and was not acquired directly or indirectly from the Government or other companies
The Contractor can demonstrate was received by it from a third party that did not require the Contractor to hold it in confidence.
Media Request

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 27
Federal EMS responses will likely attract media attention and maintaining positive relationships with the news media is important. AMR and subcontractors must take special care to ensure that communications with the media are accurate, consistent, and reflect the positions of AMR and FEMA on any matter related to the Federal EMS response. As healthcare providers, extra precautions must be taken to assure that patient privacy is protected as directed by HIPAA and other relevant laws and regulations. While it is an honor and privilege to be deployed as a Federal EMS responder, it must be understood that Federal EMS responders will defer any media request to the AMR Office of Emergency Management (OEM). This includes any media request for information, photography, video, or other medium. The OEM may be required to refer certain media requests to the FEMA PIO. Social Media Use of social media to provide and receive information to the public before, during, and after a disaster can be beneficial. Social networks can also provide an easy conduit for leakage of mission-critical and confidential information. There are several challenges associated with the use of social media during Federal deployments, especially concerning user privacy and the use of personally identifiable information (PII); the need to remove details when sharing information across multiple partners; and the security of networks, platforms, tools, and data. Misinformation can spread via social media very quickly, especially during an emergency. Federal EMS responders shall not allow the use of nonpublic information to further their own private interest or that of another. Responders using social media shall not identify themselves as part of the AMR/FEMA Federal EMS Response. All Company and Government contractor rules regarding confidential information apply in full to blogs and social networking sites. Any information that cannot be disclosed through a conversation, a note or an e-mail, also cannot be disclosed on a blog or social networking site. Transmission of any information in any forum that is discriminatory, defamatory or malicious is forbidden. Transmission of any information associated with the deployment activities is prohibited unless approved by the OEM and FEMA. HIPAA Privacy and Security Rule The Health Insurance Portability and Accountability Act of 1996 (HIPAA) required the Secretary of the U.S. Department of Health and Human Services (HHS) to develop regulations protecting the privacy and security of certain health information. The Privacy Rule, or Standards for Privacy of Individually Identifiable Health Information, establishes national standards for the protection of certain health information. The Security Standards for the Protection of Electronic Protected Health Information (the Security Rule) establish a national set of security standards for protecting certain health information that is held or transferred in electronic form. The Security Rule operationalizes the protections contained in the Privacy Rule by addressing the technical and non-technical safeguards that organizations called “covered entities” must put in place to secure individuals’ “electronic protected health information” (e-PHI). Federal EMS responders are bound by applicable HIPAA Privacy and Security Rules. Authorized Entities During Federal EMS deployments, AMR and its authorized subcontractors will provide information to authorized entities delivered in a proprietary manner. Such entities may include FEMA, U.S. Dept. of Health and Human Services (HHS) (if approved by FEMA), authorized healthcare facilities that receive patients, or State EMS regulatory agencies who by state law are authorized to receive such information. Historically AMR provides information to FEMA who in turn provides certain approved entities with quantitative information and types of services provided pursuant to the deployment, but they do not divulge any proprietary information that would identify patients or AMR’s Federal EMS subcontracted providers by name or location. AMR supports this process.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 28
Breach of Contract and Tortious Interference AMR and its subcontractors would object to providing any identifying information, except in a proprietary manner to FEMA, HHS (if approved by FEMA), authorized healthcare facilities that receive patients, or State EMS regulatory agencies. It could possibly be a breach of contract and confidentiality for AMR, as the FEMA Federal EMS Contractor, to provide any such information that may be disseminated to other parties. Furthermore, if identifying information were provided to unauthorized entities, it could impede AMR’s ability to recruit ambulance companies and other subcontractors to participate in the Federal EMS program. To intentionally interfere with AMR’s contractual relations could be considered tortious interference if it damages the contractual or business relationships. See Appendix 11: DHS Non-Disclosure Agreement.
EMS Scope of Practice, Protocols, Reciprocity, and Medical Control and Direction
Each state defines and regulates the scope of practice for EMS personnel within its borders. It is anticipated that EMS responders from various states may be deployed to disasters pursuant to the AMR/FEMA Federal EMS Contract. For EMS deployments pursuant to the AMR/FEMA Contract, the National EMS Core Content will be used to define the domain of out-of-hospital care. The scope of practice for the AMR/FEMA Contract shall be the National EMS Scope of Practice Model. In the absence of local, state, and regional EMS protocols the DHS-Wide EMS Basic Life Support (BLS) & Advanced Life Support (ALS) Protocols produced by the Department of Homeland Security’s (DHS) Office of Health Affairs (OHA) may be used. Under remote, austere, or hostile conditions, local, state, and regional pre-hospital protocols and medical direction may be inaccessible or impractical, in these situations the DHS OHA Austere Emergency Medical Support (AEMS) Field Guide1 may be used if authorized by the AMR Office of Emergency Management (OEM) medical director. For the complete Scope of Practice guide, see Appendix 6: EMS Scope of Practice, Protocols, Reciprocity, and Medical Control and Direction for AMR/FEMA Federal EMS Deployments.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 29
Appendix 1 Shift and Safety Management Plan
Overview The FEMA Federal EMS Contract requires us to supply enough personnel to provide around the clock coverage in support of contract operations. FEMA has stated that “The contractor shall develop a written management plan that details its protocols to maintain a safe and effective work environment. The contractor has the flexibility to schedule work shifts as they deem appropriate as long as it is consistent with safe, legal operation.”—FEMA Federal EMS Contract Section C, paragraph 9.7 Purpose The purpose of this policy is to comply with the requirements set forth by FEMA and to provide guidance to AMR leadership with regard to staffing and shift lengths during a federal activation. Scope This policy applies to all employees of EVHC and its subsidiaries as well as affiliate employees, including temporary employees and employees of affiliated third-party organizations. Policy Shifts Lengths - Emergency Responder shift lengths will be based on disaster criteria and environment. Factors such as workload distribution, mission intensity, time-on-task, and transport time will influence shift lengths. Typical shifts for EMS personnel in non-disaster situations are 12 hrs, 24 hrs, 36 hrs or even 48 hrs. Shift lengths longer than 12 hrs must include rest periods. The shift lengths are usually based on workload (type of work and volume). During disasters, responders are usually deployed in Strike Teams with usually 5 vehicles of the same type per Strike Team and a designated Strike Team Leader. This configuration may not be applicable in EMS disaster responses since patients are seldom all-ALS or all-BLS. Ambulances are deployed based upon patient condition, acuity level, location, biomedical needs, and overall EMS needs of the situation at hand. This provides for better operational grouping of ambulances. A supervisory element is still needed for organization command and control, and safety monitoring. According to FEMA Typed Resource Definitions – EMS, the recommended shift lengths for Ambulance Strike Team personnel is 12 – 24 hrs, depending on the number of ambulances needed, and they should be self-sufficient for 72 hrs2. Patient Transport Distance – Safety and clinical considerations of transported patients is paramount. It is assumed that transportation vehicles, i.e., buses, ambulances, helicopters and fixed wing aircraft, will make multiple round trips. During disaster evacuations, it is recommended that patients be transported to host locations that are an adequate safe distance from the disaster event but not so distant as to not allow for multiple round trips. Air ambulances are usually used for critical care patients and thus patient transport distances should be short enough that they do not require refueling with patients on board. For these reasons the following transport distance guidelines are established.
Ground Ambulances – one-way distance to transport patients by ground ambulance should not exceed 250 miles or 6 hours. This includes all ground ambulance types: ALS, BLS, Bariatric and Med-Evac Units
Paratransit Vehicles – one-way distance to transport patients by paratransit vehicle should not exceed 250 miles or 6 hours.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 30
Air Ambulance Rotary Wing – one-way distance to transport patients by rotary wing air ambulance is usually 200-400 miles depending upon the specific helicopter.
Air Ambulance Fixed Wing – one-way distance to transport patients by fixed wing air ambulance is usually 400-600 miles depending upon the specific aircraft.
Medical and Physical Fitness Screening – Health screening tool for emergency responders requires a customized risk assessment of the duties and responsibilities of the responder. It must take into consideration the specific anticipated work activities, working conditions, and work settings in which a responder is expected to perform. For this reason, it is not practical to design a comprehensive screening tool that is appropriate for a wide range of emergency personnel. Instead, this document provides a list of the general issues that should be addressed when determining the need for screening of an emergency responder Medical screening should include a medical history and review of systems, a physical examination, and, in some instances, laboratory testing, as indicated by clinical judgment and good occupational medical practice. Pre-deployment biological monitoring for exposure to hazardous chemicals is not generally recommended. Such monitoring is not practical for unanticipated exposures to hazardous chemicals. When exposures to specific chemical agents are predictable, workers should be adequately protected. However, there may be some limited instances in which obtaining baseline clinical specimens before deployment for work in environments with predictable exposures may be helpful in subsequently assessing whether the protections used during this work are adequate and performing as intended. The following are examples of the types of issues that should be considered when determining the need for medical screening. 1. Response Settings and Conditions
Austere settings (temperature stress and few services/supplies)
Disaster zone settings (physical hazards, contaminated floodwaters, infectious vectors)
Hazardous materials release or uncharacterized and complex exposure zones (industrial explosions, major structural collapses, commercial transportation crash)
Radiation or nuclear contamination settings
Long work hours
Inconsistent opportunities for rest and nutrition 2. Response Tasks
Heavy lifting or physical exertion
Hazardous duty requiring use of heavy or cumbersome protective equipment
Respiratory protection requirements 3. Personal Risk Factors
Chronic illness, degree of medical control, and ability to maintain that control in the field setting; degree of vulnerability or risk of exacerbation given field settings and resources
Drug allergies, particularly to medications used for post-exposure prophylaxis for bio-terror agents
Recent injury and likelihood of repeat injury or undue fatigue
Care, maintenance, and mobility requirements for durable medical equipment or assistance animals; ability to evacuate

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 31
Disaster responders should be healthy enough to function under austere field conditions (possibly no showers, housing in tents, portable toilets, extreme weather conditions and long periods of standing). Physical fitness for duty is assessed in relation to the level of physical activity that may be maximally required from the responder while performing his or her job. The following exemplifies the basic principles upon which medical and physical fitness standards are based when screening emergency responders:
The responder should be physically able to safely perform the usual activities of daily living without requiring direct assistance of another individual or mechanical devices.
The responder should not have an acute, progressive, or recurrent disease or condition that:
o may cause significant functional limitations while performing assigned duties within the essential functions of their response mission,
o could cause the appearance of symptoms or complications that could endanger the safety of self or others during emergency response activities,
o will or may require frequent or prolonged periods of absence from duty, o may make it difficult to wear and use appropriate personal protective gear.
The responder should not be significantly limited in musculoskeletal mobility or exercise tolerance regardless of the assignment given. Routine, ordinary physical activity should not cause undue fatigue, shortness of breath, pronounced muscular weakness, or severe pain.
The responder should be capable of receiving essential and requisite immunizations, prophylaxis, treatments, pharmaceuticals, and other interventions that are necessary to safeguard health and allow assigned duties to be successfully completed.
The responder should be able to independently travel safely to and from the assigned duty area using public or private transportation. Likewise, the individual should be capable of traveling on official business without assistance using provided transportation.
Safety - Safety for patients and crews is always the number one priority. All ambulances and paratransit services must be available for response 24/7, and the Incident Management Team (IMT) will ensure that assigned crewmembers are not fatigued to the extent that their safety, the safety of others, or their mission is compromised. 24-hour shifts carry the expectation that crewmembers have time during the shift to rest, but remain available for immediate response to an emergency. If any crewmember, Strike Team Leader, Task Force Leader, Safety Officer (SO) or other appropriate IMT representative believes crews are fatigued to the point they cannot safely carry out a mission, they will be relieved from duty and replaced with rested personnel. All crews will be equipped with some type of communication device in order to conduct well-being checks at specified intervals (usually every 4 hours), so that informed decisions can be made based on real-time information regarding the well-being of crews. Additionally, all crews are instructed that if they feel their safety is in question, they too can contact the local SO to discuss relative options to ensure their well-being. Furthermore, if long distance driving is involved, crews will trade off driving every eight to twelve hours maximum, to assure that everyone has a rest period; specifically when no patient is on board the ambulance. If transport time or the destination point is excessive, arrangements will be made for the crews to rest after unloading the patient.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 32
SAFETY OFFICER (SO) – The SO’s function is to develop and recommend measures for ensuring personnel safety and to assess and/or anticipate hazardous and unsafe situations. The SO has the authority and obligation to alter, delay, suspend, and terminate any and all operations immediately dangerous to life and health of any personnel. Only one primary incident SO will be assigned for each incident. The SO may have assistants, as necessary, and the assistants may also represent assisting agencies or jurisdictions. Safety assistants may have specific responsibilities, such as air operations, hazardous materials (HAZMAT), etc. All SOs are certified/qualified to the level of operations being performed The major responsibilities of the SO are: Participate in tactics and planning meetings, as well as other meetings and briefings as
required. Identify hazardous situations associated with the incident. Dedicate Emergency Medical Services (EMS) personnel needed for responders (ICS
206). Develop the Risk/Hazard Analysis (ICS 215a) with the Operations Section Chief (OSC). Coordinate with law enforcement to provide security and control of perimeters. Ensure the selection of Personal Protective Equipment (PPE) and other equipment
meets the needs of the incident. Ensure that personnel accountability system is in place for all personnel. Ensure that working conditions are monitored and work/rest guidelines are adhered to. Provide a mechanism for responders to report fatigue or other safety issues to the SO. If any crewmember, Strike Team Leader, Task Force Leader, Safety Officer or other
appropriate AMR or government representative believes EMS responders are fatigued to the point they cannot safely carry out a mission, the SO will relieve them of duty and replace with them rested personnel.
Designate emergency evacuation guidelines. Review the IAP for safety implications. Provide safety advice in the IAP for assigned responders. Ensure identified resources are in place to meet the mental health needs of responders. Exercise emergency authority to stop and prevent unsafe acts and notify IC. Investigate accidents that have occurred within the incident area. Assign assistants, as needed. Review and approve the Medical Plan (ICS 206). Ensure that all required agency forms, reports, and documents are completed prior to
demobilization. Brief the IC on safety issues and concerns. Have a debriefing session with the IC prior to demobilization. Maintain a Unit Log (ICS 214).

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 33
Appendix 2 Deployment Uniform Policy Overview The Office of Emergency Management (OEM) believes that individuals deployed as Federal Contractors should take pride and have integrity in their professional appearance and grooming habits. The identification and appearance of all personnel involved in a disaster response is an important concern. Whether dealing with government officials, other disaster response professionals or the public in a direct or indirect manner it is essential that all team members project a professional image and are clearly identified. Purpose The purpose of this policy is to clearly define employee appearance including uniform and grooming during activation of the Federal EMS Contract. Scope This policy applies to all AMR employees deployed in support of the Federal EMS Contract. Policy The standards of dress and grooming should be in compliance with the accepted business practices and safety considerations for disaster situations. The following guidelines provide an understanding of what AMR considers acceptable and unacceptable grooming and attire. Leaders may direct any team member who reports un-groomed or in unacceptable attire to remedy the situation. All team members shall wear an identification badge that display’s AMR’s name, delineation as a FEMA contractor, and the title or level of service of the individual. All responders shall carry their state driver’s license and healthcare provider certification at all times. Identification badges must be in plain view and located above the waist. If not readily apparent, team members shall identify themselves as “Contractors”. ERT members who are subcontractors and not AMR employees shall also carry company identification from their home organization at all times. The following guidelines provide an understanding of what AMR considers acceptable and unacceptable grooming and attire. Grooming Emergency Response Team members are to follow general hygiene principles. Team members must be cleanly shaven when reporting for duty. Sideburns, mustaches, and beards should be neatly trimmed and comply with all safety regulations. Any body piercing that interferes with the professional performance of your job is prohibited. Hair Hair must not be worn in extreme or fad styles or in such a way that exceeds length (collar) or bulk (3 in.) standards. Hair must be clean, neat and well-groomed. Excessive amounts or greasy creams, oils or sprays cannot be used on duty. Hair that is dyed should be of natural coloring. Cosmetics Make-up must be conservative and in good taste and not considered gaudy. Employees will be required to alter cosmetics if deemed inappropriate by IMT.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 34
Fingernails Nails must be neat, clean and trim. Color polish is allowed for female employees. Ornaments or nail attachments are not allowed. Jewelry
Only female employees may wear small, tight-fighting earrings. Only one earring per lobe is permitted.
Rings are allowed on one finger of each hand and should not disrupt the integrity of gloves.
Visible body piercings are not allowed. Uniforms OEM approved uniforms shall be worn at all times when on an active shift. Approved attire consists of:
AMR/Company issued uniform shirt or OEM ERT t-shirt
AMR/Company issued pants (regular or BDUs)
AMR/Company issued jacket, sweater and/or rain gear - as applicable to weather
Uniform type boots are recommend due to the potential for sharp objects
FEMA ID badge – visible and unobstructed
PPE pouch
ERT patch may be worn on uniform shirt according to local uniform policy/guideline and with permission of local leadership
Attire that is not approved for wear during a deployment (on or off shift) includes:
Beachwear –Shorts
Skirts
Swimwear
Halter tops
Sandals – flip flops allowed as shower wear
Visible piercings other than earrings ·
T-Shirts or visible tattoos depicting offensive, sexual, or hate content If in doubt whether attire is appropriate, wear something you know is appropriate and seek guidance from leadership. Accessories Wristwatches, belts, glasses and pens are allowed as long as they are not bright colors or fad designs. IMT For Incident Management Team (IMT) positions and above, modified business casual attire is required along with the appropriate IMT position vest. Official AMR Emergency Response Team labeled button-up or polo style shirts are preferred. Denim jeans may be worn. Jeans must be suitable for the environment and may not be low cut, or be excessively worn, have holes, tears or patches.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 35
Appendix 3 Deployment Check-In Forms
Personnel Registration Form

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 36
Ground Ambulance/Paratransit Check-In Form

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 37
Air Ambulance Check-In Form

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 38
Fixed Site Personnel Check-In Form

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 39
Appendix 4 Deployment Documentation ICS 214 Ground Ambulance

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 40
ICS 214 Paratransit
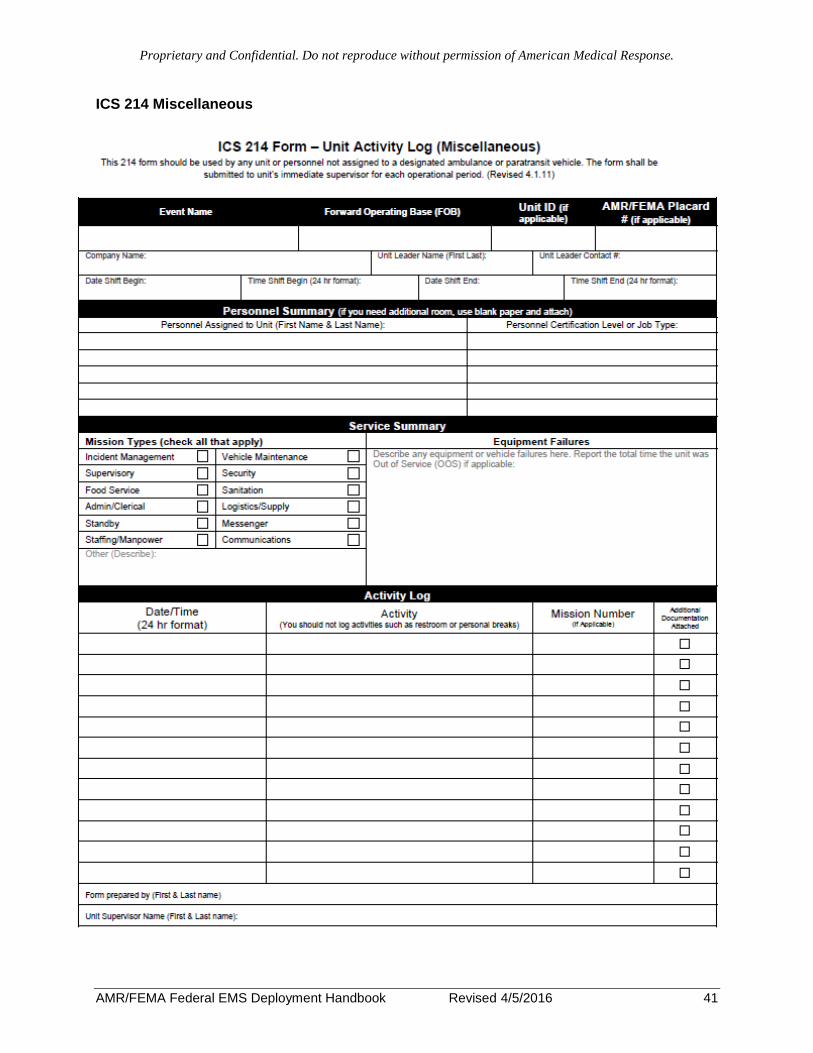
Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 41
ICS 214 Miscellaneous

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 42
ICS 214 Fixed Site & Multi-Modal Support

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 43
Disaster Patient Encounter Form

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 44
AMR Disaster Response Form Definitions Helpful Definitions related to the Ground Ambulance, Paratransit and Miscellaneous Vehicle Activity Logs (Form 214) and Disaster Patient Encounter documents. (Note: there are three different types of 214s; not all data blocks will be used on each type of 214) Demographic Data – Definitions FEMA Placard #: The Identification Number located on the Placard that should be
displayed on every response vehicle. The Placard # is used to identify a unique resource throughout a deployment.
Event Name: The name of the event or disaster. ex: Hurricane Katrina
Forward Operating Base (FOB):
The location where the deployed resources are assigned to and where they carried out the activities that they documented on the 214 Unit Log.
Company Name: The name of the home company the resource originated from. ex: Tri-County EMS, AMR San Diego.
Company Vehicle ID #:
The unit number of the vehicle. This is the bumper number, fender number or visible designation assigned to the resource by the home company. ex: Medic 34, Unit 3, Van 42.
Vehicle Type: The type of vehicle that the resource is classified. Ex: ALS Ground Ambulance, Type 1 Paratransit, command vehicle, etc.
Vehicle License Plate #:
The vehicle’s state issued license plate number.
State EMS Vehicle Permit #:
State issued EMS permit # as issued by the vehicle’s home state.
State of Origin: Indicate what state the vehicle originated from. Date Shift Begin: This is the Date that the Current Shift began for the resource. Time Shift Begin: This is the Time that the Current Shift began for the resource. 24 hour
time preferred or make sure you include AM or PM. Date Shift End: This is the Date that the Current Shift ended for the resource. Time Shift End: This is the Time that the Current Shift ended for the resource. 24 hour
time preferred or make sure you include AM or PM. Driver Name: Name of Primary Driver assigned to vehicle. Medic/Attendant Name:
Name of Primary Attendant assigned to vehicle (EMTs, Paramedics)
3rd Rider Attendant Name:
The Name of any 3rd rider or external agency assistant, navigator or observer assigned to the resource.
Certification Level: Certification levels include: EMT-B, EMT-I, Paramedic, RN, MD etc.
Mission Types – Definitions
Evacuation: An individual is being transported for the primary purpose of moving them out of harm’s way or out of a potentially dangerous area.
Repatriation: Returning an evacuee from a host location back home or if unable to return home to the place where they will be temporarily relocated.
Emergency Call: Responded to or dispatched to an emergency scene or a patient encounter that resulted in a need for transport to an emergency department for treatment of illness or injury.
Medical Transfer: A facility to facility medical transfer or other non-emergency medical transfer such as residence to dialysis or hospital discharges. If the mission is for the purpose of Repatriation or Evacuation it is not a

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 45
Medical Transfer.
Standby: The assignment is of an EMS Standby nature. Examples include: a Standby to support search & rescue operations, power or utility company operations, local police, or being posted at a shelter or distribution site for the purpose of providing ambulance service if needed.
Staffing/Manpower: The assignment does not have the potential to require the transportation of patients. Examples: EOC, Hospital, or Shelter Staffing
Utilization – Definitions Total # of Assigned Missions:
Total Missions is the total number of assignments that the resource responded to for the time period.
Total # of Patient Contacts:
Total Patient Contacts is the number of people that a resource encountered as a patient. A Disaster Patient Encounter form should be completed for each Patient Contact.
Total # of People Transported:
This is the total number of people transported throughout the course of your assigned missions.
Total Green, Yellow, Red, or Black:
Using the START Triage system, indicate the total number of each patient acuity type you encountered during your operational period.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 46

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 47
Appendix 5 Credentials and Identification Badges Overview The Office of Emergency Management (OEM) collects and maintains federally required licenses and certifications for all members of the Emergency Response Team (ERT). Each member must meet specific requirements to be eligible for the ERT (outlined below). Purpose The purpose of this policy is to clearly define required and accepted forms of credentials for all AMR employees and subcontracted personnel during activation of the Federal EMS Contract. Scope This policy applies to all employees of Envision and its subsidiaries as well as affiliate employees, including temporary employees and employees of affiliated third-party organizations. Policy EMS personnel participating in a deployment shall be appropriately licensed or credentialed in their state of origin in order to function at that skill level within federally declared disaster area. Caregivers shall keep copies of their credentials readily available at all times during a deployment should they need to be verified. Minimum credentials for caregivers shall include:
IS-100.b (Introduction to Incident Command System)
IS-700.a (National Incident Command System, An Introduction)
IS-800.b (National Response Framework, An Introduction)
State EMS Certification (EMR, EMT, AEMT, EMT-Paramedic, RN, etc.)
State Driver’s License
Hazmat Awareness
Emergency Vehicle Operations Course
Hepatitis B vaccination or signed declination statement
Additional credentials are required for Strike Team Leader/ Task Force Leader
IS-200.b (ICS for Single Resources and Initial Action Incidents)
IS-300 (Intermediate ICS)
IS 701.a (NIMS Multiagency Coordination System Course)
IS 703.a (NIMS Resource Management) More information including a detailed reference sheet concerning credentials is available online at http://www.amr.net/Emergency-Response-Team All team members shall wear an official OEM-issued ERT identification badge that displays AMR’s name, delineation as a FEMA contractor, and the title or clinical level of practice of the individual. All responders shall carry their state driver’s license and healthcare provider certification at all times. Identification badges must be in plain view and located above the waist. Identification badges are authorized for use ONLY during activation of the National Ambulance Service Contract or other OEM-approved deployments and responses. Employees shall not

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 48
wear or display OEM-issued identification badges except while performing duties directly related to officially sanctioned OEM events. NIMS Credentialing The National Incident Management System (NIMS) has established a credentialing process for validating the qualifications of personnel and assessing their background, for authorization and permitting/granting access to an incident. This process, endorsed by AMR, is required of all subcontracted network providers. It is an objective evaluation and documentation of a person’s current licensure or degree; training or experience; competence or certification, and the ability to meet a nationally accepted minimum standard; to provide particular services; and/or functions or perform particular procedures during an incident. The National Credentialing Definition and Criteria can be found at: http://www.fema.gov/pdf/emergency/nims/ng_0002.pdf Badges are renewed periodically for those members whose on-file certifications/licensees are current and up-to-date.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 49
Appendix 6 EMS Scope of Practice, Protocols, Reciprocity, and Medical Control and Direction for AMR/FEMA Federal EMS Deployments American Medical Response (AMR) is under contract with the Federal government to provide EMS in response to Federally-declared disasters and other Federal events as approved by FEMA. Each state defines and regulates the scope of practice for EMS personnel within its borders. It is anticipated that EMS responders from various states may be deployed to disasters pursuant to the AMR/FEMA Federal EMS Contract. The purpose of this guide is to establish clinical guidelines, a minimum scope of practice, and reciprocity procedures for all authorized EMS disaster providers, regardless of their state of origin. This guide is limited to those EMS responders who are officially deployed by AMR to respond to Federal disasters pursuant to the AMR/FEMA Contract. For EMS deployments pursuant to the AMR/FEMA Contract, the National EMS Core Content3 will be used to the domain of out-of-hospital care. It specifies what knowledge and skills are necessary and will also determine how these tasks will be performed. The scope of practice for the AMR/FEMA Contract shall be the National EMS Scope of Practice Model4 which specifies who (which level of practice) will perform specific skills and how much knowledge providers will have at each level. The National Model EMS Clinical Guidelines5 were approved by the National Association of State EMS Officials (NASEMSO) to provide a resource to prehospital clinical practice, maximize patient care, safety and outcomes. They are a set of clinical guidelines that can be used “as is” or adapted for use on a state or regional level to ensure a more standardized approach to the practice of patient care. In the absence of local, state, and regional EMS protocols the DHS-Wide EMS Basic Life Support (BLS) & Advanced Life Support (ALS) Protocols6 produced by the Department of Homeland Security’s (DHS) Office of Health Affairs (OHA) may be used. Under remote, austere, or hostile conditions, local, state, and regional prehospital protocols and medical direction may be inaccessible or impractical, in these situations the DHS OHA Austere Emergency Medical Support (AEMS) Field Guide7 may be used if authorized by the AMR Office of Emergency Management (OEM) medical director. Role of the National EMS Scope of Practice Model The National EMS Scope of Practice Model shall be used to identify the psychomotor skills and knowledge necessary for the minimum competence of each nationally identified level of EMS provider who responds to an event pursuant to the AMR/FEMA Federal EMS Contract. It divides the core content into levels of practice, defining the minimum corresponding skills and knowledge for each level. The Role of State Government State EMS offices have statutory authority, scope, and jurisdiction to regulate and coordinate the provision of EMS within its borders for conventional emergency care or when the need arises to provide contingency or crisis care. The state EMS office may be responsible for requesting and coordinating federal medical assets. The State determines the scope of practice of State-licensed EMS personnel within its jurisdiction. The National EMS Scope of Practice Model is a consensus-based document that was developed to improve the consistency of EMS personnel licensure levels and nomenclature among States; it does not have any regulatory authority. It represents a transition from the historical connection between scope of practice and the EMS National Standard Curricula. It is a

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 50
document, guided by data and expert opinion that reflects the skills representing the minimum competencies of the levels of EMS personnel. The Scope of Practice Model will serve EMS in the future, as it is revised and updated to include changes in medical science, new technology, and research findings. While each State has the right to establish its own levels of EMS providers and their scopes of practice, staying as close to this Model as possible, and especially not going below it for any level, will facilitate reciprocity, standardize professional recognition, and decrease the necessity of each State developing its own education and certification materials. Some states permit licensed EMS personnel to perform skills and roles beyond the minimum skill set as they gain knowledge, additional education, experience, and (possibly) additional certification. The adoption of skills and roles beyond those in the Model will diminish national consistency and may impede interstate mobility and legal recognition for EMS personnel. If the EMS regulatory authorities in disaster-affected states wish to have AMR/FEMA EMS Contract providers perform skills beyond their legal scope in their state of origin, the disaster state must provide the additional education and certification. Levels of EMS Certification Emergency Medical personnel have designations or titles based upon the amount of education and scope of care they provide to patients. The National EMS Scope of Practice Model and the National Registry of EMTs defines and describes four certification or licensure levels of EMS provider8. It establishes a framework that ultimately determines the range of skills and roles that an individual possessing a state EMS license is authorized to do in a given EMS system. The primary purpose of National EMS Certification is to protect the public by assuring EMS providers can safely and effectively practice at the entry level competencies. National EMS Certification is delivered by the National Registry of EMTs (NREMT) in all 50 states. Most states, the District of Columbia, the US Army, US Air Force, and the Department of Homeland Security require successful completion of the National EMS Certification process to obtain a license to deliver care as part of their initial licensure process. National EMS Certification also facilities interstate movement of EMS personnel as 49 states recognize the NREMT certifications for reciprocity. No EMS provider can work with National EMS Certification alone; all must possess a state license or authorizing agency designation to work. Individual state EMS rules or regulations may further define EMS provider scope of practice. Below are the designations and a description for each.
Emergency Medical Responder (EMR) The primary focus of the Emergency Medical Responder is to initiate immediate lifesaving care to critical patients who access the emergency medical system. This individual possesses the basic knowledge and skills necessary to provide lifesaving interventions while awaiting additional EMS response and to assist higher level personnel at the scene and during transport. Emergency Medical Responders function as part of a comprehensive EMS response, under medical oversight. Emergency Medical Responders perform basic interventions with minimal equipment.
Emergency Medical Technician (EMT) The primary focus of the Emergency Medical Technician is to provide basic emergency medical care and transportation for critical and emergent patients who access the emergency medical system. This individual possesses the basic knowledge and skills necessary to provide patient care and transportation. Emergency Medical Technicians function as part of a comprehensive

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 51
EMS response, under medical oversight. Emergency Medical Technicians perform interventions with the basic equipment typically found on an ambulance. The Emergency Medical Technician is a link from the scene to the emergency health care system.
Advanced Emergency Medical Technician (AEMT) The primary focus of the Advanced Emergency Medical Technician is to provide basic and limited advanced emergency medical care and transportation for critical and emergent patients who access the emergency medical system. This individual possesses the basic knowledge and skills necessary to provide patient care and transportation. Advanced Emergency Medical Technicians function as part of a comprehensive EMS response, under medical oversight. Advanced Emergency Medical Technicians perform interventions with the basic and advanced equipment typically found on an ambulance. The Advanced Emergency Medical Technician is a link from the scene to the emergency health care system.
Paramedic The Paramedic is an allied health professional whose primary focus is to provide advanced emergency medical care for critical and emergent patients who access the emergency medical system. This individual possesses the complex knowledge and skills necessary to provide patient care and transportation. Paramedics function as part of a comprehensive EMS response, under medical oversight. Paramedics perform interventions with the basic and advanced equipment typically found on an ambulance. The Paramedic is a link from the scene into the health care system. Reciprocity All EMS providers responding pursuant to the AMR/FEMA Federal EMS Contract are licensed or certified in their state of origin. The National EMS Core Content and the National EMS Scope of Practice Model are used to establish minimum competency for state licensure and practice. All states should therefore grant reciprocity to EMS providers responding pursuant to the AMR/FEMA Federal EMS Contract. The following language may be used by State Medical Directors or other licensing or regulatory authority in the affected state(s): AMR/FEMA EMS Reciprocity Authorization All EMS providers responding to (name of jurisdiction) under the AMR/FEMA Federal EMS Contract, who are currently state-licensed or certified in their home state, shall be granted reciprocity to practice at their respective level of certification or licensure while officially deployed. ________________________________________________ __________________________ (Signature & Title of granting authority) Date Scope of Practice During Disasters, Public Health Emergencies, and Extraordinary Circumstances It is virtually impossible to create a scope of practice that takes into account every unique situation, extraordinary circumstance, and possible practice situation during disasters. This is further complicated by the fact that EMS personnel are an essential component of disaster preparedness and response. In many cases, EMS personnel are the only medically trained individuals at the scene of a disaster when other health care resources may be overwhelmed.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 52
This document cannot account for every situation, but rather is designed to establish a system that works for entry-level personnel under normal circumstances. It is assumed that the scope of practice of EMS personnel may be modified or changed in times of disaster or crisis with proper education, medical oversight, and quality assurance to reasonably protect patient safety.2 Crisis Standards of Care for Use in Disaster Situations For disaster scenarios in which the health system may be stressed to its limits, it is important to describe the conditions under which standards of care would change due to shortage of critical resources. “Crisis Standards of Care” is defined as a substantial change in usual health care operations and the level of care it is possible to deliver, which is made necessary by a pervasive (e.g., pandemic influenza) or catastrophic (e.g., earthquake, hurricane) disaster. This change in the level of care delivered is justified by specific circumstances and is formally declared by a state government, in recognition that crisis operations will be in effect for a sustained period. In disaster situations, tribal or state governments should authorize appropriate agencies to institute crisis standards of care in affected areas, adjust scopes of practice for licensed or certified healthcare practitioners, and alter licensure and credentialing practices as needed in declared emergencies to create incentives to provide care needed for the health of individuals and the public. The formal declaration that crisis standards of care are in operation enables specific legal/regulatory powers and protections for healthcare providers in the necessary tasks of allocating and using scarce medical resources and implementing alternate care facility operations.9 The goal of the health and medical response to a mass casualty event is to save as many lives as possible. To achieve this goal, health and medical care will have to be delivered in a manner that differs from the standards of care that apply under normal circumstances. The U.S. Department of Health and Human Services, Agency for Health Care Research and Quality has prepared a document, Altered Standards of Care in Mass Casualty Events10, which addresses some of these issues. Some of the key elements of an EMS mass casualty response are summarized below.
The goal of an organized and coordinated response to a mass casualty event should be to maximize the number of lives saved.
Changes in the usual standards of health and medical care in the affected locality or region will be required to achieve the goal of saving the most lives in a mass casualty event. Rather than doing everything possible to save every life, it will be necessary to allocate scarce resources in a different manner to save as many lives as possible.
The basis for allocating health and medical resources in a mass casualty event must be fair and clinically sound. The process for making these decisions should be transparent and judged by the public to be fair.
Protocols for triage need to be flexible enough to change as the size of a mass casualty event grows and will depend on both the nature of the event and the speed with which it occurs.
Only the authorized healthcare regulatory authority for the disaster has the authority to activate or sanction the use of altered standards of care under certain conditions.
Legal issues related to liability, licensing, and intergovernmental or regional mutual aid agreements must be addressed.
In 2012 the National Academy of Sciences, Institute of Medicine (IOM), published the document, Crisis Standards of Care – A Systems Framework for Catastrophic Disaster

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 53
Response11 which states that public health disasters justify temporarily adjusting practice standards and/or shifting the balance of ethical concerns to emphasize the needs of the community rather than the needs of individuals. Therefore, professional care delivered in a catastrophic disaster may need to be modified to address the demands of the situation, including by focusing more intently on the needs of the entire affected community. State EMS offices and prehospital care agencies should be actively engaged in the development and implementation of crisis standards of care (CSC) plans. Adjustments to scopes of practice, treatment modalities, and ambulance staffing and call response will all figure significantly into state, local, and EMS agency-specific disaster response plans. Other areas that can be leveraged to maximize scarce EMS resources include the authority to activate restricted treatment and transport protocols, which may entail modifying the emergency medical dispatch criteria implemented at public safety answering points (PSAPs). The emergency health care system will be stressed to its limits during a mass casualty incident. Dispatch and regional call centers, local EMS agencies, and hospital will undertake contingency measures utilizing their emergency operations plans and medically approved protocols to implement surge medical capabilities. These measures may include
EMS agencies requesting assistance from neighboring jurisdictions for personnel and equipment through mutual-aid agreements;
PSAPs and call centers altering their dispatch protocols, sending fewer resources, and allowing EMS providers to respond to fewer requests for assistance;
Transport destinations being adjusted to allow transport to clinics or other alternate sites of care in addition to hospitals;
EMS personnel utilizing disaster triage system (sort, assess, life-saving interventions, treatment/transport; simple triage and rapid treatment [START]; and JumpSTART triage methods so they can assess patients within 60 seconds and categorize them for immediate or delayed care; and
EMS personnel utilizing the National Incident Management System (NIMS) incident command system (ICS), which provides a consistent model for all organizations involved in the disaster response.
Fundamental changes in prehospital care may result during a disaster, including a change in the scope of practice of EMS personnel to allow them to administer vaccines or perform other tasks for which they receive just-in-time training. EMS personnel may be asked to function in extraordinary settings, such as shelters, alternate care sites, patient receiving centers, clinics, and tented free-standing medical units. They may be asked to alter the staffing levels for an ambulance, utilizing a driver and one medical attendant; use other modes of transportation, such as vans and buses; or not transport at all by treating and releasing patients. Extraordinary circumstances may require EMS personnel to assist in the evacuation of patients at a health care facility to alternate care sites. This, in turn, may require them to provide care to patients for longer than usual for EMS providers, who normally provide care for patients at the scene and during transport and transfer. EMS in Austere Conditions “Austere EMS” is defined as the delivery of EMS care under conditions of limited personnel and equipment resources and outside the existing framework of normal EMS. Special medical support protocols and procedures may be needed under austere conditions. EMS providers

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 54
operating under remote, austere, or hostile conditions are expected to provide prehospital care in these environments with little or no support when operational security is a consideration. In some situations, communications are not assured and evacuation may be delayed significantly. Care providers in an austere situation may be forced to improvise and adapt their medical procedures based on existing circumstances to provide care for and prepare the patient for evacuation to a safer environment. The document Austere Emergency Medical Support (AEMS) Field Guide, published by the U.S. Dept. of Homeland Security, Office of Health Affairs, is intended improve the EMS providers’ capability to provide the best possible prehospital care until the patient can be transferred for definitive medical treatment. The Guide is a series of suggested best practices. Medical providers are strongly encouraged to follow these suggestions, and should consider doing so in whole or in part to the extent that his/her training or experience is sufficient. Specializations In some cases, specialty certifications may be used to respond to local needs for flexibility or to recognize continuing education. Specialty certifications may evolve to accommodate subtle differences in skills, practice environment, knowledge, qualifications, services provided, needs, risk, level of supervisory responsibility, amount of autonomy and/or judgment/critical thinking/decision making.2
Scope of Practice for Special Populations EMS professionals are expected to meet the urgent health care needs of all patients, regardless of age or co-morbidity, consistent with their defined scope of practice. Recognized special populations include, but may not be limited to, children, older patients, patients with disabilities, and patients with limited access to health care due to geographic, demographic, socioeconomic, or other reasons.2
Scope of Practice for EMS Personnel Functioning in Nontraditional Roles During disasters, EMS professionals may be required to function in health care settings other than out-of-hospital care. Common settings include, but are not limited to, emergency departments, hospital units (including critical care), shelters, urgent care settings, free-standing medical units, etc. State regulations must be clear as to the extent to which the State’s EMS scope of practice applies to EMS personnel functioning in these nontraditional roles and settings. Providing EMS Mass Medical Care with Scarce Resources In the event of a catastrophic disaster, the resulting mass casualties will likely overwhelm the local EMS resources and community health care systems. Indeed, if the event incapacitates health care workers, damages facilities, or destroys supplies, the capacity of the health care system to respond may be severely compromised. In the case of a mass casualty incident, in which emergency health care personnel, medical and transport equipment, and hospital beds are scarce, EMS personnel will be forced to modify their care from conventional to crisis care. This means moving from usual standards of care, in which the goal is to save everyone, to crisis standards of care, in which as many lives as possible are saved with the resources that are available. Resource shortages may include limited staff, supplies, and equipment; a lack of fuel or medicines; limited mutual aid; or disruption of coordination and communication functions. Strategic approaches to utilizing these scarce resources should be implemented, and should

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 55
include maximizing the use of available personnel, community response teams and health care personnel registries, disaster triage criteria, and altered transport modes and patient destinations. If other communities are faced with similar demands (as would be the case of an influenza pandemic or a nuclear detonation, for example), the arrival of additional health care resources, including assistance from the Federal Government, likely would be significantly delayed12. EMS providers from across the U.S. may be called upon pursuant to the AMR/FEMA Federal EMS Contract to provide first-responder rescue, assessment, care, and transportation and access to the emergency medical health care delivery system. In these mass casualty incidents (MCI), it may be necessary to allocate scarce resources in a manner that is different from usual circumstances but appropriate to the situation. Emergency medical services in the United States are provided through a complex system composed of highly variable organizational structures. The variability of EMS response systems is further exacerbated by important differences in EMS preparedness training, guidelines, and response capacity – posing significant coordination and communications challenges for EMS leaders and planners. The U.S. Dept. of Health and Human Resources, Agency for Healthcare Research and Quality, has published a guide, Mass Medical Care with Scarce Resources13 to address these situations and present planners with approaches and strategies that would enable them to provide the most appropriate standards of care possible under the circumstances of an MCI. It will serve as a guide for EMS disaster responders pursuant to the AMR/FEMA Contract. EMS in an MCI: Expected Shortages and Needs In the case of an MCI, many health care resources at the local and regional levels will be overwhelmed or eliminated. Those EMS response agencies that are able to remain operational likely will encounter a demand for services that will outstrip the supply and available resources. EMS systems will confront:
Personnel shortages.
Breakdowns in supply chains.
Lack of coordination and information sharing among diverse EMS providers, public safety, hospitals, trauma center, and public health.
Breakdown of logistic support for operational sustainability, including such things as fuel shortages; inadequate availability of transport vehicles; and shortages in supplies, equipment, and pharmaceuticals.
Overloading of hospital emergency departments and associated services such as intensive care capabilities; specialty services such as burn care or decontamination units; and specialized equipment such as ventilators, PPE, or negative pressure rooms.
Breakdowns in local “burden sharing” strategies (mutual aid agreements) due to overwhelming demand and lack of surge capacity.
The need to implement modified treatment protocols to meet the extraordinary conditions of the MCI that may be limited to reasonable life-sustaining activities where appropriate.
Approaches to the Allocation of Scarce Resources In the face of a catastrophic MCI, there likely will be scarcities and mismatches regarding EMS personnel, transport capacity, and destination availabilities for patient treatment. As a result, creative strategies will need to be implemented for coordinating and maximizing the use of available staff members and resources. Approaches to the allocation of scarce resources to be considered should include, but not be limited to, the following:

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 56
Maximize the availability of EMS personnel through modified or extended shifts, deployment of no more than two providers per vehicle, and use of one-person response vehicles for “patient evaluation” prior to dispatch of transport resources.
Maximize the use of available EMS personnel. Some medical protocols may be suspended (e.g., base contact for certain interventions) to allow for greater efficiency and flexibility in patient management. EMS personnel may be used in nontraditional settings (e.g., alternative care sites, hospitals, pharmaceutical distribution centers) for field triage, treatment, or transport. Their scope of practice may be extended to provide vaccinations or medications or to deliver nontraditional medical care at the scene or in the home.
Community Emergency Response Teams (CERTS)14. The CERTs program educates people on disaster preparedness for hazards that may impact their area and trains them in basic disaster response skills, such as fire safety, light search and rescue, team organization, and disaster medical operations. Using the training learned in the classroom and during exercises, CERT members can assist others in their neighborhood or workplace following an event when professional responders are not immediately available to help. CERT members also are encouraged to support emergency response agencies by taking a more active role in emergency preparedness projects in their community.
Maximize personnel protection for personnel. Universal precautions should be used for every patient encounter, if at all possible. To minimize the number of responders exposed to pathogens or chemicals, specialized protections should be used to the extent possible and adjusted to the nature of the incident (e.g., distribution of antibiotics, vaccines, or antidotes to staff and family members). In the case of chemical incidents, decontamination needs must be evaluated and addressed prior to transportation to preserve transport capability. Similarly, security personnel should be assigned to protect EMS response operations, logistics centers, and stockpile depots.
Maximize patient triage and evaluation. Specific mass casualty triage systems should be used whenever many patients require prehospital medical treatment and/or transport. This allows for an organized approach to treatment that includes a system for prioritizing the patients who require immediate medical care for survival. Triage is a continuous process; it is necessary to reevaluate patient priorities as their clinical status improves or deteriorates and more resources become available.
The Federal Interagency Committee of Emergency Medical Services (FICEMS) was created, in part to ensure coordination among the Federal agencies involved with state, local, tribal or regional EMS and 9-1-1 systems. FICEMS has statutory authority to identify the ways in which Federal agencies can streamline their processes for support of EMS. With input from the National EMS Advisory Council (NEMSAC), they recommend national implementation of the Model Uniform Core Criteria (MUCC) for mass casualty triage15. SALT Triage is compliant with the MUCC criteria and is recommended as the national standard for all mass casualty triage systems. S.A.L.T. is the acronym for Sort, Assess, Life-saving interventions, treatment and/or Transport and is a method that EMS responders use to effectively and efficiently evaluate victims during a MCI.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 57
The SALT Triage system assigns patients into one of five categories based on the urgency of their medical condition and potential for survival.
1. Minimal 2. Delayed 3. Immediate 4. Expectant 5. Dead

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 58
Triage Levels and Color Coding
Green: MINIMAL. Patients with minor injuries who will eventually require care
Yellow: DELAYED. Patients whose lives are not in immediate danger and who will require urgent, not immediate, medical care
Red: IMMEDIATE: Patients whose lives are in immediate danger and who require immediate care
Black: EXPECTANT. Patients who are either dead or who have such extensive injuries that they cannot be saved with the limited resources available.
S.A.L.T. Mass Casualty Incident Triage System (Sort-Assess-Lifesaving Interventions/Treatment-Transport)

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 59
Maximize transport capability. Public and private ambulance services should be coordinated and steps taken to ensure that they do not self-dispatch to MCIs. Paramedic-initiated alternative transport mechanisms also should be put into place (e.g., buses, taxis, privately owned vehicles). Mutual aid agreements should be in place and implemented to deploy and use available transportation assets, staff members, and staging locations. Transport assets should be loaded to their full capacity and patients taken to the closest appropriate hospital or care site. Air transport should be used to take patients to distant facilities (unless the incident presents contamination risks). Noncritical calls should be batched by geographic area. Bypass, diversion, or closure rules could be suspended to promote equitable distribution of patients and to try to avoid the overloading of any one hospital. Secondary transport needs should be anticipated so that patients can be transferred from overloaded hospitals or care sites to those that are less affected. Ambulances and paratransit vehicles should avoid transporting patients to far destinations greater than 200 miles or 6 hours, because it is anticipated they will be needed for multiple round trips. In addition, transporting patients in ground vehicles longer than 6 hours may adversely affect the patient’s clinical status.
Maximize destination choices. A centralized coordination of patient transport should be in place to minimize hospital overloading and maximize the use of other available resources, such as primary care providers, alternative care sites, medical evaluation centers, or triage centers.
Indeed, it is likely that the vast majority of victims of an mass casualty event may end up being most appropriately managed in the home setting, either because their illness or injury is not severe enough to warrant institutionalized care or because the successful outcome of such inpatient treatment in the setting of scarce and limited resources would be considered futile and potentially wasteful. Many view the community hospital as a “safe haven,” a place to go for food, shelter, protection, and medical attention. However, particularly in the event of a transmissible infectious disease in which hospitalized patients represent the sickest patients in the community, the concept of “safe haven” may not be applicable. In fact, it may be more dangerous to be in the hospital setting than to remain at home. It is important for community planners to highlight the concept of the home as a “safe haven” in their risk communication strategies and develop measures to support this concept. Emergency planners, therefore, must incorporate the likelihood of home care delivery in all aspects of their planning efforts. This planning must focus on the possibility that some rudimentary degree of medical care will need to be delivered in the home setting, often with limited outside professional assistance. Mass Evacuation Transportation The National Response Framework (NRF) assumes that up to 100,000 patients and evacuees may require transport, regulating, and tracking during a catastrophic incident. It is important to estimate the transportation resources needed to evacuate patients and evacuees from healthcare facilities and other locations. The Agency for Healthcare Research and Quality has created a Mass Evacuation Transportation Model16 that estimates the time required to evacuate patients from healthcare facilities and transport them to receiving facilities. The model considers the transportation requirements of different types of patients (for example ambulatory patients or patients requiring constant medical attention during the evacuation); the availability of ambulances, wheelchair vans, and buses; the location of evacuating and receiving facilities; and the surge capacity of receiving facilities.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 60
Unsolicited Medical Personnel Volunteering at Disaster Scenes AMR prohibits self-deployment in response to the AMR/FEMA Federal EMS Contract. Only those personnel who are officially authorized and credentialed by AMR may respond pursuant to a FEMA deployment. Furthermore, AMR concurs with the position statement of ACEP and NAEMSP regarding unsolicited medical personnel. “The American College of Emergency Physicians (ACEP) and the National Association of EMS Physicians (NAEMSP) believe an organized approach is needed for the utilization of unsolicited medical personnel who volunteer to respond to disaster scenes or mass casualty incidents. To ensure the efficient, effective, and safe mobilization of such volunteer medical resources, medical command must come under the authority of the medical director for the emergency medical services (EMS) system and the jurisdiction's established incident command system (ICS). This practice will ensure the integration of all medical functions in the area and accountability under the jurisdiction's established (ICS) without hampering authorized and established functioning rescue efforts. Volunteer medical personnel (e.g., physicians, nurses, emergency medical technicians, etc.) should not respond to a disaster scene unless officially requested by the jurisdiction's established ICS. All personnel must understand the authority and resources of local EMS and health care systems, the importance of staffing their facilities as their primary responsibility, and the dangerous conditions associated with on-site operations.”17 Disaster Clinical Protocols EMS responders who are deployed pursuant to the AMR/FEMA Federal EMS Contract shall follow the local clinical protocols in effect for the disaster area. If local EMS protocols are otherwise unavailable, disaster responders should follow state EMS protocols for the disaster-affected state, if they exist. If state protocols are unavailable, disaster responders should follow the protocols from their home location, i.e., the protocols they use back home in daily practice in non-disaster times. As a last resort, if the above options are unavailable, AMR will provide protocols to be used by its disaster responders. The guideline for these protocols shall be the DHS-Wide BLS & ALS Protocols. For a practicing provider to be proficient with these protocols, he/she must be certified and licensed at the appropriate level, and demonstrate and document all the skills and knowledge the protocols require. A provider’s scope of practice may expand (e.g., administration of intravenous therapy by BLS providers) only with additional training and confirmation of competency by a medical director. In any case, at no time should any EMS provider perform procedures that are beyond their scope of formal training and certification, regardless of the protocols in place. The following flowchart summarizes this hierarchy. DISASTER CLINICAL PROTOCOLS HIERARCHY
1. Local EMS protocols
2. State EMS protocols
3. Home location protocols

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 61
4. AMR Federal disaster protocols (DHS-OHA BLS & ALS Protocols)
Medical Control and Direction During Disasters Because the medical control of emergency medical services is within the domain of emergency medicine, it remains the responsibility of emergency physicians to provide both direct patient care and medical control of out-of-hospital emergency medical services during disasters.18 EMS responders who are deployed pursuant to the AMR/FEMA Federal EMS Contract shall follow medical control and direction of the local EMS jurisdiction if available. If local medical control is unavailable, EMS disaster responders shall follow medical control and direction from the authorized medical director of the disaster-affected state. If that is unavailable, the national ESF8 primary agency, U.S. Dept. of Health and Human Services or their delegate(s) shall provide medical control and direction. If that is unavailable, and as a last resort, the official AMR medical liaison assigned to the disaster shall provide medical control and direction. The following flowchart summarizes this hierarchy. Medical Control and Direction During Disasters
1. Local EMS / local medical control and direction
2. State EMS / State medical control and direction
3. HHS provides medical control and direction
4. Federal EMS Contractor (AMR) provides medical control and direction 3 National EMS Core Content. National Highway Traffic Safety Administration. DOT HS 809 898. July 2005.
http://www.nhtsa.gov/people/injury/ems/EMSCoreContent/index.htm 4 National EMS Scope of Practice Model. National Highway Traffic Safety Administration. DOT HS 810 657. February 2007.
http://www.nhtsa.dot.gov/portal/nhtsa_static_file_downloader.jsp?file=/staticfiles/DOT/NHTSA/Traffic% 5 National Model EMS Clinical Guidelines. National Association of State EMS Officials (NASEMSO). Volume 11-14.
https://www.nasemso.org/Projects/ModelEMSClinicalGuidelines/documents/National-Model-EMS-Clinical-Guidelines-23Oct2014.pdf 6 DHS-Wide EMS Basic Life Support (BLS) & Advanced Life Support (ALS) Protocols. U.S. Dept. of Homeland Security, Office of Health
Affairs. Created 12/2/2011, modified 9/9/2013. http://www.amr.net/Files/PDFs/DRT-References-and-Resources/DHS-FEMA-ALS-BLS-Protocols.aspx 7 Austere Emergency Medical Support (AEMS) Field Guide. U.S. Dept. of Homeland Security, Office of Health Affairs. Created 12/2/2011,
modified 4/24/2014. http://www.amr.net/Files/PDFs/DRT-References-and-Resources/DHS-Austere-EMS-Field-Guide.aspx 8 National Registry of Emergency Medical Technicians®.
https://www.nremt.org/nremt/about/becomeInvolvedInEMS.asp 9 Guidance for Establishing Crisis Standards of Care for Use in Disaster Situations: A Letter Report. Institute of Medicine of the National
Academies. ISBN: 0-309-14431-0. 2009.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 62
http://www.nap.edu/catalog/12749.html 10 Altered Standards of Care in Mass Casualty Events. Bioterrorism and Other Public Health Emergencies. Agency for Healthcare Research
and Quality, U.S. Dept. of Health and Human Services. AHRQ Publication No. 05-0043. April 2005. http://www.ahrq.gov/research/altstand/ 11 Crisis Standards of Care – A Systems Framework for Catastrophic Disaster Response. Institute of Medicine of the National Academies. ISBN 978-0-309-25347-5. The National Academies Press: Washington, DC. March 21, 2012. http://www.iom.edu/reports/2012/crisis-standards-of-care-a-systems-framework-for-catastrophic-disaster-response.aspx 12 Mass Medical Care with Scarce Resources: The Essentials (Includes Chapter on Influenza Pandemic Preparedness). U.S. Dept. of Health
and Human Services, Agency for Healthcare Research and Quality. AHRQ Pub. No. 09-0016. Sept. 2009. http://www.ahrq.gov/prep/mmcessentials/mccessent.pdf 13 Mass Medical Care with Scarce Resources, A Community Planning Guide. U.S. Dept. of Health and Human Services, Agency for
Healthcare Research and Quality. Prepared by Health Systems Research, Inc. AHRQ Publication No. 07-0001. February 2007. http://www.ahrq.gov/research/mce/ 14 CERT. The National Office of Citizen Corps – FEMA Individual and Community Preparedness Division. http://www.citizencorps.gov/cert/about.shtm 15 National Implementation of the Model Uniform Core Criteria for Mass Casualty Incident Triage – A Report of the Federal Interagency
Committee on EMS. May 16, 2014. http://www.nhtsa.gov/staticfiles/nti/pdf/811891-Model_UCC_for_Mass_Casualty_Incident_Triage.pdf 16 Mass Evacuation Transportation Model. Agency for Healthcare Research and Quality. U.S. Dept. of Health and Human Services. AHRQ
Publication No. 08-0102-1-EF. August 2008. http://www.ahrq.gov/prep/massevac/manual/massevum1.htm 17 Unsolicited Medical Personnel Volunteering at Disaster Scenes. Policy Statement - American College of Emergency Physicians Board of
Directors, June 2002. http://www.acep.org/practres.aspx?id=29842 18 Disaster Medical Services. Policy Statement - American College of Emergency Physicians Board of Directors, 1985, 1997, 2000, 2006.
http://www.acep.org/practres.aspx?id=29176

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 63
Appendix 7 Hazard Based Guidelines: Protective Equipment for Workers in Hurricane Flood Response The purpose of this National Institute for Occupational Safety and Health (NIOSH) fact sheet is to provide general guidance for personal protective equipment (PPE) for workers responding in hurricane flood zones. This guidance will be updated as additional information is available. PPE selection and use is site and task specific. General guidelines must be adapted to specific conditions. This guidance represents professional judgment based on experience from responses to past storms and floods. Additional interim recommendations will be added for clean-up and restoration operations. These recommendations focus on the following hazards associated with response activities: Hazard 1 Sharp jagged debris Hazard 2 Floodwater exposure Hazard 3 Electrical hazards Hazard 4 Contact with blood/body fluids and handling animal and human remains Hazard 5 Slick and unstable surfaces Note: This guidance is not a comprehensive list of hazards and does not include important hazards such as stress or fatigue that are not addressed via PPE. Background Disaster sites pose many occupational health and safety concerns. These hazards and exposures are a function of the unstable nature of the site, the potential for worker exposure to unknown hazardous substances and the type of work performed. An accurate assessment of all hazards may not be possible because they may not be immediately obvious or identifiable. Where possible, NIOSH has made default recommendations for PPE that we believe will meet the probable hazards. General PPE Guidance For most work in flooded areas, or areas that have been subjected to flooding, response personnel will need the following personal protective equipment: hard hats, goggles or safety glasses, heavy work gloves, watertight boots with steel toe and insole (not just steel shank), and hearing protection where excessive noise from equipment poses a risk of hearing damage. PPE should be provided in a range of sizes to ensure proper fit. For additional information on what equipment you need for protection against exposure to specific hazards, contact your local OSHA office or consult the NIOSH Pocket Guide to Chemical Hazards (http://www.cdc.gov/niosh/npg/npg.html). General Worker Safety Guidance Workers involved with hurricane or flood response should be aware of the potential dangers involved and the proper safety precautions. CDC has developed general guidance for what workers should bring with them to the flood area: http://www.cdc.gov/travel/content/relief-workers.aspx. OSHA has worker safety guidance at the following link: http://www.osha.gov/OshDoc/hurricaneRecovery.html. NIOSH Publication No. 94-123 identifies several hazards associated with the aftermath of a flood. (http://www.cdc.gov/niosh/docs/94-123/).

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 64
Because the level of experience will vary among workers, response workers must work together and look out for one another to ensure safety. Additional Information Any wounds, cuts, or animal bites should be immediately cleansed with soap and clean water. Familiarity with basic first aid is advised to self-treat any injury until medical attention can be obtained. Additional information resources include: Interim Immunization Recommendations for Emergency Responders http://www.bt.cdc.gov/disasters/disease/responderimmun.asp Emergency Wound Care After a Natural Disaster http://www.bt.cdc.gov/disasters/woundcare.asp In addition, response workers are at serious risk for developing heat stress. Excessive exposure to hot environments can cause a variety of heat-related problems, including heat stroke, heat exhaustion, heat cramps, and fainting. The need to use PPE can exacerbate heat exposures. Response workers should be familiar with heat stress symptoms. OSHA has a pocket card on heat stress available at: http://www.osha.gov/Publications/osha3154.pdf See http://www.cdc.gov/niosh/topics/heatstress/ for additional NIOSH information. NIOSH requests your assistance in disseminating this interim document to all workers involved in flood response. HAZARD 1: Sharp, jagged debris Risks: Workers handling hurricane related debris may suffer wounds. Tetanus is a potential health threat for persons who sustain wound injuries. Also, any wound has the potential for becoming infected, and floodwater exposures may add to this concern. General PPE Recommendations: Use heavy gloves to protect the hands when handling debris to minimize the chances of cuts and scrapes. Gloves designed to protect the skin from chemical exposure are not typically strong enough to protect from debris. Multiple layers of gloves (double gloving) may be necessary. Comfortable, form fitting clothing that includes long pants, long sleeve shirts, boots, eye protection (safety glasses, goggles, or face shields), and protective head covers are also appropriate. HAZARD 2: Floodwater exposure Risks: Floodwaters may contain bacteria from human and animal wastes. The most likely symptoms from an infection are stomach-ache, fever, vomiting and diarrhea. While skin contact with flood water does not, by itself, pose a serious health risk, emergency response personnel and the public should avoid direct contact with standing water when possible to minimize the chance for infection. Chemical contamination of floodwaters can also occur and contamination levels may be higher nearer to sources such as industrial locations. Work in and around moving or standing water in flooded areas presents a risk of drowning. Standing or working in water which is cooler than 75 degrees F (24 degrees C) will remove body heat more rapidly than it can be replaced, resulting in hypothermia. General PPE Recommendations: Double gloving with a waterproof glove under a heavy work glove is the best way to protect the hands from both cuts and scrapes and floodwater exposure. Boots and rain gear can be used to prevent lower body skin exposures.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 65
It is important to minimize contaminating the inside of the gloves. Gloves not disposed of should be cleaned with soap and water and dried between uses. Floodwaters are associated with strong odors, but experience in past floods and disease outbreak tracking do not suggest the need for a general recommendation for default respirator use by all personnel. As with all emergency operations, site specific information should be used to tailor recommendations to the hazards and exposures at hand. For example, use of N95 respirators might be advisable adjacent to aerated floodwater where mists are created- such as potential tasks associated with repair of pumping facilities or discharge pipes. CDC will provide additional updates as more information becomes available for specific tasks and locations. Avoid working alone and wear a Coast Guard-approved life jacket or buoyant work vest when entering flood waters or working over or near flood waters. Refer to OSHA guidance: http://www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=STANDARDS&p_id=10669 For additional information on what equipment you need for protection against chemical exposures, contact your local OSHA office or consult the NIOSH Pocket Guide to Chemical Hazards. (http://www.cdc.gov/niosh/npg/npg.html). Additional Information: Wearing wet gloves or PPE can cause dermal irritation. Long exposures to wet conditions can compromise the function of the skin barrier. Repeated use of impermeable gloves, especially in hot and humid conditions, can aggravate skin rashes. Cotton liners are sometimes used under protective gloves to improve comfort and to prevent dermatitis. Latex gloves should be avoided because of the risk of developing skin sensitivity or allergy. Open wounds and skin conditions such as eczema and psoriasis may increase your risk of infection. Contamination of wounds with water (fresh or sea water) can lead to infections caused by waterborne organisms. See: http://www.bt.cdc.gov/disasters/emergwoundhcp.asp If skin contact with floodwaters does occur, CDC strongly advises the use of soap and water to clean exposed areas. Waterless alcohol-based hand rubs can be used when soap or clean water is not available. Hands should be washed after removal of gloves. There is a wide range of damage, work scenarios, and tasks associated with hurricane response, and exposure assessments are not yet available. Local information should be used to tailor recommendations to the hazards and exposures at hand. Firefighters and others involved with responding to fires should use appropriate respiratory protection. Post fire clean-up operations occurring at industrial or chemical facilities may warrant use of protective equipment. As conditions dry out, there is some likelihood that demolition operations may generate dust exposures for construction and restoration workers. It is likely that other special tasks (e.g. welding and cutting) may generate airborne hazards and that respiratory protection will be needed. CDC will provide additional updates as more information becomes available. HAZARD 3: Electrical Hazards Risks: Electrical, overhead power lines, power junctions, and downed electrical wires and cables can cause electrocution and burns. Fallen lines can also energize other objects such as fences, ladders, or metal building parts. Use of improperly sized or operated portable generators during electrical outages can also cause "backfeed" injuries to workers performing repair work in neighboring buildings. Only trained electricians and utility workers should approach or handle electrical lines. All other response workers should avoid going near all downed lines and should treat them as if energized.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 66
General PPE Recommendations: Electricians and utility workers need to use special electrically resistant PPE including head covers, gloves, boots, and appropriate eye protection. Additional information: Special electrical PPE is only one aspect of electrical safety practice. Special training and practices to test, de-energize, isolate, and/or lockout hazardous energy sources are important. See the NIOSH electrical safety page at: http://www.cdc.gov/niosh/topics/electrical/ OSHA has electrical safety factsheets at: http://www.osha.gov/OshDoc/data_General_Facts/downed_electrical_wires.pdf http://www.osha.gov/OshDoc/data_Hurricane_Facts/elect_safety.pdf CDC has a factsheet on "backfeed" and power outage safety at: http://www.bt.cdc.gov/poweroutage/workersafety.asp Hazard 4: Contact with blood/body fluids and handling animal and human remains Risk: There is no direct risk of contagion or infectious disease from being near human remains for people who are not directly involved in recovery or other efforts that require handling dead bodies. However, workers who must have direct contact with human remains can have exposure to blood borne pathogens. Blood, bloody fluids, body fluids, and tissues are potential sources of blood-borne infections from pathogens including Hepatitis B, Hepatitis C, and HIV. Exposures to medical providers and responders may occur via a cut or puncture wound; through mucous membranes (eye, nose, mouth); and through non-intact skin (dermatitis/rashes, injuries, abrasions). General PPE Recommendations: Workers who will have direct contact with the victims, or surfaces contaminated with blood or body fluids should use universal precautions. These require use of protective barriers such as gloves, face-shields, or protective eyewear. See: http://www.cdc.gov/ncidod/dhqp/bp_universal_precautions.html The CDC has developed interim health recommendations for workers who handle human remains. http://www.bt.cdc.gov/disasters/handleremains.asp. Additional information is available from the Pan American Health Organization at: http://www.paho.org/english/dd/ped/ManejoCadaveres.htm Workers who have direct contact with the victims, bodies, or surfaces contaminated with blood or body fluids should use universal precautions identified in the interim CDC recommendations: http://www.bt.cdc.gov/disasters/handleremains.asp CDC recommends surgical masks for handling human remains. http://www.bt.cdc.gov/disasters/handleremains.asp. Organic vapor respirators can be used for nuisance odor control where needed. One option that provides odor control and universal precaution splash and eye protection is to use a full face piece respirator with N95 and organic vapor cartridges. Additional information: See the NIOSH bloodborne pathogens page at: http://www.cdc.gov/niosh/topics/bbp/ CDC recommends N95 particulate respirators for handling swine and poultry animal carcasses. http://www.bt.cdc.gov/disasters/animaldisposal.asp

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 67
Hazard 5: Slick and unstable surfaces Risk: Traumatic injuries, including serious fall injuries, from slips, trips and falls, or collapsing materials. General PPE Recommendations: Ensure that workers have a full array of PPE, including safety shoes with slip resistant soles, cut resistant gloves, eye protection, and hard hats. Ensure that workers use full protective equipment and lifelines tied off to suitable anchor points, including bucket trucks, whenever possible. Additional information: http://www.cdc.gov/niosh/topics/emres/emhaz.html

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 68
Appendix 8 Critical and Specialty Care Patient Transport, Austere EMS and Crisis Standard of Care Overview and Background The immediate response to a catastrophic disaster, act of terrorism or other emergency involves local public safety, emergency medical services, public health, and health care organizations. While most emergencies are handled locally, major incidents may require assistance from other jurisdictions, including the State and Federal governments. The National Response Framework (NRF), within the construct of the National Incident Management System (NIMS), is an all-hazards plan that provides the structure and mechanisms for national-level policy and operational coordination for domestic incident management. The NRF identifies FEMA as the lead agency for the Federal government in coordinating and leading the unified Federal Response during a major/complex incident. FEMA works in partnership with other organizations that are part of the nation’s emergency management system including state and local emergency management agencies, and Federal agencies, such as the U.S. Department of Health and Human Services (HHS) and the Department of Homeland Security (DHS) Office of Health Affairs (OHA). Purpose The purpose of the AMR/FEMA Federal EMS Agreement is to obtain Contractor-managed multi-functional support resources and capabilities as needed in support of Federal assistance. The support may be in the form of both staffed medical transport capabilities as well as licensed and certified medical personnel for augmentation beyond medical transport. FEMA has named American Medical Response as the Federal EMS contractor. AMR provides a full array of ground ambulance, air ambulance, paratransit services, and medical personnel to supplement the Federal and military response to a disaster, act of terrorism, public health emergency or other Federal event. The primary functions include patient triage, treatment and transportation and it covers the 48 contiguous Unites States which are divided into 4 FEMA zones. Scope AMR and FEMA have established medical related support services to include but not limited to:
1. Medical Transportation
a. Advanced Life Support (ALS) or Basic Life Support (BLS) Ground Ambulances
b. Paratransit support
c. Medical Airlift, including critical and specialty care transport (CCST)
2. Medical Personnel
a. Emergency Medical Technician(EMT)
b. Paramedic
3. Field Operations Team (FOT)
4. Communications Support Team (CST)
5. Planning and Exercise Support Services
Critically ill or injured patients may be transported by non-critical care personnel in the acute pre-hospital setting if critical care transport personnel are unavailable. Interfacility critical and specialty care transport (CSCT) is not generally provided by ground ambulance personnel

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 69
(EMTs and Paramedics) in the AMR/FEMA Federal EMS Contract. CSCT services are usually provided by air ambulances in this Contract. If available and authorized, critical care transport personnel (above the Paramedic level) may be used for ground ambulance transport. Example: Air Ambulance Critical Care nurses may be used to augment ground ambulance attendants to transport CSCT patients from a healthcare facility to an air ambulance. The level of medical care required to transport a critical and specialty patient includes: 1) an expert level of provider knowledge and skills appropriate to the medical needs of such patient; 2) a patient care environment commensurate with the critical care provided, including the necessary equipment and supplies; 3) the ability to address the added challenges of transport and initiate and/or maintain the continuity of tertiary or quaternary hospital care during transport; and 4) a vehicle (ground, fixed wing, or rotor wing) equipped to support the delivery of medical care to critical care patients during transport.. Both the critical care transport agency and the transport teams actually delivering the care to patients must have sufficient capability to meet the medical needs of critical care patients.1 This policy applies to all employees of Envision Healthcare and its subsidiaries as well as affiliate employees, including temporary employees and employees of affiliated third-party organizations. Policy Medical Personnel AMR and its subcontractors shall provide qualified personnel to perform all requirements specified in FEMA Task Orders issued pursuant to the Contract. All EMS personnel shall be licensed and credentialed in their State of origin. FEMA will assist in getting the affected state(s) to grant reciprocity to EMS personnel responding pursuant to this Contract. Paratransit vehicles will be staffed by licensed drivers. No medical attendants are provided. Ground ambulances will be staffed by EMTs and Paramedics according to the level of service being provided, BLS or ALS. Air Ambulances will be staffed by pilots, EMTs, Paramedics or Critical Care personnel (nurse and/or physician). The Typed Resource Definitions for AMR/FEMA Air Ambulances (fixed and rotary wing) will be used to establish overall function, level of service, personnel needed, number of patients transported per aircraft and equipment and supplies required. (See attached). Critical and Specialty Care Transport – CSCT is interfacility transportation of a critically injured or ill patient by ambulance, including the provision of medically necessary supplies and services, at a level of service beyond the scope of the Paramedic. CSCT is necessary when the patient’s condition requires ongoing care that must be furnished by one or more health professionals in an appropriate specialty area, for example, emergency or critical care nursing, emergency medicine, respiratory care, cardiovascular care, or a paramedic with additional training. The Paramedic level of care and scope of practice is set by each State. CSCT is necessary when a patient’s condition requires ongoing care that must be furnished by one or more health
1 Association of Critical Care Transport, Washington, DC. “The Critical Care Transport Standards Project”.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 70
professionals in an appropriate specialty area. Care above that level that is medically necessary and that is furnished at a level of service above the Paramedic level of care is considered CSCT. The phrase “Paramedic with additional training” recognizes that a State may permit a person who is not only certified as an Paramedic, but who also has successfully completed additional education as determined by the State in furnishing higher level medical services required by critically ill or critically injured patients, to furnish a level of service that otherwise would require a health professional in an appropriate specialty care area (for example, a nurse) to provide. “Additional training” means the specific additional training that a State requires a Paramedic to complete in order to qualify to furnish specialty care to a critically ill or injured patient during a CSCT.2 It may be necessary for the sending hospital to provide CSCT qualified clinical personnel and equipment to accompany patients when the level of care exceeds that of the ground ambulance attendant(s). Levels of Patient Acuity - In order to provide safe and effective care, provider capabilities must match the patient’s current and potential needs. It is important to have consistent terminology to define the levels of patient acuity. For each level, examples are provided of the types of needs the patient might have and the level of care likely to be required at each level.
Stable with no risk for deterioration — Oxygen, monitoring of vital signs, saline lock,
basic emergency medical care).
Stable with low risk of deterioration — Running IV, some IV medications including
pain medications, pulse oximetry, increased need for assessment and interpretation
skills (advanced care).
Stable with medium risk of deterioration — EKG monitoring, basic cardiac
medications, e.g., heparin or nitroglycerine (advanced care +).
Stable with high risk of deterioration – Patients requiring advanced airway but
secured, intubated, on ventilator, patients on multiple vasoactive medication drips
(advanced care +), patients whose condition has been initially stabilized, but has
likelihood of deterioration, based on assessment or knowledge of provider regarding
specific illness/injury.
Unstable — Any patient who cannot be stabilized at the transferring facility, who is
deteriorating or likely to deteriorate, such as patients who require invasive monitoring,
balloon pump, who are post-resuscitation, or who have sustained multiple trauma
(critical care or available crew with time considerations).3
Critical and Specialty Care Patient Types – This section can be used to assist in determining which patients would best be cared for by a CSCT Air Transport Team. Not every person in an ICU or CCU needs CSCT. The following are some examples of patient types that may require CSCT:
1. High risk for decompensation.
2. Requires mechanical ventilation.
3. High risk for deteriorating respiratory status.
2 U.S. Dept. of Health & Human Services, Centers for Medicare and Medicaid Serviced, July 29, 2010, Transmittal 130. 3 U.S. Department of Transportation, National Highway Traffic Safety Administration. “Guide for Interfacility Patient Transfer.” April 2006. DOT HS 810 599.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 71
4. Requires invasive hemodynamic monitoring (arterial line and/or central venous pressure
line)
5. Requires ongoing active resuscitation and/or lab monitoring.
6. Requires aggressive in-flight fluid/blood product administration.
7. Requires vasopressor support.
8. Requires invasive intra-cranial pressure monitoring.
9. Requires cardiac pacing.
10. Has unstable spine fracture.
11. Patient has undergone vascular reconstruction and is at high risk for clot or hemorrhage.
12. Unstable angina, unstable arrhythmia, or recent myocardial infarction.
NOTE: The following, in and of themselves, do not require automatic CSCT: 1. Chest tube
2. Epidurals with level below T10
3. Regional pain blocks
4. Patient in ICU or CCU
5. Cardiac monitor
6. Blood or plasma use
Critical and Specialty Care and Austere EMS – EMTs and Paramedics may be authorized to perform Critical and Specialty Care in certain austere conditions. “Austere EMS” is the delivery of EMS care under conditions of limited personnel and equipment resources, and outside the existing framework of normal EMS. An austere EMS environment may include elements of any of the following:
1. An ongoing physical environmental threat (e.g., heat, cold, water, wind, or altitude)
2. Limited medical supplies, technologies, or resources
3. Limited medical expertise available
4. Limited communications, including little or no access to medical direction or oversight
5. Limited availability of transportation
6. Altered condition of the medical responder
7. Urgent clinical situation requiring immediate intervention outside of standard protocols
8. Duration of care extended beyond standard operational situations
9. Any other factor or condition that alters the ability of the EMS responder to provide
necessary emergency medical care
10. Limited capacity to provide care due to security environment4
There must be an adequate legal framework for providing critical and specialty EMS care in an austere situation. An adequate legal framework would include the following:
Include a designation of the authority to declare an emergency and implement temporary
alterations in standards of care.
4 Austere Emergency Medical Support (AEMS) Field Guide. U.S. Dept. of Homeland Security, Office of Health Affairs

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 72
Define the conditions for temporary modification of laws and regulations that govern
medical care under normal conditions.
Be simple, clear, and easy to communicate to providers and the public.
Be flexible enough to accommodate the demands of events that vary in size and
velocity, such as an explosive or biological event.5
Crisis Standard of Care – In disaster scenarios the healthcare system may be stressed to its limits. It is important to describe the conditions under which standards of care would change due to shortage of critical resources. “Crisis standards of care” is defined as a substantial change in usual healthcare operations and the level of care it is possible to deliver, which is made necessary by a pervasive (e.g., pandemic influenza) or catastrophic disaster (e.g., earthquake, hurricane). This change in the level of care delivered is justified by specific circumstances and is formally declared by a state government, in recognition that crisis operations will be in effect for a sustained period. The formal declaration that crisis standards of care are in operation enables specific legal/regulatory powers and protections for healthcare providers in the necessary tasks of allocating and using scarce resources and implementing alternate care facility operations.6
5 Altered Standards of Care in Mass Casualty Events. Agency for Healthcare Research and Quality. U.S. Dept. of Health and Human Services. AHRQ Publication No. 05-0043, April 2005. 6 Guidance for Establishing Crisis Standards of Care for Use in Disaster Situation. Institute of Medicine of the National Academies. September 2009.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 73
Appendix 9 Specialty Ambulance Following are the standards that must be met regarding ALS Bariatric ambulances. ALS Bariatric ambulance
The ALS Bariatric ambulance must be staffed with at least one (1) EMT-Paramedic and one (1) EMT-Basic.
The stretcher must be rated to carry at least 700 lbs. and must either be 29" wide or compatible with a stretcher converting Bariatric board to meet the width criteria.
One of these commercial stretcher loading devices must be installed. A. A winch and ramp system configured in such a way that two responders can
easily and safely load and unload a Bariatric patient into the ambulance, or B. the stretcher must be equipped with some type of hydraulic or mechanical
system that allows for unassisted raising and lowering of a patient of at least 700 lbs.
Following are the standards that must be met regarding ALS Med-Evac buses. ALS Med-Evac bus
The ALS Med-Evac bus must be capable of transporting at least four (4) ALS stretcher patients at one time. Staffing is to be determined by the Provider but must include enough EMT-Paramedics (or other approved ALS providers) to simultaneously treat four (4) ALS patients and be available 24 hours per day. The ALS provider to patient ratio must be no less than 1:4. The ALS equipment on the bus must meet or exceed that of a licensed ALS ground ambulance and the quantity of equipment and supplies must be proportionate to the number of patients being transported.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 74
Appendix 10 Air Medical Support
Overview and Purpose
In the event that the medical systems within a disaster area are overwhelmed, there may be a need for a system to move patients out of the disaster area using air medical evacuation resources that are responsive and effective. American Medical Response (AMR) is under contract with the Federal Emergency Management Agency (FEMA) to provide medical airlift transportations services using fixed-wing and rotary-wing aircraft capable of providing basic life support (BLS), advanced life support (ALS) and critical care transport (CCT)7. AMR also has the capability of providing specialty care transport (SCT) including neonatal transports. The purpose of this document is to clearly outline the personnel, responsibilities, and processes needed to execute the AMR/FEMA Air Medical Evacuation Plan, which may be used for federally-declared disasters or other significant events.
Scope
This plan applies to all employees of AMR and its subsidiaries as well as affiliate employees, including temporary employees, subcontractors, and employees of affiliated third-party organizations that may be utilized pursuant to the AMR/FEMA Federal Emergency Medical Services (EMS) Contract. All air ambulance EMS operators shall comply with 14 CFR part 135 operations specifications during the conduct of flights with medical personnel on board.8
Revision Information Original – 03.06.2014 Revision – 02.13.2015 Revision – 02.26.2015 Revision – 08.19.2015 Revision – 09.25.2015 Revision – 03.04.2016
When to Consider Air Ambulance Service
Air ambulance service should be considered when BLS and ALS ground ambulance service is inadequate or not appropriate. Some of the situations and medical conditions that justify air medical transport or evacuation include but are not limited to:
A. Patient has a significant need of equipment or medical personnel for critical care (i.e., to prevent or manage ongoing deterioration that is an imminent threat to life, limb, or organ) available from an air medical transport and which cannot be provided via ground transport.
B. Intracranial bleeding that requires neurosurgical intervention
C. Cardiac conditions, e.g., cardiogenic shock, cardiac pacing, unstable angina, unstable arrhythmia, or recent myocardial infarction
D. Burns that require treatment in a burn center
E. Conditions that require treatment in a hyperbaric oxygen unit 7 FEMA National EMS Contracts # HSF90-12-D-0038 (zones 1 & 2) and HSFEHQ-12-D-0017 (zones 3 & 4). 8 DOT/FAA 14 CFR Parts 91, 120, and 135. Federal Register / Vol. 79, No. 35 / Feb. 21, 2014 / Rules and Regulations

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 75
F. Multiple severe injuries
G. Life-threatening trauma
H. Patient is at high risk for decompensation
I. Requires mechanical ventilation
J. High risk for deteriorating respiratory status
K. Requires invasive hemodynamic monitoring
L. Requires ongoing active resuscitation and/or lab monitoring
M. Requires aggressive in-flight fluid/blood product administration
N. Requires vasopressor support
O. Patient has unstable spine fracture
P. Patient has undergone vascular reconstruction and is at high risk for clot or hemorrhage
Q. Patient has significant potential to require a time-critical intervention, and an air medical transport will deliver the patient to an appropriate destination much faster than ground transport and improved patient outcome could be reasonably expected. As a general guideline, when it would take a ground ambulance 30-60 minutes or more to transport a patient whose medical condition at time of pick-up required immediate and rapid transport due to the nature and/or severity of the patient’s illness/injury, air transportation may be appropriate.9
R. Patient is located in a geographically isolated area that would make ground transport impossible or greatly delayed.
S. Local ground Emergency Medical Services (EMS) resources are exceeded or are unavailable to transport to the closest appropriate facility without compromising response to the primary service area.
T. Organ and/or organ recipient requires air transport to the transplant center in order to maintain viability of time-critical transplant.
U. Interfacility transports (IFT) – Air ambulance transport should be considered if transportation by ground ambulance would endanger the patient’s health and the transferring hospital does not have adequate facilities to provide the medical services needed by the patient. Examples of such specialized medical services that are generally not available at all type facilities may include but are not limited to burn care, cardiac care, trauma care, and critical care.10
V. Instability of ground transportation.
Critical Care and Specialty Care Transports AMR air ambulances are commonly used to transport critical care and specialty care patients. The Association of Air Medical Services (AAMS) defines CCT as “medical transport that includes specialized medical interventions such as intravenous infusions including vasopressors, vasoactive compounds, antiarrhythmics, fibrinolytics, tocolytics (anti-contraction medications), and/or and other parenteral pharmaceuticals unique to the patient’s special health care needs or special monitors or procedures such as mechanical ventilations, multiple monitors, cardiac balloon pump, external cardiac support (ventricular assist devices, etc.) or any other specialized device or procedure beyond the DOT/NHTSA minimum standards for EMT-Paramedic, certified by the referring physician as unique to the
9 U.S. Dept. of Health and Human Services, Center for Medicare Services. Medicare Benefit Policy Manual, Ch. 10, section 10.4.3
Time Needed for Ground Transport. https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/bp102c10.pdf 10 Ibid. Section 10.4.4 – Hospital to Hospital Transport.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 76
patient’s health care needs, commensurate with the scope of practice of a clinician with specialty care or board certification.”11 The U.S. Dept. of Health and Human Services (HHS) defines SCT as “…the interfacility transportation of a critically injured or ill [patient] at a level of service beyond the scope of the EMT-Paramedic. SCT is necessary because the patient’s condition requires ongoing care furnished by one or more professionals in an appropriate specialty area, for example, emergency or critical care nursing, emergency medicine, respiratory care, or cardiovascular care, or a paramedic with additional training.”12 Air ambulance attendants functioning at this level should be capable of delivering out-of-hospital care comparable to in-hospital intensive care unit (ICU) care. The AMR/FEMA Federal EMS Contract does not provide for CCT or SCT level of care for ground ambulance transports. Only BLS, ALS and ALS Bariatric transports are covered. Therefore, CCT or SCT personnel and equipment for ground ambulance transport can be provided as follows:
The sending and receiving hospitals provide CCT or SCT personnel and equipment on an AMR ALS ambulance, or
The CCT or SCT air ambulance crew can accompany the patients during the ground ambulance leg of the transport from the sending hospital and/or to the destination hospital
Department of Defense (DoD) Contraindications for Flight These are relative contraindications when there is no safe alternative and Shelter-In-Place is not an option. Contraindications require intense coordination. A. Any medical condition not stabilized B. Pregnancy >34 weeks (if normal pregnancy, validating flight surgeon may approve for
flight) C. Hbg <10 (depends on new anemia vs chronic anemia. Unique to each patient) D. Post-op <72 hours (depends on the type of surgery) E. Acute Coronary Syndrome (unstable angina, non-STEMI, STEMI) F. Any open-heart, craniotomy, spinal cord surgery <7 days (depends on post op course: if
uneventful, the patient may be approved for flight) G. Untreated pneumothorax (vented needle or tube) H. Pneumo-cephalus I. Detached retina or pneumoglobus J. Seizure within 2 weeks (depending on nature of seizure) K. Heart dysrhythmia within 1 week (if medically managed, may be approved for flight) L. Orthopedic casts (may need to bi-valve) M. Communicable condition (depends on condition) N. Respiratory isolation including possible TB O. Agitation (may require chemical sedation)
Bariatric Patient Evacuation “Bariatric patient” is an internationally accepted term applied to patients whose weight far exceeds recommended guidelines, and where body size restricts their mobility, health, or
11 Association of Air Medical Services, Model State Guidelines, first edition, 2012. 12 Department of Health and Human Services, Centers for Medicare and Medicaid Services. Medicare Benefit Policy Manual,
Chapter 10 – Ambulance Services. Section 30.1 – Definition of Ambulance Service. Specialty Care Transport. https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/bp102c10.pdf

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 77
access to available services. Their weight increases morbidity and mortality, and causes numerous health challenges.13 Transporting bariatric patients via air ambulance raises a number of issues. Strict aviation rules and regulations govern equipment, and the aircraft’s weight capacity. In some circumstances, the patient’s morphology may also affect whether the patient can be transported by air ambulance. There are certain physiological conditions that may be exacerbated by air ambulance transport due primarily to pressure changes. Due to narrow aircraft stretchers, patients may meet the weight restrictions but be unable to fit within the stretcher due to their girth. Because of these restrictions, a significant number of bariatric patients cannot be transport by air ambulance. Determining whether additional assistance will be needed to transport the patient between the healthcare facility and the aircraft will also need to be considered. Although the type and size of the aircraft may determine what size patient can be transported, the general maximum patient weight that an aircraft can accommodate is:
Fixed-wing air ambulance - 330 lbs.
Rotary-wing air ambulance - 264 lbs.
Bariatric ground ambulances can usually transport patients up to 700 lbs.
Patient Evacuation Process In the event that the medical systems within a disaster area are overwhelmed, there may be a need for a system to move patients out of the disaster area that is responsive and effective with limited individual patient information. When this occurs, local authorities may operate Casualty Collection Points (CCPs) that feed into embarkation points. Federal authorities may deploy appropriate assets to assist (e.g., AMR/FEMA Federal EMS Contract, Disaster Medical Assistance Teams [DMATs], HHS Public Health Service, DoD Veteran’s Affairs [VA] medical assets). If State or local authorities determine that resources are inadequate to transport or care for all patients, a request for Federal medical evacuation assistance can be initiated. The Department of Health and Human Services, Office of Assistant Secretary for Preparedness and Response (HHS/ASPR) may establish a Patient Movement Coordinating Group to move patients by air or by ground from locally operated Aerial Points of Embarkation (APOE) or Aeromedical Marshalling Points (AMPs) to medical facilities outside the anticipated [disaster] impact area. The FEMA Federal EMS Contract may be activated to support patient movement based on validated state plan requirements for ambulance (ground, air, and paratransit vehicles).14 The state Emergency Operations Center / Department of Health (EOC/DOH) is the source of all federal patient movement requests. The state EOC/DOH/Patient Movement Cell (PMC) will contain the HHS Joint Patient Assessment and Tracking System (JPATS) team(s), the Joint Patient Movement Expeditionary System (JPMES) and liaison officers from the other federal asset providers (e.g., AMR, etc.). The HHS JPATS team will have access to a national system to gain visibility of available beds in the NDMS network. HAvBED (Hospital Available Beds for Emergencies and Disasters) is a federally-mandated program that requires states to collect and report local
13 Hahler B (2002), Morbid Obesity: A Nursing Challenge, Medsurg Nursing Vol 11/No2 pp85-90 14 Hurricane Response Playbook. USDHHS/ASPR. http://www.phe.gov/Preparedness/planning/playbooks/hurricane/Pages/conops.aspx

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 78
hospital available bed data. It provides a centralized, national view of bed availability for supporting the medical response to a federal, regional, state or local emergency, disaster or disaster-training event.15 HAvBED data helps identify healthcare system capacity and demand during a public health emergency or mass casualty incident. JPEMS will have access to the Unites States Transportation Command (USTRANSCOM) Regulating and Command and Control Evacuation System (TRAC2ES). All patient movement requests should be validated by the Federal Health Coordinating Official/Emergency Support Function (ESF) #8 Lead.
AMR/FEMA Air Medical Evacuation System On the civilian side, FEMA is the main federal responder when a disaster overwhelms a state(s). When a state exhausts all of its resources or is lacking a unique capability during a disaster, it will turn to the federal government for assistance. The agency that usually responds and will coordinate the overall federal effort will be FEMA. The FEMA Federal EMS Contract with AMR may be activated for federal movement of patients. This contract provides 25 fixed and rotary winged air ambulances for three of the four contracted zones (zones 2, 3, and 4), and 29 fixed and rotary winged air ambulances for zone 1.
Ground Ambulance - The AMR/FEMA Air Medical Evacuation Plan calls for close coordination and communication with its air and ground ambulances. By utilizing both AMR/FEMA ground ambulances and air ambulances, it is possible to minimize or eliminate any unnecessary staging or holding of patients at airport embarkation points. Once AMR confirms that the air ambulance has arrived at the embarkation airport and is ready to receive patients, they would be transported from sending facilities by ground ambulances and taken to the waiting air ambulance. This would eliminate the need to off-load the patient from the ground ambulance into a holding area at the airport while waiting for the air ambulance to arrive. This process is especially beneficial for critical care patients or those with biomedical equipment who are less likely to tolerate multiple loading and unloading movements.
Helicopter Shuttle - During a massive air evacuation, it may be impossible or untimely for ground ambulances to effectively ingress and egress airports. Transport time and distance by ground ambulance from sending facilities to embarkation airports and from debarkation airports to receiving facilities may be excessive. Therefore, it may be useful to assign AMR/FEMA air ambulance helicopters to each of the embarkation and debarkation airports to shuttle patients. These helicopters would pick up patients at hospitals in the airport’s catchment area and bring them promptly to the waiting fixed-wing air ambulances and not be impaired by traffic and roadway obstacles. Likewise, they could also expedite transport from debarkation points to definitive receiving facilities.
Helicopter Point-to-Point Transport – Rotary-wing air ambulances can normally transport patients up to 200 miles, however to allow for multiple missions, maximum distances of 100 miles are recommended. When utilizing rotary-wing air ambulances, it is AMR’s preference to perform point-to-point patient transport
15 US Dept. of Health & Human Services, HAvBED User’s Guide https://havbed.hhs.gov/v3/docs/HAvBED%20User%20Guide.pdf

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 79
missions since they require the shortest out-of-hospital time. In this scenario, the patient is taken directly from the sending facility/location to the destination facility (assuming the sending and destination facilities can accommodate rotary-wing aircraft). This avoids unnecessary ground delays that may be detrimental, especially when transporting critical care patients. In the National Disaster Medical System (NDMS) system it may be necessary to transport patients to Patient Reception Areas (PRAs) designated by the Federal Coordinating Center (FCC).
DoD Aeromedical Evacuation System FEMA has many options available to help a state in need. One of those options is to request military assistance. FEMA has the ability to direct most other federal resource under its statutory authority, but it cannot direct the military, it must request the assistance. Military support is a last resort; all other local, state and federal resources must be exhausted prior to the military providing support or a unique requirement that cannot be found within the civilian or federal system. Defense Support of Civil Authorities (DSCA) is the process by which United States military assets and personnel can be used to assist in missions normally carried out by civil authorities. These missions have included responses to natural and man-made disasters, law enforcement support, special events, and other domestic activities. DSCA is the overarching guidance of how the United States military can be requested by a federal agency and the procedures that govern the actions of the military during employment. Requesting the military to respond to a disaster, manmade or natural, is done through a formal process established between FEMA and Department of Defense. While this process is pretty straight forward, it has many integrated steps that require involvement from numerous sources, both military and civilian. The DoD Aeromedical Evacuation System (AES) provides for the transport of NDMS validated patients in a DSCA operation utilizing DoD AES crew personnel, medical personnel, and patient staging capability.
National Disaster Medical System (NDMS)16 NDMS is a federally coordinated system that augments the Nation’s medical response capability. The overall purpose of the NDMS is to establish a single integrated National medical response capability for assisting State and local authorities in dealing with the medical effects of major disasters. NDMS combines Federal and non-Federal medical resources into a unified response to support State and local efforts to address medical and health needs arising from natural and man-made disasters. The statutory mission of the NDMS, as part of ESF #8, is to organize a coordinated effort by the NDMS Federal Partners (DHS, HHS, DoD, and the VA), working in collaboration with the states and other appropriate public or private entities to provide health services, health-related social services, other appropriate human services, and appropriate auxiliary services to respond to the needs of victims of a public health emergency, and to be present at locations, for limited periods of time, when such locations are at risk of a public health emergency. The NDMS will also support patient treatment requirements from military
16 IS-1900 – NDMS Federal Coordinating Center Operation Course.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 80
contingencies if the DoD Military Health System and VA Contingency Health System become overwhelmed. NDMS works with State and local governments and the private sector to fulfill three main objectives.
a) Medical Response - Provide supplemental health and medical assistance in domestic disasters at the request of State and local authorities.
b) Patient Movement - Evacuate patients, who cannot be cared for in the disaster area, to designated locations elsewhere in the nation.
c) Definitive Care - Provide a nationwide network of voluntary, pre-identified, non-Federal acute care hospitals capable of providing definitive care for the victims of domestic disaster or military contingency that exceeds the medical care capabilities of the affected local, state, or Federal medical system.
Patient Evacuation component of the NDMS uses DoD or FEMA EMS Contract aircraft. Patients are flown from airfields in the affected area to pre-identified reception sites call Federal Coordinating Centers (FCC). FCCs are maintained by the VA or DoD and provide the Definitive Care Component of the NDMS. FCCs enroll civilian hospitals into agreeing to make beds available during an incident. There are over 1600 hospitals in the NDMS network. FCCs also establish

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 81
agreements with airports and EMS providers to provide patient reception and distribution of patient into the local NDMS hospital network.17 Patient Evacuation is a component of the NDMS system. The system’s components include:
• Established methods for identifying and reporting patients for movement • The deployment of patient staging capabilities at outbound airfields • Pre-identified reception sites (FCCs) • Network of hospitals with available beds • Air transport with enroute care • Patient tracking systems • Repatriation of patients
Federal Coordinating Centers (FCC) The mission of a FCC is to receive, triage, stage, track and transport inpatients, affected by a disaster or national emergency, to a participating NDMS medical facility capable of providing the required definitive care. An FCC also has the potential to receive military patients should the DoD Health System and the Department of Veterans Affairs Contingency Hospital System be overwhelmed during a military contingency.18 FCCs are federal facilities (DoD or VA) located in metropolitan areas of the U.S., and are responsible for the day-to-day coordination of planning and operations in one or more assigned geographic NDMS Patient Reception Areas. NDMS participating medical treatment facilities (MTF) should be within 5 miles of the managing FCC. They recruit hospitals and maintain local non-Federal hospital participation in the NDMS. During system activation, FCCs coordinate the reception and distribution of patients being evacuated to the area. If designated by FEMA, patients transported by AMR-contracted air ambulances will likely be integrated into the NDMS system. In order to qualify as an NDMS patient, the transportation must have been coordinated through a FCC. FCCs are controlled by the Department of Defense and the Department of Veterans Affairs. NDMS regulated patients are considered ESF-8 patients. The ESF-8 Working Group will determine the FCCs for debarkation of patients.19
Map of FCCs (revised April 2014)
17 Patient Movement Appendix – HHS.gov
https://aspr.hhs.gov/wg/hhscapabilities/resourcedocs/Patient%20Movement%20Appendix.docx 18 NDMS FCC Guide – April 2014, p. 6. 19 Ibid. Section 3.2 FCC Alert and Activation, p. 18

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 82
Patient Reception Areas The Air Medical Evacuation Systems include transporting patients by air ambulance to PRAs20 which support patient reception and transport to local voluntary, pre-identified, non-Federal, acute care hospitals capable of providing definitive care for victims of a domestic disaster, emergency, or military contingency. PRAs are geographic locales containing:
One or more airfields;
Adequate patient staging facilities; and
Adequate local patient transport assets. Day-to-day coordination of planning and operations of NDMS PRAs is the responsibility of the FCCs21. These are facilities located in metropolitan areas of the U.S. and are managed by an FCC Director and FCC Coordinator. As part of the NDMS, FCCs:
Recruit hospitals and maintain local non-Federal hospital participating in the NDMS.
Coordinate exercise development and emergency plans with participating hospitals and other local authorities in order to develop patient reception, transportation, and communication plan.
20 Ibid. Lesson I – Introduction to NDMS. 21 Ibid.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 83
During system activation, coordinate the reception and distribution of patients being evacuated to the area.
Patients evacuated from the disaster area for definitive medical care arrive at the respective FCC’s PRA. Patients will be met by medical teams that will sort, assess, and match those patients with participating hospitals. Patients are off-loaded, re-triaged and staged at the patient reception sites pending further medical regulating and ground transport to a local NDMS hospital.
Coordinating Patient Regulating and Evacuation Operations For patient movement by DoD, once patient evacuation has been determined to be necessary and a DHS/FEMA Mission Assignment has been issued, the Global Patient Movement Requirements Center (GPMRC) will issue bed-reporting instructions to those FCCs activated for patient reception for patients transported by DoD aircraft. Patient movement by AMR/FEMA aircraft will be coordinated by AMR, FEMA, HHS and the sending state. These patients will likely be entered into the NDMS system. Note: this process does not exclude the possibility that the requirement for immediate evacuation could be so great that the scope of information collected and furnished would be minimal.22
Patient Tracking
DoD USTRANSCOM (CDRUSTRANSCOM) Within the DoD, USTRANSCOM will establish and maintain the Global Patient Movement Requirements Center to oversee DoD patient movement. They provide validation, regulation and in-transit visibility of DoD patient movement. They serve as the global functional manager for maintaining, operating, and identifying requirements for patient movement to include the United States TRAC2ES. In cooperation with the Assistant Secretary of Defense for Health Affairs and the Under Secretary of Defense for Personnel and Readiness, develop and maintain current and future patient movement Automated Identification System (AIS) to provide a global network to regulate and monitor in-transit visibility of patients, and medical non-medical attendants within the DoD patient movement system.
22 Ibid.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 84
HHS/NDMS - JPATS - Patient movement, within NDMS, includes patient evacuation, medical regulating, en-route care, and patient tracking/in-transit visibility. NDMS has developed a national patient tracking system called the Joint Patient Assessment and Tracking System (JPATS).” In scenarios requiring larger evacuations and/or operations across greater distances, JPATS may be used. JPATS was developed through an interagency agreement between the Department of Defense and the Department of Health and Human Services.23
AMR – Forward Operating Base Planning and Tracking System (FOBPATS) – AMR will utilize JPATS if available and will simultaneously use its internal tracking system known as Forward Operating Base Planning and Tracking System (FOBPATS). This is a web-based SQL database used for tracking resources, assignments and patients. The system has been designed so that multiple users can login and make edits according to their specific area of access and expertise. In addition to tracking resources, FOBPATS allows the Forward Operating Base (FOB) Incident Management Team (IMT) to create assignments and assign resources, thus allowing a dynamic and real-time view of all resources which is accessible to senior leadership of AMR’s National Command Center (NATCOM). The table below describes the comprehensive air ambulance patient movement process
23 NDMS official Web site of Force Health Protection & Readiness Policy. May 5, 2014. http://fhpr.osd.mil/

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 85
Types of Air Ambulances The AMR/FEMA Federal EMS Contract allows for five types of fixed-wing air ambulances and four types of rotary-wing air ambulances. Air Ambulance Typed Resource Definitions are attached in Appendix A.
Fixed-wing Air Ambulance Fixed-wing air ambulance may be furnished when the patient’s medical condition is such that transport by ground ambulance, in whole or in part, is not appropriate. Generally, transport by fixed-wing air ambulance is used when the patient’s condition requires rapid transport to a treatment facility, and either great distances or other obstacles, e.g., heavy traffic, preclude such rapid delivery. Transport by fixed-wing air ambulance may also be

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 86
necessary because the patient is inaccessible by a ground or water ambulance vehicle.24
Types of fixed-wing air ambulances: Type I – CC and ALS Type II – CC and ALS Type III – ALS Type IV – BLS (NOTE: It is unlikely that any aircraft would be staffed with only BLS crew) Type V – SCT and Neonatal
Air speed for fixed-wing aircraft varies depending on the type. To transport the maximum number of patients in the shortest period of time, high-speed jets are recommended. Below are approximate air speeds for various types of fixed-wing aircraft.
Jets – 360-560 mph Turbo prop – 190-350 mph Piston-engine propeller – 150-300 mph
Rotary-wing Air Ambulance Rotary-wing air ambulance may be furnished when the patient’s condition is such that transport by ground ambulance, in whole or in part, is not appropriate. Generally, transport by rotary-wing air ambulance is necessary because the patient’s condition requires rapid transport to a treatment facility, and either great distances or other obstacles, e.g., heavy traffic, preclude such rapid delivery. Transport by rotary-wing air ambulance may also be necessary because the patient is inaccessible by ground or water ambulance vehicle.25 For patients that require transport to destinations that exceed the range of helicopter air ambulances, it may be advantageous to use helicopter air ambulances to transport patients from their point of origin to nearby airports where they would be transferred to fixed-wing air ambulances.
Types of rotary-wing air ambulances: Type II –CC and ALS Type III –CC and ALS Type IV – CC and ALS Type V – SCT and Neonatal
Airports and other Ground Considerations 15.1. Hangar Space – No airport hangar space should be needed for fixed or rotary-
wing air ambulances assuming they will not be staged for extended periods. Coordination with air ambulance support resources is essential to minimize that ground time. Factors that will affect ground time include:
Load and off-load time for patients
Refueling
Crew swap
Maintenance
Medical resupply
Inclement weather
24 Ibid. Ch. 10, section 10.4 – 1. Fixed-wing Air Ambulance.
https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/bp102c10.pdf 25 Ibid. Section 10.4 – 2 Rotary-wing Air Ambulance

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 87
Air Support - Consideration should be given to designate airport space to stage Air Medical Support Teams, communications, and equipment.
15.2. Aircraft Maintenance and Additional Aircraft - Depending on the type of aircraft used, regular preventive maintenance routines must be performed after a fixed number of hours of operation. It is understood that AMR/FEMA EMS air ambulance services are intended to operate 24/7 without interruption and additional aircraft may be required to take the place of those taken out of service for maintenance.
15.3. Fixed-wing space requirements– Each fixed-wing aircraft will require a minimum of 60’ x 60’ area to stage if multiple aircraft are on the ground simultaneously. This is based on the average size fixed-wing aircraft. Runway length for air ambulances should comply with Federal Aviation Administration (FAA) regulations “Runway Length Requirements for Airport Design.”26
15.4. Rotary-wing space requirements– A heliport/helistop is designed for helicopter takeoffs and landings. A heliport has facilities such as fuel, hangaring and attendants. A helistop has no support facilities and is an area that can be multi-use, such as a parking lot, athletic field, rest area along highways, and golf course. All international standards have space requirements (both on land and in the air) for an obstacle-free area in order for the helicopter to land and takeoff. The standards for touchdown area sizes (the pad itself) are generally predicated on the size of the aircraft landing gear footprint or the rotor diameter. The obstacle-clear areas surrounding the touchdown area are generally determined by a multiplier of the aircraft’s overall length or rotor system size. They can vary from an open area of 64’ x 64’ for small helicopters to 110’ by 110’ for medium twin-engine helicopters. There are approach slope requirements for at least one approach and departure route for facility access. These airspace standards are generally based on the size of the largest aircraft using the facility. The FAA authorizes helicopters to conduct simultaneous landings or takeoffs if the distance between the landing and takeoff points is at least 200-foot minimum.27
15.5. Priority Airspace Management for Disasters—The FAA Airspace Management Plan for Disasters28 provides a nationally consistent framework and suite of supportive tools for the use of the FAA’s air traffic and airspace management operational expertise and capabilities, as well as statutory authority, to enhance the safety and effectiveness (including unity of effort) of air missions supporting response and recovery efforts during disasters. The plan also speaks to the use of these tools to safeguard persons and property on the ground.
Operational priority is given to civilian air ambulance flights when using the call sign “MEDEVAC”. Air traffic controllers should assist pilots of MEDEVAC aircraft to avoid areas of significant weather and turbulent conditions. They should also provide notifications to expedite ground handling of patients, vital organs, or urgently needed medical materials. It is recognized that heavy [air] traffic flow may affect the controller’s ability to provide priority handling. However, without compromising safety, good judgment must be used in each situation to facilitate the most expeditious movement of MEDEVAC aircraft.29
26 US DOT/FAA Advisory Circular No. 150/5325-4B. 7/1/2005 27 FAA Air Traffic Organization Policy, Order JO 7110.65V. April 3, 2014 28 FAA Airspace Management Plan for Disasters. Version 1.1 – 18 July 2012 29 FAA Air Traffic Control Policy. Order JO 7110.65V. April 3, 2014.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 88
Patient Transport Distance Safety and clinical considerations of transported patients is paramount. It is assumed that transportation vehicles, i.e., buses, ambulances, helicopters and fixed-wing aircraft, will make multiple round trips. Air ambulance transportation should be considered if the time required to transport the patient by ground ambulance as opposed to air endangers the patient’s life or health.30 During disaster evacuations, it is recommended that patients be transported to host locations that are an adequate safe distance from the disaster event but not so distant as to not allow for multiple round trips. Air ambulances are usually used for critical care patients and thus patient transport distances should be short enough that they do not require refueling with patients on board since this may adversely affect the patient. For these reasons, the following transport distance guidelines are established.
Ground Ambulances distance – One-way distance to transport clinically stable patients by ground ambulance should not exceed 200 miles or 6 hours. This includes all ground ambulance types: ALS, BLS, Bariatric and Med-Evac Units. For unstable patients whose medical condition at time of pick-up requires immediate and rapid transport due to the nature and/or severity of the illness/injury the maximum transport time should be 30-60 minutes.31
Paratransit Vehicles distance – One-way distance to transport patients by paratransit vehicle should not exceed 200 miles or 6 hours.
Air Ambulance Rotary-wing distance – Although rotary-wing air ambulances are capable of flying 200-400 miles non-stop depending on the type of aircraft, the maximum one-way patient transport distance for rotary-wing air ambulances should not exceed 100 miles. This facilitates more round-trip missions and minimizes the need for in-route refueling of aircraft, which will extend the mission time, which could be detrimental, especially to critical patients.
Air Ambulance Fixed-wing distance – Although fixed-wing aircraft are capable of transporting long distances, most missions will be transporting critical care patients, thus it is recommended that transport distance be no greater than 600 miles. This will also allow for more round trips if multiple patient transports are required. The approximate maximum range for fixed-wing aircraft without refueling is as follows:
Jets – 1,500-3,000 miles
Turbo prop – 1,250 miles
Piston-engine propeller – 850 miles
Crewmember Flight Time and Duty Period Limitations and Rest Requirements Air ambulances deployed pursuant to the AMR/FEMA Federal EMS Contract shall be available for 24/7 continuous operation. Air ambulance crewmembers shall adhere to Federal regulations on crewmember flight time and duty period limitations and rest requirements. 32 It is anticipated that multiple round-trip air ambulance missions will be performed. To provide continuous air ambulance operations, aircraft operating pursuant to the AMR/FEMA Federal EMS Contract shall consider the following: It may be necessary to send two flight crews to the originating AMP. This would ensure that two flight crew shifts were on hand. It may also be necessary for each flight crew to
30 Department of Health and Human Services, Centers for Medicare and Medicaid Services. Medicare Benefit Policy Manual,
Chapter 10 – Ambulance Services. Section 10.4.3 – Time Needed for Ground Transport. Rev. 1, 10-01-03. http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/bp102c10.pdf 31 Ibid. 32 CFR Title 14, Chapter 1, Subchapter G, Part 135, Subpart F – Crewmember flight time and duty period limitations and rest
requirements. Jan. 27, 2015.
Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 89
have an additional third pilot on board in the event that the primary and secondary pilots reach their maximum flight time. Assigning FCCs and PRAs is important. Knowing which FCCs and PRAs are to be used will allow air ambulances to calculate the number of missions that can be accomplished within a given period. FCCs/PRAs will be assigned as soon as the ESF-8 Working Group determines which FCCs will be alerted/activated. At that time, AMR and DoD can do their respective planning of missions. There should be no instance where an aircraft finds out what their destination airfield will be immediately before take-off, but AMR and DoD both need to be flexible for these possible last minute unplanned changes due to FCC closures, bed unavailability, weather issues, etc. Before commencing air ambulance transports, flight crews will calculate flight time to ensure the pilot and aircrew flight time threshold does not expire mid-flight. Flight crewmembers are not considered to be assigned flight time in excess of flight time limitations if the flights to which he/she is assigned normally terminate within the limitations but due to circumstances beyond the control of the certificate holder or flight crewmember (such as adverse weather conditions), are not at the time of departure expected to reach their destination within the planned flight time.33
Patient Loading and Off-Loading Coordination with ground ambulances on the sending and receiving end of air ambulance missions is essential. Patient loading onto aircraft at sending airports AMPs and off-loading at receiving airport PRAs is enhanced if AMR-contract ground ambulances are used. This should also improve turn-around time for multiple missions. In optimum conditions where AMR air and ground ambulances are used, patient load and unload time at sending and receiving airports should not exceed 30 minutes to load and 30 minutes of off-load each patient. Patient condition or acuity may also play a significant factor in loading and off-loading time. More critical patients with complicated biomedical equipment will take longer to load and off-load. Continuity of care from sending hospital to ground ambulance and then to air ambulance is important. At the receiving end of the mission, it is equally important that there be qualified clinicians to accept patients. It would be inappropriate for an air ambulance critical care clinician to turn over a critical patient to a ground ambulance crew who was not qualified to care for critical care patients.
Command and Control During active air evacuations, all Air Medical Support personnel shall fall under the direct authority of the Air Ambulance Group Leader who reports to the FOB Air Ambulance Branch Director who in turn, reports to the FOB Operations Section Chief or the NATCOM Incident Commander, depending on the deployment situation. In deployments where air ambulance operations involve multiple jurisdictions, or involve integrated tactical control of patient movement, the FOB Air Ambulance Branch Director will report directly to the NATCOM Incident Commander and work closely with the NATCOM Air Ambulance Branch Director. In situations where the FOB air ambulance operations are established at airheads
33 CFR Title 14, Chapter 1, Subchapter G, Part 135, Subpart F, §135.263 – Flight time limitations and rest requirements: All
certificate holders. Jan. 27, 2015.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 90
that are very remote to the ground ambulance base, there may be limited interaction with FOB Ground Ambulance and FOB Air Ambulance leaders. In this case the FOB Air Ambulance Branch may report directly and exclusively to NATCOM and the National Incident Commander (IC). AMR may also deploy Liaison Officers (LNO) to the State EOC and/or the State Health Dept. EOC. The provision of clinical patient care is but one component of a complicated air ambulance transport mission. Qualified EMS Command Staff are needed to coordinate all aspects of the air ambulance mission including logistics. Each designated AMR AMP should have the following AMR IMT Command Staff to coordinate patient movement and serve as functional leaders on the Operations Support Team:
AMP Operations Support Team
Air Ambulance Group Leader
Logistics Unit Leader
Communications Unit Leader
Documentation Unit Leader
Fixed Location Support Personnel to serve as Air Evacuation Team Members
Note that some positions may be combined, depending on the size and scope of the mission.
Air Medical Support Teams Air Medical Support Teams or Field Operations Support Teams shall be designated and assigned to each
active AMR AMP and PRA at the time of deployment. All personnel should expect to be self-sufficient for

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 91
the first 72 hours but it is AMR’s intent to establish logistics support elements at each AMP to the level required to provide basic support, re-supply, transportation, sustenance and maintenance to AMR personnel. Once personnel are assigned to Air Medical Support, they shall remain at their designated assignment until further directed by the Air Ambulance Branch Director. All Air Medical Support Ambulances will be given special placards that identify them as Air Medical Support Ambulances, helping to ensure that they are not redirected to other non-air medical support activities. Requests for air ambulance transportation will be directed to AMR NATCOM. As requests are generated for patient transportation by air, NATCOM or Area Command will alert the appropriate Air Ambulance Branch Director and inform them of the assignment. NATCOM or Area Command shall designate the appropriate Air Ambulance and Air Medical Support units and deploy them to the appropriate AMP. AMR, in coordination with the AMP Command Team, will confirm that the designated Air Ambulance is on the ground and prepared to receive the patient prior to the patient arriving at the AMP. The Air Medical Support ambulance shall meet the aircrew, transfer the patient and return immediately to service as directed by the Air Ambulance Group Leader. Air Medical Support Teams may include some or all of the following positions:
Air Ambulance Branch Director
AMP Air Ambulance Group Leader
AMP Logistics Unit Leader
AMP Documentation Unit Leader
AMP Communications Unit Leader
AMP Air Medical Support Ground Ambulances
PRA Air Medical Support Ground Ambulances
Air Evacuation Team Members – Hospital and Airport
Air Evacuation Team Members – Air Evacuation Team Members (AETM) may be stationed at sending medical facilities and/or embarkation and debarkation airports.
AETM at Sending Medical Facilities - AETM are ALS EMS personnel who are deployed to sending health care facilities to identify patients who need to be evacuated, then assess, triage and coordinate ground and air ambulance evacuation. They do not routinely determine which patients should be transported by air ambulance. These clinical decisions are made by the sending facilities or local and state authorities. The AETM will validate the Patient Movement Request against the actual patient condition and type of air ambulance available. They may be designated by AMR as the Federal EMS provider or they may be part of the local EMS system.
AETMs at the sending medical facility should confirm the patients are prepared for air medical transport. Actions would include:
A. Obtain complete medical records 1. Most recent history and physical, physician, nursing, respiratory notes 2. Medication administration records 3. Electronic or hard copies of radiologic studies 4. Most recent lab work
B. Obtain extra medications for air transport 1. Extra premixed IV infusions with medications added 2. Additional sedation / analgesic infusion

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 92
3. Insulin for diabetic patients 4. Scheduled oral medications (especially for long fixed wing transports)
C. Preparation of hospital interventions for air medical transport 1. Orthopedic interventions
a. Bi-valve all casts b. Removal of traction devices c. Removal of free hanging weights
2. Advanced airway patient management a. Bring bag-valve-mask ventilator with patient b. Keep in-line suction attached c. Obtain extra tracheostomy tube
3. Empty indwelling catheters a. Urinary catheters or ileostomy tubes b. Jackson-Pratt or other wound drains c. Fecal management system
Air Evacuation Team Member at sending medical facilities should attempt to ensure that there is no delay or interruption in continuity of care from the time patients are removed from the sending facility until they reach the appropriate AMP to: A) be placed into a waiting aircraft or B) delivered to an appropriately equipped/staffed air medical embarkation point. The approximate ratio of Air Evacuation Team Members at medical facilities to in-patients awaiting evacuation is usually one AETM to every five patients (1:5). These numbers may vary depending on the complexity of the situation, e.g., patient condition, hospital conditions, availability of other support staff, etc. There should be one additional AETM assigned to each sending healthcare facility to coordinate the evacuation and synchronize patient departure with arrival of air ambulances at embarkation airports. This person would be designated as the air evacuation team leader. AETM may be assigned from various sources:
Fixed Location Support Personnel who are not assigned to ambulance duty
Ambulance crewmembers who are assigned AETM duties
Air ambulance network personnel who are not assigned aircraft or airport duties
AETM at Airports - Airport AETM are ALS EMS personnel who are deployed to the airport patient embarkation points to assist in loading and unloading patients and to minimize any delay or interruption in continuity of care from the time patients arrive at the embarkation airport until they depart. AETM may be part of the AMR air medical support team or they may be part of the local EMS system. Many variables that may determine the number of AETMs needed at the embarkation airport. The usual ratio is two AETM per aircraft (2:1) for load/unload events since ground ambulance crews and aircraft crews should also be available to assist. If aircraft load and unload one at a time, then two AETM per airport should be sufficient. If multiple aircraft are loading and unloading simultaneously, then multiple AETMs would be needed; two for each aircraft. AETM may be Fixed Site Support Personnel who are not assigned to an ambulance, or they may be ambulance crewmembers who are assigned AETM duties. AETMs may also be needed at debarkation points (receiving airports) to assist at the PRC.
Air Medical Support Ground Ambulances Air Medical Support Ground Ambulances are ALS ground ambulances used to transport patients to/from AMPs and PRAs. Coordination with ground ambulances on the sending and receiving end of air missions is essential. Loading, unloading, and turn-around time would be enhanced if AMR contracted ground ambulances are used on the sending and receiving end of the air ambulance missions. There are many variables associated with air ambulance evacuations. In order to determine the number of ground ambulances to support air ambulance evacuation, the following information is needed:
How many AMPs and PRAs are established?

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 93
How many air ambulances are assigned to each AMP and PRA?
Are the air ambulances arriving at the AMP and PRA simultaneously, or will they be staggered?
Will there be multiple round trip missions for the air ambulances or will they make one trip only?
What is the distance from the sending hospital(s) to the AMP?
What is the distance from the PRA to the receiving hospital?
It is assumed that not all air ambulances will be on the ground and prepared to accept patients at the AMP at the same time. Usually there is a staggered loading and unloading of patients on aircraft. The usual ratio of ALS ground ambulances needed to support a single air ambulance is one ALS ground ambulance per every one air ambulance (1:1 ratio). This is to ensure there is uninterrupted flow of patient movement, especially if there are multiple aircraft at the AMP waiting to receive patients. Coordination of transferring patients to/from ground ambulance to air ambulance is essential. There should be no unnecessary idle time at the AMP or PRA with patients waiting to be loaded or unloaded to/from aircraft.
After the vehicle is checked-in correctly according to AMR procedures, the Check-In Unit Leader will (by authority of the Field Operations Incident Command) designate the specific number of ambulances required for Air Medical Support and assign them an Air Medical Support placard, which will be in addition to their initial ground ambulance deployment placard. At that time, the Air Medical Support ambulance will report to the Air Ambulance Branch Director and be given further directions.
The Air Medical Support ambulances will continue to report to the Air Ambulance Group Leader (or his/her designee) throughout the entire Air Evacuation process and will AT NO TIME deviate from those missions assigned by the Group Leader.
When the Air Evacuation process is complete, the Air Ambulance Group Leader will inform all the Air Medical Support ambulances at which time they will surrender their Air Medical Support placard and revert to functioning as a Ground Ambulances and begin reporting to the Ground Ambulance Branch Director.
Recommended Air Medical Support Resources The following air medical support resource ratios are recommended in order to maximize the efficiency of air ambulance operations.
One dedicated ALS Air Medical Support ground ambulance for every one air ambulance (1:1 ratio)
One ALS Air Evacuation Team Member- Healthcare Facility - for every five facility in-patients (1:5 ratio)
One ALS Air Evacuation Team Member at every sending healthcare facility (1:1 ratio) to coordinate the overall facility air medical evacuation for AMR.
Two ALS Air Evacuation Team Members per embarkation and debarkation point (2:1 ratio). Additional Team Members may be needed if multiple aircraft are loading or unloading simultaneously.
Four AMR IMT Command Staff per embarkation point (4:1 ratio).
Air Medical Support Vehicle Placarding
Prior Notice Event During an event with prior notice, all ground ambulance vehicles are placarded as either ALS, BLS, ALS Bariatric or ALS Med-Evac prior to deploying through AMR’s Rapid Electronic Deployment System (REDS). They will receive a unique and specific placard number that identifies the vehicle type and parent company. An official ‘Notice to Proceed’ will be issued by AMR. Once the Notice is received, all vehicles depart for the check-in location assigned to them.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 94
It is assumed that AMR will know the exact number of vehicles required to support Air Ambulance operations. After the vehicle is checked-in correctly according to AMR procedures, the Check-In Unit Leader will (by authority of the Field Operations Incident Command) designate the specific number of ambulances required for Air Medical Support and assign them an Air Medical Support placard, which will be in addition to their initial ground ambulance deployment placard. At that time, the Air Medical Support ambulance will report to the Air Ambulance Branch Director and be given further directions. Regardless of function, the ambulance should always use their original Ground Ambulance placard number for identification purposes.
No-Notice Event During an event with no-notice, all ground ambulance vehicles are placarded as ALS, BLS, ALS Bariatric or ALS Med-Evac at the time of deployment through a combination of AMR’s REDS and via communication with the NATCOM Ground Ambulance Branch Director. They receive a unique and specific placard number that identifies the vehicle type and parent company. In addition, NATCOM or the AMR Office of Emergency Management (OEM) will contact specific companies and assign Air Medical Support vehicles from them. Those companies will print out an Air Medical Support ambulance placard from their REDS profile and affix it to the vehicle. Once a Notice to Proceed is received, all vehicles depart for the check-in location assigned to them. The Air Medical Support ambulances will report to the Air Ambulance Group Leader (once established) throughout the entire Air Evacuation process and will AT NO TIME deviate from those missions assigned by the Air Ambulance Branch Director. When the Air Evacuation process is complete, the Air Ambulance Group Leader will inform all Air Medical Support ambulances at which time they will surrender their Air Medical Support placard and revert to functioning as a Ground Ambulance and begin reporting to the Ground Ambulance Branch Director. Regardless of function, the ambulance should ALWAYS use their original ground Ambulance placard number for identification purposes.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 95
Sample of Air Medical Support Placard

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 96
GLOSSARY
AAMS – Association of Air Medical Services AES – Aeromedical Evacuation System AETM - Air Evacuation Team Member (healthcare facility or airport) AIS – Automated Identification System ALS – Advanced Life Support AMP – Aeromedical Marshalling Points AMR – American Medical Response APOE – Aerial Points of Embarkation ASPR – Assistant Secretary for Preparedness and Response BLS – Basic Life Support CC – Critical Care CCP – Casualty Collection Point CCT – Critical Care Transport CDRUSTRANSCOM – Commander U.S. Transportation Command DMAT – Disaster Medical Assistance Team DoD – Department of Defense DOH – Department of Health DSCA – Defense Support of Civil Authorities EMS – Emergency Medical Services EOC – Emergency Operations Center ESF – Emergency Support Function FAA – Federal Aviation Administration FCC – Federal Coordinating Center FEMA – Federal Emergency Management Agency FOB – Forward Operating Base FOBPATS – Forward Operating Base
Planning and Tracking System GPRMC – Global Patient Movement
Requirements Center
HAvBED – Hospital Available Beds for Emergencies and Disasters HHS – Dept. of Health and Human Services IC – Incident Command ICU – Intensive Care Unit IFT – Interfacility Transport IMT – Incident Management Team JPATS – Joint Patient Assessment and
Tracking System JPMES - Joint Patient Movement
Expeditionary System LNO – Liaison Officer MEDEVAC – Medical Evacuation MTF – Medical Treatment Facility NATCOM – National Command Center NDMS – National Disaster Medical System OEM – Office of Emergency Management PMC – Patient Movement Cell PRA – Patient Reception Area REDS – Rapid Electronic Deployment System SCT – Specialty Care Transport Td Toxoid – Tetanus-Diphtheria Toxoids Tdap – Tetanus, Diphtheria and Pertussis TRAC2ES - Regulating and Command and Control Evacuation System TRANSCOM – U.S. Transportation Command VA – Veterans Administration

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 97
Appendix A
Typed Resource Definitions: Air Ambulance (Fixed-Wing) AMR/FEMA Federal EMS Contract Revised 2/11/2015
CATEGORY: Health & Medical (ESF #8) Kind: Aircraft/Team
MINIMUM CAPABILITIES: Type I Type II Type III Type IV Type V
Component Metric
Overall Function
Provides emergency
medical care, evacuation,
and transportation
services via fixed wing
aircraft. May also be
utilized to import
personnel and or
equipment/ supplies into
the area of need.
Capable of providing
clinical and transportation
services to a range of
patient conditions,
includes aircraft, staff,
equipment, and supplies.
Capable of providing
clinical and transportation
services to a range of
patient conditions,
includes aircraft, staff,
equipment, and supplies.
Capable of providing
clinical and transportation
services to a range of
patient conditions,
includes aircraft, staff,
equipment, and supplies.
Capable of providing
clinical and transportation
services in the range of
basic life support patient
conditions, includes
aircraft, staff, equipment,
and supplies.
Capable of transporting a patient
who needs unique, neonatal
specialty care support enroute,
(usually one patient is transported
but can be more depending upon
support capabilities and lift of
aircraft)
Team Request for
Mutual Aid should
specify specialty care
services as needed.
Team experienced and
actively involved in the
care and transportation of
air medical patients.
Critical Care and
Advanced Life Support
Critical Care and
Advanced Life Support Advanced Life Support Basic Life Support
Specialty transport trained and
qualified to care for the specific
patient and associated supporting
equipment
Personnel Minimum Staff
3 (pilot and 2 EMS
practitioners, one of which
is licensed as a critical
care clinician)
3 (pilot and 2 EMS
practitioners, one of which
is licensed as a critical
care clinician)
3 (pilot and 2 EMS
practitioners, one of which
is licensed as a critical
care clinician)
2 (pilot and1 paramedic)
As required for the mission and to
meet the standards of care for the
specific patient
Capability Patient Care and
Transport 2 or more litter patients 1 litter patient 2 or more litter patients 1 litter patient
Inverter for specialized medical
equipment (such as neonatal
isolette)
Aircraft Fixed-wing capabilities Day and night operations
plus IFR
Day and night operations
plus IFR
Day and night operations
VFR only
Day and night operations
VFR only As required by mission
Equipment and
Supplies
Equipment and supplies
needed to meet mission
objectives
Range of equipment and
supplies commensurate
with the mission
assignment PPE
consistent with OSHA
1910.134 and 1910.1030
requirements
Range of equipment and
supplies commensurate
with the mission
assignment PPE
consistent with OSHA
1910.134 and 1910.1030
requirements
Range of equipment and
supplies commensurate
with the mission
assignment PPE
consistent with OSHA
1910.134 and 1910.1030
requirements
Range of equipment and
supplies commensurate
with the mission
assignment PPE
consistent with OSHA
1910.134 and 1910.1030
requirements
Range of equipment and supplies
commensurate with the mission
assignment PPE consistent with
OSHA 1910.134 and 1910.1030
requirements
Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 98
Typed Resource Definitions: Air Ambulance Fixed Wing (continued)
Fixed-Wing service in a disaster is primarily for moving injured or sick people located in the disaster area to medical facilities located outside the disaster area. Fixed-Wing service providers may also be utilized to import personnel and or equipment/supplies into the area of need. Fixed-Wing services require the use of an airport of sufficient length and access to a sufficient quantity of proper fuel type for the type of aircraft requested. Backup supplies and some equipment may be required depending upon number of patients and type of event.
1. Security, transportation (including patient care crew to and from LZ for the sending and receiving medical facilities), food, and/or rest facilities will be provided by the requesting jurisdiction unless other arrangements have been made
2. In complex air operations with multiple aircraft, additional staff is recommended to ensure the ongoing availability of resources required to safely and effectively support the mission assignment.
3. Ground safety assurance and traffic control are important support requirements for injury and crash prevention. This support may be significant depending upon the size and location of the incident.
4. The estimation of the quantity of air ambulance resources needed is based on many factors such as the nature of the mission, logistics, intensity of demand, duration of service activity, and allowance for rest periods.
5. Aircraft maintenance requirements may occur during deployment. Aviation maintenance must be planned. Hangar facilities should be planned for all extended operations.
6. Aircraft communication equipment may be programmable for interoperability but this capability must be verified. Plan for augmenting existing communication equipment to allow Fixed-Wing aircraft to communicate with air operations coordination center. Coordination with ground ambulance service required.
7. A minimum of Td toxoid or Tdap (receipt of primary series and booster within the past 10 years) and a complete Hepatitis B Vaccination Series OR a waiver of liability. Also refer to immunization recommendations for emergency responders by Centers for Disease Control for additional guidance for specific responses.
8. Critical Care Clinicians are licensed healthcare professionals who can treat critically ill or injured patients who are at high risk for actual or potential life-threatening health problems. These clinicians can provide complex out-of-hospital patient care comparable to in-hospital ICU and CCU care. They provide specialized medical interventions beyond the DOT/NHTSA minimum standards and scope of practice for Paramedics.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 99
Typed Resource Definitions: Air Ambulance (Rotary-Wing) AMR/FEMA Federal EMS Contract Revised 2/11/2015
CATEGORY: Health & Medical (ESF #8) KIND: Aircraft/Team
MINIMUM CAPABILITIES: TYPE II TYPE III TYPE IV TYPE V
Component Metric
Overall Function
Provides emergency
medical care, evacuation,
and transportation services
via rotary wing aircraft. May
also be utilized to import
personnel and or
equipment/supplies into the
area of need.
Capable of providing
clinical and transportation
services to a range of
patient conditions, includes
aircraft, staff, equipment,
and supplies.
Capable of providing
clinical and transportation
services to a range of
patient conditions, includes
aircraft, staff, equipment,
and supplies.
Capable of providing
clinical and transportation
services to a range of
patient conditions, includes
aircraft, staff, equipment,
and supplies.
Capable of transporting a patient who
needs unique, neonatal specialty
care support enroute (usually one
patient is transported but can be more
depending upon support capabilities
and lift of aircraft)
Team Request for Mutual
Aid should specify care
specialty services as
needed.
Team experienced and
actively involved in the care
and transportation of air
medical patients.
Critical Care and
Advanced Life Support
Critical Care and
Advanced Life Support
Critical Care and
Advanced Life Support
Specialty transport trained and
qualified to care for the specific patient
and associated supporting equipment
Personnel Minimum staff
3 (pilot and 2 EMS
practitioners, one of which
is licensed as a critical care
clinician)
3 (pilot and 2 EMS
practitioners, one of which
is licensed as a critical care
clinician)
2 (pilot and 1 EMS
practitioner licensed as a
critical care clinician)
Appropriate level and number of
staff/specialists required for the
mission and to meet the standards of
care for the specific patient
Capability Patient Care and Transport 2 or more litter patients 1 litter patient 1 litter patient Unique to the patient(s)
Aircraft Rotary-wing with these
capabilities
Day and night operations
Plus IFR NOTE: NVG
capability must be
requested specifically
Day and night operations
VFR only NOTE: NVG
capability must be
requested specifically
Day and night operations
VFR only NOTE: NVG
capability must be
requested specifically
Tailored to fit the mission
Equipment and Supplies Equipment needed to meet
mission objectives
Range of equipment and
supplies commensurate
with the mission
assignment PPE consistent
with OSHA 1910.134 and
1910.1030 requirements
Range of equipment and
supplies commensurate
with the mission
assignment PPE consistent
with OSHA 1910.134 and
1910.1030 requirements
Range of equipment and
supplies commensurate
with the mission
assignment PPE consistent
with OSHA 1910.134 and
1910.1030 requirements
Range of equipment and supplies
commensurate with the mission
assignment PPE consistent with
OSHA 1910.134 and 1910.1030
requirements

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 100
Typed Resource Definitions: Air Ambulance Rotary Wing (continued)
1. Security, transportation (including patient care crew to and from LZ of the sending and receiving medical facilities), food, and/or rest facilities will be provided by the requesting jurisdiction unless other arrangements have been made
2. Additional staff, e.g., administrative, logistics, maintenance, is recommended to ensure the ongoing availability of resources required to safely and effectively support the mission assignment.
3. Ground safety assurance and traffic control are important support requirements for injury and crash prevention. This support may be significant depending upon the size and location of the incident.
4. The estimation of the quantity of air ambulance resources needed is based on many factors such as the nature of the mission, logistics, intensity of demand, duration of service activity, and allowance for rest periods.
5. Aircraft maintenance requirements may occur during deployment. Aviation maintenance must be planned. Hangar facilities should be planned for all extended operations. Fuel tankers or other supply points must be identified. Backup supplies and some equipment may be required depending upon number of patients and type of event.
6. Aircraft communication equipment may be programmable for interoperability but this capability must be verified. Provide communication frequencies of ground incident command and air operations coordination center. Plan for augmenting existing communication equipment.
7. Landing zones (space, clearance, and weight restrictions) must be considered. The typical civilian air ambulance requires an LZ of 150’ x 150’.
8. A minimum of Td toxoid or Tdap (receipt of primary series and booster within the past 10 years) and a complete Hepatitis B Vaccination Series OR a waiver of liability. Also refer to immunization recommendations for emergency responders by Centers for Disease Control for additional guidance for specific responses.
9. Critical Care Clinicians are licensed healthcare professionals who can treat critically ill or injured patients who are at high risk for actual or potential life-threatening health problems. These clinicians can provide complex out-of-hospital patient care comparable to in-hospital ICU and CCU care. They provide specialized medical interventions beyond the DOT/NHTSA minimum standards and scope of practice for Paramedics.
Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 101
Appendix 11 DHS Non-Disclosure Agreement (NDA)
DEPARTMENT OF HOMELAND SECURITY
NON-DISCLOSURE AGREEMENT AMR Subcontractors
I, , an individual official, employee, consultant, or subcontractor of or
to American Medical Response (the Authorized Entity), intending to be legally bound, hereby consent to the
terms in this Agreement in consideration of my being granted conditional access to certain information, specified
below, that is owned by, produced by, or in the possession of the United States Government.
(Signer will acknowledge the category or categories of information that he or she may have access to, and the signer’s willingness to
comply with the standards for protection by placing his or her initials in front of the applicable category or categories. AMR/FEMA
subcontractors and employees should initial all three categories below.)
Initials:
Protected Critical Infrastructure Information (PCII)
I attest that I am familiar with, and I will comply with all requirements of the PCII program set out in the Critical
Infrastructure Information Act of 2002 (CII Act) (Title II, Subtitle B, of the Homeland Security Act of 2002,
Public Law 107-296, 196 Stat. 2135, 6 USC 101 et seq.), as amended, the implementing regulations thereto (6
CFR Part 29), as amended, and the applicable PCII Procedures Manual, as amended, and with any such
requirements that may be officially communicated to me by the PCII Program Manager or the PCII Program
Manager’s designee.
Initials:
Sensitive Security Information (SSI)
I attest that I am familiar with, and I will comply with the standards for access, dissemination, handling, and
safeguarding of SSI information as cited in this Agreement and in accordance with 49 CFR Part 1520, “Protection
of Sensitive Security Information,” “Policies and Procedures for Safeguarding and Control of SSI,” as amended,
and any supplementary guidance issued by an authorized official of the Department of Homeland Security.
Initials:
Other Sensitive but Unclassified (SBU)
As used in this Agreement, sensitive but unclassified information is an over-arching term that covers any
information, not otherwise indicated above, which the loss of, misuse of, or unauthorized access to or
modification of could adversely affect the national interest or the conduct of Federal programs, or the privacy to
which individuals are entitled under Section 552a of Title 5, as amended, but which has not been specifically
authorized under criteria established by an Executive Order or an Act of Congress to be kept secret in the interest
of national defense or foreign policy. This includes information categorized by DHS or other government
agencies as: For Official Use Only (FOUO); Official Use Only (OUO); Sensitive Homeland Security Information
(SHSI); Limited Official Use (LOU); Law Enforcement Sensitive (LES); Safeguarding Information (SGI);
Unclassified Controlled Nuclear Information (UCNI); and any other identifier used by other government agencies
to categorize information as sensitive but unclassified.
I attest that I am familiar with, and I will comply with the standards for access, dissemination, handling, and
safeguarding of the information to which I am granted access as cited in this Agreement and in accordance with
the guidance provided to me relative to the specific category of information.
I understand and agree to the following terms and conditions of my access to the information indicated above:

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
102
1. I hereby acknowledge that I have received a security indoctrination concerning the nature and protection of
information to which I have been provided conditional access, including the procedures to be followed in
ascertaining whether other persons to whom I contemplate disclosing this information have been approved for
access to it, and that I understand these procedures. I understand and agree to the following terms and conditions
of my access to the information indicated above:
2. By being granted conditional access to the information indicated above, the United States Government has
placed special confidence and trust in me and I am obligated to protect this information from unauthorized
disclosure, in accordance with the terms of this Agreement and the laws, regulations, and directives applicable to
the specific categories of information to which I am granted access.
3. I attest that I understand my responsibilities and that I am familiar with and will comply with the standards for
protecting such information that I may have access to in accordance with the terms of this Agreement and the
laws, regulations, and/or directives
applicable to the specific categories of information to which I am granted access. I understand that the United
States Government may conduct inspections, at any time or place, for the purpose of ensuring compliance with
the conditions for access, dissemination, handling and safeguarding information under this Agreement.
4. I will not disclose or release any information provided to me pursuant to this Agreement without proper
authority or authorization. Should situations arise that warrant the disclosure or release of such information I will
do so only under approved circumstances and in accordance with the laws, regulations, or directives applicable to
the specific categories of information. I will honor and comply with any and all dissemination restrictions cited or
verbally relayed to me by the proper authority.
5. (a) For PCII - (1) Upon the completion of my engagement as an employee, consultant, or subcontractor under
the contract, or the completion of my work on the PCII Program, whichever occurs first, I will surrender promptly
to the PCII Program Manager or his designee, or to the appropriate PCII officer, PCII of any type whatsoever that
is in my possession.
(2) If the Authorized Entity is a United States Government contractor performing services in support of the PCII
Program, I will not request, obtain, maintain, or use PCII unless the PCII Program Manager or Program
Manager’s designee has first made in writing, with respect to the contractor, the certification as provided for in
Section 29.8(c) of the implementing regulations to the CII Act, as amended.
(b) For SSI and SBU - I hereby agree that material which I have in my possession and containing information
covered by this Agreement, will be handled and safeguarded in a manner that affords sufficient protection to
prevent the unauthorized disclosure of or inadvertent access to such information, consistent with the laws,
regulations, or directives applicable to the specific categories of information. I agree that I shall return all
information to which I have had access or which is in my possession 1) upon demand by an authorized individual;
and/or 2) upon the conclusion of my duties, association, or support to DHS; and/or 3) upon the determination that
my official duties do not require further access to such information.
6. I hereby agree that I will not alter or remove markings, which indicate a category of information or require
specific handling instructions, from any material I may come in contact with, in the case of SSI or SBU, unless
such alteration or removal is consistent with the requirements set forth in the laws, regulations, or directives
applicable to the specific category of information or, in the case of PCII, unless such alteration or removal is
authorized by the PCII Program Manager or the PCII Program Manager’s designee. I agree that if I use
information from a sensitive document or other medium, I will carry forward any markings or other required
restrictions to derivative products, and will protect them in the same matter as the original.
7. I hereby agree that I shall promptly report to the appropriate official, in accordance with the guidance issued for
the applicable category of information, any loss, theft, misuse, misplacement, unauthorized disclosure, or other

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
103
security violation, I have knowledge of and whether or not I am personally involved. I also understand that my
anonymity will be kept to the extent possible when reporting security violations.
8. If I violate the terms and conditions of this Agreement, such violation may result in the cancellation of my
conditional access to the information covered by this Agreement. This may serve as a basis for denying me
conditional access to other types of information, to include classified national security information.
9. (a) With respect to SSI and SBU, I hereby assign to the United States Government all royalties, remunerations,
and emoluments that have resulted, will result, or may result from any disclosure, publication, or revelation of the
information not consistent with the terms of this Agreement.
(b) With respect to PCII I hereby assign to the entity owning the PCII and the United States Government, all
royalties, remunerations, and emoluments that have resulted, will result, or may result from any disclosure,
publication, or revelation of PCII not consistent with the terms of this Agreement.
10. This Agreement is made and intended for the benefit of the United States Government and may be enforced
by the United States Government or the Authorized Entity. By granting me conditional access to information in
this context, the United States Government and, with respect to PCII, the Authorized Entity, may seek any remedy
available to it to enforce this Agreement including, but not limited to, application for a court order prohibiting
disclosure of information in breach of this Agreement. I understand that if I violate the terms and conditions of
this Agreement, I could be subjected to administrative, disciplinary, civil, or criminal action, as appropriate, under
the laws, regulations, or directives applicable to the category of information involved and neither the United
States Government nor the Authorized Entity have waived any statutory or common law evidentiary privileges or
protections that they may assert in any administrative or court proceeding to protect any sensitive information to
which I have been given conditional access under the terms of this Agreement.
11. Unless and until I am released in writing by an authorized representative of the Department of Homeland
Security (if permissible for the particular category of information), I understand that all conditions and obligations
imposed upon me by this Agreement apply during the time that I am granted conditional access, and at all times
thereafter.
12. Each provision of this Agreement is severable. If a court should find any provision of this Agreement to be
unenforceable, all other provisions shall remain in full force and effect.
13. My execution of this Agreement shall not nullify or affect in any manner any other secrecy or non-disclosure
Agreement which I have executed or may execute with the United States Government or any of its departments or
agencies.
14. These restrictions are consistent with and do not supersede, conflict with, or otherwise alter the employee
obligations, rights, or liabilities created by Executive Order No. 12958, as amended; Section 7211 of Title 5,
United States Code (governing disclosures to Congress); Section 1034 of Title 10, United States Code, as
amended by the Military Whistleblower Protection Act (governing disclosure to Congress by members of the
military); Section 2302(b)(8) of Title 5, United States Code, as amended by the Whistleblower Protection Act
(governing disclosures of illegality, waste, fraud, abuse or public health or safety threats); the Intelligence
Identities Protection Act of 1982 (50 USC 421 et seq.) (governing disclosures that could expose confidential
Government agents); and the statutes which protect against disclosure that may compromise the national security,
including Sections 641, 793, 794, 798, and 952 of Title 18, United States Code, and Section 4(b) of the
Subversive Activities Act of 1950 (50 USC 783(b)). The definitions, requirements, obligations, rights, sanctions,
and liabilities created by said Executive Order and listed statutes are incorporated into this agreement and are
controlling.
15. Signing this Agreement does not bar disclosures to Congress or to an authorized official of an executive
agency or the Department of Justice that are essential to reporting a substantial violation of law.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
104
16. I represent and warrant that as an executive in my business/agency I have the authority to enter into this
Agreement. I further agree that all subordinates within my business/agency shall abide by the terms of this
Agreement.
17. I have read this Agreement carefully and my questions, if any, have been answered. I acknowledge that the
briefing officer has made available to me any laws, regulations, or directives referenced in this document so that I
may read them at this time, if I so choose.
DEPARTMENT OF HOMELAND SECURITY
NON-DISCLOSURE AGREEMENT Acknowledgement
Typed/Printed Name of Subcontractor:
Subcontractor Business Name and Address:
Telephone Number:
I make this Agreement in good faith, without mental reservation or purpose of evasion.
Signature of Subcontractor:
WITNESS:
Typed/Printed Name of AMR OEM Official
Business Address
American Medical Response Office of Emergency Management 12020 Intraplex Parkway Gulfport MS 39503-4602
Telephone Number:
(800) 230-1584
Signature of AMR OEM Official:
This form is not subject to the requirements of P.L. 104-13, “Paperwork Reduction Act of 1995” 44 USC, Chapter 35.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 105
Appendix 12 Equipment for Ground Ambulances in Federal EMS Response
Approved by FEMA and HHS – Revised January 28, 2015 American Medical Response (AMR) is under contract with the Federal government to provide EMS in response to Federally-declared events as approved by FEMA. For incidents in which Federal assistance is provided under the Stafford Act, FEMA coordinates the assistance. For non-Stafford Act incidents, Federal response or assistance may be led or coordinated by various Federal departments and agencies consistent with their authorities. Pursuant to the National Response Framework, the primary Federal agency responsible for coordinating mass care is DHS/FEMA. These key response core capabilities include: mass care services, public and private services and resources, public health and medical services and critical transportation34. Another Federal agency responsible for coordinating public health and medical services is the U.S. Department of Health and Human Services (HHS). These services include coordination of patient movement, patient care, providing pharmaceuticals to include the distribution and delivery of medical countermeasures, equipment and supplies35. The following list represents recommendations for the equipment and supplies that will facilitate patient care activities in the out-of-hospital setting during these events. Unless otherwise regulated by applicable state law, all ambulances that deploy in response to activation of the AMR/FEMA Federal EMS Contract shall be equipped in accordance with the Joint Policy Statement – Equipment for Ground Ambulances, published jointly by the National Association of EMS Physicians, the American Academy of Pediatrics, Emergency Medical Services for Children, Emergency Nurses Association, the American College of Emergency Physicians, and the American College of Surgeons Committee on Trauma36, with the modifications set forth herein. The equipment and supplies in this document pertain specifically to basic life support (BLS) and advanced life support (ALS) ground ambulances. For purposes of this document, the following standard age-based definitions have been used. Length-based systems have been developed to more accurately estimate the weight of children and predict appropriate equipment sizes, medications doses, and guidelines for fluid volume administration.
Neonate (0-28 days old)
Infant (29 days to 1 year old)
Child (> 1 year through 11 years old) o Toddlers (1-3 years old) o Preschoolers (3-5 years old) o Middle childhood (6-11 years old)
Adolescents (12-18 years old) The contractor may choose to establish caches of reserve ambulances to be used exclusively for Federal EMS deployments. They may not be used for routine non-Federal events. Since
34 National Response Framework, Emergency Support Function #6 – Mass Care, Emergency Assistance, Temporary Housing, and Human Services Annex. NFR Second Edition, May 2013. 35 National Response Framework, Emergency Support Function #8 – Public Health and Medical Services Annex. NFR Second Edition, May 2013. 36 Joint Policy Statement - Equipment for Ambulances. Prehospital Emergency Care; January/March 2014; Volume 18, Number 1. Official Journal of the National Association of EMS Physicians. ISSN 1090-3127.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
106
they are not used for routine patient transport, they need not be licensed or permitted by the State EMS Authority in the state(s) where they are stored, and are not subject to the ambulance equipment minimum standards of the state(s). These reserve ambulances, when used for Federal deployment, will be stocked with the minimum equipment established herein. These vehicles will be marked with special placards identifying them as Federal EMS Ambulances. They may be deployed within the state(s) where the disaster has occurred or in adjacent states if needed. Some ambulances responding to Federal events pursuant to the AMR/FEMA Contract may be from states that require additional equipment, which exceeds these minimum guidelines. Use of this additional equipment must be approved by medical control authorities having jurisdiction at the deployment site(s). Under no circumstances will EMS responders be allowed to use equipment and perform skills that exceed their formal training and certified scope of practice. For EMS deployments pursuant to the AMR/FEMA Federal EMS Contract, the National EMS Core Content37 defines the domain of out-of-hospital care. The scope of practice for the AMR/FEMA National EMS Contract shall be the National EMS Scope of Practice Model38, which divides the core content into levels of practice, defining the minimum corresponding skills and knowledge for each level. The National Model EMS Clinical Guidelines39 were approved by the National Association of State EMS Officials (NASEMSO) to provide a resource to prehospital clinical practice, maximize patient care, safety and outcomes. They are a set of clinical guidelines that can be used “as is” or adapted for use on a state or regional level to ensure a more standardized approach to the practice of patient care. In the absence of local, state, and regional EMS protocols the DHS-Wide EMS Basic Life Support (BLS) & Advanced Life Support (ALS) Protocols40 produced by the Department of Homeland Security’s (DHS) Office of Health Affairs (OHA) may be used if authorized by the AMR Office of Emergency Management (OEM) medical control authorities. Under remote, austere, or hostile conditions, local, state, and regional prehospital protocols and medical direction may be inaccessible or impractical, in these situations the DHS OHA Austere Emergency Medical Support (AEMS) Field Guide41 may be used if authorized by the AMR Office of Emergency Management (OEM) medical control authorities. The National EMS Scope of Practice Model defines and describes four certification or licensure levels of EMS provider: emergency medical responder (EMR), emergency medical technician (EMT), advanced EMT (AEMT), and paramedic. Each level represents a unique role, set of skills, and knowledge base. The National EMS Scope of Practice Model establishes a framework that ultimately determines the range of skills and roles that an individual possessing a state EMS license is authorized to do in a given EMS system. Individual state EMS rules or regulations that limit provider scope of practice may impact the need for availability of certain pieces of equipment. Except for controlled substances, the Contractor shall be responsible for stocking and/or re-supplying the ambulances such that all of the equipment and supplies listed in the Joint Statement (as modified) are on board during patient care and transport. The following list is divided into equipment for basic life support (BLS) and advanced life support (ALS) emergency ground ambulances. ALS ambulances must have all of the equipment on the
37 National EMS Core Content. National Highway Traffic Safety Administration. DOT HS 809 898. July 2005. 38 National EMS Scope of Practice Model. National Highway Traffic Safety Administration. DOT HS 810 657. February 2007. 39 National Model EMS Clinical Guidelines. National Association of State EMS Officials (NASEMSO). October 2014. 40 DHS-Wide EMS Basic Life Support (BLS) & Advanced Live Support (ALS) Protocols. U.S. Dept. of Homeland Security, Office of Health
Affairs. Created 12/2/2011, modified 9/9/2013. 41 Austere Emergency Medical Support (AEMS) Field Guide. U.S. Dept. of Homeland Security, Office of Health Affairs. Created 12/2/2011,
modified 4/24/2014.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
107
required BLS list as well as equipment on the required ALS list. This list represents a consensus of recommendations for equipment and supplies that will facilitate patient care in the out-of-hospital setting. BASIC LIFE SUPPORT (BLS) GROUND AMBULANCE REQUIRED EQUIPMENT
A. Ventilation and Airway Equipment
1. Portable and fixed suction apparatus with a regulator, per federal specifications
Wide-bore tubing, rigid pharyngeal curved suction tip; tonsil and flexible suction catheters, 6F–16F, are commercially available (have one between 6F and 10F and one between 12F and 16F)
2. Portable oxygen apparatus, capable of metered flow with adequate tubing 3. Portable and fixed oxygen supply equipment
Variable flowmeter 4. Oxygen administration equipment
Adequate-length tubing; transparent mask (adult and child sizes), both non-rebreathing and valveless; nasal cannulas (adult, child)
5. Bag-valve mask (manual resuscitator)
Hand-operated, self-expanding bag; adult (>1000 mL) and child (450–750 mL) sizes, with oxygen reservoir/accumulator, valve (clear, operable in cold weather), and mask (adult, child, infant, and neonate sizes)
6. Airways
Nasopharyngeal (16F–34F; adult and child sizes)
Oropharyngeal (sizes 0–5; adult, child, and infant sizes) 7. Pulse oximeter with pediatric and adult probes 8. Saline drops and bulb suction for infants
B. Monitoring and Defibrillation
BLS ground ambulances should be equipped with an automated external defibrillator (AED) unless staffed by advanced life support personnel who are carrying a monitor/defibrillator. The AED should have pediatric capabilities, including child-sized pads and cables OR dose attenuator with adult pads.42
C. Immobilization Devices
1. Cervical collars
Rigid for children ages 2 years or older, infant, child, and adult sizes (small, medium, large, and other available sizes) OR pediatric and adult adjustable cervical collars
2. Head immobilization device (not sandbags)
Firm padding or commercial device 3. Upper and lower extremity immobilization devices
Joint-above and joint-below fracture (adult and child sizes), rigid-support appropriate material (cardboard, metal, pneumatic, vacuum, wood, or plastic)
4. Impervious backboards (long, short, radiolucent preferred) and extrication device
42 AEDs were not required in original contract and not all states require them on BLS ambulances. BLS ambulances will be equipped with AEDs if their home-state EMS authority requires it or if the government provides them.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
108
Short extrication/immobilization device
Long transport (head-to-feet length) with at least 3 appropriate restraint straps (chin strap alone should not be used for head immobilization) and with padding for children and handholds for moving patients
D. Bandages/Hemorrhage Control
1. Commercially packaged or sterile burn sheets 2. Bandages
Triangular bandages 3. Dressings
Sterile dressings, including gauze sponges of suitable size
Abdominal dressing 4. Gauze rolls
Various sizes 5. Occlusive dressing or equivalent 6. Adhesive tape
Various sizes (including 1′′ and 2′′) hypoallergenic
Various sizes (including 1′′ and 2′′) adhesive 7. Arterial tourniquet (commercial preferred)
E. Communication
In disaster areas where the communications infrastructure is intact, the Contractor must provide two-way communications to enable ambulances to communicate with medical control and dispatch. Incident Management Team (IMT) leaders should also be able to communicate. FEMA will assist in providing communications devices that are considered government furnished equipment (GFE).
F. Protocols Each ambulance should contain a printed copy of clinical and operational protocols that are used in their home jurisdiction. The authorized medical director at the disaster site will determine what protocols are to be used. If the approved protocols used for the disaster contain procedures for which the healthcare provider has not been trained and certified, s/he shall not perform any procedures that exceed their licensed scope of practice. Additional “just-in-time” training may be provided to certify EMS responders to perform these procedures if approved by the medical director. Department of Homeland Security – Office of Health Affairs (DHS-OHA) BLS and ALS protocols may be used if approved by appropriate regulatory agencies.
G. Obstetrical
1. OB Kit (separate sterile kit)
Towels, 4” × 4” dressing, umbilical tape, sterile scissors or other cutting utensil, bulb suction, clamps for cord, sterile gloves, blanket
2. Thermal absorbent blanket and head cover, aluminum foil roll, or appropriate heat-reflective material (enough to cover newborn)

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
109
H. Miscellaneous
1. Access to pediatric and adult patient care protocols 2. A length-based resuscitation tape OR a reference material that provides appropriate
guidance for pediatric drug dosing and equipment sizing based on length OR age 3. Sphygmomanometer (pediatric and adult regular size and large cuffs) 4. Adult stethoscope 5. Thermometer with low-temperature capability 6. Heavy bandage or paramedic scissors for cutting clothing, belts, and boots 7. Cold packs 8. Sterile saline solution for irrigation 9. Two functional flashlights
10. Blankets 11. Sheets (at least one change per cot) 12. Pillows 13. Towels 14. Triage tags 15. Emesis bags or basins 16. Urinal 17. Wheeled cot 18. Stair chair or carry chair 19. Patient care charts/forms or electronic capability 20. Lubricating jelly (water soluble)
I. Infection Control
(When applicable, latex-free equipment should be available)
1. Eye protection (full peripheral glasses or goggles, face shield) 2. Face protection (e.g., surgical masks per applicable local or state guidance) 3. Gloves, nonsterile 4. Fluid-resistant overalls or gowns 5. Waterless hand cleanser, commercial antimicrobial (towelette, spray, or liquid) 6. Disinfectant solution for cleaning equipment 7. Standard sharps containers, fixed and portable 8. Biohazard trash bags (color coded or with biohazard emblem to distinguish from
other trash) 9. Respiratory protection (e.g., N95 or N100 mask—per applicable local or state
guidance)
J. Injury Prevention
1. Availability of necessary age/size-appropriate restraint systems for all passengers and patients transported in ground ambulances. For children, this should be according to the National Highway Traffic Administration's document: Safe Transport of Children in Emergency Ground Ambulances
2. Fire extinguisher 3. Department of Transportation Emergency Response Guide 4. Reflective safety wear for each crewmember (must meet American National
Standard for High Visibility Public Safety Vests if working within the right of way of any federal-aid highway. Visit www.reflectivevest.com/federalhighwayruling.html for more information)

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
110
K. Optional Medications for BLS Ground Ambulances
These medications may be used if authorized by applicable medical control authorities and only if BLS provider has been trained to administer them.
1. Albuterol 2. Epi-pen 3. Oral glucose 4. Nitroglycerine (sublingual tablet or paste) 5. Aspirin
L. Optional Equipment for BLS Ground Ambulances
The equipment in this section is not mandated or required. Use should be based on local needs and resources.
1. Glucometer or blood glucose test strips (per state protocol and/or local medical control approval)
2. Infant oxygen mask 3. Infant self-inflating resuscitation bag 4. Airways
a. Nasopharyngeal (12F, 14F) b. Oropharyngeal (size 00)
5. CPAP/BiPAP capability 6. Neonatal blood pressure cuff 7. Infant blood pressure cuff 8. Pediatric stethoscope 9. Infant cervical immobilization device
10. Pediatric backboard and extremity splints 11. Femur traction device (adult and child sizes) 12. Pelvic immobilization device 13. Elastic wraps 14. Ocular irrigation device 15. Hot packs 16. Warming blanket 17. Cooling device 18. Soft patient restraints 19. Folding stretcher 20. Bedpan 21. Topical hemostatic agent/bandage 22. Appropriate CBRNE PPE (chemical, biological, radiological, nuclear, explosive
personal protective equipment), including respiratory and body protection; protective helmet/ jackets or coats/pants/boots
23. Applicable chemical antidote auto-injectors (at a minimum for crew members’ protection; additional for victim treatment based on local or regional protocol; appropriate for adults and children)

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 111
ADVANCED LIFE SUPPORT (ALS) GROUND AMBULANCE REQUIRED EQUIPMENT For paramedic services, include all of the required equipment listed above, plus the following additional equipment and supplies. For advanced EMT services (and other non-paramedic advanced levels), include all of the equipment from the BLS list and selected equipment and supplies from the following list, based on scope of practice, local need, and consideration of out-of-hospital characteristics and budget.
A. Airway and Ventilation Equipment
1. Laryngoscope handle with extra batteries and bulbs 2. Laryngoscope blades, sizes:
a. 0–4, straight (Miller), and b. 2–4, curved
3. Endotracheal tubes (if ALS service scope of practice includes tracheal intubation), sizes:
a. 2.5, 3.0, 3.5, 4.0, 4.5, 5.0, and 5.5 mm cuffed and/or uncuffed, and b. 6.0, 6.5, 7.0, 7.5, and 8.0 mm cuffed (1 each), other sizes optional
4. 10-mL non-Luer Lock syringes 5. Stylettes for endotracheal tubes, adult and pediatric 6. Magill forceps, adult and pediatric 7. End-tidal CO2 detection capability (adult and pediatric) rescue airway device, such
as the ETDLA (esophageal–tracheal double-lumen airway), laryngeal tube, disposable supraglottic airway, or laryngeal mask airway (as approved by local medical direction)
B. Vascular Access
1. Isotonic crystalloid solutions, e.g. normal saline and Lactated Ringers 2. Antiseptic solution (alcohol wipes and povidone–iodine wipes preferred) 3. Intravenous fluid bag pole or roof hook 4. Intravenous catheters, 14G–24G 5. Intraosseous needles or devices appropriate for children and adults 6. Latex-free tourniquet 7. Syringes of various sizes 8. Needles, various sizes (including suitable sizes for intramuscular injections) 9. Intravenous administration sets (microdrip and macrodrip)
10. Intravenous arm boards, adult and pediatric
C. Cardiac
1. Portable, battery-operated cardiac monitor/defibrillator
With tape write-out/recorder, defibrillator pads, quick-look paddles or electrode, or hands-free patches, electrocardiogram leads, adult and pediatric chest attachment electrodes, adult and pediatric paddles
2. Transcutaneous cardiac pacemaker
Either stand-alone unit or integrated into monitor/defibrillator
D. Other Advanced Equipment

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
112
1. Nebulizer 2. Glucometer or blood glucose measuring device with reagent strips 3. Long large-bore needles or angiocatheters (should be at least 3.25” in length for
needle chest decompression in large adults)
E. Optional Equipment for ALS Ground Ambulances The equipment in this section is not mandated or required. Use should be based on local needs and resources.
1. Respirator, volume-cycled, on/off operation, 100% oxygen, 40–50 psi pressure (child/infant capabilities)
2. Blood sample tubes, adult and pediatric 3. Automatic blood pressure device 4. Nasogastric tubes, pediatric feeding tube sizes 5F and 8F, sump tube sizes 8F–16F 5. Size 1 curved laryngoscope blade 6. Gum elastic bougies 7. Needle cricothyrotomy capability and/or cricothyrotomy capability (surgical
cricothyrotomy can be performed in older children in whom the cricothyroid membrane is easily palpable, usually by puberty)
8. Rescue airway devices for children 9. Atomizers for administration of intranasal medications
F. Medications
Drug dosing in children should use processes minimizing the need for calculations, preferably a length-based system. In general, medications may include:
1. Cardiovascular medications, such as a. Epinephrine 1:10,000 b. Atropine c. Antidysrhythmics
i. Adenosine (Adenocard) ii. Amiodarone (Cordarone) iii. Calcium Gluconate iv. Lidocaine Hydrochloride
d. Calcium channel blockers, e.g. Diltiazem (Cardizem) or Verapamil (Isoptin) e. Beta-blockers, e.g. propranolol (Inderal), metoprolol (Lopressor) f. Nitroglycerin tablets or spray g. Aspirin h. Vasopressor for infusion, e.g. Dopamine Hydrochloride or Vasopressin
(Pitressin) i. Magnesium sulfate
2. Cardiopulmonary/respiratory medications, such as a. Albuterol (or other inhaled beta agonist) b. Epinephrine 1:1,000 c. Furosemide (Lasix)
3. 50% dextrose solution (and sterile diluent or 25% dextrose solution for pediatrics)

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
113
4. Analgesics, narcotic and nonnarcotic 43 (recommended, not required)
a. Morphine Sulfate Injection, 10 mg/ml, and b. Fentanyl Injectable (Sublimaze), 0.05 mg/ml
5. Anticonvulsant medication5 (recommended, not required)
a. Lorazepam (Antivan), 2 mg/ml, and b. Midazolam (Versed), 1 mg/ml
6. Sodium bicarbonate
7. Glucagon
8. Naloxone hydrochloride (Narcan)
9. Bacteriostatic water and sodium chloride for injection Paralytics and other pharmaceutical adjuncts shall NOT be supplied to facilitate endotracheal intubation.
43 Situations beyond control of the contractor may prohibit them from providing controlled substances or narcotics during Federal deployments in which case the U.S. Dept. of Health and Human Services will supply these medications. Documentation of administration of controlled substances and narcotics will be on forms approved by the HHS Technical Representative.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 114
Appendix 13 Non-Ambulance Medical Support by Fixed Site EMS Personnel
Introduction
Under the AMR/FEMA Federal EMS Contract, non-ambulance EMTs and Paramedics may be required to provide medical support to multi-modal transportation services, e.g., buses, trains or other transportation modes utilized to transport persons/evacuees. They may also be required to support fixed sites, e.g., shelters, clinics, airheads, triage centers or other fixed sites. These EMTs and Paramedics are classified as Non-Ambulance Medical Support Personnel or Fixed Site Personnel (FSP). This Concept of Operations (ConOps) document will focus primarily on shelter medical support.
Purpose
The purpose of this plan is to outline the responsibilities, expectations and possible scenarios for non-ambulance EMS personnel. It is applicable to all FSP regardless of certification level or location assignment.
Disclaimer
Disasters are unpredictable and dynamic; this document is a resource and best practices guide and shall not be interpreted as an all-encompassing, fail-safe document.
Fixed Site Personnel
Fixed Site Personnel shall be either EMTs or Paramedics with the required certification. They may be stationed at shelters, airheads, triage centers, or other fixed location sites. EMS personnel at fixed sites will be equipped with portable and disposable medical supplies and equipment comparable to that which is required on ambulances commensurate with their level of certification, i.e., EMT equipment—BLS ambulance, Paramedic equipment—ALS ambulance. This equipment will exclude ambulance equipment such as extrication equipment, patient transportation devices, traffic safety equipment, and other equipment or supplies that are commonly used on vehicles rather than fixed sites.
Multi-Modal Assignments
Bus, Train and Other Mobile Locations
As evacuees are relocated via bus, train and other mass transportation means, FSP may be needed to accompany the evacuees to monitor their health status and provide medical care while in transit.
Fixed Site Locations
Triage Center, Clinics and Other Fixed Sites
FSP may be requested to assist with any number of services at several types of fixed sites. Outside of airheads and shelters, which have slightly more intrusive responsibilities, FSP will be performing medical care, triage and patient packaging for transport. An advanced description of duties can be found in this document in the section ‘Roles and Responsibilities’.
Airheads
Air Evacuation Team Members - Hospital (AETM-H)
One of the components of the AMR/FEMA Federal EMS Contract is to provide air ambulance services. In these situations, EMS personnel may be deployed to sending health care facilities to identify patients who need to be evacuated. The AETM-H will perform patient assessments,

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
115
triage and coordinate ground and air ambulance evacuation. AETM-H may be AMR employees or EMS subcontractors or they may be part of the local EMS system. The primary goal of these personnel is to minimize delay or interruption in continuity of care from the time patients are removed from the sending facility until they reach the appropriate Aeromedical Marshalling Point (AMP) to be either placed into a waiting aircraft or delivered to an appropriately equipped/staffed Disaster Aeromedical Staging Facility (DASF) or Mobile Aeromedical Staging Facility (MASF). The approximate ratio of AETM-H to in-patients awaiting evacuation is usually one AETM-H to every five patients. These numbers may vary depending on the complexity of the situation, e.g., patient condition, hospital conditions, availability of other support staff, etc. AETM-H may be non-ambulance Fixed Site Personnel or they may be ambulance crewmembers.
Air Evacuation Team Members – Airport (AETM-A)
Air Evacuation Team Members – Airport (AETM-A) are ALS EMS personnel who are deployed to the airport patient embarkation points (AMP, APOE, MASF, DASF, CASF) to assist in loading and unloading patients and to ensure there is no delay or interruption in continuity of care from the time patients arrive at the embarkation point until they depart. AETM-As may be part of the AMR air medical support team or they may be part of the local EMS system. There are many variables that affect the number of AETM-A needed at the embarkation point. The usual ratio is two AETM-A per aircraft (2:1) for load/unload events. If aircraft load and unload one at a time, then only two AETM-A would be needed at each airport. When multiple aircraft are loading and unloading simultaneously, multiple AETM-A will be needed; one for each aircraft. AETM-A may be non-ambulance Fixed Site Personnel or they may be ambulance crewmembers. AETM-As may also be needed at debarkation points (receiving airports) to assist at the Patient Reception Area (PRA) and Aerial Points of Debarkation (APOD).
Shelter
Shelters are essential prior to, during and after a disaster and can be the most critical element in protecting the population in times of disaster. Shelters provide mass care for people who cannot safely remain in their homes due to an emergency, disaster or event. While the scope of FSP within shelters will be dynamic and robust, they are not responsible for establishing or managing shelters. Their role is to provide EMS care at established shelters. The standard of care for FSP deployed to shelters shall be as defined in “EMS Scope of Practice, Protocols, Reciprocity, and Medical Control and Direction for AMR/FEMA EMS Deployments”. AMR-OEM, FEMA and the U.S. Dept. of Health and Human Services (HHS) have approved these standards. As shelters are established, FSP may be deployed to provide medical assessments and treatment to the shelter occupants. It is not uncommon for FSP to be redistributed to other locations as shelters are closed or consolidated.
Shelters and Relief Services
Under the American with Disabilities Act (ADA), shelters must provide equal access, including “safety, food, services, comfort, information, a place to sleep until it is safe to return home, and the support and assistance of family, friends and neighbors”. In emergency situations, the responsibility to provide accessible services often falls on a third party (such as the American Red Cross), which operates the shelter for the local government agency. These third party agencies are required to ensure accessibility unless these actions “would result in a fundamental alteration in the nature of a service, program, or activity or that would cause undue financial and administrative burdens”.
The ADA Best Practices Tool Kit for State and Local Governments states, “From the moment people begin to arrive at a shelter, good communication between staff, volunteers and residents

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
116
is essential. Accessible communications are required, but the reality often differs from the requirement.”
In its report The Needs of People with Disabilities with Psychiatric Disabilities During and After Hurricanes Katrina and Rita, the National Council on Disabilities (NCD) was alarmed to find that “first responders and emergency managers such as shelter operators often violated the civil rights requirements of the Americans with Disabilities Act and Section 504 of the Rehabilitation Act. Some of the most common forms of discrimination included: People with disabilities were segregated from the general population in some shelters while other shelters simply refused to let them enter. People with psychiatric disabilities were denied access to housing and other services because of erroneous fears and stereotypes of people with psychiatric disabilities”.
In several of the interviews carried out for this report, respondents commented that emergency managers often set up “special medical needs” shelters at which people with disabilities are to be housed during an emergency. Most people with disabilities do not have “special medical needs” and prefer to go to a general population shelter so they can be with their family and peers. In addition, the ADA Best Practices Tool Kit points out that while some communities may open shelters specifically for people with disabilities (e.g., a local school for the deaf opening a shelter for people who are deaf or hard of hearing), people with disabilities are not required to take shelter in such locations. In short, the ADA requires that general population shelters be fully accessible and ensure accessible communications. This is also a preparedness issue, in that the public should be aware in advance of what the options are going to be and should have the right to say how and where they want to shelter.
General Population Shelter
General Population Shelters are safe, temporary facilities where evacuees may be housed before, during or immediately after a disaster or until it is safe to return home or relocated to other housing facilities of a more permanent nature. General Population Shelters should accept people with minor injuries or illnesses, or those with physical or emotional limitations, who do not require close monitoring, assistance, or equipment. Generally, these shelters serve people who:
are independent in the pre-shelter phase
are capable of performing activities of daily living
are self-ambulating or with walker
are wheelchair dependent; has own caretaker if needed
are medically stable requiring minimal monitoring (e.g., blood pressure monitoring)
are oxygen dependent and has their own supplies
have medical conditions controlled by self-administered medications
are able to manage for 72 hours without treatment or replacement of medications, supplies, or special equipment.
Children and adults with mild to moderate disabilities may also occupy General Population Shelters if they are provided Functional Needs Support Services (see below). In worst-case scenarios, individuals who would qualify for Medical Needs Shelters may have little choice but to evacuate to the nearest available General Population Shelter. This decision is usually made only when there is no other option available, and when there is an immediate peril to life and safety of clients if they are not immediately moved to the closest available shelter. Local evacuation plans should recognize this as a temporary condition requiring immediate triage activities and arrange to move the patients as soon as possible to an appropriate Medical Needs Shelter or other healthcare facility.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
117
Functional Needs Support Services (FNSS)
FNSS are defined as services that enable individuals to maintain their independence in a General Population Shelter. FNSS includes:
Reasonable modification to policies, practices, and procedures
Durable medical equipment (DME)
Consumable medical supplies (CMS)
Other goods and services as needed
Personal assistance services (PAS). These are formal and informal services provided by paid personnel, personal attendants, friends, family members, and volunteers that enable children and adults to maintain their usual level of independence in General Population Shelters. These services (when necessary) may include, but are not limited to, assisting with:
o Basic personal care: Grooming Eating Bathing Toileting Dressing and undressing Walking Transferring Maintaining health and safety
o Activities of daily living: Taking medications Shopping for groceries Communicating Accessing programs and services
Historically, PAS for individuals with disabilities have not been provided in General Population Shelters. During disasters, people with and without disabilities who have access and functional needs have been re-directed to “special needs” or medical shelters. In some instances, the only shelters that would admit people with disabilities have been remotely located and have caused children and adults to be separated from their families, friends, or personal attendants. Emergency managers and planners have been encouraged to develop sheltering plans that provide PAS in General Population Shelters.
Individuals requiring FNSS may have physical, sensory, mental health, and cognitive and/or intellectual disabilities affecting their ability to function independently without assistance. They may need limited special assistance or some surveillance due to pre-existing health problems. People in this support level include, but are not limited to:
Asthmatics
Colostomy patients
Diabetics on insulin (self-administered)
Dialysis patients requiring one or two dialysis visits weekly
Heart patients with mechanical devices
Hemophiliacs
People in a non-walking cast
People on special diets
People with artificial limbs
People with epilepsy
People with HIV/AIDS asymptomatic to mildly symptomatic
People with mild to moderate muscular diseases

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
118
People with significant speech impediments
People with urinary catheters
Visually or hearing impaired people
Wheelchair-mobile individuals
Women in the late stages of pregnancy
Elders
People needing bariatric equipment Medical Needs Shelter
Medical Needs Shelters offer more specialized care by trained professionals to individuals that need assistance with medical care or personal care during evacuations and sheltering due to physical or mental impairments. If the level of care required is beyond the basic first aid offered in General Population Shelters, these individuals would be referred to a Medical Needs Shelter (unless an accompanying caregiver can provide the needed support in the General Population Shelter). The primary difference in requirements between General Population Shelters and Medical Needs Shelters is the need for space for sleeping, medical equipment, medical supplies, and medical treatment areas. Individuals appropriate for sheltering within this type of shelter are:
Bed-confined people
Comatose patients
Dialysis patients requiring more than 3 dialysis visits weekly
Paralyzed people
People in the end stage of Alzheimer's
People with advanced senile dementia
People with chronic incontinence
People with unstable Grand Mal seizure
People requiring a catheter
People requiring complex dressings and continual changes
People requiring intravenous feeding or medications
Recently discharged surgical patients (except outpatient surgery)
Severe respiratory cases (oxygen or ventilator dependent)
Severely mentally disturbed people (potentially violent)
Severely retarded people
Unstable cardiac patients
Unstable insulin dependent people EMS Staff-to-Patient Ratios in Shelters
The EMS staff-to-patient (medically fragile evacuee) ratios are recommended only as general guidance for planning purposes and should not be construed as mandatory. The acuity of the population or other factors may justify an increase or decrease in the type and number of EMS staff present. Note – EMS staff are assigned to shelters to provide approved healthcare duties only based on their level of clinical certification. They are not intended to serve as shelter managers or provide other non-EMS duties.
Suggested EMS Staff-to-Patient Ratios
General Population Shelters 1 EMT and 1 Paramedic for every 30 shelter occupants
Medical Needs Shelters 1 EMT and 1 Paramedic for every 15 shelter occupants
Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
119
EMS shelter services must be provided 24/7 therefore adequate numbers of personnel should be provided to allow for 12 hour shift rotations.
Shelter Assumptions and Limitations
During disasters, shelters will have limited communication capabilities; e.g. landline, cellular service, internet, etc.
Pre-existing conditions of patients are exacerbated during times of disaster. FSP should be aware of the potential for shelter occupants to decompensate or decline in health.
Previously healthy individuals may have new medical or mental health needs due to the disaster.
Shelters will be cramped and over-crowded.
Medically fragile individuals will arrive at General Population Shelters.
Logistics may not be established when FSP arrive at shelters.
As the mass care lead agency, the American Red Cross or other designated agency will be charged with performing essential shelter duties, e.g. registration, feeding, supplies distribution, etc.
Due to staffing shortages, FSP may find themselves as the primary caregivers in medical needs shelters
The safety of performing some of the required medical procedures may be jeopardized in uncontrolled or austere situations. It is critical that FSP only provide medical care and treatment within their scope of practice and conduct their duties in a safe manner consistent with established protocols.
Shelter Equipment and Supplies
The AMR/FEMA Contract provides for medical equipment and supplies for shelters supported by AMR EMS personnel. These shelter packages are divided into BLS and ALS packages. BLS shelter packages are used at General Population Shelters and ALS shelter packages are used at Medical Shelters. The quantities of items in these shelter packages are based on the number of shelter occupants. The shelter packages are composed of base packages and supplemental packages. The base packages contain more equipment and supplies because they constitute the core shelter package. The supplemental packages are designed to replenish disposable items that may become depleted in the base package as more shelter occupants arrive.
Shelter Packages
General Population Shelter Base Pkg 1 pkg serves 25 patients
General Population Shelter Supplemental Pkg 5 pkgs @ 25 patients per pkg = 125 patients total
Medical Shelter Base Pkg 1 pkg serves 25 patients
Medical Shelter Supplemental Pkg 3 pkgs @ 25 patients per pkg = 75 patients total
FSP should periodically review inventory to maintain adequate supply levels and communicate any supply needs to FOB immediately.
Organizational Structure
AMR Command Structure
To the extent possible, the organizational structure and operation should conform to the principles and practices of the Incident Command System (ICS). FSP, once processed through check-in, will be dispersed in groups to general population and medical needs shelters. Safety and risk, logistical needs and operational questions are directed to the EMT/Paramedic Fixed Site Personnel Director at the Forward Operating Base. The EMT/Paramedic Fixed Site

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
120
Personnel Director is your direct report and should be contacted once per operational period for updates, instructions and general information. If the EMT/Paramedic Fixed Site Personnel Director is not filled, FSPs will report to the FOB Operations Section Chief.
*Note* The Air Evacuation Team Members may report to the Air Ambulance Group Leader instead of the EMT/Paramedic Fixed Site Personnel Director. Command Structure will be communicated upon check-in.
Shelter Command Structure
Once established at the shelter, FSP will be incorporated into a separate reporting structure. The Shelter Unit Leader will organize and operate the shelter in accordance with ICS principles and practices. Generally, FSP will report to the Medical Operations Manager. If this position is not filled, the Shelter Unit Leader or his deputy will provide guidance on the command structure.
Roles and Responsibilities
Fixed Site Personnel are expected to provide care with dignity and respect, in a non-judgmental, confidential and non-discriminatory manner. FSP may be responsible for some or all of the following duties; as long as they fall within the parameters of their license or certification or skills and abilities:
Assist with medical screening
Provide basic primary care and first aid services
Assist with medication storage and administration

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
121
Assisting individuals with mobility impairments in ambulating, toileting, transfers and personal hygiene
Maintain universal precautions and infection control
Serve as technicians in infirmaries
Staff health stations
Evaluate for communicable disease
Determine when ill or injured must be transferred to a higher level of care
Readying patients for transport to higher level of care
Verify condition of shelter residents on an ongoing basis
Medical Needs Shelter – provide acute care, administer medications and troubleshoot problems with medical equipment and oxygen delivery
Movement of deceased residents to a specified area of the shelter
Keep detailed records and status reports
Participate in after action review (AAR) Basic medical supplies for first aid and primary care will be transported to the shelters by AMR logistics. FSP staffing other fixed or mobile locations will be equipped with an ALS or BLS kit depending on their certification. The complete equipment lists can be found in the appendix.
Placarding
Placard numbers are designed for the purpose of identifying and tracking a fixed site asset. Placard numbers are unique and issued sequentially, without repetition of numerical digits. Each fixed site resource will have only one unique FEMA Placard Number assigned for the duration of an event. These Placard Numbers are not to be exchanged or otherwise altered by any entity unless authorized by the Fixed Site Director located at NATCOM.
Placards will be emailed to the company head and distributed to FSP. If it is not possible to print placards, agencies should not delay response. Placards will be available at the check-in site. Once a FSP is assigned a placard number, they will keep that number for the duration of the deployment regardless of change of assignment. If, due to extenuating circumstances, a placard number needs to be changed, it must be authorized and performed through NATCOM dispatch or the discipline manager.
To properly identify and distinguish between resource types, placards were created with monikers specific to the resource and certification level. It is imperative that the certification level displayed on the placard matches the training of the FSP.
1 0 1 1 F E This is a sequential, four-digit identification number assigned to FSP according to their relationship with AMR. The numbers begin at 0001 and progress through 9999.
0001 – 4999 for AMR employees
5000 – 9999 for network providers
This letter designates a FSP.
This letter indicates the type of resource (see chart below).
In this example, this four-digit number is designated as an AMR resource.
In this example, this is an FSP.
In this example, this is an EMT.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
122
PROVIDER
A = AMR vehicle
N = Network provider vehicle
F = Fixed Site Resource
RESOURCE TYPES
A = ALS Ground Ambulance
B = BLS Ground Ambulance
C = ALS Bariatric Ground Ambulance
D = ALS Med-Evac Bus (4 or more ALS patient stretcher positions)
G = Paratransit Type 1: Minivan - 3-10 regular seats
H = Paratransit Type 2b: Minibus/Midibus/Shuttle bus – 14-35 regular seats
J = Paratransit Type 3: Coach/transit bus – 44-75 regular seats
K = Paratransit Type 4b: ADA Full size passenger van – 1-2 wheelchairs, 2-15 regular seats
L = Paratransit Type 5: ADA Minibus/Midibus/Shuttle bus – 1-3 wheelchairs, 8-30 regular seats
M = Paratransit Type 6: ADA Coach/transit bus – 1-3 wheelchairs, 35-70 regular seats
N = Paratransit Type 2a: Full size passenger van – 8-15 regular seats
P = Paratransit Type 4a: ADA Minivan – 1 wheelchair, 1-5 regular seats
F = Air Ambulance Fixed Wing
R = Air Ambulance Rotor Wing
E = EMT
I = Paramedic
X = Support Vehicle
Mobilization
Once departed home base enroute to check-in, each FSP must call NATCOM dispatch at 866-219-9253 to be entered into the NATCOM CAD. When speaking with dispatch, you will give them your placard number, name, departing location, method of transportation (flying or driving) and ETA to check-in. If you have yet to be appointed a placard number, NATCOM dispatch will assign one for you during this initial call.
For FSP driving to check-in or other designated location, periodic progress updates including current location and ETA to destination should be called into NATCOM dispatch every 2 hours. FSP flying to check-in or other designated location, will contact NATCOM dispatch at all important intervals, such as arriving at airport, boarding the plane, debarking the plane and enroute to check-in. If problems are encountered while enroute, contact NATCOM dispatch.
Demobilization
Shelters are temporary accommodations that are operated only as long as is necessary to relocate residents to facilities that are more appropriate. As shelters are closed or consolidated, FSP will be relocated or relieved of duty. FSP are to remain in place until demobilization orders are given by the Forward Operating Base (FOB) or NATCOM. Demobilization or out-processing will most likely take place at the FOB. For the rare instances when demobilization happens remotely, the FSP will be contacted by phone and issued demobilization orders and instructions. All equipment and paperwork will remain at the shelter for FOB logistics to handle. Transportation will be arranged by FOB.
Once enroute to home base, NATCOM dispatch should be notified at every important interval (arrived at airport, boarding plane, debarking plane, arrived home base). If driving, NATCOM dispatch will contact you every 3 hours. If you do not hear from a NATCOM dispatcher after

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
123
three hours, please call into NATCOM dispatch at 866-219-9253 to check-in. If you have ANY problem, call NATCOM dispatch.
Prior to departure, ensure supplies are packed adequately for relocation. Determine the proper channel for submitting paperwork and attend any after action review or debriefing. Counseling and stress debriefing is available for any FSP who needs it. Contact your EMT/Paramedic Fixed Site Personnel Director to request Critical Incident Stress Debriefing (CISD).
Documentation
Accurate documentation aids in the tracking of resources, provides information on the type of services delivered and creates a record that can be used to validate services rendered and improve future responses. FSP will be responsible for completing an Activity Log (form ICS-214) and an Aggregate Morbidity form for each operation period. The completed forms will be submitted to leadership as instructed.
A Healthcare Record must be completed anytime that a caregiver-patient relationship is established; this includes patients that refuse medical care and those who are ultimately transported for higher care. When assisting residents with self-administered medication, the FSP will complete an entry on the resident’s Medication Administration form. AMR documentation must be completed in addition to any forms required by the host organization. AMR documents are proprietary and may be subject to HIPPA privacy rules, especially if they contain personally identifiable information (PII).
Public Affairs
FSP are prohibited from discussing shelter operations, deployment specifics and all other disaster related information with the media. Government regulations dictate that all aspects of a deployment remain strictly confidential. No information is to be released without the expressed consent of the OEM. FSP will be required to sign a Department of Homeland Security Non-Disclosure Agreement during the check-in process. Requests for information from the media or other sources shall be forward to OEM Federal Liaison Officer.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
124
Sources:
Porter, W. (2011). Shelters and Mass Care. In Preplanning for EMS (pp. 103-128). Sudbury, MA: Jones
and Bartlett.
IAVM and American Red Cross (2010). Mega-Shelter Planning Guide. Coppell, TX.
The City of Pleasanton: Comprehensive Emergency Management Plan: Shelter and Mass Care. (2005)
http://www.cityofpleasantonca.gov/pdf/annex-c.pdf
Sacramento Office of Emergency Services: Mass Care and Shelter Plan. (2012)
http://www.sacramentoready.org/Documents/Mass%20Care%20and%20Shelter%20Plan%20Final%2011-5-12.pdf
Triangle J: Area Agency on Aging: In-Depth Information on Special Needs Shelters.
http://www.tjaaa.org/in-depth-information-on-special-needs-shelters.aspx
Medical Reserve Corps: Guide to Medical Special Needs Shelters.
https://www.medicalreservecorps.gov/File/Promising_Practices_Toolkit/Guidance_Documents/Emergency_Preparedness_Response/MRC-SpecialNeedsShelterGuide.pdf
FEMA: Guidance on Planning for Integration of Functional Needs Support Services in General Population
Shelters. November 2010. http://www.fema.gov/pdf/about/odic/fnss_guidance.pdf

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 125
Appendix Table
A – Equipment
A-1 Shelter Package Equipment List
A-2 ALS/BLS Kit Equipment List
B- Documentation
B-1 Fixed Site Deployment Process – Quick Reference Guide
B-2 ICS 214 Fixed Site & Multi-Modal Support
B-3 Healthcare Record
B-4 Medication Administration Log
B-5 Aggregate Morbidity Form
B-6 Contact & Emergency Numbers
B-7 Fixed Site Contact Information
B-8 Go or No Go for Flight, A Reference
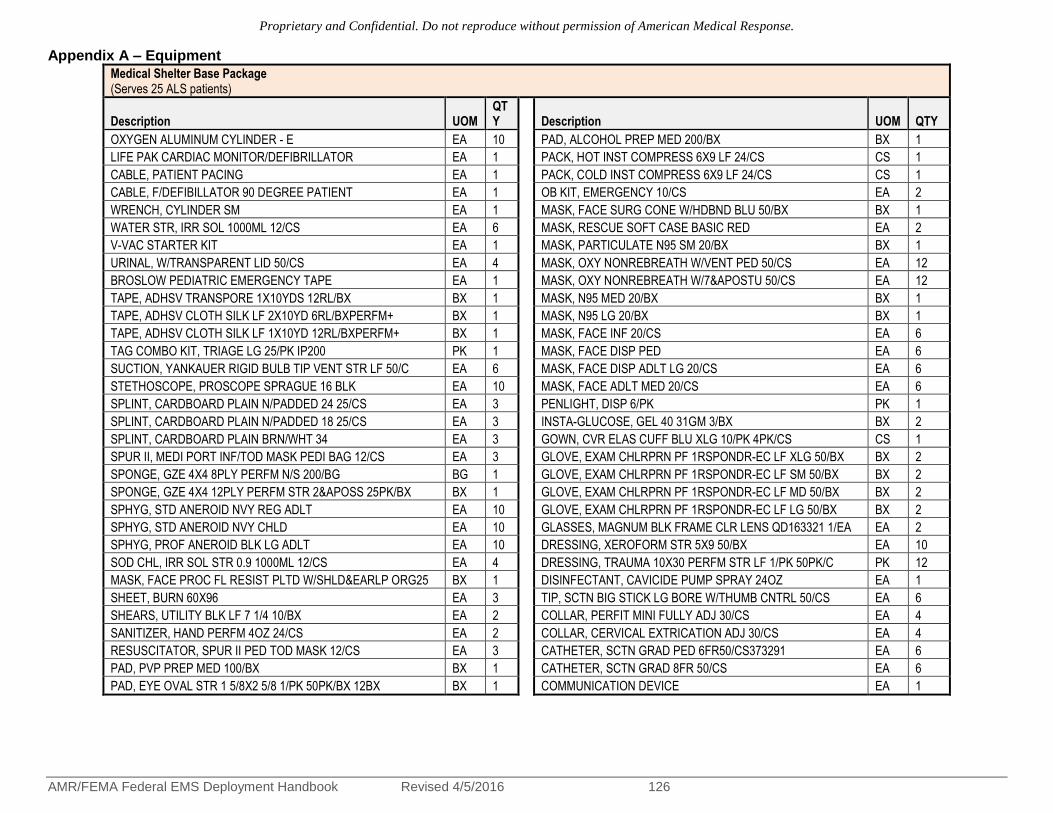
Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 126
Appendix A – Equipment
Medical Shelter Base Package (Serves 25 ALS patients)
Description UOM QTY
Description UOM QTY
OXYGEN ALUMINUM CYLINDER - E EA 10 PAD, ALCOHOL PREP MED 200/BX BX 1
LIFE PAK CARDIAC MONITOR/DEFIBRILLATOR EA 1 PACK, HOT INST COMPRESS 6X9 LF 24/CS CS 1
CABLE, PATIENT PACING EA 1 PACK, COLD INST COMPRESS 6X9 LF 24/CS CS 1
CABLE, F/DEFIBILLATOR 90 DEGREE PATIENT EA 1 OB KIT, EMERGENCY 10/CS EA 2
WRENCH, CYLINDER SM EA 1 MASK, FACE SURG CONE W/HDBND BLU 50/BX BX 1
WATER STR, IRR SOL 1000ML 12/CS EA 6 MASK, RESCUE SOFT CASE BASIC RED EA 2
V-VAC STARTER KIT EA 1 MASK, PARTICULATE N95 SM 20/BX BX 1
URINAL, W/TRANSPARENT LID 50/CS EA 4 MASK, OXY NONREBREATH W/VENT PED 50/CS EA 12
BROSLOW PEDIATRIC EMERGENCY TAPE EA 1 MASK, OXY NONREBREATH W/7&APOSTU 50/CS EA 12
TAPE, ADHSV TRANSPORE 1X10YDS 12RL/BX BX 1 MASK, N95 MED 20/BX BX 1
TAPE, ADHSV CLOTH SILK LF 2X10YD 6RL/BXPERFM+ BX 1 MASK, N95 LG 20/BX BX 1
TAPE, ADHSV CLOTH SILK LF 1X10YD 12RL/BXPERFM+ BX 1 MASK, FACE INF 20/CS EA 6
TAG COMBO KIT, TRIAGE LG 25/PK IP200 PK 1 MASK, FACE DISP PED EA 6
SUCTION, YANKAUER RIGID BULB TIP VENT STR LF 50/C EA 6 MASK, FACE DISP ADLT LG 20/CS EA 6
STETHOSCOPE, PROSCOPE SPRAGUE 16 BLK EA 10 MASK, FACE ADLT MED 20/CS EA 6
SPLINT, CARDBOARD PLAIN N/PADDED 24 25/CS EA 3 PENLIGHT, DISP 6/PK PK 1
SPLINT, CARDBOARD PLAIN N/PADDED 18 25/CS EA 3 INSTA-GLUCOSE, GEL 40 31GM 3/BX BX 2
SPLINT, CARDBOARD PLAIN BRN/WHT 34 EA 3 GOWN, CVR ELAS CUFF BLU XLG 10/PK 4PK/CS CS 1
SPUR II, MEDI PORT INF/TOD MASK PEDI BAG 12/CS EA 3 GLOVE, EXAM CHLRPRN PF 1RSPONDR-EC LF XLG 50/BX BX 2
SPONGE, GZE 4X4 8PLY PERFM N/S 200/BG BG 1 GLOVE, EXAM CHLRPRN PF 1RSPONDR-EC LF SM 50/BX BX 2
SPONGE, GZE 4X4 12PLY PERFM STR 2&APOSS 25PK/BX BX 1 GLOVE, EXAM CHLRPRN PF 1RSPONDR-EC LF MD 50/BX BX 2
SPHYG, STD ANEROID NVY REG ADLT EA 10 GLOVE, EXAM CHLRPRN PF 1RSPONDR-EC LF LG 50/BX BX 2
SPHYG, STD ANEROID NVY CHLD EA 10 GLASSES, MAGNUM BLK FRAME CLR LENS QD163321 1/EA EA 2
SPHYG, PROF ANEROID BLK LG ADLT EA 10 DRESSING, XEROFORM STR 5X9 50/BX EA 10
SOD CHL, IRR SOL STR 0.9 1000ML 12/CS EA 4 DRESSING, TRAUMA 10X30 PERFM STR LF 1/PK 50PK/C PK 12
MASK, FACE PROC FL RESIST PLTD W/SHLD&EARLP ORG25 BX 1 DISINFECTANT, CAVICIDE PUMP SPRAY 24OZ EA 1
SHEET, BURN 60X96 EA 3 TIP, SCTN BIG STICK LG BORE W/THUMB CNTRL 50/CS EA 6
SHEARS, UTILITY BLK LF 7 1/4 10/BX EA 2 COLLAR, PERFIT MINI FULLY ADJ 30/CS EA 4
SANITIZER, HAND PERFM 4OZ 24/CS EA 2 COLLAR, CERVICAL EXTRICATION ADJ 30/CS EA 4
RESUSCITATOR, SPUR II PED TOD MASK 12/CS EA 3 CATHETER, SCTN GRAD PED 6FR50/CS373291 EA 6
PAD, PVP PREP MED 100/BX BX 1 CATHETER, SCTN GRAD 8FR 50/CS EA 6
PAD, EYE OVAL STR 1 5/8X2 5/8 1/PK 50PK/BX 12BX BX 1 COMMUNICATION DEVICE EA 1

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 127
Medical Shelter Supplemental Package (Serves 25 ALS patients)
Description UOM QTY Description UOM QTY
OXYGEN ALUMINUM CYLINDER - E EA 2 ABD PAD, 5X9 STR LF PERFM+ 1/PK 20PK/BX BX 1
WATER STR, IRR SOL 1000ML 12/CS EA 3 WATER STR, IRR SOL 1000ML 12/CS EA 3
TAPE, ADHSV TRANSPORE 1X10YDS 12RL/BX BX 1 TUBE, ENDOTRACH UNCUFF 5.0MM 10/BX EA 1
TAPE, ADHSV CLOTH SILK LF 2X10YD 6RL/BXPERFM+ BX 1 TUBE, ENDOTRACH UNCUFF 4.0MM 10/BX EA 1
TAPE, ADHSV CLOTH SILK LF 1X10YD 12RL/BXPERFM+ BX 1 TUBE, ENDOTRACH UNCUFF 3.0MM 10/BX EA 1
SYRINGE, EAR BULB STR 2OZ 50/CS EA 2 TUBE, ENDOTRACH UNCUFF 2.5MM 10/BX EA 1
SUCTION, YANKAUER RIGID BULB TIP VENT STR LF 50/C EA 3 TUBE, ENDOTRACH CUFF 8.0MM 10/BX EA 1
SPUR II, MEDI PORT INF/TOD MASK PEDI BAG 12/CS EA 1 TUBE, ENDOTRACH CUFF 7.5MM 10/BX EA 1
SPONGE, GZE 4X4 8PLY PERFM N/S 200/BG BG 1 TUBE, ENDOTRACH CUFF 7.0MM 10/BX EA 1
SPONGE, GZE 4X4 12PLY PERFM STR 2&APOSS 25PK/BX BX 1 TUBE, ENDOTRACH CUFF 6.5MM 10/BX EA 1
SOD CHL, IRR SOL STR 0.9 1000ML 12/CS EA 2 TUBE, ENDOTRACH CUFF 6.0MM 10/BX EA 1
MASK, FACE PROC FL RESIST PLTD W/SHLD&EARLP ORG25 BX 1 TUBE, CHECK B 20/CS EA 2
SHEARS, UTILITY BLK LF 7 1/4 10/BX EA 1 SYRINGE, TB W/O NDL 1CC 100/BX 10BX/CS BX 1
SANITIZER, HAND PERFM 4OZ 24/CS EA 2 SYRINGE, LL 60CC 25/BX 4BX/CS BX 1
RESUSCITATOR, SPUR II PED TOD MASK 12/CS EA 2 SYRINGE, LL 5CC 100/BX 6BX/CS BX 1
PAD, PVP PREP MED 100/BX BX 1 SYRINGE, LL 3CC 100/BX 10BX/CS BX 1
PAD, ALCOHOL PREP MED 200/BX BX 1 SYRINGE, LL 30CC 25/BX 8BX/CS BX 1
PACK, HOT INST COMPRESS 6X9 LF 24/CS CS 2 SYRINGE, LL 10CC 100/BX 6BX/CS BX 1
PACK, COLD INST COMPRESS 6X9 LF 24/CS CS 2 SODIUM CHLORIDE, FTV PF 0.9 10ML 25/PK EA 3
OB KIT, EMERGENCY 10/CS EA 1 SODIUM BICARB, SYR 1MEQ/ML 8.4 50ML 25/CT EA 3
MASK, FACE SURG CONE W/HDBND BLU 50/BX BX 1 SOD CHL, IVSOL 0.9 1000ML 14/CS EA 5
MASK, RESCUE SOFT CASE BASIC RED EA 2 RAZOR, DISP SHAVE PREP DBL EDGE LF 24/BX 6BX/CS BX 1
MASK, PARTICULATE N95 SM 20/BX BX 1 PAPER, EKG LP11 & LP12 3RL/PK 6PK/CS PK 1
MASK, OXY NONREBREATH W/VENT PED 50/CS EA 6 NITROLINGUAL, SPR 0.4MG/DOSE 4.9GM 1/EA EA 1
MASK, OXY NONREBREATH W/7&APOSTU 50/CS EA 6 NEEDLE, SAFETYGLIDE IM 25GX5/8 50/BX BX 1
MASK, N95 MED 20/BX BX 1 NEEDLE, SAFETYGLIDE IM 23GX1 50/BX BX 1
MASK, N95 LG 20/BX BX 1 NEEDLE, FILTER 19GX1 1/2 TW 100/BX 5 BX 1
MASK, FACE INF 20/CS EA 2 NEEDLE, BIOPSY ILLINOIS STR 16GX3/16-1 7/8 10/CT EA 1
MASK, FACE DISP PED EA 2 NEBULIZER, MICRO-MIST SM VOL W/RESVR 50/CS EA 1
MASK, FACE DISP ADLT LG 20/CS EA 2 NALOXONE, SYR PF 2MG 2ML 10/CT EA 3
MASK, FACE ADLT MED 20/CS EA 2 LUBRICATING JELLY, 3GM FOIL PKT STR 144/BX 12 BX 1
INSTA-GLUCOSE, GEL 40 31GM 3/BX BX 1 LAMP, LARYG FROSTED LG 25/BX EA 1
GLOVE, EXAM CHLRPRN PF 1RSPONDR-EC LF XLG 50/BX BX 1 LAMP, LARNYG FROSTED SM 25/BX EA 1
GLOVE, EXAM CHLRPRN PF 1RSPONDR-EC LF SM 50/BX BX 1 IV ADMIN SET, SELECT III + NIS W/O NDL 48/CS EA 2
GLOVE, EXAM CHLRPRN PF 1RSPONDR-EC LF MD 50/BX BX 1 IPRATROPIUM BROMIDE, SOL INH 0.02MG/ML 2.5ML 25/C CT 1
GLOVE, EXAM CHLRPRN PF 1RSPONDR-EC LF LG 50/BX BX 1 INTRODUCER, FLEX GUIDE ENDOTRACHEAL EA 1

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
128
Description UOM QTY Description UOM QTY
DRESSING, XEROFORM STR 5X9 50/BX EA 5 INJECTION SITE, INTLNK 200/CS EA 4
DRESSING, TRAUMA 10X30 PERFM STR LF 1/PK 50PK/C PK 6 HOLDER, THOMAS TUBE ENDOTRACH PED 25/BX EA 1
DISINFECTANT, CAVICIDE PUMP SPRAY 24OZ EA 1 HOLDER, THOMAS TUBE ENDOTRACH ADLT 100/CS EA 1
TIP, SCTN BIG STICK LG BORE W/THUMB CNTRL 50/CS EA 2 GLUCAGEN DIAG KIT, VL 1MG EA 1
CATHETER, SCTN GRAD PED 6FR50/CS373291 EA 3 FUROSEMIDE, SYR 10MG/ML 4ML 10/PK EA 2
CATHETER, SCTN GRAD 8FR 50/CS EA 3 EXT SET, CATH W/SITE 6 50/BX EA 1
CATHETER, SCTN GRAD 18FR 50/CS EA 3 EPINEPHRINE, SYR 0.1MG/ML 10ML 25/CT EA 6
CATHETER, SCTN GRAD 10FR 50/CS EA 3 EPINEPHRINE, MDV 1MG/ML 30ML EA 1
CANNULA, NASAL CRVD TIP W/7&APOS TU 50/CS EA 10 EPINEPHRINE, AMP 1MG/ML 1ML 25/PK EA 3
CANISTER, SCTN 1200CC 48/CS EA 2 ELECTRODE, QUICK COMBO PED 1PR/PK 3010107-001 PK 1
BITE STICK, 10/PK EA 1 ELECTRODE, MEDITRACE MINI ECG FOAM 30/PK 20PK/CS PK 1
BEDPAN, FRACTURE MVE 50/CS EA 2 ELECTRODE, MEDITRACE QUICK COMBO ADLT 2/PK 10PK/C EA 1
BASIN, EMESIS 9 GLD 250/CS EA 4 ELECTRODE, EKG PED 3/PK 25PK/BX 4BX/CS BX 1
BANDAGE, TRIANGULAR LF 40X40X56 12/BX 6BX/CS BX 1 EASYCAP, CO2 DETECTOR 6/CS EA 2
BANDAGE, CNFRM STRCH 4 STR LF PERFM 12RL/BX BX 1 DOPAMINE HCL, SDV 80MG/ML 5ML 25/PK EA 3
BANDAGE, GZE FLUFF 4.5 PERFM STR 100RL/CS RL 6 DIPHENHYDRAMINE, VL 50MG/ML 1ML 25/BX EA 3
BANDAGE, ADHSV SHR STRP 1X3 PERFM 100/BX 24BX/CS BX 1 DEXTROSE, SYR 50 50ML 25/CT EA 4
BAG, VOMIT W/HND PROTECTOR 240/CS EA 5 DEXTROSE, SYR 25 10ML 10/CT EA 1
RESUSITATOR, SPUR II MED ADLT 12/CS EA 2 DEX, IVSOL 5 500ML 24/CS EA 1
BAG, BIOHAZARD RED 11X14.25 20/RL 10RL/CS CS 1 DEX, IVSOL 5 100ML 96/CS EA 1
ASPIRATOR, MECONIUM W/TRAP 40/CS EA 1 DETECTOR, CO2 END-TIDAL PED 6/CS EA 2
ARMBOARD, ADLT FOAM DISP 3X18 50/CS EA 1 CONTAINER, SHARPS SHUTTLE 24/CS EA 2
AIRWAY, ROBERTAZZI NASOPHARYN 34FR 10/BX EA 1 CONTAINER, SHARPS NEST CLR 8QT24/CS EA 1
AIRWAY, NASOPHARYN DISP 32FR 10/BX EA 1 COMBITUBE, ET DBL LUMEN AIRWAY ROLL-UP KIT 37F4/C EA 1
AIRWAY, NASOPHARYN DISP 30FR 10/BX EA 1 COMBITUBE, ET DBL LUMEN AIRWAY ROLL-UP KIT 41F4/C EA 1
AIRWAY, NASOPHARYN DISP 28FR 10/BX EA 1 CATH, IV PROTECT PLUS, 18X1 1/4 50/BX EA 10
AIRWAY, NASOPHARYN DISP 26FR 10/BX EA 1 CATH, IV PROTECT PLUS 24X3/4 50/BX EA 10
AIRWAY, NASOPHARYN DISP 24FR 10/BX EA 1 CATH, IV PROTECT PLUS 22X1 50/BX EA 10
AIRWAY, NASOPHARYN DISP 22FR 10/BX EA 1 CATH, IV PROTECT PLUS 20X 1 1/4 50/BX EA 10
AIRWAY, NASOPHARYN DISP 20FR 10/BX EA 1 CATH, IV PROTECT PLUS 16X1 1/4 50/BX EA 10
AIRWAY, GUEDEL PLAS SZ6 10/BX EA 1 CATH, IV PROTECT PLUS 14X1 1/4 50/BX EA 10
AIRWAY, GUEDEL 90MM LF 1/PK 24PK/BX PK 1 CALCIUM CHLORIDE, SYR 10 100MG/ML 10ML 10/CT EA 3
AIRWAY, GUEDEL 80MM LF 1/PK 24PK/BX PK 1 BATTERY, ALKALINE AAA 24/BX 6BX/CS BX 1
AIRWAY, GUEDEL 70MM LF 1/PK 24PK/BX PK 2 BATTERY, ALKAL C 12/BX 6BX/CS BX 1
AIRWAY, GUEDEL 60MM LF 1/PK 24PK/BX PK 1 BATTERY, ALKALINE AA 24/BX 6BX/CS BX 1
AIRWAY, GUEDEL 50MM LF 1/PK 24PK/BX PK 1 ATROPINE SULFATE, PFS 0.1MG/ML 10ML 25/CT EA 4

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
129
Description UOM QTY Description UOM QTY
AIRWAY, GUEDEL 100MM LF 1/PK 24PK/BX PK 1 ASPIRIN, TAB 81MG CHLD CHEW 36/BT EA 2
ACTIDOSE-AQUA, SUSP 25GM/120ML 120ML EA 1 ALBUTEROL, SOL INH 0.83MG/ML 3ML 25/CT CT 1
ABD PAD, 8X10 STR LF PERFM+ 1/PK 24PK/BX BX 1 ADAPTER, MULTI 15MM ID 22MM OD 50/CS EA 2
General Population Base Package (Serves 50 BLS patients)
Description UOM QTY Description UOM QTY
OXYGEN ALUMINUM CYLINDER - E EA 5 GLOVE, EXAM CHLRPRN PF 1RSPONDR-EC LF MD 50/BX BX 2
LIFE PAK 1000 AED EA 1 GLOVE, EXAM CHLRPRN PF 1RSPONDR-EC LF LG 50/BX BX 2
WRENCH, CYLINDER SM EA 1 GLASSES, MAGNUM BLK FRAME CLR LENS QD163321 1/EA EA 2
WATER STR, IRR SOL 1000ML 12/CS EA 6 EPI-PEN, SYR .3MG AUTO INJ EA 1
V-VAC STARTER KIT EA 1 EPI-PEN JR, SYR .15MG AUTO INJ EA 1
TOWELETTE, ANTIMICROBIAL VIONEX MX-1510 50/BX BX 1 DRESSING, XEROFORM STR 5X9 50/BX EA 5
TAPE, ADHSV TRANSPORE 1X10YDS 12RL/BX BX 1 DRESSING, TRAUMA 10X30 PERFM STR LF 1/PK 50PK/C PK 8
TAPE, ADHSV CLOTH SILK LF 2X10YD 6RL/BXPERFM+ BX 1 DISINFECTANT, CAVICIDE PUMP SPRAY 24OZ EA 1
TAG COMBO KIT, TRIAGE LG 25/PK IP200 PK 1 CONTAINER, SHARPS MAILBOX STYL RED 5QT 20/CS EA 1
SYRINGE, EAR BULB STR 2OZ 50/CS EA 2 TIP, SCTN BIG STICK LG BORE W/THUMB CNTRL 50/CS EA 6
SUCTION, YANKAUER RIGID BULB TIP VENT STR LF 50/C EA 6 COLLAR, PERFIT MINI FULLY ADJ 30/CS EA 4
STETHOSCOPE, PROSCOPE SPRAGUE 16 BLK EA 2 COLLAR, CERVICAL EXTRICATION ADJ 30/CS EA 4
SPLINT, CARDBOARD PLAIN N/PADDED 24 25/CS EA 3 CATHETER, SCTN GRAD PED 6FR50/CS373291 EA 6
SPLINT, CARDBOARD PLAIN N/PADDED 18 25/CS EA 3 CATHETER, SCTN GRAD 8FR 50/CS EA 6
SPLINT, CARDBOARD PLAIN BRN/WHT 34 EA 3 CATHETER, SCTN GRAD 18FR 50/CS EA 6
SPUR II, MEDI PORT INF/TOD MASK PEDI BAG 12/CS EA 3 CATHETER, SCTN GRAD 10FR 50/CS EA 6
SPONGE, GZE 4X4 8PLY PERFM N/S 200/BG BG 1 CANNULA, NASAL CRVD TIP W/7&APOS TU 50/CS EA 12
SPONGE, GZE 4X4 12PLY PERFM STR 2&APOSS 25PK/BX BX 1 CANISTER, SCTN 1200CC 48/CS EA 3
SPHYG, STD ANEROID NVY REG ADLT EA 2 BANDAGE, TRIANGULAR LF 40X40X56 12/BX 6BX/CS BX 1
SPHYG, STD ANEROID NVY CHLD EA 2 BANDAGE, CNFRM STRCH 4 STR LF PERFM 12RL/BX BX 1
SPHYG, PROF ANEROID BLK LG ADLT EA 2 BANDAGE, GZE FLUFF 4.5 PERFM STR 100RL/CS RL 12
SOD CHL, IRR SOL STR 0.9 1000ML 12/CS EA 4 BANDAGE, ADHSV SHR STRP 1X3 PERFM 100/BX 24BX/CS BX 1
MASK, FACE PROC FL RESIST PLTD W/SHLD&EARLP ORG25 BX 1 BAG, VOMIT W/HND PROTECTOR 240/CS EA 12
SHEET, BURN 60X96 EA 3 RESUSITATOR, SPUR II MED ADLT 12/CS EA 6
SHEARS, UTILITY BLK LF 7 1/4 10/BX EA 2 BAG, BIOHAZARD RED 11X14.25 20/RL 10RL/CS CS 1
SANITIZER, HAND PERFM 4OZ 24/CS EA 2 ASPIRATOR, MECONIUM W/TRAP 40/CS EA 2
RESUSCITATOR, SPUR II PED TOD MASK 12/CS EA 3 AIRWAY, ROBERTAZZI NASOPHARYN 34FR 10/BX EA 2

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
130
PAD, PVP PREP MED 100/BX BX 1 AIRWAY, NASOPHARYN DISP 32FR 10/BX EA 2
PAD, EYE OVAL STR 1 5/8X2 5/8 1/PK 50PK/BX 12BX BX 1 AIRWAY, NASOPHARYN DISP 30FR 10/BX EA 2
PAD, ALCOHOL PREP MED 200/BX BX 1 AIRWAY, NASOPHARYN DISP 28FR 10/BX EA 2
Description UOM QTY Description UOM QTY
PACK, HOT INST COMPRESS 6X9 LF 24/CS CS 1 AIRWAY, NASOPHARYN DISP 26FR 10/BX EA 2
PACK, COLD INST COMPRESS 6X9 LF 24/CS CS 1 AIRWAY, NASOPHARYN DISP 24FR 10/BX EA 2
OB KIT, EMERGENCY 10/CS EA 2 AIRWAY, NASOPHARYN DISP 22FR 10/BX EA 2
MASK, FACE SURG CONE W/HDBND BLU 50/BX BX 1 AIRWAY, NASOPHARYN DISP 20FR 10/BX EA 2
MASK, RESCUE SOFT CASE BASIC RED EA 2 AIRWAY, GUEDEL PLAS SZ6 10/BX EA 3
MASK, PARTICULATE N95 SM 20/BX BX 1 AIRWAY, GUEDEL 90MM LF 1/PK 24PK/BX PK 3
MASK, OXY NONREBREATH W/VENT PED 50/CS EA 8 AIRWAY, GUEDEL 80MM LF 1/PK 24PK/BX PK 3
MASK, OXY NONREBREATH W/7&APOSTU 50/CS EA 8 AIRWAY, GUEDEL 70MM LF 1/PK 24PK/BX PK 3
MASK, N95 MED 20/BX BX 1 AIRWAY, GUEDEL 60MM LF 1/PK 24PK/BX PK 3
MASK, N95 LG 20/BX BX 1 AIRWAY, GUEDEL 50MM LF 1/PK 24PK/BX PK 3
MASK, FACE INF 20/CS EA 6 AIRWAY, GUEDEL 100MM LF 1/PK 24PK/BX PK 3
MASK, FACE DISP PED EA 6 ACTIDOSE-AQUA, SUSP 25GM/120ML 120ML EA 1
MASK, FACE DISP ADLT LG 20/CS EA 6 ABD PAD, 8X10 STR LF PERFM+ 1/PK 24PK/BX BX 1
MASK, FACE ADLT MED 20/CS EA 6 ABD PAD, 5X9 STR LF PERFM+ 1/PK 20PK/BX BX 1
PENLIGHT, DISP 6/PK PK 1 BLOOD GLUCOSE METER EA 1
INSTA-GLUCOSE, GEL 40 31GM 3/BX BX 2 BLOOD GLUCOSE TEST STRIPS 50/BOX BX 1
GLOVE, EXAM CHLRPRN PF 1RSPONDR-EC LF XLG 50/BX BX 2 DIGITAL THERMOMETER, ORAL EA 1
GLOVE, EXAM CHLRPRN PF 1RSPONDR-EC LF SM 50/BX BX 2 ORAL THERMOMETER SHEATH 50/BOX BX 2

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 131
General Population Supplemental Package (Serves 50 BLS patients)
Description UOM QTY Description UOM QTY
OXYGEN ALUMINUM CYLINDER - E EA 1
WATER STR, IRR SOL 1000ML 12/CS EA 2 EPI-PEN JR, SYR .15MG AUTO INJ EA 1
TOWELETTE, ANTIMICROBIAL VIONEX MX-1510 50/BX BX 1 DRESSING, TRAUMA 10X30 PERFM STR LF 1/PK 50PK/C PK 4
TAPE, ADHSV TRANSPORE 1X10YDS 12RL/BX BX 1 DISINFECTANT, CAVICIDE PUMP SPRAY 24OZ EA 1
TAPE, ADHSV CLOTH SILK LF 2X10YD 6RL/BXPERFM+ BX 1 TIP, SCTN BIG STICK LG BORE W/THUMB CNTRL 50/CS EA 2
SYRINGE, EAR BULB STR 2OZ 50/CS EA 2 CATHETER, SCTN GRAD PED 6FR50/CS373291 EA 2
SUCTION, YANKAUER RIGID BULB TIP VENT STR LF 50/C EA 3 CATHETER, SCTN GRAD 8FR 50/CS EA 2
SPUR II, MEDI PORT INF/TOD MASK PEDI BAG 12/CS EA 3 CATHETER, SCTN GRAD 18FR 50/CS EA 2
SPONGE, GZE 4X4 8PLY PERFM N/S 200/BG BG 1 CATHETER, SCTN GRAD 10FR 50/CS EA 2
SPONGE, GZE 4X4 12PLY PERFM STR 2&APOSS 25PK/BX BX 1 CANNULA, NASAL CRVD TIP W/7&APOS TU 50/CS EA 5
SOD CHL, IRR SOL STR 0.9 1000ML 12/CS EA 2 CANISTER, SCTN 1200CC 48/CS EA 3
MASK, FACE PROC FL RESIST PLTD W/SHLD&EARLP ORG25 BX 1 BITE STICK, 10/PK EA 1
SHEARS, UTILITY BLK LF 7 1/4 10/BX EA 2 BANDAGE, TRIANGULAR LF 40X40X56 12/BX 6BX/CS BX 1
SANITIZER, HAND PERFM 4OZ 24/CS EA 2 BANDAGE, CNFRM STRCH 4 STR LF PERFM 12RL/BX BX 1
RESUSCITATOR, SPUR II PED TOD MASK 12/CS EA 3 BANDAGE, GZE FLUFF 4.5 PERFM STR 100RL/CS RL 8
PAD, PVP PREP MED 100/BX BX 1 BANDAGE, ADHSV SHR STRP 1X3 PERFM 100/BX 24BX/CS BX 1
PAD, ALCOHOL PREP MED 200/BX BX 1 BAG, VOMIT W/HND PROTECTOR 240/CS EA 6
PACK, HOT INST COMPRESS 6X9 LF 24/CS CS 1 RESUSITATOR, SPUR II MED ADLT 12/CS EA 3
PACK, COLD INST COMPRESS 6X9 LF 24/CS CS 1 BAG, BIOHAZARD RED 11X14.25 20/RL 10RL/CS CS 1
OB KIT, EMERGENCY 10/CS EA 1 ASPIRATOR, MECONIUM W/TRAP 40/CS EA 1
MASK, FACE SURG CONE W/HDBND BLU 50/BX BX 1 AIRWAY, ROBERTAZZI NASOPHARYN 34FR 10/BX EA 1
MASK, RESCUE SOFT CASE BASIC RED EA 2 AIRWAY, NASOPHARYN DISP 32FR 10/BX EA 1
MASK, PARTICULATE N95 SM 20/BX BX 1 AIRWAY, NASOPHARYN DISP 30FR 10/BX EA 1
MASK, OXY NONREBREATH W/VENT PED 50/CS EA 4 AIRWAY, NASOPHARYN DISP 28FR 10/BX EA 1
MASK, OXY NONREBREATH W/7&APOSTU 50/CS EA 4 AIRWAY, NASOPHARYN DISP 26FR 10/BX EA 1
MASK, N95 MED 20/BX BX 1 AIRWAY, NASOPHARYN DISP 24FR 10/BX EA 1
MASK, N95 LG 20/BX BX 1 AIRWAY, NASOPHARYN DISP 22FR 10/BX EA 1
MASK, FACE INF 20/CS EA 2 AIRWAY, NASOPHARYN DISP 20FR 10/BX EA 1
MASK, FACE DISP PED EA 2 AIRWAY, GUEDEL PLAS SZ6 10/BX EA 1
MASK, FACE DISP ADLT LG 20/CS EA 2 AIRWAY, GUEDEL 90MM LF 1/PK 24PK/BX PK 1
MASK, FACE ADLT MED 20/CS EA 2 AIRWAY, GUEDEL 80MM LF 1/PK 24PK/BX PK 1
PENLIGHT, DISP 6/PK PK 1 AIRWAY, GUEDEL 70MM LF 1/PK 24PK/BX PK 1
INSTA-GLUCOSE, GEL 40 31GM 3/BX BX 2 AIRWAY, GUEDEL 60MM LF 1/PK 24PK/BX PK 1
GLOVE, EXAM CHLRPRN PF 1RSPONDR-EC LF SM 50/BX BX 1 AIRWAY, GUEDEL 50MM LF 1/PK 24PK/BX PK 1
GLOVE, EXAM CHLRPRN PF 1RSPONDR-EC LF MD 50/BX BX 1 AIRWAY, GUEDEL 100MM LF 1/PK 24PK/BX PK 1
GLOVE, EXAM CHLRPRN PF 1RSPONDR-EC LF LG 50/BX BX 1 ACTIDOSE-AQUA, SUSP 25GM/120ML 120ML EA 1
GLOVE, EXAM CHLRPRN PF 1RSPONDR-EC LF XLG 50/BX BX 1 ABD PAD, 8X10 STR LF PERFM+ 1/PK 24PK/BX BX 1
EPI-PEN, SYR .3MG AUTO INJ EA 1 ABD PAD, 5X9 STR LF PERFM+ 1/PK 20PK/BX BX 1

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 132
BLS KIT EQUIPMENT LIST
DESCRIPTION UOM QTY DESCRIPTION UOM QTY
VHF TWO WAY RADIO COMM DEVICE EA 1 ROADSIDE WARNING DEVICE ST 1
WHEELED ROLLING COT EA 1 RAIN GEAR SET ST 2
V-VAC STARTER KIT EA 1 LEATHER WORK GLOVES PR 2
CONNECTOR, SUCTION TUBING EA 2 HI-VIS SAFETY VEST EA 2
CANISTER, SCTN 1200CC EA 2 AED LP1000 EA 1
RIGID TIP SUCTION EA 1 D SIZE BATTERIES EA 8
CATHETER, SCTN GRAD PED 6FR EA 1 PENLIGHT PK 1
CATHETER, SCTN GRAD 10FR EA 1 PEDI NRB MASK EA 2
CATHETER, SCTN GRAD 12FR EA 1 ADULT NRB MASK EA 6
CATHETER, SCTN GRAD 18FR EA 1 ADULT CANNULA EA 4
WRENCH, CYLINDER SM EA 1 PEDI CANNULA EA 2
WRENCH, CYLINDER LG EA 1 ADULT BVM EA 2
PORTABLE OXYGEN REGULATOR EA 1 TOD BVM EA 2
OXYGEN PORTABLE TANK "E" EA 4 ADULT EASYCAP CO2 EA 2
COLLAR, PEDI ADJUSTABLE EA 2 PEDI EASCAP CO2 EA 2
COLLAR, ADLT ADJUSTABLE EA 2 ADULT PACING ELECTRODES PK 2
HEAD BLOCK EA 2 PEDI PACING ELECTRODES PK 2
SPLINT, CARDBOARD 34" EA 2 COMBITUBE EA 1
SPLINT, CARDBOARD 24" EA 2 MASK, FACE INF EA 2
SPLINT, CARDBOARD 18" EA 2 MASK, FACE ADLT MED EA 2
KED TYPE DEVICE EA 1 34FR NPA EA 1
DISPOSABLE CARDBOARD LBB EA 2 30FR NPA EA 1
STRAP, DISPOSABLE ORANGE EA 6 26FR NPA EA 1
BANDAGE, TRIANGULAR EA 2 22FR NPA EA 1
BLANKET, EMERGENCY T/P YELLOW EA 4 90MM OPA PK 1
BROSLOW PEDI TAPE EA 1 80MM OPA PK 1
CHILD BP CUFF EA 1 70MM OPA PK 1
LG ADULT BP CUFF BX 1 60MM OPA PK 1
REG ADULT BP CUFF EA 1 50MM OPA PK 1
STETHOSCOPE EA 1 100MM OPA PK 1
SCISSORS EA 1 PULSE OX- ADULT/CHILD EA 1
FLASHLIGHT EA 2 BURN SHEET EA 2
BLANKET- GRAY EA 4 4X4 GAUZE BX 1
PILLOWCASE EA 4 8'X10' ABD PAD EA 6
STRETCHER SHEET EA 8 10'X30' TRAUMA DRESSING PK 2
PILLOW DISPOSABLE EA 2 4.5' KERLIX RL 4
TOWELS ROLLS EA 2 2.25" KERLIX RL 4
TOILET PAPER RL 4 BAND-AID 1" EA 10
TRIAGE TAGS- PK OF 25 PK 1 OCCLUSIVE DRESSING EA 4
VOMIT BAG EA 12 1" PLASTIC TAPE RL 2
URINAL EA 1 2" PLASTIC TAPE RL 1
MEGAMOVER CARRY DEVICE EA 1 2" SILK TAPE RL 1
CLEAR SHIELD FACE MASK EA 5 1" SILK TAPE RL 2
GOWNS EA 5 ARTERIAL TOURNIQUET EA 1
HAND SANITIZER EA 1 OB KIT EA 1
CAVICIDE DISINFECTANT EA 1 THERMOMETER, SKIN EA 4
1QT SHARPS CONTAINER EA 1 HOT PACK EA 4
5QT SHARPS CONTAINER EA 1 COLD PACK EA 4
TRASH BAGS- WHITE RL 1 STERILE SALINE IRR EA 2
RED BAG RL 1 SM GLOVES BX 2
SMALL N95 EA 4 MED GLOVES BX 2
MED N95 EA 4 LG GLOVES BX 2
LG N95 EA 4 XL GLOVES BX 2
ARMBOARD, FOAM EA 4 KY JELLY EA 10
SOFT LIMB RESTRAINT PR 2 IODINE PREP PAD EA 25
MRE CASE CS 1 ALCOHOL PREP PAD EA 25

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
133
ALS KIT EQUIPMENT LIST (In addition to the BLS kit equipment)
DESCRIPTION UOM QTY
DESCRIPTION UOM QTY
EKG PAPER RL 2 14G IV CATH EA 5
PED EKG ELECTRODE (30 EA TOTAL) PK 1 16G IV CATH EA 5
ADULT EKG ELECTRODE EA 2 18G IV CATH EA 5
LARYNGOSCOPE HANDLE EA 1 20G IV CATH EA 5
CHILD FORCEP BX 1 22G IV CATH EA 5
ADULT FORCEP EA 1 24G IV CATH EA 5
#4 MILLER BLADE EA 1 CHEST DECOMP NEEDLE EA 1
#3 MILLER BLADE EA 1 I/O NEEDLE ADULT EA 1
#2 MILLER BLADE EA 1 I/O NEEDLE CHILD EA 1
#1 MILLER BLADE EA 1 TOURNIQUET EA 10
#4 MAC BLADE EA 1 23G NEEDLE EA 5
#3 MAC BLADE EA 1 25G NEEDLE EA 5
#2 MAC BLADE EA 1 19G NEEDLE EA 5
AAA BATTERY EA 4 SELECT III EA 6
C BATTERY EA 4 NEBULIZER EA 6
LG BLADE BULB EA 1 EPI 0.1MG/10ML EA 8
SM BLADE BULB EA 1 ATROPINE EA 6
GLUCOMETER EA 1 ADENOSINE EA 3
GLUCOMETER TEST STRIPS BT 1 CARDIZEM EA 2
LANCETS EA 10 LOPRESSOR/MITROPALOL EA 2
2.0 ETT EA 1 LIDOCAINE INJ EA 3
2.5 ETT EA 1 NITRO TABS BT 1
3.0 ETT EA 1 ASPIRIN EA 1
3.5 ETT EA 1 DOPAMINE EA 1
4.0 ETT EA 1 ALBUTEROL EA 5
4.5 ETT EA 1 IPRATROPIUM EA 5
5.0 ETT EA 1 FUROSEMIDE EA 4
5.5 ETT EA 1 EPINEPHRINE, MDV 30ML EA 1
6.0 ETT EA 1 DEXTROSE 50 EA 4
6.5 ETT EA 1 ANALGESIC GEL GRX 1OZ TUBE EA 1
7.0 ETT EA 1 MORPHINE SULFATE
7.5 ETT EA 1 FENTANYL
8.0 ETT EA 1 LORAZEPAM
TUBE CHECK EA 1 MIDAZOLAM
TUBE HOLDERS- ADULT & CHILD EA 1 SODIUM BICARB EA 2
1 CC SYRINGE EA 5 MAGNESIUM SULFATE FTV 50% 20ML EA 1
5 CC SYRINGE EA 5 GLUCAGEN DIAG KIT EA 1
10 CC SYRINGE EA 10 NALOXONE EA 4
60 CC SYRINGE EA 4 CALCIUM CHLORIDE EA 2
NORMAL SALINE 1000 ML BAG EA 6 SODIUM CHLORIDE, FTV 10 ML EA 1

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 134
Appendix B – Documentation
Fixed Site Deployment Process Quick Reference Guide
Important Phone Numbers
Natcom Dispatch (866) 219-9253
Natcom Fixed Site Branch Manager (303) 481-1142
Natcom ERT Unit Leader (303) 481-1145
Enroute
Notify Natcom Dispatch immediately once
departed home operations (give placard, name, company, route of
travel and ETA)
Continue to communicate with Natcom Dispatch at
important intervals (Arrival at Airport,
Boarding plane, debarking plane, at check-in, etc.) if flying or every 2 hours if
driving
Review Fixed Site ConOps and Fixed Site Job Aide
Checked-In
Complete Personnel Registration Form and Fixed Site Personnel
Check-In Form
Remain ready for assignment in close
proximity to FSP Leader
Demobilized
Remain at Forward Operating Base until
released
Keep Natcom Dispatch informed of status and
ETA to home operations
Report home base arrival to Natcom Dispatch
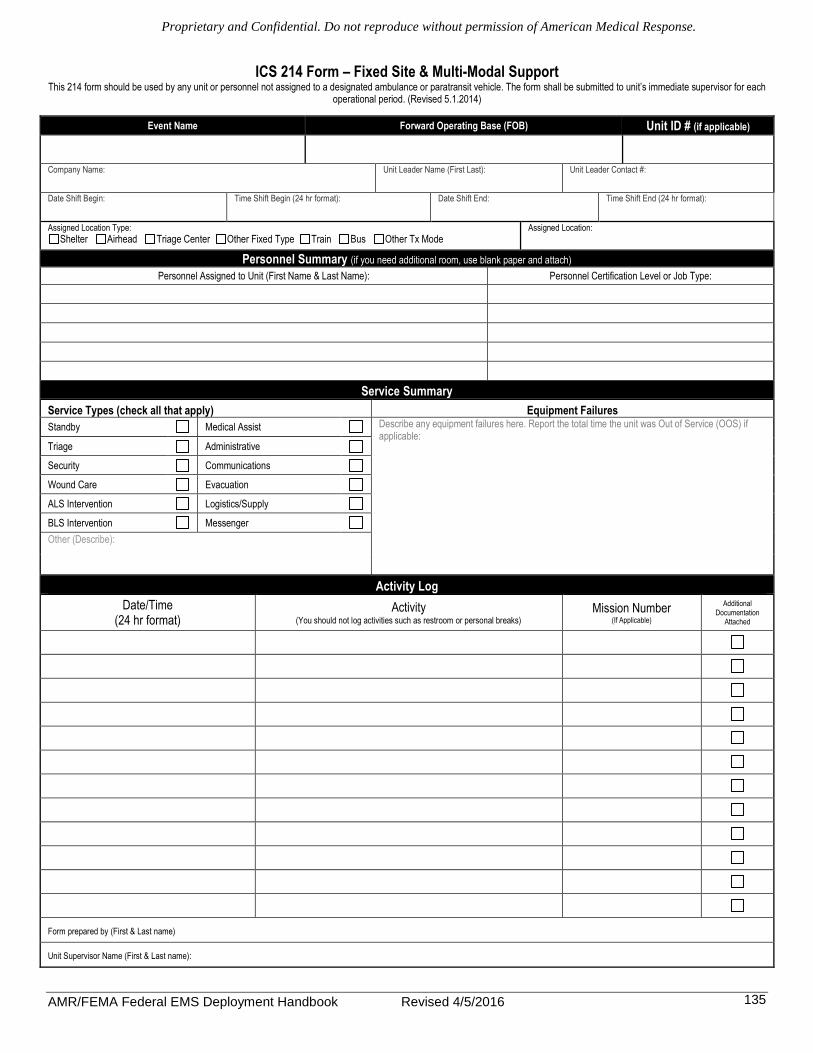
Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
135
ICS 214 Form – Fixed Site & Multi-Modal Support This 214 form should be used by any unit or personnel not assigned to a designated ambulance or paratransit vehicle. The form shall be submitted to unit’s immediate supervisor for each
operational period. (Revised 5.1.2014)
Event Name Forward Operating Base (FOB) Unit ID # (if applicable)
Company Name:
Unit Leader Name (First Last):
Unit Leader Contact #:
Date Shift Begin:
Time Shift Begin (24 hr format):
Date Shift End:
Time Shift End (24 hr format):
Assigned Location Type:
Shelter Airhead Triage Center Other Fixed Type Train Bus Other Tx Mode Assigned Location:
Personnel Summary (if you need additional room, use blank paper and attach)
Personnel Assigned to Unit (First Name & Last Name): Personnel Certification Level or Job Type:
Service Summary
Service Types (check all that apply) Equipment Failures
Standby Medical Assist Describe any equipment failures here. Report the total time the unit was Out of Service (OOS) if applicable:
Triage Administrative
Security Communications
Wound Care Evacuation
ALS Intervention Logistics/Supply
BLS Intervention Messenger Other (Describe):
Activity Log
Date/Time (24 hr format)
Activity (You should not log activities such as restroom or personal breaks)
Mission Number (If Applicable)
Additional Documentation
Attached
Form prepared by (First & Last name)
Unit Supervisor Name (First & Last name):

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
136
Demographic Data
Event Name: The name of the event or disaster. Ex: Hurricane Katrina Forward Operating Base (FOB): The location where the deployed resources are assigned to and where they carried out the activities that they documented on the 214 Unit Log. Unit ID: If you have been assigned a unit number, indicate it here.ex: Medic 34… Company Name: The name of the home company the resource originated from. Ex: Tri-County EMS, AMR San Diego Unit Leader: This is the name of the person in charge of the unit. Unit Leader Contact #: The Unit Leader’s cell phone or other contact number. Date Shift begin: This is the date that the current shift began for the resource. Time Shift begin: This is the time that the current shift began for the resource. All times should be in 24-hour format. Date Shift End: This is the date that the current shift ended for the resource. Time Shift End: This is the time that the current shift ended for the resource. All times should be marked in 24-hour time format. Assigned Location Type: Check or circle which type of location you are assigned to. Assigned Location: Indicated exactly the location you are assigned to. For example, if you have been assigned to XYZ shelter, indicate XYZ shelter.
Personnel Summary Personnel Assigned to the Unit: List the names of all personnel assigned to the resource unit. Personnel Certification Level or Job Type: List each person’s certification level or job type. Ex: ASE certified mechanic, food service specialist, administrative assistant, fuel truck driver, etc.
Service Summary Service Types: Check the type of services your unit provided. Ex: if you are standing by at a shelter, check standby. If there is not a type that fits your service, use the other box to describe your service provided. Equipment Failures: List any specific equipment failures that directly affect your ability to complete your mission.
Activity Log In this section, you should log all important activities you perform throughout your shift. For example, if you are a maintenance vehicle, you should log any maintenance runs you make or on-site repairs you do.

Proprietary and Confidential. Do not reproduce without permission of American Medical Response.
AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 137
RESIDENT’S HEALTH CARE RECORD
Assignment Name: ______________________________________________ Placard Number: ______________________ Caregiver: ________________________________
Resident Name: Resident #: DOB: Gender:
If no assigned resident number, use formula Last 4 of SSN + DOB + first and last initial.
Date Time Complaint Treatment

AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 138
MEDICATION ADMINISTRATION RECORD
Assignment: ________________________________________________________ Name: __________________________________________________ Resident #: ________________________ DOB: __________________ Allergies: _____________________________________________________________________________________________________________
Date Time Medication Dosage Route Administrator’s
Initials
Medical Personnel‘s Printed Name: _____________________________________ Initials: __________________
Medical Personnel‘s Printed Name: _____________________________________ Initials: __________________
Medical Personnel‘s Printed Name: _____________________________________ Initials: __________________
Medical Personnel‘s Printed Name: _____________________________________ Initials: __________________

AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
139
Aggregate Morbidity Report A. General Information
1. Event Name: ____________________________________
2. Report Date: ____/_____/________
3. Report Timeframe: ___________ - ____________
4. Worksite Name: _________________________________
5. Service Type (circle one): Shelter Non-shelter
C. Demographics Tally (IIII) Total (#)
Gender Male Female
Age ≤ 2 3 to 18 19 to 64 ≥ 65
B. Number of Patient Encounters
Tally (IIIII IIIII IIIII) Total (#)
E. Disposition Tally (IIII) Total (#) Provided Care Transferred to higher level of care
Refused Care Deceased
E. Patient’s Complaint (tick all that apply) Tally
(IIII) Total (#)
Tally (IIII)
Total (#)
Injury Allergic Reaction
Bite (includes ALL bites) Respiratory (includes ALL resp.)
Burn (thermal or chemical) Influenza-like-illness (ILI)
Cut/laceration/puncture Neurological, new onset
Foreign body (e.g. splinter) Other illness/symptoms
Fall/slip/trip Behavioral Mental Health Hit by or against object Agitated/disruptive/psychotic Use of machinery/tools/equip. Anxiety/stress/depressed mood
Assault Suicidal/homicidal thoughts
Carbon Monoxide (CO) exposure Substance addiction/withdrawal
Poisoning, non-CO Other mental health
Other injury Exacerbation of Chronic Illness
Illness/Symptoms Asthma
Fever (>100.4°F or 38°C) Obstructive pulmonary disease
Conjunctivitis/eye irritation Cardiovascular (HTN, CHF, CHD)
Dehydration Chronic muscle or joint pain Heat stress/heat exhaustion Diabetes
Hypothermia/cold-environment Neurological (seizure, stroke, dementia)
Oral health Previous mental health diagnosis
Pain: chest, angina, cardiac arrest Other chronic illness
Pain: muscle or joint Health Care Maintenance
Pain: head, ears, eyes, nose, throat Blood pressure check
Pain: other, not specified above Blood sugar check
Gastrointestinal (GI): diarrhea Pregnancy/post-partum care
GI: nausea/vomiting Dressing change/wound care
GI: other (constipation, GERD) Immunization/vaccination
Genitourinary (GU) Med refill (1 tick for ea. med)
Skin (includes ALL skin conditions) Other health maintenance

AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
140
Contact & Emergency Numbers
Incident Contact Information
Forward Operating Base Position Name Contact Number
NATCOM Position Name Contact Number
Air Medical Support Team Position Name Number
Fixed Site Personnel Leader(s) Name Contact Number
Other FSP on assignment Name Contact Number Name Contact Number

AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016
141
Fixed Site Contact Information
Fixed Site Support Demographics
Facility Name: Assignment Name:
Address: City: State: Zip:
Facility Management Contact Information
Medical Control Contact Information
Additional Important Person(s) Contact Information
Notes / Instructions

AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 142
Go or No Go for Flight, A Reference
Bedside Preparation for Patient Transport
ACCESS PATIENT / ARRIVAL TO BEDSIDE
Transport Assessment - Does the patient have any of the following? - Advanced Airway with Artificial Ventilation - IV Site with fluid or medication running via pump or gravity - Specialty Equipment – IAPB, CVVH, LVAD, ECMO - Foley Catheter - Chest Tube/s - Tube Feedings - Advance Directives/ DNR - Extremity Cast/ Splint - Cervical Collar - Traction Splint/ Immobilization Device - Gross Deformity or Open Wound - Weight of more than 350lbs
NO YES
Preparation Required - Advanced airway with artificial ventilation
Assure Airway Device is Secure, have Bag Valve device bedside and gastric tube clamped - IV site with fluids, blood or medication running via pump or gravity
Assure the IV site is secure, have extra quantities of infusing medications available bedside - Specialty Equipment – IAPB, CVVH, LVAD, ECMO
Assure appropriate clinician is bedside and available to assist crew, notify AMR Air Dispatch - Foley Catheter
Assure catheter is secure; empty any fluid from bag or container - Chest Tube/s
Assure tubing is secure and if attached to suction that portable device is available - Tube Feedings
Assure tube is secure, request for feeding to be stopped and flushed - Advance Directives/ DNR
Assure proper documentation of Advance Directive is available bedside - Cervical Collar
Assure correct size for the patient and applied appropriately, gather X-ray, CT or MRI Info if possible - Extremity Cast/ Splint
Confirm distal Pulse, Motor and Sensory (PMS). Need at least 2 fingers between cast and extremity - Traction Splint/ Immobilization Device
Needs to be a commercial portable device, not attached to bed. No free hanging traction weights - Gross Deformity or Open Wound
Secure deformity site. Confirm bleeding is controlled, cover wound with clean dry dressings
- Weight of more than 350lbs – Confirm Patient weight and if >350lbs contact AMR Air Dispatch
Have the above items been Addressed OR Confirmed?
YES NO
Contact Triage Coordinator/ AMR Air
Dispatch 1-800-424-7060
- Gather any available paperwork - Gather Patient Emergency Contact Info - Gather and bag any patient belongings - Assure patient is warm - If patient is on 02 have portable tank at bedside - Reassure patient (if applicable)
PATIENT IS “FLIGHT
READY”
NO GO GO

AMR/FEMA Federal EMS Deployment Handbook Revised 4/5/2016 143
END OF DOCUMENT


















