
farmakogenetika
197
Farmakogene*ka Prof.dr. Amina Kozaric 24.10.2014 PMF 1
-
Upload
amilatravnjak -
Category
Documents
-
view
213 -
download
1
description
farmakogenetika predavanje
Transcript of farmakogenetika

Farmakogene*ka
Prof.dr. Amina Kozaric 24.10.2014
PMF
1

Defini*ons
• Pharmacogenomics: Analysing en*re genomes, across groups of individuals, to iden*fy the gene*c factors influencing responses to a drug.
• Pharmacogene-cs: Studying an individual's gene*c make up in order to predict responses to a drug and guide prescrip*on.
2

Objec*ves of Pharmacogene*cs
1. Iden*fy varia*on in response 2. Elucidate molecular mechanisms 3. Evaluate clinical significance 4. Develop screening tests 5. Individualize drug therapy
3

Personalized Medicine!
Courtesy of Felix W. Frueh US FDA

Personalized Medicine!• Medicine is personal:!
– We are all different.!– Some of our differences translate into how we react to drugs
as individuals.!– This is why personalized medicine is important to
everyone.!• Why does someone need twice the standard dose to
be effective?!• Why does this drug work for you but not me?!• Why do I have side-effects and you don’t?!• Why do some people get cancer and others don’t?!• Why is anecdotal information irrelevant to your own
health and treatment?!

Variability of Disease!Variability of Disease!
Courtesy Felix W. Frueh

The Goal of Personalized Medicine!
• The Right Dose of • The Right Drug for • The Right Indica*on for • The Right Pa*ent at • The Right Time.

What is DNA?

April 1953 Drs. James Watson and
Francis Crick determined the structure of DNA (double helix)

April 2003 Human Genome Project
determined the en-re DNA sequence of a human
(3 billion le/ers)
April 1953 Drs. James Watson and
Francis Crick determined the structure of DNA (double helix)

What is Pharmacogenomics?
R X

Pharma = drug or medicine Genomics = the study of genes
R X
Pharmacogenomics?

Personalized medicine tailored to your genes
Pharma = drug or medicine Genomics = the study of genes
R X
What is Pharmacogenomics?

Case Study – Breast Cancer Pa-ents

Case Study – Breast Cancer Pa-ents
Tumoricide

16
Case Study – Breast Cancer Pa-ents

17
Case Study – Breast Cancer Pa-ents
30%

18
Helped No Effect/Hurt
Tumoricide

Helped No Effect/Hurt
Tumoricide
Why?

Your DNA
How do scien-sts make personalized medicine?

You Your cells
Your DNA
Picture credit: adapted from Riken Research: h[p://www.rikenresearch.riken.jp/eng/frontline/5514
How do scien-sts make personalized medicine?
It’s all about what makes YOUR gene-c code UNIQUE

Gene*c Code: DNA DeoxyriboNucleic Acid (DNA) contains all the informa-on
necessary to make a complete organism
DNA is composed of a combination of 4 nucleotides

Gene*c Code: DNA DeoxyriboNucleic Acid (DNA) contains all the informa-on
necessary to make a complete organism
DNA is composed of a combination of 4 nucleotides
A
Adenine

Gene*c Code: DNA DeoxyriboNucleic Acid (DNA) contains all the informa-on
necessary to make a complete organism
DNA is composed of a combination of 4 nucleotides
A T
Adenine Thymine

Gene*c Code: DNA DeoxyriboNucleic Acid (DNA) contains all the informa-on
necessary to make a complete organism
DNA is composed of a combination of 4 nucleotides
A T C
Adenine Thymine Cytosine

Gene*c Code: DNA DeoxyriboNucleic Acid (DNA) contains all the informa-on
necessary to make a complete organism
DNA is composed of a combination of 4 nucleotides
A T C G
Adenine Thymine Cytosine Guanine

DNA: A long double-‐stranded string of nucleo-des that encode for many genes.
Gene
The Central Dogma: DNAàRNAàProtein

DNA: A long double-‐stranded string of nucleo-des that encode for many genes.
Gene
RNA: A single-‐stranded copy of one gene.
RNA
The Central Dogma: DNAàRNAàProtein

DNA: A long double-‐stranded string of nucleo-des that encode for many genes.
Gene
RNA: A single-‐stranded copy of one gene.
The Central Dogma: DNAàRNAàProtein
RNA
Protein: Proteins are composed amino acids. Amino acids are made from triplets of nucleo-des called codons.

DNA: A long double-‐stranded string of nucleo-des that encode for many genes.
Gene
Protein: Proteins are composed amino acids. Amino acids are made from triplets of nucleo-des called codons.
RNA: A single-‐stranded copy of one gene.
The Central Dogma: DNAàRNAàProtein
Codon 1

DNA: A long double-‐stranded string of nucleo-des that encode for many genes.
Gene
Protein: Proteins are composed amino acids. Amino acids are made from triplets of nucleo-des called codons.
RNA: A single-‐stranded copy of one gene.
The Central Dogma: DNAàRNAàProtein
Codon 1 Codon 2

DNA: A long double-‐stranded string of nucleo-des that encode for many genes.
Gene
Protein: Proteins are composed amino acids. Amino acids are made from triplets of nucleo-des called codons.
Amino acid 1 Amino acid 2
RNA: A single-‐stranded copy of one gene.
The Central Dogma: DNAàRNAàProtein
Codon 1 Codon 2

DNA: A long double-‐stranded string of nucleo-des that encode for many genes.
Gene
Protein: Proteins are composed amino acids. Amino acids are made from triplets of nucleo-des called codons.
Amino acid 1 Amino acid 2
Protein!
RNA: A single-‐stranded copy of one gene.
The Central Dogma: DNAàRNAàProtein
Codon 1 Codon 2

A small change in the gene sequence can result in a very different protein
ATG GTG CTG TCT CCT DNA:

A small change in the gene sequence can result in a very different protein
ATG GTG CTG TCT CCT
Met
DNA:
Amino Acids/Protein:

A small change in the gene sequence can result in a very different protein
ATG GTG CTG TCT CCT
Met
DNA:
Amino Acids/Protein: Val

A small change in the gene sequence can result in a very different protein
ATG GTG CTG TCT CCT
Met Leu
DNA:
Amino Acids/Protein: Val

A small change in the gene sequence can result in a very different protein
ATG GTG CTG TCT CCT
Met Leu Ser
DNA:
Amino Acids/Protein: Val

A small change in the gene sequence can result in a very different protein
ATG GTG CTG TCT CCT
Met Leu Ser Pro
DNA:
Amino Acids/Protein: Val

A small change in the gene sequence can result in a very different protein
ATG GTG CTG TCT CCT
Met Leu Ser Pro
DNA:
Amino Acids/Protein: Val

A small change in the gene sequence can result in a very different protein
ATG GTG CTG TCT CCT
Met Leu Ser Pro
DNA:
Amino Acids/Protein: Val
ATG GTG CTG TCT ACT DNA:

A small change in the gene sequence can result in a very different protein
ATG GTG CTG TCT CCT
Met Leu Ser Pro
DNA:
Amino Acids/Protein: Val
ATG GTG CTG TCT ACT
Met Leu Ser Thr
DNA:
Amino Acids/Protein: Val

A small change in the gene sequence can result in a very different protein
ATG GTG CTG TCT CCT
Met Leu Ser Pro
DNA:
Amino Acids/Protein: Val
Words: Tom and Sam are bad
ATG GTG CTG TCT ACT
Met Leu Ser Thr
DNA:
Amino Acids/Protein: Val

A small change in the gene sequence can result in a very different protein
ATG GTG CTG TCT CCT
Met Leu Ser Pro
DNA:
Amino Acids/Protein: Val
Words: Tom and Sam are bad
ATG GTG CTG TCT ACT
Met Leu Ser Thr
DNA:
Amino Acids/Protein: Val
Tom and Sam are sad Words:

A small change in the gene sequence can result in a very different protein
ATG GTG CTG TCT CCT
Met Leu Ser Pro
DNA:
Amino Acids/Protein: Val
Words: Tom and Sam are bad
ATG GTG CTG TCT ACT
Met Leu Ser Thr
DNA:
Amino Acids/Protein: Val
Tom and Sam are sad Words:
Changes in DNA are called varia-ons or muta-ons
Variations in the DNA (genotype) can cause observable changes (phenotype) in individuals

Helped No Effect/Hurt
Tumoricide
Why does Tumoricide work on some pa-ents but not
on others?

What are the reasons a person would react differently to drugs?
1. Having the receptor (protein) to recognize the drug
2. Other physiological traits that enable you to respond to a drug
3. How your body processes the drugs a[er receiving it

Drugs and Receptors
Cell

Drugs and Receptors
Cell
Receptor (Protein)

Drugs and Receptors
Cell
Receptor (Protein)

Drugs and Receptors
Cell
Drug (Ligand) Receptor
(Protein)

Drugs and Receptors
Cell
Drug (Ligand) Receptor
(Protein)

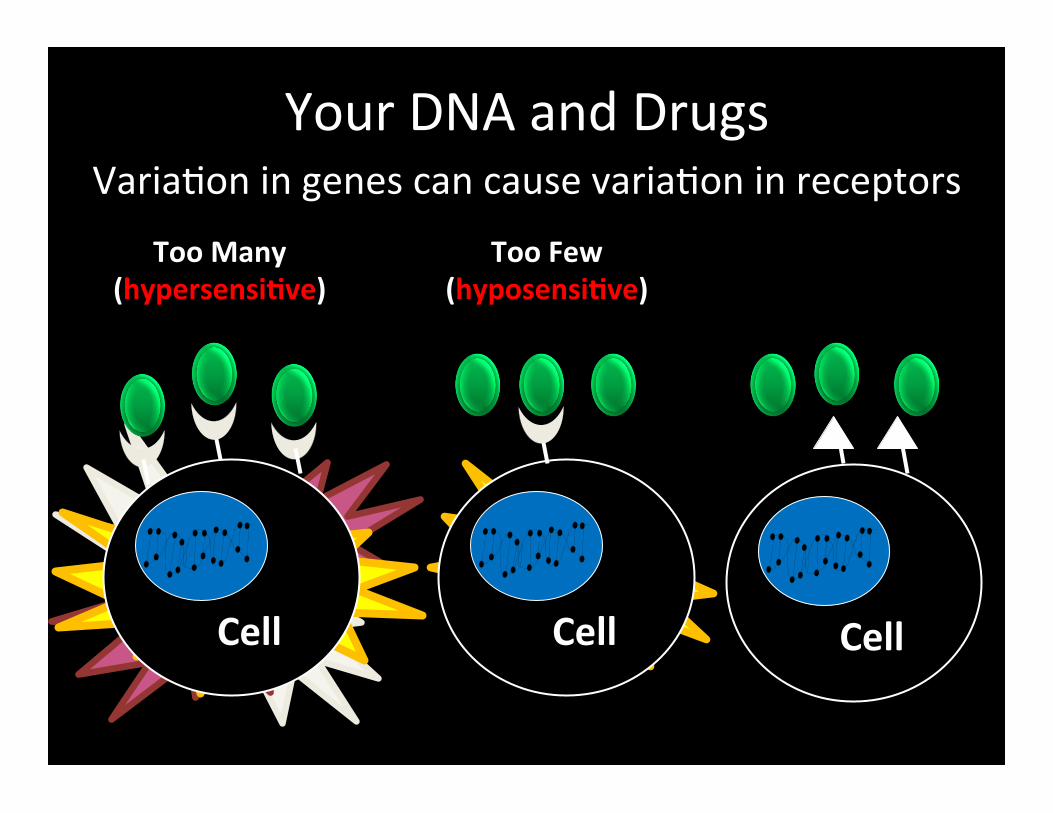
Your DNA and Drugs Varia*on in genes can cause varia*on in receptors
Cell

Your DNA and Drugs Varia*on in genes can cause varia*on in receptors
Cell

Your DNA and Drugs Varia*on in genes can cause varia*on in receptors
Cell
Cell
Cell

Your DNA and Drugs Varia*on in genes can cause varia*on in receptors
Cell
Cell
Cell
Cell
Cell

Your DNA and Drugs Varia*on in genes can cause varia*on in receptors
Cell
Cell
Cell
Too Many (hypersensi-ve)
Cell
Cell
Your DNA and Drugs Varia*on in genes can cause varia*on in receptors
Cell
Cell
Cell
Too Many (hypersensi-ve)
Too Few (hyposensi-ve)
Cell
Cell

Your DNA and Drugs Varia*on in genes can cause varia*on in receptors
Cell
Cell
Cell
Cell
Cell
Too Many (hypersensi-ve)
Too Few (hyposensi-ve)
Mutated (insensitive)

Where Drugs “Fit” In
Lock = Receptor Key = Drug

Taste cell
“This tastes bi/er!”
PTC-‐Receptor PTC
Why can some people taste PTC and others can’t?
Phenylthiocarbamide

Taste cell
“This tastes bi/er!”
PTC-‐Receptor PTC
Why can some people taste PTC and others can’t?
Taste cell
“I don’t taste anything!”
Non-‐binding PTC-‐
Receptor
PTC

Where does tas*ng PTC come from? You have two copies of every
gene: one from Mom
and one from Dad

Where does tas*ng PTC come from? You have two copies of every
gene: one from Mom
and one from Dad

Where does tas*ng PTC come from? You have two copies of every
gene: one from Mom
and one from Dad

• Your two genes are the genotype
You have two copies of every gene:
one from Mom and
one from Dad
Where does tas*ng PTC come from?

• Your two genes are the genotype • A gene can be dominant or recessive
You have two copies of every gene:
one from Mom and
one from Dad
Where does tas*ng PTC come from?

• Your two genes are the genotype • A gene can be dominant or recessive • The expressed trait is a phenotype
You have two copies of every gene:
one from Mom and
one from Dad
Where does tas*ng PTC come from?

Tas*ng PTC is dominant (T) over inability taste PTC which is recessive (t)
TT Tt [

Tas*ng PTC is dominant (T) over inability taste PTC which is recessive (t)
TT Tt [

Tas*ng PTC is dominant (T) over inability taste PTC which is recessive (t)
TT Tt [

Tas*ng PTC is dominant (T) over inability taste PTC which is recessive (t)
TT Tt [

Tas*ng PTC is dominant (T) over inability taste PTC which is recessive (t)
TT Tt [
For individuals with these genotypes, what would their phenotypes be?

TT
“This tastes REALLY bi[er!”
SUPERTASTER
Tas*ng PTC is dominant (T) over inability taste PTC which is recessive (t)
Tt [

“This tastes bi[er!” TASTER
TT
“This tastes REALLY bi[er!”
SUPERTASTER
Tas*ng PTC is dominant (T) over inability taste PTC which is recessive (t)
Tt [

“This tastes bi[er!” TASTER
TT
Tas*ng PTC is dominant (T) over inability taste PTC which is recessive (t)
Tt [
“I dont taste anything!”
NON-‐TASTER
“This tastes REALLY bi[er!”
SUPERTASTER

Drug receptor summary
Ability to taste PTC has a very strong gene-c component PTC = chemical and Drugs = chemical
Differences in ability to taste PTC is similar to
differences in reac*ons to drugs ""

Helped No Effect/Hurt
Tumoricide
Why?

Two Types of Breast Cancer
• Tumoricide is a personalized medica-on • Tumoricide only works for Her2+ breast tumors
Y Her2-‐ Her2+

80
Helped No Effect/Hurt
Tumoricide
Her2-‐ Her2+

Screening for Her2+ Cells
American Journal of Clinical Pathology. 2008;129(2):263-273
Her2-‐ Her2+

Screening for Her2+ Cells
American Journal of Clinical Pathology. 2008;129(2):263-273
+ Tumoricide = ?

Screening for Her2+ Cells
American Journal of Clinical Pathology. 2008;129(2):263-273
+ Tumoricide = ✓

Breast Cancer 1990
• Surgery • Radia-on • Chemotherapy (drugs)
2012 • Surgery • Radia-on • Chemotherapy
• Specialized treatments (for certain types of breast cancer)
http://www.ucdmc.ucdavis.edu/welcome/features/20080709_cancer_sweeney/index.html

What are the reasons a person would react differently to drugs?
1. Having the receptor (protein) to recognize the drug
2. Other physiological traits that enable you to respond to a drug
3. How your body processes the drugs a[er receiving it

The presence of receptors influence how we react to drugs like Tumoricide or chemicals like PTC
Tumoricide Works!
Tumoricide Does Not Work
Her2-‐ Her2+
Y

TT Tt [
“This tastes REALLY bi[er!”
SUPERTASTER
“This tastes bi[er!” TASTER
“I dont taste anything!”
NON-‐TASTER
The presence of receptors influence how we react to drugs like Tumoricide or chemicals like PTC

Where are the PTC receptors?

What are taste buds? Taste buds are found on papillae on your tongue

What are taste buds? Taste buds are found on papillae on your tongue
Papillae
bumps on your tongue

What are taste buds? Taste buds are found on papillae on your tongue
Taste buds cells are found on the papilla
Papillae
bumps on your tongue

What are taste buds? Taste buds are found on papillae on your tongue
Taste buds cells are found on the papilla
PTC receptors are found on the taste buds
Papillae
bumps on your tongue

What are taste buds? Taste buds are found on papillae on your tongue
PTC receptors are found on the taste buds
Papillae
bumps on your tongue
Nerve Cell Transmits signal
to brain Taste buds cells are found on the papilla

What are taste buds? Taste buds are found on papillae on your tongue
PTC receptors are found on the taste buds
Papillae
bumps on your tongue
Nerve Cell Transmits signal
to brain
Brain Wow! This tastes
really bi[er
Taste buds cells are found on the papilla

If a person has more taste buds, then he/she may be able to taste the PTC more strongly.
Are there other traits that can allow a person to more strongly taste PTC?

Coun-ng the number of tongue papillae
5 papillae 20 papillae 35 papillae

Coun-ng the number of tongue papillae
5 papillae 20 papillae 35 papillae

Ideal graph representing the number of tongue papillae related to the phenotype of PTC taste
These results support our hypothesis that the super-taster has more papillae!

Ideal graph representing the number of tongue papillae related to the phenotype of PTC taste
The number of papillae in the non-taster is variable. Why would the number of papillae be variable in a non-
taster?

What does it take to be a PTC Taster? Two traits are important for determining PTC taste sensi-vity
1) PTC receptor genotype—Do you have the receptors that
enable you to taste PTC

What does it take to be a PTC Taster? Two traits are important for determining PTC taste sensi-vity
1) PTC receptor genotype—Do you have the receptors that
enable you to taste PTC
2) The density of papillae on your tongue correlates to the sensi-vity of tas-ng PTC
taster super-taster

What are the reasons a person would react differently to drugs?
1. Having the receptor (protein) to recognize the drug
2. Other physiological traits that enable you to respond to a drug
3. How your body processes the drugs after receiving it

http://publications.nigms.nih.gov/medbydesign/chapter1.html
ADME
• Absorp-on • Distribu-on
• Metabolism
• Excre-on
A Drug’s Life

Metabolic enzymes
Liver
DNA variations in special proteins in the liver called enzymes can influence a person’s ability to metabolize
certain drugs
Drug Metabolites Enzymes

Adverse Drug Reactions (ADR) • Definition- unwanted, negative response to a
prescribed drug at normal doses and during normal use – Examples?

Adverse Drug Reactions (ADR) • Definition- unwanted, negative response to a
prescribed drug at normal doses and during normal use – Examples?
• There are multiple causes for ADRs – environmental basis – genetic basis

Adverse Drug Reactions (ADR) • Definition- unwanted, negative response to a
prescribed drug at normal doses and during normal use – Examples?
• There are multiple causes for ADRs – environmental basis – genetic basis
• Poor metabolizers can experience ADRs at normally therapeutic drug doses

Case study: Nortriptyline metabolism
Three women of the same height, weight, age, and racial background are depressed and go to the doctor. The doctor prescribes an antidepressant, Nortriptyline,
at a dose of 100 mg.
• Person A has an adverse reaction • Person B nothing happens • Person C gets better…
A
B
C

Case study: Nortriptyline metabolism
Three women of the same height, weight, age, and racial background are depressed and go to the doctor. The doctor prescribes an antidepressant, Nortriptyline,
at a dose of 100 mg.
• Person A has an adverse reaction • Person B nothing happens • Person C gets better…
A
B
C
Why?

ADME of Nortriptyline
100mg Nortriptyline
Adverse reaction Nothing happens Gets better
A B C
How much active drug in blood?

ADME of Nortriptyline
100mg Nortriptyline
Adverse reaction Nothing happens Gets better
A B C
95mg 5mg 50mg

DNA variation influence drug metabolism
Liver
Drug Metabolites Enzymes
A
Poor Metabolizer
95mg

DNA variation influence drug metabolism
Liver
Drug Metabolites Enzymes
B
Ultrarapid Metabolizer
5mg

DNA variation influence drug metabolism
Liver
Drug Metabolites Enzymes
C
Intermediate Metabolizer
50mg

2012 - What do doctors do?
A B C
Decrease Dose Increase Dose
Or change drug
Poor Metabolizer Ultrarapid Metabolizer

Today One-size-fits-all drugs
• Current drug development system develops drugs for the average patient
• No simple way to determine who will respond well and who will respond poorly
• One size does NOT fit all! • What’s the solution?

Today One-size-fits-all drugs
• Current drug development system develops drugs for the average patient
• No simple way to determine who will respond well and who will respond poorly
• One size does NOT fit all! • What’s the solution?
Pharmacogenomics (PGx) Personalized Medicine

April, 2050 You wake up feeling terrible, and you know it's time to
see a doctor. In the office, the physician looks you over, listens to your symptoms, and decides to prescribe you
a drug. But first, the doctor takes a look at your DNA.
TODAY vs. FUTURE
Today = Drugs are One-Size-Fits-All
Future = Drugs Specific for You! More effective & minimizes side effects

Summary Gene-c varia-on leads to phenotypic differences and
differences in how we all react to drugs.

Summary Gene-c varia-on leads to phenotypic differences and
differences in how we all react to drugs.
1. Having the receptor (protein) to recognize the drug PTC and HER2 receptors

Summary Gene-c varia-on leads to phenotypic differences and
differences in how we all react to drugs.
1. Having the receptor (protein) to recognize the drug PTC and HER2 receptors
2. Other physiological traits that enable you to respond to a drug Number of taste buds on tongue

Summary Gene-c varia-on leads to phenotypic differences and
differences in how we all react to drugs.
1. Having the receptor (protein) to recognize the drug PTC and HER2 receptors
2. Other physiological traits that enable you to respond to a drug Number of taste buds on tongue
3. How drugs are processed in the body Enzymes in liver metabolize drugs

Pharamcogenomics Using people’s gene-c informa-on for the right
drug at the right dose at the right -me!
R X

Pharmacogenetics & Pharmacogenomics!
• Pharmacogene*cs: The role of gene*cs in drug responses. – F. Vogel. 1959
• Pharmacogenomics: The science that allows us to predict a response to drugs based on an individuals gene*c makeup. – Felix Frueh, Associate Director of Genomics, FDA
Courtesy Felix W. Frueh

Pharmacogenetics & Pharmacogenomics"
http://www.pharmgkb.org/!• Pharmacogenetics: study of individual gene-drug
interactions, usually one or two genes that have dominant effect on a drug response (SIMPLE relationship)!
• Pharmacogenomics: study of genomic influence on drug response, often using high-throughput data (sequencing, SNP chip, expression, proteomics - COMPLEX interactions)!
– PharmGKB Website: http://www.pharmgkb.org/!

Purine Analogs: A Case Study in Pharmacogenetics!
• 6-mercaptopurine, 6-thioguanine, azathioprine!
• Used to treat lymphoblastic leukemia, autoimmune disease, inflammatory bowel disease, after transplant!
• Interferes with nucleic acid synthesis!
• Therapeutic index limited by myelosuppression!(treatment limited by immune suppression side effect)!
6-thioguanine azathioprine!6-mercaptopurine!

Metabolism of 6-MP!
L Wang and R Weinshilboum, Oncogene 25, 1629-1638 (2006)!

Pharmacogenetics: A Case Study!
Courtesy of Michelle Whirl-Carillo!

Pharmacogenetics: A Case Study!
Courtesy of Michelle Whirl-Carillo!

Pharmacogenetics: A Case Study!

Thiopurine S-methyl Transferase Activity "and Personalized Dosage!

Second Example: Codeine and Cytochrome P450 CYP2D6
• Codeine is a commonly used opioid – Codeine is a prodrug – It must be metabolized into morphine for activity
• Cytochrome P450 allele CYP2D6 is the metabolizing enzyme in the liver
• 7% of Caucasians are missing one copy of the Cytochrome P450 CYP2D6 gene – codeine does not work effectively in these
individuals

Codeine and Morphine Metabolism!

Cytochrome Oxidase P450 Enzymes!
• 57 Different active genes!• 17 Different families!• CYP1, CYP2 and CYP3 are primarily involved in
drug metabolism.!• CYP2A6, CYP2B6, CYP2C9 ,CYP2C19, CYP2D6,
CYP2E1 and CYP3A4 are responsible for metabolizing most clinically important drugs!

© 2006 American Medical Association. All rights reserved
Polymorphic!Cytochrome!P-450s!

Effect of Metabolic Rate on Drug Dosage!
© 2006 American Medical Association. All rights reserved

Warfarin: Significant Problems for Rats!!

Warfarin: Significant Problems for Humans!!
• Ranks #1 in total mentions of deaths for drugs causing adverse events (from death certificates)
• Ranks among the top drugs associated hospital emergency room visits for bleeding
• Overall frequency of major bleeding range from 2% to 16% (versus 0.1% for most drugs)
• Minor bleeding event rates in randomized control trials of new anticoagulants has been as high as 29% per year.

Warfarin: Significant Problems for Humans!!
• Case Report July 2, 2008!– Company director dies of brain hemorrhage
after heading a football!– Consultant neurosurgeon told the inquest
the warfarin effect was probably the cause of the death!
– It can happen to anyone!!
• Other Warfarin Patients!• Case Report July 2, 2008!
– Joseph Stalin!

Why Maintaining Warfarin"Therapeutic Range is Critical!
European Atrial Fibrillation Trial Study Group, N Engl J Med 1995;333:5-10.!

Finding Doses to Maintain Therapeutic Anticoagulation is Largely Trial and Error!

Warfarin Levels Depend on Two Enzymes – CYP2C9 & VKORC1!

Estimated Warfarin Dose (mg/day) Based on Genotypes!

Frequency of VKORC1 Alleles"in Various Populations!
Sconce et al. Blood 2005, Yuan et al. Human Mol Genetics 2005, Schelleman et al. Clin Pharmacol Ther 2007, Montes et al Br J Haemat 2006!

Genetic Analysis Permits!
• More rapid determination of stable therapeutic dose.
• Better prediction of dose than clinical methods alone.
• Applicable to the 70-75% of patients not in controled anticoagulation centers.
• Reduces between 4,500 and 22,000 serious bleeding events annually.
• Genetic testing now required by FDA

Another Anticoagulant Clopidogrel (Plavix) and CYP2C19 Alleles!

"!
23andMe!Drug Response!Reports!

What are Targeted Drugs?!• Often, drugs are only effective in specific “sub-
populations” (responders). • Early identification of responders can have a
dramatic effect of treatment success. • Treatment of non-responders puts these
individuals at unnecessary risk of adverse events, while providing no benefit.
• Personalized Medicine allows the identification of responders and non-responders for targeted therapies.
• This is happening today!


Personalized Drugs!• Hercep*n (breast cancer, target: Her2/neu) • Erbitux (colorectal cancer, target: EGFR) • Tarceva (lung cancer, target: EGFR) • Straeera (aeen*on-‐deficit/hyperac*vity
disorder, Metabolism: P4502D6) • 6-‐MP (leukemia, Metabolism: TPMT) • An*virals (i.e. resistance based on form of HIV)
• etc. and the list is growing rapidly ...

FDA Requires Genetic Tests"for Certain Therapies!
Courtesy of Michelle Whirl-Carillo!

Roche Chip for Cytochrome P450"Genes: CYPC19 and CYP2D6 !
Xie and Frueh, Pharmacogenomics steps toward Personalized Medicine, Personalized Medicine 2005, 2, 325-337!

AMA Course on Pharmacogenomics and Personalized Medicine!
http://ama.learn.com © 2006 American Medical Association. All rights reserved

I. Key Concepts and Terms
154
Monogenic: due to allelic variation at a single gene Polygenic: due to variations at two or more genes Polymorphic: frequently occurring monogenic variants occurring at a frequency >1%

Normal Distribution
155
Freq
uenc
y
Activity

Polymorphic Distribution
156
From Pratt WB,Taylor P. Fig 7-5b

157
GENETIC POLYMORPHISMS
Pharmacokinetic Pharmacodynamic • Transporters • Plasma protein binding • Metabolism
• Receptors • Ion channels • Enzymes • Immune molecules

158
From: Evans WE, Relling MV. Pharmacogenomics: Translating functional genomics into rational therapeutics. Science 286:487-491, 1999.

II. Genetic polymorphisms in drug metabolizing enzymes
From: Evans WE, Relling MV. Pharmacogenomics: Translating functional genomics into rational therapeutics. Science 286:487-491, 1999.

O C CH2CH2
O
(H3C)3NH2CH2C COO CH2CH2N(CH3)3
+ +
SUCCINYLCHOLINE
160
A. Atypical Plasma Cholinesterase
• a rapid acting, rapid recovery muscle relaxant - 1951 • usual paralysis lasted 2 to 6 min in patients • occasional pt exhibited paralysis lasting hrs • cause identified as an “atypical” plasma cholinesterase
Hydrolysis by pseudocholinesterase
choline succinylmonocholine

161
• Atypical plasma cholinesterase has 1/100 the affinity for succinylcholine as normal enzyme • occurs in 1:2500 individuals • tested clinically via the abilityof dibucaine to inhibit esterase hydrolysis of benzoylcholine
020406080
100
-6 -4log molar dibucaine conc.
% In
hibi
tion
Typical Atypical
Adapted from: Pharmac Ther 47:35-60, 1990.
normal enzyme inhibited > 70% abnormal inhibited < 30%

162
• Atypical plasma cholinesterase has 1/100 the affinity for succinylcholine as normal enzyme • occurs in 1:2500 individuals • tested clinically via the abilityof dibucaine to inhibit esterase hydrolysis of benzoylcholine • Family studies indicate variability in plasma cholinesterase activity consistent with 2 allelic, autosomal, codominant genes • other variant forms exist as well

163
B. Glucose-6-phosphate dehydrogenase activity Effects >100 million worldwide
R-NH2 CYP MPO PGH Synthase
R-NOH
ERYTHROCYTE
R-NOH
O2 HgbFe+2
R-NO HgbFe+3
Reactive Oxygen
NADH
NAD+ MetHgb Reductase
NADPH or GSH(?)
NADP+ or GSSG(?) HMP Shunt
G-6-PD Dependent
SOD Catalase GSH Peroxidase
Detoxification
Splenic Sequestration
Hemolytic Anemia
GSH Semi-mercaptal
sulfinamide
R-NH2

164
Drugs and Chemicals Unequivocally Demonstrated to Precipitate Hemolytic Anemia
in Subjects with G6PD Deficiency
Acetanilide Nitrofurantoin Primaquine Methylene Blue Sulfacetamide Nalidixic Acid Naphthalene Sulfanilamide Sulfapyridine Sulfamethoxazole

165
INCIDENCE OF G6PD DEFICIENCY IN DIFFERENT ETHNIC POPULATIONS
Ethnic Group Incidence(%) Ashkenazic Jews 0.4 Sephardic Jews Kurds 53 Iraq 24 Persia 15 Cochin 10 Yemen 5 North Africa <4 Iranians 8 Greeks 0.7-3

166
INCIDENCE OF G6PD DEFICIENCY IN DIFFERENT ETHNIC POPULATIONS
Ethnic Group Incidence(%) Asiatics Chinese 2 Filipinos 13 Indians-Parsees 16 Javanese 13 Micronesians <1

167
C. N-ACETYLTRANSFERASE ACTIVITY
Distribution of plasma isoniazid concentration in 483 subjects after and oral dose. Reproduced from Evans DAP. Br Med J 2:485, 1960.

168
NAT1*4 NAT2*4 NAT2*5A NAT2*6A NAT2*7A
PABA PAS SMX
PA DDS SMZ
AF Modified from Grant DM. Pharmacogenetics 3:45-52, 1993

169
ETHNIC DIFFERENCES IN THE DISTRIBUTION OF ACETYLATOR PHENOTYPE
Population % Slow % Hetero Fast % Homo Fast
South Indians 59 35.6 5.4 Caucasians 58.6 35.9 5.5 Blacks 54.6 38.6 6.8 Eskimos 10.5 43.8 45.7 Japanese 12 45.3 42.7 Chinese 22 49.8 28.2
From: Kalo W. Clin Pharmacokinet 7:373-4000, 1982.

170
XENOBIOTICS SUBJECT TO POLYMORPHIC ACETYLATION IN MAN
Hydrazines isoniazid hydralazine phenylzine acetylhydrazine hydrazine
Arylamines dapsone procainamide sulfamethazine sulfapyridine aminoglutethimide
Carcinogenic Arylamines benzidine β-naphthylamine 4-aminobiphenyl
Drugs metabolized to amines sulfasalazine nitrazepam clonazepam caffeine

171
ADVERSE EFFECTS TO SULFASALAZINE IN PATIENTS WITH
INFLAMMATORY BOWEL DISEASE
N N
COOH
OHS
O
O
HNN
SULFASALAZINE
NH2S
O
O
HNN
H2N
COOH
OH
SULFAPYRIDINE 5-AMINOSALICYLIC ACID

172
ADVERSE EFFECTS TO SULFASALAZINE IN PATIENTS WITH
INFLAMMATORY BOWEL DISEASE
Data from: Das et al. N Engl J Med 289:491-495, 1973.
Side Effect cyanosis hemolysis transient reticulocytosis
Frequency of side effect Slow Acetylators Fast Acetylators
9 1 5 0 6 0

173
0
20
40
60
80
100
120
0 20 40 60 80 100
Duration of Therapy (months)
% o
f pts
with
lupu
s
Slow AcetylatorsFast Acetylators
Relationship Between Onset of Lupus Syndrome in Fast and Slow Acetylators Receiving Procainamide. Data
from: Woosley RL, et al. N Engl J Med 298:1157-1159, 1978.

174
NH2C
O
(H3CH2C)2NH2CH2CHN
PROCAINAMIDE
NHC
O
(H3CH2C)2NH2CH2CHN CCH3
O
NHOHC
O
(H3CH2C)2NH2CH2CHN
NATCYP450
PROCAINAMIDE HYDROXYLAMINE N-ACETYLPROCAINAMIDE
175
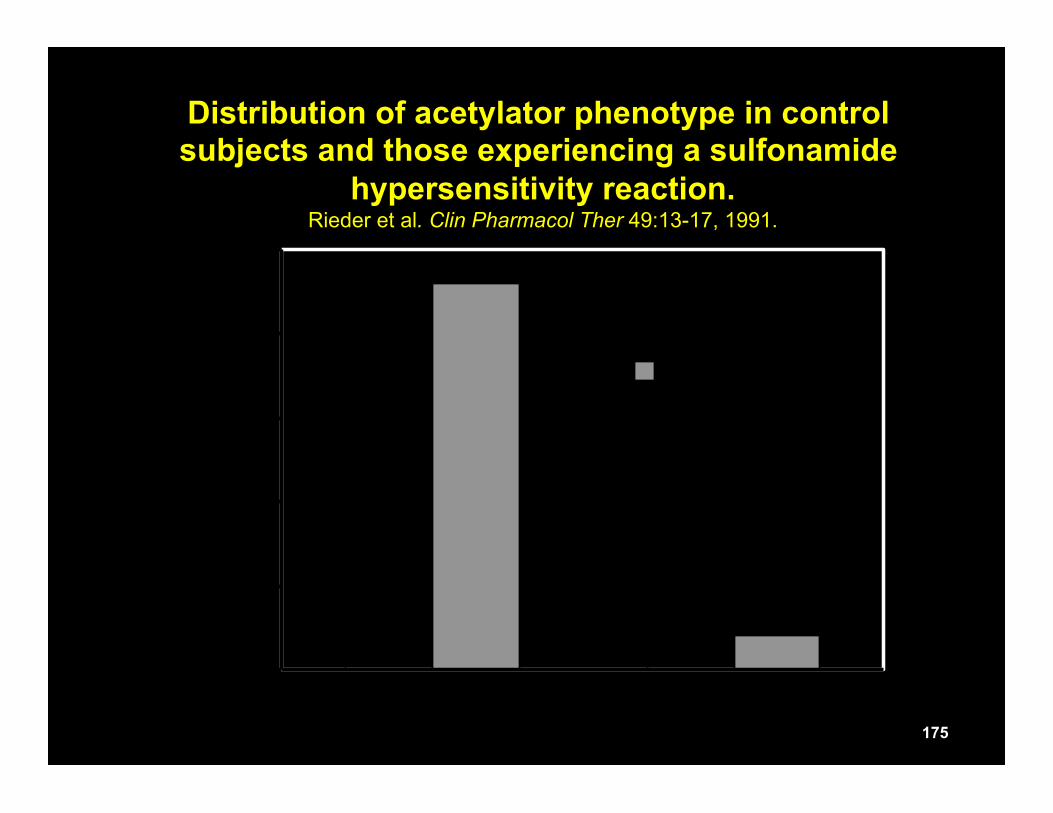
0
20
40
60
80
100
SLOW FAST
Perc
enta
ge o
f Sub
ject
s ControlHS
Distribution of acetylator phenotype in control subjects and those experiencing a sulfonamide
hypersensitivity reaction. Rieder et al. Clin Pharmacol Ther 49:13-17, 1991.

176
NAT1 N-acetyl-SMX UDPGT SMX-glucuronide
CYP2C9 MPO PGH SYNTHASE
SMX hydroxylamine Nitroso Detox
Covalent binding to cellular macromolecules/
cytotoxicity
Hypersensitivity/ Adverse Reaction
O-acetylation
Acetoxy ester
NAT1 Hydroxamic acid N,O-AT
Detoxified metabolite
Sulfamethoxazole(SMX)
NO
NH2 S
O
O
HN
CH3

177
D. CYP2D6 ACTIVITY
N C NH
NH2
N C NH
NH2
CYP2D6
OH
DEBRISOQUINE4-HYDROXYDEBRISOQUINE
H
N CH3
OCH3
H
N CH3
OH
DEXTROMETHORPHAN DEXTRORPHAN
CYP2D6

178

179
DRUGS WHOSE METABOLISM CO-SEGREGATES WITH DEBRISOQUINE
alprenolol amitriptyline bufuralol clomipramine codeine desipramine encainide ethylmorphine flecainide fluoxetine guanoxan imipramine metoprolol nortriptyline paroxetine phenformin propafenone propranolol

180
Plasma metoprolol concentrations in poor (l) and extensive (¡) metabolizers of debrisoquine after 200 mg of metoprolol tartrate administered orally. Redrawn from Lennard MS, et al. NEJM 307:1558-1560, 1982.

181
Dose requirements for nortriptyline in patients with different CYP2D6 Phenotypes. From: Meyer U. Lancet 356:1667, 2000.

182
O-demethylation morphine
N-demethylation norcodeine
6-glucuronidation codeine-6-glucuronide
M-6-G
M-3-G
normorphine
norcodeine- 6-glucuronide
CYP2D6
H3CO
NCH3
HO
O
CODEINE

183
Effect of Quinidine on the Analgesic Response to Codeine in Extensive Metabolizers of
CYP2D6 (Phenotyped with Dextromethorphan) Data from: Desmeules J, et al. Eur J Clin Pharmacol 41:23:26, 1991
0
5
10
15
20
Mo
rph
ine
Co
nc
(nM
)
0 1 1.5 2 2.5
Time (hr)
EMEM + Q
02468
10
Pa
in
Th
resh
old
(m
A)
0 1 2
Time (hr)
EMEM + Q

184
What is the cause of ‘hypermetabolizers’?

Debrisoquine phenotype in subjects with different CYP2D6 genotypes
Genotype # of Subjects
Metabolic Ratio
CYP2D6wt/(CYP2D6L)2 9 0.33
CYP2D6wt/CYP2D6wt 12 1.50
CYP2D6wt/CYP2D6(A or B) 9 2.14
CYP2D6B/CYP2D6B 6 48.84
185
(CYP2D6L)2 - gene duplication; CYP2D6A - single base deletion CYP2D6B - multiple point mutations
Data from: Agundez JG et al. Clin Pharmacol Ther 57:265, 1995.

186 From: Dalen P, et al. Clin Pharmacol Ther 63:444-452, 1998.

E. CYP2C9 ACTIVITY
187
Prescribed Daily Warfarin Dose and CYP2C9 Genotype
Warfarin Dose* Genotype 5.63 (2.56) *1/*1 4.88 (2.57) *1/*2 3.32 (0.94) *1/*3 4.07 (1.48) *2/*2 2.34 (0.35) *2/*3 1.60 (0.81) *3/*3
*Data presented as mean (SD) daily dose in mg
From: Higashi MK, et al. Association between CYP2C9 genetic variants and anticoagulation-related outcomes during warfarin therapy. JAMA 287:1690-1698, 2002.

188
F. THIOPURINE METHYLTRANSFERASE (TPMT)
N
N NH
N
SH
N
N NH
N
SCH3
TPMT
SAM SAH
6-mercaptopurine 6-methylmercaptopurine

189
TPMT Activity
Freq
uenc
y
Distribution of Thiopurine Methyl-transferase Activity. Reproduced from: Weinshelboum RM, Sladek SL. Am J Hum Genet 32:651-662, 1980.

190

G. GENETIC POLYMORPHISMS, MATERNAL SMOKING AND LOW BIRTH WEIGHT (LBW)
191
65% of all infant deaths occur among LBW infants, while LBW infants account for 7.6% of all live births
Reduction in birth wgt among smoking women Genotype Weight Reduction CYP1A1 AA 252 g CYP1A1 Aa/aa 520 g GST1 AA/Aa 285 g GST1 aa 642 g
Data from: Wang X, et al. JAMA 287:195-2002, 2002.

192
From: Esteller M, et al. Inactivation of the DNA-repair gene MGMT and the clinical response of gliomas to alkylating agents. NEJM 243:1350-1354, 2000.
Why are some gliomas resistant to nitrosourea alkylating agents? Evidence suggests this may be the result of an epigenetic phenomenon – one that does not involve a change in DNA sequence. MGMT – methylguanine-DNA methyltransferase Methylation of the promoter region of MGMT may silence the gene

193
From: Esteller M, et al. Inactivation of the DNA-repair gene MGMT and the clinical response of gliomas to alkylating agents. NEJM 243:1350-1354, 2000.

194
From: Esteller M, et al. Inactivation of the DNA-repair gene MGMT and the clinical response of gliomas to alkylating agents. NEJM 243:1350-1354, 2000.

195

196
Future Role of SNPs and Pharmacogenetics
SNP - Single Nucleotide Polymorphisms
……. G G T A A C T G …… ……. G G C A A C T G …...
AS of February 2001, 1.42 million SNPs had been identified in the human genome.

197
Patients with efficacy in clinical trials
Patients without efficacy in clinical trials
Predictive of efficacy
Predictive of no efficacy


















