Family Medicine Review Committee Update PDW June … · Family Medicine Review Committee Update PDW...
83
Family Medicine Review Committee Update PDW June 12, 2011 James Martin, MD, Chair, RC-FM Lynne Meyer, PhD, MPH, Executive Director, RC-FM
Transcript of Family Medicine Review Committee Update PDW June … · Family Medicine Review Committee Update PDW...
Family Medicine Review Committee Update
PDWJune 12, 2011
James Martin, MD, Chair, RC-FMLynne Meyer, PhD, MPH, Executive Director, RC-FM

Objectives
1. Review 2009-2010 RC-FM work2. Update New Duty Hours and Maternity Care3. Discuss Resident Survey4. Discuss proposed revisions to Family
Medicine Program Requirements

ACGME and RC-FM Structure and Information
3

ACGME Organizational Chart
ACGME Committees•ExecutiveCommittee
•Committee on Finance
•Monitoring Committee
•Governance Committee
•Council of Review Committees
•Council of Review Committee Residents
•Committee on Requirements
•JournalOversight Committee
•Bylaws and PoliciesCommittee
•Committee on Innovation
•AwardsCommittee
4
RRC Composition
• 3 appointing organizations - AAFP, ABFM, AMA• 10 voting members • 6 year terms -- except resident (2 years)• Program Directors, Chairs, Faculty• Geographic Distribution
– CO, DE, IL, MA, NJ, NY, PA, SC, TX, UT• Ex-officio members from each appointing
organization (non-voting)
RRC-FM Composition – AY 2010-2011
AMERICAN BOARD OF FAMILY MEDICINEJames Martin, MD (TX) Chair Colleen Conry, MD (CO) Co-Vice ChairMichael Magill, MD (UT) James Puffer, MD (KY), Ex-officio
COUNCIL ON MEDICAL EDUCATION (AMA)Richard Neill, MD (PA) Thomas Rosenthal, MD (NY) Suzanne Allen, MD (ID)
AMERICAN ACADEMY OF FAMILY PHYSICIANSPeter Carek, MD (SC) Co-Vice Chair Robin Winter, MD (NJ)Penelope Tippy, MD (IL) Perry Pugno, MD, (KS) Ex-officio
RESIDENT MEMBERAdam Roise, MD (IA)

RRC Review of Programs
• Peer Review – 2 reviewers for core• Reviewers use the following information to determine compliance
with the requirements:
• The questions in the PIF correspond to program requirements • Reviewers present program to Committee• Committee determines degree of compliance and assigns
accreditation status along with review cycle, range of 1-5 years
program information form (PIF)
site visitor’s report
resident survey findings
board scores

Review Cycle of Cores and Subs• Historically: Review cycle of sub was aligned with core.
– If core has a three year cycle, the sub (s) will have a three cycle. – The cycle of the sub did not exceed that of the core
• Now: RRC has un-coupled subs cycle from that of core. – Subs are still considered dependent, but the cycle of the sub can
exceed that of the core.
• ACGME document: Applying in seven easy steps: http://www.acgme.org/acWebsite/home/accreditation_application_process.asp
New Core Applications New Subspecialty Applications•Rare events•Site Visit required•12 month process•Maximum of a 3 yr cycle
•More regular occurrence•No site visit required•Need 2 months prior to meeting (agenda closing date)•Maximum of 3 yr cycle
Citation• Citation = the program has not provided evidence of compliance
with the requirements, or, an area identified by the site visitor is non-compliant

For Core Family Medicine Programs in AY 09/10, there were….
• 452 accredited programs• Specialty Length = 3 years
• 9,996/10,449 filled resident positions• Average Program Cycle Length = 4.16
• 441 programs with continuing accreditation• 9 programs with initial accreditation• 2 programs with probation
Summary of RRC Activities in AY 2009/2010• The RRC meets three
times a year – January, May, September
• During AY 2009/2010, the Committee reviewed 186 programs– Average per meeting:
• 42 core programs• 18 fellowship programs• 8 non-status
(progress & duty hours reports)

Accreditation Decisions in AY 2009/2010Core Family Medicine
Summary of Status Decisions Initial Accreditation 3
Continued Accreditation 102
Proposed Adverse Actions
4
Confirmed Adverse Actions
3
Voluntary Withdrawal 0
Total 112
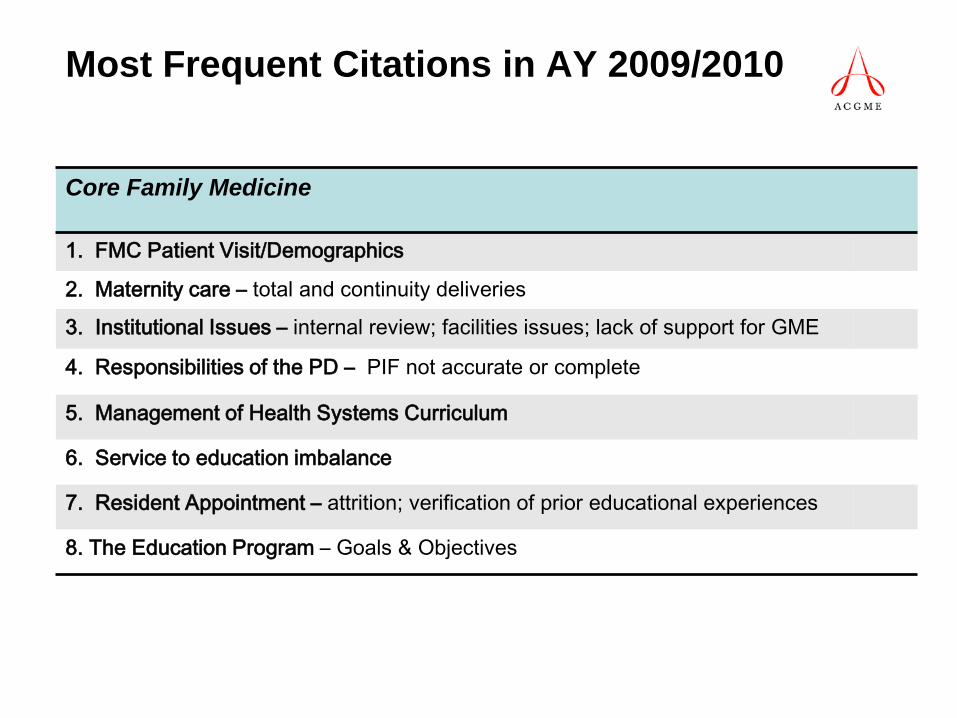
Most Frequent Citations in AY 2009/2010
Core Family Medicine
1. FMC Patient Visit/Demographics
2. Maternity care – total and continuity deliveries
3. Institutional Issues – internal review; facilities issues; lack of support for GME
4. Responsibilities of the PD – PIF not accurate or complete
5. Management of Health Systems Curriculum
6. Service to education imbalance
7. Resident Appointment – attrition; verification of prior educational experiences
8. The Education Program – Goals & Objectives

Accreditation Decisions in AY 2009/2010Subspecialties of Family Medicine
Summary of Status Decisions
Initial Accreditation 26
Continued Accreditation 27
Proposed Withhold 4
Proposed Withdrawal 0
Voluntary Withdrawal 0
Voluntary Withdrawal of Application
0
Total 57
GM – 10 programs; SM – 29; HPM – 18

For Geriatric Medicine Programs in AY 2009/2010, there were….
• 45 accredited programs• Specialty Length = 1 year
• 74/114 filled resident positions• Average Program Cycle Length = 4.21
• 33 programs with continuing accreditation• 12 programs with initial accreditation

Most Frequent Citations during AYs 08/09 – 09/10
Subspecialty of Geriatric Medicine1. Evaluation of the Program – not done annually; residents and
faculty don’t provide written, confidential evaluation; no evidence of action plan to address deficiencies; low board pass rate, not clear how this outcome data is used to improve the program
2. Scholarly Activities -- little or no faculty involvement in scholarly activity; fellow participation in scholarly activity not supported
3. Curriculum – missing or inadequate curricular components4. Sponsoring Institution -- timing of internal reviews

For Sports Medicine Programs in AY 2009/2010, there were….• 109 accredited programs• Specialty Length = 1 year
• 175/198 filled resident positions• Average Program Cycle Length = 4.27
• 89 programs with continuing accreditation• 20 programs with initial accreditation

Most Frequent Citations during AYs 08/09 – 09/10
Subspecialty of Sports Medicine1. Evaluation of Residents – documentation of ability to practice competently and
independently; multiple evaluators2. Evaluation of Program -- not done annually; residents and faculty don’t provide written,
confidential evaluation; no evidence of action plan to address deficiencies; documentation of annual meeting, composition of program evaluation committee
3. Institutional Support-Sponsoring Institution – timing of internal review; internal review committee member composition; education on fatigue;
4. Scholarly Activities -- little or no faculty involvement in scholarly activity; fellow participation in scholarly activity not supported; structured conferences such as research conferences and journal club
For Core Hospice and Palliative Medicine Programs in AY 2009/2010, there were….
• 72 accredited programs• Specialty Length = 1 year
• 153/206 filled resident positions• Average Program Cycle Length = 2.98
• 1 program with continuing accreditation• 71 programs with initial accreditation

Most Frequent Citations during AYs 08/09 – 09/10
Subspecialty of Hospice and Palliative Medicine1. Educational Program: Patient Care Experience: Care of infants, etc. – inadequate
pediatric experience due to volume – inpatient; outpatient2. Educational Program: Patient Care Experience: Other – inadequate experiences in
inpatient and long-term care; inadequate duration of experience; limited range of diagnoses; treatment to the bereaved
3. Curricular Development: Other – Long-term care; ambulatory care; interdisciplinary team/hospice
4. Scholarly Activities -- little or no faculty involvement in scholarly activity; limited fellow participation in scholarly activity

Duty Hour Information
21

Duty Hours Update1. Implementation Date: July 1, 20112. ACGME/RC-FM inconsistencies
• The RC will use ACGME wording– VI.G.5.a) PGY-1 residents should have 10 hours, and
must have eight hours, free of duty between scheduled duty periods.
– Intermediate-level residents [PGY-2] should have 10 hours free of duty, and must have eight hours between scheduled duty periods. They must have at least 14 hours free of duty after 24 hours of in-house duty.
3. Program documentation: actual vs. attestation4. Allowance of continuity experiences with
sufficient educational value.
Duty Hours – Duty Free Time
• MUST have 8 hours free of duty between scheduled duty periods
• SHOULD have 10 hours free of duty between scheduled duty periods – “Should” require a rationale if not done
• Non-violations for special continuity experiences
23

Complement Change Request Information
24

Complement Increases• Temporary complement increases: more than 3 months;
one position per year. – Note: Temporary complement requests are intended for
circumstances such as leaves of absence, remediation, off-cycle residents, etc. Temporary increases should be limited to one position per year unless unique circumstances such as accommodating residents from closed programs occur.
• RC-FM Approval: All temporary requests more than 1 per year and all permanent complement increase requests (including new federally funded programs or positions)
25

Complement Increases cont’d
• When reviewing requests, the RC-FM will pay particular attention to:– Board Scores and related previous citations– Patient Population Volume and Space and related
previous citations– Resident Survey Results– Educational Rationale: This must include why the
change is a benefit to the residents and to the program
26

Resident Survey Information
27

Resident Surveys
• Now Annual• RC Review Areas
– Duty Hours– Educational Content– Evaluation– Faculty– Resources


Sample Resident Survey Threshold Report Program Profile
ACGME Response
Proposal is for action required for programs more than 1 standard deviation from norm in 3 or more domains.
1St year-Letter to PD to develop improvement plan
2nd year-Letter requesting implementation and outcomes data
3rd year-Possible change in cycle length

Family Medicine 2010 Programs Threshold Violations
5-categories4-categories3-categories2-categories1-category
3 programs16 programs17 programs32 programs80 programs

Maternity Care Information
33

Care of the Pregnant PatientCare of the pregnant patient: Residents must have an experience in maternity care that includes a structured curriculum in prenatal, intra-partum and post-partum care. Residents must have a maternity care experience sufficient to:
-Recognize abnormal from normal pregnancy;-Care for common medical problems arising from pregnancy or
coexisting with pregnancy and assisting a patient experiencing a spontaneous precipitous birth;
-Demonstrate basic skills in managing obstetrical emergencies;-Complete a minimum of 20 deliveries; and,-Document 200 hours of labor and delivery experience, or two
blocks/months dedicated to participating in deliveries, prenatal care and post-partum care.
34

Care of the Pregnant Patient cont’dResidents may elect an advanced level of education in maternity care. Each resident wanting to achieve an advanced level must:
-Perform prenatal care,-Independently manage labor and delivery patients, including:
»Intra-partum care that includes conduction of a spontaneous vaginal delivery and management of common intra-partum complications and emergencies;»assisted deliveries (vacuum and forceps);»first assist at Caesarean section or vaginal operative deliveries; and,»obstetrical emergencies
-Perform post-partum care, including management of post-partum complications.-Perform a program total of 80 documented vaginal deliveries in a designated labor and delivery area, including a total of 10 continuity deliveries; and-Document a program total of 400 hours of labor and delivery experience or four blocks/months dedicated to resident performance of maternity care
35

Maternity Care
All programs training residents in an advanced level of education in maternity care should have at least one family physician delivering and teaching maternity care

Maternity Care Requirement Revision Process Tentative Timeline
• Review by RC-OB -- May 2011• 45 Day Posting for Public Comment (includes
impact statement and FAQs) – Summer 2011• Submission to Committee on Requirements –
Fall 2011• Approval by Committee on Requirements –
Early 2012 (programs may begin implementation of new maternity guidelines once approved)
37

Core Program Requirement Information
38

Revisions Preparation
• Prior Requirements (back to 1969 originals)• Educational papers regarding curricular needs,
educational strategies, and competency-based training and assessment
• Recommendations from AFMRD, RPS, ABFM, AAFP
• Interviews with FM thought leaders, health policy writers, other stakeholders.
39

Revision Preparation Findings
• Family Medicine not well recognized by stakeholders
• Family Medicine not well respected academically by some other disciplines
• Concern over board failure rates• Policy maker expectations
– Quality– Continuity– Expertise in PCMH
40

Family Medicine Program Requirements Revisions Strategy
1. Reemphasis on basic tenets (continuity, comprehensive care, etc.) for plurapotential graduate
2. Emphasis on FM role in healthcare reform
3. Emphasis on continuity and personal relationships

Family Medicine Program Requirements Revisions Strategy
4. Emphasis on medical home competency5. Increase flexibility6. Commitment to excellence, not minimal
standards

Areas of Revision: Institutional Issues
• PD salary support (Provide at least 70% salary support (at least 27 hours per week) for the program director as protected time to the program for administrative and non-teaching duties related to the program)
• Electronic Health Records (must)• Emphasis on quality and patient safety• Emphasis on professionalism

Program Director
• ABFM certification (if approved by ACGME Board of Directors in 2013, then must have by effective date of new program requirements)
• Faculty experience (5 years, or 4 years + NIPDD)
• Residency dedication in non-direct patient care

Faculty
• Core faculty commitment– Full time (24 hrs/wk commitment to non-
direct patient care)– Specific hours commitment– Protected administrative time
• MOC or parallel structure

Curriculum• Continuity panel• 1650 face to face encounters (plus telephone,
e-visit, group visits, etc.)• Documentation toward competency in
medical home skills• New emphasis on community and mental
health integration• Continued emphasis on hospital experiences• Continued emphasis on care of children• New procedures requirement

Required Clinical Experiences
• Family Medicine is a primary care specialty which demonstrates high quality care within the context of a personal doctor-patient relationship and with an appreciation for the individual, family and community connection.
• Continuity of comprehensive care for the diverse patient population family physicians serve is foundational to our specialty.
• Access, accountability, effectiveness and efficiency are essential elements of our discipline.
• Furthermore, the coordination of patient care within the current complicated health care arena is another vital role for the family physician.
• In order to fully prepare family physicians for the future, residency training programs should not only meet but exceed the following criteria.

Required Experiences cont’d
• 1 block/month = 100 hours (125 patient encounters)• 1 patient encounter = the continuous care of a
unique patient during a one day time period over hospitalization
• The following listed requirements include patient numbers that are in addition to the minimum of 1650 Family Medicine Practice (FMP) patient encounters unless otherwise specified
• If a FMP has adequate volume above the required minimum of 1650 continuity patients, these numbers may be met in an FMP.

Required Experiences cont’d
Required Experiences RequirementElectives 3 blocks/300 hoursCare of surgical patient 1 block/100 hoursCare of patient with musculoskeletal problems (with a documented Sports Medicine experience)
2 blocks/200 hours or 250 patient encounters
Care of the acutely ill or injured adult patient
2 blocks/200 hours or 250 patient encounters
Hospitalized adults 6 blocks/600 hours AND 750 patient encounters including 15 ICU patients
Female reproductive health 1 block/100 hours or 125 patient encounters
Management of Health Systems 1 block/100 hours

Required Experiences cont’d
Required Experiences RequirementIll children/adolescents 2 blocks/200 hours AND 250 patient
encounters including a minimum of 75 inpatient encounters and a minimum of 75 emergency department patient encounters
Newborns 40 patient encountersAmbulatory children/adolescents 2 blocks/200 hours or 250 patient
encounters

Required Experiences cont’d
Required Experiences RequirementPregnant patient 2 blocks/200 hours AND 20 deliveriesAdvanced level of maternity care elective
(Programs are not required to offer this elective. Residents should be informed as applicants whether this elective will be available.)
4 blocks/400 hours AND 80 deliveries including 10 continuity patient deliveries.
This is includes the 2 blocks/200 hours and 20 deliveries during the required maternity care experience.
FMP Demographics 1650 patient encounters.
10% of FMP patient visits must be between the ages of 0-9 years, and an additional 10% of FMP patients must be 60 years of age or older.

Required Experiences cont’dRequired Experiences RequirementOlder patient 1 block/100 hours or 125 patient
encounters.
This experience can occur in various settings such as long term care, assisted living, home care, or day care. It must include at least one home visit and a continuity experience of caring for at least two patients for 24 months in one of the settings listed above. If a skilled nursing facility is not used, the PD must describe how residents learn about the care of patients in a skilled nursing facility.
Adult inpatient encounters cannot be counted for this requirement.
Required Procedures•Anoscopy•Chest x-ray interpretation•Cryosurgery•EKG Interpretation•Endometrial biopsy•Eye fluorescein exam•Incision and drainage of abscess•Immobilization and stabilization of severe sprains•Immobilization and stabilization of non-displaced fractures
Required Procedures cont’d•Injection and aspiration of joints•Injection and aspiration of tendons, ligaments and muscles•Pap smear•Simple laceration repair with sutures•Skin biopsies: punch, excisional, incisional•Splints•Wart, fingernail, toenail, and foreign body removal•Wet Mount
Medical Home1. Personal relationships and communication
ability2. Teams training3. EHR competency4. Leadership in care coordination and chronic
disease management5. Ongoing quality and performance
improvement6. Community needs assessment and practice
modification

Scholarly Activities
56
• Scholarly Activity: – Shared by peers and contributes to knowledge– Evaluation component
• Faculty: regional or national level• Residents: local, regional or national level
• Local – at institution• Regional – outside the institution
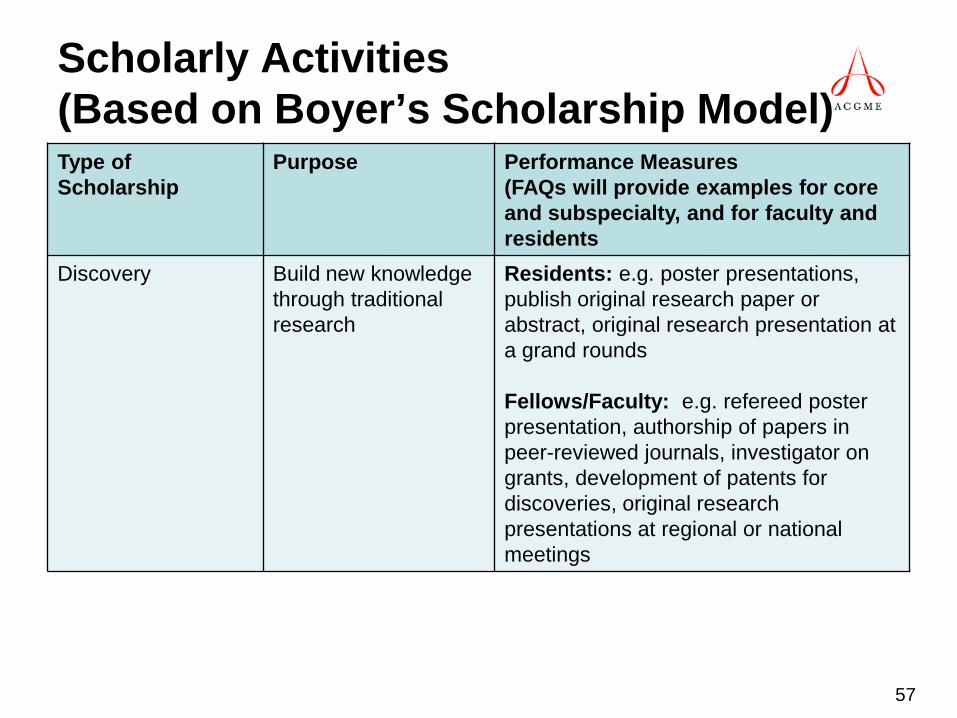
Scholarly Activities (Based on Boyer’s Scholarship Model)Type of Scholarship
Purpose Performance Measures(FAQs will provide examples for core and subspecialty, and for faculty and residents
Discovery Build new knowledge through traditional research
Residents: e.g. poster presentations, publish original research paper or abstract, original research presentation at a grand rounds
Fellows/Faculty: e.g. refereed poster presentation, authorship of papers in peer-reviewed journals, investigator on grants, development of patents for discoveries, original research presentations at regional or national meetings
57

Scholarly Activities (Based on Boyer’s Scholarship Model)Type of Scholarship
Purpose Performance Measures(FAQs will provide examples for core and subspecialty, and for faculty and residents
Integration Synthesize current knowledge to make it useful to others
Residents: e.g. case study and literaturereview presentation at local Grand Rounds, lead local patient education conference series, publish an op-ed in local newspaper regarding current public health concern, letter to editor of national medical journal analyzing results of a paper published by others
Fellows/Faculty: e.g. publish a POEM, publish a clinical review paper in peer-reviewed national journal, testify in state legislature regarding public health problem strategy, serve as editor for a state or national medical journal
58

Scholarly Activities (Based on Boyer’s Scholarship Model)Type of Scholarship
Purpose Performance Measures(FAQs will provide examples for core and subspecialty, and for faculty and residents
Application (FM Focus)
Use knowledge to improve health care, medical practice, health systems operations, public health or policy
Residents: e.g. present the design and resultsof a clinical quality improvement project; local publication of design, implementation and effects of a patient education program, risk behavior, or chronic disease management in a residency newsletter
Fellows/Faculty: e.g. present results of clinical QI program implemented in a group of practices at a regional professional meeting, present results of a practice-based research network at a national professional meeting; serving on a state or national committee developing and implementing programs to improve medical practice or education; obtainment of grant funding for practice improvement or redesign
59

Scholarly Activities (Based on Boyer’s Scholarship Model)Type of Scholarship
Purpose Performance Measures(FAQs will provide examples for core and subspecialty, and for faculty and residents
Teaching Development, implementation and evaluation of educational curriculum, courses, program, materials,and so forth for educational purposes.
Residents: e.g., preparation of an enduring curriculum for use in a residency program (needs assessment, goals and objectives development, activities, evaluation process, implementation and summarization of pilot results
Fellows/Faculty: e.g., obtain Title VII grant funding to implement new curriculum; develop, implement and report to sponsoring professional organization a new curriculum for a national professional educational course or module; publish evaluation of a new curriculum in a peer-reviewed journal
60

Program Requirement Revision Process Algorithm
Abbreviations used:• AST = Accreditation Standards Team• CoR = ACGME Committee on Requirements• EDAS = Executive Director, Accreditation Standards• EDRC = Executive Director, Review Committee• PIF = Program Information• RC = Review Committee• RDC = Requirement Development Committee
61

Program Requirement Revision Process Algorithm
1.The RDC staff prepares a worksheet identifying each requirement.2. The RDC conducts an initial review of the existing requirements and
PIF.3.The RC requests preliminary review and comment on the existing
requirements and PIF from the community either via the ACGME eCommunication or an alternative method(s).
4.The EDAS and the RDC Chair meet with the EDRC to discuss the RDC’s comments.
62
Program Requirement Revision Process Algorithm
5. The RC or a subcommittee reviews the input received from the community and the RDC, proposes revisions to the requirements and addresses the RDC’s concerns/comments. A member of the RDC provides assistance as requested.
– Additional information pertaining to the requirements, such as definitions, that will be provided in an FAQ should be developed at the same time the requirements are revised.
– The RC should also consider the impact that any substantive changes to the requirements may have on education, patient care, resources and other services/programs. These will need to be addressed in the Impact Statement.
– The RC should also review the respective Board requirements to ensure that there is no conflict with the program requirements that would result in a graduate not being Board eligible.
63

Program Requirement Revision Process Algorithm
6.The RC staff returns the worksheet with the RC’s responses to the RDC’s comments along with a copy of the annotated, revised requirements and a clean copy of the revised requirements.
7.The full RDC reviews the worksheet and revised requirements to ensure that all concerns have been satisfactorily addressed. If concerns remain, the RDC Chair communicates those to the EDRC.
8.Work on an impact statement begins. Work on a revised PIF begins. Work on FAQs continues.
9. The EDRC submits the RDC-approved draft of the revised requirements and the impact statement to the AST.
10.The AST editor reviews the requirements document. If any changes are made, the document is sent to the EDRC for approval.
64

Program Requirement Revision Process Algorithm
11.The proposed requirements and the impact statement are posted for review and comment.
12.The RC reviews the comments received, provides a response to each substantive comment, and revises the requirements accordingly. FAQs should be revised and/or new FAQs should be developed as needed.
13.RC staff returns revised requirements, revised PIF (and other data compliance sources when appropriate), and FAQ to RDC Chair.
14.Full RDC reviews all documents to ensure all concerns have been met. If concerns remain, the RDC Chair communicates those to the EDRC.
65

Program Requirement Revision Process Algorithm
15.The final draft of the requirements, impact statement, RC’s response to comments received, copies of correspondence and copies of any FAQs related to the requirements are submitted to the EDAS for CoR review and approval.
16.A CoR member reviews the material submitted and provides comment.
17.The RC Chair and EDRC respond to the comments.18.Approximately 2 weeks prior to the CoR meeting, the CoR meets in
a closed executive session via conference call to review the requirements, comments and responses. Any additional concerns are communicated to the EDRC.
66
Program Requirement Revision Process Algorithm
19.The RC Chair and EDRC attend the CoR meeting and present their responses to the CoRs concerns.
20.Once approved by the ACGME Board of Directors, the requirements and FAQ, as well as the new PIF, are finalized by the AST staff. The EDRC reviews and approves the final documents prior to posting.
67

Core Program Requirement Revision Process Tentative Timeline
• May 2011 – Revised PRs submitted for 1st Full RDC Review in May 2011 (Steps 6 and 7)
• 45 Day Posting for Public Comment – Late 2011 (Step 11)
• 2nd Full RDC Review – Mid 2012 (Steps 13 and 14)• Submission to Committee on Requirements – Fall
2012 (Step 15)• Approval by Committee on Requirements – Early 2013
(Steps 19 and 20) (Programs will be given time to implement new approved program requirements)
68

RC-FM Issues
69

Committee Issues• Commitment to a higher bar of expectations• Assure the safety and quality of care rendered to
patients in our teaching hospitals today• Assure the safety and quality of care rendered to
patients of our current residents in their future independent clinical practice
• Assure the provision of a safe and humanistic educational environment for our residents to learn and demonstrate professionalism and subordination of self interest
70

Committee Issues cont’d• Philosophical shift in educational emphasis
– Critical thinking skills– Process improvement
• Balance of time/numbers vs. competency assessment
• Efforts to increase transparency to program directors
71

Quality of Programs and Graduates
• Issue raised by other stakeholders• Future healthcare system requirements • Deteriorating graduate performance on
ABFM exam• Chronic poorly performing programs

Raising the Bar for Accreditation
• Short cycle programs• Board score thresholds• Recruiting deficiencies• Institutional support and resources• Weighting citations

RC-FM Philosophy 2011
• Flexibility but clear concept of anticipated responses and results
• Transparency• Committee Member involvement in ACGME
communications• Focus on process improvement• Commitment to excellence
Future Projects
• Integration of Milestones Project• 1-2 programs and rural programs• 3 years vs. 4 years of training
75

Recognized Concerns
• Program Resources to capture resident activity
• Numbers requirement with limited EBM• Incorporating Milestones competencies
when developed
76

Resources
77

ACGME Data Collection
• All core programs and all subspecialty programs (with 4 or more fellows) will be required to participate in the resident survey ANNUALLY
• More information is being/will be collected through ADS– Common PIF = Questions all programs need to complete
• Information on faculty/teaching staff• Residents/fellows - # completed; # transfer, withdraw; dismissed
– Responses to previous citation– Evaluation (resident, faculty and program)– Duty hours – Complement increases, PD/Institution changes– Voluntary withdrawal
RRC CommunicationsNewsletter
• Communication tool implemented in 2007
– Enhances communication between the RRC and the Family Medicine community
– Provides updates on RRC and ACGME initiatives
• Sent to all core and subspecialty program directors, coordinators, and designated institutional officials
• Sent 1 – 2 times per year• Newsletter postings announced in the weekly
e-communications email

ACGME Communications
• Weekly e-communication– Contains GME information: New requirements, newsletters; updates on
ACGME issues/initiatives• E-mail status of programs on RRC agenda
– 5 business days after meeting will receive email w/status and review cycle.
• E-mail notification when letter is available on Accreditation Data System (ADS) – Hard copies of letters not provided – Letter is posted within 60 days following the meeting
• E-mail notification of site visit date – For questions related to site visits contact:
• Ingrid Philibert: (312) 755-5003, [email protected]• Jane Shapiro: (312) 755-5015, [email protected]• Penny Lawrence (312) 755-5014, [email protected]

Program ResourcesProgram Director Guide
• Common competency questions inserted in all specialty PIFs (common but not hard-wired into ADS as in Part I of the PIF).
• PD Guide to the Common Requirements: http://www.acgme.org/acWebsite/navPages/nav_commonpr.asp
• Provides PDs: – Explanations of the intent of most of the common requirements
(particularly competency-based)– Suggestions for implementing requirements and types of
documentation expected.

www.acgme.org
• ACGME Policies & Procedures• Competencies/Outcomes Project• List of accredited programs• Accreditation Data System (ADS)• Duty hours Information/FAQ• Affiliation Agreements FAQ• General information on site visit process and your site visitor• Notable Practices• Family Medicine Webpage
– Resident complement increase policy– Program Requirements and PIFs– Archive of RRC Updates/Newsletters– FAQs

Handouts
• During this presentation, you have been emailed these handouts.
• Please help us to save trees by viewing these attachments electronically during PDW.
• Thank you!
83