February 2008 Vol. 3, No. 2 Quality Improvement...
12
IN THIS ISSUE p. 4 Data needs to instigate change Don’t waste your time collecting data unless its part of a closed control loop that leads to changes in your hospital. p. 5 Real-time data can drive up SCIP performance Even small hospitals with limited resources can perform well on Surgical Care Improvement Project measures by doing real-time data collection and getting back to clinicians immediately if there’s a miss. p. 10 Focus on infections to ensure CMS reimbursement Hospitals that plan to screen every single patient for urinary catheter–associated infections to avoid paying for preventable conditions may want to keep this in mind: The government will be watching. p. 12 The Joint Commission releases proposed NPSGs Field review focuses on medication safety, hospital-acquired infections, medication reconciliation, and patient involvement in their own care. Hourly rounding helps boost scores on HCAHPS As hospitals brace for the public unveiling of their pa- tient satisfaction scores, one expert is recommending hourly rounding as a way for organizations to improve their ratings as well as their care. “Hourly rounding is very, very popular, and it’s popu- lar for a variety of reasons,” says Deirdre Mylod, PhD, vice president of public policy for Press Ganey Associates, Inc., and an expert on Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS). “In terms of targeting some of the key drivers of pa- tients’ perceptions that go into HCAHPS . . . if you have someone checking on you on an hourly basis, you essen- tially tick off almost all of the major things that are driv- ing the important outcomes.” A 2006 study by Press Ganey of more than 2.3 million patients found the five areas that drive up overall scores. They are: Attentiveness to personal needs ➤ Responsiveness to concerns/complaints Level of courtesy/respect with which the nurses treat patients Care with which doctors listen to patients Extent of efforts by staff members to help with pain Improve in four key domains Hourly rounding, Mylod says, can improve patients’ perceptions in four of those areas. “Staff ask, ‘Is there something else I can do for you, so patients know someone is going to come back and they will never feel alone and just left here,” Mylod says. “You’ve taken care of attention to personal needs.” Checking in on patients every hour will not only help patients deal with their pain; it will also likely improve that patient’s perception of the hospital’s responsiveness to concerns and complaints, she says. And hourly check- ins forge a stronger bond between nurses and patients, thus improving ratings on the level of respect with which nurses treat patients. “It’s a very effective strategy,” Mylod says. “You get all of it in one nice package.” Kent Jackson, MA, LMSW, director of children’s specialty services, behavioral health, and leader of the patient-family experience team at St. Luke’s Hospital in Cedar Rapids, IA, agrees. St. Luke’s, which scored in the 95th percentile in 2006, won Press Ganey’s Success Story Award in 2007. That high performance is translating into good scores on the HCAHPS, although Jackson sees areas in which his 420-bed hospital could improve. “We’re just now at a point where we’re planning to implement hourly rounding later this year,” Jackson ➤ ➤ ➤ ➤ “It’s a very effective strategy. You get all of it in one nice package.” —Deirdre Mylod, PhD > continued on p. 2 February 2008 Vol. 3, No. 2 Quality Improvement REPORT Data collection strategies for The Joint Commission, CMS, and beyond
Transcript of February 2008 Vol. 3, No. 2 Quality Improvement...

IN THIS ISSUE
p. 4 Data needs to instigate changeDon’t waste your time collecting data unless its part of a closed control loop that leads to changes in your hospital.
p. 5 Real-time data can drive up SCIP performanceEven small hospitals with limited resources can perform well on Surgical Care Improvement Project measures by doing real-time data collection and getting back to clinicians immediately if there’s a miss.
p. 10 Focus on infections to ensure CMS reimbursementHospitals that plan to screen every single patient for urinary catheter–associated infections to avoid paying for preventable conditions may want to keep this in mind: The government will be watching.
p. 12 The Joint Commission releases proposed NPSGs Field review focuses on medication safety, hospital-acquired infections, medication reconciliation, and patient involvement in their own care.
Hourly rounding helpsboost scores on HCAHPS
As hospitals brace for the public unveiling of their pa-
tient satisfaction scores, one expert is recommending
hourly rounding as a way for organizations to improve
their ratings as well as their care.
“Hourly rounding is very, very popular, and it’s popu-
lar for a variety of reasons,” says Deirdre Mylod, PhD,
vice president of public policy for Press Ganey Associates,
Inc., and an expert on Hospital Consumer Assessment of
Healthcare Providers and Systems (HCAHPS).
“In terms of targeting some of the key drivers of pa-
tients’ perceptions that go into HCAHPS . . . if you have
someone checking on you on an hourly basis, you essen-
tially tick off almost all of the major things that are driv-
ing the important outcomes.”
A 2006 study by Press Ganey of more than 2.3 million
patients found the five areas that drive up overall scores.
They are:
Attentiveness to personal needs ➤
Responsiveness to concerns/complaints
Level of courtesy/respect with which the nurses
treat patients
Care with which doctors listen to patients
Extent of efforts by staff members to help with pain
Improve in four key domains
Hourly rounding, Mylod says, can improve patients’
perceptions in four of those areas. “Staff ask, ‘Is there
something else I
can do for you,
so patients know
someone is going
to come back and
they will never
feel alone and just left here,” Mylod says. “You’ve taken
care of attention to personal needs.”
Checking in on patients every hour will not only help
patients deal with their pain; it will also likely improve
that patient’s perception of the hospital’s responsiveness
to concerns and complaints, she says. And hourly check-
ins forge a stronger bond between nurses and patients,
thus improving ratings on the level of respect with
which nurses treat patients.
“It’s a very effective strategy,” Mylod says. “You get
all of it in one nice package.”
Kent Jackson, MA, LMSW, director of children’s
specialty services, behavioral health, and leader of the
patient-family experience team at St. Luke’s Hospital in
Cedar Rapids, IA, agrees. St. Luke’s, which scored in the
95th percentile in 2006, won Press Ganey’s Success Story
Award in 2007. That high performance is translating into
good scores on the HCAHPS, although Jackson sees areas
in which his 420-bed hospital could improve.
“We’re just now at a point where we’re planning to
implement hourly rounding later this year,” Jackson
➤
➤
➤
➤
“ It’s a very effective strategy.
You get all of it in one nice
package.”
—Deirdre Mylod, PhD
> continued on p. 2
February 2008 Vol. 3, No. 2
Quality Improvement RepoRt
Data collection strategies for The Joint Commission, CMS, and beyond

© 2008 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Quality Improvement ReportPage 2 February 2008
HCAHPS
says. “That alone should take care of the things where
we’re not doing as well as I think we should be.”
Not only does hourly rounding help with HCAHPS,
research shows it reduces patient falls, pressure ulcers,
and call-light usage, Jackson says.
Study best practices
St. Luke’s, he says, began its drive to improve patient
satisfaction scores back in 2004 when the hospital dis-
covered it had dropped into the 49th percentile on Press
Ganey scores.
The patient-family experience team studied best prac-
tices and immediately instituted:
Manager rounding on inpatients
A no-point policy in which staff members accompany
patients and family who look lost to their destination
instead of pointing or giving directions
➤
➤
< continued from p. 1
A scripting policy whereby staff members asked pa-
tients at the end of every encounter, “Is there any-
thing else I can do for you?”
Within six months, St. Luke’s scores shot up from the
49th percentile to the 93rd. The facility’s ratings subse-
quently rose to the 95th.
Ask patients about their priorities
St. Luke’s has undertaken many other initiatives
since 2004, including asking every patient on admis-
sion for the top two or three things it can do to provide
great care and writing those things down on the pa-
tient’s whiteboard.
More recently, the hospital has:
Instituted a “Take Five” program in which staff nurs-
es sit with patients at the beginning of every shift and
talk to them about their concerns.
Turned waiting rooms into calming rooms by stock-
ing activity carts with laptops, DVD players, movies,
and games.
➤
➤
➤Editorial Advisory Board Quality Improvement Report
Group Publisher: John Novack
Senior Managing Editor: Lisa Buckley, [email protected]
Contributing Editor: Tami Swartz
Sallie M. Gatlin, CPHQDirector, Quality Resource ManagementPampa Regional Medical Center Pampa, TX
Jane M. Jones, MT(ASCP), MSHS, CPHQPerformance Improvement Director Oaklawn Hospital Marshall, MI
Robert Marder, MDPractice Director of Quality and Patient Safety The Greeley Company Marblehead, MA
Barbara Oliver, RNPatient Safety DirectorManager of Quality Improvement Northwest Hospital Center Randallstown, MD
Geoffrey PagePerformance Improvement Coordinator Mount Sinai Hospital Chicago, IL
Bruce Siegel, MD, MPHProfessor George Washington University School of Public Health and Health Services Washington, DC
Marla Smith, MHSAAssociate Consultant, Quality and Patient SafetyThe Greeley Company Marblehead, MA
Quality Improvement Report (ISSN: 1934-5488) is published monthly by HCPro, Inc., 200 Hoods Lane, Marblehead, MA 01945. Subscription rate: $299/year. Postmaster: Send address changes to Quality Improvement Report, P.O. Box 1168, Marblehead, MA 01945. • Copyright © 2008 HCPro, Inc. All rights reserved. Printed in the USA. Except where specifically encouraged, no part of this publication may be reproduced, in any form or by any means, without prior written consent of HCPro, Inc., or the Copyright Clearance Center at 978/750-8400. Please notify us immediately if you have received an unauthor-ized copy. • For editorial comments or questions, call 781/639-1872 or fax 781/639-2982. For renewal or subscription informa-tion, call customer service at 800/650-6787, fax 800/639-8511, or e-mail: [email protected]. • Visit our Web site at www.hcpro.com. • Occasionally, we make our subscriber list available to selected companies/vendors. If you do not wish to be included on this mailing list, please write to the marketing department at the address above. • Opinions expressed are not necessarily those of QIR. Mention of products and services does not constitute endorsement. Advice given is general, and readers should consult professional counsel for specific legal, ethical, or clinical questions. QIR is not affiliated in any way with The Joint Commission, which owns the JCAHO and Joint Commission trademarks.
Facilities can suppress data
Hospitals unhappy with their patient satisfaction scores
can suppress their data until March 2009 without a finan-
cial penalty.
In January, hospitals that began submitting data on
Hospital Consumer Assessment of Healthcare Provid-
ers and Systems (HCAHPS) in October 2006 received pre-
view reports of their performance from CMS. Organizations
have 30 days to decide whether they want to suppress that
information.
“But consumers would see that,” says Deirdre Mylod,
PhD, vice president of public policy for Press Ganey Associ-
ates, Inc. “And each hospital would have to consider: ‘How
are your consumers going to react?’
Hospitals that suppress their data after March 2009 will
forfeit 2% of their Medicare payment update.
For more information, go to www.hcahps.org.

© 2008 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Quality Improvement Report Page 3February 2008
Assumed every single patient and family has some
level of anxiety that can include fear and terror.
Made follow-up calls on 100% of inpatients. Re-
search shows 25%–33% of all patients have a clini-
cal issue that needs to be addressed once they return
home, he says.
“What I’ve been saying is that the movement toward
patient safety and quality and patient satisfaction are all
part of one thing,” Jackson says. “The point is you can’t
➤
➤
do well on patient satisfaction if you’re not focused on
patient safety and quality. They’re going to get you re-
sults, but they’re also the right thing to do.”
Mylod echoes that view.
“Quality improvement is quality improvement,” she
says. “If you’re using data now, and you continue to
use your data, you will see improvement as opposed to
teaching to a test . . . It’s an issue of if you’re doing good
root-cause analysis and you’re doing best practices that
work, you will see the outcomes improve.” n
Follow these five tips for success on HCAHPS surveys
Struggling with your patient satisfaction scores? Worried
about the media onslaught once the ratings are released?
Deirdre Mylod, PhD, vice president of public poli-
cy for Press Ganey Associates, Inc., has the following five
suggestions:
1. Dealing with media coverage. Quality depart-
ments should relay to the marketing department where
the problem areas are and what they are doing about
them.
Mylod suggests telling reporters: “We are looking at
this. We are taking it seriously. We value patient views.
That’s why we’re participating voluntarily, and here’s
what we’re doing to fix it.”
“I think the voluntary part may be a helpful thing to
keep in that message,” she explains. “If the media asks
why aren’t you doing well in this area, remind them that
‘We’re for transparency; that’s why we participated before
it was required.’ ”
2. Putting whiteboards at every patient’s bed-
side. This allows nurses to communicate with each other
and keeps patients in the loop as well. The problem, Mylod
says, is that hospitals sometimes fail to update the white-
boards. “But if they’re being used well and updated every
day, it tells everybody, ‘This is the page we’re on, and this
is where we’re going.’ ”
3. Encouraging patients to ask questions. Staff
members should be trained to ask patients whether they
have any questions before leaving the room. “And when
the patient asks a question, say, ‘Thanks, I’m really glad
you asked that question,’ ” Mylod says. That way, patients
don’t feel like they’re bothering clinicians. Staff members
need to keep in mind that they’re experts in what happens
in hospitals every day, but the patients are novices and
don’t know how the processes work.
4. Share the comments on the surveys with
staff members. “When patients write something on a
survey, it does two things for you.” Mylod says. “It tells
you what is re-
ally going on,
and gives you
that evidence.
It also gives you
the patients
own words to
bring back to
the staff.” That
helps drive
home the point that this is real. “These are real patient
lives we’re talking about, and this is really what they’re
feeling and experiencing.”
5. Acknowledge staff members praised in sur-
veys. Even poorly performing hospitals receive surveys
praising particular employees.
“Remind people that this about improvement, and re-
ward those who receive positive comments,” Mylod says.
“Some hospitals will post comments about employees who
received positive comments in the unit, or the manager of
the unit will write a note to the person named.”
“ If the media asks why
aren’t you doing well
in this area, remind
them that ‘We’re for
transparency; that’s why
we participated before it
was required.’ ”
—Deirdre Mylod, PhD

© 2008 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Quality Improvement ReportPage 4 February 2008
that set point, the quality department can take action
to correct the problem.
“So if we see more falls happening, we make an ad-
justment in our fall prevention program,” Rohde says.
“As soon as our fall prevention program is doing what
we want, we keep it at that point because it’s reached
our set point, or our expectation. And that’s the key
starting point with a control loop—you have to know
what your expectations are.”
Unintended consequences
Another way control loops fail is when actions cause
unexpected consequences. Rohde uses the example of
electric blankets. If the blankets are working proper-
ly, people sample the temperature, and if it’s too cold,
they initiate an action by changing the knob to make the
blanket give off more heat. “That’s a closed control loop,
and it works well,” he says.
But if the blankets have dual controllers, one for each
side of the bed, things can go awry. Often, the monitors
for the right side of the bed get mixed up with the ones
on the left side of the bed. The person on the left side of
bed then turns up the heater, but it has no effect. The
person on the right side of the bed, in turn, becomes hot
and turns down the temperature on his or her side of the
bed, to no avail. “Both think that they have some con-
trol because they have two different knobs,” Rohde says.
“But they both have broken control loops, which are
giving them outcomes that have nothing to do with the
data, or the controls that they have.”
The same thing happens in hospitals, he says. For ex-
ample, a vice president of finance might determine that
the hospital needs to save money by cutting back on
staffing. But fewer nurses may jeopardize patient safe-
ty and malpractice lawsuits could start to rise. Then the
vice president of patient safety starts asking, “How come
we’re losing all this money because of lawsuits?”
In other words, an action taken in one area of the
hospital—in this example, finance—had an unintended
Editor’s note: This is the first article in a regular series about
how to collect and analyze data.
Don’t waste your time collecting data unless it’s part
of a closed control loop that leads to changes in your
hospital.
“The reason we measure data is because data is part
of a closed loop, and the reason we have a closed loop is
that we want to change something,” says Ken Rohde,
author of the new book Making Your Data Work: Tools
and Templates for Effective Analysis, published by HCPro,
Inc., and a senior consultant for The Greeley Company,
a division of HCPro in Marblehead, MA. “We either
want to change behaviors, or we want to say, ‘It’s
exactly at the right point; let’s keep it here,’ ” he says.
A thermostat that is working properly, he says, is an
example of a closed control loop. If the temperature
falls below a set point, say the 70oF mark, the thermo-
stat initiates an action, which is to turn on the heaters.
The air then warms up and touches the thermostat,
which samples the temperature to determine whether
the room has reached that set point, or 70oF mark, and
turns off the heater if it has.
“That’s a closed control loop, and it’s got some key
parts—it’s got the data; it’s got the set point, or the ex-
pectation; it’s got the action; and it’s got the closed feed-
back loop,” says Rohde.
In this example, a data loop breakdown may mean
that either the thermostat or heater is broken, so even if
you keep raising the temperature, the room stays cold.
A broken data loop might also result if someone has
changed the expectation, set point, or temperature, to,
for example, 90oF. The heater then works to reach an ex-
pectation that might not be the right one.
Similarly, the board of directors and senior leader-
ship might have different expectations, or set points for
medication error rates. Senior leaders need to determine
what the expectation is and clearly define it to quality
directors, so if the data show performance falling below
Data collection needs to bring about change

© 2008 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Quality Improvement Report Page 5February 2008
consequence in another area of the facility, and both vice
presidents feel out of control.
Oscillation problems
A third way control loops fail is by oscillation. For ex-
ample, you may get in your car on a wintry morning and
turn up the heat to full blast. Pretty soon, you’re boiling
hot, so you turn the temperature way down. Not
too much longer after, you get cold again, so you turn
the heat back up. Instead of initially setting the heater at
a good set point such as 70oF, the temperature, or perfor-
mance, keeps vacillating.
In a hospital, oscillation might involve a quality im-
provement team starting a performance improvement
project, abandoning it two months later, and then starting
it up again. “Program-of-the-month problems often are the
result of oscillations in our control loops,” Rohde writes in
his book. “We keep trying different things, never sticking
with one long enough to really see whether it works.”
Sampling mistakes
Another way hospitals err is by monitoring data at the
wrong sampling frequency. Organizations must separate
monitoring or reporting data from data used to control
processes, he says. For example, if you’re driving a long
distance in a car, your sampling might be every 15 or 20
minutes; you would frequently look at the gas gauge to
determine whether you have enough fuel.
But if you sampled this only on a quarterly basis, you
would almost certainly run out of gas.
Quarterly monitoring may be sufficient for presenting
data to regulators, who can use the information to deter-
mine whether the hospital should be shut down.
“But it’s nowhere near appropriate to help us run a
hospital, so we have to make sure people don’t fall into
the trap of sampling at a frequency that is designed for
monitoring and thinking that we can use that to control
our process,” Rohde says.
To effectively control processes, data may need to be
collected on a daily or even hourly basis—if you want to
see how many beds are available, for example. “But hos-
pitals don’t always do a good job of designing the sam-
pling frequency for the data to meet the control needs
they’re trying to use that data for,” Rohde says. n
Editor’s note: Go to www.hcmarketplace.com/prod.
cfm?id=5970&CFID=4257555&CFTOKEN=26313843
for more information about Rohde’s book.
Real-time data can drive up SCIP performanceEven small hospitals with limited resources can per-
form well on Surgical Care Improvement Project (SCIP)
measures by doing real-time data collection and getting
back to clinicians immediately if there’s a miss.
“You’re kind of killing two birds with one stone,” says
Jan Fitzgerald, MS, RN, director of quality and medi-
cal management for the division of healthcare quality at
Baystate Medical Center in Springfield, MA. “You’re get-
ting your data, and you’re improving your care.”
The spotlight on hospital performance has never
been brighter. In December 2007, CMS began publicly
reporting on its Web site Hospital Compare (www.
hospitalcompare.hhs.gov) about how well healthcare
facilities did on measures to prevent venous thrombo-
embolism (VTE). That followed the previous public post-
ing of hospital scores on three SCIP infection measures
about antibiotic timing, selection, and discontinuation.
As of January 1, The Joint Commission (formerly
JCAHO) began requiring hospitals that select SCIP as
one of their core measures to report about cardiac sur-
gery patients with controlled 6 a.m. postoperative serum
glucose, surgery patients on beta-blocker therapy prior
to admission who receive a beta-blocker during the
perioperative period, and surgery patients with appropri-
ate hair removal. (See the sidebar on p. 6 for Joint
> continued on p. 6

© 2008 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Quality Improvement ReportPage � February 2008
Commission and CMS requirements). “The thing that
seems to drive improvement the most is public report-
ing,” says Fitzgerald, who is also a member of the SCIP
speakers bureau. “People can see what’s going on
around the processes of care.”
Best practices at Baystate
That transparency may trouble some low-performing
hospitals, but not Baystate Medical Center, a 670-bed fa-
cility. It scored in the 98th percentile for giving patients an
antibiotic within one hour of incision; in the 92nd percen-
tile for antibiotic selection; in the 89th percentile for anti-
biotic discontinuation within 24 hours of surgery; in the
95th percentile for VTE prevention; and in the 89th per-
centile for discontinuation of antibiotics, according to Hos-
pital Compare. “We did very well,” Fitzgerald says. “We
are leading for the state of Massachusetts, as well as na-
tionally. We are very high performers for timing, duration,
and VTE prophylaxis, which is something we’ve been
working on for a long, long time.”
Indeed, Baystate began its drive to boost quality six
years ago when it became the first hospital in Massachu-
setts to take part in a national collaborative to reduce
surgical complications. Even so, the hospital sometimes
still struggles with getting physicians to prescribe the
right antibiotic. A small pocket of surgeons at Baystate,
Fitzgerald says, were prescribing the wrong antibiotic for
colon surgery, despite the hospital’s admonitions. “This
particular group of physicians had been using the wrong
drug for the last 12 months,” she says. “They finally, in
November, started using the right drugs. But we’ve been
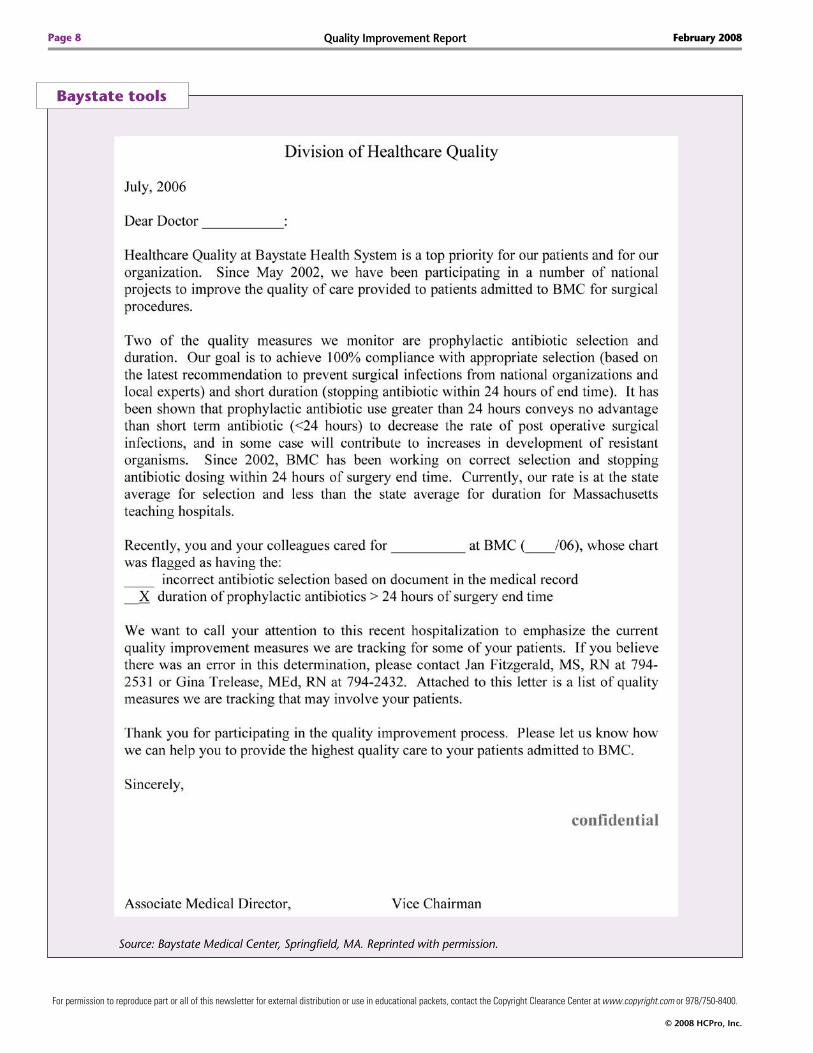
pounding on them for 12 months.” (See “Baystate tools”
on p. 8.) Two full-time equivalents are dedicated to col-
lecting SCIP data at Baystate, says Fitzgerald.
Hospitals struggling with VTE measures
Della Lin, MD, chief executive director of continu-
ing medical education at Queen’s Medical Center in Ho-
nolulu and the author of Surgical Care Improvement Project:
Improve Performance, Reduce Complications and Comply with
CMS, which is published by HCPro, says she’s seeing cli-
nicians struggling with the VTE measures. Facilities suc-
cessfully scoring higher than 90% for the infection
measures, she says, often see those scores at only the
60% or 70% range on VTE compliance.
SCIP < continued from p. 5
CMS requires reporting on five SCIP measures
Hospitals must submit the following data to CMS for
public reporting or forfeit 2% of their full market basket
Medicare update. The Joint Commission (formerly JCAHO)
also requires data from those hospitals that select Surgical
Care Improvement Project (SCIP) as one of their four core
measures.
The five SCIP measures are as follows:
SCIP-Inf 1: Prophylactic antibiotic initiated within one
hour prior to surgical incision
SCIP-Inf 2: Giving the patient the right antibiotic
SCIP-Inf 3: Prophylactic antibiotic discontinued within
24 hours after surgery end time
SCIP-VTE 1: Ordering the proper prophylaxis
SCIP-VTE 2: Making sure that the proper prophylaxis
was given to the patient
Reporting of the following measures is not yet linked to
Medicare payment, but The Joint Commission does require
hospitals to submit data about them:
SCIP-Inf 4: Controlling perioperative serum glucose
among major cardiac surgery patients
SCIP-Inf �: Appropriate hair removal for surgery patients
SCIP-Card 2: Major surgery patients receive a beta-
blocker perioperatively if they were on a beta-blocker
before admission
Hospitals may voluntarily submit data to The Joint Com-
mission about SCIP-Inf 7: Perioperative normothermia
among colorectal surgery patients. But it is not mandatory
because the measure has not received National Quality
Forum endorsement.
➤
➤
➤
➤
➤
➤
➤
➤

© 2008 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Quality Improvement Report Page 7February 2008
Another factor, Lin says, is that, although VTE is
the number one preventable hospital death, most phy-
sicians may not experience a VTE death in their prac-
tice. Instead, what they are more apt to experience is a
patient who has a postsurgical bleed from the use of an-
ticoagulants on his or her medication list. A physician
who has seen just one or two patients bleed may be re-
luctant to prescribe a VTE prophylaxis again, even if the
patient is at high risk. “As much as we say we like evi-
dence-based medicine, we go back to ‘I saw that patient
bleed; I’m not going to do that again,’ ” Lin says.
Compliance rates at Queen’s Medical Center for SCIP
are 92% for antibiotic timing; 96% for antibiotic se-
lection; 85% for antibiotic discontinuation; 63% for
physician ordering of prophylaxis to prevent VTE and
antibiotic timing; and 52% for the number of patients
who actually received the prophylaxis, according to its
publicly reported numbers on Hospital Compare. But in
the last three quarters of 2007, its VTE ordering prophy-
laxis rate has jumped to higher than 88% and patients
receiving prophylaxis has jumped to 85%.
Anesthesiologists key to antibiotic timing
Both Lin and Fitzgerald say anesthesiologists taking
ownership for antibiotic timing is critical to succeed at
the SCIP antibiotic timing measure.
“We were lucky early on, because one of our clinical
champions was an anesthesiologist,” Fitzgerald says. “We
gave him the data, and the next day he came back and
said, ‘Oh my God. Why aren’t we doing this?’ He was
pretty aggressive, and he really led the charge, and the
physicians all got it.” Baystate also made it clear that it
was a physician’s responsibility to prescribe the antibiotic
and an anesthesiologist’s job to administer it.
Lin recalls years ago hearing complaints from her
fellow anesthesiologists. “There were times where
we would sit around and talk about antibiotic timing,
and people said, ‘Well, why can’t the surgeon do it?
Why can’t the nurse do it? Why are you making me
do this? I have so many other things to do.’ ” Those con-
versations, she says, don’t happen anymore among
anesthesiologists at the 526-bed hospital, who are now
solidly behind the antibiotic measure.
A key factor in winning buy-in from the anesthesiolo-
gists, Lin says, is making them part of the process, and not
letting them feel as though they were just clinicians as-
signed to a task. Anesthesiologists at Queens now get re-
ports from the seven-person SCIP team about how they’re
doing and to see whether they’ve had any falloffs.
Immediate response to slips
At Baystate, performance on the day’s cases is collect-
ed by that afternoon. If there is a miss, a clinical cham-
pion immediately gets back to the physician to find out
what went wrong. Continuous display of data and feed-
back, Fitzgerald says, has helped sustain energy for
SCIP. “We just had our SCIP meeting yesterday, and
we probably have 30–35 people talking about it,” she
says. “Staff nurses are talking about it, surgeons are talk-
ing about it, anesthesiologists are talking about it. We’ve
done a really good job in infiltrating the front lines.” n
Editor’s note: Lin and Fitzgerald will be speaking during
the HCPro audioconference about SCIP on March 21. For more
information, go to http://www.hcmarketplace.com/help/
about.cfm. For more information about Lin’s SCIP book, go to
http://www.hcmarketplace.com/prod.cfm?id=5232&CFI
D=4257555&CFTOKEN=26313843.
We want to hear from you
How many resources do you have devoted to the Sur-
gical Care Improvement Project (SCIP)? Share information
with your colleagues about SCIP by e-mailing lbuckley@
hcpro.com the answers to the following questions:
1. What is your bedsize?
2. What is your surgical volume per month?
3. How many full-time equivalents (FTE) do you utilize to
collect information for SCIP?
4. How many FTEs do you utilize for quality/performance
improvement implementation of SCIP?
5. Who leads your SCIP initiative?
�. Who is your identified physician champion?
© 2008 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Quality Improvement ReportPage 8 February 2008
Baystate tools
Source: Baystate Medical Center, Springfield, MA. Reprinted with permission.

© 2008 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Quality Improvement Report Page �February 2008
Baystate tools (cont.)
Source: Baystate Medical Center, Springfield, MA. Reprinted with permission.

© 2008 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Quality Improvement ReportPage 10 February 2008
Focus on infections to ensure CMS reimbursementHospitals that plan to screen every single patient for
urinary catheter–associated infections to avoid paying for
preventable conditions may want to keep this in mind:
The government will be watching.
“Increased use of the present-on-admission [POA]
variable is certainly going to occur as it is implemented
in states across the country, but what we don’t want to
see happen is the unintended consequence that there’s
increase and potentially unnecessary use of diagnos-
tic testing on admission,” said Chesley Richards, MD,
MPH, FACP, deputy director of the Division of Health-
care Quality Promotion National Center for Prepared-
ness, Detection, and Control of Infectious Diseases for
the Centers for Disease Control and Prevention (CDC).
“The example we’ve already been hearing about is
people doing unnecessary testing for . . . patients who
have catheters but who are not symptomatic with uri-
nary tract infection [UTI] on admission,” said Richards,
who spoke during the December 2007 HCPro audiocon-
ference. “Before diagnosing a UTI, clinical symptoms
should be present.”
Richards said the CDC also discourages the use of an-
tibiotics as a preventive measure when there is no evi-
dence of infection. “These are the kind of behaviors we
want to discourage over time.”
CMS will monitor these issues as well, according to
Thomas Valuck, MD, MHSA, JD, medical officer and
senior advisor to Herb Kuhn, acting deputy administra-
tor of CMS.
“It is an issue that will inform the selection of condi-
tions [in the future], and if we find that the incentive
is actually encouraging bad practice of medicine, then
we’re going to have to figure out how to change the in-
centives to make sure that isn’t the case,” said Valuck.
“Practice of medicine . . . that would overtreat and/or
provide preventive services that aren’t necessarily re-
quired, that would lead toward resistance . . . we would
certainly not want to see that inappropriate practice of
medicine happening because of the payment incentive.”
Valuck and Richards urged hospitals to focus on elim-
inating hospital-acquired conditions (HAC) instead of
overusing the POA indicator and diagnostic testing.
The new payment system will no longer pay for eight
conditions unless they are documented as POA. Staff
members should not only work on eliminating HACs,
says Valuck; they will need to learn how and when
to document and code POA conditions. If hospitals un-
der the Medicare Hospital Inpatient Prospective Payment
System fail to reduce HACs and correctly document POA
conditions by October 1, they will pay the consequence.
The eight conditions CMS will no longer pay for are:
Serious preventable events—object left in surgery
Serious preventable events—air embolism
Serious preventable events—blood incompatibility
Catheter-associated UTIs
Pressure ulcers
Vascular catheter–associated infections
Surgical site infections—mediastinitis after coronary
artery bypass graft
Patient falls
Preventing HACs requires the implementation of evi-
dence-based guidelines provided by the CDC, according
to Richards. He said the CDC’s guidelines, which include
catheter-associated infection guidelines (currently under
revision), will aid hospitals seeking to implement systems
that will decrease cost and increase patient safety.
Even as early as April 1, POA claims documented
incorrectly will be returned, unpaid, and must be re-
submitted. By October 1, all claims with HAC not docu-
mented as POA will not be reimbursed by CMS.
Proper documentation and coding will be essential to
receive correct payments. The indicator must be assigned
for each principal and secondary diagnosis.
A coder looking for the POA indicator can look at
emergency department notes, history and physicals, ad-
mitting notes, progress notes, discharge summary, and
any other documentation used in other Medicare claims.
➤
➤
➤
➤
➤
➤
➤
➤

© 2008 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Quality Improvement Report Page 11February 2008
refuse to pay, or allow the patient to pay, in its renewal
contracts.
CMS is also looking ahead to proposed conditions for
2009. Currently, ventilator-associated pneumonia, staph
infection (staphylococcus aureus septicemia), deep vein
thrombosis, and
pulmonary embo-
lism are on the list
for proposed condi-
tions CMS will not
pay for.
“There are cer-
tainly evidence-
based approaches
to preventing hos-
pital-acquired
conditions,” said
Richards. “We know that for some of these conditions
there is more research that’s needed, but we do know
that if we just got hospitals to implement what we already
have in terms of recommendations, I think we would see
a dramatic decrease in hospital-acquired conditions.” n
❑ Start my subscription to QIR immediately.
Options: No.ofissues Cost Shipping Total
❑ Electronic 12 issues $299 (QIRE) N/A
❑ Print & Electronic 12 issues of each $299 (QIRPE) $24.00
Salestax (see tax information below)*
Grandtotal
QIRSubscriberServicesCoupon Yoursourcecode:N0001
Name
Title
Organization
Address
City State ZIP
Phone Fax
E-mailaddress(Required for electronic subscriptions)
❑ Payment enclosed. ❑ Please bill me.
❑ Please bill my organization using PO # ❑ Charge my: ❑ AmEx ❑ MasterCard ❑ VISA ❑ Discover
Signature(Required for authorization)
Card # Expires(Your credit card bill will reflect a charge to HCPro, the publisher of QIR.)
Orderonlineatwww.hcmarketplace.com.
BesuretoentersourcecodeN0001atcheckout!
*TaxInformationPlease include applicable sales tax. Electronic subscriptions are exempt. States that tax products and shipping and handling: CA, CO, CT, FL, GA, IL, IN, KY, LA, MA, MD, ME, MI, MN, MO, NC, NJ, NM, NY, OH, OK, PA, RI, SC, TN, TX, VA, VT, WA, WI, WV. State that taxes products only: AZ. Please include $27.00 for shipping to AK, HI, or PR.
Mail to: HCPro, P.O. Box 1168, Marblehead, MA 01945 Tel: 800/650-6787 Fax: 800/639-8511 E-mail: [email protected] Web: www.hcmarketplace.com
Fordiscountbulkrates,calltoll-freeat888/209-6554.
“The condition itself and whether it was present on
admission requires physician documentation for substan-
tiation,” said Valuck.
Each admission is also considered separate, even if it’s a
transfer, although Valuck predicts this will be addressed in
2009’s ruling. Currently, if a patient develops a HAC not
POA and is transferred, that condition would need to be
documented as POA in the second facility.
“Getting this documentation right is going to require a
lot of communication, especially in the early phases, among
the various involved parties, both within and outside of the
hospital,” said Valuck. “That communication should build
awareness, primarily with the medical staff, and also with
the coding professionals, and should provide guidance and
tools with standard approaches for getting the coding right
and monitor how it’s going,” said Valuck.
The aim is to prevent the wait for claims to come
back, he said, and many staff members should be in-
volved, from executives to compliance officers.
“Remember that this data is useful for more than just
the hospital-acquired conditions payment policy; it can
also be used for internal quality improvement purposes,”
said Valuck.
Private insurers are also beginning to consider a ban
on paying for serious preventable conditions such as
wrong-site surgery, according to The Wall Street Journal.
One insurer, Aetna, has begun to include The Nation-
al Quality Forum’s 28 “never events” as events it will
“ Getting this
documentation right
is going to require a
lot of communication,
especially in the early
phases, among the
various involved parties,
both within and outside
of the hospital.”
— Thomas Valuck,
MD, MHSA, JD
Senior Managing Editor Lisa Buckley
Telephone 781/�3�-1872, Ext. 3715
E-mail [email protected]
Questions? Comments? Ideas?

© 2008 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Quality Improvement ReportPage 12 February 2008
Proposed goals focus on infection control, med rec The Joint Commission (formerly JCAHO) in January
announced proposed 2009 National Patient Safety Goal
(NPSG) requirements and implementation expectations
(IE) for field review.
These proposed NPSGs affect hospitals and critical ac-
cess hospitals, ambulatory care and office-based surgery,
behavioral healthcare, disease-specific care, home care,
laboratories, and long-term care.
The Joint Commission seeks comments about these
potential new NPSGs and will be accepting feedback via
an online survey through February 27.
The field review focuses on the following areas:
Goal #1, patient identification
Goal #3, safe use of medications
Goal #7, hospital-acquired infections focusing on
methicillin-resistant staphylococcus aureus (MRSA)
and clostridium difficile–associated disease (CDAD);
catheter-associated bloodstream infections
(CABSI); and surgical site infections (SSI) in acute
care hospitals
Goal #8, medication reconciliation
Goal #13, patient involvement in their care
Universal Protocol for Preventing Wrong Site, Wrong
Procedure, Wrong Person SurgeryTM
In 2007, after the NPSGs were finalized, healthcare
organizations faced one new NPSG in preparation for
2008 requiring clinicians to respond rapidly to changes
in a patient’s condition, and another new requirement
about anticoagulant therapy.
Goal #1
Under the proposed revisions, Requirement 1A would
be expanded to include an IE requiring that the patient
be actively involved in the identification process, when
possible, before any venipuncture, arterial puncture, or
capillary blood collection procedure. Proposed Require-
ment 1C aims to eliminate transfusion errors related to
patient misidentification.
➤
➤
➤
➤
➤
➤
Goal #7
Perhaps most newsworthy is the inclusion of a new
proposed requirement aimed to stop drug-resistant or-
ganism infections in hospitals. Specifically, proposed Re-
quirement 7C targets MRSA and CDAD. Among its 16
IEs, 7C requires education for healthcare workers, pa-
tients, and their families, as well as the measurement
and monitoring of infection rates. It also requires lab-
based alert systems when MRSA patients are detected,
and a surveillance system for CDAD.
Requirement 7D proposes 13 IEs, including IEs for
before and after insertion of the catheter.
Goal #8
Proposed revisions to Goal #8 are composed of new
and revised requirements and IEs intended for clarifica-
tion, not alteration, of previous requirements. Revisions
have been made to Requirements 8A, 8B, and 8C for the
reconciliation of patient medication across the continu-
um of care.
Goal #13
Two IEs have been proposed to Goal #13, which tar-
gets increasing patient involvement in their own care.
The first new IE would require facilities to provide pa-
tients with information regarding infection control (e.g.,
hand hygiene or respiratory hygiene practices), and the
latter requires facilities to provide surgical patients with
information about preventing adverse events during sur-
gery (e.g., patient identification or surgical site-marking
processes).
Universal Protocol
Proposed changes to the Universal Protocol, like those
made to Goal #8, are not meant to change the overall
concept of the goal but rather to clarify existing require-
ments. According to the draft 2009 NPSGs, the Universal
Protocol contains the same concepts as it has in previous
iterations. n