FEBRUARY 2009 - mda.org.my 2009 Up and Coming ... CDE Self Assessment In Clinical Dentistry - Part...
28
FEBRUARY 2009 Up and Coming From the President’s Desk MDA/ Malaysian Armed Forces FREE Public Dental Screening Campaign Message from President - Elect The Honorary Financial Secretary’s Message Message from Honorary Publication Secretary Report of the 16th FDI / MDA Scientific Convention & Trade Exhibition 2009 COLGATE Oral Health Month Perceptions Towards Dental Auxiliaries In Malaysia: A Preliminary Survey MDA Northern Zone Reports Coming CPD Events CDE Self Assessment In Clinical Dentistry - Part xxii Part 1: An Oral Surgery Tale of 2 Ladies Answers for CDE Self Assessment In Clinical Dentistry - Part xxii Part 1: An Oral Surgery Tale of 2 Ladies MDA/Listerine Community Project Classifieds Malaysian Dental Association 54-2, Medan Setia 2, Plaza Damansara, Bukit Damansara, 50490 Kuala Lumpur, Malaysia. Tel: 603-2095 1532, 603-2095 1495 Fax: 603-2094 4670 Website: www.mda.org.my E-mail: [email protected] Honorary Publication Secretary Assoc. Prof. Dr. Seow Liang Lin Co-Editors Assoc. Prof. Dr. Seow Liang Lin Dr. Shahida Mohd Said Secretary Dr. Wey Mang Chek Treasurer Dr. How Kim Chuan Ex-officio Dr.S.Sivanesan Note: This newsletter is a publication of the Malaysian Dental Association and opinions expressed herein are that of the authors and do not necessarily reflect the opinion of the editorial board, the MDA council or the said Association. MDA NEWS shall not, without written consent of the Association, to be hired, lent, given or otherwise disposed of by way of trade or affixed to or as part of any publication or advertising, literary or pictorial matter whatsover. A Publication for Members of The Malaysian Dental Association What are inside: 25-28 June 2009 Equatorial Hotel Penang
Transcript of FEBRUARY 2009 - mda.org.my 2009 Up and Coming ... CDE Self Assessment In Clinical Dentistry - Part...

FEBRUARY 2009
Up and Coming
From the President’s Desk MDA/ Malaysian Armed Forces FREE Public
Dental Screening Campaign Message from President - Elect The Honorary Financial Secretary’s Message Message from Honorary Publication
Secretary Report of the 16th FDI / MDA Scientific
Convention & Trade Exhibition 2009 COLGATE Oral Health Month Perceptions Towards Dental Auxiliaries In
Malaysia: A Preliminary Survey MDA Northern Zone Reports Coming CPD Events CDE Self Assessment In Clinical Dentistry
- Part xxii Part 1: An Oral Surgery Tale of 2 Ladies
Answers for CDE Self Assessment In Clinical Dentistry - Part xxii Part 1: An Oral Surgery Tale of 2 Ladies
MDA/Listerine Community Project Classifieds
Malaysian Dental Association
54-2, Medan Setia 2, Plaza Damansara, Bukit Damansara, 50490 Kuala Lumpur, Malaysia. Tel: 603-2095 1532, 603-2095 1495 Fax: 603-2094 4670Website: www.mda.org.my E-mail: [email protected]
Honorary Publication Secretary Assoc. Prof. Dr. Seow Liang Lin
Co-Editors Assoc. Prof. Dr. Seow Liang Lin
Dr. Shahida Mohd Said
Secretary Dr. Wey Mang Chek
Treasurer Dr. How Kim Chuan
Ex-officio Dr.S.Sivanesan
Note:This newsletter is a publication of the Malaysian Dental Association and opinions expressed herein are that of the authors and do not necessarily reflect the opinion of the editorial board, the MDA council or the said Association. MDA NEWS shall not, without written consent of the Association, to be hired, lent, given or otherwise disposed of by way of trade or affixed to or as part of any publication or advertising, literary or pictorial matter whatsover.
A Publication for Members of The Malaysian Dental Association
MDA NEWS
What are inside:
25-28 June 2009Equatorial Hotel Penang

C
M
Y
CM
MY
CY
CMY
K
360 MICROSONIC FA OL.pdf 13/11/08 12:50:33 PM

FEBRUARY 2009 3
The turn of the year for 2009 has been a mixed bag of fortunes for many. Fortunately, for the MDA, things are still looking good and the Association and its members have every reason to envisage a good
year ahead. From prudent spending to encouraging sponsorships, the MDA has made huge strides in recent years. We hope that with the support of the membership, the MDA will continue to deliver the very objectives set out in its Constitution. The Year of the Golden Ox is in and I take this opportunity to wish our Chinese colleagues a Happy Chinese New Year. To keep you abreast of recent developments, I append the following;
Liberalisation of Services Sectors in ASEAN
The government has already set its policy to open the Service Sector and the Health sector is expected to open by 2013. Related issues such as quality healthcare, competitiveness, readiness for changes and sustainability of local expertise and identification of niche area in medical and dental practice require attention. The MMC and MDC as regulatory bodies will look into balance mechanisms to regulate the flow of foreign professionals. Competition from foreign institutions providing healthcare is being studied in areas concerning cost, quality and competency.
A recent meeting chaired by Deputy DG of Health (Medical) Datuk Dr Noor Hisham deliberated on the new package for the AFAS from the Health sector. The Dental sector has also extended a package and awaiting further discussion. The Minutes of the said meeting has been forwarded to us for our reference.
Apart from tax revenue, the liberalisation exercise will benefit the country in terms of fulfilling corporate and social responsibility which in turn will benefit the public. The Dental sector is well advised to take heed and keep pace with the recent developments.
16th MDA/FDI Scientific Convention & Trade Exhibition Hotel Istana 17th-18th January 2009.
After the 16th MDA/FDI Scientific Convention & Trade Exhibition at the Hotel Istana 17th-18th January 2009, it has become obvious that a larger venue needed to accommodate the increase in delegation as well as the trade representatives. The impending tie up of the CPD with the Annual Practicing Certificate may have something to do with the sudden awakening. Kudos to the Organising team under the leadership of Dr. V. Nedunchelian, Dr. Kathiravan and Organisng Secretary Dr. Darren Yap. With an unprecedented surplus closing RM180K before audit, the team deserves a big pat on the back for their efforts.
The 66th MDA AGM and Scientific Convention – June 25-28 Hotel Equatorial Penang
Without stealing the thunder from organizing team, I am glad to report that the June event has promised to take new heights. We await the unfurling of better things to come for the Association.
Appointment to the Malaysian Dental Council
The President has been appointed by the Minister of Health to sit on the Malaysian Dental Council for a period of 3 years. I thank the Minister YB Dato’ Seri Liow Tiong Lai for accommodating our humble request for the appointment. The MDA can now channel its concerns in a more direct fashion to the council when the need arises.
Communication from the Anti Corruption Agency
The ACA, in a recent communication to the President has completed its investigation with a general recommendation on financial procedure without penalty on any individual. We are now hopefully out of the woods from the whole episode. The official letter has been placed in our files for your viewing.
APDC Hong Kong 2009
With the APDC 2013 in the bag, our delegation has to make a commendable representation at future International dental events to make a suitable impact on foreign delegates. At present some 10 delegates from Malaysia have signed up for the event.
Amendments to the Dental Act
Dr Elise Monerasinghe from the MOH has asked for a meeting with the MDA soon to discuss the various amendments to the Dental Act being drafted. This is an extremely important meeting for the profession and a tentative date, Tues 10th March 2009 has been set with urgency. Invitations will be made out to our Affiliates to participate.
Invitation to Dental South Asia China International Expo 2009 – 26th Feb -1st March 2009 Guangzhou
The President had been invited to make an address for the meet. All expenses were borne by the organizers. This is the 2nd such invitation from the Chinese dental fraternity; the 1st one being the China Asean Forum on Dentistry in Nanning, Quangxi Province. The Dental South Asia International Expo is on its 14th year of existence and boasts of some 600 International exhibitors from Germany, France, Italy, USA, Japan, South Korea, Austria, Switzerland and others covering some 26,000 square meters in exhibition space totaling some 1600 trade booths. Over 40,000 professionals and trade delegation attend the exhibition cum conference. Other regional exhibitions just pale in comparison by just looking at the size of the event. I had the chance to meet up with several
From the President’s Desk

MDA NEWS4
Malaysian and Singapore dental traders who frequently take the opportunity to attend this expo to expand their trade horizon.
Invitation to be a Member to the USM Jawatankuasa Pengajian
An invitation to be a Member to the USM’s Jawatankuasa Pengajian bagi Mengkaji Cadangan Penawaran Sarjana Pergigian Pediatrik Secara Mod Kerja Kursus oleh Pusat Pengajian Sains Pergigian.- USM Penang has been made to the President. The invitation to the MDA will augur well for future collaboration USM and the MDA.
Seminar on Digital Dentistry 15-18 Aug 2009, Vistana Hotel Penang
Chairman of ICCDE, Dato’ Ratnanesan has extended an invitation to the MDA (in particular Northern Zone) in a joint collaboration to host the Seminar on Digital Dentistry.
CPD Programs
I took the opportunity to attend the Northern Zone AGM and CPD. The AGM was rescheduled for 15th February 2009 with a good turnout. Kudos to the NZ team. Dr Teh Tat Beng and Dr Koh Chou Huat have been returned as Chairman and Secretary of the Northern Zone respectively.
Another CPD program is due in Ipoh on 12th April 2009 and further details are on the webpage and are due in your mail soon.
The Southern Zone CPD was held on 21/02/2009 (Sunday). The SZ AGM has been rescheduled to 9th April 2009 at 7pm at the Grand Paragon Hotel .JB.
The President also led a delegation to represent the MDA at the ‘ to be’ Eastern Zone ( Kuching /Kota Kinabalu -13th and 14th December 2008). The representations for both CPD talks were good and is a fair indication of the mood to provide more via the ‘Eastern Zone’. The fate of the Eatern Zone stiil hangs in the balance as the ROS has yet to come back to us on the constitutional amendments
submitted after the AGM in 2007 due to an apparent technical glitch.
Communications from Affiliates
The MDA extends warm felicitations Dr Jaspall Singh for taking the high office of President of the MPDPA and congratulates Dr V. Nedunchelian on a successful tenure at the helm over the last three years.
On the same note, the MDA takes the opportunity to congratulate Dr Chow Kai Foo and his able team for assuming the helm of the Malaysian Oral Implant Association and Dr Yeo Kian Boon and his team at the Malaysian Association of Aesthetic Dentistry.
Flagging of the ‘Complete Your Daily Oral Care with Mouthwash’ and the ‘ Listerine Mobile Mouth’ truck
Listerine and the MDA co-launched this community service project to spread the Brush, Floss and Rinse message in Oral Health care. The event was launched by MD Joyce Lee and the MDA’s President Dr. S. Sivanesan.
Organising Chairman Dr. V. Nedunchelian, Dr. S. Ratnasothy and Past President Dr. Shubon Sinha were present at the launching ceremony. The event received widespread TV and newspaper coverage.
Colgate Oral Health Month
The month of April draws near and you would have received Colgate’s annual program and invitation to the membership to participate in the screening exercise. I thank you in advance for displaying the highest degree of professionalism during the exercise as it will be a reflection of the MDA from all aspects.
Dr. S. Sivanesan
President Malaysian Dental Association 2008/2009
FREE Public Dental Screening incollaboration with Malaysian Armed
Forces Date: 28th June 2009
Venue: Queensbay Mall Penang
Main sponsor:
Ministry of Defence Armed ForcesMalaysian Dental Association

FEBRUARY 2009 5
Dear Colleagues and Friends,
As this report was penned, we, the MDA Council cannot be oblivious to the wide spreading and engulfing global economic crisis.
Sponsorships, support in kind, advertisement spending and traders commercial activities are expected to diminish. This anticipated scenario would certainly take center stage in the coming months and the Association needs to be prudent to tide over this uncertain period.
Having said that, I am indeed pleased to note that the past and present prudence were manifestly proven in our healthy financial surplus for year ending 2008 that will be elaborated by our Honorary Financial Secretary, Dr How Kim Chuan in his accompanying report.
My focus areas shall be the following;
1. MDA E-Journal at www.mda.org.my
Dr Seow Liang Lin and I have worked hard to put up the special free access of 27 international renowned e-dental journals courtesy of John Wiley Publisher. The overwhelming responses and accolades that we received from MDA members’ manifested the approval and viability of this e-dental journal project.
Funding remains the major obstacle to grow the project to larger scale. Nonetheless, we have been steadfast in our quest for sponsorship and were duly rewarded with some sponsorships that should see the project continues to expand for the benefit of the membership. On this note, the committee would take this opportunity to thank Galla Corporation, PE lifestyle Sdn Bhd, Straumann TDI and AR Dental whom have come onboard to support this noble project for MDA members.
2. The 66th MDA AGM /MDA FDI Scientific Convention & Trade Exhibition (26th to 28th June 2009) in Penang Equatorial Hotel
This major convention is an event not to be missed. Everything has been placed to make it an international standard convention where speakers of international repute such as Professor Emeritus Niklaus Lang ,
Message From President - Elect
Professor Emeritus Malcolm Harris and many others would be sharing their expertise.
We are indeed proud to announce that TYT Gabenor of Penang has been invited to be the Guest of Honor for the MDA Formal Night and the YAB Chief Minister of Penang has also confirmed his attendance.
We are equally honored that the 66th Scientific Convention & Trade Exhibition would be officially open by the Honorable Minister of Health, YB Dato Seri Liow Tiong Lai on the 27th of June 2009 at Penang Equatorial Hotel.
3. Free Public Dental Screening Campaign at Queens Bay Mall, Penang on 28th of June 2009, in conjunction with the 66th MDA AGM.
We are indeed grateful to the Dental Director of Ministry of Defence, YB Mej Gen Dato Dr Sukri Hussin for his kind effort to collaborate with MDA to jointly conduct a free dental screening campaign for the public and underprivileged children at a premier shopping center in Penang Queens Bay Mall on the 28th of June 2009. The dental specialists and officers from the Armed Forces would be involved in the exercise.
In the campaign we would provide each public participant whom requires further dental treatment a list of dental clinics in the Penang, Perak, Kedah and Perlis region for their follow up treatment at their own expenses.
MDA members whom have registered for the 66th MDA AGM Convention are most welcome to email Dr Teh Tat Beng, the MDA Northern Zone Chairman at [email protected] or SMS him at 012-4663779 your full name, clinic address and your contactable email or hand phone for listing purpose.
Thank you for your kind attention
Warmest regards,
Dr Lee Soon Boon
President Elect Malaysian Dental Association

MDA NEWS6
The Honorary FinancialSecretary’s Message
Introduction
It is this time of the year annually that we are busying auditing accounts and presenting our “Report Card” to the members. Amidst the global financial crisis, we have witnessed the financial tsunami of an unprecedented scale and the repercussion that is going to affect us is expected to be profound. The immediate impact to our beloved Association is the sponsorship money which we depend heavily. This in turn has triggered an immediate response from me to review the budget and justify our expenditure prudently. However, I am pleased to announce that we did not cut or cancel any spending on worthy projects that were originally budgeted for. This is largely attributed to our current strong financial standing. Our past efforts of strict adherence to transparent and accountable financial policy have reaped the fruits that we now enjoy currently.
How do we fare in the Year 2008 ?
As we know, last year was a year of inflation. We have witnessed the price of crude oil raised above one hundred US dollars per barrel. This means that our utilities as well as other expenditures would also have to go up; not proportionally but exponentially. To quote you the exact figure, we spent a total of RM 1,305,791 in 2007 but last year we spent RM1, 728, 401.82. A hefty increase in expenditure by 32%! However, I need to tell you that this increase in expenditure is not fully attributable to inflationary pressure. In fact, in many respects, it was pre-budgeted and pre-approved spending based on our financial policy. You would recall that in my first message in this Newsletter, I emphasized on spending on projects that would benefit members at large. Under this financial policy, we have increased spending on CPD programmes, more CPD talks were conducted outside KL reaching out to our members in remote areas and more subsidies were given to members to make the CPD talks affordable as well as educational. The CPD programme also becomes the platform for us to interact with members. I am delighted to inform you that our policy has reaped the fruits. Not only that our CPD talks attendance has improved, our sponsorship money to support the CPD talks has also increased despite the economy downturn. I have to acknowledge Dr Muzafar Hamirrudin and Dr Haja Badrudeen for a job well done.
In addition, our maiden project, the MDA e-Journal website also took off successfully, our maiden venture into this project has received an encouraging response from the membership and the sponsors are now attracted to this innovative project that even other neighboring Associations are also talking about. What is worth mentioning is that we have been able to benefit members’ at large, increase spending and still remain self
sufficient. This is a remarkable achievement and I must pay tribute to Dr Lee Soon Boon and his team for the excellent job that they have done for the Association.
Our Newsletter and MDJ have also received many good comments from members as well as colleagues from neighboring countries. We are committed to quality MDJ articles and informative, light-hearted Newsletter contents. Thanks to the wonderful job done by our Publication Secretary Associate Professor Seow Liang Lin and her team. With the improved quality of our Newsletter, I envisage more sponsors would place in advertisements to support our MDA Newsletter.
The good news above all these is that despite increase in spending and despite the curse of economic downturn, we manage to register a record profit of RM 580, 193.24! Compare to a net surplus of RM 313, 625 made in 2007. This is a remarkable 185% jump in profit, a record that has never been achieved in the history of MDA. I would like to attribute this success to the strict adherence of our transparent financial policy as well as our well contemplated budget planning policy. In addition the full support of all Council members to cooperate in the implementation of our financial policy is also to be commended. I also wish to thank our sponsors for their relentless support to our Association, unshakably through rains or shines.
What is our current financial status?
We are now into the 3rd month or first quarter of the Year 2009. I am pleased to inform you that the first 2 months, we are still managed to secure a financial surplus of RM 92, 264 despite the shrinking economy prospect. This increase in profit is largely attributable to our ability to balance all our receivables and payables. All outstanding balance is being monitored closely; simultaneously we also pay our debtors on time without delay. This again speaks volume of our financial policy because I no longer hear complaints that we procrastinate their payment unnecessarily. We have placed another RM 200, 000 as fixed deposit. Our accrued fixed deposit is now standing at RM 2 million and our total asset is now standing at RM 3.17 million.
What is our financial policy going forward?
I attribute our current financial success to our prudent financial policy and good team spirit within the Council. Stability is the keystone for progress. Going forward, I need to caution here that many has taken our success for granted, thinking that our beloved Association is now in good surplus and began to spend money loosely and extravagantly. Complacency is the root of all failure. Amidst the deepening effect of global economic recession, we have to be extra prudent in our budget as well as spending as sponsorship money would not come as readily as it used to be. Our MDA Conference would take a toll on this impact

FEBRUARY 2009 7
as things are more expensive, hence expenditure would go up but the anticipated income is not forthcoming so readily. However, despite the difficulties, our financial policy would maintain the core spending on projects that benefits the members at large. We would look into ways to cut down unnecessary expenditure and build a healthy cash reserve to weather any unexpected financial storm. It is also my wish to be able to pick some good bargain in property during this economy recession. It is time tested investment strategy to invest in property when it falls to the lowest trough. This would shield us against deflationary pressure
and generate decent rental income. Our Predecessor Past Presidents had done this well and the property that they bought is now yielding a decent rental income of RM 33, 600 per annum for our Association. I have a dream to build a Wisma MDA for our beloved Association. It is hope that this dream would come true one day as the opportunity comes by to knock our door.
Dr. How Kim Chuan
Honorary Financial Secretary MDA 2008/2009
To the Esteemed Members of MDA,
We are “meeting” again in this first issue of MDA News in 2009. Whilst everyone is bracing to face the worst during this thriving time of global economic downturn, at the MDA front, a lot of interesting events have happened and more exciting conferences, CDP programmes etc awaits the dental healthcare providers in Malaysia and this region. Under the prudent control of Honorary Financial Secretary Dr. How Kim Chuan, President Dr. Sivanesan and the rest of the Council members, the MDA stands healthy financially.
The facet of MDA News has undergone evolution; with hope that we will be able to portrait current event or other interesting pictures. Members are strongly encouraged to send in interesting photographs to be considered as the front cover and the contributor will be duly acknowledged.
The newsletter aims to keep members informed with regards to the MDA activities and up and coming events. In this issue, efforts have been spent on collecting reports for the past few months and also provide information on events in the near future. I wish to express my sincere thanks to those who have provided the reports as named in respective reports. I also wish to congratulate the organizing teams who have worked hard to bring the various activities to members. The major up and coming event being the 66th MDA AGM/FDI Scientific Convention on 25th-28th June 2009, Penang. It is going to be an informative and exciting convention as has been illustrated by Dr. Lee Soon Boon.
As one of the regular section, the CDE Self Assessment in Clinical Dentistry presented the first part of interesting oral surgery cases. I wish to express my deepest gratitude to Dr. Wong Foot Meow for his enlightened contribution. I also would like to bring your attention to another CDE avenue that MDA has brought to the membership- E-Journal. As illustrated by Dr. Lee Soon Boon, members
Message from HonoraryPublication Secretary
can now access e-journals at the MDA secured website, it is a rare privilege dental associations would offer to their membership. I strongly encourage members to make full use of this avenue to enhance their knowledge and skills.
This newsletter is for all the MDA members and the Editorial Team welcomes constructive comments from all of you out there to improve it. Please send your comments to MDA Secretariat. I wish to record my appreciation for your support for MDA and this newsletter. I would also like to thank Dr. Sivanesan and the rest of Council Members for their tireless support rendered to me.
Assoc. Prof. Dr. Seow Liang Lin
Honorary Publication Secretary
CONGRATULATIONS!
Dato’ Prof. Dr. Hashim Yaacob, president of IUCN was conferred LIFETIME PROFESSIONAL INTEGRITY AWARD by the Balai Ikhtisas Malaysia(BIM)-Rotary International Malaysia on 3rd March 2009, in recognition for being a role model and having demonstrated courageous acts and commitments in the advancement of integrity values and beliefs. BIM is the parent body of twenty different professional organizations. Malaysia Dental Association wishes to record the highest congratulatory note to Professor Dato’ Dr. Hashim Yaacob, who has contributed immensely and selflessly to the Dental Profession.

MDA NEWS�
BriefThe International Medical University (“IMU”) is the pioneer and leading private healthcare university in Malaysia. With its extensive network of foreign partner universities and track record in providing quality healthcare academic programmes, IMU is now planning the next stage of its expansion into healthcare services.
One of the key healthcare services is the proposed IMU private dental practice. This practice will be commercially operated and is planned as an integrated team based dental and specialist referral centre. In line with this, IMU seeks a motivated candidate with a desire for accomplishment to drive the IMU private dental practice and in turn influence the Malaysian dental practice landscape.
Summary of ResponsibilityThe Candidate who will also practise in the centre will be responsible for the overall management of the practice which will be equipped with state-of-the-art equipment and full back-up imaging and lab facilities. Duties will include: - • Assembling, overseeing and supervising a team of clinicians and support staff. • Ensuring best practice in service provision, standards and adherence to relevant legislation and to
codes of professional conduct.• To provide leadership and professional direction in the development of the clinical service plan and
professional quality in keeping up with patient needs and global trends.• To develop policies and procedures including Standard Operating Procedures (SOPs) and training
programmes.
In addition to the team at the centre, the Candidate will be assisted by a Healthcare Team and Dental School Faculty in the development and management of the practice. Training will be provided to the Candidate including in the management of grouppractice which will be provided in a regional centre.
Requirements• Dental qualification(s) registrable with the Malaysian Dental Council• Possess at least five (5) years of clinical dental practice experience with at least three (3) years in the
private sector• Good knowledge of dental or health environment• Good leadership, interpersonal, communication skills and computer literate • Preferable to have relevant experience in managing staff and/or dental clinic/centre
Applicants are strongly encouraged to apply by email to [email protected] stating their email ad-dress, telephone number and the names and contact details of three referees including a curriculum vitae by attachment.
Postal application will also be accepted and should be addressed to:
The Human Resource Department (Recruitment)IMU Education Sdn Bhd (237397-W)126, Jalan 19/155B, Bukit Jalil57000 Kuala Lumpur, Malaysia
The closing date for application is 8 April 2009. Short-listed candidates will be notified by email or telephone.

FEBRUARY 2009 9
Reported by: Dr Darren Yap
2009 kicked off with MDA’s first event of the year…and it was a cracker. A record turnout of approximately 550 participants (latecomers had to be turned away) with a large representation from both the private and government sectors contributed to its success.
Hotel Istana once again hosted the event with the trade exhibition consisting of over 80 booths occupying the 3 halls. Participants thronged the exhibition in search of the latest products, bargains and freebies.
Two hands-on sessions initiated the convention on Friday, 16th of January which were conducted by the following:
Dr Leslie Ang: ‘Endodontic Retreatment’
Dr Daniel Fang: ‘Veneers-How to’
Datin Dr Norain Abu Talib once again graced the occasion with her presence during the opening ceremony by declaring open the convention on Saturday morning, 17th January, 2009, which was attended by various VIPs of the dental profession from all corners of the nation. The following were the speakers and their presentation topics:
1. Prof. Dr. Lakshman Samaranayake ( Johnson & Johnson )
Topic: Managing Biofilms for Optimal Oral & Systemic Health
2. Dr Professor Roger Ellwood(Colgate)
Topic: New approaches to detection, monitoring and treatment of early carious lesions.
3. Dr Leslie Ang ( Dentsply/ Servicom/ Carl Zeiss )
Topic: Endodontic Retreatment: Master the Science and Excel in Clinical Techniques
4. Dr Daniel Fang ( 3M )
Topic: To Veneer or not to veneer?
5. Dr Gianluca Gambarini
Topic: An introduction to New NiTi Files ( TF Files ) & Forward movement on rotary.
6. Dr Geoffrey Speiser
Topic: Practical Application of a Breath Clinic in a dental practice.
Practical Tips in the use of contemporary all ceramic restorations.
A concurrent oral presentation and poster presentation was held with winners walking away with prizes.
Sunday ended with a 60 minute Q&A session with the Oral Health Division of the Ministry of Health. This was a first of its kind and was very well received by the attendees. Led by Datin Dr Norain herself and her team of representatives from the MOH, questions and doubts from the dental fraternity were dealt with ranging from autoclave and compressor licensing to toilet doors and illegal dentistry.
Lucky draw prizes were handed out at the end including a notebook computer, hand phones, a light cure unit, MP3 players, DVD player and many more.
Many thanks to the sponsors, members of the dental trade, volunteers from the Dental colleges and others who have contributed in one way or another to the event. And kudos to the organizing committee led by Dr V. Nedunchelian.
Report of the 16th FDI / MDA Scientific Convention& Trade Exhibition 2009

MDA NEWS10
COLGATE Oral Health Month
Reported by: Dr. V. Nedunchelian
a) 6th Joint MDA / Colgate Community Project
b) The theme is “Our Mission: Zero Cavity”
c) No of Clinics participate : 566
d) No of Marquees : 4
e) Official Launching will be as follows:
Guest of Honour: Datin Dr Norain Abu Talib
Principal Director Oral Health, MOH
Date : 3rd April 2009 (Friday)
Time: 9.30 am
Venue: LG2 Concourse, Sunway Pyramid, Bandar Sunway
f ) All Council Members are invited.
R.S.V.P to Mr Steve of MDA Secretariat.
FEBRUARY 2009 11
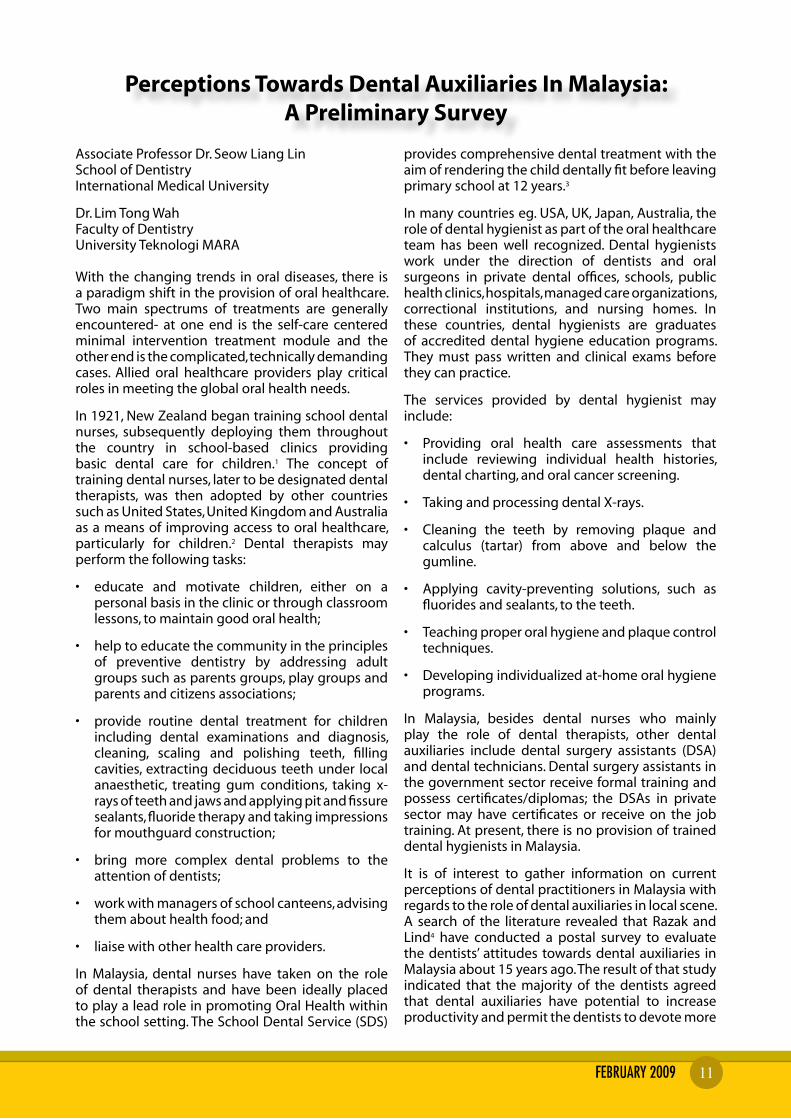
Perceptions Towards Dental Auxiliaries In Malaysia: A Preliminary Survey
Associate Professor Dr. Seow Liang Lin School of Dentistry International Medical University
Dr. Lim Tong Wah Faculty of Dentistry University Teknologi MARA
With the changing trends in oral diseases, there is a paradigm shift in the provision of oral healthcare. Two main spectrums of treatments are generally encountered- at one end is the self-care centered minimal intervention treatment module and the other end is the complicated, technically demanding cases. Allied oral healthcare providers play critical roles in meeting the global oral health needs.
In 1921, New Zealand began training school dental nurses, subsequently deploying them throughout the country in school-based clinics providing basic dental care for children.1 The concept of training dental nurses, later to be designated dental therapists, was then adopted by other countries such as United States, United Kingdom and Australia as a means of improving access to oral healthcare, particularly for children.2 Dental therapists may perform the following tasks:
• educate and motivate children, either on a personal basis in the clinic or through classroom lessons, to maintain good oral health;
• help to educate the community in the principles of preventive dentistry by addressing adult groups such as parents groups, play groups and parents and citizens associations;
• provide routine dental treatment for children including dental examinations and diagnosis, cleaning, scaling and polishing teeth, filling cavities, extracting deciduous teeth under local anaesthetic, treating gum conditions, taking x-rays of teeth and jaws and applying pit and fissure sealants, fluoride therapy and taking impressions for mouthguard construction;
• bring more complex dental problems to the attention of dentists;
• work with managers of school canteens, advising them about health food; and
• liaise with other health care providers.
In Malaysia, dental nurses have taken on the role of dental therapists and have been ideally placed to play a lead role in promoting Oral Health within the school setting. The School Dental Service (SDS)
provides comprehensive dental treatment with the aim of rendering the child dentally fit before leaving primary school at 12 years.3
In many countries eg. USA, UK, Japan, Australia, the role of dental hygienist as part of the oral healthcare team has been well recognized. Dental hygienists work under the direction of dentists and oral surgeons in private dental offices, schools, public health clinics, hospitals, managed care organizations, correctional institutions, and nursing homes. In these countries, dental hygienists are graduates of accredited dental hygiene education programs. They must pass written and clinical exams before they can practice.
The services provided by dental hygienist may include:
• Providing oral health care assessments that include reviewing individual health histories, dental charting, and oral cancer screening.
• Taking and processing dental X-rays.
• Cleaning the teeth by removing plaque and calculus (tartar) from above and below the gumline.
• Applying cavity-preventing solutions, such as fluorides and sealants, to the teeth.
• Teaching proper oral hygiene and plaque control techniques.
• Developing individualized at-home oral hygiene programs.
In Malaysia, besides dental nurses who mainly play the role of dental therapists, other dental auxiliaries include dental surgery assistants (DSA) and dental technicians. Dental surgery assistants in the government sector receive formal training and possess certificates/diplomas; the DSAs in private sector may have certificates or receive on the job training. At present, there is no provision of trained dental hygienists in Malaysia.
It is of interest to gather information on current perceptions of dental practitioners in Malaysia with regards to the role of dental auxiliaries in local scene. A search of the literature revealed that Razak and Lind4 have conducted a postal survey to evaluate the dentists’ attitudes towards dental auxiliaries in Malaysia about 15 years ago. The result of that study indicated that the majority of the dentists agreed that dental auxiliaries have potential to increase productivity and permit the dentists to devote more

MDA NEWS12
6. To the best of your knowledge, these are the roles and tasks that can be carried out by Dental Therapists:
Tasks Percentage of respondents (%)
YES No NOT SURE
MISSING DATA
i Intra & extra oral assessment 65 18 14 3
ii Scaling & polishing 71 11 16 2
iii Applying topical fluoride & fissure sealants
78 6 14 2
iv Taking dental radiographs 60 21 17 2
v Provide oral health education 84 4 10 2
vi Undertaking simple restorations on adults &children
50 28 17 5
vii Extracting deciduous teeth under local infiltration analgesia
55 25 14 6
viii Root debridement 23 53 19 5
ix Vital pulp treatments for deciduous teeth under supervision
36 39 19 5
x Placing preformed crowns on deciduous teeth under supervision
40 37 18 5
xi Taking impressions for adults & children
57 22 17 5
7. a) Will you employ or utilize dental hygienists in your practice, if legislation allowed it?
Percentage of respondents
YES 68%
NO 13%
NOT SURE 16%
MISSING DATA 3%
b) If the answer is yes, will you employ them (for private practitioner)
Percentage of respondents
FULL TIME 16%
PART TIME 5%
NOT RELEVENT 77%
MISSING DATA 2%
8. a) Will you employ or utilize dental therapists in your practice, if legislation allowed it?
Percentage of respondents
YES 49%
NO 16%
NOT SURE 32%
MISSING DATA 3%
time for more challenging tasks. However a majority felt uncomfortable to be held accountable for the performance of auxiliaries.
A questionnaire survey5,6,7 was conducted during the 65th MDA/FDI Scientific Convention June 2008, 300 questionnaires were handed out in person to the participants. 127 questionnaires were filled and returned providing response rate of 42%. The questionnaire consists of 13 questions pertaining to role of dental hygienists, dental therapists and also perceptions of dental practitioners towards these dental auxiliaries.
The first part f the questionnaire gathers demographic data. Two thirds of the respondents were local graduates and 63% of the respondents came from the government sector. 32% of the respondents came from private sector (17% from solo practice and 15% from group practice). 73% of respondents were female. 50% of the respondents were relatively new graduates (graduate from 2001 onwards).
The rest of the questions are as follow:
5. To the best of your knowledge, these are the roles and tasks that can be carried out by Dental Hygienists:
TasksPercentage of respondents
(%)
YES No NOT SURE
MISSING DATA
i Intra & extra oral assessment 57 32 8 3
ii Scaling & polishing 93 5 2 0
iii Applying topical fluoride & fissure sealants
71 17 9 3
iv Taking dental radiographs 60 27 11 2
v Provide oral health education 97 0 1 2
vi Undertaking simple restorations on adults &children
22 63 11 4
vii Extracting deciduous teeth under local infiltration analgesia
30 53 13 4
viii Root debridement 16 70 11 3
ix Vital pulp treatments for deciduous teeth under supervision
13 70 13 4
x Placing preformed crowns on deciduous teeth under supervision
15 66 15 4
xi Taking impressions for adults & children
50 33 12 5
FEBRUARY 2009 13
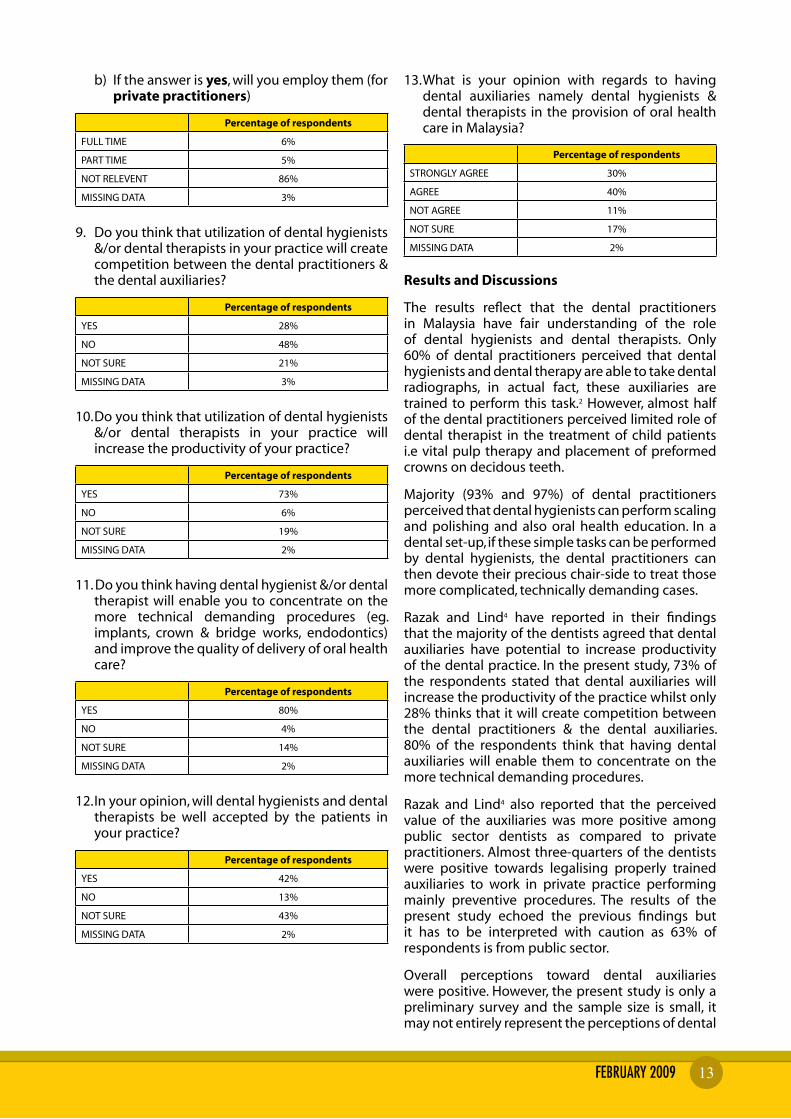
b) If the answer is yes, will you employ them (for private practitioners)
Percentage of respondents
FULL TIME 6%
PART TIME 5%
NOT RELEVENT 86%
MISSING DATA 3%
9. Do you think that utilization of dental hygienists &/or dental therapists in your practice will create competition between the dental practitioners & the dental auxiliaries?
Percentage of respondents
YES 28%
NO 48%
NOT SURE 21%
MISSING DATA 3%
10. Do you think that utilization of dental hygienists &/or dental therapists in your practice will increase the productivity of your practice?
Percentage of respondents
YES 73%
NO 6%
NOT SURE 19%
MISSING DATA 2%
11. Do you think having dental hygienist &/or dental therapist will enable you to concentrate on the more technical demanding procedures (eg. implants, crown & bridge works, endodontics) and improve the quality of delivery of oral health care?
Percentage of respondents
YES 80%
NO 4%
NOT SURE 14%
MISSING DATA 2%
12. In your opinion, will dental hygienists and dental therapists be well accepted by the patients in your practice?
Percentage of respondents
YES 42%
NO 13%
NOT SURE 43%
MISSING DATA 2%
13. What is your opinion with regards to having dental auxiliaries namely dental hygienists & dental therapists in the provision of oral health care in Malaysia?
Percentage of respondents
STRONGLY AGREE 30%
AGREE 40%
NOT AGREE 11%
NOT SURE 17%
MISSING DATA 2%
Results and Discussions
The results reflect that the dental practitioners in Malaysia have fair understanding of the role of dental hygienists and dental therapists. Only 60% of dental practitioners perceived that dental hygienists and dental therapy are able to take dental radiographs, in actual fact, these auxiliaries are trained to perform this task.2 However, almost half of the dental practitioners perceived limited role of dental therapist in the treatment of child patients i.e vital pulp therapy and placement of preformed crowns on decidous teeth.
Majority (93% and 97%) of dental practitioners perceived that dental hygienists can perform scaling and polishing and also oral health education. In a dental set-up, if these simple tasks can be performed by dental hygienists, the dental practitioners can then devote their precious chair-side to treat those more complicated, technically demanding cases.
Razak and Lind4 have reported in their findings that the majority of the dentists agreed that dental auxiliaries have potential to increase productivity of the dental practice. In the present study, 73% of the respondents stated that dental auxiliaries will increase the productivity of the practice whilst only 28% thinks that it will create competition between the dental practitioners & the dental auxiliaries. 80% of the respondents think that having dental auxiliaries will enable them to concentrate on the more technical demanding procedures.
Razak and Lind4 also reported that the perceived value of the auxiliaries was more positive among public sector dentists as compared to private practitioners. Almost three-quarters of the dentists were positive towards legalising properly trained auxiliaries to work in private practice performing mainly preventive procedures. The results of the present study echoed the previous findings but it has to be interpreted with caution as 63% of respondents is from public sector.
Overall perceptions toward dental auxiliaries were positive. However, the present study is only a preliminary survey and the sample size is small, it may not entirely represent the perceptions of dental
MDA NEWS14
practitioners in Malaysia towards dental auxiliaries. It serves to provide an idea of how well dental auxiliaries will be accepted in the oral healthcare system in Malaysia. A more comprehensive survey may be needed if we are to follow the trend of oral healthcare provision in developed countries and evaluate the repercussions in both the public and private sectors. This will also make an impact on the courses that will be provided by Dental Schools and Oral Health Science Education Centres. The authors wish to express deepest gratitude to those dental practitioners who have taken their precious time to complete the questionnaire.
References:
(1) Nash DA, Friedman JW et al. Dental Therapist: a global perspective, International Dental Journal 2008; 58(2): 61-70
(2) Baltutis L, Morgan M. The changing role of dental auxiliaries: A literature review. Australian Dental Journal 1998; 43(5): 354-358
(3) CJA Chen, R Latifah. Knowledge and Perception of Oral Health Promotion in Schools among Dental Nurses in Sarawak, Malaysia; Journal of Dental hygienists 2007; Spring;81(2):52.
(4) Razak IA, Lind OP. Dentists’ attitudes toward auxiliaries in Malaysia. Community Dental Health 1994 11(1): 24-28
(5) Haden NK, Morr KE, Valachovic RW. Trends in Allied Dental Education: An analysis of the past and a look to the future. Journal of Dental Education 2001; 65(5): 480-496
(6) Is there a shortage of dental hygienists and assistants in California? 2003 California Dental Survey
(7) The Nuffield Foundation Report: The education and training of personnel auxiliaries in dentistry (1993).
MDA Northern Zone Report for MDA News Letter
7th.Penang Dental Congress
There were 208 participants and 30 traders participated in the 7th. Penang Dental Congress which was held at Equatorial Hotel, Penang on 29th & 30th November 2008. The number of 208 participants is yet another new record for MDA Northern Zone CPD programme.The participants hailed from Perlis (in the north) to Johor (in the south), and even from Singapore and Indonesia. Amongst the speakers are Adjunct Assoc Prof. Ansgar Cheng, a prosthodontist from Singapore, Dr.Helena Lee, a periodontist, also from Singapore too. Assoc Prof. Gary Cheung, an endodontist from Hong Kong University and Assoc Prof. Seow Liang Lin from IMU. We received positive feedback from the participants and dental traders.
Assoc. Prof Dr. Seow Liang Lin, Dr. Helena Lee and Assoc. Prof. Dr. Ansgar Cheng- the speakers of the conference
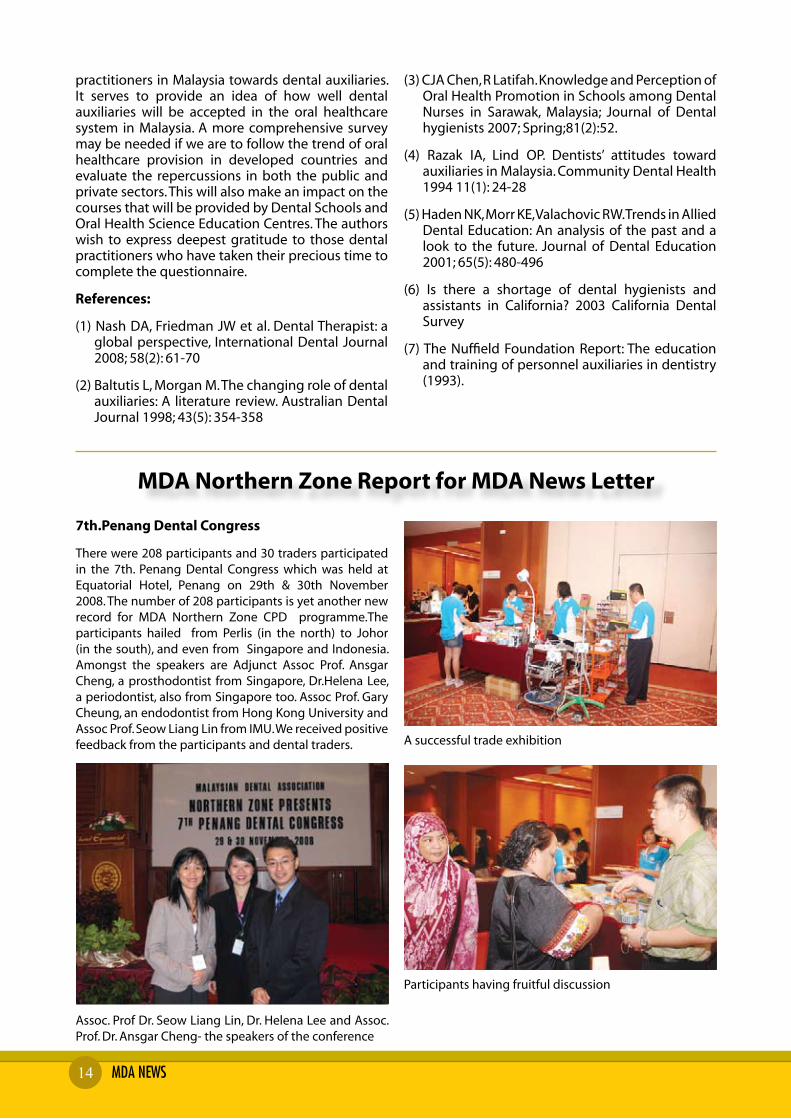
A successful trade exhibition
Participants having fruitful discussion

FEBRUARY 2009 15
Penang CPD Programme 8/2/2009
There were 99 members, 21 dental nurses and 20 dental traders participated in the CPD programme on 8th. February 2009 at G-Hotel.Penang. Dr.Rashid Tahir,a paedodontist talked on 1. Dental Caries and Restorative Material Choices in Children. 2. Tooth Defects and Their Management in Children and 3.Pulp Therapies in Children. Miss Priscilla Ho, an UK trained certified practitioner in therapeutic play skills talked about how to work with children in crisis (psychological and emotional).
Dr. Neo Gim Bok chairing the session
Dr. Rashid enlightening participants on management of child patients
Participants listening attentively to the lectures
Dr. Teh Tat Beng having a chat with traders
Participant having discussion at trade booth
Great crowd of participants

MDA NEWS16
Scientific Programme in conjunction with MDA Northern Zone AGM
67 members attended the scientific programme held in conjunction with MDA Northern Zone AGM, which was held at Bayview Hotel,Georgetown,Penang Amongst the speakers are Dato’ Prof. Dr. Hashim Yaacob, Dr. How Kim Chuan and Dr. Lee Soon Boon. Dato’ Prof.Dr. Hashim Yaacob talk about Detection of Premalignant Diseases by the General Dental Practitioner. Dr. How Kim Chuan covered 2 topic, topic 1:Preventive Interceptive Orthodontist and topic 2:Expand your clinical capability with Laser. Dr. Lee Soon Boon talked on Principles for optimizing Aesthetic Implant Restoration.
MDA Northern Zone AGM
64 members attended the MDA Northern Zone AGM. The following members were elected to the 2009/2010 Committee: Chairman : Dr.Teh Tat BengHon. Secretary : Dr.Koh Chou HuatHon. Treasurer : Dr. Tan Sock HooiCommittee Members : Dr. Lee Chee Wei : Dr. Chu Wai Weng
Hon. Auditor : Dr. Tan Siam Hong
Dr. Sivanesan presenting momento to Prof. Dato’ Dr. Hashim Yaacob.
The crowd for the MDA Northern zone AGM
Venue : Heritage Hotel, IpohDate : 12th April 2009(Sunday)Time : 8.00am to 5.30pmFee : MDA Member RM 50.00 Non-member RM 100.00 Dental Student RM 50.00CPD points : 3CPD points
Trade Exhibition: Whole day dental Trade Exhibition
Contace Person: Dr Chong Kum Soon H/P No;012-4584080 or 05-3133616
Please download the registration form from MDA website
Topic : Endodontic Manifestations-Their Challenge and clinical Management Speaker : Dr Tan Boon Tik
Topic : Coronal seal versus apical seal: Which one is more important Speaker : Dr Tan Boon Tik
Topic : Expand your clinical ability with laser Speaker : Dr How Kim Chuan
Topic : Clinical Anatomy For Dental Practitioners Speaker : Dr Wong Foot Meow
Topic : CDE Quiz And Assessment In Clinical Dentistry Speaker : Dr Wong Foot Meow
MDA-SEGi University College CPD
Upcoming CPD Event In Ipoh
Venue : SEGi University College, Subang JayaDate : 29/03/09Time : 8.30am - 1.00pm
Speakers : 1. Professor Dr K.M.Cariappa 2. Assoc. Professor Dr. Seow Liang Lin 3. Dr. Tan Boon Tik
Topics to be covered:
1. Maxillofacial Tauma - Current Acceptable Management
2. Partners in Fixed Prosthodontics - Techniques and Materials
3. Coronal Seal Versus Apical Seal: Which one is more important?

FEBRUARY 2009 17

MDA NEWS1�
CDE SELF ASSESSMENT IN CLINICAL DENTISTRYPART XXII- Part 1
AN ORAL SURGERY TALE OF 2 LADIES
Part XXII continues with the selection of 2 rather uncommon clinical cases, which will be featured in two parts. Although this presentation looks run-of-the-mill familiar, the aetiology, pathology and sequelae differs from the norm. In the management of any case with the view to avoiding complications, the fundamental importance of pre-operative assessment and treatment planning must always be strictly adhered to. The 2 cases will highlight to the practitioner that an in-depth knowledge of the clinical anatomy of oral and dental structures is essential to treat all cases consistently well. Comparison is a good teaching tool. When you hear, you forget, when you see, you remember and when you do you understand.
QUESTION 1:
This 55 year old Indian female medical practitioner from a beach resort town, complained of a soft tissue swelling on the lower (R) jaw of 6 months duration (Fig 1a). A pre-operative X-ray (Fig 1b) revealed a soft tissue shadow distal and inferior to tooth 48. Clinical examination and palpation reveal a mobile, smooth, firm elliptical swelling at the right submandibular region. Certain features indicate that this case may not be so straight forward.
Figure 1a
Figure 1b
DR WONG FOOT MEOWBDS(Mal), FDSRCPS (Glasg), FICD, AM(Mal), FICOIHonorary Associate Clinical Professor,ICE,Warwick Medical School,UK
(i) What can you see in Fig 1a? What would you ask in your history taking? What are the most likely causes of the swelling and why? What investigations would you order and would fine needle aspiration biopsy and Papanicolaou stain have a place in your armamentarium?
(ii) Fig 1c to 1i shows the sequence of a surgical procedure. What do you call this procedure? Describe what you see?
Figure 1c
Figure 1d
Figure 1e

FEBRUARY 2009 19
Figure 1f
Figure 1g
Figure 1h
Figure 1i
(iii) Discuss the surgical anatomy and what important anatomical structures would you encounter when operating in this area ?(Fig. 1L and lm)
(iv) Certain lesions present commonly in this manner in this particular general area. Looking at the dissected specimen, what do you think this lesion is (Fig 1i)? How is the wound primarily closed? (Fig 1h and 1j) Would bleeding be a problem?
What common complication can occur (Fig 1k)?
Explain the pathogenesis of this particular complication and would it leave any long term effects? (Fig 1o)
(v) What sort of test would you initially sent this specimen for and why (Fig 1i)? In this case the pathologist requested for an additional test. Why would special tests be sometimes required after a histopathology diagnosis?
(vi) List 5 features which indicate that this intricate looking lesion is benign (Fig 1g and 1i).
(vii) The post-operative scenario confirmed my deduction (Fig 1h). Why?
(viii) Oral Surgeons often have “gut feeling” on the behaviour of a tumour during an ablative operation. Why should the “benign feel” of the specimen removed be most heartening to the operator. Is this lesion in any way related to teeth (Fig 1a & 1b)?
(ix) Consider Fig 1a, 1L and 1m together and attempt to correlate and reconcile the clinical anatomical relevance. What structures should you attempt to avoid? what is the plane of your dissection ? Would haemostasis be a major problem?
Figure 1L
Figure 1m
Figure 1J Figure 1k

MDA NEWS20
ANSWERS FOR CDE SELF ASSESSMENT IN CLINICAL DENTISTRY
PART XXII- Part 1AN ORAL SURGERY TALE OF 2 LADIES
DR WONG FOOT MEOWBDS(Mal), FDSRCPS (Glasg), FICD, AM(Mal), FICOIHonorary Associate Clinical Professor,ICE,Warwick Medical School,UK
(i) History taking. Although it is a tedious process to take note of all negative findings, this process contributes to the final diagnosis. The following notes are a case in point. Notice in Fig 1a that there is an elliptical swelling several centimetres in diameter at the angle of the jaw beneath the platysma muscle. Clinical history revealed that the lump is painless, slowly enlarging without any discomfort on swallowing. Swelling size is not related to meals. (ie no pre or post-prandial swelling) The overlying skin is not inflamed, smooth, of normal texture and colour and not adherent to the tumour. The swelling does not move on swallowing. The tumour is mobile, slightly fluctuant but firm on palpation. No lymphadenopathy or enlarged lymph nodes discernable in the vicinity. Intraorally, there is no soft tissue swelling, sinus or tenderness in the sulcus adjacent to the apices of the roots. All posterior teeth are not tender to percussion. The oral mucosa appears normal and the tonsils appear to be symmetrical. All the above signs give a strong indication of the behaviour and prognosis of the swelling.
(i) a. Differential Diagnosis
A history of risk factors is very relevant to rule out the possibility of a primary malignancy or secondaries. The following will have to be considered in your differential diagnosis:
A. Benign neoplasms eg growths from salivary glands, muscle, nerves, fat or fibrous tissue. This looks to be the likeliest causative factor in this particular case.
B. Developmental causes eg Branchial cyst
C. Infectious and inflammatory causes eg glandular fever, HIV infection, and Sarcoidosis. We have seen a few cases of tuberculosis (a disease making a serious comeback in Malaysia) which needs to be considered both as a possible diagnosis
and as a factor affecting management. Most patients with cervical lymph node enlargement caused by tuberculosis have reactivation (‘secondary’ or post-primary) tuberculosis in which a previous quiescent infection becomes reactivated. This localized infection may or may not be accompanied by pulmonary disease though there may be radiological evidence of past tuberculosis on chest radiograph. Cervical tuberculous lymphadenitis is common in migrant workers especially those from the poverty stricken countries. If you see foreign estate workers on a regular basis , there is always a possibility of an acquired infection. Atypical mycobacterial infection is a disease which often affects the cervical lymph nodes but is almost always seen in children or the immunosuppressed.
D. Malignant neoplasms. As discussed earlier, the behaviour and history of this case suggest a benign rather than an aggressive lesion
E. Metastatic malignancy appears unlikely and this lesion is not typical of a cervical lymph node metastasis such that it must be considered to be malignant until proved otherwise. The combination of features that would be suggestive of metastasis is the patient’s age (should be considered a possible cause in any patient aged over 45), the site (consistent with a cervical lymph node), the firm consistency and lack of tenderness. Fixation to the skin or other structures would be almost conclusive of malignancy but is a late sign. If the patient is a smoker and drinker there will be an increased risk of malignancy. Either a squamous carcinoma or adenocarcinoma is then likely. Melanoma and other malignancies are further possible causes especially in HIV positive patients.

FEBRUARY 2009 21
F. Lymphadenitis secondary to a local cause is common and so must be considered. However there is no tenderness on palpation to suggest an inflammatory cause. The Xrays do not suggest a dental origin.(Fig 1b) If this were a reactive inflammatory enlargement, the most likely source of infection would be a dental, pharyngeal or skin infection. The patient has no potential source of dental infection in the lower right jaw, no tooth is tender to percussion nor associated with overt infection, making it an unlikely cause. The skin looks normal. (Fig 1a)
(i) b. Investigations and rationale. Clinically, all signs indicate that this lesion is benign, meaning that there is a lesser element for urgency. We therefore opted for an excision biopsy as opposed to an incisional biopsy. However the critical requirement when malignancy is suspected is to obtain tissue speedily for microscopic diagnosis. All other investigations are less important at this stage. Two techniques are in common use, the fine-needle aspiration biopsy and the surgical incisional biopsy.
In this instance a suitable combination of investigations would be fine-needle aspiration and/or excision biopsy, dental radiographs, vitality test and possibly ultrasound scan. The sialogram would have to be performed if a salivary gland origin had been thought possible after clinical examination.
Fine-needle aspiration biopsy. As this procedure is seldom encountered by the dental practitioner , a short explanation is provided here on the mechanics of this particular test.
The aspirate will show cells from the lesion spread as a single layer and stained with the Papanicolaou stain. Consider a typical finding if the needle aspiration biopsy is positive as in the case of a metastatic neoplasm. Papanicolaou dye stains the nuclei dark blue, keratin orange and the cytoplasm of nonkeratinized epithelial cells turquoise. The cells in a metastatic carcinoma are almost all epithelial cells which are shown by their prominent cytoplasm and by the presence of keratinization in some of them. The larger cells have angulate polygonal cytoplasm typical of squamous epithelial cells. In a sinister scenario, the nuclei of the cells will range markedly in size from small hyperchromatic nuclei to very large irregular
nuclei. At higher power the chromatin pattern is expected to be coarse. Such features indicate malignancy and the keratinized cells indicate a squamous carcinoma. The deduction is that if normal lymphocytes were found elsewhere on the slide, it will indicate that the carcinoma is in a lymph node and is therefore a metastasis.
(ii) Mandibular Vestibular Approach
The mandibular vestibular approach is utilised in this case as it affords a hidden oral scar and allows relatively safe access to the designated surgical area. An excision biopsy was performed by way of surgical enucleation of the tumour mass in toto vide this particular intraoral approach because of cosmetic reasons and to avoid going under General Anaesthesia so that the patient need not take many days off work. The technique involves an initial incision made in the oral vestibule through the buccinator muscle (fig. 1c and 1d) The tumour mass is defined by sharp dissection (fig 1e and 1f ) Notice the superficial nerves attached to tumour mass (fig 1g). Fig 1h shows the surgical bed of the tumour after removal. The buccal pad of fat was avoided.
(iii) Clinical Anatomy
When operating conservatively around this general area , salient aspects of oral clinical anatomy should be considered and understood as follows:
a. Vestibule. The vestibule of the mouth is bounded laterally and anteriorly by the lips and cheeks and medially by the outer surfaces of the teeth and gingiva. The lips and cheeks form a flexible wall to the oral vestibule which can therefore be distended to accommodate food, fluid or air. The lips and cheeks make up a muscular sheet covered on the outside by skin and on their inner surfaces by mucous membrane. This area should not be compromised, otherwise, post-operatively the patient will complain of food accumulation in the vestibule.
b. Buccinator. Buccinator muscle is the major muscle of the cheek. It is attached above to the maxilla and below to the mandible close to the line of reflection of the gingival mucoperiosteum from the alveolar processes in either case lateral to the molar teeth. . Posteriorly it is attached

MDA NEWS22
to the pterygomandibular raphe, through which its fibres are continuous with superior constrictor muscle. Anteriorly the fibres sweep into the upper and lower lips to intermingle with the fibres of orbicularis oris at the modiolus.
Note: The buccal nerve passes on to the outer surface of buccinator muscle from under cover of the mandible and is closely related to the external oblique line of the mandible.
c. Orbicularis Oris. The muscular sheet of the lip is orbicularis oris. Fibres arise from a variety of sources being continuous with those of buccinator muscle and other radial dilator muscles of the oral sphincter. Several slips of muscle arise from the incisive fossae of both mandible and maxilla. Bleeding into the spaces between the muscles produced the appearance seen in Fig 1k. Correlate Fig 1k with Fig 1n to appreciate the role played by muscles and tissue planes in determining the accumulation of blood if haemostasis is not secured properly after a soft tissue dissection.
d Buccal pad of fat. Relationship between the buccal fat pad and the retromolar region. Note that in Fig 1L, the buccal pad of fat extends inferiorly to just above the occlusal plane. Incisions made through the buccinator muscle superior to the occlusal plane cause entry into the fat pad and makes the dissection very messy indeed. The buccal fat pad consists of a main body and four extensions: ie buccal, pterygoid, pterygomandibular and temporal. The body is centrally positioned. The buccal extension lies superficially within the cheek and the pterygoid, pterygomandibular and temporal extensions are more deeply situated. The buccal extension is the most superficial segment of the fat pad and imparts fullness to the cheek. It enters the cheek below the parotid duct and extends along the anterior order of the masseter as it descends into the mandibular retromolar region. This is significant as it overlies the main portion of the buccinator muscle as it crosses the cheek.
Surgical considerations: (Figs 1c to 1g) In the cheek, the fat is anterior to the
ramus. Its caudal extension intraorally is on a plane tangential with the occlusal surface of the mandibular third molar. Its anterior limit is marked by the facial vessels, which are in the same plane as the buccal fat pad. Avoidance of the buccal pad of fat and hence the facial vessels will ensure a bloodless field. The buccal extension of the fat pad is limited by the masseteric fascia. A deep extension of the masseteric fascia blends with the fascia along the lateral surface of the buccinator. This fascial layer lines the deep surface of the buccal fat that is in contact with the buccinator.(Fig 1L).
After incising the oral mucosa, the dissection proceeds beyond the connective tissue and buccinator deepening to approach the superficial layer of deep cervical fascia (SLDCF) in Fig 1m.
Inferior and lateral limits of the growth. The growth is actually situated between the superficial layer of the deep cervical fascia and buccinator/periosteum. Fig 1m illustrates coronally the path of dissection. The bold dissection is made through the buccinator muscle all the way to the superficial layer of deep cervical fascia (SLDCF) . The following structures are carefully pushed aside and avoided ie the submandibular gland (SG), periosteum (P) of mandible (Mand),. FA=facial artery(in our case was merely pushed aside and not ligated as illustrated) ; MM=masseter muscle; ZA=zygomatic arch; VII=marginal mandibular branch of the facial nerve (Protected by SLDCF)
The capsule of the submandibular salivary gland was in danger of being breached during this dissection, and the gland is carefully retracted inferiorly. A consistent submandibular lymph node (node of Stahr) is usually encountered in the area of the premasseteric notch and can be retracted superiorly or inferiorly to avoid the facial artery just anterior to the node, deep to the superficial layer of deep cervical fascia. The dissection should be parallel to the inferior border of the mandible because it is the most avascular area in which the masseter and medial pterygoid muscles join.( Pterygomasseteric sling)

FEBRUARY 2009 23
(iv) The surgical defect was closed in layers after haemostasis was secured using 4’0’ chromic catgut for the deeper layers and 4”0” vicryl for the oral mucosa. Copious bleeding was not an issue as the buccal pad of fat and facial vessels were studiously avoided. The excised tumour was preserved in formalin and submitted for histopathology. The initial histopathological report was inconclusive and was reported as follows: Sections of the tissue show fibro-myxoid tissue within which are sheets of spindle shaped cells with fibrillary cytoplasmic extensions seen as elongated “bent” nuclei. In a few areas pallisading of cell nuclei are seen, Mitosis and necrosis are not present. The lesion is not infiltrative. Cystic areas are seen. The initial interpretation of the swelling is that of a benign neural tumour most probably a schwannoma or a neurofibroma.
(v) As the initial report was non-commital and inconclusive . The patient being a doctor was slightly paranoid and insisted that part of the specimen was sent for immunohistochemistry stain for a definitive diagnosis. The tumour cells were found to be immunopositive for vimentin and S100protein. They are negative for actin and desmin. The above deduction allowed for a definitive diagnosis of a benign Neurilemmoma.
(vi) Together with the findings in para 1(i) above, the additional five features which indicate this lesion is benign are that the tumour surface is comparatively avascular, smooth and spherical
with well-defined lobules. The surface texture shows normal connective tissue and dearth of tumour blood vessels indicating slow coordinated growth consistent with a benign lesion. .In addition, the specimen allows clean dissection with no infiltration, adhesions or extensions to the surrounding tissue.
(vii) Notice the bloodless surgical bed and firm normal vascular surrounding area with no tethering, adhesions or tumour supplying vessels.
(viii) During this supposedly difficult operation, well defined tissue dissection planes, bloodless field and firm texture of the specimen gives an optimistic air to the final outcome. This lesion is not related to teeth and for a diagnosis of neurilemmoma to be made in the submandibular region is indeed a rarity. Collate fig 1k and 1n. The pattern of the subcutaneous ecchymosis follows the modiolus, the facial muscles and tissue planes.
(ix) Fig 1m clearly illustrates the plane of dissection followed . The plane of dissection is between the buccinator and platysma muscle.and did not go beyond the SLDCF. As the facial vessels (artery and vein) is not breached haemorrhage and subcutaneous ecchymosis is not a problem because the masseter and medial ptyergoid muscles are relatively avascular at the inferior border of the mandible.
MDA/Listerine Community Project
Reported by: Dr. V. Nedunchelian
1) CODE NAME: “LISTERINE MOBILE MOUTH TOUR OF MALAYSIA”- The Truck equipped with OHI devices assisted by trained OH Instructors tours the Whole Peninsular Malaysia advocating the importance of mouth rinsing.
2) Launching was done by MDA President Dr. S. Sivanesan.
Date : 12th February 2009 (Thursday) Time : 10.30 am
3) Covered by most medias- STAR, SUN, UTUSAN, BERITA HARIAN, NANYANG SIANG PAU
4) Attended by:
a) Dr. S. Sivanesan - President
b) Dr. V. Nedunchelian - Chairman Community Project
c) Dr. S. Ratnasothy - Assistant Financial Secretary
d) Dr. Shubon Sinha Roy - Past President
5) Special thanks to Ms. Joyce Lee the MD and Tham Kok Jau Senior Brand Manager of J & J for their support.


Preliminary Announcement
A Multidisciplinary Approach: Solution for Optimal Clinical Success.
Scientific Convention 20 CPD points
Oral Surgery:Professor Malcolm Harris (UK)
Dr Wong Foot Meow (Malaysia)Professor Ho Kee Hai (Singapore)
Dr Ng Fooi Chin (Singapore)
Halitosis:Dr Thomas Ip (Hong Kong)
Teeth Whitening:Dr Jenny Shen (United States)
Piezo Surgery:Professor Winai Kittidumkerng (Thailand)
Periodontics:Professor Zee Kwan Yat (Australia)
Implantology:
Professor Niklaus Lang (Switzerland)
Orthodontics:Dr Derek Mahony (Australia)
Dr How Kim Chuan (Malaysia)
Prosthodontics:Professor Toh Chooi Gait (Malaysia)
Associate Professor Dr Seow Liang Lin (Malaysia)
Restorative:Dr Michael Dieter (Germany)
Practice Management:Dr William Cheung (Hong Kong)
Oral Health:Datin Dr Norain Abu Talib (Malaysia)
Oral Pathology/Oral Medicine:Dato' Prof Dr Hashim Yaccob (Malaysia)
Dental ProtectionDr Kewin Lewis (United Kingdom)
Speakers
Main Sponsor: Co-Sponsors:
Date: 25-28 June 2009Venue: Equatorial Hotel Penang
Guest of Honour: YB Dato’ Liow Tiong Lai The Honourable Minister of Health Malaysia
Hands-on Sponsors:
1. Orthodontic Mini-implant – Theory and Clinical Practice - Dr Derek Mahony (Australia) Course Fee: RM650 (Goat Jaw used) Hour: 8 hours CPD : 6 points Limited to 30 pax
2. Advance Piezo Surgery on bone graft, sinus lift and implant – Dr Winnai (Thailand) Course Fee: RM650 (Goat Jaw used) Hour: 8 hours CPD: 6 points Limited to 24 pax
3. Surgical technique on impacted wisdom tooth removal – Dr Wong Foot Meow (Malaysia) Course Fee: RM 500 (Goat Jaw used) Hour: 8 hours CPD: 6 points Limited to 30 pax
4. Creating Arts with Composite: Anterior aesthetics and posterior challenges – Dr Michael Dieter (Germany) Course Fee: RM 500 Hour: 8 hours CPD: 6 points Limited to 30 pax
5. Mediation Technique to handle conflict with patients – Dr Kewin Lewis (UK) Course Fee: RM200 Hour: 8 hours CPD : 6 points Limited to 50 pax
6. Smoking Cessation Workshop for dentist – Nicotine Addiction Research Collaboration Centre (NARCC Malaysia) Course Fee: FREE for registered participants Hour: 8 hours CPD: 6points Limited to 30 pax
25 June 2009Hands-On

MDA NEWS26
PETALING JAYA1) A very established Dental Clinic for sale.
Doctor retiring. Payment terms negotiable. Call : Dr. Paul Lee – 03-7877 5577
2) Full or part-time Dental Surgeons required to work in PJ. Favourable teems. Saturday and Sunday off. Interested please contact, Tel: 03-79567933; fax: 03-79567933
3) Dr Michael Ong Ah Hup BDS (S’pore), MSc (London, UK) Oral & Maxillofacial
Surgery, Cert IAOMS, FICD, FADI, FICCDE, Fellow of IAOMS/ Diplomate & Fellow of ICOI (USA) Consultant Oral & Maxillofacial Surgeon/ Implantologist
For appointment, please call Tel No: 03 - 74919191 ext 8875, Sunway Medical Centre.
Mobile: 017 - 3337246 Email: [email protected]
KUALA LUMPUR1) Vacancies DENTAL SURGEONS AND SPECIALISTS Attractive salary and remuneration based on your experience and expertise. Flexible working hours can be
arranged. Please direct enquiries and submit resume to: Kuala Lumpur International Dental Centre (KLIDC) No. 33, Second Floor, Jalan Yap Kwan Seng, 50450 Kuala Lumpur.
(Attn: Ms. Kok / Personal Assistant) Email: [email protected] Tel: 03-22890896 Fax: 03-22890890
2) SPECIALIST ORAL-FACIAL SURGERY 39-7, The Boulevard, Mid-Valley City,
Lingkaran Syed Putra, 59200 Kuala Lumpur. Tel 03-228 73700; Fax 03-228 74700
3) Full/Part time Dental Surgeon needed in KL. Must be regestered with MDC.Pleasant personality. Please call 016-2224756
KLANG1) GDP and / or Specialist wanted in a dental clinic in Klang. Part-time / Full-time. Please contact 03-33414007
2) Established group dental practice in Klang needs an assistant Dental Surgeon to work in Shah Alam and Pandamaran Interested contact 03-33710030
SABAH1) Dental Speacialists (any specialities) & Dental Surgeons at
Rafflesia Medical Centre Sdn Bhd; Kota Kinabalu, Sabah & their associated dental clinics. Good & attractive remuneration. More information, phone / SMS : 016-830 0183. Fax : 088-242 802. Email : [email protected]. Website : rafflesiamedicalcentre.com
2) CLINIC FOR SALE, TAWAU, SABAH Twenty two years established running clinic available for
sale, fully registered. Doctor retiring soon. If interested, please kindly contact Dr. Ghulam, 089-777277 (office);
019-8832242
IPOH Assistant Dental Surgeon Wanted Kuan Dental Surgery, 38 Lorong Taman Ipoh 1, Taman Ipoh Selatan, 31400 Ipoh, Perak. Contact No: 05-5457033
JOHOR BAHRU1) A well established dental clinic, practicing high quality
dentistry, is for sale. Please contact Dr. Tan 016-773 9924 email: [email protected]
(2) VACANCY FOR FULL-TIME DENTIST A dental clinic in Johor set up since 1999 looking for full /
part time dentist. The clinic has 2 new dental chairs & complete range of
instruments for general dentistry and credit card service. Please contact Dr. Lam at 012 – 766 2397 or Tel / Fax : 07 – 433 4452. Email : [email protected]
GOOD LOCATIONS FOR NEW CLINICSNew shophouses available in new townships for dental clinics
• Bestari de Kota, Kota Damansara• Putra Point, Putra Heights, Subang (Sime UEP project)• Pinggiran USJ, Subang (Sime UEP project)Favourable terms. Tel: 012-3240556Email: [email protected]
Autoclave For SaleTuttnauer Nova Class B autoclave for sale with certificate from DOSHBrand New condition (less than 2 years old) Interested call Mrs Teh / Michelle at 0326910553
Notice:Part-time locum/ Full time dentist required in clinic in Damansara.Attractive percentage.Pls call 019-3566519 for details.
CLASSIFIEDS

CLASSIFIEDS
C
M
Y
CM
MY
CY
CMY
K
A4 ad.pdf 11/24/2008 6:38:48 PM

C
M
Y
CM
MY
CY
CMY
K
Colgate Total 12 Ad OL.pdf 13/11/08 12:49:10 PM







![[L'angolo del PhD] Alessandro Palma - XXII Ciclo - 2009](https://static.fdocuments.us/doc/165x107/568c47271a28ab49168cb35b/langolo-del-phd-alessandro-palma-xxii-ciclo-2009-56f32311cfd2c.jpg)