
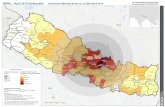
Factors Associated with ART Non-adherence in Rural Achham, Nepal
36
Achieving Millennium Development Goals Through Universal Access Factors Associated with ART Non-adherence in Rural Achham, Nepal Dr. B Organiza tion logo Organiza tion logo Dr. Bibhusan Basnet ,MBBS Nyaya Health Nepal , Bayalpata Hospital Badelgada-2, Achham
-
Upload
bibhusan-basnet -
Category
Health & Medicine
-
view
421 -
download
1
Transcript of Factors Associated with ART Non-adherence in Rural Achham, Nepal

Achieving Millennium Development Goals Through Universal Access
Factors Associated with ART Non-adherence in Rural Achham, Nepal
Dr. B
Organization logo
Organization logo
Dr. Bibhusan Basnet ,MBBS Nyaya Health Nepal , Bayalpata HospitalBadelgada-2, Achham

www.nepalaids2012.org.np
Introduction
Background• Worldwide: 40.3 million (WHO 2005)
• Asia: 4.7 million, of which newly infected/year :350,000 (WHO 2008)
• Situation in Nepal: 50,200 (UNAIDS/NCASC 2012)
• Far west accounts for 16% of total HIV infections (UNAIDS 2005)
• For successful treatment , medication adherence for patients on ART is critical. (Sethi et al.2003)

www.nepalaids2012.org.np
Statement of the problem
• ART is the cornerstone of treatment for HIV and AIDS.
• Non-adherence is a major, if not the most important factor contributing to treatment failure and development of resistance(Turner 2002)

www.nepalaids2012.org.np
Rationale / Justification
• Adherence is essential for successful treatment and sustained viral control( Carter 2005)
• Failure to ART increases risk of transmission of resistant viruses.
• Limited future treatment options due to poor adherence makes adherence a public health concern .
• Bayalpata hospital operating in far west Accham has recently been upgraded to an ART center.
• The following study was devised as an asset for quality improvement, thus enhancing the impact of ART services

www.nepalaids2012.org.np
Objectives
General •To evaluate the adherence to ART.•To determine the factors associated with ART adherence
Specific1. To determine the adherence rate
2. To determine facilitating factors and barrier to adherence
3. To assess the Karnofsky performance scale of the patient

www.nepalaids2012.org.np
Research Design and Methodology
• Cross-sectional quantitative study carried out over a 8 weeks period
• Sampling technique: Convenient sampling
• Sample size: 105 patients, attending the Out patient clinic of the hospital.
• Inclusion criteria: Patients <18 years and who have been on ART for at least 6 months.

www.nepalaids2012.org.np
Study Site : Bayalpata Hospital, Achham.

www.nepalaids2012.org.np
Data collection:
•Data collection was done using structured questionnaire on the following variables:
• Socio-economic demographics • Adherence rate • Facilitating factors and barriers associated with adherence • Health system factors • Coping strategy

www.nepalaids2012.org.np
Data Collection Tools:•Visual Analog scale(VAS) was similar to pain evaluation used for assessing adherence. (Walsh et al.2002 ,Giordano et al.2004)
• Score of 10 was considered as to never missed any medication in the last 4 weeks. i.e absolute adherence
•≤9 for missed medications in the last month.
•Any answer different from 10 was considered to represent non adherence.

www.nepalaids2012.org.np
Data Collection Tools Continued:
•Karnofsky Performance Scale was used.
• Assess a patient's performance on a regular basis, especially as the effects of HIV progress.
•Karnofsky scores over time allows patients to be classified as to their functional impairment(EM Painline 2012)
•Lower the Karonfsky score, the worse the survival for most serious illness such as HIV/AIDS.

www.nepalaids2012.org.np
Ethical Consideration
• The research received approval from NHRC.
• Verbal informed consent was taken from each study participant.
• Questionnaire was accessed by only the researcher, thus maintaining
the confidentiality of the participants.

www.nepalaids2012.org.np
Research Findings

www.nepalaids2012.org.np
Socio Demographics•Among the respondents,37 were males and 68 females.•56.2% of the patients surveyed were married, while the remainder were widowed (43.8%).•65.7% of the patients led a nuclear family or a joint family (30.5%).•Median number of dependents was found to be 3.
Married Widowed0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
56.2%
43.8%
Marital Status of patients
Nuclear Joint Living alone0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0% 65.7%
30.5%
3.8%
Type of family

www.nepalaids2012.org.np
Socio Demographics
•Majority of patients were either of the Dalit (51.4%) or chhettri(44.8%) castes.•78.1% of the respondents had farming as their most common occupation followed by shopkeeper (6.7%) and housewife (5.7%).
Brahmin Chhetri Vaishya Dalit0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
2.9%
44.8%
1.0%
51.4%
Caste
Farming Housewife Shopkeeper Teacher Laborer Other0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%Occupation

www.nepalaids2012.org.np
Socio Demographics:
• 82.9% were on first-line WHO regimen or a substituted first line regimen (17.1%).
• Median individual monthly income: NRs 2000 (range 300-10000)• Median family expenditure/year :NRs 20000 (3000-150000)

www.nepalaids2012.org.np
Socio Demographics
• Educational attainment was low with 70.5% indicating they could not read or write
Cannot read or write
Read, but cannot write
Primary school
SLC High school University0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%Education

www.nepalaids2012.org.np
Adherence
•With respect to measures of adherence 90 (85.7%) reported a VAS of 10 and 15 (14.3%) gave a score <10.
• Rates of missed doses in the past week were 6.7%, 15.2% in the past month and 25% in the past 6 months.
•Of those reporting a missed dose in the past month
70.6% missed less than 3 doses
17.6% 3 to 12 doses
11.8% more than 12 doses

www.nepalaids2012.org.np
Adherence rate by VAS<10 (n=15)
n OR 95% CI p-value
Any medication side-effects 12 1.71 0.45-6.6 0.5466
Field work or family
obligations8 32.40 6.98-150.2 <0.0001
Travel by both bus and on
foot6 4.79 1.42-16.1 0.0152
Depressed mood past month 7 3.07 1.00-9.36 0.0567
Literacy 14 4.53 0.56-36.4 0.1815Living alone 2 6.77 0.88-52.3 0.0968
Help at home 7 0.38 0.12-1.14 0.1362
Socioculture factors 5 4.50 1.26-16.1 0.0279
Time waiting, spent at clinic
or timing of ART clinic12 3.66 0.97-23.6 0.0527
Opportunistic infection last 6
months6 2.19 0.70-6.87 0.205
Coping mechanisms 8 0.76 0.25-2.23 0.778
VAS score <10 (n=15)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Factors associated with poor ad-herence
VAS Score <10 (n = 15)

www.nepalaids2012.org.np
Adherence by missed dose in last 1 week
n OR 95% CI p-value
Any medication side-effects 5 1 0.18-5.46 1
Field work or family obligations
5 27.5 4.58-165.1 0.0003
Travel by both bus and on foot
4 8.72 1.75-43.5 0.0125
Depressed mood past month4 3.69 0.77-17.6 0.1007
Literacy 6 1.58 0.18-13.9 1Living alone 1 5.28 0.48-58.7 0.2443
Help at home 3 0.35 0.07-1.65 0.2183
Sociocultural factors 2 2.87 0.50-16.5 0.2343
Time waiting, spent at clinic or timing of ART clinic
5 1.88 0.35-10.1 0.6963
Opportunistic infection last 6 months
3 2.31 0.48-11.1 0.37
Coping mechanisms 2 0.25 0.05-1.37 0.1196
Missed dose in last week (n=7)
0%
20%
40%
60%
80%
100%
Factors associated with poor ad-herence (n = 7)

www.nepalaids2012.org.np
Adherence by missed dose in last 1 month
n OR 95% CI p-value
Any medication side-effects 12 1.24 0.37-4.20 0.7771
Field work or family obligations
9 17.4 4.78-63.0 <0.0001
Travel by both bus and on foot
6 4.26 1.29-14.0 0.0219
Depressed mood past month 7 2.23 0.75-6.68 0.227
Literacy 15 4.93 0.62-39.5 0.1162Living alone 2 6.21 080-47.8 0.1091Help at home 7 0.32 0.11-0.95 0.0455Sociocultural factors 7 9.11 2.6-31.9 0.001
Time waiting, spent at clinic or timing of ART clinic
12 2.45 0.73-8.18 0.1739
Opportunistic infection last 6 months
7 2.68 0.89-8.11 0.1163
Coping mechanisms 9 2.08 0.71-6.1 0.269
Missed dose in last month (n=16)
0%
20%
40%
60%
80%
100%
Factors associated with poor ad-herence(n=16)

www.nepalaids2012.org.np
Adherence by missed dose in last 6 months
n OR 95% CI p-value
Any medication side-effects 19 1.12 0.41-3.01 1
Field work or family obligations
11 56.5 6.77-470 <0.0001
Travel by both bus and on foot
7 2.83 0.93-8.58 0.112
Depressed mood past month13 3.59 1.40-9.17 0.0112
Literacy 24 4.42 0.96-20.4 0.055Living alone 2 3.17 0.42-23.7 0.57Help at home 14 0.49 0.20-1.21 0.1516Socioculture factors 8 5.33 1.64-17.3 0.006
Time waiting, spent at clinic or timing of ART clinic
19 2.45 0.93-6.49 0.1089
Opportunistic infection last 6 months
10 2.42 0.93-6.34 0.1143
Coping mechanisms 13 0.63 0.26-1.53 0.3602
Missed dose in last 6 months (n=26)
0%
20%
40%
60%
80%
100%
Factors associated with poor adherence(n = 26)

www.nepalaids2012.org.np
Karnofsky Performance Scale
•Respondents were relatively asymptomatic
•34.3% (score of 100)- Normal; no complaints; no evidence of disease
•30.5%(score of 90)- Able to carry on normal activity; minor signs or symptoms of disease
•24.8%(score of 80)-Normal activity with effort; some signs or symptoms of disease
•only 4 patients required considerable assistance or disability related to the HIV disease
•Non significant with respect to adherence.

www.nepalaids2012.org.np
Socio Cultural Factors
•Socio-cultural factors and alternative treatments besides ART as a factor for non adherence were uncommon with only 13.3% and 14.3%, respectively.•Though uncommon, it was found to be a significant factor associated with non adherence:
VAS Score <10 (p=0.0279)
missed dose in the last month (p=0.001)
missed dose in the last 6 months (p=0.006)
Stigma and discrimination
to oneself
Fear of disclosure of status in the
community
Fear of stigma in the family
Fear of stigma in the workplace
None0.0%
10.0%20.0%30.0%40.0%50.0%60.0%70.0%80.0%90.0%
100.0%
8.6% 2.9% 1.9% 1.9%
86.7%

www.nepalaids2012.org.np
Individual Factors
Note: No statistical significance found with non- adherence
dizziness vomiting headache fever rash diarrohea candidiasis TB vaginal discharge
0%
20%
40% Individual Factors
Most common side effects Most common opporutnistic infections

www.nepalaids2012.org.np
Individual factors
•98.1% of those surveyed stated their family was aware of their HIV status.•Spouses of nearly all subjects (104/105) were aware of their HIV status (63.8%) or deceased (35.2%).•Seventy-two subjects reported use of electronic reminders.
Watch Clock Mobile Radio None0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%51.9%
10.6%
2.9% 2.9%
31.7%
Use of electronic reminders

www.nepalaids2012.org.np
Hospital Based Factors
•Twenty-five of 105 respondents (23.8%) indicated distance was a reason for non adherence.
•97.1% of the respondents reported sufficient counseling provided.
Time spent waiting to see a clinician
Time spent at the hospital and
Timing of the ART clinic0%
5%
10%
15%
20%
25%21.9%
20.0%
15.2%
Hospital based non adherent factors

www.nepalaids2012.org.np
Hospital Based Factors
•Median amount of travel time required to get to clinic was 3 hours•17 persons reported required travel both by foot and bus.•Most reported travelling by foot (73.3%) compared to travel by bus (10.5%)
•Travel by both foot and bus were significant for:
VAS of <10 (p=0.0152)
missed dose in the last week(p=0.0125)
missed dose in the last month(p=0.0219)

www.nepalaids2012.org.np
Trend towards significance:
A trend toward significance was observed for:
• VAS score and depressed mood in the past month(p=0.0567)
• VAS score and time waiting for physician/time spent at hospital/timing of ART clinic (p=0.0527)
• Missed dose in the last 6 months and literacy (p=0.055)
• Median values for monthly and yearly income was not found to be significant

www.nepalaids2012.org.np
Limitations of the study:
• The study could not be generalized. • Cross-sectional design, which correlated unique time frames of
adherence.• Recall bias• Patient’s viral load as well as CD4 count is not included in the study
secondary to unavailability of this data.

www.nepalaids2012.org.np
Conclusion
• The correlation between the four assessments of adherence was high.
• Rates of missed doses in the past week were 6.7%, 15.2% in the past
month and 25% in the past 6 months.
• Among those with a missed dose in the past month, most were less than 3 doses.
• Factors consistently associated with non-adherence across all methods of adherence were the presence of field work or family obligations.
• The presence of socio-cultural factors affecting adherence and travel by both foot and bus were significant for 3 out of 4 measures of adherence.

www.nepalaids2012.org.np
Conclusion
•Despite the availability of free ART services, accompanied by counseling, patient adherence is still an issue.
•There are individual, socio-cultural and health system factors that all influence how successful treatment of HIV with ARVs will be.
• Addressing these issues by creating a more collaborative relationship between the patient and the health care provider may be the key to achieving a 100% adherence rate.

www.nepalaids2012.org.np
Recommendations
• Timing of the ART clinic should be made more flexible.•Electronic reminders as watches was seen to be used extensively. So, could be promoted by the government.•Socio cultural factors related to stigma have been changing , yet is a factor related to non adherence.•Distance is seen as one of the major barriers so decentralization of ART centers should be increased.

www.nepalaids2012.org.np
References
•Carter, M (2005). Adherence Information series for HIV positive people. NAM. Available from: http://www.aidsmap.com [Accessed 15/5/2012]
•Emergency medicine painline (2012)Available from:http://www.empainline.org/linked_site_content/pdf/KarnofskyPerformanceStatusScale.pdf [Accessed 13/8/2012]
•Giordano ,TP, Guzman, D, Clark, R et al.(2004) Measuring adherence to antiretroviral therapy in a diverse population using a visual analogue scale,HIV Clin Trials, vol. 5,no.2,pp.74-79
•National Centre for AIDS and STD Control (2009). Cumulative HIV/AIDS situation of Nepal. Monthly Report on HIV/AIDS Statistics. Kathmandu.

www.nepalaids2012.org.np
References
•National Centre for AIDS and STD Control (2010). HIV Treatment and Care (Anti-Retroviral Therapy - ART) Centers, 2010. Available from:http://www.ncasc.gov.np/uploaded/SDP/ART_Sites_in_Nepal_2010.pdf [Accessed 15/5/2012] •Sethi, AK, Celentano, DD, Gange ,SJ, Moore, RD, Gallant, JE et al.(2003) Association between adherence to antiretroviral therapy and human immunodeficiency virus drug resistance. Clin Infect Dis vol.37,no.(8),pp.1112-8. •Turner, BJ (2002) .Adherence to antiretroviral therapy by HIV-infected patients. Journal of Infectious Disease, vol.185, no. 2, pp. 143-51. •outcome. AIDS Care, vol.16, pp. 269–277

www.nepalaids2012.org.np
References
•United Nations Program on HIV/AIDS /National Centre for AIDS and STD Control(2012).Nepal country progress report ,2012.Available from: http://www.unaids.org/en/dataanalysis/knowyourresponse/countryp
•Walsh, JC, Mandalia, S, Gazzard BG (2002) Responses to a 1 month self-report on adherence to antiretroviral therapy are consistent with electronic data and virological treatment

www.nepalaids2012.org.np
THANKYOU!!!

![a' g]kfn efule} s ;dfh{ - Nepal Geological Society...Landslide disaster of Balyalta village, Achham district Birendra Piya and S. P. Manandhar..... 40 ABSTRACTS OF PAPERS PRESENTED](https://static.fdocuments.us/doc/165x107/5f1f8e532712f40eff47b4c5/a-gkfn-efule-s-dfh-nepal-geological-society-landslide-disaster-of-balyalta.jpg)














![a' g]kfn efule} s ;dfh{ - Nepal Geological Society › demo › wp-content › uploads › 2019 › 02 › Vol...Landslide disaster of Balyalta village, Achham district Birendra Piya](https://static.fdocuments.us/doc/165x107/5f1f9017f1ae3d6f59519d82/a-gkfn-efule-s-dfh-nepal-geological-society-a-demo-a-wp-content-a-uploads.jpg)