Faculty Development Handbook PREFACE
349
Faculty Development Handbook PREFACE Authors: E. John Gallagher, MD, Marcus L. Martin, MD EMERGENCY MEDICINE, AN EMERGING ACADEMIC DISCIPLINE: At the turn of the millennium, Emergency Medicine had been recognized by the American Board of Medical Specialties (ABMS) as a freestanding entity for little more than a decade. In an explicit acknowledgment of Emergency Medicines relatively youthful status as an emerging academic enterprise, in May of 2000, the Board of Directors of the Society for Academic Emergency Medicine (SAEM) charged its Faculty Development Committee with the task of creating a handbook and website intended to provide Emergency Medicine faculty with an academic primer of basic information pertinent to career development. Because many of the SAEM members asked to contribute chapters to the handbook were chairs of academic departments, the Association of Academic Chairs of Emergency Medicine (AACEM) was invited by SAEM to become a co-sponsor of the Handbook. The Faculty Development Handbook is intended as both a supplement and sequel to the 2000 edition of the Emergency Medicine Academic Career Guide, which is an excellent, thoughtfully-written, well- organized, and lucid publication, co-sponsored by SAEM and the Emergency Medicine Residents Association (EMRA). The Academic Career Guide is available both in hardcopy and on the SAEM website at http://www.saem.org. Although the Academic Career Guide contained several chapters pertinent to junior, and, to a lesser extent, senior Emergency Medicine faculty, it was targeted primarily at graduating residents. The Faculty Development Handbook is intended to complement the Academic Career Guide by extending that focus to encompass Emergency Medicine faculty of all academic ranks, ranging from entry-level Instructor to full, tenured Professor. SCHOLARSHIP IN ACADEMIC EMERGENCY MEDICINE: The development of a successful career in any branch of academic medicine is predicated upon the systematic accumulation of a body of scholarly work. The Faculty Development Committee therefore began by seeking a working definition of the term scholarship to serve as the organizing principle for this
Transcript of Faculty Development Handbook PREFACE

Faculty Development Handbook
PREFACE
Authors: E. John Gallagher, MD, Marcus L. Martin, MD
EMERGENCY MEDICINE, AN EMERGING ACADEMIC DISCIPLINE:
At the turn of the millennium, Emergency Medicine had been recognized by the American Board of
Medical Specialties (ABMS) as a freestanding entity for little more than a decade. In an explicit
acknowledgment of Emergency Medicines relatively youthful status as an emerging academic enterprise,
in May of 2000, the Board of Directors of the Society for Academic Emergency Medicine (SAEM) charged
its Faculty Development Committee with the task of creating a handbook and website intended to provide
Emergency Medicine faculty with an academic primer of basic information pertinent to career
development. Because many of the SAEM members asked to contribute chapters to the handbook were
chairs of academic departments, the Association of Academic Chairs of Emergency Medicine (AACEM)
was invited by SAEM to become a co-sponsor of the Handbook.
The Faculty Development Handbook is intended as both a supplement and sequel to the 2000 edition of
the Emergency Medicine Academic Career Guide, which is an excellent, thoughtfully-written, well-
organized, and lucid publication, co-sponsored by SAEM and the Emergency Medicine Residents
Association (EMRA). The Academic Career Guide is available both in hardcopy and on the SAEM
website at http://www.saem.org. Although the Academic Career Guide contained several chapters
pertinent to junior, and, to a lesser extent, senior Emergency Medicine faculty, it was targeted primarily at
graduating residents. The Faculty Development Handbook is intended to complement the Academic
Career Guide by extending that focus to encompass Emergency Medicine faculty of all academic ranks,
ranging from entry-level Instructor to full, tenured Professor.
SCHOLARSHIP IN ACADEMIC EMERGENCY MEDICINE:
The development of a successful career in any branch of academic medicine is predicated upon the
systematic accumulation of a body of scholarly work. The Faculty Development Committee therefore
began by seeking a working definition of the term scholarship to serve as the organizing principle for this

Handbook. Ultimately, we settled upon a classification originally proposed a decade ago by Ernest Boyer
of The Carnegie Foundation, and subsequently adopted by the Council of Academic Societies (CAS) of
the Association of American Medical Colleges (AAMC). This taxonomy divides scholarship into four major
categories, as defined below:
1. The scholarship of discovery is that of original research. This is the predominant form of scholarship
that has traditionally found the greatest favor with medical institutions during the latter half of the 20th
century.
2. The scholarship of integration is that of trans-disciplinary merger of information from disparate
branches of science and medicine, with the goal of formulating creative and novel insights. This is often
the most difficult form of scholarship to characterize because it typically operates at the periphery of
several disciplines, and may consequently be relatively far-removed from the mainstream of any single
area of knowledge.
3. Closely allied to the scholarship of integration is the scholarship of application, which bridges the gap
between theory and practice by bringing new information to bear on practical problem-solving, e.g., bench
to bedside translocation of knowledge.
4. Finally, there is the scholarship of teaching, which requires intelligible communication of valid and
reliable information supported by thoughtful, coherent reasoning from a knowledgeable source to
students, younger physicians, and other colleagues.
Thus, academic emergency physicians may discover, integrate, apply, and teach new knowledge. As is
clearly articulated in the SAEM mission statement, the Society is dedicated to the advancement of all four
domains of scholarly activity, each in the service of improving the care we provide to our patients.
DEVELOPMENT OF SCHOLARSHIP IN THE U.S.:
American universities have struggled for centuries to define scholarship and achieve academic
equilibrium. In contrast, European countries have long viewed research as the primary, if not the sole,
focus of scholarly activity. Over much of the past century the stated mission of many American institutions
of higher learning has been to provide >teaching, research, and service. While the intent may have been
for this scholarly triad to be considered as academic equals, achieving parity has proven elusive. In

recent years, the dominant position has been one of equating scholarship with research. Prior to this in
the history of American higher education there have been two distinctly different views of scholarship:
During the 17th century, schools such as Harvard College were founded to educate exemplary teachers.
Teaching was considered an act of dedication and was honored as legitimate scholarly activity. As the
focus in the 19th century began to shift toward technology and nation-building, land grant agricultural and
technical colleges, supported by federal funding, came to embody the notion of scholarship as service.
The belief that faculty spread knowledge, which in turn improved agriculture and manufacturing, gave
impetus to this notion.
Emphasis on research as scholarship first appeared in American colleges in the 18th century. Some U.S.
scholars went abroad to Germany and other European countries to pursue research activities. However, it
was not until the mid to late 19th century that research in the United States began to gather momentum.
By the middle of the 20th century, largely as a result of World War II, the National Defense Research
Committee was formed and federal grants began to fund an extensive research enterprise whose indirect
costs subsidized many other important activities of the university. Although many American institutions
hired young faculty to teach and perform research, their academic success was almost entirely contingent
upon their contribution as investigators. As the balance of scholarly activity continued to shift toward
greater emphasis on research, teaching and service became less well rewarded and steadily lost value
as academic currency.
In the late 1980s Ernest Boyer of the Carnegie Foundation visited colleges and made the following
observation: What really is being called into question is the reward, and the key issue is what activities of
the professoriate are most highly prized. After all, it is futile to talk about improving the quality of teaching
if in the end faculty are not given recognition for the time they spend with students@. As a result of
Boyers and his colleague Glassick's work, two books were published by the Carnegie Foundation for the
Advancement of Teaching: Boyer's Scholarship Reconsidered@ in 1990, followed by Glassick's
Scholarship Assessed@ in 1997. Through these classic works, the four areas of scholarship defined
above were developed, and are now widely used by institutions of higher education throughout the nation,
including many U.S. medical schools.
THE SCHOLARSHIP OF TEACHING:
Although a critically important and rapidly growing minority of Emergency Medicine faculty are engaged in

the scholarship of application, and to a lesser degree that of discovery and integration, the majority at the
present time are clinician-educators involved primarily in the scholarship of teaching. Because so many
academic emergency physicians are appointed in the clinical track, the Faculty Development Committee
wished to ensure that this Handbook contained information pertinent to the career advancement of those
clinicians dedicated to the scholarship of teaching. This decision was based upon several considerations:
1) As academic medical centers have found it increasingly necessary to expand clinical service in order to
remain financially solvent, clinicians have been recruited as faculty in unprecedented numbers. This
phenomenon is not confined to Emergency Medicine, but now characterizes most of the 24 medical
disciplines within the American Board of Medical Specialties (ABMS).
2) Although most medical schools (about three-fourths) currently have a separate Clinical Track for faculty
whose scholarly focus is teaching, the road to promotion in this track is not as clearly demarcated or well-
traveled as its more Traditional counterpart in research.
3) Valid and reliable tools for measuring scholarship in teaching, such as educational and teaching
portfolios, are untested and less familiar to promotion and tenure committees than are traditional
curriculum vitae containing enumerated peer-reviewed citations clearly demonstrating order of authorship.
4) As the missions of medical schools and their academic teaching hospitals continue to diverge, faculty
valued for their clinical expertise and teaching in the Emergency Department at the medical center have
found academic recognition of their scholarly contributions through promotion at the medical school an
increasingly elusive pursuit. This is a logical consequence of medical colleges and universities assigning
differential values to different forms of scholarship, thus creating a scholarly hierarchy with discovery
situated squarely on top, teaching very much at the bottom, and integration and application located
somewhere in between.
THE SCHOLARSHIP OF APPLICATION:
The decision to highlight career development among clinician-educators should not be misconstrued as a
judgment about the relative merits of other forms of scholarly activity. Rather, it simply reflects the desire
of the Faculty Development Committee to apportion the information contained in this handbook in a
Ademocratic fashion. Because most academic emergency physicians are presently appointed in the
clinical track and heavily engaged in the scholarship of teaching, the Faculty Development Committee

reasoned that the first edition of this handbook should begin by preferentially targeting this majority.
We have no wish, however, to place an emphasis on clinician-educators at the expense of clinician-
scientists, who have been repeatedly characterized as an endangered species, not only in Emergency
Medicine, but throughout all of academic medicine. Indeed, it seems likely that these individuals,
particularly those engaged in the scholarship of application in the form of patient-oriented research, will
play a critically important role in Emergency Medicines maintenance of academic credibility in the future.
Twenty years ago, James Wyngaarden stated, "I continue to believe that there is now a short supply and
an impending scarcity of dedicated physician investigators, and that they are essential to the orderly
introduction of scientific advance into clinical practice." More recently, Harold Varmus of the NIH wrote:
"We simply cannot deliver the enormous promise of the genetics revolution without close attention to
careers in clinical research." In consideration of this, the Faculty Development Committee has chosen to
include a substantial amount of information in this handbook pertinent to Emergency Medicine faculty
interested in developing careers in the scholarly domain of application, particularly as it applies to Clinical
Research.
THE SCHOLARSHIP OF DISCOVERY & INTEGRATION:
Finally, an effort to emphasize the scholarship of teaching and application should not minimize the
importance of the scholarship of discovery and integration. Uncovering new knowledge to achieve a more
fundamental understanding of human illness through basic scientific research will always be a core
activity of academic medicine. Just as the scholarship of discovery increasingly requires collaboration
among different branches of the basic medical sciences, the scholarship of integration furthers the
eclectic possibilities of such interactions by bringing basic scientists together with clinician scientists and
others such as mathematicians, physicists, and engineers. Such cross-pollination logically extends itself
into the terrain of translational research and invokes the scholarship of application. Wherever scholarship
ends, whether with application or teaching, it must begin with discovery and the integration of new
knowledge into what is already known.
ORGANIZATION OF THIS HANDBOOK:

Consistent with the preceding, we have chosen scholarship as the primary organizational axis for this
Handbook. This strategy is similar to that of the Faculty Development Website, whose primary axis is also
organized along the four domains of scholarship. In contrast to the Faculty Development Website,
however, the handbook has a secondary axis, which follows the order of escalation in rank associated
with successful academic advancement:
Section I: Setting the Stage for Faculty Development, contains an introductory section of seven
chapters, intended to place faculty development in Emergency Medicine into a scholarly context; it is
targeted at individuals of Instructor rank, just out of training.
Section II: Early Faculty Development, includes ten chapters aimed at junior Emergency Medicine
faculty of Assistant Professor rank, with the goal of helping these young physicians obtain a coherent
picture of the academic landscape.
Section III: Mid-career Faculty Development, contains eight chapters directed at those academic
emergency physicians approaching Associate Professor rank, which in many institutions is the juncture at
which tenure is considered for eligible faculty.
Section IV: Career Longevity & Strategies for Continued Growth and Success, includes nine
chapters, geared toward more senior academic emergency physicians moving up the promotional ladder
to full Professor and concomitantly into leadership and key administrative roles within their departments
and institutions.
To this we have added a fifth and final section entitled:
Section V: Resources for Faculty Development, a final section that closes with a brief overview of the
Faculty Development Website followed by an extensive Annotated Bibliography of links and references
pertinent to faculty development.
Please direct any criticisms, suggestions, or other comments pertinent to the Handbook to:
The term triple-threat is attributed to an anonymous sportswriter, who used it to describe the gridiron
talents of one Paddy Driscoll, a quarterback for the Chicago Cardinals, the oldest franchise in

professional football. Driscoll, who played both offense and defense, not only passed and ran with equal
facility, but on a particularly memorable fall day in 1924, successfully drop-kicked a field goal from the 50
yard-line. One does not have to be much of a football fan to know that, as the game has evolved and
become increasingly specialized, no single individual would be expected to perform all three tasks of
passing, running, and kicking at a professional level. Hence, with the passage of time, the original
meaning of the term triple-threat has become obsolete.
The analog of the triple-threat in football is baseball's Triple Crown, awarded to the player leading his
league in homers, batting average, and runs batted in (RBI's). No one has won the Triple Crown since the
60's, and many serious observers of the national pastime believe such a feat to be so deeply improbable
that it effectively rivals the impossibility of achieving triple-threat status in the NFL.
It is tempting to conclude from the foregoing that the athletes of today are somehow made of lesser stuff
than those of earlier generations. However, other data, such as the shattering of Babe Ruth's home run
record - which had stood for more than 70 years - twice in the last half decade, belies such an assertion
as a unifying hypothesis. Indeed, the weight of evidence supports the contention that there may never
again be a Triple Crown winner, not so much because players cannot hit the ball, but rather because they
have become specialists. Thus the great hitters of recent years are either swinging for the fences, or
consistently hitting safely, but not both - and without both, the triple crown cannot be won. Baseball still
contains extraordinary hitters, as good as the Cobbs, Hornsbys, Mantles, Ruths, and Williams of the past.
Similarly in football, the Clarks, Driscolls, Hubbards, Hutsons, and Tarkentons are still out there, even
though it is no longer possible to be a triple-threat. This is because, over time, both sports have evolved
and undergone deep and fundamental changes.
In academic medicine, the game has also changed in equally deep and fundamental ways. Shortly after
the second World War, and continuing for several decades thereafter, those academic medical faculty
held up to students and house officers as role models were commonly described as "triple-threats", i.e.,
independently funded investigators, inspiring teachers, and stellar clinicians. In recent years, such
individuals have become very nearly as extinct as bird's teeth. Although extinction is among the most
natural of biological phenomena, when a highly venerated species becomes endangered because the
cultural ecosystem that once supported it can no longer be sustained in an altered intellectual climate,
there is a natural inclination to try and preserve the dying breed. Nowhere is such behavior more evident
than in academic medicine, where the triple-threat seems to have attained the unique fictional status
ordinarily reserved for myth.

Mythology, Joseph Campbell tells us, builds upon the truths and ideals of an earlier time. Viewed as
metaphor, myth is entertaining and often profoundly revealing. However, taken literally, it provokes a kind
of naive nostalgia that holds the present hostage to a selectively remembered past. This latter condition
approximates the dilemma of academic medicine currently and for the last several decades. The
consequence of any attempt, no matter how earnest, to become a triple-threat in the 21st century seems
more likely than not to result in the hollow grandiosity of a double-fake. Although the etymology of the
term double-fake is more elusive than that of triple-threat, its meaning is clear. When used in reference to
an individual, the term describes one who is not what they purport, or might otherwise appear, to be.
To maintain even a modicum of clinical expertise in caring for the nearly infinite variety of ED patients
presenting with undifferentiated illness requires constant vigilance and frequent exposure to minimize skill
decay. The challenge of supervising residents and teaching students requires additional levels of
understanding and the ability to reduce mountains of clinical complexity to molehills of clarity. Add to that,
the demands of basic or clinical extramurally funded research, and one is not only committed to a
minimum of roughly 80-100 hours per week - essentially guaranteeing the absence of any semblance of a
sustainable personal life - but is also looking down the barrel of a future that holds a likelihood of success
only marginally better than the probability of winning the Triple Crown in the American League or
becoming a triple-threat in the NFL.
Perhaps the unarticulated expectation that an individual, given sufficient talent, intelligence, and drive
should somehow be able to do it all in 2002 - as was possible 50 years ago, at a time when one might
actually have been a triple threat in academic medicine (or a Triple Crown winner in baseball) - is one of
the reasons why so many of our most talented young physicians leave residency, turn away from
academics, and enter directly into the private sector. Certainly, the enormous debt service medical
students now carry upon graduation - likened by some to the mortgage on a first home, absent the house
- plays a role in driving such a decision. Nevertheless, the dim prospects of job satisfaction, working
under a set of expectations that become increasingly difficult with each passing year, must also figure
somehow in the choice to forego an academic career.
Based on all of the preceding, we would strongly encourage young faculty to choose carefully, to 'play to
their strengths,’ and to focus their interests as narrowly as possible either on teaching and clinical care or
upon research as an area of primary concentration. Because clinical expertise often goes hand in glove
with clinical teaching, combining these two skills in the role of the clinician-educator is quite common, and
not at all unrealistic. Nor is it difficult to imagine an investigator who is also an outstanding teacher within

the circumference of that individual's research interests. However, to expect independent investigators -
who need at least 75% of their time protected from clinical responsibilities if they are to make meaningful
contributions, obtain independent extramural funding, and avoid becoming "hobbyists" - to perform at the
same level of clinical expertise as faculty colleagues who see patients daily, is a prescription for feelings
of inadequacy and burnout.
Coming to terms with the realization that virtually no one can any longer juggle all three academic balls
with equal agility for the duration of a career - is the first step toward moving beyond the myth of the triple-
threat. Then perhaps, academic physicians can establish for themselves more sensible expectations and
standards to which they can reasonably be held.
This is not to suggest that those engaged in the scholarship of teaching should never involve themselves
in the scholarship of application, nor that scholars of discovery should never set foot in the clinical arena.
Rather, each group must recognize the very substantial limits imposed on meaningful expertise in any
area by dint of the way in which the game of academic medicine has been transformed over the last half
century. Clinicians must limit their research activities to goals appropriate to their knowledge, training, and
experience. This means asking early and often for help from their colleagues in the traditional academic
(tenure) track, and taking care not to tackle unreasonably large or complex questions. There are many
forms of academic writing that are appropriate for the clinician-educator; however, few clinician-educators
should harbor expectations of obtaining RO1 funding. Likewise, successful investigators in the traditional
tracks should see patients, but with the requisite humility and respect for the extraordinary clinical
challenges of Emergency Medicine, lest they unwittingly do harm. They too should seek the frequent
consultation of their clinical counterparts within the department who care for patients regularly - just as the
latter ought to seek guidance when circumstances are reversed. It is the reciprocal relationships among
faculty as a group, fueled by mutual self-respect and a realistic, open appraisal of individual strengths and
limitations, that drives the machinery of a successful academic department. The chair must take the
responsibility for the choreography required to balance such a delicate ecosystem, in order that the
department as a single, integrated, interdependent entity - rather than each of the individual faculty
comprising that whole - becomes a triple threat.
Thus, we end the first edition of this Handbook on Faculty Development on a cautionary note. Either we
must soften the unrealistic expectations we have placed upon ourselves in the past, or risk driving some
very talented young people away from academic medicine. It is critically important that junior faculty focus
as single-mindedly as possible on an achievable goal, without regard for the lingering and slightly

pernicious mythology of the triple threat. If this can be accomplished - difficult as it may be to let go of
longstanding, cherished illusions - young faculty will at least be given an opportunity to rediscover the
enormous personal rewards and intellectual satisfaction that a career in academic medicine can provide.

Setting the State for Faculty Development
What is Faculty Development?
Author: Glenn C. Hamilton
Introduction
Faculty development is about planned change over the course of one’s academic career. Just as
learning represents changed behavior, faculty development reflects a conscious effort to recognize the
skills necessary to succeed in academic medicine, and to set about attaining them in a planned and
paced manner. It is an endeavor pursued over the entire span of one’s career and should be
consciously integrated into daily activities. Having a "Faculty Development Conference" once a year or
even once a month misses the point. It is a fundamental element of our responsibility as academicians
to our students, patients, and institutions.
Origins
There is an etymologic basis for the term "faculty development". The word "envelope" is derived from
the French term meaning to encircle or encapsulate. Therefore, to "develop" is to expand or set free. A
"faculty" is not only an academic role, but also something that "one can do". Therefore, faculty
development can be considered expanding one’s abilities to perform new and different tasks.
My own experience with faculty development began in 1981 when I became the new Chair of the
Department of Emergency Medicine at Wright State University. Moving into an academic administrative
role only a few years after residency gave immediate insight into the skills necessary to succeed in this
new role. Many of these skills were not clinical, and the focus of my academic activities to that date had
been on teaching. Employing the fundamental principle of "enlightened self interest", a skill set
necessary for me to learn was created and one that also would be exciting for the new faculty I
anticipated hiring into the department. In July, 1982, our first "scope" document was created (a faculty
development process in itself) which included an outline for fundamental skills necessary for all faculty
to succeed in the Wright State University SOM academic environment. This effort grew into
presentations at the Society of Teachers for Emergency Medicine in 1983, first published in the STEM
Newsletter. After that, it was simply a matter of working with a number of interested individuals with a
wide variety of ideas on how to institutionalize this concept as a cornerstone of our specialty growth.
That opportunity came in 1988-89 when the Resident Review Committee in Emergency Medicine was

completing one of its several iterations of the Special Requirements in Emergency Medicine. Included
for the first time was a section that expressed faculty development was a requirement of an academic
faculty and one of the accreditation criteria for a residency training program. The willingness of the
membership of the RRC in Emergency Medicine at that time to include this small addition has had
significant impact on the excellence of both faculty and training programs in the specialty. There are
obviously many other components to insure this excellence, but the fact remains Emergency Medicine is
the only one of 24 specialties that requires faculty development as part of its own Special Requirements.
This is at least one of the reasons why you are reading this now.
Fundamentals
Just like Stephen Covey’s "Seven Effective Habits", there are at least seven fundamental principles to
integrating faculty development into one’s departmental/divisional activities and individual career
planning.
Organization and Implementation is the responsibility of the department/divisional leadership.
Although individual faculty will have motivation to develop themselves, the organization and
implementation of a faculty development program should begin at and be sustained from "the top". The
Chairperson or equivalent has the vision for the institutional unit, the vestment in its success long term,
and the resources available to make planned change as both a tactical and strategic decision. Just as
Demming’s Continuous Quality Improvement principles begin at the leadership level, this kind of
sustained effort supporting faculty development must have the Chair’s understanding and personal
commitment.
Motivation methods are part of success in faculty development. Despite all good intentions, many faculty
members are uncomfortable with change or unsure how to initiate it in an effective way. They need
guidance and encouragement as well as stimulation. Guidance can come from mentorship,
encouragement from rewards, and stimulation from incorporating faculty development as part of the
evaluation process. The educational adage "evaluation drives learning" is as true with faculty as it is with
students. The goal of the rewards is to always emphasize the positive, but on occasion the negative
consequences of avoiding a planned change activity must be clearly communicated. This can only be
done by the leadership of the institutional unit, and the faculty must recognize the leader’s commitment,

or they will be tempted to side step the effort, knowing that it will "blow over" soon enough.
Link activities to the value of the school reflected in promotion criteria.
There are many tangible and intangible rewards to faculty development but one of the most prominent is
promotion. What is valued by an individual must be linked to what is valued by the institution. A faculty
who loves to teach at the bedside, but resides in an institution that only values bench research will
eventually become tired and dissatisfied with being under-appreciated by peers and the institution. It is
the Chair’s role to assure this alignment between individual talent and institutional values.
Part of this orientation is simply faculty awareness of the promotion criteria. These need to be reviewed
with new faculty and again with experienced faculty on at least an annual basis. This can be part of the
annual faculty evaluation. Another part of this evaluation should be the establishment of a promotion file
(Table 1). This simple outline gives one example of a file that can be used to maintain documentation in
anticipation of a promotion application. An annual review of this promotion file by the Chair will go far to
make sure that it is kept reasonably up-to-date. There is no reason for a faculty member to be
scrambling to try and remember what he or she had accomplished five years earlier at the time of their
being considered for Associate Professor promotion. This information is not retained in the curriculum
vitae and documentation of actual scores and performance responses must be included as part of the
document.
Another component of linking individual values to school values is to integrate planned promotion into
the job description. If it takes 8-10 papers to be considered for promotion to Associate Professor and 4-5
years as a reasonable time frame then expecting a faculty member to publish two papers per year in
peer reviewed publications is both appropriate and effective planning. Asking each faculty member to
develop goals and objectives on an annual basis, shaping those goals and objectives to fulfill promotion
criteria as well as departmental goals and tracking those goals and objectives in both private and public
forums is one means of translating individual abilities and desires into institutional recognition and
responsibility.
The "perfect faculty" is created by the assembled skills and talents of all the faculty.
The "triple threat" existence of research, service and teaching is difficult, if not impossible, to maintain
without considerable sacrifice of one’s youth and family. In addition, administrative and interpersonal

skills must be added to that triple threat capability to make it fully effective. There are few, if any,
individuals who can carry it all for a sustained time period.
Both the department leadership and individual faculty members should anticipate that their collective
interests will be served by emphasizing the individual strengths of members in such a way that
departmental goals are attained. Starting with faculty goals and incorporating them into an eventual
departmental strategy allows the individual faculty a clearer understanding of decisions and
opportunities available to other faculty. These decisions should be made in an open communication
environment. We must have mutual collegial support in our institutional units, and recognize the benefits
of differing abilities and aptitudes.
The scope of faculty development content must remain as broad as possible.
The principles of adult education must be applied.
Faculty represent one of the most sophisticated groups in which to sustain educational growth. At the
beginning, adult education principles must be integrated into any faculty development program. These
include the following:
The learner must be active in the learning process. Passivity will beget forgetfulness.
The learner must have the opportunity to practice new knowledge or skills. Learning
without responsibility for applying that learning begets forgetfulness.
The learner must receive immediate feedback about performance of new skills. Mastery
of new skills can not be assumed, and ingraining of bad habits can not be allowed.
It is essential that the underlying principles of new knowledge or skills be understood.
We don’t accept superficiality or the term "cook book" medicine in our specialty. There
is no reason to accept rote, repetitive behavior without fundamental understanding in
our faculty.
New abilities must be transferred into the real world. This is part of reinforcing new
knowledge and skills, but just as importantly making them operational to the benefit of
all.
Different learning methods of individuals must be recognized and appreciated. Taking

the time to analyze an individual faculty’s best educational means is one of the earliest
investments in faculty development.
Integrate expectation of faculty development into the evaluative process.
By making faculty development progress part of the evaluative process, the idea becomes integrated
into the departmental/divisional culture. There are many ways by which this can be approached. At our
own institution we use four components:
1. Spring Retreat - in advance of the academic year, faculty are expected to develop goals and
objectives for their activities during the upcoming year and present them to the other faculty. This
specifically includes a discussion of faculty development skills to be attained. In this discussion, it is the
Chair’s and other faculty’s roles to make suggestions about how this interest in new skills may be
translated into adult learning principles, especially active responsibilities in the department. For
example, one faculty expressed an interest in gaining internet skills. She was given the assignment to
develop the departmental/residential web site, with a time table appropriate for resident review of the
program the following Fall.
2. Fall Retreat - in addition to other topics, each faculty briefly reviews their goals and objectives at a
"mid-course evaluation", and occasional "mid-course confession and need for correction". Having the
responsibility for a public dialogue about one’s progression toward previously espoused goals adds an
appropriate accountability for accomplishing them. If two or three years pass with the same goals being
presented but not accomplished, it is reasonable for both the Chair and other faculty to suggest the
individual rethink the value they are placing on these proposals, and move on.
3. Regular Chair/Faculty Meetings - since we are a relatively small department, there is the luxury of
individual meetings with faculty on a regular basis throughout the year. Faculty development status and
means by which goal accomplishment may be facilitated are a key part of these discussions.
4. Annual Review - since 1982, we have used a 400 point scoring system to assess the performance of
the faculty on an annual basis. Included in this system is a substantial recognition of faculty
development activities.

An important part of implementing this integration of faculty development into the evaluative process is
to make sure that it is established in advance of the academic year. Faculty should understand they will
be expected to progress in the areas they choose and assignments will be made to assist them in that
progression. At the same time, specific departmental needs will be considered as a means of prioritizing
individual faculty desires for new skills.
Anticipate creativity and accept some failures.
Faculty development can not become burdensome. It has to be integrated into individual values and
become part of regular activities. The more open the discussion about specific faculty needs, the more
potential exists for creativity to occur. Bringing in outside talent, sending individuals to conferences,
collectively putting on presentations with specific themes, group writing, group reading, field trips (such
as to the genomics laboratory) are all a part of a creative approach to success in faculty development.
At the same time, failures will occur and should be expected. Those may be process failures such as
attempts for specific types of retreats that don’t work out, or collective reading efforts that gradually
taper off. There will most certainly be individual failures whereby an individual professes an interest in a
specific skill but demonstrate little aptitude for it. The Chair may support an individual for a prolonged
period of time as part of their growth and then have that individual move on to another setting where that
new skill is applied. Accepting that the end point of faculty development may be the reality of the faculty
member moving on to another venue reflects the truth of promoting individual growth.
Library for Faculty Development
One of the benefits of the maturity of our specialty, and this current monograph reflects it, is there are
now a number of valuable resources for faculty to consider in both choosing faculty development topics
and pursuing them. Listed in Table 3 is a sample library given to each new member of the faculty at
Wright State. Whether each of them reads it or not is another question. But, importantly the tone is set
from the beginning that they will be expected to gain skills and are given resources to assist them in
doing so. Over the years, it is apparent that these books are utilized as necessary, but in some way

serve as a reference based safety net for trying new things. The textbook by Carol Bland, et al.
"Successful Faculty in Academic Medicine: Essential Skills and How to Acquire Them" remains one of
the best of the genre.
Future Directions for Faculty Development.
The exciting future for faculty development is only limited by the level of creativity and interest enjoined
by all of the faculty in our specialty. The departmental/divisional leadership has responsibility for making
this occur, and most fortunately, the RRC in Emergency Medicine has assured that a regular review will
be held on this subject. Therefore, the future is bright, and only a few observations on its potential
direction remain.
A continued emphasis on academic management skills must be made. If a faculty
member can’t manage their time, productivity, and money, they will always have
problems in fulfilling their responsibilities in teaching, research and service.
Clinically based cultural competency will become an essential for faculty over the
course of the next 5-10 years. Our specialty is behind in its recruitment of minorities and
we respond academically to the cultural needs of the populations we serve in a limited
way.
Funding for faculty development in Emergency Medicine will continue to be an issue.
We have not been the recipients of generous federal dollars such as has occurred in
Family Medicine. At the same time, as well demonstrated by this handbook, it doesn’t
necessarily take a great deal of money to facilitate motivated individuals. That fact
remains the strength of our specialty.
Summary
Faculty development represents planned change in academic growth. It represents one of the significant
assets of our specialty, and remains a centerpiece of our survival efforts in the ever competitive and

complex environment of academic medicine. Lastly, the best approach to faculty development is a
mature one. To close where I began 20 years ago, approach the subject with "enlightened self-interest".
Always share the new knowledge you have learned with others.
Table 1 - Faculty Promotion File
An integral outcome of faculty development is faculty promotion. It is appropriate that each faculty
member keep a record of activities in areas that will impact on promotion and/or merit pay raises. This
type of file can be invaluable in assisting department chairmen in writing promotion/recommendation
letters, and it allows the faculty member to keep a tally of activities that may not usually be placed in
one’s curriculum vitae.
I. Teaching Activities
1. Major Conferences
2. Topics in Emergency Medicine
3. Yearly Directed Conferences
4. Small Group Conferences
5. ACLS/ATLS/PALS
B. University/Medical School
1. MS 1, 2
2. MS3
3. MS 4
C. Hospital
1. Emergency Medicine

2. Other Specialties
D. Paramedic
E. Nursing/Other
F. Regional/National
G. Evaluation of Teaching Performance
1. Chairman/Faculty
2. Resident
3. Medical Student
4. Clinical Faculty/Practitioners
5. Nursing/Other
6. Paramedic
7. Regional/National
H. Research
1. Manuscripts/Abstracts
2. Meeting Presentations
3. Projects in Progress
4. Grants Prepared
II. Non-Research Publication
1. Case Reports
2. Clinical Reviews

3. Book Chapters
4. Editorials
5. Letters
6. Other
J. Honors/Awards
K. Editorial Board Activity
L. CME
III. Professional Service/Appointments
A. University/Medical School
1. StandingCommittees
2. Task Forces
B. Department of Emergency Medicine
1. Committees
2. Assignments
3. Faculty Services
a. Advising/Counseling
b. Resident/Student Evaluation/Recommendation
c. Residency Applicant Review
4. Other Contributions
C. Community
1. EMS Council

2. Medical Society
3. Hospitals
4. Local/City Government
D. State/Regional Organizations
1. ACEP
2. SAEM
E. National Organizations
1. ACEP
2. SAEM
3. AAEM
4. ABEM
Table 2 - FACULTY DEVELOPMENT CORE CONTENT
1. Accreditation (RRC) / Certification in EM (ABEM)
2. Business Aspects of Academic EM
3. Clinical and Research Use of Statistics
4. Counseling
5. Curriculum Planning / Design
Specific Curricula

Problem-based
6. Decision Making / Analysis
7. Diversity Issues
8. EM in Health Care System
9. EMS/EMS Research in Academic Setting
10. Ethics/Legal System - applied to academics
Misconduct and Fraud
Consent
11. Evaluation Skills
12. Evidence Based Medicine
13. Faculty Development Process / Outcome
14. International Aspects of EM
15. Interpersonal skills
16. Interviewing Skills
Residents / Match Process
Faculty
17. Managerial Skills
Time Management
18. Manuscript Review
19. Media Techniques and Medical Education

20. Medical Photography
21. Medical School Structure / Activities / Roles
22. News / Media Relationships
23. Physical Wellness
24. Political Awareness / Activism
National EM Organizational Issues
Legislative Process
GME Funding
25. Research Skills
Clinical
Basic Science
Grants / Funding
Education
26. Running the Academic ED
27. Scholarly Writing/Presentation/Publications
28. Stress Management
29. Teaching Skills
30. Technology in EM

31. University Hospital organization
32. Use of computer
33. Work vs the rest of your life
Table 3: Sample Library for Faculty Development
Drucker P The Effective Executive, New York, Harper and Row, 1993. (several reprintings)
King Ls Why Not Say It Clearly. 2nd
Ed, Boston, Little Brown, 1991.
Stunk W, White EB The Elements of Style. 4th Ed, New York, MacMillan, 2000.
Whitman N, Schwenk TL The Physician as a Teacher. 2
nd Ed, Salt Lake City, Whiteman
Assoc, 1997.
Huth EJ How to Write and Publish Papers in the Medical Sciences. 3
rd Ed,
Baltimore, Williams and Wilkins, 1999.
Gehlbach SH Interpreting the Medical Literature. 3
rd Ed, New York, MacMillan,
Boston, Little Brown, 1996.
Ingelfinger JA, et al Ingelfinger, JA, et. al. Biostatistics in Clinical Medicine. 3
rd ed., New
York, Mc Graw-Hill, 1994
Sackett DL, et al Evidence-Based Medicine,Edinburgh, Churchill Livingston, 2
nd ed.
2000
Ogden TE, Goldberg IA Research Proposals. 2nd
Ed, New York, Raven Press, 1995.
General References: Bland CJ, et al
Successful Faculty in Academic Medicine Essential Skills and How to Acquire Them, New York, Springer, 1990.
Is Faculty Development Effective?
How to Evaluate the Effectiveness of a Faculty Development Program
Author: Georges Ramalanjaona
Introduction
Evaluation of the effectiveness of any faculty development program (FDP) is crucial to provide
assessment of existing programs as well as yield valid recommendations for designing future programs
that better address the needs of individual faculty members and the sponsoring institutions. Although
evaluation can be a complex and challenging process, we cannot afford to ignore the need because of its

importance for the growth and reputation of our specialty in the house of medicine.
This chapter offers pertinent suggestions on how to evaluate a FDP at local or national levels based on
current recommendations from educational literature. It will discuss the rationale for evaluation, choice of
potential evaluators, current methodology for evaluation, financing of such assessment, and suggest
future research on the topic.
Rationale
There are a number of reasons mandating the evaluation of a faculty development program in Emergency
Medicine. There is a paucity of published studies in our literature on the short or long-term impact on
participants of any educational program. SAEM instituted a national educational program beginning in
1996 but thus far has not published any peer-reviewed articles on its impact on participants or the
specialty of Emergency Medicine. Our specialty is in need of objective guidelines for evaluating existing
programs to assist in planning future activities.
Most of the research in this field has been done by other specialties such as family medicine, pediatrics,
and internal medicine. However, among the few programs that have published studies on evaluation of
their activities, data consisted mainly of satisfaction surveys collected immediately after the conclusion of
the program. Research has shown that participant satisfaction with instruction does not correlate with
change in behavior after instruction. It has been shown that educators can develop and implement more
effective evaluations that go beyond simple satisfaction data. Therefore, the FDP instituted by SAEM, as
well as other FDPs, should be subjected to a systematic, regular, and comprehensive evaluation to
assess desired outcomes on participants to determine its efficacy. We propose evaluation strategies
(validated from the literature) that include learning, performance, and satisfaction data. General principles
of faculty development program evaluation can be tailored to our national, regional or local educational
programs since there are no current uniform guidelines for evaluating faculty development programs in
emergency medicine.
Assessment of the effectiveness of any FDP can be performed by sponsoring organizations or by
independent evaluators experienced in the field for better objectivity.
The proposed methodology describes the ideal evaluation model that is available to all FDPs. However,
since the full implementation of this model is time-consuming and costly, its application should be tailored

to each individual and regional program, as well as to programs sponsored by national agencies.
Methodology
Kirkpatrick, in his Practical Guide for Supervisory Training and Development Handbook (1), has described
an evaluation model with four levels of program outcomes:
The first and simplest outcome level is reaction (satisfaction data), which focuses on
participants' satisfaction with the program (Level 1).
The next outcome level is cognitive (learning data), which refers to program influences on
changes in knowledge and learning attitudes of the participants (Level 2).
The third outcome level measures behavioral changes (performance data), which point to
measurable trainee activities outside the training environment that can be attributed to
faculty development program influences (Level 3).
The final step is the results outcome level, which focuses on the impact of a faculty
development program's influence on the learner's career (Level 4).
Many experts in the field believe that evaluators should focus on higher evaluation levels
rather than just the participants' satisfaction (Level 1) to increase stakeholder support for
the program.
Following Kirkpatrick's Model three types of data should be collected over a period of
time starting from the first day of the program and continuing until nine months after
completion. These include 1) satisfaction (reaction data), 2) learning (cognitive data) and,
3) performance data (behavioral data).
Three different types of instruments are used to collect the three types of data: 1) End of
Session Evaluation Forms, 2) Pre-Test, Post-Test, and Delayed-Post Test assessments,
and 3) Delayed Follow-Up Interviews.
1. End of Session Evaluation Forms
The focus of this instrument is to report participants' satisfaction with instructors, curriculum, facilities, and
the whole program. Learners may also be asked to provide self-assessments of their competence on
selected session topics.

2. Pre-Test, Post-Test, Delayed Post-Test
The same test is administered as the Pre-Test, Post-Test, and Delayed Post-Test to assess, respectively,
initial knowledge, changes, and retention of cognitive knowledge up to nine months later. This test
instrument should encompass all the essential elements taught during the faculty development program
(i.e. conference, workshop). Testing methods can vary between written and other testing methods
depending on budgetary and time constraints. Participants' knowledge and skills should be tested in the
following six emergency medicine domains, depending on the curriculum of the faculty development
program being evaluated: Research, Education, Grant Administration, Academic Skills, Mentoring, and
Professional Communications.
All three sets of tests (Pre, Post, and Delayed Post) should be scored independently by two raters trained
by the evaluators. To ensure inter-rater reliability, each rater independently scores all three sets of tests.
Then all three-test scores from both raters are averaged to arrive at a single score for each participant on
each test. Cohen's Kappa Test to determine inter-rater reliability should be performed if tabular marginals
are balanced. If they are unbalanced, simple proportionate interrater agreement, although unadjusted for
chance, may be methodologically preferable. . The reliability of this type of process has been reported to
be high (KAPPA > 0.75) and has both content and criterion validity. (2,3)
The effect of the faculty development program on the specialty of emergency medicine can be evaluated
by comparing the outcome scores of the participants of the program (Experimental Group) with the
outcome scores of randomly selected, non-participants (Control Group) using the Pre-test/Post-Test
design on both groups. The number of Control Group Faculty should equal those of the Experimental
Group.
3. Follow-Up Interview
This investigation has the goals of 1) gathering additional information from participants concerning
satisfaction, learning and performance data and application of session content at the participants'
institutions and, 2) determining participants' current status in academic emergency medicine, their
scholarly productivity, and assessing how well their faculty development program prepared them for their
current academic position.
Finally, the evaluator should interview the Program Director of the Faculty Development Program
(National and Regional FDP) using a separate interview protocol with open-ended questions.
Data Analysis
Data analyses should contain both quantitative and qualitative information.
For quantitative items, standard parametric and nonparametric statistics are used, depending upon the
distribution of the data and sample size. Qualitative analysis of open-ended questions is conducted by
grouping similar comments for each question and instrument.
Financing Faculty Development Evaluations
The financial support for development and implementation of evaluation of faculty development programs
can be provided by a variety of funding sources that can be used singly or in combination:
Internal institutional support: Department Chairs must use their resources not only to
balance organizational with individual faculty member's needs but to evaluate the
effectiveness of their faculty development program.
External private funding.
External public grants such as the Federal Grant Program specific for Faculty
Development in Family Medicine.
Future Research
Questions that should be raised to evaluate the effectiveness of the existing programs and the success of
future activities include:
1. How successful is the program in preparing young faculty for their academic careers?
2. Do the current Local/Regional/National Programs fulfill the academic needs of emergency medicine
participants?
3. What is the long-term impact of faculty development programs on participants' academic productivity
and professional careers?
Conclusion

We have provided a guideline for evaluation of existing faculty development programs based on the
current literature of adult medical education and research performed in the field. We need to acknowledge
that this is an evolving field even for the established medical specialties. Our involvement in the research
and application aspect of the evaluation process will be invaluable for the growth and maturity of our
specialty.
References
1. Kirkpatrick D.L. A Practical Guide for Supervisory Training and Development. Reading, Mass; Addison-
Wesley, 1971
2. Hewson M.G., Copeland L.H. Outcomes Assessment of a Faculty Development Program in Medicine
and Pediatrics. Academic Medicine. 1999; 74 (10): 568-571
3. Morzinski J.A., Schubot D.B. Evaluating Faculty Development Outcomes by Using Curriculum Vitae
Analysis. Fam. Med. 2000; 32(3): 185-9
Additional Bibliography
Bland C.J., Stritter F.T. Characteristics of Effective Family Medicine Faculty Development Programs.
Fam. Med. 1988; 20: 282-8
Hamilton G.C. Faculty Development in Emergency Medicine. Am. J. of Emerg. Med. 1988; 6(5): 540-4
Hitchcock M.A. et al. Faculty Development in the Health Professions: Conclusions and
Recommendations. Med. Teach. 1993; 14(4): 295-309
Irby D.M., Hekelman F.P. Future Directions for Research on Faculty Development. Fam. Med. 1997;
29(4): 287-9
Reid A. et al. Assessment of Faculty Development Program Outcomes. Fam. Med. 1997; 29: 242-7
Royse D.D., Thyer B.A. Program Evaluation: An Introduction Chicago: Nelson-Hall, 1996
Sheets K.J., Henry R.C. Evaluation of a Faculty Development Program for Family Physicians. Med.
Teach. 1988; 10(1): 75-8

Organization, Prioritization, and Time Management
Organization, Prioritization, and Time Management Skills
Author: Debra Perina
Introduction
One constant in the universe is that time advances regardless of how much we might wish it wouldn’t.
Day turns into night, we advance in age each year, and deadlines continue to creep up on us before
they’re even set (or so it seems)! Developing organizational skills as well as effective time management
and prioritization techniques are paramount to success as an academician. All who choose an
academic career engage to varying degrees in the components of the "three-legged stool" of clinical
practice, teaching, and research. Of course, each of these components could easily make up a 40 hour
work week. However, to have a fulfilling career and be successful in achieving promotion and tenure
one must demonstrate excellence in scholarship in at least two of these three areas, with the weighting
of each varying greatly from one institution to another. Productivity is largely dependent on effective
time management. Since we all operate with a finite amount of time, it is important to learn techniques
to optimize the time we do have, being ever mindful of the necessity to achieve a healthy balance
between the time needs of an academic career and our personal lives.
Setting Priorities
Early on in an academic career, one quickly realizes that a balancing of priorities must occur. Clinical
practice time will obviously be a constant that will be minimally affected by time management
techniques. The remaining time must be divided between teaching, administrative and research efforts.
Time must be allocated to each of these areas for career growth and success. Establishing priorities for
each of these areas must be individualized according to the career goals one has set. Teaching and
administrative activities often fill the majority of non-clinical time. However one must remember that
effective research is absolutely necessary for academic advancement. This can only be accomplished
if you develop a plan and have specific goals. In spite of this, young academicians rarely appreciate the
necessity for dedicated research time. Research time is frequently carved out of time left over from
clinical, teaching, and administrative assignments. This approach rarely leads to success. Early on, in
an academic career it is just as important to schedule dedicated time for research as it is to allocate
time to other activities. Try to schedule a dedicated time each week devoted to research and guard it
jealously. This works best if the time is spent outside the office to avoid interruptions and impromptu

meetings.
Clinical Workload
As ours is a patient centered specialty, a certain amount of clinical workload is welcomed for personal
satisfaction and clinical teaching opportunities as well as necessary to generate revenues. However, a
certain amount of protected time from clinical activities is necessary to be productive in other academic
areas. Most academic departments reduce clinical load for faculty to ensure their (and the
department’s) academic success. As changing reimbursement patterns whittle down departmental
finances, more pressure exists to offset costs with clinical revenues. In general, if clinical time exceeds
28 hours per week, it becomes extremely problematic for faculty to sustain academic productivity.
Potential ways to offset clinical time beyond negotiated work hours include clinical buy-down time from
contracts or grants, stipends for administrative assignments, or pass-through fees for lectures,
presentations or legal work.
Administrative Tasks
Emergency medicine junior faculty are frequently given more administrative assignments than junior
faculty in other departments. These assignments often require many meetings and significant office
time. If possible, try to limit the amount of administrative assignments during the first 3 years of your
career. This will allow you to establish yourself and develop a routine that can then be used to carve
out administrative time. If you are given an administrative assignment try to negotiate something in
return, such as a decreased clinical workload, more secretarial, or research help to offset the time you
will spend doing administrative tasks. If given a choice of tasks, try to choose one that is most
consistent with your areas of interest or research. Thus you can combine interests and goals to
enhance productivity. One example of this would be appointment of an individual with research
interests in patient outcomes as the quality improvement. Try to combine the research interest with
administrative tasks and design a project looking at patient outcomes that can double as a quality
improvement indicator. Get triple duty from this assignment by developing a lecture series on quality
improvement for the residency and designing a rotation as part of the administrative experience for the
residents. You have now combined the areas of research, teaching, and clinical practice into one area
that coincides with your administrative assignment. This will significantly reduce the marginal time
expenditure required to accomplish each of these tasks, compared to achieving them in unrelated

areas. This also has the added bonus of creating a "focus area" whether you intended to do so or not,
which is something that many promotion committees look for as evidence that you have an area of
excellence.
Meetings: Schedule your own meetings, or make sure that you approve all meetings before they’re
scheduled. If you do not control the number of meetings you attend, you will quickly find they take up all
your free time. Make sure you know the purpose of a meeting prior to agreeing to go. If there is no
defined purpose or the meeting does not have a direct relationship to your area of expertise or
assigned administrative duties, you may not want to invest the time unless your presence is absolutely
necessary. While offers to join committees are flattering, be aware that they can take on a life of their
own. If you are an effective contributor you will likely be solicited for further committees. Although some
committee work is necessary for career growth and can open doors for involvement in state and
national organizations, you must choose how to spend your time wisely to avoid being over-extended.
Time Management Principles
With only limited time to accomplish your goals, time management principles are the key to success
and happiness as an academician. Effective time management revolves around good planning. Experts
estimate that for every hour of planning three hours of time are gained. There are several key
components to managing time effectively. Each are discussed below and in further detail in Chapter
4.9.
Develop a mission statement: This is a statement of what you want out of life and your career in
relation to it. From this statement develop specific goals to help you achieve your personal mission
statement. These goals will help you decide how to spend your time. When faced with a new
assignment or task, compare it against your personal goals and mission statement. This will help you to
decide if the task is worth the time invested, and give you the ability to prioritize the task on your
accomplishment timeline. You should re-evaluate your personal mission statement at least once every
six months to make sure that it is still consistent with your view of what you value in life and where you
want to be.
Set goals: Goals should be set in conjunction with your mission statement. What needs to be done to
get where you want to be? Each step should be a defined goal. Setting appropriate goals can be

difficult. Remember to be realistic. Goals should be challenging, forcing you to grow and develop. If you
reach all defined goals too quickly, you are probably setting them too low. On the other hand, setting
goals that are too high or unobtainable will only frustrate you and diminish your overall productivity.
Take small steps initially building on each success to reach goals. Reset your goals frequently to
ultimately achieve the final endpoint in your mission statement. Deadlines should be set for each goal.
Setting realistic goals is very important. However, they cannot be set unless you understand your job
expectations and requirements. This is where a mentor can be invaluable. A well chosen mentor can
help you review your goals, determine if they are realistic and appropriate, and provide you with ideas
for reaching them. To achieve a balance in one’s life, personal goals should be set in conjunction with
career goals. This synergism ultimately leads to greater productivity because you naturally feel most
fulfilled if both your career and personal life coincide with your image of yourself.
Organizing calendars and prioritizing: Create a daily schedule and stick to it as much as possible. Try
to minimize the number of interruptions that may interfere with staying on schedule. Such "time
robbers" include impromptu meetings and phone calls. Get a personal organizer and keep it with you at
all times. Consult and update it frequently. Prioritize items to be accomplished. This is not simply
creating a "to-do" list, but setting out the proper priority of each task in order to achieve the best quality.
All of us have peak creative times that correspond to our natural circadian rhythms (so-called larks
(day) and owls (night)). Try to use your naturally most creative time to write publications, review
articles, or work on research projects. Since answering email is less mentally tasking, save it for other
times. Try to answer your emails only once a day, as this can be a real time sink. Although it is
important to spend office time when your colleagues and others can interact with you, an open door
policy will likely make it very difficult for you to accomplish your goals. It is better if you can spend a
portion of your office time during off-hours to avoid interruptions. Many seasoned academicians find
this to be their most productive time. Just as important as working in the office is "downtime" to
recharge your batteries. This is the time devoted to the things in life you enjoy doing recreationally.
Remember to schedule this time. It is just as important to your overall success by helping you to
maintain focus and optimum performance.
Delegate: Learn to delegate effectively! Many of us do not delegate items well, believing we can do
them faster and better than others. It is a simple fact of nature that we can’t do everything. It is
important to make the distinction between what you can assign or teach others to do versus those
tasks that only you can achieve. This type of prioritization allows you to be most effective. Others

produce some of the needed items leaving you enough time to produce the items only you can create.
Make a timeline for completion of projects and update your progress weekly. This can help you keep
tabs on how your time is spent and can also be important when asked for accountability and
productivity.
Just say no: Early in your academic career it is important to take advantage of opportunities offered
you. This said, it is equally important not to over extend yourself in order to be able to complete projects
you undertake well and within the defined timeline. Each task should be compared against your
personal mission and goals. Accept the assignment if it is consistent, and time allows you to do a good
job. Never say yes to a project if you don’t have enough time to complete it effectively. To do so will
cause you more harm then good in advancing your career. Learn to say no gracefully to projects that
do not fit with your career goals. If your Chair or others assign you more tasks than you can manage
effectively, speak up and ask which tasks can be delayed in order for you to do the best job possible
with all assignments.
Avoid Procrastination: It is human nature to procrastinate to some extent. We all occasionally defer
activities that seem overwhelming or we dislike. This is the greatest pitfall in time management. When
procrastinating on a project, it is helpful to break it up into small pieces. Working slowly to complete
each small piece will help you get over the "overwhelming" feeling of a particularly difficult project and
past the procrastination hurdle. Some find it useful to build in a series of rewards for those projects that
are particularly problematic (I’ll finish background research for that chapter, then I’ll see that movie I’ve
been wanting to). All of us are overburdened with mail and paper that form obligatory stacks on our
desks. A good way to lose time and one of the most common "time-robbers" is to procrastinate taking
care of these items and constantly reshuffle the stacks. A good rule of thumb is to not pick up a piece of
paper more than twice without taking some sort of action on it. If it has been on your desk for more than
a week without any action, then it probably didn’t really need your attention in the first place. You
should either throw it away or delegate it to others allowing you to spend your time in more productive
pursuits. Reading and answering email can not only be a time sink but can also be an effective way of
procrastinating. As noted above, try to read your email only once a day. Set aside a specific time to do
so. Resist the temptation to log on frequently throughout the day, which will likely result in a loss of
focus for completion of more complicated projects.
Recapture lost moments: Many moments are lost during the day that, if recouped, can add up to a

significant savings of time. All of us spend time commuting to work. Use this time to listen to CME tapes
or plan your day. The careful use of a hand-held dictaphone or cell phone to catch up on
correspondences and calls or create to do lists can be very time saving. Take advantage of time spent
waiting in line by carrying journals, reading mail, or reviewing your personal organizer.
Information management
If you are not computer literate, it is well worth the investment of time to acquire these skills. Using your
computer as an information resource or for database management can save countless hours.
Presentations and handouts can be quickly and expertly created. Databases can be designed or
procured for almost anything, including storing and managing references. These can be indexed and
cross-referenced with key words and a unique number can be assigned to each article. The numbers
can then be used when writing manuscripts, and the computer will automatically place the references in
correct order in the final manuscript. It is also possible to catalogue 35 millimeter slides to allow for
quick cross-referencing to create a variety of "mix and match" lectures. Become skilled in Medline
(Pubmed) and web searches. Develop an effective filing system that will allow you to retrieve
information when needed. Utilizing computer technology to document scholarly activities can also be
very useful. Not only will you quickly be able to sort items for inclusion in teaching, research, and
clinical portfolios, you will capture items otherwise long forgotten when putting your promotions packet
together. You can pre-program reminders to solicit needed promotion documentation after each activity
if it is not forthcoming.
Practice and Reap the Benefits
Effective time management requires careful planning and a great deal of concentrated effort on your
part to make the concepts part of your daily routine. Once you embrace these techniques you will
quickly find the benefits of maintaining control over time, rather than being dragged along by it, far
outweigh the effort expended. Productivity will increase, and there will be more time to do the things
you enjoy. The overall result is a more satisfying and successful career.
References:
1.Applegate WB: Career development in academic medicine. Am J Med 1990;88:263-267.

2.Perina D, Chisholm C: Physician wellness in an academic career. Hobgood C, Zink B (eds):
Academic Career Guide. Society For Academic Emergency Medicine, Lansing Michigan, 1999, pp 53-
55.
3.Sheely G: New Passages: Mapping Your Life Against Time. Random House, New York, NY, 1995.

Faculty Development for Women
Author: Rita Cydulka
Until a few decades ago, the main challenge for women in medicine was achieving access to a faculty
position. Now, women constitute almost one quarter of full time faculty in academic emergency
medicine. This closely reflects Only 5% have achieved tenure in their institutions. Compared to men,
women in emergency medicine are over represented in the lower ranks (instructor and assistant
professor) and under represented in the higher ranks (associate professor and full professor) and in
achievement of tenure. In addition, women lag behind men in leadership positions and administrative
responsibilities. Men in emergency medicine are more likely than women to spend more time performing
administrative tasks, and to hold or to have held, leadership positions. Women, on the other hand,
spend a higher proportion of their time in clinical practice and teaching. In a recent more books than
their female counterparts.
Of note, in the same survey, women were 15 times more likely than men to indicate that their career
advancement was made more difficult as a result of their gender. Although access to faculty positions is
no longer the problem it was a couple of decades ago, creating a successful and satisfying career may
still be. This monograph is intended to help women avoid some of the pitfalls in a career in academic
medicine that those who have preceded them have reported.
Upon entering a career in academic medicine, women must decide what opportunities exist and what
pathway to choose. Choices include a career in academics in the strictest sense, i.e. a grant supported,
publish or perish pathway, a career devoted to clinical medicine, a career that centers around
educational endeavors, or a career in academic administration. It is crucial that women beginning in
academic medicine understand their career path and, more important, what leads to success in that
path. It is also crucial to appreciate fully the mission of their institution and their department. Knowledge
about their institution’s structure, career path rewards, key players, and promotion procedures is crucial
to success. If the institution’s system of reward and promotion within the academic center is not "in
sync" with that of the faculty member, she will be unsuccessful.
Determining Goals
As one embarks on a new career as a woman in academic emergency medicine, consider short term

and long-term goals and ask the following questions:
Where do I want to be in one year, in five years, and in ten years?
What are my skills? Do I have particular strengths that are in demand?
Do I have all the skills I need to achieve my goals? If not, what additional skills do I
need? What extra training should I consider to be qualified to achieve my goals?
On what schedule must I advance? Who will make the determination whether I
advance? Who will evaluate me in addition to my department chair? Do non-clinical
faculty from other departments within the university influence my promotion?
What are my needs? What are my limitations?
Will the position I currently have enable me to advance toward my ultimate goal or will I
need to pursue other opportunities to meet my goals? Can I modify my current job so
that it will help me achieve my goals?
How do I respond to authority? How do I feel about being in authority?
Understanding the Environment
It is vital to understand the rules by which evaluations are determined: the written rules in the university
handbook and- perhaps more important- the unwritten rules. For example, if one chooses education as
the pathway of pursuit, one must ascertain whether teaching and clinical activities are rewarded with
academic promotion in your institution. Women in academic emergency medicine tend to spend more
time in clinical practice and teaching than do men, even though teaching and clinical time rank low
among the criteria for academic promotion in most institutions.
Many women have noted that they begin their careers at a disadvantage because of unequal footing at
the start of the race. Women must insist on the support that is needed for development. This support
includes secretarial, technological, and financial support. Women must clearly understandthe
compensation used in their departments. Is the compensation based on clinical productivity, academic
productivity or both?
Early on, note the department’s and the school’s record on 1) recruitment policies for women, 2) efforts
to recruit senior women to tenure positions, 3) mentoring of women, 4) faculty development of women,

5) salary lines of women compared to men, 6)procedures to monitor trends of appointments,
promotions, and numbers of women faculty at all ranks, 7) strategies for retaining women faculty at all
ranks, 8) family/parental leave policies that allow extended time for promotion and tenure during child
bearing years and, 9) retention records for women. A school that actively and successfully recruits
women but fails to retain them is not likely to be a school that is friendly to the needs of women. If this is
true at your medical center, stay alert!
Issues affecting the advancement of women vary from institution to institution. How these issues are
addressed, however, will affect the environment one faces in academic emergency medicine. Many
academic medical centers are examining the issue of gender equity and trying to address a particular
obstacle that affect female faculty (Carr, 1999). Women should note whether their institution is one that
has had problems with gender bias in the past and, if so, what steps (if any) are being taken to address
these problems.
Several studies have shown that women faculty continue to face disadvantages compared to men in
garnering resources, equitable compensation, and gaining promotion and tenure. Be sure that women
are starting on equal footing with male colleagues. Watch early for feelings of isolation and alienation,
not only because of outward discrimination but because of subtle forms of discrimination, such as not
being included on research projects, not being invited to discussions, and being "benignly" ignored.
Some of the reasons put forth to explain why women in academic medicine do not achieve success at
the same rate as men include a sense of isolation, sexism, cultural stereotypes, and difficulties
combining family responsibilities with professional demands.
Research has shown that as women in academic medicine progress they become more and more
isolated and feel they are subject to more intense scrutiny than men. As a result, women may
experience decreased self-confidence, exclusion from access to informal networking, and lack of
continuity of helpful relationships with colleagues.
The Value of a Mentor
Choosing a mentor or entering into a mentoring relationship is crucial. Mentors can help with knowledge
and skill transfer to the mentee, provide motivation, direction, and confidence building, actively promote
the interest of the mentee among others, and provide access to institutional resources that may

otherwise be unavailable to junior faculty. Finally, a mentor may help the mentee secure appointments
on committees and among select groups. Women should feel free to call on different individuals for help
with different goals and needs and take into account the values and characters of individuals from whom
they seek advice. Mentors can provide advice on career management, help one to understand the
values, norms, and expectations of academic emergency medicine in the institution, and can assist one
in developing and maintaining a productive network of colleagues.
Relationship and communication skills are critical to becoming a successful academician. Women must
try to discover important researchers and collaborate with them on projects that are likely to become
successful. These informal networking relationships will support one’s productivity and introduce women
to other people who are similarly productive. Research has shown that women in mentoring
relationships publish significantly more papers than do women not in mentoring relationships, but also
work significantly more hours per week.
Unfortunately, networks of women faculty have not been as effective as those of their male colleagues.
The former tend to include fewer faculty of high rank and fewer associates from previous institutions.
Perhaps the most important source for developing collegial mentoring relationships among women is
through professional associations such as SAEM or ACEP.
Communication and negotiation skills are essential for women wanting to succeed in academic
emergency medicine for defining and modifying job responsibilities, as well gaining resources, obtaining
a raise, formulating limitations on expectations, and recognizing and dealing with conflicts. To be an
effective negotiator, women must be able to recognize and deal with conflict. Women, as a group, must
overcome the desire to dodge confrontations, accommodate the other person, compromise goals, or
avoid conflict altogether. Learn to say no. As a junior faculty, one’s tendency will be to say "yes" to all
opportunities that come one’s way. Agreeing to too many tasks that won't ultimately achieve one’s
goals, which are done at the expense of tasks that are important to both the individual and to her Chair,
will ultimately prove frustrating and will negatively impact achieving one’s goals. Women must learn to
appear confident, recognize the opportunity for self promotion, and prepare for negotiations by
understanding the negotiating style of their superiors.
The Leadership Role

Women must plan to be leaders. Women in our society have been conditioned from birth to suppress
taking a leadership role. A commanding voice and fighting are considered undesirable traits in girls
while encouraged in boys. Women in medicine have developed the trait of leadership inadvertently: they
have convinced their families, college advisors, medical school administrators, and their residency
directors that they have a right to a position in medicine. Women in academic medicine should plan to
take this role one step further and advocate for a position among their departments’ leadership. They
should ask their Chairs what training he or she can offer in leadership skills. For only when women are
represented as leaders in emergency medicine will they be able to serve as role models for younger
physicians.
Balancing Career and Family Needs
There are no easy answers in addressing the family issue. Each individual (both females and males)
must decide for themselves how much time to commit to their personal relationships and family and how
much time to commit to their academic career. Successfully combining parenting with medicine takes a
lot of planning, a lot of luck, and many supportive relationships in the home and in the work place. Some
schools have acknowledged these problems and have made provisions, such as lengthened periods on
the tenure track, flexible scheduling, and job sharing. Whether choosing to work full or part time, one
must be sure of the following: clear expectations for performance are established; some time is
protected for research and writing, and time spent on committee work and administration is initially
minimized. Women must be ever vigilant that they are pulling their weight. There is no substitute for
hard work!
It has been frequently noted that when men leave work early or fail to attend a meeting because of
childcare responsibilities, they are looked at as exceptional fathers. Unfortunately, the same doesn't
hold true for women. They are labeled as uninterested in academic success or delegated to the
"mommy track". Be aware of how and why these issues are addressed by peers and department
leadership.
Conclusions
In summary, women have come a long way in academic medicine in the past few decades but still have
a long way to go in order to achieve equity with men. Planning for success is the first step in achieving

this goal.
References:
1. Anonymous. U.S. Medical School Faculty 1997: Faculty Roster System. In: Colleges AAMC, ed.
Washington, D.C., 1997.
2. Cydulka RK, D'Onofrio G, Schneider S, et al: Women in academic emergency medicine. Acad Emerg
Med 2000;7:999-1007.
3. Carr PL, Friedman RH, Moskowitz MA, et al: Comparing the status of women and men in academic
medicine. Ann Intern Med 1993;119:908-913.
4. Tesch BJ, Wood HM, Helwig AL, et al: Promotion of women physicians in academic medicine. Glass
ceiling or sticky floor? [see comments]. Jama 1995;273:1022-1025.
5. Carr P FR. Gender diversity-struggle in the glass house. Mayo Clin Proc 1999;74:201-203.
6. Bickel J: Women in academic medicine. J Am Med Womens Assoc 2000;55:10-12,19.
7. Bickel J. Scenarios for success--enhancing women physicians' professional advancement. West J
Med 1995; 162:165-169.
8. Cole JR SB. The Outer Circle: Women in the Scientific Community. In: Zuckerman H CJ, Bruer RT,
ed. A Theory of Limited Differences: Explaining the Productivity Puzzle in Science. New York: W.W.
Norton and Company, 1991.
9. Hall L. Negotiation: Strategies for Mutual Gain. Newbury Park, CA: Sage Publications, 1993.
10. Caplan P. Lifting a Ton of Feathers: A Woman's Guide to Surviving the Academic World. Buffalo,
NY: University of Toronto Press, 1993.

Faculty Development for Minorities
Author: Marcus L. Martin
In this chapter Faculty Development for Minorities is discussed. It is important first to delineate who are
considered minorities in medicine.
Minorities in medicine may be classified in broad terms to fall in the ethnic/racial groups of Asian,
Hispanic, Native American, African American and other.
The Association of American Medical Colleges (AAMC) has classified under represented minorities in
categories of black Americans, Native Americans, mainland Puerto Ricans and Mexican Americans. As
the number of underrepresented minorities (URM’s) in the US population has risen over the years
(currently between 20 – 25%) the number of medical school applicants has only attained an all time high
of around 12% or about 0.5 representation factor, (ie 20% US population only 10 to 12% medical school
applicants.)
In 1954 the US Supreme Court decision Brown vs The Board of Education ended with a mandate to
desegregate public schools. However, many schools did not desegregate until many years later. I
attended first grade in Virginia in 1954 but my school system did not desegregate until my senior year of
high school. Many school systems in Virginia shut down rather than integrate. Lower socioeconomic
status, inadequate schools, labs, and lack of well trained teachers have hurt minorities historically.
Resources and opportunities are generally better now than years gone by. The civil rights act of 1964
has helped to bring about further changes which enhance advancement of all people of color, whether it
is academic medicine or some other arena.
Underrepresented minority medical students in the 1950’s approximated 2% of the total student
population and stayed at that level throughout the 60’s. By the 1970’s the number of underrepresented
minorities in medical school had increased to around 8%. This progress to a large extent was due to the
affirmative action efforts of the AAMC and the Robert Wood Johnson Foundation’s provision of
scholarships for women and minorities. By the 1990’s the underrepresented minorities in medical school
enrollment reached 10%. During the mid to late 1990’s anti-affirmative action activity thwarted to some
degree the AAMC’s "3,000 by 2,000" efforts. The AAMC pursued achieving 3000 URM students enrolled
in the first year classes of medical schools by the year 2000. The maximum URM enrollment had

reached around 12% (about 2000 students) in the first years class by year 1998 but quickly sagged to
10% again in subsequent years.
First year medical students entering each year roughly approximates 8.0% for black Americans, 2.7%
for Mexican Americans, 0.7% for mainland Puerto Ricans, 0.8% for Native Americans and 19.3% for
Asians.
URM’s comprise about 8% of Emergency Medicine residents, while practicing URM’s in emergency
medicine equal about 5% of total emergency physicians. In academic emergency medicine URM’s
account for about 3.5% of the total faculty.
Underrepresented minorities as a population are associated with a disproportionate share of medical
and economic ills, as well as disproportionate utilization of emergency services. It is very important for
underrepresented minorities to become larger in numbers in medicine as well as academic emergency
medicine for many reasons.
1) The advancement of cultural competency. Underrepresented minorities are needed to be a part of
medical institutions and faculties, in particular emergency medicine because of the potential for
improving upon the cultural competency of patient care provided by all races/ethnicity. As we improve
upon our scientific competence, it is also important to obtain cultural competence so that we can
communicate appropriately with patients and improve patient compliance and enhancement of care.
2) Considering the low numbers, minorities in academic medicine may be viewed as an important
addition to the faculties of institutions for various reasons, not the least of which will be financial security
of the institutions required by law to actively hire minorities.
3) A diverse emergency medicine research agenda is essential, and conceptualizing health problems is
dependent upon a diverse research work force.
4) Diverse students and faculty learn and teach about cultures, values and beliefs of their communities.
5) It is important to remedy the effects of past discrimination, protect diversity of human talent, provide
rewarding career opportunities and increase the minority mentor pool.

6) Diversity among health care leaders is economically essential as medicine is a trillion dollar annual
corporate enterprise.
Faculty development needs in emergency medicine are essentially the same for URM’s as for non-
URM’s. However, this chapter covers some additional suggestions beyond the general requirements
that minorities should consider.
GENERAL REQUIREMENTS
To achieve success in academics, faculty must have achieved academic success in college and
medical school. Entry into residency programs is competitive and in past years graduation from
residency was often the primary requirement for participation as a faculty member. A resident
completing a three or four year emergency medicine residency program could apply to most academic
programs and would receive serious attention. Although this is still true to some extent today, it has
been my experience that with the addition of five year combined programs and fellowships that the
competition for these positions has become stiffer. Even in the situation where completion of a three or
four year program as a chief resident potentially makes a candidate more attractive, completion of
fellowships make the candidate far more attractive for academic faculty positions. Therefore, it is
suggested that some advanced preparation such as a fellowship in research, administration or sub-
specialty such as EMS, Toxicology, Sports Medicine, Pediatric Emergency Medicine, Neuroscience or
advanced degrees such as a Ph.D. or MPH should be considered as additional preparation for faculty
development.
INTERVIEW PROCESS FOR AN ACADEMIC FACULTY POSITION
During the interview process for a faculty position a potential new faculty member should get as much
information as possible about the job requirements and should review a written description of the
particular job and academic track in the medical school or hospital where he/she will be working. It
should be clear whether the clinician is entering the clinician-educator track/pathway or a clinician-
investigator track/pathway. There are very important distinctions between academic tracks/pathways. A

clinician-educator track usually involves more clinical work and more teaching and the clinician
investigator track usually involves more time in the lab or performing clinical research. The potential new
faculty member should receive a letter from the department chair and/or medical school dean outlining
the job description and the particular track. The letter should indicate whether the faculty member is
coming in at the instructor level (typical for fellowship positions) or the assistant professor level. You
should understand clearly how many years in rank is ordinarily required to advance from assistant
professor to associate professor and from associate professor to professor, and how long it takes to
become tenured if you are on a tenure track. You should also find out in advance of taking an academic
position what constitutes scholarly activity and excellence in the Medical School with which you will be
affiliated. Generally, research with publications that impact the specialty, constitutes scholarly activity in
the traditional track. Many institutions also consider educational development (ie, course curriculum,
teaching modules) that impact the specialty as examples of scholarly activity in the clinical track.
SCHOLARSHIP
As noted in the Preface, Scholarship was chosen as the primary organizaing principle of this Handbook.
There are four areas of scholarship as defined by Boyer. They are the scholarship of discovery, the
scholarship of integration, the scholarship of application and the scholarship of teaching. The
scholarship of discovery or research for decades has been the area of primary focus for promotion and
tenure in medical schools even though faculty have had major responsibilities in the other areas of
scholarship (Beattie). Find out what types of publications qualify at your institution, (ie will book chapters
and abstracts qualify as well as publications in peer reviewed journals?) Generally, scholarly activity is
that activity which focuses on a specific area of the specialty and which has an impact upon the
specialty, (ie education or curriculum that could be used in medical schools, residency programs or by
clinicians) and/or research that affects how we practice. Institutions may require excellence in one or
more categories such as excellence in education/teaching, clinical excellence or excellence in research.
Find out what is expected and in how many categories and to what degree you must demonstrate
excellence. Make sure during your negotiation with the chair or medical school dean that you get
everything in writing including your salary offer, the description of your position, and the promotion and
tenure information. On top of that you must make sure that supportive items such as computers, office
space, CME support, and lab space, if relevant, are all clearly spelled out in a letter.

PROMOTION AND TENURE
Minority faculty at both the assistant and associate professor rank are lagging in rates of promotion
compared to white faculty, even though their representation in academic medicine has steadily
increased over time. (Fang) Comparing cohorts from the 1980’s, by 1997 46% of white, 37% of Asian
Pacific Islanders, and 30% of URM assistant professors had been promoted. Similarly by 1997, 50% of
white, 44% Asian Pacific Islanders, and 36% URM associate professors had been promoted. (Fang)
Minority faculty are less likely to be tenured or on tenure tracks, less likely to be RO1 or other NIH
award recipients, and more likely to have appointments in private medical schools. (Fang)
In Fang’s study, compared to whites, URM assistant professors were more likely to be graduates of US
medical schools whereas Asian Pacific Islander assistant professors were more likely to have a Ph.D.
degree or be affiliated with basic science departments. URM and Asian Pacific Islander assistant
professors were more likely to be female.
BARRIERS
Thirty years ago it was clear to most people that overt racial/ethnic discrimination was a major factor in
the underrepresentation of minorities in a variety of highly desirable sectors in our society. Now the
causes for such underrepresentation are much more subtle and relate primarily to long standing
economic, social, and educational inequities which result in a low representation of minorities among
those who receive MD’s as well as Ph.D.’s in science. (Nickens)
According to Nickens, there are nine barriers to success for minority scientists. They are:
1) Educational pipeline leaks (a miniscule proportion of minority youth emerge from our national
educational system with the requisite skills to do college level science work)
2) Isolation in university departments

3) Excessive demands for time
4) Absence of mentors
5) Complexity of minority health problems. Young minority scientists have a very high probability of
being interested in a problem with direct relationships to minority population, which tend to be clinically
oriented, highly complex and difficult to research. While on one hand an interest in these complex
problems is important, it may run counter to the mind set of scientists and NIH study sections, which is
to simplify so that you minimize the number of variables for which one must adjust.
6) Deficiencies in Grantsmanship and knowledge of the NIH system (Most of the underlying causes for
underrepresentation of minorities among NIH grantees are the result of factors beyond the control of the
NIH)
7) Demographics of study sections and NIH staff (unacceptably low representation of minorities both on
NIH study section and among NIH scientific staff)
8) With contraction of resources due to increasing competition for grants, the probability of obtaining an
NIH grant becomes less likely.
9) No game plan (there is the need for an organized national strategic plan to address the nation’s
health, to increase minority health targeted research and increase minority investigators.) Likewise,
minority faculty must develop individual game plans to succeed.
SPECIAL CONSIDERATIONS FOR MINORITIES
As a faculty member and particularly as an underrepresented minority you can become overloaded with
committee work. Although any faculty member can become overloaded with committee work, since you
will most likely be only one of a few of your race/ethnicity in medicine and involved in Emergency
Medicine you will be asked by the Dean of the medical school or your Department head to be a member
of such committees as the following: Departmental committees, Hospital committees, Women and
Minority (diversity) committees, Medical School committees and other University committees where a
minority is required to participate based on state and federal mandates, (ie equal opportunity programs
which may require a minority to be available to interview prospective candidates for hire).

It is important to be involved on committees at the local, state and national level. However, an overload
of committee work can distract from scholarly activity. On the other hand involvement in committees
particularly at the national level will give you more recognition in the eyes of your peers and specialty
leaders and may serve you well eventually when it comes time for letters of recommendation from
national figures who know you. Involvement in your specialty organizations is very important and often
provides an opportunity for personal and national advancement.
Community involvement is very important but can be taxing so you will have to gauge and balance your
involvement. However, religious, school, and family activities help to sustain balance in life. Involvement
in charitable activities is also important. Promotions and tenure committees in general will be looking at
your scholarly productivity principally. Some institutions are now considering public service activities if
highlighted as part of your job description and/or promoted by your chair as important and consistent
with institutional mission.
Publications including book chapters, abstracts and other manuscripts are important, but in general P &
T committees will give more weight to original research and the resulting manuscripts/publications.
Lectures given at the local, state and national level and the quality of these lectures, though difficult to
gauge, are important. Grants obtained are very important. Keep records of all sources of money you
receive associated with your scholarly work. Bringing in research dollars always carries weight. Find out
how much weight first authorship versus second or last authorship carries on publications.
It is important to know whether or not clinical activity counts towards promotion. For instance, if you are
scheduled to work 24 clinical hours per week it may be considered (based on a 40 hour week) as 60%
clinical time as the requirements of your job description. The productivity may also be important. For
instance, some institutions record relative value units (RVU’s) or some unit of measurement to
determine how many patients you see and how much income you generate. Find out if this is an
important activity at your institution. Make sure you document your clinical productivity. Non-clinical
activity can also be formulated into relative value units.
Annual or biannual performance evaluations generally takes place at most institutions. Make sure you
get feedback from your chair or dean on how well you are doing during these evaluations. Most
importantly, make sure that there is an annual plan agreed to by yourself and your department chair

regarding your goals and objectives for the academic year. You may have simple goals such as two
publications per year. But in general you should outline what you anticipate your clinical, teaching,
education, and research goals will be annually. Also project what your 5-year goals are for academic
productivity and advancements. There may also be an administrative task associated with a title, (ie
residency program director, vice chair, research director, medical student curriculum coordinator,
prehospital division director, clinical operations director, etc…)
BE SURE TO SEEK A MENTOR
A mentor for an underrepresented minority can be someone of the same race or gender or someone of
any other race or gender. Mentorship in terms of the race/ethnicity of the mentor is not that important.
There are recognizable URM’s who are doing important research, who are chairing departments and
who run residency programs and otherwise are involved in academic emergency medicine. There are
not enough of these individuals currently to provide mentorship for all of the underrepresented minorities
who may need it. Throughout residency and fellowship and the early stages of faculty development you
should seek mentorship. Most importantly, getting involved in a specific focus area often requires a
mentor to get you started. Make sure goals are set early and follow through on those goals. The mentor
may even be someone of another specialty but whose area of interest is similar to your own.
Underrepresented Minority Medical Students who are inspired to become physicians benefit from
wisdom and guidance of seasoned physicians who can mentor them. These physicians can help
students and residents navigate through their education and training. The National Medical Association
(NMA) has established the national minority mentor recruitment network. NMA has partnered with the
National Health Services Core or the US public health service. The network was created with the goal of
providing culturally sensitive role models for African American medical students and increasing the
representation of African American primary care physicians.
Opportunities are also available through programs such as the Health Services Research Institute
(HSRI). In the spring of the year 2000, twenty nine minority faculty members were selected as HSRI
fellows. Begun in 1991 and funded by the agency for health care research and quality (AHRQ), HSRI
has helped over 100 minority faculty members improve their skills in health services research, from the
development of a concept paper to the submission of a grant application to federal funding agencies.

ISOLATION
You must have confidence in your feelings and your thoughts and your capabilities to compete in the
academic world. There may be some "behind the scene" forces that you are unable to see or control.
Within your own working group there may be someone jealous of you and feel that you may not deserve
to advance. Members of your own race/ethnicity may be jealous of you and may not necessarily help
your cause. There will be those individuals who will feel that your position or achievements have
occurred only because you are an underrepresented minority, (ie someone may say, you have obtained
your job only because you are black or because you are hispanic.) You may be placed in an
environment where your social and cultural world differs from others. Networking generally occurs in
social/cultural circles such as, golf course/country club, church, school etc. Members of your
department/institution may attend the same church and their children may attend the same school and
you and your family may not be a part of that circle. Discussions in those circles may take place about
you and the quality of your work. This is not something new in our society. You need not focus on the
networking but you should be aware that circles/networks may play a role in whether you advance or
not.
As a minority you are probably different in the way you look, talk and possibly act compared to other
physicians. I am sure you have accepted that fact and hopefully others will accept that fact as well. It is
important for you to know that when you join a faculty, become a committee member at your academic
institution and work primarily in the emergency department seeing patients you will most likely stand out
because you look different. Traditionally, making mistakes carries a heavier burden and penalty for
minorities. Minorities have historically been depicted as inferior in capabilities. This statement is made
based on experience and observation. You must understand that not only are you watched and followed
by administrators inside and outside of your department but your own peers, and coworkers look very
closely at you. Don’t be surprised when you make a recommendation in a committee or amongst a
group of people that your recommendation may not be clearly heard or accepted. Don’t be surprised
that someone already more established than you may make a comment that is clearly heard and
accepted but in essence is identical to the one that you just made. This can happen to any body but
historically women and minorities have been plagued with this type of minimization or marginalization.
Your peers can be helpful to you but beware that your peers may also pose a barrier to you and set
roadblocks. You often have to prove yourself many times over.

FACULTY DEVELOPMENT COURSES
Attend faculty development seminars early. Such seminars exist in academic emergency medicine,
such as Navigating The Academic Waters Conference that is held annually, cosponsored by AACEM
and CORD. The Association of American Medical Colleges has a Faculty Development course for
minorities (Minority Faculty Career Development Seminar). This course stresses the teachings and
understandings of the NIH Application and Research process, information technology in medical
education, conflict management, financial basics, academic writing and special challenges for minority
faculty. It is very important to understand the NIH application process since it is used as a "Gold"
standard throughout medicine. Make sure you collaborate with others within and outside your institution
and that you attend regional and national meetings.
TIME MANAGEMENT
Time management and balance of activities is extremely important for all new faculty as well as
seasoned faculty. Time management and balance of activities is not a new concept. It is even more
important in Emergency Medicine since we work our shifts around the clock, holidays and weekends. If
you have a family, you have a lot of decisions to make regarding your involvement in academic
emergency medicine. Honestly you may end up sacrificing a lot of your own personal needs, but you
should certainly look out for your health and your family’s well being. Your general goals should be
clinical/academic productivity leading to promotion, a rewarding career and a stable and happy family
life. Social and religious fulfillment is certainly very important. Avoid taking on responsibilities in areas
where you have no interest. Again, I will emphasize suggestions that you may make may be over looked
or rephrased by someone else. You may get overlooked for certain jobs. Someone else could get the
job just because of the network. Speaking up is what you should do in most cases. It’s the way you do it.
Don’t carry a chip or grudge. Acceptance will eventually come if you maintain a steady pace and you are
fair to all. Find your niche, focus on a specific area and become authoritative (not authoritarian). Be
timely and don’t be afraid to take risks or chances.. You may be in the "series of firsts": First to integrate
a certain school or church, first to integrate a residency, first to integrate a sports team or first to become
a faculty member as a representative of your race or ethnicity. You may be running interference or there
may be someone running interference for you. As you seek opportunities you may find that there are no
other, or few other, URM residents or faculty members at the institution to which you are applying.

Always keep your tools sharp. Be accountable. Be focused.
Remember that everyone you work with is a member of the human race and has frailties. Look for
signals from the chair or division head that he or she will stick with you if you are recruited to the faculty.
There is added pressure on female minority faculty members. In some cases these faculty may need
time off the tenure or promotional clock. A typical clock continues to tick (ie the requirement to advance
from assistant professor to associate within six years and another four years to become tenured.) In
some cases, institutions have expanded the time frame and will either stop the clock for or extend it for
pregnancy, childbirth and other family related leave matters.
Seek letters of support from coworkers and faculty members particularly when it comes to promotion
time. Develop national ties. Seek national recognition and participate in special forums such as the
National Medical Association meetings.
FINAL THOUGHTS
Our society must ensure that leadership in academic emergency medicine is as diverse as the
population that our medical centers serve. Underrepresented minorities must become more prominent in
numbers and position. We must examine the climate for inequities for underrepresented minorities
especially in areas of leadership, education, research, and community service. Student bodies at
universities may closely reflect a rich diversity of the American population but, our faculties in leadership
in health systems and other organizations do not reflect such diversity. There have not been adequate
mentors nor role models to encourage minority students and residents to become teachers,
researchers, and leaders. Underrepresented minorities have been undervalued. Socialized, traditional
ways of thinking and acting, perpetuated out of habit and lack of awareness have been imbedded in US
culture. It is important that changes occur and our medical culture increase representation and visibility
of underrepresented minorities in positions of authority and leadership. More mentoring programs will
need to be instituted and earlier in the educational years (ie. as early as middle school). Minorities
should utilize the professional development leadership programs that are currently in existance and our
society should create more opportunities. It is inevitable that more minorities will enter a career in
academic emergency medicine, but unwavering support and commitment from current academic
programs, other physicians, and society is essential for those careers to flourish.

REFERENCE LIST
1. Boyer EL. Scholarship Reconsidered: Priorities of the Professoriate. Princeton, NJ: The Carnegie
Foundation for the Advancement of Teaching, 1990.
2. Glassick CE, Huber MT, Maeroff GI. Scholarship Assessed: Evaluation of the Professoriate. San
Francisco, CA: Jossey-Bass 1997
3. Fang D, Moye, Colburn L, Hurley J. Racial and Ethnic Disparities in Faculty Promotion in Academic
Medicine. JAMA 2000; 284: 1085-1092.
4. Palepu A, Carr PL, Friedman RH, et al. Minority Faculty and Academic Rank in Medicine. JAMA
1998; 280: 767-771.
5. Johnson JC, Jayadevappa R, Taylor L, et al. Extending the Pipeline for Minority Physicians: A
Comprehensive Program for Minority Faculty Development. Academic Medicine 1998; 73: 237-244.
6. Nickens HW, (Vice President for Minority Health Education and Prevention. Association of American
Medical Colleges) Remarks Before NIH Clinical Research Study Group Committee. June 10, 1994,
Chicago O’Hare Airport.
7. Beattie DS. Expanding The View of Scholarship: Introduction. Academic Medicine 2000; 75: 871-876.
8. Glassick CE. Boyer’s Expanded Definitions of Scholarship, The Standards for Assessing Scholarship,
and the Elusiveness of the Scholarship of Teaching. Academic Medicine 2000; 75: 877-880.
9. Dauphinee D, Martin JB. Breaking Down the Walls: Thoughts on the Scholarship of Integration.
Academic Medicine 2000; 75: 887-894.
10. Fincher RME, Simpson DE, Menin SP, et al. Scholarship in Teaching: An Imperative for the 21st
Century. Academic Medicine 2000; 75: 887-894.

11. Shapiro ED, Coleman DL. The Scholarship of Application. Academic Medicine 2000; 75: 895-898.
12. Barchi RL, Lowery BJ. Scholarship in the Medical Faculty From the University Perspective:
Retaining Academic Values. Academic Medicine 2000; 75: 899-905.
13. Levinson W, Rubenstein AR. Integrating Clinical-Educators into Academic Medical Centers:
Challenges and Potential Solutions. Academic Medicine 2000; 75: 906-912.

Experiments Utilizing an Expanded Definition of Scholarship in Promotional Process
Mayo Clinic
The Clinician-Educator Award: A Tool to Foster Creativity in Education
Authors: Wyatt W. Decker & Thomas R. Viggiano
The past 20 years have seen major changes in health care delivery in the United States. The impact of
these changes on academic medical centers has been significant(1). An increasingly competitive health
care market has tightened budgets at academic medical centers, causing many to re-evaluate their
business strategies and refocus their efforts on clinical practice(2). During this same period, the balanced
budget act of 1997 curtailed the amount of funding available for graduate medical education (3). This has
made time and funding for education increasingly limited in academic centers in general(4)and in
academic emergency departments in particular (5,6).
Coupled with this trend of decreasing resources for medical education has been the growing recognition
among academics that being expert in practice, education and research is becoming increasingly
unrealistic(7). Within the specialty of emergency medicine, the challenges faced by an individual in
academic practice have been enumerated (8), and the literature is replete with accounts of scaling back
or leaving the academic career tract(9).
The importance of education in academic centers and within the specialty of emergency medicine has
been well documented(10,11). Therein lies the challenge: To preserve education and nurture creativity in
education in an era of fiscal constraint and minimal time available for this enterprise. In response to this
challenge, in 1998 the Education Committee at Mayo Clinic Rochester developed the Clinician-Educator
Award (12). This program provides time and resources for educational projects judged to be meritorious
by an impartial multidisciplinary panel of experienced educators(12). The Clinician-Educator Award is
funded in part by gifts from benefactors, with the remainder coming from institutional resources.
The goals of the program are to provide developmental support for scholarly innovations, and help foster
careers in biomedical education. The program design is as follows:
1) Interested faculty submit applications following a structured outline (five page maximum).
2) Each application requires two letters of endorsement; one from the department chair and a second
from the head of the teaching program concerned (e.g. Residency Program Director).
3) All applications are reviewed at the institutional level by an independent panel of peer reviewers.
4) Each application is scored, and awards are granted on a competitive basis. Criteria on which a
proposal is judged include:
? scholarly merit
Creativity and Innovation
? potential to add value to the educational
program in which it will be conducted
5) Projects that receive the award are given up to 10% faculty time and $10,000 for a one-year period.
6) All applications receive feedback from the selection panel with suggestions for enhancing the proposal.
7) Six-month progress reports and year-end reports are required of awardees.
Initial Experience
Two funding cycles have now been completed, 1999 and 2000. For these two years, 46 applications were
received and 17 were funded. The table lists examples of funded projects. The impact of this
developmental award program has been overwhelmingly positive. Faculty have expressed appreciation
for the program’s peer reviewed mentoring process for scholarly educational initiatives. Faculty are also
more motivated to develop proposals, and projects which do not qualify for award funding often go on to
be implemented through alternative funding mechanisms. It is too early to assess the impact of the
Clinician-Educator Award program on individual career advancement, although this program has become
a meaningful and effective addition to Mayo’s education and faculty development programs.
References
1. Iglehart JK: Support for academic medical centers—revisiting the 1997 Balanced Budget Act. N Engl J
Med 1999;341:299-304.
2. Alpert JS, Flanagan DM, Botsford NA: The future of academic medical centers in the United States:
Passing through the valley of the shadow of death. Arch Intern Med 2001;161:1047-1049.
3. Congressional Budget Office. Budgeting implications of the Balanced Budget Act of 1997. Washington,
DD: CBO, December 1997.
4. Kuttner R: Managed care and medical education. N Engl J Med 1999;341:1092-1096.
5. Moorhead J: The future of academic emergency medicine. Acad Emerg Med 1999;6:255-258.
6. Stead L, Schafermeyer RW, Counselman FL, et al: Effect of changes in graduate medical education
funding on emergency medicine residency programs. Acad Emerg Med 2001;8:642-647.
7. Anon: Lancet: Researcher, clinician, or teacher? 2001;357(9268):1543.
8. Syverud S: Academic juggling. Acad Emerg Med 1999;6:254-255.
9. Clark R: A midlife crisis in academic emergency medicine. Ann Emer Med 1999;34:562-564.
10. Biros H: What really matters? Educating academicians. Acad Emerg Med 1999;6:253-254.
11. Martin ML: A perspective of the process of educating academicians. Acad Emerg Med 1999;6:258-
259.
12. Viggiano TR, Shub C, Giere RW: The Mayo Clinic’s Clinician – Educator Award: A program to
encourage educational innovation and scholarship. Acad Med 2000;75:940-943.
TABLE – Selected Examples of Funded CE-10 Projects at Mayo Clinic Rochester
· Training New Physicians to Prevent Complications of Hospitalization in the Elderly.
· Introduction of Hand-Carried Echocardiography as an Extension of the Cardiac Physical Exam .

· Basic Airway Management for the Third-Year Medical Student.
· A Curriculum to Teach Ethical, Legal, and Practical Aspects of Withdrawing Life-Saving Treatments in
the Intensive Care Unit.
· Trauma Education for Mayo Medical Students.
· Development of a Course in Clinical Decision-Making.
· Development and Evaluation of a Musculoskeletal Injection Technique Curriculum.
· Development of a Web-Based Application to Facilitate Clinical Investigation.
Experiments Utilizing an Expanded Definition of Scholarship in the Promotional Process: The Medical College of Wisconsin Experience
Authors: Robert R. Leschke, Deborah E. Simpson, and Stephen Hargarten
Successful junior faculty members typically receive a great deal of advice regarding critical focus areas
during their first few years after graduation from residency. Most of the advice comes from experienced
senior colleagues who help the junior faculty member interpret the written (and unwritten) rules, values,
and expectations of an academic physician. This guidance is particularly critical in the area of faculty
promotion.
In today’s academic medical center market place, the primary foci for new junior faculty center around
efforts to boost clinical acumen, prepare for necessary board examinations, and establish new
relationships. Promotion is a topic for "the future", a foreign concept that is not of immediate importance
for most junior faculty who have emerged from a structured residency environment in which the process
by which one progresses from PGY1 to PGY3 is clear with explicit expectations. In contrast, faculty
promotion requires a sustained effort to accumulate evidence of one’s scholarly activity (e.g. papers,
grants, teaching evaluations), personal references, and institutional citizenship. Unfortunately,
promotion remains a foreign concept for some junior faculty who may have sufficient time in rank for
promotion but often find themselves empty handed scrambling for data to support their advancement.

Such is the case with the junior faculty member in the opening scenario.
The purpose of this article is to help junior faculty members avoid such a scenario using a step-by-step
approach to promotion. (See Figure 1). It will discuss the broadened concepts of scholarship1 that have
emerged in academic medicine with a focus on implications for clinician educators. Building on this
focus, it will outline how to make what you do as a faculty member "count" for promotion, and what and
how to gather and present the data necessary to get promoted. Finally, it will provide two examples of
how the process works at the Medical College of Wisconsin (MCW). One demonstrates how a lack of
guidance and documentation fails to result in promotion and the other shows how utilization of the
process ends with successful promotion.
Broadening the Concept of Scholarship
The 1980’s sought a change in academic culture to recognize the disparity between an institution’s
increasing demands for clinical teaching and its inability to sway from traditional promotional tracks.
Rarely were faculty promoted for their excellence outside of the research arena and as one institution
discovered, winners of a "Teacher of the Year" award were more likely to leave a department sooner
than nonwinners. In 1984, the Medical College of Wisconsin (MCW) approved a clinician educator
promotion track with assessment measures that primarily focused on teaching and clinical service.
Despite the establishment of this track, there was still a struggle to alter the perception that education
detracted from the "real" path to academic promotion and recognition through research. Key MCW
educators and administrators implemented a change strategy to influence beliefs about the form of
scholarship that was consistent with the role of clinicians and educators. This change strategy centered
on an expanded view of scholarship which necessitated a fundamental change in the academic culture
of MCW. MCW’s approach to building this new culture began by recognizing that without a change, the
institution would be unable to attract or retain outstanding clinical educators who are often at the
forefront of training the next generation of clinicians.
The next step was to create a tangible product, the outcome of which was a document called The
Educator’s PortfolioÓ . This system provided an evidence based approach toward documentation of an
educator’s accomplishments in a way that concretely established value. The Educator’s Portfolio
approach was then widely communicated and targeted at chairs and members of the Rank and Tenure
Committee with examples to highlight the "gold standard". Guidebooks were created for clinical

educators to model their data collection using portfolios of successfully promoted faculty.
The culture change, while slow, began to send the message that educators could be promoted when
evidence of quality was documented. Over time, faculty development initiatives and educational forums
were started in response to increasing demands for formal training in education. Not only did clinical
educators want to be recognized and rewarded, they wanted to become better educators. Today at
MCW there are formal promotion standards for clinician educators, a mission to recognize and promote
our best educators, and equal standing with traditional tracks for tenure. This strategy of change at
MCW has gone far beyond the experimental stage. It is now a part of an established culture for over a
decade.
Step 1: Does Education Count?
One of the first steps toward building a successful promotion portfolio is to understand what counts. All
institutions have promotion criteria and these criteria should be easily accessible to all faculty. However,
the degree to which institutions’ value and hence recognize the diverse roles for promotion of today’s
academic faculty vary. Recognizing what an institution will deem important allows a faculty member to
focus energies, talents, and time on promotable tasks that are consistent with scholarly interests.
Fundamentally, promotion is the result of selecting an academic focus consistent with one’s professional
values/ interests, and creating a list of promotion criteria to match those professional interests with what
is institutionally valued. Unless an academic focus is clarified, it will be difficult to say "no" to those
activities that are inconsistent with the focus and that are time consuming without promise of improving
chances at promotion.
Most junior faculty already understand that publication in peer-reviewed journals is a fast track to
promotion. But not all academicians’ roles and associated products lend themselves to "publications" in
the traditional sense. Tracing the roots of the word "publish" reveals that it emerges from the Latin word
meaning public - to make what one does visible. Publications are merely one way in which
academicians can make what they do public.
Many institutions now recognize that some of their best educators are not researchers and the "publish
or perish" philosophy causes many quality teachers to search for jobs elsewhere. In response to this,
many institutions have developed a clinical educator track that recognizes the critical role of teaching

and clinical service. Underlying all of the discussions of scholarship is the key assumption that what
faculty do is to advance knowledge in one’s field as judged by one’s peers. By approaching with
common criteria the evaluation of faculty, be they researchers, leaders in the community-academic
partnerships, or teachers, using the four-part definition of scholarship noted in the Preface to this
Handbook (discovery, application, integration, and teaching), allows the diversity of faculty roles to be
recognized and rewarded through academic promotion. What varies for each role is the type of
evidence used to judge the quality of the scholarly work that is made "public".
Traditional forms of evidence used to document scholarship for research (e.g., publications, grants, NIH
study groups ) provide evidence that one’s work is public, has been reviewed by peers, and is available
so that others may build on the work to advance what is known in the field.2 For educators, equivalent
evidence of scholarship can be presented that addresses curriculum development, teaching, and
advising. Assessment instruments that document this include student and resident evaluations, CME
ratings, data regarding student outcomes, curriculum evaluations, residency match success, or other
indicators that demonstrate the educator’s highest quality efforts.3 Research and publication in these
instances compliment, but may not be necessary for advancement if the non-traditional evidence
presents a strong and continuous record of advancing the field of education, and thereby the
scholarship of teaching.
Step 2: Deciphering the Criteria for Academic Promotion and Chair Support
Recommendation for promotion is typically determined by a faculty committee composed of appointed
and elected peers at the senior faculty ranks (associate to full professor) who advise the Dean. To allow
for flexibility, institutional criteria for promotion are often nonspecific. Understanding what counts
becomes more challenging under such circumstances. The easiest course is to contact other physicians
at one’s institution who spend a similar amount of academic time educating. Determining how they were
successful in promotion provides a model for success. This mentorship with other educators on the local
level can be an invaluable resource.
The next step is to examine the criteria for promotion from several comparable institutions that have a
well defined clinical educator track. A recent national project of the AAMC’s Group on Educational
Affairs is available to stimulate discussion about "what counts". Using several case studies of educators,
a national and regional audience of educators was asked to evaluate whether the individuals would be
promoted. The results of this project are available in an article entitled "Making a case for the teaching

scholar"4 with the actual "case studies" available on the AAMC’s Central Group on Educational Affairs
website, http://www.medlib.iupui.edu/cgea/geasclrpro.html.
By finding out what is acceptable for promotion nationally and incorporating those fundamentals into
your documentation and promotion plans one can begin to build a record of clinical educational
scholarship. Once one has a clear idea of what counts, it becomes imperative to discuss those
academic responsibilities with the chairman to evaluate the level of support s/he will have for these
national and local perspectives. If adequate scholarly evidence is present, it will be crucial to know if the
chairman will be a strong advocate for your promotion.
Gathering the Evidence
Promotion requires the clinician educator to make "public" what his or her activities are in order that
peers on the promotion committee can judge the quality of the work. What should be provided to the
promotion and tenure committee that demonstrates evidence of a successful clinical educator? Some
data are easier to collect or recover than others.
Published articles in peer-reviewed journals are easily producible at promotion time.
CME lectures are required to have evaluations in order to meet accreditation guidelines.
The institution’s CME office should have lecture evaluations and can provide data
comparing one’s ratings to similar CME lectures.
Involvement in hospital committees can be tracked through that committee’s meeting
minutes.
These data are easy to collect in retrospect.
Often, however, faculty fail to track what, over time, can become evidence of a continuous record of
excellence as a teaching scholar. What about all of those student advisees, those lectures given to a
group of residents, the time spent during clinical time explaining the salient points of some disease
process to the team of white coats following behind? The general consensus suggests a good job and
that appreciation is in order but there must be data to prove it. Trying to scramble to reconstruct events

and the evidence in hindsight is incredibly difficult.
Faculty time is important and if it is spent on an activity that could enhance the portfolio, it needs to be
accounted for and evaluated both on its own merit and in comparison to other similar activities. One
must discover what evaluation tools are currently in place at one’s institution. Clerkship evaluations that
ask students or residents to comment on the effectiveness of a faculty member’s participation in their
education provide one with the accountability of one’s time as well as an evaluation of comparative
teaching excellence. Some institutions or individual departments utilize an internet based service such
as E-value which provides an easy way for students, residents, or other faculty to conveniently evaluate
one’s performance in any capacity (e.g. teacher, advisor). This system or others like it amass the data,
which can then be analyzed for both individuals and groups to provide comparison data of excellence as
a teacher relative to others. If a faculty member acts as an advisor for a medical student, the medical
school may have a tool that allows students to comment on how beneficial the advice was. Invited
lectures provide an opportunity to document teaching excellence with a standard evaluation tool.
If there are no departmentally based evaluation tools currently in place one can be created with the
education leadership of another department or the affiliated medical school. Remember, the important
pieces to include in the tool are the accountability (what type of activity and to whom the activity is
directed) and the actual evaluation, both on its own merit and in comparison to similar activities. For
example:
Student advisees can be asked to write a letter detailing their experiences. Since most
students will not have more than one advisor, comparison data can be ascertained by
asking how strongly the student is likely to recommend the advisor to another student.
Lecture evaluations are easy to create by listing a few questions and having the
audience answer those questions based on a 1 through 5 (Likert) scale. Be sure to
identify clearly what the numbers on the scale represent. One of the last questions
should be "relative to other presenters you have heard in this venue, please rate my
performance."
The evaluation tool now has accountability (what type of lecture and to whom) as well as peer
evaluation in comparison to others.

Creating Your Promotion Document
After discovering what counts and how to collect the data necessary to document a clinical educator’s
worth, the final step is to assemble it into a finished product that is presentable to the committee. This
Educator’s Portfolio5 or teaching dossier6 should compliment a curriculum vitae written in an
institutionally specific format. Most young physicians begin this assembly process by saving everything
from invitations for lectures to attendance records at national conferences because they are not
completely sure what is ultimately important. All of these data usually wind up in a folder or large binder.
While this is a good start, since having too much information initially is better than not enough, it is very
difficult to ascertain promotion progress at any given time. One may also be lulled into a false sense of
security with a thick binder of paper before coming to the realization that quantity does not substitute for
evidence of advancing the field of education through high quality forms of scholarship.
Using the Educator’s Portfolio or a teaching dossier provides established categories. For example, the
MCW’s Educator’s Portfolio categories include: curriculum development, teaching, advising, learner
assessment, and educational administration.7 The goal of assembling data in a categorized fashion is to
assure timely quantification that is easily retrievable and understood. A category such as teaching can
be subdivided into: invited lectures, clinical teaching, or core curriculum instruction. Another choice
would be to divide a category into its audience (e.g., medical student, resident, CME, allied health, or
community.) Each time a lecture is given, the evaluation of that lecture can be easily placed in that
section of the binder.
Alternatively, some data can be organized in chronological fashion. Evaluations of clinical teaching
ability kept chronologically can then be easily trended. Other categories such as advising or committee
participation when kept chronologically can easily demonstrate increasing participation or increasing
responsibility. Compiling data in chronological fashion is important in its impact on unfavorable
evaluations. A noticeable upward trend from evaluations at the beginning of one’s career can
demonstrate progress and improvement.
As one’s career progresses, it will naturally become focused on a few targeted areas rather than in all
forms of education. The portfolio should highlight these key areas with evidence of one’s best work. It
may not be important to spend the time creating an evaluation tool for one medical student advisee to

assess quality in this area since that is not the strongest aspect of the portfolio and not likely to be the
evidence that supports promotion. In contrast, if the majority of time is spent teaching clinically and that
is the one’s scholarly focus, it is imperative to have evaluations of that activity and assemble them in a
manner that demonstrates time spent, progress, and excellence. Ongoing collaboration with an
experienced colleague to structure your portfolio can be invaluable.8
Even with real time construction of the Educator’s Portfolio and ongoing collaboration, the final product
is something that should take a considerable amount of time and effort, akin to that required for writing
an original journal article. Following are two examples of the same person’s Educator Portfolio. The first
lists work that is of significant merit. However, without guidance or a specific plan, he embarked on a
hastily prepared document that he would call his promotion portfolio. He organized it in a way that
delineated what he had done at his institution for residents, students, and other personnel. All who know
him would surely advocate for his promotion as a contributing and beneficial faculty member.
Unfortunately, what his portfolio lacks is the necessary data that demonstrates that contribution. The
Rank and Tenure Committee will therefore not be able to support his promotion. Just as a researcher
seeking promotion utilizes peer reviewed manuscripts to demonstrate quality and contribution, so must
an educator produce similar data.
The second example is the same faculty member’s portfolio after consulting with his chair and utilizing a
document like the Educator’s Portfolio for a template. It took a while to find or synthesize the data but
the end result shows strong evidence of progress and contribution. As you review these brief portfolios,
attend to:
How his accomplishments are categorized into the different arenas in which faculty may
be active as educators rather than into the type of audience toward which those
accomplishments are directed.
How actual comments are used to demonstrate the effectiveness his accomplishments
have had.
How objective data is used to demonstrate the educator’s effectiveness on its own merit
and in comparison to his colleagues.
How trended data is used to demonstrate improvement with time.
How the use of a simple pretest and post test can show the effectiveness of the

curriculum project that this faculty member wrote for the housestaff.
How asking advisees to write letters outlining the benefit of advice and listing the
ultimate success of advisees can add to the demonstration of excellence.
BENJAMIN ELLIOTT, MD
Resident Involvement
Resident Teaching
a. Full time faculty at St. Matthew’s Hospital, 1997 - 2001
b. Teacher of the Year, 2000
c. Gave two lectures per year on various topics to ED grand rounds
Advisor for one resident every year 1998 - 2001
HIV for ED Housestaff - A manual for ED housestaff describing HIV care, including basic immunology,
post exposure prophylaxis, medication regimens, and the care of opportunistic infections.
Student Involvement
Student Teaching
a. Full time faculty at St. Matthew’s Hospital, 1997 - 2001
Advisor for the following students:
a. Max Jones, 1998
b. Lisa Smith, 2000

c. Jason Evers, 2001
Clinical Procedures Rotation – This is a required course for junior medical students to introduce them to
simulated critical care settings and procedures and to train them in modified ACLS. I authored the
curriculum and implemented it.
Other Involvement
Trauma Nurse Specialist course 1999 - 2001
EDUCATOR’S PORTFOLIO
BENJAMIN ELLIOTT, MD
Section I: Curriculum Development
2000 - present Clinical Procedures Rotation
Co author Curriculum and EM director
This is a required course for junior medical students, which provides them with an
overview of critical care type settings and procedures including modified ACLS.
Evidence of quality:
College wide Curriculum and Evaluation Committee required evaluation
4.7 on a scale of 1 - 5 with 5 being outstanding
All other rotations 4.5.
Representative comments from students
"great addition to the curriculum. Exposed students to emergency situations"
"wish I would have had this information earlier in my third year"
"excellent integration of materials into a concise and useful class. I feel prepared"

1999 - present HIV for ED
A manual for ED housestaff describing HIV care including basic immunology, post
exposure prophylaxis, medication regimens, and the care of opportunistic infections.
Evidence of quality:
Housestaff averaged 86% on a pretest prior to receiving the packet and 94% after
receiving the packet.
Representative comments from housestaff
"I feel more comfortable with this type of patient scenario now "
"Clarified how I would recommend post exposure prophylaxis to my patients"
Section II: Teaching
1. Resident Teaching
a. Full time faculty at St. Matthew’s Hospital, 1997 - 2001
b. Teacher of the Year, 2000, voted by the residents
E-Value scores:
2000 - Score 4.4/5 Mean for group 4.3/5 Rank 5/14
2001 - Score 4.7/5 Mean for group 4.0/5 Rank 2/14

"One of the clinically smartest faculty we have. Very easy to work with"
"Staff member that takes the most time to teach, case by case throughout a shift"
"Points out a couple of good teaching points on most patients while allowing autonomy"
2. Student Teaching
a. Full time faculty at St. Matthew’s Hospital, 1997 - 2001
Rotating student’s faculty evaluation form results:
1998 - 7.5/10 for teaching effectiveness average other faculty = 7.0
1999 - 8.0/10 for teaching effectiveness average other faculty = 6.9
2000 - 8.7/10 for teaching effectiveness average other faculty = 7.2
3. Other Teaching
a. Trauma Nurse Specialist course 2000 - 2001
i. Gave lecture twice per year on blunt abdominal trauma
Student’s evaluation of the lecture
2000 - 4.7 / 5 total lecturers = 4.5 / 5
2001 - 4.7 / 5 total lecturers = 4.6 / 5
Section III: Advising
1. Advisor for one resident every year 1998 - 2001

100% of advisees passed board exam on first attempt
Each advisee secured job of choice after graduation
2. Advisor for the following students:
A. Max Jones, 1998
B. Lisa Smith, 2000
C. Jason Evers, 2001
All of the above students matched with their first or second choice
Please see attached letters from Ms. Smith and Mr Evers.
It is possible to be promoted successfully as a clinician educator. The Medical College of Wisconsin has
been a leader in proving this statement, and since its early work in this area, has been successful in
establishing a culture that fosters the advancement of clinician educators. Part of creating this culture
was to show that collecting data demonstrating quality in education is just as effective, just as worthy,
and just as imperative in the process of promotion as NIH study sections and peer reviewed
publications. We have outlined here how to decipher the criteria for promotion, how to gather the
evidence necessary for promotion, and have suggested a template for presentation of the data in a
concise format called the Educator’s Portfolio. Early education of these principles and continued
mentorship on this subject will make the process easier and the acceptance of educators as scholars
universal.
Figure 1: Step by Step to Clinician Educator Promotion
1. Identify yourself as a clinician educator
2. What Counts for Promotion
a. Local perspective

b. National Perspective
3. Meet with Your Department Chair Annually
a. Discuss the criteria for promotion with your Department Chair
b. Agree on focus and resources available
4. Gather the Evidence
a. Categorize major types of educational activities
b. Collect evidence for major areas of focus
i. Comparative
ii. Longitudinal
iii. Excellence
5. Creating Your Promotion Document
a. Ask for help - peer review
References
Boyer EL. Scholarship Reconsidered Priorities of the Professoriate 1990; Carnegie Foundation for the
Advancement of Teaching
Shulman L, Glassick CE, Huber MT, et al: Scholarship Assessed 1997; Jossey-Bass: San Francisco.
Fincher RE, Simpson DE, Mennin SP, et al : Scholarship in Teaching: An Imperative for the 21st
Century Acad Med 2000:75:887-894
Simpson D, Fincher R: Making a Case for the Teaching Scholar Acad Med 1999;74(12):1296-1299
Simpson D, Marcdante K, et al: Valuing Educational Scholarship at MCW Acad Med 2000;75(930-934)

Simpson De, Beecher AC, Lindemann JC; Medical College of Wisconsin. Available from the Society of
Teachers of Family Medicine Bookstore. http://www.stfm.org/bookstore/
Faculty Development Committee - Association of Surgical Educators, Teaching Dossier. Available from
Association for Surgical Educators. http://www.surgicaleducation.com/educlear/index.htm#table4
Simpson D., Morzinski J, Beecher A, et al: Meeting the challenge to document teaching
accomplishments: the educator’s portfolio. Teach. Learn. Med. 1994;6:203-206.
Seldin P. The Teaching Portfolio: A Practical Guide to Improved Performance and Promotion/Tenure
Decisions (2nd edition) Boston, MA: Anker Publishing Co: 1997

A Fellowship in Faculty Development
Author: Glenn C. Hamilton
1. Administrative Module (Year-long)
Purpose:
These discussions and assignments run over the entire 12 months of fellowship. They address the
administrative aspects of faculty with a specific orientation toward emergency medicine.
Faculty Responsible:
Chair with assistance from selected faculty and outside discussants.
Primary Reading:
Drucker PF, The Effective Executive, New York, Harper Business. 1967.
Cialdini RB, Influence, 2nd Edition, Boston, Scotts. Foreman/Little Brown, 1988.
Cohen, You can Negotiate Anything
On Leadership
Multiple Handouts
Format:
1-2 weekly discussions.
2-3 specific managerial task assignments.
Topics covered:
AAMC
Academic marketing
Addressing poor performance
Approaches to brain storming/Delphi technique
Attaining departmental status in emergency medicine

Attaining regional/national recognition
Basic financial skills, including budgetary planning
Committee structure
Communication skills: telephone vs memo vs in person
Conflict management/resolution
Counseling skills
Counseling techniques
CV vs resume
Defining personal goals and objective short and long term
Elements of being a manager
Entrepreneurship
Ethical issues in academic medicine
Funding sources for grants
NIH Structure and funding system, review or individual grants and categories
Hiring procedures/firing procedures
Identifying constituencies/scope document
Individual Societies including ACEP, SAEM, AAEM, ABEM, EMRA, CORD and others
Interpersonal skills/networking
Interviewing skills
Introduction to diversity
Leadership skills
Legal Issues in academic practice
Mentorship
Mentorship for the "problem" resident
Negotiating skills
Organizational behavior
Power and Influence
Product/Innovative development
Project management
Promotion and Tenure
Relationship with medical students as a faculty
Relationship with other faculty as a faculty
Relationship with residents as a faculty

Relationship with your immediate supervisor
Social psychology
Structural assessment medical school, LCME
Structure of academic emergency medicine
Structure of organized academic emergency medicine
Structure of the hospital, AMA/state/local medical societies
Structure of the medical school
Tactical planning vs strategic planning
Techniques/Approaches to evaluation
Technology management
Time management
Who do you trust?
Women in medicine
Working with staff
2. Writing/Publishing Module (2 months)
Purpose:
The Academic faculty must write and write well. This two month block focuses on medical writing, the
English language, the elements of a paper, editing skills, and specific computer programs helpful to
authors.
Faculty Responsible:
JS and contributions from selected faculty within Department and at WSUSOM.
Primary Reading:
Huth EJ, Writing and Publishing in Medicine, Baltimore, Williams and Wilkins, 1999.
King, Why Not Say it Clearly?
Strunk W, White EB, The Elements of Style, New York, MacMillan.
Format:

Writing in all formats: papers, chapters, letters.
Understanding and practice in use of dictation to guide writing.
Active editing of individual and Departmental projects.
Many activities will be linked to other modules.
Planned submission of 2-3 scholarly works for publication.
Opportunity to develop and submit potential chapters or book proposal.
Writing skills workshops.
Topics covered:
Essentially the index of Huth’s book .
Effective writing structure.
Developing the irresistible book proposal.
Approaches to editing.
Reviewing others scholarly work.
Writing to communicate in English.
3. Teaching/Bedside Teaching Module (2 months)
Purpose:
These two months introduce the structure of curriculum design, adult education, and bedside teaching
through a variety of readings, discussions and assignments.
Faculty Responsible:
TJ (3 Time Teaching Award Winner, WSUSOM), plus selected contributions from other faculty.
Primary Reading:
Mager, R.E. Preparing Instructional Objectives, Making Instructions Work, Measuring

Instructional Results.
Whitman, N. The Physician as Teacher, Essential Hyperteaching.
Selected readings ACEP Teacher’s Workshop.
Bedside Teaching Synopsis.
Many Handouts.
Format:
6 hours per week assigned teaching time, initially observed. Each session is graded by
recipients.
Several planned didactic lectures on a variety of topics. Initial 2-3 videotaped and
specific instructions given based on performance.
Planned design, review, and implementation of specific segment of curriculum. May be
linked to Fellow’s specific interests.
Participation in MS-IV OSCE on clinical skills and procedures.
Wide variety of observed, then unobserved teaching activities with PAs, medical
students and residents.
Specific writing projects(s) on educational activities.
Topics Covered:
Curriculum design.
Developing content for teaching.
Writing effective goals and objectives.
Planning implementation method to optimize teaching environment.
Evaluation techniques for student and teacher
Establish clear feedback mechanism to modify teaching approach and effectiveness.
4. Media Module (1 month)
Purpose:

Understanding media and the internet as a means of communication and education is
essential for any academic faculty. Specific training in computer programs to facilitate
this area is necessary.
Faculty Responsible:
Natalie Cullen, M.D. Media and Internet Coordinator
Primary Reading:
Stack, LB, et al. Handbook of Medical Photography, Philadelphia, Hanley and Belfus,
2001.
Teaching Series on PowerPoint, Digital Cameras, Internet resources, PDA, and Adobe
Photoshop.
Format:
Practical applications of PowerPoint, Word, and Excel.
Understanding and use of Digital camera in the clinical setting.
Practical applications of Adobe Photoshop.
PDA use (all Fellows will be required to purchase PDA used by EM residents at
discounted rate.
Internet as a resource.
Basic web-site development (based on Fellow interest and skills level).
Integration of electronic media into educational programs.
Topics Covered:
Internet and education, including evaluation.
PowerPoint, to enhance teaching.
Digital media, and manipulation with Photoshop.
Use of PDAs, benefits/problems.
Integration of PDAs into clinical and didactic teaching.
Internet programming skills.

5. Research Grantsmanship Module (2 months)
Purpose:
Academic advancement is often predicated on the successful design and completion of a scholarly work
or activity. During this block the fellow will: become acquainted with resources to identify funding
sources for educational, clinical and basic research, examine the requirements and limitations of a
typical grant in one of these areas, and develop a research idea into the basic elements of the grant
proposal. Additional skills related to these activities will be acquired including developing a basic
understanding of biostatistics and critically reading and analyzing pertinent primary literature.
Faculty Responsible:
JO and other staff from the Research and Sponsored Projects office and Medical Library.
Primary Reading:
Reif-Lehrer, L, Grant application writer’s Handbook, Jones and Barnett, 1995.
Ogden, T.E. and Goldberg, I.A., Research Proposals, Raven, 1995.
Bailar, J.C. III and Mosteller, F., Medical Uses of Statistics, NEJM Books, 1992.
Format:
Weekly meetings with Dr. Olson.
Participation in workshops on computer literature searches.
Participation in workshops on grant writing.
Participation in Evidence Based Medicine workshops.
Attendance at SAEM regional and national meetings.
Development and design of research project.
Completion of grant application.

Topics Covered:
Defining an area of research interest.
Biostatistics.
The environment of medical research:
Budgetary constraints
Medical and biomedical ethics
Grantor expectations
Evaluating medical research and research reports.
6. Administrative Aspects of Academic Medicine Module (1 month)
Purpose:
There are specific skills unique to academic medicine that might not be addressed in the other modules.
These topics will be introduced or reviewed during this month. Some information will be repeated from
the broader perspective during the year long Administrative Model.
Faculty Responsible:
Chair, with assistance from selected faculty and outside discussants.
Primary Reading:
The Evaluative Interview
Evaluation of Residents, American Board of Medical Specialties Services.
Maguer R, Analyzing Performance Problems, Measuring Instructional Results
Time Management
Wilson MP, McLaughlin CP, Leadership and Management in Academic Medicine,
AAMC
Role of the Academic Chair, 2nd Ed. Josey-Bass, 1999.
Additional Handouts
Format:

1-2 hour weekly discussions
One specific administrative assignment
Participation in resident candidate interviewing schedule with observation
Specific time management assignment.
Review Promotion File details.
Topics covered:
Interviewing skills
Techniques/Approaches to Evaluation
Structural assessment Medical School, LCME
Time Management
Counseling skills
Promotions and Tenure
Mentorship

Where does research fit in? Some thoughts on the Scholarship of Discovery and
Application
Why Do Research?
Author: Arthur L. Kellermann
I. Scholarship
Faculty members at medical schools are generally evaluated in 3 domains: service (including patient
care), teaching, and scholarship. For tenure-track faculty, scholarship is the most important for
promotion, and is absolutely essential to earn tenure. For clinical faculty, most medical schools require
achievement of at least "adequacy" in scholarship for promotion to the Associate Professor or full
Professor level. The sine qua non of scholarship is research.
Most promotion and tenure committees measure scholarly productivity in two ways - 1) the quality and
quantity of the candidate's publications in peer-reviewed journals, and 2) the number, size and quality of
the candidate's grants, and the role the candidate played in obtaining them.
Publications come in 2 forms - "peer-reviewed" and "non peer-reviewed". As a general rule, non-peer
reviewed papers count for little in terms of promotion; examples include review articles in "throw away"
journals and submissions to newsletters. Tenure committees favor original research that is published in
peer-reviewed specialty journals such as Annals of Emergency Medicine or Academic Emergency
Medicine; publications in highly regarded general readership journals, such as JAMA and the New
England Journal of Medicine count the most.
Evaluating the quality of scholarship is highly subjective. It is generally based on two factors - 1) the
prestige (i.e., academic rigor) of the journals in which you have published, and 2) the candid opinions, at
the time your promotion is being considered, of 2-5 professional peers as to the merit of your
publications and your overall contributions to the field. To judge the former, the committee will
sometimes ask for a representative sample of your publications. To satisfy the latter requirement, your
chief or chair will solicit letters from academic EM faculty at other institutions who hold the rank of
Associate or Full Professor. Some committees request comments from1-2 colleagues from non-EM
clinical departments at your institution as well

The quantity of publications is measured by counting the number of original, peer-reviewed papers (i.e.,
original contributions and brief reports) you have published over the course of your career. First-
authored and single authored papers are given more weight than co-authored papers, but the latter are
valuable because they demonstrate that you are willing to work collaboratively with others. Editorials,
review articles, and book chapters count as well, but they are less important than original, peer-
reviewed manuscripts. A few book chapters are good, but a lot of book chapters isn't much better.
Committees look for creativity, not rehashing the data of others. Letters to the editor and non-peer
reviewed articles don't matter very much, but include them in your CV anyway. Nothing is too minor to
leave out, particularly when you are striving for "adequacy" in scholarship.
How many papers are enough? There is no hard and fast rule. Criteria vary from school to school. It
matters whether you are being considered for promotion on the tenure track or a non-tenure (e.g.,
"clinical" or "teaching") track. Non-tenure track promotions are much less demanding in terms of paper
counts to achieve adequacy in "scholarship", because it is understood that the candidate has spent the
bulk of her/his time involved in patient care, service, or teaching. Most tenure track promotions, on the
other hand, set very high standards for scholarship. If you are in doubt about how many publications you
need, consult your chair or a senior colleague at your institution.
Research grants come in two forms as well – "intramural" and "extramural". - "Intramural" grants
originate inside the inside the institution and are generally used to support small scale studies or pilot
projects that are intended to generate preliminary data for a later grant. Getting one or more intramural
grants is considered a solid sign of your interest in research, but it won't help you much if you don't
follow them up by obtaining one or more external grants. Extramural grants, also known as external
grants, - are valued more than intramural grants because they bring research funding into the institution
from outside organizations, such as foundations or the federal government.
An informal hierarchy exits as to the value of extramural grants. It is based on the source of the funds.
National Institutes of Health (NIH) grants are the most prestigious, because they contribute to your
medical school's "NIH ranking" and therefore its status in the circles where this sort of thing matters. NIH
grants are followed closely by National Science Foundation grants, for the same reason. These two are
followed by grants from other federal agencies (e.g., Agency for Healthcare Research and Quality
(AHRQ), Centers for Disease Control and Prevention (CDC), National Highway Traffic Safety
Administration (NHTSA), Maternal and Child Health (MCH) and others. In addition to conferring status

on the investigator and the institution, federal research grants are more valuable because they pay a
higher rate of indirect costs (extra money to the institution to support its general operating costs). They
are also hard to get. Obviously, the bigger the amount of the award, the better. In the world of research
grants, size matters!
Foundation grants (such as the Robert Wood Johnson Foundation, the Gates Foundation, The Andrew
Carnegie Foundation, The Annie Casey Foundation, the Woodruff Foundation, and others) are relatively
prestigious, but they pay much lower indirect costs and are therefore considered less valuable by the
institution. Also, they don't count towards your school's NIH ranking. Foundation grants are followed by
"investigator-initiated" industry grants (i.e., you came up with the idea, designed the study, and got
industry funding). Industry-sponsored studies that involve a lot of money and/or generate an institutional
patent count for a lot, but those that don't bring in a patent or a lot of dough count for relatively little.
"Industry sponsored" studies (i.e., the study was designed by the company's in-house research staff and
your role involved little more than enrolling cases) count for very little. While the latter are useful for
learning how to conduct a clinical trial, and may even bring some money into the department, they are
not highly regarded by most P&T committees.
Role:As was the case with publications, your role in the grant matters as well. Being the Principal
Investigator or "P.I." of a study counts for more than being co-PI, since the PI is ultimately responsible
for designing the study and leading the team. Being a Co-PI (for example, acting as "site director" on a
multicenter trial) counts for more than being a co-investigator, since the former implies more managerial
responsibility. However, doing any extramurally-funded research (as PI, co-PI, or co-investigator) counts
much more than doing only intramural (i.e., internally funded) research, and conducting any research
(whether it is funded externally, internally, or not at all) counts for more than not doing research of any
sort.
Currently, most EM faculty obtain promotion on the clinical track. Generally, clinical-track faculty are
expected to compile a modest but meaningful record of publications, combined with some invited
lectureships at other institutions or at national specialty meetings. This level of accomplishment (and
ideally, some external grant funding) is generally sufficient to establish "adequacy" in scholarship in the
eyes of all but the most demanding promotion committees. This level of productivity, combined with the
high levels of teaching and service typical of a career-committed EM faculty member, should earn you
promotion.

Do not, however, take promotion for granted! Meet regularly with your Chief, or Chair to review your
progress. Her or his support will be essential when you go up for promotion.
The fact that you are an outstanding teacher, have worked a ton of shifts, served on 15 hospital,
community or departmental committees, and get along with your chair, does not guarantee that you will
earn promotion. Most candidates for promotion to Associate Professor level or above are required to
show evidence of that they have achieved a measure of national recognition in their specialty. This can
be done by establishing excellence in service (e.g., getting involved in or chairing a committee or task
force for SAEM, ACEP, or other EM organization); excellence in teaching (by giving invited talks at
regional or national meetings, "grand rounds" at other EM residency programs, and/or being visible in
other national EM education projects), and/or excellence in scholarship (by securing grants and
publishing a substantial number of high quality, peer-reviewed papers). For promotion to Professor,
institutions generally require an even higher standard of proof that you have achieved national, if not
international, standing in your field.
II. Why do research?
There are several reasons to conduct research. They can be grouped in 4 broad categories - personal
reasons, departmental reasons, specialty reasons, and societal benefit:
A. Personal reasons:
Career advancement: Most institutions require Assistant Professors to achieve at least "adequacy" in
scholarship before they can be promoted to the rank of Associate Professor or above on the clinical
track. That typically means publishing (as first author as well as co-author) several papers. To insure
that this happens, you should get involved, at the outset of your career, in some sort of research.
Residents respect you for your clinical acumen, but medical students and Deans look at your record of
publications.
"Protected time": Successful investigators (particularly those who are clever enough to secure

extramural funding for their work) generally get "protected time" to pursue their research interests. This
translates into fewer clinical shifts, fewer night shifts, and fewer weekend shifts, than a full-time clinician-
educator in the department. By the way, if your chair refuses to give you a break in your schedule to
pursue research if your time is funded by a federal grant, it is not only unfair, it's illegal.
Travel: In addition to getting to regularly attend nifty meetings like SAEM, researchers often have
opportunities to attend other scientific meetings, both inside and outside the U.S. Those who achieve
national prominence are frequently invited to give "guest lectures" at other programs as well as state,
regional, or national professional meetings. A medical school dean once noted, "Academic Medicine
doesn't pay as well as private practice, but you can't beat the travel."
Ego: It's exciting to see your name in print in a top journal like Annals of Emergency Medicine. Mothers,
fathers, and relatives will love getting reprints, and your residents will enjoy critiquing your work in
journal club!
Satisfaction: Research, no less so than patient care and teaching, is hard work. However, it is also fun
and highly satisfying. It offers an interesting break from the daily (and nightly) routine of clinical practice.
Research in EM often focuses on clinical issues, with the goal of improving our approach to care. As a
result, research can give you and your colleagues better ways to take care of patients. Given the
inherent frustrations of ED care, it is important to set aside time to drain the swamp, instead of spending
all of your time and energy battling alligators.
B. Departmental reasons:
Recognition: Deans at prestigious medical schools are judged by their institution's NIH ranking (i.e., how
many dollars in annual NIH funding the medical school secures relative to its peers). If your clinical
department contributes to the school's NIH ranking goal, your Dean will appreciate it. Academically
productive departments have greater national visibility, tend to attract high caliber residency and faculty
applicants, and maintain a higher profile at the SAEM annual meeting and other venues. Strong,
research-oriented departments tend to attract and retain strong, research-oriented faculty. Success
begets success.
Financial: In successful departments, extramural research grants provide a significant boost to

departmental revenue. To provide departments with a strong incentive to conduct research, many
Deans return a share of indirect cost recovery from grants to the departments that secured them. This
money can be used to support further research and career development. Salary support from grants
buys "release time" for faculty researchers and pays the salary of research nurses and research
assistants. It also allows your department Chair or Division Chief to hire more doctors, enhancing the
departments' size and influence.
Clout: Collaborating departments respect excellence in research. They are much more likely to include
EM faculty members as co-investigators in their own studies if they respect your program's science and
its output of publications. Research collaboration is a good way to build trust and promote cooperation
on other fronts.
Recruiting: Medical students and residents are avid readers of journals. Most, if not all, are drawn to
departments and individual faculty members who appear frequently in print. Since a program is only as
good as its personnel, anything that helps recruit and retain high-quality residents and junior faculty is
worth its weight in gold.
Pride: People like to be part of a top-tier program. Research productivity is an easily measured
parameter of a program's standing in academic EM. Programs that conduct research typically have
higher esprit de corps, and are arguably more careful about patient care, than those that do not.
C. Specialty reasons
Status: As the specialty of Emergency Medicine produces more high quality studies, and accomplished
researchers, it gains respect in the house of medicine.
Funding: Research brings substantial funds to EM investigators and the programs and laboratories in
which they work. It also helps drive clinical innovation in our specialty.
Influence: Thanks in large part to their academic achievements; Emergency Physicians are occupying
increasingly important and influential roles. An Emergency Physician serves as senior editor of JAMA;
three others currently or recently directed a major federal agency, and others are rising to the level of
Associate Dean in their medical schools. E.R.s are being assigned to study sections at NIH and other

funding agencies. The number of Emergency Physicians that have been elected to the Institute of
Medicine has reached double digits. More will be named in the years to come.
D. Societal benefit
Clinical impact: EM generated research has made a major impact on emergency cardiac care, acute
stroke management, asthma, injury control, our understanding of cellular ischemia, use of diagnostic
technologies in the ED (both lab and imaging) and other laboratory and clinical innovations. We practice
better and more efficient emergency medicine today than ever before, thanks in large part to the work of
EM researchers.
Public health - Patients who receive better and more timely ED treatment have better outcomes and live
longer than those who do not. Using the ED as a window into the health status of communities is a
powerful tool for public health.
Social Justice - Because Americans know that they can always to an ED when the chips are down,
Emergency Departments serve as barometers of the health status of a community. For this reason,
Emergency Physician researchers can use ED data to shine a spotlight on important social problems
such as the plight of the uninsured, poor access to care, substance abuse, mental illness, and domestic
violence.
III. Getting Started
The biggest hurdle to conducting research is getting started. To do that, you must overcome a number
of mental obstacles to initiating research
"I don’t have sufficient time." Make your clinical practice your "lab". There are thousands of worthwhile
projects that need to be conducted in EDs or other settings that are within the domain of Emergency
Medicine.
"I don’t have formal training." If you want it, get it. One of my top attendings went to night school on his
own to earn his MPH. Many Universities offer evening MPH courses, research seminars, Web based
learning, and other opportunities. Two semesters of Epidemiology and two semesters of Biostatistics

can go a long way. Attend Journal club and any other seminar that looks worthwhile. Learn research
methodology in courses and seminars, and then apply it to your chosen area of interest and expertise.
"All the good ideas are taken"
Rubbish! Be a good listener. Ideas are all around you. You don't have to steal them, because people
give them away all the time. Alternatively, select the most frustrating issue in your department, and
decide how you can improve it. Evaluate your efforts and viola - you are in business. That is how I
began my first two projects as a faculty member. Strive for something original, or at least fairly new.
Which type of movie do you prefer - an original film, like "the Matrix" or a worn out sequel, like "Rocky
XVIII"?
"I’m not smart enough."
If you are smart enough to read and listen, you are smart enough to be a successful researcher. Don't
invest five minutes on a project before you have spent at least two days learning what has been already
been done on the topic. You may find that the answer has already been found, or alternatively, that
there is a gaping hole in the literature that your study will fill. Once you have done that, seek out a
trusted colleague or a mentor and solicit their opinion of your idea. Listen to their feedback, and
incorporate their advice where you can.
"I can’t get money for my project" More than half of the manuscripts I have published to date (including
several in JAMA and New England Journal of Medicine) were conducted with little or no funding. Some
cost nothing more than my time. Pilot studies should be done first, to lay the groundwork for descriptive
or an analytical study. Successful descriptive or analytical studies set the stage for experimental trials.
Major universities often offer small "seed grants" that can provide the funds needed to mount a pilot
study or test a new idea. Once you have secured a start-up grant, go for something bigger.
"I don’t know how to write." If you realize this, you are better off than most. Writing is an acquired skill,
like learning how to start a central line or perform endotracheal intubation. The more writing you do, the
better you will get. Find a trusted mentor who is willing to edit your work, and don't get your feelings hurt
when he/she returns your manuscript in tatters. Learn to write simply and clearly. This is far more
effective than the turgid prose some researchers pass off as "medical writing".

"I don’t have a mentor" Some people are lucky enough to land a job in a department with a seasoned
investigator who can help them learn the ropes. Others are not so fortunate. It is not necessary for your
"mentor" to be from your own institution, or to be an emergency physician. Close proximity helps, as
does disciplinary understanding, but neither is essential to develop a productive mentoring relationship.
A mentor's willingness to give you advice, and your willingness to receive it, is more important than
whether or not they work in your department. During my research fellowship, my primary mentors were
a Neurologist and a General Internist. During my formative years as a junior faculty member, my mentor
was a Geriatrician. Over the course of my career, I have mentored young Emergency Physicians from
several programs around the country as well as my own faculty. I have also mentored young faculty at
Emory from other departments.
"I’ll be rejected, so what’s the point?" Everyone gets rejected! It's part of the process! Learn from the
feedback, pick yourself up, revise and/or try again. If one journal won't take your paper, the chances are
good that another one will. Most specialties have more journals than they need. If, however, you
discover that your paper is fundamentally flawed, ditch it and move on. You probably did not secure, or
listen to good advice at the outset - this is why thinking a study through and bouncing the idea off others
before you start is so important.
"No one respects me (or EM) anyway." They will, if you get your butt in gear. Publications (and even
more important, grants) are the coin of the realm in academic medicine. House staff respect clinical
acumen, but Deans, department chairs, and faculty members from other departments respect your
research. It is not necessary for everyone in your department to publish, but it is vital for enough
members of the department to publish to give it visibility. In an era of collaborative practice, excellence
should be defined in collective rather than individual terms.
"No one will collaborate with me (or us)."
Our colleagues need us more than we need them. You would never dream of walking up to the CCU
and expecting a cardiologist to help you do a study of thrombolytic therapy in their unit without
attribution. Why should cardiologists, neurologists, internist or surgeon expect emergency medicine to
conduct case finding in the emergency department without a similar degree of recognition? My answer
to queries from other departments is quite simple - "We may be able to help. Who in my department

have you identified to serve as your collaborator and co-author?"
IV. Secrets of success
Start simple. Many research projects sink under their own weight. Collect only the information you need,
and nothing more. Every element of a data collection instrument or questionnaire should be justified, or
left off. My fellowship research project, a study of drug screening in the ED involved far too many
variables and almost sank under its own weight.
Build on success. Small projects carried forth to completion are much more satisfying than ambitious
failures. As you acquire confidence and credibility, you can do more. (Examples from my early research
include a study of outcomes of refractory prehospital cardiac arrest, a descriptive study of gun deaths in
the home, a quasi-experimental study of dispatcher CPR, an observational study of the use of portable
pulse oximetry in the ED, and a descriptive study of patient "dumping").
Don’t put too may balls in the air at one time. Avoid the temptation to start multiple projects or construct
an "assembly line". If you are getting started, and you are attempting to run more than 2 projects, you
are over your head. During my own research fellowship, I attempted to simultaneously study drug
screening in the ED, firearm-related deaths in the home, and a landmark medical-legal case. I
eventually published work from the first two studies, but I failed to publish anything from the third. Had it
not been for my wife's demand that I focus my attention, I probably would have failed to publish
anything.
Invite criticism. If your idea is flawed, fix it. If you can't, ditch it and move on. A well-reasoned critique will
save you months of work and years of heartbreak.
Find a mentor. It is almost impossible to succeed alone. A mid-career investigator or professor who
knows the ropes is worth her/his weight in gold. If need be, go outside your discipline. My first faculty
mentor was Bill Applegate, a gerontologist. My top collaborator in the first phase of my faculty career
was Bela Hackman, a cardiologist. The co-author of my best work in injury control is Frederick Rivara, a
pediatrician.
Be an opportunist. If you see an opening, take it! Some of my best studies came from turning salesmen

into collaborators to conduct technology assessment projects (e.g., my AED and pulse oximetry
papers). Any program worth implementing is worth evaluating to determine if it works.
If you have to choose between love or money, choose love. Don't select a project you hate because it is
"fundable" or someone offers to make you co-investigator. Follow your heart. Research is hard work
when you are fascinated with the idea, pure misery if you aren't. Life is too short to work on an issue that
you don't believe in, or one that bores you to tears.
Pick a subject that matters. If you are going to do research, choose a topic that matters. The first NEJM
special article, a descriptive study of firearm fatalities in homes, did not include a single P value or
statistical test. Pick something in your department that bugs you, and turn it into a study. This is what led
me to conduct studies of patient "dumping", ambulatory visits to EDs, "bounces" and asthma treatment.
Write clearly. If your mother can't understand your research, your colleagues won't either. Turgid writing
isn't "scientific" - it's bad writing. Ask a respected colleague or mentor to edit your work before sending it
out. If you haven't worked through at least 5 to10 drafts, the odds are great that you haven't polished it
enough. Beginning writers invariably produce manuscripts that are twice as long as they need to be.
Some experienced writers do the same thing.
The best way to learn how to write a competitive grant proposal is to read a competitive grant proposal.
The first grant I ever wrote (a case-control study of violent death in the home in relation to gun
ownership) was adopted from a very well written case-control study of the relationship between breast
cancer and prior use of oral contraceptives. One of the best ways to hone grant-writing skills is to read
good grants written by others.
Have fun! - Clinical research is a great way to pace yourself through an academic career. Patient care is
exciting but wearing over time. While the satisfaction of making a difference for a patient is great, it is
also satisfying to take an idea that was generated at the bedside and use it to make a difference.

Research as a career foundation
Author: Charles V. Pollack, Jr.
Career development in academic practice is a process that begins in medical school (or even before)
with the establishment of a work ethic and areas of specific interest, continues through residency and
perhaps fellowship training with the identification of mentors and the selection of a first and then
subsequent academic positions, and then is shaped and adapted every day of our professional careers
by factors both intrinsic and extrinsic to the physician. Throughout this career-long process, however,
there are certain activities or "core competencies" that serve as foundations for intellectual and
professional development. Although it is certainly possible to have a successful academic career without
achieving specific goals or expertise in research, most academicians view research as the cornerstone--
or least one of the cornerstones--of a career that is palpably different from that of colleagues who
choose community-based over academic practice.
"Research" and "academics" are not synonymous terms, although many think that they are. The role of
research in academic practice is driven by (1) the individual’s interests, (2) the department’s degree of
involvement in research, and (3) the institution’s level of support for research. Furthermore, research in
emergency medicine (4) may or may not require specialized training; (5) may be clinical or laboratory-
based; and (6) may center on issues integral to other specialties as well as our own. In short,
"emergency medicine research" is as diverse as are practitioners of emergency medicine. The
remainder of this chapter will consider each of these six factors in some detail.
(1) The individual’s interests. Research is a frustrating, fatiguing, stress-inducing, time-consuming chore
. . . for those who do not enjoy it. The exact same regimen may be the highlight of another’s day. To
build a career in research, one must have a questioning mind, a tireless work ethic, an innate sense of
organization, the personality of a cheerleader, an enjoyment of (or at least the lack of an aversion to)
medical writing, and a willingness to take potshots from pundits, colleagues, and intellectual competitors
on a regular basis. "Research" may include medical writing (review papers, invited manuscripts,
textbook chapters), laboratory studies or analyses, retrospective clinical studies, prospective clinical
studies, and surveys. Many traditional academicians (and promotion and tenure committees) tend to
discount somewhat at least the first and last of this list, and some similarly disdain retrospective studies.
Statistical inquiries such as meta-analyses fall somewhere in between. All of these efforts, however,
involve the basic element of formulating a question, researching related issues to refine the question,

and proposing a way either to summarize or direct previous answers or to derive a new answer.
The first generation of emergency physicians attacked such questions with boundless enthusiasm,
limitless energy, and an utter lack of discipline. Lacking the framework of an established specialty,
seeing all clinical issues as being pertinent to EM, and having essentially no funding sources from which
to draw support, these pioneers studied just about everything . . . moving from asthma to urinary tract
infections to trauma to airway. Interesting data were generated that in retrospect helped define our
specialty, but these clinician-researchers with only occasional exceptions were unable to establish
"research niches" for themselves, from which they might have been able to establish ties to more
established researchers and specialties (and their funding sources). Most of these early EM researchers
eventually ascended the academic ranks, but this was often because P&T committees of the day--faced
with this new specialty about which they knew little--failed to develop and uphold consistent standards
for career milestones for emergency physicians. Today’s academicians face a much more exacting
standard, and therefore must seek to focus their research interests and energies in one or at most two
clinical areas if they are to secure funding and peer recognition.
This "focusing" need not occur on day 1 of one’s academic career, but the earlier it occurs, the more
likely one will be able to develop fully his or her potential in that area. "Areas" of focus in EM research
are exemplified by this list, which the author in no way holds as all-inclusive:
Basic science:
Resuscitation
Preconditioning
Ischemia/reperfusion
Toxicology
Infectious disease
Trauma/injury
Clinical science:
Cardiovascular
Neurovascular
Shock/resuscitation

Infectious disease emergencies
Complications/trauma in pregnancy
Trauma
Airway management
Toxicology
Emergency medical services (EMS/out-of-hospital)
Respiratory emergencies
Pediatric emergencies
Wound care
GI/GU emergencies
Gynecologic emergencies
Environmental emergencies
Endocrine emergencies
Psychosocial emergencies
Epidemiologic/population research
An important note to make in reviewing this list is that perhaps only EMS is not accompanied by a
readily apparent overlap with interests of other specialties and disciplines. If handled adroitly, this
realization may make the emergency physician researcher’s task more possible, more fundable, and
more fun. An academic environment in which two or more members of the department share similar
research interests typically results in an even more productive interplay and greater satisfaction.
In most institutions, some proficiency and demonstrated productivity in research is necessary for
continued advancement and career development. The choice not to pursue research does not
necessarily obviate the likelihood of advancement, but it may make it much more problematic.
(2) The department’s interests. The remainder of this discussion includes several factors that are
external to the individual; clearly this is one. The physician-researcher requires the tangible support of
his or her chairman in order to develop a research career, or even to develop a recognizable research
facet to a non-research-focused academic career. The currency of this support is time--time
prospectively released from other academic and clinical responsibilities so that the research can be
pursued. One may complete one’s first and even second research project in one’s "spare time," but the
dedication required to make research efforts a substantive part of one’s academic career requires paid

time away from other duties and distractions.
The other critical component a chairman can provide to nurture young investigators is seed funding,
from the department or elsewhere within the institution, to support preliminary studies that may in turn
attract outside funding. Seed funding may also be sought from a research training grant (for example,
an NIH K1 award), which may be less competitive than traditional research grants, but also require
significant institutional infrastructure to support successful applications; and from foundations such as
the Emergency Medicine Foundation (EMF) and the Fund for Academic Emergency Medicine (FAEM).
One must also be realistic, especially early on in an academic career. Most chairs do not have limitless
sources of seed funding nor of uncompensated attending time. One’s research career generally starts
"on one’s own time," a fact that results in many promising research interests being left behind. Junior
attendings who are interested in developing a significant research aspect to their careers should expect
to devote 60-70 hours per week to the combination of assigned clinical and teaching duties and the
building of one’s own "research infrastructure." Right out of residency, this may not be appealing. On the
other hand, chairs are anxious to reward and nurture the focus and early productivity in research that
can result from this effort.
In basic science research, the department’s role in encouraging research career development is to
provide laboratory space and funding, in addition to time. Unfortunately, few EM departments today
have independently funded research laboratories. It then becomes the chair’s responsibility to link the
interested emergency physician with faculty from other specialties or on the institution’s basic science
faculty with whom shared interests and "grunt work" (made available by protected time) can potentially
be parlayed into shared productivity. Many successful EM-based basic science researchers have
established themselves in other researchers’ labs prior to qualifying for their own funding. The chair’s
wholehearted support is also required in any application for funding, and must be presented along with a
pledge to cover shortfalls both of money and time for supported projects.
In clinical research, the support needed by the successful researcher starts with the chair but extends to
the entire department--attendings, residents, nurses, research clerks, consulting teams, unit secretaries,
even registration personnel. The well-developed departmental research program is primed to screen for
potential study subjects at every interaction between the patient and the "system". Only with a sufficient
example set by and mandate from the chair is this feasible. The successful researcher will learn from his

or her interactions with colleagues what reminders of ongoing studies work best, whether application of
incentives or disincentives result in better patient enrollment, and how to leverage his or her research
goals into cooperative research efforts by others, to the benefit of all. Furthermore, the researcher
cannot rely solely on the chair’s support; he or she must set the work ethic and enthusiasm example for
screening and enrolling patients if others without a vested interest in the research are expected to do
the same.
The department’s support of building attendings’ research careers is also measured by the resources
allocated to necessary equipment, to ancillary research personnel, and to special instruction (usually at
a price) for researchers-in-training. It is nearly impossible to build a research career, or even to have a
substantive research agenda within an otherwise non-research-focused career, without this level of
support. On the other hand, faculty who expect this type of support must be prepared to show
productivity--measured at least in publications and probably in (eventual) external funding as well--in
return. One must strike a proper balance between guiding and advising residents on their research
projects and maintaining time, energy, and effort for one’s own primary work.
(3) The institution’s interests. Department chairs can accomplish only so much without support from the
institution. Intrainstitutional barriers to research cooperation and mentoring must be overcome. Access
to institutional facilities and financial support must be negotiated on behalf of emergency medicine,
which may be viewed--particularly in more traditional institutions--as an interloper. Lab space, statistical
support, grant writing resources, computer equipment, seed grants, and the like are essential to
research career development in EM just as they are in other disciplines. Grants offices should be
informed about EM-specific sources of funding such as the EMF and the FAEM, and these offices in
turn should inform EM researchers about opportunities for acute care research that may be initially
targeted to other departments. Spending time developing interdepartmental relationships within the
institution or even among multiple institutions may result in cooperative funding agreements and an
enhanced productivity level for all.
The institution should also support networking; though in today’s society this is perhaps an overused
term, the exchange of ideas and opportunities among colleagues is essential in establishing and
maintaining a research career. In academic institutions, networking must cross specialty lines. An
emergency physician researcher cannot expect to be productive in a vacuum, and should seek
colleagues interested in the same areas in other clinical departments, and, if applicable, in basic science

departments as well.
(4) The need for specialized training. In general, residency training in emergency medicine provides
inadequate training in research for one who wishes to make research a significant part of an academic
career. Also in general terms, the optimal training for research is a full-time, two- to three-year
established research fellowship, usually involving pursuit of an advanced degree as well as specialized
research skills that are (hopefully) deserving of independent extramural funding. Unfortunately for the
specialty, very few emergency physicians are interested in following the fellowship route, usually due to
very legitimate concerns about income, career time, etc.
There are several options for less intensive training, but the results are predictably less far-ranging than
those earned via a formal fellowship. Many grant-writing workshops are offered nationally each year;
SAEM periodically offers a workshop more directly applicable to EM researchers at the Annual Meeting,
but one should first look for such opportunities at one’s own institution, where the benefits from
attending may be magnified by the opportunity to network with other budding researchers "at home."
ACEP offers a 13-day (in two sessions, six months apart), intensive Basic Research Skills workshop in
Dallas. Modeled after the highly successful ACEP/EMF Teaching Fellowship, this curriculum offers an
extensive introduction to issues of study design, statistical analysis, protocol formulation, and
grantsmanship. It is pertinent to clinical research only, as there simply is no "one-size-fits-all" approach
suitable for the diverse areas of basic science research pertinent to emergency medicine.
The most important aspect of "training" for research in emergency medicine is identification of a suitable
mentor. It is safe to say that a self-trained "researcher," regardless of his/her energy and enthusiasm,
will be unable to develop research into a career-defining interest without the stable guidance of an
experienced (and funded) mentor. That is not to say that writing papers and answering basic questions
cannot be done on an individual basis, but such activity is otherwise often destined to be "window
dressing" on an academic career.
There is no formula for finding a mentor. Even in highly structured research fellowships, fellows may
work with several researchers before identifying one with whom "the chemistry" and joint interests are
right. Physicians seeking a mentor outside a fellowship setting likely have an even tougher task in this
regard. This is another requirement of a supportive department chairman--the ability (and interest) to
link interested researchers with others in the department, elsewhere in the institution, or even in other

institutions, who will tend and nurture research interests into the opportunity for meaningful
accomplishments. Mentors and networking colleagues may also be sought at specialty society meetings
not usually targeted at emergency physicians, such as the American Thoracic Society if one is
interested in asthma research, or the American Heart Association for resuscitation and cardiologic
issues. Finding a mentor already funded for research with which one’s interest is shared may be an
even more efficient way of getting established in research.
(5) Clinical vs. basic science. This is an issue both of personal preference and institutional capability.
Some institutions simply do not have the physical capacity to support basic science research,
regardless of an individual’s enthusiasm for doing it. Although funding that backs up the enthusiasm
might address the problem in theory, funding agencies are unlikely to award grants to institutions
without pre-existing infrastructure. There are many areas of basic science research that are pertinent to
EM, but if lab work is to be part of one’s career development, one must choose an institution with the
appropriate capabilities. It should also be kept in mind that many techniques used in one area of
laboratory research, even when mastered, may not translate well into other areas of research. This
"subspecialization" can be a barrier to continuing one’s basic science research in the absence of
independent funding. After decreasing during the mid-1980s and 1990s, governmental funding for basic
science research is rising and can be expected to be stable for the next few years.
As opposed to laboratory work, any busy ED can potentially support a clinical research program. Again,
infrastructure--supportive staff, research clerks/nurses, the availability of computers and statisticians--
may be needed to perform clinical research of much substance, but one may "cut one’s teeth" on clinical
research early in one’s career, perhaps even as a resident. Institutional funding may be available for
small projects, especially if there is a quality improvement aspect to the work. Foundations and
governmental agencies (such as the AHRQ, formerly AHCPR, and the CDC) are increasingly interested
in supporting ED-based clinical research, and the opportunities for industry-supported research have
never been greater. Industry support for investigator-initiated protocols can be a boon both to the
researcher and the department, but protocol development and data ownership issues should be clearly
spelled out prior to signing a contract. One’s institution’s research or contracts office can provide
valuable assistance in such negotiations. Participation in industry-initiated trials (the proverbial "drug
studies") may provide needed capital for infrastructure development and may be useful for teaching
residents about informed consent, case report form preparation, and other fundamental research issues,
but rarely result in publication credit for the individual and in most institutions are not helpful in the

promotion and tenure process. Participation in industry-initiated multicenter trials should be considered
only if the researcher’s/department’s answers to each of the following questions is "yes":
Is this study pertinent to EM practice?
Does the disease being studied present to my ED with a predictable frequency?
Is the study scientifically sound?
Is this study one that will generate sufficient sustaining interest in the department
necessary to ensure completion?
Are the resources needed to complete the study either already available (with unmet
capacity) in the department, or are provided by the study?
Is the study budget reasonable to support not only the index study but also other
research activities (particularly those that are currently un- or underfunded) in the
department?
If other clinical departments are involved in execution of the study, are they willing to
participate reliably, and does the budget support payment for their contributions as
well?
Another broad area of potential research interest within EM is population-based or epidemiologic
research. The potential for meaningful contribution in this area is largely unfulfilled. Successful pursuit of
such research mandates a good working knowledge of sampling and statistical analysis techniques and,
typically, the support of colleagues from other specialties and from governmental agencies (such as
health departments).
Clinical research also offers the greatest opportunities for those academic physicians who wish to have
some research "on the CV" but are not interested in being full-time researchers. Active participation in
departmental projects can bring authorship credit as well as interesting and career-expanding
networking opportunities.
(6) Involvement of other specialties/disciplines. It has been emphasized already that very few areas of
research interest within EM do not overlap with interests of other specialties and basic science
disciplines. Furthermore, there is an acknowledged numerical deficit of seasoned mentors and funded
researchers in our young specialty. In most institutions, emergency physicians who are able to establish

research as a, or the, primary cornerstone of their academic careers do so with the assistance of
colleagues outside the ED. Such input should be sought from the very beginning on one’s academic
career.
In summary, the emergency physician who seeks to build a research career requires, first and foremost,
an inquisitive mind, a true and overriding desire to design and execute research plans, and the
enthusiasm, energy, and dedication to support that desire until a sufficient track record can be
generated to "buy down" clinical time and be able to pursue research within the context of a productive
and satisfying academic career. The second requirement is external--an understanding and supportive
(tangible and intangible) chair. This support should be specifically sought during the interview process,
whether for one’s first academic job or for one’s fifth. Given this support--which includes the real
potential for protected time, some infrastructure, perhaps some outside training--one must then develop
one’s interests, identify a potential mentor, and focus one’s enthusiasm on study development and
funding. The successful researcher always has the next two or three protocols--dependent upon the
outcome of the current studies--ready for consideration. The result of this planning and execution can be
job satisfaction, the enjoyment of networking with other physicians who share one’s interests, and
career advancement.

A Blueprint for a Successful Research Program in Emergency Medicine
Authors: W. Brian Gibler and Brian J. Zink
Introduction
The development of a successful research program remains the greatest challenge for any Department
or Division of Emergency Medicine. The patient care and teaching missions of most Emergency
Medicine programs are easier, relatively speaking, to define and achieve excellence in performance.
The purpose of this document is to provide the academic leaders of an Emergency Medicine
Department or Division a blueprint for a successful research program. Establishing a vision, setting up a
research infrastructure, recruiting research faculty, developing collaborations with other departments,
and identifying funding sources will be discussed. As the specialty of Emergency Medicine continues to
evolve as an academic discipline, it is our hope that this effort can provide a framework for a successful
research program in virtually any setting.
Establishing a Vision It is often tempting for a faculty group to pursue a wide variety of research ideas
and projects that reflects far ranging interests and expertise. Unfortunately this haphazard approach to
research results in a lack of Departmental focus and often mediocre research productivity. Establishing
a clear research focus for a Department often results in a more coherent approach to resource
allocation, faculty hiring, and grant writing. Typically every faculty group has one or two individuals that
have been effective in concentrating on a particular research area with resulting success in obtaining
funding, publishing papers, and in bringing national notoriety through presentations of work at national
and international scientific forums. The Chair of the Department, with the support of the rest of the
faculty, can then identify these one or two areas as research focus directions with the successful
researchers as leaders of the effort.
Future hiring of young researchers by the Department should support these newly declared areas of
research focus. Resources allocated by the Department should directly support these initiatives and
members of the faculty and residents should be encouraged to work with the productive researchers to
build programmatic strength. If no senior researcher is present in a newly developed academic unit,
faculty recruiting should be directed toward hiring a productive researcher to build a program around.

It is essential that the Department Chair or Division Chief possess a clear vision for the research focus
area(s) of a program. This vision must be articulated frequently to ensure that the faculty, residents, and
staff of a Department understand the common goal of the research effort. This broad understanding can
then provide support when financial and personnel resources are used to improve research productivity
in an area of focus.
Granting sources such as corporate, foundation, and federal agencies are more likely to provide funding
to organized, focused, and mature research groups. Senior faculty can bring funding to a Department
that includes support for junior faculty, fellows, residents, and support staff. These focused research
efforts also can improve collaborative relationships with other Departments within the medical center
and with other Departments of Emergency Medicine throughout the United States as well as other
countries. Funding sources are familiar with this research focus approach and typically provide monies
to support multiple members of the research team. The junior faculty member can begin to use this
"collateral" grant to develop an independent funding history to become competitive for individual
financial support in the future.
Recruiting Research Faculty The recruitment of junior or senior research faculty requires a clear vision
to determine the training, talents, and interests of the Department of Division. Successful senior faculty
researchers can serve as an effective magnet for junior faculty interested in pursuing a research career.
Most individuals finishing a residency and aspiring to become successful researchers understand that a
mentor is essential to obtain the necessary training to become an independent investigator. Ideally the
junior faculty member will pursue a fellowship position with substantial non-clinical time to learn
research methodology and grantsmanship from an established senior investigator.
The mentor does not need to be a clinician, or even a member of the Department or Division of
Emergency Medicine. A PhD scientist can offer invaluable services as a senior mentor for a young
faculty member. The Department of Emergency Medicine may actually decide to hire a PhD researcher
to lead a particular research focus area. In some instances, hiring successful PhD scientists to lead a
research program may be easier than luring a senior Emergency Medicine clinician scientist from
another program.
Hiring junior or senior level physician scientists to a Departmental research program requires significant
clinical off-load. Typically a load of 24 hours per week is considered the maximum amount of clinical

time for a successful researcher. Further reductions in clinical time can be provided as an incentive for
the researcher that successfully brings significant research dollars into the Departmental coffers. Failure
to provide clinical off-load to prospective candidates for research positions substantially hinders
recruiting efforts, particularly for the most talented prospects receiving multiple faculty offers.
Developing Collaborations with Other Departments After defining a Departmental research vision,
seeking collaboration from other Departments in a medical center can be extremely helpful. Often other
older Departments have established senior investigators with prolific funding histories. Whether an
Emergency Medicine faculty is looking for an established mentor in another Department, or simply
attempting to build a critical mass of researchers in a particular area, inter-departmental collaboration
can be exciting and financially rewarding through successful awarding of grants.
Collaboration with other Departments by emergency physicians also enhances the stature of the
Department or Division of Emergency Medicine in the medical center. Being perceived as intelligent
investigators can improve teaching and patient care relationships with other Departments. A successful
research program that contributes to the medical center research goals can lead to resource allocation
to Emergency Medicine. Presentations at the national and international level with publications in major
journals also enhance the institution’s reputation.
Areas of Focus While research in Emergency Medicine can cover many areas, developing a focus that
is fundable should be the individual researcher and Departmental goal. A number of Departments and
Divisions of Emergency Medicine have received funding in a variety of research areas, however, some
common themes emerge:
Brain Injury/Resuscitation
Heart and Lung Injury/Resuscitation
Infectious Disease
Injury Prevention
Access to Care

Outcomes Research
Environmental Emergencies
There is significant funding available in these major focus areas for Emergency Medicine researchers.
As there is precedent for expertise in Emergency Medicine in these research areas, which has led to
previous corporate, foundation, and federal funding, new research teams may be more likely to be
awarded funds.
Setting Up a Research Infrastructure The development of an infrastructure for research is considered
essential. For a basic researcher, a well equipped lab is necessary to be a productive researcher. In
many cases, a junior Emergency Medicine investigator can work in the lab of a senior scientist from
another Department. This has the dual benefits of being an inexpensive alternative to setting up a lab
prior to obtaining external funding while exposing a fledging Emergency Medicine researcher to a senior
mentor. This training period, while serving as a co-investigator, is usually necessary before receiving the
primary funding essential to build a lab.
For clinical research, the Department or Division can make real investments that can enhance the
likelihood of receiving corporate, foundation, and federal research funding. Hiring a research nurse
coordinator can serve as the nidus for clinical trial funding and investigator-initiated corporate research.
Developing an office for research in a Department or Division can help to coordinate existing trials and
developing grant proposals. As such an office becomes more sophisticated, a research nurse
coordinator and Departmental grants office can be of substantial assistance to investigators. If an
infrastructure works properly, grant submissions, IRB submissions, grant tracking and communication
with sponsors can all be facilitated for the research faculty. Most funding agencies expect a mature
research group to have a research nurse coordinator and grants office to successfully complete clinical
research studies. A minimal infrastructure for clinical research can cost $100,000, which includes
benefits and office space for non-faculty staff. Depending on the complexity of the support staff structure
for research, this cost can be increased 2-3 fold. Ideally, research funds can offset most, if not all, of the
costs of support staff.
Another important consideration in constructing a successful research program is collaboration with a

competent biostatistician. In some circumstances, the Department has to provide funds to pay for
biostatistical consultation for pilot trials or non-funded research. Subsequent grant submissions should
contain funding for data management and analyses by a biostatistics group. Again, funding agencies
expect such expenses in a grant proposal.
Identifying Funding Sources Ultimately Departments and Divisions of Emergency Medicine should
position themselves to obtain federal funded research. These funds for basic and clinical research
awards not only cover Direct or the actual costs of performing the research, but also Indirect funds
which currently total 55% of the Direct costs of the study. Medical school Deans use National Institutes
of Health (NIH) funding of Departments to judge their success as research entities, as well as Indirect
funds to provide an additional source of money to build the research and teaching infrastructure of a
medical center.
Unfortunately, most Emergency Medicine investigators are not competitive for peer-reviewed federal
funding initially. Certainly young investigators are likely not going to be considered qualified to receive
RO-a awards for investigator-initiated original research without a previous track record of publications
and funding in the area under consideration. Training grants such as K-08 for basic research and K-30
for clinical scientist training can be successfully awarded to talented Emergency Medicine researchers,
particularly when combined with an established, well-funded senior investigator. Repetitive submissions
over several grant cycles, with appropriate responses to criticisms of the grant reviewers, are often
necessary to achieve success even with an outstanding research idea.
Corporate funding of investigator-initiated research ideas is an excellent source of initial grant money for
young Emergency Medicine investigators. Such grants can help to provide the publication record
necessary to demonstrate the research focus and success necessary for subsequent peer-reviewed
federal funding such as from the NIH or the Agency for Health Research Quality (AHRQ). Certain
foundations such as Robert Wood Johnson also can be a source of grant support for research.
Foundations also tend to provide peer review of applications and can be quite competitive. Consistent
funding of a focused research area leading to outstanding peer-reviewed publications remains the goal
of any Department and its faculty investigators.
Departmental Standards for Levels of Funding Establishing levels of funding for Departments or
Divisions of Emergency Medicine may be helpful in identifying successful research programs in our
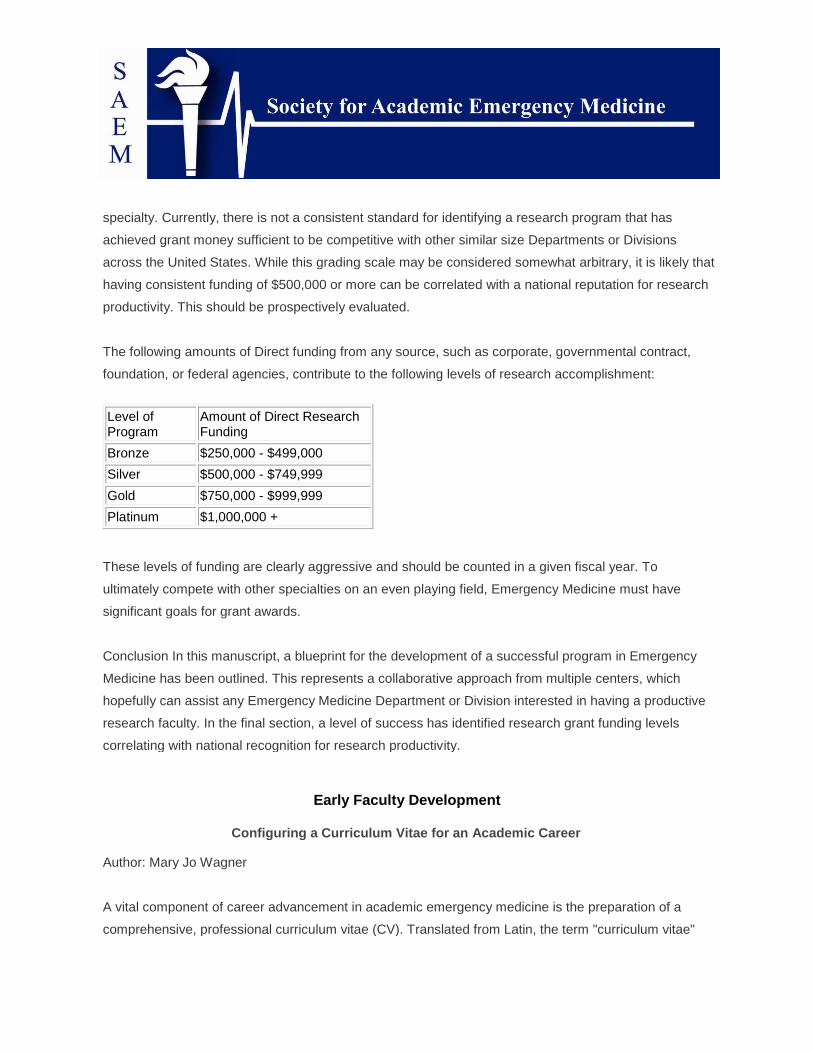
specialty. Currently, there is not a consistent standard for identifying a research program that has
achieved grant money sufficient to be competitive with other similar size Departments or Divisions
across the United States. While this grading scale may be considered somewhat arbitrary, it is likely that
having consistent funding of $500,000 or more can be correlated with a national reputation for research
productivity. This should be prospectively evaluated.
The following amounts of Direct funding from any source, such as corporate, governmental contract,
foundation, or federal agencies, contribute to the following levels of research accomplishment:
Level of Program
Amount of Direct Research Funding
Bronze $250,000 - $499,000
Silver $500,000 - $749,999
Gold $750,000 - $999,999
Platinum $1,000,000 +
These levels of funding are clearly aggressive and should be counted in a given fiscal year. To
ultimately compete with other specialties on an even playing field, Emergency Medicine must have
significant goals for grant awards.
Conclusion In this manuscript, a blueprint for the development of a successful program in Emergency
Medicine has been outlined. This represents a collaborative approach from multiple centers, which
hopefully can assist any Emergency Medicine Department or Division interested in having a productive
research faculty. In the final section, a level of success has identified research grant funding levels
correlating with national recognition for research productivity.
Early Faculty Development
Configuring a Curriculum Vitae for an Academic Career
Author: Mary Jo Wagner
A vital component of career advancement in academic emergency medicine is the preparation of a
comprehensive, professional curriculum vitae (CV). Translated from Latin, the term "curriculum vitae"

means "course of life" and is a detailed chronology of a professional career. It includes a listing of the
physician’s education, clinical, teaching, and research experience, publications and presentations,
awards received and activities in professional organizations. This is in contrast to a resume, which is a
brief overview of qualifications and experiences relative to one’s career objectives. A resume is
generally one or two pages in length and more job specific, focusing on needed skills identified by the
position to which one is applying. A CV is not limited in length, however, and should include detailed
information of the physician’s professional career with an emphasis on the academic components of
research, teaching experience, clinical expertise, and administrative service. Candidates for an
academic position will be asked to submit a CV in place of a job application. In the United States, it is
not uncommon for employers to use the terms CV and resume interchangeably, so one should clarify
the needs of the institution before preparing the document. In Europe, the terminology is reversed – the
resume is generally longer and focuses on one’s academic career and achievements.
A CV can be used to provide a background for prospective employment or promotion, grant applications
or other scholarly activities. Physicians are reticent to sell themselves and this document will provide the
opportunity to demonstrate experience without the need for overt marketing. Developing a CV may also
reinforce the writer’s self-confidence and provide a means for organizing prior experiences in order to
clarify abilities and accomplishments. The CV itself does not have career objectives or goals listed; that
information is included in the accompanying cover letter (see below.
A curriculum vitae is a formal document, and though there is no standard format, a general order and
certain sections are commonly used. (See the guide at the end of this chapter.) Depending upon
institutional convention, Items are often listed in reverse chronological order, i.e., most recent first. The
format must be uniform, with a consistency in the use of bold, italicized, or underlined fonts for section
titles and headings throughout. There should be limited use of abbreviations or acronyms. It is better to
err on the side of convention than to use informal or colloquial titles or expressions.
The first components of a curriculum vitae should be name and title (M.D., D.O.) of the candidate and
contact information. The name should be the one used in formal settings and on professional career
documents. It would be wise to list the legal name with the other basic information for completeness, if
different from the professionally recognized name. Address and contact information should include not
only a telephone number, but a fax number and email, if available. Both home and business addresses
should be included. If prospective employers should not contact the applicant at work nor make any

contact with the current place of employment, this current work information should not be listed here.
Extremely informal or vernacular email addresses might be viewed as unprofessional. Board
certification and state licensure information should conclude the introductory sections.
The next section of a CV typically describes the candidate’s education, also often presented in reverse
chronological order. The location of this section may vary; a more experienced job applicant might
choose to list his or her work experience first, before education, depending on the depth of the
professional experience. A new residency graduate should include college and medical school
graduation information as well as details on residency training. For the recent graduate, it would be
appropriate to mention the undergraduate area of concentration or major, as well as specific
distinctions, such as graduating magna cum laude. If a separate internship year or prior training was
completed in addition to residency, this should also be listed. Any fellowship training or other special
training opportunities of some length should be mentioned here. Professional certifying courses and
other short courses or brief specific training should not be included here. A section for these courses
could be added later in the document. For example, under a section entitled "Certifying Courses,"
"Ultrasound Proficiency Training, beginning and advanced courses (24 hours CME each session)" could
be listed.
Employment usually follows the section on educational background. This information should include the
official job title, institution/corporation name, city, state and inclusive dates of employment. A line may
be added to describe the job if the formal title does not make the responsibilities obvious. It is not
necessary in a CV to indicate the reason for ceasing employment. It is important to include the current
job in this section, including any academic appointment held. If the current employer should not be
contacted until a later stage in the application process, that should be noted here. Finally, individuals
who have received academic appointments from several institutions may decide to make a separate
section, following education, for academic appointments.
Many emergency physicians have practiced at multiple hospital sites, including temporary employment
(moonlighting) during their residency program and early career years. Some professionals have chosen
just to list these hospitals under a section titled "Practice Experience." For example, short-term or part-
time employment would be listed as "ED staff physician: General Hospital, Hamlet, MI 1998; City
Hospital, Village, MI 1997-8; Small-town Hospital, Burgh, MI 1997-8." Full-time career employment
should not be included under this heading, however.

The jobs held during high school and college and odd jobs done for short intervals should not be
mentioned, except for an extraordinary experience. Though an honorable job, bartending part-time
during college, for example, is neither unique nor professionally related and is not necessary to include
in a CV. If one has had limited formal employment, a young professional might put unpaid employment
experiences here, but only long-term, regularly scheduled commitments requiring professional skills
should be used (e.g., volunteer physician at a clinic for indigent patients). Most physicians place these
achievements under "Community and Extracurricular Activities", however. (see below.) As the physician
gains more experience, most non-medical practical experiences should be removed from the CV, unless
they relate directly to one’s career, e.g., computer expertise or basic science research prior to medical
school.
Professional society membership and committee activity section(s) can follow the employment section.
This section can be quite confusing if one belongs to several institutions and medical societies. Care
must be taken to assure an orderly presentation with consistent formatting. Professional organizations
could be listed in order of prestige: international, national, regional or state and local. Some
academicians list the largest organization for their specialty first, then list in decreasing size of
membership. Others may choose to identify first the most career-specific organization (e.g., National
Association for EMS Physicians, for an EMS director applicant); still others begin with the society where
they are most involved. Fellowship designation within a society can be noted in this section as well.
Committee memberships and leadership positions may be listed with the professional societies or under
a separate section, if numerous. Participation on institutional committees, including medical school as
well as hospital committees should also be recorded. Dates of service should be included in all listings.
Honors and awards is another section found routinely on a curriculum vitae. Again, these often listed in
reverse chronological order, ending with distinctive college achievements. Though some creativity may
be used to determine items which may fit in this category, list only merit-based awards and
scholarships. Record the official name of the award, the granting institution and the date presented.
Most of these will need a brief (one sentence) explanation as well, particularly if there are acronyms.
The description can often be derived from the award application, plaque or even letter of
recommendation. For example, "This award was given to the second year resident who best exemplified
compassion to patients and outstanding clinical judgment." Small grants for projects can be placed in
this category as well.

Grants received may be listed separately if there are enough of substantial distinction to merit a
separate heading. Information should include the official title, the granting organization or NIH institute,
the grant number, the principal investigator (and the participant’s role, if not the primary researcher), the
amount, and the date awarded or the timeline for funding, if multi-year. A brief explanation may be
included to clarify the purpose of the grant, although that will usually be self-evident from the title. The
monetary amount awarded should not be a determining factor in including the grant in this section. In
many institutions, it is customary to list only the amount of the award given directly to the investigator,
after the indirect costs (overhead taken by the school or university) have been subtracted. If one is
uncertain, it is entirely appropriate to list both the total and direct monetary value of the award.
For an academic emergency physician’s curriculum vitae, publications and presentations are commonly
listed next. Publications should be written in a standard, accepted format, generally in the style
recommended by the International Committee of Medical Journal Editors and the American Medical
Association.(1,2) This is the same required style found in the National Institute of Health (NIH)
Bibliography Format for its application forms (www.niehs.nih.gov/omhrmb/procedur/bibliog.htm). A
different format is used by some emergency medicine journals. All authors should be listed; some
experts advocate that the CV writer’s name be bolded or underlined. Articles not yet published should
use the phrase "in press" only if they have been accepted by a journal. Articles submitted, but not yet
accepted, may be included but must be listed appropriately (e.g., "submitted"), although in many
institutions, only accepted publications are considered appropriate content for a CV. When there are
sufficient entries, the publication section can be separated by classification. Peer-reviewed articles,
abstracts, book chapters, books, invited reviews, editorials, specialty society publications or opinion
papers, and web-based articles might be some of the categories included here. Letters to the editor, if
listed at all, should be clearly designated separately. Copies of publications should not be submitted
unless specifically requested.
The presentation section should include visiting faculty lectures and other invited speaker opportunities,
as well as abstract presentations. The title of the presentation, the date, and the group addressed
should be indicated. When there are a sufficient number of entries these also should be grouped, with
lectures categorized as international, national, visiting faculty series, regional, local. The list of abstract
and poster presentations should then be included under its own heading. If essentially the same lecture
is given to several different groups, the complete title should be listed once, with the different audiences

and dates noted separately.
It is the custom not to include lectures given locally to one’s own residents and students. By convention,
however, the same lectures given for another residency at the same location, e.g., Internal Medicine
Grand Rounds, are reportable on the CV. The numerous lectures and discussions provided to the local
EM residency need not be ignored, although they are generally more appropriate material for the
teaching portfolio of the clinician-educator (see Chapter on this topic later in this Handbook).
The section "Other Scholarly Activities" may include professional conference planning and development,
or special teaching opportunities (e.g., joint teaching to students in conjunction with a basic scientist).
Consulting engagements could fit in this section, or if the list is lengthy, it may be appropriate to create a
separate one. These items should be related to the medical profession only – the following section is the
one that allows for unrelated, interesting life experiences at institutions where this is deemed
appropriate.
The least regimented section of a curriculum vitae is "Community and Extracurricular Activities." Some
writers leave this information out completely, but many employers look at these activities as an
indication of a well-rounded physician. Chronicling service at a soup kitchen during the holidays would
be a good example of an entry here. Hobbies such as tennis or playing violin in the local orchestra, for
instance, could be included here. It is crucial that this section be written carefully, so as not to include
controversial hobbies or misleading diversions. Better to leave this section out than to appear to be
"padding" one’s CV. Ordinarily, as one develops more traditional academic credentials, this section will
disappear altogether.
Particularly if a curriculum vitae is to be used for a job search, a section on special skills is an important
inclusion. The topics in this section might cover fluency in languages, proficiency in computer
programming or expertise in ultrasonography. If an employer is known to be seeking a faculty member
with specific talents, the incorporation of this skill into a CV may encourage them to look more favorably
at the application.
In general, one’s departmental chair or division chief can advise the junior faculty member on the form
and content of their CV. Many institutions follow a standardized template, which may be required when
submitting a CV to the Promotions and Tenure Committee. It is also worth noting that the configuration

of one’s CV may vary slightly, depending upon the immediate purpose for which it is intended, e.g., a
CV submitted for promotion may look different from a CV submitted to a prospective employer. Similarly,
the CV submitted to accompany a grant application will have yet another focus. All of these issues
require the guidance of a senior faculty member.
Listing references has been discouraged in a professional curriculum vitae. One may leave this section
out completely under the assumption that references will be provided upon request. However, having a
ready list of references with whom future plans have been discussed is important. When references are
requested, they should be provided immediately.
Since the topics for inclusion in a curriculum vitae are not defined, many physicians add sections which
might highlight special talents or opportunities. An emergency physician with extensive experience in
outdoor patient care might have a section of "Wilderness Medical Care Experiences". A physician with a
strong background in education might entitle a section "Mentoring Activities," if the list of academic
advisory activities was indeed a considerable one. The CV should not be padded, but creative
presentation of unique abilities shows initiative to employers as well as highlighting special talents for
which they might be looking. However, because the appearance of "padding" can provide such a
strongly adverse impression, particularly to experienced reviewers, a good rule of thumb in CV
construction is: "When in doubt, leave it out."
Though each document will be individualized, some general techniques for writing a CV should be
followed. The title "Curriculum Vitae" or "CV" should not be written at the top. The nature of the
document should be obvious at first glance and it is more important to have the applicant’s name
prominently displayed and easily read. The applicant’s name should also be placed as a header on
each page, which should be numbered. Specific personal identifying numbers, such as a social security
number or medical license numbers should not be included for security reasons. (Listing the states in
which one is licensed, without giving the specific number, is adequate.) Although date of birth is
optional, one should avoid mentioning any social or personal items, such as ethnicity, religion. A current
photo should not be included unless specifically requested. Such items could be viewed with
discrimination and leaving them off a CV will eliminate any misunderstanding. Disabilities likewise
should be listed only if this would make the application stronger for a specific job. Including marital
status and the number or names of children can leave room for bias, specifically for women. However,
as with date of birth, there is a conflicting opinion about this. Some professionals document this

personal information if they feel it is important to represent their feelings about their family.
Conforming to traditional grammar and style is recommended for this formal document. Slang or jargon
should be avoided. Incorrect spelling or syntax is still possible with the computer "spell-check"
programs, so care should be taken to have the CV proofread several times before submitting it. The
visual layout of the CV is very important, as good first impressions clearly increase opportunities. Easily
read font style (e.g., Times New Roman) and size (12 point) create a more professional document. The
spacing of the items should be consistent, with double spacing between major topics to improve
readability. The document should have generous margins on all four sides of the page and be typed
only on a single side of the paper. There should be clear, distinct section breaks and headings. A CV
that is difficult to read will be more quickly laid aside.
Though using colored heavy stock paper has been recommended in other occupations, white
middleweight stock is most appropriate in academic medicine. Many employers are requesting material
to be faxed or copied and the coarse ivory or gray is more likely to cause difficulty with this technology.
More critical is the use of a laser printer with a new ink cartridge to avoid fading letters and difficult-to-
read type. Sending poor quality photocopies of a CV gives the impression that a mass mailing of these
items has been sent indiscriminately to many potential employers. It is not necessary to use binders,
folders, or cover pages on the curriculum vitae. These can be viewed as pretentious or just bothersome
and are not traditionally used in the medical field. Use of paper with a border or decorative pattern
detracts from the important information on the CV and should be avoided.
Writing a curriculum vitae requires a comprehensive list of all of the subject’s accomplishments. It is
very difficult to remember all the academic and professional activities in which one is involved if some
type of system is not already in place. Use of the Educator’s portfolio, discussed at length elsewhere in
this Handbook,, makes compiling this information much simpler. Once a CV is written, it is easier to
make ongoing changes than to try to update the document only on an occasional basis. The CV should
be updated immediately, for example, to include a paper accepted for publication, an abstract chosen
for presentation, or the selection of one to participate in a specialty society committee.
If the curriculum vitae is used for a job search, a cover letter should accompany this document. This
letter should be created individually for each institution to which one is applying, with specific mention of
local needs or interests. It is here that the applicant should express his or her individuality and unique

talents for a specific job. Obtaining background information about a particular opportunity can guide the
tone and emphasis of the cover letter. As this will be sent with the curriculum vitae, the focus of the
letter should be to highlight job-related accomplishments and skills. It would be appropriate to include
short term and long term goals here, if they match the needs of the organization. Some specific
personal details may also be suitable for this letter; for example, indicating family ties to a specific
geographical region or interest in residing in a particular community. Areas to emphasize in a cover
letter for an academic position in emergency medicine might include academic experiences,
administrative expertise, and research accomplishments. While the letter is a formal document, the style
can be more personal and relaxed. It should be printed on the same type of paper as the curriculum
vitae if possible. The cover letter should summarize, emphasize and personalize successes, not
reiterate items listed on the CV.
A well-organized and clearly written curriculum vitae provides a favorable first impression upon a
reviewer. Whether this document is used for employment, promotion or a grant application, a thoughtful,
carefully crafted CV can increase opportunities for its writer.
References
1. International Committee of Medical Journal Editors. Uniform requirements for manuscripts submitted
to biomedical journals. Can Med Assn J 1994;150:147-154.
2. American Medical Association. Manual of Style, 9th ed. Baltimore: Williams & Wilkins, 1998.
Further Readings
1. Logan PM and Fraser DB: Constructing a Curriculum Vitae: The radiologist’s resume. AJR 1998;171:
923-925.
2. Yenney SL. The Physician’s Resume and Cover Letter Workbook. Chicago: The American Medical
Association, 1998.
3. http://www.coloradocollege.edu/beta/publications/curriculumvitae/default.htm
Section Guide for Physician Curriculum Vitae

Name and Title
Address and Contact Information
Certification and Licensure
Education
Academic Appointments
Employment
Practice Experience
Professional Society Membership
Committee Activity
Honors and Awards
Grants
Publications
Presentations
Other Scholarly Activities
Certifying Courses
Community and Extracurricular Activities

Special Skills

Understanding the Promotion and Tenure Committee
Author: Edward A. Panacek
The process of promotion and awarding of tenure can appear daunting and mysterious, particularly to
junior faculty. Although the process varies widely among institutions, there are themes that are relatively
universal. Understanding the procedure at your own institution is critical to assuring your success as an
academic faculty member.
Faculty job descriptions and "tracks" can vary substantially among institutions. However, virtually all
institutions have an "academic" faculty series that has a formal promotion process, with or without the
awarding of tenure. This includes a formal period of review for junior faculty, which generally takes place
during the time as an "assistant professor", before being promoted to "associate professor". This period
of review usually lasts for a maximum of eight years. Because the faculty packet for consideration for
promotion is routinely assembled a full year before this period ends, the faculty member’s qualifications
for promotion are actually based on a maximum of seven years of faculty productivity. Even when
faculty have been "decelerated", most institutions have absolute rules governing the maximum period of
time that faculty can serve as an assistant professor in an academic series. At some institutions, the
same rules do not apply to faculty that are in a "clinical" series that does not have a publication or
research requirement.
Assessment Criteria
The process of formal review of a faculty member for promotion, or for the awarding of tenure, includes
activities in four specific categories at most universities. These are clinical competence, teaching,
service activities (both university and public) and research or creative work. Faculty in clinical series that
do not have a publication requirement, are generally judged by assigning greater weight to each of the
first three categories.
Professional competence is generally required for faculty in schools of medicine. This includes
demonstration of distinction in the special competencies appropriate to one’s field. In medicine, this
should include both qualitative and quantitative measures of clinical performance. The quantitative
aspects include billing summaries, RVUs generated, number of clinical shifts or clinical hours, etc. The
qualitative aspects are more difficult to measure, but usually focus on intramural peer review. Credit can
be given for organization of unique or new clinical services. Some institutions use the process of board

certification as one way of assessing clinical competence and most include it as a requirement for
promotion. Recognition or certification by appropriate national professional groups is also often used in
this assessment.
Teaching activities are theoretically highly valued when assessing a faculty member for promotion.
Quantifying the amount of teaching of students, residents, and peers tends to be the focus, since it is
more easily measured. Peer review or evaluations are used to assess the quality of the teaching,
although it is understood that this process is somewhat imperfect. The reality is that while it is easy to
identify faculty who win teaching awards, it is more difficult to identify the mediocre teachers from those
who are solid, above average, teachers. As a result, the quantitative evaluations tend to take
precedence over the qualitative in this category.
Although faculty "service" activities are generally included in packets for consideration for promotion,
they tend to be the least emphasized area. Faculty are expected to function as good citizens and to
shoulder their fair share of the administrative workload. This should be reflected in their list of service
activities recorded in their CV. This includes committees, task forces, and administrative positions held
within the division, department, school, hospital, or university. Peer reviews from colleagues within the
same department are also given some weight in assessing performance in this category. In general,
junior faculty at the assistant professor level are not expected to be given major administrative service
responsibilities.
Other academic activities can include both original research and other evidence of creative work.
Among faculty in the traditional or unmodified academic series the committee is looking for evidence of
a productive and creative mind that is making substantive contributions to the knowledge base of that
individual’s field. Although it is stated that publications, research and other creative accomplishment
should be evaluated on their individual merit and not merely enumerated, this is easier said than done.
Although no absolute numbers are provided regarding the number of publications required for
promotion, there are at least "unofficial" guidelines at many institutions that can be obtained by speaking
with one’s chair or more senior faculty. Although it is always stated that quality should take precedent
over quantity, the reality is that quantity is most easily measured Individuals serving on promotion and
tenure committees are very busy individuals, and it is easier for them to count than to read each article.
The committee is looking for evidence that the faculty candidate in the traditional track is continuously
and effectively engaged in creative activity of quality and significance.. Most institutions now require that

the faculty member, or their department chair, establish as clearly as possible the role of the faculty
candidate in their research efforts. This is particularly important for individuals actively collaborating in
joint efforts with other faculty within their division or department. It is expected that the appropriate
candidate for promotion (and tenure) in the traditional track has demonstrated an ability to function
effectively as an independent researcher. As evidence of this, the faculty applicant is expected to be first
author, or sometimes the last "senior" author, on a significant number of quality publications. Serving as
a "sandwich author" in the middle of the pack on all of the publications, can be problematic. At most
institutions, textbook chapters, review articles, case reports, and other publications that do not involve
original research are considered evidence of scholarly activity, but are not weighted as heavily toward
promotion in the traditional (non-clinical) track. Most institutions consider such publications to be of
greater importance in the clinical track, where teaching ability is weighted heavily.
The successful pursuit of extramural grant funding for research is particularly important for faculty in the
traditional track, and is considered the gold standard in assessing candidates for promotion in any
series that has a strict research requirement. Most tenure track positions fall into this category. Having
NIH grants such as an R01 is evidence of recognition within the field. Extramural appraisals are also
often carefully considered in assessing this area of candidate performance.
Changes in Faculty Series
A change in faculty series or track is an option at many institutions. Such changes are almost always out
of the traditional series with a research requirement and an emphasis on the scholarship of discovery or
application into a clinical series with an emphasis on the scholarship of teaching.
The Review Period
Each review of faculty performance, whether it is for appraisal, merit advancement, promotion, or tenure
includes a formal "review" period. This can be short as 2-3 years for a "merit advancement" at some
institutions. It generally includes a 6-7 year period to advance from assistant professor to associate
professor. Further promotions to full professor often include similar timeframes. Preparation of the
candidate promotion packet is obviously dependent upon the formal review period being considered.
Division heads or department chairs usually have information regarding the relevant period of review.

Extramural Letters
Most universities, at the time of promotion from assistant to associate or from associate to full professor,
solicit extramural letters to assist them in appraising the candidate’s performance. These letters are
solicited from specific individuals chosen from a list of candidates. The department chair may select the
list of extramural reviewers, usually with input from the faculty candidate, or the candidate may submit a
list directly to the P&T Committee. Extramural letters should only be solicited from individuals who are
highly respected in the field, and are already at a faculty appointment level that exceeds that proposed
for the candidate. The reviewer’s academic title, specific expertise, and other credentials should be
clear. These individuals are particularly important in assessing national society service activities and
providing perspectives on the candidate’s scholarly activities.
The Procedure of Promotion and Tenure
The process of identifying faculty candidates for promotion and starting the actual procedure itself
generally begins with a "call for personnel action" from the chair or appropriate review body within the
university. Those faculty who are scheduled to be candidates for consideration for promotion during the
next academic year are identified. The department then puts together the packet with early and close
involvement of the faculty candidate . The candidate should meet with the departmental chair to discuss
the packet and the process as well as identification of potential extramural reviewers.. Most institutions
have a checklist to assist in this process, and some encourage candidates to include their own brief
statement summarizing their activities in each of the four main areas of academics, teaching, clinical
care, and service. It should not repeat what is already obvious in other university files or lists of
publications. Rather, it is designed to give candidates an opportunity to discuss the unique aspects or
special significance of their scholarly career accomplishments that would not be otherwise evident. The
very extensive process of gathering materials documenting scholarly teaching activities (Educator’s
Portfolio, see Chapter 2.8.2.), service activities, clinical productivity, and research activity then begins.
Although the department assists with this process, the vast bulk of the responsibility falls on the faculty
candidate.
After the draft packet has been assembled, the department chair generally provides a cover letter of
recommendation that summarizes the candidate’s qualifications. At some institutions, the candidate can
add a second letter, particularly if they disagree with some of the assessments by the department chair,

although one should be cautious about openly airing disagreements with one’s chair, since this is
typically viewed negatively by P&T Committees. At many institutions, this then goes out to peer vote
within their own faculty group, e.g., those within the same department. At some institutions, only faulty
members with appointments at an equal or higher level are qualified to vote on the candidate’s
qualifications. In other departments, only a special committee appointed by the chair decides on who will
be put up for promotion in a given year. If a vote is held, the results of that vote, and any specific peer
comments, are then summarized in a letter that is generally forwarded to the dean’s office. Ordinarily for
a promotional packet to get to the P&T Committee, it must first pass muster within that individual’s home
department. Virtually all schools have a P&T Committee that is advisory to the dean that does further
detailed assessment of the candidate’s qualifications. This committee generally has broad
representation across all specialties. Unlike the department chair, who is generally the candidate’s
advocate, the P&T committee is designed to be less biased, and may only allow members of other
departments to vote on a given individual’s promotion The P&T committee then makes
recommendations to the dean. The dean typically has authority to make the final decisions regarding
some or most of the actions. At other institutions, there is a larger university committee on promotion
and tenure that is advisory to the chancellor or provost of the university who makes the final decisions.
The amount of feedback information given to the candidate during the process varies greatly among
institutions. At some, the candidate is informed regarding each step from the departmental vote through
the school and university committee recommendations. At other institutions, only the final decision is
communicated. If the candidate disagrees with the decision, all institutions have an appeal process
available. However, such appeals should be carefully considered after discussion with senior faculty,
associate deans, etc. Often, the chair is expected to appear before the committee on behalf of the
candidate to appeal an adverse decision.
Promoting Yourself
Although the process of consideration for promotion and tenure is usually straightforward, problems can
occur. Although the chair’s support is essential, the candidate should not depend upon the department
chair to be their sole source of advocacy. It is the faculty candidate’s own responsibility to appropriately
promote themselves and to ensure that their qualifications are viewed in the best possible light. There
are a number of ways in which faculty can effectively promote themselves:

1. Be punctual and on time with the process. Universities tend to have very strict deadlines for
submission of materials and are intolerant of substantial delays. Get a copy of the schedule and get
your materials in on time.
2. Track the process. The evaluation process can take up to an entire year. It is easy to lose track. Write
yourself reminders and keep a summary of the status of your file at every step. If a problem develops,
you want to know about it immediately, not just at the time of the final decision.
3. Keep extensive records documenting your activities. While your CV usually captures all of your
publications, most of us are not as compulsive about recording all of our teaching and service activities.
For those whose scholarship is centered about teaching, an Educator’s Portfolio is essential (see
Chapter 2.8.2. Set up a file for each to make it easier to track these. Especially for promotion from
assistant to associate professor, it is easy to lose track of activities that occurred three or more years
prior.
4. Write your support letter. At some institutions, this is required, at others it is only optional. Even if you
believe your chairman is a strong advocate for your promotion, there is great value in writing your own
support letter. At the very least, this will serve as a guide for the chair support letter and a reminder to
include items that otherwise might be overlooked
5. Solicit support and evaluation materials. When available, there is value in actively soliciting teaching
evaluations from within the medical school and residency, as well as from national organizations and
other extramural sites. This is particularly true if one has concerns about the quality of teaching
evaluations you have received at your home institution or if your department has not done an effective
job of collating those materials for you.
6. Carefully consider the candidates for your extramural letters. These should be individuals who are
very familiar with your work and are very supportive of you as an individual. If in doubt, there is no harm
in placing a phone call and specifically asking if you can list them as one of the extramural reviewers.
Ask whether they would be willing to write a strong letter of support. Even if you feel that you do not
know the individual very well, you would be surprised at how receptive most prominent faculty are to
such phone calls. If you are unsure whom to list as candidates, consider individuals who have served as
moderators for abstract sessions at which you have presented or associated editors who have handled

manuscripts you have submitted.
7. Ask to review the chair’s support letter before it is finalized. Some chairs are relatively inexperienced
at writing strong support letters; others are simply too busy. Do not take it for granted that your chair will
write a highly supportive and comprehensive letter. Ask to review it yourself and do not be hesitate to
make suggested changes. Many chairs ask the candidates to write a draft support letter themselves. If
given this opportunity, take it.
8. Consider an appeal of any negative decision. If you truly believe you have objective data
demonstrating that you have comparable qualifications to other faculty who have successfully received
promotion or tenure, consider an appeal. Make this decision relatively quickly. The window of
opportunity for an appeal can be relatively short. If you appeal, follow the rules and steps exactly and
track the process very closely. Often it will be the responsibility of the chair to make an appeal to the
committee for reconsideration of a faculty candidate.
9. Know the rules. Even if you are not planning an appeal, you should read your university regulations
regarding the process of promotion and tenure. Do not assume that your department administrator or
chair are highly familiar with these rules. A copy should be on file in your administrator’s office. Read
them while you are starting the process and highlight any elements that you think might particularly
apply to your case. Even if you never need to intervene in the process, you will rest better if you are
familiar with the rules yourself.
The good news is that the system generally works very well and most faculty candidates are
successfully promoted to the next level.

National Perspectives on Promotion and Tenure
Author: Sean O. Henderson
One of the initial steps in career development should be a review of a prospective institution’s policies
and procedures with respect to promotion and the attainment of tenure. An applicant needs to be aware
of the expectations of the department and the school to decide which track (e.g. Clinical, Research,
Tenure) 1) best suits their skill set and 2) will allow the best chance of success. Important issues that
need to be addressed are: the time allotted to complete required tasks, the track record of the
department in advancing individuals on the track that you are being hired into, as well as any other
support available to the newly hired faculty member (faculty development courses, collaborative
partners, mentors, etc.) Given that in many cases, promotion to a higher faculty rank is also
accompanied by an increase in salary, it is important to know what you are getting into on the front end
rather than 4 or 5 years into one’s academic career.
The word "tenure" is defined in the Cambridge Dictionary as "the period of time when someone holds a
job, esp. an official position, or the right to keep a job permanently." Within the setting of academia,
tenure should provide freedom of teaching, research and extramural activities and a sufficient degree of
economic security. This freedom and economic security are indispensable to the success of an
institution in fulfilling its obligations to its students and to society. As there is a cost to the institution of
such a financial obligation, appointment to, and promotion on the tenure track often carries with it a
responsibility to develop alternative funding sources and to excel in research activities, difficult tasks for
those clinical departments that stress patient-care duties.
One way to get a feel for how promotion policies vary from institution to institution is to visit the websites
of prospective employers. Posted under the "Administration" heading at most of these websites will be a
section dealing with Faculty Appointments and Promotion. Some of these sections are deliberately
vague, allowing input from the chairman and the Promotion and Tenure Committee to carry the majority
of the weight, while others are very specific, down to the number of lectures one has to give and the
number of papers written per year. In some cases, there are no options and all the faculty in the
Emergency Department are placed into the Clinical track where attainment of tenure may not be an
option.
Using the CRISP NIH database, a representative sample of the Medical Schools in the country was

taken (top 25%, middle 50%; bottom 25%) and their websites reviewed for Promotion and Tenure
policies. Excerpts from four such sites are listed below with an emphasis on the Clinical
Scholar/Clinician Teacher requirements.
SCHOOL #1
Criteria for Appointment and Advancement
Candidates in the regular Professor series and the Professor in Residence series are evaluated on:
1. Teaching
2. Research and Creative work
3. Professional competence and activity
4. University and public service
For a descriptive statement of each of these criteria see Academic Personnel Manual (APM) Section
210-1 B Instructions to Review Committees*. For discussion of teaching and research responsibilities
see those sections of this Handbook.
Evaluation of Teaching
Teaching is an essential criterion to appointment or advancement; tenure is granted only with clear
documentation of ability and diligence in the teaching role.
Department chairs are charged with gathering evidence of a candidate’s teaching ability at all levels of
instruction, from lower division to graduate courses and dissertation supervision. Such evidence may
include opinions of other members of the department, students, and alumni; the number and quality of
students guided in research or attracted to the campus by the individual’s reputation; and development
of new and effective techniques of instruction.

Departments prepare academic review records for all faculty members under consideration for merit
increases and promotion. The kinds of information on teaching normally included in the academic
review records and students’ evaluations of the faculty member’s teaching, solicited letters from former
students, descriptions of new courses prepared, and lists of Ph.D. qualifying committees chaired and
dissertations supervised.
Promotions: Promotions are based on merit; they are not automatic. Achievement, as it is
demonstrated, should be rewarded by promotion. Promotions to tenure positions should be based on
consideration of comparable work in the candidate’s own field or in closely related fields. The
department and the review committee should consider how the candidate stands in relation to other
people in the field outside the University who might be considered alternative candidates for the
position.
The department chair shall supplement the opinions of colleagues within the department by letters from
distinguished extramural informants. The identity of such letter writers should not be provided in the
departmental letter except by code.
Assessment of Evidence: The review committee shall assess the adequacy of the evidence submitted. If
in the committee’s judgment the evidence is insufficient to enable it to reach a clear recommendation,
the committee chair, through the Chancellor, shall request amplification. In every case all obtainable
evidence shall be carefully considered.
If in assessing all obtainable evidence, the candidate fails to meet the criteria set forth in Section 210-1-
d below, the committee should recommend accordingly. If, on the other hand, there is evidence of
unusual achievement and exceptional promise of continued growth, the committee should not hesitate
to endorse a recommendation for accelerated advancement.
The review committee shall judge the candidate with respect to the proposed rank and duties,
considering the record of the candidate’s performance in (1) teaching, (2) research and other creative
work, (3) professional activity, and (4) University and public service. Mentoring and advising of students
or new faculty members are to be encouraged and given recognition in the teaching or service
categories of:

1. Teaching: Clearly demonstrated evidence of high quality in teaching is an esse4ntial
criterion for appointment, advancement, or promotion.
2. Research and Creative Work: Evidence of a productive and creative mind should be
sought in the candidate’s published research or recognized artistic production in original
architectural or engineering designs, or the like.
3. Professional Competence and Activity: In certain positions in the professional schools
and colleges, such as architecture, business administration, dentistry, engineering, law,
medicine, etc., a demonstrated distinction in the special competencies appropriate to
the field and its characteristic activities should be recognized as a criterion for
appointment or promotion. The candidate’s professional activities should be scrutinized
for evidence of achievement and leadership in the field and of demonstrated
progressiveness in the development or utilization of new approaches and techniques for
the solution of professional problems. It is the responsibility of the department chair to
provide evidence that the position in question is of the type described above and that
the candidate is qualified to fill it.
4. University and Public Service: The faculty plays an important role in the administration
of the University and in the formulation of its policies. Recognition should therefore be
given to scholars who prove themselves to be able administrators and who participate
effectively and imaginatively in faculty government and the formulation of departmental,
college, and University policies. Services by members of the faculty to the community,
State, and nation, both in their special capacities as scholars and in areas beyond those
special capacities when the work done is at a sufficiently high level and of sufficiently
high quality, should likewise be recognized as evidence for promotion. Faculty service
activities related to the improvement of elementary and secondary education represent
one example of this kind of service. Similarly, contributions to student welfare through
service on student-faculty committees and as advisers to student organizations should
be recognized as evidence.
Professor of "Clinical" Series
Teaching: Excellent teaching is an essential criterion for appointment or advancement. Clinical teaching
is intensive tutorial instruction, carried on amid the demands of patient care and usually characterized

by pressure on the teacher to cope with unpredictably varied problems by patient-centered immediacy
of the subject matter, and by the necessity of preparing the student to take action as a result of the
interchange.
Professional Competence and Activity: There must be appropriate recognition and evaluation of
professional activity. Exemplary professional practice, organization of training programs for health
professionals, and supervision of health care facilities and operations comprise a substantial proportion
of the academic effort of many health sciences faculty. In decisions on academic advancement, these
are essential contributions to the mission of the University and students and former students in
academic positions or clinical practice.
Creative work: Many faculty in the health sciences devote a great proportion of their time to the
inseparable activities of teaching and clinical service and, therefore, have less time for formal creative
work than most other scholars in the University. Some clinical faculty devotes this limited time to
academic research activities; others utilize their clinical experience as the basis of their creative work.
An appointee is expected to participate in investigation in basic, applied, or clinical sciences. In order to
be appointed or promoted to the Associate or full Professor rank, an appointee shall have made a
significant contribution to knowledge and/or practice in the field. The appointee’s creative work shall
have been disseminated, for example, in body of publications, in teaching materials used in other
institutions, or in improvements or innovations in professional practice which have been adopted
elsewhere.
Evidence of achievement in this area may include clinical case reports. Clinical observations are an
important contribution to the advancement of knowledge in the health sciences and should be judged by
their accuracy, scholarship, and utility. Improvements in the practice of health care result from the
development and evaluation of techniques and procedures by clinical investigators. In addition, creative
achievement may be demonstrated by the development of innovative programs in health care itself or in
transmitting knowledge associated with new fields or other professions.
Textbooks and similar publications, or contributions by candidates to the professional literature and the
advancement or professional practice or of professional education, should be judged as creative work
when they represent new ideas or incorporate scholarly research. The development of new or better
ways of teaching the basic knowledge and skills required by students in the health sciences may be
considered evidence of creative work.
SCHOOL #2
CLINICIAN TEACHER CRITERIA
Assistant Professor
Teaching
Recognition by peers and students as being among the best teachers of medical students, residents,
fellows, or continuing medical education attendees.
Clinical Service/Scholarship
Evidence of a high level of competence in a clinical area. Use of innovative approaches, technologies,
instrumentation, or systems of patient care in a clinical discipline. Active participation in local, regional,
or national professional clinical organizations.
Publication of clinical observations, analytic studies, reviews, chapters, clinical manuals or treatment
guidelines that organize, synthesize, and convey existing knowledge in a way that enhances the
practice of medicine. Publications should describe state-of-the-art clinical practice, may disseminate
clinical knowledge, techniques, and technologies through syllabi, video and audio learning aids,
computer-based material, or professional communications.
ASSOCIATE PROFESSOR
Teaching
Continuing outstanding contributions to the teaching of medical students, residents, specialty fellows, or
postgraduate students. Recognition of high-quality teaching should be available from formal peer
evaluations, student evaluations, or teaching awards. Impact and value of teaching should be
recognized beyond the local level, as demonstrated by invitations to teach in other hospitals, other
medical schools, programs of professional societies, or continuing medical education courses.

Demonstration of scholarship through continuing development and dissemination of teaching materials,
including new curricular offerings, educational programs, textbooks, syllabi, computer programs, or
videotapes that make a unique contribution to the quality and method of teaching within and outside the
local community.
Clinical Service/Scholarship
Development of a regional or national reputation as an authority in a clinical field as demonstrated by
patient referrals, invited visiting lectureships, and elected membership in professional societies.
Introduction and evaluation of innovative approaches and/or development of standards for patient care.
May play an important role in clinical trials/clinical investigation. An effective role model and mentor for
students, residents, fellows and colleagues.
Demonstration of clinical scholarship through continuing publication of analytic studies, reviews, and
chapters, as well as clinical observations that are recognized as authoritative and that influence the
practice of medicine. May serve as editor of textbook and/or journal. May have continuing dissemination
of clinical expertise by audio and video learning aids and through computer-based material, and/or
evidence of stimulating trainees and colleagues to prepare clinical papers and reviews.
Leadership role in department or hospital, such as section or clinical division head, or medical staff
representative, and/or member of regional national professional organizations.
PROFESSOR
Teaching
Recognition for being an exceptional teacher of medical students, residents, specialty fellows or
continuing medical education participants. Impact of superb teaching should be apparent nationally and
internationally as demonstrated by invitations to serve as visiting professor, named lecturer, or to teach

in specialty societies and national continuing medical education courses.
Impact may also be recognized by success/stature of trainees. Demonstration of outstanding
scholarship by development and dissemination of original teaching materials, such as widely used
textbooks, new curricular offerings, educational programs, syllabi, video materials, or computer
programs.
Clinical Service/Scholarship
National/International reputation for excellence in clinical practice, and as an authority in a clinical field.
Significant leadership role in provision of clinical care in department/hospital/healthcare system.
Development/introduction/evaluation of new approaches to patient care. May have ongoing leadership
role in clinical trails/clinical investigation. Demonstration of scholarship by publication of analytic clinical
studies, clinical observations, comprehensive clinical reviews, or textbooks and chapters that are
recognized as exerting major influence on practice of medicine nationally. May participate in
development of national standards for patient care. May serve as editor of highly regarded and
influential textbooks or journals. May disseminate clinical expertise by audio/video learning aids, and
through computer-based material.
Evidence of being an effective role model and mentor for medical students, trainees, and colleagues.
Demonstration of leadership through active participation in prestigious professional societies, through
other academic recognition or awards, and through playing an important role in department or hospital.
SCHOOL #3
The Department of Emergency Medicine recommends titles of appointment and promotion in two
distinct designations: Assistant Professor, Associate Professor and Professor of Emergency Medicine;
and the modified designation of Assistant Clinical Professor, Associate Clinical Professor and Clinical
Professor of Emergency Medicine. Affiliated Hospital faculty are also eligible for appointment and
promotion. Candidates will be evaluated for academic advancement based on their contributions to
Emergency Medicine in the following areas: clinical service, education, scholarship, administration and
community service. The Instructor designation is reserved for Fellows and Junior Faculty who are
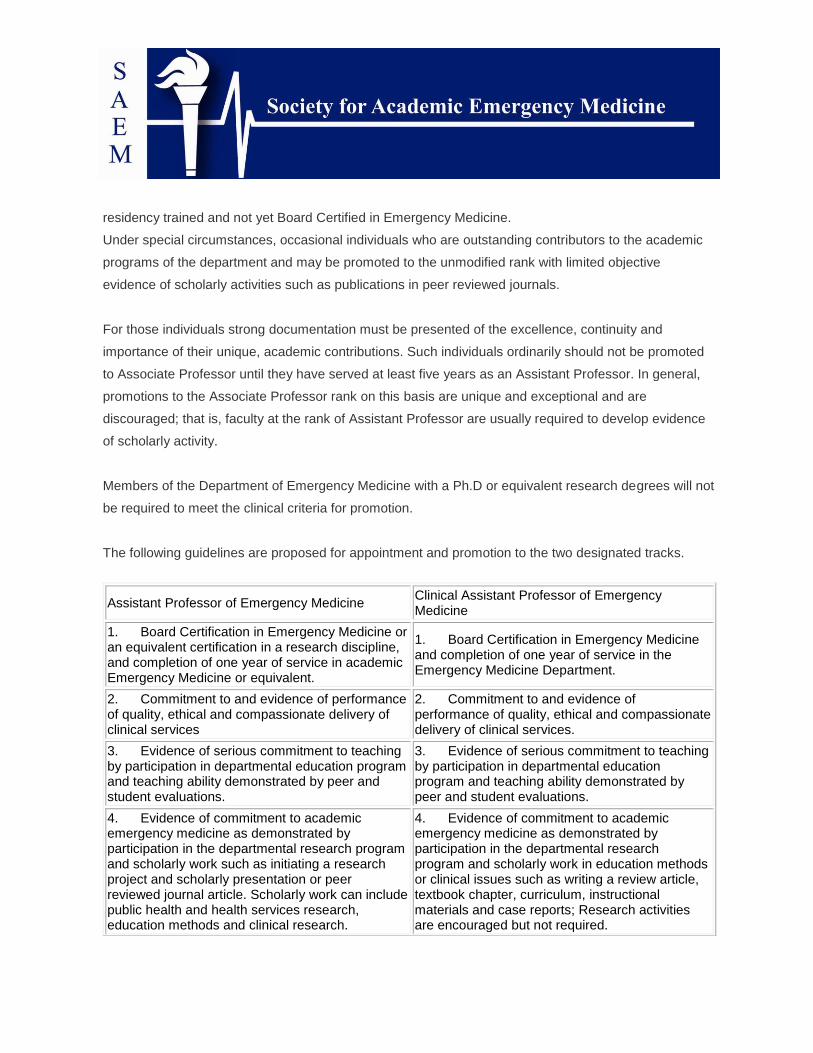
residency trained and not yet Board Certified in Emergency Medicine.
Under special circumstances, occasional individuals who are outstanding contributors to the academic
programs of the department and may be promoted to the unmodified rank with limited objective
evidence of scholarly activities such as publications in peer reviewed journals.
For those individuals strong documentation must be presented of the excellence, continuity and
importance of their unique, academic contributions. Such individuals ordinarily should not be promoted
to Associate Professor until they have served at least five years as an Assistant Professor. In general,
promotions to the Associate Professor rank on this basis are unique and exceptional and are
discouraged; that is, faculty at the rank of Assistant Professor are usually required to develop evidence
of scholarly activity.
Members of the Department of Emergency Medicine with a Ph.D or equivalent research degrees will not
be required to meet the clinical criteria for promotion.
The following guidelines are proposed for appointment and promotion to the two designated tracks.
Assistant Professor of Emergency Medicine Clinical Assistant Professor of Emergency Medicine
1. Board Certification in Emergency Medicine or an equivalent certification in a research discipline, and completion of one year of service in academic Emergency Medicine or equivalent.
1. Board Certification in Emergency Medicine and completion of one year of service in the Emergency Medicine Department.
2. Commitment to and evidence of performance of quality, ethical and compassionate delivery of clinical services
2. Commitment to and evidence of performance of quality, ethical and compassionate delivery of clinical services.
3. Evidence of serious commitment to teaching by participation in departmental education program and teaching ability demonstrated by peer and student evaluations.
3. Evidence of serious commitment to teaching by participation in departmental education program and teaching ability demonstrated by peer and student evaluations.
4. Evidence of commitment to academic emergency medicine as demonstrated by participation in the departmental research program and scholarly work such as initiating a research project and scholarly presentation or peer reviewed journal article. Scholarly work can include public health and health services research, education methods and clinical research.
4. Evidence of commitment to academic emergency medicine as demonstrated by participation in the departmental research program and scholarly work in education methods or clinical issues such as writing a review article, textbook chapter, curriculum, instructional materials and case reports; Research activities are encouraged but not required.

5. Performance of administrative functions within the department, hospital, medical school or involvement in community service project.
5. Performance of administrative functions within the department, hospital, medical school, or involvement in community service.
Associate Professor of Emergency Medicine Clinical Associate Professor of Emergency Medicine
1. A minimum of five years at the rank of Assistant Professor.
1. A minimum of five years at the rank of Assistant Professor.
2. Evidence of excellence in performance and ethical and compassionate delivery of clinical services, documented by evaluations by peers, residents and other providers, and by the findings on department CQI program.
2. Evidence of excellence in performance and ethical and compassionate delivery of clinical services, documented by evaluations by peers, residents and other providers, and the findings on departmental CQI program.
3. Evidence of assuming teaching or mentor-ship responsibilities in the departmental and medical school programs, through 1) activities such as lecturing, bedside teaching, development of curriculum or new teaching methods, videotape, textbook chapters, and 2) teaching excellence on evaluation by students and peers.
3. Evidence of assuming major administrative, teaching or mentorship responsibilities in the departmental and medical school teaching programs, by 1) demonstrating leadership in lecturing bedside teaching, curriculum development, teaching methods, videotape, textbook chapters; and 2) teaching excellence on evaluations by students and peers.
4. Evidence of continued scholarly activity and independence as an investigator demonstrated by a series of at least ten publications, half in peer reviewed journals including several original research articles in which the candidate is first author or a principal collaborator in the creation of the hypotheses, design, and analysis of study.
4. Active participation in departmental research program and five scholarly works in education or clinical issues such as a review article and case reports in peer reviewed journal, chapters in textbooks or published educational methods, videotapes or electronic media.
5. Performance of administrative functions within the department, the hospital, the medical school or community service project or providing leadership and developing novel methods in the performance of administrative functions within the department, the hospital, the medical school or community service project.
5. Performance of administrative functions within the department, the hospital, the medical school or community service project or providing leadership and developing novel methods in the performance of administrative functions within the department, the hospital, the medical school or community service project.
6. Evidence of peer recognition at the regional or national level for scholarly activities as judged by at least three external letters of reference.
6. Evidence of peer recognition at the regional or national level for education or administrative service as judged by at least three external letters of reference.

Professor of Emergency Medicine Clinical Professor of Emergency Medicine
1. A minimum of five years at the rank of associate level.
1. A minimum of five years at the rank of associate level.
2. Continued evidence of excellence in performance and ethical and compassionate delivery of clinical services, documented by evaluations by peers, residents and other providers and by the findings on department CQI program.
2. Continued evidence of excellence in performance and ethical and compassionate delivery of clinical services, documented by evaluations by peers, residents and other providers, and the findings on department CQI programs.
3. Continued evidence of assuming teaching or mentorship responsibilities in the department and medical school programs, through 1) activities such as lecturing bedside teaching development of curriculum or new teaching methods, videotape, textbook chapters and 2) teaching excellence on evaluation by students and peers.
3. Continued evidence of assuming major responsibilities for education administration, teaching or mentorship in the departmental and medical school teaching programs, by 1) demonstrating leadership in lecturing, bedside teaching, curriculum development, teaching methods, video textbook chapters; and 2) teaching excellence on evaluation by students and peers.
4. Evidence of continued scholarly activity as an independent research investigator demonstrated by publishing a series of at least twenty papers, half in peer reviewed journals including five original research articles in which the candidate is first author or a principal collaborator and by receiving external research funding
4. Active participation in departmental research program and ten scholarly works in education or clinical issues such as a review article and case reports in peer reviewed journal, chapters in textbooks or published educational methods and curriculum, videotapes or electronic media.
5. Performance of leadership and administrative functions within the medical school, department, the hospital, or community.
5. Performance of leadership and administrative functions within the medical school, department, the hospital, or community.
6. Evidence of national recognition for scholarly activities as judged by such distinctions as membership in student sections, advisory groups, election to professional societies, and funded research and at least five external letters of reference
6. Evidence of peer recognition at the national level for education or administrative service as judged by such distinctions as awards, invitations as visiting professor, election to professional societies and at least five external letters of reference.
SCHOOL #4
APPOINTMENTS
QUALIFICATIONS AND REQUIREMENTS
Qualifications for appointment, set forth below, are not intended as justification for automatic promotion;

conversely, justified exceptions may be made.
Professor. To be eligible for the rank of professor, a faculty member must have a record of outstanding
performance usually involving both teaching and research, or creativity or performance in the arts, or
recognized professional contributions. The faculty member normally is expected to hold the earned
doctor's degree and have at least nine years of effective, relevant experience.
Associate Professor. To be eligible for the rank of associate professor, a faculty member must have a
record of effective performance usually involving both teaching and research, or creativity or
performance in the arts, or recognized professional contributions. The faculty member normally is
expected to hold the earned doctor's degree and must possess strong potential for further development
as a teacher and scholar.
Assistant Professor. To be eligible for the rank of assistant professor, a faculty member normally is
expected to hold the earned doctor's degree or its equivalent and must possess strong potential for
development as a teacher and scholar.
Instructor. To be eligible for the rank of instructor, a faculty member normally is expected to hold the
master's degree plus substantial additional graduate study, such as having fulfilled the requirements for
admission to candidacy for the doctor's degree.
The qualifications for appointment to positions bearing other titles, such as lecturer or research
professor, are in the Policies and Procedures Manual.
APPOINTMENT PROCEDURES
When the provost, dean, and department chair agree that a vacancy exists, the dean or chair shall
recommend appointment as prescribed in the Policies and Procedures Manual. All vacancies shall be
advertised in accordance with the university's affirmative action policy and state and federal law.
TENURE AND PROMOTION PROCEDURES
The procedures set forth below governing tenure and promotions shall apply to all academic units of the

university. The primary responsibility for the operation of all tenure and promotion procedures shall rest
with the tenured members of the faculty of each academic unit. Final authority for recommending tenure
or promotion to the University Board of Trustees shall reside with the president, and final authority for
approving recommendations of tenure and promotion rests with the Board of Trustees.
ESTABLISHMENT AND REVIEW OF UNIT CRITERIA AND PROCEDURES
The university is committed to achievement in research (including scholarship, visual arts, or performing
arts), teaching, and service. Collectively, the faculty profile of the university and of any academic unit
should reflect performance consistent with that of major research universities. Unit criteria should reflect
the fact that a candidate who is weak in teaching or research, promotion or tenure might not be in the
best interest of the university. Although the tenured members of each academic unit formulate specific
criteria and procedures for tenure and promotion, individual unit criteria and procedures shall be
consistent with the Faculty Manual and shall generally conform to guidelines established by the
University Committee on Tenure and Promotions (UCTP).
Unit criteria for tenure and for promotion of a faculty member shall provide clear standards for the
assessment of past achievements. Criteria for all tenure and promotions decisions should require a
record of accomplishment indicative of continuing development of the faculty member in research,
teaching, and service. Criteria for promotion from associate professor to professor and for tenure at the
rank of professor should require evidence of national or international stature in a field. Unit criteria for
promotion or tenure generally shall require, at a minimum, evidence of excellence in either research or
teaching, accompanied by a strong record in the other areas.
In every instance, the record of teaching, research, and service shall be thoroughly documented, as
suggested in the UCTP guidelines. Unit procedures for the evaluation of the teaching component of the
file must require peer and student evaluations. For units in which the primary focus of the faculty is on
public service, criteria for tenure and promotions shall require evaluation of the quality of the public
service work and the relationship of the service to research or teaching.
Each unit shall submit its proposed tenure and promotions criteria and procedures through the dean to
the provost, who shall forward the proposed criteria and procedures to the UCTP along with his or her
comments. If the UCTP finds that the proposed criteria and procedures are consistent with the general

guidelines in The Faculty Manual and are sufficiently clear, the UCTP shall approve the criteria and
procedures, which then become effective immediately unless otherwise specified. If the UCTP
disapproves the proposed unit criteria and procedures, it shall return them to the unit with an
explanation of the deficiencies. The unit shall then revise and resubmit its proposed criteria or
procedures to the UCTP. Existing criteria and procedures shall be resubmitted to the UCTP for periodic
review on a rotating basis as determined by the provost.
New members of the faculty and persons transferred into tenure track positions will be informed in the
offer of appointment of the tenure regulations applicable to the position. Any change in these regulations
prior to the effective date of the appointment will be communicated to, and receipt acknowledged by, the
new faculty member in writing and made a part of the faculty member's official record. The appointment
of a non-tenured faculty member to an administrative position does not excuse the faculty member from
the unit criteria for tenure and/or promotion. A full-time administrator later appointed as a faculty
member is not excused from the unit criteria for tenure and/or promotions.
The tenured faculty of each academic unit shall serve as that unit's tenure and promotions committee.
Departments or units with fewer than five tenured members are required to submit to the UCTP a policy
for constituting the unit tenure and promotions committee so that the committee has at least five tenured
members. The unit tenure and promotions committee may create subcommittees to assist the full
committee in the performance of its work. Where possible, on matters other than consideration of a full
professor for tenure or consideration of an associate professor for promotion to full professor, a
subcommittee shall include both professors and associate professors.
By April 15 of each year, each unit tenure and promotions committee shall elect a chair for the
upcoming year and report the chair's name to the provost and Faculty Senate office.
UNIT CONSIDERATION OF TENURE AND PROMOTION FILES
At the unit level, all no tenured faculty are considered for tenure, and all faculty members below the rank
of professor are considered for promotion each year. Consideration at the unit level is automatic unless
the faculty member requests in writing that consideration be deferred until the following year (provided
that nontenured faculty cannot defer tenure consideration beyond the penultimate year of their
maximum probationary period). Unless prohibited by unit tenure policies and procedures, candidates for

faculty appointments may be recommended for tenure on appointment by a favorable vote of the
tenured faculty of equal or higher rank in the unit.
However, consistency and durability of performance are relevant factors in evaluating faculty for tenure;
therefore, the length of service which a faculty member has completed in a given rank is a valid
consideration in formulating a tenure recommendation. Faculty members appointed at the rank of
assistant professor who have not previously held tenure-track positions at another college or university
normally will not be recommended for tenure until they are in at least their fourth year. Faculty members
appointed at the rank of associate professor or professor who have not previously held tenure-track
positions at another college or university normally will not be recommended for tenure until they are in at
least their third year.
Potential candidates for tenure or promotion should be advised in writing by the dean, department chair,
or other appropriate administrator by May 1 (or within two weeks of the candidate's date of initial
appointment) of the timetable for the submission and consideration of files. This early notification of
candidates will be in addition to the official notification of potential candidates that is performed by the
dean, department chair, or other appropriate administrator at least one month in advance of the date
when the file is due.
A candidate and the academic unit should follow UCTP guidelines for putting files together. The unit is
responsible for providing a synthesis of evaluations of the candidate's teaching performance and
obtaining at least five outside evaluations of the candidate's research. A majority of the outside
evaluators must be selected by the unit. The unit should include in the file a summary of the
professional qualifications of each outside evaluator or a copy of each evaluator's curriculum vita, along
with a copy of a letter requesting the evaluation and informing the evaluator of the unit's relevant criteria
for tenure or promotion. The dean and the unit chair or other appropriate administrator shall be notified
by the unit committee chair of the pending meeting of the committee.
Each unit shall apply its criteria and procedures to determine whether a candidate qualifies for
promotion, tenure, or both. With regard to tenure recommendations, all committee members of rank
equal to or higher than the candidate shall vote by secret ballot. With regard to promotion
recommendations, all committee members of higher rank than the candidate shall vote by secret ballot.
Each member eligible to vote shall vote "yes" or "no" or "abstain." Whether an abstention vote in units
counts towards the total votes for candidates in determining an appropriate majority shall be decided at

the unit level. A record of the votes is made in all instances and must be forwarded through appropriate
channels. Written justification of all votes at the unit level shall be mandatory and shall state specifically
how the candidate meets or does not meet the unit's criteria.
Recommendations from the unit tenure and promotions committee, including the recording of votes and
all written comments, are forwarded to the unit chair or other appropriate administrator. The unit chair or
other appropriate administrator shall vote "yes" or "no" or "abstain" and shall forward his or her vote with
written justification, along with all other recommendations, statements, and endorsements to the dean.
The dean shall forward the file with his or her recommendation to the provost, who shall forward the file
with his or her recommendation to the UCTP.
A candidate's file will be sent forward if the unit tenure and promotions committee recommends tenure
or promotion. The file of a candidate for both tenure and promotion who is recommended by the unit
tenure and promotions committee for tenure or promotion, but not both, will be sent forward for
consideration of only that aspect favorably recommended by the unit. Upon written request of any
candidate dissatisfied with a negative decision by the unit tenure and promotions committee, the unit
committee shall send that candidate's file through all appropriate channels for endorsement to the
president for appropriate action.
It becomes obvious after a review of the above Policy and Procedures on Tenure and Promotion that
expectations vary greatly from institution to institution. For some, a strict set of defined criteria must be
met within a prescribed period of time. For others, eligibility for promotion is set at the departmental level
and may be tailored to meet the needs of our largely clinical specialty.
The range of expectations and the differences between the Clinical Track and the Tenure track make
the former most attractive to most beginning emergency physicians. There is a common theme however
in all of these that demands some sort of research or creative activity: it will be expected of you so you
should have an expectation of some sort of research / publishing activity as part of your academic
career. Regardless, there is a need for more than simple teaching activities: administration, national
service, creativity and research all play a part in the advancement of a faculty member.
One further point: in the majority of the guidelines for promotion there is mention of some flexibility in
these guidelines, a subjective component which appears to play an important role in the promotion

process. This might seem a beacon of hope for promotion for those of us who have chosen Emergency
Medicine with its need for innovative thinking and its high clinical load. In truth however, there remains a
rather stringent set of guidelines that must be met prior to promotion, especially with regard to promotion
in the tenure track.
In summary, when planning for future promotion, a newly arrived faculty member should expect frequent
evaluation within his/her own department by those who have been successful in promotion on that
particular track in addition to the Department Chair. Having these individuals on your side, for guidance
and support, as well as for realistic evaluations of your performance, will lead to more frequent success
in promotion regardless of the track chosen.

Academic Promotion and Tenure
Authors: Douglas A. Rund & Daniel F. Danzl.
Academic emergency medicine, as the second youngest specialty, is a relative newcomer in the house
of medicine. The American Board of Medical Specialties (ABMS) Assembly recognized the American
Board of Emergency Medicine (ABEM) in 1989 as the 23rd independent specialty board. As a result, at
this juncture in emergency medicine senior level mentors remain at a premium. There are only a handful
of tenured professors of emergency medicine, and a commensurately small number of emergency
medicine faculty who sit on medical school Promotion and Tenure (P&T) committees.
Junior faculty in emergency medicine often fail to consider promotional criteria or various faculty track
options when first entering academics. Steady progress and career development require a clear
understanding of the academic promotion and tenure process.
Institution Specific Criteria
Each University’s governance documents detail specific rules regarding promotion and tenure. The
departmental chair, and in many instances a dean for faculty affairs, will provide an introduction to the
rules of the road for newly appointed faculty. Junior faculty are also well served if they obtain a current
copy of the University’s governance, documents and review the sections on the promotion process and
tenure. Since these rules change occasionally, the latest draft may be available from the Provost or
central administrator or on the University’s web site. The specifics about preparation of the promotion
dossier or portfolio or triptych must be studied in detail during its preparation, but an advanced
understanding of the criteria early in one’s career is also helpful. Certain items such as the need to keep
and record student and resident evaluations of teaching, for example, might not be immediately
apparent at the time of initial appointment but will be necessary for the educator’s portfolio section of the
promotion package.
The faculty senate in many universities has approved governance documents that permit the medical
school unit to employ teaching faculty and clinicians on a variety of "tracks". This flexibility recognizes
the need to recruit clinician-educators in nearly all medical school environments, and particularly in
emergency medicine. In response to such needs, medical schools have gradually introduced various
non-tenure pathways to promotion that recognize clinical skill and teaching excellence.(1,2) Almost 75%

of the LCME-accredited medical schools in the United States have now developed some form of
"clinician-educator" track.
The rules regarding promotion and the possibility of tenure in each track differ from one another and
deserve careful review in both the initial selection of a track and the requirements for promotion.
Common terms for these tracks include "clinical", "regular clinical", "clinician-educator", or "clinician-
investigator". Most of these tracks are for a fixed term of years and are then renewable. A new
permutation is the "rolling term" track that automatically extends in length annually.
Some institutions permit at least one switch from track to track, but switching from the tenure track to the
clinical track may not be allowed once the tenure evaluation process has started after the 5th or 6th
year. The 7th or 8th year is typically the last year of full time employment for the faculty member denied
tenure during the probationary period.
The annual departmental or chair review should provide some indication of progress toward tenure for
eligible faculty. The process (including the interview) is an opportunity for the faculty member to
question and clarify the department’s promotion and tenure policies and to develop a plan for the
coming year. The departmental review may be reported in the form of a letter from the chair to the
faculty member, but is some cases it may be supplemented by a standard departmental evaluation that
reports success in meeting the departmental criteria. In departments sponsoring an emergency
medicine residency program, the program director is required by the national Residency Review
Committee for Emergency Medicine of the Accreditation Council for Graduate Medical Education to
participate in the evaluation process.
Each department and each university has specific policies regarding evaluation categories on faculty
tracks for promotion and tenure. In nearly all instances the mix includes four traditional components:
academics (creativity, innovation, scientific research, scholarly publication), clinical expertise, teaching,
and service.
A central expectation for promotion in most tracks is some scholarly accomplishment, which is
mandatory in the regular tenure track. Promotion criteria commonly considered in this category are

noted in the Box. Traditional research expectation in a science-based discipline such as medicine is that
the faculty member will conduct scientific research and publish the results in peer-reviewed journals.
Evidence of the quality of the research includes funding by agencies outside the university such as the
National Institute of Health (NIH). Other scholarly activity such as authorship of textbooks or chapters is
considered valuable but not at the same level as original contributions, or grant supported research.
In the various newly established clinical tracks scholarship must rightfully be assessed according to
different criteria. Most promotions committees expect fewer peer-review publications from clinician-
educators than from tenure track investigators. Scholarship for a clinician educator has been defined as
"the act of seeking, weighing, formulating, reformulating and communicating knowledge of clinical
practice or teaching".(3)
Teaching criteria commonly considered for promotion include didactic skills, mentoring, developing
educational programs and education research. Although patient care and resident teaching are often
seen as departmental priorities, a central purpose of the medical school itself is the education of medical
students. The dossier for promotion therefore, must supply information about courses taught and the
numbers of students.(4) Evaluation of teaching quality is provided by students who usually rate
instructors in a standard format and by departmental faculty who are provided the opportunity for
didactic observation.(5) Resident teaching is similarly evaluated by both the residents and by other
faculty, especially the program director. Departmental or other teaching awards are also perceived as
valuable indicators of teaching quality.
Excellent patient care and clinical service are nearly always expected of the faculty member. Other
services to the department, school or university can include participation in a committee or the
performance of medical administrative functions (such as Director of EMS or Director of one of the
medical student courses). Departments should protect tenure-track junior faculty from over-involvement
in committees and administrative activities, however, because of the time and effort required to
accomplish the research components of the faculty position. When possible, new faculty should
participate in such activities sparingly, especially in a position where considerable research effort is
required.
Tenure

In the academic setting of the University the term tenure is associated with the concept of academic
freedom. Tenure is, in essence, a status granted after a probationary period that entitles one to hold a
position that is protected from dismissal except for serious transgressions as determined by institutional
due process. The concept of academic freedom dates back centuries in Europe and has survived
various challenges in the United States. Tenure in its American form originated in the 1920’s. An
influential university philanthropist suggested that an economics professor be terminated following an
unflattering historical analysis of the family’s financial affairs.
Academic freedom establishes the right of teachers and researchers to study, conduct research, and
express their views without fear of reprisal or dismissal from the faculty.
The concept implies that the granting of tenure depends on competence as a teacher or researcher.
The maintenance of tenure requires adherence to certain standards of scholarship, teaching
accomplishment, and professional integrity rather then political views or religious beliefs.
In practice a tenured faculty member cannot be terminated arbitrarily by the University. Termination
must be "for cause" and the accused has rights to due process involving a hearing before other
professors at the same institution. The net effect of the process is that it is difficult for an administration
to terminate a tenured faculty member and the faculty member therefore has some degree of security in
maintaining employment at the University.
Most universities in this country have a specific process for granting tenure. A strict process with a
timetable is enforced because without it a faculty member beginning the eighth year of employment, for
instance, might claim de facto tenure; that tenure has, in fact, been granted to the faculty member by
virtue of many years of employment.
The granting of tenure typically involves a detailed assessment of the faculty member’s scholarly and
creative accomplishments, teaching ability, and potential for future achievements. In the traditional
medical school process a faculty member granted tenure should have demonstrated the capacity to
function as an outstanding teacher and an independent scientific investigator whose work has been
critically evaluated by intra-mural and extra-mural experts. The awarding of externally funded research

grants demonstrates favorable external review, as does publication in peer reviewed journals.
The requirements for tenure vary widely among institutions. In the most rigorous setting, the Assistant
Professor applying for promotion and tenure might be expected to demonstrate continuous NIH funding
including support for a new research project grant (RO1), fifteen to forty first author original
contributions, demonstration of outstanding teaching, and at least some service to the University. The
benchmark at many institutions is less stringent.
In the traditional setting, highly regarded important peer-reviewed publications and governmentally
sponsored research grants provide the strongest evidence of one’s capability as an independent
scientific investigator and send the signal that if tenured the faculty member will be able to fund future
research activity including release time, salary support, lab space, lab associates, equipment, supplies
and overhead.
The award of tenure is typically associated with promotion to the rank of Associate Professor, although
in other schools tenure is awarded only to a select number of full professors At some point (eg. before
the beginning of the eighth year of service), the institution must "set the hook" or "snap the line", i.e. the
faculty member on the "tenure track" must be either awarded tenure or terminated if the institution
subscribes to an "up or out" process.
The process of tenure review occurs in stages. The first 6 to 8 years of employment for tenure track
faculty is often termed the "probationary period". Faculty evaluation in the early stages of this period are
typically performed by the departmental chair and involve an annual review concluded by a letter to the
faculty member regarding needs for future growth and prospects for tenure.(6)
As the process evolves the faculty member is reviewed by more tenured faculty, who are organized into
promotion and tenure (P&T) committees. In the final stages of the process, a separate evaluation is
usually required by each successive promotion and tenure committee (department, college, university)
before moving to the next step of the process. In some rare cases the department chair or dean may be
able to forward a recommendation without P&T committee approval but the decision to do so would
have to be clearly justified

Promotion Sequence and the Administrative Process
New residency graduates are hired initially at the instructor or assistant professor level. (Figure 1) Some
institutions base promotion to assistant professor on successful completion of the ABMS board
certification process.
The assistant professor rank is typically a probationary process in tenure track positions. The faculty
member is considered for tenure at the 6th or 7th year of service and must be promoted before the 8th
year of service, which will be the final year of appointment if not granted tenure. Non-tenured faculty
tracks tend to have less rigorous requirements for promotion that can come before or after the seventh
year of service.
The next rank is associate professor and many faculty remain at that rank until retirement. In the
traditional process outlined above, promotion to the rank of full professor usually occurs after some
period of time as an associate professor (eg. seven years), during which the faculty member has
continued to demonstrate excellence in teaching and achieved a national or international reputation as a
scientific investigator (uninterrupted extramural funding, excellent and important peer-reviewed
publications and cutting edge presentations at the major national and international scientific meetings).
Because the details vary from institution to institution, each faculty member should review the specifics
of the appropriate promotion and tenure administrative process to ensure that the proper steps are
followed. In general, however, the process originates in the faculty member’s home department or
division. (Figure 2)
At the proper time for promotion the candidate assembles detailed information on grants, publications,
presentations, numbers of courses taught, numbers of students in each course, resident teaching,
evaluations of teaching, and description of University service and clinical care. In most cases some
external review will be required. Usually the chair or departmental promotion and tenure (P&T)
committee will select several external reviewers who hold faculty ranks superior to that of the candidate.
For promotion from the rank of associate professor to the rank of professor, therefore, external reviews

would be sought from other full professors. The candidate may be able to suggest a portion of the
reviewers. External reviewers may be sent the candidate’s curriculum vitae and in some cases, two or
three of the candidate’s most recent or cited publications. The reviewer should be knowledgeable
enough about the academic field to judge the quality of the candidate’s work and usually provides
written evaluation in the form of a letter to the departmental chair or P&T Committee.
When the dossier and external evaluations are assembled, the application is reviewed by a
departmental promotion and tenure committee. The recommendation of the departmental P&T
committee is accompanied by a letter from the departmental chair to the medical school’s P&T
committee summarizing the applicant’s accomplishments and a recommendation for or against
promotion. The recommendations of the departmental committee, the chair, and the medical school’s
P&T committee are then forwarded to the Dean for consideration. Their decisions are forwarded to the
Executive Committee, and then to the University by the Dean who also provides a recommendation.
Approval by the University P&T committee is usually the final hurdle because approval by the Provost,
President and the Board of Trustees is nearly always based on the recommendation of the University
P&T committee. The entire process takes months. At many medical schools, the promotion process
stops at the level of the school P&T committee’s recommendation to the Dean of the Medical School.
The specifics of the promotion and tenure process vary from institution to institution and track to track
and should ideally be reviewed by the junior faculty member prior to the initial appointment. In nearly all
instances, criteria for promotion will include some mix of the four major areas: academic activity, clinical
expertise, teaching, and service. New developments in the faculty evaluation process will undoubtedly
include greater refinement in evaluating teaching and clinical care. With the development of clinician-
educator pathways rigorous evaluation of clinical ability will become increasingly important.
The aspiring academic emergency physician must plot a course to advance. The nature of this specialty
invites excessive service and teaching loads, which are the most common cause of junior faculty
attrition. Strive for a reasonable load of administrative responsibilities, since they tend to trickle down to
assistant professors and interfere with their research and teaching activities, which are critical and
represent the basis for promotion and academic advancement.
Figure 1

The Academic Ladder
Professor
5-10 years
Associate Professor
(With or without tenure)
Associate Professor
(With or without tenure)
8 year boundary
6-8 yrs
Assistant Professor
1 to 2 yrs or Board Certified
Instructor
(Initial Appointment)
Figure 2
Pathway Toward Promotion
Board of Trustees/Governors
President
Provost (Officer of the University)
University P&T Committee
Dean-College of Medicine
Executive Committee (Department Chairs)
Promotion and Tenure (P&T) Committee (School-wide)
Chair Recommendation
Consideration and vote by departmental peer-review (P&T) committee
1.) Osborn, LM, Sostok, M, Castellano, PZ, Blount, W, Branch, WT, Recruiting and Retaining Clinician-
Educators: Lessons Learned from Three Programs, JGIM, Vol 12, April (supplement 2) 1997.

2.) Branch, WT, Kroenke, K, Levinson, W, The Clinician-Educator-Present and Future Roles, JGIM, Vol
12, April 1997.
3.) Beasley, BW et al. Promotion Criteria for Clinician-Educators in the United States and Canada: A
Survey of Promotion Committee Chairpersons. JAMA, Vol 278:9, pp 723-728, September 3, 1997
4.) Lubitz, RM. Guidelines for Promotion of Clinician-Educator, JGIM, Vol 12 (supplement 2) pp S71-
S78, April 1997.
5.) Jones, RF, Froom, JD, Faculty and Administration Views of Problems in Faculty Evaluation,
Academic Medicine, Vol 69, No. 6, pp 476-483, June 1994.
6.) Jouriles, NJ, Kuhn, GJ, Moorhead, JC, Ray, VG, Rund, DA, Faculty Development in Emergency
Medicine, Academic Emergency Medicine, Vol 4, No 11, pp 1078-1086, 1997.

Developing a Career in the Scholarship of Discovery
Author: Terry Vanden Hoek
Research and Emergency Medicine: an opportunity for a career of discovery
Unfortunately, there is no "research for dummies" book available on the bookstore shelf—I would have
bought a copy immediately if it had been available--and in starting my own research career, much good
advice has unfortunately come only after learning from mistakes that might have been prevented. What
follows are my own thoughts about what has helped me get started on what I dream will become a
successful career of discovery. My hope is that you will be inspired by the possibilities of research,
better appreciate your unique place in the house of medicine and science, and develop some
beginnings of a blueprint for success as you continue your own scientific trek. With more articles like this
from each one of us involved in research in Emergency Medicine, perhaps collectively we can become
"running partners" as we submit manuscripts, grant applications, and make discoveries that can
ultimately make a difference in emergency medical care.
Research induction sequence: good questions, mentoring, and investment
Finding a good research question
How do you induce a promising research career? Your area of research is an important and perhaps the
most fundamental decision to make in your research career. It may determine your level of passion
when you are staying up late at night to get a grant proposal finished; if it is well-honed it will help create
boundaries which will keep you focused on what is most unique about your work; and it may also
determine how well you fit into the overall mission of your section, department, institution, and field. Like
all important decisions, it is well worth the time and investigation you put into it.
1. Take advantage of the unique questions Emergency Medicine faces. Emergency Medicine physicians
are in a position to contribute to world-class research. We have an inherent advantage no amount of
postdoctoral or PhD training can ever give--exposure to a challenging clinical practice, which is filled
with individual research questions that can best be answered by our specialty. Since the Emergency
Department provides medical oversight to emergency medical services in the community and is open to
all who seek care, these questions span many issues of health service and public health not faced by

many of our colleagues. Such research questions include how to break down barriers to healthcare
access, effectively screen and refer patients affected by domestic violence, care for the homeless or
substance abuse patient, improve physician-patient communication, monitor and decrease emergency
department overcrowding, prevent medical errors, improve resource utilization for emergency medical
transport services, and improve readiness for natural and man-made disasters. Also quite unique to our
field are questions of how nightshift work may affect productivity, physician wellness and health, and
patient safety. There are of course a multitude of questions regarding rapid diagnostic and treatment
strategies for medical conditions that span all other specialties within medicine. These questions may
range from better diagnostic algorithms for pulmonary embolism to learning how to resuscitate ischemic
tissue at the molecular and cellular level. Bottom line, there is a gold mine of good research questions in
emergency medicine for those willing to ask them. These questions are keys that can open many doors
at academic institutions to investigators in other fields doing work relevant to that question.
2. Get appropriate research consultation. Emergency Medicine physicians are used to working and
consulting with other healthcare providers to create a diverse team of people tailored to meet the needs
of any given patient. For example, it is not unusual to have discussions with cardiology, neurology, and
orthopedics regarding a patient with atrial fibrillation, new focal weakness, and a hip fracture after falling
at home. These same people-skills can be used to request a "research consult" about an interesting
research question. Thus, for example, it would not be unusual to bring together a team of neurologists,
engineers, paramedics, and emergency medicine physicians to ask whether paramedics could induce
focal brain hypothermia in stroke patients, and perhaps extend the window of opportunity for treatment
with thrombolytics. If we wanted to model such a system in cellular and animal models, veterinarians
and cellular biologists might also become involved. If the question relates to effects of nightshift work,
there are many world-class sleep physiologists and patient safety experts who are waiting to receive a
phone call or visit from an emergency medicine physician willing to ask "how can we better adapt to
night shift work?" If the question relates to how to improve screening and referral for substance abuse,
then a team of social workers, sociologists, and psychiatrists/psychologists might become involved. In
addition, some of the same colleagues we interact with in the Emergency Department during patient
care could become important partners in research. Don’t be afraid to ask these other scientists for input
on your research. Be ready to give a short presentation about your work and your research question (I
like to do a less than 10 slide Powerpoint talk)—this has helped me tremendously in refining my
questions. It’s also fun to hear a completely different perspective on your work. One of the best
experiences I’ve had in giving lectures was talking about cardiac arrest to a group of physics students

and professors. They introduced me to concepts of measuring motion in my cell model--as another
index of what happens during ischemia/reperfusion to the heart--I had never considered.
3. Finding the right question. There are enormous opportunities for finding out what the cutting-edge
questions are in any given research area. Do you wonder why particular types of patients in the
Emergency Department do better and others do worse? Despite the hectic pace and stress of the
emergency department, it is often a rewarding question to ask such questions about at least one patient.
If you can, find out what your clinical consultants know and don’t know. Perhaps they are interested in
the same group of patients, and are doing research to answer some of the same questions you have.
Find out what the literature knows and what it doesn’t, and who in the world is focusing on the problem.
Important websites that may be helpful include PubMed (http://www4.ncbi.nlm.nih.gov/PubMed/). There
are thousands of abstracts of reviews performed by the Cochrane group which can be searched at
http://www.update-software.com/Cochrane/ other helpful links may include general search engines such
as http://www.google.com/ or http://vivisimo.com/ . Ask your colleagues about search strategies they
use. My own research interest began with patients who died despite being fully "resuscitated" back to a
normal blood pressure. Potential answers to this phenomenon did not appear until looking into the basic
science of reperfusion injury and apoptosis.
It’s helpful to make a list of the resources you find most helpful in knowing what is happening in your
research area of interest. Key resources include journals (look at them as scientific catalogues of
research possibilities--most academic institutions have a number of e-journals available, and I have
found it helpful to bookmark the access site to those journals on my computer and try to read each
month what is being published in my areas of interest), seminar series (these are usually posted at
academic institutions weekly or monthly, physically or electronically) and academic interest groups
(usually monthly or quarterly) relevant to your interest can also become important sources of new
insights. It took me over a year on campus as a junior faculty to realize that I was missing a visiting
professor lecture series which included internationally renowned speakers talking to groups of less than
30 people—a great opportunity to talk to some of the world’s brightest scientists. Other meetings I have
found helpful include a mitochondrial interest group (yes, this interest group really does exist at my
institution and has been extremely helpful for me), but for other faculty such meetings may include a
public policy group that meets across campus. Most clinical and laboratory research groups conduct
frequent meetings about research in progress—ask if you can attend some of these if the work being
done is of interest to you. Being interested in someone else’s research is usually considered a great

compliment. Find out what excites you, what feels important to you, and ask a lot of questions. If there
any chances to present your research interest, do it. It will help you refine your thinking about what your
research focus is, and allow others to give feedback. These presentations may include anything from
grand rounds for residents/faculty, to a more informal overhead presentation for a laboratory research
group, or a very brief presentation on a laptop to a fellow researcher on campus.
My own interest in ischemia/reperfusion injury began with talking to investigators at SAEM, the
American Heart Association, and the International Society for Heart Research. Attending at least 2 such
national meetings a year can be very helpful to get a sense of what is happening in your scientific area
of research. Poster presentations at these meetings can be important forums for asking questions about
other people’s work (pick out the posters you want to visit ahead of time, and it may be helpful to write
down your questions before visiting), and is a good way to let other people know who you are as a
person and a researcher. Making connections between other people’s work and your own observations
as a clinician and researcher can be a moment of discovery for both of you. Subsequent emails and
phone calls made possible by these interactions could also save a lot of time as you begin your own
work. My own area of research, preconditioning, was first described by a young investigator in a poster
session at a scientific meeting in the middle of Canada. That work came to life for me at a small
scientific meeting of the International Society for Heart at a hotel in Cincinnati, OH, and talking about
science at the side of a pool. Such meetings are critical for finding new ideas.
4. Look for key judo moves. The beginning of the book "The Road Less Traveled" by M. Scott Peck was
best known for it’s beginning short sentence of truth: "Life is difficult." The same can be said for
research, and even more so for research done alone. One of the key concepts of judo is to gain strength
from the momentum of others. Learning what science is going on around you, and finding a way to
incorporate your interests into that momentum to develop your own novel project leverages your
research time and can benefit everybody. As an example, I had very little expertise in studying
apoptosis, but believed that it played an important role in postresuscitation injury in our heart cell model.
By learning who was working on research in apoptosis at my institution, even though some of the
greatest momentum of that research was focused primarily on pulmonary epithelial and cancer cells, it
was beneficial to everybody to apply those same techniques to a cardiac cell model-- resulting in a
successful NIH grant application.
Learning the science environment may mean talking to other faculty within your department or section to

find out what research focuses exists at your particular institution. If you have a few areas of research in
which you have equal interest, think seriously about pursuing the area which can best "ride the wave" of
departmental and institutional momentum. To find out what funded research is happening at your own
institution, a helpful website is the Computerized Retrieval of Information on Scientific Projects (CRISP)
NIH database, located under "grant topics" on the NIH Office of Extramural Research homepage:
http://grants.nih.gov/grants/oer.htm . You can query this site by multiple search criteria, including new
and old grants funded at your institution, who the Principal Investigator is for each grant, and the
abstract of the research funded. This is a good place to look for opportunities to focus existing
successful research at your institution in new creative ways on an emergency medicine problem. Say
hello and tell them your question.
Mentoring and training
Unless you’ve had quite extensive research training, you will need a mentor to help guide you through
the initial stages (first 3-5 years) of your research career. Mentor in Homer’s Odyssey was a trusted
friend to Odysseus, later symbolizing a wise advisor who imparts the ability to mentate-- to think and
awaken to life. One author described mentoring as a transformational power: "Mentors are guides. They
lead us along the journey of our lives. We trust them because they have been there before. They
embody our hopes, cast light on the way ahead, interpret arcane signs, warn us of lurking dangers and
point out unexpected delights along the way."(1)
Two pathways help to formalize this process, and need to be seriously considered. One pathway
involves fellowship training, and opportunities include Emergency Medicine Research fellowship training
programs, The Robert Wood Johnson Clinical Scholars program (described at
http://www.uams.edu/rwjcsp/ ), or a host of postdoctoral fellowship training grants available through NIH
funding. To get a list of these opportunities at your institution, you can query the CRISP database
(http://commons.cit.nih.gov/crisp3/CRISP.Generate_Ticket) and enter "training grant" and specify your
institution. Emergency medicine programs that wish to cultivate fellowship training may want to add
some of these postdoctoral training programs onto the list of potential fellowships available for
interested residents. These programs often deal with questions very relevant to emergency medicine,
and often go begging for interested MD applicants. The principal investigator on some of those training
grants may be very interested in making some positions available for emergency medicine residents.

If you are junior faculty already, and wish to pursue a research career, another pathway (which can be
followed after or apart from a fellowship training program) for formalizing a mentorship process involves
the K career development awards via the NIH (outlined at
http://grants.nih.gov/training/careerdevelopmentawards.htm). Particularly the K08 and K23 awards are
useful for the beginning basic science or clinical researcher, and can provide up to $75,000-90,000 per
year for up to 5 years of salary support to work with a mentor and hone your research skills. Unlike the
R01 awards which are more competitive, funding as little as 20% of applications, the K applications
often have over a 50% success rate. Most importantly, these awards focus on the process put in place
to make you a better scientist—the quality of mentor chosen, what other advisors will help oversee your
progress, how much support you will have to train. Given that almost 3,000 K awards were given in the
year 2000, it should be a wake-up call for all of us that Emergency Medicine has only a handful of these
awards. Our success rate in percent applications funded is likely the same as any other specialty, but
for some reason we are not making the first critical move-- applying for these awards. One common
misconception about these awards is that they are only for very junior faculty just out of residency. More
senior faculty are eligible for these awards as well, as long as they have not received independent
federal funding in the past.
The number of submissions of K Award applications in Emergency Medicine is beginning to increase at
some institutions, and it’s an important question to consider when interviewing for a faculty appointment.
Ask how many K awards have been received among Emergency Medicine faculty and ask what support
is given for new faculty to achieve these awards. It’s a fair question to ask, since your own investment
will include significant time (probably well over 25-30 hours/week) spent in doing research and writing
for 1-2 years to compete for about $500,000 of salary support over 5 years. More importantly, this
"partnership" between yourself and your department will result in a training program designed to equip
an Emergency Medicine faculty member with the skills to design and conduct future competitive
research.
Regardless of which pathway you choose, the most important decision to be made is the mentor(s) to
whom you will entrust some of the most formative and important years of your research career. Choose
wisely. Below is a checklist to think about when evaluating a mentor:
1. Track record. Get a list of the former trainees of your candidate mentor, and see if they have become

independent investigators and are now on a career path where you would like to see yourself in a few
years. Mentors who have trained a number of fellows or mentored K Awardees who are now
successfully publishing (check in PubMed) and receiving grants (check on the CRISP database)
themselves are mentors who have the ability to help you do the same.
2. Available time. The best mentor in the world is worthless if she or he is gone most of the time, or is
effectively unavailable and too busy. Will your mentor have the time to meet initially 1-3 times per month
(1-3 hours at a time) to discuss progress? Will they be willing to get into the trenches of reading through
your initial manuscript submissions and grant proposals page by page, and line by line? Having had the
opportunity to work with a mentor who turned some of my initial manuscripts into a sea of red ink, and
another who took his research group (including me) out to his Michigan cabin in order to focus (without
distraction) on drafting one of my first manuscripts, I have come to appreciate the value of focused
attention by a mentor.
3. Personality fit. No matter how good, or how available, you and your mentor need to be able to get
along. Ideally, you need to be able to be comfortable in addressing the greatest fears and concerns of
how you’re doing. There may be "turf" issues which arise regarding research ideas since the mentor
ideally will be doing work somewhat similar and relevant to your own. Ideally you will be working with a
mentor considered by others as having integrity beyond reproach, and having a reputation for being
generous and fair.
4. Who’s going to make sure this relationship works? Some of the strongest marriages I know are
relationships in which both members have a vested interest in seeing that relationship succeed. This is
not unlike the mentor-mentee relationship. Before selecting a mentor, it’s important to ask who above
you and the mentor is invested in your proposed relationship. If for instance there is a stated
commitment between neurology and emergency medicine at the highest level that developing a stroke
research program is a high priority, and that both specialties want to support collaborative work, that will
strengthen your chances of success. Will your department head or section head be willing to make sure
the mentor fulfills his/her obligation, and will you truly receive the 80% protected time promised to the
NIH in return for your K award? These are important questions to ask ahead of time.
5. Stays focused on your research. A good mentor does not ask a mentee to do other work for him not
related to the research. Look for a mentor who is protective of your research time, and does NOT want

to see you picking up multiple administrative or extraneous projects along the way.
There is additional material, which include helpful discussions about mentorship; they are included in
the references (2, 3). Many investigators find it helpful to have more than one mentor, perhaps a senior
mentor and a junior mentor (e.g. someone who just recently completed their K08 award and recently
received funding for their first R01 NIH grant).
Research as an Investment
Good research is the result of investment, not miracles.
In most of life, we all know that something truly significant does not suddenly result from nothing. If it
does, it’s considered a miracle--not an expectation. Successful research careers are not miracles that
arise out of having no protected time and no support. If you value your sanity and your career, you will
find an academic program that wants to develop a research program through faculty investment rather
than faculty miracles performed during off hours. Successful grant applications (even K awards) have an
expectation that the applicant has already been doing some research, has institutional support to do that
research, and has preliminary results that can be presented as a result of that hard work and support.
Cutting edge research within 3 years is not an unreasonable expectation after being provided 3
days/week of protected time to do research, having at least 1 FTE as a helper to accomplish this
research, with the necessary dedicated equipment, space and supplies to do the work. This may easily
cost $300,000 or more, but could be a very small price to pay if it results in a successful research
career, which has the potential for great value. How much money and time should be invested to create
competitive research which has the potential to attract multiple million dollar grants over the course of
years, and generate excitement about Emergency Medicine at your institution among fellow faculty,
residents, medical students, and perhaps grateful patients and potential donors? Look for a program
willing to invest in your career. Help from a Research Director will not be enough—you need your own
protected time and access to good mentors who have their own independent funding and a track record
of training investigators. Of course, milestones need to be met, but you must have a means to get there.
Agree on what should be expected of you—productivity of manuscripts, K Award applications, R01
applications etc.

The value of a successful research career.
There are unparalleled opportunities for the physician-scientist to fill a unique niche and impact the
course of research today. The reasons are many and are highlighted well by others (4). Advances in
science are taking place at an accelerated rate, and yet fewer physicians are available to ask questions
about how to use these advances to improve the care of our patients. More and more physicians are
electing not to pursue a career in research for multiple reasons, not the least of which include the
financial realities of re-paying student loans, and the imposition of more clinical time due to managed
care and thinner operating margins at academic institutions. This is a most unfortunate pattern, as there
will undoubtedly be missed opportunities to advance medicine if physicians don’t actively participate.
The value of such an M.D. perspective is demonstrated by history: since World War II, about half of the
over 120 winners of the Nobel Prize in Physiology or Medicine have been given to M.D.’s. In addition,
the likelihood of success in getting an NIH grant funded is the same for M.D.’s vs. Ph.D.’s,
demonstrating that M.D.’s are capable of bringing a unique and valuable perspective to the research
table. However, fewer M.D.’s, particularly young physicians, are opting to take on a research career.
Hopefully we as a specialty will continue to work at the national level on this issue and join other
specialties in helping our national leadership to understand what is at stake.
The benefits of a successful research career to your own professional happiness and the excitement
and stability within your own department are incalculable. I love seeing patients; I also love designing
and implementing research projects. Although busy, doing such disparate yet related tasks of patient
care and research can be a lot of fun. Faculty having fun in their work are resistant to burn-out, generate
excitement in a program, and tend to stay. These are big benefits for any Emergency Medicine program.
Grants and manuscripts: monitoring your vital signs
As Emergency Medicine physicians, we appreciate how valuable changing vital signs can be in
monitoring how well or poorly our patients are doing. As researchers, there are also key vital signs
important in following how well our science is doing: They include protected time for research,
presentations about that research, abstracts submitted and accepted, manuscripts, and grant
applications. Monitoring these vital signs is important for a number of reasons. They will be important
ultimately for your promotion. From the start, it will be helpful to know what the promotions committee at

your institution will be looking for when you as a physician-scientist are considered for promotion. Do
NOT wait too long to sit down with your chairman to map out how the promotions process works for
physician-scientists, and what is considered "vital" on your biosketch over time for successful promotion.
Scientific vital signs are also worth discussing with your mentor. If a first-authored paper in a high-
impact journal is weighted more heavily than serving 3 years on a hospital committee which requires
considerable time each month, it’s easier to say no to that committee obligation and clear the calendar
on certain days each week to focus on science. The chairman of the department and the Dean’s office
may also have access to examples of individuals who have been promoted in your track—these can be
helpful to get an idea of what a successful CV looks like. Does the committee evaluate numbers of
manuscripts, position of authorship on papers, the impact score of the journal in which you publish?
Each institution weights things differently; it will be important to know what to expect in your promotions
process. Just as with patients who go unmonitored for hours, failure to monitor scientific vital signs each
year invites bad surprises.
Maintaining these vital signs also ensures that you will remain current in your scientific area of interest,
get feedback about your science, and focus on the most important questions relevant to your research
area. It’s a good idea to search each month and read any manuscripts published in your area of
research interest, and file these electronically or in hard copy in a library. These will be very useful when
putting together your next grant proposal. The phrase "no pain, no gain" definitely applies to scientific
endeavors, and some of the best advances in one’s science happen as a result of good (albeit
sometimes painful) critiques at presentations and constructive rejection of one’s work. When I look back
at the work I am most proud of today, that work was the result of multiple rejections and persistence in
trying to respond to the questions and concerns of reviewers. There will always be some unfair reviews,
but almost always there is some helpful critique. The pink review sheets from the NIH, which critique
submitted grant proposals can lay out in significant detail what you need to do to succeed in your
research. The best part of these reviews is that you don’t have to pay any consulting fees for what may
amount to excellent and career-altering advice. You do however have to submit your work for review
and persist in trying to answer good concerns raised. The only way to get this feedback is to submit
manuscripts and grant proposals.
Research maintenance: finding running partners
There are at least a couple types of research "running partners" that can help make your science easier

and more exciting, and give it a greater likelihood of success. I call them running partners because
they’re the type of people who have some interest and stake in you getting out of bed and succeeding in
your research. They complement you in that if there are some things you do not have the time or
needed skills to do—but nevertheless are important to your work—that they can do. They are people
who will hold you accountable when you agree you will submit a particular grant proposal by a particular
deadline. Two types of research running partners include administrative and scientific. Regarding the
administrative personnel, help is important in identifying grant applications and putting together grant
proposals. First of all, you need to know when grant funding relevant to your science is available. Most
institutions have a newsletter available in hardcopy and/or electronically which highlights internal and
external funding opportunities. Make sure you are on that mailing list. It also may be helpful to talk to the
grant office at your institution, to see if they provide any administrative help in letting you know when
particular grant opportunities matching your research interest become available. This type of "research
dating service" can help identify key funding opportunities. Once grant opportunities are identified, other
administrative help is very important for preparing the non-science components of grant applications—
budgets and their justification, description of personnel, assembling needed letters of support,
description of facilities, institutional grant office review and sign-off. An administrative support person
who helps with these additional aspects of grant preparation can be worth their weight in gold, and save
valuable time, which then can be directed at putting together the science of the grant proposal. They
also hold you accountable for helping to get the needed sections of the grant proposal together in a
timely fashion. Having someone in your department who either has these skills or is willing to learn them
from someone else at your institution could be a great help to you and the department.
The other type of running partner is scientific. It can be exceedingly helpful when colleagues at your
institution and elsewhere know you and your work well enough that they are willing to critique your work
at research meetings, and talk to you and send you emails about articles or grant opportunities they just
read relevant to your work. They are scientists doing work similar enough to your own to make it
worthwhile meeting regularly to discuss each other’s work, and perhaps finding ways to collaborate on
joint projects. Such meetings help you get to know the resources available (either within or outside your
own department) that could complement your work and help advance each other’s science. These are
also people who can preview your work prior to submitting it as a manuscript or grant proposal. I will
never forget the person who served as both a mentor and scientific colleague who helped get my first
manuscript regarding cardiac ischemia/reperfusion started. He ultimately insisted that I and my other
Emergency Medicine colleague come out to his cabin 1 hour outside Chicago without our beepers for

the weekend so that we would be less distracted and more focused, since he had an interest in my work
as a cardiac physiology Ph.D. scientist and wanted to see our work published. He reminded me that it’s
easy to get distracted, and of the importance of having other people around who care whether one’s
work succeeds and stays on track. These people can be found at research meetings and grand rounds.
They can be collaborators or former mentors, or new faculty recruited into your department to
complement and expand the research you are already doing. Such a "critical mass" of research running
partners who actually talk to each other and are invested in each other’s work is important for the long
haul of ongoing science. When those first letters of rejection arrive regarding a manuscript or grant
proposal, these research running partners can be very helpful in getting you back out there to finish the
work.
Our successes.
There are more and more examples of success stories in Emergency Medicine in establishing
independent research. As our specialty continues to mature, it will be important that we learn from each
other what works, and what doesn’t in building research careers. I feel like I have a lot to learn yet, and
hope I don’t make too many mistakes along the way. I hope any of your successes will be reported to
SAEM, so that we can all appreciate what research is being done in our field. I also hope others will
write chapters like this to share their own insights into what they’ve learned. Don’t hesitate to email me
about questions or your own insights after reading this chapter; I would love to hear them:
[email protected]. And have fun with your own career of discovery…
REFERENCES
1. Daloz LA. Effective Teaching And Mentoring: Realizing The Transformational Power Of Adult
Learning Experiences. San Francisco: Josey Bass, 1986.
2. Chin MH, Covinsky KE, McDermott MM, Thomas EJ. Building a research career in general internal
medicine. J Gen Intern Med 1998;13:117-122.
3. Gray J. Mentoring the young clinician-scientist. Clinical and Investigative Medicine 1998;21:279-282.
4. Rosenberg LE. The physician-scientist: an essential--and fragile--link in the medical research chain. J

Clin Invest 1999;103:1621-1626.

Developing a Career in the Scholarship of Discovery
Author: Terry Vanden Hoek
Research and Emergency Medicine: an opportunity for a career of discovery
Unfortunately, there is no "research for dummies" book available on the bookstore shelf—I would have
bought a copy immediately if it had been available--and in starting my own research career, much good
advice has unfortunately come only after learning from mistakes that might have been prevented. What
follows are my own thoughts about what has helped me get started on what I dream will become a
successful career of discovery. My hope is that you will be inspired by the possibilities of research,
better appreciate your unique place in the house of medicine and science, and develop some
beginnings of a blueprint for success as you continue your own scientific trek. With more articles like this
from each one of us involved in research in Emergency Medicine, perhaps collectively we can become
"running partners" as we submit manuscripts, grant applications, and make discoveries that can
ultimately make a difference in emergency medical care.
Research induction sequence: good questions, mentoring, and investment
Finding a good research question
How do you induce a promising research career? Your area of research is an important and perhaps the
most fundamental decision to make in your research career. It may determine your level of passion
when you are staying up late at night to get a grant proposal finished; if it is well-honed it will help create
boundaries which will keep you focused on what is most unique about your work; and it may also
determine how well you fit into the overall mission of your section, department, institution, and field. Like
all important decisions, it is well worth the time and investigation you put into it.
1. Take advantage of the unique questions Emergency Medicine faces. Emergency Medicine physicians
are in a position to contribute to world-class research. We have an inherent advantage no amount of
postdoctoral or PhD training can ever give--exposure to a challenging clinical practice, which is filled
with individual research questions that can best be answered by our specialty. Since the Emergency
Department provides medical oversight to emergency medical services in the community and is open to
all who seek care, these questions span many issues of health service and public health not faced by

many of our colleagues. Such research questions include how to break down barriers to healthcare
access, effectively screen and refer patients affected by domestic violence, care for the homeless or
substance abuse patient, improve physician-patient communication, monitor and decrease emergency
department overcrowding, prevent medical errors, improve resource utilization for emergency medical
transport services, and improve readiness for natural and man-made disasters. Also quite unique to our
field are questions of how nightshift work may affect productivity, physician wellness and health, and
patient safety. There are of course a multitude of questions regarding rapid diagnostic and treatment
strategies for medical conditions that span all other specialties within medicine. These questions may
range from better diagnostic algorithms for pulmonary embolism to learning how to resuscitate ischemic
tissue at the molecular and cellular level. Bottom line, there is a gold mine of good research questions in
emergency medicine for those willing to ask them. These questions are keys that can open many doors
at academic institutions to investigators in other fields doing work relevant to that question.
2. Get appropriate research consultation. Emergency Medicine physicians are used to working and
consulting with other healthcare providers to create a diverse team of people tailored to meet the needs
of any given patient. For example, it is not unusual to have discussions with cardiology, neurology, and
orthopedics regarding a patient with atrial fibrillation, new focal weakness, and a hip fracture after falling
at home. These same people-skills can be used to request a "research consult" about an interesting
research question. Thus, for example, it would not be unusual to bring together a team of neurologists,
engineers, paramedics, and emergency medicine physicians to ask whether paramedics could induce
focal brain hypothermia in stroke patients, and perhaps extend the window of opportunity for treatment
with thrombolytics. If we wanted to model such a system in cellular and animal models, veterinarians
and cellular biologists might also become involved. If the question relates to effects of nightshift work,
there are many world-class sleep physiologists and patient safety experts who are waiting to receive a
phone call or visit from an emergency medicine physician willing to ask "how can we better adapt to
night shift work?" If the question relates to how to improve screening and referral for substance abuse,
then a team of social workers, sociologists, and psychiatrists/psychologists might become involved. In
addition, some of the same colleagues we interact with in the Emergency Department during patient
care could become important partners in research. Don’t be afraid to ask these other scientists for input
on your research. Be ready to give a short presentation about your work and your research question (I
like to do a less than 10 slide Powerpoint talk)—this has helped me tremendously in refining my
questions. It’s also fun to hear a completely different perspective on your work. One of the best
experiences I’ve had in giving lectures was talking about cardiac arrest to a group of physics students

and professors. They introduced me to concepts of measuring motion in my cell model--as another
index of what happens during ischemia/reperfusion to the heart--I had never considered.
3. Finding the right question. There are enormous opportunities for finding out what the cutting-edge
questions are in any given research area. Do you wonder why particular types of patients in the
Emergency Department do better and others do worse? Despite the hectic pace and stress of the
emergency department, it is often a rewarding question to ask such questions about at least one patient.
If you can, find out what your clinical consultants know and don’t know. Perhaps they are interested in
the same group of patients, and are doing research to answer some of the same questions you have.
Find out what the literature knows and what it doesn’t, and who in the world is focusing on the problem.
Important websites that may be helpful include PubMed (http://www4.ncbi.nlm.nih.gov/PubMed/). There
are thousands of abstracts of reviews performed by the Cochrane group which can be searched at
http://www.update-software.com/Cochrane/ other helpful links may include general search engines such
as http://www.google.com/ or http://vivisimo.com/ . Ask your colleagues about search strategies they
use. My own research interest began with patients who died despite being fully "resuscitated" back to a
normal blood pressure. Potential answers to this phenomenon did not appear until looking into the basic
science of reperfusion injury and apoptosis.
It’s helpful to make a list of the resources you find most helpful in knowing what is happening in your
research area of interest. Key resources include journals (look at them as scientific catalogues of
research possibilities--most academic institutions have a number of e-journals available, and I have
found it helpful to bookmark the access site to those journals on my computer and try to read each
month what is being published in my areas of interest), seminar series (these are usually posted at
academic institutions weekly or monthly, physically or electronically) and academic interest groups
(usually monthly or quarterly) relevant to your interest can also become important sources of new
insights. It took me over a year on campus as a junior faculty to realize that I was missing a visiting
professor lecture series which included internationally renowned speakers talking to groups of less than
30 people—a great opportunity to talk to some of the world’s brightest scientists. Other meetings I have
found helpful include a mitochondrial interest group (yes, this interest group really does exist at my
institution and has been extremely helpful for me), but for other faculty such meetings may include a
public policy group that meets across campus. Most clinical and laboratory research groups conduct
frequent meetings about research in progress—ask if you can attend some of these if the work being
done is of interest to you. Being interested in someone else’s research is usually considered a great

compliment. Find out what excites you, what feels important to you, and ask a lot of questions. If there
any chances to present your research interest, do it. It will help you refine your thinking about what your
research focus is, and allow others to give feedback. These presentations may include anything from
grand rounds for residents/faculty, to a more informal overhead presentation for a laboratory research
group, or a very brief presentation on a laptop to a fellow researcher on campus.
My own interest in ischemia/reperfusion injury began with talking to investigators at SAEM, the
American Heart Association, and the International Society for Heart Research. Attending at least 2 such
national meetings a year can be very helpful to get a sense of what is happening in your scientific area
of research. Poster presentations at these meetings can be important forums for asking questions about
other people’s work (pick out the posters you want to visit ahead of time, and it may be helpful to write
down your questions before visiting), and is a good way to let other people know who you are as a
person and a researcher. Making connections between other people’s work and your own observations
as a clinician and researcher can be a moment of discovery for both of you. Subsequent emails and
phone calls made possible by these interactions could also save a lot of time as you begin your own
work. My own area of research, preconditioning, was first described by a young investigator in a poster
session at a scientific meeting in the middle of Canada. That work came to life for me at a small
scientific meeting of the International Society for Heart at a hotel in Cincinnati, OH, and talking about
science at the side of a pool. Such meetings are critical for finding new ideas.
4. Look for key judo moves. The beginning of the book "The Road Less Traveled" by M. Scott Peck was
best known for it’s beginning short sentence of truth: "Life is difficult." The same can be said for
research, and even more so for research done alone. One of the key concepts of judo is to gain strength
from the momentum of others. Learning what science is going on around you, and finding a way to
incorporate your interests into that momentum to develop your own novel project leverages your
research time and can benefit everybody. As an example, I had very little expertise in studying
apoptosis, but believed that it played an important role in postresuscitation injury in our heart cell model.
By learning who was working on research in apoptosis at my institution, even though some of the
greatest momentum of that research was focused primarily on pulmonary epithelial and cancer cells, it
was beneficial to everybody to apply those same techniques to a cardiac cell model-- resulting in a
successful NIH grant application.
Learning the science environment may mean talking to other faculty within your department or section to

find out what research focuses exists at your particular institution. If you have a few areas of research in
which you have equal interest, think seriously about pursuing the area which can best "ride the wave" of
departmental and institutional momentum. To find out what funded research is happening at your own
institution, a helpful website is the Computerized Retrieval of Information on Scientific Projects (CRISP)
NIH database, located under "grant topics" on the NIH Office of Extramural Research homepage:
http://grants.nih.gov/grants/oer.htm . You can query this site by multiple search criteria, including new
and old grants funded at your institution, who the Principal Investigator is for each grant, and the
abstract of the research funded. This is a good place to look for opportunities to focus existing
successful research at your institution in new creative ways on an emergency medicine problem. Say
hello and tell them your question.
Mentoring and training
Unless you’ve had quite extensive research training, you will need a mentor to help guide you through
the initial stages (first 3-5 years) of your research career. Mentor in Homer’s Odyssey was a trusted
friend to Odysseus, later symbolizing a wise advisor who imparts the ability to mentate-- to think and
awaken to life. One author described mentoring as a transformational power: "Mentors are guides. They
lead us along the journey of our lives. We trust them because they have been there before. They
embody our hopes, cast light on the way ahead, interpret arcane signs, warn us of lurking dangers and
point out unexpected delights along the way."(1)
Two pathways help to formalize this process, and need to be seriously considered. One pathway
involves fellowship training, and opportunities include Emergency Medicine Research fellowship training
programs, The Robert Wood Johnson Clinical Scholars program (described at
http://www.uams.edu/rwjcsp/ ), or a host of postdoctoral fellowship training grants available through NIH
funding. To get a list of these opportunities at your institution, you can query the CRISP database
(http://commons.cit.nih.gov/crisp3/CRISP.Generate_Ticket) and enter "training grant" and specify your
institution. Emergency medicine programs that wish to cultivate fellowship training may want to add
some of these postdoctoral training programs onto the list of potential fellowships available for
interested residents. These programs often deal with questions very relevant to emergency medicine,
and often go begging for interested MD applicants. The principal investigator on some of those training
grants may be very interested in making some positions available for emergency medicine residents.

If you are junior faculty already, and wish to pursue a research career, another pathway (which can be
followed after or apart from a fellowship training program) for formalizing a mentorship process involves
the K career development awards via the NIH (outlined at
http://grants.nih.gov/training/careerdevelopmentawards.htm). Particularly the K08 and K23 awards are
useful for the beginning basic science or clinical researcher, and can provide up to $75,000-90,000 per
year for up to 5 years of salary support to work with a mentor and hone your research skills. Unlike the
R01 awards which are more competitive, funding as little as 20% of applications, the K applications
often have over a 50% success rate. Most importantly, these awards focus on the process put in place
to make you a better scientist—the quality of mentor chosen, what other advisors will help oversee your
progress, how much support you will have to train. Given that almost 3,000 K awards were given in the
year 2000, it should be a wake-up call for all of us that Emergency Medicine has only a handful of these
awards. Our success rate in percent applications funded is likely the same as any other specialty, but
for some reason we are not making the first critical move-- applying for these awards. One common
misconception about these awards is that they are only for very junior faculty just out of residency. More
senior faculty are eligible for these awards as well, as long as they have not received independent
federal funding in the past.
The number of submissions of K Award applications in Emergency Medicine is beginning to increase at
some institutions, and it’s an important question to consider when interviewing for a faculty appointment.
Ask how many K awards have been received among Emergency Medicine faculty and ask what support
is given for new faculty to achieve these awards. It’s a fair question to ask, since your own investment
will include significant time (probably well over 25-30 hours/week) spent in doing research and writing
for 1-2 years to compete for about $500,000 of salary support over 5 years. More importantly, this
"partnership" between yourself and your department will result in a training program designed to equip
an Emergency Medicine faculty member with the skills to design and conduct future competitive
research.
Regardless of which pathway you choose, the most important decision to be made is the mentor(s) to
whom you will entrust some of the most formative and important years of your research career. Choose
wisely. Below is a checklist to think about when evaluating a mentor:
1. Track record. Get a list of the former trainees of your candidate mentor, and see if they have become
independent investigators and are now on a career path where you would like to see yourself in a few

years. Mentors who have trained a number of fellows or mentored K Awardees who are now
successfully publishing (check in PubMed) and receiving grants (check on the CRISP database)
themselves are mentors who have the ability to help you do the same.
2. Available time. The best mentor in the world is worthless if she or he is gone most of the time, or is
effectively unavailable and too busy. Will your mentor have the time to meet initially 1-3 times per month
(1-3 hours at a time) to discuss progress? Will they be willing to get into the trenches of reading through
your initial manuscript submissions and grant proposals page by page, and line by line? Having had the
opportunity to work with a mentor who turned some of my initial manuscripts into a sea of red ink, and
another who took his research group (including me) out to his Michigan cabin in order to focus (without
distraction) on drafting one of my first manuscripts, I have come to appreciate the value of focused
attention by a mentor.
3. Personality fit. No matter how good, or how available, you and your mentor need to be able to get
along. Ideally, you need to be able to be comfortable in addressing the greatest fears and concerns of
how you’re doing. There may be "turf" issues which arise regarding research ideas since the mentor
ideally will be doing work somewhat similar and relevant to your own. Ideally you will be working with a
mentor considered by others as having integrity beyond reproach, and having a reputation for being
generous and fair.
4. Who’s going to make sure this relationship works? Some of the strongest marriages I know are
relationships in which both members have a vested interest in seeing that relationship succeed. This is
not unlike the mentor-mentee relationship. Before selecting a mentor, it’s important to ask who above
you and the mentor is invested in your proposed relationship. If for instance there is a stated
commitment between neurology and emergency medicine at the highest level that developing a stroke
research program is a high priority, and that both specialties want to support collaborative work, that will
strengthen your chances of success. Will your department head or section head be willing to make sure
the mentor fulfills his/her obligation, and will you truly receive the 80% protected time promised to the
NIH in return for your K award? These are important questions to ask ahead of time.
5. Stays focused on your research. A good mentor does not ask a mentee to do other work for him not
related to the research. Look for a mentor who is protective of your research time, and does NOT want
to see you picking up multiple administrative or extraneous projects along the way.

There is additional material, which include helpful discussions about mentorship; they are included in
the references (2, 3). Many investigators find it helpful to have more than one mentor, perhaps a senior
mentor and a junior mentor (e.g. someone who just recently completed their K08 award and recently
received funding for their first R01 NIH grant).
Research as an Investment
Good research is the result of investment, not miracles.
In most of life, we all know that something truly significant does not suddenly result from nothing. If it
does, it’s considered a miracle--not an expectation. Successful research careers are not miracles that
arise out of having no protected time and no support. If you value your sanity and your career, you will
find an academic program that wants to develop a research program through faculty investment rather
than faculty miracles performed during off hours. Successful grant applications (even K awards) have an
expectation that the applicant has already been doing some research, has institutional support to do that
research, and has preliminary results that can be presented as a result of that hard work and support.
Cutting edge research within 3 years is not an unreasonable expectation after being provided 3
days/week of protected time to do research, having at least 1 FTE as a helper to accomplish this
research, with the necessary dedicated equipment, space and supplies to do the work. This may easily
cost $300,000 or more, but could be a very small price to pay if it results in a successful research
career, which has the potential for great value. How much money and time should be invested to create
competitive research which has the potential to attract multiple million dollar grants over the course of
years, and generate excitement about Emergency Medicine at your institution among fellow faculty,
residents, medical students, and perhaps grateful patients and potential donors? Look for a program
willing to invest in your career. Help from a Research Director will not be enough—you need your own
protected time and access to good mentors who have their own independent funding and a track record
of training investigators. Of course, milestones need to be met, but you must have a means to get there.
Agree on what should be expected of you—productivity of manuscripts, K Award applications, R01
applications etc.
The value of a successful research career.

There are unparalleled opportunities for the physician-scientist to fill a unique niche and impact the
course of research today. The reasons are many and are highlighted well by others (4). Advances in
science are taking place at an accelerated rate, and yet fewer physicians are available to ask questions
about how to use these advances to improve the care of our patients. More and more physicians are
electing not to pursue a career in research for multiple reasons, not the least of which include the
financial realities of re-paying student loans, and the imposition of more clinical time due to managed
care and thinner operating margins at academic institutions. This is a most unfortunate pattern, as there
will undoubtedly be missed opportunities to advance medicine if physicians don’t actively participate.
The value of such an M.D. perspective is demonstrated by history: since World War II, about half of the
over 120 winners of the Nobel Prize in Physiology or Medicine have been given to M.D.’s. In addition,
the likelihood of success in getting an NIH grant funded is the same for M.D.’s vs. Ph.D.’s,
demonstrating that M.D.’s are capable of bringing a unique and valuable perspective to the research
table. However, fewer M.D.’s, particularly young physicians, are opting to take on a research career.
Hopefully we as a specialty will continue to work at the national level on this issue and join other
specialties in helping our national leadership to understand what is at stake.
The benefits of a successful research career to your own professional happiness and the excitement
and stability within your own department are incalculable. I love seeing patients; I also love designing
and implementing research projects. Although busy, doing such disparate yet related tasks of patient
care and research can be a lot of fun. Faculty having fun in their work are resistant to burn-out, generate
excitement in a program, and tend to stay. These are big benefits for any Emergency Medicine program.
Grants and manuscripts: monitoring your vital signs
As Emergency Medicine physicians, we appreciate how valuable changing vital signs can be in
monitoring how well or poorly our patients are doing. As researchers, there are also key vital signs
important in following how well our science is doing: They include protected time for research,
presentations about that research, abstracts submitted and accepted, manuscripts, and grant
applications. Monitoring these vital signs is important for a number of reasons. They will be important
ultimately for your promotion. From the start, it will be helpful to know what the promotions committee at
your institution will be looking for when you as a physician-scientist are considered for promotion. Do
NOT wait too long to sit down with your chairman to map out how the promotions process works for
physician-scientists, and what is considered "vital" on your biosketch over time for successful promotion.

Scientific vital signs are also worth discussing with your mentor. If a first-authored paper in a high-
impact journal is weighted more heavily than serving 3 years on a hospital committee which requires
considerable time each month, it’s easier to say no to that committee obligation and clear the calendar
on certain days each week to focus on science. The chairman of the department and the Dean’s office
may also have access to examples of individuals who have been promoted in your track—these can be
helpful to get an idea of what a successful CV looks like. Does the committee evaluate numbers of
manuscripts, position of authorship on papers, the impact score of the journal in which you publish?
Each institution weights things differently; it will be important to know what to expect in your promotions
process. Just as with patients who go unmonitored for hours, failure to monitor scientific vital signs each
year invites bad surprises.
Maintaining these vital signs also ensures that you will remain current in your scientific area of interest,
get feedback about your science, and focus on the most important questions relevant to your research
area. It’s a good idea to search each month and read any manuscripts published in your area of
research interest, and file these electronically or in hard copy in a library. These will be very useful when
putting together your next grant proposal. The phrase "no pain, no gain" definitely applies to scientific
endeavors, and some of the best advances in one’s science happen as a result of good (albeit
sometimes painful) critiques at presentations and constructive rejection of one’s work. When I look back
at the work I am most proud of today, that work was the result of multiple rejections and persistence in
trying to respond to the questions and concerns of reviewers. There will always be some unfair reviews,
but almost always there is some helpful critique. The pink review sheets from the NIH, which critique
submitted grant proposals can lay out in significant detail what you need to do to succeed in your
research. The best part of these reviews is that you don’t have to pay any consulting fees for what may
amount to excellent and career-altering advice. You do however have to submit your work for review
and persist in trying to answer good concerns raised. The only way to get this feedback is to submit
manuscripts and grant proposals.
Research maintenance: finding running partners
There are at least a couple types of research "running partners" that can help make your science easier
and more exciting, and give it a greater likelihood of success. I call them running partners because
they’re the type of people who have some interest and stake in you getting out of bed and succeeding in
your research. They complement you in that if there are some things you do not have the time or

needed skills to do—but nevertheless are important to your work—that they can do. They are people
who will hold you accountable when you agree you will submit a particular grant proposal by a particular
deadline. Two types of research running partners include administrative and scientific. Regarding the
administrative personnel, help is important in identifying grant applications and putting together grant
proposals. First of all, you need to know when grant funding relevant to your science is available. Most
institutions have a newsletter available in hardcopy and/or electronically which highlights internal and
external funding opportunities. Make sure you are on that mailing list. It also may be helpful to talk to the
grant office at your institution, to see if they provide any administrative help in letting you know when
particular grant opportunities matching your research interest become available. This type of "research
dating service" can help identify key funding opportunities. Once grant opportunities are identified, other
administrative help is very important for preparing the non-science components of grant applications—
budgets and their justification, description of personnel, assembling needed letters of support,
description of facilities, institutional grant office review and sign-off. An administrative support person
who helps with these additional aspects of grant preparation can be worth their weight in gold, and save
valuable time, which then can be directed at putting together the science of the grant proposal. They
also hold you accountable for helping to get the needed sections of the grant proposal together in a
timely fashion. Having someone in your department who either has these skills or is willing to learn them
from someone else at your institution could be a great help to you and the department.
The other type of running partner is scientific. It can be exceedingly helpful when colleagues at your
institution and elsewhere know you and your work well enough that they are willing to critique your work
at research meetings, and talk to you and send you emails about articles or grant opportunities they just
read relevant to your work. They are scientists doing work similar enough to your own to make it
worthwhile meeting regularly to discuss each other’s work, and perhaps finding ways to collaborate on
joint projects. Such meetings help you get to know the resources available (either within or outside your
own department) that could complement your work and help advance each other’s science. These are
also people who can preview your work prior to submitting it as a manuscript or grant proposal. I will
never forget the person who served as both a mentor and scientific colleague who helped get my first
manuscript regarding cardiac ischemia/reperfusion started. He ultimately insisted that I and my other
Emergency Medicine colleague come out to his cabin 1 hour outside Chicago without our beepers for
the weekend so that we would be less distracted and more focused, since he had an interest in my work
as a cardiac physiology Ph.D. scientist and wanted to see our work published. He reminded me that it’s
easy to get distracted, and of the importance of having other people around who care whether one’s

work succeeds and stays on track. These people can be found at research meetings and grand rounds.
They can be collaborators or former mentors, or new faculty recruited into your department to
complement and expand the research you are already doing. Such a "critical mass" of research running
partners who actually talk to each other and are invested in each other’s work is important for the long
haul of ongoing science. When those first letters of rejection arrive regarding a manuscript or grant
proposal, these research running partners can be very helpful in getting you back out there to finish the
work.
Our successes.
There are more and more examples of success stories in Emergency Medicine in establishing
independent research. As our specialty continues to mature, it will be important that we learn from each
other what works, and what doesn’t in building research careers. I feel like I have a lot to learn yet, and
hope I don’t make too many mistakes along the way. I hope any of your successes will be reported to
SAEM, so that we can all appreciate what research is being done in our field. I also hope others will
write chapters like this to share their own insights into what they’ve learned. Don’t hesitate to email me
about questions or your own insights after reading this chapter; I would love to hear them:
[email protected]. And have fun with your own career of discovery…
REFERENCES
1. Daloz LA. Effective Teaching And Mentoring: Realizing The Transformational Power Of Adult
Learning Experiences. San Francisco: Josey Bass, 1986.
2. Chin MH, Covinsky KE, McDermott MM, Thomas EJ. Building a research career in general internal
medicine. J Gen Intern Med 1998;13:117-122.
3. Gray J. Mentoring the young clinician-scientist. Clinical and Investigative Medicine 1998;21:279-282.
4. Rosenberg LE. The physician-scientist: an essential--and fragile--link in the medical research chain. J
Clin Invest 1999;103:1621-1626.

The scholarship of integration
E. John Gallagher
In 1922, when T.S. Eliot, who was to receive the Nobel Prize for Literature a quarter of a century later,
published The Waste Land, he was widely criticized for its highly "derivative and unoriginal" features. To
his critics he replied simply: "Good poets don't borrow, they steal." Indeed, Eliot stole with impunity not
just from other works of literature, but also from history, linguistics, religion, music, and philosophy. He
had interwoven allusions to Ovid, Buddha, Wagner, Whitman, Dante, St. Augustine, and Shakespeare,
to list only a few, ending his epic of free verse with a concatenation of fragmentary lines in no less than
five languages. More than a century after his birth, one might argue quite cogently that Eliot, the self-
proclaimed literary thief, was in fact engaged, both literally and literarily, in the scholarship of integration.
Ultimately, his amalgam of seemingly disparate words, disconnected phrases, and diverse ideas, drawn
from a stunning array of sources, was to become one of the most coherent, unique, and enduring artistic
achievements of the 20th century.
Of the four forms of scholarship that constitute the primary organizational axis for this Handbook
(discovery, integration, application, and teaching), that of integration is the most difficult to characterize.
An unfortunate corollary to this is "...of the several forms of scholarly work, the scholarship of integration
has received the least attention." (American Association for Higher Education Eighth Annual Conference
of Faculty Roles and Rewards, February 3-6, 2000. Washington, DC: AAHE.
http://www.aahe.org/FFRR/preview/emphasis3.htm Accessed July, 2001.)
Charles Glassick of the Carnegie Foundation defines the scholarship of integration as "the performance
of serious, disciplined work that seeks to interpret altogether and bring new insights to bear. It is the
capacity to make connections, ... to illuminate... in new and revealing ways... to do scholarship at the
boundaries where fields converge." (Glassick C: How Is Scholarship Rewarded? Address given October
15, 1997. http://www.duc.auburn.edu/administration/horizon/glassick.html Accessed July, 2001.) Thus,
by its very nature, integrative scholarship is difficult to define and recognize. This is presumably
because it operates on the periphery of disciplines at a locus relatively far removed from the central
activity of any one of the several bodies of knowledge upon which it draws.
In the biosciences, the scholarship of integration may encompass work occurring at the edges of two or
more basic sciences, or, more relevant to Emergency Medicine and this Handbook, might bridge the

gap between the basic and clinical realms in a way that is distinct from the scholarship of application.
The latter, which is the trajectory followed by most clinician-scientists, tends to be relatively linear; by
contrast, the scholarship of integration is likely to trace a decidedly nonlinear model of inquiry.
Faculty engaged in the scholarship of integration are rare, not only in medicine, but in other fields as
well. This is not only because comprehension of fundamentally different discipline-specific paradigms is
a prerequisite that is difficult to acquire in the silo structure of traditional academics, but also because
such scholarly activity is considered "risky" to one's career. As Glassick has pointed out:
There is a lack of collaboration in those areas where people develop quantitative measures for
promotion and tenure; that is, ten points for a book and so on. The scholars told us that this leads to
short, safe research projects. They weren't willing to take any chances, and they certainly didn't want to
mess around with other people...(Baird D. Scholarship reconstructed: An interview with Charles
Glassick. Royal Melbourne Institute of Technology University Melbourne, Australia, 1997.)
The scarcity of integrative scholars in Emergency Medicine parallels their low prevalence in other
medical disciplines. Indeed, the Faculty Development Committee was unable to find any academic
emergency physician who felt sufficiently comfortable with the topic to contribute a chapter on the
development of a career in this mode of scholarly endeavor.
Nevertheless, integrative scholarship is extremely important, and is described here by example in the
hope that some young Emergency Medicine faculty may find the concept sufficiently compelling to
explore it further.
Chaos Theory and Nonlinear Dynamic Biological Systems
One example of the possibilities for intellectual satisfaction that the scholarship of integration offers can
be found in the ostensibly implausible link between chaos theory and clinical diagnostic reasoning at the
bedside. Contrary to the conventional meaning of the word chaos, implying complete disorder, the term
is used in mathematics and the physical sciences to describe a specific kind of nonlinear dynamics.
Some recent work in this area has suggested that - contrary to Claude Bernard's longstanding principles
of homeostasis, in which the stability of biological systems is contingent upon their invariance - chaos
theory argues that maintenance of the homeostatic equilibrium characteristic of health may in fact

depend upon continuous, subtle, and apparently erratic fluctuations in baseline state driven by complex
and dynamic interaction between sets of physiologic "oscillators". Data on heart rate variability, which
shows a reduction in normal beat-to-beat variation associated with the onset of serious illness, is
consistent with such an assertion. As a corollary to this, degradation in the biocomplexity of any
interactive physiological system may signal a loss of the internal elasticity needed for an organism to
adapt quickly and efficiently to the broad range of stimuli arising from its external environment. By
extension, clinical bedside diagnosis would then depend upon identification of pathologic states that
decay from the complex interactive variability of health to a simpler, more recognizable kind of
stereotypic linearity, evident to us at the bedside as a pattern of illness. Fortunately, clinicians are not
called upon to make the diagnosis of health - which would be a daunting task, given its biocomplexity -
but rather of disease, which tends to conform to a finite number of less complex and more identifiable
final common pathways.
Much of nonlinearity at first seems counterintuitive because traditional reductionism does not lead to
comprehension of the observed phenomenon, i.e., a meticulous dissection of the component parts of a
nonlinear system may stubbornly refuse to add up. Rather, because many of these components are
"coupled", they are prone to interact in seemingly anomalous ways that do not conform to well-behaved,
linear paradigms. For example, because proportionality is not a feature of nonlinear systems,
remarkably small changes may produce large and unanticipated effects that would not be predicted by a
linear model. Probably the best known example of this is the so-called "butterfly phenomenon", in which
the flutter of a butterfly's wing in, say, Crete produces an almost imperceptible change in nearby air
currents. Over time, these currents alter the state of the proximate atmosphere, extending subsequently
to a distant locale creating, perhaps, a typhoon in the South China Sea, which otherwise might not have
developed. The "butterfly phenomenon" has become a central metaphor for the characteristic loss of
proportionality associated with nonlinear dynamics and "chaos theory".
Descartes’ Error
A second example of integrative scholarship can be found in the dominant theme of a relatively recent
publication, entitled Descartes' Error, by Antonio Damasio, an investigator who has made substantial
contributions to our understanding of the neurobiology of memory and language. Drawing upon prior
work, Damasio provides compelling evidence in support of the interconnectedness of mind and body.
This evidence leads him to conclude that the fundamental error of Cartesian dualism was the axiomatic

assertion that the two are divisible entities. In fact, Damasio argues, their continual interdependent
interaction is fundamental to consciousness and individuality.
Damasio extends his assertions to question a related false dichotomy perpetuated in Neurology and
Psychiatry since the middle of the 20th century. Prior to World War II, these two specialties were
frequently housed under the same academic roof. This conjoint history is reflected today by the fact that
the two disciplines continue to share a single ABMS Board structure (the American Board of Psychiatry
and Neurology). However, as the reigning paradigm for Psychiatry (the mind afflicted by "functional"
illness, dominated largely by psychoanalytic theory) continued to diverge from that of Neurology (the
brain, affected by "organic" disease), common ground eroded, leaving little territory for interdisciplinary
work in psychobiology or neuropsychology. Gradually, as it has become increasingly apparent that
psychiatric disease has a potent genetic and biological substrate, more integrative scholarship is taking
place at the interface between the two disciplines. This has resulted in remarkably salutary
consequences for patients, particularly those with affective disorders. It now seems possible that,
through the scholarship of integration - rather than through further reductionism - we may achieve an
improved understanding and treatment for the most profoundly disturbing and intractable group of
neuropsychiatric illnesses, the thought disorders.
The Compact Disk
Yet another example of the scholarship of integration is offered by Dauphinee and Martin, who borrow it
from the physicist and educator, Geoffery Norman (Dauphinee D, Martin JB: Breaking Down the Walls:
Thoughts on the Scholarship of Integration. Acad Med 2000;75:881-886). It is the story of the
development of the compact disc (CD), which has forever altered the way in which we think about,
transfer, and store information. Norman describes four apparently disconnected discoveries occurring
over widely spaced intervals that ultimately required the ingenuity of scholarly integration in order for the
CD to be "invented":
1. Charles Townes' work in quantum mechanics, for which he received a 1964 Nobel Prize, led to the
discovery of lasers, which read the tiny pits "burnt" into the CD.
2. Einstein's photoelectric effect, for which he received a Nobel Prize in 1921, provided the theoretical
basis for the conversion of light reflected from the CD into electrical signals.

3. Work in semiconductors, for which William Shockley received a 1956 Nobel Prize, led to invention of
the transistor, which made possible the development of integrated circuitry capable of rapid
transmission of complex electronic signals.
4. In spite of this aggregation of 20th century brilliance, there remained the problem of fidelity of data
transfer. The extraordinary amount of information converted from reflected photons into electrons
produced roughly 1,000 errors per second. This problem was solved by application of a redundant
coding system derived from set theory, developed by a French mathematician, Gauloise. This was the
only contribution of the four that did not result in a Nobel Prize. However, Gauloise developed set theory
in the 18th century, and Alfred Nobel did not invent dynamite until the middle of the 19th.
Evidence-based Medicine and The Hierarchy Of Evidence
Finally, and certainly closer to home, the scholarship of integration has been fundamental to the
development of Evidenced-based Medicine. A prototypic example of this is Brian Haynes' pyramid of
evidence, which integrates evidence with bedside care through the marriage of thoughtfully gathered
information with technology (Haynes RB: Of studies, syntheses, synopses, and systems: the "4S"
evolution of services for finding current best evidence. ACP J Club 2001;134:A11-A13). Haynes'
evolutionary hierarchy depicts four tiers of evidence organized in a pyramidal shape. Original studies
published in peer-reviewed journals form the base of the structure. These are followed, in order, by
"syntheses" (systematic reviews or metaanalyses), "synopses" (encapsulations of systematic reviews),
and finally, at the apex of the pyramid, "systems" in the form of computerized decision support systems,
or CDSSs. Individuals who aggregate the information contained in clinical trials (performed by those
engaged in the scholarship of application as clinician-scientists) into critically appraised "syntheses" and
"synopses", to be finally embedded in "systems" that inform everyday clinical decision-making are
functioning as integrative scholars.
Although CDSSs do not yet appear equal to the task of generating a differential diagnosis, their utility
has been demonstrated in drug dosing and preventive care (Hunt DL, Haynes BR, Hanna MA, et al:
Effects of computer-based clinical decision support systems on physician performance and patient
outcomes. A systematic review. JAMA 1998;280:1339-1346). It seems probable that, over time,
increasingly sophisticated evidence-based decision support systems, devised and maintained by
scholars of integration, will come to play an increasingly important role in the provision of care to our

patients and the education of our residents and students.

The Scholarship of Teaching
Choosing Instructional Strategies
Author: Dane Chapman
As professional mentors and teachers of Emergency Medicine, we have come to utilize various
instructional strategies to teach the content and procedural skills of our specialty. Instructional strategy
refers to both the determination of major instructional objectives and the teaching steps used to
optimally fulfill each major instructional objective (1). An instructional system is a prepared set of
instructional materials used to teach instructional objectives according to the instructional strategy for
each objective, using any of a variety of instructional formats such as lectures, small group discussions,
or computer modules.
Instructional Strategies and Instructional Objectives
Two common instructional strategies have been described as the "bucket technique" and the "SOCO"
method (2). Unfortunately the "bucket technique" is still commonly used in medical education and comes
with the assumption that medical school faculty are "all knowing" and that medical student or resident
minds are like empty buckets. The goal of the instructional session is to fill the empty learner "buckets"
with knowledge or "pearls of wisdom" from the faculty. The problem with this method is that it is teacher-
focused, not learner-focused and most often it is associated with the lecture format without clearly
defined, learner-centered instructional objectives. The learner then is expected to regurgitate all the
knowledge in some useful order. Since the knowledge is rarely learned around patient presentations,
recall is difficult when needed in the clinical setting as it has been memorized as a list of facts.
The single overriding communicating objective or "SOCO" method more effectively promotes learning,
Retention, and application of information to new situations. A brief teaching session, such as at the
bedside, might have only one single overriding communication objective (SOCO). A longer session,
such as a Grand Rounds presentation, may have three or four SOCO’s. Such objectives should be
learner-centered, measurable, and appropriate for the level of the medical student or resident. There
may also be "enabling objectives" that must be met before the learner will be able to successfully meet
each single overriding communicating objective.
How Adults Learn

Certain principles of adult learning need to be incorporated into any instructional strategy. Adults learn
best in a supportive environment where they are encouraged and have the opportunity to support one
another. Joining together around a table or bedside with close interaction among all members of the
group facilitates adult learning. Adults especially appreciate teachers who provide learning significance,
ie. the "need to know," and who share the responsibility of learning with the students. By providing clear
goals and objectives, adult learners can "prepare mentally" for the instructional session without hidden
expectations that promote unnecessary anxiety. Adults have a wealth of prior experience that can also
be harnessed and built upon as new information and skills are taught. Adult learners remember best
when they are actively experiencing learning in a problem-based or case-based format, during active,
student-centered instruction with plenty of positive verbal and written feedback. Perhaps these
principles of adult learning are said best in the triplet: "Tell me…I forget; Show me…I remember; Involve
me…I understand." (2).
Studies of learning have demonstrated that only about 7% of information recall is dependent upon the
actual content, and 93% of recall relates to how the content was presented (2). Accordingly,
instructional strategies are most effective when they involve the learner. Since so much of what is
effectively acquired and retained by the learner depends upon how it was presented, principles of oral
communication should be followed closely, especially when using the lecture and small group
discussion formats. The mood for learning can be set by: 1) approaching the class with real excitement
and enthusiasm, 2) adding vocal variety for interest and clarity, 3) including purposeful pauses, 4)
maintaining effective eye contact with each learner throughout the presentation, 5) showing a desire to
communicate without over-dependence on notes, 6) actively involving the learner and, 7) ending using a
strong conclusion with vitality! Being enthusiastic in the presentation is key to effective oral
communication. Compared to written communication, oral speech has more personal references, more
first and second person pronouns, shorter length of thought units, greater repetition, more mono syllabic
words and more familiar words (2).
Instructional Strategy and Teaching Steps
Nine teaching steps or "events of instruction" have been described in the educational literature (1).
These provide the framework for teaching in the classroom, small group discussion or when developing
an instructional system to be adapted as an interactive computer module or simulation (See Table 1).

Utilizing these "events of instruction" or teaching steps gives the mentor or teacher an organized
instructional strategy for optimally transmitting knowledge and assessing competency.
Step 1: Gaining Attention
Gaining attention techniques clearly vary with the type of audience and level of training of the learners.
Techniques include appealing to some learner interest, simply pausing until learner attention has been
obtained, using humor, or asking a question like: "Who wants to learn how to save a life by performing a
cricothyrotomy?"
Maintaining attention is also a key instructional strategy which can be achieved by changing the media
or nature of the activity, referring to a longer-term goal, or referring to an overview or outline to help the
learner keep perspective of the big picture. A sudden change of plans is a useful technique for gaining
or maintaining attention, because it allows the teacher the opportunity to seize upon an unexpected
happening that could illustrate an instructional objective.
Step 2: Goals and Objectives
Informing learners of the instructional objective is only fair as it helps focus students and residents and
guides them through the information or skill to be learned. When defining goals and objectives, the
distinguishing characteristic between them is that a goal is a general statement about what is to be
accomplished in an instructional session. Objectives, however, are statements used to identify key
instructional outcomes and must be measurable in order to determine whether or not they have been
met. Instructional objectives state what the learner will be able to do at the end of the presentation and
are best provided in behavioral and learner-centered terms, appropriate to the learner’s level of
knowledge or skill, and achievable in the time allotted for the learning. Objectives are constructed by
considering what the learner will do, not by focusing on what the teacher will present to the learners.
The key to developing instructional objectives is to complete the sentence, "By the end of this session,
the learner will be able to…."
A goal example would be: "The goal of this chapter on instructional strategies is to enable faculty to
develop their own successful instructional systems, whether lectures, small group, or computer-
assisted, that incorporate adult learning principles."

An objective example would be: "After reading this chapter on instructional strategies, faculty will be
able to: a) formulate the goals and objectives for their own instructional system, b) select an appropriate
media format for presentation, and c) organize the instructional system to include the nine events of
instruction."
Formulating the goal and instructional objectives is considered by some to be the first step in effective
teaching, and occurs during the planning stage of instruction. During the actual teaching sessions,
faculty implement their objectives. Finally, after the teaching session, faculty should assess whether the
instruction has enabled learners to meet the stated objectives. This is also a good time to make notes
about what went well and what needs to be revised in the presentation while learner comments and
performance feedback are fresh in mind. The two most common reasons for failing to meet instructional
objectives are insufficient framing of objectives and misjudging of learner’s prerequisite knowledge level
(2-4).
Step 3: Stimulating Recall of Prerequisite Learning
Stimulating recall of prior learning is especially important for complex knowledge or skills that are built
upon simpler knowledge or component skills. For example, before thoracotomy procedural skills can be
taught effectively, learners must be able to recall important prerequisite anatomy of the thorax (5). The
best instructional systems build upon common knowledge or skill(s) that can be easily recalled by the
majority of learners in the class or group. With that level as the starting point, new information and
skill(s) can be readily integrated, and remembered.
Step 4: Presenting the Stimulus Material
The nature of the stimulus presentation depends upon the type of learning (i.e. facts to be memorized,
rules to be understood, problems to be solved or procedures to be performed). It is best to present only
5-10 paired associates (eg. surgical instrument picture and name) to be memorized at a time. When
presenting information that has order or a relationship, it is useful to provide the learner with the
organizational framework or "advanced organizer" so that the information can be organized in a
meaningful way, aiding both initial learning and later recall (1). Patient presentations serve as a useful
structure for organizing many discrete facts that would otherwise be difficult to recall. When facts are
memorized around a patient presentation (eg. signs and symptoms), learning and recall are facilitated.
Learning can be further facilitated if the presentation includes periodic review or summary statements,
with pacing for interactive questioning and corrective feedback.

When presenting discriminative tasks such as distinguishing congestive heart failure (CHF) from an
acute exacerbation of chronic obstructive pulmonary disease (COPD) in a patient presenting with acute
shortness of breath, the distinctive features of each disease should be pointed out to the learner. Once
the distinctive features are formalized into rules, learners can practice their understanding of the rules
when presented with novel examples for practice and corrective feedback (eg. new patients with either
CHF or COPD).
Step 5: Providing Learning Guidance
Some medical students and residents become more engaged in their own learning when they are given
a problem, and asked to "discover" the solution. Learners tend to remember well what they discover in
this manner because their learning has been an "experience" (ie. experiential learning). When medical
students and residents are assigned to see patients with diseases not previously encountered, they
typically use discovery learning. While this strategy of learning promotes attention and interest among
learners, it can also result in frustration and is a rather inefficient method for learning. The axiom,
"experience is a great teacher, fools will learn in no other way" illustrates this point. If we fail to learn
from another’s experience, we are left to discover truth for ourselves. Faculty can provide various
degrees of guidance through the discovery learning process in order to decrease learner frustration and
make the learning session more efficient. One of the downfalls of problem-based learning (PBL), a form
of discovery learning, is that students do not learn as much information as medical students using a
traditional curriculum. Yet, what they do learn can be better applied to the clinical environment. Learning
is often better retained and generalized to other clinical presentations when instruction follows the PBL
format.
In summary, providing learning guidance by direct prompting is useful for rote memorization. For rule-
using and problem-solving, learning guidance can be provided using a hint or indirect prompt at first,
gradually increasing the directness of later prompts until learners successfully solve the given problem.
Specific types of faculty providing learning guidance for various types of learning (1) are presented in
Table 2.
Step 6: Eliciting the Performance (Formative Evaluation)
After the instructional session using lecture, small group or individualized instruction with a book or
computer simulation it is necessary for learners to demonstrate that they have learned the key concepts
or skills presented. If lists of facts are taught, students and residents should be able to regurgitate the
facts either orally or in writing. If rules or algorithms (e.g. clinical pathways) are presented, then novel

cases can be given to determine whether or not the learner can demonstrate the appropriate application
of the rule. True understanding of a rule requires the demonstration of skills using examples that are
"new" to the learner In order to be sure answers to a few previously given examples have not just been
memorized. For example, if a clinical pathway on the diagnosis and management of acute shortness of
breath had been taught and illustrated using various examples of patients with congestive heart failure,
acute asthma exacerbation, or pulmonary embolism during the instructional session, then, new patient
presentations with these same diagnoses would need to be presented to elicit "rule using" performance
by the medical student or resident. Likewise, when eliciting problem-solving, problems not previously
presented to the learner must be used to determine if problem-solving mastery has occurred.
Regardless of the domain of learning (i.e. cognitive, affective or psychomotor), eliciting the performance
is an important instructional step to assure the learner and teacher that learning has taken place (i.e.
formative evaluation). Otherwise, additional instruction is required to develop competency before the
formal test of mastery occurs (i.e. summative evaluation). For example, in the psychomotor skill
domain, performance of component critical procedural steps need to be elicited separately (e.g.
"opening the chest", pericardiotomy, aortic cross-clamping) (formative evaluation) before the entire skill
(e.g. thoracotomy) is assessed by a test (summative evaluation) (5).
Step 7: Providing Feedback
After the performance has been elicited, learners must receive feedback to know whether it was
performed correctly. This is a key step in learning. Without corrective feedback, learning rarely occurs.
Feedback follows formative evaluation but not summative evaluation. When a performance is only partly
adequate, feedback will help the learner define exactly where additional study or practice is needed.
Step 8: Assessing Performance (Summative Evaluation)
Eliciting the performance (formative evaluation) with corrective feedback may be done several times in
the sequence of learning a single instructional objective. In contrast "assessing" performance is done
only after the learning and instruction have been completed for the entire objective. When assessing
performance, the assessment instrument must be reliable and valid. Since high stakes decisions—eg.
passing a course, graduating from medical school or advancing to the next year of residency—are made
based upon the "assessment", these summative evaluation instruments must be psychometrically
sound. A test is reliable if the results are reproducible or internally consistent. For example, if four
questions on a given test assess the same content area such as acute coronary syndrome, a highly
reliable (internally consistent) test would result in learners responding to all four questions similarly—(ie.

those missing one would likely miss all four, those answering one correctly would likely answer all four
correctly).
Summative assessment instruments also need to be valid—meaning that they are measuring what they
are purported to measure. Resident performance on a valid test of cricothyrocotomy (eg. on a cadaver
model) would be predictive of whether or not the learner would be competent in performing a
cricothyrotomy upon an actual patient in respiratory distress following a failed intubation. Validity can be
measured by correlating the test with actual performance, where a high correlation represents the
presence of validity.
Step 9: Enhancing Retention and Transfer
The last "event of learning" or "teaching step" is to help learners generalize and transfer what they have
learned to new situations. The more learners are able to practice what they have learned, the better
they will recall isolated facts, organized information, or skills. Moreover, as learners apply what they
have learned to a range of practical situations, they are more likely to retain that knowledge or skill.
In medicine, experts in clinical decision-making use pattern-recognition and decision-making algorithms
and clinical pathways, rather than the more mentally taxing hypothetico-deductive reasoning process
(6). As a result, discrete facts previously memorized about particular diseases are often forgotten by the
expert who easily retains the ability to diagnose and manage patients efficiently, but must struggle to
maintain "the edge" in factual recall. Clearly organized information or information memorized around a
structural framework like rules or algorithms are easier to recall and transfer to new situations than are
isolated facts. Psychomotor skills like critical emergency medicine procedural skills are easily retained
once sufficiently practiced. Yet, it remains unclear how many procedures must be performed to achieve
mastery. There is some evidence to suggest that 10-12 procedures performed correctly may be a
sufficient number to achieve mastery of complex psychomotor procedural skills like emergent
thoracotomy and cricothyrotomy (7). It is less clear how frequently such procedures must be performed
to maintain skill proficiency (7,8).
Optimizing Instructional Formats
This section addresses the pros and cons of various instructional formats of lecture, small-group
discussion, workshop and individualized instruction.
Lectures

Lectures are one of the most efficient of all teaching formats where large numbers of learners can
receive instruction simultaneously. Unfortunately, one of the greatest determinants of whether
knowledge is acquired depends on the degree of interaction between the learner and the teacher (2).
Using this format, it is difficult, but not impossible, to involve the audience effectively (2-4). The
instructor can for example, direct questions to the audience throughout the lecture, use handouts with
questions to be answered during the presentation, and roleplay (3,4). An effective method is to organize
medical information around a meaningful case that can then be applied directly to the clinical
environment. Too often medical information is discussed during medical school as lists of facts without
much thought to how the information could be used to help diagnose a patient’s problem.
Information not organized around a patient’s presenting signs and symptoms is much more difficult to
learn and to retain. Accordingly, good lectures often begin with an interesting unknown case that
illustrates some aspect of the content to be discussed in the body of the lecture. As the case unfolds,
decision points can then be amplified and differential diagnoses discussed with special attention being
given to those distinguishing signs, symptoms, or diagnostic study results that differentiate the correct
diagnosis from a long list of differential diagnoses that have some of the same signs, symptoms, and
diagnostic study results in common with the correct diagnosis.
The downside of lectures is primarily the difficulty in actively involving the learner throughout the
presentation (2). The learner has a special challenge of maintaining attention and it is quite easy to fall
asleep during lectures when the lighting is turned down for slides. The instructor typically does not
engage learners with enough interaction to keep all learners attentive and interested. However, when
the instructor is engaging, lectures can be very effective (3,4).
Small Group Discussions
The optimum size for small group learning has been found to be a maximum of twelve learners per
group (2). Twelve or fewer learners can interact reasonably well with a single instructor such that all are
kept involved and engaged in active learning. The disadvantage of small group learning is that it
requires more teachers or discussion group leaders than the lecture format. However, if the instructor
can train one or more group members to be group facilitators, then this is a very effective method of
teaching. Focus groups utilize this method in discovery learning to create a solution to a common
problem. The small group format is also optimal for teaching procedures.
Small group discussions have been used successfully in medicine in the form of medical and surgical
attending rounds. A patient presentation is given that forms the basis for instruction. Using this case-
based approach, medical educators have successfully taught trainees to memorize common

presentations or "disease frames" that can later be drawn upon to make diagnostic and therapeutic
decisions (6,9). Key elements of the small group method are interactivity and involvement of the learner.
Workshops
Workshops typically include both lecture and small group break out sessions to take advantage of the
efficiency of the lecture format in presenting facts, and the small group discussion format in teaching the
application of those facts presented during the lecture session. For example, the latest development in
anti-platelets, thrombolytic therapy and cardiac catheterization could be presented in a Grand Rounds
lecture format, with break-out sessions directed toward the application of principles learned to novel
cases presented in a small group format. Typically, workshops provide a standard learning exposure for
a limited content or skill area that can be fully presented in 2-5 hours.
A sample workshop for faculty development was recently undertaken to enhance the questioning skills
of faculty and residents (3). A basic discussion of thinking skills and a review of various types of
questions is presented in a lecture format. Next, in small groups, participants critique previously
produced videotape vignettes that demonstrate good and poor questioning techniques. The workshop
concludes with a paper case where participants are able to apply what they had learned by writing
questions directed toward different levels of learning . These are then discussed in a larger, combined
group interactive forum.
Computer-Assisted Instruction (CAI)
CAI can maximize learner involvement, which translates into more active learning and better retention of
information or skills presented. Learners have the advantage of learning when they feel most like
learning—provided they have access to the CAI systems. The CAI format maximizes interactivity, but
falls behind the lecture and small group format in efficiency. A combination of CAI and small group study
has been shown to optimize both methodologies and learners appear to learn better from CAI when
they study in groups of 2-3 rather than alone (9).
Becoming the Optimum Teacher
Instructional strategies provide a useful framework for any form of instruction and involve clearly
defined, learner-centered instructional objectives and teaching steps. Principles of adult learning have
been presented as they relate to instructional strategies. However, application of these principles alone
will not allow us to become the best teachers that we can be. To become our best teacher is to discover
the teacher within us, to be who we really are, to be ourselves (10). As we are more willing to be

ourselves in front of our medical students and residents, willing to admit our weaknesses and
inadequacies, learners will respond to our humility with their own willingness to learn. They will feel a
genuine respect for us because they will know that we care more about them than we care about our
reputation or our image. Such high regard for students triggers similar feelings in return. Ample
research has demonstrated that when students value their teacher, their commitment to learning is
enhanced (10).
In contrast, when teachers are more concerned about their own image in front of the group, they
insulate themselves from personal involvement with their students’ lives. To them, the teaching role is
defined solely in terms of the teacher’s performance. Such teacher-centered faculty will find that the
greater they try to control their students or residents, the more superficial will be learner commitment.
The more they try to motivate, the less motivated learners will become. The more elegant their lectures,
the more sporadic will be the attendance (10).
Learner-centered teachers humble themselves before their students and unpretentiously perform the
highest form of teaching. They use instructional strategies to serve and uplift, not to control or
manipulate. They engage the learner in a mutual obligation to learn and they worry less about being
seen as "experts" or "authorities." Learner-centered teachers place learners in control of their own
learning, serving as facilitators of the instructional session. As academic pride is stripped away, such
teachers humbly influence students’ lives for good and become master teachers (See Table 3). Master
teachers focus upon the students’ need to learn well rather than upon their own need to teach well. May
we each allow ourselves to be such teachers as we discover the teachers within us!
TABLE 1: INSTRUCTIONAL STRATEGY TEACHING STEPS TO OPTIMIZE LEARNING
1. Gaining attention of learner
2. Informing the learner of the objective
3. Stimulating recall of prerequisite learning
4. Presenting the stimulus material (new content, skill, etc.)
5. Providing "Learning Guidance"
6. Eliciting the performance from the learner
7. Providing feedback to learner about performance correction
8. Assessing the performance
9. Enhancing retention and transfer of content or skill learned

TABLE 2: LEARNING GUIDANCE APPROPRIATE FOR VARIOUS TYPES OF LEARNING*
Type of Learning Outcome
Form of Guidance to Learning
Discrimination Point to distinctive features of objects to be discriminated
Concrete Concepts Give cues to identifying attributes
Defined Concepts Provide codes or memory bridges
Names and Labels Provide codes or memory bridges
Facts Provide meaningful context
Organized Knowledge Provide prompting in context of the organizational framework
Rules Show how component concepts make up the rule
Problem-Solving Provide minimum cues needed to lead learner to select and apply applicable rules
Motor Skills Stimulate recall of sequence of acts; provide practice with feedback
Attitudes Establish respect for human model; show his behavior and how he is reinforced
*adapted from Briggs, 1977, page 211.
Table 3: The Master Teacher*
Invites rather than compels
Acts in the best interest of students, leading them to truth and clarity, and away from confusion
Focuses on residents as individuals, not on content or skill being taught
Teaches out of high regard for the student rather than from duty
Identifies the life demand or driving force that will motivate residents to receive truth
Has traveled the path so can help refine an idea, polish a skill, and give honest feedback; but, is sensitive to each residents’ limit to handle the feedback
Is okay with guiding students to the correct path and letting them discover the solutions themselves
*Adapted from Osguthorpe, RT. The Education of the Heart. Covenant Communication, Inc, American Fork, UT, 1996, pp 83-101.
Acknowledgements
I would like to acknowledge Debra Palecek for her wonderful help in preparing this manuscript almost
single handedly.
References
1. Briggs, LJ. Designing the strategy of instruction, Chapter 7 in Briggs, LJ (ed) Instructional Designing

Principles and Applications, Educational Technology Publications, Englewood Cliff, NJ, pp 179-218,
1977.
2. Kelliher, GT, et.al. Effective Teaching: Improving Your Skills. Workshop presented by the Office of
Education, Medical College of Pennsylvania/Hahneman University. June 3-7, 1996.
3. Sachdeva, AK. Use of effective questioning to enhance the cognitive abilities of students. J. Cancer
Education
4. Kelliher, GT, Sachdeva, AK, Fleetwood, J. Preserving the best of the art of teaching. Acad Med
1996;71:248-250.
5. Chapman, DM, Marx, J, Honigman, B, et al. Emergency Thoracotomy: Comparison of medical
student, resident and faculty performance written computer and animal model assessments, Acad
Emerg Med 1995;1:373-381.
6. Chapman, DM, Char, DM, and Aubin, C. Clinical Decision-Making, Chapter 10 in John A. Marx
et.al.,(eds). Emergency Medicine: Concepts and Clinical Practice (5th Edition), Mosby Publishing Co,
2001.
7. Chapman, DM and Cavanagh, SH. Using receiver operating characteristics (ROC) analysis to
establish previous experience for critical procedural competency. Acad Med1996;71:57-59.
8. Long, DM. Competency-based residency training: The next advance in Graduate Medical Education.
Acad Med 2000;75:1178-1183.
9. Chapman, DM, Calhoun, JG, Davis, WK, et al. Acquiring clinical reasoning competency: Group
versus individual practice using patient management computer simulations. Acad Emerg
Med1997;4:511-512.
10. Clark, DC. The Teacher Within: A Voyage of Discovery. Orem Utah: Granite Publishing and
Distributing, 2000 pp. 17-23.


The Educator's Portfolio
Author: Gloria Kuhn, D.O., Ph.D., FACEP
The Educator's Portfolio (also known as a teaching portfolio or teaching dossier) is a tracking device for
collecting materials that document and demonstrate excellence as an educator. The Portfolio can serve
many different functions in its capacity for demonstrating teaching expertise. This article will discuss the
many uses of the portfolio, creating a portfolio, and finally how to create a portfolio that can be submitted
to a Promotion/Tenure (PT) Committee.
Uses of the Educator's Portfolio
Promotion and Tenure
Many institutions are using the Portfolio in the P&T process. This enables the P&T Committee to see,
and therefore, judge, the accomplishments of a faculty member applying for promotion. Faculty
members frequently forget to record the many and varied educational activities in which they have been
engaged over the years of their career or they may not feel that the activities are "important" enough to
record. They cannot subsequently include supporting materials about these activities in a file that is
submitted to a P&T committee. While these activities may not have great weight individually, in
aggregate they reveal the many and varied talents of the educator and the valuable role that the
individual plays in the growth of the institution. Because the Portfolio provides an ongoing methodology
for collecting materials as they are generated, preparing a document for a P&T committee is easier,
faster, and more accurate. Trying to remember past activities and collect documentation at the time the
decision is made to apply for promotion leads to frustration and a sparse file that cannot represent the
value of the educator fairly.
Evaluation
Department Chairs can use the Portfolio when performing periodic evaluations of their department
members. The Portfolio aids the faculty member and Chair to put past accomplishments in perspective
when used for this purpose. Future goals and activities can then be planned which will build upon the
knowledge gained during past activities. It aids the Chair in determining the productivity of department
members and in generating a report to the Dean of the productivity of the whole department. From the
perspective of the faculty member it makes preparing for periodic evaluations very easy as all of the
material is already assembled.

New Positions
The faculty member can use the Portfolio when applying for a new position to demonstrate scholarly
accomplishments and experience. This was the original purpose of portfolios as used by artists and
architects to display his/her best work to a potential patron or client. Many teachers use the Portfolio
they have assembled when looking for a new job or applying for a promotion. One of the most valuable
uses is to assist a faculty member in rapidly updating and keeping current his/her curriculum vitae, an
activity that is necessary for any application.
Reflection on Teaching
Many of those who have assembled a Portfolio have stated that it has aided in their growth as an
educator. The very act of looking at past accomplishments and activities has led them to examine what
actions have been successful and why, what they would change in the future, and what direction their
career has taken. This act of self-reflection often results in growth as a teacher and leads to a higher
level of ability. Educators who have assembled Portfolios state that when instructional activities have
been less than successful the Portfolio has helped to make this apparent to them. They then have had
the opportunity to devise methods that have proven more successful in accomplishing their teaching
goals. It has been argued that this reflection-on-teaching and the resultant growth in ability as an
educator is the most valuable aspect of the Portfolio.
The Portfolio as Incentive and Reward
Most educators in medicine are highly motivated. They do not wish to have an empty Portfolio. The very
existence of the Portfolio acts as an incentive towards accomplishing goals. The self-reward occurs
when the educator is able to look at past activities and see the many accomplishments and career goals
that have been attained.
Creating the Educator's Portfolio
The contents of the Portfolio will vary because of the many activities in which educators are engaged.
One of the easiest ways to create a Portfolio is to use a tabbed three-ring binder. The Portfolio should
contain the following sections: 1) Activities, 2) Philosophy of Education, Accomplishments, and Future
Goals, 3) Recognition of Excellence and, 4) Courses and Study to Increase Expertise as an Educator.
The materials gathered for each of these sections will be highly individualized to reflect the activities of
the educator. It is critical to determine if your institution has guidelines on how the portfolio should be

structured so that you can follow them.
The Activities Section should include the educational activity, any materials generated as a result of the
activity, and any evaluations by peers or learners. Examples of activities might include courses taught,
lectures given, a list of students advised, committees or panels upon which the educator was asked to
serve, and any clinical supervision given to medical students or residents. Publications and authored
educational materials such as educational software may be included in this section. It is important to
remember that many institutions require national and even international recognition for promotion to full
professor. Educators may want to have separate areas in their Activities Section for national and
international endeavors.
The section dealing with your Philosophy of Education may be the hardest to generate. But doing this
early in your career will pay huge dividends in the future. The end of the academic year is a perfect time
to look through the contents of the Activities Section and reflect on what has been accomplished and
what still needs to be done. At this time, it is relatively easy to write a short statement as to how you feel
you can best teach, what motivated the activities in which you were engaged, what value you feel these
had to the institution, how these activities implemented your philosophy of education, and what your
future goals are (place a copy of the lithe list of goals for the coming year in a new Portfolio which will be
filled in the coming academic year). The discussion should only take a few pages but it needs to
articulate your beliefs and activities as an educator. This statement is then placed in the Philosophy of
Education Section. This is also a good time to look at both activities and evaluations to determine if they
are in line with your career goals. This section should be re examined periodically so that it can be
modified to reflect changes in your teaching philosophy and methods. It is this re examination that
allows for "reflection upon action" which is so important for expertise in an area to develop. In fact, many
who have studied the use of teaching portfolios consider this act of reflection to be the most important
use of the portfolio.
The Section for Recognition of Excellence will depend on how you have been recognized during the
year. Include any awards or honors, whether national, local, or institutional. Recognition by residents
and medical students for excellence in teaching is of great value. Do not forget to include any thank you
letters received as a result of educational activities from course directors or students you have
supervised, mentored, or advised. While these are not formal awards, they document your excellence in
teaching from a variety of sources.

Listing self-study and formal courses taken to increase your expertise in teaching is of great value. It
demonstrates your commitment as an educator and the credentials you have accumulated in the area of
education.
Generating a Portfolio is of most value when the contents are kept for future use. All of the materials
collected during the academic year is saved, either in a file or the three-ring binder, and a new Portfolio
is begun for the new academic year.
Preparing a Portfolio for the P&T Committee
The first step should be to examine the contents of the Portfolios that you have archived. Read the
statements you wrote for the Philosophy of Education Sections and then spend some time thinking
about your accomplishments, your goals, and how your activities and actions have benefited your
students, residents, and the institution.
After this reflection you are ready to begin preparing a Promotion Portfolio. Include the activities that you
feel best represent your accomplishments. Compose a narrative of three to eight pages that discusses
your philosophies, your accomplishments, your growth as an educator, and activities of which you feel
proud. You can include tables or graphs that display your successes. Include samples of educational
materials you have generated in labeled appendices. Make it easy for the members of the P&T
committee to understand what you wanted to achieve and how you went about ensuring your success in
these endeavors.
It is often of value to ask someone who has prepared a Promotion Portfolio to look at your Portfolio and
give you advice. You may want to ask members of your Departmental Peer Review Committee to look
at the Portfolio prior to its official submission to them to see if there are any suggestions as to contents
or format. Use their suggestions to strengthen the document. You may want to let some time pass and
reexamine the Portfolio to be sure that it is complete, reflects your best work, and adequately represents
you as an expert educator.
Finally, pretend that you are a member of the P&T committee of your institution and that the Portfolio
belongs to a stranger. Is it easy to read and does it demonstrate expertise? Is it the Portfolio of

someone whom you feel deserves promotion? If the answers are "yes", submit it. If the answers are
"no", keep working.
The following references are recommended if you would like to learn more about Portfolios. Those that
are starred show examples of Portfolios. The examples they contain are varied and demonstrate the
creativity used to document expertise.
Recommended Bibliography
1. Beasley, B., S. Wright, et al. (1998). "Promotion criteria for clinician-educators in the United States
and Canada." JAMA 278(9): 723-8.
2. Beecher, A., J. Lindemann, et al. (1997). "Use of the educator's portfolio to stimulate reflective
practice among medical educators." Teaching and Learning in Medicine 9(1): 56-9.
3. Carroll, R. (1996). "Professional development: A guide to the educator's portfolio." Am J Physiol
271(6P&T 3): S 10-13.
4. Roth, L. (1998). "Teaching portfolios: Reflecting upon and improving teaching." J Cancer Educ 13(4):
194-6.
5. Seldin, P. (1997). The Teaching Portfolio. A practical guide to improved performance and
promotion/tenure decisions. Bolton, MA, Anker Publishing Company Inc. *
6. Shulman, L. (1990). "The Educator's Portfolio." Presentation at Conference on Assessment in Higher
Education.
7. Simpson, D., A. Beecher, et al. (1998). The Educator's Portfolio. Milwaukee, WI. Medical College of
Wisconsin. *
8. Speer, A. and D. Elnicki (1999). "Assessing the quality of teaching." Am J Med 106(4): 381-4.
9. Zubizarreta, J. (1999). "Teaching portfolios: An effective strategy for faculty development in

occupational therapy." Am J Occup Ther 53(1): 51-5.

Developing a Career in the Scholarship of Teaching as a Clinician-Educator
Author: Stephen R. Hayden
Introduction
Clinical bedside teaching is nothing new. It was Hippocrates (circa 400 BC) who abandoned temple
based medicine for a practice that valued direct observation, the exact recording of the features of
disease, and adherence to the principal that "You must go to the bedside, it is there alone that you can
learn disease." In his address to the New York Academy of Sciences, Sir William Osler stated that there
should be "No teaching without a patient for a text, and the best teaching is that taught by the patient
himself." Despite this legacy there has been gradual erosion in time spent teaching at the bedside.
Thirty years ago over 75% of medical teaching occurred at the patient's bedside. Several authors have
recently examined the time devoted to attending rounds on inpatient medical services. They estimated
that only 16 - 20 % of the time devoted to attending rounds was spent in the presence of the patient. In
other studies using direct observation or videotaping it was found that the average time spent at the
bedside was only 2 - 3 minutes compared with approximately 60 minutes in the classroom. In 25 % of
instances teachers never saw the patient at all, whether during the case presentation or afterward.
Although a number of studies have shown that approximately 85 % of patients preferred bedside
rounds, only 35 % of attending physicians did so, 4 % of students, and 2 % of house staff.
The emergency department (ED) has always been regarded as a rich environment for clinical teaching
with the wealth and diversity of diseases that present to our doors. Yet most academic emergency
physicians are experiencing intense pressure from external sources to improve the efficiency,
documentation, and cost effectiveness of emergency medicine (EM) practice. I have heard many of my
colleagues lament that this results in less time for teaching residents and students in the ED. If you
believe that the best teaching occurs in the doctors workstation, conference room, or lecture hall then it
is understandable that you would feel this way. I'm going out on a limb here, however, and suggesting
that recent external forces that require attending EM physicians to personally see and examine all
patients in the ED may be the best thing that has happened to clinical teaching in EM. We have been
handed a golden opportunity. As a faculty physician you now need to be there anyway, take a resident,
or student, by the hand and lead them with you back to the bedside where a multitude of teaching
moments can occur.

In this chapter we will discuss characteristics of good clinical teachers, perceived obstacles to effective
bedside teaching, strategies to overcome them, the components of good bedside teaching, and a
number of practical models to use in clinical instruction.
Characteristics of Good Clinical Teachers
There are a number of characteristics that great clinical teachers in medicine share:
Teachers are knowledgeable
Presentations are clear and well organized
They are enthusiastic and able to interact skillfully with students and residents
Provide simultaneous teaching and clinical supervision
Demonstrate clinical skills to learners
Model professional characteristics
Good clinical teachers also display numerous intangible qualities such as:
Being available
Being approachable
Having infinite patience
Staying calm in difficult situations
Osler described this as equanimity, and suggested "In the physician or surgeon no quality takes rank
with imperturbability."
Superb clinical teachers also use effective teaching skills including:
Explaining concepts at the learners level

Providing timely feedback
Modeling their behavior for students
Illuminating how their thought process works
Instructing in small digestible "teaching bites"
Guiding learning with questions
This last item bears repeating: Good clinical teachers guide learning with questions. This means asking
questions that require synthesis and interpretation of information and evidence rather than simple
regurgitation.
Examples of such high yield questions are:
Why do you believe that to be true?
How did you reach that conclusion?
What lead you to that decision?
Why is X approach better than Y?
Why is that information important?
What will happen if you don't do X?
What is the association between X and Y?
Obstacles to Effective Clinical Teaching
Concern for the Privacy and Well-being of the Patient
The argument is often made that to present case histories and physical findings in front of patients, and
possibly their families, would prove embarrassing or uncomfortable to them. On the contrary, the
available evidence suggests that patients are in fact appreciative of the attention being devoted to them
by so many health-care professionals. When conducted tactfully and empathetically bedside
presentation is not a traumatic emotional experience but rather educates and reassures patients. The
overwhelming majority of patients feel that they understand their illness better and have a better
opportunity to get their questions answered. Patients want the attending physician to introduce
themselves, to state the purpose of bedside rounds, and to be sensitive to the need to translate medical

jargon into terms that they can understand.
Medical Chauvinism
Some doctors believe that it is not appropriate to involve patients in the process of making major
decisions regarding their health-care. Consequently this may be responsible for moving case
presentations and discussions away from the bedside. These physicians also do not want to display
weaknesses in front of patients or families in discussing their own problems associated with data
collection, interpretation, and synthesis. Again, the available evidence would indicate that active
involvement of the patient, as well as the patients observation of our deliberations, can lead to an
honest, open, and mature doctor patient relationship where both the physician and patient assume
appropriate responsibility for decisions made.
Passive View of Education
Here the old idiom that education is the transfer of knowledge from teacher to student is applicable. This
view purports that teaching on rounds means a series of mini-lectures by the attending on topics that
happened to arise, often followed by a more lengthy discussion in the doctors workstation, conference
room, or classroom. Trainees support this arrangement since it requires little active work on their part
and conforms to their prior educational experiences as passive listeners in a lecture hall. They are used
to the doughnuts and coffee, the comfort of sitting around a conference table or at a work desk, and the
cloak of early morning or post-meal semiconsciousness. In order to combat this, the skilled emergency
medicine faculty will know how to actively engage the student or resident by guiding learning with
appropriate questions. The attending facilitates group or individual learning by assisting the trainees to
discover for themselves the important clinical issues and develop a strategy to solve the clinical
problem.
Emergency Medicine Faculty Discomfort at the Bedside
Many teachers are uncomfortable discussing subject matter in which they feel less than expert. The
bedside is avoided where the reality of the patient's situation or difficult questions might draw them on to

intellectually thin ice. They prefer the workstation, the conference room, or even worse the hallway,
where they can turn the discussion to subjects with which they are far more comfortable. There will be
no patient and no family in attendance to ask embarrassing questions that force us to say, "I don't
know." Furthermore, there is our discomfiture with physical diagnosis. All of these barriers may be easily
overcome. Create a safe and comfortable environment for asking questions and discussing answers.
Become comfortable with saying, "I don't know but here is how we will find out." If you don't know the
answer to a specific question, tactfully turn the question to other members of the group. If none of the
group members know the answer, then an individual may be assigned to search for the answer. Such
questions generated at the bedside during the course of patient evaluation and care are the most useful
and relevant questions for teaching purposes; encourage rather than avoid them. Even without specific
expertise with the particular disorder presented, other skills may be taught at the bedside, including
history taking, demonstration of interpersonal skills, and teaching trainees to be skilled observers. The
bedside teacher's role is transformed into one that focuses attention and generates clinical inquiry.
Lack of Interactive Skills
Faculty physicians themselves may be uncomfortable interacting with certain types of patients. This may
be especially true in the emergency department. In fact some studies have found that most teachers go
to the bedside only to check on abnormal physical findings. As a consequence, bedside time may be
kept to a minimum and trainees may lose the opportunity to observe an experienced clinician in action
with the patient.
Social learning theory emphasizes the learning that occurs by observation and imitation of role models.
From this viewpoint, the quality of the interaction between the attending physician and the patient is
likely to be imitated by the resident in interactions with their own patients. Faculty should practice what
they preach and model the kind of communication patterns they expect residents to use with patients.
Bedside teaching fosters a wonderful link with the past. Trainees watch you as carefully as does a child
his parent; they watch you attend to the patient, watch you observe. They observe your powers of
diagnosis, the respect you hold for other human beings, your attitude, and your caring. Students witness
your own dignity, and the love and enthusiasm you have for medicine and teaching. And so true
mentoring begins.

Components of Good Clinical Teaching
Figure 1
As depicted in Figure 1, the process of clinical teaching can be thought of as two connected cycles each
with a number of components. When teaching at the bedside, the experience cycle will come before the
explanation cycle. The preparation phase involves preparation by both the teacher as well as the
student. Think about what you expect your students/residents to be able to do when you take them to
the bedside. What are they ready for? What is their ability level? These are important considerations
when you plan what you hope to accomplish at the bedside. Learning must be targeted at the level of
ability and knowledge of the student/resident; your teaching goals will be different for learners at
different stages in their clinical training. This may seem obvious, but it is all too often forgotten.
Faculty need to prepare themselves for the experience cycle. First target your learner, and assess their
learning needs. Have a focused, and feasible teaching goal for each clinical encounter. In a busy
emergency department keep these goals simple and do not attempt to teach everything in one
encounter; one or two teaching goals per clinical encounter is appropriate. Save other specific teaching
objectives for the next patient experience. You may have to do a little homework yourself prior to
teaching regularly at the bedside. Refresh your own physical diagnosis skills, develop a set of index
cards or use your Palm Pilot to keep important diagnostic criteria, key references, or specific numbers at
your fingertips. You may even decide to do "theme days" where you may pick a specific physical finding
(type of heart murmur, back pain exam, etc.) or a clinical presentation (cough, abdominal pain, sore
throat, etc.) to focus your teaching on that day. It is then much easier to review appropriate physical
examination techniques, lookup relevant references, and prepare briefly for teaching on your next shift.
The next step in the experience cycle is briefing. Briefing prepares both the patient, and the
student/resident for the clinical encounter. The patient can make a considerable contribution to a
teaching session. As a clinical teacher, set a good example and introduce yourself to the patient and
give the patient a brief indication of the purpose of the bedside encounter. Something as simple as the
following will set the stage with the patient for the rest of the clinical encounter: "Hi, I'm Dr. Hayden and
I'm the doctor in charge of the emergency department today. We're making rounds right now to see how

you are doing. I'm going to have Dr. Sloane tell me briefly what he has learned from you so far and then
we will ask you a few more questions and examine you further. If there is anything you don't understand
just let us know and we will be happy to explain it to you, and feel free to ask questions, or clarify
something for us at any time." All the studies of bedside teaching consistently report that patients prefer
clinical teachers to introduce themselves in such manner, to inform them what the bedside session is all
about, and to translate medical jargon so that they can follow the discussion.
Briefing the student/resident is likewise important. This can be done at the doctor's workstation or just
outside the patient's room. Instructions can be given on what is expected, the rules about what to do
and what not to do, and limits set about how far to go in the encounter. How much does the patient
know about his or her condition? What may or may not be said in front of the patient or family?
Negotiate the rules; what will the resident do? What will the faculty do? If a procedure is to be
performed, the student's familiarity with the technical and cognitive skills may be assessed. What
uncertainties are there in the student/residents' minds, and what questions do they have? Briefing will
make the subsequent clinical encounter go much more smoothly.
During the clinical encounter there are a multitude of teaching goals that may be achieved. Focus
specific goals on the learner's level of experience and limit your teaching to just one or two points. One
of the major goals of bedside teaching is to cultivate the skills of acute observation. As Florence
Nightingale once said, "the most important practical session that can be given is to teach students what
to observe, how to observe, what symptoms indicate improvement and which the reverse, which are of
importance and which are not." Interpretation comes into play only after the features have been carefully
observed and described. The role of the clinical teacher during a clinical encounter is quite variable, yet
however that role is seen, some of the most powerful teaching flows from your own modeling of
politeness, concern, discretion, gentleness, honesty and specific techniques of history taking and
physical examination. The environment should be one of openness and encouragement to both ask
questions and to voice ideas. The teaching skills in this setting lie principally in:
Guiding communication with the patient and explaining clearly to the students/residents
Demonstrating a variety of clinical signs and symptoms and how to elicit them
accurately
Supervising performance and providing gentle but firm feedback

Questioning and challenging interpretations of the data
Modeling professional style with the patient and persistence in obtaining the necessary
clinical information
Before leaving the bedside, solicit questions from the patient about what just happened and what their
understanding is of the diagnostic and management plan.
Debriefing after the clinical encounter allows the clinical teacher to review with the learners what went
on to the bedside. It provides an opportunity to talk about the experience, to express to the teacher how
the clinical interaction was understood, and to raise questions. Additionally, debriefing checks that
appropriate information has been recognized and interpreted accurately. Learning from the case can be
synthesized giving the student a sense of achievement, ensuring resolution of any feelings aroused
during the clinical encounter, and devising learning plans for future interactions.
The explanation cycle begins with reflection, where the teacher and student literally step back from the
immediate experience to link practice with theory, and other evidence that can shed light on the clinical
events. The shift is from "What went on?" to "What did it mean?" Reflection is the time for learners to
think aloud and the teacher's purpose at this stage is to allow free flow of their thoughts, which you help
clarify and link to other learning. Reflection connects this patient with other patients, and with previous
learning.
Explication can be described as a search for how the questions of practice can be helped by biomedical
science and current best evidence. The purpose is to link the clinical experience with theory and
research relevant to the case. Explication may come from journals, textbooks, and clinical experiences
of the teacher and other experts. The rule is that the most current, best available evidence is sought. It
is also valuable at this stage to make assignments for obtaining necessary information including
questions to be asked of the medical literature, or further history from other sources such as family or
private physicians.
The last step in the explanation cycle is the derivation of clinical working knowledge from the clinical
experience. In other words it is "What would I do next time?", "What practical ideas have I picked up
from thinking about this patient?", "What could I have done differently?" The learners create working
rules, or rules of thumb, for use in future practice and clinical teachers guide them through this process.

This practical knowledge then contributes to the preparation for the next patient, which brings us to the
beginning of the next experience cycle.
The Five-minute "Microskills" Model of Clinical Teaching
You are probably saying at this point that this kind of clinical teaching is all well and good but there is no
time in the ED to do this. In an ideal teaching setting, maybe during a "teaching shift" or the equivalent,
all phases of the experience and explanatory cycles can be done in their pure form. In a busy ED,
however, a more condensed version is necessary that still retains key elements of the clinical teaching
process. Such a five-minute model has been developed:
Get a commitment
Probe for supporting evidence
Discuss a "teaching pearl"
Reinforce what was done right
Correct mistakes
Getting a commitment up front involves asking the learner to interpret or synthesize the clinical
information obtained from the patient encounter. It allows the teacher to immediately diagnose the
learner's needs, and gives you a sense whether the student/resident is in the ballpark regarding this
patient's situation. Examples of this are "What do you think is going on with this patient?", "Why do you
think the patient is noncompliant?", "Which of the many complaints will you focus on this visit?" Probing
for supporting evidence takes this a step further by getting learners to reveal their thought processes. It
allows you to identify their knowledge gaps. You might ask "What findings led to your diagnosis?",
"What else did you consider?"
Discussing a teaching pearl gives you the opportunity to introduce key elements of the case in question.
This may include important diagnostic features, appropriate diagnostic testing, a variety of management
issues from an emergency medicine perspective, and current best evidence that pertains to the specific
clinical situation. This pearl, or "teaching bite" should be focused, easily digestible, and targeted to the
learners level of understanding. Examples may include "The key features of this case are...", "In the ED,

when a patient presents with X, your top three priorities are..."
Reinforcing what was done right solidifies the behavior you want from learners. Give specific, and timely
feedback. "Sandwich" constructive criticism between two layers (statements) of positive feedback.
Correcting mistakes is extremely important at this stage. Omissions, errors, misinterpreting data, will
become habit and part of "muscle memory" if not corrected at the time they occur. This should be done
in an appropriate setting. It may not be suitable to correct serious errors in front of patients, nursing
staff, or other students/residents. For example, "Next time that happens, try the following...", "I agree the
patient may be drug seeking, but it is still important to do a careful history and physical examination"
You may not even be able to use this five-minute model on every patient encounter in the ED. Be
selective, choose a limited number of patients of the greatest teaching value during a given shift. You
can listen for clues during the case presentation to select such patients; inconsistencies or confusing
aspects of the history, abnormal findings described on the physical examination, may be clues that this
patient can provide a "teachable moment". Alternately you can ask the student/resident which of their
patients they want to see with you at the bedside making teaching learner-centered. An additional
strategy is to grab one resident (this works with either a senior or junior EM resident) during a given shift
and do periodic bedside rounds on the patients they are responsible for.
Evidence Based Emergency Medicine at the Bedside
Evidence based medicine (EBM) can be defined as asking a focused, relevant clinical question and
answering it based on the best most current evidence available. It is often stated that the place for EBM
is in journal clubs or in reading articles in the library and that there is no time for this approach in a busy
ED. A skilled clinical teacher, however, can bring elements of EBM to the bedside in a busy ED.
At the bedside in the ED, use questions about the history and physical examination for teaching basic
principles of EBM. Take a single item of history or examination and think of it as a "diagnostic test."
Take a combination of history and physical examination features as a clinical prediction rule. It is an
opportunity to discuss concepts such as pretest probability, precision (simple agreement, kappa) and
accuracy (likelihood ratio, positive (PPV) and negative predictive value (NPV)) of diagnostic tests, utility
of diagnostic tests, and using these properties to move from pretest probability estimates to posttest
probability of disease.

Start with pretest probability, use the HPI to establish baseline probability of a given condition. Discuss
where pretest probabilities come from; ideally from well done published studies, or quality assurance
studies done in your own ED, or based on clinical experience. Next focus on the specific elements of the
history or examination. For example, meningismus, Murphy's sign, effort syncope, etc. In your briefing
session review how to elicit the specific findings prior to assessing the patient. After assessing the
patient, review these key elements of history or examination; discuss interrater, and intrarater reliability.
Highlight the difference between simple agreement, and the agreement beyond that due to chance
alone (kappa). You do not have to calculate a likelihood ratio, or PPV/NPV at the bedside to discuss the
accuracy of a diagnostic test. Do your homework and have these numbers immediately available and
show how to use a likelihood ratio to modify the pretest odds and derive a posttest odds of disease that
can then be converted back into posttest probability. Question learners on how further diagnostic testing
will alter disease probability and guide treatment and disposition decisions. For residents at higher
training levels discuss the accuracy of combinations of signs and symptoms derived during a patient
encounter and the management implications of clinical decision rules.
The skilled clinical teacher will not attempt to get through all of these teaching goals for every patient.
Take one concept that seems most relevant to the current patient, and save other concepts for
subsequent similar patients seen in the course of the shift. Choose clinical conditions that you
commonly see in the ED to prepare for. We all see suspected appendicitis, pharyngitis, exacerbations of
asthma, and many other such conditions on a daily basis. The medical literature is replete with articles
on clinical findings for various diseases. When searching the literature use terms such as "physical
examination", "medical history taking", "observer variation", or "interrater reliability". JAMA has a series
called the Rational Clinical Examination that contains this information for many common disease
presentations. Have the likelihood ratios or sensitivity/specificity of various signs and symptoms readily
available for these common conditions. Then when the teachable moment arises you'll be ready to
pounce.
Conclusions
External forces, such as recent CMS regulations, have pushed academic EM faculty into a situation
where we need to spend a great deal of time personally evaluating patients. Rather than lament the loss
of teaching time in the doctors workstation, grease board, or conference room, this is a unique

opportunity to go back to the bedside with our residents and students and teach them firsthand medical
history taking, physical examination skills, clinical acumen, and model professional interpersonal skills
with patients.
This paradigm shift requires that academic EM physicians refine their clinical teaching skills. Learn to
recognize and seize the "teaching moment." Have a number of "teaching bites" readily available to use
when such moments arise. Become skilled at recognizing your learner's knowledge gaps and exploit
them for teaching. Guide learning with high yield questions that require synthesis and interpretation.
Most of all, enjoy the opportunity to learn from your students/residents at the bedside as much as they
learn from you. As Osler stated in his farewell address to The Johns Hopkins Hospital in 1905, "By far
the greatest work of The Johns Hopkins Hospital has been the demonstration to the profession and to
the public of this country how medical students should be instructed in their art. Personally, there is
nothing in life in which I take greater pride than in the introduction of the old-fashioned methods of
practical instruction. I desire no other epitaph than the statement that I taught medical students on the
wards, as I regard this by far the most useful and important work I have been called upon to do."
Suggested Reading
1. Neher JO, Gordon KC, Meyer B, Stevens N. A five-step "microskills" model of clinical teaching [see
comments]. J Am Board Fam Pract. 1992;5:419-24.
2. Stone MJ. The wisdom of Sir William Osler. Am J Cardiol. 1995;75:269-276.
3. Cox K. Planning bedside teaching--1. Overview. Med J Aust. 1993;158:280-282.
4. Cox K. Planning bedside teaching--2. Preparation before entering the wards. Med J Aust.
1993;158:355-357.
5. Cox K. Planning bedside teaching--3. Briefing before seeing the patient. Med J Aust. 1993;158:417-
418.
6. Cox K. Planning bedside teaching--4. Teaching around the patient. Med J Aust. 1993;158:493-495.

7. Cox K. Planning bedside teaching--5. Debriefing after clinical interaction. Med J Aust. 1993;158:571-
572.
8. Cox K. Planning bedside teaching--6. Reflection on the clinical experience. Med J Aust.
1993;158:607-608.
9. Cox K. Planning bedside teaching--7. Explication of the clinical experience. Med J Aust.
1993;158:789-790.
10. Cox K. Planning bedside teaching--8. Deriving working rules for next time. Med J Aust. 1993;159:64
11. Sapira JD. The Art And Science Of Bedside Diagnosis. Williams & Wilkins, 1990, Baltimore, MD
Mid-Career Faculty Development
Developing a Career in the Scholarship of Teaching as a Clinician-Educator
Author: Stephen R. Hayden
Introduction
Clinical bedside teaching is nothing new. It was Hippocrates (circa 400 BC) who abandoned temple
based medicine for a practice that valued direct observation, the exact recording of the features of
disease, and adherence to the principal that "You must go to the bedside, it is there alone that you can
learn disease." In his address to the New York Academy of Sciences, Sir William Osler stated that there
should be "No teaching without a patient for a text, and the best teaching is that taught by the patient
himself." Despite this legacy there has been gradual erosion in time spent teaching at the bedside.
Thirty years ago over 75% of medical teaching occurred at the patient's bedside. Several authors have

recently examined the time devoted to attending rounds on inpatient medical services. They estimated
that only 16 - 20 % of the time devoted to attending rounds was spent in the presence of the patient. In
other studies using direct observation or videotaping it was found that the average time spent at the
bedside was only 2 - 3 minutes compared with approximately 60 minutes in the classroom. In 25 % of
instances teachers never saw the patient at all, whether during the case presentation or afterward.
Although a number of studies have shown that approximately 85 % of patients preferred bedside
rounds, only 35 % of attending physicians did so, 4 % of students, and 2 % of house staff.
The emergency department (ED) has always been regarded as a rich environment for clinical teaching
with the wealth and diversity of diseases that present to our doors. Yet most academic emergency
physicians are experiencing intense pressure from external sources to improve the efficiency,
documentation, and cost effectiveness of emergency medicine (EM) practice. I have heard many of my
colleagues lament that this results in less time for teaching residents and students in the ED. If you
believe that the best teaching occurs in the doctors workstation, conference room, or lecture hall then it
is understandable that you would feel this way. I'm going out on a limb here, however, and suggesting
that recent external forces that require attending EM physicians to personally see and examine all
patients in the ED may be the best thing that has happened to clinical teaching in EM. We have been
handed a golden opportunity. As a faculty physician you now need to be there anyway, take a resident,
or student, by the hand and lead them with you back to the bedside where a multitude of teaching
moments can occur.
In this chapter we will discuss characteristics of good clinical teachers, perceived obstacles to effective
bedside teaching, strategies to overcome them, the components of good bedside teaching, and a
number of practical models to use in clinical instruction.
Characteristics of Good Clinical Teachers
There are a number of characteristics that great clinical teachers in medicine share:
Teachers are knowledgeable
Presentations are clear and well organized
They are enthusiastic and able to interact skillfully with students and residents

Provide simultaneous teaching and clinical supervision
Demonstrate clinical skills to learners
Model professional characteristics
Good clinical teachers also display numerous intangible qualities such as:
Being available
Being approachable
Having infinite patience
Staying calm in difficult situations
Osler described this as equanimity, and suggested "In the physician or surgeon no quality takes rank
with imperturbability."
Superb clinical teachers also use effective teaching skills including:
Explaining concepts at the learners level
Providing timely feedback
Modeling their behavior for students
Illuminating how their thought process works
Instructing in small digestible "teaching bites"
Guiding learning with questions
This last item bears repeating: Good clinical teachers guide learning with questions. This means asking
questions that require synthesis and interpretation of information and evidence rather than simple
regurgitation.
Examples of such high yield questions are:
Why do you believe that to be true?

How did you reach that conclusion?
What lead you to that decision?
Why is X approach better than Y?
Why is that information important?
What will happen if you don't do X?
What is the association between X and Y?
Obstacles to Effective Clinical Teaching
Concern for the Privacy and Well-being of the Patient
The argument is often made that to present case histories and physical findings in front of patients, and
possibly their families, would prove embarrassing or uncomfortable to them. On the contrary, the
available evidence suggests that patients are in fact appreciative of the attention being devoted to them
by so many health-care professionals. When conducted tactfully and empathetically bedside
presentation is not a traumatic emotional experience but rather educates and reassures patients. The
overwhelming majority of patients feel that they understand their illness better and have a better
opportunity to get their questions answered. Patients want the attending physician to introduce
themselves, to state the purpose of bedside rounds, and to be sensitive to the need to translate medical
jargon into terms that they can understand.
Medical Chauvinism
Some doctors believe that it is not appropriate to involve patients in the process of making major
decisions regarding their health-care. Consequently this may be responsible for moving case
presentations and discussions away from the bedside. These physicians also do not want to display
weaknesses in front of patients or families in discussing their own problems associated with data
collection, interpretation, and synthesis. Again, the available evidence would indicate that active
involvement of the patient, as well as the patients observation of our deliberations, can lead to an
honest, open, and mature doctor patient relationship where both the physician and patient assume
appropriate responsibility for decisions made.

Passive View of Education
Here the old idiom that education is the transfer of knowledge from teacher to student is applicable. This
view purports that teaching on rounds means a series of mini-lectures by the attending on topics that
happened to arise, often followed by a more lengthy discussion in the doctors workstation, conference
room, or classroom. Trainees support this arrangement since it requires little active work on their part
and conforms to their prior educational experiences as passive listeners in a lecture hall. They are used
to the doughnuts and coffee, the comfort of sitting around a conference table or at a work desk, and the
cloak of early morning or post-meal semiconsciousness. In order to combat this, the skilled emergency
medicine faculty will know how to actively engage the student or resident by guiding learning with
appropriate questions. The attending facilitates group or individual learning by assisting the trainees to
discover for themselves the important clinical issues and develop a strategy to solve the clinical
problem.
Emergency Medicine Faculty Discomfort at the Bedside
Many teachers are uncomfortable discussing subject matter in which they feel less than expert. The
bedside is avoided where the reality of the patient's situation or difficult questions might draw them on to
intellectually thin ice. They prefer the workstation, the conference room, or even worse the hallway,
where they can turn the discussion to subjects with which they are far more comfortable. There will be
no patient and no family in attendance to ask embarrassing questions that force us to say, "I don't
know." Furthermore, there is our discomfiture with physical diagnosis. All of these barriers may be easily
overcome. Create a safe and comfortable environment for asking questions and discussing answers.
Become comfortable with saying, "I don't know but here is how we will find out." If you don't know the
answer to a specific question, tactfully turn the question to other members of the group. If none of the
group members know the answer, then an individual may be assigned to search for the answer. Such
questions generated at the bedside during the course of patient evaluation and care are the most useful
and relevant questions for teaching purposes; encourage rather than avoid them. Even without specific
expertise with the particular disorder presented, other skills may be taught at the bedside, including
history taking, demonstration of interpersonal skills, and teaching trainees to be skilled observers. The
bedside teacher's role is transformed into one that focuses attention and generates clinical inquiry.

Lack of Interactive Skills
Faculty physicians themselves may be uncomfortable interacting with certain types of patients. This may
be especially true in the emergency department. In fact some studies have found that most teachers go
to the bedside only to check on abnormal physical findings. As a consequence, bedside time may be
kept to a minimum and trainees may lose the opportunity to observe an experienced clinician in action
with the patient.
Social learning theory emphasizes the learning that occurs by observation and imitation of role models.
From this viewpoint, the quality of the interaction between the attending physician and the patient is
likely to be imitated by the resident in interactions with their own patients. Faculty should practice what
they preach and model the kind of communication patterns they expect residents to use with patients.
Bedside teaching fosters a wonderful link with the past. Trainees watch you as carefully as does a child
his parent; they watch you attend to the patient, watch you observe. They observe your powers of
diagnosis, the respect you hold for other human beings, your attitude, and your caring. Students witness
your own dignity, and the love and enthusiasm you have for medicine and teaching. And so true
mentoring begins.
Components of Good Clinical Teaching
Figure 1
As depicted in Figure 1, the process of clinical teaching can be thought of as two connected cycles each
with a number of components. When teaching at the bedside, the experience cycle will come before the
explanation cycle. The preparation phase involves preparation by both the teacher as well as the
student. Think about what you expect your students/residents to be able to do when you take them to
the bedside. What are they ready for? What is their ability level? These are important considerations
when you plan what you hope to accomplish at the bedside. Learning must be targeted at the level of
ability and knowledge of the student/resident; your teaching goals will be different for learners at
different stages in their clinical training. This may seem obvious, but it is all too often forgotten.
Faculty need to prepare themselves for the experience cycle. First target your learner, and assess their
learning needs. Have a focused, and feasible teaching goal for each clinical encounter. In a busy

emergency department keep these goals simple and do not attempt to teach everything in one
encounter; one or two teaching goals per clinical encounter is appropriate. Save other specific teaching
objectives for the next patient experience. You may have to do a little homework yourself prior to
teaching regularly at the bedside. Refresh your own physical diagnosis skills, develop a set of index
cards or use your Palm Pilot to keep important diagnostic criteria, key references, or specific numbers at
your fingertips. You may even decide to do "theme days" where you may pick a specific physical finding
(type of heart murmur, back pain exam, etc.) or a clinical presentation (cough, abdominal pain, sore
throat, etc.) to focus your teaching on that day. It is then much easier to review appropriate physical
examination techniques, lookup relevant references, and prepare briefly for teaching on your next shift.
The next step in the experience cycle is briefing. Briefing prepares both the patient, and the
student/resident for the clinical encounter. The patient can make a considerable contribution to a
teaching session. As a clinical teacher, set a good example and introduce yourself to the patient and
give the patient a brief indication of the purpose of the bedside encounter. Something as simple as the
following will set the stage with the patient for the rest of the clinical encounter: "Hi, I'm Dr. Hayden and
I'm the doctor in charge of the emergency department today. We're making rounds right now to see how
you are doing. I'm going to have Dr. Sloane tell me briefly what he has learned from you so far and then
we will ask you a few more questions and examine you further. If there is anything you don't understand
just let us know and we will be happy to explain it to you, and feel free to ask questions, or clarify
something for us at any time." All the studies of bedside teaching consistently report that patients prefer
clinical teachers to introduce themselves in such manner, to inform them what the bedside session is all
about, and to translate medical jargon so that they can follow the discussion.
Briefing the student/resident is likewise important. This can be done at the doctor's workstation or just
outside the patient's room. Instructions can be given on what is expected, the rules about what to do
and what not to do, and limits set about how far to go in the encounter. How much does the patient
know about his or her condition? What may or may not be said in front of the patient or family?
Negotiate the rules; what will the resident do? What will the faculty do? If a procedure is to be
performed, the student's familiarity with the technical and cognitive skills may be assessed. What
uncertainties are there in the student/residents' minds, and what questions do they have? Briefing will
make the subsequent clinical encounter go much more smoothly.

During the clinical encounter there are a multitude of teaching goals that may be achieved. Focus
specific goals on the learner's level of experience and limit your teaching to just one or two points. One
of the major goals of bedside teaching is to cultivate the skills of acute observation. As Florence
Nightingale once said, "the most important practical session that can be given is to teach students what
to observe, how to observe, what symptoms indicate improvement and which the reverse, which are of
importance and which are not." Interpretation comes into play only after the features have been carefully
observed and described. The role of the clinical teacher during a clinical encounter is quite variable, yet
however that role is seen, some of the most powerful teaching flows from your own modeling of
politeness, concern, discretion, gentleness, honesty and specific techniques of history taking and
physical examination. The environment should be one of openness and encouragement to both ask
questions and to voice ideas. The teaching skills in this setting lie principally in:
Guiding communication with the patient and explaining clearly to the students/residents
Demonstrating a variety of clinical signs and symptoms and how to elicit them
accurately
Supervising performance and providing gentle but firm feedback
Questioning and challenging interpretations of the data
Modeling professional style with the patient and persistence in obtaining the necessary
clinical information
Before leaving the bedside, solicit questions from the patient about what just happened and what their
understanding is of the diagnostic and management plan.
Debriefing after the clinical encounter allows the clinical teacher to review with the learners what went
on to the bedside. It provides an opportunity to talk about the experience, to express to the teacher how
the clinical interaction was understood, and to raise questions. Additionally, debriefing checks that
appropriate information has been recognized and interpreted accurately. Learning from the case can be
synthesized giving the student a sense of achievement, ensuring resolution of any feelings aroused
during the clinical encounter, and devising learning plans for future interactions.

The explanation cycle begins with reflection, where the teacher and student literally step back from the
immediate experience to link practice with theory, and other evidence that can shed light on the clinical
events. The shift is from "What went on?" to "What did it mean?" Reflection is the time for learners to
think aloud and the teacher's purpose at this stage is to allow free flow of their thoughts, which you help
clarify and link to other learning. Reflection connects this patient with other patients, and with previous
learning.
Explication can be described as a search for how the questions of practice can be helped by biomedical
science and current best evidence. The purpose is to link the clinical experience with theory and
research relevant to the case. Explication may come from journals, textbooks, and clinical experiences
of the teacher and other experts. The rule is that the most current, best available evidence is sought. It
is also valuable at this stage to make assignments for obtaining necessary information including
questions to be asked of the medical literature, or further history from other sources such as family or
private physicians.
The last step in the explanation cycle is the derivation of clinical working knowledge from the clinical
experience. In other words it is "What would I do next time?", "What practical ideas have I picked up
from thinking about this patient?", "What could I have done differently?" The learners create working
rules, or rules of thumb, for use in future practice and clinical teachers guide them through this process.
This practical knowledge then contributes to the preparation for the next patient, which brings us to the
beginning of the next experience cycle.
The Five-minute "Microskills" Model of Clinical Teaching
You are probably saying at this point that this kind of clinical teaching is all well and good but there is no
time in the ED to do this. In an ideal teaching setting, maybe during a "teaching shift" or the equivalent,
all phases of the experience and explanatory cycles can be done in their pure form. In a busy ED,
however, a more condensed version is necessary that still retains key elements of the clinical teaching
process. Such a five-minute model has been developed:
Get a commitment

Probe for supporting evidence
Discuss a "teaching pearl"
Reinforce what was done right
Correct mistakes
Getting a commitment up front involves asking the learner to interpret or synthesize the clinical
information obtained from the patient encounter. It allows the teacher to immediately diagnose the
learner's needs, and gives you a sense whether the student/resident is in the ballpark regarding this
patient's situation. Examples of this are "What do you think is going on with this patient?", "Why do you
think the patient is noncompliant?", "Which of the many complaints will you focus on this visit?" Probing
for supporting evidence takes this a step further by getting learners to reveal their thought processes. It
allows you to identify their knowledge gaps. You might ask "What findings led to your diagnosis?",
"What else did you consider?"
Discussing a teaching pearl gives you the opportunity to introduce key elements of the case in question.
This may include important diagnostic features, appropriate diagnostic testing, a variety of management
issues from an emergency medicine perspective, and current best evidence that pertains to the specific
clinical situation. This pearl, or "teaching bite" should be focused, easily digestible, and targeted to the
learners level of understanding. Examples may include "The key features of this case are...", "In the ED,
when a patient presents with X, your top three priorities are..."
Reinforcing what was done right solidifies the behavior you want from learners. Give specific, and timely
feedback. "Sandwich" constructive criticism between two layers (statements) of positive feedback.
Correcting mistakes is extremely important at this stage. Omissions, errors, misinterpreting data, will
become habit and part of "muscle memory" if not corrected at the time they occur. This should be done
in an appropriate setting. It may not be suitable to correct serious errors in front of patients, nursing
staff, or other students/residents. For example, "Next time that happens, try the following...", "I agree the
patient may be drug seeking, but it is still important to do a careful history and physical examination"
You may not even be able to use this five-minute model on every patient encounter in the ED. Be
selective, choose a limited number of patients of the greatest teaching value during a given shift. You
can listen for clues during the case presentation to select such patients; inconsistencies or confusing

aspects of the history, abnormal findings described on the physical examination, may be clues that this
patient can provide a "teachable moment". Alternately you can ask the student/resident which of their
patients they want to see with you at the bedside making teaching learner-centered. An additional
strategy is to grab one resident (this works with either a senior or junior EM resident) during a given shift
and do periodic bedside rounds on the patients they are responsible for.
Evidence Based Emergency Medicine at the Bedside
Evidence based medicine (EBM) can be defined as asking a focused, relevant clinical question and
answering it based on the best most current evidence available. It is often stated that the place for EBM
is in journal clubs or in reading articles in the library and that there is no time for this approach in a busy
ED. A skilled clinical teacher, however, can bring elements of EBM to the bedside in a busy ED.
At the bedside in the ED, use questions about the history and physical examination for teaching basic
principles of EBM. Take a single item of history or examination and think of it as a "diagnostic test."
Take a combination of history and physical examination features as a clinical prediction rule. It is an
opportunity to discuss concepts such as pretest probability, precision (simple agreement, kappa) and
accuracy (likelihood ratio, positive (PPV) and negative predictive value (NPV)) of diagnostic tests, utility
of diagnostic tests, and using these properties to move from pretest probability estimates to posttest
probability of disease.
Start with pretest probability, use the HPI to establish baseline probability of a given condition. Discuss
where pretest probabilities come from; ideally from well done published studies, or quality assurance
studies done in your own ED, or based on clinical experience. Next focus on the specific elements of the
history or examination. For example, meningismus, Murphy's sign, effort syncope, etc. In your briefing
session review how to elicit the specific findings prior to assessing the patient. After assessing the
patient, review these key elements of history or examination; discuss interrater, and intrarater reliability.
Highlight the difference between simple agreement, and the agreement beyond that due to chance
alone (kappa). You do not have to calculate a likelihood ratio, or PPV/NPV at the bedside to discuss the
accuracy of a diagnostic test. Do your homework and have these numbers immediately available and
show how to use a likelihood ratio to modify the pretest odds and derive a posttest odds of disease that
can then be converted back into posttest probability. Question learners on how further diagnostic testing
will alter disease probability and guide treatment and disposition decisions. For residents at higher

training levels discuss the accuracy of combinations of signs and symptoms derived during a patient
encounter and the management implications of clinical decision rules.
The skilled clinical teacher will not attempt to get through all of these teaching goals for every patient.
Take one concept that seems most relevant to the current patient, and save other concepts for
subsequent similar patients seen in the course of the shift. Choose clinical conditions that you
commonly see in the ED to prepare for. We all see suspected appendicitis, pharyngitis, exacerbations of
asthma, and many other such conditions on a daily basis. The medical literature is replete with articles
on clinical findings for various diseases. When searching the literature use terms such as "physical
examination", "medical history taking", "observer variation", or "interrater reliability". JAMA has a series
called the Rational Clinical Examination that contains this information for many common disease
presentations. Have the likelihood ratios or sensitivity/specificity of various signs and symptoms readily
available for these common conditions. Then when the teachable moment arises you'll be ready to
pounce.
Conclusions
External forces, such as recent CMS regulations, have pushed academic EM faculty into a situation
where we need to spend a great deal of time personally evaluating patients. Rather than lament the loss
of teaching time in the doctors workstation, grease board, or conference room, this is a unique
opportunity to go back to the bedside with our residents and students and teach them firsthand medical
history taking, physical examination skills, clinical acumen, and model professional interpersonal skills
with patients.
This paradigm shift requires that academic EM physicians refine their clinical teaching skills. Learn to
recognize and seize the "teaching moment." Have a number of "teaching bites" readily available to use
when such moments arise. Become skilled at recognizing your learner's knowledge gaps and exploit
them for teaching. Guide learning with high yield questions that require synthesis and interpretation.
Most of all, enjoy the opportunity to learn from your students/residents at the bedside as much as they
learn from you. As Osler stated in his farewell address to The Johns Hopkins Hospital in 1905, "By far
the greatest work of The Johns Hopkins Hospital has been the demonstration to the profession and to
the public of this country how medical students should be instructed in their art. Personally, there is
nothing in life in which I take greater pride than in the introduction of the old-fashioned methods of

practical instruction. I desire no other epitaph than the statement that I taught medical students on the
wards, as I regard this by far the most useful and important work I have been called upon to do."
Suggested Reading
1. Neher JO, Gordon KC, Meyer B, Stevens N. A five-step "microskills" model of clinical teaching [see
comments]. J Am Board Fam Pract. 1992;5:419-24.
2. Stone MJ. The wisdom of Sir William Osler. Am J Cardiol. 1995;75:269-276.
3. Cox K. Planning bedside teaching--1. Overview. Med J Aust. 1993;158:280-282.
4. Cox K. Planning bedside teaching--2. Preparation before entering the wards. Med J Aust.
1993;158:355-357.
5. Cox K. Planning bedside teaching--3. Briefing before seeing the patient. Med J Aust. 1993;158:417-
418.
6. Cox K. Planning bedside teaching--4. Teaching around the patient. Med J Aust. 1993;158:493-495.
7. Cox K. Planning bedside teaching--5. Debriefing after clinical interaction. Med J Aust. 1993;158:571-
572.
8. Cox K. Planning bedside teaching--6. Reflection on the clinical experience. Med J Aust.
1993;158:607-608.
9. Cox K. Planning bedside teaching--7. Explication of the clinical experience. Med J Aust.
1993;158:789-790.
10. Cox K. Planning bedside teaching--8. Deriving working rules for next time. Med J Aust. 1993;159:64

11. Sapira JD. The Art And Science Of Bedside Diagnosis. Williams & Wilkins, 1990, Baltimore, MD

The Role of the Chair in Promotion
Author: Bill Barsan
Introduction
The departmental chair plays a critical role in facilitating promotion at any academic medical center. It is
fair to say that the chair's responsibilities for a) clearly defining the criteria for promotion and b)
objectively evaluating faculty members each year, will be the key elements in achieving promotion. This
applies to promotion in not only the research or tenure track but the clinician educator track as well. In
this chapter, I have defined the key roles played by the chair as determination of department balance,
recruitment, resource allocation, evaluation and support for promotion. Although other chairs may
define the roles somewhat differently, I think that most would include all of these areas somewhere in
their summary of key roles.
Determination of Departmental Balance
In overseeing the entire department, the chair should attempt to determine the appropriate balance
between research or tenure track faculty and clinician educator faculty. Some of the factors, which will
impact this balance, would include not only the individual needs of the department but also the
academic milieu in which the department exists. In general, it is advisable to have the Department of
Emergency Medicine look similar to other academic departments within the medical school in regard to
the proportion of tenure track and clinical track faculty. Currently, this is not always the case. A survey
from 1997 showed that only about one-third as many emergency medicine faculty members are
tenured compared with faculty members in other specialties at the same institutions. The department
chair also has to consider the different administrative roles to be performed within the department. In
general, roles with heavy administrative responsibilities are not going to be appropriate for faculty
working towards tenure as these responsibilities will not enable enough time for the faculty member to
pursue any meaningful research program. The other issue of departmental balance relates to any
specific research interests for prospective faculty. In general, it is preferable to match up research
interests with research expertise. For example, if a prospective faculty member had research involving
neuronal cell cultures and nobody in the institution or the department had any experience with neuronal
cell cultures, that faculty member's chance for success in that research area would be limited. Ideally,
the chair should try to recruit young faculty with similar research interests to experienced researchers
already in the department or in the institution.

The Recruitment Process
The chair's role is obviously critical and pivotal in the recruitment process. In addition to selecting the
prospective faculty member on personal, clinical, research and balance concerns, the chair also needs
to clearly define where a prospective recruit fits in. Specifically, the chair should identify during the
recruitment process whether the prospective faculty member will likely be a clinical track or tenure track
faculty member. The chair will also have to give the prospective recruit the definitions and factors
critical to achieving promotion in the different tracks. The chair can't assume that a recruit will have any
automatic understanding of these issues. The criteria for promotion and tenure and the different tracks
available vary widely from institution to institution and need to be clearly defined in each individual
circumstance. At the completion of the recruitment process, both the chair and the prospective faculty
member should have a clear idea of the prospective faculty member's role in the department, which
academic track they will pursue and the critical elements for success in that particular track.
Provision of Resources
The area of resources is frequently cited as the most important responsibility of the chair toward faculty
promotion. The most important resources provided by the chair for faculty are financial support for
research, adequate time and mentors.
The amount of financial resources committed towards an individual faculty member will depend on the
academic track as well as the specific area of research. In general, clinician educator faculty members
typically need little, if any, allocation of financial resources over and above traditional commitments of
CME monies. For faculty members pursuing a tenure track, a commitment of financial resources is
critical. The general approach taken by many academic departments at the University of Michigan is
that the department is responsible for providing financial resources to pay for the first two years of a
faculty member's research, after which period of time the faculty member should start to procure some
extramural funding to support further research. For people involved in laboratory research, this
commitment of two years funding may be quite expensive. Additionally, laboratory researchers will
need a laboratory to perform their research and adequate facilities in the lab to conduct the type of
research to be performed. In some circumstances this may mean fully outfitting a departmental
laboratory and in other circumstances, the faculty member may be able to work in laboratories with
individuals from other departments.
Providing adequate time for faculty to meet their requirements for promotion and tenure is critical and

has always been a hot topic in academic emergency medicine. Although there are no hard and fast
rules, it is generally assumed that working more than 22-24 clinical hours per week will not be
compatible with achieving promotion in the research track. Besides this limitation in clinical hours, the
chair needs to make sure that the faculty member is not loaded up with other duties during their non-
clinical time. The faculty member in the tenure track should for the most part limit their non-clinical
activities to pursuing their research and should not assume major departmental roles like assistant
program director, EMS director, operations director, etc. The chair should be responsible for working
with the faculty member to limit these other responsibilities. Another way to increase a faculty
member's efficiency with limited time is to provide some ancillary support. This may be in the form of
secretarial support or laboratory technical support or providing monies to hire students or others for
tasks such as data entry, chart abstraction, etc.
Perhaps the most important item that a chair can provide to a young faculty member is a mentor.
Particularly for individuals in the research or tenure track, a mentor or mentors play a very important
role. These individuals can advise and direct the young faculty member on their research as well as
help them with grant writing and development of new areas for research. The mentor should be a
senior faculty member at the associate professor level or higher and one who has significant expertise
and hopefully evidence of extramural funding in the faculty's area of research. Although some faculty
members are able to identify their own mentors, it is critically important that the chair help them find a
mentor if they don't already have someone in mind. One of the common practices in emergency
medicine is to team up young faculty with mentors exclusively in your own department. Because
emergency medicine is still a relatively young field and there is a paucity of tenured faculty members, it
is advantageous to locate mentors outside of the department as well. In most major academic medical
centers, there are a number of tenured faculty members in other departments with research interests in
different areas. Many of these individuals are more than willing to serve as mentors for junior faculty
from EM. The quality of research and personal characteristics of the mentor are far more important
than the department in which they have their primary appointment. For faculty in the clinician educator
track, it is usually easier and makes more sense to have mentors from within the department. Often this
may end up being the chair but could easily be other senior faculty members as well.
Evaluation
After the faculty member clearly understands the requirements for promotion and is equipped with
appropriate mentorship and any needed start up money, the faculty member's job is to try to fulfill the

needed requirements for promotion. The chair's role in this process is to perform timely evaluations
either once or twice a year and help the faculty member track his/her progress toward achieving
promotion. A yearly conference is an opportunity for the chair to work with the faculty member to set
goals for the coming year and track whether or not the faculty member is appropriately progressing
towards completion of his or her goals in eventual promotion. If a faculty member is having difficulty in
meeting the goals that have been set, the chair needs to work with the faculty member to decide
whether the goals are unrealistic, there is a resource issue, or other issues affecting the faculty
member's performance. It is important that these yearly assessments be realistic and the goals
reachable. Particularly for instructional or tenure track faculty members, it's extremely important for the
chair to let the faculty member know whether or not they are on track for eventual promotion at the end
of the required time or whether this will be difficult or impossible.
The Promotion Process
Ultimately, the department chair will have to make the determination of when a faculty member should
be put up for promotion. This is obviously not a unilateral decision and will need the input of the
individual faculty member as well. The yearly evaluations of the faculty member should usually include
long term plans for when promotion will be sought so that the decision of when to go for promotion is
not a surprise. In addition to determining whether or not the faculty member is ready for promotion, the
chair typically will have to write a support letter that highlights the ways in which the faculty member
has reached the criteria necessary to be promoted. It is ultimately the chair's responsibility to make
sure that supporting documentation is present in the promotion packet as required by the institution.
Request for promotion will typically be reviewed by a departmental promotions committee prior to
review by the institution's promotions committee. The department chair needs to be sure that the
departmental committee has knowledgeable individuals who can sufficiently evaluate each promotional
recommendation. Because emergency medicine is a new specialty and there may be a relative lack of
senior faculty members, it may be advisable to have one or two "guest" members from other
departments who have more extensive knowledge and experience of the promotions process in that
institution.
If the chair believes that a given faculty member is worthy of promotion and this is supported by the
departmental committee, there may be occasions where the institution's promotions committee will vote
not to promote the individual. In cases where the chair believes that the institution's promotions
committee is overlooking some important information, he or she should not be reluctant to appeal the

committee's decision. In circumstances where a faculty member is being heavily recruited elsewhere
and the decision not to promote could affect a decision to stay, most promotions committees will take
this under serious consideration in their decision.
In cases where promotion is denied, the promotions committee will typically give their reasons for
denial. In those cases, it is the chair's job to work with the faculty member to try to correct the
deficiencies present prior to resubmitting for promotion.
Conclusion
While the specifics of the promotion process may vary from institution to institution, the chair will play a
key role in helping faculty to achieve promotion. The faculty member's responsibility is to work with the
chair and develop a plan, which will be successful. The chair's job is make sure the faculty member
clearly understands the requirements for promotion, has the necessary resources to perform the work
required and advice on the progress and timing of promotion.

Advanced Degrees for Academic Emergency Physicians
Author: Gregory P. Conners
Why would an academic emergency physician want a graduate degree? Phrased differently: will the
career enhancement be worth the investment of time and money? The pressures of day-to-day life can
make obtaining a graduate degree difficult. Clinical and family schedules may seem overwhelming and
inflexible; additional tuition bills will certainly be unwelcome. The ultimate answer, of course, will vary for
each individual. The purpose of this chapter is to help you determine the right answer for yourself.
Medical school and residency provide excellent foundations for the clinical practice of emergency
medicine. However, although expectations vary, the academic physician is typically expected to be not
only a top-notch clinician, but an excellent teacher, a productive researcher, and to take on various
administrative assignments. While any and all of these may be learned on the job, an advanced degree
is a way to rapidly develop proficiency in one or more of these areas. Less obviously, being a graduate
student provides contacts with graduate faculty and other students. This networking may lead to new
ideas, collaborations, and other opportunities. Finally, having an advanced degree may serve as an
additional credential, providing credibility in a competitive academic world. Similar arguments may be
made about fellowship; in fact, it is not uncommon to pair fellowship with pursuit of an advanced degree,
such as an M.P.H.
Graduate study requires a considerable investment of time, money, and energies, whether full- or part-
time. Graduate programs require reading, homework, studying for tests, and, often, preparation of final
projects. The vagaries of grades may be ego-challenging. We can always find another way to
productively use our time, our most precious resource, whether it is in enhancing our academic careers,
moonlighting, or spending time with our families and friends. On the other hand, investing in graduate
study now may make the career-oriented time we spend in the decades to follow more productive. For
example, graduate training may allow us to approach and smoothly and effectively complete a complex
project or goal that previously might have been difficult or even impossible.
Location and availability of graduate training are also important considerations. Those working in a
university setting or a large city may have easy access to a wide variety of relevant graduate programs;
others may not. Fortunately, high-quality distance learning programs are now available in many fields,
and are growing steadily. Judging relative quality of graduate programs, whether distance learning or

traditional, is difficult. Annual rankings compiled by the U.S. News & World Report, while imperfect, may
be of interest http://www.usnews.com/usnews/edu/beyond/bcrank.htm; the website also offers links to
some ranked programs.
Some strategies have emerged from academic emergency physicians who have successfully obtained
graduate degrees. First and foremost, you will need to focus. Just as in medical school, you will need to
marshal your energies when it is sometimes difficult, and will need family or other social supports.
Having an idea of your ultimate goal, whether it is a successful career in academic emergency medicine,
commanding a military hospital, or a medical school or hospital leadership position, can help keep you
motivated. Those who successfully obtain graduate degrees while conducting academic careers
typically describe having made their commitment to graduate study an important part of their lives.
Although a few become full-time students, most try to carve out time for part-time study while a full-time
faculty member (or fellow). This is probably most easily accomplished when you are beginning a new
job, and still apportioning your time to various areas. However, the benefits of graduate training are not
limited to those beginning their careers or changing jobs. In fact, it is not uncommon to initiate graduate
training a few years into an academic career, spurred perhaps by realizing that, while you are truly
interested in having a successful academic career, it is not going as well as you would like. Academic
physicians may believe that proposing graduate study will be negatively received by departmental or
medical school leadership. However, department chairs and deans may develop an interest in training
to properly conduct the large-scale projects that their positions now make available.
Another important strategy is to remember that not all the time and money to be invested must be your
own. Some academic positions offer tuition benefits as a standard benefit (when it is job-related, tuition
benefits are not subject to federal income tax, at least right now). Whether you are just starting out,
changing jobs, or even if you are an established faculty member, consider negotiating, along with salary
and other considerations, a graduate degree package, typically including such features as clinical
flexibility or tuition reimbursement. A sabbatical, perhaps funded by the SAEM Scholarly Sabbatical
Grant, may also provide an opportunity for graduate education. Remember, your department chair and
dean sincerely want you to succeed, and a graduate degree may make the difference. Be sure to point
out how your new degree will enhance your academic career and the department in general; no chair
will want to spend scarce discretionary funds to help you make more money in industry.
A third strategy is to make school work do double or triple duty. For example, if you take a course on

decision analysis, use it to analyze an important clinical problem, then present your work at a national
meeting and publish it in the medical literature, while improving your own practice. If you do a research
thesis, use it as a way to learn new techniques, to work with accomplished senior collaborators, and to
publish at least two papers (a literature review based on the background information you have gathered,
and an original research paper). Many who adopt this policy are surprised to find their academic
productivity actually going up while obtaining an advanced degree, due to the focused, deadline-driven
nature of the course work. Similarly, if supervised teaching is part of your graduate degree program, try
to teach a course that will meet faculty teaching requirements, or at least enhance your standing with
your department chair or dean. If your initial negotiations for financial or time backing with your
department chair were unsuccessful, a few such academic successes may provide an opportunity for re-
negotiation.
A final strategy: try to do something you enjoy. If you are uncertain, try enrolling in a course or two
before committing to a degree program. You may find yourself drawn to unexpected areas, and may
ultimately dramatically alter, and enhance, your career. If you dislike it, at least you can get out early!
Discussion of three areas of particular interest, public health, administration, and education, follow. They
offer general as well as specific ideas in those areas. Reading this chapter may offer insights to those
interested in pursuing any of these or even a different field all together. Because the time commitment
required to earn a doctoral degree is typically difficult (but not impossible!) to reconcile with an ongoing
academic career, the majority of the discussion is geared to those seeking certificate or Master's degree
training, but the information will also be of interest to those considering doctoral programs. Those who
have further questions after reading the discussions should seek advice from others who have earned
graduate degrees. Degree program directors often have experience and insight regarding the
application of their training that is unavailable elsewhere; it is always worth meeting with a potential
program director well before formally applying to a program.
Public Health
The most common graduate degrees obtained by academic emergency physicians are probably in
public health. Most popular is the Master of Public Health (M.P.H.) degree, but there are many
variations, including Master of Health Science (M.H.S.), Master of Science in Public Health (M.S.P.H.),
Master of Science in Clinical Epidemiology (M.S.C.E.), or Master of Science in Health Services

(M.S.H.S.). Doctoral programs in such related areas as epidemiology, health services research, and
health policy are also widely available. Certificate programs are also available, leading to non-degree
training in specific topics.
The variety of master's level programs in public health and related areas is incredible, especially for
those more familiar with lock-step M.D. and residency programs. From general surveys of public health
to those with a specialized area of focus and requiring a thesis, the M.P.H. degree can represent a wide
spectrum of training. This allows great freedom for emergency physicians to study what interests them
the most. Programs will typically have core courses in biostatistics, epidemiology, environmental health
sciences, health services administration, and social and behavioral sciences; these are the five areas of
knowledge considered basic to public health and required for accreditation by the Council on Education
for Public Health (CEPH). Enrolling at an M.P.H. program that is accredited by CEPH (or its equivalent
in related fields) is preferable, as accredited programs must maintain demonstrated high quality to meet
the standards. Advanced coursework is typically available in all these five areas as well, along with
other upper-level courses that reflect the strengths of each program. These may include such diverse
areas as informatics, public policy, international health, ethics, maternal & child health, health care
policy, and many more. Spending some time at the CEPH web site, www.ceph.org, which has links to
accredited programs, will provide insight into what is available both in your area and around the United
States.
The tendency go directly from residency to an academic faculty position can put emergency physicians
at a disadvantage when competing in the academic realm. Having an M.P.H. can help you overcome
some of these disadvantages, both by actual improvement in academic skills and by having an
additional credential. Since so many academic emergency physicians do clinical research without
specific training, an advanced degree in public health can pay off by providing important skills in the
design and conduct of clinical research. This will lead to better research which is likelier to lead to actual
improvements in the field of emergency medicine. Grant proposals made by an emergency physician
with an M.P.H. are also likelier to be funded, both because of the additional formal credential and
because formal or informal training in grant-writing may be part of the curriculum.
Although mentorship is crucial to academic success, many academic emergency physicians have
trouble finding suitable mentors. Public health training provides access to successful medical scholars,
some of whom will be willing to collaborate with and mentor an emergency physician working to

establish an academic career. Also, do not forget that fellow students may also be looking for
collaborators; many are already accomplished in their specific areas, or may be members of successful
research teams that would love to add a hard-working academic emergency physician with public health
training to their group. Their access to patients in the acute phases of illness make emergency
physicians attractive to many research efforts; those with abilities in research design and conduct are
especially valuable.
There are two typical venues for studying public health: graduate schools of public health, and graduate
programs in community health/preventive medicine. The latter are typically based in a department of a
medical school; some are based in a school of health and human services, allied health, or the like.
National rankings of public health school-based programs may be found at the U.S. News & World
Report website, www.usnews.com/usnews, by clicking the "education" tab, then looking at graduate
school rankings for public health. Given their scale and focus, the schools of public health usually offer a
richer array of public health programs. Smaller-scale programs, however, should not be overlooked, as
they may offer excellent educational opportunities in areas of specific interest, and lots of flexibility. For
those at a distance from any programs, quality distance learning programs, such as the "career MPH"
offered by the Rollins School of Public Health at Emory University, are available
www.sph.emory.edu/CMPH/index.html.
Management and Leadership
As much as any medical specialty, and more than most, emergency medicine requires physicians to be
adept clinician-managers. There are numerous opportunities for those interested in going beyond
patient-level management to take on a variety of Emergency Department administrative tasks, such as
clinical directors, division chiefs, department chairs, EMS director, and quality managers, as well as
hospital- and medical school-level leadership positions. As emergency medicine matures, an increasing
number of leadership positions will go to those with management experience and specific training. Many
of these will be physicians whose academic careers have led them to leadership positions for which
they would like to become better-trained; thus, a mid-career investment in a management degree is
becoming increasingly common.
There are numerous benefits to formal management training. Although there is a role for a combination
of innate ability and on-the-job training in management and leadership, graduate training is widely

available and perhaps a more reliable path to successful leadership, whether specifically in Emergency
Medicine or elsewhere in health care. Far from learning how to sell used cars or take advantage of HMO
customers, management training focuses on such areas as understanding systems, budgeting
resources, strategic planning, and aligning incentives. Academic emergency physicians address these
sorts of issues regularly, giving even the most general business management training a feeling of
relevance and immediate usefulness in daily academic practice. However, a caveat often mentioned by
management authorities is worth repeating here. Those seeking to escape from the business aspects of
the practice of modern medicine by going into health care leadership will almost certainly be even more
dissatisfied with management jobs. Therefore, those seeking leadership / management will be happiest
and the most successful if they do so as a means of achieving a goal rather than avoiding the pressures
of clinical practice.
Graduate training in administration and leadership is available at two levels. A wide variety of non-
degree "certificate programs" offer introductions to management principles for health professionals or
instruction in specific health-related leadership or management topics. These programs are typically
offered at university medical schools, business or management schools, or schools of public health.
They are generally expensive. Most offer CME credits; some double as introductory courses for formal
degrees. Notable examples of certificate courses include the wonderful offerings in health care
leadership of the Harvard University School of Public Health www.hsph.harvard.edu/ccpe/. Although
most are site-based, several distance learning programs are available. For example, the University of
South Florida has a distance learning Business of Medicine Certification Program for physicians, which
may be extended into a distance learning executive M.B.A. for physicians program
www.coba.usf.edu/programs/docs/.
It is important for potential physician managers to be aware of The American College of Physician
Executives (ACPE). This organization of more than 12,000 physician managers offers a wide variety of
distance learning and conference-based educational programs in medical management. Distance
learning formal degrees are also available to its members. These include the Master of Medical
Management (M.M.M.) degree, in conjunction with either the University of Southern California, Tulane
University, or Carnegie Mellon University www.acpe.org/Degrees/index.htm. A Master of Science in
Administrative Medicine (M.S.A.M.) program is also available, in association with the University of
Madison-Wisconsin Medical School www.medsch.wisc.edu/adminmed/.

Formal management degree programs, both health care specific and in general management, are
widely available. Most common is the Master of Business Administration (M.B.A.), which may be general
or have a health care concentration. Several other health care management degrees are also available,
depending on the curriculum and university preference. These include the M.M.M. or M.S.A.M. degrees
as noted above, Master in Health Administration (M.H.C.A.), and the like. An interesting variation is the
Master of Public Administration (M.P.A.), Master in Health Care Administation (M.H.C.A.), and the like.
An interesting variation is the Master of Public Administration (M.P.A.) degree; New York University, for
example, has a highly-regarded M.P.A. program with a specific focus in Health Policy and Management
(see www.nyu.edu/wagner/programs1.html). A national ranking of programs in health care
administration is available at http://www.usnews/com/usnews click on the "education" tab, then search
the graduate schools listings. Many physicians seeking management training, however, prefer to enroll
in programs without a specific health care focus, either in general management (usually an M.B.A.) or
with an emphasis in another area, such as marketing or finance (M.B.A. or M.S. degree). For some, this
is a specific decision to obtain more flexible, general training; many find that such a program may simply
be the most convenient.
Since a full-time degree is often impractical and part-time study may take several years, the two-year
executive M.B.A. format has become popular for physicians. Both general M.B.A. and health care-
oriented executive M.B.A. programs are available. For example, the Olin School of Business at
Washington University offers both general and health services management executive M.B.A. programs
www.olin.wustl.edu/execed. Classes typically meet on Fridays, alternate weekends, or some similar
schedule, and have significant team-based non-class assigned projects. Although they are rigorous,
graduates of executive programs often speak highly of their training.
Education
The role of the Clinician-Teacher in the academic medical center is being increasingly recognized.
Curriculum re-design and sophisticated educational objectives and assessments are becoming
common. As the rewards for medical school teaching excellence and leadership slowly become greater
and more apparent, more academic physicians are finding formal graduate training in education an
attractive choice. Those with formal educational training are in an excellent position to conduct research
into educational interventions and their assessments. The wide variety of teaching methods and the
availability of learners at all levels in academic medical centers offer many opportunities for research

that can truly improve medical education and practice. Formal educational training may make those
seeking administrative advancement especially good candidates for clerkship or residency directorships,
or even dean-level positions, both at the medical school and university levels.
Master's degrees in education are widely available, and vary widely in quality. Along with general
educational offerings, university schools of education typically offer specialized training that may be of
particular interest to academic physicians, such as the M.S. in administration with a concentration in
higher education available at the University of Rochester's Warner School of Education and Human
Development www.rochester.edu/Warner/programs/elhigher1.html. Those seeking excellent short-
course experiences may be interested in the Harvard Macy Institute Program for Physician-Educators
and Program for Leaders in Medical Education www.hms.harvard.edu/oed/macy/. Additionally, many
medical schools and universities offer faculty development seminars in teaching the adult learner, an
area in which many of us can improve.
Summary
Advanced graduate education has much to offer the academic emergency physician, but requires time,
energy, and commitment. Those interested in more rewarding or effective academic careers and those
seeking administrative advancement may find a formal graduate degree program an enjoyable and
effective tool in achieving these goals. Along with the degree itself, the process of graduate education,
such as interactions with other students and faculty, will be beneficial. The academic emergency
physician with well-established goals and an advanced degree is in an excellent position for future
academic success.
Acknowledgments: Thanks to E. John Gallagher, M.D, Sandra M. Schneider, MD, and Frank L.
Zwemer, Jr., MD, MBA for critical readings of drafts of this chapter.
Making the Move From Regional to National Prominence
Author: Arthur L. Kellermann
What is "national prominence"?

Many promotion and tenure committees require candidates for promotion to the rank of Associate
Professor level to achieve "national prominence" in their field. Virtually all promotion and tenure
committees require achievement of "national prominence" for promotion to the rank of Professor.
Unfortunately, there are no explicit criteria for what constitutes "national prominence". Perhaps the
best definition for "national prominence" is the one given by Justice Hugo Black of the U.S. Supreme
Court when he was asked to define the term "pornography" – "I know it when I see it".
How is "national prominence" determined?
Since national prominence is subjectively defined, identifying it requires the concurrence of a majority
(if not a consensus) of the group of individuals who is tasked with the responsibility of weighing the
merits of faculty promotions at your institution. At most hospitals or universities, this group is known as
the "Promotions and Tenure (P&T) Committee", or some closely related term.
When you are ready for promotion, you will be asked to prepare a packet of information that includes
an up-to-date CV, perhaps a copy of your teaching portfolio, and 2-5 representative reprints of articles
you have authored or co-authored. This packet will be accompanied by a "Chairman's letter" that
presents a succinct case for why you merit promotion. If you belong to a "Division" or a "Section" of
Emergency Medicine in another clinical department rather than in an autonomous academic
department of EM, your division or section chief will most likely write this letter for your department
chair. The task of writing this letter will be much easier if you can provide concrete evidence that you
have made, and are making, an impact on Emergency Medicine at a national level.
The vast majority of the members of institutional Promotions and Tenure (P&T) committees are drawn
from departments other than the candidate's own. To validate your chair's assertion of the value of
your contributions, most P&T committees will ask senior EM faculty at other institutions to
independently evaluate the significance of your work, and your prominence in your field. This creates a
paradox for most EM chairs and faculty members. While the demands of academic EM are great
(clinical shifts, student and residency lectures, mentoring, and departmental and hospital committee
work) these efforts don't count as much as they should when it comes time for promotion. The blunt
truth is that giving an excellent lecture given at a national meeting or another medical school counts far
more towards establishing your "excellence in teaching" and "national prominence" than giving the

same excellent lecture at your own institution! This leads to the following warning: if you spend all of
your professional time and energy working inside your institution for your own department, and are not
well known outside your own institution, you may encounter difficulty gaining promotion beyond the
rank of Assistant Professor. As a department chair, I can assure you that it is very hard to claim that a
member of my faculty has achieved "national prominence" in his/her field if the faculty member has not
taken the time to become visibly involved in specialty activity at a national level.
What do you need to do to achieve "national prominence"?
Fortunately, achieving national prominence in Emergency Medicine is not as hard as it sounds.
Academic EM is still a fairly small club. There is plenty of room for anyone who wants to get involved in
organizational activities at a regional or national level. The number of "alphabet soup" national EM
organizations (e.g., ACEP, SAEM, ABEM, CORD, AAEM, NAEMSP,) is large, and insures ample
opportunities for you to get involved. . Given the meritocracy of Emergency Medicine at the national
level, anyone with talent, energy and commitment can quickly gain entry to the national scene.
There are several ways you can achieve regional and/or national prominence:
1. Show up – Given the crazy schedules that most Emergency Physicians work, it takes a
considerable amount of effort to cluster your free days together in order to attend a state, regional or
national meeting. Do it. You won't get known outside your institution if you don't make an effort to meet
your colleagues at regional and national professional meetings.
2. Speak up – If you have something to say at a meeting, say it. If you have a special interest or
expertise that an EM organization can use, offer it. At academic meetings like SAEM, making periodic
trips to the microphone to ask cogent questions or offer useful insights is a good way to increase your
visibility and become engaged in the intellectual discourse of the meeting. Like anything else, this can
be overdone. Don't hog the microphone!.
3. Volunteer – Committee assignments can be a blessing, or a curse. Service on a national committee
or task force is a great way to meet colleagues from around the country and become better known. If,
however, you are not careful, committee work can become a tremendous drain on your time and
energy. Beware of becoming overextended by volunteering for too many assignments, or getting

drawn into a long or complex project that has little hope of success. If you are unsure of what to do,
consult a senior colleague or ask your chair.
4. Network – It is fairly easy to get placed on a committee or task force; all you have to do is submit a
written expression of interest within the time frame requested by the organization. You can enhance
your chances by asking your chair, chief, or a key faculty colleague to lobby on your behalf, or by
contacting the chair of the task force directly. If you know a board member of the organization, they
may be able to speak on your behalf. Emergency Medicine is a remarkably egalitarian organization.
Those of us who are fortunate enough to have reached a position of leadership within EM haven't
forgotten what it was like to be a resident or a new faculty member. We are very approachable. If you
don't know a colleague who are active at a national level, the odds are great that your chair, chief, or a
faculty colleague does – work through them to secure the support you need.
5. Produce – It is not enough to show up and volunteer. You also have to produce. If you undertake a
research project, produce high quality work. If you accept assignment to a national committee, you are
duty-bound to follow through on your assignments and responsibilities, including showing up at the
meeting and participating in conference calls. If you don't, the likelihood that you will be picked for
future service will be markedly diminished. Committee and task force chairs are generally selected
from the ranks of committee members who have logged the time, followed through on their
assignments, demonstrated initiative, and acquired the experience they need to be effective leaders.
6. Focus – Emergency Medicine, by its very nature, is broad. In addition to maintaining your clinical
and teaching skills, you should try to develop concentrated expertise in one or at most a very limited
set of topics. Most of the leading figures in academic EM are respected for their expertise in a
relatively focused area of knowledge. Figure out what you want to be known for, and develop your skill
and/or expertise in that topic or area of endeavor. Once you have acquired in-depth knowledge of the
issue, you will be ready to publish one or more high-quality case reports or review articles on the topic,
give national-quality lectures at other programs or national venues, and initiate research to expand
your (and the specialty's) understanding of the issue.
7. Present your work – Presenting a research abstract at a national meeting is fun and ego-enhancing.
It is also a great way to earn a spot on your program's "traveling squad"! Preparing interesting didactic
sessions at SAEM or a strong course at ACEP Scientific Assembly, Winter Symposium, or another EM

organization's annual meeting is a great way to boost your visibility and add "national talks" to your
CV. Don't overlook opportunities to present at International meetings. While they carry a particular
mystique and often impress P&T committees, it is typically easier to get a paper accepted at one of
them than it is at a competitive national meeting like SAEM! The reason this is true is that the
organizers of these meetings are often highly dependent on registration fees to fund the event. Since
they know that few people will incur the time and expense to fly across the ocean to simply "attend"
their meeting, they generally accept most (if not all) submitted papers to boost attendance. The
downside for you (and your program) is cost. Don't be surprised if your chair has a stroke when you
ask for program support to present a paper at a meeting in Europe or Asia. My advice is to float the
idea in advance.
8. Publish your work – Presenting papers and posters at national meetings is fun, but the effect is
transient. The only way you will make a lasting contribution to Emergency Medicine is by publishing
your work in a peer-reviewed journal. The same can be said for the written product(s) of many
organizational committees and task forces. If one of the objectives of your committee is to produce a
report, position paper, or other document, make sure you make enough of a contribution to warrant
inclusion as a co-author, if not the lead author. In addition to raising your national visibility, publications
are essential to meet another criterion for promotion – demonstrating at least "adequacy" in
scholarship (see related chapter: Why do Research?).
9. Persist – Few of us were lucky enough to succeed the first time out. Don't be discouraged if your
first abstract or manuscript is rejected, if you lose an election (all of us have), or you are passed over
for a committee or task force. Learn what you can from the experience, be gracious in defeat, and try
again. .
10. Maintain balance – If you want to succeed in academic emergency medicine, you have to stay in it
for the long haul. High-quality research can take years to produce. Leadership roles in EM
organizations can take even longer. If you try to take on too many projects, or tackle too much too
soon, you will burn out and abandon the quest.
11. Help others along the way – As you begin to climb the ladder of academic success, don't overlook

opportunities to advise, mentor or help others. Remember all of the favors done for you, and extend
the same courtesy for those who come behind you. Seek to advance the careers of your colleagues,
whether they work at your institution or at another program. By helping others freely and willingly, you
will advance the interests of emergency medicine, and make countless friends. Someday, they (or
their friends) may be in a position to repay the favor. One more thing – if you achieve national
prominence in EM, the day will come when you will be asked by a "Promotions and Tenure"
Committee from another institution to provide written comments on the merits of promoting a worthy
colleague. If that happens (and once it does, it will happen again and again) give this and all
subsequent requests the same level of care and attention that senior EM colleagues gave your
promotion.
12. Don’t forget your colleagues back home – Once you achieve a measure of national recognition,
don't be surprised if this stirs jealousy or resentment among your colleagues back home. To minimize
the likelihood of this happening, freely acknowledge their role in your success, make sure you carry
your share of the load, and use your newly won recognition for the good of the program. If you are a
"name" that applicants to your program will recognize, make sure you help on interview days. If you
get time off to attend a national EM meeting, make a point of repaying your colleagues when they
need time off for special trips or family activities. If you are rewarded with a reduced clinical load
(a.k.a., "protected time") to conduct research or participate in national activities, make sure that you do
your fair share of nights, evenings and weekends.
13. Don’t forget your family at home – Travel is exciting and service to national organizations is a real
ego trip, particularly when both are new. There is a great danger, however, in letting success go to
your head. Take the time to count the number of nights and weekends that you spend traveling, and
add them to your night and weekend shifts. This is the amount of time you are away from your family.
Too many organizations expect their leaders to sacrifice their families or their most important
relationships to the job. It is a bogus and self-defeating expectation. It is up to all of us to redefine the
terms of "success" so that gifted academic emergency physicians can contribute to the specialty and
achieve "national prominence" without sacrificing those who make it all worthwhile.
Conclusion:
Academic Emergency Medicine rarely pays as well as comparable efforts in private practice, but it

offers rewards that more than offset this economic difference. One of them is the satisfaction of
teaching – whether it involves medical students, EM residents, rotating house staff from other
specialties, paramedics, or professional colleagues through continuing education. Another reward is
the opportunity to push the boundaries of the specialty through basic and applied research. A third is
the opportunity to travel, both nationally and internationally, with the attendant opportunity to interact
with energetic and visionary colleagues who share your values and ideals. Finally, academic EM offers
an opportunity to make a difference – whether it is locally, regionally, nationally or internationally – and
in the process, earn recognition for your contributions. In short, academic EM offers a ready path to
achieving "national prominence" in your field – along with the satisfaction, and the opportunities, that
this brings. .
Opportunities for Faculty Development in National Organizations
American Academy of Emergency Medicine
Author: Robert McNamara
Introduction
The American Academy of Emergency Medicine (AAEM) was founded in 1993 primarily to address the
needs of the clinical emergency physician and to promote the importance of Board Certification in
Emergency Medicine. Our current membership is approximately 3,500 and we have expanded our
mission by providing educational offerings, political representation, and practice assistance to

emergency physicians. There are numerous opportunities for faculty and leadership development
available to the academic emergency physician.
Educational Programs
AAEM offers a yearly Scientific Assembly that is geared to the level of the practicing board-certified
emergency physician. For example the 2002 offering included:
1. Airway Management Course - covers difficult airway, new techniques and equipment.
2. Ultrasound Course - comprehensive 11.5 hour course with live models.
3. Pediatric procedures course - advanced techniques, hands on instruction.
4. Tour of a CA vineyard - designed to enhance your status at medical staff dinners.
Teaching Opportunities
AAEM offers another venue for national speaking engagements at our Scientific Assembly. In addition,
we have partnered with the European Society for Emergency Medicine to initiate biannual conferences
in the Mediterranean region. The first held in Stresa, Italy in September 2001 was a huge success.
Currently, we are planning a conference for 2003 in Barcelona. Opportunities also exist for teaching at
our board review courses.
Publications
AAEM has recently created, in conjunction with Emedicine, an internet-based textbook for laypersons
where authorship roles are available. The Journal of Emergency Medicine is our official journal. In
addition to traditional scientific articles we seek articles and editorials related to the AAEM mission. As
an example, JEM recently published an article about our joint effort with SAEM and CORD regarding
resident moonlighting. Our national newsletter, Common Sense, and the California chapter's California
Journal of Emergency Medicine are also open for submissions. AAEM periodically publishes
monographs for the membership and is willing to review ideas for such products.
Leadership Roles
Promotion committees are always impressed with national society leadership roles and such roles can

raise one's stock in the eyes of the medical school leadership. AAEM is notable for its open path to
leadership roles. Through our one member, one vote system open pathways exist for leadership in
national AAEM and our state chapters (currently organized in CA, TX, LA, WI and starting in FL and
OH). We have a standard complement of the requisite committees and pride ourselves on responding to
member input by quickly formulating task forces to address specific items. For example, we recently
created a task force to examine the use of thrombolytics in acute stroke. A message to [email protected]
is all it takes to be considered for these roles. On the more traditional side, AAEM appoints two
Associate Editors for the Journal of Emergency Medicine and an Editorial panel for our newly developed
charting template.
Appointment/Liaisons
As a national organization, we receive frequent requests to send representatives to interdisciplinary
meetings/working groups and rather than select from an "insider" pool we generally solicit nominations
directly from the members via e-mail.
Other Opportunities
1. Annual resident research forum - members participate as abstract reviewers and judges.
2. State Chapter creation - if ambitious we are always looking for folks to create new state chapters. We
have laid out the requisite steps in a document you can request.

American Board of Emergency Medicine
Author: Robert Hockberger
THE AMERICAN BOARD OF MEDICAL SPECIALTIES
The concept of board certification in medical specialties (ie, the administration of a single standardized,
nationwide examination to graduates of training programs in a specific medical discipline) began in the
United States with the establishment of the American Board of Ophthalmic Examinations in 1917. The
specialties of Otolaryngology, Dermatology and Obstetrics and Gynecology soon followed suit. In 1933,
representatives from these specialty boards participated in a conference with the American Hospital
Association, the Association of American Medical Colleges, the Federation of State Medical Boards, the
American Medical Association Council of Medical Education, and the National Board of Medical
Examiners. As a result of that conference, the American Board of Medical Specialties (ABMS) was
founded with the mission of "maintaining and improving the quality of medical care by assisting member
boards in their efforts to develop and utilize professional and educational standards for the evaluation
and certification of physician specialists."
By 1949, all existing medical specialties were represented within the ABMS. In 1969, the ABMS
introduced the concept of periodic recertification, i.e., periodic retesting to assess continued
competence over time. In 1999, the ABMS organized an effort of its member boards to develop the
components of a maintenance of certification program to promote lifelong learning and improvement in
clinical practice over time. The components of the program are:
1. Evidence of professional standing.
2. Evidence of a commitment to lifelong learning and involvement in a periodic self-assessment process.
3. Evidence of cognitive expertise.
4. Evidence of evaluation of performance in practice.
Each board is currently developing its own maintenance of certification program using these
components. Individual boards may implement their programs as early as 2003.
THE AMERICAN BOARD OF EMERGENCY MEDICINE
The American Board of Emergency Medicine (ABEM) became the 23rd member-board of the ABMS in
1979. This was accomplished with the support of the American College of Emergency Physicians, the

University Association for Emergency Medicine (now the Society for Academic Emergency Medicine)
and the American Medical Association. Over the past two decades, ABEM has become a recognized
and respected member of the ABMS due to its development of both oral and written examinations that
are based upon a scientific analysis of the practice of emergency medicine (i.e., the Emergency
Medicine Core Content), its use of high-quality research to assess and improve the validity and reliability
of its examinations, and its willingness to play a leadership role in innovations pioneered by the ABMS.
ABEM plans to implement its maintenance of certification program, termed the Emergency Medicine
Continuous Certification (EMCC) Program, in 2004.
Mission and Purpose
The mission of ABEM is "to protect the public by providing and sustaining the integrity, quality, and
standards of training in and practice of emergency medicine."
To accomplish that mission, the purposes of ABEM are scientific and educational and include
the following:
To improve the quality of emergency medical care;
To establish and maintain high standards of excellence in the specialty of emergency
To improve medical education and facilities for training emergency physicians;
To evaluate specialists in emergency medicine applying for certification and
recertification (soon to be continuous certification);
To grant and issue to qualified physicians certificates or other recognitions of special
knowledge and skills in emergency medicine and to suspend or revoke same;
To serve the public, physicians, hospitals, and medical schools by furnishing lists of
those diplomats certified by ABEM.
To accomplish these purposes, ABEM participates in the following endeavors:
The development and administration of certification, recertification and residency in-
service examinations.
The development of a continuous certification program with an expected

implementation date of 2004.
The conduct of research to assess and improve the reliability and validity of its
examinations.
The performance of an ongoing longitudinal study of emergency physicians to
determine those factors that promote and detract from a successful and satisfying
career in emergency medicine.
The annual publication of demographic information about emergency medicine
residency programs.
The contribution of proposed changes to the Special Requirements for Emergency
Medicine that are used by the Emergency Medicine Residency Review Committee to
accredit training programs.
The analysis of proposals to develop combined training programs and subspecialties
within the field of emergency medicine.
The participation in joint endeavors with other emergency medicine organizations to
benefit the field of emergency medicine.
Opportunities for Involvement
Item Writer
ABEM annually administers certification, recertification and residency in-service examinations using a
databank of approximately 7,000 items (questions) that is constantly being updated and expanded by a
team of item writers. Item writers are expected to write 24 questions per year. They meet with the exam
editors and staff each summer at a retreat where new item writers are trained and all item writers are
given feedback on their performance during the previous year.
Item writers are appointed by the Test Development Committee, based upon recommendations of
committee members; however, individuals are welcome to send CVs and letters of interest to the
committee for consideration. To be eligible for appointment one must 1) have successfully completed an
ACGME-or RCPSE-approved emergency medicine residency, 2) be an ABEM diplomate for at least 5
years, and 3) be actively involved in the practice of clinical emergency medicine. Experience and
background in medical writing is also considered. Item writers are appointed for a 3-year term, and may
seek reappointment for a total of 2 terms.

Oral Examiner
ABEM annually administers two oral examinations using a pool of trained examiners. The qualifications
for appointment as an oral examiner are the same as those for item writers. Nominations most often
originate as suggestions from current examiners and directors of the board; however, individuals may
apply directly by submitting a letter of interest, current CV and brief description of their clinical practice
to the chair of the Test Administration Committee. For a nomination to be considered it must be
supported by a current or senior director of the board.
Oral examiners are appointed for a 3-year term, and may seek re-appointment for a total of 3 terms.
During the appointment period, examiners are expected to be available to participate in at least one of
the two 4-5 day examinations that are administered annually in the spring and fall. Examiners are
provided with training and feedback about their performance, and also participate in the data collection
phase of the board’s ongoing quality control of its examination.
Oral Examination Team Leader
Team leaders supervise a "team" comprised of 8-12 examiners at each oral examination. They train
their team to administer the examination cases, monitor the performance of those individuals, and
provide them with appropriate feedback. They also participate with the chief examiners and staff in
reviewing the cases at the end of each examination. To be selected as a team leader an examiner must
have 1) participated as an examiner on all 3 examination teams, 2) received consistently good
evaluations for their performance as examiners, and 3) exhibited a high level of medical knowledge and
leadership skills through their participation as examiners.
Senior Oral Case Reviewer
Senior oral case reviewers are periodically selected to review, update and edit oral examination cases.
They often present their recommendations to a case review panel that convenes at each oral
examination. These individuals are selected from the current pool of oral examiners.
Case Selection Panel Member

The Test Administration Committee selects one team leader each year to participate in the selection of
cases to be administered at the following year’s examinations.
Case Development Panel Member
The board periodically selects several individuals to participate with members of the Test Development
Committee in developing new cases for the oral examination. These individuals are selected from the
current pool of team leaders and oral examiners. Each participant is expected to develop several cases
using real patient encounters from their own practice and the board’s guidelines for case development.
All panel members then participate in a meeting to discuss, modify and finalize the cases, which are
then field tested at subsequent examinations.
Subspecialty Subboard or Examination Committee Member
ABEM has collaborated with several other boards to develop subspecialties in Medical Toxicology,
Pediatric Emergency Medicine, Sports Medicine, and Undersea and Hyperbaric Medicine. ABEM
appointees to subboards or subspecialty examination committees must be board certified in the
particular subspecialty. Nominations are usually submitted by the individual subboards or by ABEM
directors. Sub-board members develop the examinations for subspecialty certification and
recertification, review candidate subspecialty applications, and recommend examination and training
standards.
Director
Individuals selected to be ABEM directors must be residency-trained and board certified in emergency
medicine and, in the opinion of current board members, possess the knowledge and expertise
necessary to help the board accomplish its mission and purpose. New directors are elected by current
board members from a slate of nominees submitted from either a sponsoring organization (ACEP,
SAEM or the AMA) or by the ABEM Nominating Committee.
Directors are elected for a 4-year term, and are eligible for reelection for a second term. They are
expected to serve on one or more of the board’s committees or task forces, and to attend the semi-

annual 5-day board meetings that take place in the summer and winter. Some of the directors serve as
liaisons to the sub-boards, many participate as team leaders and chief examiners for the examinations,
and most participate in presenting the "ABEM Presentation to Training Programs (PTP)" to emergency
medicine residencies throughout the country.
ABEM’s major committees include the Credentials Committee, the Test Development Committee, the
Test Administration Committee, and the Academic Affairs Committee. ABEM’s current task forces
include the Oral Examination Task Force, the Maintenance of Certification Task Force, and the
Presentation to Training Programs Task Force, the Longitudinal Study Task Force, and the Residency
Information Task Force. Directors serve as ABEM’s representatives on joint task forces with other
emergency medicine organizations in efforts to advance the specialty. Recent examples include the
Emergency Medicine Core Content Task Force and the Scope of Training Task Force. Directors also
serve on ABMS committees and as representatives to the AMA.
Senior Director
Current directors become senior directors following their terms of appointment on the board. Senior
directors may participate in the PTP program, may be selected by the board for appointment to the
Emergency Medicine Residency Review Committee, and may be supported by the board in ongoing
involvement within the ABMS.
A Final Thought
ABEM’s Longitudinal Study shows that the major factors that promote career satisfaction in emergency
medicine are 1) emergency medicine residency training, 2) perceived low levels of stress and fatigue
(largely related to the particular job that one chooses), and 3) the perception that emergency medicine is
exciting and challenging (largely related to "keeping up" medically and "getting involved" in emergency
medicine outside of one’s clinical practice). Involvement with ABEM or other emergency medicine
organizations not only benefits those organizations in their efforts to develop and advance our specialty,
but also benefits the individual by creating a sense of accomplishment within an environment that
promotes the development of strong personal and professional relationships that are often lifelong and
sustaining.

American College of Emergency Physicians
Author: Robert Schafermeyer
The American College of Emergency Physicians (ACEP) believes that the support of academic
emergency medicine is essential to the success of the residency programs, of the faculty and,
ultimately, to the success of the specialty. ACEP currently provides the following programs or activities
for faculty development.

Teaching Fellowship
For over 10 years ACEP has implemented the teaching fellowship program. The program is a 12-day
course covered in two separate sessions (August and March). Session topics include instructional
system design, curriculum development, effective teaching methods, evaluation methods, the RRC-EM
process, funding and grantmanship, mentoring and research, scientific writing and publishing, and life
management skills. The program is designed for faculty in residency programs who want to improve
their skills, for residents interested in an academic career, and other physicians who have responsibility
for teaching emergency medicine. This program is updated regularly based on evaluations and needs
assessment.
Research Training
The Emergency Medicine Basic Research Skills (EMBRS) workshop is a 4 year-old program that was
developed for junior faculty with limited research experience. Also, it was developed for physicians in
academic and community medical centers who are interested in research but have little training in
research basics, for physicians involved in mentoring young researchers, and for fellows in non-
research fellowships. The workshop is a 12-day course covered in two separate sessions (November
and April). Edward A. Panacek, MD, MPH, FACEP, is the course director. Topics include design basics
for clinical research, research methods, statistics, IRB and informed consent, presenting research, grant
writing, and finding funding sources. This program is updated on a regular basis, similar to the one
utilized for the teaching fellowship.
Research Forum
This annual program, held in conjunction with ACEP's Scientific Assembly, provides a forum for
researchers to discuss original emergency medicine research. The program includes oral and poster
presentations as well as a moderated session on the best and most interesting scientific presentation.
The Emergency Medicine Foundation (EMF) presents awards for the best paper and for the young
investigator. The awards support emergency medicine faculty and residents in their academic
achievement efforts.

National Case Presentation Competition (CPC)
The finals competition is sponsored by CORD, SAEM, EMRA and ACEP. Cases are presented by
emergency medicine residents and then discussed by residency program attending physicians.
National Faculty Teaching Award
This annual award honors up to 10 outstanding emergency medicine faculty. This award is designed to
support emergency medicine faculty in their academic efforts, particularly for emergency medicine
faculty in tenure track positions. The award is based on significant contributions in the traditional
academic areas of clinical teaching, lecture presentations at their institution and at a state and regional
level, research, specialty society and community service.
Emergency Medicine Foundation (EMF) Grants
EMF provides several $50,000 career development grants, a $50,000 established investigator award,
and several $35,000 research fellowship grants each year. The career development awards are
intended for emergency medicine faculty at the instructor or assistant professor level who need seed
money or release time to begin a promising research project. They are designed to be career launching.
The $50,000 established investigator award is intended to fund projects by established researchers who
may wish to try a pilot project or undertake research in a new area.
The $35,000 research fellowships are designed for emergency medicine residency graduates who will
spend another year acquiring specific basic or clinical research skills and further didactic training in
research methodology.
Advocacy Policies
Through its collaborative efforts with other emergency medicine organizations and through its Academic
Affairs Committee activities, ACEP develops policies that support residency programs and faculty.
Examples of current activity include collaboration with CORD on development of a residency closure
process, and in conjunction with SAEM development of a policy on faculty sabbaticals. ACEP has

wellness policies on family leave, physician impairment, and shift work.
ACEP supports legislative and regulatory efforts through activities in the Washington, DC office. The
office monitors graduate medical education legislation to identify key issues, to introduce legislative
efforts, to amend pending legislation and to coordinate efforts with the AAMC and SAEM. The office
regularly responds to the Health Care Finance Administration (HCFA) through public comment letters
and through meeting with officials at HCFA.
All of these programs and advocacy efforts are provided to enhance the academic faculty's ability to
enhance their career and to provide quality emergency medical residency training.

Society for Academic Emergency Medicine
Author: Brian J. Zink
Overview of SAEM
The Society for Academic Emergency Medicine (SAEM) is the largest academic organization in
emergency medicine (EM). SAEM was formed by the 1989 merger of the University Association of
Emergency Medicine and the Society for Teachers of Emergency Medicine. Approximately 2,100 of the
5,000 members of SAEM are active members who hold faculty positions at the nation's academic
emergency medicine programs. About 2,000 are resident members, and the remainder are medical
student and associate members. SAEM's Executive Headquarters in Lansing, Michigan, are staffed by
an Executive Director and a staff of about 5-6 people. The Society sponsors Academic Emergency
Medicine, a journal of peer-reviewed EM literature.
The SAEM Board of Directors, consisting of 11 elected members, is responsible for developing policies
and meeting the Society's mission of "improving patient care by advancing research and education in
emergency medicine". The work and activities of SAEM primarily take place through the Board of
Directors and the committees, task forces, and interest groups of the organization. Currently, there are
16 committees and task forces, and 27 interest groups. Interest groups vary from a minimum of 20
members up to over 100 members. The SAEM committees and task forces are responsible for carrying
out the yearly objectives that are developed in conjunction with the Board of Directors. Each of the
objectives involves a process or activity that relates to advancing research or education in the specialty.
The interest groups have a looser structure and develop their own objectives. Interest group projects
may range, for example, from attempting to influence federal policy in their area, to developing
educational products, to conducting multi-center research investigations. Interest groups serve as
breeding grounds and think tanks for innovative academic ideas.
The Annual Meeting

Each year SAEM sponsors an Annual Meeting that is the world's largest forum for the presentation of
original research in emergency medicine. The meeting also highlights educational presentations,
programs and projects. A variety of sessions each year are targeted toward the developing faculty
member; this might include a grant-writing workshop, a luncheon with senior researchers, a didactic
session on statistics, a teaching skills session, or a panel discussion on how to become involved in
health policy. The Meeting is an excellent time for networking with academic emergency physicians from
other programs, and for receiving advice and counsel from more experienced academicians. A large
amount of Society work also takes place at the Annual Meeting. Committees, tack forces, and interest
groups meet, organize, and initiate their work for the year.
Faculty Development Opportunities in SAEM
SAEM can play a key role in an individual's faculty development. The spectrum of SAEM involvement
can extend from simply reading the Society's journal, Academic Emergency Medicine and attending
didactic sessions at the Annual Meeting, to being elected to serve on the Board of Directors. As an
emergency medicine faculty member develops and seeks promotion, one common requirement for
advancement to the Associate Professor level is documentation of scholarly activity on a national level.
While this can occur through a faculty member's specific research and educational activities, it can also
occur through serving an important role in a national academic organization like SAEM.
A Stepwise Guide for SAEM Involvement
For those faculty who may be interested in career development that includes active SAEM involvement,
I would propose the following steps. This process does not happen overnight - it may take 5-10 years to
complete the steps listed below.
1. Become a member, subscribe to and read Academic Emergency Medicine, and the SAEM
Newsletter, and visit the SAEM website, www.saem.org. A great deal of information on the organization
and opportunities for academicians is found in these sources.
2. Attend and participate in the Annual Meeting. Ideally this will start as a resident physician. The Annual
Meeting is a great opportunity to get to know national figures in EM, and to network and interact with

peers and colleagues and mentors in the areas of research and education. Presentation of an abstract
or educational project at the Annual Meeting will increase a faculty member's standing in academic EM,
and will often result in that person being brought into a sphere of like-minded academicians.
3. Interest group involvement - Most young faculty members will define an area of research or
educational interests. En route to developing expertise in this area, the faculty member will have to get
to know the leaders in the focus area, and become familiar with their work. One good way to do this
within SAEM is to become involved in an interest group in the focus area. SAEM has 27 interest groups,
which cover a wide spectrum of topics and areas. Most junior faculty can find one or more interest
groups that deal with their academic interests. If an interest group does not exist for the faculty
member's area of interest, it is possible for a faculty member to start an interest group by finding 20
other members who are willing to pay the interest groups dues and initiate a new interest group. The
SAEM Executive Office can help with this process. There is no selection process for interest group
members, and the only requirement is the payment of a modest dues fee. It is possible for a junior
faculty member to rise to a leadership role in most interest groups within a few years by being an active
and eager participant. Some interest groups have committees and sub-committees, and heading up one
of these can be a good administrative experience. SAEM interest group involvement often provides a
young faculty member the opportunity to establish a mentor relationship with someone who is at a
different institution, and may have unique insights and experiences.
4. Committee and Task Force involvement - The next step to becoming more involved in the workings of
SAEM is to become a committee or task force member. Each year a committee and task force interest
form is sent out to SAEM members. Members submit their name for consideration to the President-Elect
who selects committee and task force rosters. The potential committee member is asked to describe
why he or she is interested in the particular committee, and what they could bring to the committee. The
President-Elect will attempt to have broad and diverse representation on committees and task forces.
Each year about 1/3 of the committee and task force rosters are turned over to allow participation of
new members. Surprisingly, fewer than 10% of active SAEM members submit a committee or task force
interest form. Therefore, the chances of being named as a committee or task force member are fairly
good. Table 1 lists the current SAEM committees and task forces. Since committee and task force
members normally do not serve more than 3 years, it is important to be an active, involved committee
member. The work that is done by members of the SAEM committees and task forces is voluntary, and
must be begged, borrowed, or stolen from other academic time. This makes it a challenge for even the

most well-meaning members to actively participate and results in relatively few people doing much of
the work of the Society. A high level of interest and hard work by a committee member counts as much
as experience, and it is possible for the committee member, even at a relatively junior level, to be able
to become a sub-committee chair, or even to be recommended as the next chair of the committee.
Therefore, those members who are able to work harder and put in more time than the average member
are usually "rewarded" with more responsibility.
5. Chairing a Committee or Task Force - After a period of distinguished service as a committee or task
force member, the next step is to chair a committee or task force. Usually a direct discussion with the
President-Elect is needed to determine if this position would be possible or appropriate as the faculty
member is moving up within the Society. As chair of a committee or task force, the faculty member
assumes greater responsibility for meeting the objectives that are laid out each year. This normally
involves the completion of projects, such as an educational product, position paper, or development of a
policy statement. By serving as chair, the faculty member develops administrative skills in managing a
fairly large and diverse group of committee or task force members. The Chair must also work with a
Board of Directors liaison and the Executive Office. Excellent communication skills are obviously an
important prerequisite to holding this position. It is difficult to estimate the number of hours that are
spent carrying out the duties of a SAEM committee chair, but it probably falls in the range of 5 to 20
hours per month.
6. Holding an Elected Position in SAEM: The elected positions in SAEM are as follows:
President
President-Elect
Board of Directors Members
Secretary/Treasurer
Nominating Committee Members
Constitution and By-laws Committee Members
Those who wish to be considered for elected positions must be nominated or nominate themselves to
the Chair of the Nominating Committee, who is the President-Elect. All nominations are considered by
the Nominating Committee, and the nominees are notified if they have been selected as candidates.
Most members who are nominated for these positions have made a progression in the Society from

committee or task force members to leadership positions on committees or task forces, to this next step.
Most members who are nominated for the Board of Directors will have chaired committees or task
forces, and have an excellent working knowledge of the organization. The duties of elected positions
vary considerably. Members of the Nominating Committee and Constitution and By-laws Committee will
have periods of relatively heavy work during the year, but the amount of work involved is not nearly as
much as for the President, President-Elect, Board of Directors, and Secretary/Treasurer. The Board of
Directors and Officers commit significant amount of time to SAEM activities. The reward for this time
commitment is the acquisition of a national understanding of the workings of academic emergency
medicine, and the establishment of contacts and acquaintances that can be valuable assets throughout
ones career.
Summary
The developing EM faculty member can utilize SAEM in a number of ways to promote his or her career.
This can range from scholarly activities in research and education at the Annual Meeting or Regional
Meetings to participation in scientific and educational projects in interest groups, to administrative work
within the SAEM. It is a simple process to become involved in SAEM, and once a member becomes
acquainted with the organization, it is not difficult to progress within the Society to play a larger role. By
following the above steps, with a little extra work and a positive, collaborative approach, it is possible for
almost anyone to become a significant contributor to the organization. This type of work gives the
member a national perspective that help in research and education activities, and will also be valuable
when the promotion and tenure are considered.
Career Longevity & Strategies for Continued Growth & Success
The Rank of Associate Professor. . . How to Get There
Author: Brooks F. Bock & Gloria J. Kuhn
The rank of Associate Professor is a laudable goal and worthy of the necessary efforts required to
achieve it. Physicians working within an academic environment will find that promotion brings not only
prestige but is also public acknowledgement of substantial contribution to the knowledge, education and
service within one's discipline. This recognition adds to the respect of the department and specialty in
which one works. The academic community understands well the concept of promotion. It is the "coin of

the realm" in which academicians have chosen to reside.
In practical terms, promotion makes a faculty member more mobile if he or she chooses to pursue an
academic position in another institution. It helps with negotiating protected time because it suggests
productivity. It is particularly useful when working with faculty members from other departments.
Assistant Professors are "junior faculty" while those with the rank of Associate Professor or Professor
are "senior faculty." This seniority carries weight in collaborative efforts with faculty members from other
departments.
Unfortunately, those who have spent a lifetime in academic practice and never achieved promotion are
viewed with suspicion simply because their accomplishments have not been recognized and rewarded.
This suspicion is best exemplified by the fact that inability to attain promotion results in dismissal from
some, but not all, universities after a certain period of time.
Those who are productive and capable, which most of us are, can achieve promotion by continuing to
do the things we do and adding some planning and forethought to our activities. Ideally, this plan should
be a first step in faculty development.
Faculty often experience promotion to the rank of Associate Professor within an LCME accredited
Medical School as the most difficult academic step on the promotion and tenure continuum. The
purpose of this chapter is to aid faculty members in planning their careers with the goal of successful
attainment of the rank of Associate Professor.
The Promotion and Tenure Process
Almost all Medical Schools initially appoint accredited residency program graduates at the Instructor or
Assistant Professor level. After this, the promotion/tenure (P/T) process is unique to each individual
institution.1 This variability should encourage each faculty member to read their institution's by-laws,
learn about the promotion process, and understand what constitutes scholarly activity within their
academic environment.
Medical School faculty are generally evaluated, and therefore promoted, on the basis of three major
activities; teaching, other academic activity, and service (which, in many institutions includes clinical

expertise). The P/T committee is made up of faculty members who have already achieved promotion
and may be tenured. These individuals are charged by the institution with the task of insuring that all
faculty who are promoted have achieved expertise in an academic area, are excellent teachers, have
fulfilled service requirements, and have contributed in a meaningful way to the mission of the institution.
In the past, this meant that a faculty member had to become a successful researcher as demonstrated
by grants funded from external, preferably national, sources and authored a number of peer-reviewed
original contributions. Overwhelming weight was given to original research compared to teaching and
service.
A revolution is taking place in the academic community. Today many institutions are recognizing and
accepting the concept of "expanded scholarship" as articulated by Ernest Boyer.2 As Boyer noted, while
the scholarship of discovery (original research) is vital to the academic community it needs to be
expanded by the scholarships of integration, application, and teaching. It is often in these three latter
types of scholarship that clinical faculty members excel. This expanded view has opened the way for
clinical faculty to achieve deserved recognition and reward for their work and contribution to their
institutions.
The P/T committee has always required documentation of productivity and demonstration of expertise,
but the value awarded to teaching and service has increased and the type of activity recognized as
scholarly has broadened. What has not changed is the need for excellence and expertise. There is
recognition that clinical and teaching excellence are not scholarship until shared with the academic
community outside of one's own institution.3,4 This sharing usually takes the form of published
materials. The University of Allegheny has stated, "…teaching excellence and innovation are not
scholarship until they are made public in some form where other educators have access to them…"
Many institutions now recognize published curricula, videotape, and software, in addition to peer
reviewed articles, as suitable evidence of scholarship. The degree to which these materials may be
used in support of the promotion/tenure process remains institution-specific.
To accommodate this change in philosophy, many institutions have formed "tracks" for faculty. Each
track has different requirements and guidelines for promotion. The exact titles of the tracks may vary by
institution and there may be divisions within tracks to accommodate unique roles. Still, there are
generally two or three broad tracks that are universally recognized.

One, identified as a Research-Educator track is intended for individuals of doctoral rank in both basic
science and clinical departments with a major career commitment to basic science or clinical research
that is likely to result in funding by peer-review granting agencies. Such individuals are provided with
protected time to pursue their research interest and to participate in teaching and service activities.
The second track, identified as the Clinician-Educator track is intended primarily for clinical faculty and
represents a scholarly academic track of equal stature/status as the Research-Educator track. Research
and service activities are expected. This track emphasizes and recognizes the unique role of the
clinician-educator at the forefront of faculty within the School/College of Medicine.
The third track, identified as the Research track is designed for individuals of doctoral rank with a career
dedicated to research. These faculty members are provided with time and space to carry out their
research objectives and are generally funded by national peer-review agencies. Teaching and service
activities may not be required but some contribution to the intellectual ambience of the academic
community is expected. The promotion process varies by university. Many institutions combine these
three options into two tracks: The so-called traditional track, with an emphasis on research, either
clinical or basic science, and the clinical track, which may include both the clinician-educator and
clinician-researcher career paths.
Some general guidelines for success are useful. The press of clinical responsibility combined with the
significant expectation of a university P/T committee mitigates against advancement of clinically oriented
faculty like those in Emergency Medicine. It is therefore vital that faculty members carefully plan their
careers and manage their time appropriately. Being a "jack of all trades" is interesting but not particularly
useful when your portfolio is placed before a peer-review committee. This committee looks for evidence
of excellence and focus in an area of academic endeavor.
Appropriate scholarship has traditionally been evidenced by publications of original research in peer
reviewed journals. Research focus in a particular area is highly desirable and increases the potential for
external grant support and promotion. Many institutions will only award tenure to those who can
demonstrate ability to obtain funding through outside grants. The expanded view of scholarship now
enables articles that are not based solely on the discovery of new scientific knowledge to be used when
attempting to demonstrate productivity and excellence in scholarship. Examples include published

curricula, syllabi, and multimedia materials that have been used for teaching.
Excellence in teaching is demonstrated through the acceptance of major teaching responsibilities that
are completed successfully. Student and resident evaluations play a major role in this area. Frequently,
institutions judge teaching excellence through peer evaluation. Teaching awards, both internal and
external to the home institution, carry great weight as proof of excellence.
Anticipated service activity includes evidence of peer recognition as an academic professional at the
regional and/or national level as well as willingness to accept and effectively assume administrative and
committee responsibilities. Faculty members may demonstrate clinical excellence by documenting the
application or integration of innovations in medical practice and describing these in teaching or printed
material. In all instances, objective evidence of excellence in the performance of professional activities,
specialty board certification, and membership in appropriate selective professional organizations is
expected but is not, in and of itself, sufficient to obtain promotion.
It is crucial that physicians read their institutional by-laws. Ideally this should be done during the initial
interview process when applying for a faculty position. The by-laws determine how faculty are promoted
and rewarded within the academic community. It is also important to find out if the institution has an
active faculty development program.
Academically oriented emergency physicians should understand the consequence of accepting a tenure
track appointment. This environment generally requires the physician to achieve promotion within a
finite period of time or seek employment elsewhere. The advantage of this system is that pressure is
placed on the department to ensure promotion and the department chair not only becomes expert in
helping faculty accomplish the tasks that are necessary, but also is closely involved in monitoring
progress. Conversely, the faculty member may feel a great deal of pressure to engage in research,
obtain grants, and publish in peer-reviewed journals.
Non-tenure track positions don't usually involve specific time frames for promotion. Thus, the chair may
not monitor faculty performance leading to promotion as carefully as s/he would monitor tenure track
faculty. Additionally, the faculty member may not feel the same amount of pressure to be promoted and
so may not work as hard in the scholarly arena.

The following questions are useful in assessing the potential of promotion within a specific department.
1. How many faculty members have been promoted in the department?
2. Does the Chair help faculty manage time so that scholarly activities can be accomplished?
3. Has a mentoring program been created within the school and/or department to support faculty
development?
4. Is adequate secretarial support available?
5. Will financial support to attend educational meetings be available?
A mentoring program is crucial as research has shown that faculty members who have mentors achieve
a higher rate of promotion within the academic community. However, the most important variable is
time. If the clinical commitment is very heavy and the clinical schedule onerous it takes an extremely
dedicated, committed, and organized individual to succeed in meeting the scholarly requirements
necessary for promotion.
A job description and duties should be part of one's contract. The amount of clinical service required
should be clearly stated. Additionally, evaluations conducted by the chair should state clearly whether
the faculty member has fulfilled all obligations so that s/he remains on track for promotion.
Planning for Promotion
The aspiring faculty member needs to develop a plan, generally formulated in conjunction with his/her
Chair, to determine what will be expected prior to being recommended for promotion to the Associate
Professor level. As mentioned, this plan may involve a time clock. This is especially true in institutions
whose by-laws demand that all faculty members be tenured. This clock is usually set for between seven
to nine years. This means that the faculty member must complete all of the requirements for promotion
within that time period or leave the faculty. Many faculty members, with the support of their chair,
choose the non-tenure track position to avoid this concern.
Documentation for Promotion
P/T committees sometimes lack the documentation necessary to demonstrate expertise as an educator,

scholar and clinician.5 The deficits are usually found in the teaching and clinical area. Research
experience, if present, is easily assessed through grant listings and publications.
Because of this difficulty with lack of documentation, many universities have turned to the
teaching/educator portfolio as a way to document productivity.6 It is analogous to the portfolio used by
artists and architects to demonstrate the scope and caliber of their work. Some institutions now require
that their faculty members maintain a portfolio. There are a number of articles/books which detail how a
teaching portfolio can be constructed and used for purposes of evaluation and promotion.7-9
When the portfolio is used for evaluation it should contain documentation of all that has been
accomplished. When used for promotion purposes it should contain a statement of how the faculty
member has contributed to the scholarly community and added to the value of the institution. It should
provide examples of the faculty member's best works supporting the premise that the faculty member
has academic expertise in one of the four major domains of scholarship: Discovery, application,
integration, or teaching.
Universities place great weight on evaluations by students and residents and these should be included
in documentation supplied to the P/T committee. Any evaluations of teaching by peers are of value.
Teaching awards or awards granted for service to professional organizations help to demonstrate
excellence either in the educational or clinical arena.
An up to date curriculum vitae (CV) is essential. Suggestions for how to construct one are included in
Chapter 2.1 in this Handbook (see Table of Contents). It is vital that the submitted CV conform to the
format specified by the individual institution. A complete bibliography of authored work should be
prepared.
Conclusion
Attaining promotion to the level of Associate Professor requires planning that should ideally begin at the
start of an academic career. Engaging in activity that allows a faculty member to gain teaching expertise
and a focus of research is essential. Clinical excellence is a requirement unless one is engaged solely in
the Research Track. Documentation of accomplishments that demonstrate the value of the individual to
the institution and show how that individual has contributed to the scholarly environment are mandatory.

The rewards of achievement are well worth the effort for they attest to recognition by the academic
community that a faculty member has been successful in adding to the value of that community and
helping fulfill its mission of teaching, research, and service.
Bibliography
1. Levinson, W, Branch W, Kroenke K. Clinician-educators in academic medical centers: A two-part
challenge. Ann Internal Med, 1998;129:59-64.
2. Boyer E., Scholarship Reconsidered: Priorities of the Professoriate, 1990, Princeton, NY: Carnegie
Foundation for the Advancement of Teaching.
3. Barchi R, Lowery B. Scholarship in the medical faculty from the university perspective: Retaining
academic values. Acad Med, 2000;75:899-905.
4. Nieman, L., et al. Implementing a comprehensive approach to managing faculty roles, rewards, and
development in an era of change. Acad Med 1997;72:496-504.
5. Jones R, Froom J. Faculty and administration views of problems in faculty evaluation. Acad Med,
1994;69:476-483.
6. Beasley B, Wright S, Confrancesco J. Promotion criteria for clinician-educators in the United States
and Canada. JAMA 1998;278:723-728.
7. Seldin, P., The Teaching Portfolio. A practical guide to improved performance and promotion/tenure
decisions. 2nd ed. 1997, Bolton, MA: Anker Publishing Company Inc.
8. Shulman, L., "The Educator's Portfolio." 1990: Presentation at Conference on Assessment in Higher
Education.
9. Simpson, D., A. Beecher, and J. Lindemann, The Educator's Portfolio. 4th ed. 1998, Milwaukee, WI:
Medical College of Wisconsin.
Mentoring Faculty Members to the Next Level
Authors: David W. Wright and Jerris R. Hedges
Other sections of this faculty development guide will address aspects of seeking a mentor and
interacting with that individual. This section will focus upon the faculty member serving as a mentor.
Because Emergency Medicine is a relatively young specialty, many faculty members, even those at the
Instructor and Assistant Professor level, have taken on leadership and mentoring roles. This can result
in only a few years of experience separating the mentor from the mentee.
Two problems exist with this model. First, one of the most important benefits of a mentor is guidance
provided through past experience. Young mentors rarely have had the opportunity to gain the wisdom
and experience, or develop the world view, needed to be a good mentor. Ignorance, or lack of insight,
can have a disastrous result for someone’s career. Also, the inexperience of the mentoring relationship
can lead to an unstructured mentoring program and poor guidance for the mentee.

Despite these problems, mentoring of junior faculty, even by junior faculty, can be rewarding and
educational for both parties. Most problems can be avoided by following two key principles. First, even
the junior mentor should have a good senior mentor. The experience of a senior mentor can be
transmitted through the junior mentor to his/her mentee, and provide a great learning experience for the
mentor "in-training." Second, the development of a well-organized mentoring plan will provide structure
and stability to a mentoring relationship between faculty members of all levels.
As the junior faculty member looks to achieve promotion to Associate Professor and subsequently to
Full Professor, she/he should expect to have mentorship serve an important role in the promotion. This
chapter will focus on the following 1) why be a mentor?; 2) the mentoring relationship; 3) key steps on
how to be a great mentor; 4) mentoring in specific areas; 5) what are the pitfalls of a mentor/mentee
relationship?; and 6) how does one take credit for serving as a mentor?
Why be a mentor?
Mentorship is a special form of educational service. The relationship is highly personal and individual.
As such, it can be immensely rewarding. Mentoring may help create a career-long relationship between
individuals with overlapping academic interests. Such a relationship is most likely to impart a certain
degree of permanence or immortality to the academic efforts of the mentor – producing "academic
progeny".
On a more practical basis, the relationship provides mentors with junior faculty members who will
collaborate on shared scholarship, clinical service, and educational goals. A team approach will
generally be more productive than solo efforts. Further, when applying for promotion, an important
aspect of the application process is demonstration that one's academic efforts have influenced the
academic efforts of other faculty members. Mentoring relationships are important examples of one's
influence on the careers of others. To this end, it is wise to provide mentorship not only in one's own
department or institution, but to provide that service on a national level.
From a personal perspective, mentees in a mentoring relationship become extensions of the mentor.
Mentees recognize and share new academic opportunities with the mentor. The relationship opens the
mentor to new academic perspectives. Therefore, the relationship is intellectually stimulating, gratifying
on a personal level, and academically symbiotic.

The mentoring relationship
In Greek mythology, Ulysses entrusted his son's development to his old and trusted friend Mentor, when
he departed for the Trojan War. (1) Mentor served as a surrogate father for Telemechus. Just as
parental relationships can be complex, so can academic mentoring. Generally the rules of life and
academic practice have a limited instruction manual. The rules are often flexible and situationally
dependent.
Key steps on how to be a great mentor
To help guide the mentee through their academic career, gather up the tenure and promotion guidelines
for the University and the academic Department. Determine the goals and objectives of the University
and the Department and review how success is measured. Then, meet with the mentee and develop
short-term and long-term goals based on the goals of the mentee, along with the expectations of the
University and Department. These short-term and long-term goals will allow you and your mentee to
develop a comprehensive career plan that maps out a successful career path for the mentee. Create a
timeline for specific achievements based on the short-term and long-term goals, and keep to the
schedule. Set regular mentoring sessions, initially 1 –2 hours a week, to assess the success of the
short-term objectives. Keep a file and a checklist of the goals and objectives of the mentee. Also,
require the mentee to keep a checklist of their goals and objectives that includes the timeline, the tenure
and promotions guidelines, and a teaching portfolio. Review the mentee's folder on a regular basis.
When questions arise that you can’t answer, ask your senior mentor.
Mentoring in specific areas
The Research Mentor
The ultimate objective for a research mentor is for their mentee to become an independent researcher
as defined by a continuous record of publications and extramural funding ( preferably NIH). As an
independent researcher, the mentee has learned critical thinking skills, idea development, hypothesis

generation, project design, grant writing and funding skills, proper ethics in research, and manuscript
writing. This does not mean that the mentor has to teach all of these skills, but rather identifies
resources and opportunities for the mentee to obtain them. Also, the mentor can help pull a
multidisciplinary research team together to support the mentee. The mentor can identify colleagues with
similar interests at other institutions and propose a broader policy role that can broaden the impact of
the mentee's research findings. The mentor can help the mentee in acquisition of a study section
membership to further the mentee's influence and learning. The development of a research career for
junior faculty is a long and arduous process, and the wisdom of an experienced mentor can mean the
difference between rapid success and a slow painful failure. The mentor should create a plan for the
mentee's research development that includes learning the skills necessary for independent research.
The Education Mentor
Education has many facets and many styles. The mentor can expose the mentee to a variety of styles
and help determine the best fit for the mentee. The mentor can demonstrate organizational skills and
the effective incorporation of multimedia into didactic lectures. The mentor can share lecture skills and
review the role of lectures outside the department on a regional and national level in career
development. The mentor can assist with curriculum development, methods of evaluating learner
knowledge and skill acquisition and retention, and publishing educational scholarship. The mentor can
help in the development of the teaching portfolio and use it as a guide for the continuing development of
the mentee-educator ( 2) The portfolio should contain the essential elements of the mentee's teaching
philosophy and how he or she is going to accomplish their goals. The education mentor can teach the
mentee skills for interacting with students, residents, and colleagues and how to use these skills to the
best educational advantage.
The Administrative Mentor
Mentoring an individual who has aspirations for administration requires an open honest assessment of
the mentee's personnel management skills. Some individuals may require extensive leadership training.
The training can involve personality assessment and development, faculty and staff interaction skills,
delegation skills, management skills, and strategic planning. The mentor can demonstrate the balance
between support of an assigned administrative responsibility and retaining clinical skills and producing
scholarship. The mentor can introduce the mentee to key clinicians and administrators in other areas of

the medical center and within national organizations focusing on this administrative role. Developing a
meaningful working relationship with these individuals, and understanding their background,
contributions to the administrative field, and related priorities can be of immense value to the mentee.
The mentor can help the mentee apply management tools and better understand interpersonal and
group dynamics in theory and practice that influence group thought and action. People skills and day-to-
day interactions are the most difficult and important skills for the mentee to master.
The Clinical Mentor
The clinical mentor demonstrates the essential skills for critical thinking and problem solving. The
mentor can share methods for retention of clinical knowledge and acquisition of new clinical skills and
understandings. The mentor can demonstrate the advantages and disadvantages of technical
innovations (e.g., ultrasound techniques, procedural skills, parenteral sedation methods), which will
facilitate clinical practice. The mentor can develop systems of care and standardized approaches to the
evaluation of common or difficult clinical presentations to share with the mentee. The clinical mentor can
teach the mentee skills entailed in interacting with patients, nurses, support staff and colleagues , along
with time management skills. The key to all mentoring is an open sharing of one's experience and
knowledge. It need not be structured, but it must be frequent enough to sustain enthusiasm, information
acquisition, and to positively influence progress.
What are the pitfalls of mentoring?
The relationship
Certainly, impediments which block the information sharing must be avoided. Poor communication is as
bad as a personality conflict between the mentee and mentor. Both individuals must find value in the
relationship and make the effort to sustain the exchange. Like any relationship, there will be moments of
doubt. One party may question the sincerity or motivation of the other. While it is important to have
priorities, clear goals, and mutual commitments, plans must be flexible. Mentors must adjust to the
mentee's life changes. The mentoring relationship may even be placed on hold during extended periods
of time. However, the mentor and mentee should look for opportunities to advance their mutual plans
rather than excuses to set them aside.

Expectations
Another concern is that a mentor may believe that she/he must meet all of a mentee's needs. While the
mentor can address many needs, the mentee should seek a variety of mentors who can provide support
for different needs. (3) Mentors also must understand their limits. They can facilitate, but they cannot
accomplish goals on behalf of the mentees. Publications and grants cannot be guaranteed.
Experimental outcomes cannot be predicted with accuracy. Indeed, perhaps some of the best lessons
are provided by these "teachable moments" when things do not go right. The mentor can provide much
wisdom and guidance when the mentee has reached an impasse .
Planning
A sure plan for failure is not developing a plan with, and for, the mentee. The importance of short-term
goals, long-term goals, and measurable benchmarks cannot be overemphasized. These goals chart the
course for the mentoring relationship.
How does one take credit?
Arguments over ownership of an idea or priority of discovery have killed many a scholarly mentoring
relationship. The mentor must recognize that the mentee will often feel less empowered and may
hesitate to discuss these issues openly. Hence, it is critical that the mentor take the initiative and
discuss options with the mentee before deeply pursing a project that will consume much time and
energy on the part of both individuals. The result of such discussions should be written down wherever
possible.
Quite often, the contributions made by the mentor are not of a creative nature. Often the recognition
should be limited to an acknowledgment on a paper, thesis, or presentation. Again, the mentor should
be realistic and seek to promote the mentee and not her/himself in such circumstances where the
contribution is more a service than a creative venture.
It is wise for the mid career- or senior-level faculty member to keep a list of junior faculty members for

whom she/he has served as a mentor, whether in the same or another department. Demonstrating the
mentorship of these individuals with a listing of the mentee's accomplishments makes a powerful
argument that the faculty member has added educational or service value to the institution. These
contributions should be shared with and acknowledged by the faculty mentor's departmental chair on a
yearly basis. They should be highlighted in the promotional dossier created at the time the mentor
applies for promotion.
Final thoughts
While it is up to the mentee to seek mentors, the faculty member who highlight's the efforts of her/his
mentees will be sought after. Such a faculty member must balance the commitment to mentoring in the
same manner that she/he balances the many other academic commitments. It is a rewarding activity
and should be a part of everyone's academic role. (4)
References
1. Clutterbuck D. Everyone needs a mentor; fostering talent at work. 2nd Ed. Institute of Personnel
Management, 1992.
2 Seldin P. The Teaching Portfolio : A Practical Guide to Improved Performance and Promotion/Tenure
Decisions. Anker Publishing Co; 2nd edition, 1997
3. Morahan P. How to find and be your own best mentor. Acad Physician & Scientist
(November/December 2000); 8.
4. National Academy of Sciences, National Academy of Engineering and the Institute of Medicine:
Advisor, teacher, role model, friend. National Academy Press, Washington, D.C. 1997

Mentoring Faculty Members to the Next Level
Authors: David W. Wright and Jerris R. Hedges
Other sections of this faculty development guide will address aspects of seeking a mentor and
interacting with that individual. This section will focus upon the faculty member serving as a mentor.
Because Emergency Medicine is a relatively young specialty, many faculty members, even those at the
Instructor and Assistant Professor level, have taken on leadership and mentoring roles. This can result
in only a few years of experience separating the mentor from the mentee.
Two problems exist with this model. First, one of the most important benefits of a mentor is guidance
provided through past experience. Young mentors rarely have had the opportunity to gain the wisdom
and experience, or develop the world view, needed to be a good mentor. Ignorance, or lack of insight,
can have a disastrous result for someone’s career. Also, the inexperience of the mentoring relationship
can lead to an unstructured mentoring program and poor guidance for the mentee.
Despite these problems, mentoring of junior faculty, even by junior faculty, can be rewarding and
educational for both parties. Most problems can be avoided by following two key principles. First, even
the junior mentor should have a good senior mentor. The experience of a senior mentor can be
transmitted through the junior mentor to his/her mentee, and provide a great learning experience for the
mentor "in-training." Second, the development of a well-organized mentoring plan will provide structure
and stability to a mentoring relationship between faculty members of all levels.
As the junior faculty member looks to achieve promotion to Associate Professor and subsequently to
Full Professor, she/he should expect to have mentorship serve an important role in the promotion. This

chapter will focus on the following 1) why be a mentor?; 2) the mentoring relationship; 3) key steps on
how to be a great mentor; 4) mentoring in specific areas; 5) what are the pitfalls of a mentor/mentee
relationship?; and 6) how does one take credit for serving as a mentor?
Why be a mentor?
Mentorship is a special form of educational service. The relationship is highly personal and individual.
As such, it can be immensely rewarding. Mentoring may help create a career-long relationship between
individuals with overlapping academic interests. Such a relationship is most likely to impart a certain
degree of permanence or immortality to the academic efforts of the mentor – producing "academic
progeny".
On a more practical basis, the relationship provides mentors with junior faculty members who will
collaborate on shared scholarship, clinical service, and educational goals. A team approach will
generally be more productive than solo efforts. Further, when applying for promotion, an important
aspect of the application process is demonstration that one's academic efforts have influenced the
academic efforts of other faculty members. Mentoring relationships are important examples of one's
influence on the careers of others. To this end, it is wise to provide mentorship not only in one's own
department or institution, but to provide that service on a national level.
From a personal perspective, mentees in a mentoring relationship become extensions of the mentor.
Mentees recognize and share new academic opportunities with the mentor. The relationship opens the
mentor to new academic perspectives. Therefore, the relationship is intellectually stimulating, gratifying
on a personal level, and academically symbiotic.
The mentoring relationship
In Greek mythology, Ulysses entrusted his son's development to his old and trusted friend Mentor, when
he departed for the Trojan War. (1) Mentor served as a surrogate father for Telemechus. Just as
parental relationships can be complex, so can academic mentoring. Generally the rules of life and
academic practice have a limited instruction manual. The rules are often flexible and situationally
dependent.

Key steps on how to be a great mentor
To help guide the mentee through their academic career, gather up the tenure and promotion guidelines
for the University and the academic Department. Determine the goals and objectives of the University
and the Department and review how success is measured. Then, meet with the mentee and develop
short-term and long-term goals based on the goals of the mentee, along with the expectations of the
University and Department. These short-term and long-term goals will allow you and your mentee to
develop a comprehensive career plan that maps out a successful career path for the mentee. Create a
timeline for specific achievements based on the short-term and long-term goals, and keep to the
schedule. Set regular mentoring sessions, initially 1 –2 hours a week, to assess the success of the
short-term objectives. Keep a file and a checklist of the goals and objectives of the mentee. Also,
require the mentee to keep a checklist of their goals and objectives that includes the timeline, the tenure
and promotions guidelines, and a teaching portfolio. Review the mentee's folder on a regular basis.
When questions arise that you can’t answer, ask your senior mentor.
Mentoring in specific areas
The Research Mentor
The ultimate objective for a research mentor is for their mentee to become an independent researcher
as defined by a continuous record of publications and extramural funding ( preferably NIH). As an
independent researcher, the mentee has learned critical thinking skills, idea development, hypothesis
generation, project design, grant writing and funding skills, proper ethics in research, and manuscript
writing. This does not mean that the mentor has to teach all of these skills, but rather identifies
resources and opportunities for the mentee to obtain them. Also, the mentor can help pull a
multidisciplinary research team together to support the mentee. The mentor can identify colleagues with
similar interests at other institutions and propose a broader policy role that can broaden the impact of
the mentee's research findings. The mentor can help the mentee in acquisition of a study section
membership to further the mentee's influence and learning. The development of a research career for
junior faculty is a long and arduous process, and the wisdom of an experienced mentor can mean the
difference between rapid success and a slow painful failure. The mentor should create a plan for the
mentee's research development that includes learning the skills necessary for independent research.

The Education Mentor
Education has many facets and many styles. The mentor can expose the mentee to a variety of styles
and help determine the best fit for the mentee. The mentor can demonstrate organizational skills and
the effective incorporation of multimedia into didactic lectures. The mentor can share lecture skills and
review the role of lectures outside the department on a regional and national level in career
development. The mentor can assist with curriculum development, methods of evaluating learner
knowledge and skill acquisition and retention, and publishing educational scholarship. The mentor can
help in the development of the teaching portfolio and use it as a guide for the continuing development of
the mentee-educator ( 2) The portfolio should contain the essential elements of the mentee's teaching
philosophy and how he or she is going to accomplish their goals. The education mentor can teach the
mentee skills for interacting with students, residents, and colleagues and how to use these skills to the
best educational advantage.
The Administrative Mentor
Mentoring an individual who has aspirations for administration requires an open honest assessment of
the mentee's personnel management skills. Some individuals may require extensive leadership training.
The training can involve personality assessment and development, faculty and staff interaction skills,
delegation skills, management skills, and strategic planning. The mentor can demonstrate the balance
between support of an assigned administrative responsibility and retaining clinical skills and producing
scholarship. The mentor can introduce the mentee to key clinicians and administrators in other areas of
the medical center and within national organizations focusing on this administrative role. Developing a
meaningful working relationship with these individuals, and understanding their background,
contributions to the administrative field, and related priorities can be of immense value to the mentee.
The mentor can help the mentee apply management tools and better understand interpersonal and
group dynamics in theory and practice that influence group thought and action. People skills and day-to-
day interactions are the most difficult and important skills for the mentee to master.
The Clinical Mentor
The clinical mentor demonstrates the essential skills for critical thinking and problem solving. The
mentor can share methods for retention of clinical knowledge and acquisition of new clinical skills and

understandings. The mentor can demonstrate the advantages and disadvantages of technical
innovations (e.g., ultrasound techniques, procedural skills, parenteral sedation methods), which will
facilitate clinical practice. The mentor can develop systems of care and standardized approaches to the
evaluation of common or difficult clinical presentations to share with the mentee. The clinical mentor can
teach the mentee skills entailed in interacting with patients, nurses, support staff and colleagues , along
with time management skills. The key to all mentoring is an open sharing of one's experience and
knowledge. It need not be structured, but it must be frequent enough to sustain enthusiasm, information
acquisition, and to positively influence progress.
What are the pitfalls of mentoring?
The relationship
Certainly, impediments which block the information sharing must be avoided. Poor communication is as
bad as a personality conflict between the mentee and mentor. Both individuals must find value in the
relationship and make the effort to sustain the exchange. Like any relationship, there will be moments of
doubt. One party may question the sincerity or motivation of the other. While it is important to have
priorities, clear goals, and mutual commitments, plans must be flexible. Mentors must adjust to the
mentee's life changes. The mentoring relationship may even be placed on hold during extended periods
of time. However, the mentor and mentee should look for opportunities to advance their mutual plans
rather than excuses to set them aside.
Expectations
Another concern is that a mentor may believe that she/he must meet all of a mentee's needs. While the
mentor can address many needs, the mentee should seek a variety of mentors who can provide support
for different needs. (3) Mentors also must understand their limits. They can facilitate, but they cannot
accomplish goals on behalf of the mentees. Publications and grants cannot be guaranteed.
Experimental outcomes cannot be predicted with accuracy. Indeed, perhaps some of the best lessons
are provided by these "teachable moments" when things do not go right. The mentor can provide much
wisdom and guidance when the mentee has reached an impasse .
Planning

A sure plan for failure is not developing a plan with, and for, the mentee. The importance of short-term
goals, long-term goals, and measurable benchmarks cannot be overemphasized. These goals chart the
course for the mentoring relationship.
How does one take credit?
Arguments over ownership of an idea or priority of discovery have killed many a scholarly mentoring
relationship. The mentor must recognize that the mentee will often feel less empowered and may
hesitate to discuss these issues openly. Hence, it is critical that the mentor take the initiative and
discuss options with the mentee before deeply pursing a project that will consume much time and
energy on the part of both individuals. The result of such discussions should be written down wherever
possible.
Quite often, the contributions made by the mentor are not of a creative nature. Often the recognition
should be limited to an acknowledgment on a paper, thesis, or presentation. Again, the mentor should
be realistic and seek to promote the mentee and not her/himself in such circumstances where the
contribution is more a service than a creative venture.
It is wise for the mid career- or senior-level faculty member to keep a list of junior faculty members for
whom she/he has served as a mentor, whether in the same or another department. Demonstrating the
mentorship of these individuals with a listing of the mentee's accomplishments makes a powerful
argument that the faculty member has added educational or service value to the institution. These
contributions should be shared with and acknowledged by the faculty mentor's departmental chair on a
yearly basis. They should be highlighted in the promotional dossier created at the time the mentor
applies for promotion.
Final thoughts
While it is up to the mentee to seek mentors, the faculty member who highlight's the efforts of her/his
mentees will be sought after. Such a faculty member must balance the commitment to mentoring in the
same manner that she/he balances the many other academic commitments. It is a rewarding activity
and should be a part of everyone's academic role. (4)

References
1. Clutterbuck D. Everyone needs a mentor; fostering talent at work. 2nd Ed. Institute of Personnel
Management, 1992.
2 Seldin P. The Teaching Portfolio : A Practical Guide to Improved Performance and Promotion/Tenure
Decisions. Anker Publishing Co; 2nd edition, 1997
3. Morahan P. How to find and be your own best mentor. Acad Physician & Scientist
(November/December 2000); 8.
4. National Academy of Sciences, National Academy of Engineering and the Institute of Medicine:
Advisor, teacher, role model, friend. National Academy Press, Washington, D.C. 1997

Assuming a Leadership Position: a checklist for success
Author: Sandra M. Schneider
To be chosen among your peers to lead is indeed a great honor. Whether it is leadership at the local,
regional, or national level; whether in a professional or community venue, leadership carries significant
responsibilities and rewards. In many ways your life will be different. Your actions and words now will
carry greater weight, reflecting the entire enterprise. Casual suggestions can become law; off-handed
comments become official declarations. Time commitments, particularly those that take away from
family, can be costly. The feeling of honor, duty and ego satisfaction may lead you to accept the
leadership position, but then find yourself ill prepared and even frustrated when the real work of
leadership begins.
Preparation:
Have you mastered the basics? The first step is to master the basic skills of your profession. There is no
shortcut around this. You should take every opportunity to learn. If asked to go to some ‘boring’ meeting,
go and listen and learn. If you hear jargon you are unfamiliar with, write it down and ask about it. Take
advantage of every opportunity to see how the system works. Woody Allen said, "90% of life is showing
up". Although humorous at first glance, it is profoundly true. Finally take every opportunity to meet
people and get to know them.
Do you have a good reputation? Learn to network at organizational functions. Be friendly. Never utter a
negative word about anyone. Learn to be professional in your interactions. Be wary of becoming a
single issue person. Though it is easier to build a reputation by taking a stand on a volatile issue, a true
leader must represent the entire constituency.
Do you have the management and leadership skills necessary? Learn about leadership. Read, attend

seminars, listen and learn. Learn how to use your personality and talents as a leader. Leaders are not
born, but are made.
Finding a mentor or mentors can be very important. Although many may find the right path by
themselves, having a mentor to open doors and give directions at the right times can make the best use
of your time. There are a few essentials to every leadership position – time management, conflict
negotiation, constructive feedback, basic finance. These are the tools of the trade. No leader can be
successful without competency in each of these. There is a myriad of courses, self-help books, and
videos available in each of the areas.
Are you enjoying the work required to get to a leadership position? Have fun learning and working your
way up. Leadership is most rewarding when it is not initially sought. If you are not having fun getting to
the top, you will not have fun once you are there. And if you are not having fun in the leadership role, not
only should you question why you have bothered, but also it is likely that you will fail as a leader.
The right (?) opportunity:
Are your motives for wanting this position genuine? First and foremost you should examine motivation.
Why are you interested in a position that offers more work and more accountability? Is it the opportunity
to effect change, the self-satisfaction that comes from being selected, or the money and power that
come with the title? Especially in the military, is it the chance to lead or to command? An honest
examination of these questions will help to guide your leadership style. Guarding against a tendency to
command or rule may require constant diligence. The lure of money may prolong a leadership term
beyond what is good for either party. The quest for personal power can be devastating to the
organization.
Are you aware of the organization’s motives? Is there expectation of major change or maintenance of
the status quo? What are the priorities for the organization at this time?
Are you passionate about the organization? A leader must first and foremost have a passion. Passion
cannot be taught; it must come naturally from within. One must believe in the organization. That belief
may include needed change to organizational process, but you must believe in the basic values of the

organization. For example, you may assume the position of department chief primarily to effect a major
overhaul in services. Your passion is the organization as a whole and your vision is to create the
changes that will bring your department in line with the organization
Do you know what you want to accomplish as a leader? Although some claim to identify a natural
leader, what they are generally identifying is a person with creativity, passion and vision; a person
unafraid to go along a different path and the communication skills and vision to get others to follow. The
key is simply identifying the area that excites the individual. Vision can be molded if not taught. Passion
is the key. From there vision is derived from creative thinking, strategic analysis, experience and
mentoring. Vision is creativity tempered with knowledge gained from experience.
The leader must articulate a vision. Every organization needs something to strive for (we will be number
1, we will increase our membership, etc). The vision should be clear to all. Slogans, laminated cards
with mission and vision statements, reciting of mottoes, etc are tools to ingrain the vision into the group.
The vision should hold something for everyone. It must make all the work and energy worthwhile to the
individual. While the vision should appear to be attainable, be careful not to reach it too quickly. Once
the vision becomes reality, either a new vision or new leader will be needed. Nevertheless, the leader
must show the vision and the path to get there.
Does your skill set match the organization’s? Mastery of the skills leading to the position of leadership is
essential. If the organization is a clinical department or educational organization then the leader must
have proven skills in that area. He should be a master teacher, an exceptional clinician. His skills in
these areas should be above reproach. If he is to be the leader of an organization, then he should be
recognized as a master of the qualities the organization exemplifies. For example, if it is a research
organization he should be a respected researcher, first. If it is a political organization, he should have
proven political skills.
Day to day operations
Are you comfortable with your (new) peer group? Once you have assumed a position of leadership, you
are the organization. Your actions and words reflect on the organization. Candid conversations casting
doubt on decisions made will at best condemn them and may confuse the listener. Disagree in private,
support in public. Whatever the body (i.e. board of directors) decides can be discussed vigorously in

private deliberations but must be strongly supported outside the boardroom. You may and will take the
blame for something you have violently opposed.
Do you have the necessary support away from the organization? Leadership is very lonely. Your former
peers may now be you subordinates. Relationships change. Some want favor; some want access and
influence. You need support from outside the organization to survive.
Do you have the necessary support of your superiors? Do you know what they expect of you? Often the
true agendas are hidden. ‘We want a good clinical department’ may actually mean ‘We want you to fix
the finances’. Understanding their priorities is essential. Be cautious of using your superiors to fight your
battles. YOU need to be viewed as the problem solver, not the problem maker or problem identifier.
Do you have the support of your subordinates? Do they respect you? The leader of a clinical
department that cannot work clinically can be problematic. The leader of an academic department that
cannot teach or perform research gives fuel to disgruntled constituents.
Do you have the support of the support staff? A great personal assistant is invaluable. They will offer
helpful hints, keep track of the rumor mill, and make acceptable excuses for your failures. A disgruntled
support staff can easily sabotage you. Simply consider how many ways a personal assistant can break
an appointment.
Do you know the culture of the organization? Do your homework. You must know your job and
demonstrate your competency. Analyze the organization and its work habits. Are communications oral
or written? Are meetings cordial or caustic? Each organization has a unique culture. Cultural errors are
tolerated for only a brief period. After this ‘honeymoon’ cultural errors will be interpreted as social
clumsiness and detract from your leadership.
Do you have a thick skin? Just as your words and actions reflect the organizations, people will treat you
as if you are the organization. Frustration about the global state of the organization (or world) will be
directed to you personally. At times it may feel that you are responsible for all that is bad and nothing
that is good. People will hold you accountable for financial and economic swings. It is hard not to take

these comments personally. However they are really not addressed to you, but rather to the position you
temporarily hold. Remember that you must in time surrender the leadership position you hold. When
that day comes, it will no longer be you, but now your successor who holds that responsibility.
Are you a good communicator? Most of your job is communication. You must communicate your vision.
You must listen to your constituency. You must communicate your organization’s view to outside
agencies and individuals. You must listen to your constituency. You must interpret interactions with
outside agencies to your organization..
Are you a people person? You must know your constituency on a human basis. Find out what is
important. Remember special dates, events, and issues in their lives. Celebrate successes and
empathize with losses. Many leaders find tickle files and prompting cards valuable to remember
spouse/children’s names, special events, etc. Don’t be surprised if your relationship with your
colleagues abruptly changes. Those who were your dearest friends may become less open, those who
were previously distant may suddenly want to be close. You will find yourself not welcome at certain
occasions designed to let off steam.
Are you approachable? Your constituents will need to communicate with you freely and openly. You in
turn must answer back as the organization. In each conversation there is need to assess the who, what,
when, and why. Who does this individual represent, himself or a group? What does he want, change, a
chance to vent, reassurance? When do you need to act on his comments, today, after further
discussion, perhaps never? Why has he chosen today, was there a sentinel event, a growing
insurrection? Each conversation leads to an action. Again these can be analyzed in the who, what,
when, and why sequence. Who needs to act on this, you, a higher or lower power? Be careful what you
‘kick upstairs’. You have been appointed a problem solver. If you must rely on a higher authority for an
action, go prepared with a solution and a reason. There is much to be said for using a lower authority to
negotiate in your place. What needs to be done? You can simply note the complaint or act to correct it.
Consensus may need to be built first. When should the action be taken? Why does it need to be done?
Do you need to make a change to keep a valuable employee or because it is the right thing to do? What
are the implications for others if this change is made? Will another group suffer because of concessions
made? What is the precedent that is being set? Finally every action carries its own implementation. Who
will make and articulate the change? What change will need to occur and what impact will that have on
others? When is the best time to make a change?

Are you decisive? Learn to make decisions quickly and fairly. Do not agonize over small items.
Whenever possible, concede early minor issues that ‘cost’ nothing. Let the group decide issues that are
not crucial to your vision or the running of the organization.
Can you make change? Making change is a part of leadership. Change is difficult and uncomfortable,
even if the change is universally acknowledged for the good. There must be a reason to endure the
uncomfortable change. A crisis unites a group against an ‘enemy’ and gives the power to endure
change. History shows the value of an enemy and crisis such as the race to the moon or the attack on
Pearl Harbor. If there is no crisis or enemy, there is both value and danger in creating a crisis. A crisis is
necessary for change but a contrived crisis (such as some of the famine at the start of the Soviet Union)
will lead to anger and distrust if detected. An outside party vilified to unite your forces may someday
need to be your friend or collaborator. Often leaders are judged by their ability to inspire their
constituency as well as to cooperate with peer leaders. Vilifying other organizations/organizational
leaders will provide short-term gains, but negative long-term consequences. The best enemies are
vague. Managed care is a better enemy than the Surgery Department.
Change requires buy-in from the constituency. People will not readily make change. In any change there
are 3 groups of people. The core believers understand and readily adopt the change. The core
disbelievers will never understand or adapt to the change. If change is adopted these people will likely
leave the organization. The last group is the most crucial. These are the swing voters, the group for
which change has less impact. The size of this group and its final inclination will determine whether
change is enacted. Mandated change will nearly always fail.
Perhaps the most common mistake made in creating change is failing to plan the implementation. Once
a course of action is decided, communication of the change and implementation must be carefully
planned. In fact, this phase of the change process should receive the greatest emphasis and
consideration. For every proposed change there is a correct time, person and crisis. All three must be
correct or the change will not occur. For example a change in trauma care may need to wait until there
is a change of leadership in Surgery.

Do you know the history of the organization? Beware of the power of history. Within every organization
is at least one person who will hold steadfastly to history. While we clearly must learn from history, we
must be wary of dominating all future interactions. Organizations grow and change (especially when
leadership changes). Rivalries and emotions precipitated by past events may preclude future beneficial
alliances.
Are you being asked to give special consideration/privileges? Be wary of change to accommodate an
individual. A strange or unusual organizational pattern generally grows out of the need to accommodate
an individual rather than for the betterment of the organization. Convoluted reporting structures,
redundancies in responsibilities, and layers of bureaucracy often surround a powerful but inept
individual. Awareness should not lead to immediate replacement of that individual; after all they got
there because of their political power. However, for every change there is a right time, person, and
crisis.
Closure
Is your ego tied to the position? All leadership positions must come to an end. Recognizing the need to
step down or step aside is difficult. Even when there is a defined term limit it is difficult to completely
sever the ties to leadership. Past presidents struggle with letting go of power, watching another step in
and (even worse) improve on your successes. As a leader you must constantly reassess your political
strength. Do you remain a visionary? Are your political skills still sharp? Can you maintain the energy
and enthusiasm to continue the battle for success? Long before the day comes when these questions
lead to a decision to step down, you must begin to groom your replacement. A truly successful leader
has already identified potential leaders and mentored them. Although one of these may at some time
replace you, the best leader is not threatened by the growth of a subordinate. Instead a truly great
leader anticipates the end of their term and rejoices in the successes they have spawned.
A word of caution:
"There was, as Squealer was never tired of explaining, endless work in the supervision and organization
of the farm. Much of this work was of a kind that the other animals were too ignorant to understand. For
example, Squealer told them the pigs had to expend enormous labors every day upon mysterious things
called "files," "reports," minutes," and "memoranda." These were large sheets of paper which had to be
closely covered with writing, and as soon as they were so covered, they were burnt in the furnace. This
was of the highest importance for the welfare of the farm, Squealer said. But still, neither pigs nor dogs

produced any food by their own labor; and there were very many of them, and their appetites were
always good… All animals are equal, but some animals are more equal than others." Animal Farm, by
George Orwell.
How to Evaluate a Potential New Opportunity
Author: John Marx
Opportunities in academic emergency medicine can be assiduously sought or just rise out of the
proverbial blue. These may occur at any point in one's career and at any age and stage of one's life.
DISCOVER THE OPPORTUNITY
Active Approach: There are three basic search methods.
Letters of Approach: One tactic is to send out a letter of introduction containing your curriculum vitae.
This is not an unusual tactic for the senior resident. The letter can be sent out as a mass mailing, that is
to every program in the United States, or in a manner targeted toward a specific geography or types of
programs. Success of this method relies heavily upon timing. These letters can be delivered at any time
but will likely be read with greater interest in the late winter and early spring when chairs are sizing up
their needs for the coming academic year. While the subject has not been studied, empiricism suggests
that a large proportion of these letters prompt generic and empty responses or wind up in the
bottomless circular file.
Human Resources: People who know people are the luckiest people. The fact is that individuals within
programs are the first to know about good positions soon to become available. It's a smart idea to check
in with colleagues in those programs and parts of the country you desire. Putting out feelers like this
requires a bit of moxie but can be very productive.
Advertising: A simple way of getting a sense for what's out there is to "review the literature". Peer-review
journals in emergency medicine, newsletters, web sites and the like enumerate scores of opportunities.
These tend to surface one to several months after the host department has publicly stated the need.
Certain programs prefer to subscribe to the informal advertising approach of sending a letter to the
chairs of programs across the country stating that a certain type of position is available and would those

chairs please forward the names of any members of their faculties as potential candidates.
Passive Approach
In this scenario, you wait to be asked to the prom. This is likely to occur in two circumstances. In the
first, you've been an outstanding resident and the chair of your department would like to have you on the
faculty. In the second, you've been around a while, have established a reputation, and are being sought
for a higher level position, for example, chair, program director, or research director. If you're a senior
resident or young faculty, then passive approach is risky, at best.
Timing
For the senior resident, it's appropriate to begin the search in the late summer or early fall. A second hot
spot is in the spring when individuals who have promised to take certain positions on certain faculties
have opted out at the last minute. At that point, chairs are a bit more on the desperate side.
For the individual already on a faculty, these same kinetic principles apply. But, positions can open at
any time of the year, and it's a matter of being fortunate enough to hear about the openings or
constantly being on the hunt for them.
RESEARCH THE OPPORTUNITY
Preliminary Fact-finding
It makes no sense to rush off to an interview without having done considerable groundwork in advance.
Interviews are no walk in the park for either side. These take time, effort and money and should never
be taken lightly. There is no reason to proceed to that stage until you have a reasonable sense that a
legitimate opportunity exists. Likewise, the chair wants to size you up as much as possible and avoid the
rigor of interviewing a candidate who's a bad fit or never had interest in the first place.
Telephone Interview: You and the chair should spend a good measure of time sorting out the basics of
the position, the faculty, and the training program. Useful data can also be acquired from other members
of the faculty, particularly those in an area of your interest. Newer faculty will have a good sense of what
you should be asking about and what surprises might be in store. A bit harder to find but even more

valuable are those faculty who have recently departed.
Disclosure: Some applicants want to keep secret the fact that they are looking at another job. This is
only partly reasonable. If you're happy where you are, it's understandable that you don't want to be an
unsettling influence. Sometimes you wind up making your fellow faculty and chair nervous or cause
them to believe that you don't like them or your role there any longer. If you wind up staying where you
are or until you leave, this can make for a discomfiting situation. At this preliminary stage, you might be
able to get away with closed conversations with the department where you're interested in finding a
spot. However, at some point or another, and usually much earlier than you like (or realize), the outside
chair will make contact with your department in order to acquire a reference, thereby spilling the beans.
In this case, you're far better off having alerted the key individuals of your current faculty to this prospect
and hopefully ensuring their willingness to provide you a fair evaluation. Other candidates are
deliberately outspoken around their own institution about their prospects elsewhere. Those in this latter
category may be looking to improve their existing situation by insinuating their disappointment with
what's in hand and emoting the need to improve their lot in life by going elsewhere.
Miscellaneous: It's reasonable to spend a bit of effort researching the program. The RRC accreditation,
program history, faculty profile, and departmental accomplishments can be found through various
sources, including the program's own website.
Onsite Evaluation
This constitutes the interview process. The program will set up your itinerary as far as being toured
through the facility and meeting with various individuals. It's reasonable to provide input into this,
particularly if there are key figures with whom you wish to spend time. The number of visits that will be
sponsored by the host department may be zero, is usually one and can be more, particularly if you are
searching for a higher level position, notably the chair. You are certainly welcome to visit the program as
many times as you wish or need at your own expense. In this case, you should simply let the chair know
that you're coming and that you're interested in visiting with certain members of their or other faculties or
administrators.
Interviews: You'll want to spend time with the chair especially, various faculty (particularly those with
whom you would interrelate position-wise), the departmental administrator, and the head nurse.

Clinical Site: It is very worth your while to spend at least a shift working side by side with one or more
faculty attendings. This can be a real eye opener into how the department operates, the role of
emergency medicine residents in the department and the perception toward emergency medicine within
the institution. This is also a wonderful opportunity to speak with nurses and paramedics. It is also a
chance to appraise ancillary services.
WHAT'S IMPORTANT TO YOU
Know Yourself
This may not be the sole lame aphorism in this chapter, but it may well be the most important. Try to
take the time to understand what you want professionally and personally, how many hours you wish to
commit to your profession and where you'd like to be in the next 5, 10, or 25 years. Some of us are
incredibly compulsive in planning every little detail in our lives. Others of us are much more the day-to-
day existentialist and have trouble scripting these plans. Where- ever you lie on the spectrum, this is a
helpful self-appraisal technique. In fact, it should be repeated on an annual basis as if you were
preparing resolutions for the new academic year.
Certainly, the author of these plans is not just you but rather, you and the key members of your life. In
addition, taking the time to "interview" others in the field, particularly those with considerable experience,
can be very rewarding and enlightening.
The Role
Many factors deserve your careful consideration.
Clinical: How many hours will you work, which hours will these be (especially vs. others on the faculty),
and how will these change over time are all of considerable interest. As importantly, what is your role as
the clinical attending? What is expected of you as far as direct care provision, care supervision, problem
solving, documentation and teaching? You should get the specifics of this from the chair, the working
knowledge from the faculty, and the general sense of the playing field from your observations during
your interview.

Academics: The academic horn of plenty includes didactic teaching, writing, clinical research, bench
research, program development, and roles in academic societies. It's critical to understand which and
when these opportunities will be available to you. Certain roles beg specific conversations. For example,
if your wish is to have a predominant part of your nonclinical time spent in bench research, you would
want to know what facilities, equipment, personnel, and protected time are being proffered. For this and
most other roles, the chair will be the go-to individual. In addition, the chair should be able to speak to
the amount of commitment the department is willing to give to various endeavors. This commitment
includes adjustments in clinical hours, changes in administrative responsibility, and hard dollar support.
Administration: You may wish and you most certainly will be expected to take on administrative
responsibility within the department and the hospital. Specific needs will likely exist, and the existing
faculty may attempt to scramble their administrative load, leaving something less desirable for you to
scoop up. However, likes and dislikes vary widely within a faculty. You will want to express your
preferred administrative role, be willing to accept what is available and negotiate to be next in line or a
role player in that area to which you aspire.
The Players
For most, there is nothing more important than the people with whom you will work over the next few to
many years. Integrity, honesty, commitment, and selflessness are among attributes to hope for and
emulate in your fellow faculty.
Your Department: You clearly want to have a good sense for the chair as to manner of leadership and
departmental goals. You can derive a sense for this from your interviews with the chair, the
conversations held with other members of the department and perhaps sitting in on a faculty meeting if
able. The chair should be able to espouse clearly the mission of the department and the fellow faculty
can corroborate or refute whether the chair, faculty and hospital have resolve toward this mission.
Administration: Is the departmental administrator responsive to the needs of the department and
sufficiently empowered to see to their solution?
Other Departments: The chairs, program directors, and research directors of other departments can be
extremely influential in regard to emergency medicine generally and your role on the faculty, specifically.

The Place
The medical center is a key building block.
Financial Status: There is little that is more crucial these days in medical education across America.
This information can be difficult to derive. A good sense can be gotten from review of 5 years of overall
and operating budgets for the hospital, the division of medical education, and emergency medicine
specifically. Likewise, have positions been cut through the hospital or in emergency medicine? Valued
positions that can be cut include physicians, of course, but also key support personnel, for example, in
research.
Support of Medical Education: Hopefully, emergency medicine carries the same stature as other
departments in the eyes of the dean or senior administrator in medical education. Roles on committees,
access to financial and personnel support, and budgetary allocations are measures to be considered.
Benefits
Compensation: This includes base salary, merit increase, and performance incentives. Comparative
standards are available through the AAMC and the SAEM Salary Survey.
Perquisites: This is a complex area that includes health and dental benefits, disability, liability, vacation,
and retirement plans.
Support Services: These include Information Services, secretarial support, office space, research
equipment, the grants and contracts office, biostatistical support, and medical arts. Never to be
forgotten, of course, is parking.
Advancement
This can be considered in various forms.
Promotion and Tenure: It's worth spending an hour studying the "bylaws" of the P&T Committee. In
addition, the chair and members of the department should be able to provide a sense for what's needed
to get to the next level as well as the department's success in doing so.

Intra-departmental: It's tough to discover at the front end whether and when you'll be able to move up
the ladder within the department. This depends in large part on your own efforts but also on whether
certain positions will become available. At some point, you may feel compelled to move elsewhere
because you're stuck in a particular spot.
Special Opportunities: Check the track record of the members of the faculty as to positions held in
medical societies and academic societies. Will these be open to you and will the chair be supportive of
your taking on these additional roles?
Niche: The typical academic emergency physician begins to develop a special interest early on. Over
time, you as a faculty member should be able to acquire expertise and academic opportunities within
your niche such that you will become recognized for this, and therefore be sought accordingly for
collaborative efforts, grant writing, speaking opportunities and non-peer-writing projects.
WHAT'S IMPORTANT TO THE DEPARTMENT
Needs
The respective department will seek you for a specific need. You may come on as a utility infielder
where you'll play various positions but not take on a high profile role. Or, you are moving into a newly
vacated position or one that has just been created. It is very important that you understand what they
want, expect, and will accept both in the present and in the future.
Performance Standard
Whether you're a senior resident, young faculty, or senior member, the chair and department you're
interviewing with will want to know as much about you as possible. Your curriculum vitae will provide a
start. More importantly, the chair in particular should certainly check your references carefully as
regards your potential, your personality, and most importantly, whether you'll be a good fit.
NEGOTIATIONS
Dealmaker

You should and will want to work entirely with the chair. The chair, of course, answers to both the faculty
and to administration and will have limitations set by both. However, the chair should understand these
limitations at the front end and be empowered to deliberate with you. The wise chair will, of course,
listen carefully to the faculty and their impressions of the candidates.
Style
It's understandable that candidates want to shine themselves up a bit, but it's only right to be honest and
be yourself. Pretending to be otherwise will result in disappointment, if not disaster, for you the applicant
as well as for the receiving department. Hope for a win-win situation by achieving much of what you
desire but being flexible and accepting certain responsibilities or benefits that aren't your favorites.
As far as deadlines, it's understandable that you may be considering a position on one or more faculties
at the same time. You should not be pressured to make a decision before the match burns out. On the
other hand, asking for extension after extension on the deadline is unfair to a department who will need
to move quickly to fill the position that you turn down.
Contractuals
You will sign a contract, and you will certainly want to study that contract carefully and seek the
assistance of one more expert than you in this arena. You can take the legal beagle approach and ask
for every single detail and subdetail to be written into the contract. Or, you can rely mostly on a
handshake. The smartest strategy depends on what you're comfortable with but lies somewhere in
between these two. Neither the handshake nor the 100 page contract is fail-safe, particularly given the
dynamic situation of health care and medical education.
WRAPUP
Try to find out who you are and what you would like to do and be in your life. Certainly, this is easier
said than done. Then, it's a matter of finding the role and making the most of it. In this game, your talent
and most especially, your effort, make up 90% of the equation and is far more important than the actual
position or place where that position resides. There is luck of course, or if you will, fate, but you'll have
no control over that. Finally, understand that academic emergency medicine provides fertile ground for

an extraordinarily wide variety of people who wish to give something back as teachers, care providers,
and role models.
Bibliography
1. Marx JA. Academic emergency medicine in the year 2000. (eds: Hobgood,Cherri MD, Zink Brian,
MD) Emergency Medicine: An Academic Career Guide. Published by SAEM and EMRA. 2000. P 9-12.
2. Iserson KV, Adams J, Cordell WH, Graff L, Halamka J, Ling L, Peacock WF, Sklar D, Stair T.
Academic emergency medicine's future. Acad Emerg Med 1999;6:137-144.
3. Kristal SL, Randall-Kristal KA, Thompson, BM, Marx JA. 1998-1999 SAEM Emergency Medicine
Faculty Salary and Benefits Survey. Acad Emerg Med 1999;12:1261-1271.
4. 4. Ling LJ, Wilkinson J, Holroyd B. New models for emergency and ambulatory care at academic
health centers-Part III: Boston and Alberta, Canada. Acad Emerg Med 1995;2:1001-1006.
5. Lewis LM, Callaham ML, Kellerman AL, Marx JA, White DJ: Collaboration in emergency medicine
research: A consensus statement. Acad Emerg Med 1998;5:152-156.

Becoming a chair of an academic department
Author: W. Brian Gibler
Introduction
An academic emergency physician may be tempted by the opportunity to pursue the position of Chair of
a Department or Chief of a Division of Emergency Medicine. How can the successful
clinician/teacher/researcher decide if such a move makes sense, career-wise? The decision to pursue a
leadership role in an academic Department of Emergency Medicine should be obvious to the individual,
as well as to his/her peers. Hopefully the following information, offered from my perspective, will help
you decide if a Chair position is right for you.
Antecedents
Are leaders born or made? The likely answer is a combination of natural and learned characteristics. In
your life experiences thus far, you probably have been exposed to a number of individuals that people
naturally follow. Sports teams, families, clubs, organizations, and work groups all tend to be led by one
or two members that define the goals, direction, and ultimately the vision of the entire body. A number of
characteristics including athletic skill (Michael Jordan), charisma (John F. Kennedy), strength (Attila the
Hun), drive (Bill Gates), and intelligence (Abraham Lincoln) cause others to follow. Most of us are not
born with the expression of these characteristics at a level that would allow us to become historical
figures or cultural icons. There are many individuals, however, that have a combination of
characteristics, which can be honed and cultivated over time to allow one to lead a group. If you served
as the organizational center for groups in the past, created organizations to serve a need, were elected
team captain, chief resident, or purposefully chose to be the first to have a new experience or job, you
have the basic core of a leader. A mentor interested in developing your leadership skills can often

identify these characteristics and experiences.
Requirements
Chair candidates for Emergency Medicine positions in academic medical centers typically undergo the
same scrutiny as candidates for other academic departments. In high-powered, academic medical
centers, Chair candidates are expected to achieve success nationally as clinicians, teachers, and
researchers. Ideally, these individuals also have administrative experience that includes managing
people as well as developing a budget. In some circumstances, serving as a Residency Director or Vice
Chair provides this valuable exposure to management.
Search committees at research-intensive institutions expect to hire clinician scientists that have been
extremely successful at obtaining peer-reviewed federal and foundation funding. In addition, individuals
interested in becoming the Chair at such centers should have a national and sometimes international
reputation achieved through major peer-reviewed publications. Other less research-intensive academic
medical centers may emphasize clinical teaching experience with previous management training.
Goals Must Change: I to We
While obtaining the credentials as a clinician, teacher, and researcher necessary to be competitive for a
Chair position, you must be focused on your own career. While this self-centered approach to a career
is essential to achieving national prominence, this behavior can be disastrous for a Chair. The
successful Chair must literally become a coach, cheerleader, and mentor for his/her faculty and
residents. While the Chair is expected to continue to pursue interests and expertise that provides
national prominence for a Department, faculty in particular must be mentored and supported. Rather
than receiving satisfaction from one’s own accomplishments as a Chair, the success of the team (the
Department) becomes essential.
Begin With the End in Mind
This phrase is borrowed from Stephen Covey, author of Seven Habits of Highly Effective People. If you
are considering the pursuit of a Chair position, even in the relatively distant future, as a new faculty
member you must carefully build your career to be competitive for this position. Seeking a Chair job,
particularly at a major academic institution, requires career planning which can cover a decade or more.
First, identify a mentor that will work with you to achieve this leadership position. Hopefully, someone
that has successfully performed in this leadership role will be willing to help you climb this ladder.
Developing a focused research career while obtaining external corporate, foundation, and federal

funding provides the national prominence necessary to be competitive in a Chair search process.
Clinical expertise is a given and this should be a natural companion to bedside and didactic teaching.
Most academic emergency physicians enjoy clinical medicine and are enthusiastic teachers of the
specialty.
Obtaining the administrative experience necessary to gain people and budgetary management skills is
the area where your mentor can be most helpful to you. While the research, clinical, and teaching
accomplishments require your long term drive and tenacity, a Chair mentor can provide you with
important leadership positions within a Department that allow you to achieve management success.
Obviously you have a 7-10 year career plan, which allows you to "build" your Curriculum Vitae to
maximize your competitiveness for a Chair job.
Mostly Positives, But Some Negatives
If you enjoy team victory and the success of others, being a Departmental Chair is an ideal position.
There is perhaps no greater career satisfaction than to see your faculty successfully obtain funded
grants, publish important papers, and ultimately receive academic promotion. It truly is a greater thrill
than achieving these milestones in your own career. Developing a synergistic Department where faculty
and residents work together to accomplish goals that coincide with your vision of the future can be an
amazing experience.
While the clinical, teaching, and research efforts can be invigorating, the current financial climate of
medicine in general can make the Chair’s job a difficult one. In the past, financial skills were not as
essential as they are in the current environment. Understanding Departmental budgets, hospital
finances, decreasing reimbursement, and managed care can be difficult for the
clinician/teacher/researcher initially and often are not nearly as exciting as clinical diagnosis or scientific
discovery. If you do not enjoy finances and budgetary issues, I would not advise seeking a Chair
position.
The general financial climate for academic medical centers is also stormy. Reimbursement for resident
education, patient care, and medical student education seems to be in nearly constant flux. Federal and
State funding sources are subject to the vagaries of the current political climate. Clearly this has caused
many academic Emergency Departments to form alliances with community hospital EDs with expected
difficulties bridging these often very different cultures.

For some of these reasons, many outstanding academic emergency physicians decide to remain as
clinician/teacher/researchers without pursuing leadership positions in Departments. Knowing your own
talents, frustration level, and ability to give others credit can help you decide if a Departmental Chair
position is for you. Leadership can be extremely exciting as decisions that you make can have
significant impact on the Department and everyone that works for the Department. This level of
responsibility can take a substantial toll on your personal life, if you allow it to do so.
Conclusion
In this chapter, some of the issues involved in helping you make the decision to pursue an academic
Chair position are discussed. Becoming a Departmental leader can be extraordinarily rewarding for any
academic emergency physician. Faculty and residents working together to achieve a common vision
represents a career accomplishment for a Chair, which exceeds any individual achievements. This job is
not easy, however. Theodore Roosevelt expressed this eloquently:
"It is not the critic who counts, not the man who points out how the strong man stumbles, or where the
doer of deeds could have done better. The credit belongs to the man who is actually in the arena;
whose face is marred by dirt and sweat and blood; who strives valiantly; who errs and comes up short
again and again; who knows the great enthusiasms, the great devotions, and spends himself in a worthy
cause; who at best knows in the end the triumph of high achievements; and who at worst, if he fails, at
least fails while daring greatly so that his place shall never be with those cold timid souls who know
neither victory nor defeat."
My friends, it would be my pleasure to have you join me in the muck of the arena.

Academic Emergency Physicians as Institutional Leaders
Authors: Louis Ling, Gail Anderson Jr., Ann Harwood-Nuss, and Mark Steele
INTRODUCTION
For emergency physicians who develop a special skill for administrative problem-solving there are
many opportunities. Academic emergency physicians are well trained and well prepared to become

part of the hospital and medical school administration. The specialty of emergency medicine enables its
practitioners to develop goal directed behavior, the ability to prioritize, and fully utilize available
resources. The application of these learned skills in the area of administration is invaluable.
A background in emergency medicine also exposes its physicians to the broad scope of other medical
specialties, the challenges they face, and the individuals involved. Residency training includes off-
service rotations and the daily clinical practice of emergency medicine places us in the "fishbowl" where
we interact with almost every other specialty. Emergency medicine faculties rely on other specialties to
develop off-service rotations as well as to train non-emergency medicine resident physicians in the
emergency department. Few other specialties that have the opportunity to know and understand the
majority of other disciplines in quite the manner an emergency physician does. This knowledge is
extremely valuable in the administrative arena and places emergency physicians in a unique position to
serve the medical staff and educational programs on their campus. The emergency physician in a
leadership position can understanding the clinical, educational and administrative challenges faced by
our colleagues, represent their needs and support their goals. This gives emergency physicians the
unique opportunity to develop rapport and understand challenges facing this wide array of other
specialties.
As a hospital based specialty, a hospital will frequently turn to emergency physicians to improve
hospital affairs. Successful emergency physicians have learned to be diplomatic and can communicate
well with other physicians in a collaborative fashion. Frequently, emergency physician develop a
problem solving approach similar to their busy practice, which is direct and efficient, enabling us to
solve problems and help other physicians. After several years of this type of interchange, it is no
wonder that a successful emergency physician may develop a reputation as a problem-solver and a
team player, ideal skills needed for an institutional leader.
Several case studies demonstrate how several academic emergency physicians have evolved during
their career to include increasing institutional responsibilities.
CASE STUDIES
Gail Anderson, Jr., is Medical Director at the Harbor-UCLA Medical Center and Assistant Dean at the
UCLA School of Medicine. In addition, he is currently serving as the acting chief medical officer for the

hospital’s parent organization, the Department of Health Services (DHS) of the County of Los Angeles.
Previously, he had served as the Senior Vice President of Medical Affairs at the Grady Health System
and Associate Dean at the Emory University School of Medicine in Atlanta. Although his interest in
medical administration had origins from residency experiences, his role in directing Grady’s Surgical
Emergency Clinic and completion of a MBA program in the 1980s contributed to his appointment as the
hospital’s Associate Medical Director. His activities at the state and national level in ACEP as well as
participation in the Hospital Medical Staff Sections of the Medical Association of Georgia and the AMA
provided exposure to organized medicine and the broad constituency of medical staff issues.
Appreciation of the frequent diversity of clinical and academic perspectives was important in gaining the
support of the two medical school faculties who ultimately pressed for his appointment as Grady’s chief
medical officer when his predecessor was not re-appointed. When he was recruited to Harbor in 1998,
the need for building consensus among the medical staff was an important issue. His initial focus was
helping the hospital to achieve a successful JCAHO survey before turning to the recruitment of
department chairs and local staff problems prior to a request for him to serve as interim Associate
Director for Los Angeles County’s DHS.
Ann Harwood-Nuss has drawn on past experiences as well, prior to her appointment as Associate
Dean for Educational Affairs at the University of Florida College of Medicine at Jacksonville.
Administrative opportunities during her career in academic emergency medicine included program
director, chair, Director of Graduate Medical Education, and Assistant Dean for Educational Affairs, as
well as national leadership positions with ACEP. These experiences provided a rich opportunity to
master the scope of accreditation issues and graduate medical education. Her clinical experiences
enabled exposure to other medical specialties, thus preparing her for the administrative oversight role
in the Dean's Office of all GME programs. Knowledge gaps were present, however, and the acquisition
of new knowledge about the principles behind federal support for GME was essential for job
performance and support of the residency programs. Dr. Harwood-Nuss believes that preparation for
administrative leadership within a University system might include preliminary or concurrent training,
such as an MBA. Increasing federal and State regulations commonly require understanding of statute
language and federal financing of GME, a knowledge base not inherently intuitive to clinicians. In her
current position, a close collaboration exists with the teaching hospital Reimbursement Office, and an
optimal blend of effort based on a thorough understanding of GME and federal regulations.
Louis Ling is Associate Medical Director for Medical Education at Hennepin County Medical Center in

Minneapolis, MN since 1990. He used his past experience as a resident member on the Residency
Review Committee (RRC) to assist the faculty and eventually became the Associate Residency
Director for Emergency Medicine. Knowledge of the accreditation process was helpful to other
specialties in the hospital and he was frequently called on to give advice on these and soon other
medical education topics. Getting involved in national committees at SAEM and ACEP as well as
continued membership on the RRC gave opportunities to discuss these topics and to learn new
concepts to improve the home institution which in turn gave experience that could be shared nationally.
He was asked to coordinate hospital-wide educational affairs when his predecessor became the
medical director.
Mark Steele, is Chief Medical Officer (CMO) at Truman Medical Center (TMC) and Associate Dean for
TMC Programs at the University of Missouri - Kansas City (UMKC) School of Medicine in Kansas City,
Missouri and has been since 1999. He served as Program Director for the UMKC/TMC Emergency
Medicine Residency Program for seven years and Vice-chairman and then Chair of the Department of
Emergency Medicine for thirteen years. Just prior to becoming the CMO and Associate Dean, he
served as President of the TMC Medical Staff and President of the systems physician practice plan. As
a result of these leadership roles, he was asked to apply for the newly created CMO/Associate Dean
position. This position became necessary when a non-physician was hired as CEO. In his current role,
Dr. Steele oversees all of the medical affairs of the hospital, coordinates the resident and student
rotations, and other residency related activities including the NRMP "match" and resident graduation
ceremony. He is in a position to significantly impact other residency-related needs such as the resident
salaries, resident/student call quarters and conference and meeting space, and he helps to coordinate
the research infrastructure for the institution. Opportunities to impact clinical care at the hospital is
significant. He is involved in physician recruitment for several of the hospital-based specialties and
deals with issues of a multidisciplinary nature such as ED overcrowding and ambulance diversion,
issues of obvious importance to EP’s. He is also heads up the PI and Risk Management activities of the
hospital including the evaluation of sentinel events, as well as matters relating to credentialing and
privileging of the medical staff.
PITFALLS OF INSTITUTIONAL POSITIONS
The dual life as an institutional official and emergency physician presents some challenges. One
difficulty is learning to give up responsibilities in the emergency department to others. It is important not
to speak for the emergency department but to ensure that a separate individual can represent that

perspective. Otherwise, the institutional role is crippled by the constant conflict of interest or perceived
conflict between the institution and the emergency department priorities. Sensitivity to the possibility of
favoritism while conversely avoiding the opposite (over compensation) is challenging. Balancing the
needs of the hospital, university and physician practice group is always an issue.
It is important to have a good understanding of responsibilities with the emergency department chair,
especially if there is clinical salary support. Consider an exit plan if this administrative position does not
work out and whether you think this is a permanent or temporary career change. Increased institutional
and especially financial responsibility makes it more likely that you may fail or need to leave because of
political pressures out of your control when the institutional leadership changes, or with organizational
restructuring or mergers. Consider whether you will be comfortable rejoining the department faculty full-
time or would want to leave the institution to continue an administrative career.
ACADEMIC EXPECTATIONS CHANGE
Academic promotion may or may not progress in the traditional manner. The amount of time available
to pursue teaching/ research activities is usually severely curtailed. The busy medical director may
have to sacrifice some coveted academic recognition and achievements to fulfill duties to the institution.
Frequently, faculty members in such appointments maybe placed in an academic series delineated for
administrative physicians. Ultimately, the joy and satisfaction that comes from the work is making a
broader impact on patient care and helping to craft an environment that will allow fellow physicians to
effectively practice their profession and flourish in their teaching and research endeavors.
Academic productivity will certainly decrease but is not necessarily abolished. It may be possible to
lecture to the EM residents regularly and maintain participation in research such as Mark Steele with
the EMERGENCY ID NET research group. Ann Harwood-Nuss and Louis Ling have both continued to
edit textbooks but it is certainly a challenge for any administrative physician to maintain these activities
given the significant administrative burden.
SUCCEEDING IN THE INSTITUTION
Requirements of the medical director/associate dean position most importantly include good
communication skills, respect of ones colleagues, and common sense. A willingness to do what is right
and in the best interest of patient care is also important.

Prior administrative experience in a leadership role is probably the most important preparation for this
type of position. Mark Steele participated in a three-part medical director course jointly sponsored by
the National Association of Public Hospitals (NAPH) and the Wagner School of Public Health Service.
Similar leadership type courses are available through the Harvard School of Public Health and the
AAMC, which offers an Executive Development Seminar. They cover topics typical of most leadership
courses, including such as negotiation skills, media training, effective communication, budgeting, etc.
The opportunity to network with others in similar positions may be the most helpful part of these
courses. While taking at least one such course is recommended, it alone will obviously not turn one into
an effective administrator/leader overnight.
According to Gail Anderson, The foundation of a successful medical director is built on trust. The
support of the department chairs/chiefs is fundamental to making any significant progress. As a group,
these individuals must believe that the chief medical officer will deal with each of them in a fair and
forthright manner. Likewise, the other administrative colleagues must believe that the medical director
will honestly represent the needs of the institution and its patients. Perception that certain interests are
favored at the expense of others can be destructive to institutional morale. Thus, an emergency
physician needs to very careful to avoid being seen as using the role to advance the goals of the ED
over those of other departments. As long as the best interests of the patients are in the forefront, the
medical director’s support can remain firm.
The dynamic tensions that exist between various groups in academic medical centers provide an
opportunity for the chief medical officer to impact clinical care, education of house staff and students,
and research programs. If you happen to be an expert in these issues, the contribution can be more
obvious than when the matter is outside your specialty area. After considering input from reliable faculty
sources, and sometimes external individuals, the medical director often has to make decisions that may
or may not be pleasing to all parties. Usually, however, if appropriate inclusion, consideration and
discussion has taken place, the personality and influence of the office can be effective in guiding the
parties to reach a satisfactory solution. This is the real gratification of the job – creating the right mix to
catalyze very talented individuals to a point where they can achieve a previously elusive resolution.
NETWORKING
After joining the hospital or medical school administration, it is critical to develop a network of others
with the same interests. To keep this network it is critical to be active in different organizations such as

the American Association of Medical Colleges (AAMC) or Association for Hospital Medical Education
(AHME) or the medical school section of the American Medical Association (AMA) and to volunteer for
others such as the ACGME. The actual organization matters less than the exchange and interaction.
Some of these organizations are outside the usual emergency medicine realm but in time, as more
emergency physicians evolve into these roles, they have also become more visible in these
organizations.
TO SEE OR NOT TO SEE PATIENTS
Mark Steele believes- it is very important to remain clinically active to maintain credibility with the
medical staff. He is 75% administrative, 25% clinical (20% time clinical or one eight hour shift/week and
5% reserved for educational/research activity within the ED). This is not dramatically different from his
breakdown as chair (65% administrative, 35% clinical) but the administrative piece has certainly
changed. The ED staff allows him the flexibility to choose his shifts and as a result, he does not work
weekends for the most part but though they have offered to allow him to not work nights but he has
chosen to do so. He sensed a change in the way he was treated by fellow physicians almost overnight
after assuming his new role. One day soon after his appointment, one of the staff neurologists saw him
and said "there’s the administrator." She later saw him in scrubs when he was working in the ED and
she seemed surprised but pleased to learn that he still did clinical work.
According to Louis Ling, it is a constant challenge to stay competent clinically with less clinical time and
less time to spend on current reading. To remain up to date, the academic setting is advantageous for
the high number of state-of-the-art conferences, especially case conferences. Case conferences allow
discussion and thinking about challenging cases to which administrative physicians have less
exposure. The setting and the amount of clinical practice will vary but should probably involve exposure
to patients every week, but since he is half time paid by emergency medicine, his clinical shifts are
distributed through the weekends and nights proportionately.
The nature of faculty "shifts" in the Emergency Department make active clinical practice somewhat
difficult. The administrator’s normal duties occur during the traditional workweek, whereas an
emergency physician’s duties occur around the clock, seven days a week. Active clinical participation in
evening, night and weekend shifts may result in excess absence at a variety of administrative
gatherings. Ann Harwood-Nuss restricts her clinical activities to weekend ED shifts to avoid this conflict.

Gail Anderson notes that the ability to remain clinically active will vary with the demands of the
particular position and institution. At the associate medical director level, it may be possible and even
desirable to have some direct patient care activity. It is difficult to imagine that anyone can be credible
in the chief medical officer role without having demonstrated competence as a clinician. However, in
today’s highly complex health care environment a considerable amount of time, attention, and energy is
required to meet the myriad external regulatory requirements as well as the internal clinical operational
issues. "Protected" clinical time may be a luxury, at least in large public teaching institutions where
there is an expectation of immediate access to the top medical administrative officer when pressing
issues frequently arise. One should not be caught in a tug of war between a direct patient care
obligation and a duty to simultaneously attend to a critical institutional problem.
CONCLUSION:
When emergency medicine was young, it was at a disadvantage because the establishment was
unable to understand the emergency medicine perspective. That could only change as emergency
physicians matured and became the establishment. Emergency physicians are well trained and well
positioned take on leadership roles. The opportunities exist and emergency physicians should take
advantage of them. It is good for the individual, good for the specialty and good for the institution
On Becoming the Dean
On Becoming the Dean
Author: Vincent P Verdile, MD
Any emergency physician who has entertained the travails of a lifelong commitment to academic
medicine understands clearly the pathway to a successful career. A demonstrated mastery in the
endeavors of research, clinical practice and teaching are all essential. Medical schools have well
established academic promotion and tenure guidelines that articulate the pre-requisites for advancing
from Instructor to tenured Professor. To succeed in academia, one must focus on the long-term
objective of promotion. While success is measured in many ways, understandably, for those dedicated
to academia, becoming a tenured professor in emergency medicine is a recognizable milestone.
Perhaps the most coveted title in a medical school however, is that of the Dean. The Dean of a medical
school represents the highest authority in the academic medicine hierarchy. The scope of responsiblities
for the contemporary Dean crosses the entire spectrum of an academic health science center (AHCS)

including but not limited to patient care, education, research, and the business of medicine.
Unfortunately, since emergency medicine is such a ralatively new discipline in the house of Medicine,
there are few mentors and generally there are no established guidelines for emergency physicians to
follow to become a Dean. If an emergency physician wishes to obtain a deanship, where does the
process begin? While each medical school can have it's own unique system; this chapter will outline the
issues for emergency physicians to better comprehend to process.
Selection of the Dean
The nature of the selection process varies depending on the institution and the scope of responsibilities
for the Dean. Larger universities with multiple health care related educational programs might require a
different Dean than a small, single mission medical school. Whether or not a physician practice is part of
the medical school and the extent to which research and the research enterprise is focal to the
university's profile are all relevant and will determine the type of Dean that is sought after.
Traditionally a decanal search, commissioned by the Board of Directors/Trustees (BOD) of the
university or medical school, would be initiated as soon as they are made aware that an incumbent
Dean is stepping down. These searches can be resource intensive for an institution and can take a
considerable amount of time to complete (6 –18 months). Search firms can be retained to the do the
screening and queuing of candidates for an internal search committee. While search firms can expedite
the process, they will usually make it more expensive.
At anyone point in time there may be a fair number of the 125 Dean positions open and with active
searches underway. Currently, according to the Association of American Medical College's directory,
there are 13 acting or interim Deans in place with many active searches in progress. This can prompt a
BOD to test internal candidates in the role as "interim" or "acting". This can work both ways for the
candidate serving as interim in that great success may mean the permanent job is offered, and anything
less than great success, by whatever metric, can mean the search for the permanent will not result in
the interim getting the job. Internal candidates have an advantage in knowing the institution, the politics
and the scope of the position. The disadvantage is that there would be no honeymoon if selected and
the managerial style will be well known to the other leaders in the institution.
For external candidates, the challenge is to learn as much as possible about the medical school or
university during the interview process. This should include, but not be limited to the extent of the
endowment, the National Institutes of Health (NIH) ranking of the institution, the scope of the

responsibilities and the general hierarchical structure of the dean within the framework of the entire
AHSC. Depending on the by-laws of the university or medical school, the BOD usually retains the
responsibility to install a Dean once the selection process produces a candidate. For internal
candidates, deanships are frequently thrust upon them, first as interim to stabilize an organizational
crisis, and then depending on the decanal search process, becoming permanent. Whether internal or
external, the appointment of a Dean of a medical school is a chance to serve in an AHSC at a level
where strategic directions can be set and legacies can be established.
The AAMC estimates that between 1980 and 1992, Deans held the position for an average of 31/2 years.
While the high rate of turnover is clearly multifactorial, it begs the question of the validity of the
traditional deacanal search process. Clearly, given the dynamic forces affecting AHSC's in this country,
the qualities of a successful medical school leader must be identified.
Qualities of the Dean
In my opinion, the qualities that make for a successful emergency physician lend themselves very well
to the Dean's position. The Dean must be able to multi-task, move from topic to topic in rapid
succession, and not be perturbed by the emotional roller coaster that comes with the position. There are
many different constituents that must be satisfied, and any successes achieved by the medical school
faculty must not be shared while any failures rest entirely with the Dean. The analogies to caring for
patients in the emergency department is remarkable.
The Dean must have impressive interpersonal skills. Communication is paramount to success, as is a
sense of fairness, consensus building and empowering faculty and staff. While the responsibility for
delivering successful education, research and patient care missions rests with the Dean, the ability to
delegate is essential to getting the job done.
The Dean must have credible credentials, be dedicated to all the constituents…. faculty, students,
patients and staff and be honest. A key factor in producing the missions is having the trust and loyalty of
the faculty and promoting faculty empowerment. Because of the current health care and health
education environment, the Dean must also have balance and the ability to adapt to change. Knowledge
and analytic skills are essential to understand the ever-changing landscape of the medical education
and research environment. Familiarity with state and federal policies that impact medical schools and
their missions is paramount.

The final quality that must be emphasized for a successful dean is that of being able to make decisions
and sometimes with not all of the necessary data. Indecisiveness will paralyze the medical school, and
weaken the Dean's position of power in the AHSC. Being decisive, may lead to an erroneous decision,
but this can always be corrected at a later time. A Dean who is unable to make decisions and see them
through to fruition will never be successful.
Responsibilities of the Dean
The Dean will be expected to have a mastery over the business of the physician practice. Many medical
colleges are highly dependent on the revenue from the clinical practice to fuel the less than optimal
revenue generating missions. This financial reality ties the success of the education and research
mission to the clinical enterprise. Therefore the Dean must be an astute clinician, financially savvy and a
born entrepreneur.
Next the Dean must be the guardian of the educational mission. Many AHSC are under siege because
of financial exigencies. The education mission, while revenue generating, often can not sustain itself
given the true costs of educating physicians and scientists. The Dean must be willing to advocate for the
educational imperatives and negotiate tenaciously for every dollar needed to deliver the mission. While
expertise in adult education methodology is helpful, more importantly the Dean must be able to develop
an educational strategic plan, critically evaluate the educational process, determine the desired
outcomes, and hold the faculty and academic administration accountable for the mission. As clinical
faculties are pushed harder and harder to generate clinical revenue, the time spent in medical education
is infringed upon. The Dean must be able to demonstrate the compensation for medical education as
well as articulate the deliverables for the clinical faculty.
As long as the NIH continues to increase the amount of federal dollars available for research, medical
schools will intensely compete for those dollars. The benefits to the research program and the medical
school are enormous because of the indirect revenues from NIH grants. Furthermore, to the extent that
it is valued, the NIH ranking of medical schools based on the funding can be an important metric for
students interested in medical education or basic science training.
The Dean must be sure that the science of the medical school is pointed towards the areas that the NIH
is funding and plan accordingly. Analogous to the clinical faculty, the basic scientists have limited time

for the education mission as they are forever pressured to generate grants. It is incumbent upon the
Dean to be sure the scientists have a clear understanding of the expected role they play in both the
graduate studies and medical education programs.
Another quality to mention, also pertaining to research is that of research compliance. In many medical
schools the Dean serves as the Research Compliance Officer for all human and animal research
programs. While being a champion of the research mission it is imperative that the compliance with
federal assurances for safe research practices is maintained in order to stay in the research business
for the long term. It is encumbent upon the Dean to be sure the medical school fosters an intellectual
milieu that is ever curious about science but ever sensitive to the needs of patients.
The resources available to any Dean are finite. Given an unlimited budget, most Dean's would over
spend! Therefore, it is important for Dean's to spend considerable time raising money for the medical
school's missions. Fund raising takes on increasing importance for Deans at medical schools with small
endowments or in the face of new demands (i.e. new buildings) on fixed resources. Alumni are the
natural first choice to solicit support, but foundations, corporations, grateful patients and the general
public are also potential benefactors. Fund raising can and perhaps should consume a fair amount of a
Dean's time to help secure the future financial viability of the medical school.
Perhaps the least exciting and yet undeniably important responsibility of the Dean is to be an effective
administrator. Any medical school, large or small, has at its core a business, facilities, employees,
contracts, and strategic planning. Furthermore an essential responsibility of the Dean is to select
department chairs and medical school administrators (Associate and Assistant Deans), which will
directly impact on the effectiveness administration. Appointments will reflect on the Dean's ability to
manage the medical school. Administratively, the Dean must possess all of the skills of an accountant,
an organizer, a social worker and a visionary.
The Dean will be in a position of power and have all of the responsibilities of the position in any
institution that places value on the tripartite mission…. education, research and patient care.
Conclusion
The attainment of a deanship at one of one hundred twenty five medical schools in this country is clearly
one of the most recognized and coveted positions in academic medicine today. While the pathway to a

deanship is infrequently through academic emergency medicine, it is likely that given the training,
decision making ability, and ever growing stature in academic medicine that emergency physicians will
be recruited to participate in the searches for leadership in medical schools.
This chapter has outlined some of the issues that will confront emergency physicians interested in
becoming the Dean. The dynamics that are shaping the future of AHCS's will require a non-traditional
Dean. Emergency physicians as our history has shown, have been non-traditionalists in the House of
Medicine and in this author's opinion make superb candidates for deanships.
SUGGESTED READINGS
1. Hellman S. Tales of the unnatural: Return from the dean (d). JAMA 1998;280:1657-1658.
2. Davis BC. Ten questions every dean should ask. Currents 1998;28-32.
3. Cullinan M. But what does a dean do? The Chronicle of Higher Education March 9, 2001, B5.
4. O'Connell GE, Grosch WN. Using quality management to balance the economic and humane
imperatives in behavioral healthcare. J Qual Improv 2001;27:107-116.
5. Pardes H. The perilous state of academic medicine. JAMA 2000;283:2427-2429.
6. Griner PF, Danoff D. Sustaining change in medical education. JAMA; 2000:283:2429-2431.
7. Aaron HJ. The plight of academic medical centers. Brookings Policy Brief. 2000;59:1-8.
8. Bonner TL. Crushing the commercial spirit in academic medicine: A crusade that failed. Acad
Med 1999;74:1067-1071.
9. Bentsen T. Getting personal could be key to deans' durability. AAMC Reporter 1998;7:1-3.
10. Clawson DK, Wilson EA. The medical school dean, reflections and directions. McClanahan
Publishing House, Lexington, KY 1999. www.aamc.org/about/cod/opendeanship/start.htm
11.

Prophylaxis Against Academic Burnout
Author: Carey D Chisholm
Introduction
The academic career has many unique challenges and sources of stress. Over time the risk of
"academic burn-out" will confront many if not most emergency physicians engaged in academics.
Fortunately, many of the very sources of burn-out may in fact serve as resources for career longevity
and fulfillment.
Potential sources of stress in academic emergency medicine revolve around the lack of set limits within
one’s job setting. The job is simply never "finished". In fact, there are frequently simultaneous and
possibly conflicting tasks that may pull one in multiple directions. The grant deadline, manuscript
revision, textbook chapter deadline, national committee task, hospital and departmental committees,
medical student letter of recommendation and resident counseling are simply layers added onto one’s
clinical responsibilities. Without proper planning and the correct frame of mind, these constant deadlines
and tasks can create a sense of personal chaos and job dissatisfaction. Furthermore, one’s ethical
responsibilities to mentor and teach medical students and residents creates the need to approach tasks
with a perfectionistic inclination.

Fortunately, there are many components of an academic career that can counterbalance these
stressors and perhaps assist in preventing job dissatisfaction and burn-out. While multiple jobs may be
taxing, they also prevent one from becoming numbed by repetition and the rut of routine. Intellectually,
the myriad of challenges poised by our patient population, inquisitive medical students and assertive,
intelligent EM residents serve as daily challenges for us to remain a student for life. Intellectual curiosity
is valued and cherished in the academic setting. As one progresses in their career, areas of true
expertise are developed, and are highly valued by medical students, residents and colleagues at a
national or international level. Opportunities abound to learn new skill sets, accept new administrative or
teaching challenges, and engage in professional growth opportunities.
Have a mission statement or a personal vision. Ideally this integrates your personal and professional
life with both the home and work environment. Failure to do so will result in conflicts, often
subconscious, that result in long term insidious stressors. Without this personal mission statement, it
becomes impossible to prioritize tasks and budget how one should allocate their time. The personal
mission statement is your rudder, and those who fail to have one will risk drifting aimlessly through their
career.
Develop Time Management skills. This is the most important stress management and productivity tool
that one can have. If you have not had formal training in time management, it is almost certain that you
are working twice as hard and accomplishing only two-thirds of what you are capable of doing. Learn
and develop this skill set for your professional future and family sanity. You must have a personal
mission statement, a prioritized task list and a planning device that is comfortable for you to carry and
use. Time management experts estimate that for every hour spent "planning" you "save" an additional 3
hours. Perhaps most important is the sense of personal control that comes with time management.
Personal Planner (Organizer)
This device must be portable and kept with you at all times. Computer based models are popular, but
the bottom line is that no device is effective if not used, and there’s nothing "wrong" with a paper based
system if preferred. A month at a glance scheduling calendar is the minimum, although most academic
physicians will need a week or even a day at a glance. Recurring dates such as monthly committee
meetings must be entered (include social events such as birthdays too). "Retrograde planning" of
preparatory steps can then be entered into the task planner. This critical skill begins with a final product

deadline (e.g. presentation at a national meeting) and breaks it into component parts. Each component
part is then assigned a deadline in your planner, allowing a stepwise progression towards the final goal.
The more specific each component part, the better. Building in a buffer for each component completion
deadline allows unexpected crises (or opportunities) to be addressed. Tasks are prioritized each day to
channel your activities towards obtaining your most important goals and meeting upcoming deadlines.
This is not simply a "to do" list, as it isn’t the number, but rather the quality, of the tasks accomplished
that is important. Such a device should also contain contacts (never look up a phone number more than
once) and serve as a repository for "brainstorms" that fleetingly emerge from our subconscious. At least
weekly you need to sit down and plan your upcoming week in some detail, while looking ahead over the
next month. At least once a month, look ahead for the next 6 months to refresh your memory about
upcoming projects and deadlines.
Learn to say "NO". This is a common skill among almost all successful academic faculty members. At
some point, usually about the 5-10th year of our career, we realize that we cannot continue to add new
responsibilities and fulfill existing obligations and tasks well. As more and more tasks are added,
projects become rushed and deadlines are missed. Frustration mounts as it becomes evident that we
are no longer producing high quality work. Before taking on a new task or responsibility, examine it
critically to see if it meets your professional (and personal) mission statement. If it does, develop an
accurate assessment of the time commitment. Where will those hours come from? Select another
current activity of equal time commitment and off-load it before accepting the new challenge. And be
careful to maintain a "crisis buffer" of time as invariably family illnesses, or other unexpected events will
develop. Failure to do so assures that the "crisis management" comes out of personal (family) time or
means missed deadlines.
Delegation: Many of us do not delegate tasks well. This is often rationalized by thinking that only you
are capable of performing the task (correctly), or concern that your value to the organization may be
diminished (and you therefore may become expendable) if others are taught to do tasks for which you
are responsible. Remember however that you can delegate authority to do a task, but you cannot
delegate responsibility for assuring the product is completed. Learn what items can be assigned to
others to accomplish for you. The time invested in training an assistant will pay off many times over in
the time you save by effective delegation. This is also key in developing our future leaders and an
invaluable component of the mentoring process. Develop priorities and stick to them. Decide the t time
with which projects need to be accomplished, and request weekly updates of the progress made.

Work smarter, not longer. Americans work longer hours than any other industrialized nation. Our
ability to work hard serves as a source of pride and has been integral to our productivity. However, the
candle can be burned at both ends for only a finite period of time. By focusing 80% of our efforts on the
critical 20% of high priority tasks, we can increase productivity without increasing our work week.
Indeed, as one progresses in their career, prolonged work hours may serve more as a red flag of
personal disorganization rather than a badge of honor. It’s not how many hours you work that
matters…it’s how productive you are with your hours worked. Almost everyone can easily learn to work
more efficiently through the application of basic time management skills. Workaholics develop
dysfunctional coping strategies and ultimately lose their creativity and productivity. The Starling curve
analogy applies here.
Block out "protected time" every week. This should include both personal as well as professional
time. During such times, accept no phones calls or office visits. This is your private, focused time.
Whenever possible, arrange this during periods of intellectual and physiologic peaks in terms of your
circadian rhythm. Your office door must remain closed in order to discourage passersby from
interrupting you. Use this time also to protect yourself physiologically from the stress of shift work. For
instance, if you are between 2 night shifts, do not allow yourself to be scheduled for a committee
meeting in the mid-afternoon. How many of those attending would be willing to meet with you at 0200
hours in the morning? Use e-mail or a telephone call to convey critical information that may impact
decisions at the meeting. A well run meeting will have both an agenda as well as good minutes, allowing
two opportunities for your input if you choose to miss the meeting. Time for aerobic exercise (minimum
of 20 minutes 3 times a week) should also be guarded from intrusion.
Guard your schedule carefully
Once you create a daily schedule, try to stick to it. This will be extremely difficult as there are many
interruptions that will rob you of time. Phone calls, impromptu meetings, non-scheduled visitors, and
email are all "time robbers". Being available and flexible is important up to a point, but a complete "open
door" policy will likely cause you so many interruptions that you will be left with little quality time to
perform your daily tasks. Unless expecting a phone call, try letting voice mail take messages, batch
them, and return them when taking a break from other tasks. If appropriate, answer by email, which
takes considerably less time. Speaking of email, try to do this only once a day. Many individuals find that
reading and answering email takes less mental concentration than writing publications, reviewing

articles, or designing projects. Consider saving email for the end of the day thereby protecting the more
mentally alert morning hours for important (higher priority) other tasks. If possible, spend some portion
of your office time during off-hours. Many successful academicians will tell you that their most
productive office time is before 9am or after 5pm as this minimizes interruptions and impromptu
meetings by others who "just notice you" in the office.
Other Time Management Tricks
Use your commute time wisely: This can be a source for CME (educational tapes), the major venue to
keep up with current events, an opportunity to plan your next week, or even accomplish work. The use
of a small hand-held Dictaphone is particularly useful for generating letters or organizing your "to do" list.
For drivers, be wary about the use of the phone while operating a vehicle. Books on tape can also
create a recreational outlet.
Record TV programs: This allows you to watch them on your schedule, not theirs, and best of all
allows you to fast forward through all of those mind-numbing commercials. For instance a 3.5 hour
football game can be watched in 1.5 hours by recording it (while you’re outside enjoying the sunshine at
the park). By purchasing your own exercise equipment, you can multi-task even more by watching the
tape while working out. DVD, with subtitles, offers a way to watch movies while exercising.
Take advantage of small chunks of time: Five or six minutes waiting in a line may seem only a minor
annoyance. Ten such episodes in a day quickly add up (over 2 weeks a year!). EM physicians are
masters of multi-tasking, and of turning attention from one thing to another. Capture these otherwise
wasted minutes by keeping your personal planner at hand (or your cell phone, perhaps even that
magazine, journal or novel).
Avoid procrastination: All of us are procrastinators up to a point. This is perhaps the greatest time sink
of all. Deferring activities that we dislike, appear overwhelming, or make us uncomfortable is human
nature. Divide such activities into small "bite-size" pieces, and work slowly (yet progressively) towards
their completion. Build in a series of rewards for those particularly undesirable tasks ("I’ll register the car
today, but go to that movie afterwards"). Finally, a good rule of thumb is to try not to pick up a piece of
paper more than twice without taking some sort of action on it. If you have let it lay for a week without
taking action on it, then likely it isn’t that important anyway. You should strongly consider throwing it
away, or delegating it to someone else to save yourself time better spent in more productive pursuits.

Other Concepts About Burn-Out
EM is a clinical specialty. Accept this, and the clinical work in the ED that accompanies this. Clinical
teaching remains a key activity for EM faculty, and should never be denigrated as a chore. Value your
clinical time and protect it from incursions from other areas of your job. For instance, I do not accept any
non-patient care telephone calls during ED shift time. Trying to solve a difficult administrative problem or
plan a teaching event or committee meeting will result in two inadequate performances, and raise rather
than lower one’s stress levels. Your patients and your students/residents need your focused attention
during these times, and your professional obligation lies with them. Caveat: one cannot maintain the
same clinical work schedule as one’s community colleagues and expect to be academically productive.
Academicians often work unrealistically high clinical workloads.
Institutional alignment. Academicians who remain in their positions for extended periods of time have
developed a sense of "alignment" with the values of their academic center. If the values diverge, conflict
results and longevity is unlikely. New chairmen, Deans, or hospital CEO/CFO’s all may impact an
academic center’s institutional values. Perhaps the best strategy to avoid unpleasant surprises is to
work at centers that have EM departmental representation in search committees for key institutional
personnel.
Play hard. This means that you need to have a personal life and identity that as separate from your role
as an academic EM physician. Your family and close friends require appropriate investment of time and
energy on your part. One of the most frequent themes among business executives is that they wished
they had spent more time with their family than they did. Talk to older mentors and you will be surprised
how pervasive this is. Only strong attention to this and proper planning will allow you to avoid making
this tragic mistake. On a personal level, it is easier to empathize with our patients and our
colleagues/students at work if we are well-rounded and have an active extracurricular life. Family
outings should be part of your regular planning, and never become the victim of meeting a deadline.
"Medicine free" evenings are critical when out with work colleagues at events that include non-medical
spouses and friends. I encourage you to envision how bored you would be if you sat at a dinner table
with a group of accountants and listened to them discuss their "great accounts" all evening. Younger
faculty have more difficulty with this, but with agreement that "medical talk is taboo" (and a few pregnant
pauses the first time you try this), it is surprising how enriching the social event becomes. Non-medical

friends and family are intrigued with the humanistic aspects and stories of our practice, so if you must
revisit the workplace, focus on these (but be careful not to violate patient confidentiality). Vacations
should be exactly that: time away from professional obligations to use for personal relaxation, growth
and family time. Work during a vacation is an oxymoron. Leave it behind and DO NOT feel guilty about
not working. Learn to relax! Your productivity is enhanced by this activity. Set goals for personal
development. For instance, decide to develop a new hobby every other year. This complements your
"student for life" role as a faculty role model, and enriches your life with new knowledge, experiences
and friendships. We read so much material in our professional lives that it is easy to lose track of the joy
of pleasure reading. Again, make a goal to regularly engage in non-medical reading.
Other Wellness Tips
Exercise
This is a critical component of any wellness program. A well designed exercise program not only
increases energy and stamina but also bolsters the immune system. Doing this in combination with
watching TV, pleasure reading, or with a group of friends makes it a social event as well. Exercise not
only provides health benefits for the body, it is also a great stress reliever. Remember going for a walk
to clear your mind when studying for tests? Muscular activity triggers the sympathetic nervous system
and helps keep you mentally alert. Even stretching exercises at your desk may afford a needed mental
break and result in better creativity. As noted above, a minimum of 20 minutes of aerobic exercise or
resistance training three times a week is recommended. Try to schedule some regular time at the gym,
walking, jogging, or other physical activities to maintain peak performance.
Pleasure reading
For reasons discussed earlier, this activity augments one’s humanistic qualities as a physician, adds
social interests, provides an escape from stress and breaks the rut of reading only professional material.
Reading "humanities" books (how other people live and think) allows a broader perspective and
potential for empathy. Setting a goal, such as reading one novel a month, increases the likelihood that
this will be accomplished.
Some of the material in this chapter also appears in the chapter "Physician Wellness in an Academic
Career" co-authored with Debra Perina, MD in the SAEM-EMRA Emergency Medicine: An Academic
Career Guide.

References
Andrew LB, Pollack ML, Wellness for Emergency Physicians, ACEP, Dallas, Texas, 1995.
Gallery ME, Whitley TW, Klovis LK, et al, A study of Occupational Stress and Depression among
Emergency Physicians, Ann Emerg Med, 31, 1992, 58-64.
Hall JN, et al, Factors Associated with Career Longevity in Residency-Trained Emergency Physicians,
Am J Emerg Med, 21, 291, 1992.
Hallery ME, et al, A Study of Occupational Stress and Depression Among Emergency Physicians, Am J
Emerg Med, 21:58, 1992.
Keller KH, Koenig WJ, Management of stress and prevention of burnout in emergency physicians, Ann
Emerg Med, 18, 1989, 79-84.
Meyers MF, Doctors Marriages: A Look at the Problems and their Solutions, Plenum Medical Book Co.,
New York, NY, 1994.
Pfifferling JH, Burnout Self-Appraisal, Center for Professional Well-being, Durham, NC, 1986.
Phifferling JH, Things I Wish They Taught in Medical School, Resident and Staff Physician, 36:85, 1990.
Quill TE, Williamson PR, Health Approaches to Physician Stress, Arch Intern Med, 150, 1990, 1857-
1861.
Sheehy G, New Passages: mapping your life against time, Random House, New York, NY, 1995.
Sotile W, The Medical Marriage: A Couples Survival Guide, Birch Lane Press, 1996.
Whitehead DC, Thomas H, Slapper D, A Rational Approach to Shiftwork in Emergency Medicine, Ann
Emerg Med, 21, 1992, 1250-1258.
Further reading
Alec Mackenzie The Time Trap 3rd
edition, 1997 AMACOM
Alan Lakein How to Get Control of Your Time and Your Life. 1973 Signet
Susan Silver Organized to be the Best. 1995 Adams – Hall Publications
Jane B. Burka & Lenora M. Yuen Procrastination : Why You Do It, What to Do About It 1990 Perseus
Press

Resources for Faculty Development
FACULTY DEVELOPMENT LINKS
The brief annotated bibliography that follows was drawn from the indexed Emergency Medicine
literature using the unmodified search term 'faculty development'. Compared to other specialties,
particularly Family Practice, Emergency Medicine has published relatively little on the subject of faculty
development among academic emergency physicians.
The Champions Project: A Two-tiered Mentoring Approach to Faculty Development
http://www.academicmedicine.org/cgi/content/full/75/5/553
Faculty in Wayne State University's Department of Family Medicine have undertaken the Champions
Project, a systematic, collaborative effort to achieve higher levels of professional performance in the five
domains of patient-centered clinical practice and teaching, evidence-based medicine, practice-based
research, professional academic skills, and leadership and organizational skills. Although facilitated by a
medical educator who coordinates departmental faculty development, each domain is 'championed' by a
core department faculty member who has both skill and interest in the targeted area of faculty
development. In turn, each champion chooses a national-level domain expert for long-term consultation

to design objectives, instruction, and outcome measures for the content area. These faculty create and
deliver, on an ongoing basis, a faculty development curriculum through which department members can
continuously keep their knowledge up to date and improve their skills in each domain. Acad Med
2000;75:553-554.
Faculty Development Site of the Faculty of Medicine of McGill University
http://www.medicine.mcgill.ca/facdev/
This site provides information about faculty-wide workshops at McGill, Medical Education Rounds,
Teaching Scholars Program, and links to medical education sites of interest.
A Faculty Development Workshop on "Developing Successful Workshops"
http://www.academicmedicine.org/cgi/content/full/75/5/554
This workshop was designed to give participants a framework for developing successful workshops and
to take them through each of the planning steps. On the first day, workshop modules consisted of
defining participant needs, setting appropriate objectives, matching content to objectives, and matching
teaching methods to content. On the second day, participants had an opportunity to apply the steps
discussed on the first day to a workshop they were planning to conduct in their own setting, and to
review strategies for evaluating workshops. They worked in pairs to design (or refine) their workshop
content, and then presented their plan to the larger group for feedback and discussion. The last day of
the workshop emphasized facilitation skills for both interactive large-group presentations and small-
group discussions, and each participant was asked to present a part of his or her own workshop to the
group. Each workshop module was introduced by a brief plenary session that summarized the key
issues for discussion and was supplemented by a detailed handout designed to guide workshop
planning. However, most of the activities took place in small groups. Acad Med 2000; 75:554-555.
Faculty Professional Development Workbook
http://www.mcphu.edu/col/wkbkcontents.htm

This website and its links describe the Annual Goals and Objectives process that accompanies the
Faculty Professional Development Conference used at MCP-Hahnemann to assess individual faculty
achievement and offer guidance for professional growth.
A Computer "Boot Camp" for Academic Medicine Faculty
http://www.academicmedicine.org/cgi/content/full/75/5/555-a
The Office of Medical Education Research and Development (OMERAD) at Michigan State University
sponsors an annual faculty development seminar series dedicated to training academic physicians in
essential faculty skills. Computer skills such as word processing, preparing scientific presentations,
information retrieval and management, electronic communication, and bibliographic reference
management are imperative to professional productivity and development. Because most academic
medicine faculty never receive training in computer skills, a series of workshops was developed in 1998
based on Carroll's minimalist design principles. Using Carroll's principles, and the analogy to the military
approach to training, the seminar series was named Computer Boot Camp. Acad Med 2000;75:555-556.
Using the Internet Effectively
http://www.medinfo.ufl.edu/cme/inet/
This program is intended for anyone interested in using the Internet as an effective medical resource. It
includes a complete 25 minute RealAudio lecture with synchronized slides by the Director of Medical
Informatics at the University of Florida.
Medical Informatics for Faculty Development
http://www.omerad.msu.edu/reznich/homepage5.html
The purpose of this site is to introduce physicians and other health professionals and learners 1) to the
many uses of the Internet and 2) to computer skills that will support the academic side of medicine and
medical education. All modules for electronic mail, newsgroups and the web are based upon versions of

the Netscape tool package. Modules that address academic medicine computer skills are based upon
common computer productivity tools such as Microsoft Word.
The Faculty Self-efficacy Scale: A Tool for Evaluating Faculty Development Interventions
http://www.academicmedicine.org/cgi/content/full/75/5/559
The Faculty Self-Efficacy Scale is designed to measure faculty physicians' perceived self-efficacy for
performing tasks within three professional role domains: (1) teaching, including teaching in clinical and
classroom settings; (2) scholarship, including developing and evaluating curricula within an area of
expertise and writing for publication; and (3) professional development, including planning career
strategies and employing key interpersonal skills, such as collaborating and sharing feedback with
colleagues, negotiating professional role boundaries, and managing conflict. The instrument consists of
nine scenarios, each of which describes a common, yet challenging situation pertaining to one of the
three professional role domains. Each scenario is followed by a set of concrete tasks identified by
medical educators as important for effectively addressing the situation described. For example, a
scenario on delivering formal presentations is followed by, "How confident are you that you can: (1)
prepare a presentation focused on a few essential learning points; (2) design slides to enhance your
presentation; (3) use a delivery style that keeps your audience engaged; and (4) incorporate audience
participation methods in your presentation?" Faculty physicians completing the instrument are asked to
rate their perceived capability to carry out each task on an 11-point scale ranging from "cannot do at all"
(0) to "certain can do" (10). Acad Med 2000;75:559-560.
Teaching & Testing:
http://www.academicmedicine.org/cgi/reprint/75/11/1144.pdf
Purpose. Faculty development programs and faculty incentive systems have heightened the need to
validate a connection between the quality of teaching and students’ learning. This study was designed
to determine the association between attending physicians’ and residents’ teacher ratings and their
students’ examination scores. Method. From a database of 362 students, 138 faculty, and 107 residents
in internal medicine, student-faculty (n = 476) and student-resident (n = 474) pairs were identified. All
students were in their third year, rotating on inpatient general medicine and cardiology services, July

1994 through June 1996, at a single institution. The outcome measure for students’ knowledge was the
NBME Subject Examination in internal medicine. To control for students’ baseline knowledge, the
predictors were scores on the USMLE Step 1 and a sequential examination (a clinically-based pre- and
post-clerkship examination). Teaching abilities of faculty and residents were rated by a global item on
the post-clerkship evaluation. Faculty’s ratings used only scores from prior to the study period;
residents’ ratings included those scores students gave during the study period. Results. Multivariate
analyses showed faculty’s teaching ratings were a small but significant predictor of the increase in
students’ knowledge. Residents’ teaching ratings did not predict an increase in students’ knowledge.
Conclusion. Attending faculty’s clinical teaching ability has a positive and significant effect on medical
students’ learning. Acad Med. 2000;75:1144-1146.
Faculty Development in Women's Health
http://www.academicmedicine.org/cgi/reprint/75/11/1095.pdf
The authors present a strategy for residency faculty development in women's health, the reasons that
such a strategy is necessary (e.g., women's health encompasses much more than reproductive and
disease issues, and is cross-disciplinary and intrinsic to all of family practice), and their residency
program's experience with its development and implementation from 1994 to the present. In creating the
program, the residency program's faculty used as a context some lessons learned from family medicine,
since the rapid growth of family medicine provides a historical example of dealing with a critical shortage
of faculty for new residency programs and the need for a new way to train educators. Also, the faculty
reviewed the literature about faculty development in medicine, models of teaching and learning from
women's studies, and group theory, specifically the skills concerning conflict and diversity. They used
the salient elements from each (which the authors outline) in fashioning their new faculty development
program. The resulting program also grew out of focus groups with patients, input from staff, residents,
and faculty, and meetings and workshops, including some intense and highly charged discussions in
which the faculty participants, both men and women, confronted their own views and biases and worked
hard to successfully forge a common and relevant vision of women's health. The program has fostered
faculty who are knowledgeable about the diverse educational skills required to teach women's health.
They use these skills in all curricular content, thus demonstrating a new way to educate residents as
well as faculty. Acad Med. 2000;75:1095-1101.

Council of Emergency Medicine Residency Directors
http://www.cordem.org/facdev/2000prog.htm
The above link is to the Council of Emergency Medicine Residency Directors’ web site. CORD and
AACEM co-sponsors a yearly conference entitled "Navigating the Academic Waters", which touches
upon many topics relating to Faculty Development. Topics available for download include: Common
reasons for manuscript rejection, networking lab, and time management skills.
The Association of American Medical Colleges
http://www.aamc.org/meded/facaffs/biblio/biblio.htm
An extensive bibliography complied by the AAMC containing references to faculty appointment,
promotion, tenure, evaluation of teaching, research, and clinical practice, productivity, and strategies for
further development of teaching and research skills.
Scholarship in Medical Education
AAMC/GEA Project
http://www.medlib.iupui.edu/cgea/geasclrpro.html
Medical schools now recognize that the professional development, reward, and promotion of faculty who
support the core mission of education has been limited by the inability to critically evaluate candidate's
scholarship in this arena. To address this need, the AAMC undertook a project on educational
scholarship in an effort to develop, disseminate, and facilitate implementation of a renewed concept of
scholarship as it relates to medical education. The project steering committee began with a definition of
scholarship and subsequently developed a set of "teacher as scholar" scenarios to explore teaching as
scholarship. These scenarios are provided here as tools to stimulate critical discussion regarding
teaching as scholarship.

Mentors at University of Virginia
http://www.med.virginia.edu/ed-programs/cme/fdp/fdp.html
The University of Virginia medical school provides its junior faculty with a list of mentors at the associate
or full professor level. The goals of the mentor-protégée relationship are: Orienting new faculty,
facilitating introductions, mentoring in research, reviewing grants and manuscripts, evaluating teaching,
supplementing annual career review, preparing professional portfolios, and serving as advocate both
within and beyond the institution. Their faculty development program also includes a year long lecture
series on such topics as teaching with multimedia, searching medical literature, patents, intellectual
property and technology transfer, the new ABCs of Medicine: ICD, CPT, and RVU, a practical workshop
on writing for medical and scientific journals, preparing teaching portfolios for evaluation and promotion,
grant writing workshop, preparing your portfolio for promotion & tenure, keys to effective presentation, &
handouts.
The University of Virginia School of Medicine's website also offers links to other medical schools' web-
based instructional materials for these disciplines:
Anesthesiology / Basic Medical Ethics / Biochemistry / Cardiology / Cell and Tissue Structure /
Dermatology / Doctor-Patient Illness / Endocrinology / Environmental Medicine / Epidemiology / General
Topics / Genetics and Biostatistics / Geriatrics / Gross Anatomy / Introduction to Clinical Medicine /
Microbiology / Nephrology / Neurology / Neuroscience / Obstetrics and Gynecology / Ophthalmology /
Orthopedics / Pathology / Pediatrics / Pharmacology / Physical Diagnosis / Physiology / Primary Care-
AMB Medicine / Psychiatry / Pulmonary / Radiology / Surgery / Toxicology / Trauma
Wright State Faculty Resources
www.med.wright.edu/fca/profdev
The Wright State School of Medicine offers extensive resources for its faculty. These resources are
organized into five categories: (1) Teaching Skills, (2) Clinical Practice, (3) Research, (4) Technical
Skills Development, and (5) Promotion. The school has four main centers that provide these resources:
the Center for Teaching and Learning, the Department of Computing and Telecommunication, the

Center for Professional Development, and University Library Services. Specific skills that can be
acquired include:
Database Network Services
Internet
PowerPoint Presentation
Spreadsheet
Computer Literature Searching
Computer Assisted Learning
Distance Learning
Multimedia Presentation
Teaching Aids (e.g., anatomical models)
Visual Aids (e.g., preparing slides)
Database creation and management
http://www.med.wright.edu/fca/promo/index.html
WSU frequently features articles relevant to faculty development.
"Advice on Preparing Your Dossier"
a) Regarding evaluation documents:
1) Keep evaluations of your teaching and scholarly activities.
2) Summarize evaluations annually to avoid calculating multiple years at the time of promotion review.
When using a Likert scale, you don’t need to calculate percentages of responses; totals are sufficient.
3) Record the number of students (or others) surveyed (i.e., n=3).
4) Include a comments section with the evaluation summary to explain the level of faculty involvement
and type of teaching.

b) Regarding letters of reference
1) Consult with your chair about obtaining letters of reference. The chair, the P&T Committee, or the
Dean’s office, not the candidate, will contact your references about writing a letter.
2) Request their letters early. Frequently, reference letters are the last pieces of the dossier to arrive.
3) Explain in your dossier file why each reference person was chosen (e.g., expert in the field).
c) Regarding publications
Indicate whether the articles are peer reviewed, using "R" for (peer) reviewed, "N" for not peer reviewed,
and "I" for invited.
From: Rx for the Top Ten Mistakes in Promotion Documents
10) Time in rank should not be compressed, even if the faculty member has been perceived as
exceptionally productive.
9) Information must be relevant to faculty member’s productivity at this institution.
8) To be complete, a promotion dossier must address and document all three categories-teaching,
research, and service.
7) Whether teaching 2 or 200, faculty must document each teaching effort and the methods they have
used to evaluate their teaching.
6) When documenting service, faculty are to name each committee, their term of service, and if
appropriate, the leadership role they performed.
5) When describing research in letters of reference, try to avoid using technical language.
4) For articles to have validity in a promotion document, they must be published or in press. Promotion

review committees will not consider articles that are submitted, or in preparation.
3) University guidelines require that teaching be documented and the documentation include student
evaluations and at least two other forms of evaluations.
2) When requesting letters of reference (from internal or external contacts) for a faculty promotion
dossier, chairs should neither state nor imply a bias for or against the candidate up for promotion.
1) Letters of recommendation-from the department’s promotion committee, and the department chair-
should give evidence of the faculty member’s credentials from their perspective rather than referring to
the other letters.
The Chair in Perspective
http://www.med.wright.edu/fca/Articles/ChairPerspect.html
An excellent article on faculty development from one of the leaders in emergency medicine, Dr.Glen
C.Hamilton.
Teaching at OSU
www.osu.edu/education/ftad
The Office of Faculty and Teaching Associate Development (FTAD) at The Ohio State University exists
to help faculty and teaching associates excel in teaching and experience the satisfaction that results
from teaching well. The site contains a listing of readings on teaching, and offers individual
consultations.
2. FACULTY DEVELOPMENT PAPERS:

Jouriles NJ, Kuhn GJ, Moorhead JC, et al: Faculty development in Emergency Medicine. Acad Emerg
Med. 1997;4:1078-1086.
In this excellent article, academic emergency physicians discuss aspects of faculty development,
including: 1) "A chair's method for developing individual faculty" (John Moorhead, MD); 2) "Traditional
promotion and tenure" (Douglas Rund, MD); 3) "Faculty development in a new department" (V. Gail
Ray, MD); and, 4) "Personal development" (Gloria Kuhn, DO). One of the many excellent points in this
article is "beginning with the end in mind". Determine what your long term goal is (long term meaning
>10 years) and "it becomes easier to decide what steps need to be taken to get there. Short term goals
are those steps."
Kuhn GJ, Krome RL: Career planning and development for emergency medicine faculty. J Emerg Med
1997;15:381-385.
The authors propose a methodology to be used by emergency medicine faculty members interested in
career planning and faculty development on an individual basis. The basic competencies needed by
faculty and methods of setting goals are described. Educational courses, workshops, seminars, and
self-study strategies to provide the basic competencies and meet defined goals are described, including
the advantages and disadvantages of each method, the time commitment, and needed resources. The
advantage of this methodology is the ability to customize a program to meet individual needs and fit into
the constraints of available time and monetary resources.
Hamilton GC: A library to assist in the development of academic faculty in emergency medicine. J
Emerg Med 1988;6:551-553.
The author defines faculty development as a training process that strives continually to improve the
creativity, productivity, and longevity of individuals committed to the practice of academic medicine.
From a more than 80-volume personal library, 15 recommended texts in 11 major topics are selected.
This library is designed to assist emergency physicians in obtaining useful sources of information as
part of their continuing education as academic faculty.
Hewson MG: A theory-based faculty development program for clinician-educators. Acad Med

2000;75:498-501.
This essay describes the development, implementation, and evaluation of a theory-based faculty
development program for physician-educators in medicine and pediatrics at The Cleveland Clinic.
Wilkerson L: Strategies for improving teaching practices: a comprehensive approach to faculty
development. Acad Med 1998;73:387-396.
This article details the four components of successful faculty development : (1) professional
development (new faculty members should be oriented to the university and to their various faculty
roles); (2) instructional development (all faculty members should have access to teaching-improvement
workshops, peer coaching, mentoring, and/or consultations); (3) leadership development (academic
programs depend upon effective leaders and well-designed curricula; these leaders should develop the
skills of scholarship to effectively evaluate and advance medical education); (4) organizational
development (empowering faculty members to excel in their roles as educators requires organizational
policies and procedures that encourage and reward teaching and continual learning).
Lemkau JP, and Ahmed SM: Helping junior faculty become published scholars. Acad Med
1999;74:1264-1267.
This article describes how faculty who are novices to publishing can get started, beginning with a
description of the types of scholarship and examples of work that fits into each category. The article also
emphasizes the importance of mentorship from senior faculty.
Rubeck RF: Faculty development: a field of dreams. Acad Med 1998;73(9 Suppl):S32-S37.
This article describes the faculty development efforts of the eight schools that participated in The Robert
Wood Johnson Foundation's "Preparing Physicians for the Future: Program in Medical Education." It
explores the faculty development topics and methods, both shared and unique, among the eight
schools. It then looks at the ways the schools motivated their faculties to participate in their programs.
Finally, it describes some of the outcome measures that were used to gauge the effectiveness of the
faculty development programs. The authors present lessons learned from the successes and failures of
the various programs.

Reid A: Assessment of faculty development program outcomes. Fam Med 1997;29:242-247.
This paper summarizes outcomes reported and methods used in published studies of faculty
development programs in Family Medicine since 1980.
Meurer LN: Published literature on faculty development programs. Fam Med 1997; 29:248-250.
Published faculty development program evaluation articles often leave the program description
incomplete, making it difficult for new program planners to build on previous work. The authors
examined faculty development literature for the inclusion of important program elements. They found
that many important program components, including local needs assessment, leadership and resource
support, stakeholder input, implementation barriers, participant attendance, and cost were each
discussed in fewer than 30% of published articles. The context, input, process, and product framework
is proposed as a guiding model for future program reports.
Ullian JA: Types of faculty development programs. Fam Med. 1997;29:237-241.
This paper offers an overview of faculty development program types, with references to specific
programs described in the recent literature. Faculty development programs have been categorized in a
number of ways. This review uses a variation of those typologies and suggests six types of faculty
development activities: 1) organizational strategies, 2) fellowships, 3) comprehensive local programs, 4)
workshops and seminars, 5) continuing medical education, and 6) individual activities. While these
categories provide a conceptual basis for distinguishing among programs, actual programs in use often
contain elements of more than one type.
Skeff KM: Clinical teaching improvement: past and future for faculty development. Fam Med
1997;29:252-257.
This article discusses 1) the rationale for providing faculty development for clinical teachers, 2) the
competencies needed by clinical teachers, 3) the available programs to assist faculty to master those
competencies, and 4) the evaluation methods that have been used to assess these programs.

Hitchcock MA: Faculty development in the health professions: conclusions and recommendations. Med
Teach 1992;14:295-309.
This report summarizes recent literature reviews and resource books on faculty development. Nine
conclusions about faculty development in the health professions are drawn: (1)the concept of faculty
development is evolving and expanding; (2) research skills are becoming a major focus of faculty
development; (3) teaching skills are still a prominent aspect of faculty development; (4) fellowships are
being used effectively to recruit and train new faculty; (5) the institutional environment has become a
focus of faculty development; (6) faculty evaluation is an effective approach to faculty development; (7)
the efficacy of faculty development needs better research documentation; (8) model curricula have been
developed for different types of faculty; and (9) comprehensive faculty development centers are gaining
in popularity. A set of recommendations based on the conclusions drawn is offered for those planning
faculty development interventions.
Rose EA, Roth LM, Werner PT, Keshwani A, Vallabhaneni V: Using faculty development to solve a
problem of evaluation and management coding: a case study. Acad Med 2000;75:331-336.
The authors used the need to implement CMS (formerly HCFA) regulations as a way to create a faculty
development program. They describe their curriculum, which includes: (1) coding theory; (2) chart
auditing for coding; (3) teams and team building; (4) effective meetings; and (5) structured problem
solving. Following the implementation of their initiative, they found fewer medical coding errors, but also
an improved sense of ability amongst the faculty.
Bennett NL, Davis DA, Easterling WE, et al: Continuing medical education: a new vision of the
professional development of physicians. Acad Med 2001;75:1167-1172.
The authors describe their vision of what continuing medical education (CME) should become in the
changing health care environment. They first discuss six types of literature (e.g., concerning learning
and adult development principles, problem-based/practice-based learning, and other topics) that
contribute to ways of thinking about and understanding CME. They then state their view that the
Association of American Medical Colleges (AAMC) has made a commitment to helping CME be more
effective in the professional development of physicians.

Evans CH: Faculty development in a changing academic environment. Acad Med 1995;70:14-20.
The author outlines a new model of faculty development, explaining that the traditional model of faculty
development is obsolete in the face of shrinking government support, changes in the sophistication,
costs, funding of biomedical research, changes in the reimbursement systems for hospitals and
physicians, a general loss of respect for the medical and scientific professions, and radical changes in
the structure of the health care delivery system.
Bland CJ, Schmitz CC: A guide to the literature on faculty development. In Jack H. Schuster, Daniel W.
Wheller, eds. Enhancing Faculty Careers: Strategies for Development and Renewal. San Francisco:
Jossey-Bass Publisher, 1990 (pp. 298-328).
Bland CJ, Schmitz CC, Stritter FT, et al: Successful Faculty in Academic Medicine: Essential Skills and
How to Acquire Them. New York: Springer Publishing Co., 1990.
Pereira J, Peden J, Campbell K: Instructional technology in medical education: lessons learnt. J
Telemedicine & Telecare 2000;Suppl 2:S56-S58.
New instructional technologies, especially Web-based applications, may play an increasing role in
medical education, particularly for distance and distributed learning. As medical educators turn to this
medium, numerous benefits and opportunities, as well as challenges and pitfalls, will arise. The
successful development and implementation of instructional technologies in medicine require an
appreciation of the medium's heterogeneous nature, its strengths, weaknesses, and limitations. These
in turn rely on partnerships with various experts and the early adoption of evaluation. We have
summarized the lessons learnt from developing Web-based courses on palliative care in a framework
for adopting instructional technologies. This framework incorporates development, implementation, and
evaluation.
Roop SA. Pangaro L: Effect of clinical teaching on student performance during a medicine clerkship. Am
J Med 2001;110:205-209.
PURPOSE: To measure what proportion of student clerkship performance can be attributed to teachers'
educational skills as reported by students. SUBJECTS AND METHODS: From August 1992 to June

1994, we collected critiques of teacher skills from 314 third-year students at the end of a 12-week
medicine clerkship. Interns, residents, attending physicians, and student preceptors were rated (on a 1
to 5 scale) on teaching behaviors from the 7 categories of the Stanford Faculty Development Program
framework. A linear regression model was used to determine the relative contributions of the rated
teaching behaviors in predicting final student performance and improvement across the clerkship
("student growth"), measured using end-of-clerkship variables (clinical grades, National Board of
Medical Examiners medicine shelf examination, practical laboratory examination, and an analytical
essay examination) and preclerkship variables (pre-third-year grade point average [GPA], United States
Medical Licensing Examination, Step I, and clerkship pretest). RESULTS: Data were available for 293
(93%) of 314 students, who completed a total of 2,817 critiques. The students' preclerkship GPA
accounted for the greatest percentage of variance in student performance (28%). Clinical teaching
behaviors accounted for an additional 6% of the variance. For student growth across the clerkship,
teaching accounted for 10% of the variance. Among the 7 Stanford educational categories, teaching
behaviors promoting control of session (r2=5%) and fostering understanding and retention (r2=4%) had
the greatest effect. The resident had the most effect on student growth (r2=6%) when compared with
other teaching levels. Teaching had a greater effect on growth for students with preclerkship GPA above
the mean (16% versus 6%), for older students (24% versus 7%), and for students with a nonscience
undergraduate degree (33% versus 9%). CONCLUSION: The preclerkship GPA, reflecting 2 years of
work, was the most important predictor of student performance. Teaching behavior, as measured by
student assessments, also affected student performance.
Wear D: Asian/Pacific Islander women in medical education: personal and professional challenges.
Teaching & Learning in Medicine 2000;12:156-163.
The purpose of this qualitative study was to identify the complex issues facing Asian/Pacific Islander
(API) women students at one Midwestern medical school as they subjectively experience their medical
training. Of particular interest was how students navigated family influences, career planning, and ethnic
and gender stereotypes. Sixty-five percent of the students reported that their parents exerted various
degrees of encouragement or pressure to enter medicine. The remaining students said that the decision
was entirely theirs (20%) or that the decision had been made for them (15%). Many reported the larger
Asian "community" as a source of influence. A slight majority of students thought they were perceived by
faculty as being "quiet," often too quiet. With only 1 exception, all of the students believed that their
cultural identity influenced their specialty choice. Stressors reported by students centered on

competition, achievement, and formation of intimate relationships (i.e., dating). The authors conclude
that medical educators who provide personal and professional support for API women students should
be keenly aware of the career, gender, and family issues that emerge at the intersection of API and
Euro-American cultures. Faculty development should include an educational component on issues of
concern to API students, men and women. Faculty also need to wrestle with the cultural values of
"modesty, respect for authority, public self-consciousness, and other directness" as they intersect with
assertion as a primary value found in Euro-American culture in general and in medical education in
particular.
Rider EA, Federman DD, Hafler JP: Residents as teachers--a faculty development approach to
programme development. Medical Education 2000;34:955-956.
The authors present a strategy for residency faculty development in women's health, the reasons such a
strategy is necessary (e.g., women's health encompasses much more than reproductive and disease
issues, and is cross-disciplinary and intrinsic to all of family practice), and their residency program's
experience with its development and implementation from 1994 to the present. In creating the program,
the residency program's faculty used as a context some lessons learned from family medicine, since the
rapid growth of family medicine provides a historical example of dealing with a critical shortage of faculty
for new residency programs and the need for a new way to train educators. Also, the faculty reviewed
the literature about faculty development in medicine, models of teaching and learning from women's
studies, and group theory, specifically the skills concerning conflict and diversity. They used the salient
elements from each (which the authors outline) in fashioning their new faculty development program.
The resulting program also grew out of focus groups with patients, input from staff, residents, and
faculty, and meetings and workshops, including some intense and highly charged discussions in which
the faculty participants, both men and women, confronted their own views and biases and worked hard
to successfully forge a common and relevant vision of women's health.
Orlander JD: Co-teaching: a faculty development strategy. Med Educ 2000;34:257-265.
This paper describes a model in which paired physicians focus on developing their teaching skills while
sharing the clinical supervision of residents and medical students. Vignettes, taken from the experiences
of the authors, are used to demonstrate how the model is used to develop effective solutions to
problems and to help in the maturation of one's skill as an educator.

Bazarian JJ, Davis CO, Spillane LL, et al: Teaching emergency medicine residents evidence-based
critical appraisal skills: a controlled trial. Ann Emerg Med 1999;34:148-154.
The objective of this trial was to compare the performance of an evidence-based medicine (EBM)
approach and a traditional approach to teaching critical appraisal skills to emergency medicine
residents. The authors found that compared with a traditional approach, an EBM approach to teaching
critical appraisal did not appear to improve the critical appraisal skills of emergency medicine residents.
However, the trial enrolled only 32 residents.
Johnson CE: Developing residents as teachers: process and content. Pediatrics 1996;97(6 Pt 1):907-
16.
This article is a review of the 3-year experience with the teaching program implemented for the pediatric
residency program at Harvard Medical School--from conceptualization to realization to evaluation-- and
provides one model for others to use in developing a curriculum on teaching.
Hafler JP, Lovejoy FH: Scholarly activities recorded in the portfolios of teacher-clinician faculty. Acad
Med 2000;75:649-652.
The purpose of this article was to explore what contributions to scholarship teacher-clinician faculty list
in the portfolios that they use as evidence for promotion. While the faculty members' portfolios continue
to emphasize original articles as evidence of scholarship (and those mostly in their medical
subspecialties, and less in education), new forms of evidence, such as teaching materials, chapters in
textbooks, syllabi, computer programs, and videotapes, have emerged. Faculty members are also
recording their participation in broad-based teaching activities; their leadership roles for student,
resident, fellow, and continuing medical education levels; and their educational leadership positions
locally, regionally, and nationally on committees that enhance the educational enterprise. This article
nicely compares the number of such achievements reported by assistant, associate and full professors.
Seldin P: The Teaching Portfolio. A practical guide to improved performance and promotion/tenure
decisions. 2nd ed. Bolton, MA: Anker Publishing Company Inc. 1997.
Simpson D, Beecher A, Lindemann J. The Educator's Portfolio. 4th ed. Milwaukee, WI: Medical College
of Wisconsin; 1998.
3. PROMOTION AND TENURE
http://www.dml.georgetown.edu/schmed/faculty/guidelines.html
The appointment, promotion and tenure guidelines for the Georgetown University School of Medicine,
including the non-tenure tracks of Clinician-Educator and Full-time Clinician as well as the tenure tracks
of Research. There are also criteria for Part-time Paid, or Voluntary Faculty.
http://www.aamc.org/about/progemph/access/sum25nod.htm
This link, also referenced above, is to an excellent article entitled "Summary Findings - Changes in
Faculty Promotion Guidelines to Recognize Teaching Effort and Quality". In it, the author discusses the
challenges of academic promotion and the recognition of teaching as a means of attaining promotion.
http://its.hsc.missouri.edu/~medicine/byfapt.shtml
This link to the University of Missouri-Columbia School of medicine’s Faculty Appointment, Promotion
and Tenure Committee covers the requirements for attaining the different professorial ranks. The criteria
are divided into the three categories of teaching, research/creative work/scholarly endeavor, and
service/administration.
http://inside.gwumc.edu/edu/policy/senate/Document/CRITERIA89.htm
Criteria for Promotion and Tenure for the Faculty of the School of Medicine and Health Sciences at the
George Washington University.
http://info.med.yale.edu/faculty/appendixc.htm
Curriculum vitae format for appointment or promotion at the Yale University school of medicine

http://biomed.brown.edu/Medicine/Administration/OMFA/handbk/cvform.html
Recommended CV format for faculty at the Brown University School of Medicine

Afterword
Triple-threat or Double-fake? The Dilemma of Academic Medicine in the 21st
Century
Author: Latha Stead
The term triple-threat is attributed to an anonymous sportswriter, who used it to describe the gridiron
talents of one Paddy Driscoll, a quarterback for the Chicago Cardinals, the oldest franchise in
professional football. Driscoll, who played both offense and defense, not only passed and ran with equal
facility, but on a particularly memorable fall day in 1924, successfully drop-kicked a field goal from the
50 yard-line. One does not have to be much of a football fan to know that, as the game has evolved and
become increasingly specialized, no single individual would be expected to perform all three tasks of
passing, running, and kicking at a professional level. Hence, with the passage of time, the original
meaning of the term triple-threat has become obsolete.
The analog of the triple-threat in football is baseball's Triple Crown, awarded to the player leading his
league in homers, batting average, and runs batted in (RBI's). No one has won the Triple Crown since
the 60's, and many serious observers of the national pastime believe such a feat to be so deeply
improbable that it effectively rivals the impossibility of achieving triple-threat status in the NFL.
It is tempting to conclude from the foregoing that the athletes of today are somehow made of lesser stuff
than those of earlier generations. However, other data, such as the shattering of Babe Ruth's home run
record - which had stood for more than 70 years - twice in the last half decade, belies such an assertion
as a unifying hypothesis. Indeed, the weight of evidence supports the contention that there may never
again be a Triple Crown winner, not so much because players cannot hit the ball, but rather because
they have become specialists. Thus the great hitters of recent years are either swinging for the fences,
or consistently hitting safely, but not both - and without both, the triple crown cannot be won. Baseball
still contains extraordinary hitters, as good as the Cobbs, Hornsbys, Mantles, Ruths, and Williams of the
past. Similarly in football, the Clarks, Driscolls, Hubbards, Hutsons, and Tarkentons are still out there,
even though it is no longer possible to be a triple-threat. This is because, over time, both sports have
evolved and undergone deep and fundamental changes.
In academic medicine, the game has also changed in equally deep and fundamental ways. Shortly after

the second World War, and continuing for several decades thereafter, those academic medical faculty
held up to students and house officers as role models were commonly described as "triple-threats", i.e.,
independently funded investigators, inspiring teachers, and stellar clinicians. In recent years, such
individuals have become very nearly as extinct as bird's teeth. Although extinction is among the most
natural of biological phenomena, when a highly venerated species becomes endangered because the
cultural ecosystem that once supported it can no longer be sustained in an altered intellectual climate,
there is a natural inclination to try and preserve the dying breed. Nowhere is such behavior more evident
than in academic medicine, where the triple-threat seems to have attained the unique fictional status
ordinarily reserved for myth.
Mythology, Joseph Campbell tells us, builds upon the truths and ideals of an earlier time. Viewed as
metaphor, myth is entertaining and often profoundly revealing. However, taken literally, it provokes a
kind of naive nostalgia that holds the present hostage to a selectively remembered past. This latter
condition approximates the dilemma of academic medicine currently and for the last several decades.
The consequence of any attempt, no matter how earnest, to become a triple-threat in the 21st century
seems more likely than not to result in the hollow grandiosity of a double-fake. Although the etymology
of the term double-fake is more elusive than that of triple-threat, its meaning is clear. When used in
reference to an individual, the term describes one who is not what they purport, or might otherwise
appear, to be.
To maintain even a modicum of clinical expertise in caring for the nearly infinite variety of ED patients
presenting with undifferentiated illness requires constant vigilance and frequent exposure to minimize
skill decay. The challenge of supervising residents and teaching students requires additional levels of
understanding and the ability to reduce mountains of clinical complexity to molehills of clarity. Add to
that, the demands of basic or clinical extramurally funded research, and one is not only committed to a
minimum of roughly 80-100 hours per week - essentially guaranteeing the absence of any semblance of
a sustainable personal life - but is also looking down the barrel of a future that holds a likelihood of
success only marginally better than the probability of winning the Triple Crown in the American League
or becoming a triple-threat in the NFL.
Perhaps the unarticulated expectation that an individual, given sufficient talent, intelligence, and drive
should somehow be able to do it all in 2002 - as was possible 50 years ago, at a time when one might
actually have been a triple threat in academic medicine (or a Triple Crown winner in baseball) - is one of

the reasons why so many of our most talented young physicians leave residency, turn away from
academics, and enter directly into the private sector. Certainly, the enormous debt service medical
students now carry upon graduation - likened by some to the mortgage on a first home, absent the
house - plays a role in driving such a decision. Nevertheless, the dim prospects of job satisfaction,
working under a set of expectations that become increasingly difficult with each passing year, must also
figure somehow in the choice to forego an academic career.
Based on all of the preceding, we would strongly encourage young faculty to choose carefully, to 'play to
their strengths,’ and to focus their interests as narrowly as possible either on teaching and clinical care
or upon research as an area of primary concentration. Because clinical expertise often goes hand in
glove with clinical teaching, combining these two skills in the role of the clinician-educator is quite
common, and not at all unrealistic. Nor is it difficult to imagine an investigator who is also an outstanding
teacher within the circumference of that individual's research interests. However, to expect independent
investigators - who need at least 75% of their time protected from clinical responsibilities if they are to
make meaningful contributions, obtain independent extramural funding, and avoid becoming "hobbyists"
- to perform at the same level of clinical expertise as faculty colleagues who see patients daily, is a
prescription for feelings of inadequacy and burnout.
Coming to terms with the realization that virtually no one can any longer juggle all three academic balls
with equal agility for the duration of a career - is the first step toward moving beyond the myth of the
triple-threat. Then perhaps, academic physicians can establish for themselves more sensible
expectations and standards to which they can reasonably be held.
This is not to suggest that those engaged in the scholarship of teaching should never involve
themselves in the scholarship of application, nor that scholars of discovery should never set foot in the
clinical arena. Rather, each group must recognize the very substantial limits imposed on meaningful
expertise in any area by dint of the way in which the game of academic medicine has been transformed
over the last half century. Clinicians must limit their research activities to goals appropriate to their
knowledge, training, and experience. This means asking early and often for help from their colleagues in
the traditional academic (tenure) track, and taking care not to tackle unreasonably large or complex
questions. There are many forms of academic writing that are appropriate for the clinician-educator;
however, few clinician-educators should harbor expectations of obtaining RO1 funding. Likewise,
successful investigators in the traditional tracks should see patients, but with the requisite humility and

respect for the extraordinary clinical challenges of Emergency Medicine, lest they unwittingly do harm.
They too should seek the frequent consultation of their clinical counterparts within the department who
care for patients regularly - just as the latter ought to seek guidance when circumstances are reversed.
It is the reciprocal relationships among faculty as a group, fueled by mutual self-respect and a realistic,
open appraisal of individual strengths and limitations, that drives the machinery of a successful
academic department. The chair must take the responsibility for the choreography required to balance
such a delicate ecosystem, in order that the department as a single, integrated, interdependent entity -
rather than each of the individual faculty comprising that whole - becomes a triple threat.
Thus, we end the first edition of this Handbook on Faculty Development on a cautionary note. Either we
must soften the unrealistic expectations we have placed upon ourselves in the past, or risk driving some
very talented young people away from academic medicine. It is critically important that junior faculty
focus as single-mindedly as possible on an achievable goal, without regard for the lingering and slightly
pernicious mythology of the triple threat. If this can be accomplished - difficult as it may be to let go of
longstanding, cherished illusions - young faculty will at least be given an opportunity to rediscover the
enormous personal rewards and intellectual satisfaction that a career in academic medicine can
provide.