Fat Chance: The Bitter Truth about Sugar 6/19/13 Robert...
28
Fat Chance: The Bitter Truth about Sugar 6/19/13 Robert H. Lustig, MD BIOGRAPHY: Robert H. Lustig, M.D. is Professor of Pediatrics, in the Division of Endocrinology at University of California, San Francisco. Dr. Lustig is a neuroendocrinologist who performs research and clinical care on patients with obesity and diabetes. For the last decade, Dr. Lustig’s clinical research has focused on the regulation of energy balance by the central nervous system. He is currently investigating the contribution of biochemical, neural, hormonal, and genetic influences in the expression of the current obesity epidemic both in children and adults. He is interested in the hypothalamic signal transduction of the hormones insulin and leptin, how these two systems interact, and how they become dysfunctional in obesity. He is studying the interplay between the changes in the nutritional environment and defective hormone signaling; in particular, the role of fructose and lack of fiber in the genesis of the metabolic syndrome. He is assessing the cardiovascular morbidity associated with insulin excess, and developing methods to evaluate and prevent this phenomenon in children. Dr. Lustig graduated from MIT in 1976, and received his M.D. from Cornell University Medical College in 1980. He completed his pediatric residency at St. Louis Children’s Hospital in 1983, and his clinical fellowship at UCSF in 1984. From there, he spent six years as a research associate in neuroendocrinology at The Rockefeller University. He is the author of many academic works, and of the popular book “Fat Chance: beating the odds against sugar, processed food, obesity, and disease”. Dr. Lustig is also President of the non‐profit Institute for Responsible Nutrition, a think tank devoted to improving our food supply.
Transcript of Fat Chance: The Bitter Truth about Sugar 6/19/13 Robert...

Fat Chance: The Bitter Truth about Sugar 6/19/13
Robert H. Lustig, MD
BIOGRAPHY: Robert H. Lustig, M.D. is Professor of Pediatrics, in the Division of Endocrinology at University of
California, San Francisco. Dr. Lustig is a neuroendocrinologist who performs research and clinical care
on patients with obesity and diabetes. For the last decade, Dr. Lustig’s clinical research has focused on
the regulation of energy balance by the central nervous system. He is currently investigating the
contribution of biochemical, neural, hormonal, and genetic influences in the expression of the current
obesity epidemic both in children and adults. He is interested in the hypothalamic signal transduction of
the hormones insulin and leptin, how these two systems interact, and how they become dysfunctional in
obesity. He is studying the interplay between the changes in the nutritional environment and defective
hormone signaling; in particular, the role of fructose and lack of fiber in the genesis of the metabolic
syndrome. He is assessing the cardiovascular morbidity associated with insulin excess, and developing
methods to evaluate and prevent this phenomenon in children.
Dr. Lustig graduated from MIT in 1976, and received his M.D. from Cornell University Medical College in
1980. He completed his pediatric residency at St. Louis Children’s Hospital in 1983, and his clinical
fellowship at UCSF in 1984. From there, he spent six years as a research associate in neuroendocrinology
at The Rockefeller University. He is the author of many academic works, and of the popular book “Fat
Chance: beating the odds against sugar, processed food, obesity, and disease”. Dr. Lustig is also
President of the non‐profit Institute for Responsible Nutrition, a think tank devoted to improving our
food supply.

6/14/2013
1
Hudson Street Press (Penguin USA)Fourth Estate (Harper Collins UK)
• No disclosures
Past
2001
Currently there are 30% more obese than undernourished people worldwide
(World Health Organization)
366 million diabetics in 2011
(5% of the world‘s population)(International Diabetes Federation)
Present
8 March 2013
Diabetes Costs The US $245 Billion A Year Says New Report
Diagnosed diabetes cost the United States
an estimated $245 billion in 2012, according
to new research released by the
American Diabetes Association (ADA) this week.
The new figure represents a 41% rise in five years.
In 2007, when the cost were last estimated,
it came to $174 billion.
Experts predict:
165 million Americans will be obese by 2030(4 part obesity series in Lancet, 8/26/11)
42% of Americans will be obese by 2030 (Finkelstein et al. Am J Prev Med epub 5/7/12)
100 million Americans will have diabetes by 2050(CDC Division of Diabetes Translation, 2011)
Future

6/14/2013
2
“Exclusive” view of obesity and metabolic dysfunction
Obese (30%)
Normal weight (70%)
240 million adults in U.S.
72 million
168 million
Obese (30%)
Obese and sick(80% of 30%)
Normal weight (70%)
240 million adults in U.S.
72 million
168 million
Total: 57 million sick
“Exclusive” view of obesity and metabolic dysfunction
Obese (30%)
Normal weight (70%)
240 million adults in U.S.
72 million
168 million
“Inclusive” view of obesity and metabolic dysfunction
Obese (30%)
Normal weight (70%)
240 million adults in U.S.
Normal weight,Metabolic dysfunction
(40% of 70%)
Obese and sick(80% of 30%)
57 million 67 million
Total: 124 million sick
72 million
168 million
“Inclusive” view of obesity and metabolic dysfunction
Relation between visceral and subcutaneous obesity:(thin on the outside, fat on the inside)
Thomas et al. Obesity doi: 10.1038/oby.2011.142, 2011
Obesity is not the problem

6/14/2013
3
Obesity is not the problem
Metabolic Syndrome: where all the money goes(75% of all healthcare dollars)
Obesity is not the problem
Metabolic Syndrome: where all the money goes(75% of all healthcare dollars)
DiabetesHypertension
Lipid abnormalitiesCardiovascular disease
Non-alcoholic fatty liver diseasePolycystic ovarian disease
CancerDementia
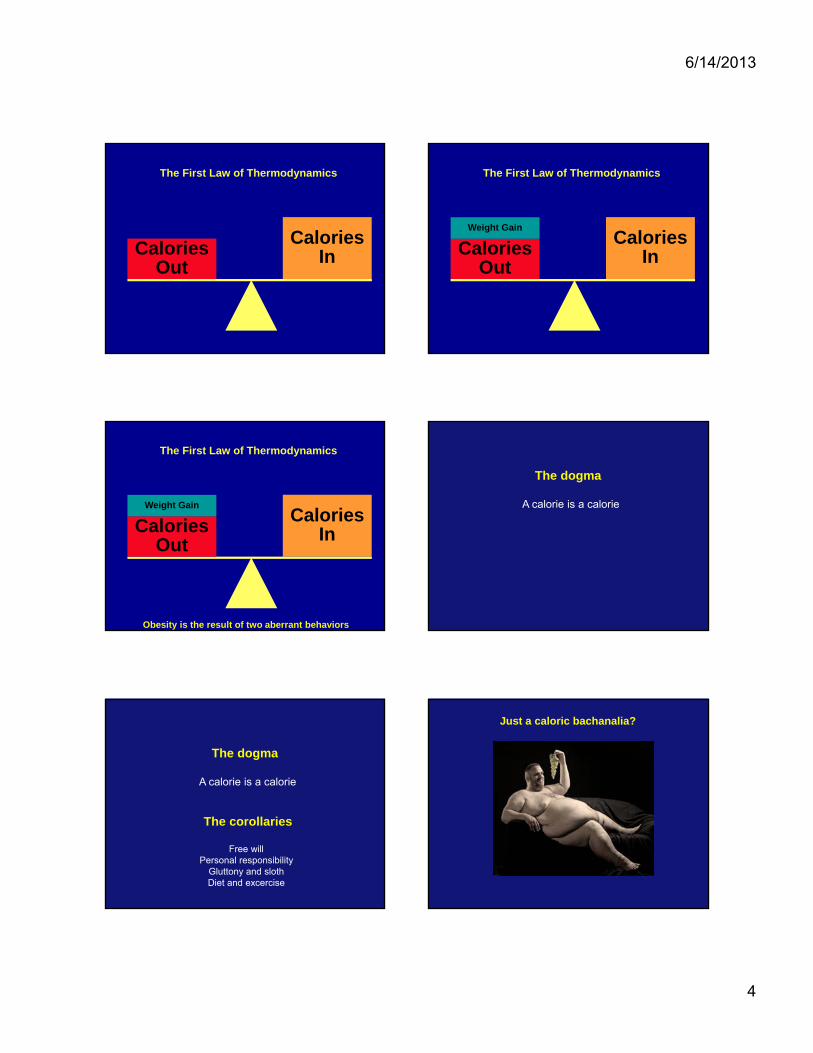
The First Law of Thermodynamics
The total energy inside a closed system remains constant.
The First Law of Thermodynamics
The total energy inside a closed system remains constant.
Two interpretations:
The First Law of Thermodynamics
CaloriesIn
The First Law of Thermodynamics
6/14/2013
4
CaloriesInCalories
Out
The First Law of Thermodynamics
CaloriesInCalories
Out
Weight Gain
The First Law of Thermodynamics
CaloriesInCalories
Out
Weight Gain
The First Law of Thermodynamics
Obesity is the result of two aberrant behaviors
The dogma
A calorie is a calorie
The dogma
A calorie is a calorie
The corollaries
Free willPersonal responsibility
Gluttony and slothDiet and excercise
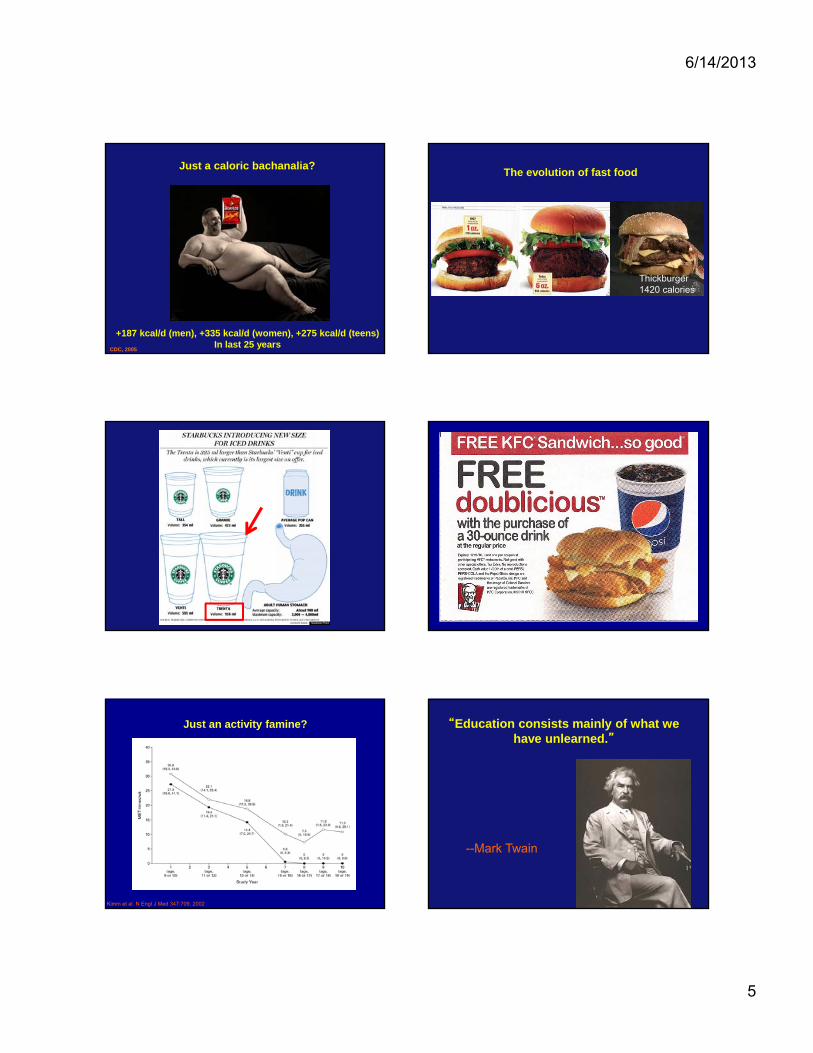
Just a caloric bachanalia?
6/14/2013
5
Just a caloric bachanalia?
+187 kcal/d (men), +335 kcal/d (women), +275 kcal/d (teens)In last 25 years
CDC, 2005
The evolution of fast food
Thickburger1420 calories
Just an activity famine?
Kimm et al. N Engl J Med 347:709, 2002
“Education consists mainly of what we have unlearned.”
--Mark Twain
6/14/2013
6
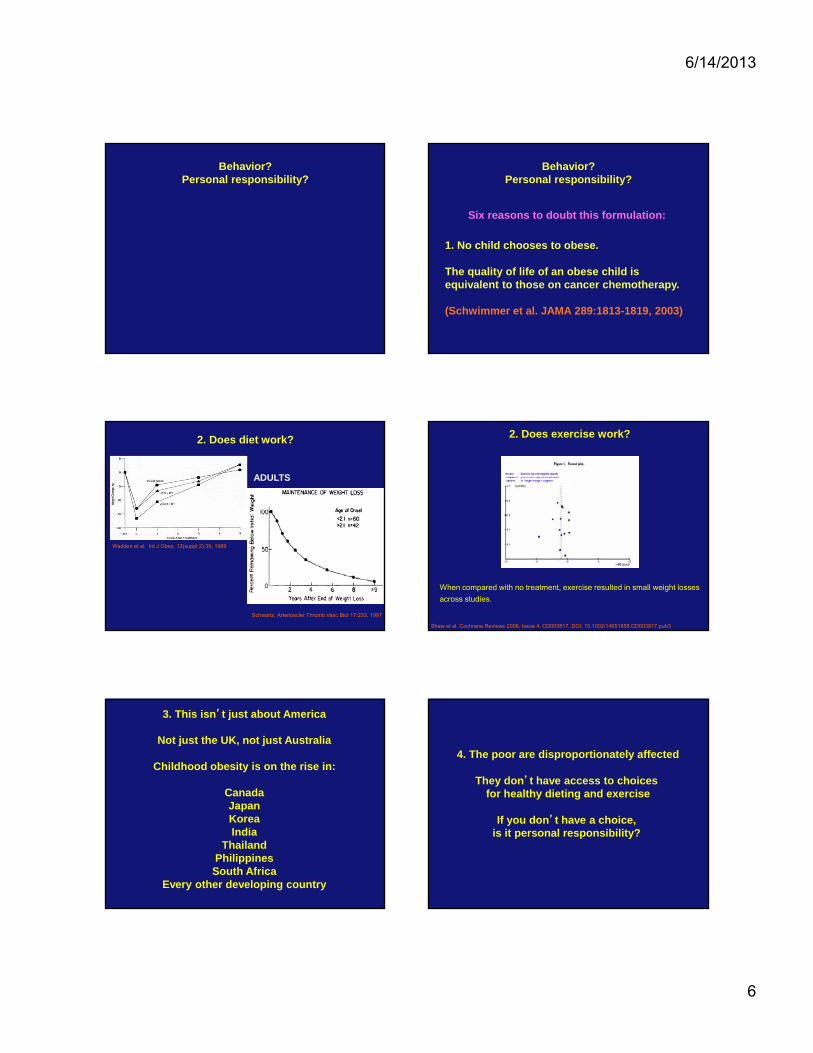
Behavior?Personal responsibility?
Behavior?Personal responsibility?
1. No child chooses to obese.
The quality of life of an obese child is equivalent to those on cancer chemotherapy.
(Schwimmer et al. JAMA 289:1813-1819, 2003)
Six reasons to doubt this formulation:
Wadden et al. Int J Obes. 13(suppl 2):39, 1989
Schwartz, Arterioscler Thromb Vasc Biol 17:233, 1997
2. Does diet work?
ADULTS
2. Does exercise work?
Shaw et al. Cochrane Reviews 2006, Issue 4: CD003817. DOI: 10.1002/14651858.CD003817.pub3.
When compared with no treatment, exercise resulted in small weight losses
across studies.
3. This isn’t just about America
Not just the UK, not just Australia
Childhood obesity is on the rise in:
CanadaJapanKoreaIndia
ThailandPhilippinesSouth Africa
Every other developing country
4. The poor are disproportionately affected
They don’t have access to choices for healthy dieting and exercise
If you don’t have a choice, is it personal responsibility?

6/14/2013
7
5. The prevalence of obesity in children is going up even faster than in adults
6. We even have an epidemic of obese 6-month olds
They don’t exhibit any of these behaviors
(Kim et al, Obesity 15:1107, 2006)
So any hypothesis that attemptsto explain the obesity epidemic,
must be able to explain this as well
• Gestational diabetes has increased in prevalence
• Birthweight has increased by 200 grams
throughout the world
South AfricaIsrael
RussiaU.S.
DEXA scans for body compositionshow greater fat depostion
Behavior
Stedman’s Medical Dictionary
Def. A stereotyped motor response to a physiological stimulus
Behavior
Stedman’s Medical Dictionary
Def. A stereotyped motor response to a physiological stimulus
Corollary: Behavior has a biochemical basis
Behavior
Stedman’s Medical Dictionary
Def. A stereotyped motor response to a physiological stimulus
Corollary: Behavior has a biochemical basis
What are the biochemical underpinnings of gluttony and sloth?
6/14/2013
8
The neuroendocrinology of energy balance
If you give a 5 year old kid a cookie:
PARADOX:
PARADOX:
If you give a 5 year old kid a cookie:
Leptin stimulates the SNS
Mark et al. Acta Physiol Scand 177:345, 2003
But if you give a 5 year old obese kid a cookie:
PARADOX:
But if you give a 5 year old obese kid a cookie:
PARADOX:

6/14/2013
9
The leptin negative feedback loop
Farooqi et al. N Engl J Med 341:913, 1999
Leptin promotes weight loss in a leptin-deficient patient Leptin Tx in LeptinDeficiency
Age 3.5 yearsAge 3.5 years Age 8 yearsAge 8 yearsO’Rahilly et al JCI Oct 2002
Obese subjects are leptin resistantWhat’s blocking leptin from working?
If we could solve that, we could solve obesity
X?
6/14/2013
10
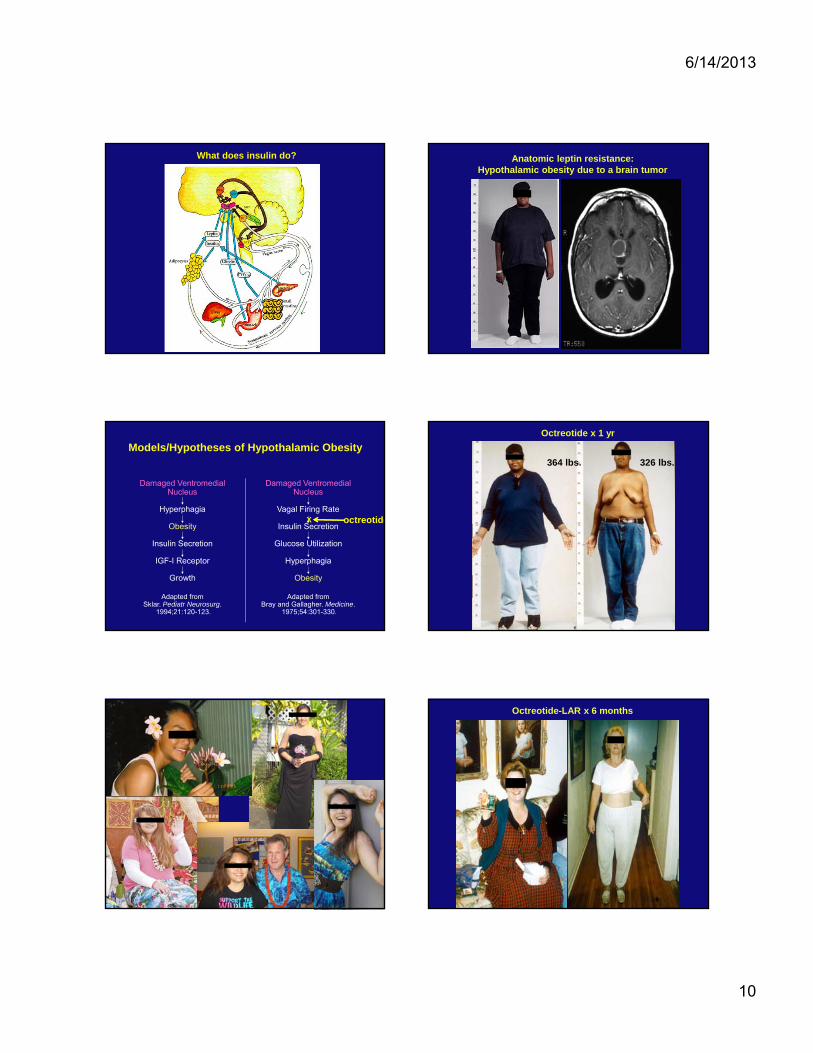
What does insulin do? Anatomic leptin resistance:Hypothalamic obesity due to a brain tumor
Models/Hypotheses of Hypothalamic Obesity
Damaged VentromedialNucleus
Hyperphagia
Obesity
Insulin Secretion
IGF-I Receptor
Growth
Adapted fromSklar. Pediatr Neurosurg.
1994;21:120-123.
Damaged VentromedialNucleus
Vagal Firing Rate
Insulin Secretion
Glucose Utilization
Hyperphagia
Obesity
Adapted fromBray and Gallagher. Medicine.
1975;54:301-330.
X octreotide
Octreotide x 1 yr
364 lbs. 326 lbs.
Octreotide-LAR x 6 months
6/14/2013
11
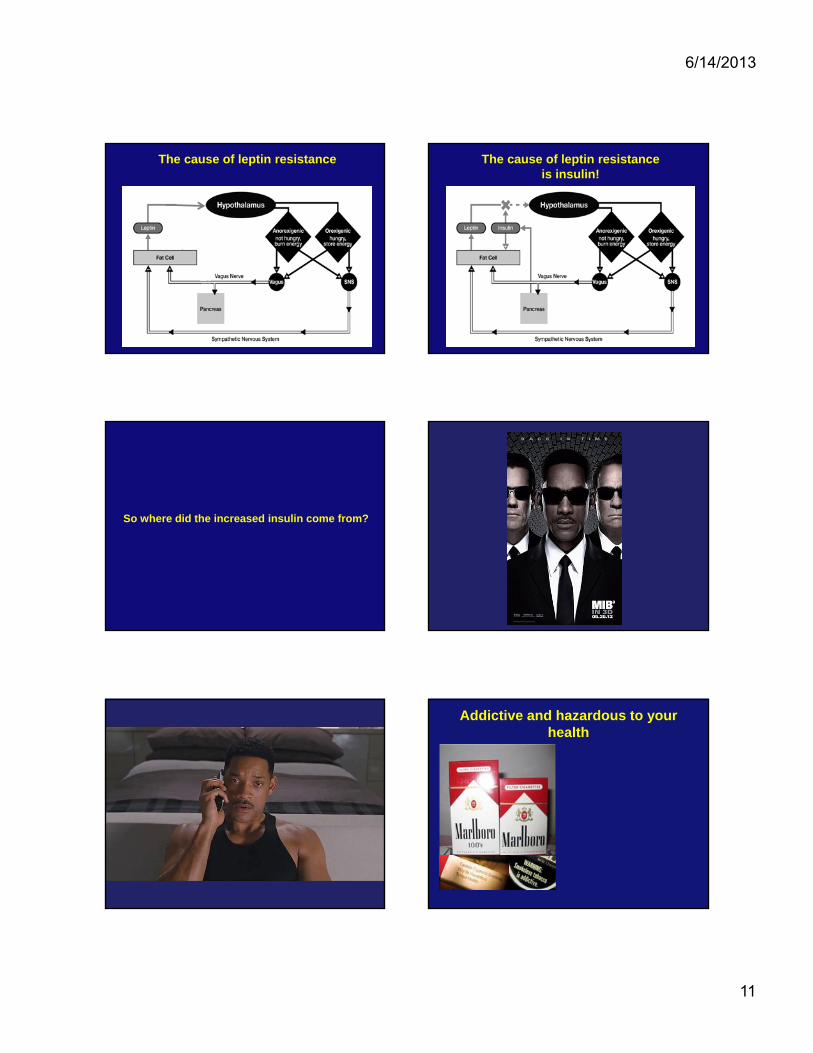
The cause of leptin resistance The cause of leptin resistanceis insulin!
So where did the increased insulin come from?
Addictive and hazardous to your health

6/14/2013
12
Addictive and hazardous to your health
New York Times, April 17, 2011
Nature 487:27-29, Feb 1, 2012
Hazardous to your health
“A calorie is NOT a calorie”
High Fructose Corn Syrup is 42-55% Fructose;Sucrose is 50% Fructose
Glucose Fructose
Sucrose
Bray, Am J Clin Nutr 86:895, 2007; Vos et al. Medscape Med J 10:160, 2008
Secular trend in U.S. fructose consumption
Natural consumption of fruits and vegetables • 15 gm/day
Prior to WWII (estimated):• 16-24 gm/day
1977-1978 (USDA Nationwide Food Consumption Survey):• 37 gm/day (8% of total caloric intake)
1994 (NHANES III): • 54.7 gm/day (10.2% of total caloric intake)
Adolescents: • 72.8 gm/day (12.1% of total caloric intake)• 25% consumed at least 15% of calories from fructose
Adulteration of our food supply
Addition of fructose
• palatability (esp. with decreased fat)
• browning agent
Removal of fiber
• shelf life
• freezing
Substitution of trans-fats
• hardening agent, shelf life
• now being removed due to CVD risk

6/14/2013
13
Mozaffarian et al. N Engl J Med 364:2392, 2011
Foods that cause weight gain
Mozaffarian et al. N Engl J Med 364:2392, 2011
Foods that cause weight gain
Mozaffarian et al. N Engl J Med 364:2392, 2011
Foods that cause weight gain
Loweringsugar
Raisingsugar
Effects of sugar on obesity (meta-analysis)
Te Morenga et al. BMJ 345:e7492, 2013
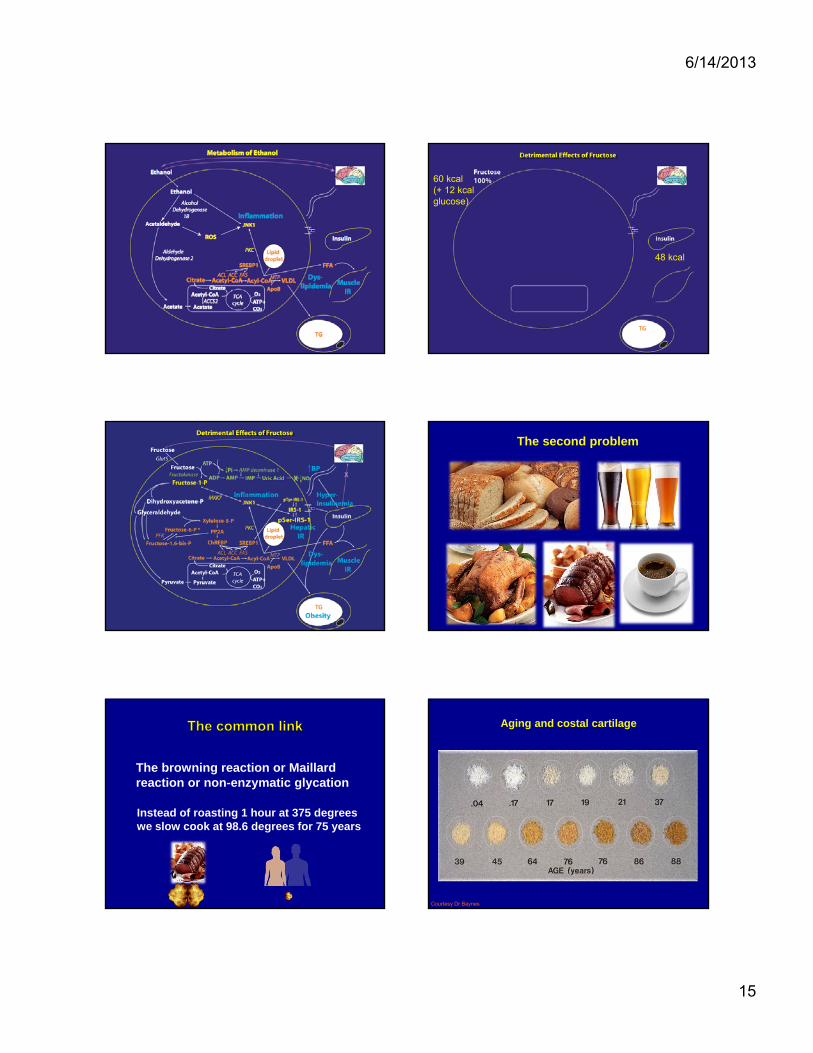
The first problem
Common wisdom: “Sugar is just “empty calories”
But:
• Hepatic fructose metabolism is different
• Chronic fructose exposure promotes the Metabolic Syndrome
Elliot et al. Am J Clin Nutr, 2002Bray et al. Am J Clin Nutr, 2004Teff et al. J Clin Endocrinol Metab, 2004Gaby, Alt Med Rev, 2005
Le and Tappy, Curr Opin Clin Nutr Metab Care, 2006Wei et al. J Nutr Biochem, 2006Johnson et al. Am J Clin Nutr 2007Rutledge and Adeli, Nutr Rev, 2007Brown et al. Int. J. Obes, 2008
Hepatocyte
24 kcal
96 kcal

6/14/2013
14
Ethanol is a carbohydrate
Ethanol is a carbohydrate
CH3-CH2-OH
Ethanol is a carbohydrate
CH3-CH2-OH
But ethanol is also a toxin
Acute ethanol exposure
• CNS depression
• Vasodilatation, decreased BP
• Hypothermia
• Tachycardia
• Myocardial depression
• Variable pupillary responses
• Respiratory depression
• Diuresis
• Hypoglycemia
• Loss of fine motor control
Acute fructose exposure
6/14/2013
15
60 kcal(+ 12 kcalglucose)
48 kcal
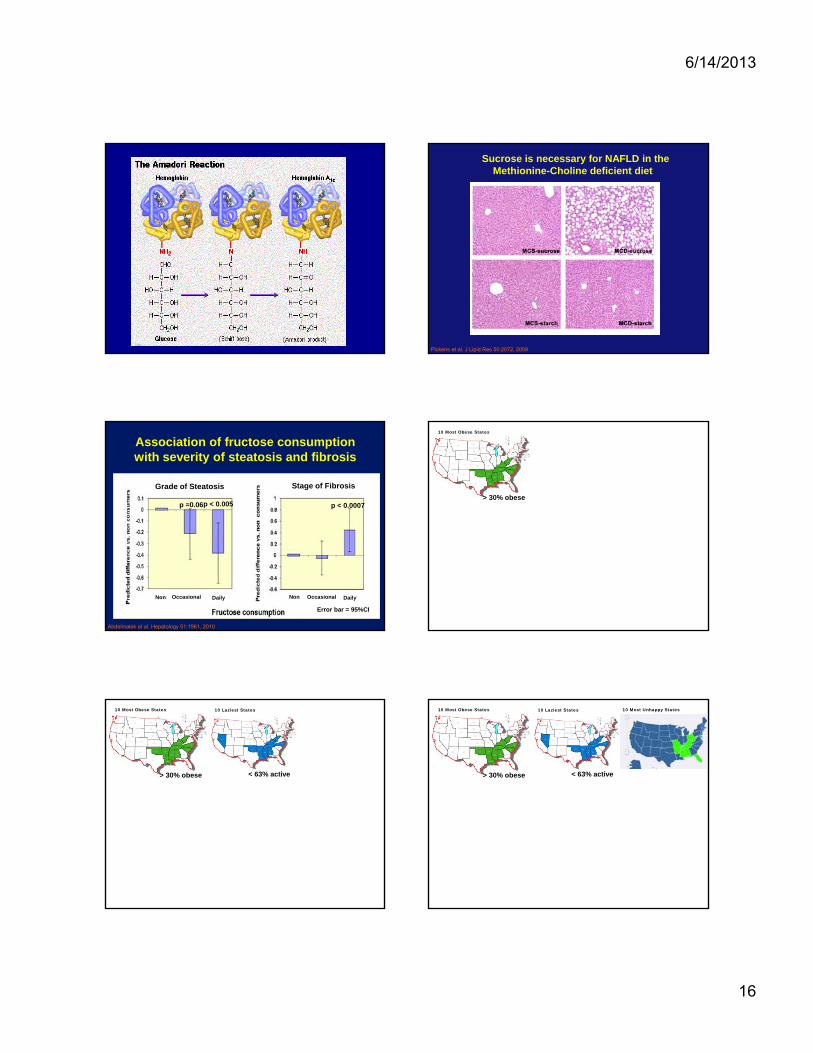
The second problem
The browning reaction or Maillard reaction or non-enzymatic glycation
Instead of roasting 1 hour at 375 degreeswe slow cook at 98.6 degrees for 75 years
Aging and costal cartilage
Courtesy Dr Baynes
6/14/2013
16
Sucrose is necessary for NAFLD in theMethionine-Choline deficient diet
Pickens et al. J Lipid Res 50:2072, 2009
Association of fructose consumption with severity of steatosis and fibrosis
Grade of Steatosis
p =0.06p < 0.005
Stage of Fibrosis
p < 0.0007
Non NonOccasional OccasionalDaily Daily
Error bar = 95%CI
Abdelmalek et al. Hepatology 51:1961, 2010
10 Most Obese States
> 30% obese
10 Most Obese States 10 Laziest States
> 30% obese < 63% active
10 Most Obese States 10 Laziest States
> 30% obese < 63% active
10 Most Unhappy States

6/14/2013
17
10 Most Obese States 10 Laziest States
> 30% obese < 63% active
10 Most Unhappy States 10 Most Obese States 10 Laziest States
> 30% obese < 63% active
10 Most Unhappy States
Adult Heart Disease Rate
10 Most Obese States 10 Laziest States
> 30% obese < 63% active
10 Most Unhappy States
Adult Heart Disease Rate
Global consumption of sugar/sugarcropsCalories per day, 2007
Data from Food and Agriculture Organization, World Health Organization, 2007
Prevalence of diabetes, 2010102
Correlation is not causationCorrelation is not causation
But we have causation tooBut we have causation too

6/14/2013
18
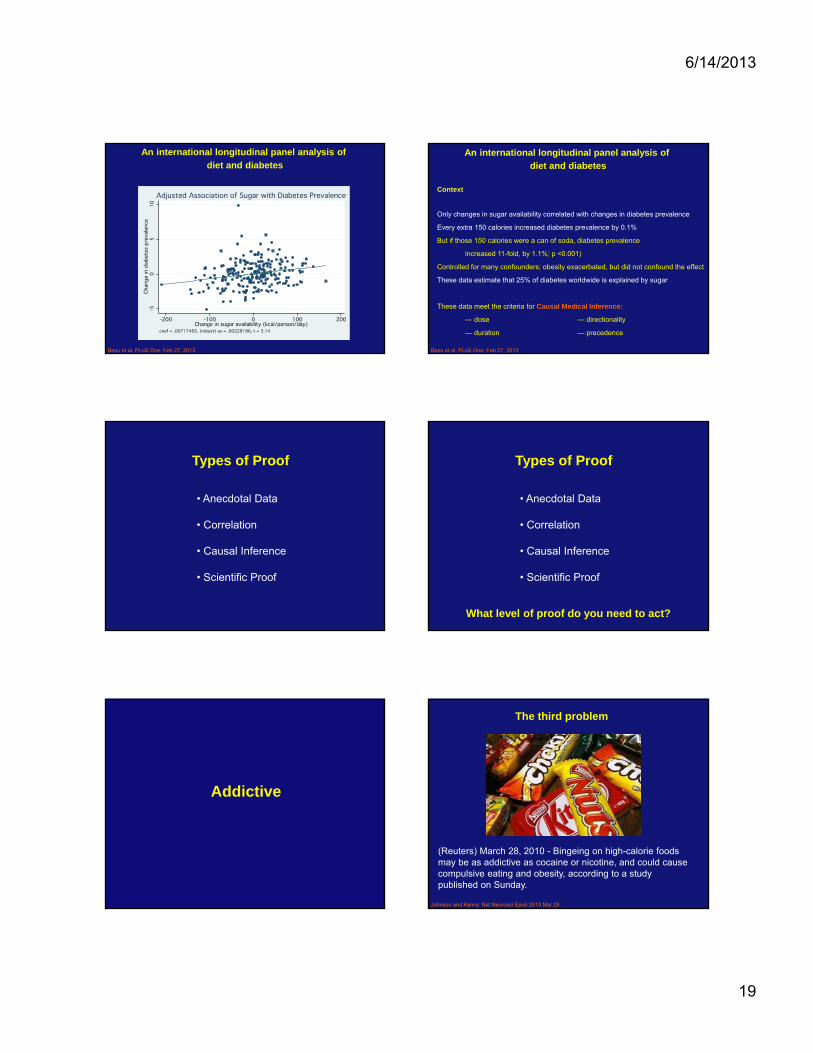
An international longitudinal panel analysis of
diet and diabetes
Food and Agriculture Organization (FAO); FAOSTATFood Supply data in kcal/capita/day calculation: Food Supply= ∑Supply Elements - ∑Utilization Elements =
(Production + Import Quantity + Stock Variation – Export Quantity) - (Feed + Seed + Processing + Waste).
Only industrial waste factored in.
Extracted Food Supply data for 2000 and 2007:Total Calories Roots & Tubers, Pulses, Nuts, Vegetables Fruits-Excluding Wine MeatOils CerealsSugar, Sugarcrops & Sweeteners
International Diabetes Federation (IDF)2000 (1st ed) and 2007 (3rd ed)
The World Bank World Development Indicators DatabaseGDP expressed in purchasing power parity in 2005 US dollars for
comparability among countries Basu et al. PLoS One, Feb 27, 2013
Total 204 countries; complete data for 154 countries (50 not different)
An international longitudinal panel analysis of
diet and diabetes
Basu et al. PLoS One, Feb 27, 2013
Total 204 countries; complete data for 154 countries (50 not different)
Data monitoring and quality
Generalized estimating equations
Conservative fixed effects approach (Hausman test)
Hazard model to control for selection bias (Heckman selection model)
Longitudinal data to determine what preceded diabetes (Granger causality)
Period effects controlled for secular trends that may have occurred as a
result of changes diabetes detection capacity or importation policies.
An international longitudinal panel analysis of
diet and diabetes
Basu et al. PLoS One, Feb 27, 2013
Total 204 countries; complete data for 154 countries (50 not different)
Data monitoring and quality
Generalized estimating equations
Conservative fixed effects approach (Hausman test)
Hazard model to control for selection bias (Heckman selection model)
Longitudinal data to determine what preceded diabetes (Granger causality)
Period effects controlled for secular trends that may have occurred as a
result of changes diabetes detection capacity or importation policies.
Controlled for:
GDP per capita % population living in urban areas
Obesity % of population over age 65
physical inactivity
An international longitudinal panel analysis of
diet and diabetes
Basu et al. PLoS One, Feb 27, 2013
An international longitudinal panel analysis of
diet and diabetes
Diabetes prevalence rose from 5.5% to 7.0% for 204 countries 2000-2007
Basu et al. PLoS One, Feb 27, 2013
An international longitudinal panel analysis of
diet and diabetes
Diabetes prevalence rose from 5.5% to 7.0% for 204 countries 2000-2007
Sugar
Sugar+controls
Sugar+controls+period
Overall
Model # countries Effect (95% CI)
Basu et al. PLoS One, Feb 27, 2013
6/14/2013
19
An international longitudinal panel analysis of
diet and diabetes
Basu et al. PLoS One, Feb 27, 2013
An international longitudinal panel analysis of
diet and diabetes
Context
Only changes in sugar availability correlated with changes in diabetes prevalence
Every extra 150 calories increased diabetes prevalence by 0.1%
But if those 150 calories were a can of soda, diabetes prevalence
increased 11-fold, by 1.1%; p <0.001)
Controlled for many confounders; obesity exacerbated, but did not confound the effect
These data estimate that 25% of diabetes worldwide is explained by sugar
These data meet the criteria for Causal Medical Inference:
— dose — directionality
— duration — precedence
Basu et al. PLoS One, Feb 27, 2013
Types of Proof
• Anecdotal Data
• Correlation
• Causal Inference
• Scientific Proof
Types of Proof
• Anecdotal Data
• Correlation
• Causal Inference
• Scientific Proof
What level of proof do you need to act?
Addictive
(Reuters) March 28, 2010 - Bingeing on high-calorie foods may be as addictive as cocaine or nicotine, and could cause compulsive eating and obesity, according to a study published on Sunday.
The third problem
Johnson and Kenny, Nat Neurosci Epub 2010 Mar 28.
6/14/2013
20
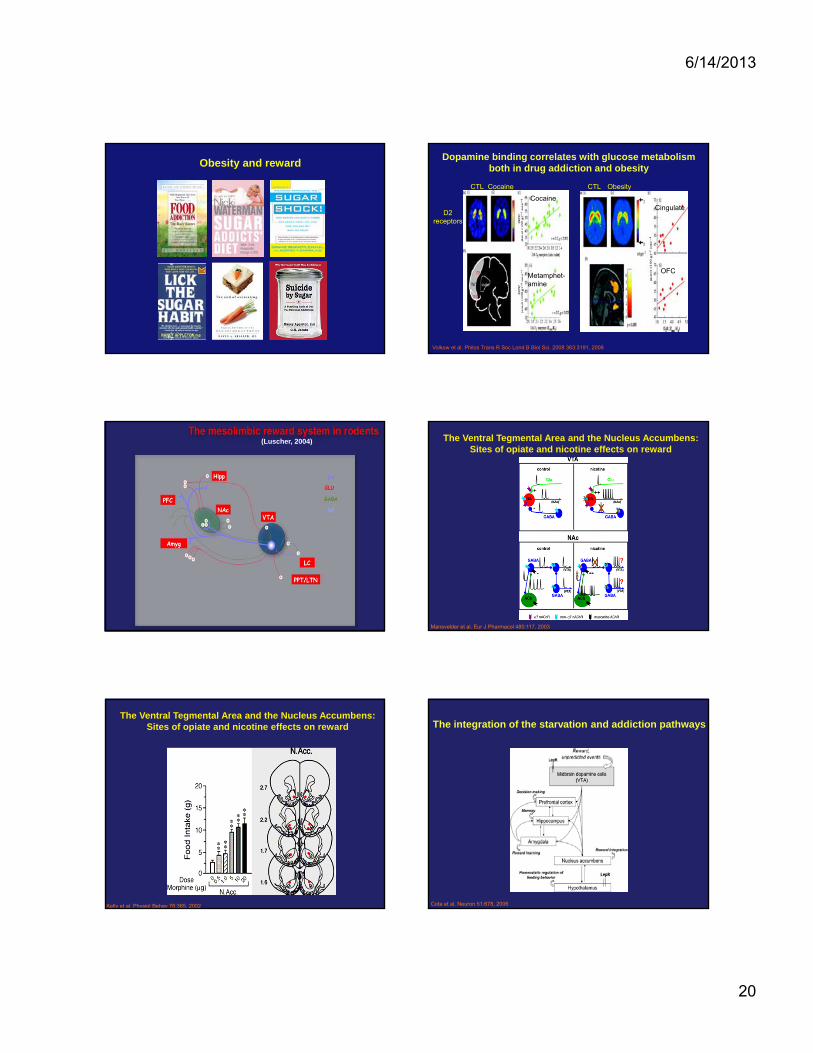
Obesity and reward
Volkow et al. Philos Trans R Soc Lond B Biol Sci. 2008 363:3191, 2008
Dopamine binding correlates with glucose metabolism both in drug addiction and obesity
CTL Cocaine
D2receptors
CTL Obesity
Cocaine
Metamphet-amine
Cingulate
OFC
(Luscher, 2004) The Ventral Tegmental Area and the Nucleus Accumbens:Sites of opiate and nicotine effects on reward
Mansvelder et al. Eur J Pharmacol 480:117, 2003
Kelly et al. Physiol Behav 76:365, 2002
The Ventral Tegmental Area and the Nucleus Accumbens:Sites of opiate and nicotine effects on reward The integration of the starvation and addiction pathways
Cota et al. Neuron 51:678, 2006
LepR
6/14/2013
21
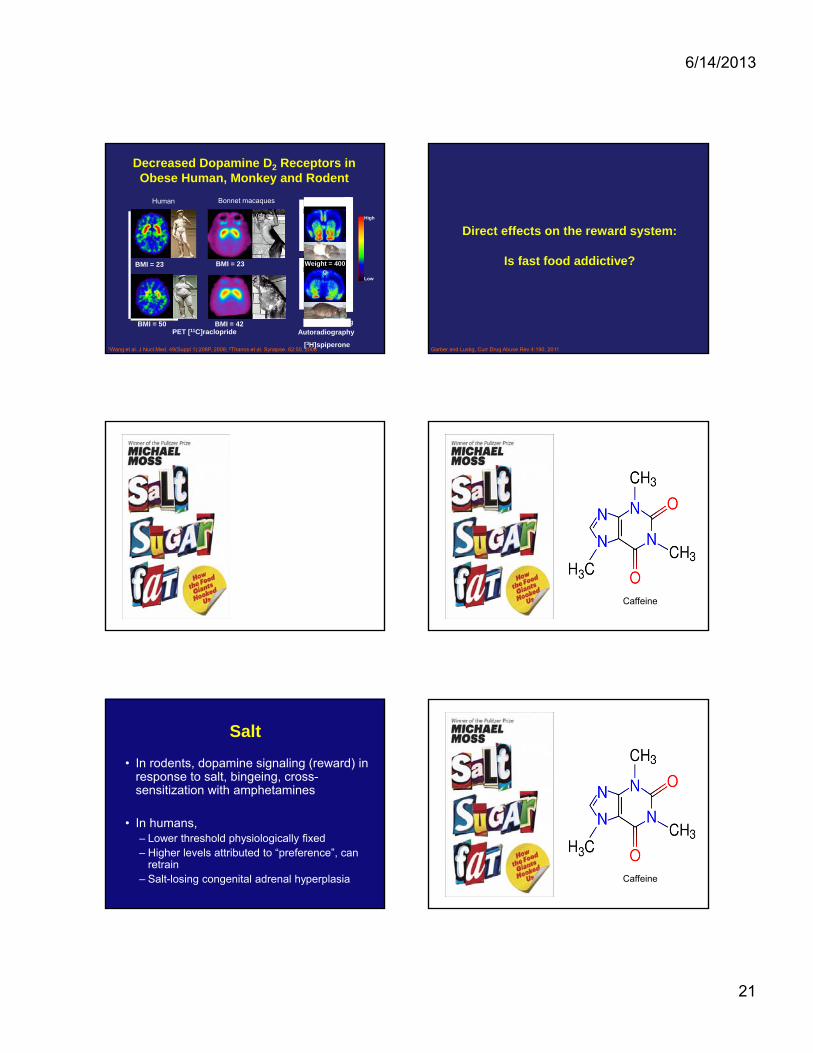
Decreased Dopamine D2 Receptors in Obese Human, Monkey and Rodent
PET [11C]raclopride
High
Low
Bonnet macaquesHuman
Autoradiography
[3H]spiperone
BMI = 42BMI = 50 Weight = 650 g
BMI = 23BMI = 23 Weight = 400 g
Zucker rat2
1Wang et al. J Nucl Med. 49(Suppl 1):208P, 2008; 2Thanos et al. Synapse. 62:50, 2008
Direct effects on the reward system:
Is fast food addictive?
Garber and Lustig, Curr Drug Abuse Rev 4:190, 2011
Caffeine
Salt
• In rodents, dopamine signaling (reward) in response to salt, bingeing, cross-sensitization with amphetamines
• In humans, – Lower threshold physiologically fixed– Higher levels attributed to “preference”, can
retrain– Salt-losing congenital adrenal hyperplasia Caffeine
6/14/2013
22
Caffeine
Fat
• Rodents binge but no signs of dependence• In humans, binge foods are high fat but
also high carb/sugar (e.g. pizza, ice cream)– Likely synergy, adding sugar increases
preference for fatty foods [Drewnowski et al.]
• Atkins diet does not show dependence• Energy density: stronger association with
obesity, metabolic syndrome
Caffeine Caffeine
Caffeine
• “Model drug” of dependence
• In humans, dependence shown in children, adolescents and adults– 30% who consume it meet DSM criteria for
dependence
– Physiologic addiction established: headache (increased cerebral blood flow). Impaired task performance, fatigue Caffeine

6/14/2013
23
Caffeine
Direct effects on the reward system:
Is sugar (fructose) addictive?
Garber and Lustig, Curr Drug Abuse Rev 4:190, 2011
Sugar and opioids
Sweet-Ease increases endogenous opioids to reduce pain,Even in neonates
Is there really such a thing as sugar addiction?
Need to look for similarities to drugs of dependence
• nicotine
• morphine
• amphetamine
• cocaine
• ethanol
Criteria for addiction
Cross-sensitizationIncreased
ConsumptionEnhanced locomotion
BINGEING
WITHDRAWAL
Tolerance
CRAVING
Negative emotion
Anticipation
Avena et al. Neurosci Biobehav Rev 32:20, 2008 (Courtesy Dr. B. Hoebel)
6/14/2013
24
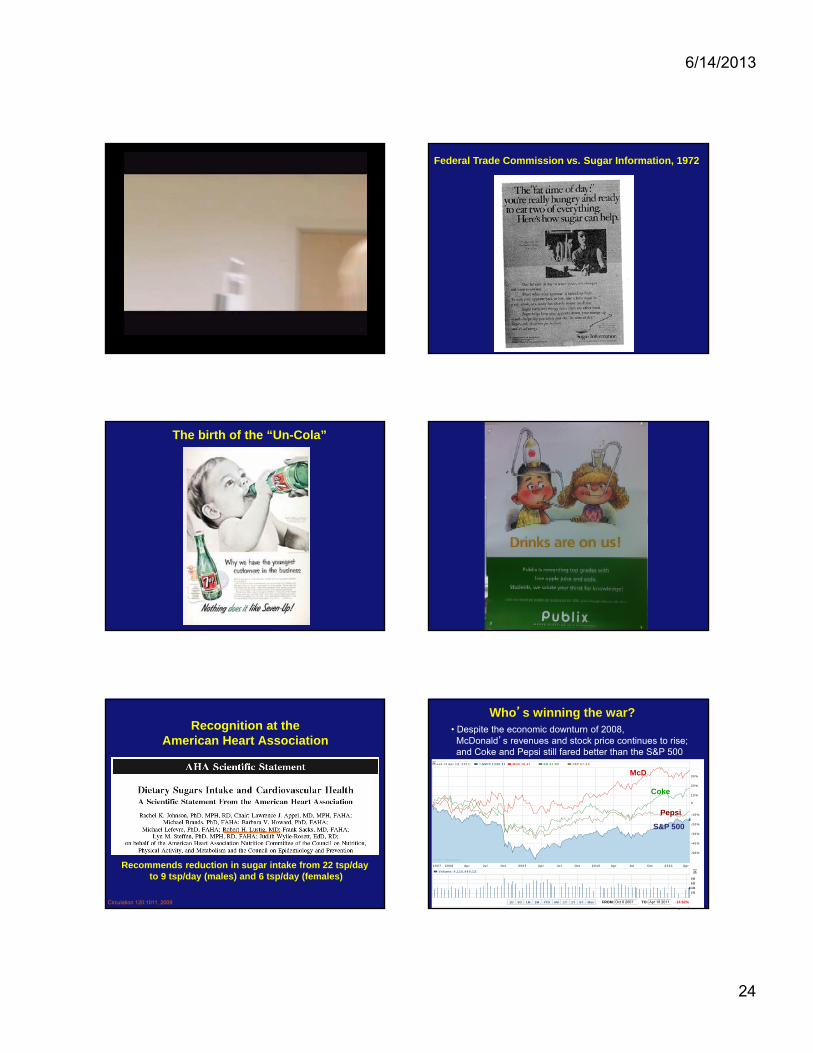
Federal Trade Commission vs. Sugar Information, 1972
The birth of the “Un-Cola”
Recognition at the American Heart Association
Circulation 120:1011, 2009
Recommends reduction in sugar intake from 22 tsp/day to 9 tsp/day (males) and 6 tsp/day (females)
Who’s winning the war?• Despite the economic downturn of 2008,McDonald’s revenues and stock price continues to rise; and Coke and Pepsi still fared better than the S&P 500
Week of Apr 18, 2011: ^GSPC 1330.36 MCD 78.40 KO 67.85 PEP 67.33
© 2011 Yahoo! Inc.
0
-50%
-40%
-30%
-20%
-10%
10%
20%
30%
2007 2008 Apr Jul Oct 2009 Apr Jul Oct 2010 Apr Jul Oct 2011 Apr
1D 5D 1M 3M YTD 6M 1Y 2Y 5Y Max FROM: Oct 8 2007 TO: Apr 18 2011 -14.82%
Volume: 4,115,440,128
2B4B6B8B
Pepsi
McD
Coke
S&P 500
6/14/2013
25
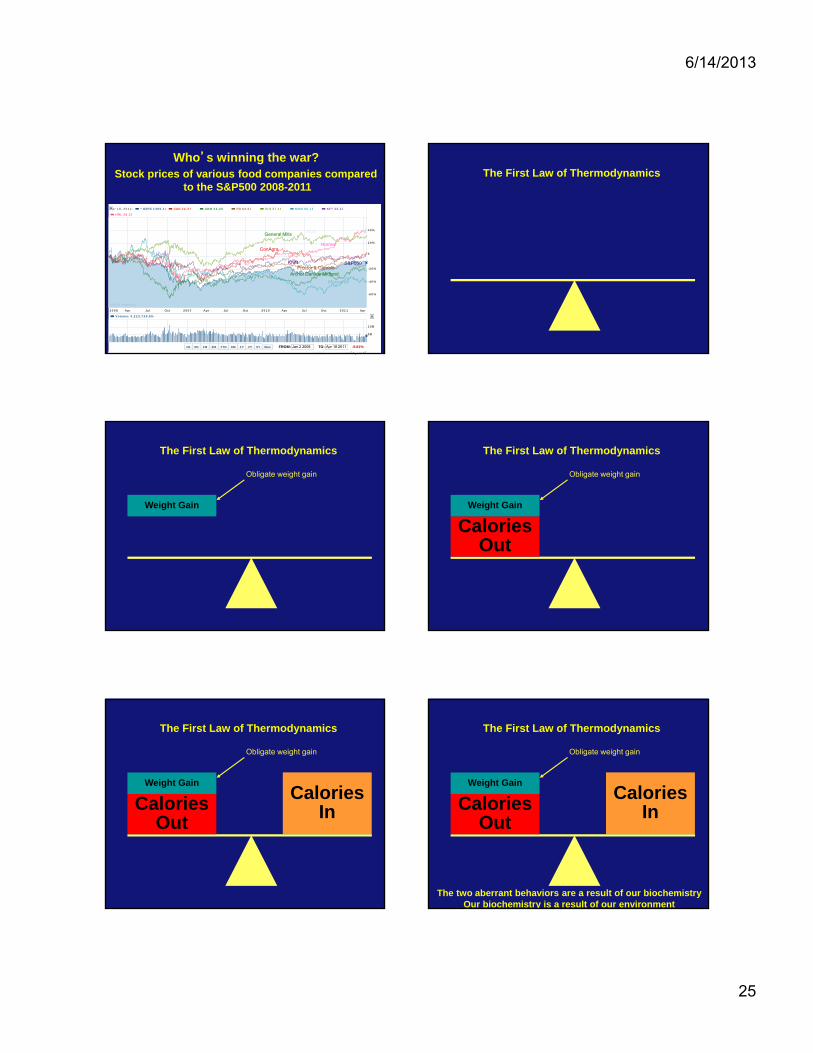
Stock prices of various food companies comparedto the S&P500 2008-2011
S&P
Who’s winning the war?
Apr 18, 2011: ^GSPC 1305.14 CAG 24.37 ADM 34.45 PG 64.00 GIS 37.18 MON 66.18 KFT 33.22
HRL 28.29
© 2011 Yahoo! Inc.
0
-60%
-40%
-20%
20%
40%
2008 Apr Jul Oct 2009 Apr Jul Oct 2010 Apr Jul Oct 2011 Apr
1D 5D 1M 3M YTD 6M 1Y 2Y 5Y Max FROM: Jan 2 2008 TO: Apr 18 2011 -9.81%
Volume: 4,223,739,904
5B
10B
Archer Daniels MidlandProctor & Gamble
Kraft
Monsanto
General Mills
ConAgraHormel
S&P500Kraft
The First Law of Thermodynamics
Weight Gain
Obligate weight gain
The First Law of Thermodynamics
CaloriesOut
Weight Gain
The First Law of Thermodynamics
Obligate weight gain
CaloriesInCalories
Out
Weight Gain
The First Law of Thermodynamics
Obligate weight gain
CaloriesInCalories
Out
Weight Gain
The First Law of Thermodynamics
Obligate weight gain
The two aberrant behaviors are a result of our biochemistryOur biochemistry is a result of our environment
6/14/2013
26
Question 1:
Can our “toxic environment” be changed
without government/societal intervention?
Especially when there are potentially addictive
substances involved?
Question 2:
Can we afford to wait to enact public health measures
when health care will be bankrupt due to
chronic metabolic disease?
Nat Rev Gastroenterol Hepatol 7:251, 2010
J Am Diet Assoc 110:1305, 2010
Further reading
Arterioscler Throm Vasc Biol 25:2451, 2005
Is fast food addictive?
Andrea K. Garber, Robert H. Lustig
Curr Drug Abuse Rev 4:146, 2011
Pediatric Annals 41:23, 2012
Further reading
Arterioscler Throm Vasc Biol 25:2451, 2005
Andrew A. Bremer, M.D., Ph.D.a, Michele Mietus-Snyder, M.D.b, Robert H. Lustig, M.D.c*
Pediatrics 129:557, 2012
Advances in Nutrition 4:1, 2013
Annals NY Academy of Sciences, 1, 2013
Further reading
PLoS One 8:e57873, 2013
Further reading
Current Opinion Gastroenterology, 29:170, 2013

6/14/2013
27
Hudson Street Press (Penguin USA)