Faculty Disclosure Information10/1/2012 2 Prevalence of CSHCN NY US CSHCN Prevalence Percent of...
13
10/1/2012 1 Healthcare Transition: Current Recommendations and their Application October 3, 2012 Patience White, MD, MA Vice President, Public Health Arthritis Foundation Professor of Pediatrics and Medicine George Washington University School of Medicine and Health Sciences Faculty Disclosure Information • In the past 12 months, I have had no relevant financial relationships with the manufacturer(s) of any commercial product(s) and/or provider(s) of commercial services discussed in this CME activity. • I do not intend to discuss an unapproved/investigative use of a commercial product/device in this presentation. Opening Questions About Your Transition • What do you remember about your adolescent/young adult years and health care- when did you leave your pediatrician and move to an adult health care provider? • Was your health care continuous or was there a gap? • Did you leave actively (plan your transfer to an adult HCP) or passively? Learning Objectives • Define health care transition and related data from those involved in HCT • List the key elements of the AAP/ACP/AAFP clinical report on practice-based implementation of transition planning for all youth beginning in early adolescence. • Discuss DC Learning Collaborative process and outcome • Identify opportunities within one's own practice for improvement in the transition of youth from pediatric to adult medical care Who Are CYSHCN? “ Children and youth with special health care needs are those who have or are at increased risk for a chronic physical, developmental, behavioral, or emotional condition and who also require health and related services of a type or amount beyond that required by children generally.” Source: McPherson, M., et al. (1998). A New Definition of Children with Special Health Care Needs. Pediatrics. 102 (1); 137-139. What is a Medical Home? • The American Academy of Pediatrics (AAP) definition: • Primary care that is accessible, continuous, comprehensive, family centered, coordinated, compassionate, and culturally effective • Not a building, house, or hospital, but an approach to providing comprehensive care Source: McPherson, M., et al. (1998). A New Definition of Children with Special Health Care Needs. Pediatrics. 102 (1); 137-139.
Transcript of Faculty Disclosure Information10/1/2012 2 Prevalence of CSHCN NY US CSHCN Prevalence Percent of...

10/1/2012
1
Healthcare Transition: Current Recommendations and their Application
October 3, 2012
Patience White, MD, MAVice President, Public HealthArthritis FoundationProfessor of Pediatrics and MedicineGeorge Washington UniversitySchool of Medicine and Health Sciences
Faculty Disclosure Information
• In the past 12 months, I have had no relevant financial relationships with the manufacturer(s) of any commercial product(s) and/or provider(s) of commercial services discussed in this CME activity.
• I do not intend to discuss an unapproved/investigative use of a commercial product/device in this presentation.
Opening Questions About Your Transition
• What do you remember about your adolescent/young adult years and health care-when did you leave your pediatrician and move to an adult health care provider?
• Was your health care continuous or was there a gap?
• Did you leave actively (plan your transfer to an adult HCP) or passively?
Learning Objectives
• Define health care transition and related data from those involved in HCT
• List the key elements of the AAP/ACP/AAFP clinical report on practice-based implementation of transition planning for all youth beginning in early adolescence.
• Discuss DC Learning Collaborative process and outcome• Identify opportunities within one's own practice for
improvement in the transition of youth from pediatric to adult medical care
Who Are CYSHCN?
“ Children and youth with special health care needs are those who have or are at increased risk for a chronic physical, developmental, behavioral, or emotional condition and who also require health and related services of a type or amount beyond that required by children generally.”
Source: McPherson, M., et al. (1998). A New Definition of Children with Special Health Care Needs. Pediatrics. 102 (1); 137-139.
What is a Medical Home?
• The American Academy of Pediatrics (AAP) definition:
• Primary care that is accessible, continuous, comprehensive, family centered, coordinated, compassionate, and culturally effective
• Not a building, house, or hospital, but an approach to providing comprehensive care
Source: McPherson, M., et al. (1998). A New Definition of Children with Special Health Care Needs. Pediatrics. 102 (1); 137-139.

10/1/2012
2
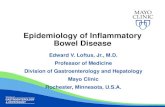
Prevalence of CSHCN NY US
CSHCN Prevalence
Percent of children who have special health care needs
15.0% 15.1%
CSHCN Prevalence by Age
Age 12-17 years 17.9 18.4
CSHCN Prevalence by Sex
Male 17.2 17.4
Female 12.5 12.7
CSHCN Prevalence by Poverty Level
0-99% FPL 16.7 16.0
100-199% FPL 14.8 15.4
200-399% FPL 13.5 14.5
400% FPL or more 14.8 14.7
NY US
CSHCN Prevalence by Hispanic Origin and Race
Non-Hispanic 15.3 16.2
White 15.5 16.3
Black 17.2 17.5
Other 10.5 13.6
Hispanic 13.2 11.2
Spanish Language Household 19.7 8.2
English Language Household 7.4 14.4
Prevalence of CSHCN: NY vs. US
Prevalence U.S. (%)Proportion of Youth with Special Health Care Needs, Ages 12-17
18%(4,581,950)
Proportion of YSHCN with functional limitations 24
Proportion of YSHCN with 2 or more chronic conditions 62
Proportion of YSHCN with emotional, behavioral, or developmental conditions
64
Source: National Survey of Children with Special health Care Needs, 2009/10
How Many Youth Need Transition Services?
What is Health Care Transition?Transition is the deliberate process of moving seamlessly from child-oriented health care to adult-oriented health care.
Components:• Self-Determination• Person-Centered Planning• Prep for Adult Health Care• Work/Independence • Inclusion in Community Life • Start Early
The Transition Process
Transfer of Care
Pediatric Care Adult Care
Transition
SOURCE: Rosen DS. Grand Rounds: all grown up and nowhere to go: transition from pediatric to adult health care for adolescents with chronic conditions.
Presented at: Children’s Hospital of Philadelphia; 2003; Philadelphia, PA
Start Early-How Early?
• Data from studies in Europe and the US suggest age to start transition process is
11-13:
– Youth with SHCN 12-13 yrs: most interested in involvement with future career like their peer group without SHCN
– For YSHCN < 14yrs: there is less of a gap in standardized QoL and life skills measures and show more improvement with transition intervention services than those > 14yrs
– Bottom line: • Transition planning starting at ages 12-13 enabled CYSHCN to stay
on developmental milestones as they grew up compared to those starting transition planning later
WHAT DO DATA TELL US?
What do youth say they want in transition?

10/1/2012
3
Youth are less interested in any transition organized around
medical issues andmore interested in a
transition to financial and social independence.
THE FUTURE JOB MARKET How to be prepared:
• Get as much education as possible• Keep upgrading your skills-retrain• Sharpen career exploration/development
skills to keep up with fast changing technology and global economy
• Expect to change careers - not just jobs -three or four times during the working years
-US Dept. of Labor
Data on Adolescent Work in the USA• Employers rank prior work experience, attitude and
communication skills most important in hiring decisions
• Work patterns of teenagers during the school year:- 40% 7th and 8th graders - 80% high school students
• Parents underestimate youth work hours• Educational level attained relates to survival, future
income level and probability of labor force participation
Post-Secondary Education Issues
• Selection of school: College visits and/or Career training with support services
• Medical supports needed at school, visit to campus (where is the health unit?) and the DDS office, campus size, and plans for local rheumatology care and emergency care.
• Insurance Coverage (is it adequate and is it one plan or a patch of plans)
• Modifications: Work Load, Housing, medications
FACTORS ASSOCIATED WITH RESILIENCE for youth with disabilities: Which is MOST important?
Self-perception as not “handicapped”
Involvement with household chores
Having a network of friends
Having non-disabled and disabled friends
Family and peer support
Parental support w/out over protectiveness
Source: Weiner, 1992
WHAT DO DATA TELL US?
What proportion of parents report receiving adequate transition support for their YSHCN?

10/1/2012
4
Proportion of Youth with Special Needs Who Receive Services
Needed to Make Transition to Adult Health Care
U.S. (%)Total YSHCN meeting transition measure
40%(1,708,799)
GenderMale 37Female 44
Race/EthnicityBlack 28White 46Hispanic 25
InsurancePrivate insurance only 50Public insurance only 26Uninsured 20
Presence of a medical homeWith a medical home 55Without a medical home 29
NA = sample size too small for reliable estimates.
Source: NS-CSHCN 2009/2010
Adolescents Meeting Transition Outcomes: NY and US
Performance on Core Transfer Outcomes NY US
Overall Performance 40% 40%
Gender
MaleFemale
3743
3744
Medical Home
With Without
6324
5529
WHAT DO DATA TELL US?
How prepared are youth for managing their care in the adult health care system?
Internal Medicine Nephrologists (n=35)Survey Components Percentages
Percent of transitioned patients < 2% in 95% of practices
Transitioned patients came with an introduction 75%Transitioned patients know their meds 45%Transitioned patients know their disease 30%Transitioned patients ask questions 20%Parents of transitioned patients ask questions 69%Transitioned adults believed they had a difficult transition 40%
Source: Maria Ferris, MD, PhD, MPH, UNC Kidney Center 2011
Prepare for the Realities of Culturally Different Pediatric and Adult Health Care Services
• Pediatric Services: Family Driven
• Adult Services: Consumer Driven
The youth and family finds themselves between two medical worlds
…….that often do not communicate….
Difference Between Systems
Pediatric Adult
Age-related Growth, development and future focused
Maintenance/decline; optimize the present
Focus Family IndividualApproach Proactive, paternalistic Reactive, collaborative
Shared decision-making With family/parent With patient who is a self-advocate
Insurance/services Entitlement Qualify/eligible
Non-adherence More assistance More tolerance
Procedural Pain Lower threshold Higher threshold # of patients Fewer Greater

10/1/2012
5
What do pediatric and adult physicians say they do and need to assist YSHCN?
WHAT DO DATA TELL US?
AAP Periodic Survey #71 2008 Results*
• 47% assisted with a referral to family or internal medicine• 45% Refer to adult specialists• 33% discussed consent and confidentially issues prior to
age 18• 32% Assist with finding a medical doctor• 27% Create a portable medical record summary• 23% offered education and consultative support to families
or adult providers• 19% assisted in identifying insurance options after age 18• 12% create an individualized health care transition plan
* For all or most of their adolescents
Barriers to transition care for Pediatricians (both major and minor barriers combined):
• 88% lack of their knowledge of community resources • 85% fragmentation of adult health care • 84% lack of adolescent knowledge about their health
condition and skills to self advocate during health care visits
• 80% lack of adult primary care and specialty providers, • 80% difficulty breaking bond with adolescents and
parents • 79% lack of office staff skills in transition • 76 % lack of reimbursement for transition activities
2008 AAP Periodic Survey# 71
Areas to Consider to Bridge the HCT Gap: Provider Needs/Activities
Adult HCP Pediatric HCP • 95% want initial and ongoing communication
with previous providers• 100% request a medical history (written
summary) and disease info
• 47% assist youth with referral to adult physician • 27% create portable medical record• 23% offer consultative support to family or
internal medicine physicians• 80% find it difficult to break the bond with
youth/family
• Youth ready to make independent health decisions
• Disease management skills (know disease/meds/make appt/refill prescriptions, etc.)
• Youth guardianship issues clarified
• 84% of youth lack knowledge about condition• 33% of pediatricians discuss consent and
confidentially issues before 18• 12% of pediatricians create Individual transition
plan
• Medical home • Financing (insurance), infrastructure• Increase medical knowledge of pediatric
diseases• More adult providers (gen and sub)
• Medical home • Financing (insurance), infrastructure• Assist in medical knowledge of adult providers• More adult providers (gen and sub)
Source: DC Provider Survey, AAP Periodic Survey, Annals Int Med Adult Provider Survey
What to do? Where to start?
General Assumption #1
•
• Every youth deserves a continuous medical home as they
grow into adulthood utilizing a transition plan that
matches:
– the youth’s capacity for independent decision making (both well and crisis care)
– the complexity and course of the medical condition(s) – and capacity of family and a circle of support

10/1/2012
6
Health Care Transition ServicesIn the past and currently…• Medical transition services provided by:
– patchwork of pediatric clinics mostly in university subspecialty setting – less common to have transition services in primary care setting– Med-Peds physicians seen as logical providers of transition care services but few
available
• National data reveal little progress made in transition from pediatric to adult health care in last decade despite a 2002 Consensus statement by AAP/ACP/AAFP including identifying core transition knowledge and skills and recommending transition plans
• Literature reviews reveal inconclusive evidence regarding role of transition programs to facilitate transition. Only evidence for improved outcomes suggests meeting adult providers before transfer improves post transfer access and quality of care (Bloom 2012)
• Surveys of pediatricians, family physicians and internists point out the need for more information and support re: transition
New Health Care Transition Clinical Reportbackground
• 2 years ago, AAP/ACP/AAFP appointed a Transition Authoring Group to develop a clinical report based on data and clinical practice
• Clinical Report: Provides practical, detailed guidance (including a step-by-
step algorithm) on how to plan and implement better health care transitions for all patients
Integrates transition planning into the medical home and ongoing chronic care management
Provides guidance for financial support of HCT• Publication: “Supporting the Health Care Transition from
Adolescence to Adulthood in the Medical Home” (Pediatrics, July 2011) – clinical report jointly authored by the AAP, the AAFP, and the ACP
Health Care Transition Clinical Report
• Targets all youth, beginning at age 12 and links the process to the medical home
• Algorithmic structure provides logical frameworkBranching for youth with special health care needsApplication for primary and specialty practices serving
children and adults with variety of conditions Structure for training, continuing education, & research
• Provides explicit practice-based guidance for planning, decision making, and documentation processes
• Extends through the transfer of care to an adult medical home and adult specialists
Health Care Transition Milestones(transition visits from the algorithm)
• Age 12 – Youth and family aware of the practice’s health care transition and transfer policy
• Age 14 – Health care transition planning initiated
• Age 16 – Discussion of youth and parental expectations and preferences regarding adult health care
• Age 18 – Transition to adult model of care even if remain in a pediatric setting before moving to adult model of care (appropriate guardianship issues addressed for cognitive ability)
• Age 18-22 – Transfer of care to adult medical home and specialists with privacy policies and self management skills assessments

10/1/2012
7
National Health Care Transition Center • MCHB-funded resource center, GotTransition.org
• Responsible for developing transition tools aligned with clinical report and fostering practice changes
• Use of Learning Collaborative (LC) methodology used by the National Initiative for Children’s Healthcare Quality (NICHQ) and pioneered by the Institute for Healthcare Improvement (IHI). Primary care expert panel in DC led the way developing
o LC charter oThe 6 core HCT elements based on the algorithm oTransition tools oHCT index for evaluation
LCs in DC, Denver, Boston, NH
For more information: www.GotTransition.org
Methodology: Evidence for Learning Collaboratives
• Learning collaboratives (LCs) – Shown to improve several aspects of pediatric care – Effective method of improving the quality of care delivered by pediatric
practices
• Collaborative teams have achieved dramatic results, including:– Reducing wait times by 50%– Reducing worker absenteeism by 25%– Reducing ICU costs by 25%– Reducing hospitalizations for patients with CHF by 50%
Transition Intervention: 6 Core Elements For Practice Transformation
Pediatric Health Adult Health
1. Transition Policy 1. Privacy and Consent Policy
2. Transitioning Youth Registry 2. Young Adult Patient Registry
3. Transition Preparation 3. Transition Preparation
4. Transition Planning 4. Transition Planning
5. Transition and Transfer of Care 5. Transition and Transfer of Care
6. Transition Completion 6. Transition Completion
Designing a LC for Health Care Transition
• Unique featuresDyads of pediatric and adult practices Involvement of care coordinatorsConsumer involvementWorking across organizations and
systems to improve care throughquality improvement project
• Design and timelinesTeaching and learning strategies Incorporate elements to fit each
practice’s processesPractice, accountability, shared learning
DC as a National Transition Model: Learning Collaborative Teams
Howard University Hospital Team
Children’s National
Medical Center Team
Georgetown University Hospital Team
George Washington University Medical Center TeamCNMC Children’s Health Center -
Adam’s Morgan Team

10/1/2012
8
Goal of Learning Collaboratives:incorporate the 6 core elements into their practice processes
• Develop a written health care transition (privacy and consent) policyfor families, patients, and staff
• Develop a transition registry to know which patients are in the process and tracking major steps in their progress
• Test and use transition preparation and planning tools Portable medical summary Readiness assessments Healthcare transition plans Chronic condition fact sheets Transfer checklists
• Utilize an adult model of care at 18 yrs (if cognitively appropriate)
• Transfer prepared youth/young adults to adult medical homes
FIRST STEP in The HCT Transition QI Process
• Do you have a transition Policy for your practice?A transition policy is an explicit office policy describing thepractice’s approach to health care transition, including the ageand process at which youth shift to an adult model of care(pediatric) or describing the practice’s privacy and consent policy(adult).
• If yes, do you post it for parents and youth to see and give it to all new patients in your practice?
How do we create a systems change so that the rookie learns the rules of the game and we leave no knot untied between pediatric
and adult healthcare?
• Research states policies and procedures among stakeholders are essential– Ensures consensus– Ensures mutual understanding of
the processes involved– Provides structure for evaluation
and audit
Transition Policy Template
• Definition-what is it? See transition definition of Soc
Adolescent Med/BMCH
• Outcome- when the youth has left my practice, he/she should know/have…..
• Timeline- age of initiation and explanation of exceptions
• Components- see AAP consensus statement
• Practice Processes• Evaluation- PDSA cycle
Adolescent Clinic Transition Policy
The Adolescent Health Center is committed to helping all of our patients make a smooth transition from pediatric to adult health care.
This process requires working with you to plan and prepare your transition starting around your 14th birthday.
According to hospital policy, all patients are expected to transition from CNMC to an adult primary care medical home by age 22 years.
We will provide you with ongoing resources to help you to take increasing responsibility for your own health care to the best of your abilities.
We are also able to help you select a medical provider that participates with your insurance, to organize your medical records, and to support all other aspects of planning for this important transition as part of lifelong preparation for a successful and well adult life.
Transition Policy• Challenges
– Getting practice/team consensus, especially regarding age limits– Posting and having policy distributed systematically– Difficulties when consent, privacy, and guardianship issues have not been
discussed prior to age 18. Many parents unaware of HIPAA requirements and want to be present during visit.
– Assessing patient’s decision-making ability
• Benefits– Patient Satisfaction-Families who reviewed the pilot policy said they were
grateful for the information. Many wished they’d had it when their older children were transitioning
– Provider Satisfaction-practice consistency– Clarifies roles of youth/young adults and parents in decision-making– Creates a safe and comfortable environment for those 18 and over to discuss
private concerns regarding their health– Improved adherence and outcomes

10/1/2012
9
Types of Decision Making Support• Informal Supports – Family, friends, and “circle of support” • Money Management – Joint or trust accounts, direct deposit,
direct payment, Social Security representative payee, financial power of attorney, conservator
• Health Care - Health-Care Decisions Act, Durable Power of Attorney for Health Care
• Temporary/Limited / full Guardianship-The specific type of guardianship is defined in the applicable laws for each state/jurisdiction.
• References:– Guardianship webinar available at
http://www.gottransition.org/about-us-news/broadcasts – dcqualitytrust.org: Quality Trust for Individuals with Disabilities
Health & Wellness-The Basics:Yes I do this
I wantto do this
I need To learn
Someone else will have to do this - Who?/NA
1. I understand my health care needs and my chronic illness/disability 2. I can explain my illness, medications and health care needs to others3. I have a list/ can explain my medications and their side effects to others4. I carry my health insurance card everyday
5. I know and pay attention to my baseline health and wellness
6. I track and schedule my own medical appointments
7. I know when to call my provider for prescription refills 8. I know how to call the pharmacy for my refills
9. Before an appointment I prepare written questions to ask or list any concerns I have10. I know what to do when my condition
changes such as when to call my doctor
11. I know what to do in an emergency and have ICE information in my cell phone
Transition Readiness Assessment- For Youth/Young Adults
Transition Readiness Assessment: Challenges
• Addressing range of patient education levels into youth and parent assessment that can be used by entire practice
• Identifying practice process for how all youth/young adults and parents receive and fill out assessment
• How to incorporate readiness assessment into transition plan and into visit discussions/follow-up
• How to incorporate readiness assessment into EMR so it can be updated
• Have available updated readiness assessment for transfer packet for adult provider
• Time constraints
Transition Readiness Assessment: Benefits
• Solicits greater involvement of patients/families in understanding their ability to manage their own health and health care
• Evaluate youth and young adults’ current healthcare knowledge base and skills and identify areas that need further education
• Ultimately, improves the management of chronic condition and the independence of youth/young adults in their own care
What is Your Changing Role in the Transition Process?
Shared Management Model to changing roles
Provider Parent/Family Young Person
Major responsibility
Provides care Receives care
Support to parent/family and child/youth
Manages Participates
Consultant Supervisor Manager
Resource Consultant Supervisor
Portable Medical Summary • Components of portable medical summary
Basic patient personal and contact information Build Health Family Tree https://familyhistory.hhs.gov/ Medical providers, emergency contacts Diagnosis Pertinent history Current medications, equipment needs Allergies Immunizations Special notes — guardianship status, communication preferences Prevention Actions– General: nutrition, physical activity guidelines, routine screenings, tests
according to age– Specific actions/screenings required due to the family health tree eg heart
disease• Portable and electronic and share with young adult/family (before age 18) &
providers• Developed with institution’s HIT team to generate from EMR

10/1/2012
10
Portable Medical Summary: Benefits
• Improves understanding and self-care management
• Prevents duplication of tests/procedures
• Youth/young adults/parents don’t have to repeatinformation to multiple providers
• Improves patient safety
• Ensures adult providers have accurate information
Discuss the Process to find the “Right” Adult Provider for Your youth/young adult
• Prepare a list of desired qualities• Prepare a list of questions• Solicit recommendations from provider/family-friend
network• Check out the internet• Call the adult office to ask how the process works
(attitude, convenience, appointments, cost/insurance, reaching the doctor, hospital, etc.)
• Appointment for an “interview”?
Health Care Transition Transfer of Care Checklist
<Patient Name> <Date of Birth> Date Transfer of care policy discussed with youth and family
Transfer of care options discussed with youth and family
Pediatric primary care practice confirms transfer with adult primary care practice
Final youth readiness assessment completed
Transfer of care package prepared or updated (for all youth, for YSHCN) includingportable medical summary, readiness assessment, emergency care plan, transition planand medical condition fact sheets
Transfer of care packagecommunicated to adult primary care provider via best available means (mail, fax, email, electronic health information transfer)
Initial visit with new adult primary care provider scheduled
Follow-up communication with emerging adult (and family as appropriate)by pediatric primary care team regarding completion of transfer of care and level of satisfaction with result
Follow-up communication with new adult primary care team by pediatric primary care team regarding completion of transfer of care and level of satisfaction with results; identify any future plans/needs for on-going communication or consultation
Risk Stratification/Complexity Score for Practice Communication Strategy
CSHCN Complexity Rating Description Examples Practice Communication Strategy
Low(1 point)
Chronic conditions well-controlled OR
Significant past medical history, quiescent or
resolved
Asthma, mild per.
Repaired ventricular septaldefect
Moderate(2 points)
2 or more chronic conditions, with either
unstable
AsthmaGERD
Asthma with ER visitType 2 diabetes mellitus
Asthma + ADHD
Call between MDs
Complex(3 points)
Any tech. dependent patients
Moderate/ severe cognitive delays
(wheelchair, walker, GT, Trach)
MR, autism, group home respirator
Call between MDs and care coordinators
(+1 point) Language barrier Non-English Speaker(+1 point) Behavioral Disorder OCD, Anxiety in addition to
above(+1 point) Family/ Social
ComplicationsDivorce
(+1 point) Guardianship issues Guardianship not legally established
Total Complexity Score
Developed by The National Alliance to Advance Adolescent HealthAdapted from Chapel Hill Pediatrics
Evaluation: Medical Home Health Care Transition Index
• Indicator #1: Office health care transition (privacy and consent) policy
• Indicator #2: Staff and provider HCT knowledge and skills and coordination of care
• Indicator #3: Identification of transitioning youth/young adults (registries)
• Indicator #4: Transition preparation (readiness assessments)
• Indicator #5: Transition planning (transition plans)
• Indicator #6: Transfer of care or transition to adult model of careAssessments for pediatric and adult practicesEach HCT team self assess at baseline and 9 months4 levels for each indictor and 2 options (partial or complete) within each
indicator
Level 1 (Basic) Level 2 (Responsive)(Includes Level 1)
Level 3 (Proactive)(Levels 1 & 2)
Level 4 (Comprehensive)(Includes Levels 1, 2, 3)
Transition support and services vary among practice providers; staff members are informally aware of these supports and services; families/youth are informed of their individual clinician’s approach to transition as the youth’s needs arise.
There is a uniform, but not necessarily written, transition and transfer of care policy that is agreed upon by all providers and is made clear to staff; families/youth are informed of the office transition policy by age 18 and/or in response to inquiries prior to age 18.
A written transition and transfer of care policy addresses age of transition to adult model of care and (if necessary) age range for transfer to adult health care settings; the policy and its rationale are communicated to families/youth by age 12-14 during encounters and through brochures, posters, and website content
In addition to Level 3, the written health care transition and transfer of care policy addresses preparation, planning, process for transition to an adult model of care and transfer to adult health care settings. By age 18, guardianship, decision-making, and information access rights are determined and clearly identified in the medical record. Practice services include transition encounters, care coordination, & monitoring of steps/progress.
Pediatric Transition Index: #1 Office health care transitionpolicy: each level is rated Partial or Complete

10/1/2012
11
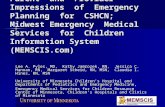
Health Care Transition Index ResultsDC Transition Project-Pediatric Practices
Baseline February 2011
Average scores of four practices: three pediatric, one family medicine
Core elements of health care transition
[Basic]
[Responsive]
[Proactive]
[Comprehensive]
DC LC Pediatric and Adult Practices HCT Index Data
Average total score for each element
Additional Transition Activities• LC spread within each institution• DC transition website –dctransition.org• Collaboration with HSCSN on CME and enduring CME• Collaboration with AJE on parent and youth transition training• Transition payment pilot with HSCSN• Transition and EPSDT with DHCF and new work gorup• Additional training to community health centers, school
nurses, etc.
Final Thoughts
Choose and Do…complete at least two health care transition improvements in the next month
• Ask the youth with SHCN in your practice if they are involved in doing household chores
• Read and share with staff the new AAP clinical report on HCT• Remove, copy, and post the algorithm• Discuss health care transition at office staff meeting• Identify responsible person/team for improving HCT in the office• Draft and adopt a Health Care Transition policy, share with staff, make visible to
and discuss with youth and families• Adopt a Health Care Transition checklist or agenda for office visits from age 14
and older• Actively support the identification of an adult/pediatric medical home practice
and develop open communication and plan transition/transfer processes to improve the transition process for all involved
Learning Objectives
• Define health care transition and related data from those involved in HCT
• List the key elements of the AAP/ACP/AAFP clinical report on practice-based implementation of transition planning for all youth beginning in early adolescence
• Discuss DC Learning Collaborative process and outcome
• Identify opportunities with one’s own practice for improvement in the transition of youth from pediatric to adult medical care

10/1/2012
12
Thank [email protected]
http://www.gottransition.org/
http://healthytransitionsny.comhttp://www.medicalhomeinfo.org/how/care_delivery/transitions.
aspx
http://www.childhealthdata.org/
http://nccc.georgetown.edu/

10/1/2012
13
www.fcsn.org www.fvkasa.org
??? NYLNwww.nyln.org/www.ncwd-youth.info/index.html