February/March 2012, Vol 4, No 1
16
CTRC-AACR SABCS ANNUAL MEETING Adding Everolimus to Exemestane significantly Prolongs Remission in Patients with breast cancer Updated results of pivotal BOLERO-2: potential paradigm change By Caroline Helwick ©2012 Novellus Healthcare Communications, LLCs Continued on page 9 Continued on page 8 consider gnRh Agonist to trigger ovulation in women at Risk of ovarian hyperstimulation syndrome By Wayne Kuznar The Offical Publication of The Official Publication of ASRM ANNUAL MEETING . . . . . . . . 7 Low-intensity IVF: how does it stack up? NEW WHO GUIDELINES............ 8 Which guidelines should fertility clin- ics follow when undertaking semen analysis? INFERTILITY UPDATES . . . . . . . . .13 Viability of single-embryo transfer as method to reduce multiple birth rates Do low AMH levels rule out in vitro fertilization as an option? PATIENT AWARENESS AND IDENTIFICATION . . . . . . . . . . . . . . . 14 One fertility center’s approach to testing NONSURGICAL INTERVENTION . . . . . . . . . . . . . . . . . 14 A look at pelvic organ prolapse INSIDE CTRC-AACR SABCS ANNUAL MEETING Dual hER2 blockade with Pertuzumab substantially Delays Disease Progression By Audrey Andrews fEbRuARy/MARch 2012 www.thEobgyNNuRsE.coM Vol 4, No 1 Continued on page 9 Gabriel Hortobagyi, MD, Chair of Breast Medical Oncology, The University of Texas MD Anderson Cancer Center, Houston. We thank Watson Pharmaceuticals, Inc., for their gold level support. Estradiol Route of Administration Does Not Affect Pregnancy Rate By Wayne Kuznar San Antonio, TX – It is becoming increasingly clear that 2 agents are bet- ter than 1 in treating HER2-positive advanced breast cancer. The latest evi- dence comes from the results of the phase 3 clinical trial CLEOPATRA (Clinical Evaluation of Pertuzumab and Trastuzumab), which were presented at the 2011 CTRC-AACR San Antonio Breast Cancer Symposium by Jose Baselga, MD, PhD, professor of medi- cine, Harvard Medical School and associate director of the Massachusetts General Hospital Cancer Center, Boston. Adding pertuzumab to a combina- tion of trastuzumab and docetaxel chemotherapy as first-line treatment for patients with metastatic disease extended progression-free survival (PFS) by a median of 6.1 months com- pared with patients who received only trastuzumab-docetaxel, Dr Baselga reported. “This is huge. It is very uncommon to have a clinical trial show this level of improvement in PFS,” Orlando, FL – Consider leuprolide acetate, a gonadotropin releasing hor- mone (GnRH) agonist, instead of a tra- ditional human chorionic gonadotropin (hCG) as a trigger for final oocyte mat- uration in in vitro fertilization (IVF) in patients at risk of ovarian hyperstim- ulation syndrome (OHSS), advised Orlando, FL – The route of estradiol administration does not influence the pregnancy rate in frozen embryo transfer (FET) in vitro fertilization cycles, found investigators at the University of Connecticut Health Center, Farmington. No studies have been performed com- paring pregnancy rates with different routes of estradiol administration, prompting the investigators to perform a review of FET at their institution, com- paring pregnancy rates for patients undergoing cycles with transdermal, oral, or a combination of routes of estra- diol administration. They presented their findings in poster format at the 2011 meeting of the American Society for Reproductive Medicine. There were 479 FET cycles reviewed in women aged 44 years and younger. Patients on vaginal estradiol or with nonfunctioning ovaries were excluded. All FET cycles were downregulated with leuprolide acetate starting in the San Antonio, TX – Updated results from the phase 3 Breast Cancer Trials of Oral Everolimus (BOLERO-2) showed that adding everolimus to the treatment regimen with the aromatase inhibitor exemestane more than dou- bled progression-free survival (PFS) in patients with advanced estrogen Continued on page 6
-
Upload
novellus-healthcare-communications-llc -
Category
Documents
-
view
215 -
download
1
description
obgyn february/march 2012 issue
Transcript of February/March 2012, Vol 4, No 1

CTRC-AACR SABCS ANNUAL MEETING
Adding Everolimus toExemestane significantlyProlongs Remission inPatients with breast cancerUpdated results of pivotal BOLERO-2: potential paradigm change
By Caroline Helwick
©2012 Novellus Healthcare Communications, LLCs
Continued on page 9
Continued on page 8
consider gnRh Agonist totrigger ovulation in women atRisk of ovarian hyperstimulationsyndromeBy Wayne Kuznar
The Offical Publication ofThe Official Publication of
ASRM ANNUAL MEETING . . . . . . . . 7Low-intensity IVF: how does it stack up?
NEW WHO GUIDELINES . . . . . . . . . . . . 8Which guidelines should fertility clin-ics follow when undertaking semenanalysis?
INFERTILITY UPDATES . . . . . . . . .13Viability of single-embryo transfer asmethod to reduce multiple birth rates
Do low AMH levels rule out in vitrofertilization as an option?
PATIENT AWARENESS AND
IDENTIFICATION . . . . . . . . . . . . . . . 14One fertility center’s approach to testing
NONSURGICAL
INTERVENTION . . . . . . . . . . . . . . . . . 14A look at pelvic organ prolapse
INSIDE
CTRC-AACR SABCS ANNUAL MEETING
Dual hER2 blockade withPertuzumab substantiallyDelays Disease ProgressionBy Audrey Andrews
fEbRuARy/MARch 2012 www.thEobgyNNuRsE.coM Vol 4, No 1
Continued on page 9
Gabriel Hortobagyi, MD, Chair of Breast Medical Oncology, The University of Texas MDAnderson Cancer Center, Houston.
We thank Watson Pharmaceuticals, Inc.,for their gold level support.
Estradiol Route ofAdministration Does NotAffect Pregnancy Rate By Wayne Kuznar
San Antonio, TX – It is becomingincreasingly clear that 2 agents are bet-ter than 1 in treating HER2-positiveadvanced breast cancer. The latest evi-dence comes from the results of thephase 3 clinical trial CLEOPATRA(Clinical Evaluation of Pertuzumab andTrastuzumab), which were presented atthe 2011 CTRC-AACR San AntonioBreast Cancer Symposium by JoseBaselga, MD, PhD, professor of medi-cine, Harvard Medical School andassociate director of the Massachusetts
General Hospital Cancer Center,Boston.Adding pertuzumab to a combina-
tion of trastuzumab and docetaxelchemotherapy as first-line treatmentfor patients with metastatic diseaseextended progression-free survival(PFS) by a median of 6.1 months com-pared with patients who received onlytrastuzumab-docetaxel, Dr Baselgareported. “This is huge. It is veryuncommon to have a clinical trial showthis level of improvement in PFS,”
Orlando, FL – Consider leuprolideacetate, a gonadotropin releasing hor-mone (GnRH) agonist, instead of a tra-ditional human chorionic gonadotropin
(hCG) as a trigger for final oocyte mat-uration in in vitro fertilization (IVF) in patients at risk of ovarian hyperstim-ulation syndrome (OHSS), advised
Orlando, FL – The route of estradioladministration does not influence thepregnancy rate in frozen embryo transfer(FET) in vitro fertilization cycles, foundinvestigators at the University ofConnecticut Health Center, Farmington.No studies have been performed com-
paring pregnancy rates with differentroutes of estradiol administration,prompting the investigators to perform areview of FET at their institution, com-paring pregnancy rates for patients
undergoing cycles with transdermal,oral, or a combination of routes of estra-diol administration. They presentedtheir findings in poster format at the2011 meeting of the American Societyfor Reproductive Medicine.There were 479 FET cycles reviewed
in women aged 44 years and younger.Patients on vaginal estradiol or withnonfunctioning ovaries were excluded.All FET cycles were downregulated with leuprolide acetate starting in the
San Antonio, TX – Updated resultsfrom the phase 3 Breast Cancer Trialsof Oral Everolimus (BOLERO-2)showed that adding everolimus to the
treatment regimen with the aromataseinhibitor exemestane more than dou-bled progression-free survival (PFS) in patients with advanced estrogen
Continued on page 6



Crinone® 4% Crinone® 8%(progesterone gel)
For vaginal use only. Rx only
BRIEF SUMMARYFor full prescribing information, see package insert. INDICATIONS AND USAGEAssisted Reproductive TechnologyCrinone 8% is indicated for progesterone supplementation or replacement as part of an Assisted Reproductive Technology (“ART”) treatment for infertile women withprogesterone deficiency.Secondary AmenorrheaCrinone 4% is indicated for the treatment of secondary amenorrhea. Crinone 8% is indi-cated for use in women who have failed to respond to treatment with Crinone 4%.CONTRAINDICATIONSCrinone should not be used in individuals with any of the following conditions: knownsensitivity to Crinone (progesterone or any of the other ingredients); undiagnosed vaginalbleeding; liver dysfunction or disease; known or suspected malignancy of the breast orgenital organs; missed abortion; active thrombophlebitis or thromboembolic disorders,or a history of hormone-associated thrombophlebitis or thromboembolic disorders.WARNINGSThe physician should be alert to the earliest manifestations of thrombotic disorders (throm-bophlebitis, cerebrovascular disorders, pulmonary embolism, and retinal thrombosis).Should any of these occur or be suspected, the drug should be discontinued immediately. Progesterone and progestins have been used to prevent miscarriage in women with a his-tory of recurrent spontaneous pregnancy losses. No adequate evidence is available to showthat they are effective for this purpose.PRECAUTIONSGeneral1. The pretreatment physical examination should include special reference to breast and
pelvic organs, as well as Papanicolaou smear.2. In cases of breakthrough bleeding, as in all cases of irregular vaginal bleeding, non-
functional causes should be considered. In cases of undiagnosed vaginal bleeding,adequate diagnostic measures should be undertaken.
3. Because progestogens may cause some degree of fluid retention, conditions whichmight be influenced by this factor (e.g., epilepsy, migraine, asthma, cardiac or renaldysfunction) require careful observation.
4. The pathologist should be advised of progesterone therapy when relevant specimensare submitted.
5. Patients who have a history of psychic depression should be carefully observed andthe drug discontinued if the depression recurs to a serious degree.
6. A decrease in glucose tolerance has been observed in a small percentage of patientson estrogen-progestin combination drugs. The mechanism of this decrease is notknown. For this reason, diabetic patients should be carefully observed while receivingprogestin therapy.
Information for PatientsThe product should not be used concurrently with other local intravaginal therapy. If otherlocal intravaginal therapy is to be used concurrently, there should be at least a 6-hourperiod before or after Crinone administration. Small, white globules may appear as avaginal discharge possibly due to gel accumulation, even several days after usage.Drug InteractionsNo drug interactions have been assessed with Crinone.Carcinogenesis, Mutagenesis, Impairment of FertilityNonclinical toxicity studies to determine the potential of Crinone to cause carcinogenicityor mutagenicity have not been performed. The effect of Crinone on fertility has not beenevaluated in animals.Pregnancy Crinone 8% has been used to support embryo implantation and maintain pregnanciesthrough its use as part of ART treatment regimens in two clinical studies (studiesCOL1620-007US and COL1620-F01). In the first study (COL1620-007US), 54 Crinone-treated women had donor oocyte transfer procedures, and clinical pregnancies occurredin 26 women (48%). The outcomes of these 26 pregnancies were as follows: one womanhad an elective termination of pregnancy at 19 weeks due to congenital malformations(omphalocele) associated with a chromosomal abnormality; one woman pregnant withtriplets had an elective termination of her pregnancy; seven women had spontaneous abor-tions; and 17 women delivered 25 apparently normal newborns.In the second study (COL1620-F01), Crinone 8% was used in the luteal phase support ofwomen undergoing in vitro fertilization (“IVF”) procedures. In this multi-center, open-label study, 139 women received Crinone 8% once daily beginning within 24 hours ofembryo transfer and continuing through Day 30 post-transfer.Clinical pregnancies assessed at Day 90 post-transfer were seen in 36 (26%) of women.Thirty-two women (23%) delivered newborns and four women (3%) had spontaneousabortions. Of the 47 newborns delivered, one had a teratoma associated with a cleftpalate; one had respiratory distress syndrome; 44 were apparently normal and one waslost to follow-up.Geriatric UseThe safety and effectiveness in geriatric patients (over age 65) have not been established.Pediatric UseSafety and effectiveness in pediatric patients have not been established.Nursing MothersDetectable amounts of progestins have been identified in the milk of mothers receivingthem. The effect of this on the nursing infant has not been determined.
ADVERSE REACTIONSAssisted Reproductive TechnologyIn a study of 61 women with ovarian failure undergoing a donor oocyte transfer procedurereceiving Crinone 8% twice daily, treatment-emergent adverse events occurring in 5% ormore of the women were: bloating (7%), cramps not otherwise specified (15%), pain (8%),dizziness (5%), headache (13%), nausea (7%), breast pain (13%), moniliasis genital (5%),vaginal discharge (7%), pruritus genital (5%). In a second clinical study of 139 women using Crinone 8% once daily for luteal phase support while undergoing an IVF procedure, treatment-emergent adverse events reported in 5% or greater of the women were: abdominal pain (12%), perineal pain female (17%),headache (17%), constipation (27%), diarrhea (8%), nausea (22%), vomiting (5%), arthral-gia (8%), depression (11%), libido decreased (10%), nervousness (16%), somnolence(27%), breast enlargement (40%), dyspareunia (6%), nocturia (13%). Secondary Amenorrhea In three studies, 127 women with secondary amenorrhea received estrogen replacementtherapy and Crinone 4% or 8% every other day for six doses. Treatment-emergentadverse events during estrogen and Crinone treatment that occurred in 5% or more ofwomen treated with Crinone 4% or Crinone 8% respectively were: abdominal pain (5%,9%), appetite increased (5%, 8%), bloating (13%, 12%), cramps not otherwise specified(19%, 26%), fatigue (21%, 22%), headache (19%, 15%), nausea (8%, 6%), back pain(8%, 3%), myalgia (8%, 0%), depression (19%, 15%), emotional lability (23%, 22%),sleep disorder (18%, 18%), vaginal discharge (11%, 3%), upper respiratory tract infec-tion (5%, 8%), and pruritus genital (2%, 6%).
Additional adverse events reported in women at a frequency of less than 5% in CrinoneART and secondary amenorrhea studies and not listed above include: autonomic nervoussystem–mouth dry, sweating increased; body as a whole–abnormal crying, allergic reaction,allergy, appetite decreased, asthenia, edema, face edema, fever, hot flushes, influenza-likesymptoms, water retention, xerophthalmia; cardiovascular, general–syncope; central andperipheral nervous system–migraine, tremor; gastro-intestinal–dyspepsia, eructation,flatulence, gastritis, toothache; metabolic and nutritional–thirst; musculo-skeletal system–cramps legs, leg pain, skeletal pain; neoplasm–benign cyst; platelet, bleeding & clotting–purpura; psychiatric–aggressive reactions, forgetfulness, insomnia; red blood cell–anemia; reproductive, female–dysmenorrhea, premenstrual tension, vaginal dryness;resistance mechanism–infection, pharyngitis, sinusitis, urinary tract infection; respiratorysystem–asthma, dyspnea, hyperventilation, rhinitis; skin and appendages–acne, pruritus,rash, seborrhea, skin discoloration, skin disorder, urticaria; urinary system–cystitis,dysuria, micturition frequency; vision disorders–conjunctivitis.
OVERDOSAGEThere have been no reports of overdosage with Crinone. In the case of overdosage, how-ever, discontinue Crinone, treat the patient symptomatically, and institute supportivemeasures.As with all prescription drugs, this medicine should be kept out of the reach of children.DOSAGE AND ADMINISTRATIONAssisted Reproductive TechnologyCrinone 8% is administered vaginally at a dose of 90 mg once daily in women who requireprogesterone supplementation. Crinone 8% is administered vaginally at a dose of 90 mgtwice daily in women with partial or complete ovarian failure who require progesteronereplacement. If pregnancy occurs, treatment may be continued until placental autonomyis achieved, up to 10-12 weeks.Secondary AmenorrheaCrinone 4% is administered vaginally every other day up to a total of six doses. Forwomen who fail to respond, a trial of Crinone 8% every other day up to a total of sixdoses may be instituted. It is important to note that a dosage increase from the 4% gel can only be accomplishedby using the 8% gel. Increasing the volume of gel administered does not increase theamount of progesterone absorbed.HOW SUPPLIEDCrinone is available in the following strengths:4% gel (45 mg) in a single use, one piece, disposable, white polyethylene vaginal applica-tor with a twist-off top. Each applicator contains 1.45 g of gel and delivers 1.125 g of gel.NDC 52544-283-24 - 6 Single-use prefilled applicators.8% gel (90 mg) in a single use, one piece, disposable, white polyethylene vaginal applica-tor with a twist-off top. Each applicator contains 1.45 g of gel and delivers 1.125 g of gel.NDC 52544-284-12 - 15 Single-use prefilled applicators.Each applicator is wrapped and sealed in a foil overwrap.Store at 20-25°C (68-77°F). [See USP controlled room temperature.]Rx only
Address medical inquiries to:WATSONMedical CommunicationsP.O. Box 1953Morristown, NJ 07962-1953800-272-5525
Distributed by: Watson Pharma, Inc., Morristown, NJ 07962 USA
Manufactured by: Fleet Laboratories Ltd., Watford, Herts WD18 7JJ UK
Revised: July 2010
9:34 AM

FEbRUARY/MARCH 2012 l VOLUME 4, NUMBER 1 5
From the Editor
As spring approaches, it is exciting to experiencethe new beginnings that a fresh season brings.For me and all my coworkers, this season is
muted by the loss of an esteemed mentor, colleague, andfriend. This journal was developed to highlight the multifac-
eted elements that make OB/GYN extraordinary. Theseelements may be clinical or personal, and they influencehow we structure the care we provide to our patients. In
saying this, it is important to take time to reflect on the people who havemade an impact in shaping our professional careers and defining how we pro-vide patient care.As nurses, our role is to provide quality patient care. The care we provide
defines us as clinicians and makes a permanent impression on our patients. Asnurses advance into clinical management, these responsibilities are expand-ed. Successful managers have the ability to go beyond a generic job descrip-
tion to elevate the quality of care that is applied to all patients and staff, set-ting a bar for a standard of care that defines a medical practice. It is very rareto work in partnership with someone who has completed such a monumen-tal task, and in doing so, made a tremendous impact on the practice of fertil-ity nursing.As an operations manager, Pat Cullen translated her exemplary personal
standard of care to establish the practice standard for patient-centered care.She effectively touched the lives of thousands of patients and staff in her 30+years of fertility nursing service. I am very proud to have had the honor andprivilege of working with one of the leaders in fertility nursing. In tribute toPat, and the many other nursing leaders that our profession has lost, pleaseremember to acknowledge your mentors, validate your coworkers, strive forquality in everyday care, and appreciate the impact that you are making onthe lives of the patients that you touch.
Sue Jasulaitis, RN, MSIn memory of Patricia Cullen, RN BSN
Director of Operations, Fertility Centers of Illinois
CO-EDITOR-IN-CHIEFSue Jasulaitis, RN, MSClinical Research Manager
Fertility Centers of Illinois,
Chicago
CO-EDITOR-IN-CHIEFDebra Moynihan, WHNP-BC,MSNWomen’s Health Nurse
Practitioner
Carolina OB/GYN, Myrtle Beach, SC
Margaret-Rose Agostino, DNP,MSW, RN-BC, IBCLCAssistant Professor
Department of Nursing
Delaware State University
Barbara Alice, RN, APN-C, MSNNursing Manager, IVF
Coordinator
South Jersey Fertility Center
Monica R. Benson, BSN, RNCNurse Manager
Third Party Reproduction,
RMA New Jersey
Melissa B. Brisman, EsqOwner
Reproductive Possibilities, LLC
Surrogate Fund Management,
LLC
Montvale, NJ
Kit Devine, MSN, ARNPAdvanced Nurse Practitioner
Fertility & Endocrine Associates,
Kentucky
Richard P. Dickey, MD, PhDDirector, Reproductive Medicine
Fertility Institute of New
Orleans, LA
Gina Paoletti-Falcone, RN, BSNClinical Services Manager
Freedom Fertility Pharmacy
Byfield, MA
Donielle Farrington, RNCClinical Nursing Manager
Brunswick Hills OB/GYN, NJ
Sandra Fernandez, RPh,PharmDPharmacist
Mandell’s Clinical Pharmacy, NJ
Jennifer Iannaccone, RNCNursing Manager, IVF
Coordinator
IVF New Jersey
Carolyn E. Keating, BSN, RNC, NPPiedmont Reproductive and
Endocrinology Group
Greenville, SC
Cheryl Kilbourne, RNClinical Director
Women and Children Services
Waccmaw Hospital, SC
Juergen Liebermann, PhD,HCLDIVF Laboratory Director
River North Fertility Centers of
Illinois, Chicago
Mary M. Macgregor, RNCIVF Nurse Coordinator
Fertility Institute of New
Orleans, LA
Jill Marchetti, RNDirector, Egg Donor Program
IVF New Jersey
Donna Makris, RN, BSN, IBCLCParent Education Coordinator
OB/GYN, St. Peter’s Medical
Center, NJ
Norah S. Nutter, MSN, WHNP-BC, IBCLCWomen’s Health Nurse
Practitioner
Magnolia OB/GYN
Myrtle Beach, SC
Kutluk Oktay, MD, FACOGDirector, Division of ReproductiveMedicine & Infertility,Department of Obstetrics &Gynecology, New York MedicalCollege; Director, Institute forFertility Preservation, NY
Cyndi Gale Roller, PhD, RN,CNP, CNMProgram Director, Women’s
Health
College of Nursing
Kent State University, OH
Patricia Rucinsky, RN, BSNClinical Nurse Manager
IRMS at Saint Barnabas, NJ
Elizabeth A. Shrader, MSN,APN-CIVF Nurse Coordinator
DVIF&G
Marlton, NJ
Christopher S. Sipe, MDOB/GYN & Reproductive
Endocrinology
Fertility Centers of Illinois,
Chicago
Dale C. Smith, RN, MPH, MSNNFP Nursing Supervisor
DHEC Region 6
Conway, SC
Harvey J. Stern, MD, PhDDirector, Reproductive Genetics
Genetics & IVF Institute
Fairfax, VA
Kriston Ward, RN, MS, NP-CStrong Fertility Center
University of Rochester Medical
Center, Rochester, NY
Joan Zaccardi, MS, DrNPAdministrative Practice
Manager
Urogynecology Arts of New
Jersey
Editorial Board

6 FEbRUARY/MARCH 2012 l VOLUME 4, NUMBER 1
In This Issue
Adding Everolimus...Continued from page 1
CTRC-AACR SABCS Annual Meeting
NEw who guIDElINEs
Which guidelines should fertility clinics follow when undertaking semen analysis?
INfERtIlIty uPDAtEs
Viability of single-embryo transfer as methodto reduce multiple birth rates
Do low AMH levels rule out in vitrofertilization as an option?
PAtIENt AwARENEss AND
IDENtIfIcAtIoN
One fertility center’s approach to testing
NoNsuRgIcAl INtERVENtIoN
A look at pelvic organ prolapse
AsRM ANNuAl MEEtINg
Low-intensity IVF: how does it stack up?
PUBLISHING STAFF
PublisherRussell [email protected]
Editorial DirectorKristin [email protected]
Managing EditorJim [email protected]
Editorial Assistant Jennifer Brandt
Senior Production ManagerMarie RS Borrelli
Quality Control DirectorBarbara Marino
Business ManagerBlanche Marchitto
Editorial Contact:Telephone: 732-992-1536Fax: 732-656-7938
MISSION STATEMENTThe OB/GYN Nurse-NP/PA is the officialpublication of the American Academy ofOB/GYN and Infertility Nurses. The OB/GYNNurse-NP/PA provides practical, authoritative,cutting-edge information on the physiologic,medical, and psychological aspects of women’shealth, focusing on the role of the OB/GYNpractitioner, including nurses, NPs, and PAs, inpatient care. Our journal offers a forum fornurses, NPs, PAs, administrators, researchers,and all others involved in OB/GYN andwomen’s health to discuss the entire scope ofcurrent and emerging diagnostic and therapeuticoptions, as well as counseling and patientfollow-up for women throughout theirreproductive years and beyond. Written bynurses for nurses, The OB/GYN Nurse-NP/PApromotes peer-to-peer collaboration among allnursing professionals toward the advancement ofintegrated services for optimal delivery ofpatient care and offers continuing education forall nurses, NPs, and PAs involved in theseinterrelated fields of women’s health.
The OB/GYN Nurse, ISSN 2153-6562 (print);ISSN 2153-6546 (online), is published byNovellus Healthcare Communications, LLC,241 Forsgate Drive, Suite 205D, Monroe Twp,NJ 08831. Copyright ©2012 by NovellusHealthcare Communications, LLC. All rightsreserved. The OB/GYN Nurse is a trademark ofNovellus Healthcare Communica tions, LLC.No part of this publication may be reproducedor transmitted in any form or by any means nowor hereafter known, electronic or mechanical,including photocopy, recording, or anyinformational storage and retrieval system,without written permission from the Publisher.Printed in the United States of America.
The ideas and opinions expressed in TheOB/GYN Nurse do not necessarily reflect thoseof the Editorial Board, the Editors, or thePublisher. Publication of an advertisement orother product mentioned in The OB/GYN Nurseshould not be construed as an endorsement ofthe product or the manufacturer’s claims.Readers are encouraged to contact themanufacturers about any features or limitationsof products mentioned. Neither the Editors northe Publisher assume any responsibility for anyinjury and/or damage to persons or propertyarising out of or related to any use of thematerial mentioned in this publication.
SUBSCRIPTIONS/CHANGE OFADDRESS should be directed to CIRCULATION DIRECTOR, The OB/GYNNurse, 241 Forsgate Drive, Suite 205D,Monroe Twp, NJ 08831; Fax: 732-656-7938.
WWW.THEOBGYNNURSE.COM
receptor (ER)-positive breast cancerwhose disease had become refractory tohormonal therapy. “The addition of everolimus in ad -
vanced breast cancer could represent aparadigm shift in the management of this patient population,” said leadinvestigator Gabriel Hortobagyi, MD,chair of Breast Medical Oncology, TheUniversity of Texas, MD AndersonCancer Center, Houston, at the 2011CTRC-AACR San Antonio BreastCancer Symposium. Nearly all ER-positive patients with
advanced cancer will develop resistanceto hormonal therapies. Resistance tohormonal therapy in breast cancer hasbeen associated with overactivation ofthe mTOR pathway. Everolimus targetsthe mTOR pathway, interfering withtumor cell proliferation, angiogenesis,and cell metabolism. “Everolimus is the first treatment to
significantly enhance the efficacy ofhormonal therapy in this patient popu-lation, where this remains a significantunmet need,” Dr Hortobagyi noted.
bolERo DetailsThe new findings represent an addi-
tional 6 months of patient follow-upfrom the data first presented at theEuropean Multidisciplinary CancerCongress in September 2011, garneringmuch attention. The updated analysispresented in San Antonio showed thattreatment with everolimus plus hormon-al therapy more than doubled PFS, from3.2 months with exemestane alone to 7.4months with the addition of everolimus,representing a highly significant 56%reduction (P <1 × 10-16) in the risk of
progression. “While this analysis wasdone with local tumor assessment,another assessment by central inde-pendent review found even greater benefit, with PFS of 11.0 months versus4.1 months, a 64% risk reduction (P <1 × 10-16),” Dr Hortobagyi reported. In remarking on the robustness of
the findings at a media briefing, DrHortobagyi noted that the prolongation
of progression far exceeded the investi-gators’ expectations. “The study de mo -nstrated not the 26% reduction in pro-gression, as we had expected, but a 56%reduction in progression events, with aP value for which I don’t have enoughfingers to count.” Disease-free survival
rates at 1 year were 31% in the combi-nation arm versus 10% in the exemes-tane-alone arm. Side effects were consistent with
those previously reported with ever -olimus. The most common grade 3 orgrade 4 adverse events were stomati-tis, anemia, hyperglycemia, dyspnea,fatigue, and pneumonitis, all occurringin <10% of patients receiving the com-bination. The addition of everolimusdid not impact the patients’ quality oflife, according to Global Health Scores.As of December 2011, deaths had
occurred in 29.3% of the placebo armand 23.1% of the everolimus arm. Themanufacturer is planning a regulatorysubmission for everolimus based on theBOLERO-2 results. n
“Everolimus is the firsttreatment to significantlyenhance the efficacy ofhormonal therapy in thispatient population….Thestudy demonstrated notthe 26% reduction inprogression, as we hadexpected, but a 56%reduction in progressionevents, with a P value forwhich I don’t have enoughfingers to count.”
—Gabriel Hortobagyi, MD
AT A GLANCE
‰Nearly all ER-positive patientswith advanced cancer will developresistance to hormonal therapies
‰The addition of everolimus tohormonal therapy more thandoubled PFS, from 3.2 monthswith exemestane alone to 7.4months
‰These new results demonstrateda 56% reduction in disease pro-gression, nearly twice theexpected rate
‰At 1 year, disease-free survivalrate is 31% in the everolimus-exemestane combination armversus 10% in the exemestanealone arm

FEbRUARY/MARCH 2012 l VOLUME 4, NUMBER 1 7
ASRM Annual Meeting
Orlando, FL – Low-intensity in vitro fer-tilization (IVF), a milder ovarian stimu-lation that is gaining in popularity, sig-nificantly reduces the chance ofpregnancy, according to data from apilot study by Norbert Gleicher, MD.Low-intensity IVF, also known as
Eco-IVF, is allegedly more cost-effectiveand patient friendly while hypothetical-ly producing better embryo quality, sayits advocates. But in a poster presenta-tion delivered at the 2011 meeting ofthe American Society for ReproductiveMedicine, Dr Gleicher offered datashowing that fewer cryopreservedembryos were produced, resulting infewer live births, using low-intensityIVF compared with standard IVF.Low-intensity IVF has never been
compared with standard IVF in a nonin-feriority trial. Based on the lower oocytenumbers with mild ovarian stimulation,“one has to conclude that cumulativepregnancy chances from low-intensityIVF have to be lower,” according to DrGleicher, medical director of the Centerfor Human Reproduction, New YorkCity.To investigate whether low-intensity
IVF offered compensatory benefits, DrGleicher and colleagues studied 14 low-intensity IVF and 14 age-matched stan-dard intensity IVF cycles in womenyounger than 38 years with normal ovar-ian reserve. Women in low-intensitycycles were stimulated with clomiphenecitrate, 100 mg daily on days 3 to 7, aug-mented by human menopausalgonadotropin (hMG), 10,000 IU, untilovulation induction with human chori-onic gonadotropin (hCG), 10,000 IU.Women in standard IVF cycles werestimulated with hMG, 10,000 IU, afterdownregulation with agonist (leuprolideacetate, luteal start, 1 mg once dailyuntil the suppression phase, followed by0.5 mg daily, until induction withhCG).Patients using low-intensity IVF used
less gonadotropin and had fewer oocytesretrieved (2.7 vs 15.6) resulting in fewercryopreserved embryos (0 vs 4.7) com-pared with women using standard IVF. With an identical number of embryos
transferred, after adjusting for age,patients using standard IVF demonstrat-ed 7-fold better odds for pregnancy anda cumulative pregnancy rate that wasmore than 6 times higher than thatachieved in patients using low-intensityIVF cycles. There were 10 live birthsamong women using standard IVF com-pared with 5 among those using low-intensity IVF. The costs per live birth (cumulative)
were similar between the 2 groups:
$23,100 when low-intensity IVF cycleswere used and $20,333 when standardIVF cycles were used. The significantlyreduced chances of pregnancy with low-intensity IVF eliminated the potentialcost advantages, said Dr Gleicher. “Even
with normal ovarian reserve, therefore,low-intensity IVF can be considered nei-ther patient friendly nor cost-effective.” With diminished ovarian reserve,
low-intensity IVF should be even lesssuccessful, he indicated, even though it
is in this population that low-intensityIVF is used most frequently. “Low-inten-sity currently lacks clinical and econom-ic foundations, and therefore should beoffered only under experimental studyconditions,” Dr Gleicher concluded. n
Embryo Donation Services Center
This material was developed and distributed with funding support from the U.S. Department of Health and Human Services under grant #6 EAAPA111017-01-01.The statements expressed are those of the Embryo
Donation Services Center and do not necessarily represent the views of the Department.
INFERTILITY PROFESSIONALS:
FREE ANSWERS TO
EMBRYO DONATION’SLIFE-CHANGING QUESTIONSFOR YOU AND YOUR PATIENTS
www.embryocenter.org(719)213-7680
low-Intensity IVf Reduces Pregnancy chancesby Wayne Kuznar

8 FEbRUARY/MARCH 2012 l VOLUME 4, NUMBER 1
Guidelines
Estradiol Route...Continued from page 1
midluteal phase of the previous cycle.Serum estradiol levels were monitoredand the doses of estradiol were adjustedaccordingly.Of these 479 women, 37 received oral
estradiol only (group A), 244 receivedtransdermal estradiol only (group B),and 198 started on transdermal but hadoral estradiol added to achieve targetedestradiol levels during the FET cycle(group C). Intramuscular progesteronewas started if the endometrial lining was7 mm or greater. If the beta humanchorionic gonadotropin was positive,estradiol and progesterone supplemen-
tation were continued until 12 weeks’gestation.The mean age in each group was
about 35 years. There were no signifi-cant differences between the 3 groups inday 3 follicle stimulating hormone or inthe number of patients undergoingintracytoplasmic sperm injection. Meanbody mass index (BMI) was significant-ly greater in group A (30.2 kg/m2) com-pared with group B (25.1 kg/m2) andgroup C (27.9 kg/m2).The number of embryos transferred
and the implantation rates were not sig-nificantly different between the groups.
The clinical pregnancy rates were not
significantly different between the
groups: 56.8% for group A; 50.0% forgroup B; 51.0% for group C. The ongo-ing pregnancy rates were also not signif-icantly different: 48.6% for group A;41.0% for group B; 42.9% for group C.There were no differences in the clini-cal or ongoing pregnancy rates whencontrolling for BMI.While the route of estradiol adminis-
tration does not appear to affect preg-nancy rates in FET cycles, the authorsurge monitoring of estradiol levels, “asincreasing the dose or adding a secondform of administration maintains preg-nancy rates.” n
New who guidelines for semen Analysis Not up tothe task, Expert contends
Toronto, Ontario – Which guidelinesshould fertility clinics follow whenundertaking semen analysis? That ques-tion is difficult to answer now that twocompeting systems have been devel-oped. They are the fifth edition of theWorld Health Or ganization’s manual forsemen analysis, released last year andreferred to as ‘WHO5’, and the semenanalysis recommendations of theEuropean Society of Human Repro -duction & Endocrinology (ESHRE)Andrology Special Interest GroupEducation Subcommittee, which werefirst presented in a semen-analysiscourse in June 2011.At the Canadian Fertility and
Andrology Society’s 2011 AnnualMeeting, David Mortimer, PhD, aninfertility-clinic consultant and one ofthe authors of the ESHRE guidelines,described the advantages of the ESHREapproach over WHO5. Paul Claman,MD, a professor of obstetrics and gyne-cology at the University of Ottawa whoattended Dr. Mortimer’s presentationagreed with most of his criticisms ofWHO5.“As a clinician I can’t see how
WHO5 helps in the evaluation of theinfertile couple. It defines normal spermparameters based on statistical variancesin a population of fertile men, whichdoes not help to define which men areless fertile than others,” Dr Claman said.“It is sad that this most respected healthauthority has not considered the practi-cal clinical problem of evaluating theinfertile couple when publishing their
updated heretofore important laboratorymanual for the evaluation of semen.”WHO5 contains numerous inconsis-
tencies, errors, and unjustified compli-cations relating to established tech-niques that unnecessarily increaseworkload without improving accuracyor precision in the results obtained, Dr Mortimer, President of OozoaBiomedical Inc, West Vancouver, toldmeeting attendees. He added, “In addi-tion, the reduction of the differentialmotility assessment to only three cate-gories by eliminating the assessment ofpercentage rapid progressive, is a back-ward step that eliminates this biologi-cally, and hence clinically, importantpiece of information from basic semenanalysis.” Dr. Mortimer also said thatalmost immediately after WHO5 waspublished it was “widely criticized….For example, two of the members of thecommittee of experts who wrote therevised WHO guidelines wrote refuta-tions of parts of it.”One of the major problems in
WHO5, according to Dr. Mortimer, isthat it abandons the distinctionbetween grade A sperm, which swimforward fast in a straight line, and gradeB sperm, which swim forward but eitherslowly or along a curved or crookedpath. The reason given for this decisionby the WHO committee is that grade Ais too subjective and cannot be assessedreliably by eye. However, Dr. Mortimercontends data show that distinction ofgrade A sperm from others can belearned rapidly by using a standardized
technique and that many in the fieldagree this is an essential factor in semenanalysis.Other problems and errors in WHO5
identified by Dr Mortimer are that ituses 4% ‘normal’ forms as a referencelimit for sperm morphology; uses mis-leading terminology such as oligo-
zoospermia, “which is not a diagnosis”;and provides multiple methods for someassessments, which “can cause confu-sion.” Dr Mortimer also said thatWHO5 presents protocols in a nonlin-ear way; uses “illogical, imprecise, andarbitrary” criteria for sperm vitality;requires unnecessary extra work, such asduplicates for vitality assessments and a
new, laborious method for low-concen-tration samples; and presents problemsin its sperm preparation method,including allowing centrifugal washingfor “good-quality” semen samples,“although such samples cannot be iden-tified reliably until after the sperm pro-cessing has commenced.” In addition,the reference ranges for various parts ofthe semen analysis do not take intoaccount individual, biological, andmethodological variability and ignorethe fact that “establishing clear cutofflimits is impossible” due to factors suchas overlaps in results between groups ofmen with and without reduced fertilitypotential, said Dr. Mortimer.In contrast, the textbook for the
ESHRE semen-analysis course providesconsensus-based, “detailed, logical,unambiguous SOP-type methodsdesigned to minimize technical errors,avoid unnecessary effort, and facilitatequality control,” according to DrMortimer. These methods include“well-defined criteria for ‘normality’ insperm morphology and the use of spermfunctional analysis in managing infer-tile couples,” the latter of which he pioneered.“For semen analysis to be useful,
robust validated methods must beemployed by trained, competent per-sonnel in order to provide accurateresults,” concluded Dr Mortimer.“WHO5 has significant limitations inproviding reliable methods for perform-ing such testing efficiently and effec-tively.” n
“As a clinician I can’t seehow WHO5 helps in the evaluation of the infertile couple. It defines normalsperm parameters basedon statistical variancesin a population of fertilemen, which does not helpto define which men areless fertile than others.”
—Paul Claman, MD
Serum estradiol levelswere monitored andthe doses of estradiolwere adjustedaccordingly.

FEbRUARY/MARCH 2012 l VOLUME 4, NUMBER 1 9
CTRC-AACR SABCS Annual Meeting
Dr Baselga emphasized. Pertuzumab is designed to work in
combination with trastuzumab as adual blockade of the HER2 growth fac-tor. Both drugs are monoclonal anti-bodies that bind to the HER2 receptorprotein in different regions.Pertuzumab prevents the receptor fromlinking to HER3, which stops the for-mation of a “dimer” that couldenhance tumor growth. “Pertuzumab is the first in a new
class of drugs called ‘dimerizationinhibitors,’ and its combination withtrastuzumab produces dual HER2blockade, shutting down differentmechanisms responsible for HER2 sig-naling,” Dr Baselga said.
the clEoPAtRA study CLEOPATRA randomly assigned
808 postmenopausal women withmetastatic breast cancer, but withoutprevious treatment for metastatic dis-ease, to trastuzumab and docetaxelchemotherapy with the addition ofeither pertuzumab or placebo. The PFSwas 18.5 months for patients receivingpertuzumab along with trastuzumab-
docetaxel compared with 12.4 monthsfor trastuzumab-docetaxel alone, a 38%reduction in the risk of progression.
Adding pertuzumab to the combinationalso raised the objective response rate to80.2% compared with 69.3% fortrastuzumab-docetaxel alone.Although survival outcomes are not
mature, 69 deaths were reported amongthe 402 patients who were treated withthe 3-drug regimen versus 96 deathsamong the 406 patients receiving the 2-drug regimen; this amounts to a 36%reduction in mortality.The 3-drug combination was
“remarkably safe and well tolerated,”Dr Baselga noted, reporting that per-tuzumab added only minimal toxicity.Enrollment is already underway in a
new double-blind, randomized clinicaltrial, APHINITY, that will test the useof pertuzumab as adjuvant treatmentfor early-stage HER2-positive breastcancer – “the setting in which you canreally cure patients,” Dr Baselga noted. “We are looking forward to getting
pertuzumab approved as soon as possi-ble. The sooner the better,” Dr Baselgacommented. Genentech recently sub-mitted a biologic license applicationfor pertuzumab in HER2-positivemetastatic breast cancer.Lisa Carey, MD, medical director,
the University of North CarolinaBreast Cancer Center, Chapel Hill,moderated a press conference andcommented that findings from the
BOLERO-2 study that involvedanother breast cancer drug,everolimus, extend the findings fromneoadjuvant studies and smaller, lessdefinitive trials “that dual HER2blockade has a marked advantage oversingle blockade of HER2. The chal-lenge will be figuring out whichpatients need both these drugs.” n
Meredith Provost, PhD, MD, at the2011 meeting of the American Societyfor Reproduction Medicine.In her study, retrieval efficiency of
oocytes per follicle was equivalent orbetter with leuprolide acetate comparedwith hCG. The use of GnRH agonists asa method to trigger ovulation has gainedfavor in recent years and can “virtuallyeliminate the risk of ovarian hyperstim-ulation syndrome,” said Dr Provost,Department of Obstetrics andGynecology, Banner Good SamaritanMedical Center, Arizona ReproductiveMedicine Specialists, Phoenix. Originalconcerns about a lower pregnancy rateassociated with the use of GnRH ago-nists have been reversed with aggressiveluteal phase support. Although, accord-ing to Dr Provost, “There still remainsome concerns about lower egg retrievalrate efficiencies.”Dr Provost reviewed 820 cycles (312
IVF and 506 intracytoplasmic sperminjection [ICSI]) with final oocyte mat-uration triggered using either hCG at a
dose of 5,000 IU or 10,000 IU orleuprolide acetate at a dose of 2 mg or 4mg in the evening followed by an injec-tion the next morning. All patientswere on an antagonist protocol andreceived follicle stimulating hormone,the starting dose of which was deter-mined by individual criteria. Ma -turation rate, fertilization rate (IVF andICSI), and retrieval efficiency were theprimary outcomes. Retrieval efficiencywas defined in 2 ways: oocytesretrieved/follicle >15 mm (efficiency I)and oocytes retrieved/estradiol level(efficiency II).“The criteria to use leuprolide acetate
varied over time to adapt to changingclinical conditions,” Dr Provost said,with the current criteria being an estra-diol level in excess of 3,500 pg/mL andthe total number of follicles greaterthan 11 mm ≥20. The only demographic factors that
predicted outcomes were gravida,which predicted retrieval efficiency I,and estradiol, which predicted retrieval
efficiency II. The retrieval efficiencywas not different between the leupro-lide acetate and hCG groups.Leuprolide acetate, 4 mg, did performsignificantly better on the outcomes ofICSI maturation rate and ICSI fertiliza-tion rate compared with hCG at eitherdose, Dr Provost reported.The IVF fertilization rate and the
number of oocyte embryos transferred
and retrieved were also similar betweenthe groups. “None of our LA [leupro-lide acetate] cycles had no oocytesretrieved; there were oocytes retrievedin every cycle that we did,” Dr. Provostsaid. The better safety profile of aGnRH agonist with respect to OHSSargues for consideration of leuprolideacetate instead of a traditional hCGtrigger, she concluded. n
Dual hER2 blockade with Pertuzumab...Continued from page 1
“Pertuzumab is the first ina new class of drugscalled ‘dimerizationinhibitors,’ and itscombination withtrastuzumab producesdual HER2 blockade,shutting down differentmechanisms responsiblefor HER2 signaling.”
—Jose Baselga, MD, PhD
AT A GLANCE
‰Adding pertuzumab to a combi-nation of trastuzumab and doc-etaxel chemotherapy extendedPFS by a median of 6.1 months
‰Pertuzumab is the first in a newclass of drugs called “dimeriza-tion inhibitors”; its combinationwith trastuzumab produces dualHER2 blockade
‰ In the CLEOPATRA phase 3trial, the 3-drug regimen reducedmortality by 36%
‰Dual HER2 blockade demon-strated a significant advantageover a single blockade
consider gnRh Agonist...Continued from page 1
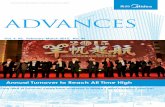
Table Comparison of Leuprolide Acetate and Human Chorionic Gonadotropin
Outcome LA 2 mg LA 4 mg hCG 5,000 hCG 10,000Retrieval efficiency I 1.18 1.20 1.25 1.30Retrieval efficiency II 5.54 6.30 7.74 7.20ICSI maturation rate 77.8 82.3 78.3 77.2ICSI fertilization rate 76.5 76.2 73.1 70.8IVF fertilization rate 65.2 65.9 63.9 66.6Embryos/oocyte 0.33 0.34 0.33 0.30
LA indicates leuprolide acetate; hCG, human chorionic gonadotropin; retrieval efficiencyI, oocytes/follicle >15 mm; retrieval efficiency II, oocytes retrieved/estradiol level; ICSI,intracytoplasmic sperm injection; IVF, in vitro fertilization.
ASRM Annual Meeting



Crinone® 4% Crinone® 8%(progesterone gel)
For vaginal use only. Rx only
BRIEF SUMMARYFor full prescribing information, see package insert. INDICATIONS AND USAGEAssisted Reproductive TechnologyCrinone 8% is indicated for progesterone supplementation or replacement as part of an Assisted Reproductive Technology (“ART”) treatment for infertile women withprogesterone deficiency.Secondary AmenorrheaCrinone 4% is indicated for the treatment of secondary amenorrhea. Crinone 8% is indi-cated for use in women who have failed to respond to treatment with Crinone 4%.CONTRAINDICATIONSCrinone should not be used in individuals with any of the following conditions: knownsensitivity to Crinone (progesterone or any of the other ingredients); undiagnosed vaginalbleeding; liver dysfunction or disease; known or suspected malignancy of the breast orgenital organs; missed abortion; active thrombophlebitis or thromboembolic disorders,or a history of hormone-associated thrombophlebitis or thromboembolic disorders.WARNINGSThe physician should be alert to the earliest manifestations of thrombotic disorders (throm-bophlebitis, cerebrovascular disorders, pulmonary embolism, and retinal thrombosis).Should any of these occur or be suspected, the drug should be discontinued immediately. Progesterone and progestins have been used to prevent miscarriage in women with a his-tory of recurrent spontaneous pregnancy losses. No adequate evidence is available to showthat they are effective for this purpose.PRECAUTIONSGeneral1. The pretreatment physical examination should include special reference to breast and
pelvic organs, as well as Papanicolaou smear.2. In cases of breakthrough bleeding, as in all cases of irregular vaginal bleeding, non-
functional causes should be considered. In cases of undiagnosed vaginal bleeding,adequate diagnostic measures should be undertaken.
3. Because progestogens may cause some degree of fluid retention, conditions whichmight be influenced by this factor (e.g., epilepsy, migraine, asthma, cardiac or renaldysfunction) require careful observation.
4. The pathologist should be advised of progesterone therapy when relevant specimensare submitted.
5. Patients who have a history of psychic depression should be carefully observed andthe drug discontinued if the depression recurs to a serious degree.
6. A decrease in glucose tolerance has been observed in a small percentage of patientson estrogen-progestin combination drugs. The mechanism of this decrease is notknown. For this reason, diabetic patients should be carefully observed while receivingprogestin therapy.
Information for PatientsThe product should not be used concurrently with other local intravaginal therapy. If otherlocal intravaginal therapy is to be used concurrently, there should be at least a 6-hourperiod before or after Crinone administration. Small, white globules may appear as avaginal discharge possibly due to gel accumulation, even several days after usage.Drug InteractionsNo drug interactions have been assessed with Crinone.Carcinogenesis, Mutagenesis, Impairment of FertilityNonclinical toxicity studies to determine the potential of Crinone to cause carcinogenicityor mutagenicity have not been performed. The effect of Crinone on fertility has not beenevaluated in animals.Pregnancy Crinone 8% has been used to support embryo implantation and maintain pregnanciesthrough its use as part of ART treatment regimens in two clinical studies (studiesCOL1620-007US and COL1620-F01). In the first study (COL1620-007US), 54 Crinone-treated women had donor oocyte transfer procedures, and clinical pregnancies occurredin 26 women (48%). The outcomes of these 26 pregnancies were as follows: one womanhad an elective termination of pregnancy at 19 weeks due to congenital malformations(omphalocele) associated with a chromosomal abnormality; one woman pregnant withtriplets had an elective termination of her pregnancy; seven women had spontaneous abor-tions; and 17 women delivered 25 apparently normal newborns.In the second study (COL1620-F01), Crinone 8% was used in the luteal phase support ofwomen undergoing in vitro fertilization (“IVF”) procedures. In this multi-center, open-label study, 139 women received Crinone 8% once daily beginning within 24 hours ofembryo transfer and continuing through Day 30 post-transfer.Clinical pregnancies assessed at Day 90 post-transfer were seen in 36 (26%) of women.Thirty-two women (23%) delivered newborns and four women (3%) had spontaneousabortions. Of the 47 newborns delivered, one had a teratoma associated with a cleftpalate; one had respiratory distress syndrome; 44 were apparently normal and one waslost to follow-up.Geriatric UseThe safety and effectiveness in geriatric patients (over age 65) have not been established.Pediatric UseSafety and effectiveness in pediatric patients have not been established.Nursing MothersDetectable amounts of progestins have been identified in the milk of mothers receivingthem. The effect of this on the nursing infant has not been determined.
ADVERSE REACTIONSAssisted Reproductive TechnologyIn a study of 61 women with ovarian failure undergoing a donor oocyte transfer procedurereceiving Crinone 8% twice daily, treatment-emergent adverse events occurring in 5% ormore of the women were: bloating (7%), cramps not otherwise specified (15%), pain (8%),dizziness (5%), headache (13%), nausea (7%), breast pain (13%), moniliasis genital (5%),vaginal discharge (7%), pruritus genital (5%). In a second clinical study of 139 women using Crinone 8% once daily for luteal phase support while undergoing an IVF procedure, treatment-emergent adverse events reported in 5% or greater of the women were: abdominal pain (12%), perineal pain female (17%),headache (17%), constipation (27%), diarrhea (8%), nausea (22%), vomiting (5%), arthral-gia (8%), depression (11%), libido decreased (10%), nervousness (16%), somnolence(27%), breast enlargement (40%), dyspareunia (6%), nocturia (13%). Secondary Amenorrhea In three studies, 127 women with secondary amenorrhea received estrogen replacementtherapy and Crinone 4% or 8% every other day for six doses. Treatment-emergentadverse events during estrogen and Crinone treatment that occurred in 5% or more ofwomen treated with Crinone 4% or Crinone 8% respectively were: abdominal pain (5%,9%), appetite increased (5%, 8%), bloating (13%, 12%), cramps not otherwise specified(19%, 26%), fatigue (21%, 22%), headache (19%, 15%), nausea (8%, 6%), back pain(8%, 3%), myalgia (8%, 0%), depression (19%, 15%), emotional lability (23%, 22%),sleep disorder (18%, 18%), vaginal discharge (11%, 3%), upper respiratory tract infec-tion (5%, 8%), and pruritus genital (2%, 6%).
Additional adverse events reported in women at a frequency of less than 5% in CrinoneART and secondary amenorrhea studies and not listed above include: autonomic nervoussystem–mouth dry, sweating increased; body as a whole–abnormal crying, allergic reaction,allergy, appetite decreased, asthenia, edema, face edema, fever, hot flushes, influenza-likesymptoms, water retention, xerophthalmia; cardiovascular, general–syncope; central andperipheral nervous system–migraine, tremor; gastro-intestinal–dyspepsia, eructation,flatulence, gastritis, toothache; metabolic and nutritional–thirst; musculo-skeletal system–cramps legs, leg pain, skeletal pain; neoplasm–benign cyst; platelet, bleeding & clotting–purpura; psychiatric–aggressive reactions, forgetfulness, insomnia; red blood cell–anemia; reproductive, female–dysmenorrhea, premenstrual tension, vaginal dryness;resistance mechanism–infection, pharyngitis, sinusitis, urinary tract infection; respiratorysystem–asthma, dyspnea, hyperventilation, rhinitis; skin and appendages–acne, pruritus,rash, seborrhea, skin discoloration, skin disorder, urticaria; urinary system–cystitis,dysuria, micturition frequency; vision disorders–conjunctivitis.
OVERDOSAGEThere have been no reports of overdosage with Crinone. In the case of overdosage, how-ever, discontinue Crinone, treat the patient symptomatically, and institute supportivemeasures.As with all prescription drugs, this medicine should be kept out of the reach of children.DOSAGE AND ADMINISTRATIONAssisted Reproductive TechnologyCrinone 8% is administered vaginally at a dose of 90 mg once daily in women who requireprogesterone supplementation. Crinone 8% is administered vaginally at a dose of 90 mgtwice daily in women with partial or complete ovarian failure who require progesteronereplacement. If pregnancy occurs, treatment may be continued until placental autonomyis achieved, up to 10-12 weeks.Secondary AmenorrheaCrinone 4% is administered vaginally every other day up to a total of six doses. Forwomen who fail to respond, a trial of Crinone 8% every other day up to a total of sixdoses may be instituted. It is important to note that a dosage increase from the 4% gel can only be accomplishedby using the 8% gel. Increasing the volume of gel administered does not increase theamount of progesterone absorbed.HOW SUPPLIEDCrinone is available in the following strengths:4% gel (45 mg) in a single use, one piece, disposable, white polyethylene vaginal applica-tor with a twist-off top. Each applicator contains 1.45 g of gel and delivers 1.125 g of gel.NDC 52544-283-24 - 6 Single-use prefilled applicators.8% gel (90 mg) in a single use, one piece, disposable, white polyethylene vaginal applica-tor with a twist-off top. Each applicator contains 1.45 g of gel and delivers 1.125 g of gel.NDC 52544-284-12 - 15 Single-use prefilled applicators.Each applicator is wrapped and sealed in a foil overwrap.Store at 20-25°C (68-77°F). [See USP controlled room temperature.]Rx only
Address medical inquiries to:WATSONMedical CommunicationsP.O. Box 1953Morristown, NJ 07962-1953800-272-5525
Distributed by: Watson Pharma, Inc., Morristown, NJ 07962 USA
Manufactured by: Fleet Laboratories Ltd., Watford, Herts WD18 7JJ UK
Revised: July 2010
9:34 AM

FEbRUARY/MARCH 2012 l VOLUME 4, NUMBER 1 13
Infertility Updates
Toronto, Ontario – Allowing couples tohave only single-embryo transfer (SET)during each cycle of in vitro fertilization(IVF) can be a viable policy, accordingto a study at the Center for AdvancedReproductive Care, University of IowaCarver College of Medicine, Iowa City,Iowa. Data released at the CanadianFertility and Andrology Society’s 2011annual meeting, and in press in Fertilityand Sterility, show that the live-birth ratehas slightly increased since this policywas implemented on June 1, 2004,whereas multiple-birth rates havedecreased by 50%.After implementation of mandatory
single-embryo transfer (mSET) at thecenter, live-birth rates increased from51.1% to 55.9% and multiple-birth ratesfell from 34.8% to 17.5%. The centermandates SET for women who are thebest candidates for successful IVF,including those who are younger than 38years and have never failed IVF.“Insurance companies are now giving
us a bonus – they have for a few years –because we’re costing them less moneysince we’ve lowered our rates of twinsand triplets, and they’re associated withhigher levels of morbidity,” explainedGinny Ryan, MD, MA, assistant profes-sor, Division of Reproductive Endo -
crinology and Infertility, University ofIowa Carver College of Medicine.However, Carol Wheeler, MD,
Center for Reproduction and Infertility,Women & Infants, Warren AlpertMedical School of Brown University,Providence, Rhode Island, commentedthat it is unlikely this policy will beimplemented in other centers. “It is a
very hard sell for patients; if they thinkthere’s even a 1% higher chance of get-ting pregnant by having 2 embryos trans-ferred rather than 1 – even if the data
show that’s not correct – they’re going towant 2,” said Dr Wheeler. “I can’t imag-ine mSET will spread in this country.…It is a very competitive field, and whilein Iowa there aren’t a lot of other clinics,in other states there are, so people willvote with their feet.”Although the University of Iowa is 1
of only 2 fertility clinics in the state, DrRyan and her colleagues are hoping thepolicy will proliferate. “It is one strategyto stop the epidemic of iatrogenic multi-ple pregnancies,” she said, and added,“An effort has to be made to lobby localinsurers to improve coverage based onmSET and the associated reduction incosts. I think it would be great if insur-ance companies said to patients, ‘We willfund your IVF if you go to this clinicbecause they follow best practices andhave mSET.’”Meanwhile, Dr Ryan is hoping the
data might bring some other clinics onboard. Iowa is one of the majority ofstates in the US where insurance cover-age is not mandated for IVF.In July 2004 the clinic brought mSET
into effect for women who:• Are under age 38 and using autolo-gous oocytes in a fresh embryo transfer
• Have no history of failed IVF at theUniversity of Iowa
• Have at least 6 blastocysts that are fitto be cultured
• Have at least 1 ‘good’ or ‘excellent’blastocyst on the day of embryo trans-ferThe women who meet these criteria
are given significant education about thebenefits of SET and the risks associatedwith having twins.Dr Ryan and her colleagues compared
the 5-year period prior to mSET imple-mentation, June 1, 1999, to May 31,2004, to the 5-year period immediatelyafter, June 1, 2004, to May 31, 2009.They found their clinic’s volume was notsignificantly changed, with 2412 cyclesin the first time period and 2389 in thesecond. Overall, they performed SET in33.8% of cycles in women under 38 yearsof age. The live-birth rate significantlyincreased, despite a decrease in the aver-age number of embryos transferred from2.10 to 1.65. Furthermore, the multiple-birth rate dropped drastically.The team also surveyed 462 patients in
a separate study (Fertility and Sterility, inpress). They found 94% of the patientssupported the mSET policy. More over,95% felt they had the “right amount ofinput” in their IVF treatment, and 87%said they believed they had the correctnumber of embryos transferred. n
single-Embryo transfer Associated with higher birthRates and fewer Multiple birthsBut single-center data appear unlikely to cause policy to spreadBy Rosemary Frei, MSc
“Insurance companies arenow giving us a bonus –they have for a few years– because we’re costingthem less money sincewe’ve lowered our ratesof twins and triplets, andthey’re associated withhigher levels of morbidity.”
—Ginny Ryan, MD, MA
Orlando, FL – An extremely low levelof anti-Müllerian hormone (AMH) isnot an absolute contraindication for invitro fertilization (IVF). Data obtainedfrom women referred to the Center forHuman Reproduction, New York City,for an evaluation for infertility revealedclinical pregnancies and live births inwomen with AMH levels ≤0.4 ng/mL,found Andrea Weghofer, MD, PhD.The data confirm the Center’s prior
findings that suggested “surprisinglyrobust pregnancy chances, even atundetectable to extremely low AMHlevels.” Dr Weghofer presented herfindings in a poster at the 2011 meetingof the American Society for Repro -ductive Medicine. The study included128 women with AMH levels ≤0.4ng/mL who were referred for an infertil-ity workup and subsequently started an
IVF cycle. An AMH level of ≤0.4ng/mL was chosen because it was shownin the published literature to be a pre-dictor of poor response to controlledovarian hyperstimulation. The meanage of the patients was 40.8 years.Prior to IVF, all women with dimin-
ished ovarian reserve were supple-mented with dehydroepiandrosterone(DHEA), 25 mg 3 times daily, for atleast 6 weeks. All women who under-went IVF received microdose agoniststimulation with a daily gonadotropindosage of 600 IU. Ovulation inductionand oocyte retrieval were performed inall women who presented with at least1 follicle of 17 mm.There were 20 clinical pregnancies
recorded (7.9% per cycle start), 15.6%cumulatively, resulting in 13 live birthsin 12 women. Eight women miscarried.
Eight deliveries occurred after the firstIVF cycle (6.3% per cycle start) and 4after subsequent IVF cycles (3.2%).In the 70 women 42 years old and
younger, there were 16 clinical preg-nancies that resulted in 10 deliveries. Inthe 58 women older than 42 years,there were 4 clinical pregnancies thatresulted in 2 deliveries, which was a sig-nificantly lower rate of pregnancychance and delivery compared with theyounger cohort.The data demonstrate a “moderate
but still reasonable pregnancy chanceand live birth rates” in women withAMH levels up to 0.4 ng/mL, accordingto Dr Weghofer, an attending facultyphysician, Department of Gyne col -ogical Endocrinology and Repro ductiveMedicine, Medical University ofVienna; and an affiliate at the Center
for Human Reproduction. She alsonoted, “To the best of our knowledge,this represents the largest cohort ofwomen with extremely compromisedAMH levels who conceived and deliv-ered in the course of assisted reproduc-tive technology.” Supplementation with DHEA has
been demonstrated to improve preg-nancy chances in women with dimin-ished ovarian reserve. The findings inthis study, therefore, may not apply toall women with low AMH levels, DrWeghofer cautioned, but she conclud-ed, “Though these post hoc observa-tions need further confirmation inother (not treated with DHEA)patients, extremely low AMH levels donot seem to represent an appropriatemarker for withholding fertility treat-ment.” n
Extremely low AMh levels Do Not Rule out In Vitro fertilization by Wayne Kuznar

14 FEbRUARY/MARCH 2012 l VOLUME 4, NUMBER 1
Patient Awareness
Infertility affects approximately 15%of the reproductive-age population,which is currently estimated at
about 7.5 million people. Because of thehigh prevalence of this condition, aswell as the media and Internet atten-tion to this problem, young women andmen are becoming increasingly aware oftheir own fertility potential. In relation to other species, humans
are poor reproducers, with an estimated20% chance of conception monthly.
When the potential for miscarriage isfactored in, the actual chance of con-ception falls to approximately 10% to12% each month. This is largely due tothe prevalence of chromosomal abnor-malities of the oocytes, causing failedconception or miscarriage. In a womanyounger than 35 years, it is estimatedthat 60% of eggs contain inherent chro-mosomal abnormalities. By age 40, thispercentage increases to more than 80%,and by age 45, it is estimated that 90%of a woman’s eggs are affected.
The single most important factor inpredicting pregnancy is the age of thefemale partner. It is commonly knownthat as age increases, the chance ofpregnancy decreases. At the same time,the rate of spontaneous miscarriage andchance of having a child with chromo-somal abnormality increases withincreasing age. Both the age at whichwomen are having their first child andthe age of marriage are noted to beincreasing. A recent study by the CDCshowed that women in the US andother developed countries are waitingsignificantly longer before becomingpregnant than women of a generationago. The average age of first-time moth-ers in the US jumped from 21.4 years in1970 to 25 in 2009. The average age ofmarriage has similarly increased from 23years in 1970 to 28.2 in 2010. Aswomen choose to delay marriage andchildbearing, the likelihood of futureinfertility increases. The monthlychance of achieving pregnancy gradual-ly but significantly begins to decline atage 32 and decreases more rapidly afterage 37.The Fertility Awareness checkup at
Fertility Centers of Illinois is a simpletest performed on cycle day 3 that iscomposed of blood tests to check folli-cle stimulating hormone (FSH) andestradiol levels, an antral follicle countto measure ovarian reserve, and semenanalysis to assess sperm parameters.Ovarian reserve refers to the ability ofthe ovary to respond to ovulationinduction treatment and produce a rea-sonable quantity and quality of oocytes,therefore enabling a woman to achieve
pregnancy. There are several methodsto test for ovarian reserve, and the sim-plest include day 3 FSH and estradiol.FSH is elevated due to the aging ovarynot producing adequate amount ofinhibin, the hormone that suppressesFSH. Estradiol is elevated due to anincrease in FSH earlier in the menstru-al cycle. An FSH level <10 mIU/mLand an estradiol level <70 pg/mL areconsidered within the range for normal
ovarian reserve. Antral follicle count isanother test of ovarian reserve per-formed on day 3 of the cycle. It usestransvaginal ultrasonography to meas-ure small follicles <10 mm in diameter.A bilateral total number of small folli-cles between 10 and 20 is consideredwithin the range for normal ovarianreserve.Since male infertility is a factor in
approximately 40% of all couples withdifficulty achieving pregnancy, a semenanalysis is an important step in the fer-tility assessment. The standard refer-ence range for normal semen analysesis: volume 1.5 to 5 mL, concentration>15 million/mL, motility >40%, andstrict morphology >14%. An abnormaltest will most likely result in a recom-mendation to repeat the semen analysiswith further follow-up as indicated. This simple combination of 4 tests to
check for ovarian reserve and semenquality constitutes the FertilityAwareness checkup. The results may behelpful to patients who will be makingfamily planning decisions currently or inthe near future. This evaluation is pro-vided to patients at a low cost, and theyreceive the completed results within 1week. The results do not give a definitiveanswer but may provide an estimate of apatient’s fertility potential. Patients aremade aware that these tests do not guar-antee future fertility, although the resultsmay help them answer questions aboutwhen to start planning their family andwhat direction their family planningcould most likely take. If patients decideto consult further with a physician, theevaluation fee is credited toward futuretreatment services. While the exact causes of roughly
one third of all fertility problems arestill unknown, there are many repro-ductive dysfunctions that can be over-come with treatment. Identifyingpatients who require treatment is neces-sary to prevent future compoundedinfertility, and it all starts with a fertili-ty assessment. n
fertility Awareness checkupBy Meike L. Uhler, MD
Patients are made aware that these tests do not guarantee future fertility, although the results may help them answerquestions about when tostart planning their familyand what direction theirfamily planning could most likely take.
Pelvic organ Prolapse May Respond to Nonsurgical treatmentsBy Rosemary Frei, MSc
Evidence is accumulating thatalternate approaches may givesurgery a run for its money in
treating pelvic organ prolapse. A Cochrane Review examined
whether selective estrogen receptormodulators (SERMs) are effective forpreventing or treating pelvic organ pro-lapse in postmenopausal women (IsmailSI, et al. Cochrane Database Syst Rev.2010;9:CD007063). Although only 1meta-analysis and 2 original trials metthe investigators’ inclusion criteria and
had “meaningful” data, the researchersconcluded that 1 SERM, oral raloxifene(Evista, Lilly USA), may reduce theneed for pelvic organ prolapse surgeryin women aged older than 60 years.However, they stressed that long-term,rigorous, randomized, controlled trialsare needed to verify whether estrogenpreparations are indeed useful in thisapplication. The review was conducted by a team
led by Sharif Ismail, MD, attendingphysician, Urogynecology Unit,
Singleton Hospital, Swansea, Wales. DrIsmail noted that the study was under-taken because estrogens are used inclinical practice – often as adjuncts toimprove the prolapse outcomes fromother treatments, such as surgery ordiaphragm-type devices – without clearevidence to support these practices.Overall, the 2 trials and 1 secondaryanalysis of 3 studies included in theCochrane Review showed a significantreduction in the need for surgery forpelvic organ prolapse in women aged
older than 60 years treated with ralox-ifene and tamoxifen.“I’d like to stress that raloxifene is not
normally used for pelvic organ prolapse,and hence, this potential reduction inthe need for pelvic organ prolapse surgeryneeds further investigation,” Dr Ismailsaid.Matthew Barber, MD, associate pro-
fessor of surgery, Center of Uro -gynecology and Reconstructive PelvicSurgery, Cleveland Clinic Lerner
Continued on page 15
Meike Uhler, MD.

FEbRUARY/MARCH 2012 l VOLUME 4, NUMBER 1 15
Nonsurgical Intervention
Pelvic organ Prolapse…Continued from page 14
College of Medicine, Case WesternReserve University, and vice-chair ofclinical research, OB/GYN & Women’sHealth Institute, Cleveland Clinic,agreed that more research is needed. “Idon’t think we have enough informationto say whether estrogen or SERMs aregoing to be helpful for treating or pre-venting prolapse,” Dr Barber said. “Somestudies have suggested that post-menopausal hormone replacement canactually predispose women to stress uri-nary incontinence, a condition relatedto prolapse, so it is important that morerigorous studies be performed beforeadvocating estrogen or SERMS for pro-lapse generally.”
Dr Ismail’s co-investigator, SuzanneHagen, PhD, led an earlier CochraneReview on conservative managementof pelvic organ prolapse (Hagen S, et al.Cochrane Database Syst Rev.2006;4:CD003882). She and her col-leagues had also concluded that therewas insufficient evidence to make a rec-ommendation and could not advise cli-nicians whether their patients shouldreceive pelvic floor muscle training.Ingeborg Hoff Braekken, PhD, PT,
and colleagues at the Department ofSports Medicine, Norwegian School ofSport Sciences in Oslo, Norway recent-ly attempted to fill this void with amedium-sized trial (Braekken IH, et al.Am J Obstet Gynecol. 2010;203:170.e1-
7). They randomly assigned 59 womenwith prolapse stages I, II, and III topelvic floor muscle training, and ran-domized another 50 women to standardtreatment, including learning how tocontract their pelvic floor musclesbefore and during increases in abdomi-
nal pressure.Among women in the pelvic floor
muscle training group, 19% (11) im-proved by 1 Pelvic Organ Prolapse Quan -tification System stage, compared with8% (4) in the control group. The pelvicfloor muscle training group also experi-
enced a significantly greater elevation inthe bladder and rectum, and re-duced fre-quency and bother of symptoms.“Pelvic floor muscle training is with-
out adverse effects and can be used astreatment for prolapse,” the investiga-tors concluded. n
��� �� ��� ���Editor in ChiefSagar Lonial, MDAssociate Professor of Hematology and Oncology Emory University School of Medicine
Editor in ChiefStephanie A. Gregory, MDThe Elodia Kehm Chair of Hematology Professor of MedicineDirector, Section of HematologyRush University Medical Center/Rush University
Topics include:• Newly Diagnosed Patients• Maintenance Therapy• Transplant-Eligible Patients• Retreatment• Transplant-Ineligible Patients• Cytogenetics• Side-Effect Management• Bone Health
Newsletter Series
���������������� ���������������� �� ���
������ ��������� ���
Topics include:• Hodgkin Lymphoma• Follicular Lymphoma• Mantle Cell Lymphoma• Waldenstrom’s Macroglobulinemia• Diffuse Large B-Cell Lymphoma• T-Cell Lymphoma
���������������� ������������������
������ ��������������
Target AudienceThese activities were developed for physicians, nurses, and pharmacists.
AccreditationThis activity has been approved for 1.0 AMA PRA Category 1 Credit™ (a total of 14.0 credit hours will be issued for completion of all activities). Nursing and Pharmacy credit hours will also be provided.For complete learning objectives and accreditation information, please refer to each activity.
This activity is jointly sponsored by Global EducationGroup and Medical Learning Institute, Inc.
Coordination for this activity provided by Center of Excellence Media, LLC.
������� �������� ����������� ����� ������������
YOUR QUESTIONS ANSWERED
COEAsize40611MM
For information about the physician accreditation of this activity, please contact Global at 303-395-1782 or [email protected].
This activity is supported by educational grant from Cephalon Oncology,Millennium Pharmaceuticals, Inc., and Seattle Genetics, Inc.
This activity is supported by an educational grant from Millennium Pharmaceuticals, Inc.
� �� �������� ���������
“Raloxifene is not normallyused for pelvic organprolapse, and hence, thispotential reduction in theneed for pelvic organprolapse surgery needsfurther investigation.”
—Sharif Ismail, MD
IF YOU MISS ANYNEWSLETTER
IN THE SERIES…
LOG ON TO:www.infertilityrepronews.com
www.theobgynnurse.com