FEBRILE SEIZURES AS SEEN IN THE
139
1 FEBRILE SEIZURES AS SEEN IN THE CHILDREN’S EMERGENCY ROOM OF THE UNIVERSITY COLLEGE HOSPITAL, IBADAN, NIGERIA BY OLUMIDE OLATOKUNBO JARRETT MBBS (IBADAN) 1994 A DISSERTATION SUBMITTED TO THE NATIONAL POSTGRADUATE MEDICAL COLLEGE OF NIGERIA IN PART FULFILMENT OF THE REQUIREMENTS FOR THE FELLOWSHIP OF THE FACULTY OF PAEDIATRICS NOVEMBER, 2006
Transcript of FEBRILE SEIZURES AS SEEN IN THE

1
FEBRILE SEIZURES AS SEEN IN THE
CHILDREN’S EMERGENCY ROOM OF THE
UNIVERSITY COLLEGE HOSPITAL, IBADAN, NIGERIA
BY
OLUMIDE OLATOKUNBO JARRETT
MBBS (IBADAN) 1994
A DISSERTATION SUBMITTED TO THE NATIONAL
POSTGRADUATE MEDICAL COLLEGE OF NIGERIA IN PART
FULFILMENT OF THE REQUIREMENTS FOR THE FELLOWSHIP OF
THE FACULTY OF PAEDIATRICS
NOVEMBER, 2006

2
DECLARATION
I hereby declare that this work is original unless otherwise
acknowledged and that it has not been presented to any other
college for a fellowship or submitted elsewhere for publication.
Dr Olumide Olatokunbo Jarrett, MBBS (1994)

3
CERTIFICATION
The study reported in this dissertation was carried out by Dr. Olumide
Olatokunbo Jarrett under our supervision .We also supervised the writing of
the dissertation.
____________________________
DR O. J. FATUNDE MBBS, FMCPaed Consultant Paediatrician
University College Hospital
Ibadan. ________________________ PROF K. OSINUSI Professor of Paediatrics University College Hospital Ibadan.

4
DEDICATION
I dedicate this work to my Heavenly Father who makes all things
beautiful in His time.
Eccle 3:11

5
ACKNOWLEDGEMENTS
I give all glory to the Almighty God, the Lord Jesus Christ and the Holy Spirit
for granting me help on all sides throughout the period of my residency
programme and especially in the course of this study.
My sincere appreciation goes to my supervisors, Dr OJ Fatunde and Prof K
Osinusi for guiding this project from its inception and for impacting valuable
knowledge to me.
I also specially thank Drs Lagunju and Owoaje for the invaluable support
and encouragement that I received from them in the execution of this
project. I appreciate all the resident doctors in the Department of Paediatrics
for their support and love.
I am grateful to Mr Adewole and Mr James who were very helpful in the
analysis of my results. Special thanks go to Mr Fashina and Adeola Oloko for
their immerse assistance in making sure I had laboratory analysis done
accurately.
I appreciate the unflinching support of my beloved husband Mr Elvonuel BS
Jarrett who encouraged me to stay in the programme even when things were
tough. My lovely children; Bankoleoluwa, Emmanuel, and the twins, Esther
and Ruth, were very patient, enduring several moments when mummy just
could not be at home for them.
Many thanks to all my parents both Spiritual and Physical, who were always
in support of my progress.
May the Good Lord reward you all Amen.

6
TABLE OF CONTENTS
Page no.
Declaration---------------------------------------------------------- ii
Certification--------------------------------------------------------- iii Dedication----------------------------------------------------------- iv
Acknowledgements------------------------------------------------- v
Table of contents--------------------------------------------------- vi
Glossary of Abbreviations----------------------------------------- vii List of Tables-------------------------------------------------------- viii
Summary------------------------------------------------------------ x
Introduction -------------------------------------------------------- 1
Literature Review -------------------------------------------------- 4 Aims and Objectives ----------------------------------------------- 57
Subjects and Methods -------------------------------------------- 58
Results -------------------------------------------------------------- 70
Discussion --------------------------------------------------------- 98
Conclusions ------------------------------------------------------- 109 Recommendations ----------------------------------------------- 110
Limitations of study ---------------------------------------------- 111
References --------------------------------------------------------- 112
Appendix 1 ------------------------------------------------------- 130
Appendix 2--------------------------------------------------- 131

7
GLOSSARY OF ABBREVIATIONS
AVP Arginine vasopressin
AAP American Academy of Pediatrics
BPA British Paediatric Association
CSF Cerebrospinal fluid
CHES Child Health Education Study
EEG Electroencephalogram
FBC Full Blood Count
GABA Gamma aminobutyric acid
IQ Intelligence Quotient
Kg Kilogram
MRI Magnetic resonance imaging
NMDA N- methyl D-aspartate
NCPP National Collaborative Perinatal Project
OFC Occipito Frontal Circumference
OTCHEW Otunba Tunwase Children’s Emergency Ward
PGE2 Prostagladin E2
PHC Primary Health Care
RBM Roll Back Malaria
SPSS Statistical Package for Social Sciences
TNF Tumor necrosis factor
UCH University College Hospital
UTI Urinary tract infection
URTI Upper respiratory tract infection
UNICEF United Nations Children’s Fund
WHO World Health Organization

8
LIST OF TABLES
Table
Title Page no No
Table 1
Table 2
Table 3
Table 4
Table 5
Table 6
Table 7
Table 8
Table 9
Table 10
Table 11
Table 12
Table 13
Age and Sex distribution of 147 children in the study.
Classification of children into seizure categories.
Type of seizures in relation to the age of children with febrile seizures.
The socioeconomic class of parents in relation to the type of febrile seizures in the children of the study.
The socioeconomic class of parents in relation to past history of seizures in the children of the study.
Pre-hospital management given to 59 children with febrile seizures.
Pre-hospital intervention in relation to the socioeconomic class of the parents.
Pre-hospital intervention by mothers in relation to
recurrence of febrile seizures in children of the study.
The type of pre-hospital intervention given by mothers in relation to the type of seizures in the children with febrile
seizures.
Relationship between the etiology of fever and age of the children in the study.
Relationship between aetiology of fever and the pattern of
febrile seizures.
The degree of parasitaemia in relation to the type of seizure in the children in the study.
Packed cell volume values in 147 children with febrile seizures.
71
72
73
74
76
79
80
81
81
83
86
87
89
9
Table 14
Table 15
Table 16
Table 17
Packed cell volume in relation to the etiology of fever.
The white blood cell counts in relation to the etiology of
fever in 147 children with febrile seizures. Cerebrospinal fluid sugar in relation to the aetiology of
fever in the children studied.
Cerebrospinal fluid -protein in relation to the aetiology of fever in the children studied.
89
91
94
95
10
SUMMARY
A prospective study was carried out at the University College
Hospital (UCH), Ibadan, between November 2002 and December 2003
to determine the prevalence, aetiology and short-term prognosis of
febrile seizures in childhood.
One hundred and forty-seven children with febrile seizures
admitted into the Children Emergency Room of the UCH Ibadan were
studied. Their ages ranged from four months to sixty months (five
years) with a mean age (SD) of 26.35 (13.76) months.
A detailed history was taken and a thorough physical
examination was carried out on each patient, while investigations
performed were recorded in a proforma. The duration of hospital stay
and the presence of neurological deficits were also recorded.
The proportion of children who presented with febrile seizures
amongst the paediatric admission into the hospital during the study
period was 9.9 %. There was a slight male preponderance among those
with febrile seizures, with a male to female ratio of 1.3:1.Complex
febrile seizures occurred more frequently with a simple to complex
ratio of 1:2.1.
The leading causes of febrile seizures were malaria (40.1%),
septicaemia (15%), urinary tract infection (12.3%) and pneumonia
(8.2%). Other less common causes were otitis media, measles and
gastroenteritis.

11
Pre-hospital intervention was given to 59 patients (40.1%). Of
these, native concoction was given to 15(25.4%) children. There was
statistically significant relationship between pre-hospital management
and socioeconomic class of parents (P value = 0.008). The mean (SD)
duration of hospital stay of the children studied was 6.37 + 8.067
days. Children with bacterial infections spent a longer period in the
hospital as compared with children with malaria.
Two (1.3%) of the 147 children died. Neurological deficits, mainly
cranial nerve palsies and hypertonia, were found in six survivors.
It is concluded that febrile seizures remain a major cause of
morbidity in children presenting to the Children’s Emergency Room of
UCH, Ibadan and that the major aetiological factor is malaria.
Therefore, measures to control malaria amongst our children should
be improved to reduce its prevalence. Effective health education of the
general public should be undertaken emphasizing the relative benign
nature of this condition, thus allaying the fear and apprehension and
panic associated with the disease, the dangers of offering harmful
methods of intervention should also be highlighted.

12
INTRODUCTION
A febrile seizure is a seizure occurring in infancy or childhood
usually between three months and five years of age associated with
fever but without evidence of intracranial infection or a defined cause.1
Seizures with fever in children who have had afebrile seizures are
excluded.1
Febrile seizures are a common problem encountered in
emergency paediatric practice occurring in about 2-4% of children
under 5years of age.2,3 It has been found to contribute significantly to
childhood morbidity in our environment,2 complicating common
childhood febrile illnesses such as malaria, which was responsible for
45% of the febrile illnesses associated with febrile seizures in the
study by Familusi et al.2 Conditions likely to precipitate febrile
seizures vary depending on the most prevalent fever-inducing illness
or disease in a given location.4
A febrile seizure causes intense parental anxiety.5 This coupled
with some degree of ignorance, is usually responsible for the various
forms of intervention offered by parents and caretakers when a child
has an episode. These interventions include the use of cow urine
concoction,2, 3 burning of parts of the body, application of substances
to the eyes and mouth and so on.2 Such practices may account for

13
the high mortality of 6.4% obtained in the previous study at our
centre.2
There is a genetic predisposition to febrile seizures with an
autosomal dominant inheritance pattern having been demonstrated.6
The risk of recurrence and epilepsy are important issues in
febrile seizures. The temperature at time of seizure, the age of onset
and the record of family history of febrile seizures determines the
probability that there would be a recurrence.7,8 Recurrence refers to a
situation whereby a child who has had a previous febrile seizure goes
on to have a repeat episode during another febrile illness.1, 9 The type
of febrile seizure, family history of non-febrile seizures and abnormal
neurologic or developmental status prior to febrile seizures are some of
the factors that determine the risk of developing epilepsy.7,8
The issue of relevant investigations and their indications has
also been the subject of study.10 For example; lumbar puncture is
perhaps the most relevant investigation to be carried out in order to
rule out the presence of meningitis.10
While there have been previous reports on febrile seizures in
Nigerian children, 2,4,11-18 only one of such studies has been conducted
at our centre more than 30 years ago.2 It is important to review the
subject from time to time in order to document changes, if any, in the
presentation, causes and management of the condition.

14
The purpose of this study was therefore to determine the current
pattern and aetiology of febrile seizures in children seen at the
Children Emergency Ward of the University College Hospital, Ibadan,
as well as the practice of caregivers with regard to febrile seizures. The
results will help to focus on possible interventions needed to change
perceptions about this disorder in bid to reduce morbidity and
mortality.
LITERATURE REVIEW
Definition
15
A seizure is an abnormal involuntary paroxysmal neuronal
discharge from the brain, which could manifest as motor
abnormalities and/or sensory and autonomic disturbances with or
without loss of consciousness. 1, 19
The definition of febrile seizures has been the subject of
controversy in recent times. 1,20,21 The Joint Working Group of the
Research Unit of the Royal College of Physicians and the British
Paediatrics Association20 defined febrile seizures as “an epileptic
seizure occurring in a child aged six months to five years precipitated
by fever arising from infection outside the nervous system”.1, 20 They
considered that it was proper to use the term ‘epileptic’ in so far as the
neurophysiological substrate of a febrile convulsion is a paroxysmal
neurological discharge as it is in an epileptic seizure.
Wallace,21 however, felt that the definition should not be
restricted because she felt once restrictions such as intracranial
infection, presence of chronic neurological disorder or duration or
lateralization of convulsion are placed on the definition it becomes
extremely difficult to decide whether a convulsion should be
characterized as ‘febrile’ or not. She accordingly defined it as ‘any
seizure occurring in association with any febrile illness’.
Arguments have ensued because of these varying views in terms of
exclusive and inclusive criteria and therefore, this amongst other issues
necessitated a consensus meeting.19 The Panel18 defined febrile seizure

16
as “an event in infancy or childhood usually occurring between three
months and five years of age associated with fever but without evidence
of intracranial infection or defined cause.” Members concluded that
febrile seizures are to be distinguished from epilepsy, which is
characterized by recurrent non-febrile seizures. Febrile seizures cannot
be referred to as “epileptic” because this is the term used in describing
non-febrile recurrent seizures. The definition by the panel appears to
properly define the condition with emphasis on the absence of an
intracranial involvement.
Epidemiology
Febrile seizures are a common problem encountered in
emergency paediatrics practice.2, 6, 11, 21 It is the commonest cause of
seizures in children younger than five years.2 Its prevalence varies
from one geographical location to the other.2, 11,12, 22-24
In the United States of America, studies have shown that 2-4%
of children will experience a febrile seizure prior to the age of five
years1,3 Costeff25 reported an incidence of 3% amongst Israeli children,
while Webb26 found an incidence of 5.1% in India. Nakayama et al27 in
a population- based study, reported an incidence of 7% amongst
Japanese children. Incidence is as high as 9.7% in a country like
Ghana.11

17
In Nigeria, the few studies2, 11-18 that have been carried out
reveal a somewhat higher incidence of febrile seizures when compared
to other parts of the world.2 Familusi et al2 in 1971 reported a 15.1%
prevalence of febrile seizure in children admitted to an emergency
room in Ibadan. Izuora and Azubuike13 in 1977 reported an prevalence
of 15.6% among admissions to the University of Nigeria Teaching
Hospital Emergency Paediatric Unit in Enugu, while Angyo et al18
reported a prevalence of 8.08% in Jos.
In contrast to the very high prevalence reported from Ibadan and
Enugu, Scott-Emuakpor and Longe12 reported a lower prevalence of
5.8% at the children’s emergency unit of the University of Benin
Teaching Hospital. Out of the 1,207 children admitted to the
emergency unit during the study, 104 (8.6%) had a provisional
diagnosis of febrile seizures, but 34 were later excluded because of the
presence of metabolic derangement and features of meningitis.
All the Nigerian studies were hospital-based and can thus be a
gross misrepresentation of the actual population affected. Also, the
hospitals involved are all referral centres and so some bias could have
been introduced. Since the occurrence of a seizure will in many cases
prompt the parents to take the child to a health facility, it is to be
expected that these hospital-based figures will be higher than those
obtained in population –based studies. These factors can account for
the higher prevalence reported from Nigeria.

18
Febrile seizures are primarily a disease of infants and young
children, 2, 3, 11, 12, 20, 21-23 which occur more in the first year of life.2, 24
In the past, the age range for febrile seizures was set at 6
months to 6 years2, 29 but in recent times this age limit has been
reviewed.19 The National Institute of Health Consensus Development
Conference in its definition stated that febrile seizures are ‘… seizures
occurring in children between 3 months and 5 years associated with
fever…’.19 The majority of cases of febrile seizures occurred between
six months and 4 years of age in the study by Familusi et al2 and
occurred rarely below the age of 6 months or above the age of 5 years.
However 29(4.9%) out of the 590 patients with febrile seizures studied
were less than 6 months of age, while 42(7.1%) were over 5 years of
age.
The peak age for febrile seizures is between the age of 6 months
and 12 months, 23 but12-14 months has been noted in some review.6
Febrile seizures have been shown to have a slight male
preponderance.2, 4 They, Fagbule et al4 reported M: F ratio of 1.3:1,
Familusi et al2 a ratio of 1.36:1 and Angyo et al18 a ratio of 2:1.
Seasonal variation has also been observed.4 In the tropics, about
two thirds of episodes of febrile seizures occur during the rainy
season,4 which corresponds to the season of highest incidence of
malaria. Racial differences in prevalence rates have also been reported
being 3.5% in whites and 4.2% in blacks.9

19
The socioeconomic status of the parents of children with febrile
seizures could affect the prevalence and outcome of febrile seizures.5
Parmer et al5 reported in their study that prior awareness of febrile
seizures was significantly higher in the upper and middle social class,
so also was awareness of correct measures to take in prevention and
treatment of febrile seizures.
Pathogenesis of Fever
Fever is an elevation of body temperature mediated by an
increase of the hypothalamic heat regulatory set point.29 The
hypothalamic thermoregulatory centre controls body temperature by
balancing signals from peripheral cold and warm receptors. Another
regulatory factor is the temperature of blood circulating in the
hypothalamus. The integration of these signals maintains normal core
temperature at the set point of 370C ± 0.50C.30
In the pathogenesis of fever, there is usually a stimulus.29,, 30 Most
often these are bacteria and their endotoxins, viruses, yeasts,
spirochetes, protozoa, immune reactions, several hormones,
medications and synthetic polynucleotides. These substances are
commonly called exogenic pyrogens. Cells stimulated by exogenic
pyrogens form and produce cytokines called endogenic pyrogens. The
most important endogenic pyrogens are interleukin1, interleukin 6 and
cachetin also called Tumours Necrosis Factor (TNF). Endogenic
pyrogens are glycoproteins that also have other important effects.30

20
Interleukin 1 and TNF increase the immune response by activation of T
cells and stimulation of interleukin 2 production. Interleukin 1 enhance
B cell proliferation. Fever and specific effects of interleukin 1 and TNF
form highly integrated processes that are involved in the response to
infection and acute inflammation processes. Interleukin 1 and TNF are
produced not only by monocytes and macrophages but also by
endothelial cells and astrocytes.30 Other endogenic pyrogens include
interleukin beta and gamma.
In the presence of sepsis, there is usually increasing levels of
interleukin 1 and TNF which are transported by blood. In the
hypothalamus, they trigger the synthesis of prostaglandin of group E
(PGE2) from the arachidonic acid of cytoplasmic membrane of target
cells.29 The precise mechanism by which PGE2 resets the central
thermostat is not known. PGE2 alters the hypothalamus heat-
regulating set point resulting in heat generation and heat
conservation.29 Heat generation is brought about by increased cell
metabolism, muscle activity and involuntary shivering, while heat
conservation is by vasoconstriction and heat preference behaviour.
Glucocorticoids inhibit the production of interleukin 1 and TNF
while Aspirin and other non- steroidal- anti- inflammatory drugs
inhibit cyclooxyygenase responsible for PGE2 production.29In the
majority of diseases, fever is caused by pyrogens. There are situations
however when fever may be caused directly by changes in the centre of

21
thermoregulation without the participation of exogens and endogenic
pyrogens. This occurs in brain tumors, intracranial bleeding and
thrombosis. 30
Pathogenesis of Febrile Seizures
Febrile seizures result from an age- dependent hyper excitability
of the brain that is induced by fever.31 Although there are important
genetic influences that render a febrile child more likely to develop
seizures, it is the fever per se that causes the seizures.31
Various authors have reviewed the mechanism by which fever
leads to seizures in these children.32-36 These studies were mostly
carried out on animals. Some reported that the height and rapidity of
body temperature were pathogenetic while another author reported
that a lack of arginine vasopressin increased the threshold for febrile
seizures or prevented it altogether.32 GABA (gamma aminobutyric
acid) has also been impilicated.33,34 A study reported low levels of
GABA in the animals they studied33 while another study by Knight et
al34 did not report any significant difference in the levels of GABA in
children with febrile seizures and those without.
Loscher and Siemens35 reported that the concentration of PGE2
in the central nervous system was significantly elevated in children

22
before febrile seizures and there was a significant positive correlation
between temperature and PGE2 levels.
Another report suggested that N-methyl L-D aspartate (NMDA)
receptor- mediated mechanisms may be involved in the production of
febrile seizures in response to hyperthermia.36 This is because its
antagonist produced dose- dependent increases in latency to the onset
of seizures. NMDA receptors are the major group of glutamate
receptors in the central nervous system upon which excitatory amino
acid neurotransmitters (glutamate and asparate) act to generate the
neuronal impulse that may be manifested as a seizure. It was deduced
that fever may lead to the generation of the NMDA receptor agonist.36
Genetics
The fact that there is a genetic predisposition to febrile seizures
cannot be doubted.27,35,37-39 The most useful information comes from
studies of children preferably in a large area.1 The American National
Collaborative Perinatal Project found family history to be the major
identified contributor to vulnerability to febrile seizures1.
The mode of inheritance of febrile seizures has been the subject
of considerable debate. Some workers have postulated an autosomal
mode of inheritance.6 There have also been suggestions of a polygenic
mode of inheritance but no report of sex linked inheritance has been
postulated.12 Tsuboi and Okada40 in a population and family- based
study, in Fuchu City, Japan, assessed 6,706 children aged 3 years.

23
Four hundred and fifty children had febrile seizures while 620
randomly children selected served as controls. The incidence of febrile
seizures amongst siblings of the 450 children with febrile seizures was
21.9% compared to 6.2% amongst the controls. Surprisingly, the
incidence amongst sisters was more than amongst brothers. This is at
variance with previous studies which showed a male predilection in
febrile seizures.6 The incidence among siblings was higher if one
parent had had febrile seizures and lower if neither parent had had
seizures.40 The incidence was highest if there were two family members
with febrile seizures, lowest if no family member had had a seizure
and intermediate if one relative had a history of febrile seizure.40 The
differences among these 3 categories were significant. Tsuboi and
Okada40 concluded that a multifactoral inheritance was most likely
involved.
Scott Emuakpor et al12 in a hospital-based study carried out at
the University of Benin Teaching Hospital reported the risk of full
siblings having febrile seizures to be 50%, indicating an autosomal
dominant mode of inheritance, with complete penetrance. This study
cannot, however, conclusively claim this, since several generations of
the families would have to be analyzed and the behavior of the gene
studied to come to this conclusion. Secondly, since the study was
hospital-based, samples were highly selective and may not necessarily
portray accurately what occurs in the general population.

24
Eric et al38 reported another autosomal dominant febrile
convulsion locus on chromosome 19p. This study brought to light the
fact that febrile seizures occur with higher frequency in families where
there was already a documented history of febrile seizures with
children from such families showing a three-fold or greater risk than
the general population of children with febrile seizures.
Recently, Nakayama et al27 reported the existence of a gene on
chromosome 5q 14-q15 which confers susceptibility to febrile seizures.
This study was however hospital based. Pieffer et al39 reported a large
family with 21 members affected by febrile seizures inherited as
autosomal dominant trait. Linkage analysis, genome wide scan and
subsequent fine mapping revealed significant evidence for a febrile
seizure locus on chromosome 2q 23-24.39 The findings from these
studies38,39 suggest that there may be at least four possible loci for
febrile seizures.
Other predisposing factors
There is evidence that maternal habit/ill health can predispose a
child to febrile seizures.1 These include prenatal maternal cigarette
smoking, and maternal alcohol intake, maternal seizures and
maternal renal problems. In a case- control study, Cassario et al41
found that prenatal cigarette smoking doubled the risk of simple
febrile seizures while alcohol intake doubled the risk of complex febrile
seizures.

25
Maternal medication during pregnancy has also been
implicated.21 Examination of the types of drugs given in pregnancy
shows that those known to have an effect on the central nervous
system for example, barbiturates, antidepressants and antiemetics
were frequently implicated in a report by Wallace.42 It seems
possible that these agents have adverse effects on the developing
cerebrum. Diuretics were given significantly more often to mothers of
patients. Diuretics, in altering electrolyte balance and in the case of
thiazides, carbohydrate metabolism, they could adversely affect the
fetal environment during brain maturation. Prolonged use of these
drugs during pregnancy could be deleterious to the growing fetus.
Perinatal predisposing factors that have been implicated include
breech presentation, antepartum hemorrhage, delivery by caesarian
section and intrauterine growth retardation.21
There are two bodies of opinion on the relationship between
pregnancy and perinatal factors and the risk of febrile seizures.
Wallace43 compared the birth history of 132 patients with febrile
seizures with the birth history of 180 of their siblings without febrile
seizures, 80(61%) of the children with febrile seizures had perinatal
and neonatal problems while only 39(22%) of their normal siblings had
abnormal perinatal history. Wallace43 concluded that abnormal
pregnancy with brain damage might be important in the pathogenesis
of febrile seizures.
26
Lennox44 in a hospital-based study reviewed the records of 240
children with a history of febrile seizures. He reported that 74% had a
normal birth history, while 26% had an abnormal perinatal history.
This included breech delivery, placenta praevia with severe bleeding,
use of high or middle forceps, caesarian delivery, twin birth and
prematurity. The author, however, did not proceed to determine the
importance of individual factors to the subsequent development of
febrile seizures.
In contrast to the foregoing report, the CHES45 in a population
study did not find any appreciable contribution of pregnancy and birth
factors to the risk of febrile seizures. Zhao et al46 in china, in a case
control study also found that none except maternal acute respiratory
infection was associated with increased risk.
Aetiology of the fever associated with Febrile seizures
The leading aetiology for the fever depends on which infection is
commonest in the environment.14 Virtually any cause of fever other
than central nervous system diseases is a potential etiology in febrile
seizures.14
Documented causes include: 2,14 malaria, pneumonia, upper
respiratory infections, (tonsillitis, pharyngitis), otitis

27
mediasteomyelitis, cellulitis, urinary tract infection, septicaemia or
bacteraemia, gastrointestinal infections and viral infections e. g.
measles.
In both the Northern and Southern parts of Nigeria, the etiology
of fever causing febrile seizures is similar.2,4,12,18 In a study by
Familusi et al2 at the University College Hospital Ibadan, it was found
that the commonest cause of fever that triggered off seizures was
malaria. This is similar to what Fagbule et al4 reported from Ilorin
where 71.1% of the children with febrile seizures had Plasmodium
falciparum infection. Malaria was also the commonest cause of fever in
studies by Angyo et al18 in Jos, Iloeje15 in Enugu and Akpede47 in
Benin. Malaria being the commonest aetiological agent is not
surprising in this country considering the fact that Nigeria is stable for
the malaria infection which necessitated our being a member of the
Roll back malaria programme (RBM) as a nation.48 RBM is a
partnership working worldwide to halve the burden of malaria by
2010.48,49 Malaria is responsible for over one million deaths each year
all over the world, about 3,000 a day; the majority of victims being
children. The policy of malaria control should be maintained. If
malaria could be properly controlled the incidence of febrile seizures
will be reduced.
In contrast, Lewis et al50 in their study of children with
febrile seizures in a temperate country traced a viral etiology in 86% of

28
the children. The viral infections manifested as various infections like
pharyngitis, tonsillitis, gastrointestinal infection, otitis media and
measles.
Familusi et al2 isolated viruses from 14(13.3%) of the 105
children that had viral studies. Fagbule et al4 did not carry out viral
studies. This could have affected the results obtained.
McIntyre et al51 in their retrospective study on occult
pneumococcal bacteraemia and febrile seizures, reported that 10 out
of the 29 patients managed in their hospital at Liverpool with
bacteraemia, had been admitted and managed as cases of febrile
seizures. They inferred that bacteraemia could be an important cause
of febrile seizures and those complications of focal infections; e.g.
meningitis and pneumonia were issue for concern. In another study by
the same author, positive blood cultures were obtained in 12 (4.3%) of
the 282 patients they reviewed, six of whom actually had a clinical
picture suggestive of septecaemia while the other 6 did not.51 They
concluded that bacteraemia are detected more frequently in children
who are admitted to hospital with febrile seizures when cultures are
performed as a routine. Teah et al52 also in a retrospective study
reported a 2.9% incidence of septicaemia in the patients they
reviewed.
There is a significant difference between the pattern of
bacteraemia seen in children in the temperate and tropical countries.53, 54

29
This has been attributed to the difference in climatic conditions. While
the predominant organism isolated from cultures in the temperate
regions are streptococcus pneumonia and Haemophilus influenza, 55
Staphylococcus aureus is more predominant in the tropics.54
Prevalence of bacteraemia also defer in the tropics and
temperate countries, being as low as 3% in the latter and as high as 11%
- 12.4% in the former.53,54 The report by Lepage et al53 gave the
prevalence of 12.4% among Rwanda children while Teele et al56 reported
a prevalence of 3 – 4% among young febrile children who were sent home
at first visit with bacteraemia in a walk in clinic in boston. Akpede et al47
found an incidence of 11% in one of their reports.
There is no specific symptom and sign associated with malaria.
In the tropics acute fever without localizing signs is often equated with
malaria and the risk of bacteraemia in such children has remained
unknown.47 Although malaria is a predominant infection in healthy
under-fives with fever without localizing signs in the tropics, bacteraemia
with or without malaria occur with an important high frequency and
some have recommended that while presumptive treatment of malaria is
justified in such children, evaluation for bacteraemia should be given
consideration.47 In the study by Akpede54 12 of the 14 children with
bacteraemia had concurrent malaria infection.
The higher prevalence of bacteramia in the tropics could be due to
the influence of malaria. Hemolysis induced by malaria cause

30
hypotransferinaemia, which can enhance susceptibility to staphylococcus
aureus infection.47 Sequestration of erythrocytes containing maturing
schizonts of plasmodium falciparum in deep tissues; capillaries,
including that of the gut, causes microinfarct formation which can
enhance blood stream invasion by enterobacteriae. Acute malaria
infection is also known to cause immunosupression.
Although asymptomatic parasitaemia is a frequent problem in
febrile patients in endemic areas, those with double infection of malaria
and other bacterial infections experience greater morbidity and
mortality.54 Hendrickse57 reported in 500 severely ill children in the
emergence room showed that 25% of the 20 children with malaria and
bacterial infection died as compared to 3.7% of 164 children with malaria
alone. In contrast, Lepage et al53 found no significant difference in the
mortality rate between children with bacteria infection and the control
group with malaria alone. It would be, however, unwise to disregard the
presence of bacteria infection in children with malaria.
In the study by Musa-Aisien et al 58 UTI prevalence was 9%.
Prevalence was higher in girls than in boys. Angyo et al18 reported a
prevalence of only 3(1.8%) of the 163 patients studied, while Fagbule et
al4 did not report any case of UTI in their study. This is not surprising
since urine culture was not done routinely in the patients they studied
but was restricted to patients in whom UTI was suspected. Familusi et
al2 reported a diagnosis of UTI in 2.8% of their patients. They stated

31
that this was probably an under-representation since the number of
children who had urine culture was small. A study in South Africa by
Jeena et al 59 had a very high yield of 17%, gram negative organism being
responsible for 87.5% of the cases. Teah et al52 in Washington DC,
reported a 0.7% yield of bacteria pathogens in a retrospective study
where the incidence of UTI in children with febrile seizures was reviewed.
Trainer et al60 found an incidence of 5.9% amongst 171 patients in a
retrospective study in Chicago while Lee et al61 in Wales reported an
incidence of 8%.
In the report by Lewis et al50 it was implied that though majority of
the causes of febrile seizures they saw were elucidated by a systemic viral
illness, some had generalized bacterial infection. There were cases where
bacteria pathogens were isolated in the blood, along with a virus being
isolated from body fluids. In temperate regions the occurrence of a virus
isolated in a febrile child does not exclude a possibility of a super-
imposed bacterial infection hence the need for proper clinical assessment
and evaluation of a febrile child and cultures taken in these children in
spite of the obvious viral infection.
Immunization seems to precipitate febrile seizures only rarely.62
Only 1.4% of the children in the NCPP (National Collaboration
Perinatal Project) who had had seizures in the first seven years of life
had been immunized within two weeks of the episode and in about one
third of them, other potential causes of fever were present. DPT

32
(diphtheria, pertussis, tetanus) vaccine has been implicated
particularly the pertussis component. 63 In a study following
administration of DTP vaccines 9 out of 15,752 children developed
convulsions meanwhile none of the 784 children with DT (diphtheria,
tetanus) vaccine convulsed.
Types of Febrile Seizures
There are two types of febrile seizures
1. Simple: defined as a primarily generalized seizure lasting less
than 15 minutes and not recurring within 24 hours or during
that particular febrile illness;7 and
2. Complex: defined as a seizure which is focal, or prolonged
(>15minutes) and or recurring within 24 hours of the initial
seizure.7 Focal seizures may involve an arm, leg or face on one
side only or eye deviation towards one side.
Out of the 590 children studied by Familusi et al, 2 only
27(4.6%) had focal seizures, it was however not stated explicitly the
number of children with complex febrile seizures. In a study of Saudi
Arabian children64 8.4% had complex febrile seizures. However, In this
study, children were recruited after their first febrile seizure. This
would, therefore, not have included patients with multiple seizures in
a febrile episode. Excluding this latter group of patients would have
reduced the proportion of patients with complex febrile seizures.

33
Fagbule et al4 found that 58.5% of cases had one episode of
seizures in 24 hours, 20.8% had 2 episodes, while another 20.8% had
3 or more episodes in 24 hours. Thus 41.6% of the children had
complex febrile seizures based on occurrence of multiple seizures in a
24-hour period. Iloeje15 in Enugu stated that 67(38.9%) of the 172
children studied had seizures lasting longer than 30minutes while
Angyo et al18 in Jos did not mention the pattern of seizures in the
children they studied.
Investigations
Several authors10,23, 65- 72 have reviewed the indications, cost and
benefits of various laboratory tests in the child with febrile seizures.
This issue has generated the most controversial aspects in the
evaluation of febrile seizures.10
The investigations that have been considered as ‘work up’ after a
febrile seizure have included: 10
Full blood count;
Blood culture;
Lumbar puncture;
Skull X-ray;
Electroencephalogram;
Electrolytes;
Urinalysis and culture; and
Random blood sugar

34
In the tropics, blood film for malaria parasites has been included
in this list especially as malaria is the commonest cause of fever in
febrile seizures.2,4 .The above laboratory investigations are expensive,
being worth much as 286 dollars in one study.10 In University College
Hospital Ibadan, with the current pricing of laboratory tests, this
would cost well over five thousand naira (40 dollars). The value of
these procedures to the clinicians in assessing the child with febrile
seizures is reviewed below.10, 23, 65 - 72
Lumbar Puncture Meningitis is the most important differential
diagnosis in the child with a febrile seizure.10 Most febrile seizure
episodes are benign and self-limited and do not require treatment.28
Several studies, 23,28,65-72 however, have shown that meningitis can
occasionally occur with a clinical picture indistinguishable from febrile
seizures.28
Thirteen percent of children with meningitis have convulsions
with fever and these seizures are almost always brief and
generalised.23,65 In 30% to 35% of these children (primarily those
children younger than 18 months) meningeal signs and symptoms
may be lacking.23 A recognized source of fever e.g. otitis media,
pneumonia, does not exclude the presence of meningitis. 23,66
The wide spectrum of presenting clinical manifestations and the
high degree of morbidity associated with the delayed treatment of
bacterial meningitis makes it essential to separate the child with

35
meningitis from among those with febrile seizures as soon as
possible.66
Although there is universal concern about the possibility that
meningitis may not be diagnosed quickly enough; there is
disagreement about the indicators for lumbar puncture.69 Some
reports are in support of routine lumbar puncture in all children
presenting with fever and seizure aged less than 18months while some
are not.16,64,67 A 6.3% yield for meningitis in a study by Laditan66 on
routine lumbar puncture after first febrile seizure, made him to
recommend continued performance of lumbar puncture in such
children especially under the age of 18months. So also did Rutter et
al67 report that it is not sufficient to limit lumbar puncture to the
children who did not have localizing signs of infection, for example a
child with a pneumonia could have a co-existing bacterial meningitis.
Another author65 argued that lumbar puncture is a reasonable
screening procedure and avoids unnecessary admission to the hospital
of children less than 18 months with simple febrile siezures.65 Only
those children who actually have meningitis are at risk of herniation
from the procedure but need a diagnostic tap anyway especially in a
hospital where supervision from experienced clinician is not always
available.
Lorber and Sunderland68 and Akpede16 had a different view
about routine lumbar puncture. Akpede et al16 reported a 4.2% yeild

36
of meningitis amongst the 522 children with fever and seizure.
Although six (27.3%) of the children with meningitis lacked the
classical signs, they had other indications for lumbar puncture
including; age less than six months, focal or multiple seizures,
absence of a past or family history of seizures, unrousable coma, and
an extracranial focus of infection. Akpede et al16 concluded that the
decision on the need for a lumbar puncture in children with febrile
seizures should not only be guarded by clinical evidence of meningitis,
but should take account also of features such as complex febrile
seizures, state of consciousness and previous or family history of
seizures. This also agrees with the recommendation of the RCP and
BPA.20
Lorber and Sunderland68 in the same vein argued that the risk of
coning/herniation after a lumbar puncture should be an indication for
not performing it routinely in febrile seizures. Review by an
experienced member of staff (senior resident, consultant) successfully
identified all cases of meningitis with the exception of one case of viral
meningitis in a group of 452 children with fever and seizure in their
study. It was however, not stated what parameters were considered in
the evaluation.
Some children with initial negative lumbar puncture later can go
to develop meningitis.67,68 This was observed by Rutter et al67 who
reported the case of 2 children who developed menigits withn 1- 2

37
days of a negative LP. This could be very dangerous considering the
prognosis of meningitis is related to the promptness of diagnosis and
early commencement of proper treatment in other to reduce morbidity
and mortality.
A major argument for the continuation of routine lumbar
puncture in children with fever and seizure in developing countries is
that other diagnosis such as Tuberculosis meningitis may be missed
or that it is not possible to exclude cerebral malaria.71 It is pertinent to
note that the simple addition of a broad spectrum antibiotic such as
chloramphenicol in a situation where pyogenic meningitis is a
possibility but LP is considered unsafe might no longer be adequate
because of the increasing problem of antibiotic drug resistance. The
differentiation of cerebral malaria from pyogenic meningitis is of
therapeutic importance bearing in mind that the use of
dexamethasone could be deleterious in cerebral malaria but
considered beneficial and desirable in pyogenic meningitis.71
Treatment of both infections concomitantly may be an unbearable
extra financial burden for some families.
Performing an LP in a person who has bacteraemia may cause
meningitis.71 Teele et al56 found an important association between LP
during bacterial infection and meningitis. This was most prominent in
children under the age of one year.

38
The American Academy of Pediatrics (AAP) and the Provisional
Committee on Qualitative Improvement in collaboration with expert
neurologists have developed a practice algorithms on the
neurodiagnostic evaluation of the child with the first febrile seizure.23
They reviewed over 200 medical journals and articles addressing the
diagnosis and evaluation of febrile seizures and concluded that an
increased risk of failure to diagnose meningitis occurs in:
1. Children less than eighteen months of age, who may show no
signs of meningitis.
2. Children who are evaluated by a less experienced health care
provider; and
3. Children who may be unavailable for follow-up.
It was concluded that the cerebrospinal fluid was more likely to
be abnormal in children initially seen with fever and seizures who
have had:
1. Suspicious findings on physical and neurological
examination;
2. Complex febrile seizures;
3. Physician visit within 48 hours before the seizures;
4. Seizures on arrival at emergency department;
5. Prolonged post ictal state; and
6. Initial seizures after 3 years of age.
They therefore made these recommendations:

39
1. After the first episode of seizures with fever in an infant less
than 12 months, performance of a lumbar puncture be
strongly considered, because the clinical signs and symptoms
associated with meningitis may be minimal or absent in this
age group;
2. In a child between 12 and 18 months a lumbar puncture
should be considered because signs of meningitis may be
subtle;
3. In a child older than eighteen months, although lumbar
puncture is not routinely warranted, it is recommended in the
presence of meningeal signs and symptoms (i.e. neck
stiffness, Kernig’s and Brudzuki’s signs) or for any child
whose history or examination results suggest the presence of
intracranial infection; and
4. In infants and children who have had febrile seizures and
have received prior antibiotics treatment, clinicians should be
aware that treatment could mask the signs and symptoms of
meningitis. As such a lumbar puncture should be strongly
considered.
In summary the AAP and the BPA recommended lumbar
puncture in every child less than 18months with their first febrile
seizure; a child older than 18 months if on antibiotics already before
the seizure; the presence of signs of meningeal irritation and after a
40
complex febrile seizure or if the child is unduly drowsy or irritable or
systemically ill.20,23
Full Blood Count (FBC) Full blood count is a routine investigation. In
a febrile child the presence of a leucocytosis of > 15,000/mm3 could be
an indication of a bacteraemia especially in children with acute fever
without localizing signs.71,72 AAP stated that FBC is useful in the
evaluation of fever in young children as the incidence of bacteraemia
in children younger than 2years with or without febrile seizures is the
same.23 By combining age, temperature and white blood count it is
possible to delineate a group of children with a very high incidence of
bacteraemia.71 Mc Gowan et al74 found a 28% incidence of
bacteraemia in children aged 7- 14 months with temperature > 39.5oC
and white blood count of > 20,000/mm3. Ayoola et al72 reported that
age less than 6months, restlessness and a WBC of > 15,000/mm3 are
associated with significantly increased risk of bacteraemia. Thirty-
eight percent of the infants with fever had bacteraemia in their report.
When fever is present, the decision regarding the need for
laboratory testing should be directed towards identifying the source of
fever rather than as part of the routine evaluation of the seizure
itself.23 Leucocytosis in the presence of a neutrophilia is an indication
of an underlying bacterial infection.71 The result of a segmented
Neutrophil count > 10,000/mm3 or a band neutrophil count >
5,000/mm3 increased the risk of severe bacterial infection to 80%. All

41
of their patients with occult bacteraemia had high white cell and
neutrophil counts.71
Blood Culture There is adequate data existing to show that
bacteraemia is a relatively common disease in young apparently mildly
ill febrile children.56 Although bacteraemia resolves spontaneously in
some children, many remain ill. Some have persistent bacteraemia, in
others a focal infection develops and in a few, severe disease like
meningitis occurs.
The problem of accurate diagnosis in children presenting with
fever especially without a localizing sign cannot be underrated. In the
tropics children presenting with fever could have positive malaria
parasitaemia but studies have shown this does not rule out the
presence of a bacteraemia or even a urinary tract infection.54,56 Blood
cultures have been considered an important part of the evaluation of
febrile children with underlying illnesses and those with selected soft
tissue infections.55 The issue arises of whether to do routine blood
culture in these children as they present in the clinic and also whether
treatment with an antimicrobial empirically is beneficial. The presence
of bacteraemia without a soft tissue focus is a therapeutic challenge
and the use of empirical antimicrobial has been suggested.55 There
are reports on this issue.56,75 In some reports, the outcome of children
sent home at first visit with unsuspected bacteraemia indicated that
children treated at first visit had a superior outcome when compared

42
to those left untreated.56,75,76 There is still no non invasive readily
available technique for distinguishing the febrile child with a non
bacterial infection who is likely to have spontaneous resolution from
the child with invasive bacterial infection requiring aggressive
management hence adequate clinical assessment should be done with
consideration of age of the child, temperature at presentation and
white blood cell count because they have been found to be indices of
the presence of bacterial infection.54,56,75
In a report, the outcome of children sent home at first visit with
unsuspected bacteraemia indicated that children treated at first visit
had a superior outcome when compared to those left untreated.76 It is
believed that presumptive therapy is warranted for the children from 6
– 24 months of age who have both a fever of > 38.90C and a WBC of >
15,000/mm.3
The use of blood culture in the out-patient department could be life
saving would help in accurate and prompt management of children with
fever.
Patients with simple febrile seizures are at approximately the
same risk for bacteraemia as children with fever alone.70 Out of the 93
patients with simple febrile seizures that James et al 70 studied, 5.4%
had positive blood culture. It was discovered that neither age nor
history of febrile seizures affected the risk of bacteremia. They argued
that patients with simple febrile seizures should be treated in the
43
same manner as other patients of the same age with regards to the
performance of blood culture.
Occult pneumococal bacteraemia may be an important cause of
febrile seizures. A study carried out on children in the outpatients
department showed that occult pneumococal bacteraemia occurred
frequently in young febrile children whose illness seemed trivial, and
thus did not warrant blood samples being taken.72 Persistent
bacteraemia and the development of focal infection including
pneumonia and pneumococal meningitis have been reported.72 Ayoola
et al72 suggested that age less than six months; restlessness and a
white blood count of 15,000/mm3 are associated with significantly
increased risk of bacteraemia. Thirty-eight percent of the infants with
fever in their study had bacteraemia.
A history of febrile seizures should not dissuade the
emergency room physician from performing blood culture.
Electroencephalogram (EEG) The EEG is abnormal in 90% of
children on the day after the febrile seizure. During the first week,
tracings are abnormal in about one third of cases, but afterwards only
5% or less are abnormal.10
Paroxysmal abnormalities in the EEG are not predictive of
recurrent febrile seizures.16 Some have found that the EEG predicts

44
later epilepsy,77,78 but others23 have not. The AAP’s review23 also
stated that there was no evidence that an abnormal EEG after the 1st
febrile seizure is predictive of either the risk of recurrence or the
development of epilepsy. Since EEG is expensive and unhelpful in
management, it should not be routinely carried out in children with
febrile seizures.
Skull X-rays The expense, radiation exposure, and lack of clinical
value suggests that skull x-rays, should be done only if there is a
suspicion of underlying brain disease or afebrile seizure.10 However in
current practice, Computerized Topographic Scan or Magnetic
Resonance Imaging may be more useful in these conditions.
Electrolytes These tests are rarely indicated and should be reserved
for children in whom significant fluid loss and dehydration occurs.10
Hospitalization
Several authors 10,69 have reviewed the issue of routine
hospitalization of children with febrile seizures and it was concluded
that admission should be considered only in those in whom serious
underlying disease is suspected.69
Some authors 10,69 state that clinicians often give parental
anxiety as an indication for admission10 but recommend that the
physician should emphasize the benign nature of febrile seizures and
not reinforce parental fears by admitting the child.69

45
There are principles guiding the issue of whether a child with
febrile seizures should be admitted or not. In UCH, children with
febrile seizures are not routinely admitted rather each child is
stabilized, a good history and examination done and the child is
assessed for cause of the fever and the severity of the illness. If it is a
first episode of febrile seizure, lumbar puncture is done to rule out
meningitis while other investigations are done as indicated. If the child
is alert, active after a period of observation the child is sent home on
medications to be seen on follow up. If the child’s condition, depending
on the cause of the fever, indicates further monitoring, then admission
is imperative.
The RCP/BPA joint working group decided that the following
factors would favor admission after a first febrile seizures:
Complex febrile seizures
Child less than 18 months
Unusual parental anxiety or inability of the parents to cope
Doctor not easily available to review at home20
The child should be kept for observation for few hours while
awaiting retrieval of CSF results and other basic investigations.
Hospitalization of patients with febrile seizure should not be
routine, rather each child’s case should be judged appropriately by the
attending physician who has been trained and is skilled to do so.

46
Parental Role and Socioeconomic factors in the outcome of
febrile seizures
It has been observed that the majority of parents have gross
misconceptions about febrile convulsions and hence take inappropriate
or even harmful actions in an attempt to control the convulsions.11 It is
believed that their social attitudes and behavior contribute immensely
to the high morbidity and unfavorable prognosis of febrile seizures in
this part of the world.2, 11
Iloeje11 carried out a population study of 845 Enugu parents
regarding their views of the causes, prognosis, best treatment options
and prophylaxis in febrile seizures. The parents were also asked to
state what steps they took whenever their children had fever with or
without seizures. Most (64.9%) of them gave a native concoction.
Others (16.9%) took harmful actions such as burning of the so le of
the feet, scarification, etc. Fifteen parents (9.4%) took measures to
bring down the child’s temperature such as tepid sponging and
fanning the child; only 14 parents (8.8%) took the child immediately to
the hospital. Many (56%) of parents either did not know the cause of
the convulsion or attributed them to evil spirits, God or as secondary
to constipation. Familusi et al 2 also recorded a high number (52%) of
parents administering native concoction (cow urine concoction) to
their children with febrile seizures. This was found to be contributory
to the high mortality rate of 6.4%.

47
With respect to the reaction of people who witnessed the attack,
Rutter et al79 reported that the reaction of the first person to witness
the convulsion was often one of fear and panic. They usually shouted
for help from the household or from neighbours. Some called their
doctor or an ambulance at once. Reactions towards the child are also
extremely variable. Some would lie the child down, others would place
the child in the sitting position while some would hit the child on the
back or even try to prise the child’s clenched teeth apart. Some
parents are known to actually attempt mouth-to-mouth resuscitation.
In the study by Rutter et al 79 30% of the parents interviewed
spontaneously volunteered that they thought their child was dying or
dead. These observations were further buttressed by Parmer et al5 who
reported that up to 90% of parents thought their child was dying
during the convulsion. After the acute episode, recurrence and
epilepsy were the major parental concerns. Most parents thus show a
severe psychological reaction to their child’s convulsion. This,
however, contrasts with the doctor’s consideration of febrile seizures
as a benign phenomenon. It is possible that these contrasting
perceptions are a result of the communication between the doctor and
parents being ineffective in imparting the right information and
knowledge. It is therefore essential that the physician know about
parental concern and anxieties in order to establish a meaningful
dialogue and allay their fears effectively.5

48
It has also been shown that parental anxiety and apprehension is
related to inadequate knowledge of fever and febrile seizures.80
Maternal education plays an important role in the quality of health
care a child receives.81 Children of mothers with no formal education
are at least twice as likely to die before age five than children of
mothers with post primary education.81
Correct and adequate knowledge of the relationship between fever and
febrile seizures, and its usual good prognosis, are important for
lessening the parental anxiety and apprehension associated with
febrile seizures. Many parents even develop fever phobia and each
febrile episode in the child can be a nightmare for the parents.5,79
Mothers constitute a good target group for specific health
education. Basley as cited by Oseni14 reported those parents with
previous knowledge of febrile seizures took more appropriate measures
during a convulsion than parents without such knowledge. It is
therefore very important that caregivers are educated on the
acceptable ways of managing febrile seizures when a child is brought
to the hospital. This is particularly relevant, given the propensity for
recurrence of seizures in the same child. Mothers irrespective of their
educational of social background should be taught on specific things
they should do when a child has a seizure.
Specific things to do when a child has a seizure include;
don’t panic

49
remove the child from harmful substances
lay him/her on the side and hold the child
If seizure does not stop after 10 minutes take to the hospital.
In places where there are home services the doctor could be
called in.
Basic health education can be incorporated into the curriculum
in both the primary and secondary schools. If topics such as
management of febrile seizures are taught, especially emphasizing
what not to do during a seizure, the impact on the children of such
students when they become parents will be appreciable. Such basic
health education can also be offered in programmes in the print and
the electronic media. In this way, even people who have not had the
opportunity of formal education can benefit.
Treatment
A rational approach to the management of febrile seizures
should take into account that the long-term prognosis is excellent,
and that there is no evidence that prophylaxis reduces the risk of
subsequent non-febrile seizures.19
An initial work up of febrile seizures should include a complete
history and complete physical examination with emphasis on
neurological examination, including characterization of the febrile

50
illness, degree of temperature elevation and complete description of
the febrile seizures.19
The management of a child with febrile seizures involves
1. Acute Stage
a. Control of seizures
- Some children are be brought into the hospital
convulsing and hence need to be resuscitated by
maintenance of airway, oxygen administration and
aborting the seizures .21
b. Control of fever
This is achieved by administration of antipyretics.1, 21
Acetaminophen produces relatively prompt lowering of the
temperature. However, some studies have shown that
antipyretics therapy is not effective in preventing febrile
seizures.20,21 This may partly be because the seizures can
occur during the rapid rise of temperature even before the
elevated temperature is noticed by the care-giver. The child
could also benefit from tepid sponging and fanning. It is
advisable to offer these latter therapies about 30 minutes
after the administration of acetaminophen, otherwise tepid
sponging will induce shivering which can increase the
temperature again.80
c. Treatment of the aetiology of the febrile illness.

51
Since febrile seizure is always a symptom of a generalized
illness, adequate physical examination and appropriate
laboratory investigations should be carried out and specific
treatment given for specific illness e.g. antimalarials for
malaria and antibiotics for pneumonia.
2. Prophylaxis
This is usually with the use of anticonvulsants.1, 82
There are two types:
(1) Intermittent: medications are given whenever the
temperature is greater than 380C and is continued
throughout the febrile illness.
(2) Prolonged or continuous: medication is given on a daily
basis.19
The use of prophylactics for treating febrile seizures is
controversial.83 Some doctors think that long term treatment with
phenorbarbitone is indicated after one episode,84,85 others do not.86
Some believe long term treatment with phenorbarbitone prevents
recurrence84,87 others consider it of limited or no prophylactic value.88
However, nearly all agree that side effects and non compliance are
common.84-88
Fransten et al89 reported a one year recurrence rate of 25% in
172 children who were not given any anticonvulsant treatment as
52
compared to 16% obtained in Knudsen et al”s study90 in which
diazepam or phenobarbitone was administered.
In a report by Wallace91 of 116 children who did not receive
anticonvulsants after their first febrile seizures, 55(47%) had a
reccurence with a subsequent febrile illness. A significantly increased
risk was present in:
Those with perinatal neurological abnormality
With a complicated initial fit
Males with history of convulsion disorder in parents and
wards
Females with age of onset less than 19 months.
The findings could be used for selecting children with a
higher possibility of a recurrence.
Regular administration of phenobarbitone significantly reduced
the recurrence rate of febrile seizures when compared to no
treatment or intermittent treatment in a study by Wolf.87
Fifty percent of febrile seizures occur in the first 24hours of an
illness.85 Knowledge of pharmacology indicates the futility of
administering phenobarbitone for the prevention of febrile seizures
when fever is detected.92 It must be administered for at least 5 half
lives to achieve a steady level of the drug in the serum. While the half-
life may be variable and age dependent, at least several days of
administration is required to achieve an effective therapeutic level of

53
15micro gram per milliliter when the usual therapeutic doses of 3 – 5
mg/kg are prescribed.92
The condition for an effective intermittent prophylalaxis of febrile
seizures with diazepam must be to give the drug in sufficient dosage
and to give it on time as soon as the symptoms and signs of ill health
occur in the child.93 In a report by Dianese, et al93 the parents of 101
children were interviewed about the children who had had febrile
seizures for recurrence and also all the records of readmissions as a
result of a new febrile seizure or other illnesses were reviewed. Of
these, 90 had febrile episodes after the first febrile seizure and met the
criteria for intermittent prophylaxis. Forty-eight received diazepam
adequately and in the doses suggested, 42 did not.
Continuous phenobabitone (3-5mg/kg/d) and short-term
diazepam (0.3-0.5mg/kg/dose 8 hourly, rectally) at the first sign of
febrile illness till the second day of complete recovery have been
compared.14 They were all found to be effective in the prevention of
febrile seizures but there is controversy on the choice of drugs because
of the problem of side effects.
The side effects of phenobarbitone which include; irritability,
hyperactivity, negativistic behaviour and rashes are sometimes severe
enough to warrant withdrawal of the drug or produce poor compliance
in other cases.94.

54
Evidence suggests that the frequency of febrile seizures may be
reduced by the prompt administration of diazepam per rectum at the
onset of acute febrile illness.19, 82,83 Side effects include lethargy,
ataxia, irritability and sedation, though these are rarely seen.
Knudsen and Vestermark90 carried out a cohort study
comparing, the rate of recurrence of febrile seizures after the first
episode in two groups of children. The first group was given
intermittent diazepam (suppositories) any time temperature was
greater than 38.50C whilst the other group was given daily
phenorbabitone. It was discovered that the recurrence rate was
similar and so also the duration of seizures. They concluded that
long-term treatment with phenobarbitone offered no advantage over
intermittent diazepam.
Sodium valproate at a dose of 20 – 40mg/kg/day has been
reported to be effective, but hepatic toxicity following the prolonged
use has been reported.10,95 However in a study by Ogunmekan et al95
no patient receiving Sodium valproate as the first anticonvulsant
prophylactic drug experienced a second during the first 6months. In
patients who had previously received phenobarbitone, there was a
90% reduction in seizure recurrence. Recurrence was also decreased
in 3 of the 4 children who had had side effects to phenobarbitone
before withdrawing it. There was no significant side effect with sodium
valproate.

55
Recurrence
It has been suggested that each seizure makes it easier for
another to occur.1 Of the children with febrile seizure, 30-40% who do
not receive prophylactic therapy will experience a second.19
There have been various reports on the recurrence rates of
febrile seizures.9, 14,43 Most of the recurrences occur within six to
twelve months of the initial febrile seizure.7
The risk of recurrence is influenced by the neurological status of
the child prior to the seizures, the age of the patient at the time of the
first seizure and the character of the seizure.92
Risk factors for recurrence include; 7,21
- Family history of febrile seizures and or epilepsy.
- Age less than fourteen months at the first seizure
- A short duration of illness (<24hrs) prior to febrile seizures
- Low temperature at time of febrile seizure
- Attendance in day care centre
- Developmental delay.
The single most important factor in predicting recurrence is the
age at the time of the seizures.95 Nelson and Ellenberg96 found 50%
recurrence rate in children with onset of febrile seizures in the first
year of life as opposed to a 28% recurrence rate with onset after the
first year of life. In a population- based study by Nelson et al9 it was

56
found that a third of the children (30%) who experienced a febrile
seizure had at least one recurrence and half of those who had at least
one recurrence had a further episode. Nine percent of the 1706
children they studied had over 3 or more recurrences. Males and
females and blacks and whites did not differ significantly in their
vulnerability to recurrence in the study. It was postulated that the
likelihood of recurrence was related to age at onset of febrile seizures.
In children who experienced their first episode of febrile seizures
before their first birthday, 30% later experienced multiple recurrences,
while only 11.1% of those whose first episode occurring after their first
birthday experienced multiple recurrences.
Airede97 found that patients with moderate degrees of pyrexia
(39-39.90C) at first febrile seizure were 10 times more likely to have
subsequent recurrence than those with low or high degree of pyrexia.
This is at variance with what is popularly stated that recurrence is
more likely when first seizure occurs at a lower temperature.7
Imuekheme17 from Benin, measuring serum CSF Copper and
Zinc levels on admission in febrile seizure patients found low serum
zinc levels on admission to be significantly associated with recurrence
of the seizure and therefore helpful in deciding the risk of recurrence.
Complications
Epilepsy Only 2-4% of children with febrile seizures develop
57
epilepsy.7 Risk factors for developing epilepsy include a family history
of non-febrile seizures, abnormal neurological or developmental status
prior to febrile seizures and atypical febrile seizures.
Nelson and Ellenberg96 carried out a prospective population
study of 1706 children with febrile seizures over a period of years till
age 7 years. They discovered that only 3% of these children developed
afebrile seizures by the seventh year of life. Lennox,78 reported a
higher incidence of 5- 12% amongst the 240 children febrile seizures
studied over a 3 year period. However, the number of febrile seizures
these children had had in the past was not stated.
Abnormal neurological or developmental status, occurrence of
complex first febrile seizures and history of non- febrile seizures in a
parent or older sibling were found to be significant predictors of
epilepsy in a report by the NCPP.9 The number of episodes of febrile
seizures has also been found to have a positive relationship with
epilepsy as reported by Lennox44 and Wallace.77
In a retrospective study by Annegers et al 8 the medical histories
of residents of Rochester, Minnesota who had a diagnosis of febrile
seizures within a period of 40 years were reviewed. The relative risk of
epilepsy following febrile seizures declined with increasing age. They
reported further that the occurrence of subsequent partial unprovoked
seizures was strongly associated with all the three complex features
whereas the occurrence of subsequent generalized seizures was

58
associated with the number of febrile seizures and a family history of
unprovoked seizures.
Pathogenesis of epilepsy following febrile seizures may be
different amongst various seizure types.98-100 Konishi et al98 studied
the clinical, EEG and developmental factors of 46 epileptic children
following febrile seizures. Eleven hade generalized seizures while 34
had partial seizures. Intractable seizures were recognized in 9% of the
partial seizure group. Motor and mental defects were more frequently
associated with the partial seizure group than with the group with
generalized epilepsy following febrile seizures. Complex febrile seizures
are associated with increased risk of epilepsy.3 A study by kanemoto
et al99 confirmed the close association between complex febrile
seizures and temporal lobe epilepsy.
Hippocampal sclerosis is the most common pathology in
intractable temporal lobe epilepsy.101 Bower et al 101 in reviewing the
relationship between the degree of hippocampal atrophy and the
incidence of febrile seizure in patients with temporal lobe epilepsy,
reported that the degree of MRI-determined hippocampal atrophy was
not related to a history of febrile seizures. They were more in support
of the hypothesis that hippocampal sclerosis is a pre-existing
abnormality in patients with febrile seizures who later develops of
temporal lobe epilepsy.

59
It is therefore apparent that the issue of later onset of recurrent
non-febrile seizures should be addressed when managing cases of
febrile seizures, with emphasis on taking a good history, especially
the premorbid neurological status, family history of seizures and the
nature of the seizures.
Neurological Deficits
The child with febrile seizures may have neurological deficits
such as motor deficits, sensory and perception abnormalities.19
There is some controversy regarding the effects of cow’s urine
mixture. Some authors2,102 believe cow urine mixture is responsible for
the neurological complications seen in patients with seizures while
some do not.103 Some authors believe hypoglycemia which is induced
by some unknown component of cow urine mixture is responsible for
the permanent neurological sequelae and prolonged coma seen in
some patients given this mixture,2,57,102,104 while some do not see any
correlation between the administration of cow urine mixture to
children with seizures and the incidence of hypoglycemia, neurological
sequelae and death.103
Familusi et al2 reported persistent neurological deficits in 49
(8.3%) of the 590 children with febrile seizures. The neurological
deficits included generalized spasticity, behavior disturbances,
hemiplegia, decerebrate rigidity, blindness, deafness and
choreathetosis. However, the deaths and neurological deficit were

60
more common among patients to whom traditional concoctions (cow
urine) were administered for control of seizures. Thirteen percent of
the 309 patients who received cow’s urine mixture developed
permanent neurological sequelae as compared with only 2% of the 197
patients who did not receive the mixture.
The popular native concoction used in the part of the country
where this study was done is the cow’s urine concoction. This contains
tobacco leaves, garlic leaves, basil leaves, lemon juice, rock salt, bulb
of onions all soaked in cow’s urine or human urine in varying
strengths and for varying lengths of time.105 Oyebola106 in his review of
the chemical components and pharmacological actions of cow’s urine
concoction reported the deleterious effects of native concoction on the
brain and other body systems. These include; cardiovascular effects
like tachycardia, blood pressure and electrocardiographic changes.
Respiratory complications include: respiratory depression and
respiratory failure while other effects are profound hypoglycaemia,
reduced neutrophil and monocyte counts (thus increasing the risk of
infection), restlessness, spasms, intracranial haemorrhage, paraplegia,
coma and death.
The clinical findings in patients given cow’s urine mixture are,
on the whole compatible with nicotine poisoning and the occurrence of
toxic symptoms in those who have only had the mixture rubbed into

61
the skin supports the concept of nicotine poisoning because of the
known ease with which nicotine is absorbed from the skin.57 Some
findings in cow’s urine mixture poisoning, such as prolonged coma
and permanent neurological sequelae do not however accord with
nicotine toxicity and suspicion has long centered on hypoglycemia
induced by unidentified constituents of the concoction, as the cause of
these complications. This suspicion has been reinforced by the
frequent detection of hypoglycemia in patients given cow’s urine.107
Familusi et al2 found hypoglycemia and low CSF glucose in 19% of
patients given cow’s urine mixture, but in only 1.5% of those not
given. Severe hypoglycemia was also found in 24 out of 70 epileptics
known to have had the mixture.104, These are indications but not proof
of a causal relationship between cow’s urine poisoning and
hypoglycemia. In a study by Ojewole et al102 on rats, they reported a
firm evidence of a time and dose related hypoglycemic effect of the
cow’s urine mixture. The mechanism by which it is induced is however
not known. Some authors do not agree with this correlation, Ransome
kuti et al103 reported that there was no correlation between the
administration of cow urine to children with convulsion and the
incidence of hypoglycemia, neurological sequelae and death
Verity et al45 reported speech problems in patients with febrile
seizures. Curiously, it was children who had had simple rather than
complex febrile seizures that were affected. Eleven out of the 42

62
children they studied had recovered fully within 5years and only one
case was said to have been severe. Aicardi et al 107 in a series of 402
patients with febrile seizures hospitalized or seen as outpatients
reported that 37(9.2%) had neurological sequelae out of which 24%
had hemiplegia. Wallace111 reported that 27 out of 100 children
followed up for 2-4years after hospitalization for febrile seizures had
evidence of seriously disturbed behavior.
Some authors are however, of the opinion that these neurological
deficits usually antedate febrile seizures.1, 19 Their argument is that
there is no epidemiological evidence that these deficits reflect
neurological injury at the time of the febrile seizure. It is therefore
possible that neurological deficits following febrile seizures are not
purely as a result of the seizures. Rather, they may represent the
premorbid status of the patient or are secondary to the form of
treatment offered.
Intellectual Outcome
In children admitted to hospital with febrile seizures Lennox109
found mental retardation at follow up in 22%. However the author did
not do a premorbid IQ assessment of the children. About half the
reports reviewed by Wallace21 reported that 5-10% of their patients
were retarded. Nelson and Ellenberg96 selected 431 children from the
1,706 with febrile seizures in the National Collaborative Perinatal

63
Project. Siblings in the study who had not had febrile seizures acted
as control for intellectual testing at seven years of age. Children who
were normal before any febrile seizure did not differ in intelligence
quotient (1Q) from their normal seizure- free siblings, while children
who were suspect or mentally challenged before the first febrile
seizures scored significantly lower IQs than their siblings. Neither
recurrent seizures nor seizures lasting longer than 30 minutes were
associated with IQ deficit. A population based study in the United
Kingdom101 also found little difference in intelligence outcome between
children with febrile seizures and their peers if the children with
febrile seizures had no other known neurological abnormality. It is
therefore doubtful if recurrent febrile seizures have any significant
effect on IQ.

64
AIM AND OBJECTIVES
The general objective of this study was to evaluate the pre- hospital
management, pattern, aetiology and outcome of febrile seizures in
children seen at the Children’s Emergency Ward of the University
College Hospital, Ibadan.
The specific objectives are;
1. To determine the prevalence of febrile seizures amongst children aged
3months - 5years admitted into the Children’s Emergency Ward of the
University College Hospital Ibadan.
2. To determine the pattern of febrile seizures in affected children.
3. To determine the underlying cause of fever in children with febrile
seizures.
4. To determine the influence of socioeconomic class and maternal
education on the type of pre-hospital management given to children
with febrile seizures.
5. To determine the short-term morbidity and case fatality rate
among affected children with febrile seizures.
65
SUBJECTS AND METHODS
STUDY SITE
This study was carried out between November 2002 and
December 2003 at the University College Hospital (UCH), a tertiary
health institution with 805 beds in Ibadan, Oyo State, Nigeria. UCH
caters for patients from Ibadan and its environs and sometimes for
patients from other parts of Nigeria.
The Paediatric unit is made up of an emergency ward named
Otunba Tunwase Children’s Emergency Ward (OTCHEW) and 5 other
wards for the admission of patients. Most of the patients admitted to
the wards are initially seen in the emergency ward, while a few
patients, usually with chronic illnesses are admitted to the wards from
the outpatient clinics. A patient with an emergency such as febrile
seizures would be seen initially in the emergency ward. For this reason,
the study was conducted at the OTCHEW.
The emergency ward has a resuscitation area where critically ill
children are nursed till stable before being transferred to the ward
area. There is also a general ward, measles bay, a diarrhea therapy
unit, a neonatal ward, a laboratory, a pharmacy and a records and
accounts unit.
Children brought to OTCHEW are seen by the registrar on duty

66
who does a brief clinical assessment and resuscitates the child
depending on how critical the case is. There are house physicians
and nurses on the ward to assist in managing the children. The senior
registrars conduct wardrounds regularly and see to the smooth
operation on the ward.
Children stay for a maximum of 48hrs and afterwards they are
either discharged to follow up or transferred to the other wards hence
creating room for more admissions.
The cases seen in OTCHEW include: - severe malaria, severe
anaemia, acute respiratory infections, neonatal problems, burns,
measles, tetanus, diarrhea cases, septicaemic illnesses, severe
malnutrition, seizures, coma cases and so on.
67
SAMPLE SIZE ESTIMATION
The sample size was calculated using the formula110 n =Z2pq d2
nf =n
1 + n N Where,
n = the desired sample size when the population is greater than
10,000.
nf = the desired sample size when the population is less than 10,000.
z = the standard normal deviate, usually set at 1.96, which
corresponds to the 95% confidence level.
p = the proportion of the target population estimated to have a
particular characteristic (0.04) q = 1.0 –p
d = degree of accuracy desired usually set at 0.03. N = the estimate of the population size. The admission records of the last year preceding this study were
reviewed and these showed that, 1640 patients were admitted into the
children’s emergency ward. Of these, (3.7%) had febrile seizures.
The estimated prevalence (p) is 60 1640

68
= 0.037
= 3.7% n = (1.96)2 (0.037) (0.963)
(0.03)2 = 152 nf = 152 1 + 152 1640
= 139
The calculated minimum sample size was 139. However, the
sample size was increased to 147 to accommodate for attrition.
Procedure
This was a 14-month prospective study carried out at the University
College Hospital Ibadan, from November 2002 to December 2003.
Children were recruited from the OTCHEW. Inclusion Criteria
The following inclusion criteria were used to select children for the
study.
(i) age 3 months to 5 years
(ii) History of seizures in the presence of a fever ( axillary
temperature >37.50C) at presentation in hospital or fever and
seizure occurring while in the hospital.
(iii) normal cerebrospinal fluid.
69
Exclusion Criteria
(i) children below 3 months and above 5 years of age.
(ii) children with previous or on-going nonfebrile seizures
(iii) children with acute head trauma associated with seizures
(iv) children with congenital or acquired central nervous system
abnormality
(v) children with abnormal cerebrospinal fluid.

70
RECRUITMENT OF PATIENTS AND CONDUCT
OF THE STUDY
Ethical Clearance
Ethical clearance for the study was obtained from the Joint
University of Ibadan/University College Hospital Ethical Committee.
(Appendix I)
The investigator evaluated all new patients admitted into the
paediatric emergency room of the University College Hospital Ibadan
on the first day of admission into the hospital to identify those with
febrile seizures and this was done on a daily basis over the period of
the study.
Methodology
The investigator obtained verbal consent from the parents or
caregivers of the children before they were recruited into the study. A
history of the illness was obtained from the caregivers and the patients
when this was possible. The name, age, sex, presenting complaints,
duration of symptoms before presentation, birth weight if available,
and pre-hospital management were recorded in a proforma designed
for the study (Appendix II). A thorough physical examination was
performed on each patient at admission with particular emphasis on
the central nervous system. Anthropometric measurements were taken.

71
These included weight (kg) on admission, occipitofrontal circumference
(OFC) in cm, and the length or height (cm).
Temperatures were taken using clinical mercury-in-glass
thermometers. The bulb of the thermometer was placed at the apex of
the axilla, halfway between the anterior and the posterior margins of the
axilla and read after four minutes.111 Children less than two years of
age were weighed using the Way Master Model 1615K Infant Scale (Way
Master Co Reading, England) while those aged two years and above
were weighed using a flat scale (Hanson, Model: 89p, Ireland), and the
weight measured to the nearest 0.5kg. The scale was checked for zero
error before weighing. The OFC was measured by passing a tape
measure around the forehead and the occiput without the measuring
finger getting in between the tape and the head. Length was measured
using a tape measure from the vertex to the heel of the child in patients
who could not stand. Older children were made to stand with the heels
of the bare feet against a wall on which was a tape accurately calibrated
in centimeters. The findings on examination were recorded on the
proforma (Appendix II). The clinical diagnosis, the results of
investigations and the final diagnosis were also recorded on the
proforma (Appendix II). All the patients were seen and examined by the
investigator.
Laboratory Investigations
72
The extent of laboratory investigations was determined by the
clinical diagnosis. However, the following investigations were
performed on each recruited patient irrespective of the clinical
diagnosis: packed cell volume, full blood count, blood film for malaria
parasites, blood culture, urine microscopy, culture and sensitivity,
random blood sugar and CSF analysis. The Technologists in the
Microbiology, Haematology and Chemical Pathology departments who
routinely analyzed such specimens performed the laboratory analyses.
Lumbar puncture was performed on each child at presentation. The
patient was placed in the lateral recumbent position while an assistant
flexed the neck and legs of the patient. The skin of the lower back was
thoroughly cleaned with methylated spirit. A 23 or 21 gauge needle
was introduced into the midsaggittal plane at L4/5 or L3/4 spinal
space directed slightly in the cephalic direction. About 2 mls of
cerebro-spinal fluid was obtained for microscopy, culture and
sensitivity and also for sugar and protein content.
One to three mls of venous blood was obtained from a peripheral
vein after the skin surface had been cleaned with methylated spirit. A
new hypodermic needle was then attached to the syringe containing
the blood and the blood was injected into a culture bottle containing
glucose broth for the detection of organisms after cleaning the rubber
cap of the culture bottle with methylated spirit. This culture bottle was
immediately taken to the laboratory to be incubated. This was done
73
aerobically at 370C for 7 to 10 days. Facility for anaerobic culture was
not available in our centre during this study. Venous blood was also
taken for packed cell volume, full blood count and random blood
sugar. The sample for random blood sugar was taken before the
lumbar puncture was performed. Peripheral blood films (thick and
thin) were prepared in a standard manner, Giemsa stained and
examined under oil immersion; 200 thick film fields were examined
before findings were declared negative. Parasitaemia was graded from
+1 to +4 where one plus = 1 to 10 parasites per 100 thick fields, two
pluses = 11 to 100 parasites per 100 thick film fields, three pluses = 1
to 10 parasites per one thick film field and four pluses = more than 10
per one thick film field. One to three millilitres of “clean catch” urine
was collected in to a sterile universal bottle and sent to the
microbiology laboratory for microscopy, culture and sensitivity. The
samples were processed within one hour of collection. Chest X-rays
were done in children who had clinical evidence of lower respiratory
tract infection.
The patients were followed up till discharge with regular
examinations to detect neurological deficits and the total duration of
hospital stay was noted.
In UCH, lumbar puncture is done on every child presenting with
the first febrile seizure but for the purpose of this study, every child
presenting with fever and seizure had a lumbar puncture done.

74
Treatment and Monitoring of Patients
Convulsions were aborted with deep intramuscular injection of
paraldehyde (1ml/year of life to a maximum of 5mls) or intravenous
diazepam at 0.1-0.3mg /kg given slowly until the seizure stopped with a
maximum dose of 10mg. Repeated convulsions were controlled with a
loading dose of intramuscular phenobarbitone at 15-20mg/kg stat then 3-
5mg/kg/day in two divided doses.
Patients who had packed cell volume less than 15% had packed red
cell transfusion. In children with malaria parasitemia, antimalarial
therapy was instituted. Uncomplicated malaria where only one episode of
febrile seizure had occurred was treated with oral chloroquine. If
chloroquine had been used previously, alternatives in the form of
amodiaquine or primethaime/sulfadoxine were used. In the presence of
repeated seizures or other indications of complicated malaria, quinine or
artemisinine was the drug of choice. In children with clinical diagnosis of
septicaemia, urinary tract infection or other bacterial infection,
appropriate antibiotic therapy was instituted based on the usual drugs
normally administered to treat various infections pending results of
investigations.
Statistical Analysis
Data analysis was done using Statistical Package for Social
Sciences (SPSS) version 10 and exported into Epi info version 5

75
software package for formal analysis on anthropometry. The initial
frequencies of the variables were done to generate the mean, standard
deviation, minimum and maximum values. Categorical data were
compared using Chi-squared test and Fisher’s exact test where
applicable. Differences were deemed to be statistically significant
where p<0.05.
Anthropometric analysis
The formal analysis on anthropometry was done by taking the
weight and height measurements and comparing them with the
National Centre for Health Statistics (NCHS) growth charts (these now
constitute the World Health Organization international growth
reference curves). using the Epinut analysis module of Epi Info
version5.112,113 To determine the proportion of stunting, wasting,
underweight and over-weight the following cut off points were used:
Stunting: z score of height for age <-2SD; wasting: z score of weight for
height <-2SD; under-weight: z score of weight for age <- 2SD; over-
weight: z score of weight for height >+ 2SD.114 `
Socioeconomic classification
The socioeconomic classification was done using Oyedeji’s
method.115 This classification considers the level of education and the
occupation of both parents:
No formal education 5 unemployed/housewife/farmer 5

76
Primary education 4 unskilled worker 4
Secondary education 3 skilled worker 3
Post secondary nonprofessional (secondary
education 2 school teacher/senior civil
servant/well to do business-
University/HND 1 man or woman) 2
Professionals 1
The scores are added together for both parents and the average score
obtained. A score of 1-2 = upper class, 3 = middle class, and 4-5 =
lower class.

77
RESULTS
During the 14-month period of this study, from November 2002
to December 2003, 147 children admitted to the OTCHEW at the UCH,
Ibadan, Nigeria, satisfied the criteria for inclusion into the study.
Prevalence of febrile seizures
There were a total of 1,487 paediatric admissions into OTCHEW
during the study period. Of these 147 were cases of febrile seizures
giving a prevalence of 9.9%.
Age and Sex Distribution
Table I shows the age and sex distribution of the children studied.
There were 83(56.5%) males and 64(43.5%) females giving a male:
female ratio of 1.3:1. The ages of the children ranged between
4months and 60 months (5 years) with a mean + standard deviation of
26.35 + 13.76 months. The mean age of the males was 25.71 + 13.24
months while that of the females was 27.19 + 14.4 months. The
highest numbers of children were in the13 - 24 age groups.
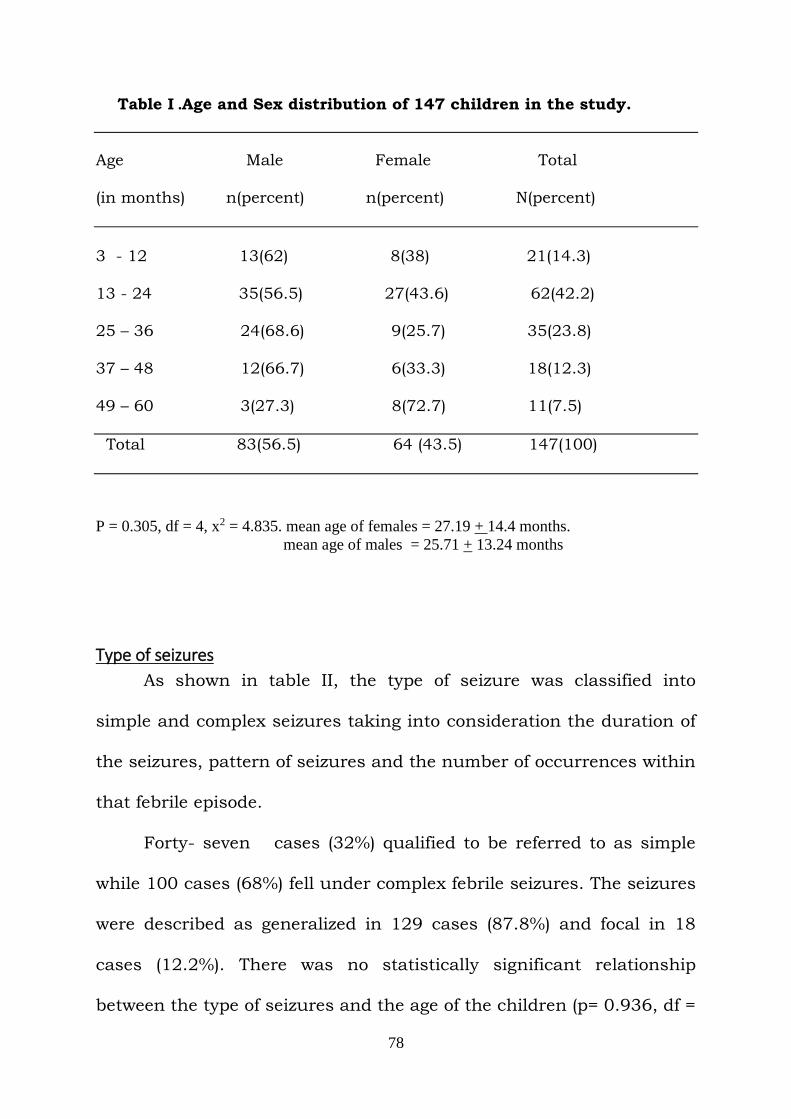
78
Table I .Age and Sex distribution of 147 children in the study.
Age Male Female Total
(in months) n(percent) n(percent) N(percent)
3 - 12 13(62) 8(38) 21(14.3)
13 - 24 35(56.5) 27(43.6) 62(42.2) 25 – 36 24(68.6) 9(25.7) 35(23.8)
37 – 48 12(66.7) 6(33.3) 18(12.3)
49 – 60 3(27.3) 8(72.7) 11(7.5)
Total 83(56.5) 64 (43.5) 147(100)
P = 0.305, df = 4, x2 = 4.835. mean age of females = 27.19 + 14.4 months.
mean age of males = 25.71 + 13.24 months
Type of seizures
As shown in table II, the type of seizure was classified into
simple and complex seizures taking into consideration the duration of
the seizures, pattern of seizures and the number of occurrences within
that febrile episode.
Forty- seven cases (32%) qualified to be referred to as simple
while 100 cases (68%) fell under complex febrile seizures. The seizures
were described as generalized in 129 cases (87.8%) and focal in 18
cases (12.2%). There was no statistically significant relationship
between the type of seizures and the age of the children (p= 0.936, df =
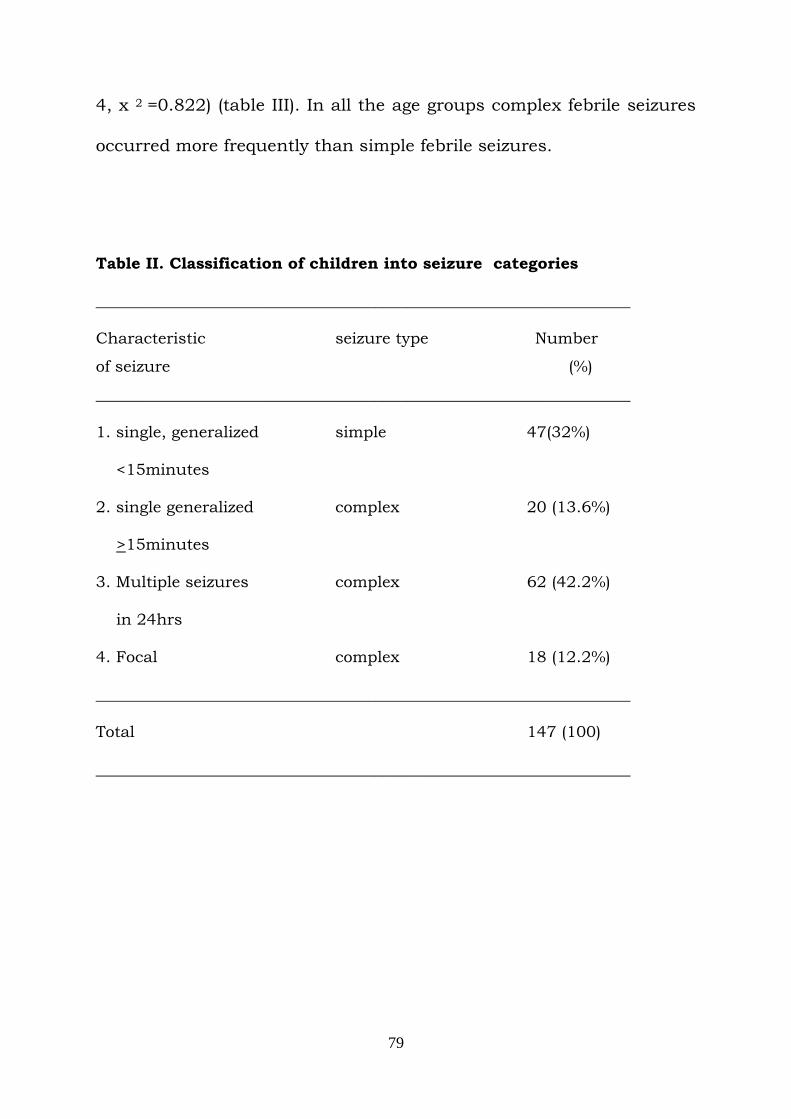
79
4, x 2 =0.822) (table III). In all the age groups complex febrile seizures
occurred more frequently than simple febrile seizures.
Table II. Classification of children into seizure categories
___________________________________________________________________
Characteristic seizure type Number
of seizure (%)
___________________________________________________________________
1. single, generalized simple 47(32%)
<15minutes
2. single generalized complex 20 (13.6%)
>15minutes
3. Multiple seizures complex 62 (42.2%)
in 24hrs
4. Focal complex 18 (12.2%)
___________________________________________________________________
Total 147 (100)
___________________________________________________________________

80
Table III: Type of seizures in relation to the age of children with febrile
seizures
___________________________________________________________________
Age in months Simple Complex Total
N(percent) N(percent) N(percent)
___________________________________________________________________
3- 12 8(38) 13(62) 21(14.3)
13- 24 18(29) 44(71) 62(42.2)
25- 36 12(34.3) 23(65.7) 35 (23.8)
37- 48 6(33.3) 12(66.7) 18(12.2)
49- 60 3(27.3) 8(72.7) 11(7.5)
__________________________________________________________________
Total 147(32) 100(68) 147(100.0)
P = 0.936, df = 4, x2 = 0.822.
Demographic Characteristics of the Parents
The socioeconomic status of the parents of the children in the
study is highlighted in Tables IV and V. The socioeconomic status of
the parents of these patients was determined using Oyedeji’s
method.119 Forty (27.2%) parents belonged to the upper class, 75(51%)
to the middle class and 32(21.8%) the lower socioeconomic class.
As shown in table IV, there was no statistically significant
difference in the type of seizure in relation to the socioeconomic class
of the parents.(p = o.658, df = 2, x2 = 0.838).
Table IV. The socioeconomic class of parents in relation to the type of

81
febrile seizures in the children of the study.
___________________________________________________________________
socioeconomic class simple complex Total
n (percent) n(percent) N(percent)
___________________________________________________________________
Upper 15(37.5) 25(62.5) 40(27.2)
Middle 23(30.7) 52(69.3) 75(51)
Lower 9(28.2) 23(71.9) 32(21.8)
___________________________________________________________________
Total 47(32) 100(68) 147(100)
___________________________________________________________________
p = 0.658, df = 2, x2 = 0.838.
Past Medical History and Family History
A family history of febrile seizure in a first degree relative was
obtained in 42(29%) cases of the 147 children studied. A history of
febrile seizures in one or more of their siblings was present in
23(15.7%) patients. Nine (6.1%) mothers knew that they had
convulsions in childhood, while 10(6.8%) fathers were similarly
affected.
A past history of febrile seizures was volunteered in 23(15.6%) of
the patients, most first recurrences occurred within a year of the first
episode in 17(74%); 16 had one previous episode, 3 had 2 episodes,
and 4 patients had 3 or more episodes. Age at first episode in the
82
children with recurrence varied from 3 months to 48 months. Twenty
(87%) of the 23 patients with recurrence in this study had their first
episode at age one year and above, with only 3(13%) being less than a
year at first episode. The mean age at first episode was 20.29 + 12.75
months compared with 27.4 + 15.4months obtained in the general
group. Only in one instance was a history of epilepsy in the family
obtained. Eight (34.8%) of the 23 patients with recurrent febrile
seizures had a family history of febrile seizures compared with
36(28.1%) of the 127 cases presenting with their first episode of febrile
seizure. The difference was not statistically significant (P value = 0.53,
X2 = 0.39). Nine of the 23 children (39%) had or were attending day
care centers.
Table V. The socioeconomic class of parents in relation to past
history of seizures in the children of the study

83
_______________________________________________________________
socioeconomic class recurrent non-recurrent Total(percent)
_______________________________________________________________
upper 7 33 40(27.2)
middle 10 65 75(51)
lower 6 26 32(21.8)
_______________________________________________________________
Total 23 124 147(100)
_______________________________________________________________
P= 0.726,df = 2, x2= 0.642
Predisposing Factors
Sixty-four (43.5%) of the children studied had attended or were
attending day care while nine (6.1%) were born preterm.
History of medication in pregnancy was obtained in 130(88%).
The medications included mostly haematinics (85%) like folic acid and
iron tablets and multivitamins. Four mothers had taken one form of
antibiotic or the other while none use of native concoction. History of
perinatal abnormalities was obtained in 19(12.9%) cases: 7 mothers
had antepartum haemorrhage, 1 had severe anaemia, 2 had breech
delivery and 6 caesarian section delivery.
Temperature
The temperature on admission or at the time of seizure varied in

84
the children studied. In 3(2%) children temperature at admission was
less than 37.5OC, 142(96.6%) had temperatures between 37.50C and
400C. Only two patients (2%) had temperatures above 40.00C. There
was no difference in the mean temperatures (38.30C) of the children
with recurrence and those without.
Pre-hospital intervention given
Out of the 147 patients studied only 59(40.1%) were given a pre-
hospital treatment of some sort after or during the seizure. (Tables VI
to IX). Fifteen (25.4%) out of the 59 gave native concoction. Nine
(15.3%) children had substances applied to the eyes. The substances
included salt, wine, onions, coconut oil, palm oil and metholatum.
One child had subsequent visual impairment. Three children (5%)
were subjected to burning of parts of the body e.g. both feet and
buttocks and one had to have plastic surgery done as a result of this.
One child had deep knife incisions inflicted on her face, feet and
trunk. Other forms of treatment given included application of things
like eucalyptus oil, palm oil, pepper, kerosene, lime and adiagbon
(coconut oil) to the body. The children to whom substances were given
by mouth also had the same substance rubbed on the body. None of
the children was tepid sponged or given any drug to stop the seizure
associated with fever.
Table VII shows that of the 59 parents who treated their children

85
at home, 9(15%) were in the upper class, 36(61%) were in the middle
class while 14(23.7%) were in the lower class. Seventeen percent of the
children in the upper class had pre-hospital intervention, 47% of the
76 in the middle class and 44% of the children in the lower class.
There was a statistically significant difference between the types of
pre-hospital intervention given in the different socioeconomic classes.
(p= 0.008,df = 8, X2 = 20.8). None of the children in the upper class
had native concoction.
Forty- seven of the 124 children with first febrile seizure versus
12 of the 23 with recurrent febrile seizures had pre-hospital
intervention. (P = 0.25,df = 1, X2 = 1.32) (Table VIII). There was no
statistically significant relationship in the type of seizure and the pre-
hospital intervention administered in the children (p= 0.981, df = 1, x2
= 0.002)(table IX).

86
Table VI. Pre-hospital management of 59 children with febrile seizures
___________________________________________________________________
Type of intervention Frequency Percent
___________________________________________________________________
1. Agents given by mouth
Native concoction 15 25.4
Salt and water 8 13.6
Milk 4 6.8
Anointing oil 2 3.4
Palm oil 1 1.7
Pepper 1 1.7
2. Agents rubbed into eyes
onions 3 5.1
metholatum 1 1.7
canel oil 1 1.7
palm oil 1 1.7
wine 1 1.7
salt 1 1.7
3. Burning of body 2 3.4
4. Cut to the body 3 5.1
5.water to the body 8 13.6
5. Others 7 11.9
___________________________________________________________________
Total 59 100
___________________________________________________________________

87
Table VII. Pre-hospital intervention in relation to the socioeconomic
class of the parents.
_________________________________________________________
Type of intervention upper middle lower total
___________________________________________________________________
Native concoction 0 7 8 15(10.2)
Other agents to drink 2 12 2 16(10.9)
B&C/S 2 10 1 13(22)
Others 5 7 3 15(10.2)
No intervention 30 40 18 88(60)
___________________________________________________________________
Total 39 76 32 147(100)
___________________________________________________________________
X2 = 20.8, P value =0.008,df = 8.
B&C/S = Burning and cutting of parts of the body or application of
substances to the eyes
others = kerosene, lime, adiagbon, eucalyptus oil and pepper

88
Table VIII. Pre-hospital intervention by mothers in relation to
recurrence of febrile seizures in children of the study
___________________________________________________________________
Intervention recurrence non-recurrent Total (percent)
__________________________________________________________________
Yes 12(20.3) 47(79.7) 59(40.1)
No 11(12.5) 77(52.4) 88(59.9)
___________________________________________________________________
Total 23(15.7) 124(84.4) 147(100)
___________________________________________________________________
p = 0.251, X2 = 1.32, df = 1)
Table IX. The type of pre-hospital intervention given by mothers in
relation to the type of seizures in the children with febrile seizures
__________________________________________________________________
Intervention simple complex total
N(percent) n(percent) n(percent)
__________________________________________________________________
Yes 19(32.2) 40(67.8) 59(40.1)
No 28(31.8) 60(68.2) 88(59.9)
_________________________________________________________________
Total 47(32) 100(68) 147(100)
_________________________________________________________________
( p = 0.981, X2 = 0.002, df = 1)

89
Aetiology of fever in children with febrile seizures
Tables X and XI show the causes of the fever that provoked
seizures in these children.. Malaria was responsible for 59(40.1%) of
the cases. Septicaemia was diagnosed in 22(15%) of the cases while
18(12.3%) had urinary tract infection. Twelve patients (8.2%) had
positive cultures of both blood and urine.
Two children with UTI were correctly identified and commenced
on antibiotics before culture results were obtained while three children
with septicaemia were correctly diagnosed clinically and commenced
on antibiotics before culture results were obtained.
The predominant organism isolated from the blood of these
patients was staphylococcus aureus found in 22(68.8%) of the 32
patients with positive blood culture. Other organisms were Salmonella
species 3(9.4%), Pseudomonas species 2(6.3%), unidentified gram-
negative bacilli 4(12.5%) and Klebsiella species in one (3%) patient.
The predominant organism isolated from the urine of these
children studied was Escherichia coli in 16 (53.3%) of the 30 children
with UTI; the other organisms were Klebisella species 8 (25%)
Staphylococcus aureus 3 (1%) and non- Haemolytic streptococcus 2
(6.7%). A patient had Candida albican infection (3.3%).
Table X. Relationship between the etiology of fever and age of the
children in the study.
_____________________________________________________________________

90
Etiology 3-12 13-24 25-36 37-48 49-60 total
_____________________________________________________________________
Malaria 7 26 14 9 3 59
Septicaemia 1 9 7 1 4 22
UTI 2 10 3 2 1 18
Pneumonia 3 6 1 2 0 12
Sept & UTI 3 3 4 1 1 12
Unknown 2 6 4 3 1 16
Others 3 2 2 0 1 8
_____________________________________________________________________
total 21 62 35 18 11 147
_____________________________________________________________________
(P = 0.79, df = 4, X2 = 18.265)
UTI = urinary tract infection
Sept & UTI = septicaemia & urinary tract infection
Others = measles, otitis media, gastroenteritis, typhoid enteritis and
tonsilopharyngitis
3 patients with pneumonia, 13 patients with septicaemia, 11 patients with
UTI and 7 patients with other infections also had malaria
The antibiotics that were sensitive to the organisms cultured
were mostly the cephalosporins like Ceftazidine and Cefuroxine and

91
also quinolones like ofloxacin, Ciprofloxacin and Sparfloxain. Amoxil
and genticin were also included in the drugs sensitive to the
organisms. Resistant drugs included Septrin, chloramphenicol and
tetracycline.
Pneumonia was diagnosed and confirmed by chest x-rays in
12(8.2%) children. Two children had clinical features in keeping with
measles. Two children presented with otalgia, ear discharge and
examination of the ear revealed pus in the middle ear and perforation
of the tympanic membrane. They both had positive ear swab cultures.
One child each was diagnosed with gastroenteritis and typhoid
enteritis. Two children had inflamed tonsils while in 16 (10.9%)
children the cause(s) of the fever could not be ascertained. There was
no statistically significant relationship between etiology of fever and
the age of the children (table X) (P = 0.79, df = 4, X2 = 18.265).
Malaria apart from occurring in some of the children alone it also
was seen in the children with other infections. Malaria was found in
13 of the cases of Septicaemia, 11 in the UTI cases, 3 in the
pneumonia cases and in 7 children with other infections. Table XI
shows the relationship between the etiology of fever and the type of
febrile seizures. Complex febrile seizure was more frequently seen in
all the etiological groups. Only one of the 18 children with UTI had
simple febrile seizures (0.1>p > 0.05). There was no statistically
significant difference in the type of seizure in relation to the degree of

92
parasitaemia (p= 0.089,
df = 2, x2 = 4.835)(table XII).
Twenty-five children had one plus of malaria parasitaemia, 11
had 2 pluses, 13 had 3 pluses while 10 had 4 pluses amongst the 54
with malaria only. There was no statistically significant relationship
between the degree of malaria parasitaemia and the type of seizure
(table XII) (P = 0.115, df = 2, x2 = 4.319).
There was no statistically significant difference in the aetiology of
fever among the different socioeconomic class (p = 0.50, df = 12, x2 =
11.37), and the type of pre-hospital intervention offered these children
(p = 0.10, df = 18, x2 = 5.86).
Table XI. Relationship between aetiology of fever and the pattern
of febrile seizures
_______________________________________________________________

93
Aetiology of fever simple complex total
(percent) (percent) (percent)
_______________________________________________________________
Malaria 24(40.7) 35(59.3) 59(40.1)
Septicaemia 7(31.8) 15(68.2) 22(15)
UTI 1(5.6) 17(94.4) 18(12.3)
Pneumonia 6(50) 6(50) 12(8.1)
Septicaemia
And UTI 4(33.3) 8(66.7) 12(8.1)
Unknown 3(18.8) 13(81.2) 16(10.9)
Others 2(25) 6(75) 8(5.4)
_______________________________________________________________
Total 47(32) 100(68) 147(100)
_______________________________________________________________
p = 0.082, df = 6, x2 = 11.212
Others = measles, otitis media, gastroenteritis, typhoid enteritis and
tonsilopharyngitis
3 patients with pneumonia, 13 patients with septicaemia, 11 patients with
UTI and 7 patients with other infections also had malaria.
Table XII. The degree of parasistaemia in relation to the type of
seizure in the children in the study.
_______________________________________________________________

94
degree of parasitaemia complex simple total
(percent) (percent) (percent)
_______________________________________________________________
< ++ 23(63.9) 13(36.1) 36(61.1)
> +++ 12(52.2) 11(47.8) 23(38.9)
_______________________________________________________________
total 35(59.3) 24(40.7) 59(100)
_______________________________________________________________
p = 0.115, df = 2, x2 = 4.317.
Packed cell volume
Table XIII shows the PCV values in the patients studied. The
mean PCV was 25.3 + 9.4 %. Anaemia was present in 89 patients
(61%), with 30 of them having a PCV of < 15% and 52 (35.4%) of the
patients having severe anaemia.
The least PCV was 8% while the highest value was 49%. There
was no relationship between the packed cell volume and the pattern of
seizures, socioeconomic status and the degree of parasitaemia. There
was no statistically significant difference in the packed cell volume in
the children with malaria (p = 0.55, df = 16, X 2 = 14.63). There was
however a statistically significant relationship in the PCV and the
etiology of fever in these patients(p = 0.01, df = 6, x2 = 16.81)(tableXIV)

95
Table XIII. Packed cell volume values in 147 children with febrile
seizures
_______________________________________________________________
PCV No of cases Percent
(percent)
_______________________________________________________________
<15 30 20.7
15 – 20 22 15
21 – 25 14 9.5
26 – 30 30 20.4
> 30 51 34.7
_______________________________________________________________
total 147 100
_______________________________________________________________
PCV = Packed cell volume
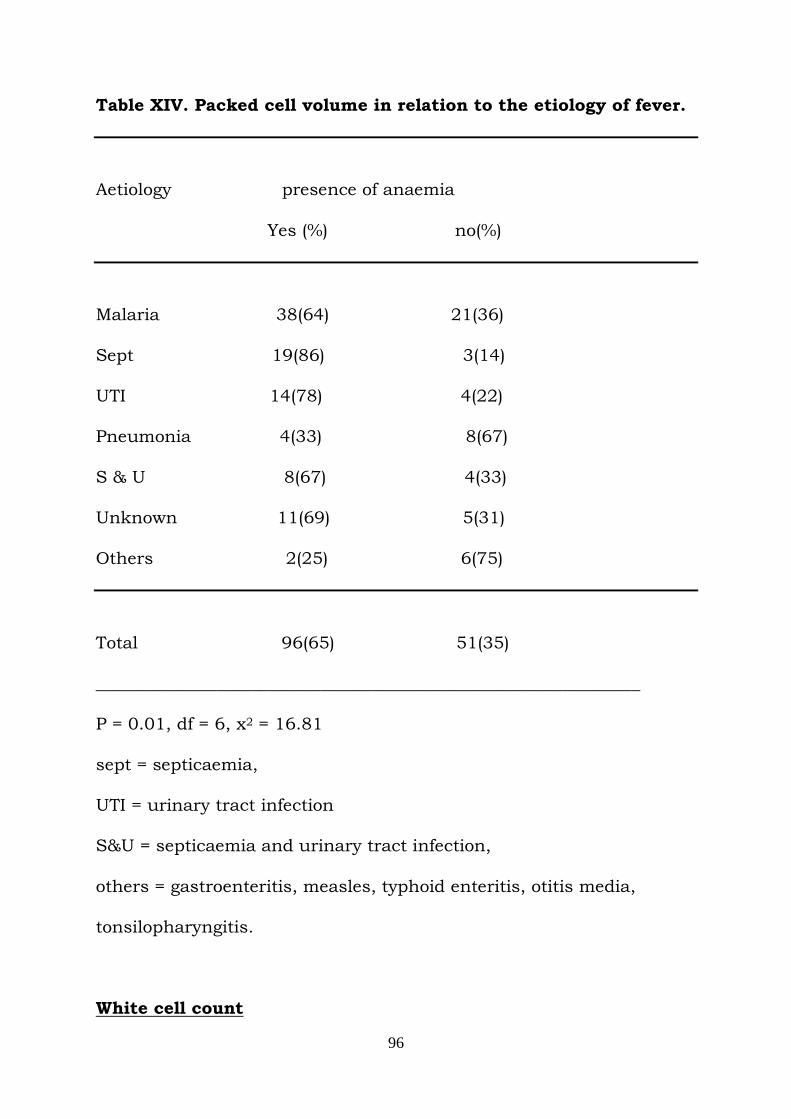
96
Table XIV. Packed cell volume in relation to the etiology of fever.
Aetiology presence of anaemia
Yes (%) no(%)
Malaria 38(64) 21(36)
Sept 19(86) 3(14)
UTI 14(78) 4(22)
Pneumonia 4(33) 8(67)
S & U 8(67) 4(33)
Unknown 11(69) 5(31)
Others 2(25) 6(75)
Total 96(65) 51(35)
_______________________________________________________________
P = 0.01, df = 6, x2 = 16.81
sept = septicaemia,
UTI = urinary tract infection
S&U = septicaemia and urinary tract infection,
others = gastroenteritis, measles, typhoid enteritis, otitis media,
tonsilopharyngitis.
White cell count

97
Table XV shows the white blood cell count in relation to the aetiology
of fever. Normal levels were found in 83(56.5%) of the children. There
was no statistically significant difference in the white cell count
amongst the different aetiological groups.
(p = 4.81, df = 18, x2 = 17.62).
Table XV. The white blood cell counts in relation to the etiology

98
of fever in 147 children with febrile seizures
_______________________________________________________________
WBC mal sept uti pneu s&u others un total
_______________________________________________________________
a 18 5 6 3 1 4 3 40
b 28 15 10 8 8 3 11 83
c 12 1 1 0 3 1 1 19
d 1 1 1 1 0 0 1 5
_______________________________________________________________
Total 59 22 18 12 12 8 16 147
_______________________________________________________________
p = 4.81, df = 18, x2 = 17.62
a = <5,000/mm3
b = 5,000 – 10,000/mm3
c = > 10,000 - < 15,000/mm3
d = > 15,000/mm3

99
Cerebro-spinal fluid
Tables XVI to XVII give details of the CSF findings in the patients
studied. The CSF protein was <10mg/100mls in 24.5% of the children,
while the highest value was 45mg/100mls seen in 2 patients. The CSF
protein mean and SD value was 23.98 + 0.774 mg/100mls.
The CSF sugar mean and SD value was 65.84 +
29.28mg/100ml. In 11 patients CSF sugar was less than
40mg/100ml.
The mean (SD) RBS was 97.42 + 36.38 mg/100ml. The RBS was
< 40mg/100mls in 4 children while 28 patients had RBS >
120mg/100mls. In every case, including the cases of hypoglycemia,
the CSF sugar was 50% or more of the blood sugar. The cellular
contents of the CSF were within normal limits in all the children
studied. There was no statistically significant relationship between the
CSF sugar levels, aetiology of fever and the pre-hospital intervention
given in the children studied (p = 0.686, df = 12, x2 = 9.202) (table
XVI). (p = 0.23, df = 6, x2 = 8.07) There was no statistically significant
relationship between the CSF protein and the aetiology of fever in the
children studied (p = 0.7, df = 12, x2 = 19.503)(table XVII).
There was no statistically significant relationship between the
CSF protein, CSF sugar and the pattern of seizures. (p = 0.339, df = 2,
x2 = 2.162) (p = 0.606, df = 2, x2 = 1.003).

100
In the 10 children with hypoglycorhachia 2 had simple febrile
seizures while the others (10) had complex febrile seizures. Four of
them had malaria, 1 had Septicaemia,3 had UTI, 1 had both positive
blood and urine cultures while 1 had pneumonia. The 2 children with
hypoglycemia had complex febrile seizure and fever was caused by
malaria and UTI respectively.
Table XVI. Cerebrospinal fluid sugar in relation to the aetiology of
fever in the children studied.

101
_____________________________________________________________________
CSF sugar mal sept pneu uti s&u others un total
_____________________________________________________________________
< 40 3 4 1 1 1 0 1 11
40 – 80 38 14 7 13 9 4 12 97
> 80 18 4 4 4 2 4 3 39
_____________________________________________________________________
Total 59 22 12 18 12 8 16 147
_____________________________________________________________________
p = 0.686, df = 12, x2 = 9.202
sept = septicaemia,
UTI = urinary tract infection
S&U = septicaemia and urinary tract infection
Mal = malaria
Pneu = pneumonia
Un = unknown
Others = gastroenteritis, measles, typhoid enteritis, otitis media,
tonsillopharyngitis.
Table XVII. Cerebrospinal fluid protein in relation to the aetiology
of fever in the children studied.

102
_____________________________________________________________________
CSF protein mal sept pneu uti s&u un others total
_____________________________________________________________________
<10 13 5 1 2 4 8 3 36
10 – 40 46 17 11 16 8 7 5 110
41 – 80 0 0 0 0 0 1 0 1
_____________________________________________________________________
Total 59 22 12 18 12 16 8 147
_____________________________________________________________________
p = 0.077, df = 12, x2 = 19.503
sept = septicaemia,
UTI = urinary tract infection
S&U = septicaemia and urinary tract infection
Mal = malaria
Pneu = pneumonia
Un = unknown
Others = gastroenteritis, measles, typhoid enteritis, otitis media,
tonsillopharyngitis.
Outcome
Duration of hospital stay
The duration of hospital stay ranged from 24hrs to 90 days. The
mean duration (SD) of stay was 6.37 + 8.067 days. Forty-four (29.9%)
103
were discharged within 72 hours of admission, 71 (48.3%) after a
period of 4 – 7 days while 2 (1.3%) stayed for a period of more than 4
weeks.
Majority (75%) of the patients with malaria stayed for less than a
week. None stayed beyond 2 weeks. Patients with bacterial infection
spent a longer period in the hospital as compared to patients with
malaria.
Neurological deficit
At the time of discharge persisting neurological deficits were seen
in 6 of the 145 survivors. Four of them had generalized hypertonia
while 2 children each had 6th and 7th cranial nerve palsies. Five of the
children presented with complex febrile seizures while one had simple
febrile seizures.
There was no statistically significant relationship between the
occurrences neurological deficits pre-hospital intervention and the
etiology of fever. (P = 0,0602, df = 6, x2 = 523).
Mortality amongst the 147 patients with febrile seizures
Two patients died giving a case fatality of 1.4%. One was a 30-
month-old child with severe malaria who had greater than 10
parasites per high power field and also had severe anaemia. He had

104
blood transfusion and antimalarial therapy administered, but died
after 5 days of admission. The other child was a 5-year-old child with
typhoid perforation who died 4 days after surgery. None of the deaths
could be directly attributed to febrile seizures.
105
DISCUSSION
Febrile seizures remain one of the commonest emergencies in
Nigeria.116 – 119 The prevalence rate of 9.9% obtained in this present
study is lower than that obtained by famulusi et al2 in the same centre
over 30 years ago. It is also lower than figures obtained by Izuora and
Azubuike13 of 15.6% in Enugu. It is however higher than what was
obtained in Jos by Angyo18 and in Benin by Scott-Emuakpor et al12
where a prevalence of 5.8% was reported.
Though there seems to be an improvement by the reduced
prevalence, the figures are still higher than what is obtained in
developed countries.
Our poor environmental hygiene makes a young child infection
prone. Poor health care delivery system in the midst of economic
instability limits availability, accessibility and affordability of health
services as well as prompt diagnosis and management of fever and
this may contribute to higher prevalence. The sociocultural habits and
beliefs can contribute immersely to the high prevalence rate of febrile
seizures.11
While dealing with children with fever and seizures who are
under 6 months and above 5 years it is particularly necessary to rule
out meningitis in them because there is a greater risk of mistaking
serious illness such as pyogenic meningitis for febrile seizures in this
age group. Onset of febrile seizures before the age of 6 months is
106
uncommon as evident in this study as only 2 children were less than 6
months old. The age distribution in the present study is similar to that
reported by previous workers.2,4,14,18
This study showed only a slight male preponderance with a male
to female ratio of 1.3:1. This is similar to previous reports.2,4 In Jos
Angyo18 however obtained a male: female of 2:1.
In this study complex febrile seizures occurred more commonly
than simple febrile seizures with a ratio of 2.2: 1. This agrees with the
report of Akpede et al47 but at variance with what is reported in
literature including previous reports from Nigeria.4,14,64 Berg et al3
reported 35% of complex febrile seizures amongst first febrile seizure
children and 41.2% complex febrile seizures amongst children with
recurrent febrile seizures in a study in New York. Poor reckoning of
the duration can lead to wrong diagnosis of complex febrile seizures.
A convulsing child presents an alarming picture and onlookers
very often exaggerate the duration of the seizure.
The author in interviewing the caregivers of the patients in the study
took particular care in trying to obtain reasonable estimates of the
duration of the seizure. In spite of this, it is possible that a number of
children were wrongly classified as having complex febrile seizures
based on the duration of seizures. It is notable though that only 14 of
the seizures were classified as complex based solely on the prolonged
duration of a single generalized seizure.

107
Another possible explanation for the predominance of complex
febrile seizures is the fact that this is a hospital-based study. It is
more likely that a child who has had a prolonged or multiple seizures
would be rushed the hospital than the child who has had a single brief
attack. This will tend to exaggerate the proportion of complex febrile
seizures among hospital patients when compared with its occurrence
in the general population.
A family history of febrile seizures in the first-degree relatives of
29% is higher than what was obtained at this centre in previous
reports.2, 119 Osuntokun et al119 reported 3.9%, while Familusi et al2
reported 18.1% prevalence of positive family history of febrile seizures
in Ibadan. Reports from Shagamu118 and Ilesha14 were 12.3% and
43.5% respectively. Livingstone120 reported a prevalence of 58% while
Lennox121 in America, reported a rate of 45%. Positive history is
defined primarily by parental recollection and willingness to disclose
information. Low figures obtained in previous studies in this center
could be attributed to denial as a result of social stigma attached to
convulsions in this part of the world. The result of the present study
suggests increased level of parental education and enlightenment as
compared to the past, as the rate of disclosure by the informant
reflects.
It has been reported that most recurrences occur within
6 – 12 month of the initial seizure.7 The finding in this study is in

108
keeping with this. Twenty-three (15.6%) of the patients studied had a
history of recurrence, 17(74%) had the 2nd episode within a year of the
first. It has been reported that the risk of recurrence is influenced by
the age of the patient at the time of the first seizure.92, 95 This is not
supported by the results of this study. The results also do not support
literature reports of family history as a risk factor for recurrence.
The aetiology of the fever causing febrile seizures in the children
studied bears several similarities to what has been previously
documented in our area.2, 4, 18 Malaria plays a significant role in febrile
seizures in this geographical area.4 The role of malaria in these
children is in keeping with past observations that malaria is the
commonest cause of fever in children in the tropics.47 The 40.1%
prevalence of malaria in the study is similar to the prevalence of
45.2% earlier reported in Ibadan,2 but lower than the prevalence of
71.2% and 74.8% reported in Ilorin4 and Jos 18 respectively. It’s
however surprising that a higher prevalence of malaria is reported in
the middle belt.
The policy of malaria control should be maintained. If malaria
could be properly controlled the incidence of febrile seizures will be
reduced.
The finding in this report supports previous reports about the
possible co-existence of malaria with other infections.47,54
Community acquired bacteria is an important problem in the

109
tropics.47 Septicaemia was the 2nd commonest cause of fever in this
study and it was responsible for 15% of the causes of fever. The
predominant organism isolated was staphylococcus aureus (68.8%).
The results are in keeping with some previous reports, 53,54 but at
variance with some other reports. 2,18,51,52
Akpede et al47, 54 reported incidence of bacterial infections in
children of 9% and 11% in 2 different studies done in Nigeria.
Lepage53 reported an incidence of 12.4% among Rwanda children.
Familusi et al2 and Angyo et al18 reported bactiraemia in 3.3% and
3.7% respectively in the children they studied while James et al70
reported 5.4% and Teah et al52 a 2.9% incidence. James and Teah’s
studies were retrospective and not all the children studied had blood
culture, Familusi et al2 and Angyo et al18 studies were prospective
however not all the children studied had blood culture.
Bacteraemia in young children is a reasonably frequent
occurrence with occasionally serious sequelae; most patients however,
do quite well. The problem is more perplexing in infants and young
children with high fever and no focus.122
A history of febrile seizures should not dissuade an emergency
room physician from performing a blood culture.70 In a study by
James et al70 2 of the 5 patients with bacteraemia had had febrile
seizures. Documentation of parasitaemia does not exclude other

110
infections but can be misleading in sick child, this is confirmed in this
present study. Other reports53, 54 have highlighted the problems of
concurrent infections, including bacteraemia in children with malaria.
In an endemic area for malaria like Nigeria, febrile children should be
investigated for the presence of bacteraemia and other infections even
with a positive malaria parasitaemia.
Septicaemia is a serious infection, which can lead to multiple
complications and even death. Therefore the possibility of this
diagnosis should be kept in mind when managing a child with febrile
seizures.
Urinary tract infection was the 3rd commonest aetiological factor
found in this study. It accounted for 12.3% of the cases. The finding in
this study is similar to that of James et al70 and Ibadin et al58 in which
incidences of 17% and 9% were reported respectively, but were at
variance with other reports.2, 18,52,60 The difference may be related to
differences in methodologies. This study was prospective whereas
others52, 60 were not. All the patients in this study had a urine culture
whereas not all the patients in these other studies did.2, 18,51,60
Pneumonia was responsible for fever in 8.2% of the children
studied rating as the fourth commonest cause of fever in the study.
Only 2 children had Upper respiratory tract infection (URTI). This is at
variance with what obtained in previous reports2, 4,18 which had higher
incidences.

111
Viral agents account for a large proportion of fever causing
febrile seizures in temperate regions. The role of viruses in this study
will remain undetermined since viral studies were not done. It would,
however, have been very informative to compare the results of viral
studies with Familusi et al’s2 finding of virus isolates in 14(13.3%) of
the 105 patients with febrile seizures. This is an area for further
research.
The problem of multiple infections in children is highlighted in
this study and this could make assessment and management of these
children very challenging for the Paediatrician.
The role of predisposing factors in febrile seizures could not be
fully assessed in this study because there were no controls to compare
with. However, the fact that 64(43.5%) of the children were attending
daycare might be a pointer to its contribution to the disease. Nineteen
(12.9%) children had perinatal abnormalities in the study. This
supports the finding of Wallace42 but not that of CHES19 and Zhao.46
Pre-hospital intervention was given to 59(40.1%) children. Eight-
eight (59.9%) of the parents did not administer anything harmful but
rather brought the children straight to the hospital. This is
comparable with the report by Familusi et al2 where 60% did not give
any form of harmful intervention. Native concoction was administered
to 10.2% of the children studied. This is considerably lower than the
52.4% reported by Familusi et al2 in the same hospital in 1971. Also

112
2.7% children had parts of their body burnt or knife incisions made on
them compared with 7.8% in Familusi’s study. The difference between
the 2 studies could be a reflection of the degree to which health
education has been able to impact on the use of harmful measures by
people when managing febrile seizures. Native concoction are popular
remedies used all over the country for the treatment of febrile seizures.
This is shown by reports from other parts of Nigeria.2,4,12,18 It is
important to educate caregivers when they present at the health
centre because some of them are rather fixed in their ways handling
situations. They need to be enlightened on the dangers of persisting in
such practices for example, risk of infections, gangrene, neurological
sequelae and even death.
This study showed that socioeconomic status influenced the type
of pre-hospital intervention administered. None of the parents in the
Upper class gave native concoction, majority (76.9%) of them took
their children to the Hospital. Mothers contribute a good target group
for specific health education.
There was a relationship between the duration of hospital stay
and the aetiology of fever causing febrile seizures. Majority of the
children with malaria stayed for less than a week. This is expected
since malaria is usually effectively treated in three to seven days.
However, children with Septicaemia, UTI, and other bacterial and
mixed infections are usually admitted for several days of intravenous

113
antibiotics. This was similar to what was reported in other studies.18
Various neurological complications of febrile seizures have been
reported from Nigeria. Familusi et al2 and Angyo et al18 reported
neurological complications in 8.3% and 1.8% respectively while
Imuekheme17 reported a rate of 12.5%. However, in this present study,
only six children (4%) had neurological deficits. This is within the
reported range of 1.8 – 12.5%. 2,17,18
The finding of 28(19%) patients with hyperglycemia is not
unusual and agrees with previous reports.124 Seizure is known to
produce an increase in circulating levels of both cortisol and
adrenaline and these raise the blood sugar by their anti- insulin
action.124 Only four (2.7%) of our patients had hypoglycemia, whereas
Familusi et al2 reported 13% prevalence. The occurrence of
hypoglycemia could have been as a result of anorexia or vomiting
preventing feeding which could usually follow some childhood illnesses
especially malaria.
Severe anaemia (< 20%) was present in 35.4%) of the patients.
This could be related to the high incidence of malaria plus the problem
of malnutrition. It also agrees with previous reports.2,4
The children with septicaemia were more likely to have anaemia
in this study so also were the children with urinary tract infections.
This could also have been as a result of the co – existence of malaria
with these infections.

114
The case fatality rate of 1.4% in this study is comparable to that
reported by Angyo et al18, Oseni14 and fagbule4, however, it is at
variance with the 6.4% reported by Familusi et al2 and the 9.2% by
Ejeheri.125 The report is in conformity with several reports from
developed countries like USA.126,127
Febrile seizures are generally considered benign with a
favourable outcome.128, 129 In our environment certain adverse factors
combine to bring about poor outcome. The administration of native
concoction to convulsing children is a common practice associated
with poor outcome. This is responsible for most of the deaths, which
occurred, in the previous study at our centre.2 All the 4 children that
died in Fagbule’s study4 also had native concoction administered. The
use of these concoction must be rigorously discouraged through
health education.
115
CONCLUSIONS
1) The prevalence of febrile seizures among children admitted to the
Children’s Emergency Ward of UCH, Ibadan has declined to
9.9% from 15.1% about 3 decades ago.
2) Complex febrile seizure is the predominant type of febrile seizure
in children presenting to the UCH.
3) Malaria is the commonest cause of febrile seizures in children
presenting to the UCH, but Septicaemia, Urinary Tract infection
and Pneumonia are also important causes.
4) Significantly fewer people are now administering native
concoctions to children with febrile seizures, when compared
with 30 years ago.
5) Socioeconomic status has an effect on the type of pre-hospital
management given to children with febrile seizures.
6) The mortality and neurologic sequelae rates in children with
febrile seizures at the UCH has declined considerably
since 30 years ago.
7) The low incidence of adverse neurological outcome and mortality
could be related to the less frequent use of native concoctions in
the home management of the disease.
8) The presence of bacterial or other infections does not rule out
malaria infection in children.

116
RECOMMENDATIONS
1) The general public especially mothers need to be educated on
the correct attitude to febrile seizures and appropriate
management of the convulsing child.
2) Malaria control in this environment should be intensified,
especially the recognition of symptoms and early treatment at
home.
3) Bacteraemia and UTI oftentimes present with non-specific
manifestations and a high index of suspicion is required in
diagnosis.
117
LIMITATIONS OF STUDY
1) Viral studies were not done as part of the search for aetiology of
the fever in these children because of financial constraints.

118

119
REFERENCES
1. Verity CM. Febrile convulsions. In Hopkins A, Shovon S,
Casino G (eds) Epilepsy. London; Chapman and Hall
[Publisher] 1995: 355-68.
2. Familusi JB, Sinnette CH. Febrile convulsion in Ibadan
Children. Afr J Med Sci 1971; 2: 135-49.
3. Berg AT, Shinnar S. Complex Febrile Seizures. Epilepsia
1996; 2: 126-33.
4. Fagbule D, Chike-Obi UD, Akintunde EA. Febrile
convulsions in Ilorin. Nig J Paediatr. 1991; 18: 23-7.
5. Parmer RC, Sahu DR, Bavdekar SB. Knowledge, attitudes
and practices of parents of children with febrile convulsions.
J Postgrad Med. 2001; 47: 19-23.
6. Chesney RW. Febrile seizures. In Behrman RE, Khegman RM,
Arvin AM (eds). Nelson Text book of Paediatrics. Philadelphia,
WB Saunders Company (publishers). 2000; 1818-9.
7. Update on febrile seizures Paediatrics database.
www.icondata.com/health/pedbase/files/febriles.HTM-7k.
8. Annegers JF, Hausa WA, Elveback LR, Kurland LT. The risk
of epilepsy following febrile convulsions. Neurol 1979; 29:
297-303.
9. Nelson KB, Ellenberg JH. Prognosis in children with febrile
seizures. Paediatrics 1978; 61: 720-7.

120
10. Wolf SM. Laboratory evaluation of the child with a febrile
convulsion. Paediatrics 1978; 62: 1074 - 6.
11. Iloeje SO. The impact of sociocultural factors in febrile
convulsions in Nigeria. Afr J Med. 1989; 8: 54-8.
12. Scott-Emuakpor AB, Longe AC. Some aspects of the genetics
of febrile convulsions. Nig J Paediatr 1985; 12:49-55.
13. Izuora GI, Azubuike JC. Prevalence of seizure disorders in
Nigerian children around Enugu. Afr Med J 1977; 54:276-80.
14. Oseni SBA. Febrile seizures in Wesley Guild Hospital Ilesha.
A study of the pattern and some of the associated factors.
Dissertation 1997. (National Postgraduate Medical College)
15. Iloeje SO. Febrile convulsions in a rural and an urban
population of Anambra State of Nigeria. Dissertation 1984.
(National Postgraduate Medical College).
16. Akpede GO, Sykes RM, Abiodun PO. Indications for lumbar
puncture in children presenting with convulsions and fever of
acute onset experience in the children emergency room of the
University of Benin Teaching Hospital Nigeria. Ann Trop
Paediatr 1992; 12: 385-9.
17. Imuekheme SO. Serum and cerebrospinal fluid copper and
zinc levels in children with febrile seizures seen in University
of Benin Teaching Hospital. Dissertation 1987. (National
Postgraduate Medical College).

121
18. Angyo IA, Lawson JO, Okpeh ES. Febrile convulsions in Jos.
Nig J Paediatr 1997; 24: 7- 13.
19. Consensus Development Conference of Febrile Seizures by the
National Institute of Health. Febrile seizures: long term
management of children with fever-associated seizures.
Paediatrics 1980; 6:1009.
20. Joint Working Group of the Research Unit of the Royal
College of Physicians and the British Paediatric associations.
Guidelines for the management of convulsions with fever.
Brit Med J 1991; 303: 634-6.
21. Wallace SJ. Seizures in children. In Laidlaw J, Richens A,
Chadwick D (eds). A textbook of epilepsy. Edinburgh,
Churchill Livingstone [publishers]. 1993; 96-107.
22. Nealis JGT, Rosman NP, de Piero TJ, Quellette EM.
Neurological sequelae of experimental febrile seizures. Neurol
1978; 28: 246-50.
23. Provisional Committee on Quality Improvement
Subcommittee of Febrile Seizures. Practice parameter: The
neurodiagnostic evaluation of the child with a first simple
febrile seizure. Paediatrics 1996; 97: 769-72.
24. Aicardi J. Epilepsy. In Forfar JO, Arneil GS (eds). Textbook of
Paediatrics. Edinburgh London. Melboune. New York
Churchill Livingstone (publishers). 1984; 677-893.

122
25. Costeff H. Convulsions in childhood: their natural history and
indications for treatment. N Engl J Med 1968; 273: 1410-3.
26. Webb JKG. Convulsive disorders in childhood. Indian J
Pediatrics 1955; 22: 18-28.
27. Nakayama J, Klamano K, Iwaseki N. Significant evidence for
linkage of febrile seizures to chromosome 5q 14-q15. Human
Mole Genet 2000; 9: 87-91.
28. Joffe A, McCormick M, De Angelis C. Which children with
febrile seizures need lumbar puncture? Am J Dis Child 1983;
137: 1153-6.
29. Evans HE. Pathogenesis of fever In Begrman RE, Kliegman
RM, Arvis AM. (eds). Nelson textbook of Paediatrics. (14th
Edition). Philadelphia, W.B Saunders Company (publishers).
1490-6.
30. Stvrtinova V, Jakubovsky J, Hulin I. Inflammation and fever.
Pathophysiologic principles of diseases. Academic Electronic
Press (publishers). 1995;1-113.
31. Rosman NP. Evaluation of the child who convulses with fever.
Paediatr Drugs 2003; 5: 457-61.
32. Kesting NW, Veale WL, Cooper KE. Vasopressin may mediate
febrile convulsions. Brain Res 1981; 213: 327-33.
33. Lennox-Buchthal MA. Febrile convulsions. In Laidlaw J &
Richens A (eds). A Textbook of Epilepsy. Edinburgh London

123
Melbourne Newyork. Churchill Livingstone (publishers) 1982;
68-88.
34. Knight M, Ebert J, Parish RA, Berry H, Fogelson MH.
Gamma aminobutyric acid in CSF of children with febrile
seizures. Arch Neurol 1985; 42:474-5.
35. Loscher W, Siemens H. Increased concentration of PGE2 in
CSF of children with febrile convulsion. Epilepsia 1988; 29:
307-10.
36. Pedder SC, Wilcox RI, Tiche KJM, Johnson DD, Crawford RD.
Attenuation of febrile seizures in epileptic chicks by N methyl
- D-asparate receptors antagonist. Can J Physiol Pharmacol
1990; 68:84-8.
37. Takayuki T. Genetic aspects of febrile convulsions. Hum
Genet 1977; 38: 169-73.
38. Eric WJ, Dubovsky J, Stephen SR, Cormac A. Evidence for a
novel gene for familial febrile convulsions FBB2, linked to
chromosome l9p in an extended family from the Midwest.
Hum Mole Genet. 1998; 7: 63-7.
39. Pieffer A, Thompson J, Charlier C et al. Locus of febrile
seizures [FEB3] maps to chromosome 2q 23-24. Ann of
Neurol 1999; 46: 671-8.
40. Tsuboi T, Okada S. Seasonal variation of febrile seizures in
Japan. Acta Neurol Scad 1984; 69:282-92.

124
41. Cassario PA, Koepsal D, Farwell JR. Risk of febrile seizures in
childhood in relation to prenatal maternal cigarette smoking
and maternal alcohol intake. Am J Epidemiol.1990; 132:462
–73.
42. Wallace SJ. Aetiological aspects of febrile convulsions.
Archives of Disease in Childhood. 1972; 47: 171-8.
43. Wallace SJ. Recurrence of febrile convulsions. Arch Dis Child
1974; 49: 763-5.
44. Lennox MA. Febrile convulsions in childhood: their relationship
to adult epilepsy. J Paediatr 1949; 35:427-35.
45. Verity CM, Butler NR, Golding J. Febrile convulsions in a
National Cohort followed up from birth II. Medical history and
intellectual ability at five years of age. Brit Med J. 1985;
290: 1311-5.
46. Zhao F, Emoto SE, Lavinal. Risk factors for febrile seizures in
the peoples Republic of China: a case Control Study.
Epilepsia 1991; 32: 510-4.
47. Akpede GO, Abiodun PO, Sykes RM. Relative contribution of
Bacteraemia and Malaria to acute fever without localizing
signs of infection in under-five children. J of Trop Paediatr
1992; 38:295- 8.
48. World Health Organization. Roll back malaria Advocacy
guide. Switzerland 2000.

125
49. World Health Organization. The African summit of roll back
malaria, Abuja. 2000.
50. Lewis HA, Parry JV, Parry RP, Davies H, Sanderson J, Tyrrel
D, Valman H. Role of viruses in febrile seizures. Arch Dis
Child. 1979; 54:869-76.
51. Mc Intyre PB, Gray SV, Vance C. Unsuspected bacteraemia
infections in febrile seizures. Med J Austr 1990; 152: 183-6.
52. Teah SJ, Geil PA. Incidence of bacteraemia, UTI and
unsuspected bacterial meningitis in children with febrile
seizures. Paediatr Emer Care 1999; 15:9- 12.
53. Lepage P, Bogoerts J, Ntaharatab M et al. Community-
acquired bacteraemia in African children. The Lancet 1987;
1458- 61.
54. Akpede GO, Sykes RM. Malaria with bacteraemia in acutely
febrile preschool children without localizing signs:
Coincidence or association/complication? . J of Trop Med
Hygiene 1993; 96:146- 50.
55. Mc Carthy PL, Grundy GW, Spiesel SZ et al. Bacteremia in
children: An outpatient clinical review. Paediatr 1976;
57:861- 7.
56. Teele DW, Marshall R, Klein JO. Unsuspected bacteraemia in
young children, A common and important problem. Paediatr
Clinic of North America 1979; 26: 773-83.

126
57. Hendrickse RG, Hasan AH, Olumide LO, Akinkunmi
A.Malaria in early childhood. Annals Trop Med Parasitology
1971; 654: 1 – 19.
58. Musa-Aisien AS, Ibadin OM, Udoh G, Akpede GO. Prevalence
and microbial sensitivity pattern in UTI in febrile under-fives
at a children’s emergency unit in Nigeria. Ann Trop Paed
2003; 23: 39 – 45.
59. Jeena PM, Coovadia HM, Adhikari MA. Bacteraemia in
children attending a Primary Health care clinic: prospective
study of catheter stream urine samples. Ann Trop Paediatr
1996; 16: 293 – 8.
60. Trainer JL, Hampers LC, Krug SE, Listernick R. Children
with first time simple febrile seizures are at low risk of
serious bacterial illness. Acad Emer Med 2001; 8: 781 -7.
61. Lee P, Verrier JK. UTI in febrile convulsions. Arch Dis
Child.1991; 66: 1287-90.
62. Hirtz DG. Nelson KB, Ellenberg JH. Seizures following
childhood Immunization. J Paediatr 1983; 102:14-8.
63. Cody CL, Baraff LJ, Cherry JD, Marcy SM, Manclark CR.
Nature and rates of adverse reactions associated with DTP
and DT immunizations in infants and children. Paediatr
1981; 68: 650 – 8.

127
64. Laditan AAO. Analysis of the results of routine lumbar
puncture after a first febrile convulsion in Hofuf AI- Hassa,
Saudi Arabia. East Afr Med J 1995; 376-8.
65. Rateliffe JC, Wolf SM. Febrile convulsion caused by
meningitis in young children. Ann Neurol 1977; 1:285.
66. Finley AH. Lumbar puncture in children who have had fever
and convulsion. Lancet 1980; 2: 83. (Letter)
67. Rutter N, Smales QRC. Role of routine investigations in
children presenting with their first febrile convulsions. Arch
Dis Child 1977; 52:188-91.
68. Lorber J, Sunderland R. Lumbar puncture in children with
convulsions associated with fever. Lancet 1980; 1:785-6.
69. Michael A, Gerber MD, Benjamin C, Berliner MD. The child
with a simple febrile seizure. Appropriate diagnostic
evaluation. Am J Dis Child 1981; 135: 431-3.
70. James M, Chamberlian MD, Richard L, Gormas MD. Occult
bacteraemia in children with simple febrile seizure. Am J
Dis Child 1988; 142: 1073-6.
71. McIntyre P, Kennedy R, Haris F. Occult pneumococcal
bacteraemia and febrile convulsions. Brit Med J. 1983; 286:
203-6.

128
72. Ayoola OO, Adeyemo AA, Osinusi K. Predictors of
bacteraemia among febrile infants in Ibadan, Nigeria. J
Health Popul Nutr 2002; 20: 223-9.
73. Akpede GO, Ambe JP. Cerebral herniation in pyogenic
meningitis: prevalence and related dilemmas in emergency
room populations in developing countries. Dev Med Child
Neuro 2000; 42: 462-9.
74. McGowan JE, Bratton L, Klein JO, Finland M. Bacteraemia in
febrile children seen in a “walk-in” paediatric clinic. New Eng
J Med 1973; 288: 1309-12.
75. Klein JO. The febrile child and occult bacteremia. New Eng J
Med 1987; 317: 1219- 20.
76. Cbratton L, Teele DW, Klein JO. Outcome of unsuspected
pneumococcemia in children not initially admitted to the
hospital. J Paed 1977.90:703.
77. Wallace SJ. Spontaneous fits after convulsions with fever.
Arch Dis Child. 1977; 52:192-6.
78. Lennox MA. Febrile convulsions in childhood: their
relationship to adult epilepsy. J Paediatr 1949; 35:427-35.
79. Rutter N, Metalfe DH. Febrile convulsions - what do parents
do? Brit Med J. 1978; 2:1345-6.
80. Rehm KP. Fever in infants and children. Current Opinion
Pediatrics. 2001; 13:83 -8.

129
81. United Nations Children’s fund (UNICEF). Poverty and
children: lessons of the 90’s fore least developed countries.
New york. 2001.www.unicef.org.
82. Ganfranco D. Prophylactic diazepam in febrile convulsion.
Arch Dis Child 1979; 54:244-5[Letter].
83. Knudsen FU. Recurrence risk after first febrile seizures and
effect of short-term diazepam prophylaxis. Arch Dis Child
1985; 60:1045-9.
84. Faero O, Kastrup KW, Neilsen EL, Malchior JC, Thorn I.
Sucessful prophylaxis of febrile convulsions with
Phenobarbital . Epilepsia 1972; 13: 279-85.
85. Lennox-Bucthal MA. Febrile convulsions. In: Laidlaw J and
Richen A (eds). A textbook of Epilepsy. Edinburgh London
Melbourne New York. Churchill Livingstone (publishers).
1982: 68-88.
86. Quellette EM. The child who convulses with fever. Paediatr
Clinics North Amer 1974; 21: 467-81.
87. Wolf SM, Carr A, Davis DC, Davdson S. The value of
Phenobarbital in a child who has had a single febrile seizure:
a controlled prospective study. Paediatr 1977; 59: 378-85.
88. Heckmatt JZ, Hoston AB, Clow DJ. Stephenson JBP, Dodd
KL, et al. Failure of phenobarbitone to prevent febrile
convulsions. BMJ 1976; 1: 559- 61.

130
89. Frantzen E, Lonnox-Buhthal MA, Nygaard A, Stene J. A
genetic study of febrile convulsions. Neurol 1970, 20: 909-17.
90. Knudsen FU, Vestermark V. Prophylactic diazepam or
phenobarbitone in febrile convulsions: a prospective
controlled study. Arch Dis Child 1978; 53: 660-3.
91. Wallace SJ. Recurrence of febrile convulsions. Arch Dis
Childhood 1972; 47: 171-8.
92. Marvin A, Fishman MD. Febrile seizures: the treatment
controversy. J Paediatr 1979; 94:177-84.
93. Dianese G, Faccoli G. Efficacy of diazepam prophylaxis
intermittent therapy in febrile convulsion. Convergno su ile
epilessia infantile benign. Verona 1978 (press) (Italian).
94. Wolf SM, Forsythe A. Behaviour disturbances, phenorbarbital
and febrile seizures. Paediatr 1978; 61: 728 – 31.
95. Ogunmekan AO. Prevention of febrile convulsions with
sodium valproate. Centr Afr J Med 1984; 30: 277-9.
96. Nelson KB, Ellenberg JH. Predictors of Epilepsy in children
who have experienced febrile seizures. N Engl J Med 1976;
295:1029-33.
97. Airede AI. Febrile convulsions: factors and recurrence rate.
Trop Georg Med 1992; 44: 233-7.
98. Konishi T, Naganuma Y, Hongo K, Murakami M,
Yamatani M, Okada T. Clinical evaluation of the patients

131
with epilepsy following febrile convulsions. No To
Hattatsu (Japanese). 1990; 22: 230-4.
99. Kanemoto K, Takuji N, Kawasaki J, Kawai I.
Characteristics and treatment of temporal lobe epilepsy
with a history of complicated febrile convulsions. J Neurol
Neurosurg Psychiatry 1998; 64:245-8.
100. Michael A, Pollack MD. Continuous phenobarbital treatment
after a simple febrile convulsion. Am J Dis Child 1978; 132:
87-9.
101. Bower SPC, Kilpatrick CJ, Vogrin SJ, Morris K, Cook MJ.
Degree of hippocampal atrophy is not related to history of
febrile seizures in patients with proved hippocampal
sclerosis. J Neurol Neurosurg Psychiatry 2000; 69:733-8.
102. Ojewole JA, Olusi SO. Effects of cow’s urine concoction on
plasma glucose concentration in fasted rats. J Trop Med
Hygiene 1976; 79: 241-3.
103. Ransome kuti O, Elebute O, Augusto-Odutola T. Malignant
convulsions in childhood in Nigeria. J Nig Med Ass 1971; 1:
23.
104. Osuntokun BO, Odeku EL, Sinette CH. Convulsive disorders
in Nigerian. East Afri Med J 1969; 46: 385.
105. Atalabi O. Cow’s urine poisoning. Dokita.1964; 6: 1-4.

132
106. Oyebola DDO. Cow’s urine concoction: it’s chemical
composition, pharmacological actions and mode of lethality.
Afr J Med Med Sci 1983; 12:57-63.
107. Aicardi J, Chevrie JJ. Febrile convulsions: neurological
sequalae and mental retardation. In Bazor MAB, Coceani F
(eds). Brain dysfunction in infantile febrile convulsions. New
York. Raven Press (publishers). 1976; 247-57.
108. Wallace SJ. Annotation. Febrile convulsion: their significance
for later intellectual development and behavior. J Child
Psychol 1984; 25:15-21.
109. Lennox MA. Febrile convulsions in childhood. A clinical and
electroencephalographic study. Am J Dis Child. 1949;
78:868-82.
110. Fisher A, Laig J, Stokel J (eds). Handbook for Family
planning operations research design New york 1983; 31-3.
111. Osinusi K, Njinyam MN. Comparison of body temperatures
taken at different sites and reliability of axillary temperature
in screening for fever. Afri J Med Sci 1997; 163-6.
112. Sullivan K, Gorstein J. Programs for nutritional
anthropometry. In Dean AG, Dean JA, Burton AH, Dicker RC
(eds). Epi info, version 5: a word processing and statistics

133
program for epidermiology on microcomputers. Georgia, WHO
publication.1990; 23:175-92.
113. NCHS growth curves for children. US. Department of
Health, Education and Welfare. Washington DC.1977; 78-
165.
114. WHO. Use and interpretation of anthropometric indicators
of nutritional status. WHO Working group. Bulleting of the
World Health Organisation.1986; 64: 929-41.
115. Oyedeji GA. Social economic and cultural background of
hospitalized children in Ilesha. Nig J Paediatr 1985; 12: 111-
7.
116. Osuntokun BO. Neurology of malaria. Postgrad Doctor
(Africa) 1983; 5: 420-6.
117. Igbogboja IS, Angyo I, Okolo AA, Szlachetka R. Morbidity and
mortality patterns of paediatric emergencies in Jos, Nigeria.
Nig Med Pract 1995; 30:15-8.
118. Olowu AA, Olanrewaju DM. Pattern of febrile convulsions in
hospitalized children. Nig J Paediatr 1992; 19: 1 – 5.
119. Osuntokun BE, Odeku EL, Sinnette CH. Convulsive disorders
in Nigerians: the febrile convulsions (an evaluation of 155
patients). E Afr Med J 1969; 46: 385 – 94.
120. Livingstone S. Infantile febrile convulsions. Dev Med Child
Neurol 1968; 10: 374 – 6.

134
121. Lennox MA. Febrile convulsion in childhood. Am J Dis Child.
1949; 78: 868 – 82.
122. Mclellan D, Giebink GS. Perspectives on occult bacteremia in
children. J Paediatr 1986 ;109:1 –8.
123. World Health Organization. A growth chart for International
use in Maternal and child health care. Guidelines for PHC
personnel. Geneva. 1978.
124. Rutter N, Smales ORC. Calcium, magnesium and glucose
levels in blood and CSF of children with febrile convulsions.
Arch Dis Child 1976; 51: 141 –3.
125. Ejeheri NA, Obi JO, Alakija W. Childhood febrile seizures
(Benin experience). Ann Trop Paediatr 1994; 14: 211 – 4.
126. Graitcher PL, Gentry EM. Measuring children: one reference
for all. Lancet 1988; 2:297.
127. Ajayi IO, Akinyinka OO. Evaluation of the nutritional status
of first year school children in Ibadan, Nigeria. Afr J Kmed
Sci. 1999; 28: 59 –63.
128. Gilberg C. Epilepsy and other seizure disorders. In J Aicardi
J(ed). Disease of the nervous system in childhood. MacKeith
press (publishers). 1992:958 –61.
129. Hirtz DG, Nelson KB. The natural history of febrile seizures.
Ann Rev Med 1983; 34:453 –71.

135

136
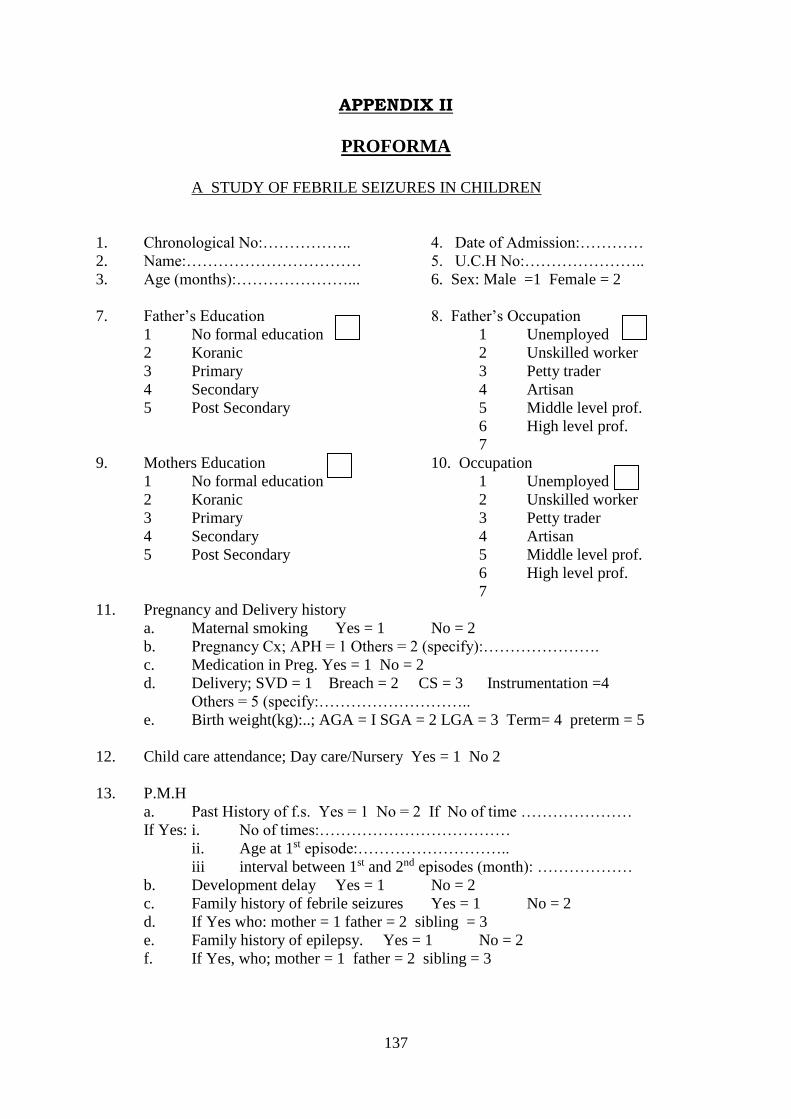
137
APPENDIX II
PROFORMA
A STUDY OF FEBRILE SEIZURES IN CHILDREN
1. Chronological No:…………….. 4. Date of Admission:…………
2. Name:…………………………… 5. U.C.H No:…………………..
3. Age (months):…………………... 6. Sex: Male =1 Female = 2
7. Father’s Education 8. Father’s Occupation
1 No formal education 1 Unemployed
2 Koranic 2 Unskilled worker
3 Primary 3 Petty trader
4 Secondary 4 Artisan
5 Post Secondary 5 Middle level prof.
6 High level prof.
7
9. Mothers Education 10. Occupation
1 No formal education 1 Unemployed
2 Koranic 2 Unskilled worker
3 Primary 3 Petty trader
4 Secondary 4 Artisan
5 Post Secondary 5 Middle level prof.
6 High level prof.
7
11. Pregnancy and Delivery history
a. Maternal smoking Yes = 1 No = 2
b. Pregnancy Cx; APH = 1 Others = 2 (specify):………………….
c. Medication in Preg. Yes = 1 No = 2
d. Delivery; SVD = 1 Breach = 2 CS = 3 Instrumentation =4
Others = 5 (specify:………………………..
e. Birth weight(kg):..; AGA = I SGA = 2 LGA = 3 Term= 4 preterm = 5
12. Child care attendance; Day care/Nursery Yes = 1 No 2
13. P.M.H
a. Past History of f.s. Yes = 1 No = 2 If No of time …………………
If Yes: i. No of times:………………………………
ii. Age at 1st episode:………………………..
iii interval between 1st and 2nd episodes (month): ………………
b. Development delay Yes = 1 No = 2
c. Family history of febrile seizures Yes = 1 No = 2
d. If Yes who: mother = 1 father = 2 sibling = 3
e. Family history of epilepsy. Yes = 1 No = 2
f. If Yes, who; mother = 1 father = 2 sibling = 3

138
14. Presenting complaints
a. Fever ; duration (in days):…………………..
b. Seizures
i. No of times: Once = 1 twice = 2 > thrice = 3
ii. Focal = 1 or generalized = 2
iii. Duration:………………………………….
iv. Post ictal state:…………………………….
c. Other symptoms; cough = 1 vomiting = 2 diarrhea = 3
Ear pain/ discharge = 4 others = 5 (specify):………………….
15. Pre hospital treatment. Yes = 1 No = 2
a. Native concoction = 1 salt and water = 2 milk = 3 other = 4
b. Other treatment; substances applied to eyes = 1 burning of part of body = 2
(specify):………………… Others = 3 (specify):………………….
16. Physical Examination
a. Weight (kg):……… (b) Ht (cm):…… (c) OFC (cm):…………..
d. Temperature (oC) (at admission/time of seizure):…..
17. Clinical Diagnosis; Malaria = 1 ARI = 2 UTI = 3 G.E = 4 Others = 5
(specify):……………………………
18. CNS examination;
level of con : lethargy = 1, drowsy = 2, Alert = 3, coma = 4,
Neck stiffness :present =1,absent = 2
kerning sign : post = 1,neg = 2.
Brudzuki’s sign : post = 1, neg = 2
Tone : normal = 1, red = 2, increased = 3
Reflexes : normal = 1, red = 2, increased = 3.
19. Investigations
a) CSF: (i)wbc:………….. (ii)rbc:………………..(iii) protein:……………..
(iv)sugar:…………………. (v)rbs:……………………………
b) blood film for malaria parasite……………………..
c)PCV………………………………………………...
d) FBC………………………………………………...
e) Blood culture………………………………………
f) Urine culture……………………………………….
g) others(specify)…………………………………….
20. Final Diagnosis:……………………………………………………………
21. Outcome: Discharge = 1 Died = 2
22. If discharged duration of stay (in days):……………………………..
23. Neurological deficit (specify):…………………………………………

139