
Fall T.I.P.S. Training - Mass General · – Discuss the role of the PCA in fall prevention ... •...
38
Fall T.I.P.S. Training
-
Upload
trinhtuyen -
Category
Documents
-
view
221 -
download
3
Transcript of Fall T.I.P.S. Training - Mass General · – Discuss the role of the PCA in fall prevention ... •...
Fall T.I.P.S. Training
Overview• Fall TIPS “Super User” Training (this presentation)
– Review the types of patient falls– Review the components of an evidence-based fall
prevention program• Universal fall precautions (all patients)• 3-Step Fall Prevention Process
1. Fall risk assessment2. Personalized fall prevention planning3. Strategies to ensure consistent implementation of
the fall prevention plan– Discuss the role of the PCA in fall prevention
• Review evidence re: Fall TIPS• Discuss roll-out of Fall TIPS
TYPES OF PATIENT FALLSIs My Patient At Risk For Falling?
Types of Falls: Preventable
Accidental falls:• Occur in those who have no risks for falling • Usually caused by environmental hazard/error
in judgment• 14% of falls
Source: Morse, J.M. (2009). Preventing patient falls. (2nd ed). New York: Springer. Published, 2009.
Prevented through universal fall precautions

Types of Falls: Preventable
Anticipated physiological falls:• Occur in those who have risk for falling• The fall risk assessment (Morse Fall Scale)
completed by the nurse every shift predicts this type of fall.
• 78% of falls
Source: Morse, J.M. (2009). Preventing patient falls. (2nd ed). New York: Springer. Published, 2009.
**Prevented through fall risk assessment,personalized care planning, and carrying out
the planned interventions consistently**

Types of Falls: Not Preventable
Unanticipated physiological falls:• Occur in those who have no risks for falling • Caused by physiologic changes
—Such as seizure
• 8% of falls
Source: Morse, J.M. (2009). Preventing patient falls. (2nd ed). New York: Springer. Published, 2009.
Most difficult to prevent. Some may not be preventable.
FALL PREVENTION STRATEGIES
Is My Patient At Risk For Falling?
Evidence-based Fall Prevention Strategies
• Universal Fall Precautions• 3-Step Fall Prevention Process
Universal Fall Precautions
• Cornerstone of any hospital fall prevention program
• Apply to all patients at all times Clear pathways. Wipe up spills
immediately. Provide access to call
bell. Provide non-skid
footwear.

3-Step Fall Prevention Process
1. Fall risk assessment (FRA)
2. Care plan tailored or personalized to each area of risk identified through FRA
3. Consistent preventative interventions (based on tailored plan)

Fall Risk Assessment at MGH• Morse Fall Scale• Document Morse Fall Scale
every 24 hours or more often as patient condition warrants
• Used to identify each patient’s individual risk factors for falling
• Used to identify the interventions to decrease patient risk for falling
Risk Factors for Falls Identified by Morse Fall Scale
• History of falling• Secondary diagnosis
—Associated with incontinence, vision problems, multiple medicines, orthostatic hypotension
• Ambulatory aid• IV therapy/heparin (saline) lock• Gait • Mental status
Source: Morse, JM. Predicting Patient Falls. CA: Sage Publications, 1997.

Recommended InterventionsHistory of falling (in past 3 months): Most significantindicator for falling • Use safety precautions. • Communicate risk status via plan of care, change of
shift report, and signage. • Document circumstances of previous fall.
PCA: Ask the patient about previous falls. Collaborate with the nurse on implementing a plan to prevent similar falls.
Patient who have fallen in the past are likely to fall again and under similar circumstances. Plan accordingly!

Recommended Interventions, cont.Secondary diagnosis• Think about factors that may increase risk for
falls that are related to symptoms of multiple medical problems and side effects from the medications to treat medical problems:
—Illness/multiple medicines—Side effects such as dizziness,
frequent urination, and unsteadiness
—Vision problems PCA: Ask the nurse if the patient requires frequent rounding/toileting due to symptoms of medical problems or medication side effects.

Recommended Interventions, cont.
Ambulatory aid• Use ambulatory aid at bedside
if needed.• Review dangers of using
furniture or hospital equipment as an ambulatory aid.
• Assess ability to use ambulatory aid.
• If no ambulatory aid but needs it, consider PT consult
PCA: Make sure patients have their ambulatory aid when walking. Remind patient about the dangers of using furniture as an aid in the hospital.

Recommended Interventions, cont.IV therapy/heparin (saline) lock• Implement toileting/rounding schedule. • Tell patient to call for help with toileting. • Review side effects of IV medicines.
PCA: Remind the patient that the IV will cause them to urinate more frequently and to call for help with toileting. Conduct frequent rounding.
Recommended Interventions, cont.Gait• Help patient get out of bed. • Assess gait when patient has
ambulatory aid as baseline• Consider PT consult.
PCA: Make sure patients have their ambulatory aid when walking.
Normal gait: Walks with head erect, arms swinging freely at the side, striding without hesitation.Weak gait: Stooped, but able to lift head without losing balance. If furniture required, uses as a guide (feather-weight touch). Short steps, may shuffle.Impaired gait: Difficulty rising from chair (needs to use arms; several attempts to rise. Head down; watches ground while walking. Cannot walk without assist; grabs at furniture or whatever available. Short, shuffling gait.
Recommended Interventions, cont.Mental status• Use bed or chair alarm.• Place patient in visible location. • Encourage family presence. • Do frequent rounding.
PCA: make sure bed/chair alarm are turned on when leaving the room. Do not leave patients in the bathroom unattended.
Mental status test: “Are you able to go to the bathroom alone, or do you need assistance?”• Normal: Patient response is consistent with orders or kardex.• Overestimates/forgets limits: Patient response is inconsistent with orders or unrealistic.

ABCS of Harm• Patient is at high risk for injury if they fall with:
– Age: 85 years old or older, frailty– Bones: osteoporosis, risk or history of
fracture, etc– Coagulation: risk for bleeding, low platelet
counts, or taking anticoagulation– Surgery (recent): lower limb amputation,
major abdominal or thoracic surgery
• Fall TIPS (Tailoring Interventions for Patient Safety)– 2 year mixed methods study funded by Robert
Wood Johnson Foundation:• Qualitative phase:
– why hospitalized patients fall?
– what interventions are effective and feasible in hospital settings?
• Randomized control trial: to test an EHR-based fall prevention toolkit designed to address issues identified during qualitative phase.
Supported by the Robert Wood Johnson Foundation, Dykes PI
Evidence re: Using the EHR for Fall Prevention Care Planning

21
There were fewer falls in intervention units than in
control units
No significant effect was noted in fall related injuries
Findings:
Patients aged 65 or older benefited most from the Fall
TIPS toolkit
Patient falls were significantly reduced on intervention units

Fall Prevention Lessons Learned
Strategies and tools to facilitate the 3-step fall prevention process will prevent patients from falling!
Fall Prevention Lessons Learned
• Fall TIPS reduced falls by 25% but >90% of falls are preventable…what happened?– Why did some patients with access to the Fall TIPS Toolkit fall?
• What factors are associated with falls in younger patients?• What factors are associated with falls in older patients?
– Secondary analysis of fallers (cases) n=48 and 144 matched controls exposed to the Fall TIPS toolkit*
– Found that in all cases, planned interventions were not followed consistently by the patient (most frequently) or the nurse• i.e., Out of bed with assistance
How do we get patients to CONSISTENTLY follow their fall prevention plan?
Dykes PC, I-Ching EH, Soukup JR, Chang F, Lipsitz S. A case control study to improve accuracy of an electronic fall prevention toolkit. AMIA Annu Symp Proc. 2012; 2012:170-9.
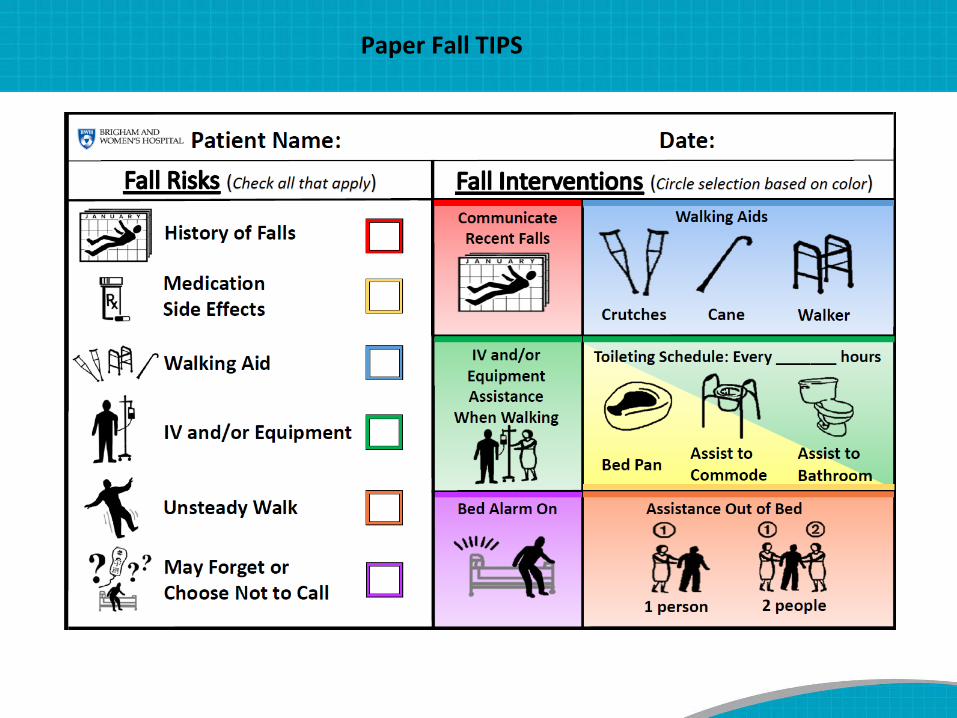
Paper Fall TIPS
Fall risk assessment Tailored plan based on patient’s determinants of risk
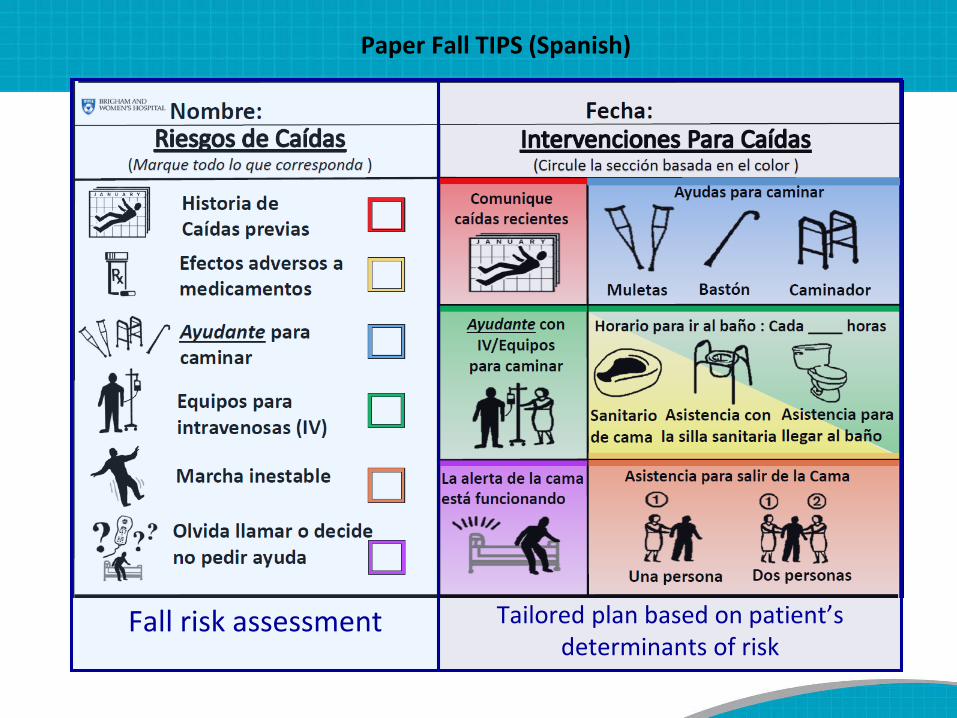
Paper Fall TIPS (Spanish)
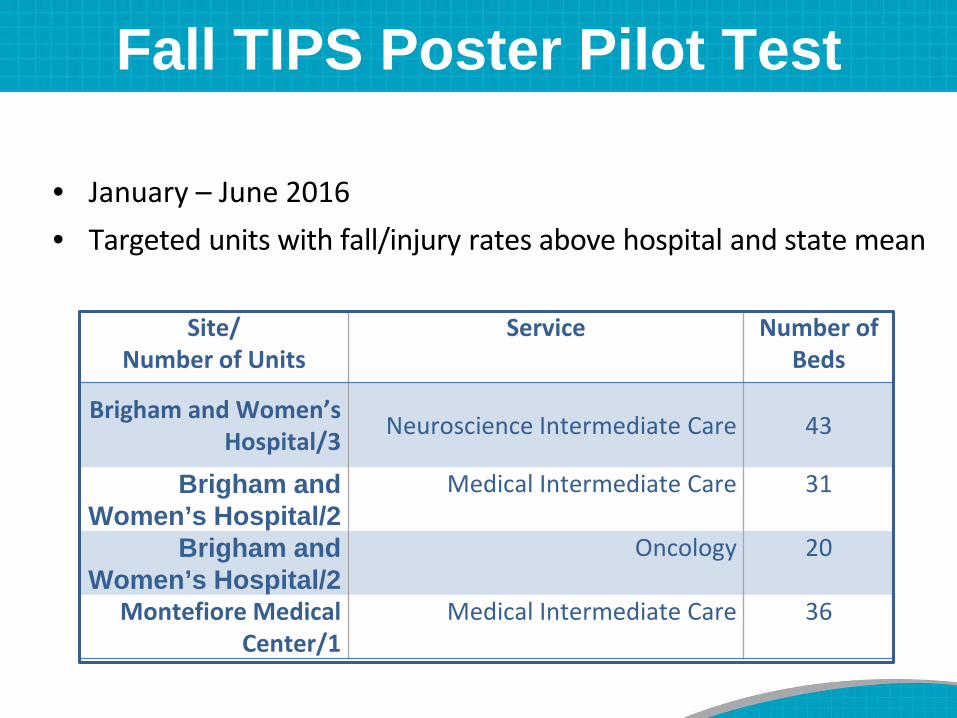
Fall TIPS Poster Pilot Test
• January – June 2016• Targeted units with fall/injury rates above hospital and state mean
Site/ Number of Units
Service Number of Beds
Brigham and Women’s Hospital/3 Neuroscience Intermediate Care 43
Brigham and Women’s Hospital/2
Medical Intermediate Care 31
Brigham and Women’s Hospital/2
Oncology 20
Montefiore MedicalCenter/1
Medical Intermediate Care 36

Fall TIPS Pilot Test Results: BWH
0
20
40
60
80
100
0.001.002.003.004.005.006.00
Perc
ent o
f Fal
l TIP
S co
mpl
ete
alls
per t
hous
and
patie
nt d
ays
Average Fall Rate 2015 vs. 2016 with Average Fall TIPS Completion
2015
2016
Average Fall TIPS Completion
Pre-intervention mean fall rate: 3.28
Post-intervention mean fall rate: 2.80
0102030405060708090100
0.00
0.50
1.00
1.50
2.00
2.50
Perc
ent o
f Fal
l TIP
S co
mpl
ete
Falls
with
inju
ry p
er th
ousa
nd p
atie
nt
days
Average Fall Rate with Injury 2015 vs. 2016 with Average Fall TIPS Completion
2015
2016
Average Fall TIPSCompletion
Pre-intervention mean fall with injury rate: 1.00
Post-intervention mean fall with injury rate: 0.54
Fall TIPS Adherence: 82%
Pre-Fall TIPS Fall Rate: 3.28
Post Fall TIPS Fall Rate: 2.80
Pre-Fall TIPS Injury Rate: 1.00
Post Fall TIPS Injury Rate: .54
In Press: Joint Commission Journal of Quality and Safety

Rationale for Patient Engagement in 3-Step Fall Prevention Process
• Facilitates patient understanding of personal fall risk status and the plan to prevent a fall.
• Promotes patient understanding of their role in fall prevention.
• Facilitates patient (and family) partnership in ensuring that the plan is carried out consistently.
*Dykes PC, I-Ching EH, Soukup JR, Chang F, Lipsitz S. A case control study to improve accuracy of an electronic fall prevention toolkit. AMIA Annu Symp Proc. 2012; 2012:170-9.
A common reason why patients fall is that planned interventions are not followed consistently by the patient (most frequently) or the team*
Patient Engagement Audits• Fall TIPS Champions on each unit will conduct
and submit 5 audits/month with the following data:
1. Is the patient’s Fall TIPS poster updated and hanging at the bedside?
2. Can the patient/family verbalize the patient’s fall risk factors?
3. Can the patient/family verbalize the patient’s personalized fall prevention plan?
Electronic Fall TIPS• Fall TIPS is integrated into Epic
– HealthStream module available• All clinical nurses will complete HealthStream module• Unit champions’ role:
– Complete “super user training” (this class)– Complete HealthStream module– Check off clinical nurses completing Fall TIPS at the
bedside with a patient including providing patient education and posting Fall TIPS poster
– Fall TIPS audits (5/month/unit)
Tools to Support Fall TIPS Rollout
• Fall TIPS training module (HealthStream or power point)
• eCare TIPS sheet• Fall TIPS audit tool• Fall TIPS RN Guide• Fall TIPS email:


EPIC Documentation:Two ways to access the MFS risk assessment and Fall TIPS
1) Click: “Navigators”– Click “Admission”– Click “Falls Mobility”– Click “Morse Fall Risk” and document assessment.
2) Click: “Summary”– Click “Flowsheets”– Click “Daily Cares/Safety”– Scroll to Morse Fall Risk
Note: “Clear intervention” waschanged to “Remove intervention” on Sept. 6th
This documentation ensures that intervention icons that are no longer relevant (i.e. the patient does not have an IV any more and therefore does not need assistance with IV pole) are not saved in eCare and that the Laminated Fall TIPS poster will match your eCare documentation.

3-STEP FALL PREVENTION PROCESS CASE STUDY
Evidence-based Fall Prevention
Case Study• John, an 82-year-old man with diabetes was admitted to
BWH medical unit with chest pain and shortness of breath. On admission, the patient was found to be alert and oriented. He had an IV and was placed on a cardiac monitor.
• During the admission interview, John reported that with his cane, he was independent with walking and transfers. However, the nurse noted that the doctor’s order was for walking with cane and assistance only.
• With further questioning, the patient reported that he had fallen at home several times over past year, most recently last month.
• As the nurse assisted John to bathroom, she noted that initially he used the bedside table and other furniture as guides and needed to be reminded to use his cane.
• Once he was given his cane, John walked with short, steady steps to bathroom.
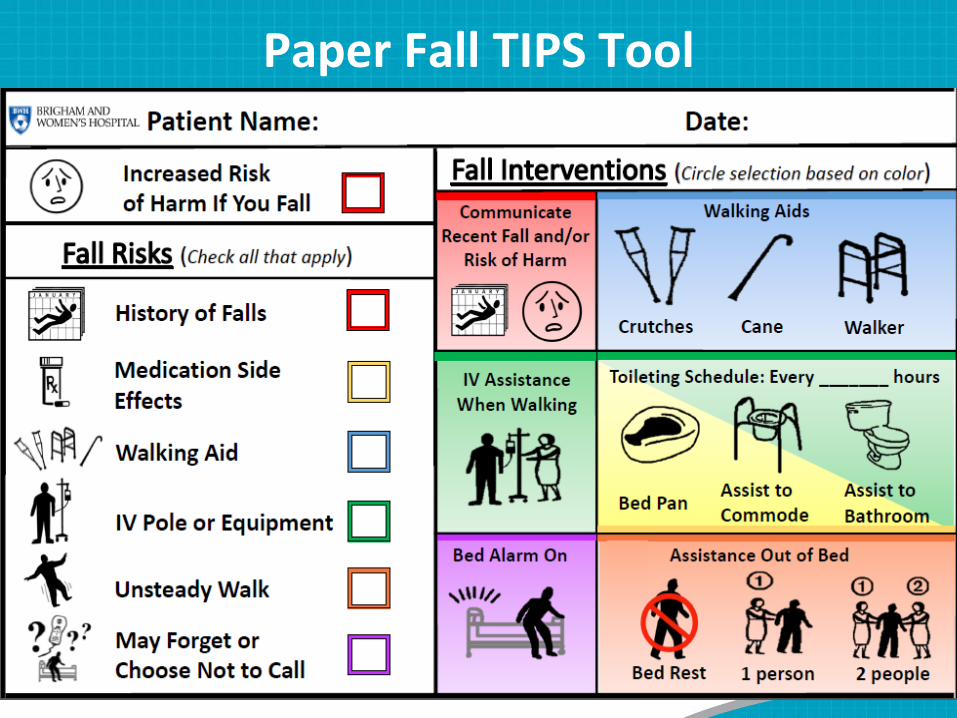
Paper Fall TIPS Tool

1
Answers
John 05/12/2016


















