
Faculty of Medicine Ramathibodi Hospital Mahidol ... · of both internal fixation methods (DHS and...
32
Faculty of Medicine Ramathibodi Hospital, Mahidol University RACE 698/8 Dissertation Master of Science Program in Medical Epidemiology (International Program) Natthapong Hongku ID 5936423 Title: Fracture Fixation versus Hemiarthroplasty for Unstable Intertrochanteric Fractures in Elderly Patients, Which one is lower morbidity and mortality rates? : Systematic Review and Network Meta- Analysis of Randomized Controlled Trials Research Proposal 1 |
Transcript of Faculty of Medicine Ramathibodi Hospital Mahidol ... · of both internal fixation methods (DHS and...
Faculty of Medicine Ramathibodi Hospital,
Mahidol University
RACE 698/8 Dissertation
Master of Science Program in Medical Epidemiology
(International Program)
Natthapong Hongku
ID 5936423
Title: Fracture Fixation versus Hemiarthroplasty for Unstable
Intertrochanteric Fractures in Elderly Patients, Which one is lower
morbidity and mortality rates? : Systematic Review and Network Meta-
Analysis of Randomized Controlled Trials
Research Proposal
1 |
Contents INVESTIGATOR AND SUPERVISORS 3 1. BACKGROUND AND RATIONALE 4 1.1 Background and Rationale 1.1.1 Magnitude of problem 1.1.2 Disease burden or impacts 1.1.3 Treatment and goals of treatment 1.2 Literature review and rationale for conducting study 1.3 Research Question 1.4 Research Objectives 2. METHODOLOGY 9 2.1 Study design
2.2 Location of studies 2.3 Selection of studies
2.4 Data extraction 2.5 Risk of bias assessment 2.6 Statistical Analysis 2.6.1 Direct meta-analysis 2.6.2 Network meta-analysis 2.7 Time Frame ACKNOWLEDGEMENTS 16 REFERENCES 17 FIGURES 21-23 APPENDICES
Appendix 1: Search term and results 24 Appendix 2: Data extraction forms 26 Appendix 3: Risk bias assessment forms 30 Appendix 4: Timeline for research 32
2 |

FRACTURE FIXATION VERSUS HEM IARTHROPLASTY FOR
UNSTABLE INTERTROCHANTERIC FRACTURE IN ELDERLY
PATIENTS, WHICH ONE IS LOWER MORBIDITY AND MORTALITY
RATES? : SYSTEMATIC REVIEW AND NETWORK METAANALYSIS
OF RANDOMIZED CONTROLLED TRIALS
Investigators and Affiliation:
1. Natthapong Hongku
Department of Orthopedic, Faculty of Medicine Vajira hospital, Navamindradhiraj University
Section for Clinical Epidemiology and Biostatistics, Faculty of Medicine Ramathibodi
Hospital, Mahidol University
E-mail: [email protected]
2. Lertkong Nitiwarangkul
Section for Clinical Epidemiology and Biostatistics, Faculty of Medicine Ramathibodi
Hospital, Mahidol University
Department of Orthopedic, Police General Hospital
E-mail: [email protected]
Supervisors:
1. Sasivimol Rattanasiri, Assistant Professor, PhD
E-mail: [email protected]
2. Patarawan Woratanarat, Associate Professor, PhD
E-mail: [email protected]
3. Ammarin Thakkinstian, Professor, PhD
E-mail: [email protected]
Section for Clinical Epidemiology and Biostatistics, Faculty of Medicine, Ramathibodi
Hospital, Mahidol University
3 |
CHAPTER 1
BACKGROUND AND RATIONALE
1.1 Background and rationale
1.1.1 Magnitude of problem
Elderly populations are increasing due to improvement in health care systems
following with rising of population’s life expectancy. One of the most important health
problems in elderly populations is osteoporosis, which led to more than 90% of the fragility
fracture after simple fall especially fracture around the hip joint (1). The incidence of
osteoporotic hip fracture has been forecasted to be increased doubling in each decade of life
after age 50 years, and it was common in female than male (2, 3).
1.1.2 Disease burden or impacts
There are three types of osteoporotic hip fracture base on location of fracture, i.e.,
intracapsular neck fracture, intertrochanteric fracture, and sub trochanteric fracture (4) as
shown in figure 1. Intertrochanteric fracture is the most common osteoporotic hip fracture
which commonly occurred in patients aged 70 years or older. A mortality rate after
intertrochanteric fracture was varied but still as high as 14 to 36%(5, 6); this was due to their
underlying disease and independent status in carrying out daily life activity(7). In addition, a
lot of major morbidity occurred after fracture including pressure sore, pneumonia, urinary
tract infection, and venous thromboembolism. Furthermore, 25% of patients might need long-
term life cares, and 50% of them need assistance in daily life activity (8). These morbidities
could be prevented by early mobilization, early weight bearing, and early return to pre-injury
activity level as soon as possible
4 |

Intertrochanteric fracture is additionally classified into stable and unstable fractures
depend on location (i.e., lesser or greater trochanter), patterns of fracture line, and
configuration of fracture. The unstable intertrochanteric fractures are defined as fracture of
lesser trochanter (9), reverse oblique fracture pattern with presence of comminution of
posteromedial fragment (10, 11), and breaking of lateral cortex (12) as shown in figure 2.
Conversely, the stable fractures are defined as non-displacement and non-comminution of
fracture site.
1.1.3 Treatment and goals of treatment
Two treatment management options are available for intertrochanteric fracture (i.e.,
operative and non-operative treatment managements). Choosing appropriated treatments
depend on various factors such as patient’s status, their co-morbidity and expectations.
Patients with severe co-morbidity, high risk of surgery, and bedridden status may be more
appropriated to receive non-operative treatments. Contrastingly, patients without these
conditions may be suit with operation treatments, which aimed as anatomical reduction with
stable fixation and promote fracture healing leading to early mobilization with appropriated
weight bearing ambulation.
The surgical options for reduction and internal fixation are divided into extra-
medullary devices (i.e. dynamic or sliding hip screw: DHS) and intra-medullary devices (i.e.
proximal femoral nail: PFN) as shown in figure 3. Not only type of implant, but also bone
quality in osteoporotic fracture play a role on operation results. For stable intertrochanteric
fracture, internal fixation either extra or intra-medullary device might yielded good results
but not for unstable intertrochanteric osteoporotic fracture (13) which might be due to
5 |

difficulty in maintain a stable fixation. Moreover the reoperation due to implant failure may
occur in patients who could not protect of full weight bearing after operation (14, 15)
Recently, bipolar hemiarthroplasty or total hip arthroplasty (THA) for femoral neck
fracture which is another common hip fracture in elderly patients showed good clinical result
in term of clinical outcome and lower reoperation rate (16) as shown in figure 4 but were still
controversial for unstable intertrochanteric fracture especially in osteoporotic elderly
populations.
The Advantages of internal fixation fracture with intramedullary devices in
intertrochanteric fracture included less soft tissue trauma from minimal invasive surgical
techniques, less blood loss (17), no complications related with prosthesis such as prosthetic
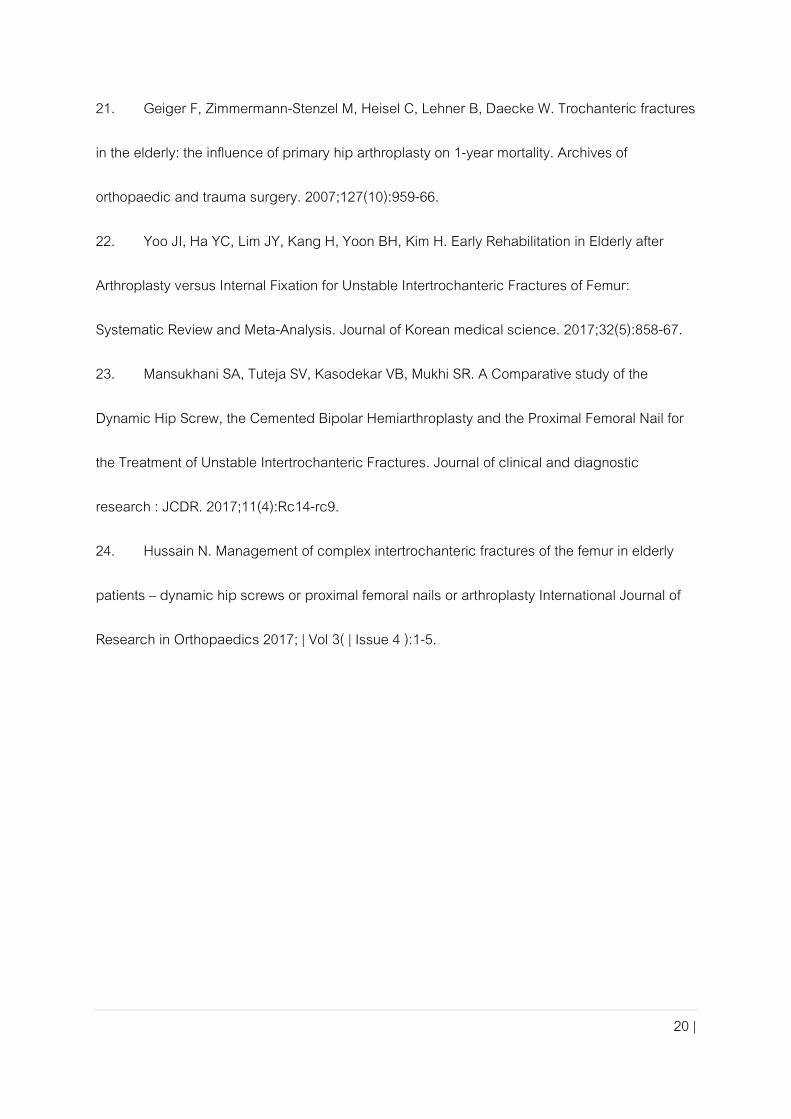
dislocation or periprosthetic fracture. However, previously evidence showed that the internal
fixation were risk to fail for fracture fixation, loss of fracture reduction, femoral head or
fracture site collapse (18) as shown in figure 5. The most acceptable advantages of
hemiarthroplasty for unstable intertrochanteric fracture were allowing to full weight bearing
immediately postoperative, in which patients could early ambulation (19), avoid bony
collapse at fracture site (20), problems of fracture malunion or nonunion as shown in figure 6
and also prevent any complication due to prolong immobilization such as pressure sore,
pneumonia, deep vein thrombosis. But the complications related to the difficult of procedure
were also reported including increase operative time, increase intraoperative blood loss, need
more surgical experienced, high risk of prosthetic dislocation and periprosthetic fracture (21).
6 |

1.2 Literature review and rationale for conducting study
Results of management options for unstable intertrochanteric fractures were still
controversial. A recently systematic review and meta- analysis (22) combined data from 2
randomized controlled trials (RCTs) and 8 retrospective cohort studies, which demonstrated
that both hemiarthroplasty and fracture fixation were not significant different in term of
overall mortality, reoperation rate, and complications; but hemiarthroplasty was superior in
functional outcomes especially earlier mobilization compared to fracture fixation.
However, this review was mainly based on observational studies which prone to bias results.
The questions of which surgical treatment management was the best in term of high efficacy
and low complications for unstable intertrochanteric fractures in elderly patients was still
unanswerable.
There were few RCTs published (23, 24) since then we therefore, updated a
systematic review and performed network meta-analysis to assess efficacy and complications
of both internal fixation methods (DHS and PFN) and hemiarthroplasty. Failure and
reoperation were compared across three surgical treatment managements. In addition, the
function score measured by Harris Hip Score (HHS) was also compared. Finally, probability
being best management (i.e. low complications and high functions) was estimated and rank
accordingly.
7 |

1.3 Research question
Among all of the available surgical treatment for unstable intertrochanteric fractures
in elderly patients, which one between fracture fixations and hemiarthroplasty will provide
better clinical results in term of lower complication events?
1.4 Research objectives
• To compare surgical complication results such as failure and re-operation rates of
surgical treatment between fracture fixation and hemiarthroplasty for unstable
intertrochanteric fractures in elderly patients
• To compare clinical outcomes such as Harris hip score between fracture fixation and
hemiarthroplasty for unstable intertrochanteric fracture in elderly patients
8 |

CHAPTER 2
METHODOLOGY
2.1 Study design
Systematic review with direct and network meta-analysis
2.2 Location of studies
2.2.1 Sources
The relevant studies will be searched by two reviewers (N.H. and L.N.) using
MEDLINE via PubMed (www.ncbi.nlm.nil.gov/pubmed), SCOPUS via Scopus
(www.scopus.com) and reference lists from selected articles and previous meta-analysis
articles.
2.2.2 Search strategy
Search terms will be constructed according to population (P), intervention (I) and
comparator (C) filtering for only RCT. The search terms for outcomes (O) will be ignored
because we would like to retrieve outcomes as much as possible given interested
interventions. Search terms for P, I, and C are as follows: for P “Unstable* intertrochant*”,
“Unstable intertrochant*”*”, “Unstable *intertrochant*”*”: for I and C, Fixation* for any
type of fracture fixations, “Dynamic hip screw” or “Sliding hip screw” in term of first
specific type of fixation, “Proximal femoral nail” or “Intramedullary nail” in term of second
specific type of fixation, “Gamma nail” in term of third specific type of fixation, “Medoff
plate” in term of fourth specific type of fixation, “Less Invasive Stabilization System” or
LISS in term of last specific type of fixation, and Hemiarthroplasty for comparators.
These search terms will be combined within and between domains using conjunction “OR”
and “AND”, respectively as show in Appendix 1.
9 |
2.3 Selection of studies
All relevant studies from both database will be imported into the Endnote program
version 8.0. RCTs published in English will be included if they met following criteria:
• Studies in elderly patients aged 60 years or older who had unstable intertrochanteric
fractures.
• Studies which compared different technique of fracture fixations and hemiarthroplasty
(cementless or cemented)
• Studies which reported at least one of following outcomes: mortality, any
complications (e.g., reoperation and/or fixation failure), clinical outcomes such as
operative time, intra-operative blood loss, length of hospital stays, Harris hip score,
and mobility score.
The studies were excluded if they included patient with bilateral fracture or duplicated
report of the same studies patients, and insufficient data for pooling after three times contact
the author.
10 |

2.4 Data extraction
The data will be extracted by two reviewers (N.H. and L.N.) independently using
standardized data extraction forms. The difference of extracted results will be discussed and
consensus by senior and supervisor (A.T.). The data extraction forms consisted of four
domains, i.e. general study’s information (i.e., name of title, author, study setting, and name
of journal, publication year, volume and page of studies); study’s characteristics (i.e., study
design, treatment management, and outcomes); patient’s characteristics (i.e., mean age,
gender, side, type of fracture and classification, bone disease by Singh index, American
Society of Anesthesiologists (ASA) grade, time to surgery periods, follow-up time, and
number of loss to follow-up patients); and data for pooling for both dichotomous and
continuous outcomes. Aggregated data of contingency cells for interventions and outcomes
will be extracted. Mean values along with standard deviation for continuous outcomes will be
also extracted. Details of data extraction forms were demonstrated in Appendix 2
Interventions
The interested intervention were fracture fixation managements and hemiarthroplasty
including cementless and cemented types.
Outcome of interests
The primary interested outcomes were rate of failure and reoperation after performed
operation, other complications including mortality rate, medical and surgical complications.
The secondary interested outcomes were functional score (HHS) at less and more than 3
months, length of hospital stay, and operative times.
11 |

Mortality was due to surgery if it was death within 6 weeks. Reoperation was defined
accordingly to criteria used by the original studies. Briefly, patients required to repeat
operation if they had dislocation of prosthesis or revised from internal fracture fixation to
joint replacement surgery. Failure was defined as patients who had any problems related
with prosthesis or implant (i.e., avascular necrosis of femoral head, hardware cutting-off,
mal- or non-union of fracture, deformity of bone, breakage of screw, re-displacement or
collapse of fracture around implant, and shortening of fracture site). Medical complication
was defined as complications due to medical problems within 6 weeks post-operatively. For
example, patients were pulmonary, cardiovascular or neurological complication, pressure
sore, deep vein thrombosis, urinary tract infection, thrombophlebitis, sepsis. Surgical
complication was defined superficial or deep wound infection, and dislocation of hip
prosthesis within 6 weeks after surgery.
2.5 Risk of bias assessment
The risk of bias was independently assessed for each RCT by two reviewers (N.H and
L.N.) using Cochrane risk of bias assessment tool for RCTs. Six domains were assessed
including random sequence generation, conceal treatment allocation, blinding of patients and
outcome assessors, incomplete data, and outcome assessment selective outcome report, and
other biases. Each domain was graded as ‘yes’ and ‘no’ if there was evidence of low and high
risk of bias, respectively. If there was in sufficient information to judge, it was classified as
‘unclear’. The details of risk of bias assessment forms were presented in Appendix 3.
12 |

2.6 Statistical analysis plan
2.6.1 Direct meta-analysis
For dichotomous outcomes (i.e., mortality, reoperation, failure of the operation,
medical and surgical complication events data of surgical treatment options), a relative
treatment effects (i.e., risk ratios, RRs) will be estimated for individual studies. For the
continuous outcomes measured using the same scales (i.e., operative time, intra-operative
blood loss, and length of hospital stay), mean differences (MD) will be estimated otherwise
the standardized mean difference (SMD) will be estimated for HHS and mobility scores.
Then RRs, MDs and SMDs will be pooled across studies using appropriate pooling models
(fixed-effect or random effect model) depend on whether treatment effects were
heterogeneous. If not, a fixed-effect model by Inverse-variance method will be used,
otherwise a random-effect model by DerSimonian and Laird method will be used.
Heterogeneity was present if the Cochrane’s Q statistic was significant (P value ≤ 0.1) or the
I2 statistic ≥ 25%. The possible source of heterogeneity will be explored using meta-
regression analysis model by fitting clinical factors (i.e., mean age, gender, type of fracture
classification, follow up time, number of loss follow up) or methodological factors (i.e., type
of outcome measurement, definition of each outcome, setting of the study) one by one in the
meta-regression model. If the including that factors resulted in decreasing degree of
heterogeneity (I2), subgroup analysis will be performed accordingly.
Publication bias was assessed using funnel plot and Egger test. If one of them showed
asymmetry. A contour enhanced funnel plot was used for distinguish asymmetry of the funnel
was from publication bias or heterogeneity.
13 |
2.6.2 Network meta-analysis
Network meta-analysis with two-stage approach was applied to indirectly compare
relative treatment effects across studies. Firstly, regression analysis will be applied with
appropriated link function depend on type of interested outcomes (i.e., logit link function for
dichotomous outcomes, identity link for continuous outcomes), to estimate relative effect for
each study. The interested interventions was coded as 1, 2, and 3 for DHS, PFN, and
hemiarthroplasty as the reference when fitting. Second, the multivariate meta-analysis will be
applied to pool relative intervention effects [e.g., log (RR) or MDs] across studies using a
consistency model. The multiple comparison of DHS versus PFN, DHS versus HA, and PFN
versus HA will be then estimated.
The inconsistency assumption, i.e., agreement of direct and indirect treatment effects
was then checked using design-by-treatment interaction inconsistency model. In addition,
transitivity was indirectly explored by assessing distribution of factors effect on interested
outcome between intervention arms. These included mean age, type of fracture classification,
definition of outcomes, study setting, follow up period, and risk of bias assessment. If these
characteristics were not much different across intervention comparisons, transitivity may be
assumed. Probability of being the best intervention was estimated and rank using surface
under the cumulative ranking curve (SUCRA) and Rankogram plot. Publication bias for
network meta-analysis was assessed using adjusted funnel plot. All statistical analysis will be
performed using STATA software program version 14.2. P value of less than 0.05 will be
considered as significance. However, for the heterogeneity test, the significant level P value
less than 0.1 will be use.
14 |

2.7 Time Frame
The timeline of this systematic review and network meta-analysis is demonstrated in
Appendix 4.
15 |

ACKNOWLEDGEMENTS
This research proposal is a part of the dissertation for Natthapong Hongku’s training in M.Sc
(Medical Epidemiology), Faculty of Medicine Ramathibodi Hospital and Faculty of Graduate
Studies, Mahidol University.
Funding source: none
16 |
Reference
1. Baker SP, Harvey AH. Fall injuries in the elderly. Clinics in geriatric medicine.
1985;1(3):501-12.
2. Gallagher JC, Melton LJ, Riggs BL, Bergstrath E. Epidemiology of fractures of the
proximal femur in Rochester, Minnesota. Clinical orthopaedics and related research.
1980(150):163-71.
3. Hedlund R, Lindgren U. Trauma type, age, and gender as determinants of hip fracture.
Journal of orthopaedic research : official publication of the Orthopaedic Research Society.
1987;5(2):242-6.
4. Zuckerman JD. Hip fracture. The New England journal of medicine. 1996;334(23):1519-25.
5. Kesmezacar H, Ayhan E, Unlu MC, Seker A, Karaca S. Predictors of mortality in elderly
patients with an intertrochanteric or a femoral neck fracture. The Journal of trauma.
2010;68(1):153-8.
6. Vestergaard P, Rejnmark L, Mosekilde L. Has mortality after a hip fracture increased?
Journal of the American Geriatrics Society. 2007;55(11):1720-6.
7. Blomfeldt R, Tornkvist H, Eriksson K, Soderqvist A, Ponzer S, Tidermark J. A randomised
controlled trial comparing bipolar hemiarthroplasty with total hip replacement for displaced
intracapsular fractures of the femoral neck in elderly patients. The Journal of bone and joint
surgery British volume. 2007;89(2):160-5.
17 |

8. Lu-Yao GL, Keller RB, Littenberg B, Wennberg JE. Outcomes after displaced fractures
of the femoral neck. A meta-analysis of one hundred and six published reports. The Journal of
bone and joint surgery American volume. 1994;76(1):15-25.
9. Barton TM, Gleeson R, Topliss C, Greenwood R, Harries WJ, Chesser TJ. A comparison
of the long gamma nail with the sliding hip screw for the treatment of AO/OTA 31-A2 fractures of
the proximal part of the femur: a prospective randomized trial. The Journal of bone and joint
surgery American volume. 2010;92(4):792-8.
10. Dimon JH, Hughston JC. Unstable intertrochanteric fractures of the hip. The Journal of
bone and joint surgery American volume. 1967;49(3):440-50.
11. Evans EM. The treatment of trochanteric fractures of the femur. The Journal of bone and
joint surgery British volume. 1949;31b(2):190-203.
12. Gotfried Y. The lateral trochanteric wall: a key element in the reconstruction of unstable
pertrochanteric hip fractures. Clinical orthopaedics and related research. 2004(425):82-6.
13. Bannister GC, Gibson AG, Ackroyd CE, Newman JH. The fixation and prognosis of
trochanteric fractures. A randomized prospective controlled trial. Clinical orthopaedics and
related research. 1990(254):242-6.
14. Kayali C, Agus H, Ozluk S, Sanli C. Treatment for unstable intertrochanteric fractures in
elderly patients: internal fixation versus cone hemiarthroplasty. Journal of orthopaedic surgery
(Hong Kong). 2006;14(3):240-4.
15. Kim SY, Kim YG, Hwang JK. Cementless calcar-replacement hemiarthroplasty
compared with intramedullary fixation of unstable intertrochanteric fractures. A prospective,
18 |

randomized study. The Journal of bone and joint surgery American volume. 2005;87(10):2186-
92.
16. Blomfeldt R, Tornkvist H, Ponzer S, Soderqvist A, Tidermark J. Comparison of internal
fixation with total hip replacement for displaced femoral neck fractures. Randomized, controlled
trial performed at four years. The Journal of bone and joint surgery American volume.
2005;87(8):1680-8.
17. Boldin C, Seibert FJ, Fankhauser F, Peicha G, Grechenig W, Szyszkowitz R. The
proximal femoral nail (PFN)--a minimal invasive treatment of unstable proximal femoral fractures:
a prospective study of 55 patients with a follow-up of 15 months. Acta orthopaedica
Scandinavica. 2003;74(1):53-8.
18. Jones HW, Johnston P, Parker M. Are short femoral nails superior to the sliding hip
screw? A meta-analysis of 24 studies involving 3,279 fractures. International orthopaedics.
2006;30(2):69-78.
19. Davison JN, Calder SJ, Anderson GH, Ward G, Jagger C, Harper WM, et al. Treatment
for displaced intracapsular fracture of the proximal femur. A prospective, randomised trial in
patients aged 65 to 79 years. The Journal of bone and joint surgery British volume.
2001;83(2):206-12.
20. Green S, Moore T, Proano F. Bipolar prosthetic replacement for the management of
unstable intertrochanteric hip fractures in the elderly. Clinical orthopaedics and related
research. 1987(224):169-77.
19 |
21. Geiger F, Zimmermann-Stenzel M, Heisel C, Lehner B, Daecke W. Trochanteric fractures
in the elderly: the influence of primary hip arthroplasty on 1-year mortality. Archives of
orthopaedic and trauma surgery. 2007;127(10):959-66.
22. Yoo JI, Ha YC, Lim JY, Kang H, Yoon BH, Kim H. Early Rehabilitation in Elderly after
Arthroplasty versus Internal Fixation for Unstable Intertrochanteric Fractures of Femur:
Systematic Review and Meta-Analysis. Journal of Korean medical science. 2017;32(5):858-67.
23. Mansukhani SA, Tuteja SV, Kasodekar VB, Mukhi SR. A Comparative study of the
Dynamic Hip Screw, the Cemented Bipolar Hemiarthroplasty and the Proximal Femoral Nail for
the Treatment of Unstable Intertrochanteric Fractures. Journal of clinical and diagnostic
research : JCDR. 2017;11(4):Rc14-rc9.
24. Hussain N. Management of complex intertrochanteric fractures of the femur in elderly
patients – dynamic hip screws or proximal femoral nails or arthroplasty International Journal of
Research in Orthopaedics 2017; | Vol 3( | Issue 4 ):1-5.
20 |

Figure 1: Types of osteoporotic hip fracture classified as intracapsular femoral neck, intertrochanteric, and subtrochanteric fracture (from left to right)
Figure 2: Unstable intertrochanteric fracture as fracture of lesser trochanter (left), reverse oblique fracture pattern with presence of comminution of posteromedial fragment (middle), and breaking of lateral cortex (right)
21 |

Figure 3: The method of reduction and fixation of intertrochanteric fracture with extra-medullary device: dynamic or sliding hip screw (left) and intra-medullary device: proximal femoral nail (right)
Figure 4: Pre and postoperative radiographic of patients who presented with fracture of the right femoral neck performed total hip replacement (middle) and bipolar hemiarthroplasty (right) and showed good clinical outcome.
22 |
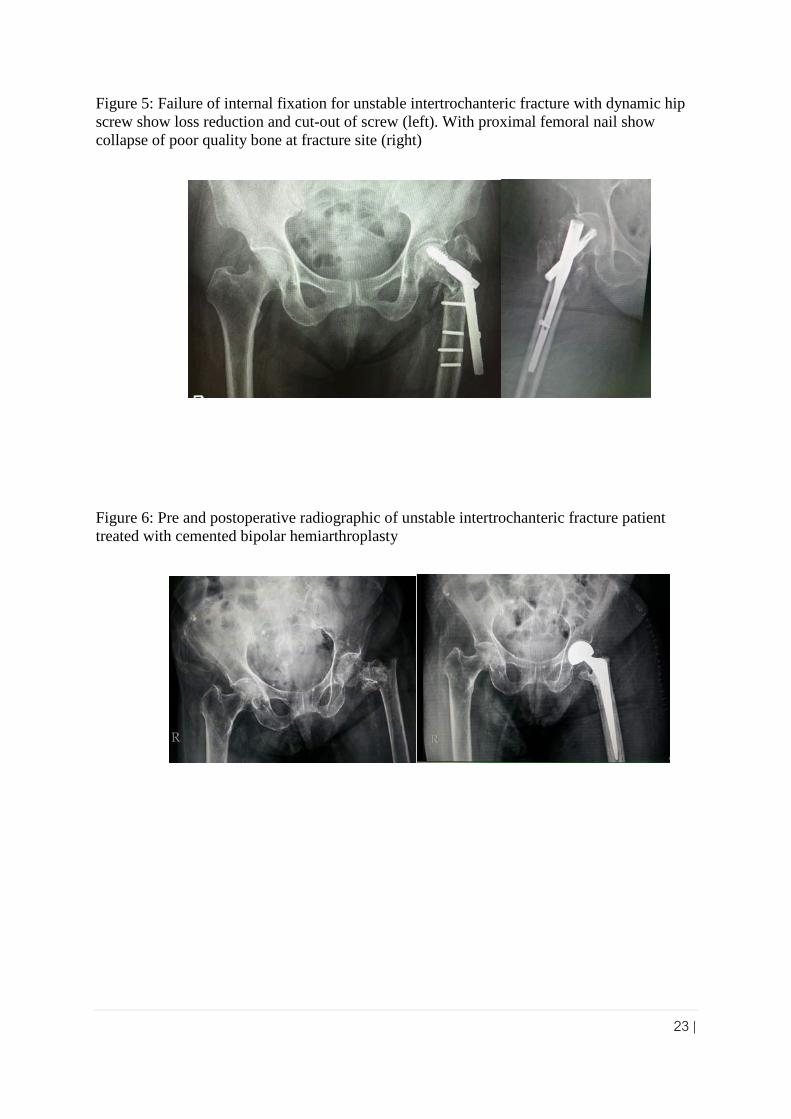
Figure 5: Failure of internal fixation for unstable intertrochanteric fracture with dynamic hip screw show loss reduction and cut-out of screw (left). With proximal femoral nail show collapse of poor quality bone at fracture site (right)
Figure 6: Pre and postoperative radiographic of unstable intertrochanteric fracture patient treated with cemented bipolar hemiarthroplasty
23 |

Appendix 1: Search term and results
a) Search results from PubMed Domains
Search Terms Results
Populations (P)
#1 "unstable* intertrochant*" 71,183 #2 "unstable intertrochant*" 71,154 #3 “unstable *intertrochant*” 71,154 #4 #1 OR #2 OR #3 71,183
Interventions and Comparators (IC)
#5 Fixation* 188,983 #6 “Dynamic hip screw” 673 #7 “Sliding hip screw” 252 #8 #6 OR #7 902 #9 “Proximal femoral nail” 302 #10 "Proximal* nail” 224 #11 “Intramedullary nail” 2,040 #12 #9 OR #10 OR #11 2,528 #13 "Gamma nail" 354 #14 "Medoff plate” 12 #15 "Less Invasive Stabilization System" 127 #16 LISS 3,662 #17 #15 OR #16 3,685 #18 Hemiarthroplasty 2,470 #19 #5 OR #8 OR #12 OR #13 OR #14 OR #17 OR #18 194,982
Filters (Study design)
#20 "Randomized controlled trial" 453,509 #21 "Clinical trial" 640,333 #22 "Randomized trial" 36,559 #23 Random* 1,120,653 #24 #20 OR #21 OR #22 OR #23 1,468,184
Populations, Interventions and Comparators, Filters
#25
#4 AND #19 AND #24
479
24 |

b) Search results from SCOPUS
Domains
Search Terms Results
Populations (P)
#1 "unstable* intertrochant*" 1,398 #2 "unstable intertrochant*" 1,938 #3 “unstable *intertrochant*” 1,400 #4 #1 OR #2 OR #3 2,032
Interventions and Comparators (IC)
#5 Fixation* 567,139 #6 “Dynamic hip screw” 2,481 #7 “Sliding hip screw” 1,282 #8 #6 OR #7 2,950 #9 “Proximal femoral nail” 1,185 #10 "Proximal* nail” 570 #11 “Intramedullary nail” 10,328 #12 #9 OR #10 OR #11 11,335 #13 "Gamma nail" 1,916 #14 "Medoff plate” 16 #15 "Less Invasive Stabilization System" 1,083 #16 LISS 299,981 #17 #15 OR #16 299,750 #18 Hemiarthroplasty 8,189 #19 #5 OR #8 OR #12 OR #13 OR #14 OR #17 OR #18 797,833
Filters (Study design)
#20 "Randomized controlled trial" 1,375,028 #21 "Clinical trial" 2,109,384 #22 "Randomized trial" 954,550 #23 Random* 5,005,941 #24 #20 OR #21 OR #22 OR #23 5,822,362
Populations, Interventions and Comparators, Filters
#25
#4 AND #19 AND #24
924
25 |
Appendix 2: Data extraction forms
Data extraction form (1)
Fracture Fixation versus Hemiarthroplasty for Unstable Intertrochanteric
Fractures in Elderly Patients, Which one is lower morbidity and mortality rates?
: Systematic Review and Network Meta-Analysis of Randomized Controlled
Trial Study ID …………………………..
Part 1: General study information
1. Title
2. First author name
3. Study setting/Country
4. Journal name
5. Year of publication
6. Volume
7. Page
Reviewer Natthapong Lertkong
DEF version Date
26 | P a g e
Data extraction form (2)
Fracture Fixation versus Hemiarthroplasty for Unstable Intertrochanteric
Fractures in Elderly Patients, Which one is lower morbidity and mortality rates?
: Systematic Review and Network Meta-Analysis of Randomized Controlled
Trials Study ID …………………………..
Part 2: General study characteristics
Study design
RCT
Treatment interventions
Dynamic hip screw Proximal femoral nail Hemiarthroplasty
Type of outcomes
Mortality Reoperation Failure operation Medical complications ………………………………………………………… Surgical complications ………………………………………………………… Harris hip score at less than 3 months Harris hip score at more than 3 months Operative time Length of hospital stay
Reviewer Natthapong Lertkong
DEF version Date
27 | P a g e

Data extraction form (3)
Fracture Fixation versus Hemiarthroplasty for Unstable Intertrochanteric
Fractures in Elderly Patients, Which one is lower morbidity and mortality rates?
: Systematic Review and Network Meta-Analysis of Randomized Controlled
Trials Study ID …………………………..
Part 3: General patient characteristics
Characteristics
Intervention
Overall
DHS
PFN
Hemiarthroplasty
Number
Age (Mean)
Sex-Male: Female
(% male)
Side-Right: Left
(% Right side)
Type of fracture Classification
Percentage of unstable type*
Type of anaesthesia - GA:RA
(%GA)
ASA grade
Percentage of ASA class > 2
Follow up time (month)
Number of loss follow up
* Unstable type defined as fracture classification AO 31A2.2 – AO31A3.3 or Evan type II, III, IV, V
Reviewer Natthapong Lertkong
DEF version Date
28 | P a g e

Data extraction form (4) Fracture Fixation versus Hemiarthroplasty for Unstable Intertrochanteric
Fractures in Elderly Patients, Which one is lower morbidity and mortality rates?
: Systematic Review and Network Meta-Analysis of Randomized Controlled
Trials Study ID …………………………..
Part 4: The pooling Data for dichotomous outcomes
Interventions
Mortality Reoperation Failure Medical complications
Surgical complications
N no. (%)
N no. (%)
N no. (%)
N no. (%)
N no. (%)
Dynamic hip screw
Proximal femoral nail
Hemiarthroplasty
Part 5: The pooling data for continuous outcomes
Intervention Operative time Intra-operative blood loss
Hospitalization Harris Hip Score Mobility Score
n Mean SD n Mean SD n Mean SD n Mean SD n Mean SD
Dynamic hip screw
Proximal femoral nail
Hemiarthroplasty
Reviewer Natthapong Lertkong
DEF version Date
29 | P a g e

Appendix 3: Risk bias assessment form (1) Fracture Fixation versus Hemiarthroplasty for Unstable Intertrochanteric Fractures in Elderly Patients, Which one is lower morbidity and mortality rates? : Systematic Review and Network Meta-Analysis of Randomized Controlled Trials
Study ID ………………………….. Domain Question Assessment Selection bias
1. Was the allocation sequence generated adequately?
Yes No Unclear
2. Were participants analyzed within the groups they were originally assigned to?
Yes No Unclear
3. Was the allocation of treatment adequately?
Yes No Unclear
4. Did the study apply inclusion/exclusion criteria uniformly to all comparison groups?
Yes No Unclear
Performance bias
1. Did the study blinding of participant / assessors
Yes No Unclear
Attrition bias
1. Were missing data handled appropriately (e.g., intention-to-treat analysis and imputation)?
Yes No Unclear
Detection bias
1. Was the length of follow-up different between the groups?
Yes No Unclear
2. Were interventions/exposures assessed/defined using valid and reliable measures?
Yes No Unclear
3. Were outcomes assessed using valid and reliable measures?
Yes No Unclear
Reporting bias
1. Were the potential outcomes prespecified by the researchers?
Yes No Unclear
2. Are all pre-specified outcomes reported?
Yes No Unclear
If answer is “Yes” in all domains would place a study at “Low Risk of Bias” If answer is “No” in any of the domains would place a study at “High Risk of Bias” If answer is “Unclear” in any of the domains would place the study at “Unclear Risk of Bias”
Reviewer Natthapong Lertkong RAF version Date
30 | P a g e

Risk bias assessment form (2)
Fracture Fixation versus Hemiarthroplasty for Unstable Intertrochanteric
Fractures in Elderly Patients, Which one is lower morbidity and mortality rates?
: Systematic Review and Network Meta-Analysis of Randomized Controlled
Trials Study ID …………………………..
Domain Low risk High risk Unclear Quote; Comment
Selection bias
1. Random sequence generation
2. Allocation concealment
Performance bias
1. Blinding of participants
2. Blinding of assessors
Attribution bias
Incomplete outcome data
Detection bias
1. Blinding of outcome assessment
Reporting bias
1. Selective outcome reporting
Reviewer Natthapong Lertkong
RAF version Date .
31 | P a g e
Appendix 4: Timeline of research
Item TOR Nov Dec Jan Feb Mar Apr 1. Develop research proposal
2. Prospero registration
3. Defend research proposal
4. Conduct research
5. Develop 1st manuscript
• Introduction
• Methods
• Results
• Discussion
6. Submit 1st manuscript (RACE 618)
systematic review
7. Write thesis
• Chapter 1: Introduction
• Chapter 2: Methods
• Chapter 3: Results
• Chapter 4: Discussion
8. Defend thesis
32 | P a g e


















