
Familial Risk And Pathological Outcomes Of Colorectal Cancer In An Asymptomatic General Population...
26
Familial Risk And Familial Risk And Pathological Outcomes Pathological Outcomes Of Colorectal Cancer In Of Colorectal Cancer In An Asymptomatic General An Asymptomatic General Population Cohort Population Cohort By: Michelle By: Michelle Medina Medina
-
Upload
theodore-wilkerson -
Category
Documents
-
view
220 -
download
5
Transcript of Familial Risk And Pathological Outcomes Of Colorectal Cancer In An Asymptomatic General Population...

Familial Risk And Familial Risk And Pathological Outcomes Of Pathological Outcomes Of Colorectal Cancer In An Colorectal Cancer In An Asymptomatic General Asymptomatic General
Population CohortPopulation Cohort
By: Michelle By: Michelle MedinaMedina
Simplified TitleSimplified Title
To find if heredity has anything to do To find if heredity has anything to do with the actual risk of contracting with the actual risk of contracting colorectal cancer in patients that colorectal cancer in patients that show no symptomsshow no symptoms

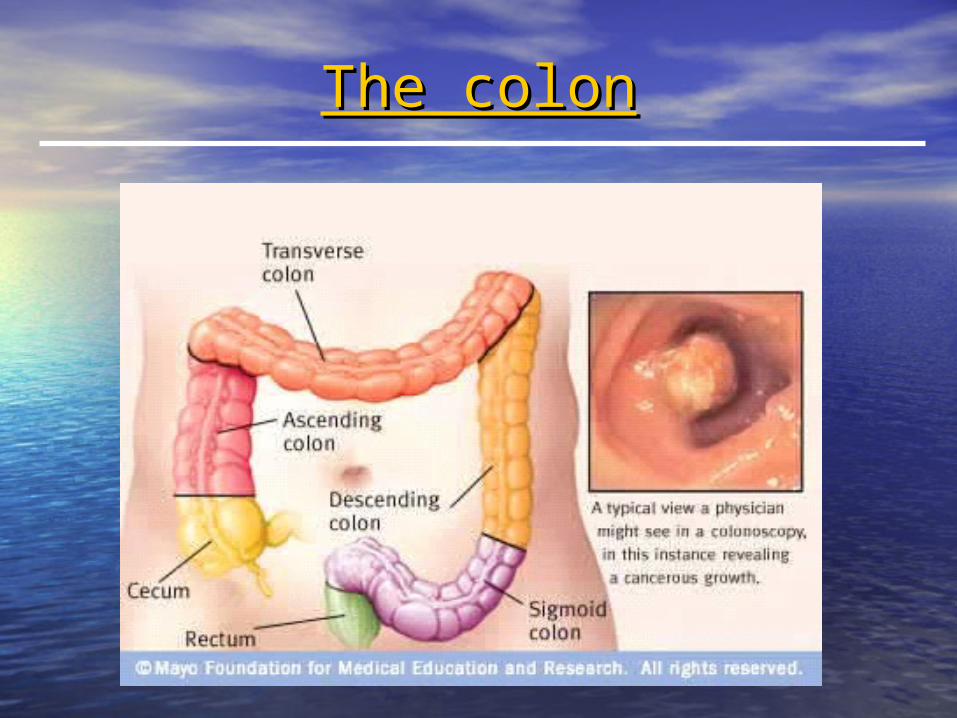
What is Colorectal Cancer?What is Colorectal Cancer?
• Colorectal cancer, also known as Colorectal cancer, also known as colon cancer or bowel cancer, colon cancer or bowel cancer, includes cancerous growths in the includes cancerous growths in the colon, rectum and appendix.colon, rectum and appendix.
• Most cases begin as small benign Most cases begin as small benign polyps. polyps.
• It is the third most common form of It is the third most common form of cancer and the second leading cause cancer and the second leading cause of death in the Western World.of death in the Western World.

Colorectal CancerColorectal Cancer

Who gets colorectal cancer?Who gets colorectal cancer?
• Everyone is affected by colorectal cancer.Everyone is affected by colorectal cancer.
• People older than fifty are more People older than fifty are more susceptible to it.susceptible to it.
• Death rates for colorectal cancer among Death rates for colorectal cancer among African Americans are about 30% higher African Americans are about 30% higher than among Whites and more than two than among Whites and more than two times higher than for Asian Americans, times higher than for Asian Americans, Pacific Islanders, American Indians, and Pacific Islanders, American Indians, and Hispanics. Hispanics.

Risk Factors of Colorectal Risk Factors of Colorectal CancerCancer
• age age
• polyp growth polyp growth
• history of cancerhistory of cancer
• heredityheredity
• virus exposure virus exposure
• diabetesdiabetes
• Crohn’s disease Crohn’s disease
• sclerosing sclerosing cholangitischolangitis
• dietdiet
• physical inactivityphysical inactivity
• alcohol alcohol consumptionconsumption
• smokingsmoking
Symptoms of Colorectal Symptoms of Colorectal CancerCancer
• change in bowel change in bowel habits habits
• blood in the stoolblood in the stool
• rectal bleedingrectal bleeding
• bowel obstructionbowel obstruction
• fatiguefatigue
• jaundicejaundice
• narrow stoolnarrow stool
• anemiaanemia
• unexplained weight unexplained weight lossloss
• hepatomegalyhepatomegaly
• gasgas
• crampingcramping
• abdominal painabdominal pain
• feeling of partially full feeling of partially full bowelbowel

Screening Methods for Screening Methods for Colorectal CancerColorectal Cancer
• FOBT – Fecal Occult Blood TestingFOBT – Fecal Occult Blood Testing
• IFOBT – Immunochemical FOBTIFOBT – Immunochemical FOBT
• Double-Contrast Barium EnemaDouble-Contrast Barium Enema
• Flexible SigmoidoscopyFlexible Sigmoidoscopy
• ColonoscopyColonoscopy
• Virtual ColonoscopyVirtual Colonoscopy

Purpose of StudyPurpose of Study
• To establish a correlation between To establish a correlation between family history of colorectal cancer family history of colorectal cancer and present cases.and present cases.
• To determine if race is a major risk To determine if race is a major risk factor for colorectal cancer factor for colorectal cancer susceptibility.susceptibility.

EligibilityEligibility
• Age 50-69 (40-69) Age 50-69 (40-69) – Men and women in ~ equal numbersMen and women in ~ equal numbers
• No prior colonoscopy or recent No prior colonoscopy or recent sigmoidoscopysigmoidoscopy
• No IBD, FAP, colorectal cancerNo IBD, FAP, colorectal cancer
• No prior use of an implanted defibrillatorNo prior use of an implanted defibrillator
• No serious comorbidityNo serious comorbidity– Exclusions: MI (past year) and other heart Exclusions: MI (past year) and other heart
problems, anticoagulants, cancer therapyproblems, anticoagulants, cancer therapy

Genetics Review CriteriaGenetics Review Criteria
• Amsterdam IIAmsterdam II– At least 3 At least 3 relatives with HNPCC associated cancers relatives with HNPCC associated cancers (one a (one a
FDR of the other two)FDR of the other two)• CRC, Endometrial, Kidney, Ovarian, Stomach, Small Bowel, Renal CRC, Endometrial, Kidney, Ovarian, Stomach, Small Bowel, Renal
Pelvis/UreterPelvis/Ureter
– At least At least 22 successive generations affected successive generations affected– At least 1At least 1 diagnosed with cancer before the age of 50 diagnosed with cancer before the age of 50– No FAP No FAP
• First DegreeFirst Degree– At least one immediate family member diagnosed with At least one immediate family member diagnosed with
colorectal cancer prior to the age of 60.colorectal cancer prior to the age of 60.
• Standard RiskStandard Risk– No outstanding family history of colorectal cancerNo outstanding family history of colorectal cancer
MethodsMethods
• Patients who have already been reviewed by Patients who have already been reviewed by the genetics review committee were the genetics review committee were analyzed.analyzed.
• Each participants’ colonoscopy results were Each participants’ colonoscopy results were queried.queried.
• Those with First Degree risk and those Those with First Degree risk and those meeting the Amsterdam II criteria were sent meeting the Amsterdam II criteria were sent high risk letters advising them to go see a high risk letters advising them to go see a genetics counselor.genetics counselor.
• Those who were at standard risk were sent Those who were at standard risk were sent standard risk letters advising them they had standard risk letters advising them they had no outstanding risk for colorectal cancer.no outstanding risk for colorectal cancer.

MaterialsMaterials
• FOBT Cards: The fecal occult blood FOBT Cards: The fecal occult blood test chemically checks your stool for test chemically checks your stool for hidden blood. hidden blood.

Materials Cont.Materials Cont.
• Flexible Sigmoidoscope: A short, Flexible Sigmoidoscope: A short, flexible, lighted tube which transmits flexible, lighted tube which transmits an image of the inside of the distal an image of the inside of the distal bowel about 60 cm into the colon.bowel about 60 cm into the colon.

Materials Cont.Materials Cont.
• Colonoscope: A thin, lighted tube Colonoscope: A thin, lighted tube used to look all around the inside of used to look all around the inside of the colon. the colon.

Materials Cont.Materials Cont.
• Baseline Questionnaires: Collects Baseline Questionnaires: Collects participants’ information.participants’ information.
Materials Cont.Materials Cont.
• Family History Questionnaires: Family History Questionnaires: Collects patients’ family history of Collects patients’ family history of cancer.cancer.

Materials Cont.Materials Cont.
• Pathology Review Form: Used by our Pathology Review Form: Used by our pathologist to review colonoscopy pathologist to review colonoscopy specimens.specimens.

Genetics Review ResultsGenetics Review Results
435435401401992525TotalTotal
193(44)193(44)182(45)182(45)3(33)3(33)8(32)8(32)Unknown Unknown Race n(%)Race n(%)
55(13)55(13)50(12)50(12)1(11)1(11)4(16)4(16)MinoritiesMinorities
n(%)n(%)
187(43)187(43)169(42)169(42)5(56)5(56)13(52)13(52)CaucasianCaucasian
n(%)n(%)
TotalTotalStandarStandard Riskd Risk
AmsterdaAmsterdam IIm II
First First DegreDegre
ee
Familial Familial RiskRisk

Genetics Review ResultsGenetics Review Results
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
First Degree Amsterdam II Standard Risk
Caucasian
Minorities
Unknown Race
Perc
enta
ge
Perc
enta
ge
of of
Part
icip
an
Part
icip
an
tsts
Familial Risk Familial Risk

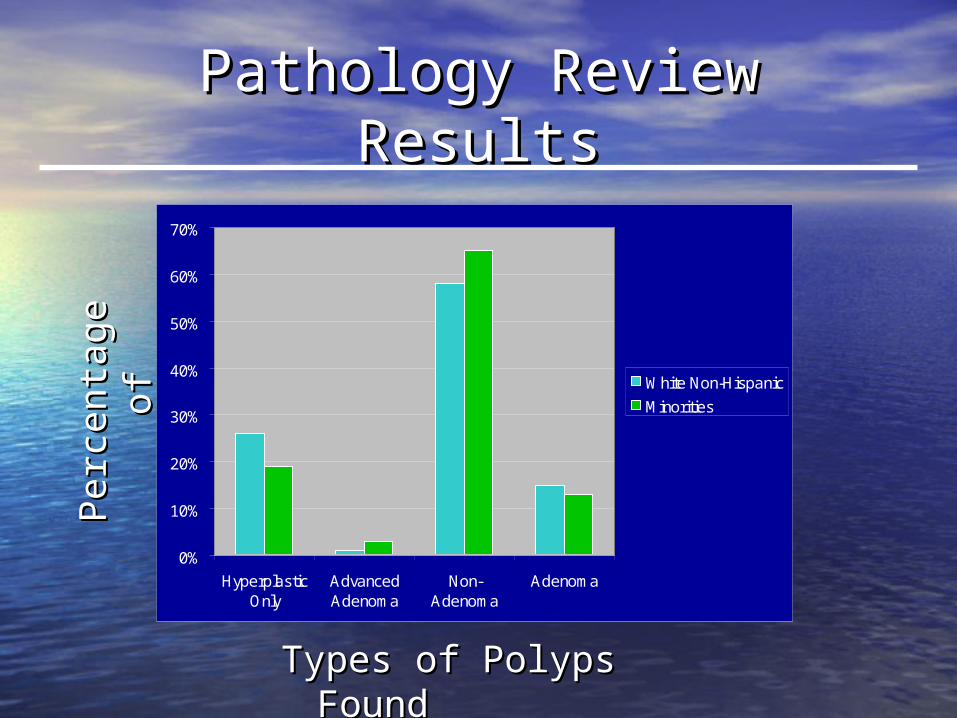
Pathology Review ResultsPathology Review Results
20820820(10)20(10)188(90)188(90)Non-Adenomas Non-Adenomas n(%)n(%)
51514(8)4(8)47(92)47(92)Adenomas Adenomas n(%)n(%)
3543543131323323TotalTotal
551(20)1(20)4(80)4(80)Advanced Advanced Adenomas Adenomas
n(%)n(%)
90906(7)6(7)84(93)84(93)Hyperplastic Hyperplastic Only n(%)Only n(%)
TotalTotalMinoritiesMinoritiesWhite Non-White Non-HispanicsHispanics
Polyp Polyp ClassificationClassification
Pathology Review ResultsPathology Review ResultsPerc
enta
ge
Perc
enta
ge
of of
Part
icip
an
Part
icip
an
ts
ts
Types of Polyps Types of Polyps Found Found
0%
10%
20%
30%
40%
50%
60%
70%
HyperplasticOnly
AdvancedAdenoma
Non-Adenoma
Adenoma
White Non-Hispanic
Minorities
ConclusionConclusion
• More data is still needed for results More data is still needed for results to be conclusive.to be conclusive.
• The National Colonoscopy Study still The National Colonoscopy Study still has three more years before it ends has three more years before it ends therefore there is still more to be therefore there is still more to be learned and much more data to be learned and much more data to be acquired.acquired.
ReferencesReferences
• Colon and Colorectal CancerColon and Colorectal Cancer. 18 July 2006 <www.medicinenet.com>. . 18 July 2006 <www.medicinenet.com>. • "Colon Cancer: Untangling Its Genetics." "Colon Cancer: Untangling Its Genetics." South African Medical Research CouncilSouth African Medical Research Council. July 2005. 17 July 2006 . July 2005. 17 July 2006
<http://www.mrc.ac.za/mrcnews/july2005/colon/html>. <http://www.mrc.ac.za/mrcnews/july2005/colon/html>. • Colon CancerColon Cancer. Mayo Clinic. 2005. 17 July 2006 . Mayo Clinic. 2005. 17 July 2006
<http://www.mayoclinic.com/health/colon-cancer/DS00035/DSECTION=7>. <http://www.mayoclinic.com/health/colon-cancer/DS00035/DSECTION=7>. • Colorectal CancerColorectal Cancer. Molecular Diagnostic Laboratory. . Molecular Diagnostic Laboratory. The Colorectal Cancer Group at MDLThe Colorectal Cancer Group at MDL. Molecular Diagnostic . Molecular Diagnostic
Laboratory. 18 July 2006 <www.mdl.dk/design/assets/images/CRC1_big.jpg>. Laboratory. 18 July 2006 <www.mdl.dk/design/assets/images/CRC1_big.jpg>. • "Colorectal Cancer." "Colorectal Cancer." WikipediaWikipedia. 28 July 2006. 17 July 2006 <http://en.wikipedia.org/wiki/Colorectal_cancer>. . 28 July 2006. 17 July 2006 <http://en.wikipedia.org/wiki/Colorectal_cancer>. • Detailed Guide: Colon and Rectum CancerDetailed Guide: Colon and Rectum Cancer. American Cancer Society. 2006. 1-5. 17 July 2006 . American Cancer Society. 2006. 1-5. 17 July 2006
<http://www.cancer.org/docroot/CRI/content/CRI_2_4_2X_What_are_the_risk_factors_for_colon_and_rectum_cancer.a<http://www.cancer.org/docroot/CRI/content/CRI_2_4_2X_What_are_the_risk_factors_for_colon_and_rectum_cancer.asp>. sp>.
• Fuchs, Charles S., Edward L. Giovannucci, Graham A. Colditz, David J. Hunter, Frank E. Speizer, and Walter C. Willett. Fuchs, Charles S., Edward L. Giovannucci, Graham A. Colditz, David J. Hunter, Frank E. Speizer, and Walter C. Willett. "A Prospective Study of Family History and the Risk of Colorectal Cancer." "A Prospective Study of Family History and the Risk of Colorectal Cancer." New England Journal of MedicineNew England Journal of Medicine 331 331 (1994): 1-13. 17 July 2006 <http://content.nejm.org/cgi/content/short/331/25/1669>. (1994): 1-13. 17 July 2006 <http://content.nejm.org/cgi/content/short/331/25/1669>.
• Iammarino, Nicholas K. Iammarino, Nicholas K. African Americans & CancerAfrican Americans & Cancer. Intercultural Cancer Council. 2001. 17 July 2006 . Intercultural Cancer Council. 2001. 17 July 2006 <http://iccnetwork.org/cancerfacts/cfs1.htm>. <http://iccnetwork.org/cancerfacts/cfs1.htm>.
• Kelley, Robert B., Frank J. Domino, and Carolyn Lopez. "Colorectal Cancer Screening." Kelley, Robert B., Frank J. Domino, and Carolyn Lopez. "Colorectal Cancer Screening." Family DoctorFamily Doctor. 2006. 17 July . 2006. 17 July 2006 <http://familydoctor.org/556.xml>. 2006 <http://familydoctor.org/556.xml>.
• Minorities and Colorectal CancerMinorities and Colorectal Cancer. Cancer Research and Prevention Foundation. Alexandria, VA, 2006. 17 July 2006 . Cancer Research and Prevention Foundation. Alexandria, VA, 2006. 17 July 2006 <http://www.preventcancer.org/colorectal/facts/minorities.cfm>. <http://www.preventcancer.org/colorectal/facts/minorities.cfm>.
• Weaver, Charles H. Weaver, Charles H. Genetiv Testing for Colorectal CancerGenetiv Testing for Colorectal Cancer. Ed. C. D. Buckner. Cancer Consultants. 2004. Sept. 2004 . Ed. C. D. Buckner. Cancer Consultants. 2004. Sept. 2004 <http://patient.cancerconsultants.com/print_tnpv.aspx?id=739>. <http://patient.cancerconsultants.com/print_tnpv.aspx?id=739>.
• "Overview: Colon and Rectum Cancer." "Overview: Colon and Rectum Cancer." American Cancer SocietyAmerican Cancer Society. 16 Mar. 2006. American Cancer Society. 11 Aug. . 16 Mar. 2006. American Cancer Society. 11 Aug. 2006 <http://www.cancer.org/docroot/CRI/content/CRI_2_2_1X_What_is_colon_and_rectum_cancer_10.asp>.2006 <http://www.cancer.org/docroot/CRI/content/CRI_2_2_1X_What_is_colon_and_rectum_cancer_10.asp>.
• "Hyperplastic Polyp." Def. 1. "Hyperplastic Polyp." Def. 1. DictionaryDictionary. 18 Aug. 2006 <http://dictionary.reference.com/browse/hyperplastic. 18 Aug. 2006 <http://dictionary.reference.com/browse/hyperplastic%20polyp>.%20polyp>.
• "Adenoma." Def. 1. "Adenoma." Def. 1. DictionaryDictionary. 18 Aug. 2006 <http://dictionary.reference.com/browse/adenoma>.. 18 Aug. 2006 <http://dictionary.reference.com/browse/adenoma>.• Cancer Can Occur Anywhere in the Colon, So It's Important to Have Screening Tests That Examine the Entire Colon.Cancer Can Occur Anywhere in the Colon, So It's Important to Have Screening Tests That Examine the Entire Colon.
Colon CancerColon Cancer. Mayo Clinic. 18 Aug. 2006 . Mayo Clinic. 18 Aug. 2006 <http://images.google.com/imgres?imgurl=http://health.yahoo.com/media/mayoclinic/images/image_popup/<http://images.google.com/imgres?imgurl=http://health.yahoo.com/media/mayoclinic/images/image_popup/colon.jpg&imgrefurl=http://health.yahoo.com/topic/other/other/article/mayoclinic/13D504C5-40A0-40DA-colon.jpg&imgrefurl=http://health.yahoo.com/topic/other/other/article/mayoclinic/13D504C5-40A0-40DA-9F61138EEAAE162F%3B_ylt9F61138EEAAE162F%3B_ylt%3DA9htfoyTUixEjRIA_y3aNs4F&h=303&w=400&sz=17&hl=en&start=7&tbnid=WenUos6fXOQcMM:&tbnh=94&tbn%3DA9htfoyTUixEjRIA_y3aNs4F&h=303&w=400&sz=17&hl=en&start=7&tbnid=WenUos6fXOQcMM:&tbnh=94&tbnw=124&prev=/images%3Fq%3DColorectal%2BCancer%26svnum%3D10%26hl%3Den%26lr%3D>. w=124&prev=/images%3Fq%3DColorectal%2BCancer%26svnum%3D10%26hl%3Den%26lr%3D>.
Acknowledgments Acknowledgments
• Victoria Serrano (our mentor)Victoria Serrano (our mentor)
• Epidemiology and Biostatistics Epidemiology and Biostatistics DepartmentDepartment
• Dr. Sat BhattacharyaDr. Sat Bhattacharya
• Harlem Children SocietyHarlem Children Society
• Memorial Sloan Kettering Cancer Memorial Sloan Kettering Cancer CenterCenter